Oral Pathology module: Connective Tissue disorders1
Introduction: Histology of the Oral Mucosa2
The oral mucosa is composed of three layers:
- ==Epithelium: A covering of stratified squamous epithelium, which can be keratinized or non-keratinized. Many previously discussed disorders, like leukoplakia, originate here.==
- ==Lamina Propria: This is the fibrous connective tissue layer beneath the epithelium. Its main components are:==
- ==Fibroblasts: Spindle-shaped cells.==
- ==Collagen fibers: Abundant fibrous protein.==
- Blood vessels and nerves.
- This lecture focuses on disorders originating in the lamina propria.
- ==Submucosa: The deepest layer, which can contain muscle, adipose tissue, and minor salivary glands. It may be attached directly to bone (e.g., gingiva, hard palate) or other soft tissues (e.g., soft palate, buccal mucosa).==
Soft-tissue tumours derived from mesenchymal components of connective tissue
Classification of Connective Tissue Disorders34
Pathogenesis
Connective tissue disorders are broadly categorized based on their pathogenesis:
- Reactive/Congenital:
- Reactive: A response to a stimulus (e.g., chemical, mechanical, physical trauma). These are very common in dental practice.
- Congenital: Present from birth, often related to hereditary genetic mutations.
- Neoplastic: Triggered by genetic mutations. Risk factors include environmental factors (smoking, alcohol, pollution), aging, and systemic medical conditions.
| Group | Reactive/congenital | Neoplasms |
|---|---|---|
| Fibrous | •Fibroma /fibroepithelialpolyp •Peripheral giant cell granuloma •Peripheral ossifying fibroma •Epulis fissuratum (inflammatory fibrous hyperplasia) •Inflammatory papillary hyperplasia •Generalized gingival hyperplasia | •Giant cell fibroma •Myofibroma •Aggressive Fibromatosis •Solitaryfibrous tumor •Fibrosarcoma •Fibrous histiocytoma, benign and malignant •Nodular fasciitis |
| Vascular | •Pyogenic granuloma •Varix; other acquired malformations •Benign vascular malformation •Lymphangioma | •Hemangioma •Angiosarcoma •Kaposi’s sarcoma •Hemangiopericytoma |
| Neural | •Traumatic neuroma | •Neurofibroma •Granular cell tumor •Schwannoma (neurilemoma) •Mucosal neuromas of MEN III •Palisaded encapsulated neuroma •Malignant peripheral nerve sheath tumor |
| Adipose tissue | •Herniated fat pad | •Lipoma and Liposarcoma |
| Muscle | •Smooth muscle •Striated muscle | •Leiomyoma and Leiomyosarcoma •Rhabdomyoma and Rhabdomyosarcoma |
Fibroma (“Bite” or “Irritation” Fibroma, Fibroepithelial or Fibrovascular Polyp), and Giant Cell Fibroma5
Aetiology
-
A reaction to chronic, low-grade irritation or physical trauma, such as cheek biting, lip biting (a stress-relief habit for some), or sharp edges on teeth or restorations.
-
This occurs at any age group without sex predilection and consists of a dome-shaped nodule or papule that may be white/keratotic, mucosa-colored, or ulcerated. It is located in areas readily traumatized by biting (i.e., buccal mucosa, lateral tongue, and lower lip mucosa) or on the gingiva where plaque accumulates.
-
It can be sessile (broad-based) or pedunculated (attached by a stalk).
-
It is less common on the hard or soft palate, where a similar-looking lesion is more likely to be neoplastic.
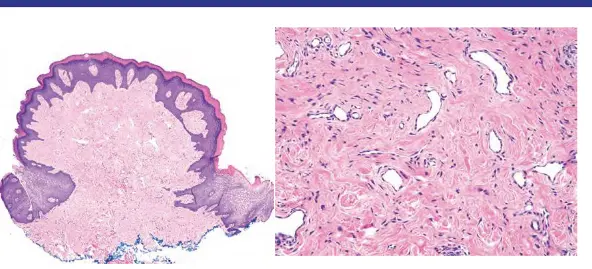
- A nodular mass of dense fibrous connective tissue
- Normal, hyperkeratotic, or ulcerated surface epithelium
Treatment67
- Simple surgical excision.
