Case Portfolio 20191
Final Year Student
Doctor of Dental Medicine (DMD)
University of Western Australia
 |  |  |
 |  |  |
 |  |  |
 |
1. Aesthetic removable restorative case2
- 1.1 Presenting complaint (Page 3)
- 1.3 Medical history (Page 3)
- 1.17 Problem list (Page 14)
- 1.18 Diagnosis (Page 14)
- 1.19 Treatment options (Page 15)
- 1.20 Management plan (Page 18)
- 1.22 Before and after treatment photographs (Page 26)
2. Functional removable restorative case
- 2.1 Presenting complaint (Page 27)
- 2.3 Medical history (Page 27)
- 2.15 Problem list (Page 36)
- 2.16 Diagnosis (Page 36)
- 2.17 Treatment options (Page 37)
- 2.28 Management plan (Page 39)
- 2.19 Before and after treatment photographs (Page 42)
3. Aesthetic fixed restorative case
- 3.1 Presenting complaint (Page 43)
- 3.3 Medical history (Page 43)
- 3.14 Problem list (Page 51)
- 3.15 Diagnosis (Page 51)
- 3.16 Treatment options (Page 52)
- 3.17 Management plan (Page 55)
- 3.18 Before and after treatment photographs (Page 60)
4. Functional fixed restorative case
- 4.1 Presenting complaint (Page 61)
- 4.3 Medical history (Page 61)
- 4.15 Problem list (Page 70)
- 4.16 Diagnosis (Page 70)
- 4.17 Treatment options (Page 71)
- 4.18 Management plan (Page 73)
- 4.19 Before and after treatment photographs (Page 77)
5. Multidisciplinary case
- 5.1 Presenting complaint (Page 78)
- 5.3 Medical history (Page 78)
- 5.16 Problem list (Page 90)
- 5.17 Diagnosis (Page 90)
- 5.18 Treatment options (Page 91)
- 5.19 Management plan (Page 93)
- 5.20 Before and after treatment photographs (Page 98)
6. References
- References (Page 99)
Case 1: Aesthetic Removable Restorative Case
Presenting Complaint3
- “I hate the appearance of my lower teeth, I want them all pulled out”.
- “Three of my teeth have snapped off”.
- “My upper denture keeps falling out”.
 |  |
History of Presenting Complaint
- Aesthetics: The patient decided she can no longer tolerate the appearance of her lower teeth following negative comments from colleagues. This is the main driving factor for treatment.
- Denture Stability: The upper denture requires daily use of PolyDent Denture Adhesive since the loss of an upper tooth.
- Dental History and Attitude:
- Long-term deteriorating dentition due to patient neglect and multiple missed/cancelled appointments.
- Patient expresses embarrassment and admits to allowing decay and gum disease to progress.
- Loss of faith in the dental profession due to the failure of previous restorations (falling out or recurring decay).
Clinical Presentation and History
Medical History Summary
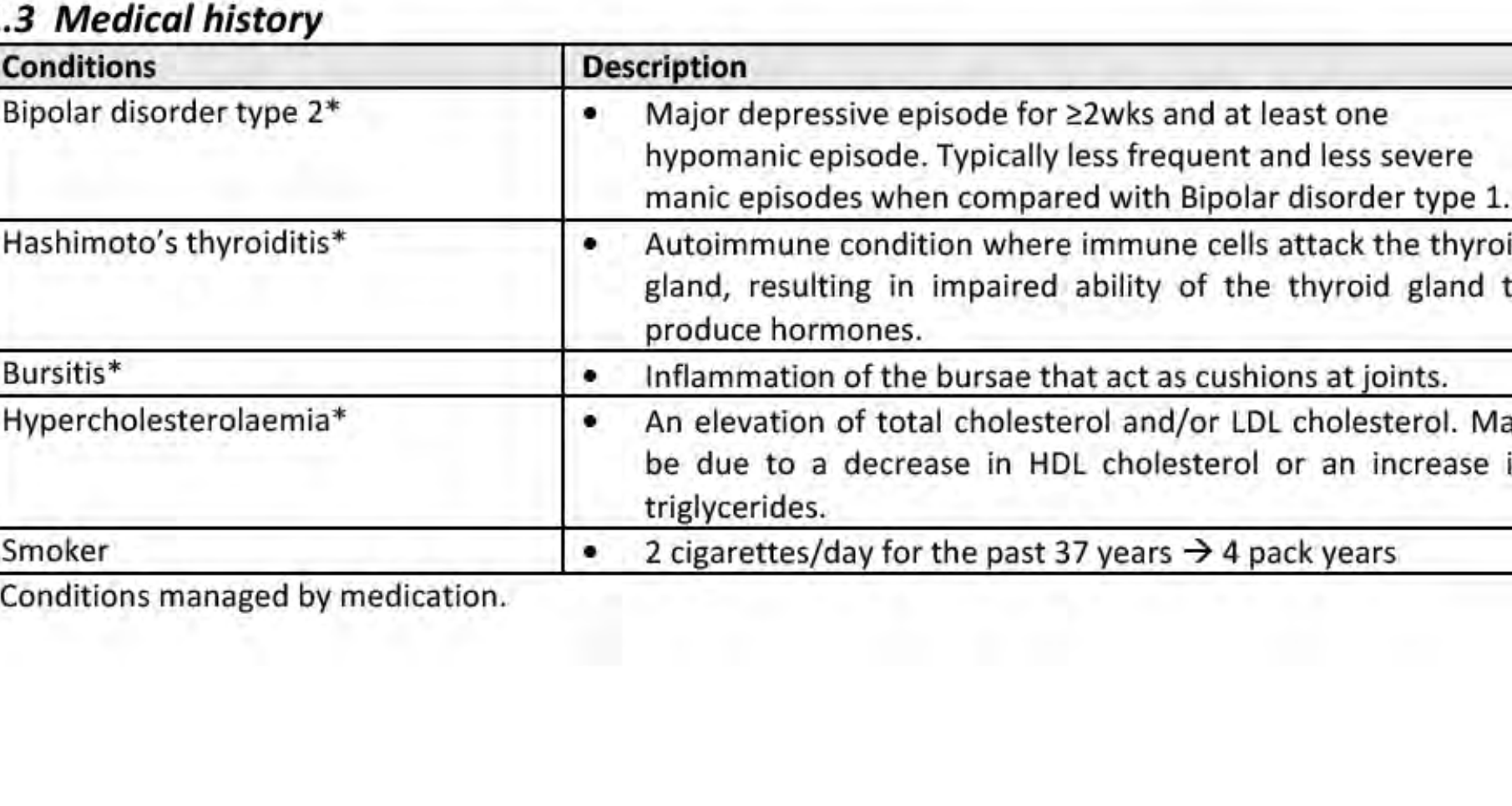
- Bipolar Disorder Type 2: Characterized by major depressive episodes (≥2 weeks) and at least one hypomanic episode.
- Hashimoto’s Thyroiditis: Autoimmune condition resulting in impaired thyroid hormone production.
- Bursitis: Inflammation of the joint bursae.
- Hypercholesterolaemia: Elevated total or LDL cholesterol.
- Smoking Status: 2 cigarettes/day for 37 years (4 pack years).
Medical History and Medications
Current Medications4
| Medication | Dosage | Use / Mechanism | Dental Implications |
|---|---|---|---|
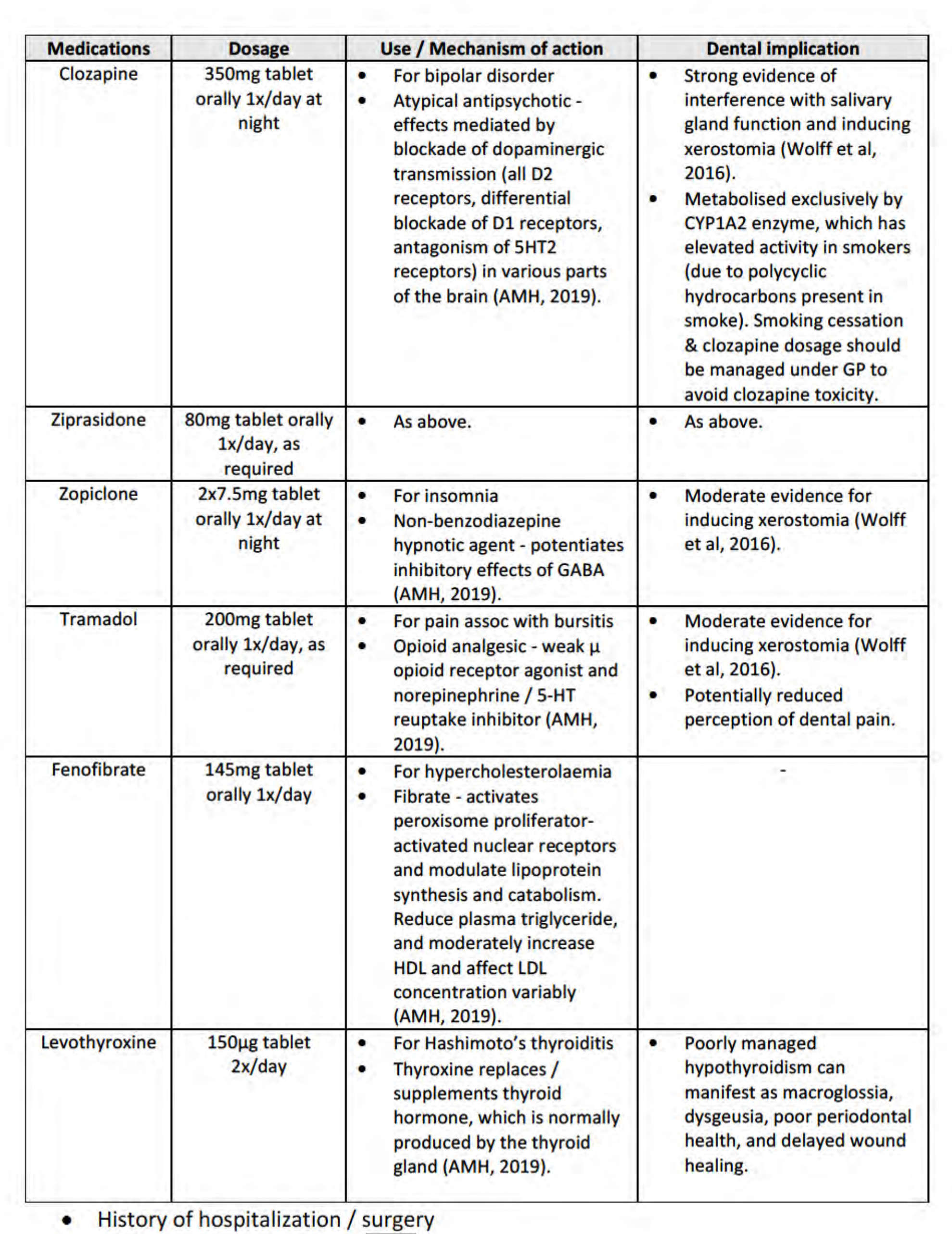
| Clozapine | 350mg daily (night) | Atypical antipsychotic for bipolar disorder. | Strong evidence of xerostomia. Metabolized by CYP1A2; smoking cessation requires GP management to avoid toxicity. |
| Ziprasidone | 80mg daily (PRN) | Atypical antipsychotic for bipolar disorder. | Risk of xerostomia. |
| Zopiclone | 15mg daily (night) | Non-benzodiazepine hypnotic for insomnia. | Moderate evidence for inducing xerostomia. |
| Tramadol | 200mg daily (PRN) | Opioid analgesic for bursitis pain. | Moderate evidence for xerostomia; potentially reduced perception of dental pain. |
| Fenofibrate | 145mg daily | Fibrate for hypercholesterolaemia. | None noted. |
| Levothyroxine | 150μg 2x/day | Thyroid hormone replacement. | Poorly managed hypothyroidism may cause macroglossia, dysgeusia, and delayed healing. |
Hospitalization and Allergies
- Surgery: Laser eye surgery.
- Allergies: No known allergies.
Clinical Examination5
Dental and Social History6
- Restorative History: Repeated temporary restorations for rampant caries over the past 5 years. Multiple teeth lost or fractured due to untreated caries and periodontal disease.
- Prosthetic History: Chrome Cobalt partial denture (CrCo P/-) made 4 years ago; patient is dissatisfied with retention following the fracture of an abutment tooth.
- Oral Hygiene: Brushes 2x/day with an electric toothbrush and charcoal (non-fluoridated) toothpaste. No interdental cleaning.
- Social Factors: Works in a bakery; lives alone but has regular family visits. Occasional alcohol consumption (1-2 times per month).
 |  |
Extra-Oral Examination Findings
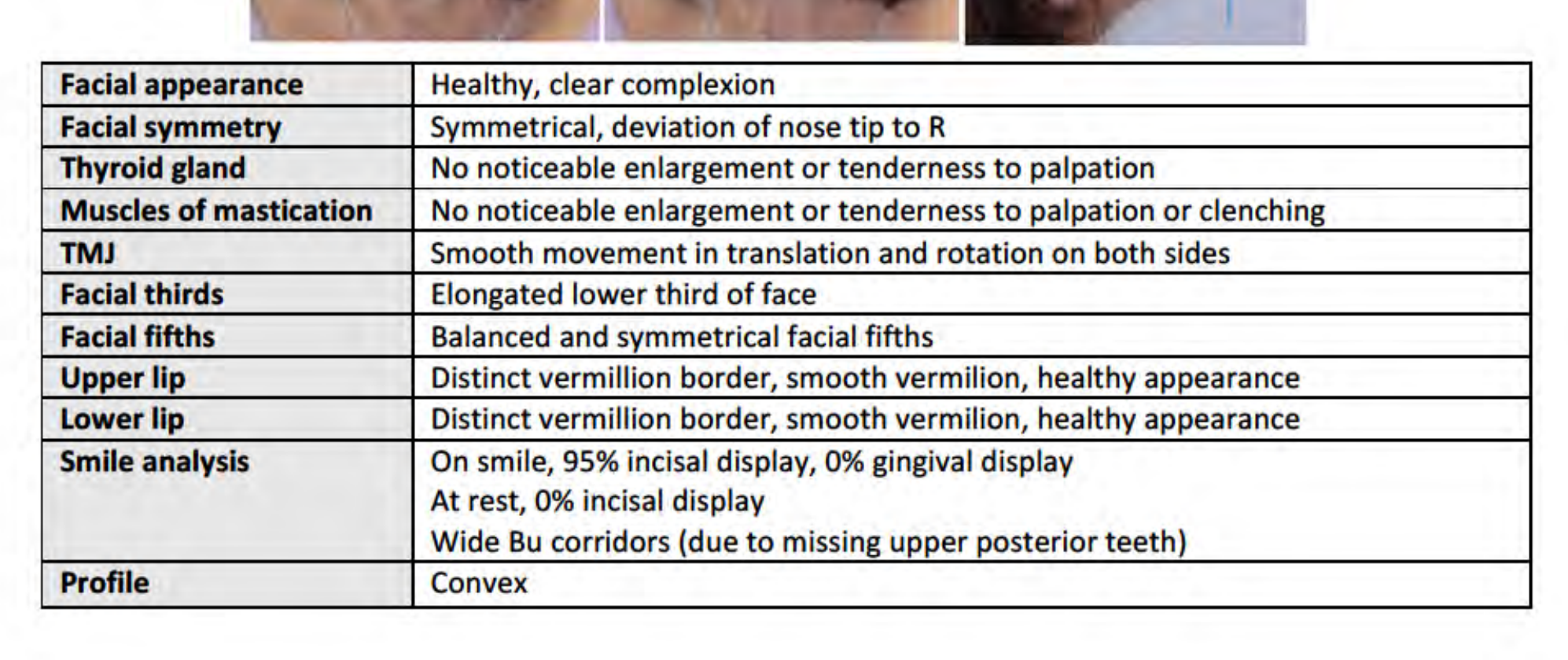
- Facial Features: Symmetrical face with a slight deviation of the nose tip to the right. Healthy complexion.
- Anatomy: No enlargement or tenderness of the thyroid gland or muscles of mastication. TMJ shows smooth movement in translation and rotation.
- Proportions: Elongated lower third of the face; balanced facial fifths. Convex profile.
- Lips: Distinct vermillion borders with a healthy appearance.
- Smile Analysis:
- 95% incisal display on smile; 0% gingival display.
- 0% incisal display at rest.
- Wide buccal corridors due to missing upper posterior teeth.
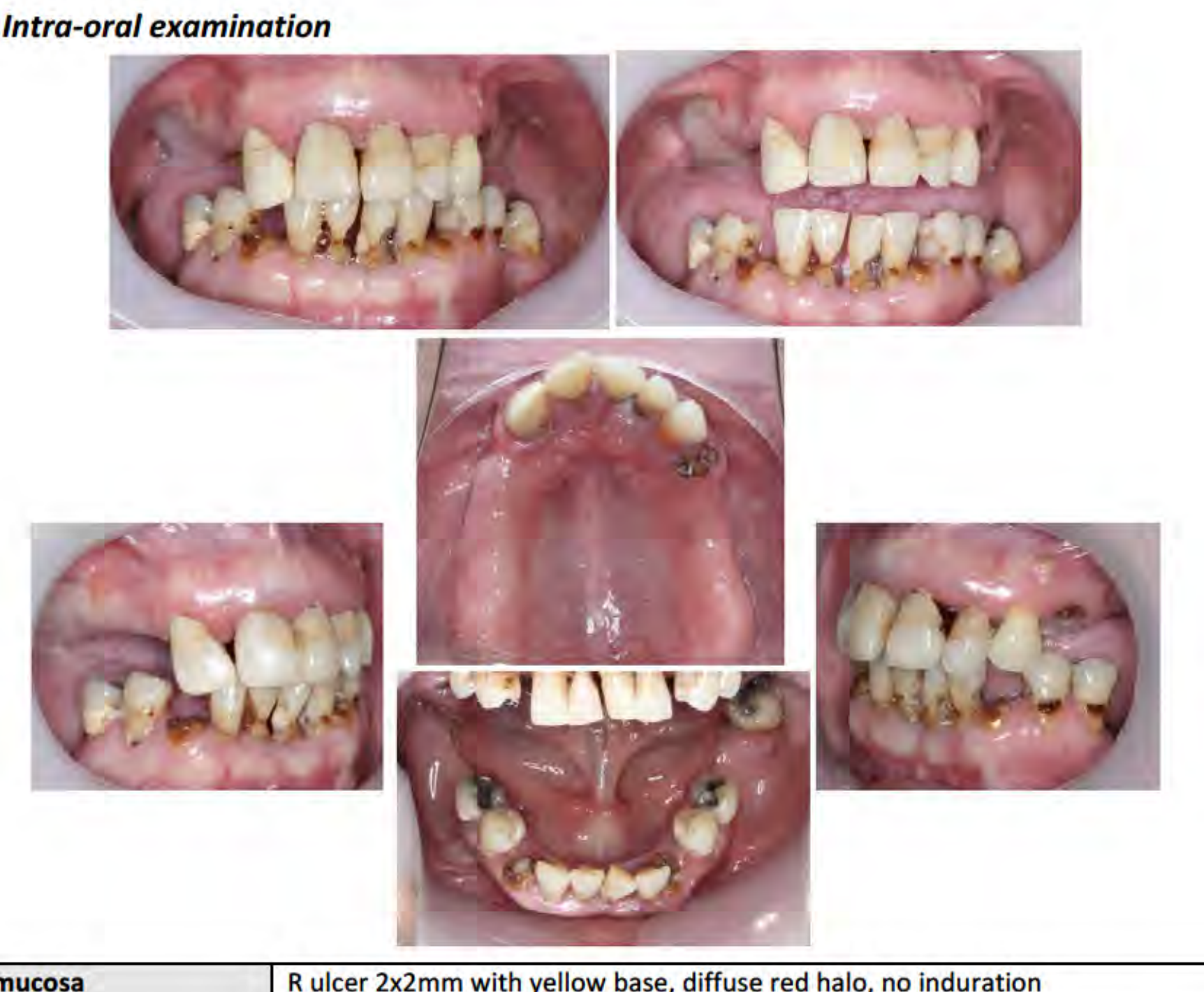
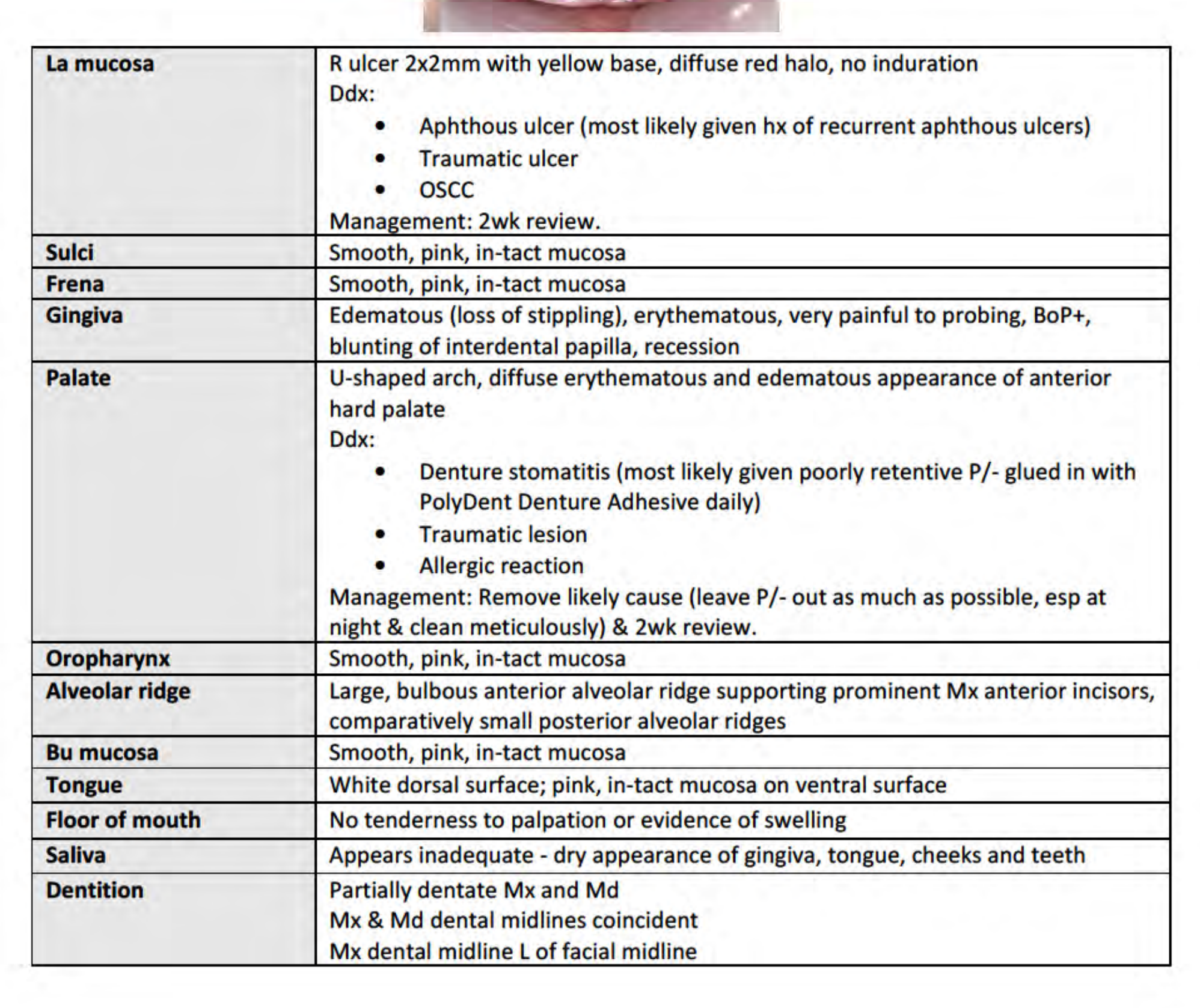
Intra-Oral Soft Tissue Examination7
- Labial Mucosa: 2x2mm ulcer with yellow base and red halo (Right side). Differential Diagnosis: Aphthous ulcer (most likely), Traumatic ulcer, or OSCC. Management: 2-week review.
