Case Presentation1
Dr Lyndon P Abbott
Patient Profile and History2
- Age/Gender: 68-year-old male
- Chief Complaint: Progressive shortness of breath and dry cough over the past six months.
- Medical History:
- Hypertension (controlled with Lisinopril)
- Type 2 Diabetes Mellitus (managed with Metformin)
- No history of asthma or known allergies
- Social History:
- Former smoker (20 pack-years, quit 15 years ago)
- Retired construction worker with potential occupational dust exposure
Clinical Presentation
Upon physical examination, the patient exhibited fine bibasilar inspiratory crackles (velcro-like) and mild digital clubbing. Oxygen saturation was 92% on room air at rest, dropping to 88% during a six-minute walk test.
Diagnostic Investigations3
-
Pulmonary Function Tests (PFTs):
- Restrictive pattern observed
- Reduced Forced Vital Capacity (FVC)
- Decreased Total Lung Capacity (TLC)
- Significantly reduced Diffusion Capacity of the Lungs for Carbon Monoxide (DLCO)
-
Imaging:
- Chest X-ray: Showed increased reticular markings in the lower lung zones.
- High-Resolution Computed Tomography (HRCT): Revealed subpleural honeycombing, traction bronchiectasis, and reticular opacities consistent with a Usual Interstitial Pneumonia (UIP) pattern.
Laboratory Results
- Autoimmune serology (ANA, RF, anti-CCP) returned negative, ruling out common connective tissue diseases as the primary cause of the interstitial lung disease.
Case Presentation General Principles
Presenter Information4
- Dr Lyndon P Abbott
- Graduated DMD in 2019
- Current Dental Graduate Officer at UWA
 |  |
Purpose of the Examination5
The case presentation exam ensures you are safe to practice ethical, appropriate and evidenced based dentistry.
Presentation Objectives6
- Showcase your hard work
- Convince the examiners you can practice ethical, appropriate and evidenced based dentistry
Factors Outside Your Control7891011
- Date and time
- Venue
- Projector, IT
- Questions
Factors Within Your Control
-
Chosen patient
-
Examination and diagnosis
-
Amount of research papers you read
-
Amount of tutors you talk to
-
Amount of time spent preparing and rehearsing your case presentation
-
Date and time
-
Venue
-
Projector, IT
-
Questions
-
Chosen patient
-
Examination and diagnosis
-
Amount of research papers you read
-
Amount of tutors you talk to
-
Amount of time spent preparing and rehearsing your case presentation
Start early.
- PLAN
- PREPARE
- PERFORM
Examination and Treatment Planning Guidelines
Purpose and Scope12
The aim of this Clinical Guideline is to provide advice to OHCWA students and clinicians regarding comprehensive oral exam and treatment planning. Evidence-based clinical guidelines are intended to provide guidance, and are not a standard of care, requirement, or regulation. However, the application of clinical guidelines in publicly-provided oral health services allows for consistency to occur across large patient cohorts with a variety of oral health clinicians.
This Clinical Guideline plans to:
- Standardise the way in which all patients are assessed
- Establish a standardised sequence for a thorough comprehensive examination to reduce overlooking any area to be examined
Goals of Dental Treatment
The aim of dental treatment is to assess, restore and maintain the health, function and efficiency of dental and related tissues, and thereby improve the oral, general and psychological health of a patient. Treatment should be designed to prevent further dental disease and to restore lost tissue and function. Patients should be educated to an awareness of the importance of their dental health and how such health may be maintained.
Examination Template (011)13
-
P/C (Presenting Complaint):
- Pain/discomfort:
- Loss of function:
- Appearance:
- Expectations:
-
HPC (History of Presenting Complaint):
-
MH (Medical History): updated, see medical notes
- Adverse Drug Reactions: none declared
Consent obtained to carry out dental examination
-
EO (Extra-oral): TMJ, MOM, LN, thyroid, lips – all NAD
-
IO (Intra-oral): Buccal mucosa, hard palate, soft palate, glossopharyngeal, tongue, FOM – all NAD
-
Teeth as per odontogram:
- TTP:
- TT pal:
- Mobility:
-
Occlusion:
- OJ:
- OB:
- Molar class:
- Crossbite:
- Crowding:
- Super-eruption:
Patient Selection and Preparation14
Selection Strategy15
- Patient selection
- Multidisciplinary
- Select your patients early and treat all patients as possible case presentation patients
Take photos!!!
Patient Background16
- Patient Details
- Importance of Social History
- Medical History
- How does this medical history impact the overall dental management of this patient
 |  |
 |  |
Clinical Diagnosis and Problem List
Presentation of Diagnoses17
- Have a systematic way of presenting the patient’s examination
- Don’t waste time just listing diagnoses but instead use your time to explain the critical thinking underpinning each diagnosis
Treatment Planning and Communication
Treatment Planning Strategy18
- Discuss the different options
- Keep all the dental diagnosis and problem lists in context with the overall patient
- Treatment alternative tables
- Delivery of Treatment
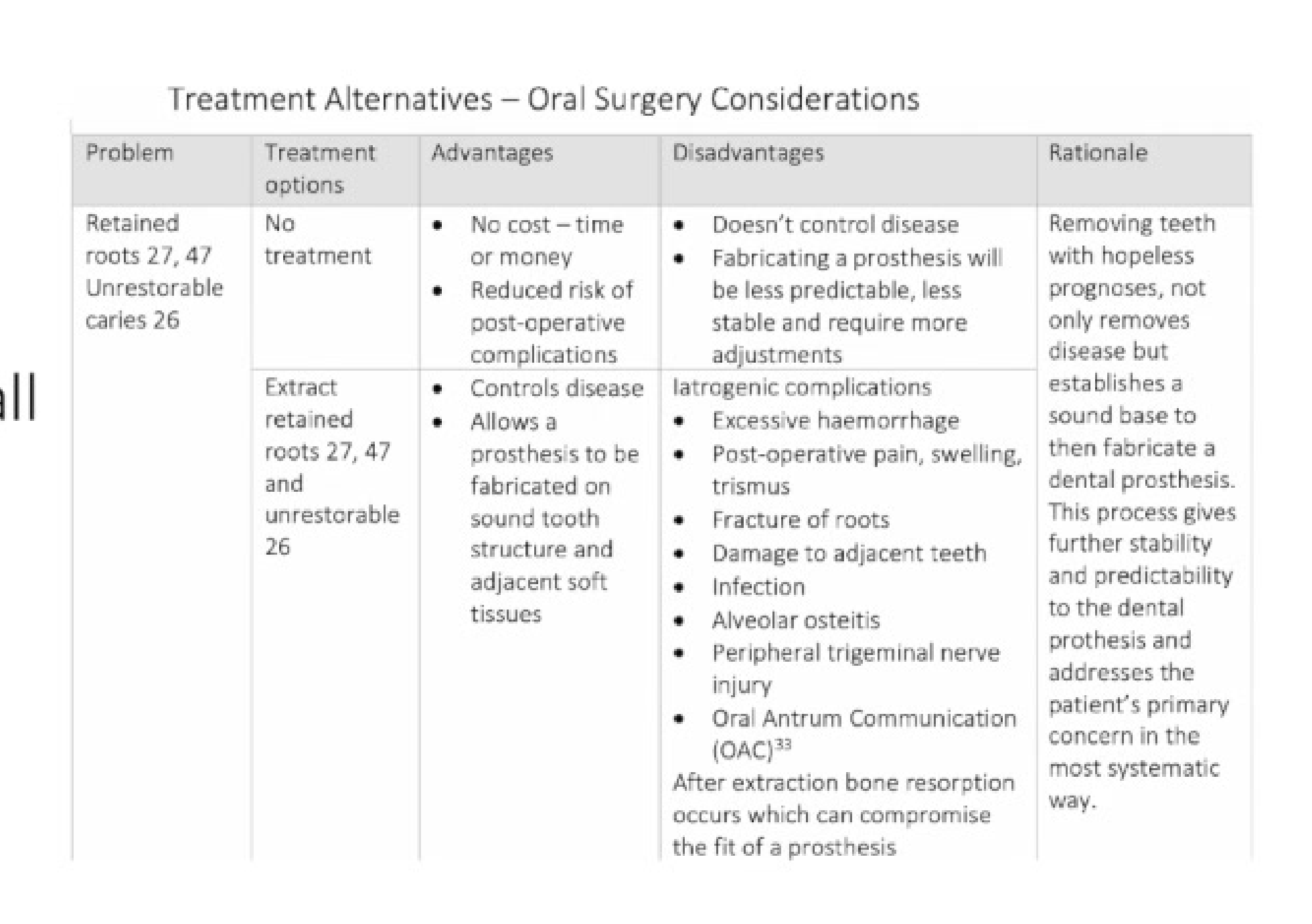
Treatment Alternatives – Oral Surgery Considerations
| Problem | Treatment options | Advantages | Disadvantages | Rationale |
|---|---|---|---|---|
| Retained roots 27, 47; Unrestorable caries 26 | No treatment | - No cost – time or money - Reduced risk of post-operative complications | - Doesn’t control disease - Fabricating a prosthesis will be less predictable, less stable and require more adjustments | Removing teeth with hopeless prognoses not only removes disease but establishes a sound base to then fabricate a dental prosthesis. This process gives further stability and predictability to the dental prosthesis and addresses the patient’s primary concern in the most systematic way. |
| Extract retained roots 27, 47 and unrestorable 26 | - Controls disease - Allows a prosthesis to be fabricated on sound tooth structure and adjacent soft tissues | - Iatrogenic complications - Excessive haemorrhage - Post-operative pain, swelling, trismus - Fracture of roots - Damage to adjacent teeth - Infection - Alveolar osteitis - Peripheral trigeminal nerve injury - Oral Antrum Communication (OAC) - After extraction bone resorption occurs which can compromise the fit of a prosthesis |
Communication and Rehearsal19
- Practice makes perfect
- Consider writing a script and having things on the slides to help jog your memory
- Time yourself
- Deep breaths to slow your heart rate
Handling Questions20
- The questions will be related to your case so prepare answers by researching relevant topics to your patient
- See this as an opportunity to demonstrate your breath of knowledge
- The examiners want you to do well
Strategic Treatment Planning21
- Formulate a comprehensive treatment plan that addresses the patient’s primary concerns while ensuring clinical efficacy.
- Prioritize procedures based on urgency, patient health, and long-term stability.
- Develop alternative treatment options to provide the patient with a range of choices regarding cost, time, and complexity.
Effective Patient Communication
- Use clear, non-technical language to explain diagnoses and proposed interventions.
- Utilize visual aids, such as digital scans, radiographs, or intraoral photos, to enhance patient understanding.
- Ensure informed consent by discussing the risks, benefits, and potential outcomes of each treatment path.
- Address patient expectations early to align clinical goals with the patient’s desired results.
Patient Case Background
Patient Information and Social History22
Patient Information and Details Kym Duane Hales 57 years old (28/09/1962) Currently unemployed – bricklayer by trade Not married, lives alone Date of first dental appointment: 8/3/2018
Medical History and Risk Factors2324252627282930
Medical History
• No current medications • No known allergies • Hypertension - 150/85 • Myocardial infarction 2007 • Smokes 20 cigarettes per day for 30 years (30 pack years) • interested in quitting • Drinks 20 standard alcoholic drinks per week
• Virdis A, Giannarelli C, Fritsch Neves M, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Current pharmaceutical design. 2010 Aug 1;16(23):2518-25. • Johnson N, Bain C. Tobacco and oral disease. British Dental Journal. 2000 Aug 26;189(4). • Johnson GK, Guthmiller JM. The impact of cigarette smoking on periodontal disease and treatment. Periodontol 2000. 2007 Jun;44(1):178-94. • Wong, Tsc, and Wiesenfeld, D. “Oral Cancer.” Australian Dental Journal 63.S1 (2018): S91-S99.
