Oral Pathology module1
Salivary gland diseases
CLASSIFICATION OF SALIVARY GLAND DISEASES2
A. DEVELOPMENTAL
- Congenital aplasia/agenesis
- Congenital hypoplasia
- Atresia
- Aberrance / ectopic gland
- Diverticuli
- Accessory duct
- Congenital fistula
Anatomical Reminder
The lecture emphasizes the importance of understanding the anatomy and histology of both major salivary glands (Parotid, Submandibular, Sublingual) and minor salivary glands (600-1,000 distributed throughout the oral cavity).
B. INFLAMMATORY3
- ACUTE OR CHRONIC
- STAPHYLOCOCCAL
- STREPTOCOCCAL
- ACTINOMYCOSIS
- TUBERCULOSIS
- VIRAL INFECTION
- MUMPS
- CYTOMEGALO VIRUS INFECTION
- PARAINFLUENZA
- SARCOIDOSIS
- MELKERSON-ROSENTHAL SYNDROME
- ALLERGY
- SALIVARY FISTULA
- **POST IRRADIATION TO ORAL TUMOUR
Post-Radiation Sialadenitis
Radiation therapy for head and neck cancer causes significant salivary gland damage, leading to severe dysfunction and xerostomia.
**
C. SIALOLITHIASIS4
- DUE TO STRICTURE OF DUCT
- DUE TO TRAUMA OR INFECTION
- DUE TO SALIVARY STONE
- MUCOUS PLUG
D. CYSTS
- MUCOCELE
- RANULA
- LYMPHO EPITHELIAL CYST
- Commonly seen on the posterior side of the tongue.
- BRANCHIAL CYST
E. F. SIALADENOSIS
G. SJOGRENS SYNDROME5
**I. NEOPLASMS
Note
Salivary gland tumors are relatively uncommon but are challenging to diagnose and manage. The WHO classification is extensive, with the 2022 version listing 38 different entities.
**
BENIGN EPITHELIAL
- ADENOMA
- ONCOCYTOMA
- WARTHINS TUMOUR
- PLEOMORPHIC ADENOMA
MALIGNANT EPITHELIAL
- ADENOCARCINOMA
- MUCOEPIDERMOID CARCINOMA
- ADENOCYSTIC CARCINOMA
- ACINIC CELL CARCINOMA
- MALIGNANT PLEOMORPHIC ADENOMA
BENIGN MESENCHYMAL6
- HEMANGIOMA
- LYMPHANGIOMA
- NEUROFIBROMA
- SCHWANNOMA
- LIPOMA
MALIGNANT MESENCHYMAL
- RHABDOMYOSARCOMA
- HEMANGIOENDOTHELIOMA
OTHERS
- LYMPHOMA-HODGKINS & NON HODGKINS
- METASTATIC
Sialolithiasis (Salivary Stones)7
- Sialoliths are calcified and organic matter that form within the secretory system of the major salivary glands. The etiology of sialolith formation is still unknown;
- however, several factors contribute to stone formation. Inflammation, irregularities in the duct system, local irritants, and anti-cholinergic medications may cause pooling of saliva within the duct, which is thought to promote stone formation.
Etiology
Formation requires a central nidus or core (e.g., a cell or mucus plug) around which calcium salts can deposit in layers. Systemic conditions can contribute to their formation.
-
It is believed that a nidus of salivary organic material becomes calcified and gradually forms a sialolith.
