Additional Diagnostic Steps in Clinical Examination
Overview of Diagnostic Procedures1
Historically described as “special tests,” these procedures extend beyond the standard clinical examination to provide a comprehensive assessment.
- The diagnostic process involves gathering history and clinical evidence; patients often return with more clarity or additional history after considering initial discussions.
- The examination process leads to the development of a "problem list" derived from observations, such as identifying issues associated with restorations.
Common Diagnostic Modalities
- Radiographs
- Pulp tests
- Periodontal charting
- Articulated study models
- Photographs
- Other specialized analyses:
- Dietary analysis
- Plaque score
- Saliva analysis
Rationale for Additional Testing2
- Clinical Consolidation: Provides the clinician time to consolidate and review clinical findings.
- Patient Consideration: Offers the patient a “cooling off period” to consider issues raised during the initial examination.
- Diagnostic Verification: Confirms clinical findings and supports the final diagnosis.
- Documentation: Serves as essential clinical records.
- Visual Evidence: Utilizes the principle that “a picture speaks a thousand words” for better communication and recording.
- The decision to perform additional tests should be based on how much new information will be gained to aid the diagnostic process.
- Consideration must be given to what can be controlled from an iatrogenic perspective regarding the dental tube.
Radiographic Imaging
Common Radiographic Modalities3
- OPG radiograph (panoramic film)
- Plain film periapical and bitewings
- Plain film occlusal
- CT scan and 3D imaging
Clinical Application4
- Supplement clinical examination
- Knowledge of anatomy, health, and pathologic structures

Plain Film Radiography567
 |  |
 |
Diagnostic Indicators for Plain Films8
- Interproximal, deep, or large restorations
- Overhangs
- Caries and secondary caries
- Note: Approximately 30-40% demineralisation is required before becoming visible on plain film
- Radiolucent restorations
- Supporting structures
- Pulp and periapical tissues
- Previous Root Canal Fillings (RCF)
- Perforations and fractures

Occlusal Radiographs and Sialoliths
Clinical Uses of Occlusal Radiography9
- Identify bucco-palatal/lingual positioning of lesions
- Detection of sialoliths
- Assessment of impacted canines

Radiation Safety and Diagnostic Intervals
Radiation Principles and Diagnostic Intervals10
- Radiation Safety: Adherence to ALARA (As Low As Reasonably Achievable) principles.
- Diagnostic, Record Keeping, and Baseline Requirements:
- OPG Radiographs:
- Active treatment: Every 2 years.
- Onward referral: Within the last 6-12 months.
- Bitewing (BW) Radiographs:
- Check for interproximal (IP) lesions; left and right posterior views every 2 years.
- OPG Radiographs:
Guiding Principle
- These intervals serve as a guiding principle and are not absolute.
Advanced Three Dimensional Imaging
Applications of 3D and Advanced Imaging11
- Three-dimensional (3D) visualization
- Comparison of Conebeam CT vs. conventional CT
- TMJ imaging
- Planning for dental implants
- Assessment of fractures and Head & Neck Cancer (Ca.)
- Evaluation of sinus lesions
- Analysis of superimposed structures

Clinical Case Studies in Diagnosis12
Case studies in assessment and diagnosis.
Case Study One Jess
Patient Profile and History13
- 56-year-old nurse
- Toothache for 18 months on the left-hand side (LHS)
- Intermittent symptoms associated with tooth 26
 |  |
Clinical Consultations and Findings
- Consulted two general dentists
- No existing restorations
- Dental radiographs showed no abnormalities
Specialist Referrals and Imaging
- Medical GP referral
- ENT referral
- CT imaging
Diagnosis and Specialist Assessment14
- Provisional diagnosis: Cracked tooth
- Endodontist assessment:
- Evaluated size of lesion and duration of symptoms
- Prognosis determined to be poor to hopeless

Treatment and Rehabilitation
- Extraction of tooth 26 performed by Oral and Maxillofacial Surgeon (OMFS)
- Prolonged healing period
- Sinus augmentation
- Implant placement at the 26 site
Case Study Two Ling15
 |  |
Patient Profile and Initial Presentation16
- 36-year-old graphic designer
- Tooth 26 sore and tender to bite
- Tooth 26 was crowned 6 months ago
- Ongoing symptoms post-treatment