- ==Crucially, the causative factor (irritant) must be identified and removed to prevent recurrence. If the trauma is not eliminated, the lesion will likely return.==
Ossifying fibrous epulis (peripheral ossifying fibroma)8
- A common, swelling of the gingiva characterized by a core of fibrous connective tissue exhibiting the formation of variable amounts of amorphous deposits of calcifications
- Mostly seen in children and young adults
- A reactive lesion to local irritation
Clinically:
-
Red to pink, firm gingival nodule
-
typically arise from the interdental papilla
-
smooth surfaced, can be ulcerated
-
1 cm in diameter; can be larger
-
Often shows calcification on radiograph
-
==Imaging (e.g., OPG or periapical X-ray) is essential to rule out a central lesion (i.e., a lesion originating within the bone, like central ossifying fibroma, which can be destructive).==
-
A nodular mass of cellular fibrous connective tissue
-
contains bone, or cementum-like material
-
covered by normal or ulcerated surface epithelium
Treatment67
- Surgical excision down to the periosteum.
- The origin is thought to be related to cells of the periodontal ligament, so thorough scaling and root planing of the adjacent teeth is recommended to reduce the risk of recurrence.
A microscopic image showing a fibrous mass.
Angiogranuloma (pyogenic granuloma)9
- A common reactive vascular lesion
Aetiology
- A reactive lesion to local irritation or trauma
- Some are attributed to the effect of female hormones
- Tumour-like overgrowth of granulation tissue
Clinical features10
-
F>M; the prevalence is higher in women during pregnancy
-
Most common on the gingiva (75% of all oral cases)
-
tongue, lips, and buccal mucosa
-
Bright-red to dark-red, soft nodule
- smooth or lobulated surface; often ulcerated
- often bleeds easily
- <1 cm in diameter, can be larger
-
Pregnancy tumour (granuloma gravidarum): a pyogenic granuloma that develops on the gingiva during pregnancy
-
Epulis Granulomatosa: a pyogenic granuloma that develop in a healing extraction socket
-
Nodular mass of granulation tissue
-
dilated blood vessels in a loose fibrous stroma, with acute and chronic inflammatory infiltrate
-
normal or ulcerated overlying surface epithelium
Peripheral Giant Cell Granuloma (Giant Cell Epulis)1112
- A relatively common growth on the gingiva or the alveolar ridge characterized by a proliferation of multinucleated giant cells that resemble osteoclasts.
Aetiology
- A reactive lesion to local irritation or trauma
Clinical features10
-
Exclusively on the gingiva or edentulous alveolar ridge
- Red to blue-purple, firm gingival nodule
- typically arise from the interdental papilla
- smooth surface; may or may not be ulcerated
- typically <1 cm in diameter; can be larger
- may cause cupping resorption of the underlying alveolar bone
-
==Imaging is important to differentiate it from a central giant cell granuloma, a more significant lesion that originates within the jawbone. Central lesions can be destructive and are sometimes associated with hyperparathyroidism (in which case they are called ‘brown tumors’).==
Microscopy13
- A nodular proliferation composed of osteoclast-like multinucleated giant cells in a cellular and haemorrhagic background
- osteoclast-like multinucleated giant cells // multinucleated giant cells b/fsen monocytes
- cellular fibrous stroma
- extravasated RBCs, and haemosiderin pigmentation
(a brownish pigment from broken-down blood), which contributes to the lesion's clinical color
- normal or ulcerated overlying surface epithelium
Epulis Fissuratum (Inflammatory fibrous hyperplasia; denture epulis)14
A reactive overgrowth of fibrous connective tissue in response to an ill-fitting denture
Aetiology
- Trauma from an overextended or ill-fitting denture
Clinical features14
- In the alveolar vestibule adjacent to a denture flange
- more frequently along the anterior vestibule
Histopathology15
- A hyperplasic mass of fibrous connective tissue
- often with folds and grooves
- Hyperplastic, hyperkeratotic, or ulcerated surface epithelium
Treatment67
- Surgical excision of the excess tissue.
- Fabrication of a new, properly fitting denture is required to prevent recurrence. In some cases, pre-prosthetic surgery to improve the bone contour may be needed.
Reactive Gingival Nodules16
Differential Diagnosis by Appearance
The microscopic composition of these nodules directly influences their clinical appearance (color, consistency), which aids in differential diagnosis.
Diagnosis
| Condition | Appearance | Key Histological Features |
|---|---|---|
| Fibroma | Pink, pale, and firm | Densely collagenous fibrous tissue, scattered vessels, variable edema/inflammation. |
| Pyogenic granuloma | Red/purple, soft, bleeds easily | Proliferation of endothelial cells and small, dilated capillaries, often ulcerated and inflamed. |
| Peripheral ossifying fibroma | Pink or red and firm | Spindled fibroblast-like cells with deposition of osteoid, woven bone, or cementum droplets. |
| Peripheral giant cell granuloma | Reddish-purple or blue and firm | Proliferation of monocytic and multinucleate giant cells (osteoclast-like), fresh hemorrhage, hemosiderin deposits. |
Inflammatory Papillary Hyperplasia (Denture Papillomatosis)17
- A pebbly overgrowth of the oral mucosa, usually occurs beneath a denture
Aetiology
- Ill-fitting denture, a denture that is worn 24 hours a day, or denture stomatitis
Clinical features10
-
Multiple, pink to red, edematous or fibrous papules
-
On the hard palate beneath a denture base
- mainly the palatal vault
Microscopy13
- Multiple papules of edematous fibrous connective tissue
- Normal or hyperplastic surface epithelium
Treatment67
- Improving denture hygiene, removing the denture at night, and treating any fungal infection.