The University of Western Australia
Medical History
-
No current medications
-
No known allergies
-
Hypertension - 150/85
-
Myocardial infarction 2007
-
Smokes 20 cigarettes per day for 30 years (30 pack years)
- interested in quitting
-
Drinks 20 standard alcoholic drinks per week
-
Vrdis A, Giannarelli C, Fritsch Neves M, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Current pharmaceutical design. 2010 Aug 1;16(23):2518-25.
-
Johnson N, Bain C. Tobacco and oral disease. British Dental Journal. 2000 Aug 26;189(4).*
-
Johnson GK, Guthmiller JM. The impact of cigarette smoking on periodontal disease and treatment. Periodontology 2000. 2007 Jun;44(1):178-94.*
-
Wong, T.c, and Wiesenfeld, D. “Oral Cancer.” Australian Dental Journal 63.51 (2018): S91–S99.
-
No current medications
-
No known allergies
-
Hypertension - 150/85
-
Myocardial infarction 2007
-
Smokes 20 cigarettes per day for 30 years (30 pack years)
- interested in quitting
-
Drinks 20 standard alcoholic drinks per week
-
Virdis A, Giannarelli C, Fritsch Neves M, Taddei S, Ghiadoni L. Cigarette smoking and hypertension. Current pharmaceutical design. 2010 Aug 1;16(23):2518-25.
-
Johnson N, Bain C. Tobacco and oral disease. British Dental Journal. 2000 Aug 26;189(4).
-
Johnson GK, Guthmiller JM. The impact of cigarette smoking on periodontal disease and treatment. Periodontology 2000. 2007 Jun;44(1):178-94.
-
Wong, Tsc, and Wiesenfeld, D. “Oral Cancer.” Australian Dental Journal 63.S1 (2018): S91-S99.
Medical History
-
No current medications
-
No known allergies
-
Hypertension - 150/85
-
Myocardial infarction 2007
-
Smokes 20 cigarettes per day for 30 years (30 pack years)
- interested in quitting
-
Drinks 20 standard alcoholic drinks per week
-
Viridis A., Giannarelli C., Fritsch Neves M., Taddei S., Ghiadoni L. Cigarette smoking and hypertension. Current pharmaceutical design. 2010 Aug 16(23):2518-25.
-
Johnson N., Bain C. Tobacco and oral disease. British Dental Journal. 2000 Aug 26;189(4).
-
Johnson GK., Guther Miller JM. The impact of cigarette smoking on periodontal disease and treatment. Periodontology 2000. 2007 Jun;44(1):178-94.
-
Wong Tsc, and Wiesenfeld D. “Oral Cancer.” Australian Dental Journal 63.51 (2018): 591–599.
 |  |
 |
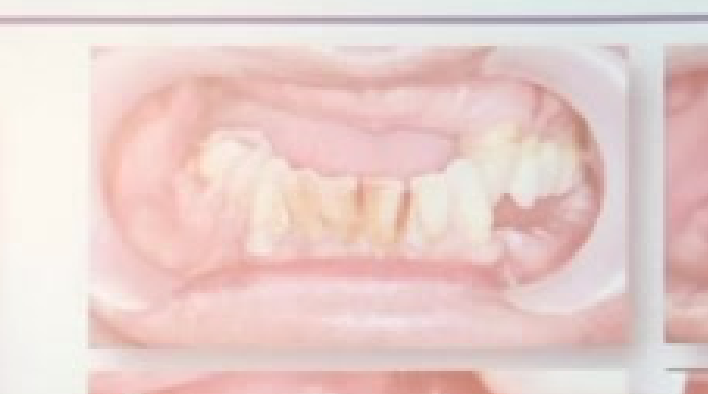
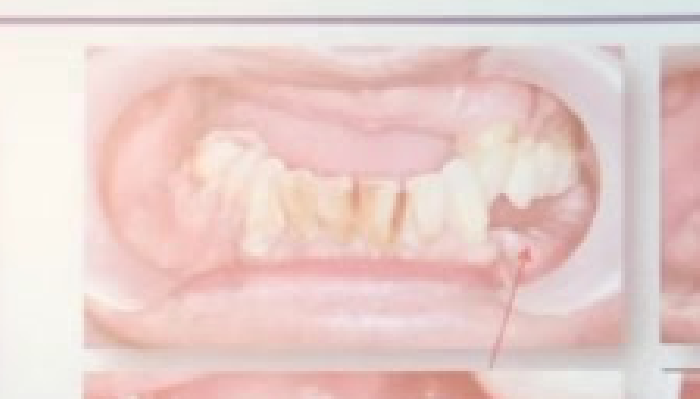
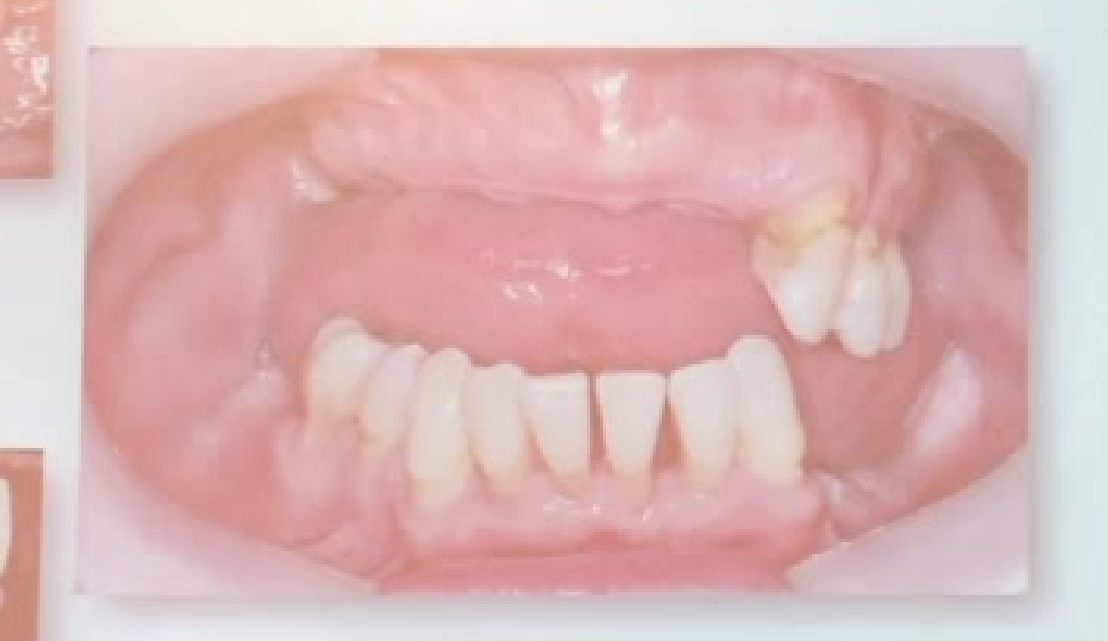
Presenting Complaint and Dental History3132
Presenting complaint, Dental History Presenting Complaint
- Would like to replace his missing teeth
- Trauma – 2013 years ago aluminium flashing hit front teeth
- Longstanding dental neglect
Dental History
- Hasn’t visited the dentist in 10 years
- No current pain or discomfort from dentition
- Lack of function due to multiple missing teeth
- Socially, very self conscious and doesn’t like leaving his house
- Expectations are to replace his currently missing teeth and improve function
Oral Hygiene: Brushes teeth twice per day with manual toothbrush and fluoridated toothpaste. Doesn’t floss or use interdental brushes
Presenting complaint, Dental History
{%mark%}
Presenting Complaint
- Would like to replace his missing teeth
- Trauma – 2013 years ago aluminium flashing hit front teeth
- Longstanding dental neglect
Dental History
- Hasn’t visited the dentist in 10 years
- No current pain or discomfort from dentition
- Lack of function due to multiple missing teeth
- Socially, very self conscious and doesn’t like leaving his house
- Expectations are to replace his currently missing teeth and improve function
Oral Hygiene: Brushes teeth twice per day with manual toothbrush and fluoridated toothpaste. Doesn’t floss or use interdental brushes
{%endmark%}
 |  |
Patient Examination and Assessment3334353637
The University of Western Australia
Dr Thomas F. Melia BSc, DASV, PGDM, ADC
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |
Clinical Presentation and History38
The patient is a 64-year-old male who presented with a primary complaint of persistent discomfort and localized swelling in the lower right quadrant of the mandible.
Physical Examination Findings
- Extraoral Examination: No significant lymphadenopathy or facial asymmetry was noted. The temporomandibular joints functioned within normal limits.
- Intraoral Examination:
- Moderate gingival inflammation and recession were observed in the posterior mandible.
- A localized, firm swelling was palpable on the buccal aspect of the alveolar ridge near the second molar.
- Tooth #31 exhibited Grade II mobility and was sensitive to percussion.
Periodontal Assessment
- Probing Depths: Generalized 3–4 mm, with localized 6–8 mm pockets around the distal and buccal aspects of tooth #31.
- Bleeding on Probing (BOP): Present in 45% of sites, indicating active periodontal inflammation.
- Attachment Loss: Significant clinical attachment loss was noted in the lower right molar region.
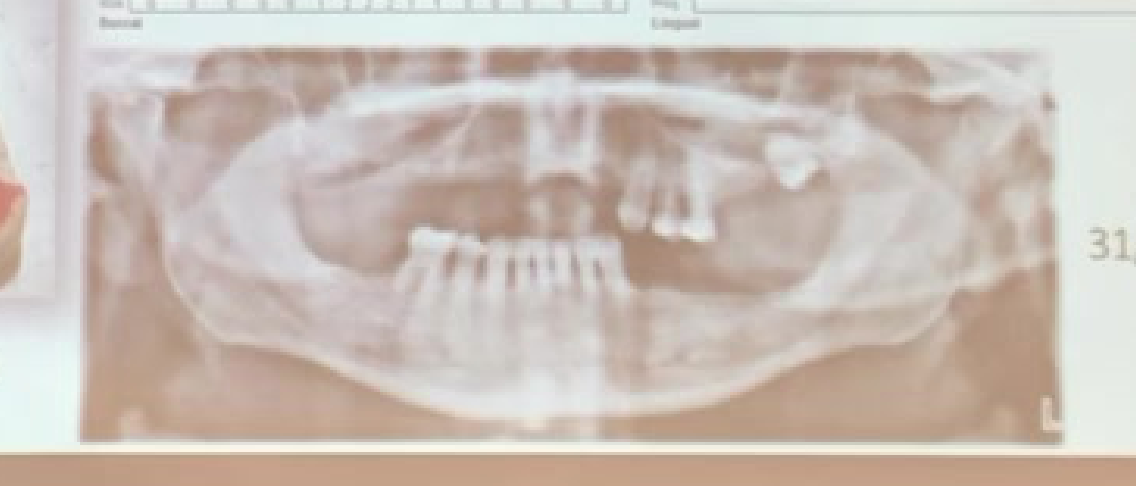
Radiographic Analysis
- Periapical and Bitewing X-rays: Revealed extensive horizontal bone loss throughout the arch.
- Specific Findings for Tooth #31:
- Vertical bone defect on the distal aspect.
- Evidence of furcation involvement (Class II).
- Widened periodontal ligament space, suggesting secondary occlusal trauma.