- Palate: Diffuse erythematous and edematous appearance of the anterior hard palate. Differential Diagnosis: Denture stomatitis (most likely due to poor retention and adhesive use), Traumatic lesion, or Allergic reaction. Management: Leave denture out at night, clean meticulously, and 2-week review.
- Gingiva: Edematous, erythematous, and painful to probing. Positive Bleeding on Probing (BoP+), blunting of interdental papilla, and recession.
- Saliva: Inadequate volume; dry appearance of gingiva, tongue, cheeks, and teeth.
- Alveolar Ridge: Large, bulbous anterior maxillary ridge; comparatively small posterior ridges.
- Other: White dorsal surface of the tongue. Sulci, frena, oropharynx, buccal mucosa, and floor of mouth appear healthy and intact.
 |  |
Occlusion and Alignment
- Partially dentate Maxilla (Mx) and Mandible (Md).
- Dental midlines are coincident, but the Mx dental midline is left of the facial midline.
The page contains no unique text content beyond the header context.
Diagnostic Findings and Risk Assessment8
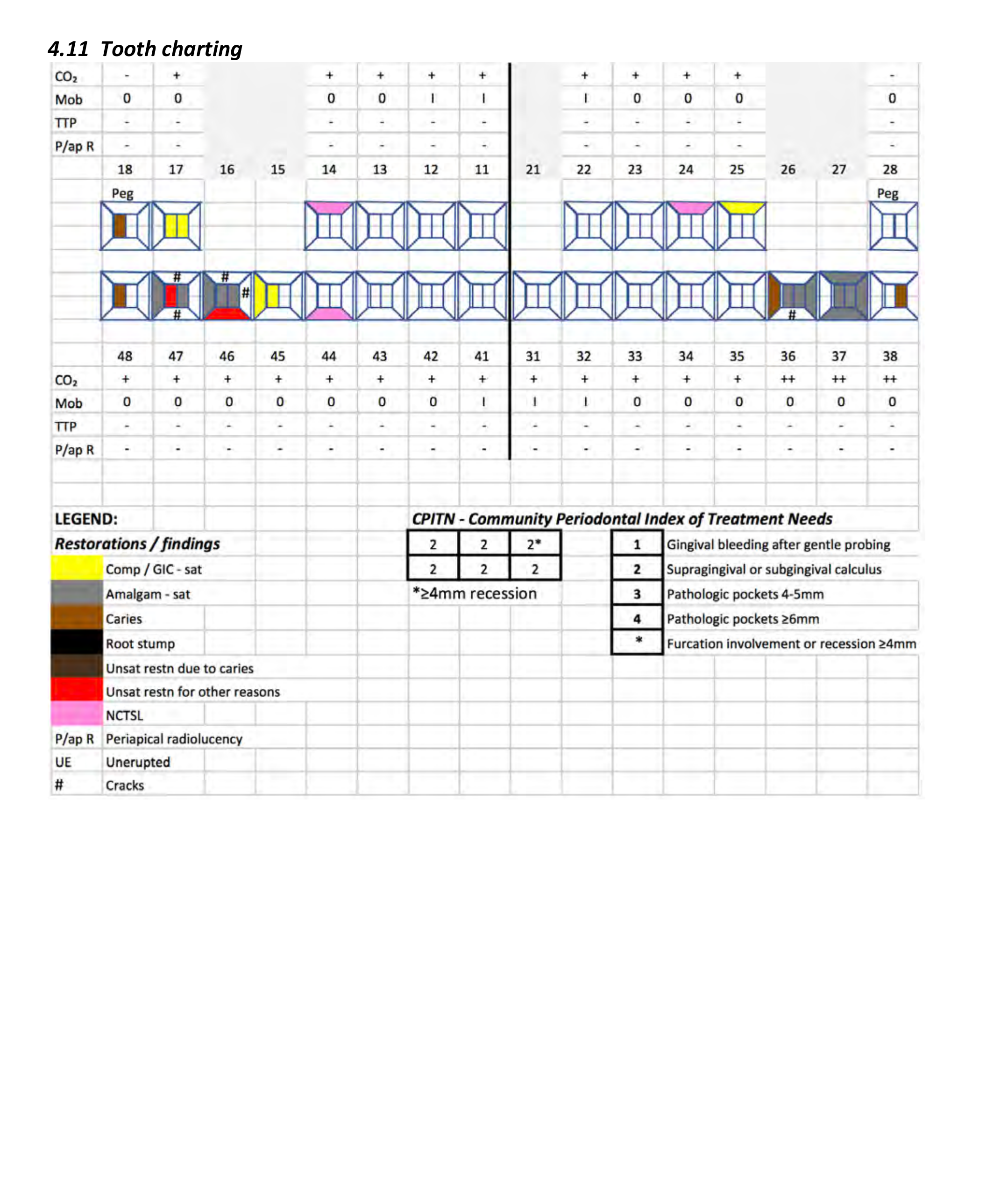
Tooth Charting and Vitality Testing9
Maxillary Findings:
- Vitality (CO2): Negative for 13, 21, 24. Positive for 22, 23.
- Mobility: Grade II (21, 22), Grade I (24).
- Radiographic Findings: Periapical radiolucencies (P/ap R) noted at 13 and 21.
Mandibular Findings:
- Vitality (CO2): Positive for 48, 47, 45, 44, 43, 31, 32, 36. Negative for 46, 42, 41.
- Mobility: Grade II (45, 44, 43, 42), Grade I (48, 47).
- Radiographic Findings: Periapical radiolucencies (P/ap R) noted at 41 and 31.
- Tenderness to Percussion (TTP): Positive at 36.
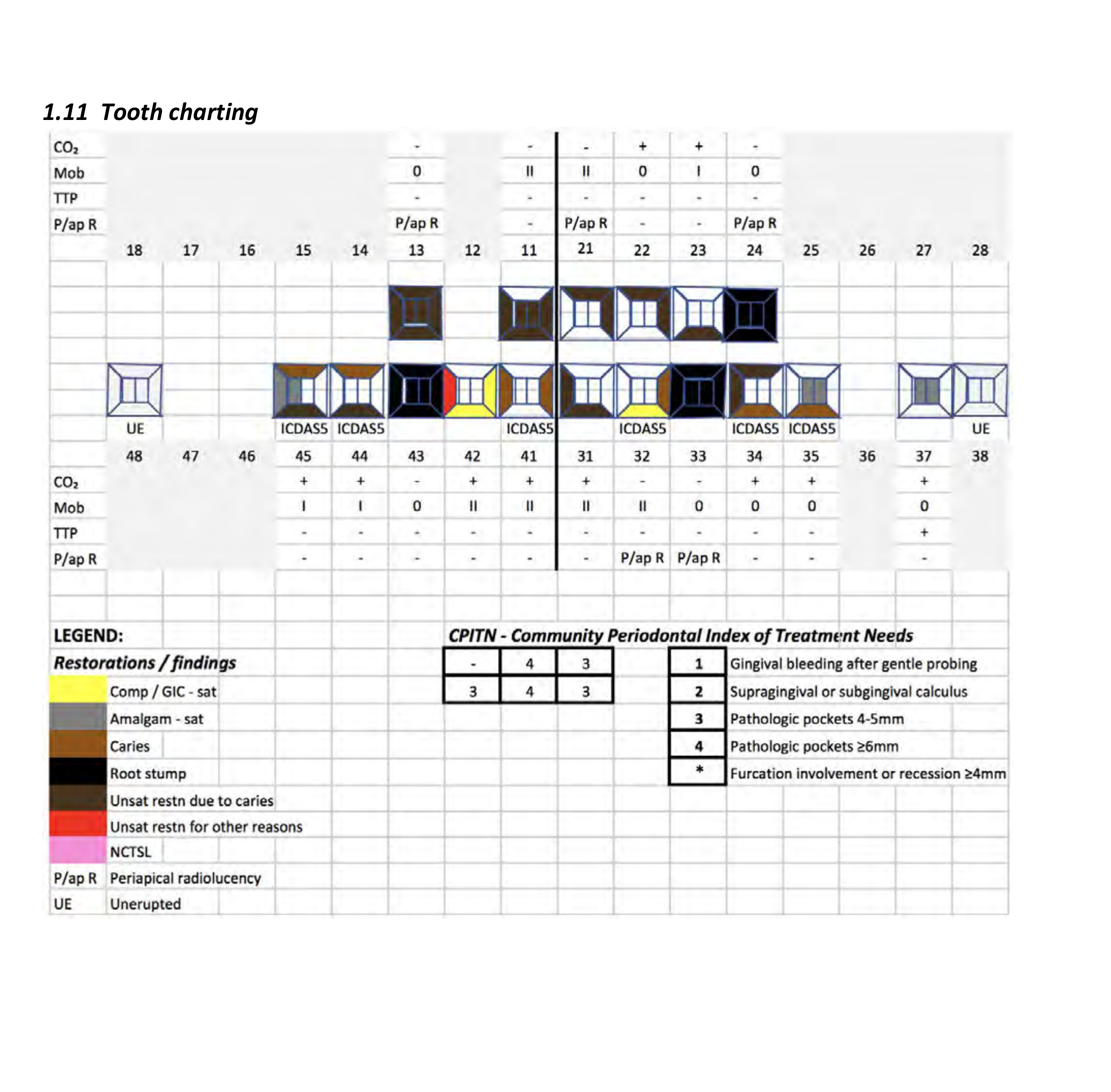 |  |
Charting Legend
- Caries: Dark Brown
- Root Stump: Black
- Unsatisfactory Restoration (Caries): Maroon
- Unsatisfactory Restoration (Other): Red
- Non-Carious Tooth Surface Loss (NCTSL): Pink
- Sound Restorations: Yellow (Comp/GIC), Gray (Amalgam)
Community Periodontal Index of Treatment Needs (CPITN)
- Gingival bleeding after gentle probing
- Supragingival or subgingival calculus
- Pathologic pockets 4-5mm
- Pathologic pockets ≥6mm
- Furcation involvement or recession ≥4mm
The page contains no unique text content beyond the header context.
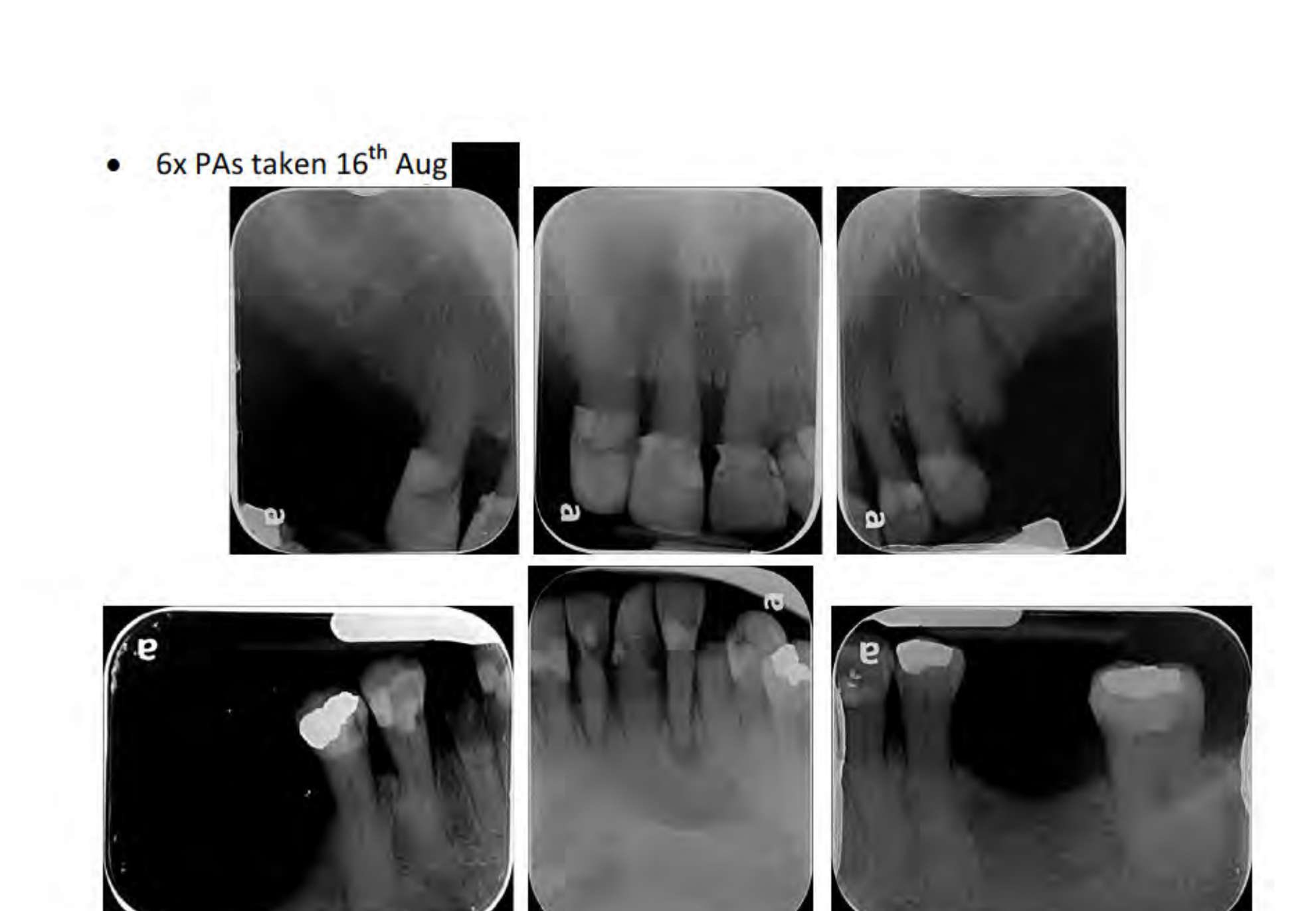
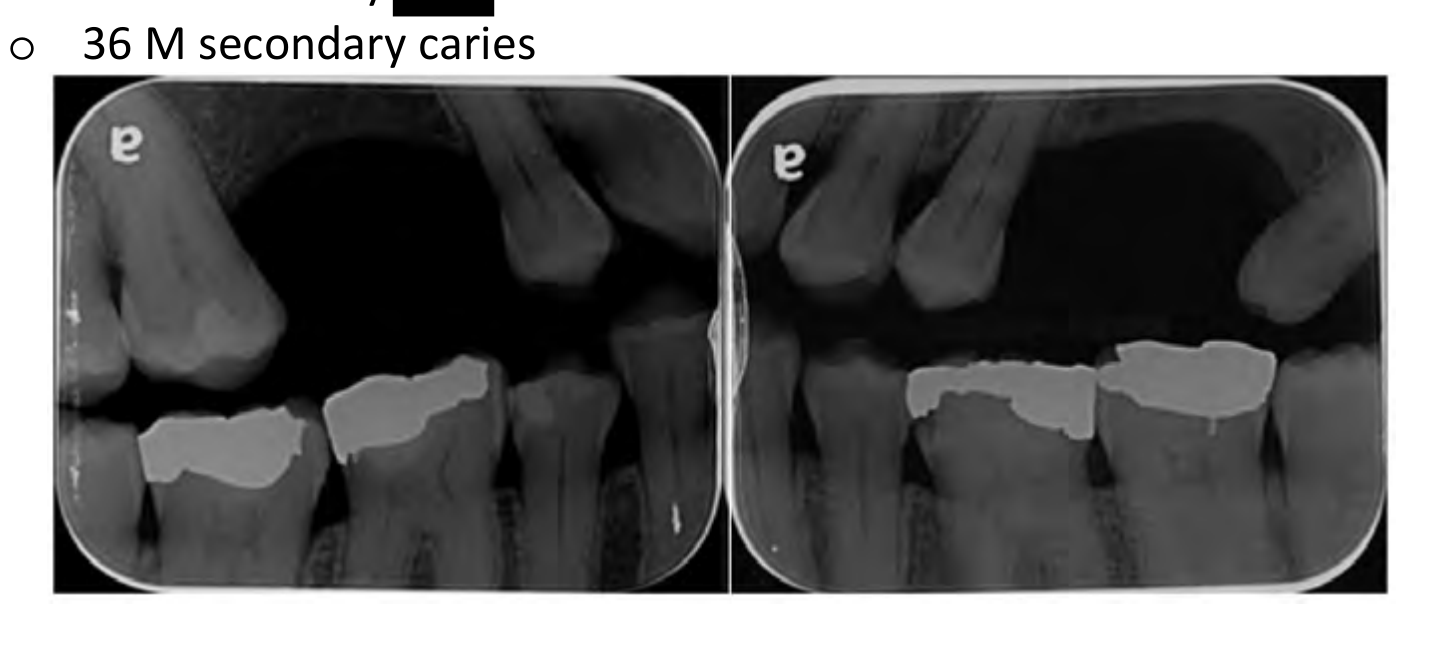
Radiographic Interpretation10
- Comparison (2016 vs 2018): Significant increase in caries experience.
- Caries: Frank cavitation now affects almost every tooth.
- Endodontic Status: Periapical lesions involving teeth 13, 21, 24, 33, and 32.
- Periodontal Status: Moderate to severe bone loss. Bone levels have remained relatively constant between recent imaging intervals.
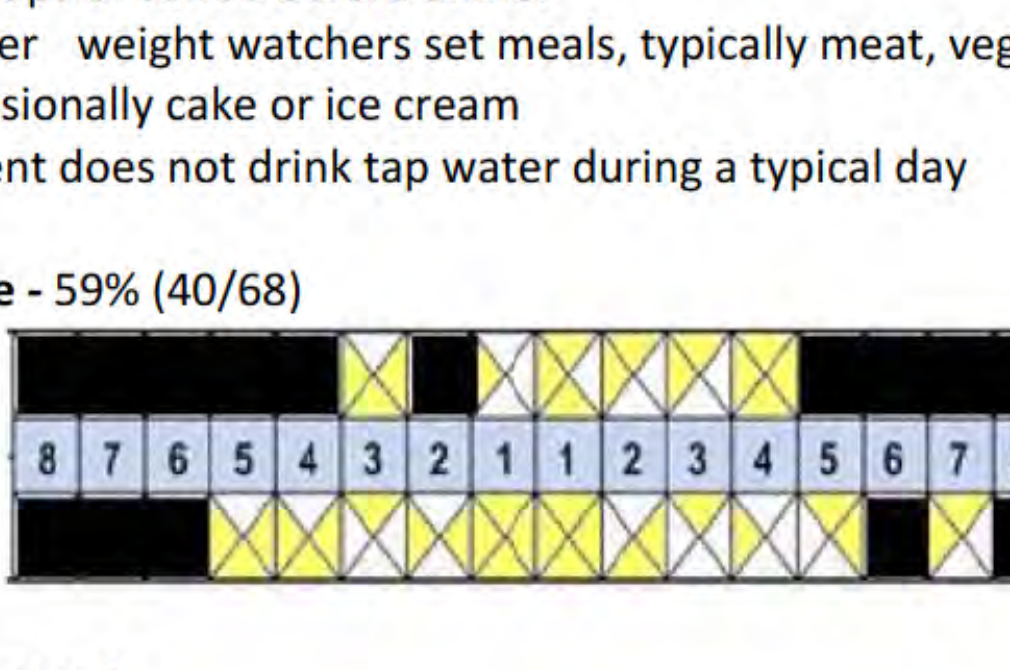
Diet and Plaque Assessment11
- Dietary Habits: High frequency of sugar and acid. Includes 3-5 cups of coffee with sugar, sweet lollies, cake/pastries at work, and Pepsi Max sipped throughout the afternoon. No tap water consumption.