Clinical Observations and History
- Disto-palatal marginal deficiency noted
- Prior to crown placement, the tooth was assessed by an endodontist
- Initial assessment deemed the pulp clinically healthy and periapical tissues normal
Ling
Surgical Findings and Diagnosis17
- Sectioning of the 26 crown yielded granulation tissue in the disto-palatal cavity
- Root resorption defect identified:
- Deep disto-palatal location
- Tooth determined to be non-restorable

Treatment Outcome
- Extraction of tooth 26
- Lengthy healing process
- Placement of 26 implant
Comparative Analysis of Outcomes
Case Similarities18
- Both Jess and Ling involved tooth 26 (coincidence)
- Both presented with unusual clinical symptoms
- Final outcome was identical: 26 Implant
Clinical Management and Patient Experience
- Initial management was reasonable and handled effectively by general dentists and subsequent specialists
- Successful management resulted in:
- Avoidance of potential complaints
- Patient acceptance of the outcome
- Clinicians felt worn out but not burnt out
- Overall perspective: Both patients felt they were looked after well.
Pulp Sensibility Testing
Diagnostic Modalities19
- Percussion and mobility: Evaluates the periapical and periodontal response to applied forces.
- Thermal testing:
- Cold
- Heat
- Electric testing

Clinical Objectives of Sensibility Testing20
- Assess the nerve supply to gain an understanding of the health or pathologic status of the pulp.
- Evaluate the caries process and the ability of the pulp to “wall off” through the formation of reparative or secondary dentine.
- Establish a baseline by comparing results to adjacent teeth.

Thermal Testing and Clinical Observations
Cold Testing Methods21
- Dry ice / CO2
Clinical Observations and Comparisons
When comparing the target tooth to adjacent teeth, observe the following responses:
- Healthy unrestored tooth: Responds normally.
- Restored tooth: Responds normally.
- Heavily restored tooth: May show a slower response or no response.
Responses in Pulp Pathology
- Reversible Pulpitis: The tooth responds; the sensation lingers and is sometimes heightened.
- Irreversible Pulpitis: Characterized by a heightened and lingering response.
- Necrotic / Pulpless: No response to testing.
Electric Pulp Testing
Indications and Utility22
- Nerve Conductivity: Primarily measures the integrity of nerve fibers.
- Heavily Restored or Calcified Teeth: Useful for teeth with obliterated pulps where cold tests may suggest no response.
- Necrosis Confirmation: Used to confirm a lack of response in necrotic or pulpless teeth.
Periodontal Assessment and Charting
Digital Documentation Tools23
- Periodontal Charting Tab
- Periodontal Electronic Form (e-form)
Study Models and Articulation24
Requirements for Articulated Study Models25
- Accurate Study Models
- Alginate impressions
- Polyvinyl Siloxane (PVS)
- Buff stone for pouring
- Articulation and Registration
- Bite registration or articulation in maximum intercuspation
- Use of an articulator
- Facebow recording

