Case 1 : Pyogenic Granuloma
 Of course. Let’s break down where each of these microscopic features can be seen on your slides. The features described are classic for a pyogenic granuloma, also known as a lobular capillary hemangioma.
Of course. Let’s break down where each of these microscopic features can be seen on your slides. The features described are classic for a pyogenic granuloma, also known as a lobular capillary hemangioma.
Here is a guide to identifying those features on your images:
🔬 Low Magnification View (Top Image)
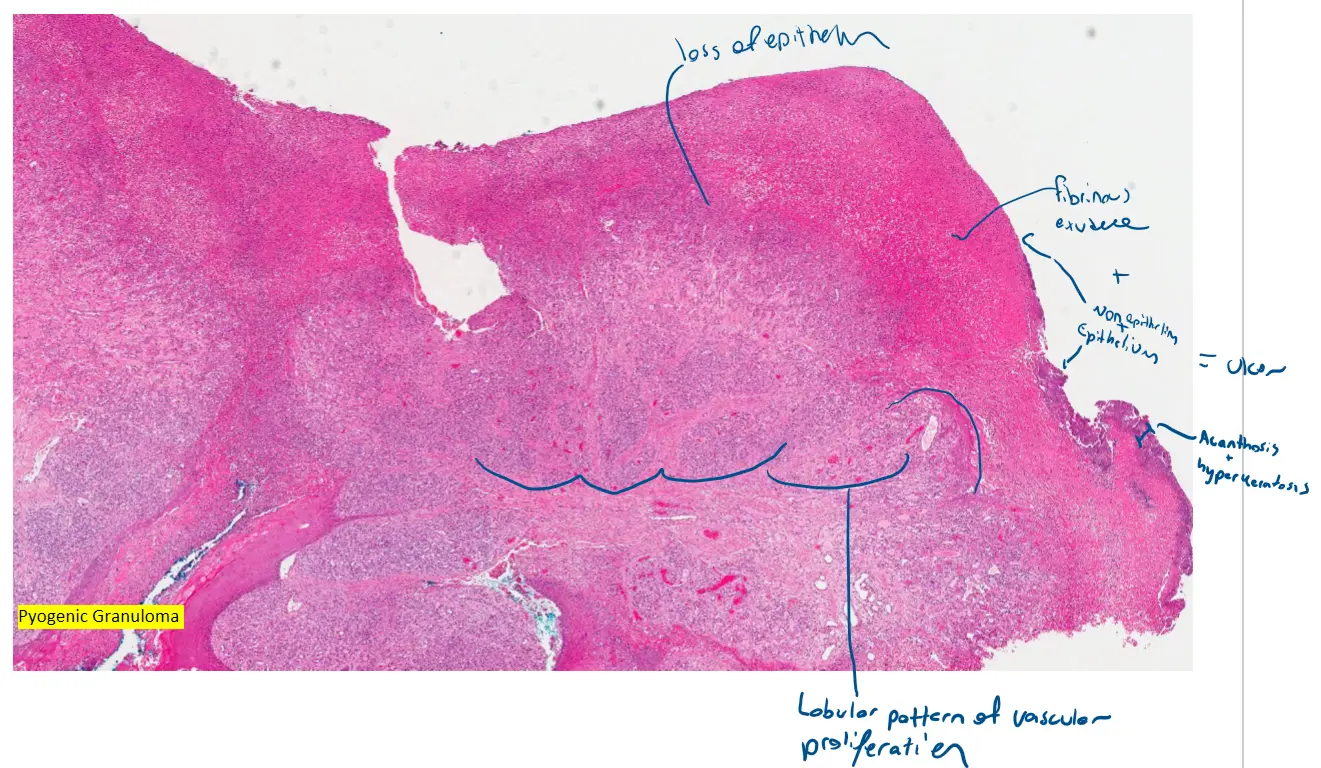
This image provides the overall architecture of the lesion.
-
Lobular pattern of vascular proliferation: The entire pink and purple mass growing underneath the surface layer is composed of these lobules. You can see it’s arranged in distinct clusters or nodules, especially in the upper half.
-
Thin epidermis at top with variable ulceration: Look at the very top surface. In the center, the surface layer (epidermis) is completely missing, which is the ulceration. To the right and left of the ulcer, you can see the epidermis is stretched and very thin over the dome of the lesion.
-
Acanthosis and hyperkeratosis at sides: At the “shoulders” or edges of the lesion, you can see the epidermis thickens and grows downwards, appearing to cup or “hug” the base of the lesion. This border is called an epidermal collarette and is the site of the acanthosis (thickening) and hyperkeratosis (extra keratin).
-
Deep lesions often lack edema and inflammation: Compare the top of the lesion (just under the ulcer) with the bottom. The top portion appears more purple and has more space between the cell clusters due to inflammation and edema. The deeper part at the very bottom of the image appears more compact, solid, and pink, with less inflammation.
