Managing Concurrent Endodontic and Periodontal Diseases
Concurrent endodontic & periodontal diseases
Info
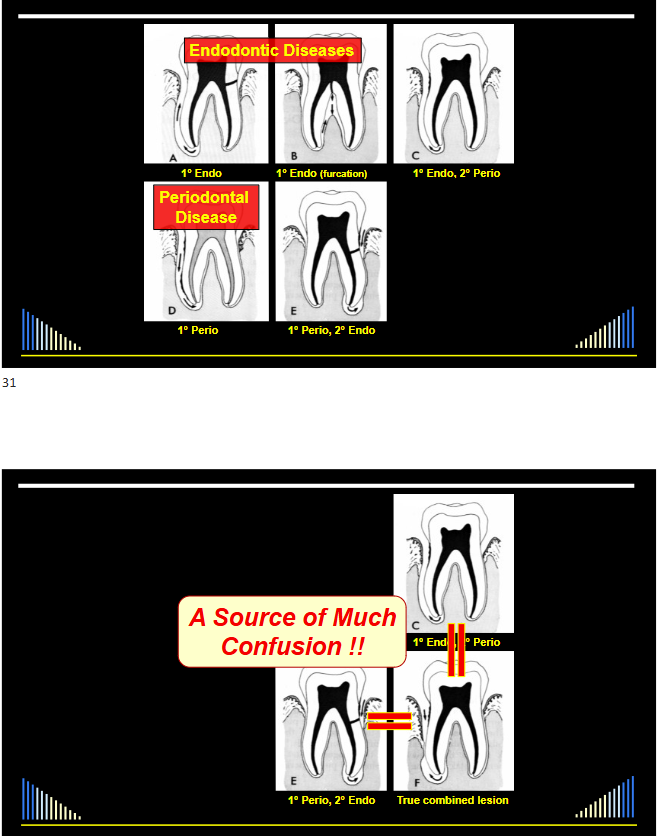
Concurrent endodontic and periodontal diseases are particularly difficult cases to treat and are a source of significant confusion for the dental profession. This lecture aims to clarify this uncertainty by discussing classifications, the interrelationship between the pulp and periodontium, and a sequential management strategy.
Concurrent endodontic & periodontal diseases: a source of confusion1
Sources of Confusion
TWO main reasons for this confusion:
- The “all inclusive” approach
- Many textbooks and journals group various distinct conditions under the umbrella of 'endo-perio lesions' simply because they have both endodontic and periodontal implications.
- The diagnostic classifications used
- Historical and even some modern classifications are often not clinically useful, meaningful, or based on accurate disease terminology.
Broad Interactions (Conditions with Both Endodontic and Periodontal Implications)
-
Cracked cusps
-
Root caries
-
Grooved roots
-
Traumatic occlusion
-
Lateral periodontal cyst
-
Developmental anomalies
-
Orthodontic complications
-
Resorption
-
Perforations
-
Transplanted teeth
-
Restoration margins
-
Vertical root fractures
-
Horizontal root fracture
-
Dentine hypersensitivity
-
All may have Endodontic & Periodontal implications / symptoms / signs
-
BUT they are not “Concurrent Endodontic and Periodontal Diseases”
-
They are distinct diseases / conditions - with their own causes and specific management options
Some examples of broad conditions that are not concurrent disease
Root Perforation23
-
==An iatrogenic event, such as a post-placement error, can cause periodontal pocketing and may lead to an infected root canal system.==
-
==The primary diagnosis is root perforation, not a concurrent disease.==
-
Manifested by rapid increased probing depth, suppuration, increased mobility, pain/awareness with function
Horizontal Root Fractures
-
A fracture in the root can cause periodontal pocketing and abscess formation.
-
==The primary diagnosis is horizontal root fracture.==
-
Manifested by rapid increased probing depth, suppuration, increased mobility, pain/awareness with function
Vertical Root Fractures4
-
==These fractures can lead to periodontal pocketing, an infected root canal system, and apical periodontitis.==
-
==The primary diagnosis is vertical root fracture.==
-
Manifested by rapid increased probing depth, suppuration, increased mobility, pain/awareness with function
External Invasive Root Resorption
-
This condition can manifest with periodontal abscesses and ankylosis.
