Oral Cancer
Oral Malignant Neoplasms
- Common: OSCC
- Less common:
- Salivary gland tumours
- Malignant melanoma
- Lymphoma
- Neoplasms of bone and connective tissue
- Some odontogenic tumours
- Maxillary antral carcinoma
- Metastatic neoplasms
- Kaposi sarcoma Oral cancer ranks 12th among all cancers in prevalence worldwide (Khalili, 2008) and when combined with pharyngeal cancer, it ranks 6th (Warnakulasuriya, 2009).
Epidemiology of OSCC
- Over 95% of Oral Cancer are Squamous Cell Carcinomas
- High mortality and morbidity.
- Survival rate has not changed (50% for 5 years)
- Over 60% of patients present locally or regionally advanced disease.
- Trends in the age and sex groups
OSCC epidemiology --- key patterns and takeaways
- Global burden is uneven. OSCC makes up a small fraction of all cancers in high-income countries (~2% in the UK/US), but a major share in South Asia (India, Pakistan, Bangladesh, Sri Lanka), where oral cancer can account for ~40% of all cancers. High rates are also seen in parts of China, Southeast Asia, Brazil, France, and Eastern Europe---closely tracking tobacco/areca-nut habits.
osccepi - Men are affected more than women, but the gap is narrowing. Historically male-predominant due to higher tobacco/alcohol exposure; in some regions (e.g., UK) the male:female ratio has fallen to ~1.5:1, with a small uptick in younger women. OSCC is largely a disease of older adults (median diagnosis just over 60; >95% >40 years).
osccepi - Anatomical pattern: Within the mouth, the posterolateral tongue is the most common site of primary disease. (Note: do not mix oral cavity with oropharynx---different epidemiology and drivers.)
osccepi - Risk factors are dominated by tobacco (smoked & smokeless) and alcohol; betel quid/areca nut is the lead driver across South/Southeast Asia. Sunlight mainly affects the lip. HPV plays a minor role in the oral cavity (but is a major risk in the oropharynx---another reason to separate datasets).
osccepi - Trend lines diverge by region. Many developed countries saw declines over decades (lagging improvements after reduced smoking), but the UK shows a slow rise in oral cavity cancers. Apparent “surges” in some reports often reflect bundling oral cavity with oropharyngeal cancers (HPV-related), which inflates the oral numbers. Meanwhile, tobacco consumption is declining in the US, Australia, and northern Europe but increasing in parts of the developing world, suggesting future shifts in burden.
osccepi - Oceania snapshot (big variation):
- Papua New Guinea stands out with very high ASRs for both sexes---among the highest in the region.
- Australia/New Zealand sit in the moderate range.
- Pacific Islands vary widely (e.g., French Polynesia/New Caledonia higher; Guam/Samoa lower).
These differences mirror local tobacco/areca-nut practices and access to care. (GLOBOCAN 2012 data summarized in the Oceania review.)
osccepi
- Prevalence & incidence concentration: On absolute counts, India dominates global 5-year prevalence and new cases, followed (at a distance) by large populations like the USA and China; South Asian countries (e.g., Pakistan, Bangladesh) also carry heavy burdens relative to size.
osccepi - Looking ahead: Even if age-specific rates stabilize or fall in some places, total cases and deaths are projected to rise by 2035 because of population growth and aging, with a larger male burden worldwide.
osccepi - Data caveat: Many registries pool lip, oral cavity, and oropharynx---this obscures true oral cavity trends; careful separation is essential for accurate interpretation and policy.
osccepi
Risk factors
- Betel nut
- This is why in india oscc is the number one oral cancer
- Cigarettes and vaping
- HPV
- Increasing oral sex habits
- Alcohol
- Sunlight (lip only)
- Patients without risk factors
- A small proporition of patients appear to hve no risk factors, most are elderly and female
ORAL CANCER: Pathogenesis
Cancer arises by progressive accumulation of genetic damage. About 6-8 gene mutations are typical, each must confer a growth advantage on the cell.