Clinical Protocols for Articulation
Technical Procedures and Quality Control26
- Model Preparation
- Accurate study models
- Pour-up as soon as possible (ASAP)
- Inspection for blebs, drags, or distortion
- Clinical Recordings
- Facebow recording
- Occlusal recording
- Assessment of tooth-to-tooth contacts
- Management of tooth separation (use of bite wafer)
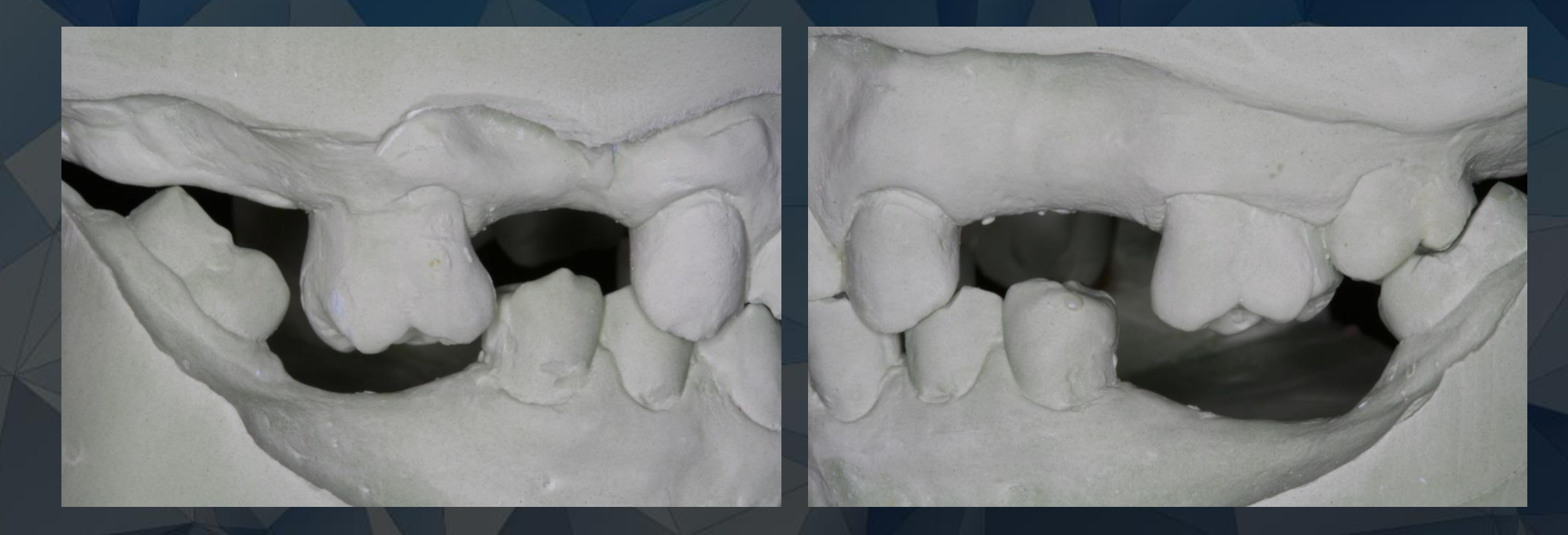
Diagnostic Benefits of Study Models
Clinical Advantages27
- Visualization and Analysis
- Visualize study models and dentition without the interference of soft tissues.
- Patient and Professional Interaction
- Facilitate communication and treatment discussion.
- Treatment Planning
- Diagnostic wax-up.

Digital Scanning and Data Collection
Digital Scanning Protocols28
- Scanning Scope
- Scan cases for arch or full mouth.
- Application is currently limited to tooth-based restorations.
- Dentures continue to follow conventional protocols.
Implementation and Integration
- Ongoing Integration (3-6 Months)
- Refinement of clinical protocols.
- Development of facilities.
- Staff familiarity and training.
Academic Requirements
- Conventional study models are to be completed as directed by the unit co-ordinator.
Dietary and Saliva Analysis
Assessment Criteria for Dietary Analysis29
Dietary analysis relies on patient reporting to evaluate the following factors:
- Cariogenic and Periodontal Risks: Identification of sugars and sticky carbohydrates that promote plaque formation, leading to caries and periodontal disease.
- Erosive Potential: Identification of acids that contribute to tooth wear (which is often multi-factorial).
- Consumption Habits: Evaluation of the specific patterns of food intake.