-
==The diagnosis is external invasive resorption (e.g., a Class 4 Heathersay type), which often necessitates extraction.==
-
Manifested by bleeding on probing, sometimes with ankylosis, sometimes with suppuration if infected, otherwise asymptomatic
Caries, Restorations, Cracks5
-
==Dental caries, failing restorations (e.g., with overhangs), or cracks (e.g., cracked cusp) can independently lead to both pulp disease and periodontal problems.==
-
These are specific causative factors and should be diagnosed accordingly.
-
36 - caries, restoration breakdown, root-filled & infected root canal system
-
Distal root - crack and periodontal pocketing
Clarification on Broad Interactions
- All have Endodontic & Periodontal implications / symptoms / signs
- BUT they are not “Concurrent Endodontic and Periodontal Diseases”
- They are distinct diseases / conditions - with their own causes and specific management options
Warning
This lecture focuses exclusively on true cases of concurrent endodontic and periodontal diseases, where a tooth simultaneously presents with both an endodontic disease (originating from the pulp) and a separate periodontal disease (originating from the marginal periodontium).
Classifications of endodontic and periodontal conditions67
Problematic Terminology: “Endo-Perio Lesions”
Bug
The term ‘lesion’ is defined as an injury or wound. A periapical radiolucency is a host defense reaction to infection, not an injury itself. Therefore, ‘disease’ is a more accurate term. The term ‘endo-perio lesion’ is problematic and should be avoided.
Failure
Conclusion: This classification is not clinically useful. The terms are not meaningful (e.g., they don’t specify the type of pulp or periodontal disease), and it wrongly includes conditions that are purely endodontic or purely periodontal.
Clinical Classification (Modified from Torabinejad and Trope 1996)8
Problematic Terminology
A New Clinical Classification (Abbott and Castro Salgado - ADJ 2009)9
- Concurrent Endodontic & Periodontal Diseases
- → Without communication
- → With communication
Terminology Definitions
-
Concurrent ✅ occurring simultaneously
- ==Concurrent is a more accurate descriptor for teeth that have both diseases, whether they are communicating or not.==
-
Disease ✅ a pathological condition; a harmful deviation from normal
- ==Disease better describes the processes involved.==
Success
The recommended terminology is Concurrent Endodontic and Periodontal Diseases.
Application of the New Classification10
Concurrent Endodontic & Periodontal Diseases → Without communication → With communication
Applies to teeth that have BOTH:
- An infected root canal system causing some form of apical periodontitis
- AND: some form of marginal periodontal disease
Todo
This approach requires the clinician to make two separate diagnoses for the same tooth:
- A specific endodontic diagnosis for the pulp, root canal, and periapical tissues.
- A specific periodontal diagnosis using the standard periodontal classification.
Classifications of Pulp, Root Canal and Periapical Conditions11
Specific Conditions Included
In Particular … Teeth With:
PULP / ROOT CANAL CONDITIONS
- Necrotic and infected pulp
- Pulpless and infected root canal system, or
- Root-filled and infected root canal system
PERIAPICAL CONDITIONS
- 2° acute apical periodontitis
- Chronic apical periodontitis
- 2° acute apical abscess
- Chronic apical abscess
- Extra-radicular infection
- Pocket cyst
- True cyst, or
- Foreign body reaction
Plus …
- Advanced chronic periodontitis
- ➤ Loss of attachment to the apical foramina
- ■ With pulp implications
- Or PERHAPS teeth with early-moderately advanced chronic periodontitis
- ➤ If a lateral canal foramen is involved
- ■ Since may be pulp implications
Inter-relationships: root canal system & periodontium1213
Communication Pathways14
-
Apical Foramen
-
Dentine Tubules
-
Lateral Canals
- More common in the apical third of the root (approx. 8.8%) and less common in the coronal third (1.6%), where periodontal pockets typically begin.
- From the main canal laterally to the PDL
-
Accessory Canals
- Canals from the pulp chamber to the furcation
-
Developmental Grooves
- Such as palato-radicular grooves, which can harbor plaque and provide a direct pathway to the pulp.
-
Cracks / Fractures
Microbiological Evidence15
Similarities in the microflora of root canals and deep periodontal pockets
- There are significant similarities in the types of anaerobic bacteria found in infected root canals and deep periodontal pockets.
Kerekes K, Olsen I. Endod Dent Traumatol 1990; 6: 1-5
- A review showing similarities between the microflora of infected root canals and deep periodontal pockets provides evidence supporting the concept that infection can spread from one site to the other.