- Carcinogenesis is a multi-step process
Oral squamous cell carcinoma
- A long-standing white patch
- A small exophytic growth (possibly with no ulceration)
- A long-standing red patch
- These lesions are generally painless
Certain features should be viewed with suspicion
- Ulceration
- Induration
- Fixation to underlying structures
- Bone destruction
Case Study: SQUAMOUS CELL CARCINOMA
Case History
This 70—year—old man presented with a several—month history of a slow—growing lesion on the right lateral oral tongue that started as a small white patch (leukoplakia) associated with some discomfort and tenderness. He was a heavy smoker.
Differential Clinical Diagnosis
- Squamous cell carcinoma. This is the primary consideration due to persistent white patch, rapid growth, pain, and location.
- Fungal infection. May present as a white patch, but usually not painful or indurated. Easily scraped off.
- Lichen planus. Presents as white patches, but rarely painful or indurated and typically bilateral.
Diagnosis
Squamous cell carcinoma
Histopathology
Biopsy shows an invasive squamous cell carcinoma with areas of verrucous carcinoma arising from a severe squamous dysplasia or carcinoma in situ.
Discussion
Squamous cell carcinoma (SCC) is the most common cancer of the oral cavity and oropharynx and is more prevalent in men than in women. Over 90% of cancers affecting the head and neck are SCC, but the prevalence is decreasing as the prevalence of human papillomavirus (HPV) infection increases. Up to 80% of patients with SCC of the oral cavity are heavy smokers. Other important risk factors include alcohol consumption, sun exposure, immunosuppression, and genetics. SCCs have a predilection for the posterior and lateral borders of the tongue, floor of the mouth, soft palate, and tonsillar pillars. Early lesions are usually asymptomatic and appear as white patches (leukoplakia) or red patches (erythroplakia) or a combination of both. Indurated, ulcerated lesions are usually painful and occur in later stages of the disease. Definitive diagnosis is obtained by biopsy. Treatment varies and includes surgery (primary treatment), radiation therapy, and/or chemotherapy depending on the stage and location of the tumor. Radiation therapy is effective alone or in combination with surgery for both primary lesions and cervical lymph node metastasis. Chemotherapy is recommended for patients with advanced disease or recurrence. The 5—year survival rate is between 40%—50%.