Radiographic Examination3940
 |  |
 |  |
Clinical Findings and Charting
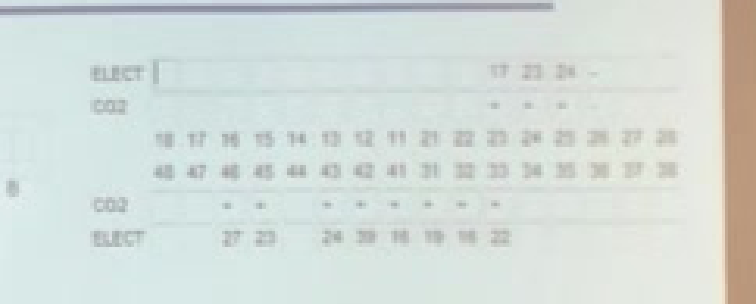
Vitality Testing (8/3/2018)41
- Electric Pulp Test (EPT):
- Teeth 17, 23, 24: Responded
- Teeth 27, 23, 24, 26, 16, 22: Responded
- CO2 Thermal Test:
- All teeth tested (18-28 and 48-38)
- Tooth 26: Unresponsive
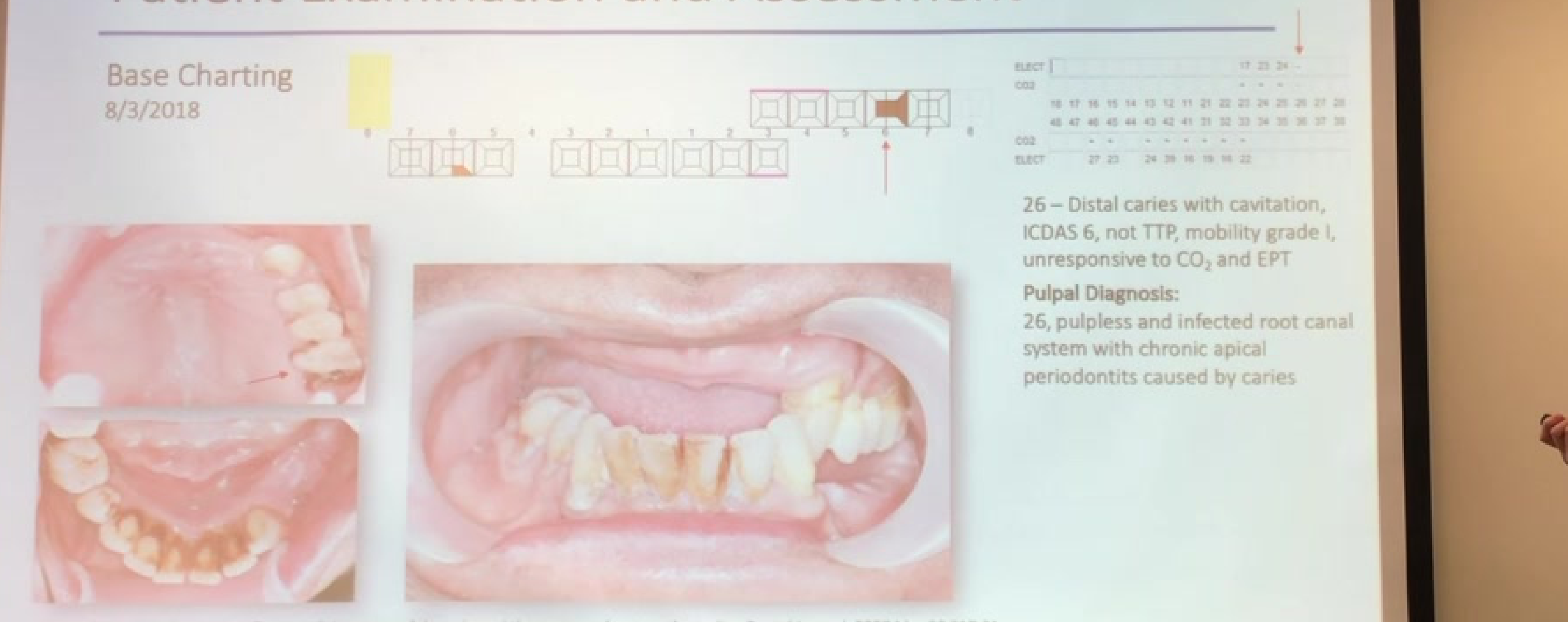
Clinical Findings: Tooth 26
- Distal caries with cavitation (ICDAS 6)
- Not tender to percussion (TTP)
- Mobility: Grade I
- Vitality: Unresponsive to CO2 and EPT
Pulpal and Periapical Diagnosis
- Tooth 26: Pulpless and infected root canal system with chronic apical periodontitis caused by caries.
Periodontal Screening (8/3/2018)42
CPITN Scores:
- Maxillary: 3 | 4*
- Mandibular: 3 | 4 | -
Gingival Assessment43
- Colour: Erythematous free gingival margin
- Texture: Oedematous free gingival margin
- Contour: Loss of interdental papilla, blunted
- Biotype: Normal
Plaque Control
- Plaque Score (17/4/2018): 95%
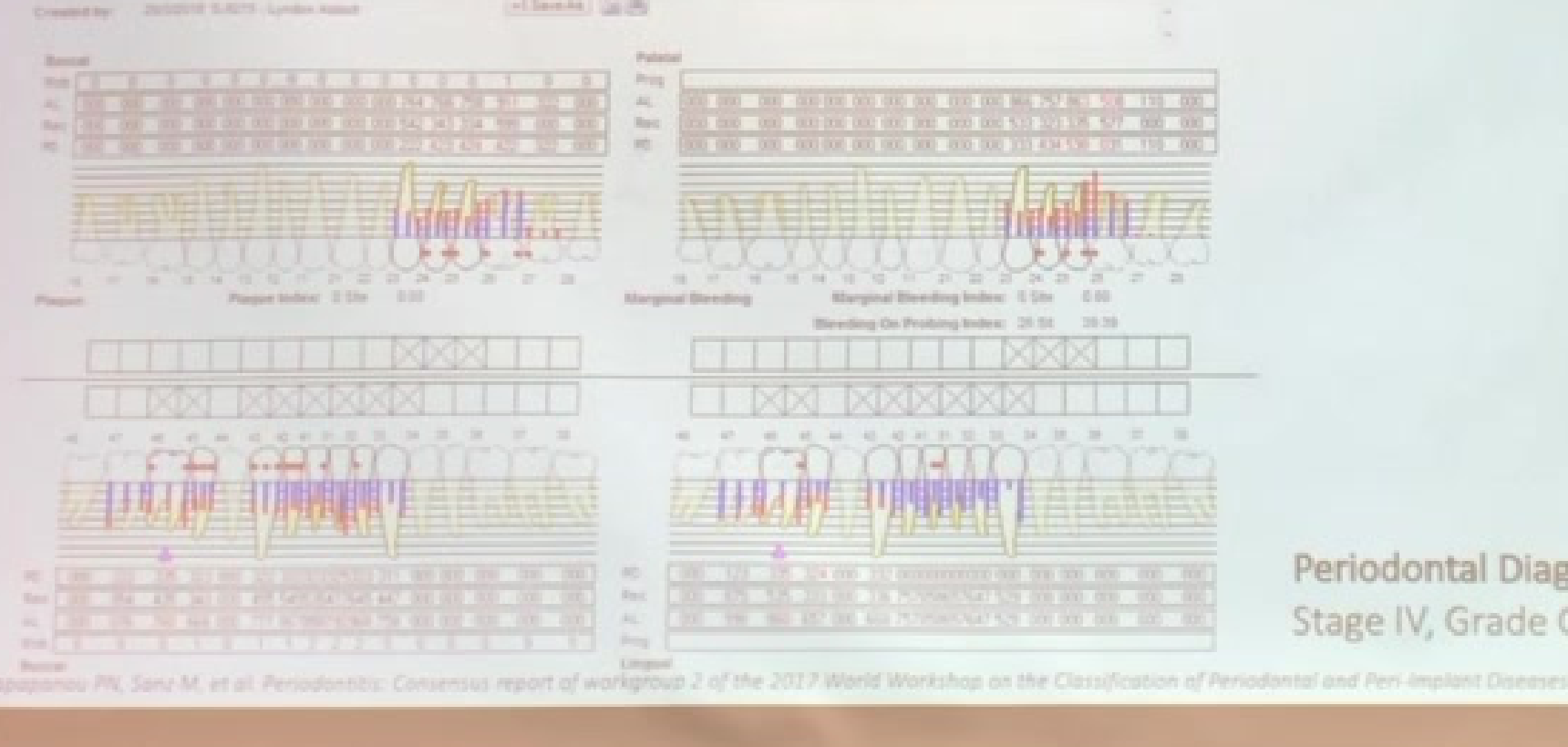
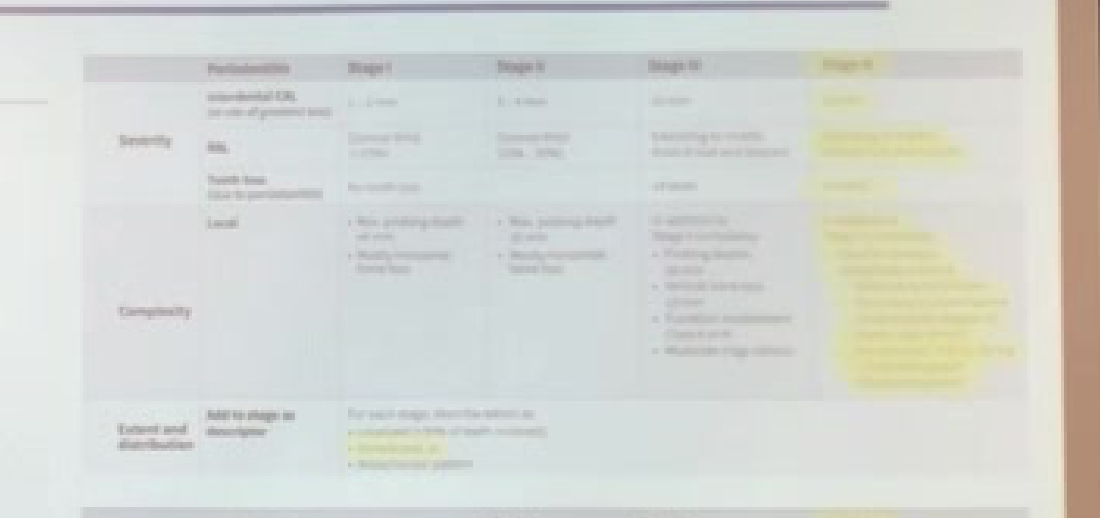
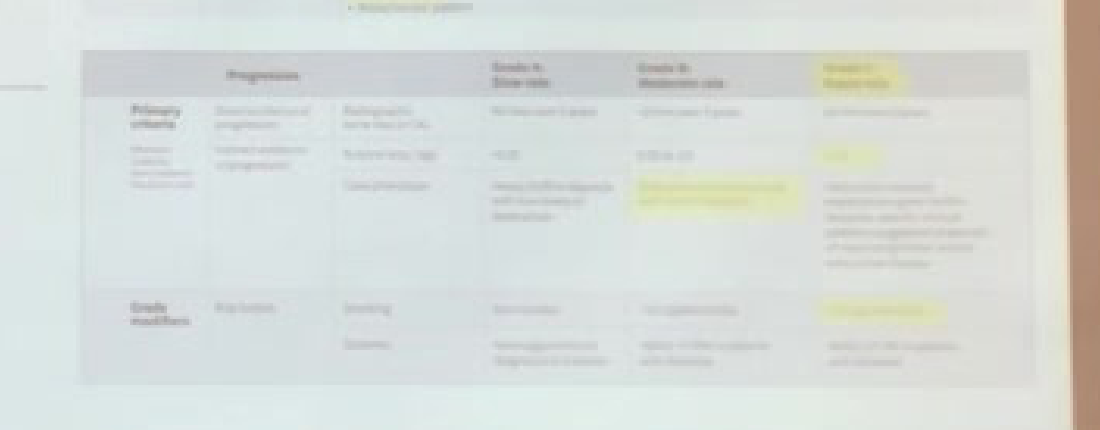
Periodontal Diagnosis
- Generalised periodontitis Stage IV, Grade C
Risk Assessment and Problem List4445
 |  |
Biological and Behavioral Factors46
- Biological: Normal salivary flow, multiple missing teeth, history of trauma.