Infection Spread and Treatment Precautions16
Evidence for the concept that infection can spread from one site to the other
-
Cross-infecting organisms:
- Highly motile
- Survive in highly reduced environments
-
Precautions must be taken:
- To prevent in vivo cross seeding of these micro-organisms during treatment
- Especially in compromised teeth
- → i.e. those with concurrent diseases
-
It is crucial to take precautions during treatment to prevent cross-seeding of bacteria, e.g., from an infected pocket into a cleaned root canal or vice-versa.
Key Findings from Jansson 1995
Study by Jansson et al. found that intracanal infection correlates with deeper periodontal pockets and more attachment loss over 6 years.
Managing Teeth with Concurrent Endodontic and Periodontal Diseases17
Diagnosis
- Must differentiate between Endodontic and Periodontal Diseases
- In order to provide appropriate management
Basis for Diagnosis
Diagnosis must be based on ALL of the following:
- History
- Symptoms
- Visual appearance of tissues
- Caries, restorations, etc
- Radiographic findings
- Clinical tests:
- Pulp sensibility tests
- Periodontal probing
- Palpation, percussion, mobility, etc.
i.e., a THOROUGH Examination !!
Essential Diagnostic Tools18
- Four “absolute essentials”
- CO₂ Pulp Tester
- For cold testing.
- Electric Pulp Tester
- Both cold and electric tests are necessary as teeth may respond to one but not the other.
- Periodontal Probe
- A narrow, ball-ended probe is ideal for detecting the deep, narrow pockets often associated with endodontic issues or root cracks.
- Periapical Radiograph
- For assessing bone levels and periapical status.
- CO₂ Pulp Tester
Treatment Sequencing19
What treatment should be done first? Depends on the DIAGNOSIS !!!
- Key decision:
- → Is there an ACUTE condition?
- OR
- → Are both the periapical & periodontal diseases CHRONIC?
Acute Cases
- Diagnose the source of the pain &/or swelling
- → ? Periapical or ? Periodontal
- Treat this problem first
- This emergency treatment effectively converts the acute problem into a chronic one, which can then be managed comprehensively.
- → Convert the acute problem into a chronic one
- Follow soon after with other treatment
Chronic Cases20
- i.e. - no pain or swelling
- Ideally sequence the treatment to avoid any cross-seeding of bacteria and the effects of the intracanal infection on the periodontal tissues and the healing response
- you should perform endodontic treatment first!
The Debate: Periodontal Treatment First?21
This approach is not recommended for several reasons:
-
Root canal infection significantly affects periodontal healing.
- ==The existing infected root canal system will significantly impair periodontal healing, leading to less pocket depth reduction and more epithelial downgrowth (Jansson, 1995).==
-
Pocket depth reduction is significantly less in the presence of root canal infection.
-
More marginal epithelium over cementum defects if the root canals are infected.
-
Cementum removed - will expose dentinal tubules:
-
If bacteria in the root canal
- → Promotes Ext. Inflammatory Resorption
- Scaling and root planing removes cementum, exposing dentine tubules. This can allow bacteria from the infected canal to cause external inflammatory root resorption.
-
May expose periodontal tissues to toxic medicaments if used in the root canal
- → Not so critical in areas with recession
- Exposed tubules can also allow toxic intra-canal medicaments to leak out and damage periodontal tissues.
-
The Debate: Endodontic Treatment First?22
Tip
This is the preferred approach as it addresses the endodontic infection, which is critical for successful periodontal healing. However, there is a significant caveat.
- ✓ Cementum layer is kept intact until the root canal infection is removed
- ➤ No exposed dentine on root surface
- ➤ Reduced chance of ext. root resorption
- ➤ Improved periodontal healing
- ➤ BUT root canal fillings do NOT seal canals
- ➤ All we can do is FILL the main root canal(s)
- ➤ But NOT the root canal SYSTEM
- ➤ FILLING and SEALING are NOT the same thing!!!
Bacterial Migration in Root-Filled Teeth23
- Many studies have demonstrated that bacteria can readily migrate through root-filled roots from Coronal → Apical.
Representative Studies on Bacterial Migration
Range: 2 – 86 days
- Numerous laboratory studies show that bacteria placed at the coronal end of a root-filled tooth can migrate to the apex in as little as 2 to 86 days.
Implications of Bacterial Migration24
-
==If a tooth with a communicating concurrent disease is root-filled while the periodontal pocket is still infected, bacteria from the pocket can reinfect the root canal system via the apical foramen, lateral canals, or exposed dentine tubules.==
- “Cross-seeding” is the term used to described the phenomenon above
Revised Endodontic-First Approach25
Info
To prevent reinfection, the final root canal filling should be delayed until the periodontal infection has been resolved. The canal should be kept dressed with an antibacterial medicament during this period.