🔬 High Magnification View (Middle Image)
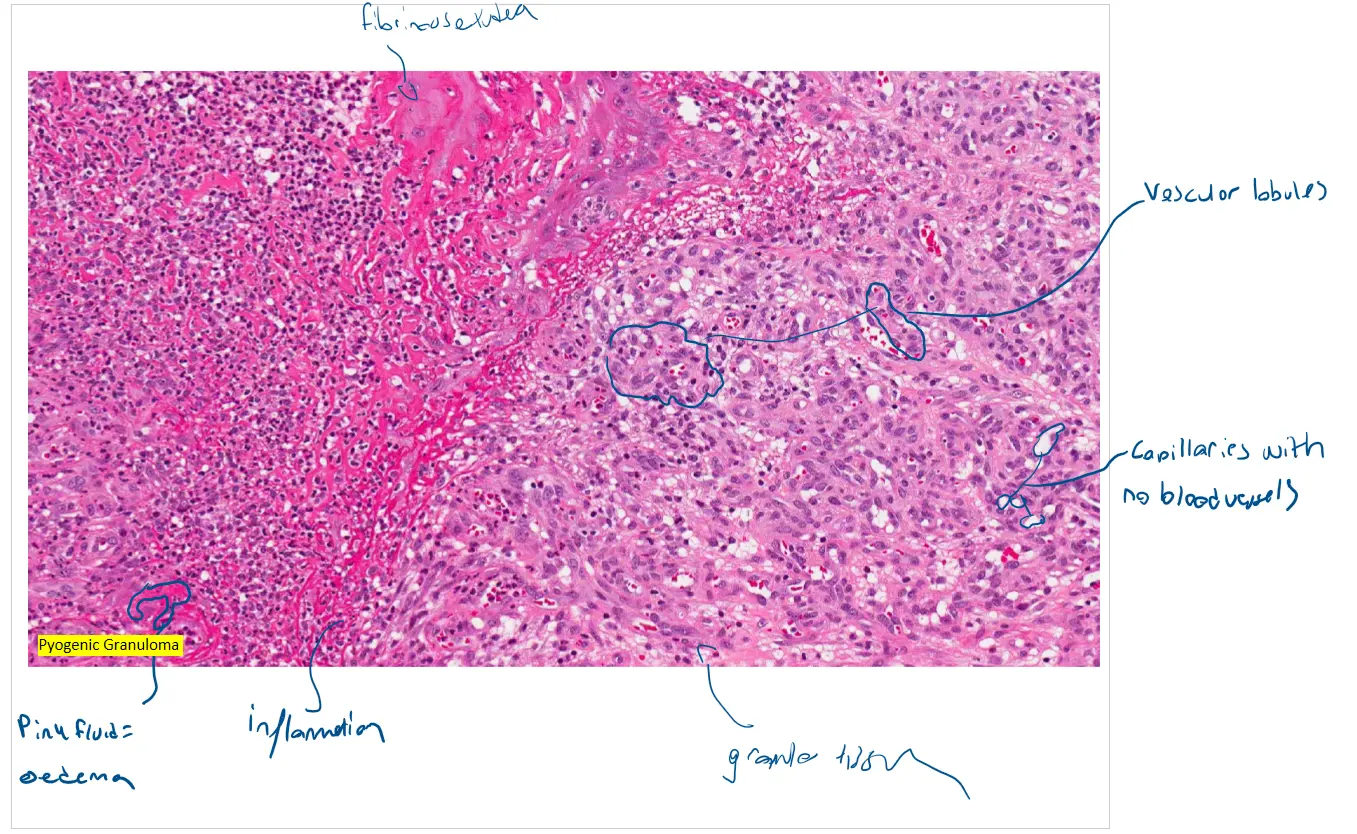
This image zooms in on the lobules themselves.
-
Vascular lobule… surrounded by endothelial cells: The entire field of view is filled with these vascular lobules. They are the well-defined clusters of cells with many purple nuclei. The cells that make up these lobules are the endothelial cells.
-
Central branching vessel… with no/rare red blood cells: Within the lobules, you can see small, slit-like or circular white spaces. These are the capillaries (the small vessels). Notice that they are mostly empty and do not contain many red blood cells (which would appear as bright pink circles).
-
Inflammation and edema: The cells scattered between the lobules are the inflammatory cells (the small, dark purple dots). The pale pink, slightly separated background in these inflammatory areas is the edema (fluid buildup).
-
Variable mitotic activity: Mitotic figures (cells in the process of dividing) would appear as small, very dark, and irregularly shaped nuclei within the endothelial cells of the lobules. They can be difficult to spot without very high magnification but are expected to be present in this type of lesion.
In summary, the images you provided are excellent examples that clearly display all the microscopic features listed. The top image shows the overall lobular structure and its relationship with the epidermis, while the middle image shows the detailed composition of the capillaries, endothelial cells, and inflammation.
Would you like me to explain the clinical significance of these findings or what typically causes a pyogenic granuloma?
Case 2 Fibroepithelial Polyp
 Of course. Here is a breakdown of the features for the fibroepithelial polyp, commonly known as a skin tag or acrochordon.
Of course. Here is a breakdown of the features for the fibroepithelial polyp, commonly known as a skin tag or acrochordon.
This is a benign lesion characterized by a core of connective tissue covered by skin.
🔬 Low Magnification View (Top Image)
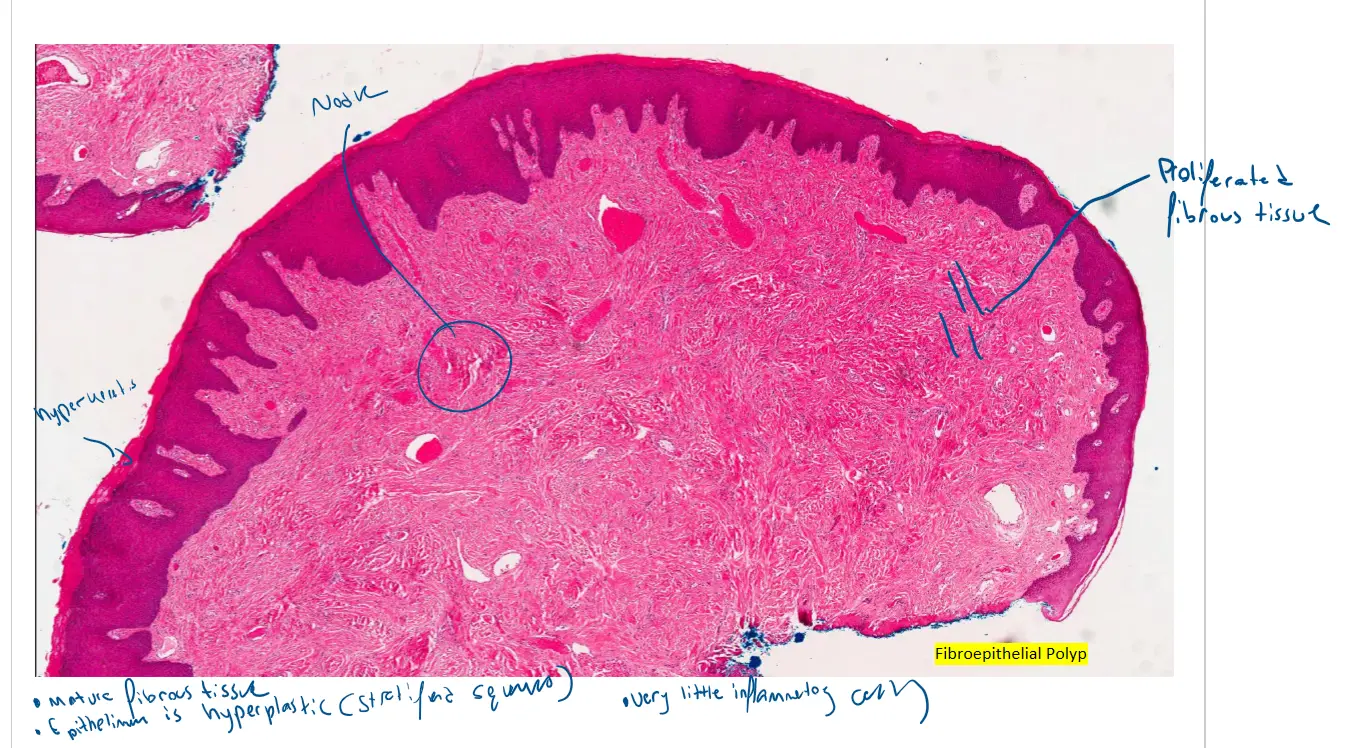
This view shows the overall structure of the polyp, which is a stalk-like projection of skin.
