Immune-Mediated Oral Conditions1
This lecture covers a range of immune-mediated and allergic disorders affecting the oral cavity, focusing on their clinical features, pathogenesis, and histopathology.
Introduction to Immune-Mediated Conditions
The immune system is crucial for distinguishing the body’s own cells (self) from foreign antigens. An autoimmune disease occurs when there is a failure to discriminate between harmful and harmless antigens, leading the body to react aggressively against itself.
- ==Variability in Response: The clinical presentation of these conditions varies significantly among individuals. This is due to differences in how each person’s immune system reacts, which can be influenced by factors like genetic predisposition. Some individuals may have a severe reaction to a minor trigger, while others show no response.==
Clinical Presentation
-
Onset is generally in the second and third decades of life with a 2:1 female predilection, and lesions diminish in severity with age with complete resolution by age 50 in most cases.
-
While the exact cause is unknown, they are associated with trauma, physical and emotional stress.
-
Ulcers are episodic but may be continuous in severe/complex cases, be single or multiple, and occur almost exclusively on the nonkeratinized mucosa.
NOTE
They are typically found on movable mucosa like the buccal mucosa, labial mucosa, and floor of the mouth.
They are sharply demarcated and painful, and composed of a yellow fibrin membrane with surrounding erythema.
There are three principal forms of RAUs: minor, herpetiform, and major.
Definitions
- ==Ulcer: A complete loss of the epithelium, exposing the underlying connective tissue. Clinically, it often appears as a defined area covered by a yellowish fibrinous exudate and surrounded by an erythematous (red) halo.==
- ==Erosion: A partial loss of the epithelium without exposing the connective tissue.==
- ==Atrophy: A thinning or decrease in the thickness of the epithelium.==
Causes of Ulcers
- ==Most Common: Trauma==
- ==Other Causes: Viruses, systemic conditions, and immune-related disorders.==
Allergic and Hypersensitivity Reactions
These are inflammatory reactions caused by direct contact with an offending allergen.
Allergic Contact Mucositis (Stomatitis)
This condition is an inflammatory reaction caused by direct contact with an allergen.
- ==Common Allergens in Dentistry:==
- Latex (e.g., gloves, orthodontic elastics)
- Oral hygiene products (e.g., compounds in toothpaste, mouthwashes)
- Denture base acrylics
- Dental metals
- ==Clinical Presentation:==
- ==Contact Dermatitis: Presents with rashes and an asymmetric surface.==
- ==Contact Mucositis: Appears as an erythematous (red), edematous (swollen), or atrophic (thinned) area.==
- ==Mucosal Sloughing: Some products, like certain toothpastes or mouthwashes, can cause the superficial layers of the mucosa to easily exfoliate.==
- ==Ulcers/Blisters: In some cases, blisters may form, which are fluid-filled, rupture easily, and leave behind ulcers.==
- ==Diagnosis: A detailed patient history is critical to identify the source of the reaction. It’s important to ask about product use, diet, and family history of allergies. Patch testing may be necessary.==
Plasma Cell Gingivitis
This is a distinct form of gingivitis characterized by a significant allergic response.
- ==Clinical Presentation:==
- Diffuse, widespread, erythematous (bright red) enlargement of the free and attached gingiva.
- ==The gingiva has a
- Plasma cell gingivitis has become relatively common since oral health care products containing hypersentitive reagents
- Microscopically, many plasma cells are present when the tissue is biopsed.
- treatment involves discontinuing the use of allergen.
- Topical anti-inflammatory agents may be needed to resolve mucositis
Forms of Recurrent Aphthous Ulcers (RAUs)2
-
Minor, Herpetiform and Major
-
Minor ulcers are the most common (80%), are ≤1 cm in size, and last 1 to 2 weeks; the number of episodes each year varies depending on the individual.
-
Usually 1-2 ulcers appear at a time and heal without scarring.
- if its more frequent → systemic cause
- Minor ulcers usually happen in non-keratinized epithelium
-
Herpetiform ulcers are uncommon and number more than 10 small ulcers (usually 0.1–0.5 cm) at each episode and last t to 2 weeks.
-
The small ulcers often coalesce (merge) to form large, irregular, and extremely painful ulcerated surfaces.
-
Major ulcers are the least common, are larger than 1 cm in size, last for weeks or months, and may be associated with scarring.