-
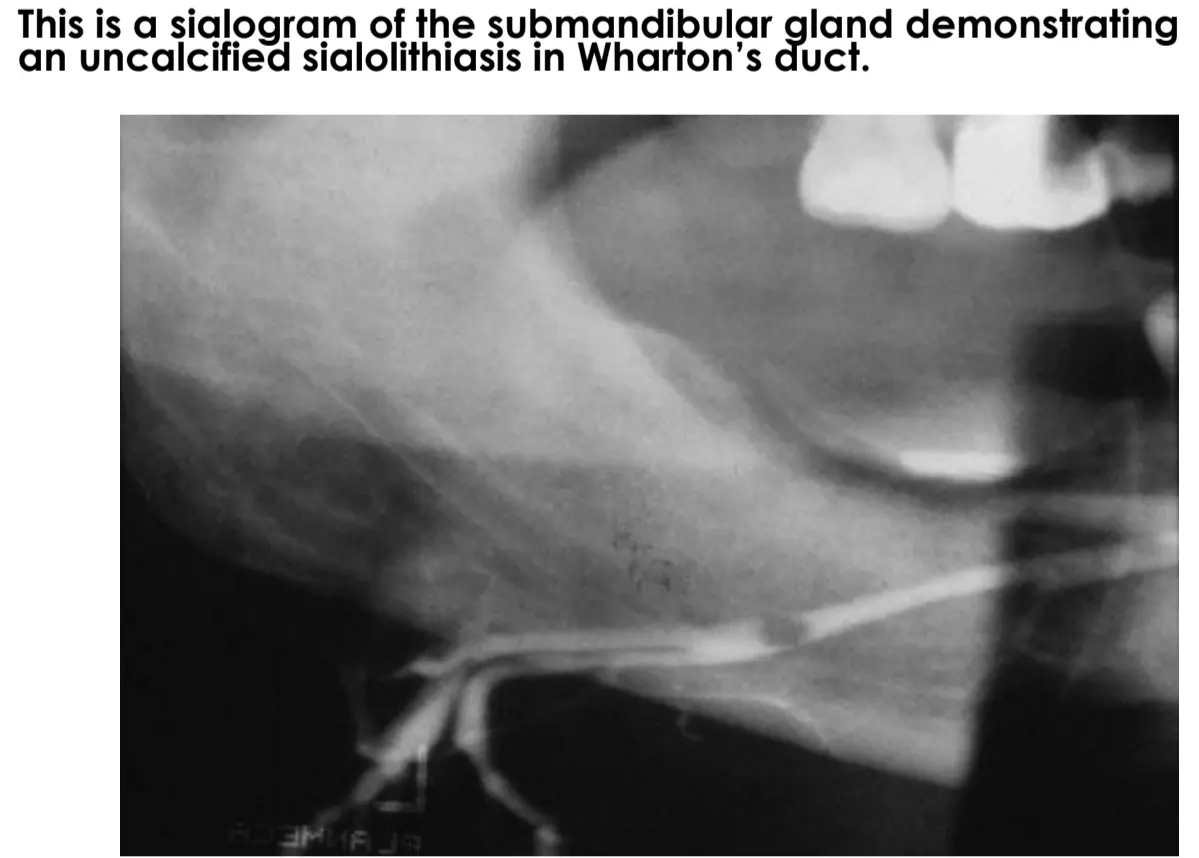
The submandibular gland is the most common site of involvement, and 80 to 90% of sialoliths occur in this gland.
-
Diagnosis: ==Imaging, such as a sialogram, is used to visualize the gland’s ductal system and identify blockages.==
-
-
Clinical Presentation: Can sometimes be palpated as a yellowish, firm, hard swelling within the duct.
-
Histopathology: ==The ductal epithelium may undergo metaplasia as an adaptive response to the chronic irritation and blockage.==
-
Treatment: ==Small, accessible stones can be removed with a simple incision. Deeper stones or extensive gland damage often require surgical removal of the entire gland (sialadenectomy).==
-
A) Lamellated calculi were found within the lumen of a dilated minor salivary duct
-
B) Squamous metaplasia of the excretory ductal epithelium and exfoliated epithelium were observed in the minor salivary glands
Mucocele8910
“Mucocele” is a clinical term that describes swelling caused by obstructed minor salivary gland duct.
Mucoceles are classified as
- Extravasation
- Retention types.
- A large form of mucocele located in the floor of the mouth is known as a RANULA.
Clinical Presentation
Extravasation mucoceles most frequently occur on the lower lip, where trauma is common. Buccal mucosa, tongue, floor of the mouth, and retro molar region are other commonly traumatized areas where mucous extravasation may be found. Mucous retention cysts are more commonly located on the palate or the floor of the mouth.
- Appears as a soft, bluish, dome-shaped swelling.
- The size can fluctuate; it may shrink as the body's inflammatory cells process the pooled mucin and then enlarge again as more saliva accumulates.