-
Fibrous tissue proliferation: The entire central core of the polyp—the extensive pink area beneath the dark purple surface layer (epidermis)—is the proliferated fibrous tissue. This mature, collagen-rich tissue makes up the bulk of the lesion and gives it its substance.
-
Inflammatory infiltrate: In this view, the inflammatory infiltrate is very subtle. It would be seen as a sparse collection of tiny, dark purple dots within the pink fibrous core, most likely just beneath the epidermis. These are often present due to minor irritation or trauma to the skin tag.
🔬 High Magnification View (Middle Image)
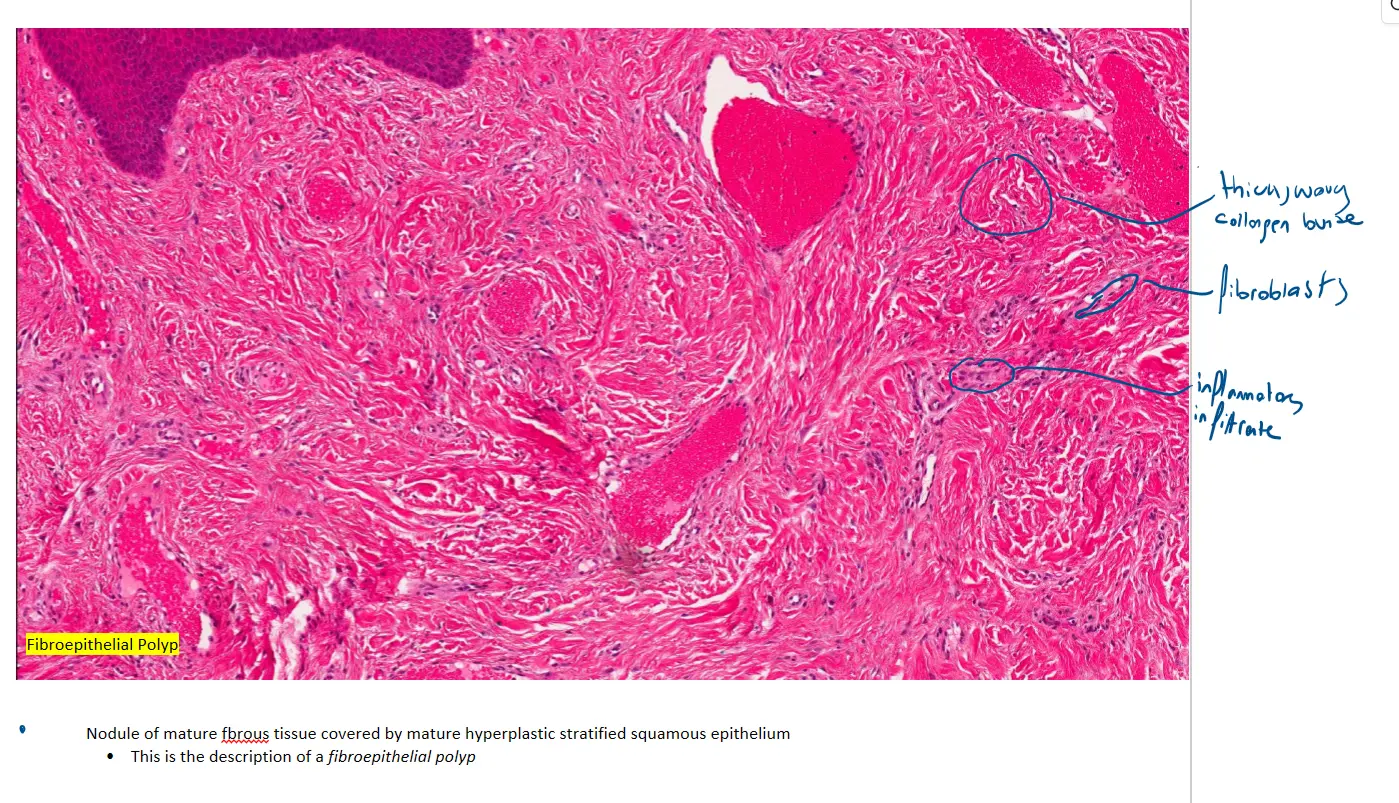
This image zooms into the fibrous core, revealing its composition.
-
Fibrous tissue proliferation: This view provides a perfect look at the fibrous tissue. It is composed of thick, wavy, pink bundles of collagen. The small, elongated or spindle-shaped purple nuclei scattered throughout are the fibroblasts, which are the cells that produce the collagen.
-
Inflammatory infiltrate: You can more clearly see the mild inflammatory infiltrate here. Look for the small, round, dark purple cells, which are distinct from the paler, flatter fibroblast nuclei. They are sparsely scattered, often clustering around the small blood vessels visible in the tissue.
In summary, your images clearly show a polypoid structure with a core made of mature, collagenous fibrous tissue and a sparse inflammatory infiltrate, which are the key features of a fibroepithelial polyp.
Would you like to compare the key differences between this fibroepithelial polyp and the pyogenic granuloma from the previous example?
Case 3 : Denture Related Hyperplasia
 Certainly. Let’s go through the features of this denture-related hyperplasia, a condition also known as inflammatory fibrous hyperplasia or epulis fissuratum. This is a reactive growth of tissue caused by chronic irritation from the edge of an ill-fitting denture.
Certainly. Let’s go through the features of this denture-related hyperplasia, a condition also known as inflammatory fibrous hyperplasia or epulis fissuratum. This is a reactive growth of tissue caused by chronic irritation from the edge of an ill-fitting denture.