Teaching Points
SCC is the most commonoral cancer; it is often preceded by leukoplakia or erythroplakia; it is usually associated with smoking and alcohol consumption; and it requires early diagnosis and treatment to improve the survival rate.
Question
What is the most common cancer of the oral cavity, which is usually found in an older male who is a heavy smoker or alcohol consumer?
Answer
Squamous cell carcinoma. Another classic presentation:
- Exophytic mass of the lower lip
Destructuve lesion of the nose
- The cause is sniffing of cocaine
Histopathological features
- Dysplastic stratified squamous epithelium that extends through the basement membrane and into the underlying fibrous connective tissue without attachment to the surface
- Malignant epithelial cells show eosinophilic cytoplasm, hyperchromatic nuclei, pleomorphism, mitotic activity, individual cell keratinization and intercellular bridging
- Superficial or microinvasion can be used to describe the earliest moment of invasion
- Malignant epithelium can invade fibrous connective tissue in islands, cords or individual cells
- Keratin pearls of round, eosinophilic, concentric layers of keratin can be seen and are associated with well differentiated tumors
- 3 histologic grades for conventional squamous cell carcinoma include well, moderately and poorly differentiated based on amount of keratinization, mitotic activity, cellular and nuclear pleomorphism, pattern of invasion and host response
- Below shows epithelial cells with lots of connective tissue
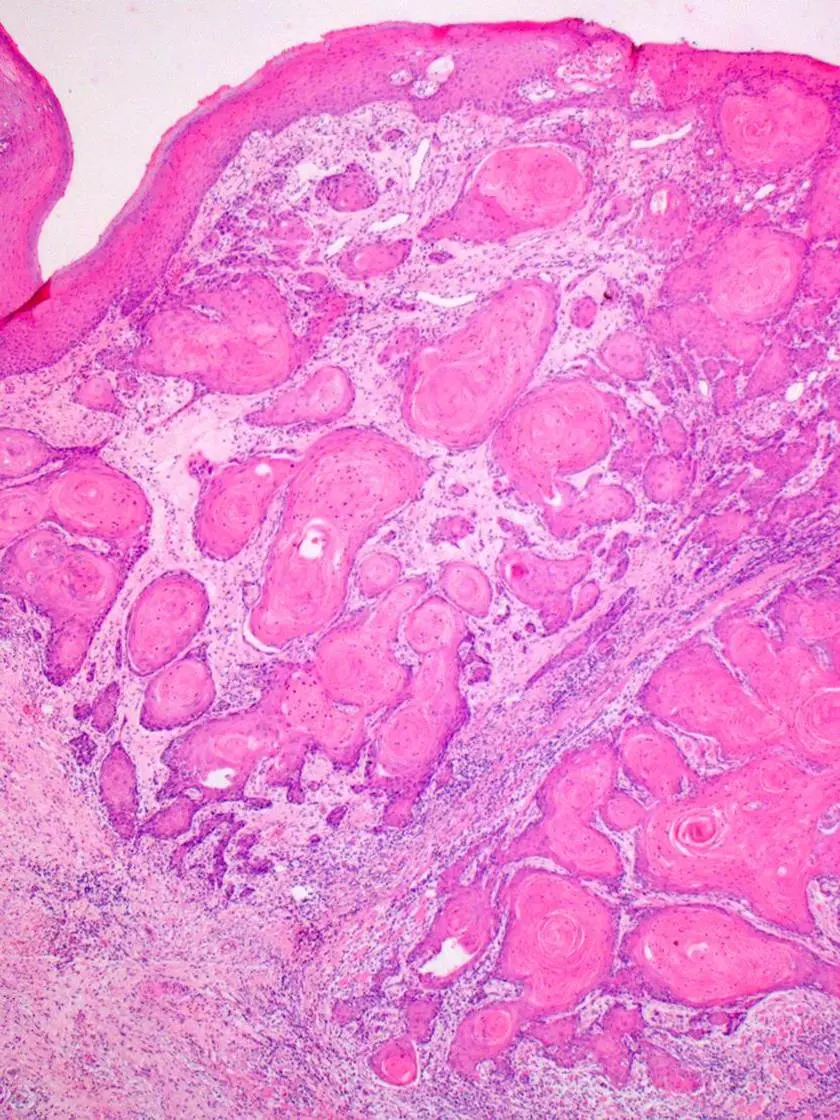
Well-differentiated OSCC
- Lots of keratin pearls
- Thus while the cells are differentiated but they still produce keratine
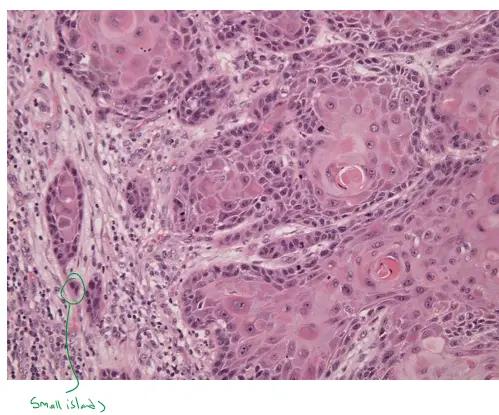
Moderately-differentiated OSCC
- The amount of keratin is less, but you see atypical cells
- The cells start to form smal llittle islands