- Behavioral: Poor oral hygiene, cariogenic diet, smoker.
- CAMBRA: High Caries Risk.
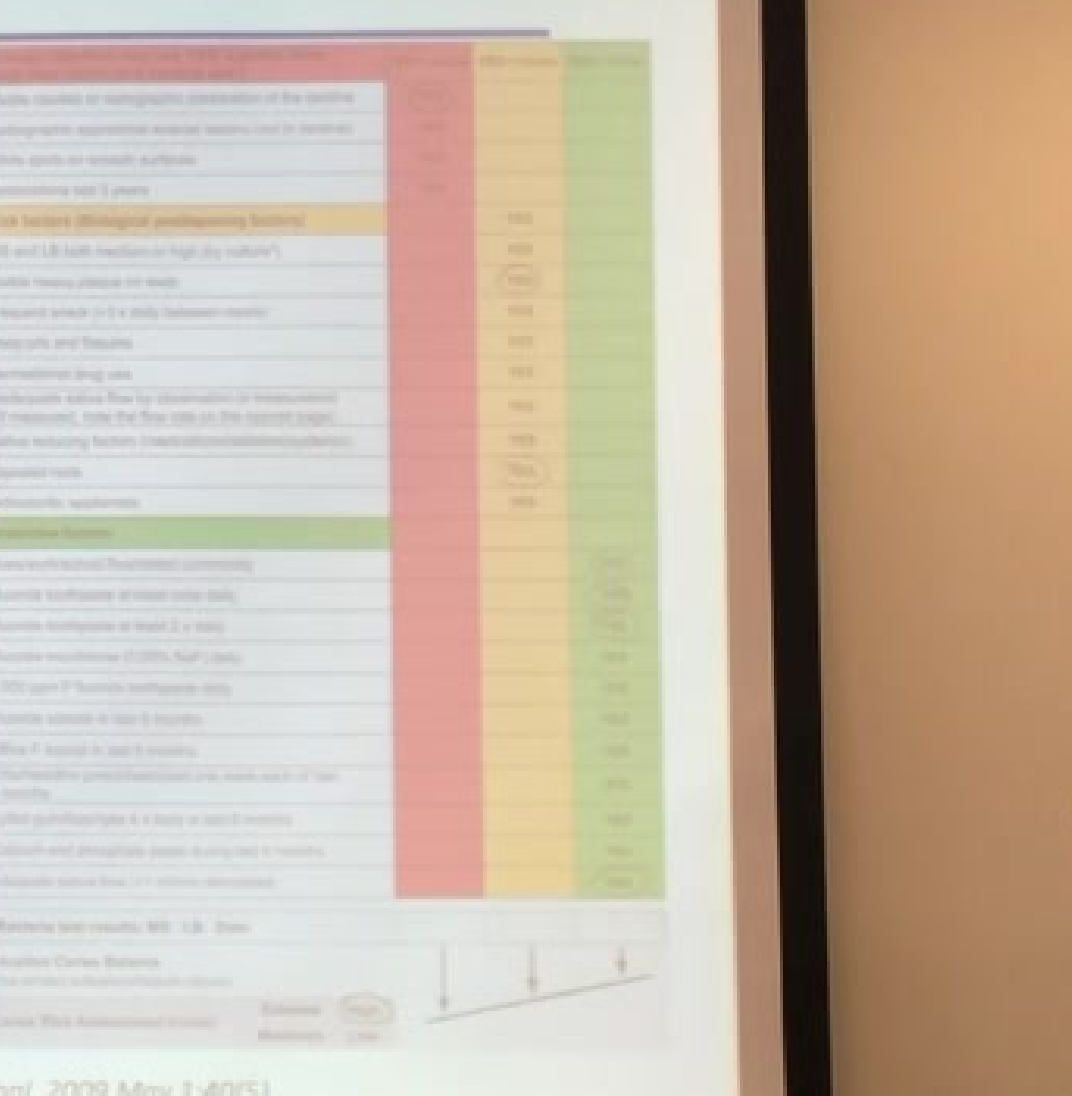
Saliva and Diet Analysis (22/3/2018)
- Saliva Screening:
- pH: 7.0
- Quantity: Normal
- Buffering capacity: Normal
- Dietary Habits:
- High consumption of simple carbohydrates.
- Five cups of coffee per day with 2 teaspoons of sugar each.
- Minimal snacking between meals.
Financial and Personal Factors
- Motivated for treatment and understands current needs.
- Realistic aesthetic expectations.
- Currently unemployed (financial consideration).
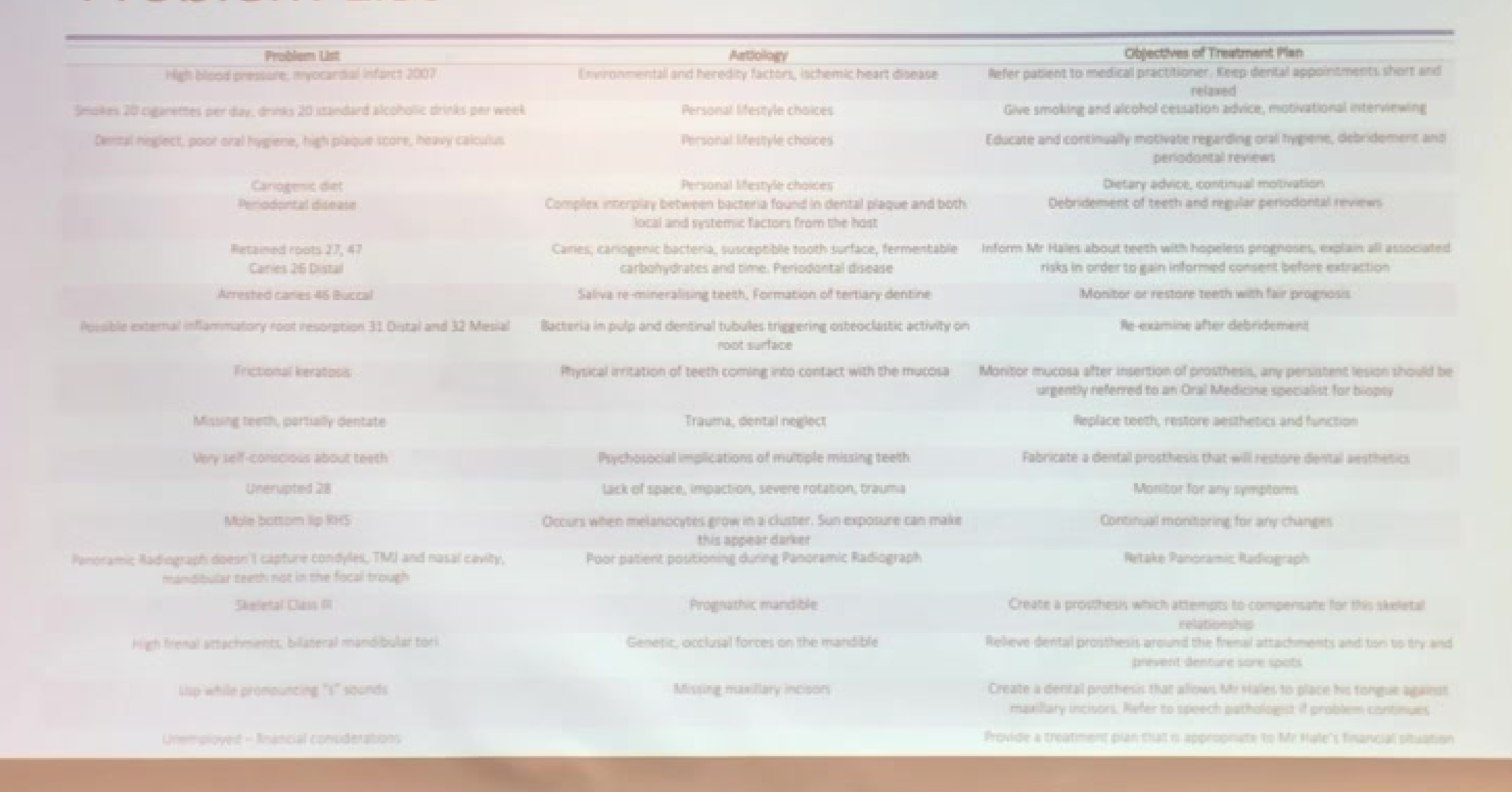
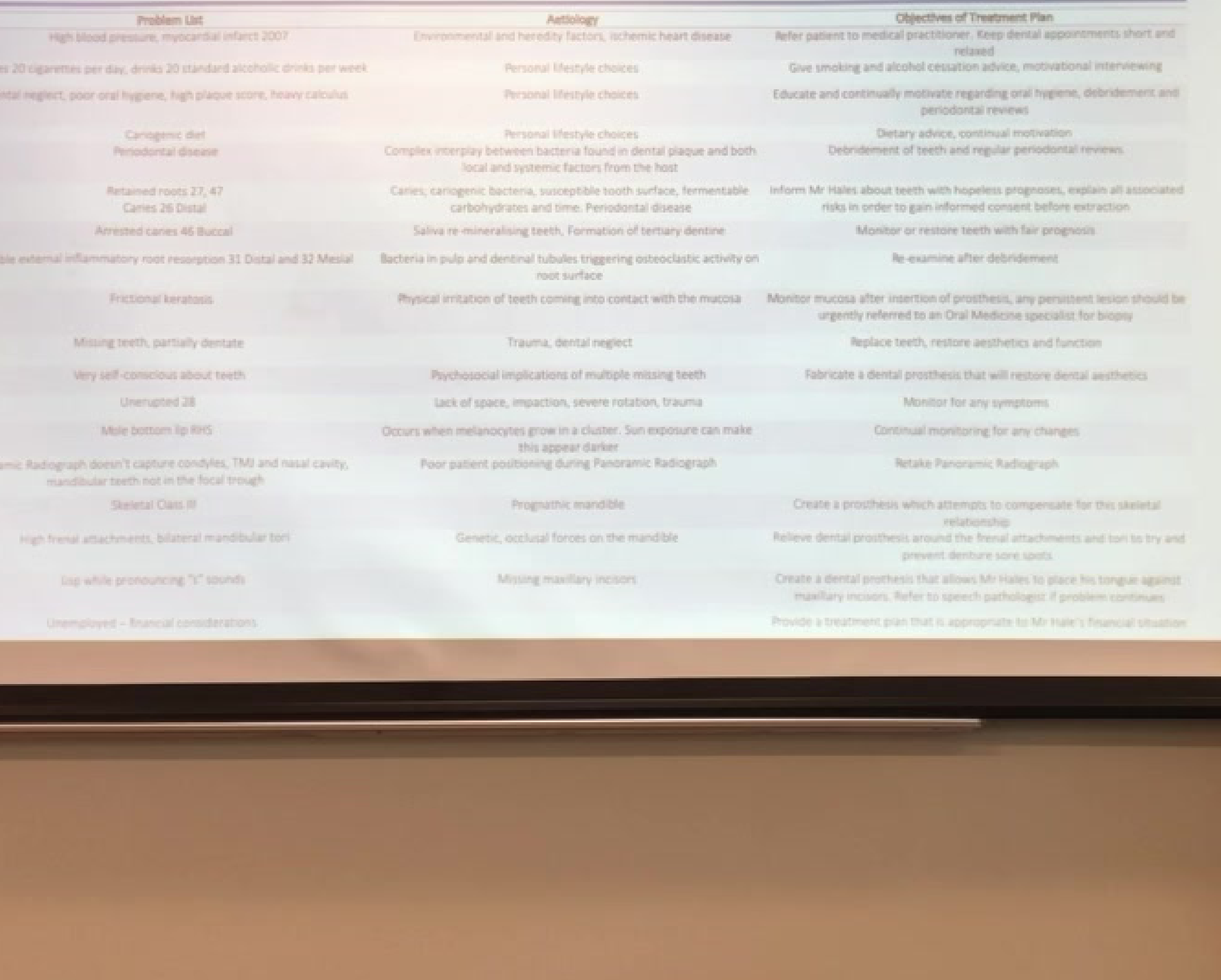
| Problem List | Aetiology | Objectives of Treatment Plan |
|---|---|---|
| High blood pressure, myocardial infarct 2007 | Environmental/heredity factors, ischemic heart disease | Medical referral; short, relaxed appointments |
| Smokes 20 cigarettes/day, 20 standard drinks/week | Personal lifestyle choices | Smoking and alcohol cessation advice |
| Dental neglect, poor hygiene, high plaque/calculus | Personal lifestyle choices | Oral hygiene education, debridement, reviews |
| Cariogenic diet | Personal lifestyle choices | Dietary advice and motivation |
| Periodontal disease | Bacterial plaque and host factors | Debridement and regular reviews |
| Retained roots 27, 47; Caries 26 Distal | Caries and periodontal disease | Informed consent for extractions |
| Arrested caries 46 Buccal | Remineralisation/tertiary dentine | Monitor or restore |
| Possible external inflammatory root resorption 31, 32 | Bacterial triggers | Re-examine after debridement |
| Frictional keratosis | Physical irritation | Monitor; refer if persistent |
| Missing teeth, partially dentate | Trauma, dental neglect | Restore aesthetics and function |
| Self-conscious about teeth | Psychosocial implications | Aesthetic dental prosthesis |
| Unerupted 28 | Lack of space/impaction | Monitor for symptoms |
| Mole bottom lip RHS | Melanocyte cluster | Continual monitoring |
| Suboptimal Panoramic Radiograph | Poor patient positioning | Retake radiograph |
| Skeletal Class II | Prognathic mandible | Compensatory prosthesis design |
| High frenal attachments, mandibular tori | Genetic/occlusal forces | Relieve prosthesis to prevent sore spots |
| Speech issues (“S” sounds) | Missing maxillary incisors | Prosthesis for tongue placement; speech pathology referral if needed |
| Unemployed | Financial considerations | Appropriate treatment plan for financial situation |
| Problem List | Pathology | Objectives of Treatment Plan |
|---|---|---|
| High blood pressure, myocardial infarct 2007 | Environmental/heredity factors, ischaemic heart disease | Medical referral; short, relaxed appointments |
| Smokes 20 cigarettes/day, 20 standard drinks/week | Personal lifestyle choices | Smoking and alcohol cessation advice |
| Dental neglect, poor hygiene, high plaque/calculus | Personal lifestyle choices | Oral hygiene education, debridement, reviews |
| Cariogenic diet | Personal lifestyle choices | Dietary advice and motivation |
| Periodontal disease | Bacterial plaque and host factors | Debridement and regular reviews |
| Retained roots 37, 47; Caries 28 Distal | Caries and periodontal disease | Informed consent for extractions |
| Arrested caries 46 Buccal | Remineralisation/tertiary dentine | Monitor or restore |
| Possible external inflammatory root resorption 31, 32 | Bacterial triggers | Re-examine after debridement |