Plaque Scoring and Oral Hygiene
Clinical Utility of Plaque Scoring30
- Oral Hygiene Instruction (OHI): Serves as an effective tool for demonstrating plaque location and removal techniques to the patient.
- Clinical Documentation: Substantiates the clinical description of “Good” versus “Poor” oral hygiene with objective data.
- Patient Motivation and Monitoring: Demonstrates relative improvement between the initial visit, subsequent cleaning/OH regimes, and review appointments to help motivate the patient.
 |  |
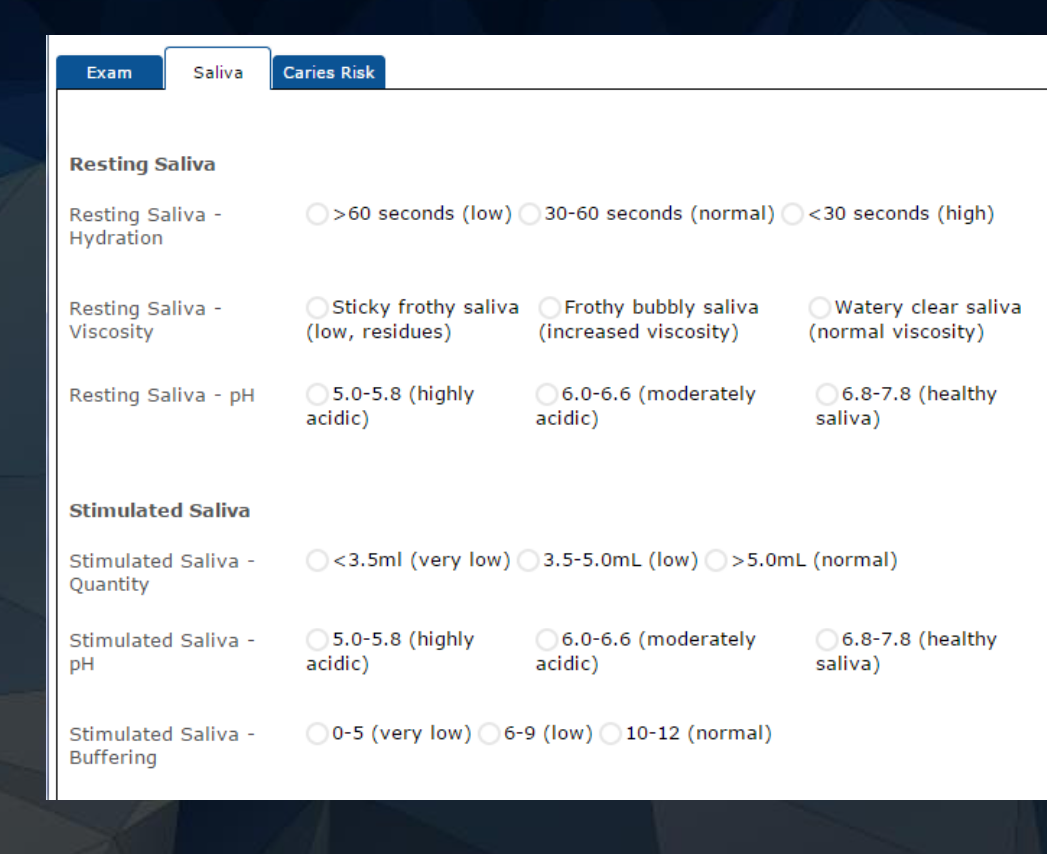
Saliva Analysis for Caries and Wear31
Saliva analysis is utilized to assess and manage the following clinical conditions:
- Caries: Evaluating risk factors and disease activity.
- Tooth Wear: Investigating systemic or local salivary factors contributing to erosion.
- Prosthetic and Restorative Complications: Addressing problems with dentures and the longevity of adhesive restorations.
Clinical Photography and Documentation3233
 |  |
 |  |
Clinical Applications of Photography34
Photographs serve as essential tools for clinical records and documentation, allowing for the longitudinal assessment of patient conditions. Key uses include:
- Monitoring minor tooth wear over time
- Documenting baseline conditions pre-bleaching
- Assisting in accurate shade taking and communication

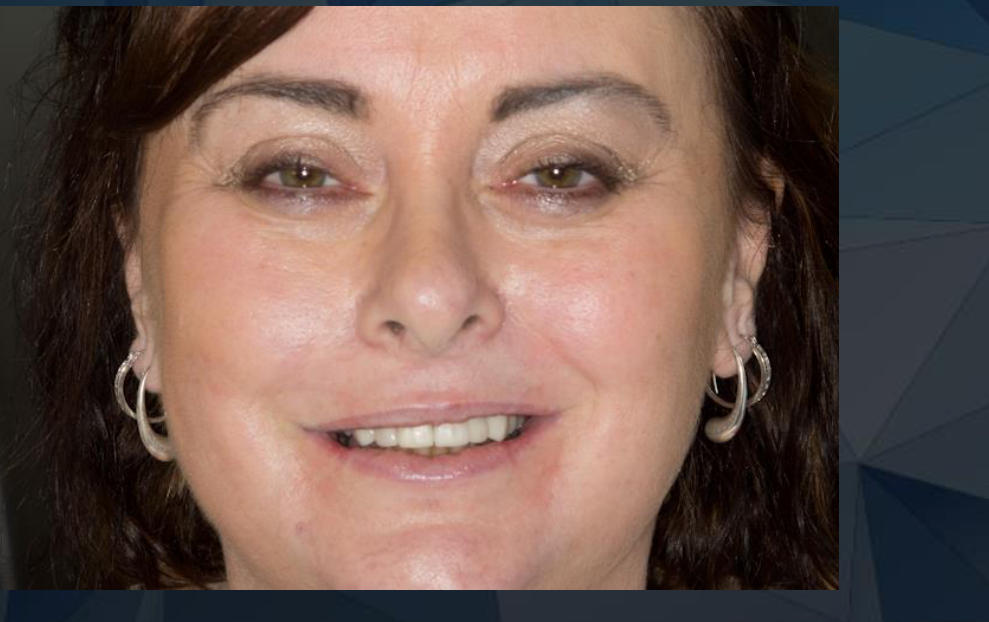
Extraoral and Intraoral Techniques
Extra-oral Photography Standards35
- Subject: Full face and profile views
- Patient Posture: Standing up in a natural head position
- Environment: Utilize a neutral background to ensure clarity and focus on the subject