- ✔ Canal sterility is more likely while there is a dressing in the root canal
- ■ Therefore delay the RCF until the periodontal infection has been removed
- ○ To reduce chance of bacterial “cross-seeding”
Treatment Strategy by Communication Status
WITHOUT communication
-
==Sequence: Perform root canal treatment first, followed by periodontal treatment.==
-
The final root filling can be placed after the usual medication period, as the risk of reinfection from the separate periodontal pocket is low.
-
■ Do Endodontic treatment first
- → Can complete RCF after usual medication period
-
■ Then do Periodontal treatment soon after
Case Example: WITHOUT communication26
WITH communication
This situation requires a more prolonged, staged approach.
-
==Sequence: Start endodontic treatment first, but defer the final root filling.==
-
==Use long-term intra-canal dressings while the periodontal treatment is performed and healing is assessed.==
-
Start the Endodontic treatment first
- Use long-term dressings and defer RCF until overall prognosis re-assessed and favourable
-
Do the Periodontal treatment while the root canals are still medicated
Intra-canal Medicaments27
CS/AB (e.g. Ledermix paste)
- Corticosteroid (triamcinolone)
- → Anti-inflammatory
- → Inhibits clastic cells
- → Prevents & arrests inflammatory resorption
- Antibiotic (demeclocycline)
- → Anti-bacterial - BUT limited
- → Increased mineralisation of bone
- → Inhibits clastic cells
Calcium hydroxide
- Anti-bacterial
- Prevent & arrest inflammatory resorption
- Stimulates hard tissue formation
- BUT - it is toxic:
- → Tissue necrosis
- → If no cementum:
- • Increased ankylosis
- • Increased replacement resorption
** combination Ledermix + Ca(OH)₂ pastes**28
-
==Recommended Combination: A 50/50 mixture of Ledermix and Calcium Hydroxide is often the best choice.==
-
==Benefits: Combines the advantages of both materials. The Ledermix paste reduces the toxicity of the calcium hydroxide, and the combination provides broad-spectrum antibacterial and anti-inflammatory action.==
-
Combines advantages of both materials with no reduction in therapeutic properties
-
Maintains all active components in the canal for a longer period of time
-
Ledermix paste reduces the toxicity of the calcium hydroxide and therefore reduces the harmful side effects
Management Protocol
This protocol applies to cases WITH communication.
Initial Management
- ==Access and Assess: Remove old restorations, caries, and cracks to assess the tooth’s restorability and periodontal prognosis. Probe again after access is gained.==
- ==Chemo-mechanical Preparation: Clean and shape the root canal system.==
- ==Medicate: Place an intra-canal medicament (e.g., 50/50 Ledermix/Ca(OH)₂).==
- ==Interim Restoration: Place a well-sealed interim restoration (e.g., glass ionomer), using an orthodontic band only if necessary and ensuring it does not impede oral hygiene or periodontal access.==
- Ketac silver or ketac fil with or without an ortho band
- ==Wait: Leave the initial dressing for a minimum of 4 weeks to allow the medicament to become fully effective within the dentine.==
- Ensure adequate interim restoration throughout all phases of treatment
- Allow normal oral hygiene
- Avoid SS band if possible
Follow-up Management29
- ==Periodontal Treatment: After the initial 4-week endodontic phase, the patient undergoes non-surgical periodontal treatment.==
- ==Review (3 months later): Reassess the periodontal healing.==
- ==Re-treat if Necessary: If periodontal healing is incomplete, more periodontal treatment (e.g., further root planing, surgical access) may be needed. At this point, the intra-canal dressing should be changed.==
- ==Repeat Cycle: Continue the cycle of periodontal management and changing the intra-canal dressing every ~3 months until a favorable and stable periodontal outcome is achieved.==
- ==Final Treatment: Only when the periodontal prognosis is deemed favorable should the root canal filling be completed and a definitive restoration placed.==
Case Studies concurrent endo perio WITH communication30
Prognosis and Alternative Treatments31
Prognosis of Teeth with Concurrent Endodontic and Periodontal Diseases
-
==The overall prognosis depends mainly on the periodontal prognosis.==
-
==Disinfecting the root canal system is relatively predictable.==
-
Achieving ideal periodontal healing is more challenging due to factors like complex root anatomy and patient oral hygiene.