-
==This form is also known as Sutton’s Disease, and the ulcers often have a slightly raised border.==
Histopathology3
**fib
- Ulcers consist of a fibrin membrane with enmeshed neutrophils and underlying granulation tissue with acute and chronic inflammatory cells confined to the lamina propria and sometimes involving superficial skeletal muscle fibers.
NOTE
The surface is covered by an exudate containing numerous neutrophils (acute inflammation), while the underlying tissue shows chronic inflammation (lymphocytes).
-
The adjacent epithelium exhibits spongiotic pustules and reactive atypia such as basal cell hyperplasia, nuclear hyperchromasia, and slight pleomorphism.
-
These reactive changes, like spongiosis (intercellular edema), occur as the epithelium attempts to heal and cover the defect.
- granular tissue
- blood vessels
- fibroblasts
- epithelial cells
- granular tissue
Clinical notes4
- Traumatic ulcers should clearly be distinguished from RAUs based on the patient’s history. The patient will report injuring himself or herself in the area of the ulcer or the clinician might observe a defective restoration or prosthesis contacting the ulcer.
- Treating a traumatic ulcer with topical anti-inflammatory medication, an acceptable treatment for RAU, may lead to delayed healing and possible infection in a traumatic ulcer.
- Ulcers on the gingiva or hard palate are not recurrent aphthous ulcers. RAUs only occur on nonkeratinized tissue. The gingiva and hard palate are keratinized.
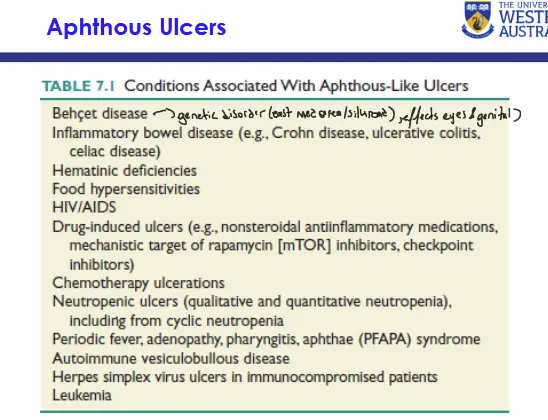
TABLE 7.1 Conditions Associated With Aphthous-Like Ulcers5
 |
Info
A systemic vasculitis associated with specific HLA alleles.
Info
Celiac disease is a gluten-sensitive enteropathy.
| Cause of Oral Ulcers |
|---|
| Inflammatory bowel disease (e.g., Crohn disease, ulcerative colitis, celiac disease) |
| Hematinic deficiencies |
| Food hypersensitivities |
| HIV/AIDS |
| Drug-induced ulcers (e.g., nonsteroidal antiinflammatory medications, mechanistic target of rapamycin [mTOR] inhibitors, checkpoint inhibitors) |
| Chemotherapy ulcerations |
| Neutropenic ulcers (qualitative and quantitative neutropenia), including from cyclic neutropenia |
| Periodic fever, adenopathy, pharyngitis, aphthae (PFAPA) syndrome |
| Autoimmune vesiculobullous disease |
| Herpes simplex virus ulcers in immunocompromised patients |
| Leukemia |
TRAUMATIC ULCERATIVE GRANULOMA WITH STROMAL EOSINOPHILS, EOSINOPHILIC ULCER OF TONGUE67
- Traumatic ulcerative granuloma is secondary to deeply penetrating inflammation involving the underlying skeletal muscle and is most often associated with trauma although less than 50% of patients report such a history. It may be primary or secondary to trauma to another preexisting condition.
- There is an ulcer with acute and chronic inflammation that penetrates into the muscle with separation and degeneration of muscle fibers, sometimes with a “checkerboard” pattern, proliferation of macrophages, and many eosinophils. However, eosinophils may be sparse or even absent, depending on the stage of the ulcer.
TUGSE vs. Squamous Cell Carcinoma
This is a specific, non-healing ulcer that can be misdiagnosed as squamous cell carcinoma, typically appearing on the lateral border of the tongue. The key diagnostic feature is the presence of a large number of eosinophils within the granulation tissue. These lesions often require surgical excision to heal properly.
Erythema Multiforme8
- Erythema multiforme (EM) a self-limiting disease that causes a characteristic skin rash and often severe outbreaks of painful ulcerations of the mucous membranes.