- Plaque Score: 59% (40/68 sites).
 |  |
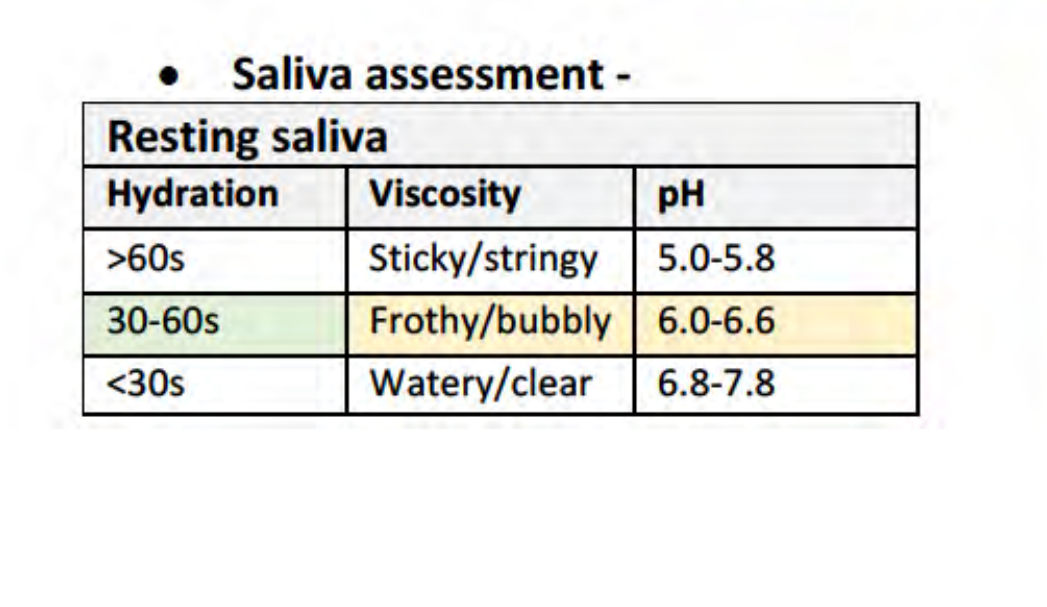 |  |
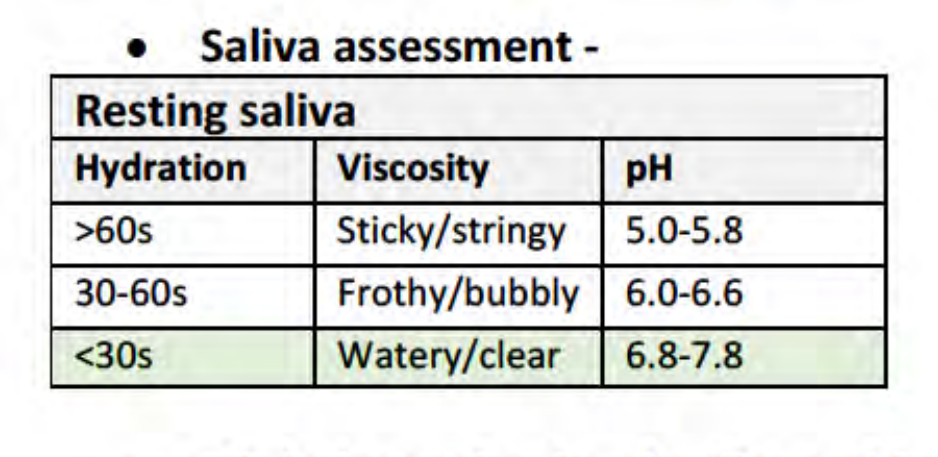
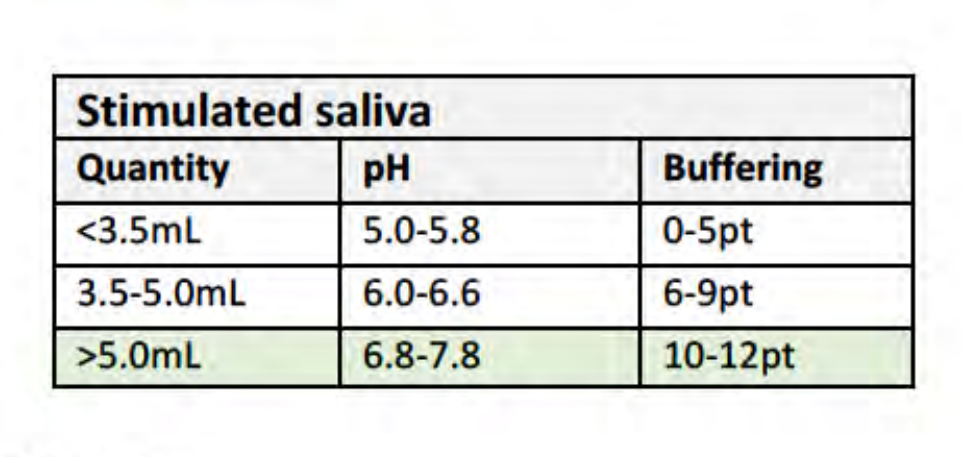
Saliva Assessment
Resting Saliva:
- Hydration: >60s (Poor)
- Viscosity: Sticky/stringy
- pH: 6.0-6.6
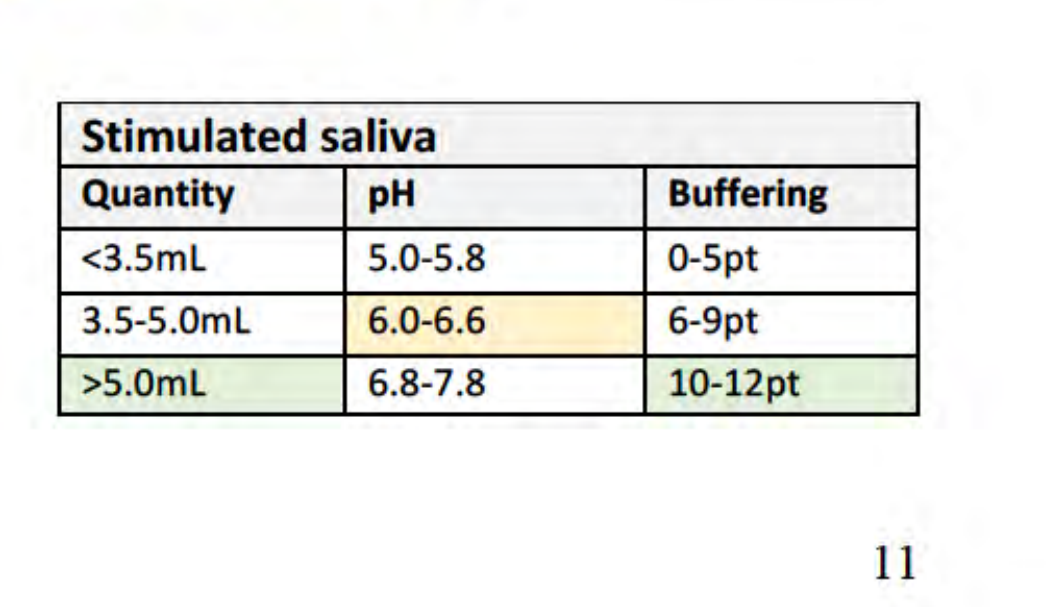
Stimulated Saliva:
- Quantity: 3.5-5.0mL (Low-Normal)
- pH: 6.0-6.6
- Buffering: 10-12pt (High)
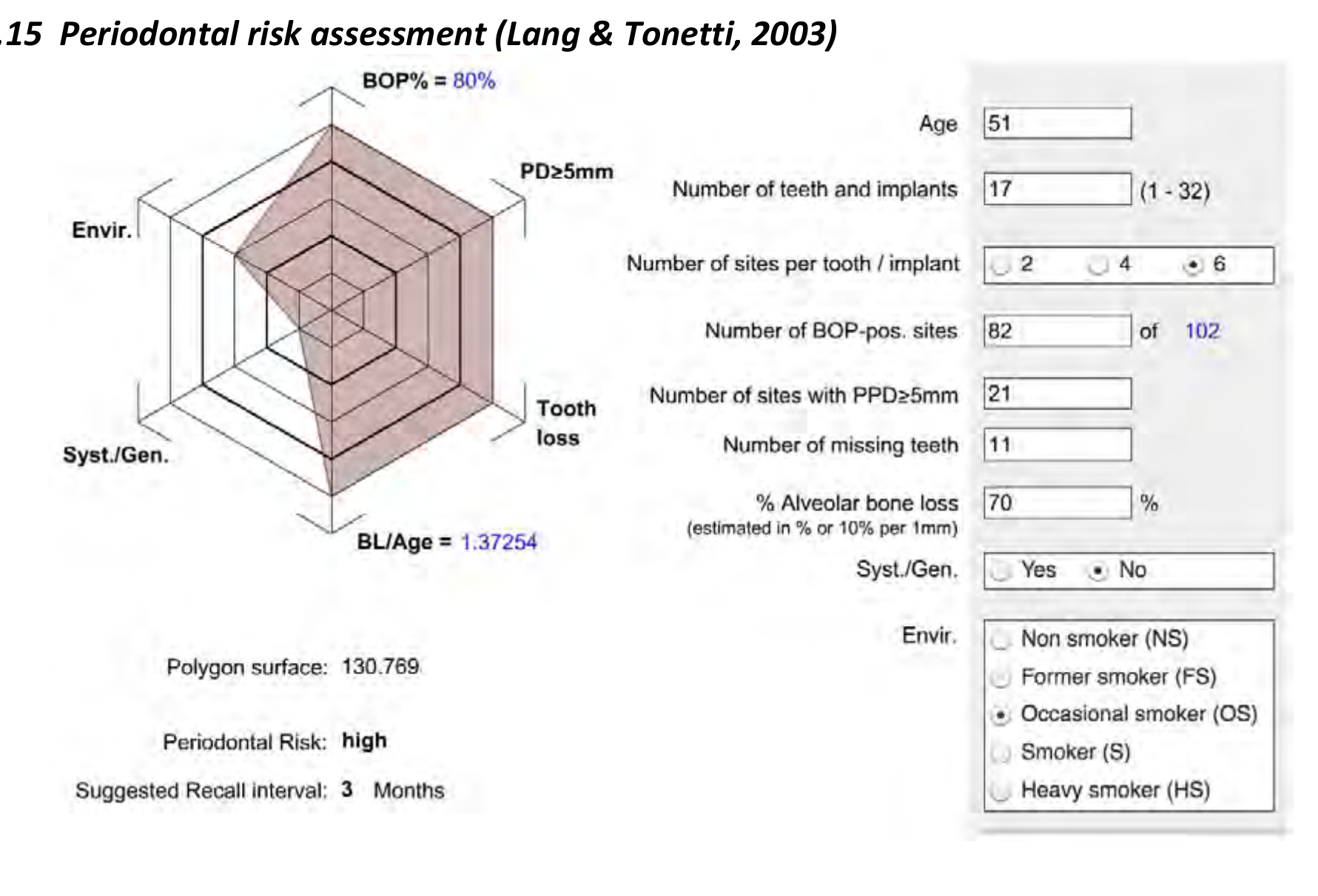
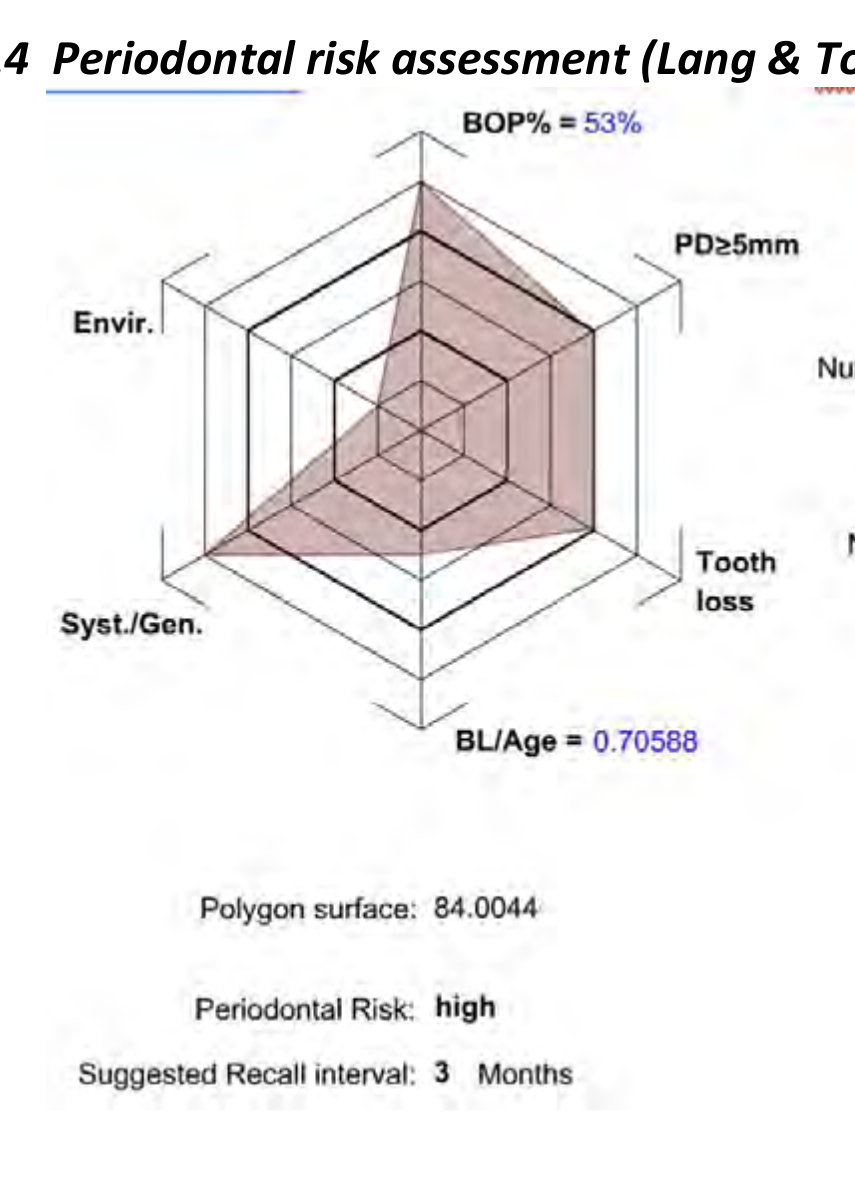
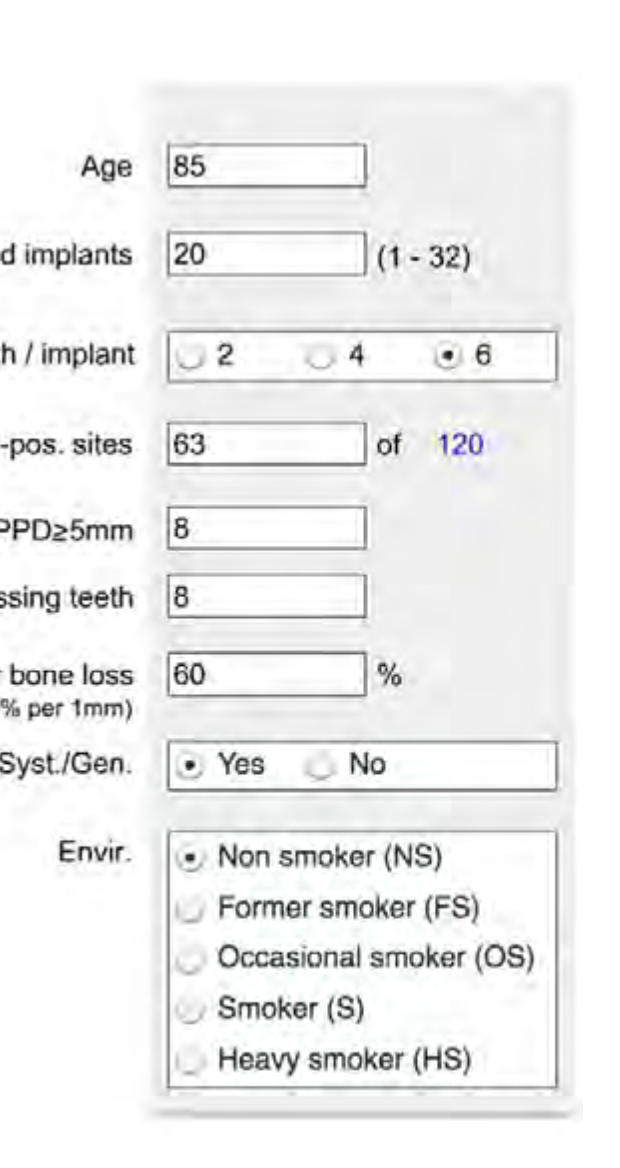
Risk Summary12
-
Caries Risk: HIGH
- Multiple untreated frank cavities.
- Deep carious lesions extending into pulp chambers.
- Multiple periapical radiolucencies.
-
Periodontal Risk: HIGH
- Bleeding on Probing (BOP): 80% (82 of 102 sites).
- Probing Depths: 21 sites with PPD ≥5mm.
- Bone Loss: Estimated at 70% (BL/Age ratio = 1.37).
- Missing Teeth: 11.
- Environmental Factors: Occasional smoker.
- Recall Interval: 3 months suggested.
Problem List and Prognosis
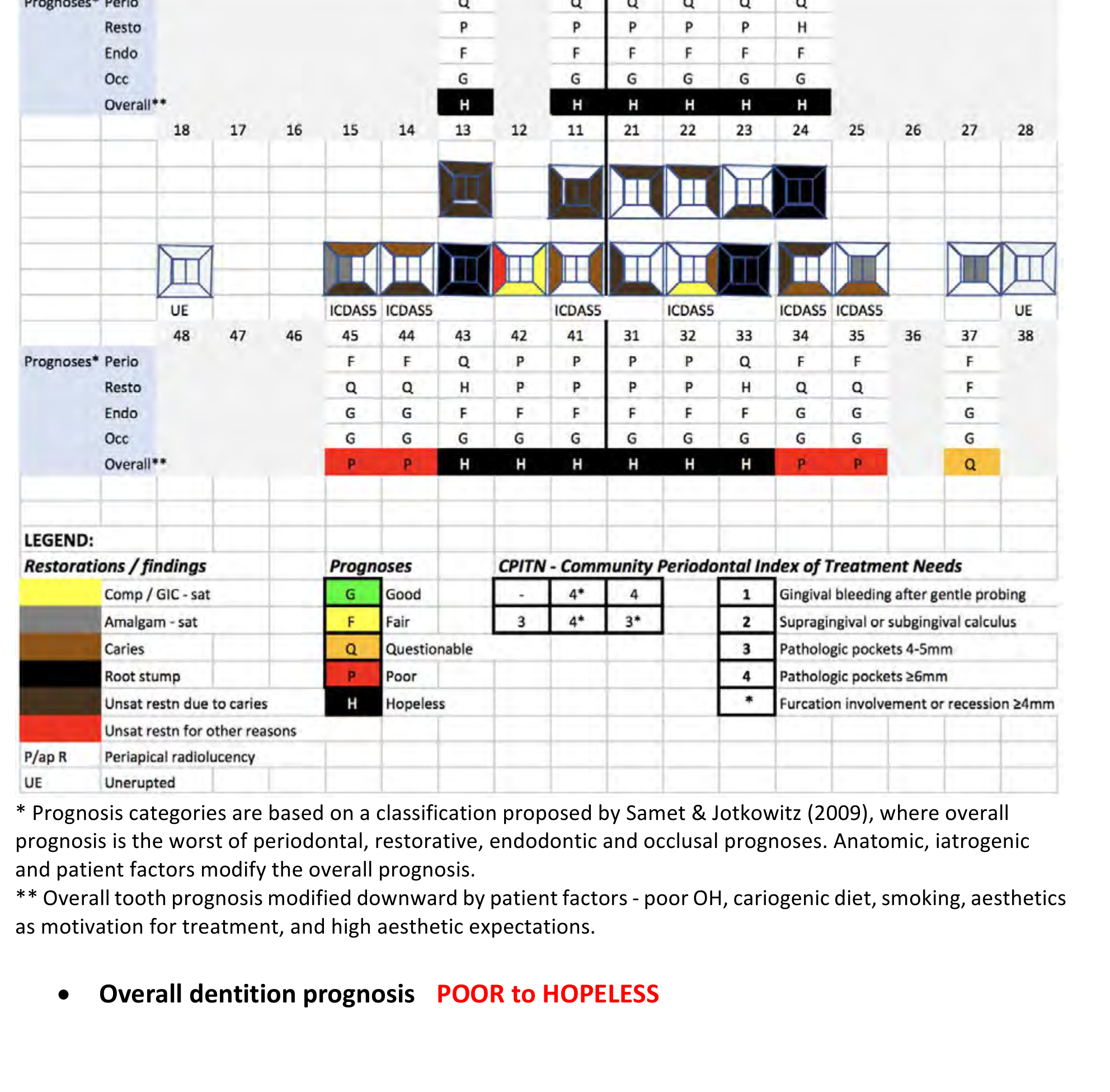
Individual and Overall Prognosis13
- Prognosis Determination: Based on Samet & Jotkowitz (2009), integrating periodontal, restorative, endodontic, and occlusal factors.
- Modifying Factors: Prognosis is adjusted downward due to poor oral hygiene, cariogenic diet, smoking, and high aesthetic expectations.
- Overall Dentition Prognosis: POOR to HOPELESS.
Problem List14
Aesthetics and Prosthetics:
- Poor smile aesthetics and unsatisfactory CrCo P/-.
- Multiple root stumps and carious discoloration.
- Fractured abutment tooth (24) causing loss of denture retention.
Host and Behavioral Factors:
- Systemic: Bipolar disorder and hypothyroidism (medicated).
- Oral Environment: Dry mouth (xerostomia).
- Habits: Smoker; frequent high intake of sugar/acidic food and drinks.
- Compliance: Questionable oral hygiene and attendance record.
Pathology:
- Carious root stumps: 24, 33, 43.
- Frank cavitation: 11, 13, 21, 22, 23, 31, 32, 34, 35, 41, 44, 45.
- Periodontal: Stage 4 Grade C Periodontitis (modified by smoking).
- Endodontic: Infected root canal systems and chronic apical periodontitis (24, 32, 33).
- Soft Tissue: Recurrent aphthous ulcers and denture stomatitis.
Morphology:
- Skeletal/Dental: Class II Division 1.
- Impactions: Vertically impacted 38, 48.
- Anatomy: Hypercementosis (multiple teeth); large bulbous maxillary anterior ridge.
- Arch Status: Maxillary Kennedy Class I; Mandibular Kennedy Class II Modification 1; loss of posterior support.
Diagnoses15
- Poor smile aesthetics and unsatisfactory CrCo P/-.
- Unrestorable teeth / Root stumps.
- Dental Caries.
- Periodontal Disease.
- Endodontic Involvement.
- Maxillary Kennedy Class I.
- Mandibular Kennedy Class II Modification 1.
Treatment Options and Management Plan1617
Rejected Treatment Options18
Option 4: Limited Restoration and Denture Modification
- Description: Stabilize remaining teeth and add tooth 24 to existing CrCo P/-.
- Advantages: Fastest address of complaint.
- Disadvantages: Short-term outcome; highly compromised result.
Option 5: Full Clearance and Complete Dentures (F/F)
- Description: Immediate or conventional full dentures.
- Advantages: Significant aesthetic improvement; eliminates all dental disease.
- Disadvantages: Difficult transition to edentulous state; poor retention of mandibular denture.
Option 6: No Treatment
- Advantages: No patient action required.
- Disadvantages: Unpredictable progression of pain and infection; worsening aesthetics; eventual tooth loss.
Selected Treatment Plan19
Option 1: Immediate Acrylic Maxillary Full / Mandibular Partial Denture (F/P)
Rationale for Selection:
- Significant aesthetic improvement potential.
- Relatively low cost.
- Reduction of disease burden via extraction of hopeless teeth.
- Simplified treatment course.
- Patient refusal to be without teeth during healing.