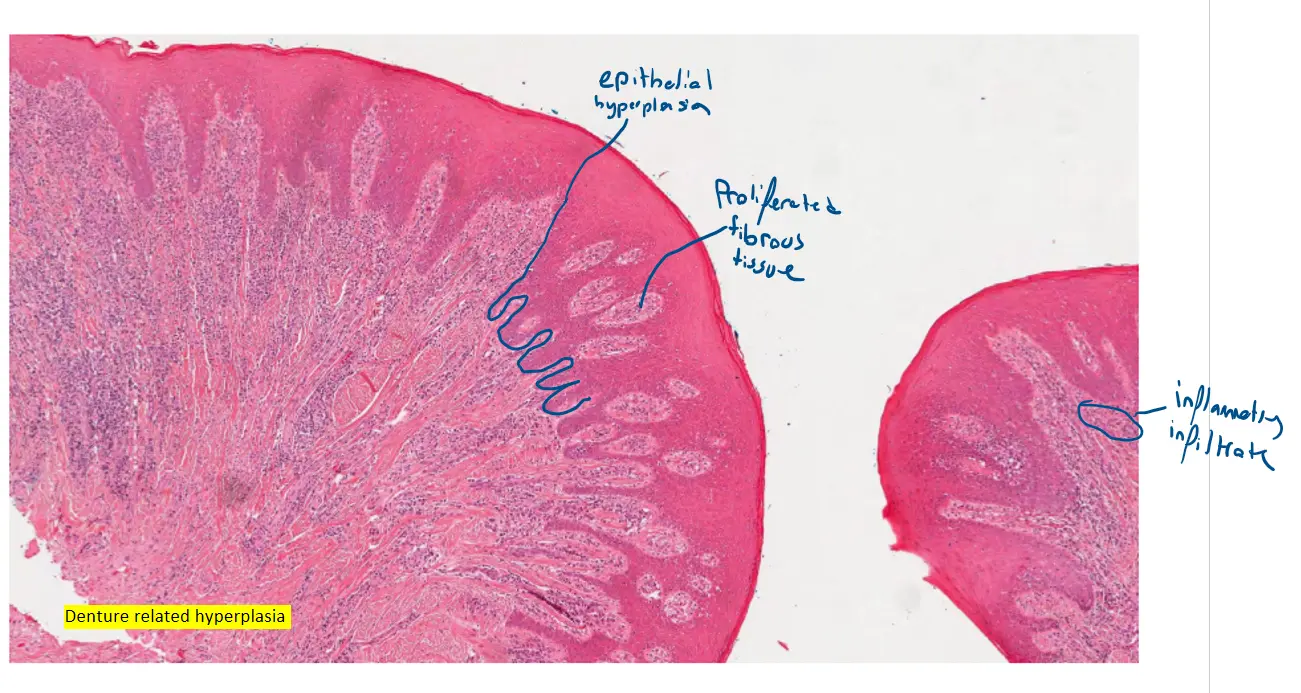
🔬 Low Magnification View (Top Image)
This image shows the characteristic folded, leaf-like overall structure of the lesion.
-
Epithelial hyperplasia: The most striking feature here is the markedly thickened, dark purple surface layer (the epithelium). Note how it grows downwards into the underlying tissue in long, thin, and sometimes interconnected, finger-like projections. This is a very prominent form of epithelial hyperplasia.
-
Fibrous tissue proliferation: The pink tissue that forms the core of these folds is the proliferated fibrous tissue. This is the bulky connective tissue that makes up the mass of the lesion, lying underneath the hyperplastic epithelium.
-
Inflammatory infiltrate: You can clearly see a dense, dark purple band of cells within the pink fibrous tissue, concentrated just below the epithelium. This represents a significant inflammatory infiltrate, which is expected given the chronic irritation that causes this lesion.
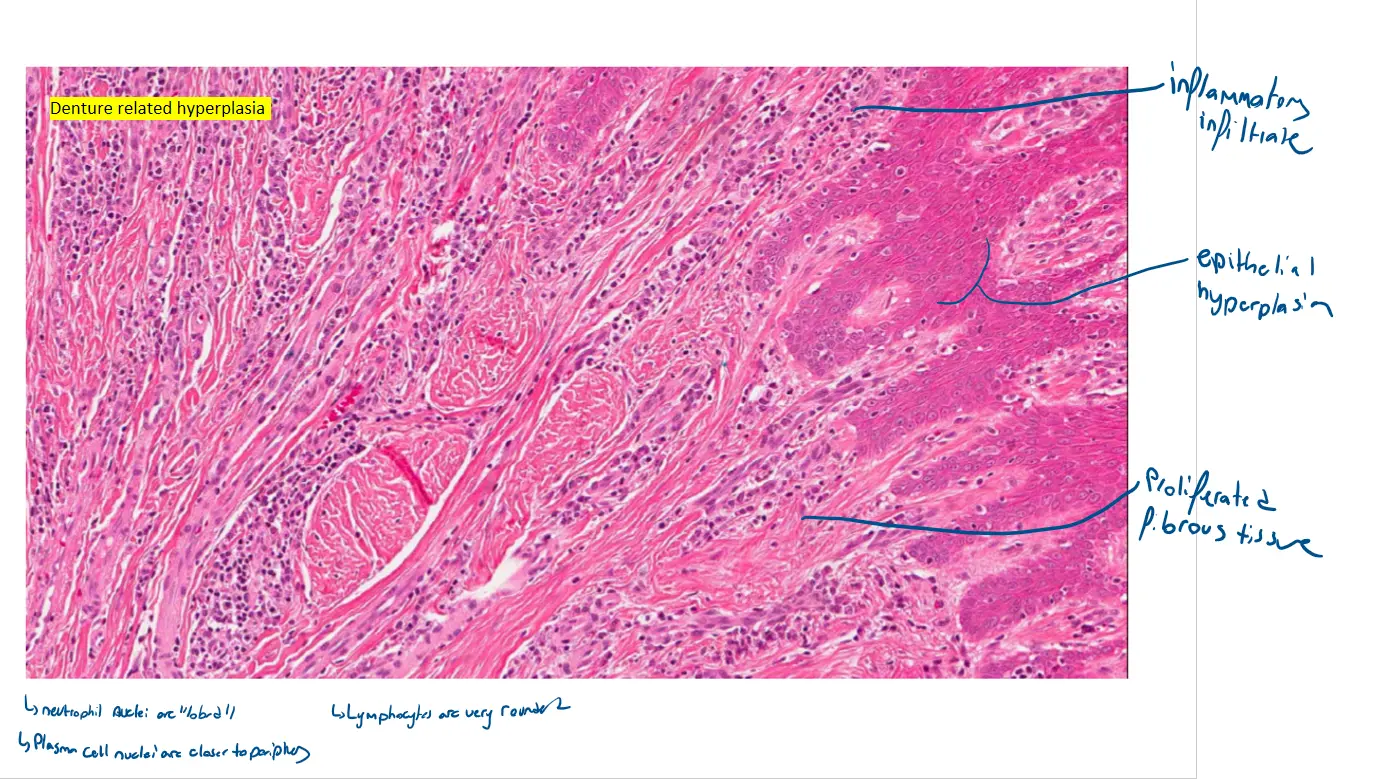
🔬 High Magnification View (Middle Image)
This is a close-up view of the fibrous core and the inflammatory cells within it.