- EM most commonly occurs in young adults and affect males more often than females. EM differs from the three forms of RAU in that EM has a more generalized distribution of ulcerations and erosions accompanied by severe pain.
- A severe form of EM is Stevens-Johnson syndrome, also called erythema multiforme major. In addition to the skin and oral lesions, patients develop eye and genital lesions
Lichen Planus9
- Controversial
- some believe benign
- others OPMD
- at OCHIWA = OPMD with CCC change
- can effect any tissue
- Lichen planus is a common disease of both skin and mucous membranes. Its name is derived from the appearance of the reticular form of the disorder that resembles lichens that grow on rocks and trees.
- It is most commonly seen in middle-aged women, but men comprise many patients.
- OLP is a common condition, with a prevalence of between 0.5-2.2% of the population.
- The aetiology of lichen planus is still under investigation.
- Typical age of presentation is between 30-60 years of age.
- Various forms of clinical presentation are encountered:
NOTE
The hallmark of oral lichen planus is that lesions are bilateral and more or less symmetrical.
- Reticular
- ==The most common form, presenting as a network of fine, white, interlacing lines known as Wickham’s striae.==
- Linear
- Papular
- Plaque-like
- Atrophic
- Erosive/ulcerative
- These forms cause pain and burning and have the highest risk of malignant transformation.
- Bullous
Definition of LICHEN PLANUS10
A chronic inflammatory disorder of unknown etiology with characteristic relapses and remissions, displaying white reticular lesions, accompanied or not by atrophic, erosive and ulcerative and/or plaque type areas.
OPMD
It is considered an oral potentially malignant disorder (OPMD).
Lesions are frequently bilaterally symmetrical. Desquamative gingivitis may be a feature
Info
When lichen planus extensively involves the gingiva, it can present as desquamative gingivitis, which is a clinical description for red, peeling gums, not a diagnosis in itself.
Aetio-pathogenesis11
The mechanisms involved in the aetio-pathogenesis of OLP are multifactorial and likely to be synergistic:
Info
It is understood to be a T-cell mediated autoimmune response (Type IV hypersensitivity), where a band-like infiltrate of lymphocytes attacks the basal layer of the epithelium, causing degeneration.
- cell-mediated immune response (Type IV hypersensitivity)
- role of the humoral immune response
- non-specific immune mechanisms;
- genetic factors.
Diagnostic criteria1213
ORIGINAL ARTICLE
| Clinical criteria | Histopathological criteria |
|---|---|
| •Presence of bilateral, more or less symmetrical white lesions affecting buccal mucosa, and/or tongue, and/or lip, and/or gingiva •Presence of a white papular lesions and lace-like network of slightly raised white lines (reticular, annular, or linear pattern) with or without erosions and ulcerations •Sometimes presents as desquamative gingivitis | •Presence of a well-defined band-like predominantly lymphocytic infiltrate that is confined to the superficial part of the connective tissue •Signs of vacuolar degeneration of the basal and/or supra basal cell layers with keratinocyte apoptosis •In the atrophic type, there is epithelial thinning and sometimes ulceration caused by failure of epithelial regeneration as a result of basal cell destruction. A mixed inflammatory infiltrate may be found |
Lichen Planus- Malignant transformation14
SPECIAL ISSUE ARTICLE
Oral lichen planus has a very low malignant transformation rate: A systematic review and meta-analysis using strict diagnostic and inclusion criteria
Follow-Up is Critical
Patients with oral lichen planus, especially the erosive type, require regular, long-term follow-up and should be referred to an oral medicine specialist for management.
Pemphigus vulgaris15
- The term pemphigus refers to a group of autoimmune blistering diseases of the skin and mucous membranes.
- The most common form, pemphigus vulgaris, is a potentially life-threatening mucocutaneous (both skin and mucous membranes) disorder that often manifests initially in the oral cavity.
Info
It was once potentially life-threatening but is now manageable with modern therapies.
- steroids + immunosuppresive meds have greatly improved prognosis.
- Pemphigus is derived from the Greek word pemphix, meaning bubble or blister.
Pathophysiology16
- Autoantibodies are produced against proteins called desmogleins, which form the desmosomes, the structural units that bind epithelial cells to each other.
NOTE
Specifically, the autoantibodies attack Desmoglein 3 (primarily in mucosa) and Desmoglein 1 (primarily in skin). This attack disrupts cell-to-cell adhesion, a process called acantholysis, which leads to the formation of an intraepithelial blister.