- If it ruptures, a clear, viscous fluid (saliva) is released.
Mucous extravasation cyst11
Epithelioid macrophages forming a pseudocyst around the extravasated mucin, no true epithelium is present.
Pathogenesis of Extravasation Cysts
- Cause: Trauma (e.g., lip or cheek biting) ruptures a salivary duct, causing saliva to spill into the surrounding connective tissue.
- Response: The spilled mucin acts as a foreign material, triggering an inflammatory response. A wall of granulation tissue containing phagocytes (macrophages) forms around the mucin.
- Histopathology: It is a pseudocyst because it lacks a true epithelial lining. Instead, it is lined by granulation tissue and inflammatory cells.
- Treatment: Surgical excision is required. It is crucial to remove the associated, damaged minor salivary glands to prevent recurrence.
Mucous Retention Cyst
This is a less common type where the cyst forms within the duct itself due to an obstruction, leading to ductal dilation. It is a true cyst with an epithelial lining.
XEROSTOMIA12
CAUSES OF XEROSTOMIA-
- TEMPORARY-psychological (anxiety), duct calculi, sialoadenitis, drug therapy( anticholinergic, sympathomimetic, etc.)
- PERMANENT-
- Salivary gland aplasia, sjogrens syndrome, following radio therapy, surgical desalivation
Info
Permanent xerostomia is caused by irreversible destruction of the salivary gland parenchyma (the saliva-producing tissue), which is replaced by fibrous or adipose tissue.
- Common
- Especially in middle to late life
- USA: 17% of 65-84 year olds had symptoms of oral dryness
- Europe: 29% of persons in a may have symptoms of dry mouth
BUT little correlation with objective measurements
Note
In Australia, it is estimated to affect around 20% of the population, with rates as high as 80% in patients over 65.
Causes1314
Common
- Drugs
- Radiotherapy to head and neck
- Sjogren’s syndrome
- Psychogenic?
- HCV disease?
- HIV disease?
Uncommon
- Chronic graft versus host disease
- Sarcoidosis
- Cystic fibrosis
- Diabetes mellitus
- Amyloidosis
- Haemochromatosis
- Wegener’s disease
- Salivary gland agenesis
- Triple A syndrome
- Cholinergic dysautonomia
- Others
Clinical Features15
-
Dysarthria
-
Dysphagia
-
Mucosal adhesion
-
“Stringy saliva”
-
Caries
-
==A glossy, atrophic appearance of the tongue.==
-
The dental mirror sticking to the buccal mucosa is a classic sign.
-
==Increased risk of dental caries, particularly cervical caries.==
-
==Increased susceptibility to oral infections, especially candidiasis.==
Discrete swelling in gland16
- Define location – clinical, imaging MRI – is it in the gland?
- Exclude infectious causes
- Fine needle aspiration
- Excisional biopsy if thought benign
- Incisional biopsy if thought malignant
Classification of salivary tumours1718
Benign:
- Pleomorphic adenoma
- Warthin’s tumour
Malignant:
- Mucoepidermoid carcinoma
- Polymorphous low-grade adenocarcinoma
- Adenoid cystic carcinoma
- Carcinoma ex pleomorphic adenoma
Site prevalence of salivary neoplasms19
- Parotid
- probably benign (85%)
- Submandibular
- probably benign (70%)
- Minor glands
- palate 45% malignant
- sublingual
- almost certainly malignant
Clinical Rule of Thumb
Any lump in a minor salivary gland, especially in the upper lip, should be considered suspicious for malignancy until proven otherwise.
Distinguishing Benign vs. Malignant Tumours2021
| Benign | Malignant |
| Circumscribed | Poorly circumscribed |
| Mobile | Fixed |
| Slow-growing | Induration (difficult) |
| Painless | Ulceration |
| Symptoms only cosmetic or pressure | Pain |
| Metastasis | |
| Nerve signs | |
| Sometimes rapid growth |
Key Distinctions
- Nerve Signs: The presence of numbness, paresthesia, or facial nerve palsy is a strong indicator of malignancy.
- Fixation: Malignant tumors are often fixed to adjacent structures, whereas benign tumors are mobile.
- Capsule: Benign tumors are typically encapsulated, while malignant ones are not.