| Frictional keratosis | Physical irritation | Monitor; refer if persistent |
| Missing teeth, partially dentate | Trauma, dental neglect | Restore aesthetics and function |
| Self-conscious about teeth | Psychosocial implications | Aesthetic dental prosthesis |
| Impacted 28 | Lack of space/impaction | Monitor for symptoms |
| Mole bottom lip RHS | Melanocyte cluster | Continual monitoring |
| Suboptimal Panoramic Radiograph | Poor patient positioning | Retake radiograph |
| Skeletal Class III | Prognathic mandible | Compensatory prosthesis design |
| High frenal attachments, mandibular tori | Genetic/occlusal forces | Relieve prosthesis to prevent sore spots |
| Speech issues (“S” sounds) | Missing maxillary incisors | Prosthesis for tongue placement; speech pathology referral if needed |
| Unemployed | Financial considerations | Appropriate treatment plan for financial situation |
Individual Tooth Assessment and Prognosis47
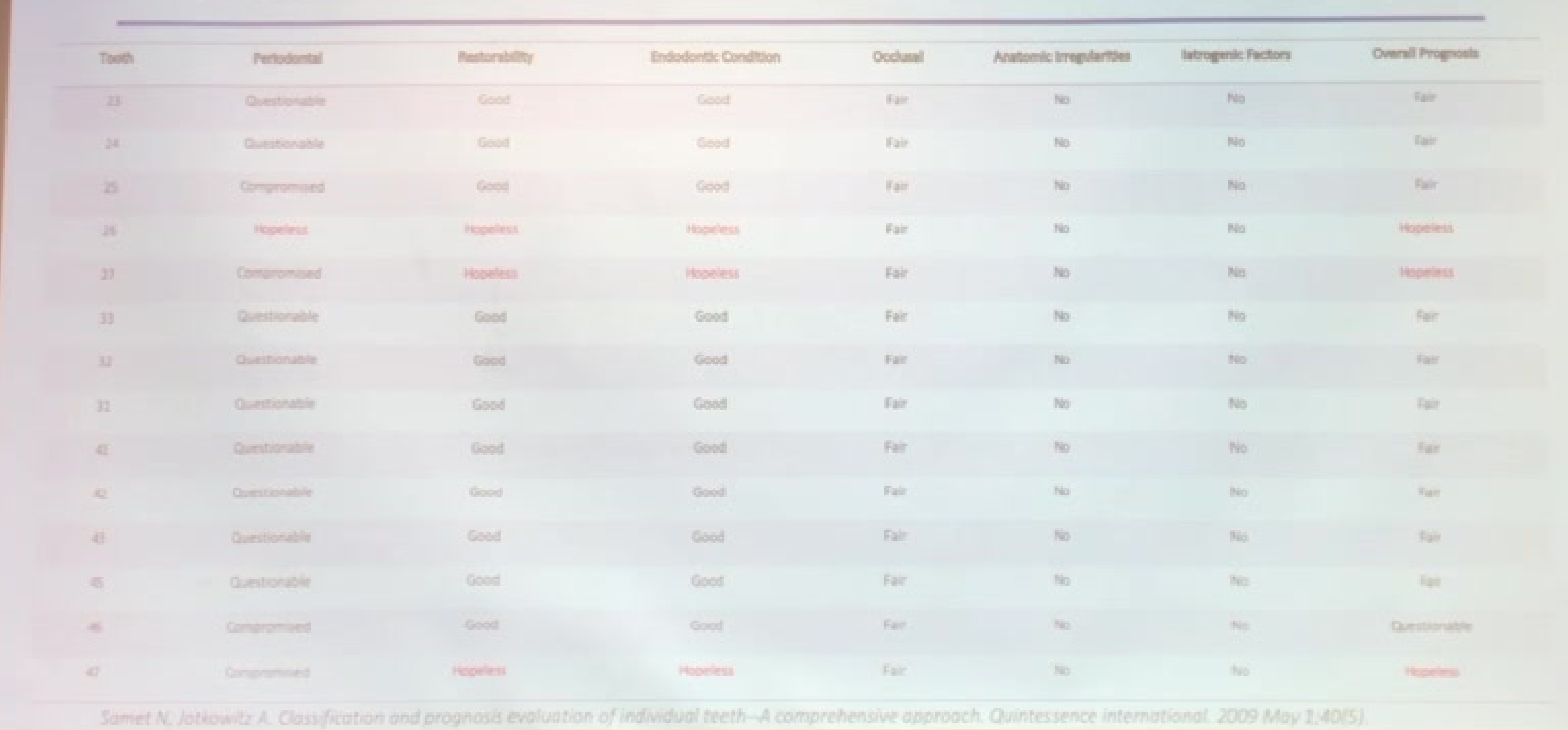
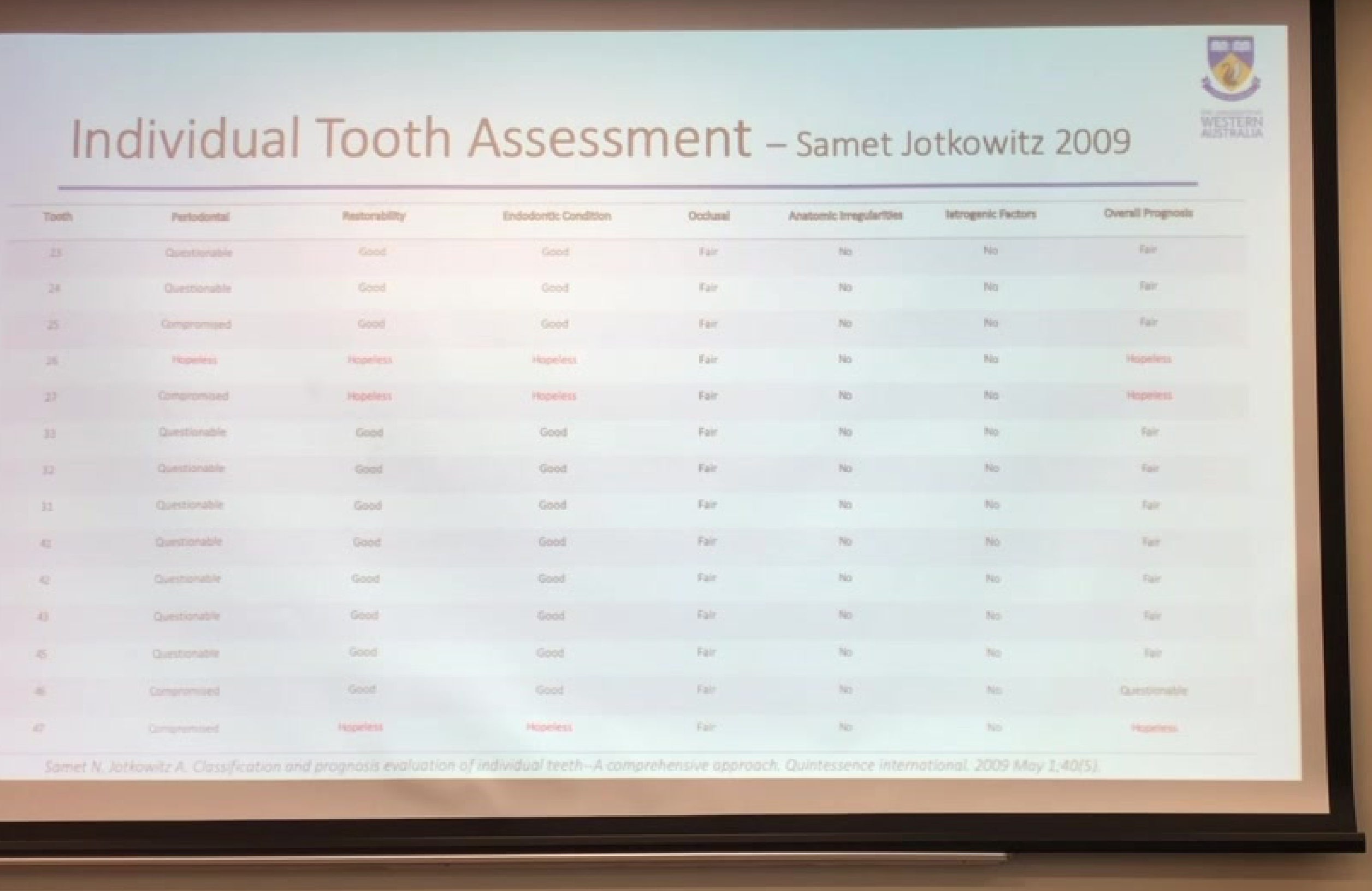
Individual Tooth Assessment (Samet & Jotkowitz, 2009)48
| Tooth | Periodontal | Restorability | Endodontic | Occlusal | Anatomic | Iatrogenic | Overall Prognosis |
|---|---|---|---|---|---|---|---|
| 23 | Questionable | Good | Good | Fair | No | No | Good |
| 24 | Questionable | Good | Good | Fair | No | No | Fair |
| 25 | Compromised | Good | Good | Fair | No | No | Fair |
| 26 | Hopeless | Hopeless | Hopeless | Fair | No | No | Hopeless |
| 27 | Compromised | Hopeless | Hopeless | Fair | No | No | Hopeless |
| 33 | Questionable | Good | Good | Fair | No | No | Fair |
| 32 | Questionable | Good | Good | Fair | No | No | Fair |
| 31 | Questionable | Good | Good | Fair | No | No | Fair |
| 41 | Questionable | Good | Good | Fair | No | No | Fair |
| 42 | Questionable | Good | Good | Fair | No | No | Fair |
| 43 | Questionable | Good | Good | Fair | No | No | Fair |
| 45 | Compromised | Good | Good | Fair | No | No | Questionable |
| 47 | Compromised | Hopeless | Hopeless | Fair | No | No | Hopeless |
| Tooth | Periodontal | Restorability | Endodontic | Occlusal | Anatomic | Iatrogenic | Overall Prognosis |
|---|---|---|---|---|---|---|---|
| 23 | Questionable | Good | Good | Fair | No | No | Fair |
| 24 | Questionable | Good | Good | Fair | No | No | Fair |
| 25 | Compromised | Good | Good | Fair | No | No | Fair |
| 26 | Hopeless | Hopeless | Hopeless | No | No | No | Fair |
| 27 | Compromised | Hopeless | Hopeless | Fair | No | No | Hopeless |
| 33 | Questionable | Good | Good | Fair | No | No | Fair |
| 32 | Questionable | Good | Good | Fair | No | No | Fair |
| 31 | Questionable | Good | Good | Fair | No | No | Fair |
| 41 | Questionable | Good | Good | Fair | No | No | Fair |
| 42 | Questionable | Good | Good | Fair | No | No | Fair |
| 43 | Questionable | Good | Good | Fair | No | No | Fair |
| 45 | Questionable | Good | Good | Fair | No | No | Fair |
| 46 | Compromised | Good | Good | Fair | No | No | Questionable |
| 47 | Compromised | Hopeless | Hopeless | Fair | No | No | Hopeless |
Treatment Alternatives
Periodontal Considerations4950
Periodontal Diagnosis51
- Generalised Periodontitis Stage IV, Grade C
Treatment Options
- No treatment
- Advantages
- Disadvantages
- Periodontal Debridement of teeth
- Advantages
- Disadvantages
Rationale
- Rationale for selected approach provided in clinical assessment.