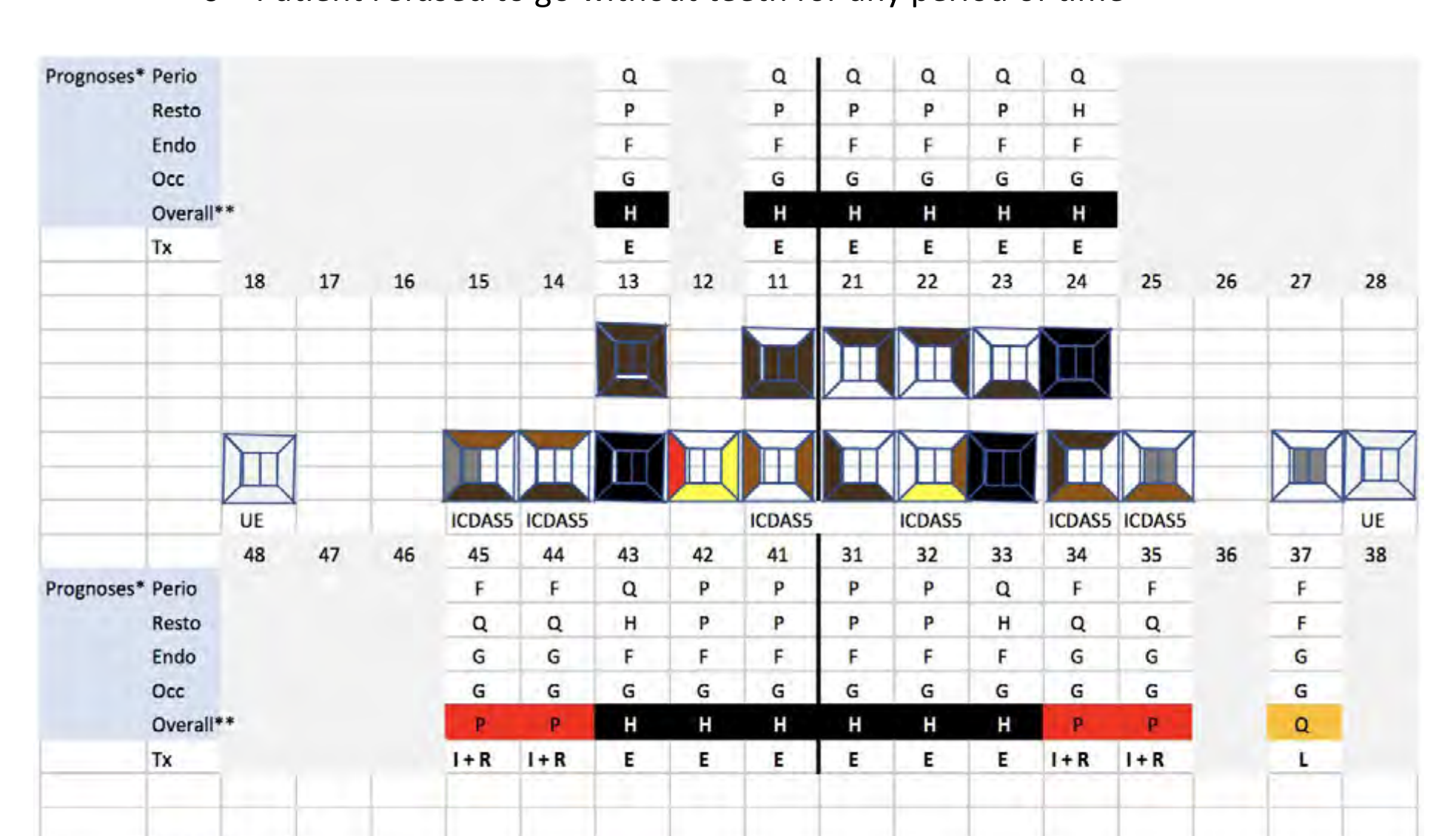 | 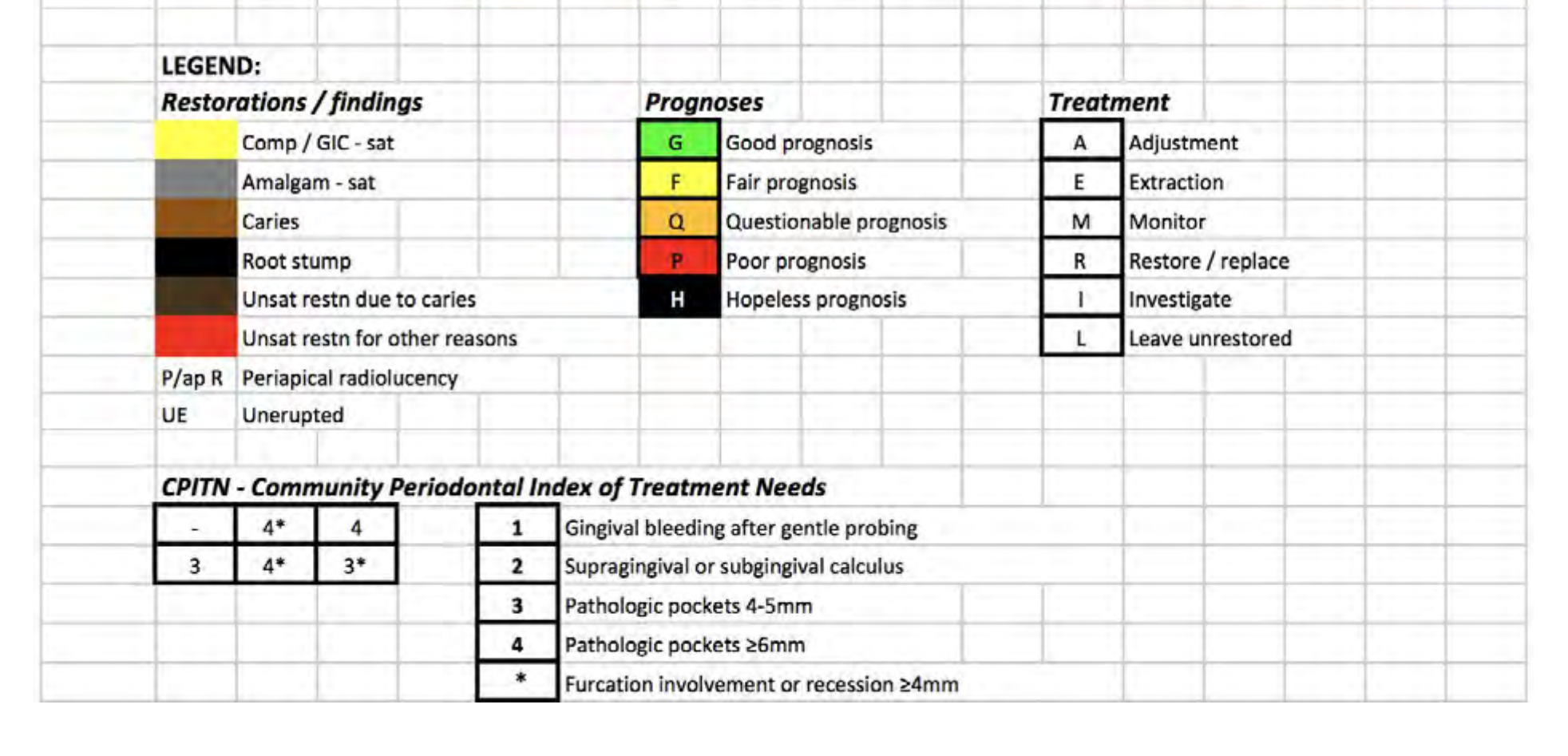 |
Clinical Coding Legend
- Prognosis: Good (P), Questionable (Q), Hopeless (H), Fair (F), Extraction (E).
- Treatment: Adjustment (A), Restore/Replace (R), Leave Unrestored (L), Monitor (M).
- CPITN: 1 (Bleeding), 2 (Calculus), 3 (4-5mm pockets), 4 (≥6mm pockets).
The page contains no unique text content beyond the header context.
Clinical Procedures and Reviews
Prosthetic Fabrication Procedures20
- Registration: Base and rims fabricated for facebow and bite registration, maintaining existing Occlusal Vertical Dimension (OVD).
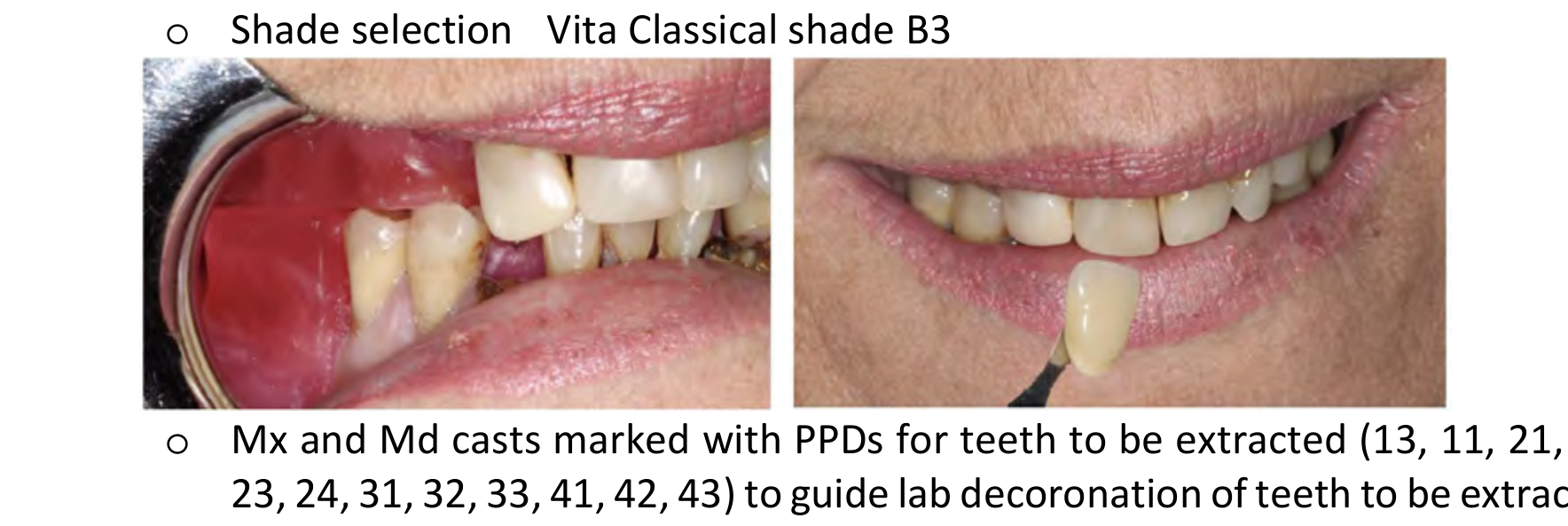
- Shade: Vita Classical shade B3.
- Lab Instructions:
- Maxillary and Mandibular casts marked with PPDs to guide decoronation.
- Reduce maxillary incisal display by 1-2mm.
- Set maxillary teeth following palatal surfaces of natural teeth to reduce overjet and Class II appearance.
- Set mandibular teeth following the line of occlusion.
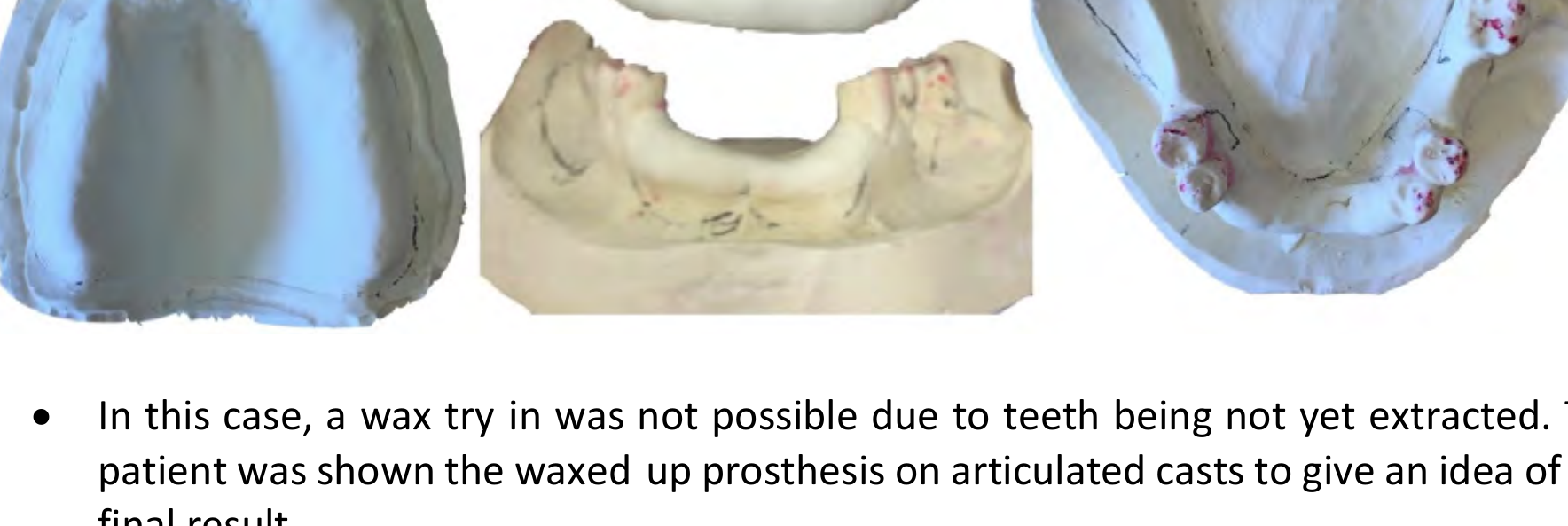
- Try-in: Wax try-in was not possible due to remaining teeth; patient viewed the wax-up on articulated casts.
 |  |
Pre-Operative Counseling21
- Surgical Risks: Patient informed of risks including bleeding, bruising, swelling, and infection.
- Immediate Denture Expectations:
- Significant adjustment period for speech and mastication.
- Post-extraction soreness and pain expected during initial healing.
- Looseness expected within 4-6 weeks due to bone resorption.
- Requirement for temporary chairside relines every 3-4 weeks.
- Definitive reline planned for 6-12 months post-extraction.
- Possibility of unsatisfactory fit/aesthetics requiring a complete remake.

Definitive Phase22
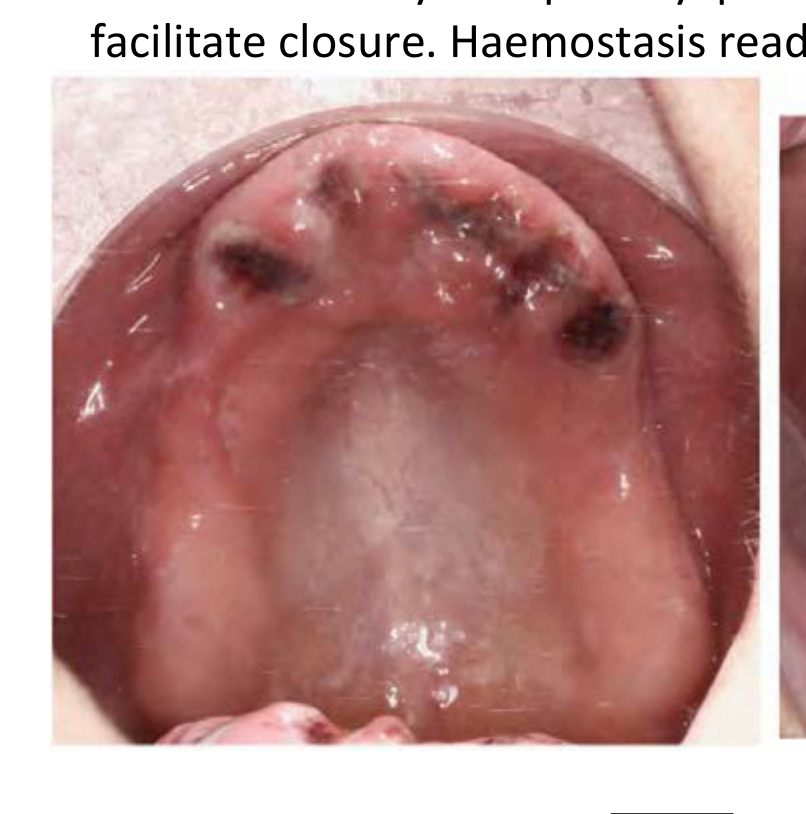
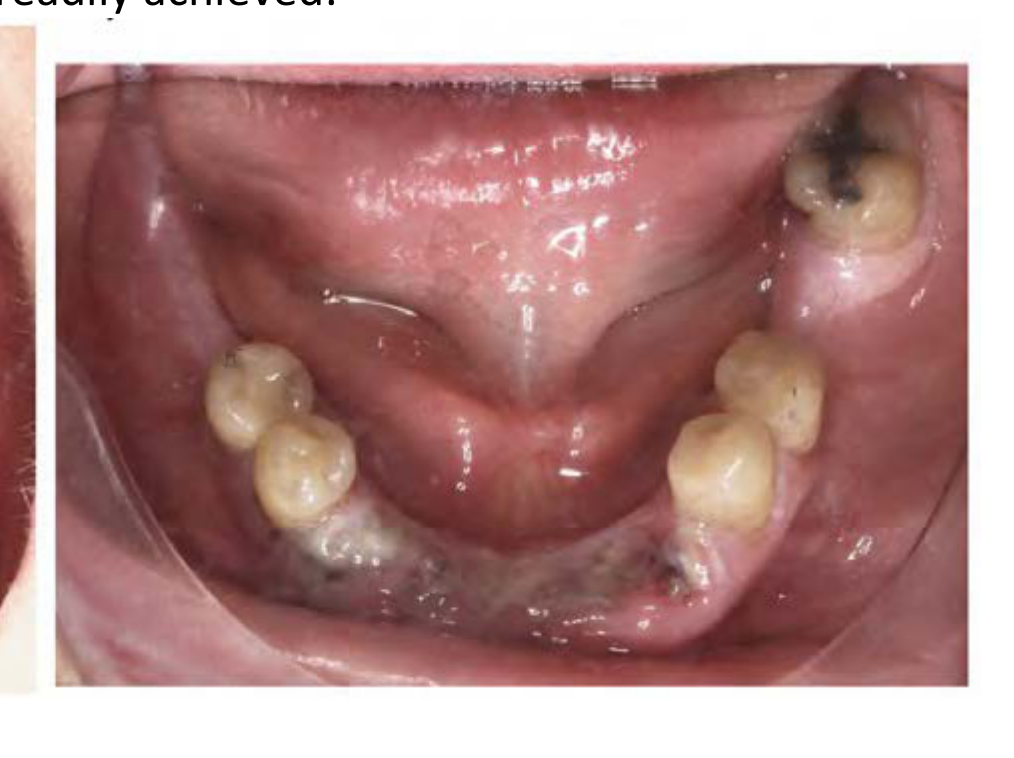
- Execution of extractions.
- Insertion of the immediate acrylic F/P denture.
- Provision of post-operative instructions for both the extractions and the new prosthesis.
 |  |
24-Hour Review23
- Patient Status: Sore and swollen but extremely pleased with the aesthetic result.
- Clinical Actions:
- Occlusion checked and refined for balanced contacts.
- Reinforced post-operative instructions and home care routine.
- Advised that a future remake may be necessary if significant changes occur.
 |  |
 |
Follow-up Reviews24
1-Week Review:
- Patient reported high satisfaction and positive feedback from others.
- Soreness and swelling mostly resolved.
- Minor adjustments made to relieve sore spots.
- Reiteration of expected looseness due to bone resorption.
First 3-4 Week Review:
- Patient reported slight looseness of the F/P.
- Minor adjustments to sharp edges.
- Action: Viscogel soft liner added to the intaglio surface to improve retention and stability.
 |  |
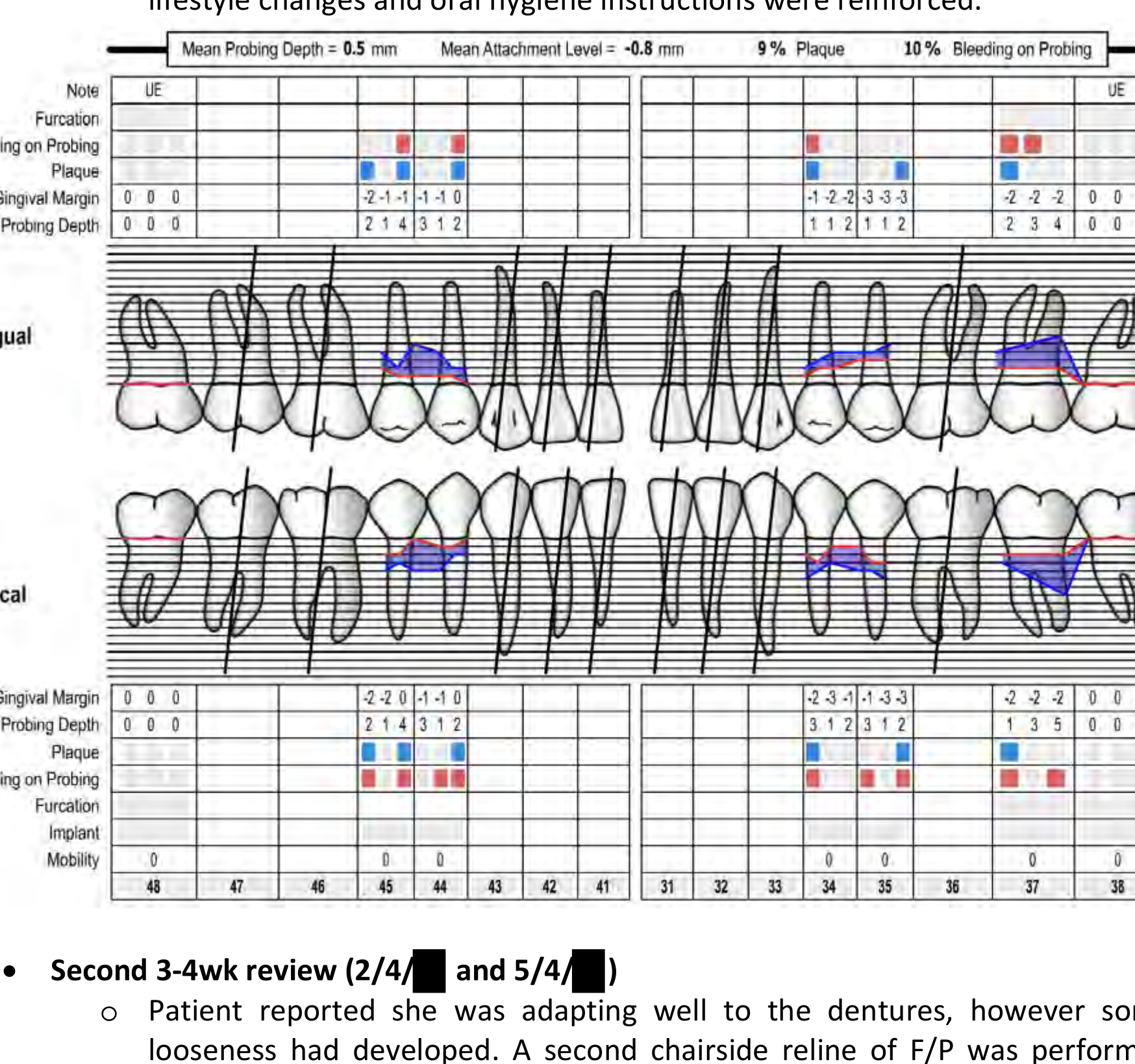
Periodontal and Maintenance Reviews25
Periodontal Review:
- Significant improvement in oral hygiene (Plaque 9%, BoP 10%).