-
Epithelial hyperplasia: The thick epithelial layer can be seen at the top right of this image.
-
Fibrous tissue proliferation: The majority of the image is composed of the fibrous tissue. You can see the pink, wavy bundles of collagen that have proliferated to form the lesion.
-
Inflammatory infiltrate: This view provides an excellent look at the dense inflammatory infiltrate. It is composed of the numerous small, round, dark purple cells that are heavily interspersed within the pink fibrous tissue. The presence of such a heavy, chronic inflammatory infiltrate is a key feature of this reactive process.
In essence, your images perfectly demonstrate the tissue’s reaction to chronic irritation: the surface epithelium thickens and grows downward, while the underlying connective tissue expands with both fibrous tissue and a heavy infiltration of inflammatory cells.
Would you like to explore the clinical management for this condition, or compare the epithelial changes seen here with the previous examples?
Case 4: Schwannoma (neurilemoma)
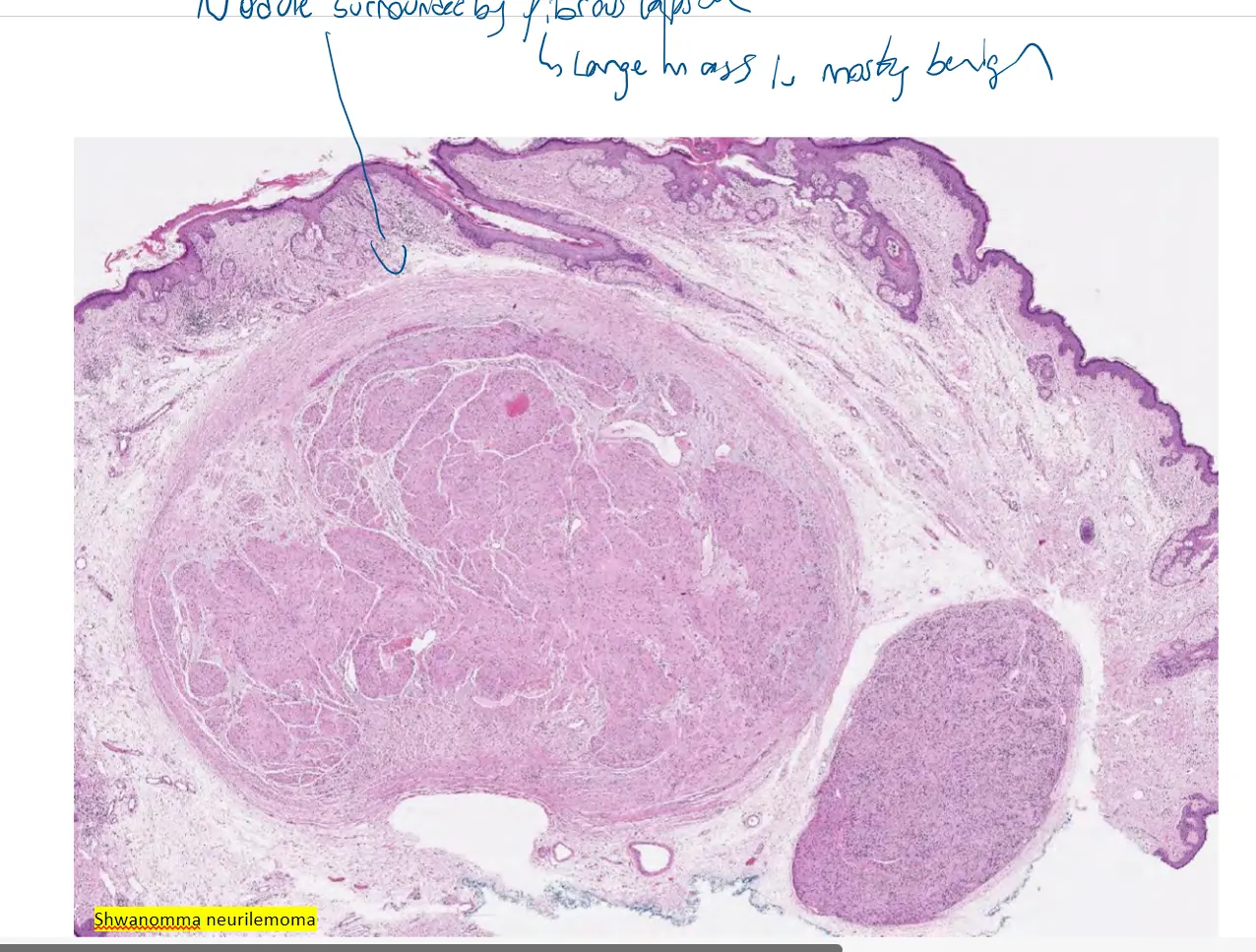
 Of course. Let’s break down the microscopic features for this schwannoma.
Of course. Let’s break down the microscopic features for this schwannoma.
This is a benign tumor that arises from Schwann cells, which are responsible for producing the myelin sheath that covers peripheral nerves. The image you’ve provided is a classic example.