References
-
Latheef P, Sirajuddin S, et al. Suppl 1: M7: Iatrogenic Damage to the Periodontium Caused by Periodontal Treatment Procedures. The open dentistry journal. 2015,9:203.
-
Generalised Periodontitis Stage IV, Grade C
- No treatment
- Advantages
- Disadvantages
- Periodontal Debridement of teeth
- Advantages
- Disadvantages
-
Rationale for selected approach provided in clinical assessment.
-
Latheef P, Sirajuddin S, et al. Suppl 1: M7: Iatrogenic Damage to the Periodontium Caused by Periodontal Treatment Procedures. The open dentistry journal. 2015;9.203.
Oral Surgery Considerations
Problem: Retained Roots and Unrestorable Teeth52
- Affected Teeth: Retained roots 27, 47; unrestorable 26
- Options:
- No treatment
- Advantages
- Disadvantages
- Extraction of 26, 27 and 46
- Advantages
- Disadvantages
- No treatment
- Rationale: Clinical justification for surgical intervention.
Problem: Retained Unerupted Tooth
- Affected Tooth: Retained unerupted 28
- Options:
- No treatment
- Advantages
- Disadvantages
- Extraction of 28
- Advantages
- Disadvantages
- No treatment
- Rationale: Clinical justification for surgical intervention.
References
- Steed MB. The indications for third-molar extractions. The Journal of the American Dental Association. 2014 Jun 1;145(6):570-3.
Problem: Retained Roots and Unrepairable Teeth53
-
Affected Teeth: Retained roots 27, 47; unrepairable 26
-
Options:
- No treatment
- Advantages
- Disadvantages
- Extraction of 26, 27 and 46
- Advantages
- Disadvantages
- No treatment
-
Rationale: Clinical justification for surgical intervention.
-
Affected Tooth: Retained unerupted 28
-
Options:
- No treatment
- Advantages
- Disadvantages
- Extraction of 28
- Advantages
- Disadvantages
- No treatment
-
Rationale: Clinical justification for surgical intervention.
-
Steele, MS. The indications for third-molar extractions. The Journal of the American Dental Association. 2014 Jun 1;145(6):570-0.
Prosthodontic Considerations5455
Problem: Missing Teeth56
- Partially dentate status.
Treatment Options
- No treatment
- Partial acrylic maxillary and mandibular dentures
- Full maxillary acrylic denture and partial acrylic mandibular denture
- Partial Co/Cr maxillary and mandibular denture
- Implant supported removable or fixed prosthesis
Clinical Evaluation
- Advantages
- Disadvantages
- Rationale
Clinical Philosophy
“Whatever treatment mode is selected should minimize the long-term biological and soft tissue costs to the patient” — McCord, Smales 2012
References
-
Suwal P, Singh RK, Ayer A, Ray DK, Roy RK. Cast Partial Denture versus Acrylic Partial Denture for Replacement of Missing Teeth in Partially Edentulous Patients. Journal of Dental Materials and Techniques. 2017 Mar 1;6(1):27-34.
-
McCord F, Smales R. Oral diagnosis and treatment planning: part 7. Treatment planning for missing teeth. British dental journal. 2012 Oct;213(7):341.
-
Petridis H, Hempston TJ. Periodontal considerations in removable partial denture treatment: a review of the literature. The international journal of prosthodontics. 2001;14(2):164-72.
-
Partially dentate status.
-
No treatment
-
Partial acrylic maxillary and mandibular dentures
-
Full maxillary acrylic denture and partial acrylic mandibular denture
-
Partial Co/Cr maxillary and mandibular denture
-
Implant supported removable or fixed prosthesis
-
Advantages
-
Disadvantages
-
Rationale
“Whatever treatment mode is selected should minimize the long-term biological and soft tissue costs to the patient” — McCord, Smales 2012
- Suwal P, Singh RK, Ayer A, Roy DK, Roy RK. Cast Partial Denture versus Acrylic Partial Denture for Replacement of Missing Teeth in Partially Edentulous Patients. Journal of Dental Materials and Techniques. 2017 Mar 1;6(1):27-34.
- McCord F, Smales R. Oral diagnosis and treatment planning: part 7. Treatment planning for missing teeth. British dental journal. 2012 Oct;213(7):341.
- Petridis H, Hempton TJ. Periodontal considerations in removable partial denture treatment: a review of the literature. The international journal of prosthodontics. 2001;14(2):164-72.
Delivery of Treatment
Control Phase
Treatment Timeline57
8/3/2018
- Referral to medical practitioner
10/4/2018
- Informed consent to carry out treatment plan
- Extraction of teeth 26, 27, and 47
17/4/2018
- Review of extraction sockets
- Periodontal debridement
30/4/2018
- Periapical radiograph (PA): 25 distal arrested caries
8/5/2018
- Dietary advice
- Oral hygiene instruction
- Fluoride application
- Motivational interviewing for smoking and alcohol cessation
 |  |
Holding Phase
Clinical Reviews and Preparations58
23/5/2018
- Periodontal review
- Periapical radiograph (PA): 41 and 31 for possible external inflammatory resorption
- Plaque score: 50%
- Oral hygiene instruction
- Periodontal debridement
13/7/2018
- Diagnostic base and rim
26/7/18
- 46 Buccal (BUC) composite restoration
- Pulp testing to reassess abutment teeth
31/7/18
- Panoramic radiograph
The holding phase of treatment focused on maintaining the progress achieved during the intensive intervention period while gradually transitioning the patient toward self-management. This phase was characterized by a reduction in the frequency of clinical sessions and an increased emphasis on the patient’s application of learned strategies in real-world environments.
 |  |
 |
Clinical Objectives and Monitoring59
- Stability Maintenance: Regular check-ins were conducted to ensure that the patient remained stable and that there was no regression in functional gains.
- Symptom Surveillance: Ongoing monitoring for any emerging symptoms or triggers that might necessitate a temporary return to more intensive support.
- Medication Management: Continued oversight of the pharmacological regimen to ensure adherence and to evaluate the long-term efficacy of the prescribed dosages.
Transition to Self-Management
- Skill Generalization: Encouraging the patient to utilize coping mechanisms and behavioral techniques independently in various social and professional contexts.
- Support System Integration: Strengthening the patient’s reliance on their natural support networks, including family, friends, and community resources, to decrease clinical dependency.
- Relapse Prevention Planning: Refining the patient’s individualized relapse prevention plan, ensuring they could identify early warning signs and knew the specific steps to take if symptoms exacerbated.