- Mean Probing Depth: 0.5mm; Mean Attachment Level: -0.8mm.
- Subgingival Debridement (SRD) performed on remaining teeth.
Subsequent Denture Reviews:
- Second 3-4 Week Review: Further looseness addressed with a second Viscogel soft liner application.
- Third 3-4 Week Review: Patient reported minimal looseness and high satisfaction with comfort and appearance.
- Final Chairside Reline: Performed with Viscogel.
- Long-term Plan: Definitive reline scheduled for November, as soft tissue stability has been achieved.
Initial Clinical Assessment26
The patient presented with a chief complaint regarding the poor aesthetics and lack of stability of her existing maxillary partial denture. Clinical examination revealed:
- Multiple missing maxillary teeth.
- Advanced periodontal bone loss on remaining abutments.
- Generalized mobility of the remaining maxillary dentition.
- Compromised occlusal vertical dimension.
Treatment Planning and Sequence
Following a comprehensive evaluation, a treatment plan was developed to restore function and aesthetics using a removable prosthetic approach. The sequence included:
-
Phase I: Stabilization
- Periodontal therapy and extraction of non-retainable teeth.
- Fabrication of a transitional maxillary complete denture to evaluate aesthetics and vertical dimension.
-
Phase II: Definitive Restoration
- Final impressions using a border-molded custom tray technique.
- Maxillomandibular relationship records at the established vertical dimension.
- Trial evaluation of the wax tooth arrangement to confirm phonetics and lip support.
Final Delivery and Follow-up
The definitive maxillary removable prosthesis was processed and delivered. Post-insertion reviews focused on:
- Occlusal Harmony: Verification of bilateral simultaneous contacts in centric relation.
- Tissue Adaptation: Assessment of the intaglio surface for pressure points.
- Patient Satisfaction: The patient reported significant improvement in confidence, speech, and masticatory efficiency.
Case 2: Functional Removable Restorative Case
Presenting Complaint27
- “My upper denture is loose. It comes out when I chew.”
- “I’ve never really liked the look of the big tooth in the middle of my bottom denture.”
 |  |
 |
History of Presenting Complaint
- Patient has noticed over the past 2–3 months that his upper denture dislodges when he eats hard foods.
- Otherwise, the upper denture stays in place (e.g., when speaking, laughing, or sneezing).
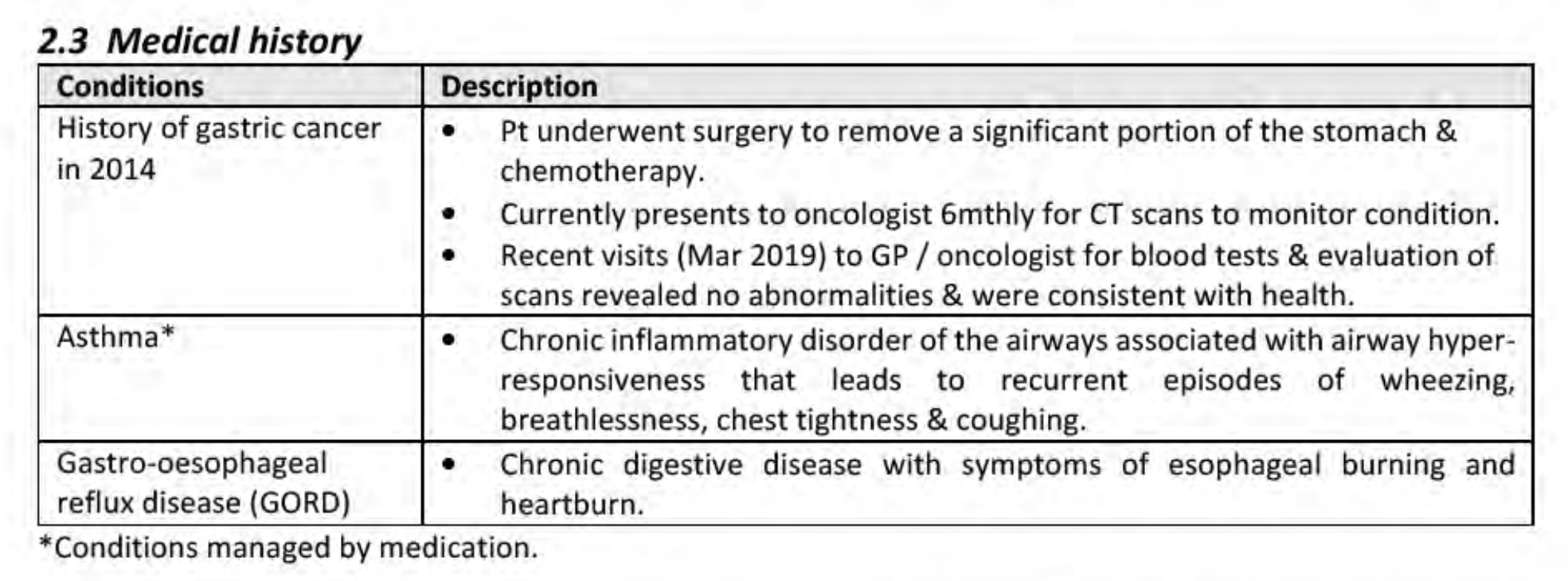
Medical History
| Conditions | Description |
|---|---|
| History of gastric cancer (2014) | - Pt underwent surgery to remove a significant portion of the stomach & chemotherapy. - Currently presents to oncologist 6-monthly for CT scans to monitor condition. - Recent visits (Mar 2019) to GP / oncologist for blood tests & evaluation of scans revealed no abnormalities & were consistent with health. |
| Asthma* | - Chronic inflammatory disorder of the airways associated with airway hypersensitivity that leads to recurrent episodes of wheezing, breathlessness, chest tightness & coughing. |
| Gastro-oesophageal reflux disease (GORD) | - Chronic digestive disease with symptoms of esophageal burning and heartburn. |
Clinical Presentation and History28
*Conditions managed by medication.
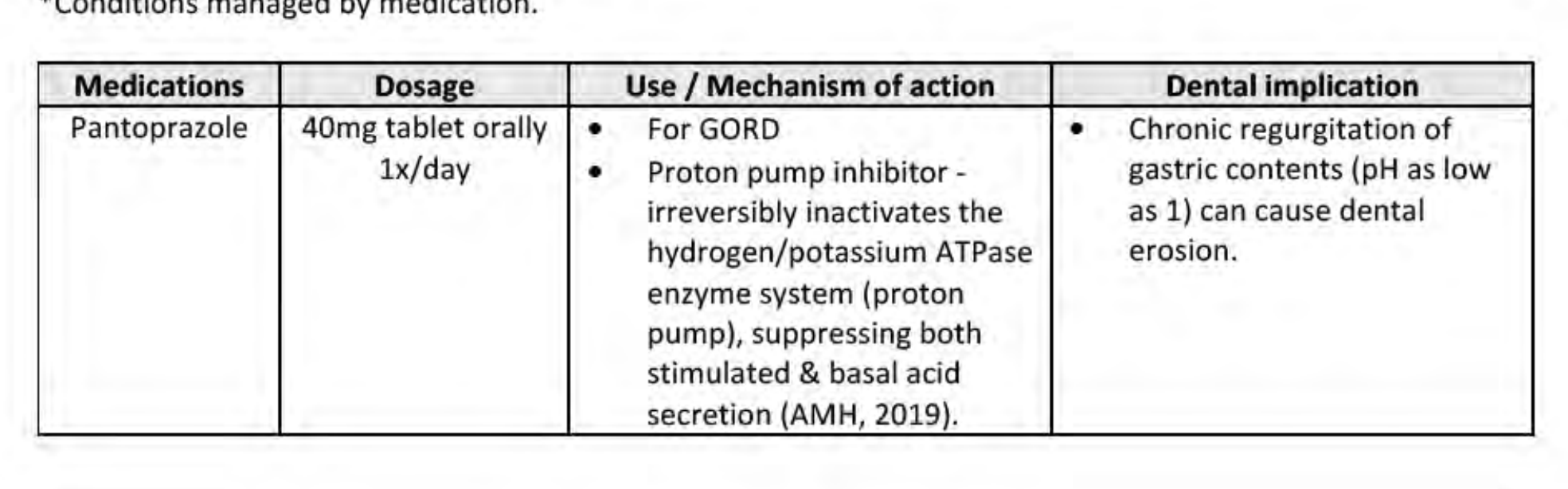
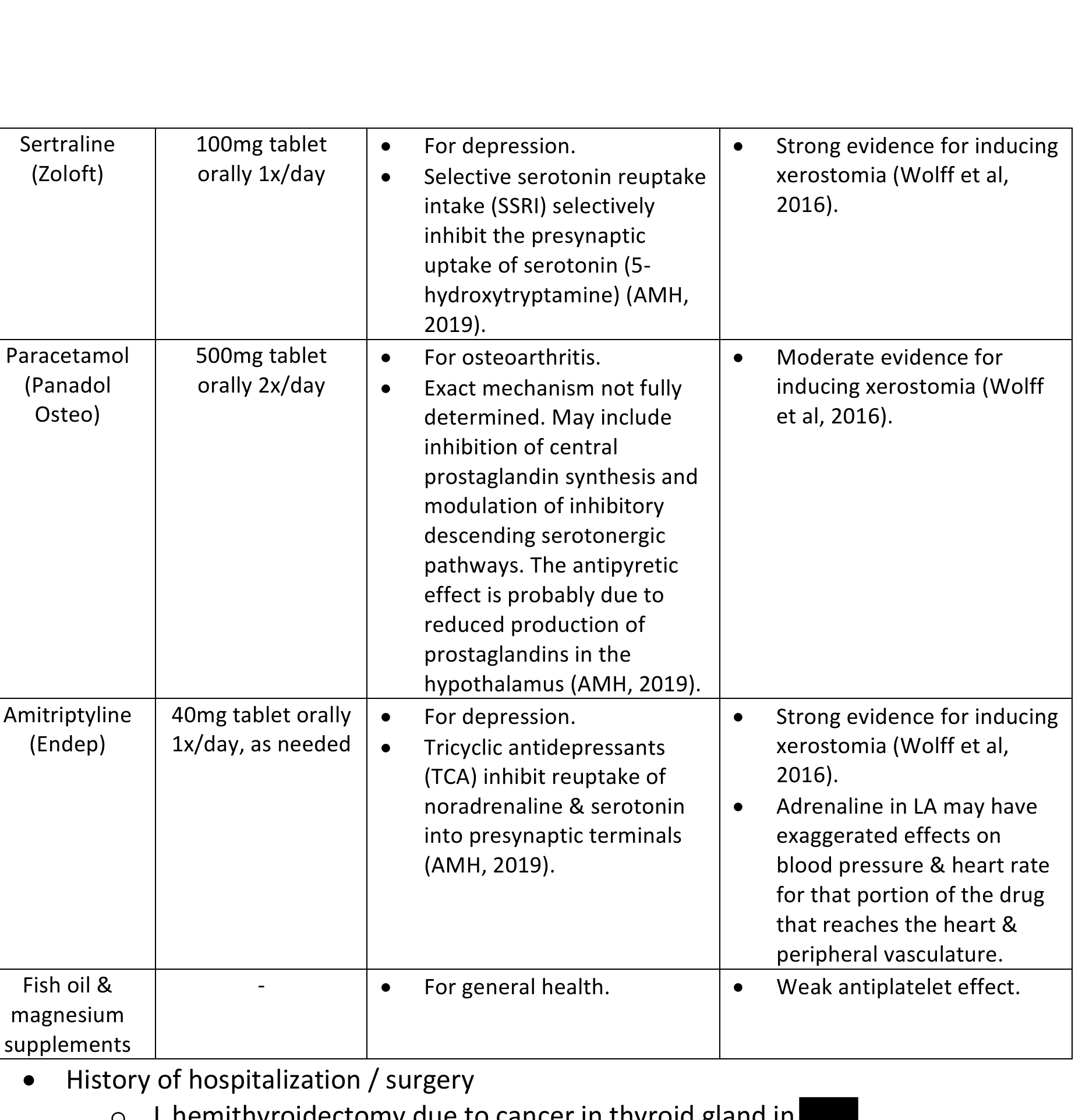
Medications
| Medications | Dosage | Use / Mechanism of Action | Dental Implication |
|---|---|---|---|
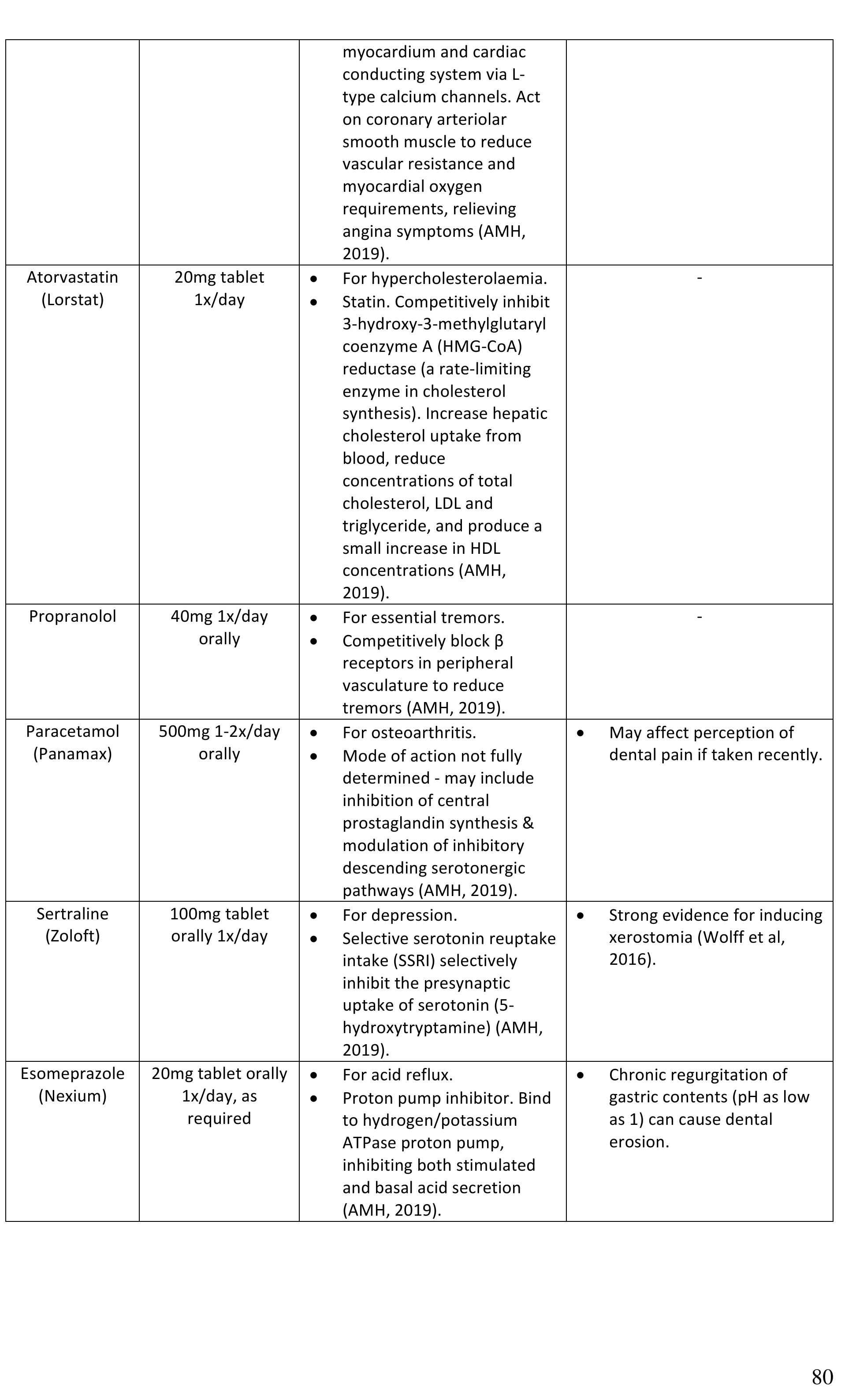
| Pantoprazole | 40mg tablet orally 1x/day | - For GORD - Proton pump inhibitor - irreversibly inactivates the hydrogen/potassium ATPase enzyme system (proton pump), suppressing both stimulated & basal acid secretion (AMH, 2019). | - Chronic regurgitation of gastric contents (pH as low as 1) can cause dental erosion. |
| Medications | Dosage | Use / Mechanism of Action | Dental Implication |
|---|---|---|---|
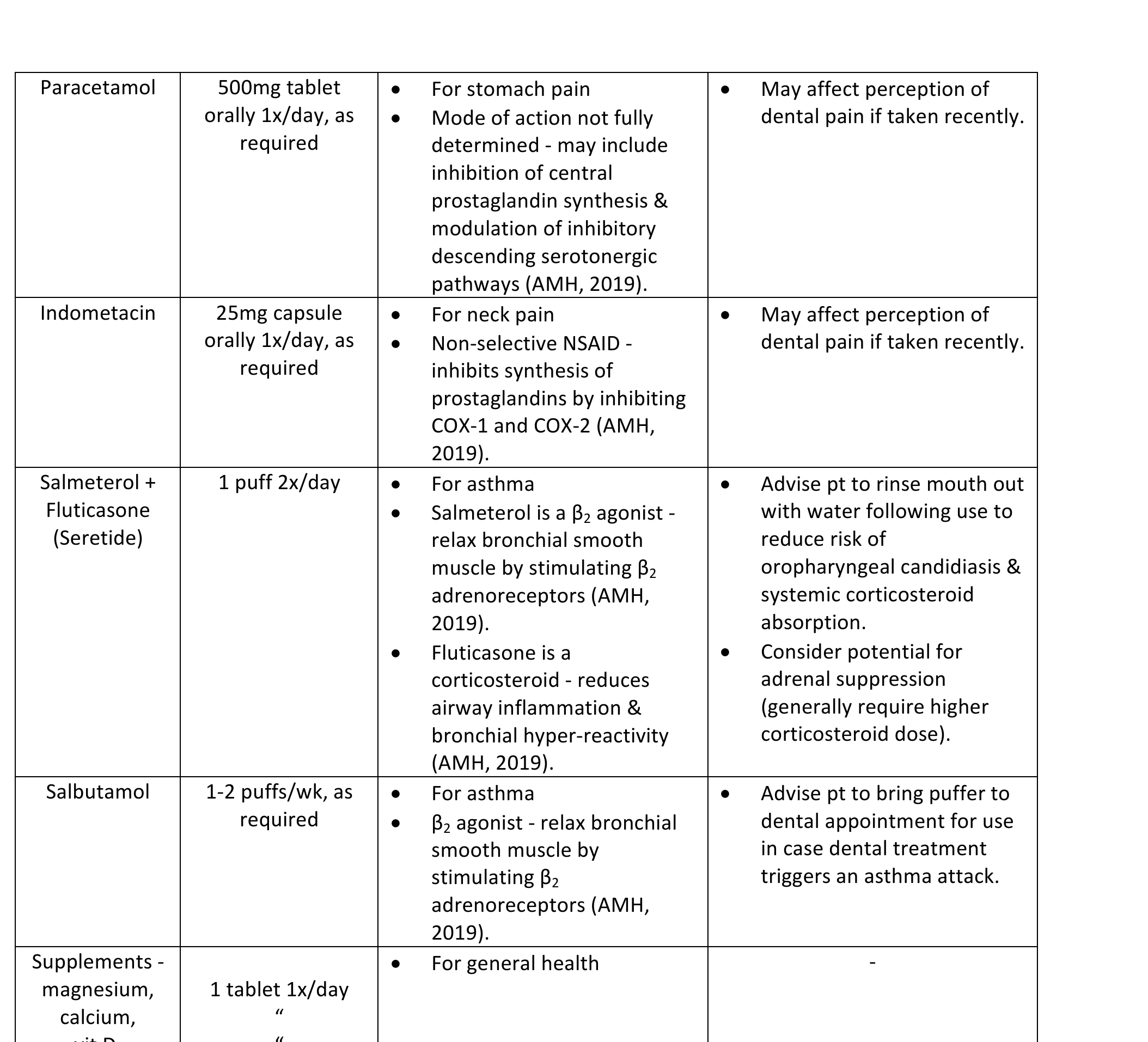
| Paracetamol | 500mg tablet orally 1x/day, as required | - For stomach pain - Mode of action not fully determined - may include inhibition of central prostaglandin synthesis & modulation of inhibitory descending serotonergic pathways (AMH, 2019). | - May affect perception of dental pain if taken recently. |
| Indometacin | 25mg capsule orally 1x/day, as required | - For neck pain - Non-selective NSAID - inhibits synthesis of prostaglandins by inhibiting COX-1 and COX-2 (AMH, 2019). | - May affect perception of dental pain if taken recently. |
| Salmeterol + Fluticasone (Seretide) | 1 puff 2x/day | - For asthma - Salmeterol is a β2 agonist - relax bronchial smooth muscle by stimulating β2 adrenoreceptors (AMH, 2019). - Fluticasone is a corticosteroid - reduces airway inflammation & bronchial hyper-reactivity (AMH, 2019). | - Advise pt to rinse mouth out with water following use to reduce risk of oropharyngeal candidiasis & systemic corticosteroid absorption. - Consider potential for adrenal suppression (generally require higher corticosteroid dose). |
| Salbutamol | 1-2 puffs/wk, as required | - For asthma - β2 agonist - relax bronchial smooth muscle by stimulating β2 adrenoreceptors (AMH, 2019). | - Advise pt to bring puffer to dental appointment for use in case dental treatment triggers an asthma attack. |
| Supplements | 1 tablet 1x/day | - Magnesium, calcium, vit D, folic acid (5mg) for general health. | - |
Hospitalization and Surgery29
- 2014 gastric surgery for stomach cancer.
Allergies
- No known allergies.
Dental History
- Acrylic F/ made 6 years ago as immediate denture.
- Acrylic /P made 4 years ago.
- Previous private practice patient who regularly attended 12-monthly dental recalls.
Oral Hygiene
- Toothbrushing 2x/day with manual toothbrush and 1000ppm fluoride toothpaste.
- Interdental brushes (Piksters) 1x/day.