- In advanced cases, surgical removal of the hyperplastic tissue is necessary before fabricating a new denture.
Epulis18
- Epulis = a growth arising from the gingiva
- it means “on the gum”
- Often used to describe localized hyperplastic gingival lesions
- Fibrous epulis (firm mass on the gingiva)
- Vascular epulis (angiogranuloma on the gingiva)
- Fibrous epulis with calcification (peripheral ossifying fibroma)
- Giant-cell epulis (peripheral giant cell granuloma)
- Denture epulis (epulis fissuratum)
Outdated Theory
An old, unsupported theory suggested that these lesions could progress from one type to another (e.g., starting as a vascular epulis and becoming more fibrous over time). This hypothesis is not validated by current evidence.
Generalized gingival enlargements
| Lesion or condition | Special characteristics |
|---|---|
| Hyperplastic gingivitis | Examples: associated with puberty, pregnancy, diabetes |
| Drug-related gingival hyperplasia | Examples: phenytoin, calcium channel blockers cyclosporine; may be fibrotic |
| Gingival fibromatosis | May be hereditary; onset in childhood |
| Leukemic infiltrate | Gingival swelling and bleeding |
| Wegener’s granulomatosis (granulomatosis with polyangitis) | ‘Strawberry gingivitis’; may have palatal ulceration and destruction of kidney, lung or nasal septum involvement; often with a skin rash, conjunctivitis or hearing loss |
| Scurvy | Vitamin C deficiency |
Giant Cell Fibroma19
- A variant of fibroma with distinctive features
Nature
This is considered a benign neoplasm, not a reactive lesion.
-
Compared to the common “irritation” fibroma:
- does not appear to be caused by trauma
- occurs most frequently on the gingiva
- many demonstrate rough, papillary surface
- can be mistaken for a papilloma
- large stellate, multinucleated fibroblasts microscopically
-
These are distinct from the osteoclast-type giant cells seen in a peripheral giant cell granuloma.
Retrocuspid Papilla
- Small, pink papules on the lingual gingiva of the lower cuspids
- frequently bilateral lesions
- microscopic features similar to giant cell fibroma
- do not require excision
Vascular Anomalies [Hemangiomas and Vascular Malformations]20
Clinical Caution
Lesions with a significant vascular component pose a risk of bleeding. If unsure of the diagnosis or management, it is best to refer the patient to a specialist.
Major types: ▪vascular tumours and vascular malformations
Classification of Vascular Anomalies
Vascular Tumours
- Infantile Hemangioma
- Superficial
- Deep
- Congenital Hemangioma▪
- Noninvoluting congenital hemangioma (NICH)
- Rapidly involuting congenital hemangioma (RICH)
Vascular Malformations
- Capillary malformation
- Venous malformation
- Arteriovenous malformation
- Lymphatic malformation
Common Malformation: Lingual Varices
These are very common, especially with aging. They appear as dilated, purple veins on the ventral surface of the tongue and can be accidentally lacerated during dental procedures, leading to bleeding.
General Features21
Hemangiomas
- Benign tumors
- the most common tumors of infancy
- Most lesions are not present at birth (arise during the first 8 weeks of life)
- few present at birth
- Display a rapid growth phase (endothelial cell proliferation)
- typically followed by gradual involution
- some show rapid involution or do not undergo involution
Vascular Malformations 20
- Hamartomatous growths composed of blood or lymphatic vessels with normal endothelial cell turnover
- Present at birth and persist throughout life
- Categorized according to the type of vessel involved into:
- capillary, venous, or arteriovenous, or lymphatic
- Categorized according to the hemodynamic features into:
- low-flow vs. high-flow
Congenital Hemangioma22
Info
This is a type of vascular tumor (hamartoma) that can be superficial or deep and appears as red plaques.
