Three types of candidal infection cause white patches and are relatively common.
Thrush (acute candidosis) is readily distinguishable from other white lesions. The patches can easily be wiped off, and the condition is sore.
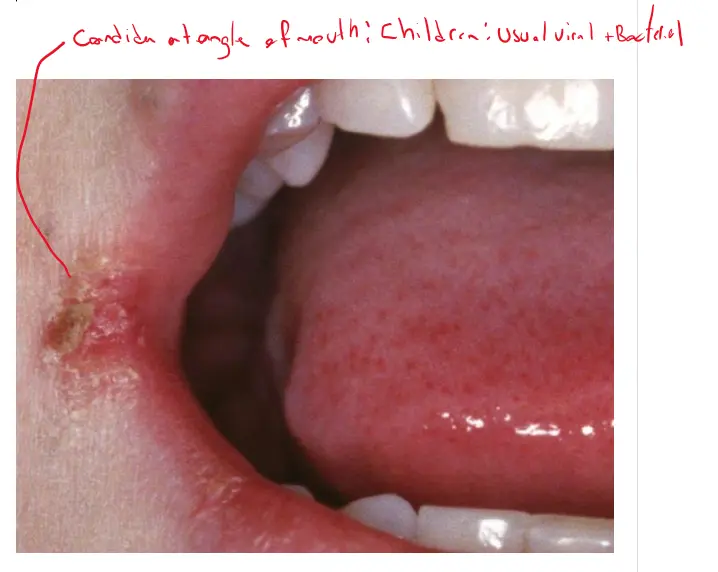
a. Common in babies because they don’t have a good microflora so its transferred from mother easily
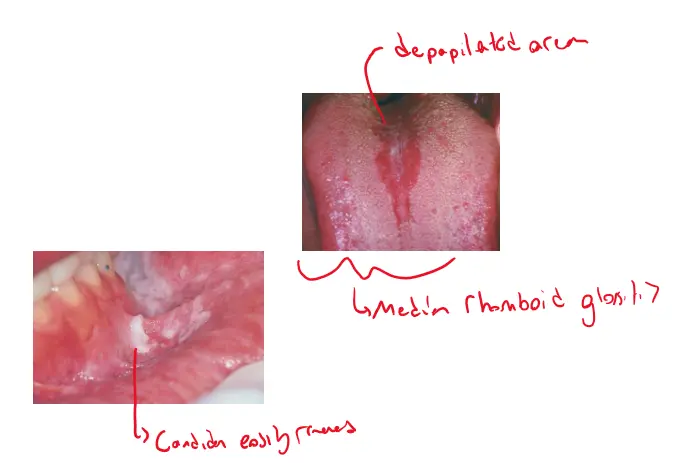
Chronic hyperplastic candidosis
chronic mucocutaneous candidosis
Candidosis forms discrete white plaques similar clinically to other types of leukoplakia
Tetracyclines (including the semisynthetic minocycline and doxycycline),
Quinoline antimalarial medications (including hydroxychloroquine, mepacrine, and quinacrine)
Psychotropic drugs such as retigabine, clofazimine and imatinib, a tyrosine kinase inhibitor.
Medication induced pigmentation falls under “Diffuse Mucosal Pigmentation”
Breakdown products of antimalarial drugs, minocycline, and imatinib chelate with iron or melanin and deposit within the lamina propria. Birth control pills lower cortisol levels and increase adrenocorticotrophic hormone (ACTH) levels, leading to the stimulation of melanocytes.
Discrete, usually solitary (sometimes multiple), tan-to-brown-to-black, painless macules are evenly pigmented, less than 1 cm, and frequently occur on the lower vermilion (labial melanotic macule, 33% of cases), gingiva and palatal mucosa, or buccal mucosa
[Multiple melanotic macules may be idiopathic Addison disease, and in syndromes such as the Laugier-Hunziker syndrome (with melanonychia)]{.underline}, neurofibromatosis, Peutz-Jeghers syndrome, McCune-Albright syndrome, Carney syndrome complex, LEOPARD
Relationship between Melanotic Macule, Postinflammatory Hypermelanosis, and Melanoacanthosis
Most common site is the palatal mucosa (34% to 44%), with other sites being the mucobuccal fold, buccal mucosa, lip vermilion, and gingiva.
They may be brown, blue-grey, black, or nonpigmented.
The frequency in the oral cavity is as follows: intramucosal nevus (64% to 80%), blue nevus (8% to 17%), and compound nevus (6% to 17%); junctional and combined nevi are uncommon.
Melanocytic nevi derive from melanocytes that originate from the neural crest.
This is a combination of intramucosal and junctional nevus with nests of benign melanocytes clustered within the lower part of the epithelium, often forming bulbous rete ridges
Clinically they look similar to melanotic macules but they have a different histological appearance
To identify a melanotic lesion clinically you have to rule out that its not vascular
If it disappears when pressed by glass then it’s a vascular lesion
Discrete proliferation of spindled melanocytes with variable melanin and benign spindled nuclei exhibiting dispersed chromatin and small nucleoli, scattered within densely collagenous stroma without hyperplasia of melanocytes within the epithelium
Comparison of Melanocytic Lesions
Macule
Nevi
Melanoacanthoma
OMM
Prevalence in melanocytic lesions
62% (48, 49)
15% (48, 49)
0.8% (48, 49)
0.7% (48, 49)
Color
Gray to brown to black
Brown, bluish-gray or black, 15% non-pigmented 0.5cm
Brown or black
Variable
Size (mean diameter)
<1 cm
Several centimeters
4 cm
Shape
Flat, solitary & well-circumscribed
Well-demarcated but elevated
Flat or slightly raised
Asymmetric with irregular outline
Commonly occurred site
Lip & gingiva
Palate
Buccal mucosa
Hard palate & maxillary gingiva
Causative factor
Melanin deposition
Proliferation of melanocytes
Proliferation of keratinocytes & melanocytes
Uncontrolled growth of melanocytes
Histopathologic features
Melanin accumulation without an increase in melanocytes.
Polygonal & epithelioid nevus cells in the superficial. Cytoplasm transparent to light stained.
Many dendritic melanocytes, processes containing melanin & melanophagocytes in all strata of epithelium.
Large, vesicular nucleus & prominent nucleoli. Aggregated into sheets or alveolar groups. Neurotropic or desmoplastic configurations.
Diagnostic Flowchart: Single White Spot or Plaque
Question: Has a topical drug recently been applied to the area?
Yes: Chemical burn
No:
Question: Is it made out of stripes or papules or a spot or plaque on the dorsum of the tongue?
Yes: Lichenoid lesions or early lichen planus
No:
Question: Is it on the palate with small red spots?
Yes: Stomatitis nicotina
No:
Question: Is it on the edge of the tongue?
Yes:
Question: Is it formed of parallel white stripes perpendicular to the edge?