Pleomorphic (salivary) adenoma22
- So-called ‘mixed tumour”
- Commonest salivary neoplasm
- Most in major glands but common in minor
- Benign (but may transform to malignancy)
- Encapsulated (but must not be enucleated)
- Painless, slow-growing
Malignant Transformation
While benign, if left untreated for many years (e.g., >10 years), it can transform into a highly aggressive Carcinoma ex Pleomorphic Adenoma, which has a very poor prognosis (patients often die within 18 months).
Cellular Origin
Arises from two cell types: intercalated duct cells and myoepithelial cells. The term “mixed tumour” is now obsolete.
Clinical features232425262728
- †Mean age – 40 yrs
- †Slight female predilection; 2:1
- Incidence in major and minor salivary glands is 10:1,
- Appears as a painless, slowly growing, smooth surfaced, dome shaped, firm mass
Histopathology Summary
The tumor is encapsulated and shows a pleomorphic (mixed) appearance with three main components:
- Epithelial Component: Duct-like or sheet-like structures formed by cuboidal cells.
- Myoepithelial Component: Cells can be spindle-shaped or have a distinct plasmacytoid (plasma cell-like) appearance.
- Stromal Component: The supporting connective tissue is highly variable and can be hyalinized (glassy), myxoid (mucoid), or even form cartilage (chondroid stroma).
Warthin’s tumour29303132
-
‘Adenolymphoma’ not a lymphoma!!
-
Almost all in parotid gland
-
Elderly patients
-
Benign, mobile, firm to fluctuant
-
Sometimes multiple
-
Encapsulated neoplasm
-
Synonym: Papillary cystadenoma lymphomatosum
-
Site: Tail of parotid
-
Bilateral occurrence
-
Age: 6th –7th decade
-
Male predominance
-
Associated with smoking
Macroscopic Appearance
The cystic fluid is often thick, brown, and described as ‘chocolate-like.’
- Varying proportions of papillary cystic structures lined by bilayered oncocytic epithelial cells and surrounded by a lymphoid stroma including germinal centers
Histopathology Summary
The name Papillary Cystadenoma Lymphomatosum describes its key features:
- Cystic Spaces: Contains multiple cysts with papillary projections.
- Epithelial Lining: A characteristic double layer of oncocytic epithelial cells.
- Lymphoid Stroma: The stroma is densely packed with lymphoid tissue, often forming germinal centers.
High power view showing papillary structures lined by bilayered oncocytic epithelial cells, surrounded by a lymphoid stroma
Mucoepidermoid carcinoma3334
- Most common
- Site: Major & minor salivary glands
- 2nd to 7th decade
- Female predilection
- Site:
- Palate
- Tuberosity
- Retromolar region
- Tongue
- Floor of the mouth
- Asymptomatic swelling + pain + facial nerve palsy
Histopathology
The name reflects its three cellular components:
- Muco- (Mucous cells): Cells with cloudy, pale cytoplasm that produce mucin.
- -epidermoid (Squamous cells): Islands of cells resembling stratified squamous epithelium.
- Intermediate cells: Smaller, basaloid-type cells. The tumor grows in a combination of solid sheets and cystic spaces.
1112/02 Mucoepidermoid carcinoma, low-grade
Adenoid cystic carcinoma353637
- Infrequent but very important
- May arise in any salivary gland
- Vague presenting symptoms (eg ‘funny feeling’)
- Slow-growing but highly infiltrative
- Late diagnosis common
- Good 5-year prognosis, very poor 15-year
Hallmark Feature: Perineural Invasion
This tumor has a strong tendency for perineural invasion (invading along nerve sheaths), which explains the common symptoms of pain and paresthesia (numbness) and is associated with a poorer prognosis.
- Synonym: Cylindroma
- Site: Minor salivary gland
- Age: Mid aged adults, 5th –7th decade
- Slow growing swelling
- Swelling + dull ache + facial nerve paralysis
- Late metastasis
- Prognosis: Worse
- Complications:
- CNS involvement
Adenoid cystic carcinoma
Questions38394041
- Slow growing swelling
- Swelling + dull ache + facial nerve paralysis
- Late metastasis
- Prognosis : Worse
- Complications :
- CNS involvement
Adenoid cystic carcinoma353637
Histopathology
- Composed of small, dark-staining basaloid cells.