- The pattern of invasion (Mild , moderate , well differentiated) as well as the margins will determine the prognosis of the tumor
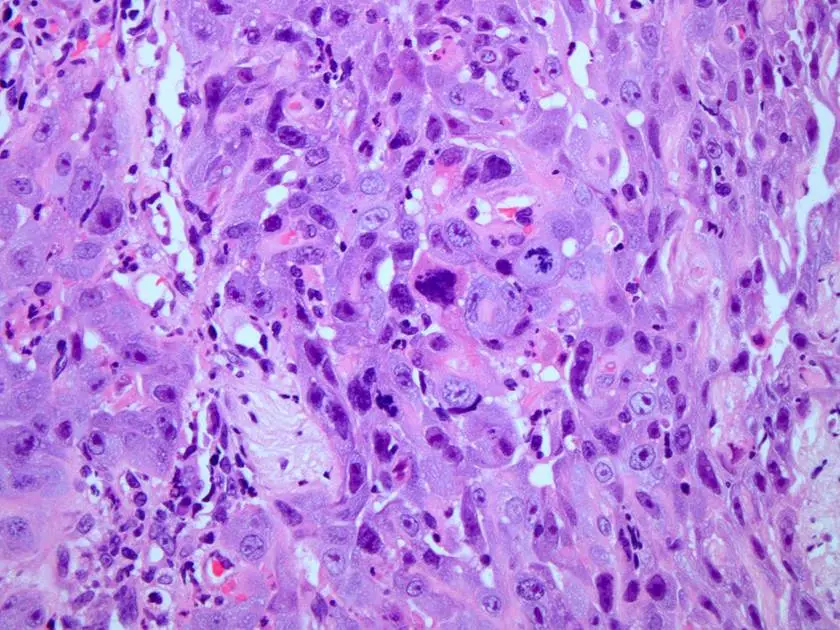
Poorly-differentiated OSCC
-
Cells are changed, but we can’t tell its hard to tell if cells are epithelial or mesenchymal
-
In this patient the cancer invaded the bone
-
Tumour in the tongue extending to the nose
- They cut the whole tongue, and did a neck dissection
- Lymph nodes in the neck are common sites for metastasis, that’s why lymph nodes are included in clinical exams!
 Midline Section
Midline Section
-
**One important factor is the *resection margin ***
- You can call it clear if it has 5 mm margin at lease
- If there is less than you know that the tumour has invaded Lymphovascular and neural invasion
-
When tumour cells invaded nerves they can cause severe pain
- This is called perineural invasion
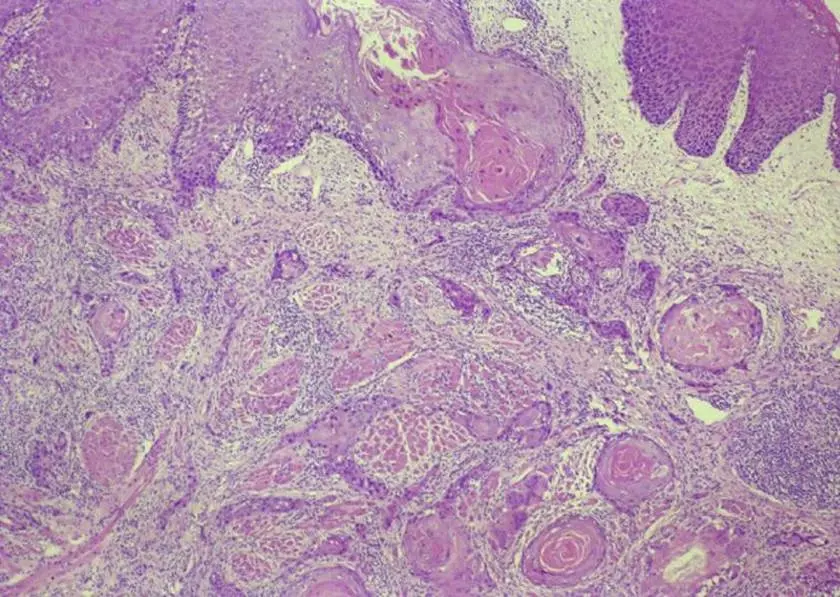 Poorly differentiated squamous cell carcinoma
Poorly differentiated squamous cell carcinoma
-
Cells become atypical in their appearance and they infiltrate the musc Poorly differentiated SCC and here are the different crops of this image to help you see better, use these only as hints:
Diagnosis and Staging
Local imaging and metastatic work-up
- MRI ± CT, PET scan (oral cavity and neck)
- Chest X-ray and thoracic spiral CT
- Esogastroscopy
TNM staging
- TNM classification (AJCC Cancer Staging Manual, 9th edition)
- The extent of the t umo r ( T )
- The spread to nearby lymph n ode s ( N )
- The spread ( m etastasis) to distant sites ( M ) Photograph showing a radical bilateral neck resection with hemi-mandibulectomy and floor of the mouth. The neck lymph nodes are included because the tumour often spreads via the lymphatic system. 1023/07 Extra: Management of the neck Neck Management in OSCC
- Therapeutic neck dissection: Performed when lymph node metastases are detected. It removes cervical lymph nodes from the skull base to clavicle, including submandibular, submental, and posterior triangles. Sometimes also sacrifices sternomastoid, jugular vein, or accessory nerve. May be needed for access in flap reconstruction.