-
Wait and reassess
- wait an assess until you can see the outcome
- Outcome will depend largely on the periodontal response and prognosis
- wait an assess until you can see the outcome
-
Essential to keep monitoring all aspects:
- → Periodontal
- → Endodontic
- → Restorative
- → And any other aspects
Alternative Treatments for Teeth with Concurrent Endodontic and Periodontal Diseases
-
Root resection
-
Hemisection
- Involves sectioning a lower molar through the furcation and removing one half, or separating the roots to be restored as two individual premolars.
- with r without root removal
- Involves sectioning a lower molar through the furcation and removing one half, or separating the roots to be restored as two individual premolars.
-
Extraction
-
Sometimes extraction is the only option.
- ==Replacement with an implant may be complicated. These sites often have significant bone loss, and patients with generalized periodontal disease may be poor candidates for implants.==
- Or other prosthesis
Root Resections32
- Involves removing one root of a multi-rooted tooth (e.g., mesiobuccal root of an upper molar).
Lander et al J Perio 1981; 52: 719-22
- A 1981 study following resected molars for 10 years found a survival rate of 62%, indicating it is a viable long-term procedure. Modern techniques may yield even better results.
SUMMARY
- ==Definition: A tooth with a concurrent disease has both an infected root canal system (with a periapical condition) AND a co-existing periodontal disease.==
- ==Diagnosis: Make separate, specific diagnoses for the endodontic and periodontal conditions. Do not confuse these true concurrent diseases with other conditions like root fractures or resorption.==
- ==Management: The treatment sequence significantly influences the outcome.==
- ==The endodontic treatment should always be initiated first to eliminate the infection that hinders periodontal healing.==
- ==In cases WITH communication, the final root canal filling must be delayed until the periodontal condition is stable and healed to prevent bacterial cross-seeding and reinfection.==
- ==Prognosis: The ultimate prognosis is primarily determined by the predictability of the periodontal treatment and the patient’s ability to maintain oral hygiene.==
- ==Patience is Key: These cases require patience and regular reassessment before proceeding to the final restorative phase.==
Footnotes
-
Original PDF page 3: O4 EndoPerio, p.3 ↩
-
Original PDF page 4: O4 EndoPerio, p.4 ↩
-
Original PDF page 5: O4 EndoPerio, p.5 ↩
-
Original PDF page 6: O4 EndoPerio, p.6 ↩
-
Original PDF page 7: O4 EndoPerio, p.7 ↩
-
Original PDF page 8: O4 EndoPerio, p.8 ↩
-
Original PDF page 9: O4 EndoPerio, p.9 ↩
-
Original PDF page 18: O4 EndoPerio, p.18 ↩
-
Original PDF page 20: O4 EndoPerio, p.20 ↩
-
Original PDF page 21: O4 EndoPerio, p.21 ↩
-
Original PDF page 22: O4 EndoPerio, p.22 ↩
-
Original PDF page 23: O4 EndoPerio, p.23 ↩
-
Original PDF page 24: O4 EndoPerio, p.24 ↩
-
Original PDF page 25: O4 EndoPerio, p.25 ↩
-
Original PDF page 26: O4 EndoPerio, p.26 ↩
-
Original PDF page 27: O4 EndoPerio, p.27 ↩
-
Original PDF page 29: O4 EndoPerio, p.29 ↩
-
Original PDF page 30: O4 EndoPerio, p.30 ↩
-
Original PDF page 31: O4 EndoPerio, p.31 ↩
-
Original PDF page 32: O4 EndoPerio, p.32 ↩
-
Original PDF page 33: O4 EndoPerio, p.33 ↩
-
Original PDF page 34: O4 EndoPerio, p.34 ↩
-
Original PDF page 35: O4 EndoPerio, p.35 ↩
-
Original PDF page 36: O4 EndoPerio, p.36 ↩
-
Original PDF page 37: O4 EndoPerio, p.37 ↩
-
Original PDF page 38: O4 EndoPerio, p.38 ↩
-
Original PDF page 39: O4 EndoPerio, p.39 ↩
-
Original PDF page 40: O4 EndoPerio, p.40 ↩
-
Original PDF page 41: O4 EndoPerio, p.41 ↩
-
Original PDF page 42: O4 EndoPerio, p.42 ↩
-
Original PDF page 45: O4 EndoPerio, p.45 ↩
-
Original PDF page 46: O4 EndoPerio, p.46 ↩