- Acrylic F/P removed at night, brushed with toothpaste & soaked overnight in Sterident solution.
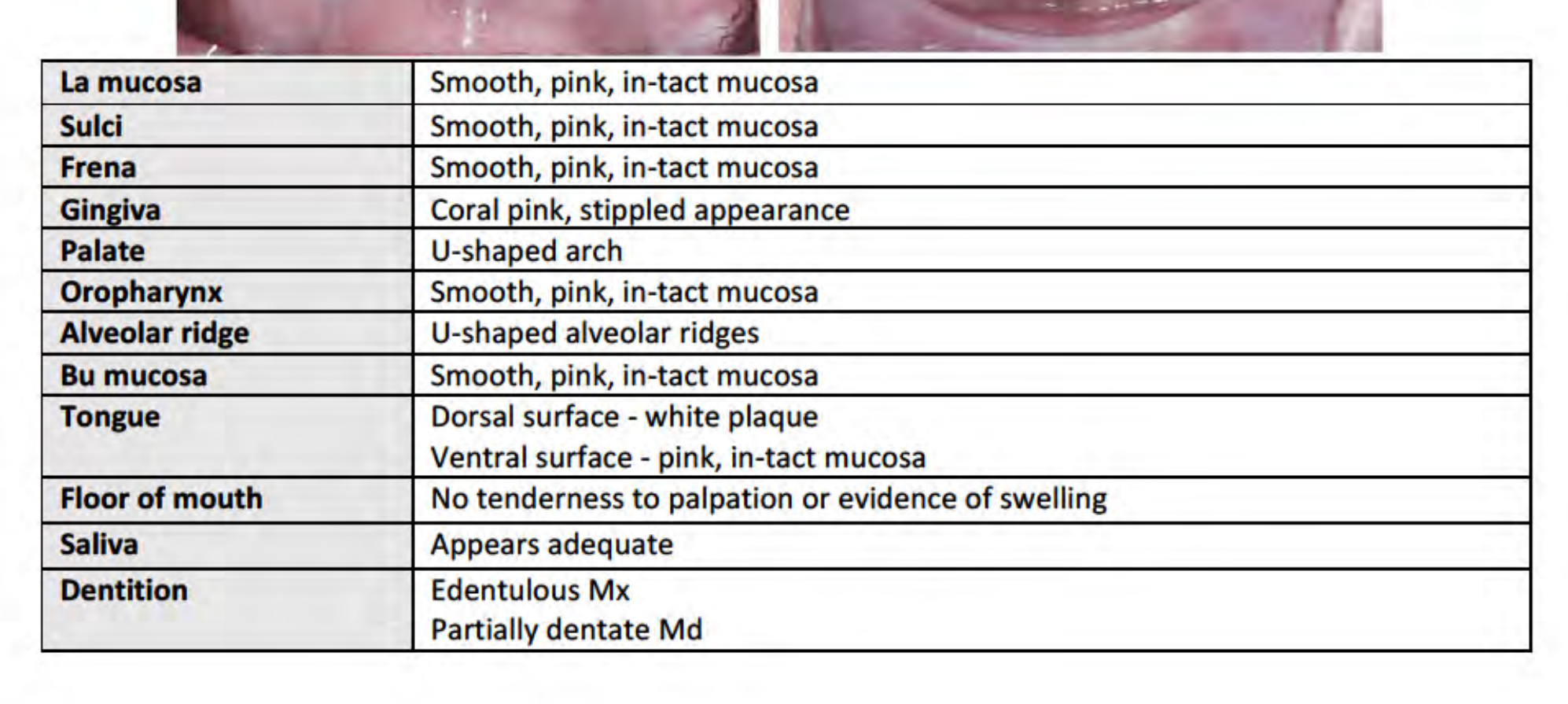
Clinical Examination and Charting30
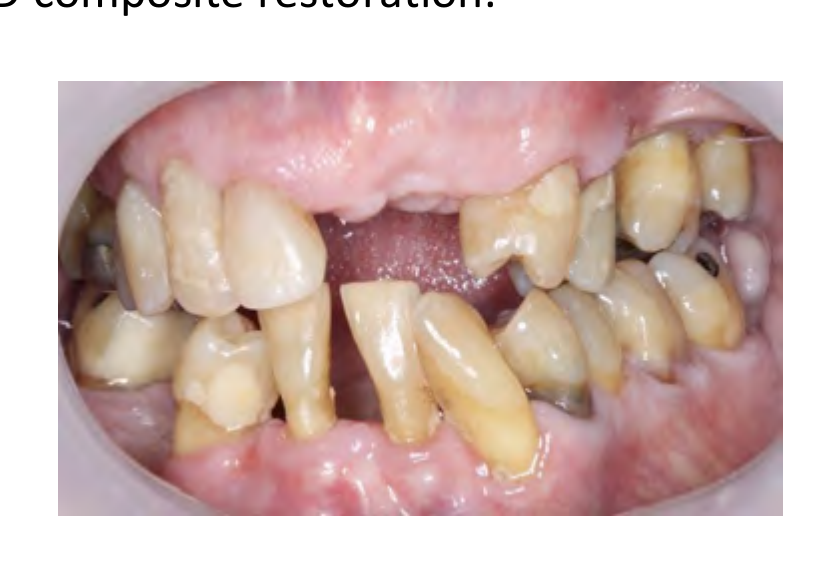
Intra-oral Examination31
| Feature | Findings |
|---|---|
| Labial Mucosa | Smooth, pink, intact mucosa |
| Sulci | Smooth, pink, intact mucosa |
| Frena | Smooth, pink, intact mucosa |
| Gingiva | Coral pink, stippled appearance |
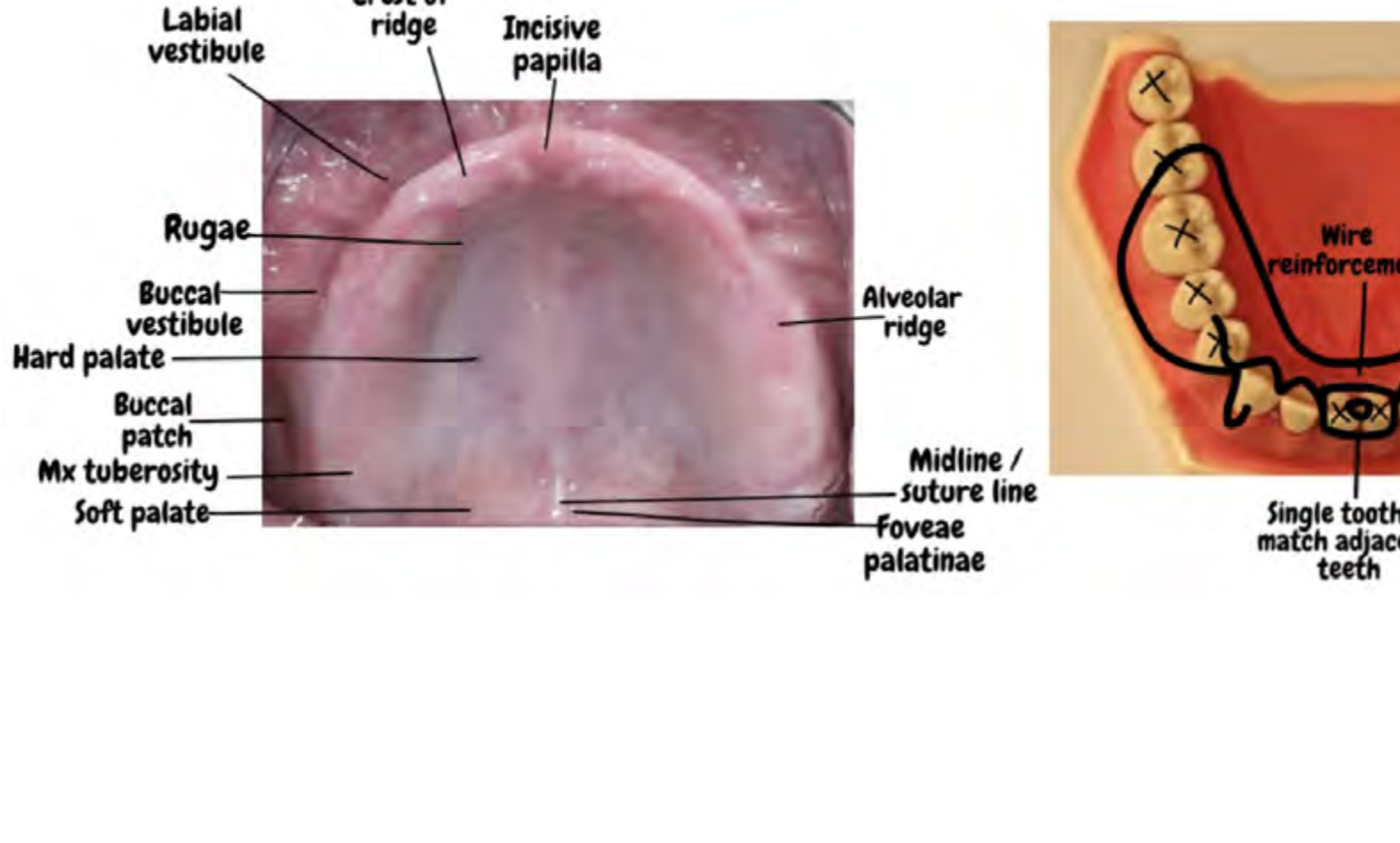
| Palate | U-shaped arch |
| Oropharynx | Smooth, pink, intact mucosa |
| Alveolar Ridge | U-shaped alveolar ridges |
| Buccal Mucosa | Smooth, pink, intact mucosa |
| Tongue | Dorsal surface: white plaque; Ventral surface: pink, intact mucosa |
| Floor of Mouth | No tenderness to palpation or evidence of swelling |
| Saliva | Appears adequate |
| Dentition | Edentulous Maxilla (Mx); Partially dentate Mandible (Md) |
 |  |
 |  |
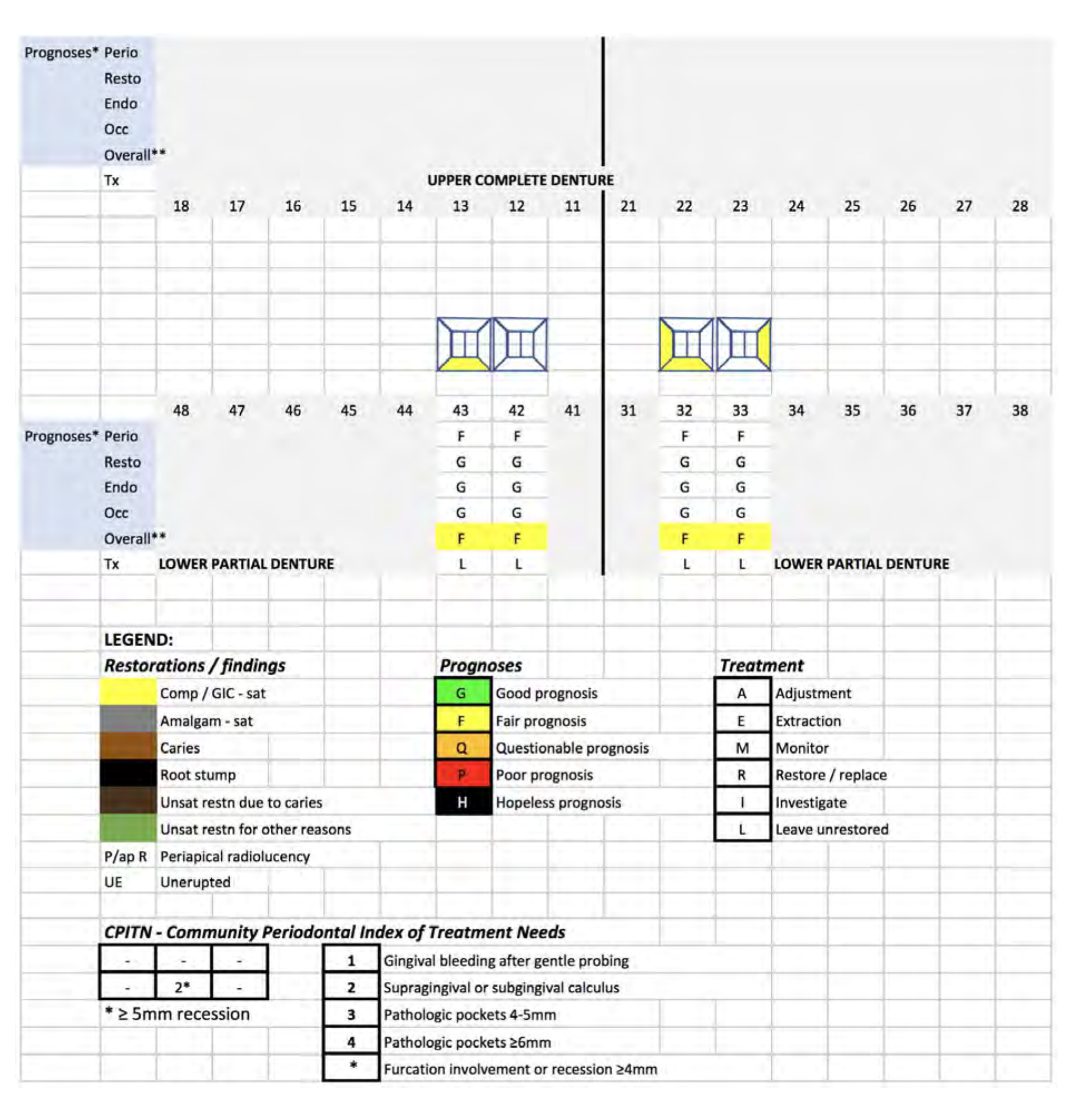
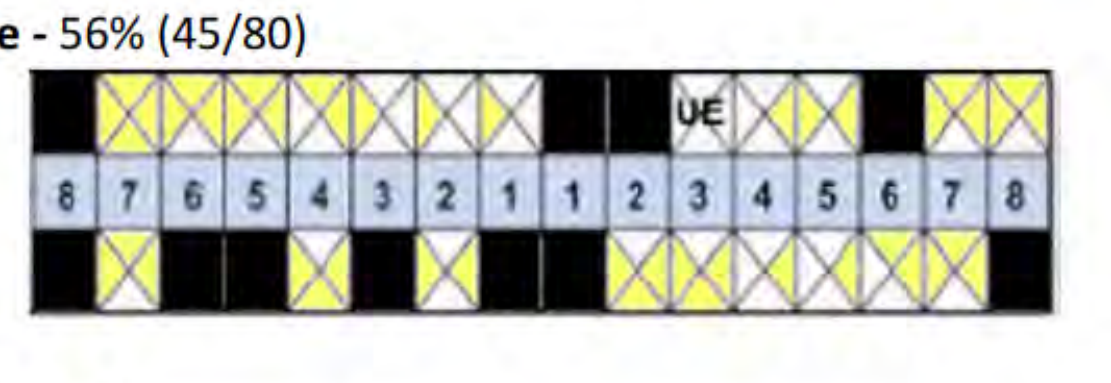
Tooth Charting32
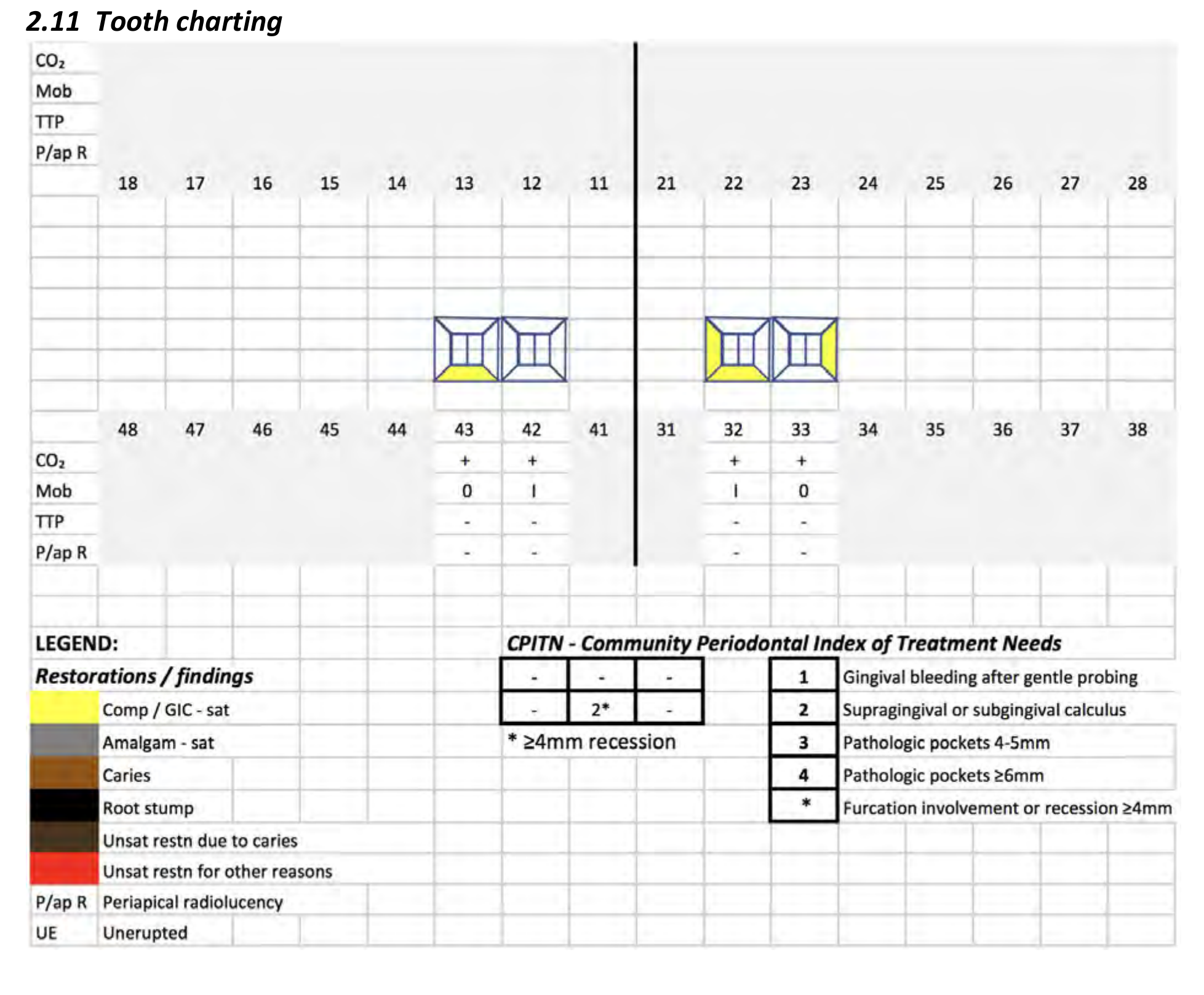
Diagnosis and Risk Assessment33
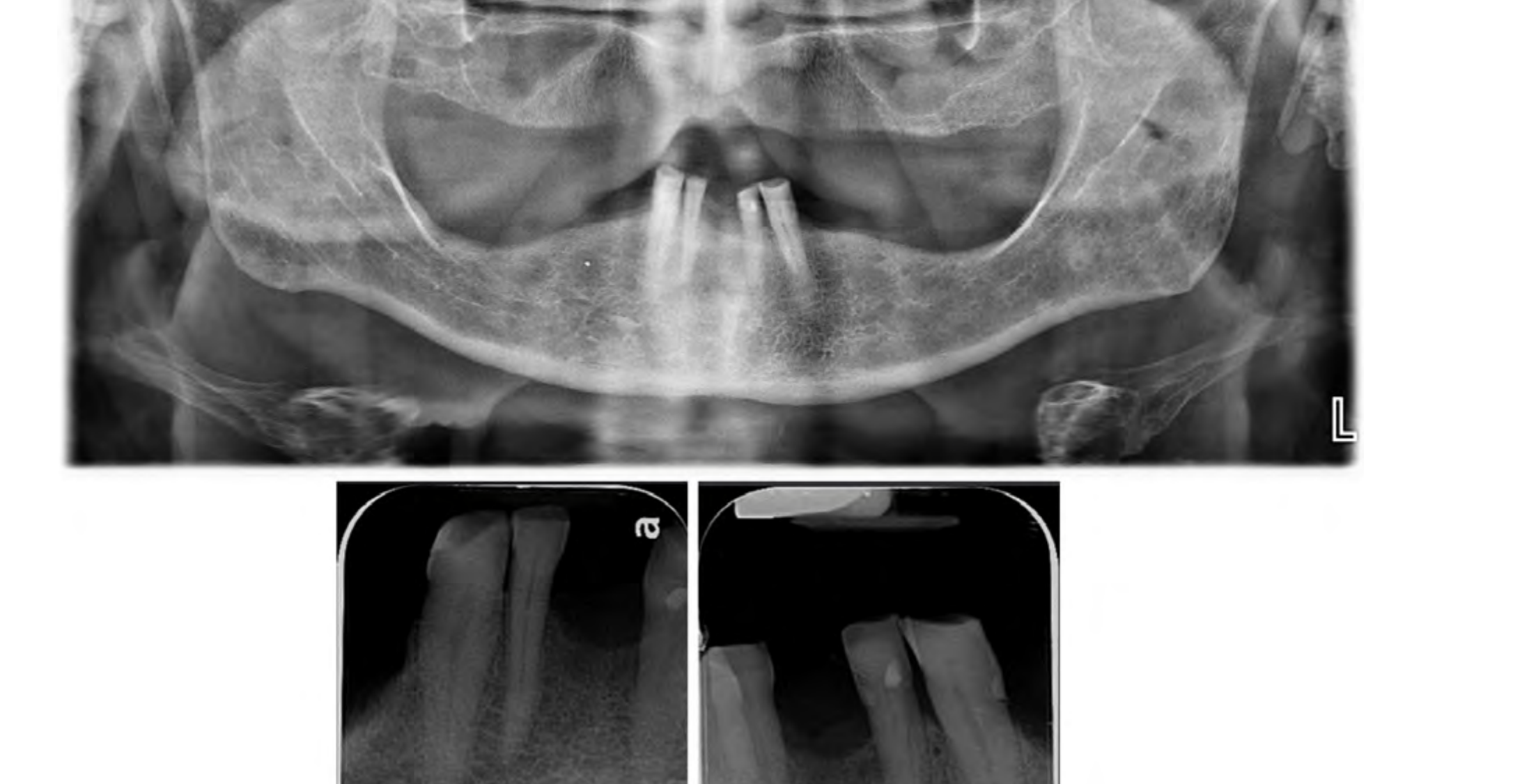
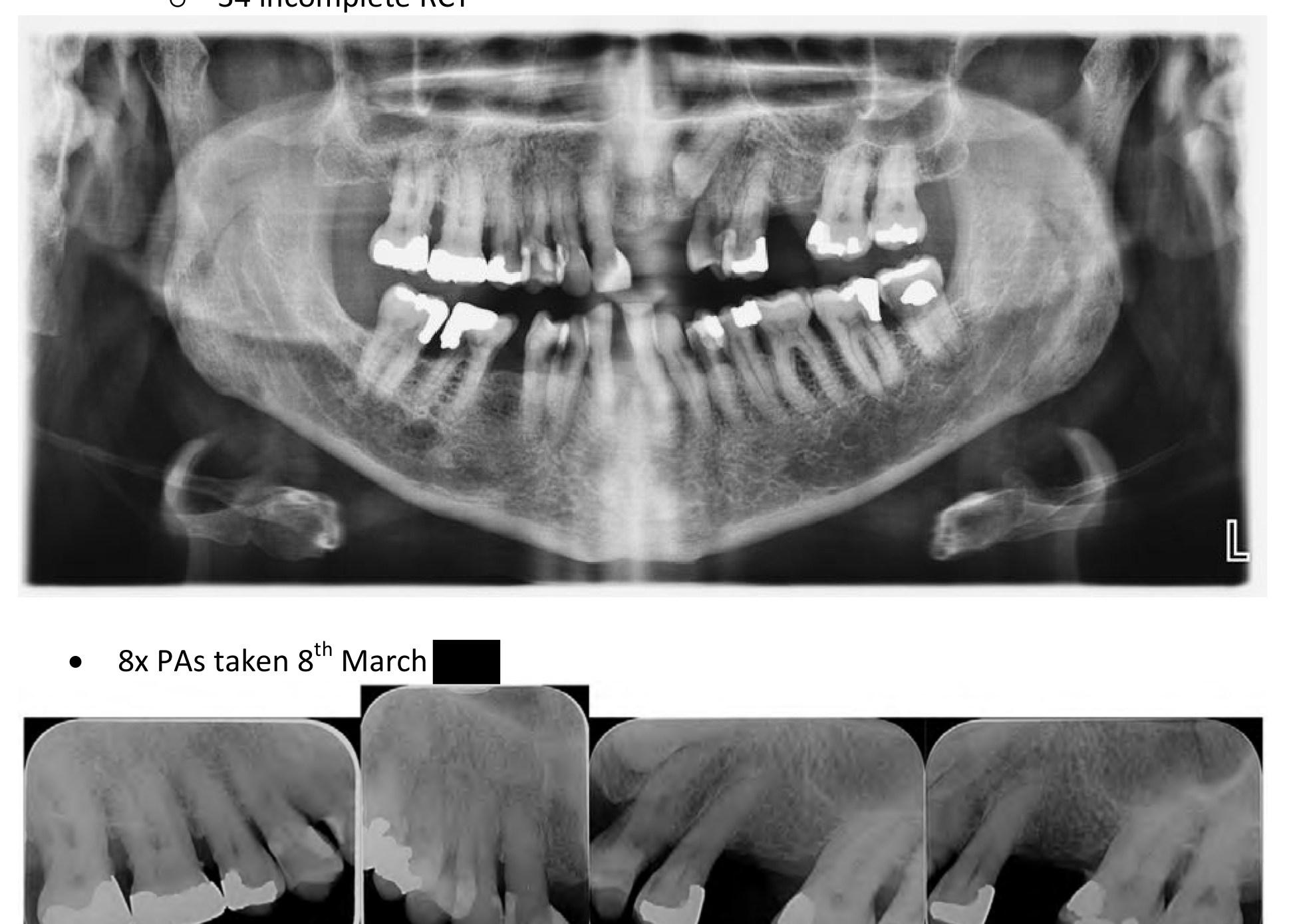
Radiographic Findings34
- OPG taken 18th Sept [redacted]
- 2x PAs taken 22nd Oct [redacted]
- Findings: No evidence of caries, adequate bone support, incisal wear.