Anterior View Requirements36
- Use of retractors is required for clear visualization of the anterior segment.

Intra-oral Equipment and Views37
- Retractors: Essential for soft tissue management
- Occlusal Mirrors: For capturing maxillary and mandibular arches
- Buccal/Lingual Mirrors: For specialized lateral or internal views

Privacy and Social Media Guidelines
Equipment and Data Security38
- Approved Devices: Use OHCWA cameras only. Personal cameras or phone cameras are not to be used at this stage.
- Data Protection: Make reasonable attempts to secure photos stored on:
- SD cards
- Computers
- Tablets
- Ethics: Maintain strict patient confidentiality and privacy at all times.
Professionalism and Social Media39
- Community Context: Recognize that Perth is a small dental community; professional conduct is paramount.
- Privacy Considerations: Always consider the privacy of patients and staff before posting online.
- Impact: Content with potential for public access reflects directly on the individual, the university, and the broader dental community.
Consolidating Information and Patient Communication
Information Management and Communication40
- Time Management: Utilize down time or waiting periods to discuss clinical issues.
- Follow-up Protocols:
- Schedule separate appointments for follow-up discussions, especially for complex treatment plans.
- Utilize written correspondence for formal communication.
- Within certain systems like Titanium, there may only be a small field available to describe a diagnosis.
- It is essential to discuss the treatment with the patient, including any risks of rare complications.
- Ensure the patient's primary complaint is addressed during the process, rather than focusing solely on disease control.

Tooth Assessment and Prognosis Determination41
Integrating tooth assessment
Key Literature and Strategic Considerations42
- Zitzmann et al. 2010: Strategic considerations in treatment planning.
- Jotkowitz and Samet 2009: Classification and prognosis evaluation of individual teeth—a comprehensive approach.
- Jotkowitz A, Samet N. 2010: Rethinking ferrule - a new approach to an old dilemma.
Definitions and Systematic Approaches43
Defining Prognosis44
- The possible outcomes of a disease or condition and the anticipated frequency of those outcomes.
- A prediction of the probable course and outcome of a disease.
- The likelihood of recovery from a disease.
- A forecast or prediction.

Systematic Arch Assessment45
Evaluating the prognosis of each tooth in the arch involves a systematic approach to identify key teeth and assess their utility for:
-
==Consideration of the shortened dental arch concept as a factor in overall assessment.==
-
==Identification of questionable teeth based on their ability to respond to treatment or the extent of the lesion/evasion.==
-
Abutments:
- Bridges
- Dentures
-
Maintenance of:
- Aesthetics
- Function (Mastication, Occlusion, Speech)
Zitzmann 2010 JPD