- The cells arrange in various patterns, with the most classic being the cribriform (‘Swiss cheese’) pattern, featuring multiple small, punched-out cystic spaces.
- Perineural Invasion: Tumor cells can be seen surrounding and infiltrating nerve bundles, which is a key diagnostic feature.
Footnotes
-
Original PDF page 1: L13 SalivaryGlandDiseases, p.1 ↩
-
Original PDF page 4: L13 SalivaryGlandDiseases, p.4 ↩
-
Original PDF page 5: L13 SalivaryGlandDiseases, p.5 ↩
-
Original PDF page 6: L13 SalivaryGlandDiseases, p.6 ↩
-
Original PDF page 7: L13 SalivaryGlandDiseases, p.7 ↩
-
Original PDF page 8: L13 SalivaryGlandDiseases, p.8 ↩
-
Original PDF page 9: L13 SalivaryGlandDiseases, p.9 ↩
-
Original PDF page 10: L13 SalivaryGlandDiseases, p.10 ↩
-
Original PDF page 11: L13 SalivaryGlandDiseases, p.11 ↩
-
Original PDF page 12: L13 SalivaryGlandDiseases, p.12 ↩
-
Original PDF page 13: L13 SalivaryGlandDiseases, p.13 ↩
-
Original PDF page 14: L13 SalivaryGlandDiseases, p.14 ↩
-
Original PDF page 15: L13 SalivaryGlandDiseases, p.15 ↩
-
Original PDF page 16: L13 SalivaryGlandDiseases, p.16 ↩
-
Original PDF page 17: L13 SalivaryGlandDiseases, p.17 ↩
-
Original PDF page 18: L13 SalivaryGlandDiseases, p.18 ↩
-
Original PDF page 19: L13 SalivaryGlandDiseases, p.19 ↩
-
Original PDF page 20: L13 SalivaryGlandDiseases, p.20 ↩
-
Original PDF page 21: L13 SalivaryGlandDiseases, p.21 ↩
-
Original PDF page 22: L13 SalivaryGlandDiseases, p.22 ↩
-
Original PDF page 23: L13 SalivaryGlandDiseases, p.23 ↩
-
Original PDF page 24: L13 SalivaryGlandDiseases, p.24 ↩
-
Original PDF page 25: L13 SalivaryGlandDiseases, p.25 ↩
-
Original PDF page 26: L13 SalivaryGlandDiseases, p.26 ↩
-
Original PDF page 27: L13 SalivaryGlandDiseases, p.27 ↩
-
Original PDF page 28: L13 SalivaryGlandDiseases, p.28 ↩
-
Original PDF page 29: L13 SalivaryGlandDiseases, p.29 ↩
-
Original PDF page 30: L13 SalivaryGlandDiseases, p.30 ↩
-
Original PDF page 31: L13 SalivaryGlandDiseases, p.31 ↩
-
Original PDF page 32: L13 SalivaryGlandDiseases, p.32 ↩
-
Original PDF page 33: L13 SalivaryGlandDiseases, p.33 ↩
-
Original PDF page 34: L13 SalivaryGlandDiseases, p.34 ↩
-
Original PDF page 35: L13 SalivaryGlandDiseases, p.35 ↩
-
Original PDF page 36: L13 SalivaryGlandDiseases, p.36 ↩
-
Original PDF page 37: L13 SalivaryGlandDiseases, p.37 ↩ ↩2
-
Original PDF page 38: L13 SalivaryGlandDiseases, p.38 ↩ ↩2
-
Original PDF page 39: L13 SalivaryGlandDiseases, p.39 ↩ ↩2
-
Original PDF page 40: L13 SalivaryGlandDiseases, p.40 ↩ ↩2
-
Original PDF page 41: L13 SalivaryGlandDiseases, p.41 ↩ ↩2
-
Original PDF page 42: L13 SalivaryGlandDiseases, p.42 ↩ ↩2
-
Original PDF page 43: L13 SalivaryGlandDiseases, p.43 ↩ ↩2