 |  |
 |
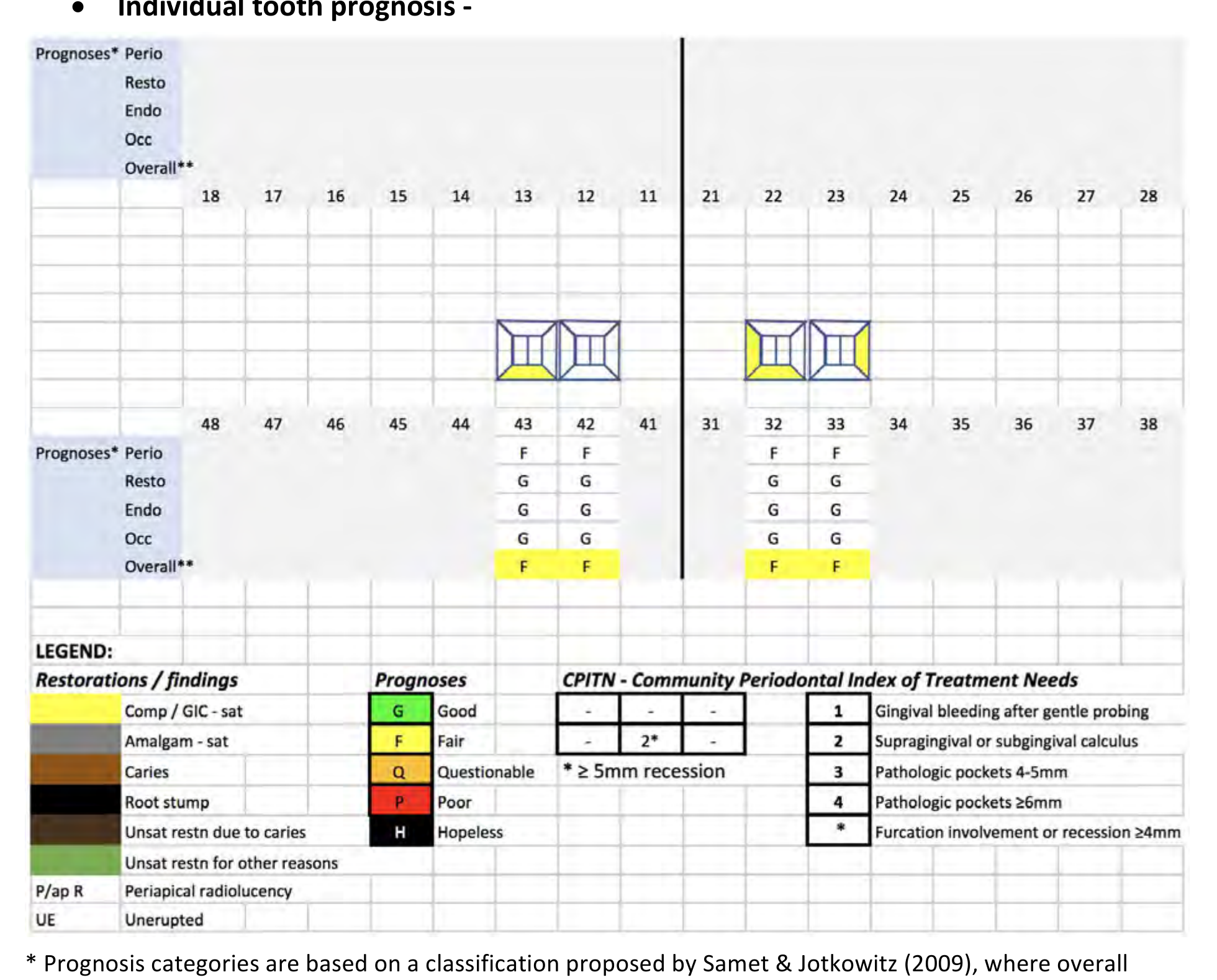
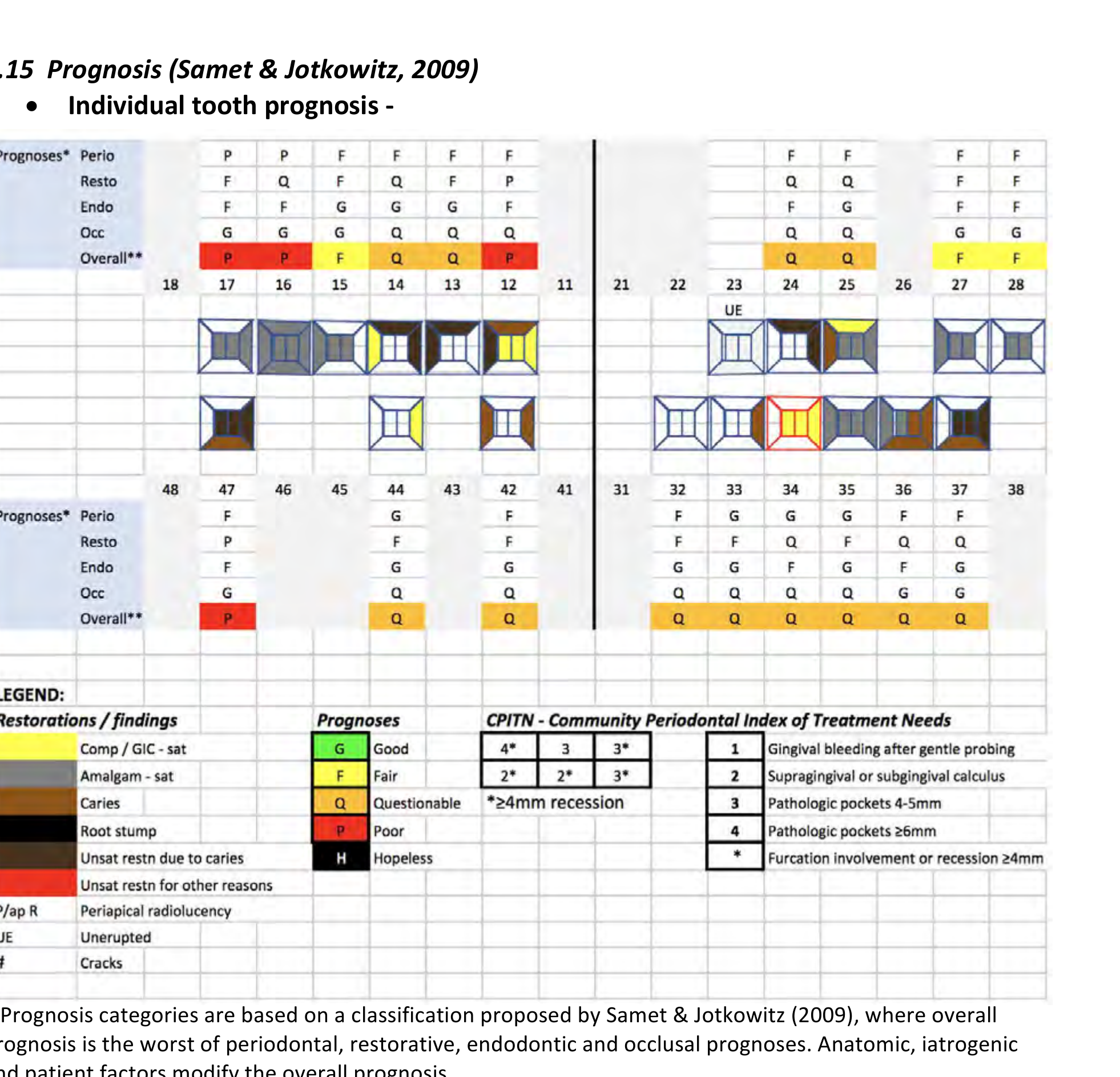
Prognosis (Samet & Jotkowitz, 2009)35
Individual Tooth Prognosis Legend:
| Restorations / Findings | Prognoses | CPITN (Periodontal Index) |
|---|---|---|
| Comp / GIC - sat (Green) | G Good | 1 Gingival bleeding after gentle probing |
| Amalgam - sat (Yellow) | F Fair | 2 Supragingival or subgingival calculus |
| Caries (Orange) | Q Questionable | 3 Pathologic pockets 4-5mm |
| Root stump (Red) | P Poor | 4 Pathologic pockets ≥6mm |
| Unsat restn due to caries (Black) | H Hopeless | * Furcation involvement or recession ≥4mm |
| Unsat restn for other reasons (Green) | ||
| P/ap R (Blue) Periapical radiolucency | ||
| UE (Grey) Unerupted |
Notes on Prognosis:
- Prognosis categories are based on a classification proposed by Samet & Jotkowitz (2009), where overall prognosis is the worst of periodontal, restorative, endodontic and occlusal prognoses.
- Anatomic, iatrogenic and patient factors modify the overall prognosis.
- Overall tooth prognosis modified downward by patient factors: poor OH, cariogenic diet, smoking, aesthetics as motivation for treatment, and high aesthetic expectations.
Overall Dentition Prognosis: FAIR (Yellow)
 |  |
Treatment Planning and Management
Problem List3637
- Unsatisfactory F/P (Presenting Complaint)
- Lack of posterior support leading to loss of retention during function.
- Patient unhappy with appearance of lower middle denture tooth.
- Host Related
- N/A
- Pathology
- Mild generalized gingivitis on a reduced periodontium.
- Morphology
- Class III skeletal relationship.
- Missing teeth: Maxilla (Mx) edentulous, Mandible (Md) Kennedy Cl I Mod 1.
- Lack of posterior support.
- Negative smile arc.
Diagnoses
- Unsatisfactory F/P (presenting complaint)
- Gingivitis
- Mx edentulous
- Md Kennedy Cl I Mod 1
- Lack of posterior support
- Negative smile arc
Treatment Selection38
Patient decided on treatment option 1: remake acrylic F/P due to:
- Patient happy with existing F/P aside from loss of retention in function.
- Able to improve aesthetics & occlusion.
- Relatively low cost of treatment.
Management Plan: Foundational Phase39
-
Address the Presenting Complaint
- Explain to patient that loss of retention of F/ occurs during function due to lack of posterior support provided by F/P.
- Because it is an occlusal problem, both dentures will need to be replaced to address the issue.
- A new set of dentures will also address the aesthetic complaints.
-
Address Lifestyle Factors / OH Routine (4/10)
- Diet (Evans et al, 2008): Patient encouraged to continue balanced diet with low sugar intake, and to drink tap water regularly.
- Oral Hygiene and Dental Visits (Evans et al, 2008):
- Patient encouraged to continue good OH habits for natural teeth.
- For denture hygiene, recommended using a separate toothbrush and brushing the dentures with detergent & water.
- Patient to leave dentures out at night dry in the denture case.
- Patient encouraged to continue attending recall appointments; emphasized that dentures require maintenance as oral tissues change over time.
-
Clinical Procedures
- Scale and clean, prophylaxis paste applied (4/10).
Management Plan: Definitive Phase
- Acrylic F/P Work-up (9/10 - 22/1)
- Mx & Md primary alginate impressions → primary casts.
- Mx & Md special tray fabrication → Mx & Md alginate PVS impressions → secondary / master casts.
- Base & rims fabrication for facebow & bite registration → mounted master casts.
- /P denture design to include lingual wire reinforcement if insufficient thickness of acrylic achievable for torsional strength.
Management Plan: Definitive Phase (Continued)40
- Shade and Try-in
- Shade selection: Vita Classical shade A3.5.
- Anterior tooth try-in to confirm patient is happy with aesthetics.
- Posterior tooth try-in to confirm satisfactory occlusion.
 |  |
 |  |
Initial Phase and Stabilization41
- Oral Hygiene Instruction (OHI): Comprehensive review of brushing and flossing techniques to improve periodontal health.
- Periodontal Therapy: Full mouth debridement and scaling and root planing (SRP) to address existing periodontal concerns.
- Caries Management:
- Tooth #14: Composite restoration.
- Tooth #19: Composite restoration.
- Tooth #31: Composite restoration.
Endodontic and Restorative Preparation
- Endodontic Treatment: Root canal therapy (RCT) performed on tooth #20.
- Post and Core Build-up: Placement of a post and core on tooth #20 to provide adequate structural support for future restoration.
- Provisionalization: Fabrication of a long-term provisional crown for tooth #20 to assess stability and function prior to final restoration.
Definitive Restorative Phase42
- Fixed Prosthodontics: Fabrication and delivery of a Porcelain-Fused-to-Metal (PFM) crown for tooth #20, designed with a distal rest seat to support the planned removable prosthesis.
- Removable Prosthodontics:
- Design and fabrication of a Mandibular Cast Partial Denture (CPD).
- Framework try-in and adjustment.
- Final delivery of the mandibular CPD to restore missing dentition and improve masticatory function.
Maintenance and Follow-up
- Post-Insertion Care: Evaluation of the fit, occlusion, and patient comfort following the delivery of the PFM crown and partial denture.
- Recall Schedule: Establishment of a 6-month periodic oral examination and prophylaxis schedule to monitor oral health and the integrity of the restorations.
Case 3: Aesthetic Fixed Restorative Case
Presenting Complaint43
- “I’ve had a toothache on and off for the past year in one of my upper right back teeth.”
- “I’ve never liked that two of my teeth on the left hand side are stained.”
 |  |
History of Presenting Complaint
Clinical Presentation and History44
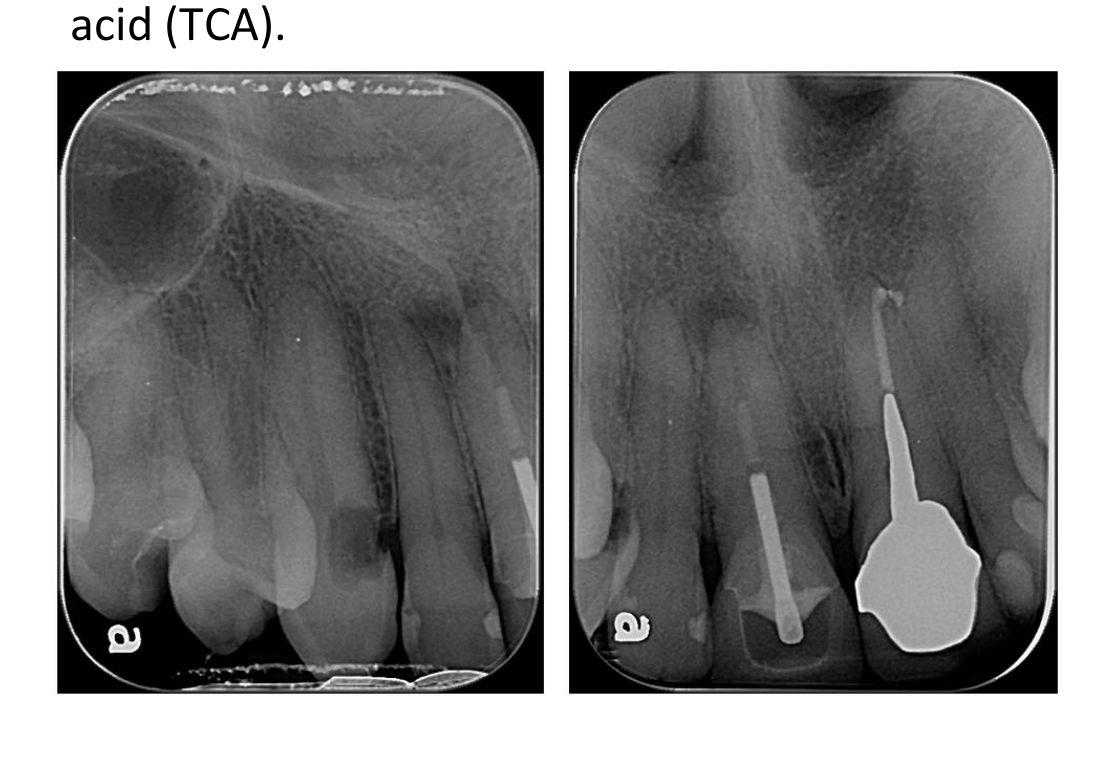
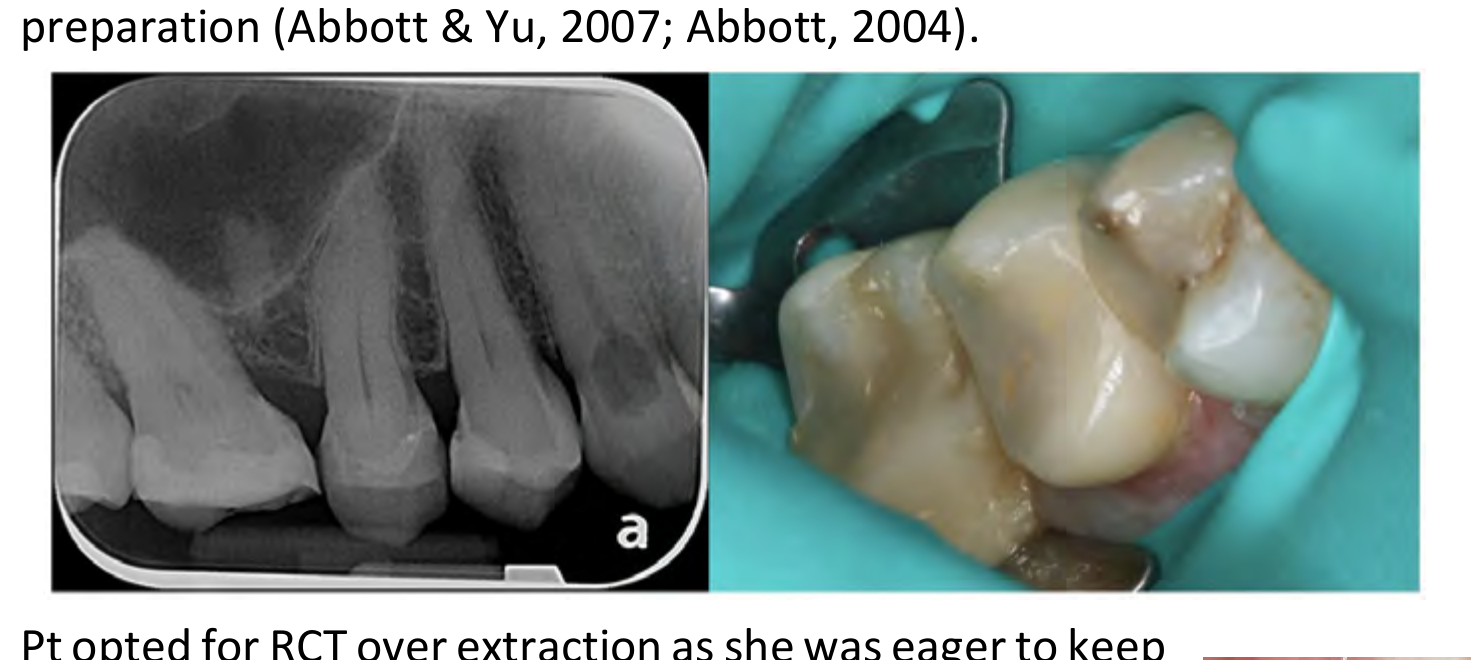
- Spontaneous dull aching sensation on/off in upper right posterior starting February (12 months ago). Pain is exacerbated by hot/cold food and drink. Pain lingers for about an hour.