Periodontal and Restorative Factors4647
 |  |
 |
Prognostic Criteria Table (Zitzmann et al.)48
| Factors | Good | Questionable | Hopeless |
|---|---|---|---|
| Periodontal | PPD ≤3 mm, BoP-, PAL loss ≤25%, FI degree ≤1 | Residual PPD ≥6 mm and BoP+, PAL loss ~50%, FI degree II or III, root proximity | Insufficient residual attachment |
| Endodontics | No clinical signs; absence of or decreasing radiolucency | No clinical signs; persisting radiolucency | Symptomatic situation and radiolucency; no further treatment feasible |
| Implants | Absence of BoP, suppuration, bone loss | BoP with/without bone loss | Mobility |
| Prosthetic | Sufficient residual tooth substance, adequate retention/resistance (4mm wall height, 15-20° convergence, 1.5-2mm ferrule) | Reduced retention/resistance (<3mm wall height and/or >25° convergence) | Insufficient residual tooth substance (<1.5mm circular ferrule), no crown lengthening or extrusion feasible |
Suppuration Legend:
- + / - = ✓: No (Negative for presence of disease)
- + / - = ✗: Yes (Positive for presence of disease)
- + / - = N: Not determined (Indeterminate result)
- + / - = U: Unable to determine
- + / - = ?: Not applicable
Abbreviations: PPD: probing pocket depth; BoP: bleeding on probing; PAL: probing attachment level; FI: furcation involvement (degree 0 to 3)
14, 15

Clinical Options and Interventions49
- Composite
- Crown
- +/- Post
- +/- Core
- Crown lengthening
- Extrusion
- Extraction
- Assessment as an abutment for a partial denture
Treatment Sequencing and Disease Control
Practitioners must decide on the sequence of care, often starting with initial therapy, stabilization, and disease control. Some treatments, such as definitive restorations or specific procedures like “closed lighter” steps for dentures, may be held until the oral environment is controlled and a better clinical picture is established.

A Comprehensive Approach to Individual Tooth Evaluation50
Treatment planning requires the analysis of individual teeth, accurate diagnosis, and prognosis evaluation following a complete patient evaluation.
Key dimensions for determining relative tooth prognosis include:
- Periodontal perspective
- Restorative perspective
- Endodontic perspective
- Occlusal plane perspective
This system assesses the condition of individual teeth and enables a relative prognostic value based on tooth condition and patient-level factors (Quintessence Int 2009;40:377–387).
Biologic and Behavioral Risk Factors
Patient and Host Risk Factors51
Biologic Risk Factors
- Medical conditions impairing immune function and healing
- Impaired salivary flow/function
- Medical condition or disability limiting oral hygiene
- High Streptococcus mutans and Lactobacillus salivary count
- Positive for interleukin-1 genotype
- Family history
- Other missing teeth
Behavioral Risk Factors
- Compromised or poor oral hygiene
- Cariogenic diet
- Low exposure to fluoride
- Parafunctional habits
- Ability and willingness to adhere to long-term maintenance
- Smoking
Financial and Personal Risk Factors
- Motivation for treatment
- Available resources (finances, time, and effort)
- Attitude toward losing teeth
- Understanding of condition and treatment
- Esthetic expectations
- Low dental IQ

Anatomic Irregularities and Risk Factors52
According to Jotkowitz and Samet (2009), specific anatomic factors can influence prognosis:
- Irregularly shaped roots
- Multiple canals and/or roots
- Thin and/or short roots
- Excessively conical roots
Iatrogenic Compromising Factors (Jotkowitz and Samet 2009)53
| Factor | Condition and Outcome |
|---|---|
| Iatrogenic Factors: - Perforations - Extensive post preparations - Minimal tooth structure thickness after prep - Irremovable dental materials | No active pathology: Prognosis may be fair to good. |
| Complicating Signs: - Further treatment planned for tooth - Presence of clinical/radiographic signs or symptoms | Active pathology present: → Prognosis level drops |