- Present at birth
- Subtypes:
- Rapidly involuting congenital hemangioma (RICH)
- shows rapid regression, with full involution by 9 to 14 months of age
- Noninvoluting congenital hemangioma (NICH)
- does not undergo involution
- Rapidly involuting congenital hemangioma (RICH)
Microscopy
- Early phase – a proliferation of plump endothelial cells forming indistinct vascular lumina
- Mature phase – capillary-sized vascular spaces lined by flattened endothelial cells
- Involution phase – get replaced by fibrous connective tissue
Venous Malformation23
- Low-flow anomaly
Clinical features
-
Blue-purple mass
- present at birth
- thrombi and phleboliths can form within (because of slow blood flow)
-
==A common example is lingual varices, which appear as dilated, tortuous, purple veins on the ventral (underside) and lateral borders of the tongue.==
-
They are considered a variation of normal anatomy that becomes more prominent with age.
-
==Clinical Significance: Dentists should be aware of their presence to avoid accidental laceration during procedures, which can cause significant bleeding.==
Microscopy
- Dilated thin-walled veins
Treatment
- Observation, sclerotherapy, or surgical excision
- Sclerotherapy: injection of sclerosing agents into the lesion to induce fibrosis
Kaposi Sarcoma24
- A vascular malignancy caused by human herpes virus 8
Clinical Significance
It is highly relevant in dentistry as it can be an early oral sign of HIV/AIDS. A patient may present with this lesion before they are aware of their HIV status.
Etiology
- Human herpesvirus 8 (HHV-8)/Kaposi sarcoma-associated herpesvirus (KSHV)
Subtypes
I. Classic II. Endemic III. Iatrogenic (transplant-associated) IV. Epidemic (AIDS-related)
AIDS-Related Kaposi Sarcoma
Clinical
- Mainly manifests as multiple lesions on the skin or oral mucosa
- oral lesions are seen in more than 50% of patients
- Predilection for adult homosexual males
- Considered as an AIDS-defining cancer
Oral lesions25
-
strong predilection for the palate and gingiva
-
early lesions appear as purple macules ↔︎ plaques and nodules
-
==Classically, the lesion is described as raised, velvety, and black, blue, or purple.==
Microscopy13
- A cellular proliferation of spindle cells surrounding slit-like vascular spaces
Treatment67
- Often regresses with combined antiretroviral therapy (cART)
- Other options include surgery, irradiation, intralesional chemotherapeutic agents (e.g. vinblastine), intralesional sclerosing agents (sodium tetradecyl sulfate), and systemic chemotherapy
Footnotes
-
Original PDF page 1: L12 Connective Tissue disorders annotated, p.1 ↩
-
Original PDF page 3: L12 Connective Tissue disorders annotated, p.3 ↩
-
Original PDF page 4: L12 Connective Tissue disorders annotated, p.4 ↩
-
Original PDF page 5: L12 Connective Tissue disorders annotated, p.5 ↩
-
Original PDF page 6: L12 Connective Tissue disorders annotated, p.6 ↩
-
Original PDF page 7: L12 Connective Tissue disorders annotated, p.7 ↩ ↩2 ↩3 ↩4 ↩5
-
Original PDF page 8: L12 Connective Tissue disorders annotated, p.8 ↩ ↩2 ↩3 ↩4 ↩5
-
Original PDF page 9: L12 Connective Tissue disorders annotated, p.9 ↩
-
Original PDF page 11: L12 Connective Tissue disorders annotated, p.11 ↩
-
Original PDF page 12: L12 Connective Tissue disorders annotated, p.12 ↩ ↩2 ↩3
-
Original PDF page 13: L12 Connective Tissue disorders annotated, p.13 ↩
-
Original PDF page 14: L12 Connective Tissue disorders annotated, p.14 ↩
-
Original PDF page 15: L12 Connective Tissue disorders annotated, p.15 ↩ ↩2 ↩3
-
Original PDF page 16: L12 Connective Tissue disorders annotated, p.16 ↩ ↩2
-
Original PDF page 17: L12 Connective Tissue disorders annotated, p.17 ↩
-
Original PDF page 18: L12 Connective Tissue disorders annotated, p.18 ↩
-
Original PDF page 19: L12 Connective Tissue disorders annotated, p.19 ↩
-
Original PDF page 21: L12 Connective Tissue disorders annotated, p.21 ↩
-
Original PDF page 22: L12 Connective Tissue disorders annotated, p.22 ↩
-
Original PDF page 23: L12 Connective Tissue disorders annotated, p.23 ↩ ↩2
-
Original PDF page 24: L12 Connective Tissue disorders annotated, p.24 ↩
-
Original PDF page 25: L12 Connective Tissue disorders annotated, p.25 ↩
-
Original PDF page 26: L12 Connective Tissue disorders annotated, p.26 ↩
-
Original PDF page 27: L12 Connective Tissue disorders annotated, p.27 ↩
-
Original PDF page 28: L12 Connective Tissue disorders annotated, p.28 ↩