- Elective neck dissection: Considered when no nodes are clinically involved, but microscopic spread may exist. It removes potential hidden metastases but often overtreats patients, exposing them to morbidity without benefit.
- Sentinel node biopsy: A less invasive alternative. A radioisotope (day before surgery) and blue dye (during surgery) highlight the first draining nodes. These are removed and examined.
- If negative, further dissection is avoided.
- If positive, full neck dissection follows.
- Benefit: Saves many patients from unnecessary surgery---metastases are actually found in only ~80% of therapeutic and ~33% of elective neck dissections.
TNM/AJCC Classification: T (Tumor)
- Tis: Carcinoma in situ
- T1: Tumor 2 cm or less in greatest dimension
- T2: Tumor > 2 cm but ⩽ 4 cm in greatest dimension
- T3: Tumor > 4 cm in greatest dimension
- T4 (lip): Tumor invades adjacent structures (through cortical bone, inferior alveolar nerve, floor of mouth, skin of face)
- T4 (oral cavity): Tumor invades adjacent structures (through cortical bone, into deep muscle of tongue, maxillary sinus, skin.)
TNM/AJCC Classification: N (Node)
- N0: no regional node metastasis
- Nx: regional nodes cannot be assessed
- N1: single ipsilateral node, ≤ 3 cm
- N2a: single ipsilateral node, > 3 cm and ≤ 6 cm
- N2b: multiple ipsilateral nodes, ≤ 6 cm
- N2c: controlateral or bilateral nodes, ≤ 6 cm
- N3: node > 6 cm
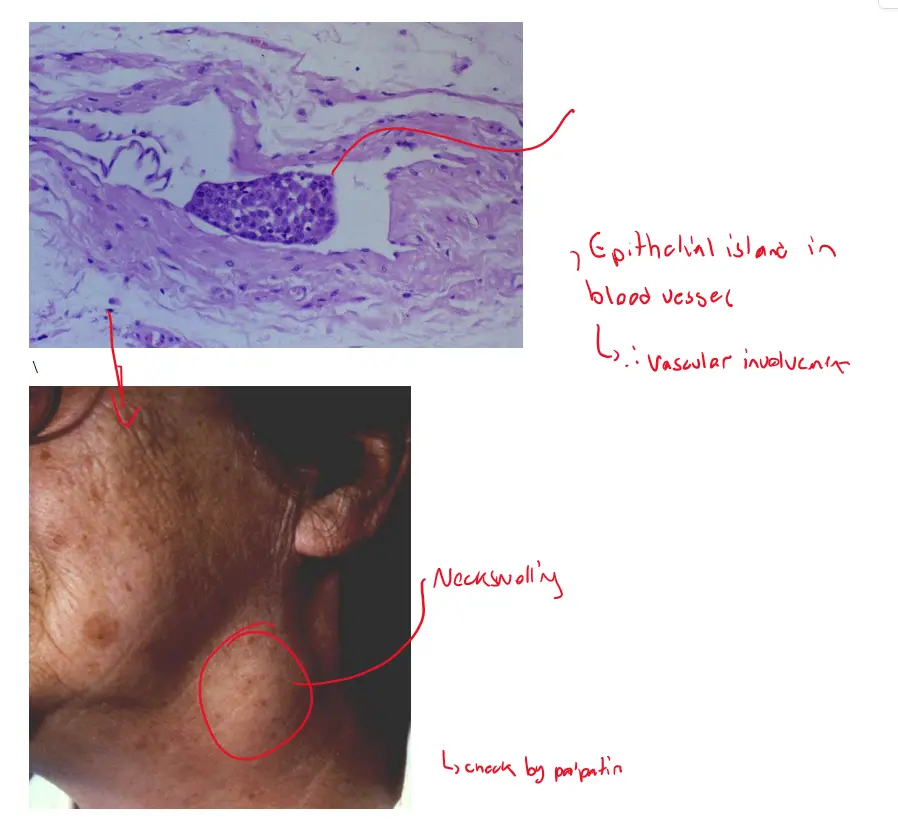
Example of advanced disease
- Patient has space with lymph node involvement
TNM/AJCC Classification: M (Metastasis)
- Mx: Distant metastasis cannot be assessed
- M0: No distant metastasis
- M1: Distant metastasis
Management
- Five year survival rates
- Stage I: > 80%
- Stage II: ~60%
- Stage III: ~35%
- Stage IV: < 15%
Prevention
Prevention of Head and Neck Cancer in Primary Care Practice
- Identify patients who use tobacco and alcohol products.
- Counsel patients to stop using tobacco and alcohol products.
- Maintain high index of suspicion.
- Conduct comprehensive exams.
- Attend to common symptoms.
- Evaluate symptomatic patients.
- Maintain close medical surveillance of patients in high-risk occupations.