Comprehensive Classification Systems
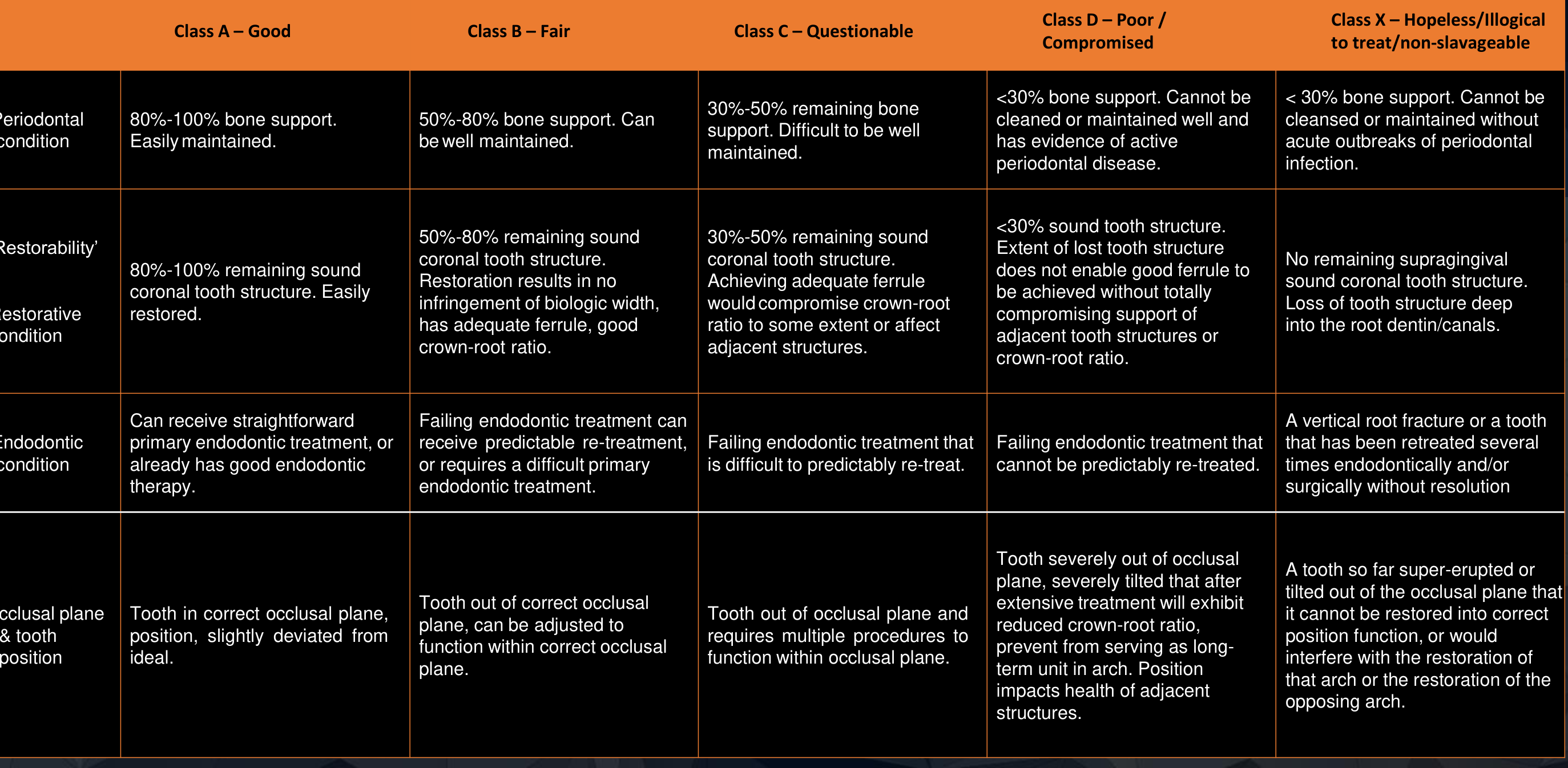
Comprehensive Classification System (Jotkowitz and Samet 2009)54
| Category | Class A (Good) | Class B (Fair) | Class C (Questionable) | Class D (Poor) | Class X (Hopeless) |
|---|---|---|---|---|---|
| Periodontal | 80-100% bone support. Easily maintained. | 50-80% bone support. Well maintained. | 30-50% bone support. Difficult to maintain. | <30% bone support. Active disease; cannot be cleaned well. | <30% bone support. Acute outbreaks; non-maintainable. |
| Restorative | 80-100% sound coronal structure. Easy to restore. | 50-80% sound structure. No biologic width infringement; adequate ferrule. | 30-50% sound structure. Ferrule needs may compromise crown-root ratio. | <30% sound structure. Cannot achieve ferrule without compromising adjacent structures. | No supragingival sound structure. Loss deep into root dentin/canals. |
| Endodontic | Straightforward primary treatment or existing good therapy. | Failing RCT with predictable retreat or difficult primary RCT. | Failing RCT; difficult to predictably retreat. | Failing RCT; cannot be predictably retreated. | Vertical root fracture or multiple failed surgical/non-surgical attempts. |
| Occlusal/ Position | Correct plane/position or slight deviation. | Out of plane; can be adjusted to function. | Out of plane; requires multiple procedures to correct. | Severely tilted/out of plane. Treatment compromises crown-root ratio or adjacent health. | Severely super-erupted/tilted. Cannot be restored; interferes with arch/opposing arch. |
Footnotes
-
Original PDF page 1: L4 Diagnostic, p.1 ↩
-
Original PDF page 2: L4 Diagnostic, p.2 ↩
-
Original PDF page 3: L4 Diagnostic, p.3 ↩
-
Original PDF page 4: L4 Diagnostic, p.4 ↩
-
Original PDF page 6: L4 Diagnostic, p.6 ↩
-
Original PDF page 7: L4 Diagnostic, p.7 ↩
-
Original PDF page 8: L4 Diagnostic, p.8 ↩
-
Original PDF page 5: L4 Diagnostic, p.5 ↩
-
Original PDF page 9: L4 Diagnostic, p.9 ↩
-
Original PDF page 10: L4 Diagnostic, p.10 ↩