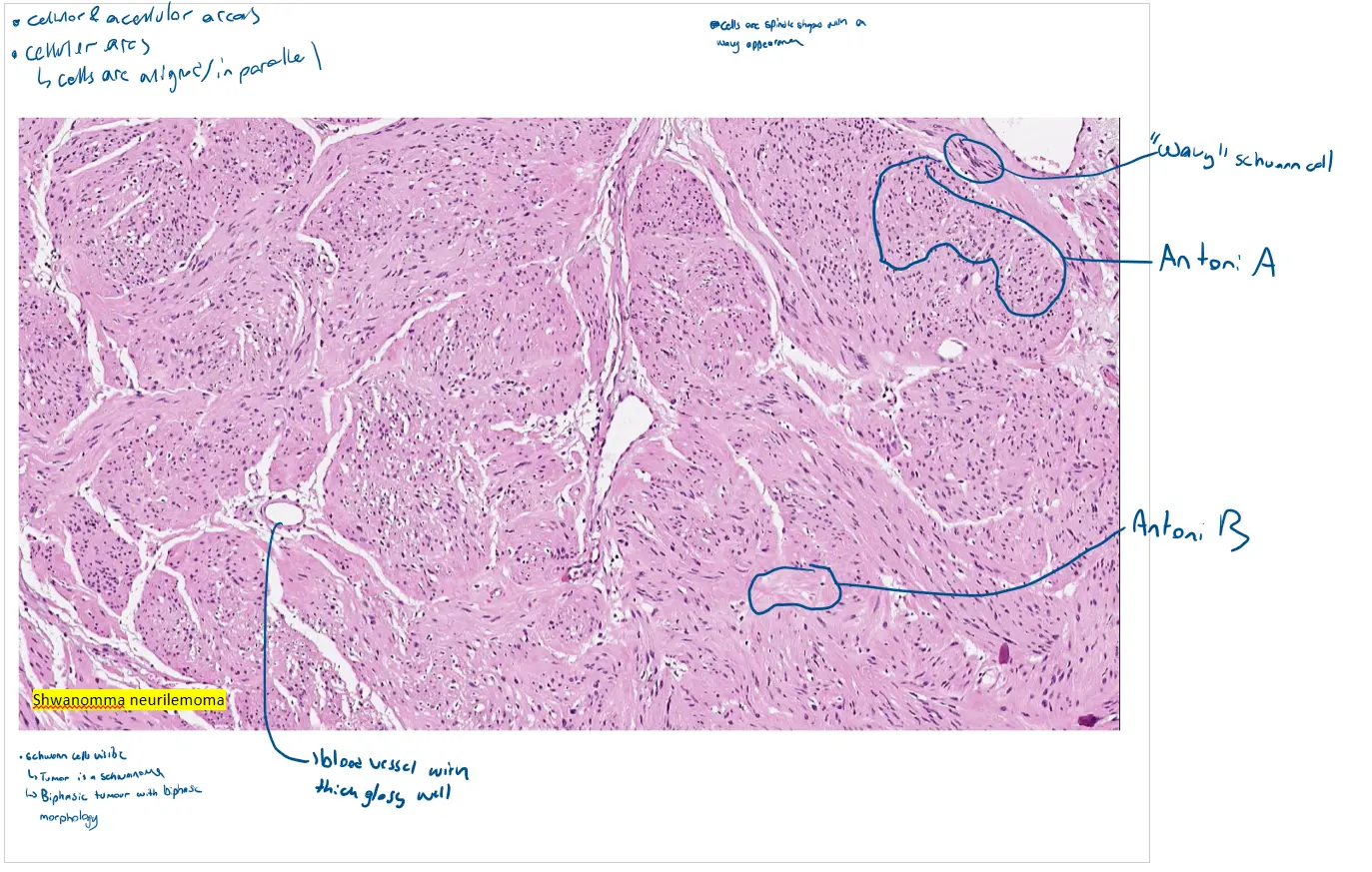
🔬 Analysis of the Microscopic View
Your image is a medium-power view that beautifully displays the key architectural patterns of a schwannoma.
-
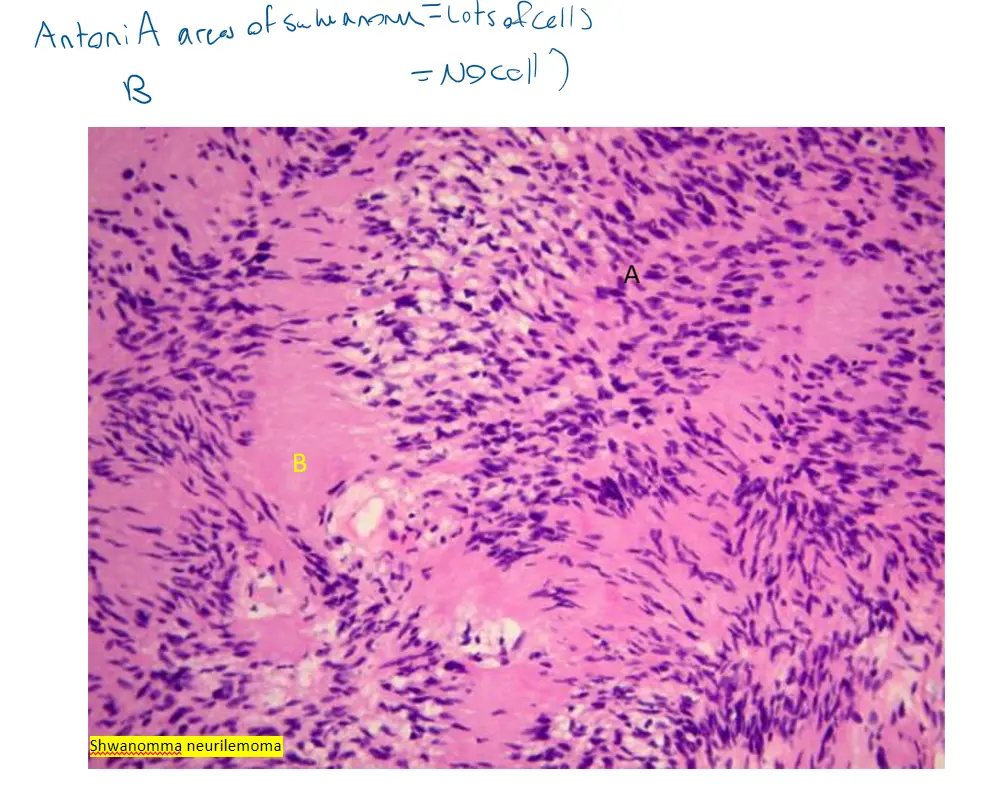
Biphasic: compact hypercellular Antoni A areas and myxoid hypocellular Antoni B areas: This is the most important low-power feature, and it is clearly visible across the entire image.
