Post-Operative Pain Control1
Note
This lecture focuses on the principles and practical strategies for managing a patient’s pain after dental treatment has been completed, building upon the concepts of managing pain during treatment.
Managing Dental Pain: The 3-D’s
- Diagnosis
- Dental Treatment
- *Drugs
The 3 D's Explained
- Diagnosis: A thorough process involving history taking, clinical examination, and special tests to arrive at an accurate diagnosis. This is the foundation for all subsequent steps.
- Dental Treatment: Performing the correct dental procedure based on the diagnosis to address the source of the pain.
- Drugs: The use of medication to manage any residual or post-operative pain. If the first two D’s are performed well, the need for powerful drugs is often reduced.
The 3 D’s - Principles for Managing Dental Pain2
① Diagnosis (Image: Clinical photos and radiograph illustrating diagnostic procedures)
② Dental Treatment (Image: Clinical photos showing dental treatment procedures)
Pain Relief after Dental Treatment3
Note
Even with a correct diagnosis and well-executed treatment, patients may still experience post-operative pain.
- A study on patients given a placebo after appropriate dental treatment showed that while pain levels drop dramatically (especially for those with severe pre-operative pain), they do not fall to zero immediately.
- Pain can take several days to resolve completely.
- In cases of mild to moderate pre-operative pain, there can be a temporary increase in post-operative pain before it begins to taper off.
Study: Hargreaves & Baumgartner - 2006
Study Conclusion
This data underscores that some level of post-operative pain is expected, making post-op drugs necessary
The 3 D’s - Principles for Managing Dental Pain2
- Diagnosis
- Dental Treatment
- Drugs
If these former two are done correctly, then drugs are very rarely needed
Managing Dental & Oral Pain with Drugs / Medication
- Local
- Systemic
Local Medication4
-
Local Anaesthetic
- Effective intra-operative anaesthesia helps to reduce post-operative pain
- Can use long-acting LA
- e.g. Bupivacaine + adrenaline (Marcaine)
-
Topical
- Mouthwashes, creams, gels, ointments
- After surgery, trauma, etc.
- Mouthwashes, creams, gels, ointments
-
Intra-dental
- Pastes → Intra-canal
- Cements → On dentine
-
Materials like Zinc Oxide Eugenol (e.g., IRM) or calcium hydroxide liners (e.g., Dycal) use their chemical properties for therapeutic effects on the dentine-pulp complex.
Advantages of Local Medication56
-
Deliver drugs to the site of required action
- e.g. pulp, periapical tissues, periodontal tissues
-
Faster action
- No time delay waiting for GIT absorption
-
Safer
- Avoids systemic complications and side effects
-
*No patient compliance problems
-
Proven Efficacy
- ==A study comparing post-operative pain relief showed that an intracanal corticosteroid (dexamethasone) was significantly more effective and provided more rapid pain reduction than oral ibuprofen or a placebo.==
Systemic Medication for post op pain relief7
-
Anti-microbial
-
Analgesic
-
Anti-inflammatory
-
the choice for postop systemic medication Depends on the DIAGNOSIS !!!
Analgesics8
- Paracetamol (acetaminophen)
- Codeine
Mechanism of Action (“Centrally”)9
- Paracetamol
- Selectively inhibits prostaglandin release in the CNS
- Codeine
- Metabolises to form morphine
- Inhibits neurons in the brain and dorsal horn of the CNS
- BUT need at least 30 mg to be effective in adults
- Poor metabolisers of codeine to morphine:
- 7 - 10% of Caucasians
- 1 - 2% of Asians
- 0 - 20% of Africans
- Do not increase the dose of codeine in low metabolizers as this causes constipation and drowsiness
Clinical Note
If a patient reports that codeine doesn’t work for them then theres no point giving it to htem as they are probably poor metabolizers
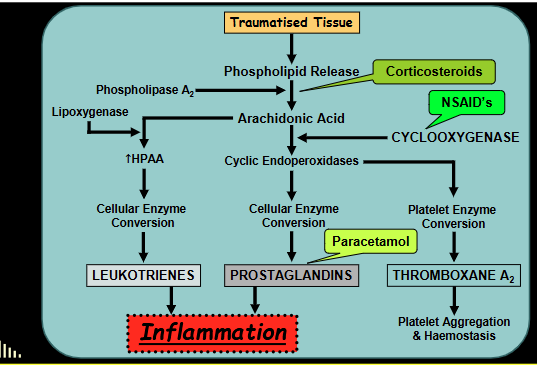
Anti-inflammatory (NSAID’s)10
- Non-steroidal anti-inflammatory drugs
- Work both “locally” and “centrally”
- Inhibit cyclo-oxygenase which reduces the synthesis of inflammatory mediators (e.g. prostaglandins from arachidonic acid)
- Common examples:
- Aspirin
- Ibuprofen
Dosage Effects of NSAIDs11
- Low doses → pain relief
- → e.g. 200mg Ibuprofen
- High doses → anti-inflammatory action
- → At least 400mg Ibuprofen
- → But need to use as a “course of medication”
- → i.e. take at regular intervals (4 hourly is ideal)
- This is done to maintain a therapeutic level in the bloodstream, rather than waiting for pain to return.