Holding Stage Review60
- 31/7/2018
 |  |  |
 |  |
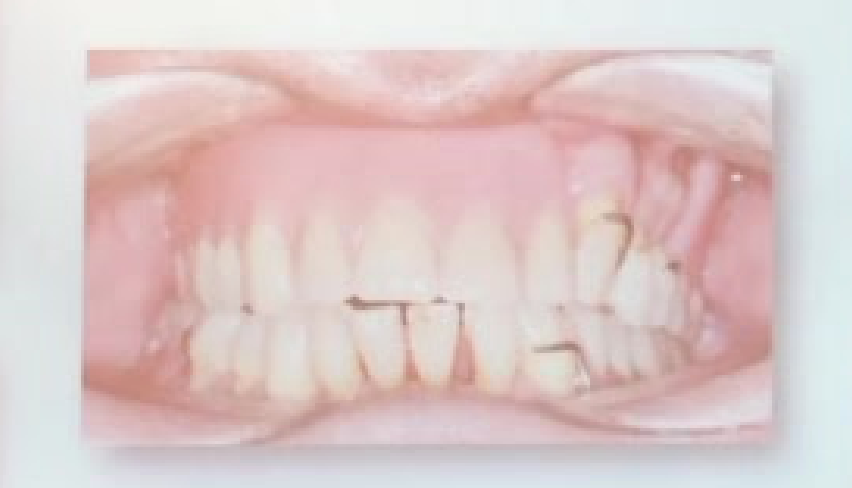
Reconstructive Phase61
 |  |  |
 |  |
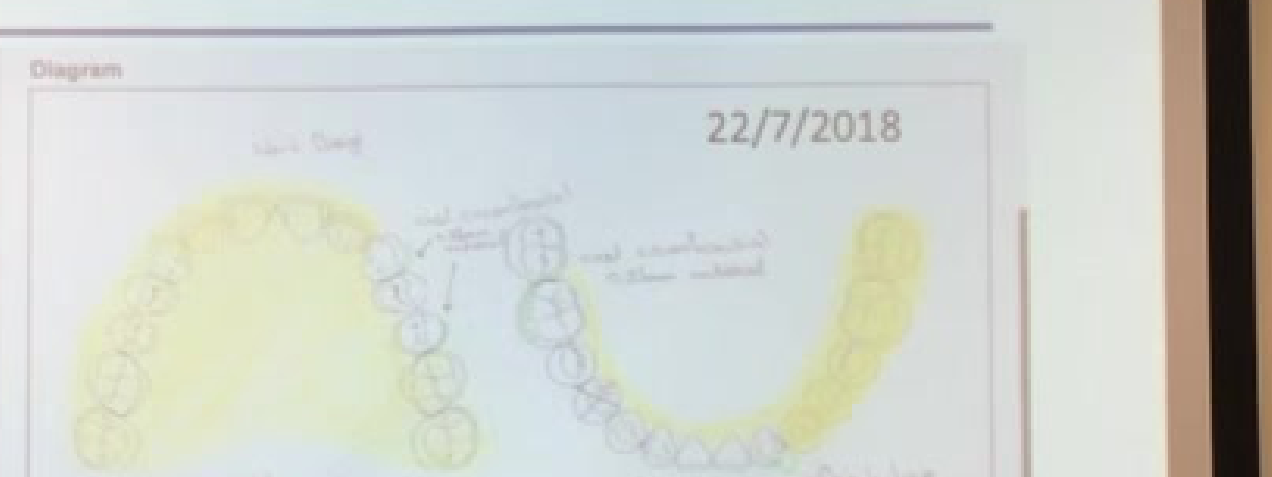
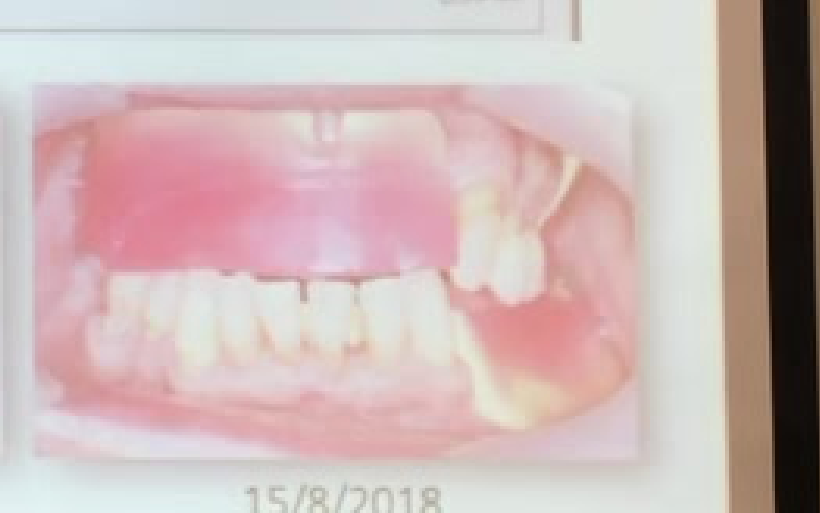
Clinical Timeline62
- 22/7/2018: Denture design sign off
- 31/7/2018: Secondary impressions and Face-bow
- 15/8/2018: Maxillomandibular Relationship (MMR)
- 5/9/2018: Anterior tooth set up
- 14/9/2018: Posterior tooth set up
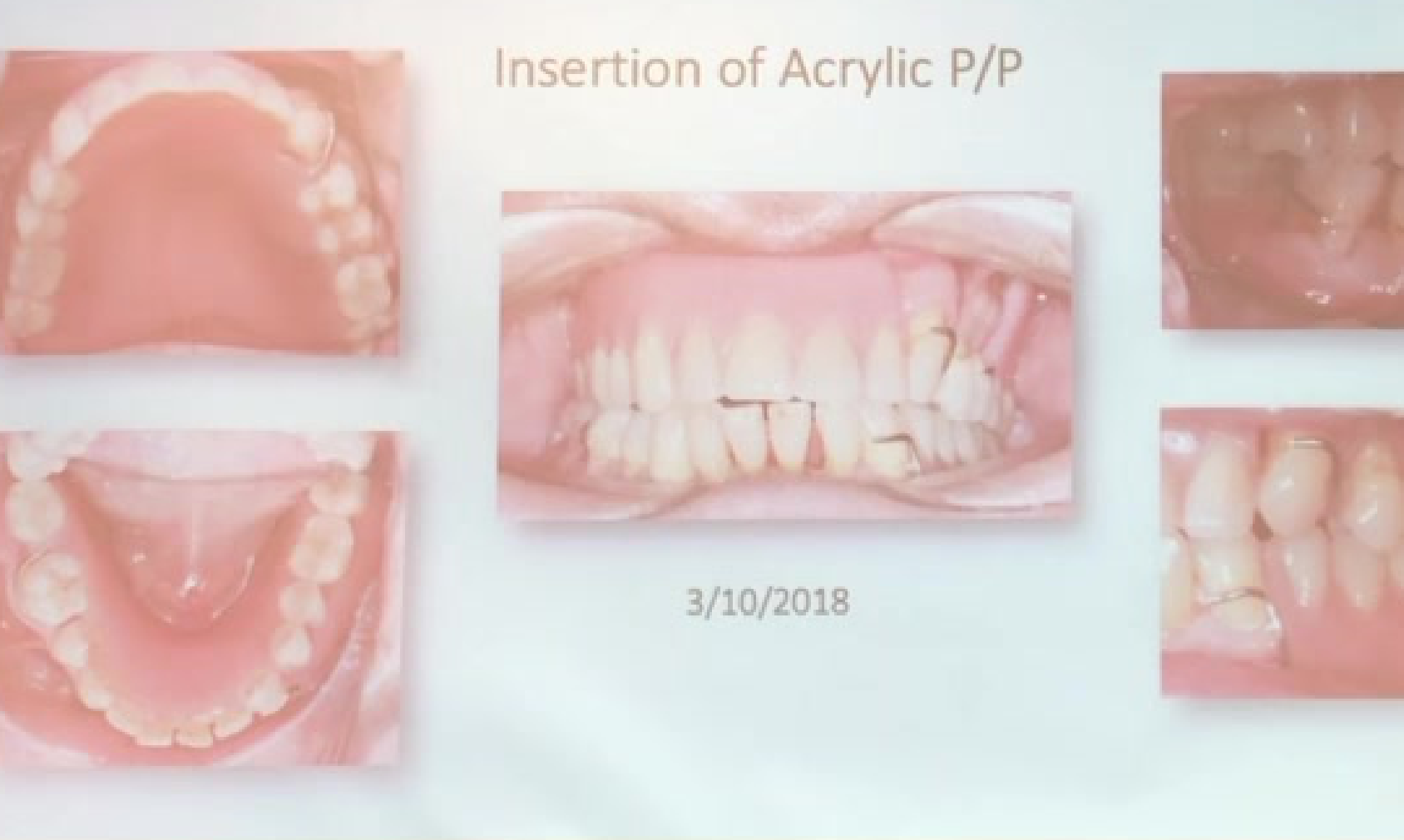
- 3/10/2018: Insertion of P/P acrylic denture
 |  |
 |
References
- Davenport JC, Basker RM, et al. Prosthetics: A system of design. British dental journal. 2000 Dec; 189(11): 586.
Insertion of Acrylic P/P63
- 3/10/2018
Dental presentation slide showing various views of a mouth with an acrylic prosthesis in place, head and shoulders of presenter.
Maintenance Phase64
 |  |
 |  |
Clinical Timeline65
- 10/10/2018: Denture review
- 19/10/2018: Denture review 2
- 21/1/2019:
- Periodic oral examination
- Plaque score 30%
- CPITN:
- 2 2
- 2 -
- Debridement
- Fluoride application
- 6/6/2019:
- Periodic oral examination
- Full periodontal chart
- Debridement
- Refer to oral surgery
- 5/7/2019:
- Oral hygiene review
- Removal of calculus (subsequent visit)
- Fluoride application
- 13/11/2019:
- Periodic oral examination
- Full periodontal chart
- 19/11/2019:
- Debridement
- Motivation for oral and denture hygiene
Review Appointment66
-
6/6/2019
-
Denture in situ
-
6/6/2019
-
Denture in situ
Clinical Outcomes and Complications
Periodontal Staging and Grading Summary Table67
| Staging | Flinard Phase | Stage 1 | Stage 2 | Stage 3 | Stage 4 |
|---|---|---|---|---|---|
| Severity | Stage I-III | Stage I-IV | Stage V | Stage VI | Stage VII |
| Complexity | Localised | Moderate | Severe | Generalised | Generalised |
| Reference Distribution | Add to degree of involvement | Add to degree of involvement | Add to degree of involvement | Add to degree of involvement | Add to degree of involvement |
| Progression | Moderate | Moderate | Moderate | Moderate | Moderate |
| Reference Classification | No reference | No reference | No reference | No reference | No reference |
| Staging | Staging | Staging | Staging | Staging | Staging |
Periodontal Diagnosis: Generalised periodontitis Stage IV, Grade C
 |  |
 |
References
- Papapanou PN, Sanz M, et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. Journal of periodontology. 2018 Jun;89(5):173-82.
Treatment Complications and Issues68
Clinical Issues (8/5/2018)69
- Arrested Caries: Detected on 25 Distal after 26 was extracted.
- Management: PA, Fluoride, Monitor.
- Secondary Impressions: Overfilled the maxillary special tray with PVS.
- Oral Hygiene: Requirement for continual motivation.
- Aesthetics: Maxillary midline alignment during anterior tooth set up.
- Eruption Issues: Partially erupted 28.
References
-
Evans RW, Pakdaman A, Dennison PI, Howe EL. The Caries Management System: an evidence-based preventive strategy for dental practitioners. Application for adults. Australian dental journal. 2008 Mar;53(1):83-92
-
After the 26 was extracted arrested caries was detected on 25 Distal PA
-
Fluoride
-
Monitor
-
Secondary impressions: Overfilled the maxillary special tray with PVS
-
Oral Hygiene: Continual motivation
-
Maxillary midline during anterior tooth set up
-
Partially erupted 28
-
Evans RW, Pakdaman A, Dennison PJ, Howe EL. The Caries Management System: an evidence-based preventive strategy for dental practitioners. Application for adults. Australian dental journal. 2008 Mar;53(1):83-92
Periodontal Prognosis7071
 |  |
Prognostic Factors72
- Dependent of the ability of the patient to maintain their oral environment.
- Success Rates: 95% success rate after five years (Buchmann, Nunn 2002).
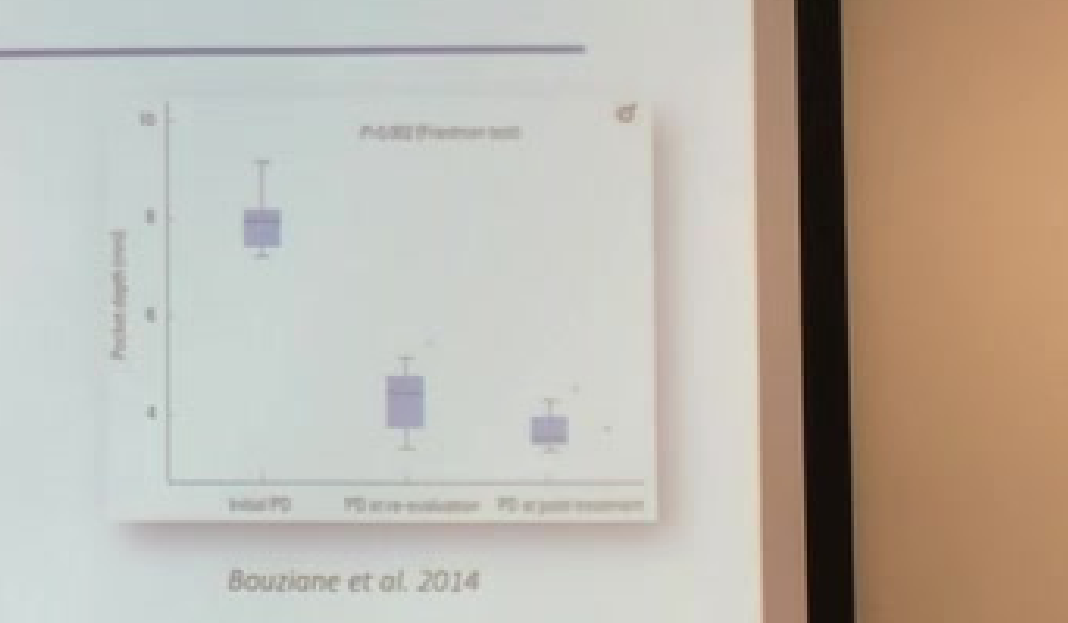
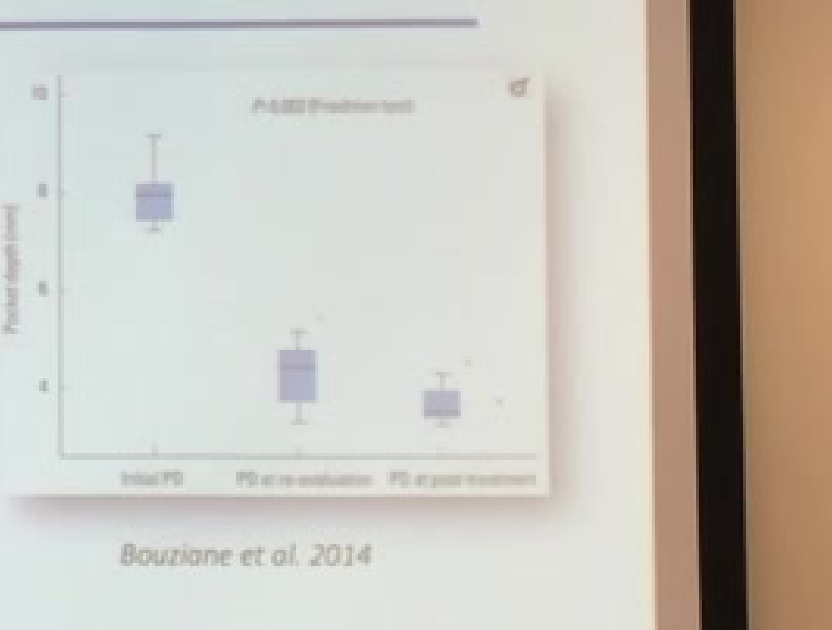
- Treatment Outcomes (Bouziane, Benrachadi 2014):
- Baseline: 7.94mm
- Re-evaluation: 4.33mm
- Post-treatment: 3.54mm
- Inflammation was resolved and angular bone defects were repaired in all cases.