-
Antoni A areas: These are the dense, highly cellular regions that appear more intensely pink and purple. They are composed of compact, swirling bundles (fascicles) of spindle cells. You can see these areas making up most of the tissue in the upper left, center, and bottom of the image.
-
Antoni B areas: These are the looser, paler, and less cellular (hypocellular) regions. Notice the areas, particularly in the right-middle portion of the image, where the cells are spread apart in a pale pink, edematous background.
-
-
Nuclear palisading around fibrillary process (Verocay bodies): This is the hallmark feature of a schwannoma and is found within the Antoni A areas. While a perfect, textbook Verocay body isn’t in sharp focus, the characteristic pattern is definitely present. Look within the dense Antoni A areas for zones where the elongated nuclei align themselves in parallel rows (a pattern called palisading). The pink, cell-free zones between these rows of nuclei are the “fibrillary processes” that make up the Verocay body.
-
Cells are narrow, elongate, wavy with tapered ends: This describes the individual Schwann cells. If you look closely within the Antoni A areas, you can see the nuclei are not straight but have a characteristic wavy, “serpentine,” or buckled appearance with pointed ends.
-
Large irregularly spaced vessels: Notice the prominent blood vessel in the upper central part of the image. It is large and has a very thick, pink, hyalinized (glassy) wall. This type of vessel is very characteristic of schwannomas.
-
Other features:
-
Degenerative nuclear atypia (ancient change): This refers to some tumor cells having very large, dark, and bizarrely shaped nuclei. While not prominent in this specific field, it’s a common finding and does not indicate malignancy.
-
Rare mitotic figures, no axons: As a benign tumor, schwannomas have very low mitotic activity. Axons (the functional part of a nerve) are not found within the tumor itself because the tumor grows from the sheath and pushes the nerve aside.
-
In summary, your image is an excellent illustration of a schwannoma, perfectly demonstrating the defining biphasic pattern of Antoni A and Antoni B areas, along with the beginnings of Verocay body formation and characteristic hyalinized blood vessels.
Would you like to discuss the clinical presentation of a schwannoma or how it differs from a neurofibroma, another common peripheral nerve sheath tumor?
Case 5
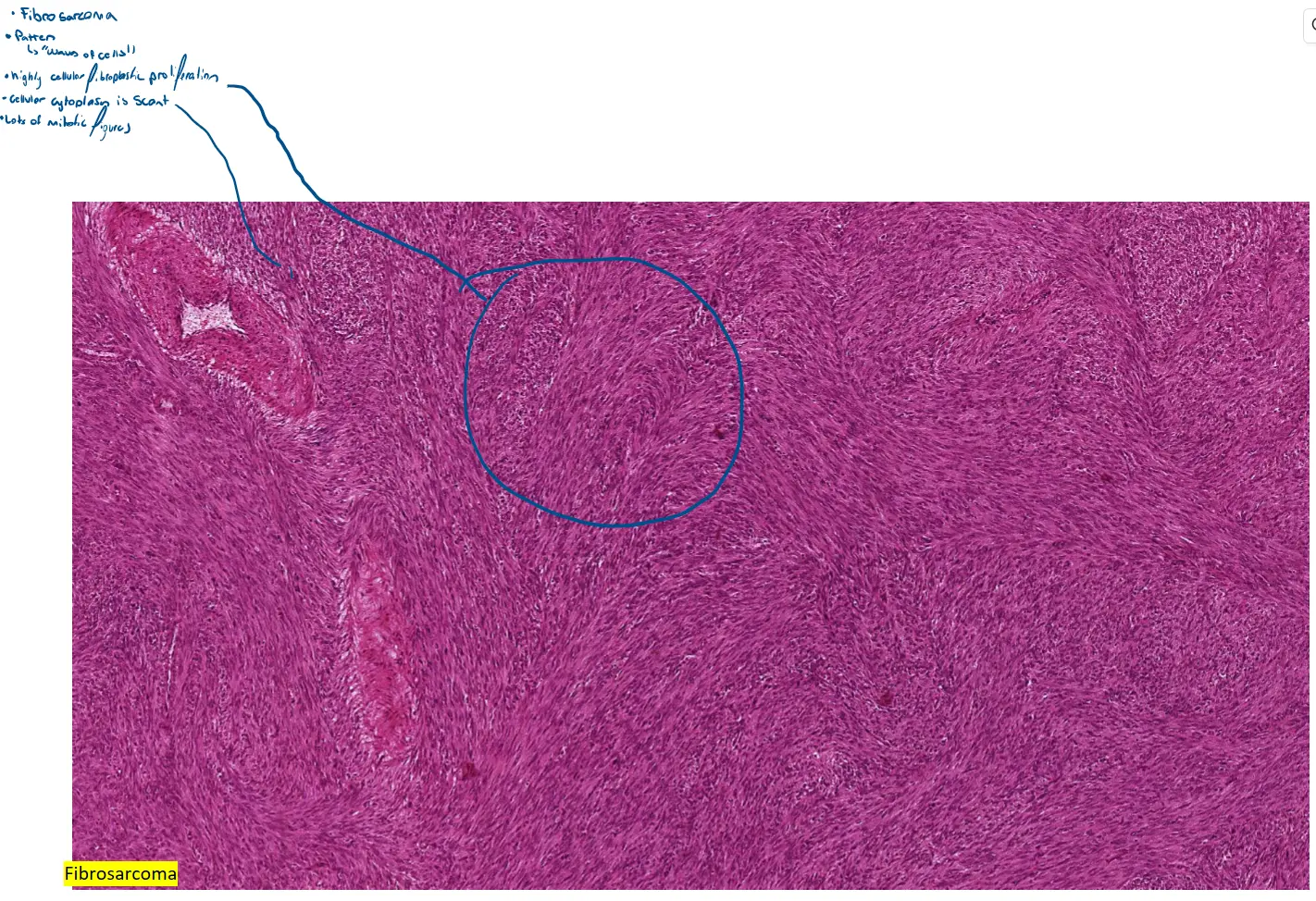
 Of course. Let’s analyze the microscopic features of this fibrosarcoma. This is a malignant tumor composed of cancerous fibroblasts. The images provided are excellent examples of a high-grade, poorly differentiated tumor.