Combination Preparations12
- Nuromol
- Ibuprofen 200 mg + Paracetamol 500 mg
- Panafen Plus
- Ibuprofen 200 mg + Codeine 12.8 mg
- Nurofen Plus
- Ibuprofen 200 mg + Codeine 12.8 mg
Codeine dose too low for most adults in combination preperations
Clinical Studies on Pain Relief13
Post-Operative Pain after 3rd Molar Surgery (Mehlisch et al - Clin Therap 2010)
- Tested Ibuprofen with Paracetamol for moderate to severe post-operative pain after 3rd molar surgery.
- Ibuprofen 400 mg + Paracetamol 1000 mg
- → Sig. better than the same dose of either drug alone
- Ibuprofen 200 mg + Paracetamol 500 mg
- → Sig. better than the same dose of either drug alone
- → Sig. better than Paracetamol 1000 mg
- → But NOT sig. better than Ibuprofen 400 mg
Pain Relief after Root Canal Treatment (Menhinick et al - IEJ 2004)
- Compared the efficacy of:
- Ibuprofen 600 mg
- Ibuprofen 600 mg + Paracetamol 1000 mg
- Placebo
- Largest pain intensity reduction was using Pbicuprofen and paracetamol combo
Availability of Pain Medications14
Patient Confusion
Patients face a confusing array of choices at pharmacies and supermarkets, often without expert guidance. Pharmacists may lack specific knowledge of dental pain and the treatment provided, making clear instructions from the dentist essential.
Pain Relief with Different Systemic Medications15
The Oxford League Table of Analgesic Efficacy
- shows drug efficacy and is constantly updated
Analgesic Efficacy Data161718
Why NSAIDs are More Effective for Dental Pain
NSAIDs like Ibuprofen are particularly effective because they act earlier in the inflammation pathway
Practical Guide to Pain Relief after Dental Treatment19
Four Questions to Consider
- How much pre-treatment pain has there been?
- ➤ FIVE times more likely to have moderate to severe pain after treatment if moderate to severe pain present prior to treatment
- Pain during treatment
- ➤ More likely to have post-operative pain (esp. long-term chronic pain) if pain during treatment - due to central sensitisation
- How much pain is likely after treatment?
- ➤ Mild ? ➤ Moderate ? ➤ Severe ?
- Can the patient use NSAID’s?
- ➤ Check for: Asthma, peptic ulcer, drug interactions, etc.
Clinical Nuance for Asthma
If a patient has asthma but has used ibuprofen before without issue, it may be safe to prescribe. However, they must be warned of the potential risk and advised to stop if they experience any breathing difficulties.
Recommended Pain Relief Regimens2021
| Pain Level: | MILD | MODERATE | SEVERE |
|---|---|---|---|
| NSAID’s can be taken | 400 mg Ibuprofen every 4 hours | 400 - 600* mg Ibuprofen 4 hourly PLUS 1000 mg Paracetamol every 4 hours
(This can be simplified by prescribing a combination tablet like Nuromol, 2 tablets) | 400 - 600* mg Ibuprofen PLUS 1000 mg Paracetamol with 60 mg Codeine ** every 4 hours |
| NSAID’s contra-indicated | 1000 mg paracetamol every 4 hours | 1000 mg paracetamol with 60 mg codeine every 4 hours | 1000 – 1500* mg paracetamol with 60 – 90* mg codeine every 4 hours |
NOTES:
-
ALL cases: 1 - 3 days usually sufficient. If still pain, review and reassess
-
* Only take higher dose on 1 or 2 occasions
-
Loading Dose: ==For moderate or severe pain, an initial
-
** Alternate Ibuprofen & Paracetamol / Codeine at 2-hourly intervals
-
Patient Instructions: ==It is crucial to give patients clear, written instructions, as the recommended regimen (e.g.,
Alternating Medication Schedule
Rationale for Alternating Schedule
This strategy is highly effective for severe pain. It ensures that as the effect of one drug begins to wane, the other is reaching its peak therapeutic level, providing continuous and superior pain coverage.