- Refer high-risk patients with persistent symptoms and no findings to a head and neck surgeon.
Factors Delaying the Diagnosis of Head and Neck Cancers
- Patient procrastination in seeking medical attention
- Physician delay in diagnosis
- Patient remains asymptomatic for a prolonged period
Prevention strategies
- Late diagnosis contributes to advanced stage disease and poor prognosis
- Smoking cessation and alcohol drinking
- Early detection is so important in improving the survival rate
- Oral cancer screening (insufficient evidence)
- Squamous cell carcinoma is a malignant epithelial tumour. If you have a practice which has 20,000 patients you would expect to see one case of the disease every year. Dentists are often more effective than medics in detecting the early stages of oral cancer
Clinical Tips and Guidelines
’Red flag’ features of oral mucosal disease**
- oral ulcers that have lasted for more than 2 weeks
- orals ulcers that recur
- nontraumatic oral ulcers in children
- pigmented lesions on the oral mucosa
Assessment of oral mucosal disease
- red, white or mixed red and white lesions on the oral mucosa of unknown origin or with features of potentially malignant disease, such as:
- induration
- ulceration with rolled margins
- fixation to underlying tissues
- lesions in high-risk sites (eg lateral tongue, floor of mouth)
- facial or oral paraesthesia
- Paraesthesia without a clear cause is a huge red flag
- persistent oral mucosal discomfort with no obvious cause
- lumps or swellings, including lymphadenopathy
- swelling, pain or blockage of a salivary gland, suggestive of salivary gland disease (eg see Figure 13.9 for common causes of salivary gland swellings)
- suspected allergy or adverse reaction to dental materials (eg oral lichenoid lesion )
- dry mouth that is not adequately relieved with artificial salivary products and nonpharmacological methods
- dry mouth caused by systemic disease
- suspected oral manifestations of systemic disease (eg syphilis, Behçet syndrome, HIV, inflammatory bowel disease, lichen planus, pemphigoid)
- lesions occurring in immunocompromised patients (eg patients with neutropenia or HIV infection)
8 Steps of Oral Cancer Screening
Step Area