-
Original PDF page 11: L4 Diagnostic, p.11 ↩
-
Original PDF page 12: L4 Diagnostic, p.12 ↩
-
Original PDF page 13: L4 Diagnostic, p.13 ↩
-
Original PDF page 14: L4 Diagnostic, p.14 ↩
-
Original PDF page 16: L4 Diagnostic, p.16 ↩
-
Original PDF page 15: L4 Diagnostic, p.15 ↩
-
Original PDF page 17: L4 Diagnostic, p.17 ↩
-
Original PDF page 18: L4 Diagnostic, p.18 ↩
-
Original PDF page 19: L4 Diagnostic, p.19 ↩
-
Original PDF page 20: L4 Diagnostic, p.20 ↩
-
Original PDF page 21: L4 Diagnostic, p.21 ↩
-
Original PDF page 22: L4 Diagnostic, p.22 ↩
-
Original PDF page 23: L4 Diagnostic, p.23 ↩
-
Original PDF page 25: L4 Diagnostic, p.25 ↩
-
Original PDF page 24: L4 Diagnostic, p.24 ↩
-
Original PDF page 26: L4 Diagnostic, p.26 ↩
-
Original PDF page 27: L4 Diagnostic, p.27 ↩
-
Original PDF page 28: L4 Diagnostic, p.28 ↩
-
Original PDF page 29: L4 Diagnostic, p.29 ↩
-
Original PDF page 30: L4 Diagnostic, p.30 ↩
-
Original PDF page 31: L4 Diagnostic, p.31 ↩
-
Original PDF page 33: L4 Diagnostic, p.33 ↩
-
Original PDF page 34: L4 Diagnostic, p.34 ↩
-
Original PDF page 32: L4 Diagnostic, p.32 ↩
-
Original PDF page 35: L4 Diagnostic, p.35 ↩
-
Original PDF page 36: L4 Diagnostic, p.36 ↩
-
Original PDF page 37: L4 Diagnostic, p.37 ↩
-
Original PDF page 38: L4 Diagnostic, p.38 ↩
-
Original PDF page 39: L4 Diagnostic, p.39 ↩
-
Original PDF page 40: L4 Diagnostic, p.40 ↩
-
Original PDF page 41: L4 Diagnostic, p.41 ↩
-
Original PDF page 42: L4 Diagnostic, p.42 ↩
-
Original PDF page 45: L4 Diagnostic, p.45 ↩
-
Original PDF page 43: L4 Diagnostic, p.43 ↩
-
Original PDF page 44: L4 Diagnostic, p.44 ↩
-
Original PDF page 47: L4 Diagnostic, p.47 ↩
-
Original PDF page 48: L4 Diagnostic, p.48 ↩
-
Original PDF page 46: L4 Diagnostic, p.46 ↩
-
Original PDF page 49: L4 Diagnostic, p.49 ↩
-
Original PDF page 50: L4 Diagnostic, p.50 ↩
-
Original PDF page 51: L4 Diagnostic, p.51 ↩
-
Original PDF page 52: L4 Diagnostic, p.52 ↩
-
Original PDF page 53: L4 Diagnostic, p.53 ↩
-
Original PDF page 54: L4 Diagnostic, p.54 ↩