-
Alternate at 2 hourly intervals:
- → 400 mg Ibuprofen - start immediately
- → 1000 mg Paracetamol + 60 mg Codeine - start 2 hrs later
-
Paracetamol + Codeine - stop next day
-
Ibuprofen - continue for 2-3 days
- Use as a “course” of medication
- For its anti-inflammatory action
- Even once the pain has reduced
Maximum Daily Doses - for Adults22
| Drug | Maximum Daily Dose (mg) | Typical Tablet or Capsule (mg) | Maximum Tabs/Caps per Day | Allowable Regime |
|---|---|---|---|---|
| Ibuprofen | 2,400 | 200 | 12 x 200 | 2 tabs 4 hourly |
| Paracetamol | 4,000 | 500 | 8 x 500 | 2 tabs 4 hourly BUT only 4x/day (i.e. NOT 6x/day) |
| Codeine | 360 | 30 | 12 x 30 | 2 tabs 4 hourly |
Paracetamol / Acetaminophen Dosage Guidelines23
- USA: In 2011 - reduced maximum daily dose to 3000 mg
- i.e. From 8 tabs. to 6 tabs. per day
- To reduce number of overdoses
- Overdose can cause acute liver failure & death
- UK: also 3000 mg
- BUT: Australia, NZ, Canada - 4000 mg
Prescribe REST
-
Tooth ( + restoration)
- “Relieve the bite”
-
General rest
- Sleep
- No work, etc
-
This is especially important for patients who were in severe pain and may not have slept.
- WARNING: Patients taking codeine must be warned not to drive or operate machinery.
Summary: Managing Dental Pain24
- Diagnose the CAUSE and TYPE of pain
- Inflammation
- and / or
- Infection
Medications available for dental pain
| Type of Drug | Method of Use |
|---|---|
| Anti-inflammatory | Local |
| Analgesic | Systemic |
| Antibiotic |
Depends on the CAUSE and TYPE of pain
Achieving Predictable Pain Relief25
- Thorough assessment of the presenting problem
- Adequate treatment / management Of the patient, tooth, pulp, gingiva, mucosa, muscles, etc.
- Appropriate medication → PREDICTABLE Pain Relief
The 3-D’s
- Diagnosis
- Dental Treatment
- Drugs
Follow-up: The 3-R’s26
- Review - has the pain gone?
- Reassess - the diagnosis
- Reconsider - the management
Footnotes
-
Original PDF page 1: O1B PostOperativePainManagement, p.1 ↩
-
Original PDF page 2: O1B PostOperativePainManagement, p.2 ↩ ↩2
-
Original PDF page 3: O1B PostOperativePainManagement, p.3 ↩
-
Original PDF page 5: O1B PostOperativePainManagement, p.5 ↩
-
Original PDF page 6: O1B PostOperativePainManagement, p.6 ↩
-
Original PDF page 7: O1B PostOperativePainManagement, p.7 ↩
-
Original PDF page 8: O1B PostOperativePainManagement, p.8 ↩
-
Original PDF page 9: O1B PostOperativePainManagement, p.9 ↩
-
Original PDF page 10: O1B PostOperativePainManagement, p.10 ↩
-
Original PDF page 11: O1B PostOperativePainManagement, p.11 ↩
-
Original PDF page 12: O1B PostOperativePainManagement, p.12 ↩
-
Original PDF page 13: O1B PostOperativePainManagement, p.13 ↩
-
Original PDF page 14: O1B PostOperativePainManagement, p.14 ↩
-
Original PDF page 15: O1B PostOperativePainManagement, p.15 ↩
-
Original PDF page 17: O1B PostOperativePainManagement, p.17 ↩
-
Original PDF page 18: O1B PostOperativePainManagement, p.18 ↩
-
Original PDF page 19: O1B PostOperativePainManagement, p.19 ↩
-
Original PDF page 20: O1B PostOperativePainManagement, p.20 ↩
-
Original PDF page 21: O1B PostOperativePainManagement, p.21 ↩
-
Original PDF page 22: O1B PostOperativePainManagement, p.22 ↩
-
Original PDF page 24: O1B PostOperativePainManagement, p.24 ↩
-
Original PDF page 23: O1B PostOperativePainManagement, p.23 ↩
-
Original PDF page 25: O1B PostOperativePainManagement, p.25 ↩
-
Original PDF page 26: O1B PostOperativePainManagement, p.26 ↩
-
Original PDF page 27: O1B PostOperativePainManagement, p.27 ↩
-
Original PDF page 28: O1B PostOperativePainManagement, p.28 ↩