Of course. Let’s analyze the microscopic features of this fibrosarcoma. This is a malignant tumor composed of cancerous fibroblasts. The images provided are excellent examples of a high-grade, poorly differentiated tumor.
🔬 Architectural Pattern (Visible in All Images)
-
Highly cellular fibroblastic proliferation: The first thing you’ll notice in all the images is that the tissue is extremely dense and purple. This is because it’s highly cellular, meaning it’s packed wall-to-wall with tumor cells, leaving very little room for the pink collagen stroma.
-
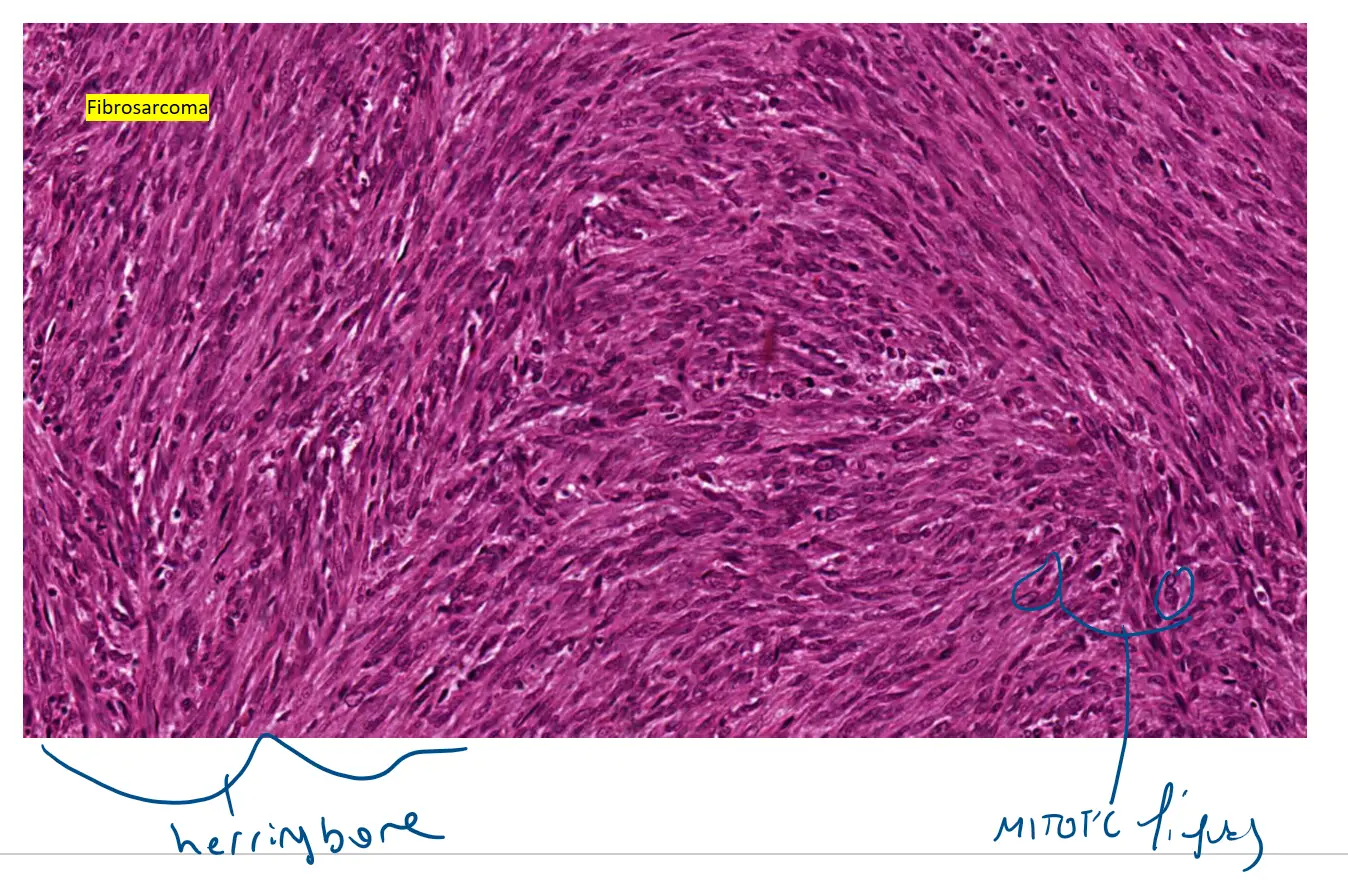
Herringbone pattern: This is the classic architectural clue for fibrosarcoma and is best seen in the middle and bottom high-power images. Notice how the spindle cells are not randomly arranged but are aligned in bundles (fascicles) that intersect each other at sharp angles. This intersecting pattern is what’s known as a herringbone or chevron pattern.
🔬 Cellular Details (Best Seen in High-Power Images)
-
Cells have scant cytoplasm, tapering elongated dark nuclei: If you look closely at the individual cells in the middle and bottom images, you can see they are spindle-shaped with very little cytoplasm. The nuclei are the most prominent feature—they are elongated, dark (hyperchromatic), and irregular in shape with tapered ends.
-
Mitotic activity present, often with abnormal forms: This is a critical feature that confirms malignancy. Throughout the high-power field, you must look for mitotic figures. These will appear as small, intensely dark, condensed, and often irregularly shaped nuclear material (they can look like dark smudges or tiny starbursts). The presence of frequent and/or abnormal-looking mitotic figures is a hallmark of a high-grade sarcoma.
-
Variable collagen: Unlike the benign fibrous lesions we’ve seen that have abundant pink collagen, this malignant tumor produces very little. The overwhelming purple appearance is due to the high density of tumor cells relative to the collagen.
-
No pleomorphism: While the nuclei are clearly malignant, the cells themselves are relatively monotonous—they are all spindle-shaped. This lack of significant variation in cell size and shape (pleomorphism) is characteristic of classic fibrosarcoma and helps distinguish it from other high-grade sarcomas.
In summary, your images perfectly demonstrate a malignant spindle cell tumor with the high cellularity, intersecting herringbone pattern, and atypical nuclei characteristic of a fibrosarcoma.
Would you like me to create a table comparing the key features of the benign fibrous lesions versus this malignant fibrosarcoma to highlight the differences?