- When the autoantibodies attack the desmosomes, individual epithelial cells lose the ability to adhere to each other. Hemidesmosomes are not affected.
Histology and Clinical Features17
Pemphigus vulgaris
-
Biopsy of pemphigus vulgaris shows a split in the epithelium above the basal layer. Individual keratinocytes, referred to as Tzanck cells, appear to be floating away from each other, providing evidence that the desmosomes have been destroyed.
-
Mild trauma to the area may induce vesicle and bulla formation, leading to tissue sloughing similar to the Nikolsky’s sign seen in mucous membrane pemphigoid.
Pemphigus Vulgaris Patients
Patients develop fragile blisters (bullae) that are filled with fluid, rupture very easily, and leave large, painful, raw ulcerated surfaces.
- More than 50 % of patients with pemphigus vulgaris have oral lesions before they develop skin lesions.
- Oral lesions may affect any anatomic surface, but tend to appear on the buccal mucosa, palate, and gingiva.
Immunofluorescence1819
- Direct immunofluorescence shows intercellular deposition of IgG in a distinctive mesh- or netlike pattern. Epitope spread may account for the production of antibodies against multiple antigens.
- Indirect immunofluorescence studies for circulating autoantibodies performed on monkey esophagus or human skin, and enzyme-linked immunosorbent assay (ELISA) to identify autoantibodies against Dsg-1 and/or Dsg-3 should be performed because levels correlate with disease activity and as such, are useful for monitoring response to therapy.
Mucous membrane pemphigoid
- Mucous membrane pemphigoid (MMP) is a type 2 hypersensitivity reaction to specific hemidesmosomal proteins in the basement membrane of the epithelium called laminins. Autoantibodies produced by plasma cells destroy this hemidesmosomal “glue” that holds the epithelium to the underlying connective tissue.
Info
MMP is a type 2 hypersensitivity reaction to specific hemidesmosomal proteins in the basement membrane of the epithelium called laminins.
Histology and Clinical Features17
- Biopsy of mucous membrane pemphigoid shows a split between the full thickness of epithelium and the underlying connective tissue. Connective tissue and nerves are exposed to the oral environment, resulting in significant pain for the patient. Direct immunofluorescence is essential to confirm the diagnosis where IgG antibodies and C3 deposits are found on the basement membrane.
- Mild trauma may induce vesicle and bulla formation, leading to tissue sloughing, a phenomenon referred to as Nikolsky’s sign.
Footnotes
-
Original PDF page 1: L11 Immune Medated Disorders -annotated, p.1 ↩
-
Original PDF page 15: L11 Immune Medated Disorders -annotated, p.15 ↩
-
Original PDF page 16: L11 Immune Medated Disorders -annotated, p.16 ↩
-
Original PDF page 17: L11 Immune Medated Disorders -annotated, p.17 ↩
-
Original PDF page 18: L11 Immune Medated Disorders -annotated, p.18 ↩
-
Original PDF page 19: L11 Immune Medated Disorders -annotated, p.19 ↩
-
Original PDF page 20: L11 Immune Medated Disorders -annotated, p.20 ↩
-
Original PDF page 21: L11 Immune Medated Disorders -annotated, p.21 ↩
-
Original PDF page 22: L11 Immune Medated Disorders -annotated, p.22 ↩
-
Original PDF page 23: L11 Immune Medated Disorders -annotated, p.23 ↩
-
Original PDF page 24: L11 Immune Medated Disorders -annotated, p.24 ↩
-
Original PDF page 25: L11 Immune Medated Disorders -annotated, p.25 ↩
-
Original PDF page 26: L11 Immune Medated Disorders -annotated, p.26 ↩
-
Original PDF page 27: L11 Immune Medated Disorders -annotated, p.27 ↩
-
Original PDF page 28: L11 Immune Medated Disorders -annotated, p.28 ↩
-
Original PDF page 29: L11 Immune Medated Disorders -annotated, p.29 ↩
-
Original PDF page 30: L11 Immune Medated Disorders -annotated, p.30 ↩ ↩2
-
Original PDF page 31: L11 Immune Medated Disorders -annotated, p.31 ↩
-
Original PDF page 32: L11 Immune Medated Disorders -annotated, p.32 ↩