- Impact of Smoking:
- Smoking showed a 3.8 times increase in non-responding patients (Hughes, Syed 2006).
- Smokers had a 0.7mm less reduction in pocket depths (Darby, Hodge 2005).

References
-
Buchmann R, Nunn ME, et al. Aggressive periodontitis: 5-year follow-up of treatment. Journal of Periodontology. 2002 Jun;73(6):675-83.
-
Bouziane A, Benrachadi L, et al. Outcomes of nonsurgical periodontal therapy in severe generalized aggressive periodontitis. Journal of periodontal & implant science. 2014 Aug 1;44(4):201-6.
-
Hughes FJ, Syed M, et al. Prognostic factors in the treatment of generalized aggressive periodontitis: II. Effects of smoking on initial outcome. Journal of clinical periodontology. 2006 Sep;33(9):671-6.
-
Darby IB, Hodge PI, et al. Clinical and microbiological effect of scaling and root planing in smoker and non-smoker chronic and aggressive periodontitis patients. Journal of clinical periodontology. 2005 Feb;32(2):200-6.
-
Dependent of the ability of the patient to maintain their oral environment
-
Buchmann, Nunn 2002: 95% success rate after five years
-
Bouziane, Benrachadi 2014:
- Baseline 7.94mm
- Re-evaluation 4.33mm
- Post-treatment 3.54mm
- Inflammation was resolved and angular bone defects were repaired in all cases
-
Smoking Impact:
- 3.8 times increase in non-responding patients (Hughes, Syed 2006)
- 0.7mm less reduction in pocket depths (Darby, Hodge 2005)
-
Buchmann R, Nunn ME, et al. Aggressive periodontitis: 5-year follow-up of treatment. Journal of Periodontology. 2002 Jun;73(6):675-83.
-
Bouziane A, Benrachadi L, et al. Outcomes of nonsurgical periodontal therapy in severe generalized aggressive periodontitis. Journal of periodontal & implant science. 2014 Aug 1;44(4):201-6.
-
Hughes FI, Syed M, et al. Prognostic factors in the treatment of generalized aggressive periodontitis: II. Effects of smoking on initial outcome. Journal of clinical periodontology. 2006 Sep;33(9):671-6.
-
Darby IB, Hodge PJ, et al. Clinical and microbiological effect of scaling and root planing in smoker and non-smoker chronic and aggressive periodontitis patients. Journal of clinical periodontology. 2005 Feb;32(2):200-6.
Prosthodontic Prognosis

Footnotes
-
Original PDF page 1: Case Presentation - Dr Lyndon P Abbott slides, p.1 ↩
-
Original PDF page 2: Case Presentation - Dr Lyndon P Abbott slides, p.2 ↩
-
Original PDF page 3: Case Presentation - Dr Lyndon P Abbott slides, p.3 ↩
-
Original PDF page 4: Case Presentation - Dr Lyndon P Abbott slides, p.4 ↩
-
Original PDF page 5: Case Presentation - Dr Lyndon P Abbott slides, p.5 ↩
-
Original PDF page 6: Case Presentation - Dr Lyndon P Abbott slides, p.6 ↩
-
Original PDF page 7: Case Presentation - Dr Lyndon P Abbott slides, p.7 ↩
-
Original PDF page 8: Case Presentation - Dr Lyndon P Abbott slides, p.8 ↩
-
Original PDF page 9: Case Presentation - Dr Lyndon P Abbott slides, p.9 ↩
-
Original PDF page 10: Case Presentation - Dr Lyndon P Abbott slides, p.10 ↩
-
Original PDF page 11: Case Presentation - Dr Lyndon P Abbott slides, p.11 ↩
-
Original PDF page 12: Case Presentation - Dr Lyndon P Abbott slides, p.12 ↩
-
Original PDF page 13: Case Presentation - Dr Lyndon P Abbott slides, p.13 ↩
-
Original PDF page 15: Case Presentation - Dr Lyndon P Abbott slides, p.15 ↩
-
Original PDF page 14: Case Presentation - Dr Lyndon P Abbott slides, p.14 ↩
-
Original PDF page 16: Case Presentation - Dr Lyndon P Abbott slides, p.16 ↩
-
Original PDF page 17: Case Presentation - Dr Lyndon P Abbott slides, p.17 ↩
-
Original PDF page 18: Case Presentation - Dr Lyndon P Abbott slides, p.18 ↩
-
Original PDF page 19: Case Presentation - Dr Lyndon P Abbott slides, p.19 ↩
-
Original PDF page 20: Case Presentation - Dr Lyndon P Abbott slides, p.20 ↩
-
Original PDF page 21: Case Presentation - Dr Lyndon P Abbott slides, p.21 ↩
-
Original PDF page 22: Case Presentation - Dr Lyndon P Abbott slides, p.22 ↩
-
Original PDF page 23: Case Presentation - Dr Lyndon P Abbott slides, p.23 ↩
-
Original PDF page 24: Case Presentation - Dr Lyndon P Abbott slides, p.24 ↩
-
Original PDF page 25: Case Presentation - Dr Lyndon P Abbott slides, p.25 ↩
-
Original PDF page 26: Case Presentation - Dr Lyndon P Abbott slides, p.26 ↩
-
Original PDF page 27: Case Presentation - Dr Lyndon P Abbott slides, p.27 ↩
-
Original PDF page 28: Case Presentation - Dr Lyndon P Abbott slides, p.28 ↩
-
Original PDF page 29: Case Presentation - Dr Lyndon P Abbott slides, p.29 ↩
-
Original PDF page 30: Case Presentation - Dr Lyndon P Abbott slides, p.30 ↩
-
Original PDF page 31: Case Presentation - Dr Lyndon P Abbott slides, p.31 ↩
-
Original PDF page 32: Case Presentation - Dr Lyndon P Abbott slides, p.32 ↩
-
Original PDF page 33: Case Presentation - Dr Lyndon P Abbott slides, p.33 ↩
-
Original PDF page 34: Case Presentation - Dr Lyndon P Abbott slides, p.34 ↩
-
Original PDF page 35: Case Presentation - Dr Lyndon P Abbott slides, p.35 ↩
-
Original PDF page 36: Case Presentation - Dr Lyndon P Abbott slides, p.36 ↩
-
Original PDF page 37: Case Presentation - Dr Lyndon P Abbott slides, p.37 ↩
-
Original PDF page 38: Case Presentation - Dr Lyndon P Abbott slides, p.38 ↩
-
Original PDF page 39: Case Presentation - Dr Lyndon P Abbott slides, p.39 ↩
-
Original PDF page 40: Case Presentation - Dr Lyndon P Abbott slides, p.40 ↩
-
Original PDF page 41: Case Presentation - Dr Lyndon P Abbott slides, p.41 ↩
-
Original PDF page 42: Case Presentation - Dr Lyndon P Abbott slides, p.42 ↩
-
Original PDF page 43: Case Presentation - Dr Lyndon P Abbott slides, p.43 ↩
-
Original PDF page 45: Case Presentation - Dr Lyndon P Abbott slides, p.45 ↩
-
Original PDF page 46: Case Presentation - Dr Lyndon P Abbott slides, p.46 ↩
-
Original PDF page 44: Case Presentation - Dr Lyndon P Abbott slides, p.44 ↩
-
Original PDF page 48: Case Presentation - Dr Lyndon P Abbott slides, p.48 ↩
-
Original PDF page 47: Case Presentation - Dr Lyndon P Abbott slides, p.47 ↩
-
Original PDF page 50: Case Presentation - Dr Lyndon P Abbott slides, p.50 ↩
-
Original PDF page 51: Case Presentation - Dr Lyndon P Abbott slides, p.51 ↩
-
Original PDF page 49: Case Presentation - Dr Lyndon P Abbott slides, p.49 ↩
-
Original PDF page 52: Case Presentation - Dr Lyndon P Abbott slides, p.52 ↩
-
Original PDF page 53: Case Presentation - Dr Lyndon P Abbott slides, p.53 ↩
-
Original PDF page 55: Case Presentation - Dr Lyndon P Abbott slides, p.55 ↩
-
Original PDF page 56: Case Presentation - Dr Lyndon P Abbott slides, p.56 ↩
-
Original PDF page 54: Case Presentation - Dr Lyndon P Abbott slides, p.54 ↩
-
Original PDF page 57: Case Presentation - Dr Lyndon P Abbott slides, p.57 ↩
-
Original PDF page 58: Case Presentation - Dr Lyndon P Abbott slides, p.58 ↩
-
Original PDF page 59: Case Presentation - Dr Lyndon P Abbott slides, p.59 ↩
-
Original PDF page 60: Case Presentation - Dr Lyndon P Abbott slides, p.60 ↩
-
Original PDF page 63: Case Presentation - Dr Lyndon P Abbott slides, p.63 ↩
-
Original PDF page 61: Case Presentation - Dr Lyndon P Abbott slides, p.61 ↩
-
Original PDF page 62: Case Presentation - Dr Lyndon P Abbott slides, p.62 ↩
-
Original PDF page 66: Case Presentation - Dr Lyndon P Abbott slides, p.66 ↩
-
Original PDF page 64: Case Presentation - Dr Lyndon P Abbott slides, p.64 ↩
-
Original PDF page 65: Case Presentation - Dr Lyndon P Abbott slides, p.65 ↩
-
Original PDF page 67: Case Presentation - Dr Lyndon P Abbott slides, p.67 ↩
-
Original PDF page 69: Case Presentation - Dr Lyndon P Abbott slides, p.69 ↩
-
Original PDF page 68: Case Presentation - Dr Lyndon P Abbott slides, p.68 ↩
-
Original PDF page 71: Case Presentation - Dr Lyndon P Abbott slides, p.71 ↩
-
Original PDF page 72: Case Presentation - Dr Lyndon P Abbott slides, p.72 ↩
-
Original PDF page 70: Case Presentation - Dr Lyndon P Abbott slides, p.70 ↩