- In February, an amalgam restoration on tooth 15 was replaced with an indirect composite onlay prepared and cemented in a single visit. Patient reports toothache began after onlay was prepared and did not improve with time.
- In June/July, the patient’s private GDP recommended RCT for tooth 15 but was unavailable for treatment. When the patient re-presented to the private GDP clinic, she was seen by a different GDP who believed “cracks” in the tooth were responsible for symptoms. A “sealant” was placed over the cracks, but symptoms persisted. Patient would like the toothache resolved.
- Patient identified “stained” teeth as 22 and 24. Patient recalls the staining appeared some time ago.
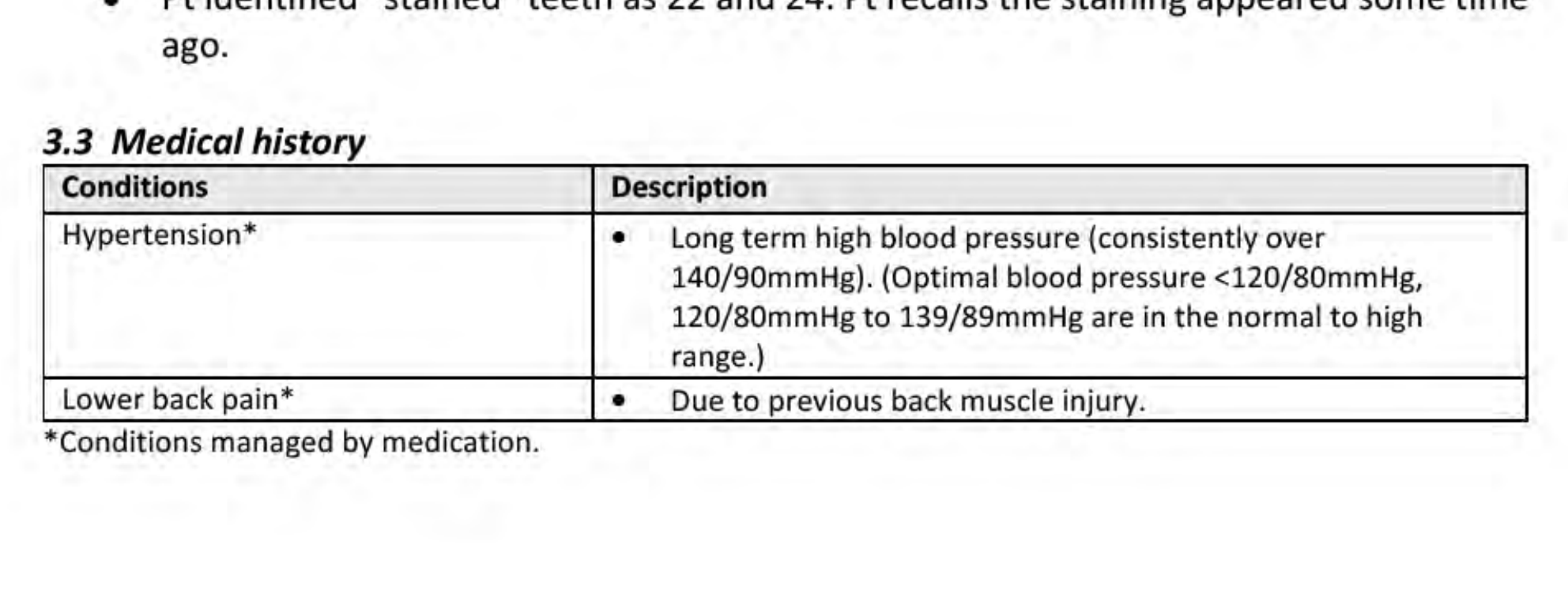
Medical History
- Hypertension: Long term high blood pressure (consistently over 140/90mmHg). (Optimal blood pressure <120/80mmHg; 120/80mmHg to 139/89mmHg are in the normal to high range). Managed by medication.
- Lower back pain: Due to previous back muscle injury. Managed by medication.
Clinical Examination and Radiographs454647
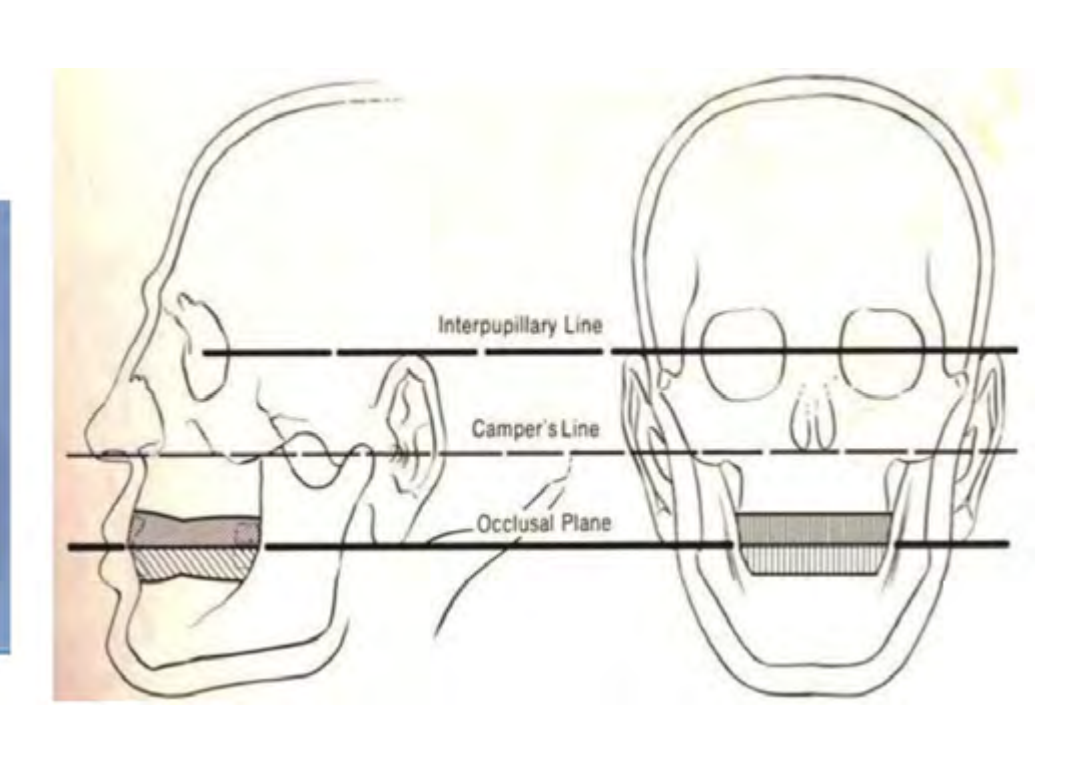
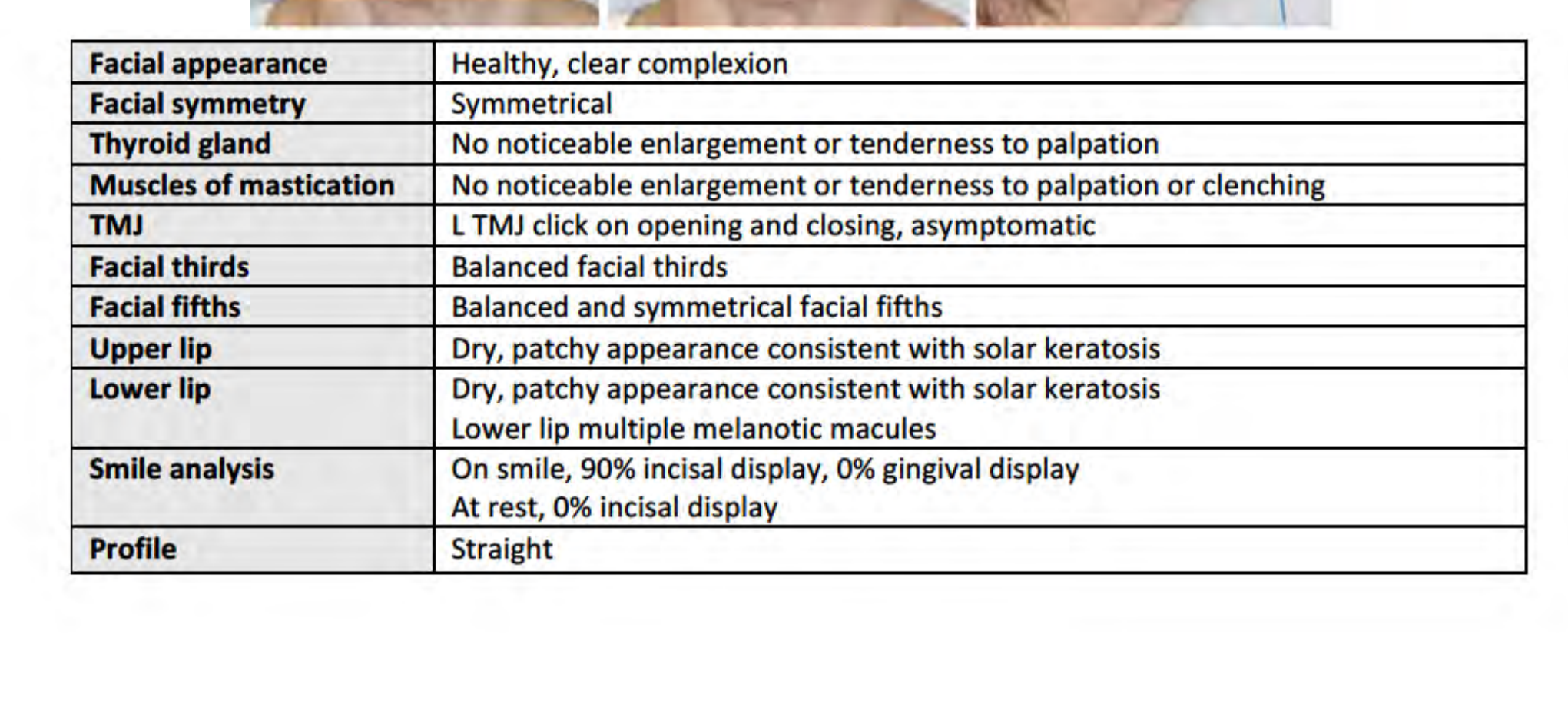
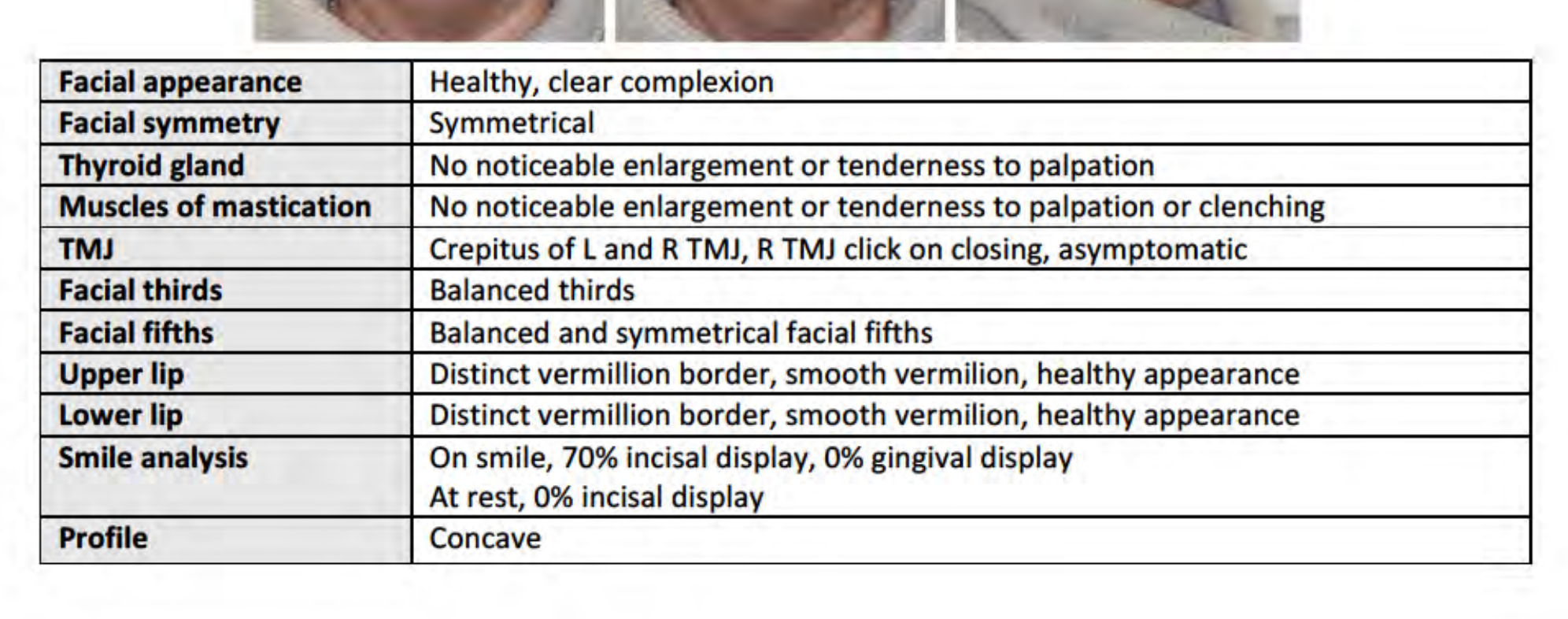
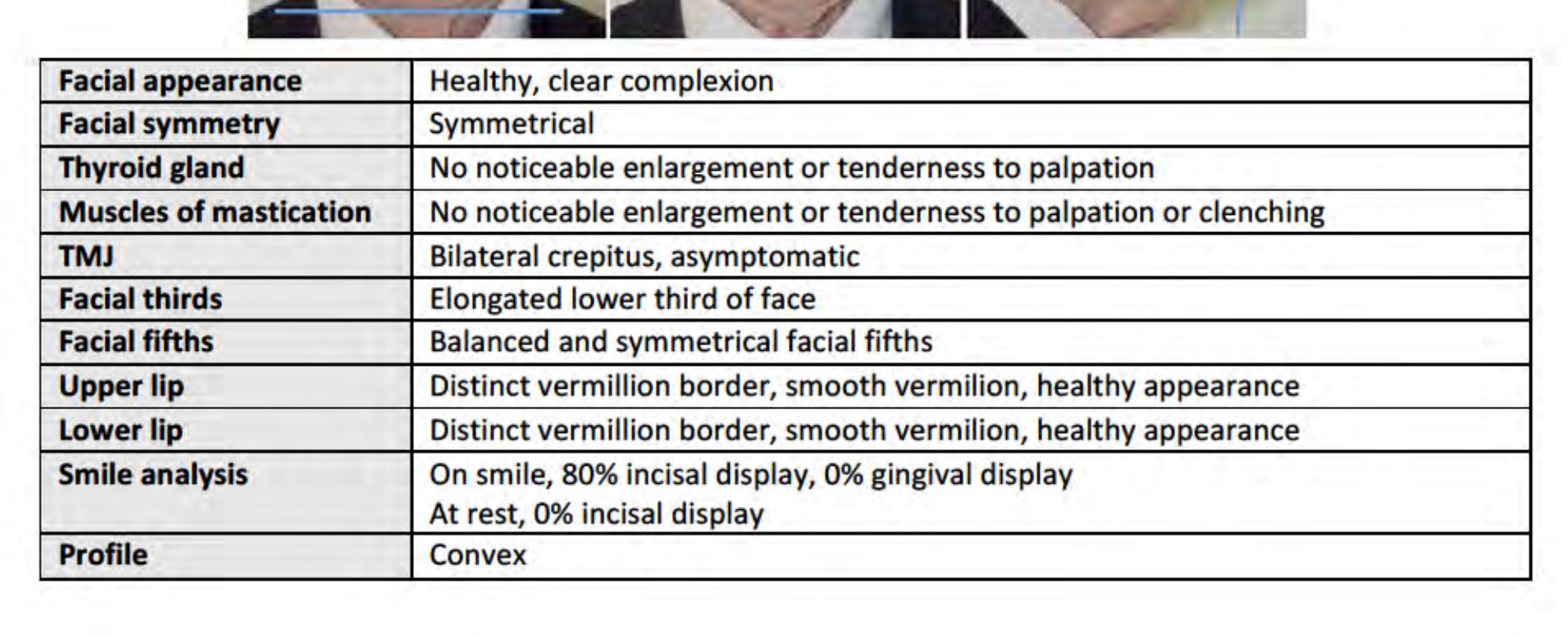
Extra-oral Examination48
- Facial appearance: Healthy, clear complexion
- Facial symmetry: Symmetrical
- Thyroid gland: No noticeable enlargement or tenderness to palpation
- Muscles of mastication: No noticeable enlargement or tenderness to palpation or clenching
- TMJ: Left TMJ click on opening and closing, asymptomatic
- Facial thirds: Balanced facial thirds
- Facial fifths: Balanced and symmetrical facial fifths
- Upper lip: Dry, patchy appearance consistent with solar keratosis
- Lower lip: Dry, patchy appearance consistent with solar keratosis; multiple melanotic macules
- Smile analysis: On smile, 90% incisal display, 0% gingival display. At rest, 0% incisal display
- Profile: Straight
 |  |
Tooth Charting49
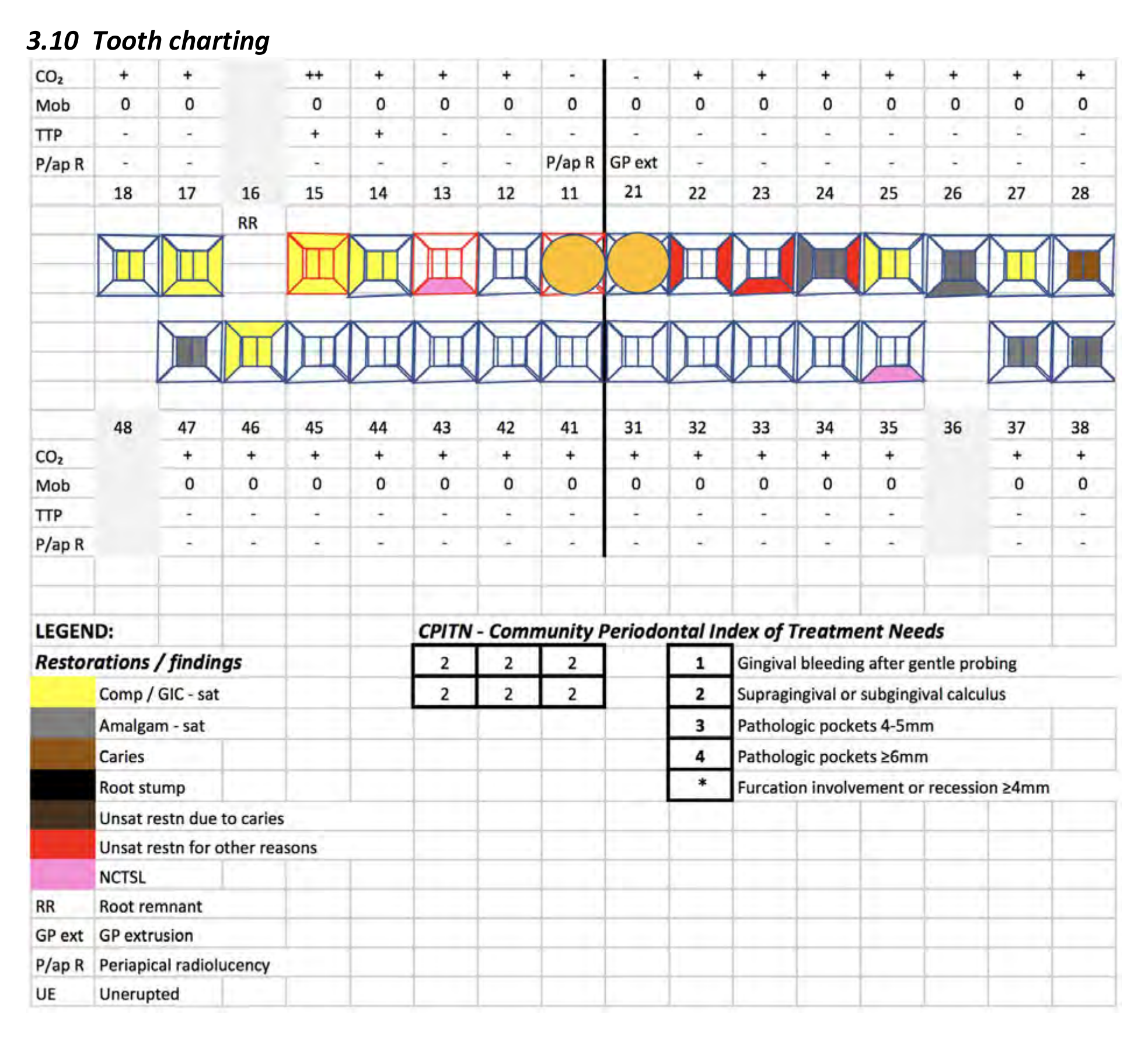
Radiographic Findings50
OPG (taken 20th March)
- 11, 21: Previous RCT
- Heavily restored dentition
- Missing tooth 36; mesially tilted 37 & 38
3x PAs (taken 13th February)
- 16: Root remnant at sinus floor; no periapical radiolucency or clinical evidence of infection
- 13: External invasive resorption Class III
- 14, 15, 24: No evidence of periapical radiolucencies
- 11: Previous RCT, technically inadequate & periapical radiolucency
- 23: Unsatisfactory distal restoration
- 24: Non-ideal distal contact
 |  |
Diagnosis and Problem List5152
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |  |  |
 |
Problem List53
Presenting Complaints
- 15: Chronic irreversible pulpitis with primary acute apical periodontitis due to tooth preparation.
- Discolouration: Associated with 22 and 24 restoration breakdown.
Pathology
- Generalised mild gingivitis.
- 11: Previous root canal treatment (technically unsatisfactory), infected root canal system, and chronic apical periodontitis due to restoration breakdown.
- 13: External invasive resorption Class III.
- 28: Occlusal caries.
- 23: Restoration breakdown.
- 35: Buccal Non-Carious Cervical Tooth Surface Loss (NCTSL).
Morphology
- Skeletal Class I.
- Stable MIP, acceptable VD, canine guidance in dynamic occlusion.
- 16: Root remnant at Right sinus floor.
- Missing 36.
- Mesially tilted 17 & 37.
Diagnoses
- Endodontically involved teeth (includes presenting complaint)
- Discoloured teeth (presenting complaint)
- Gingivitis
- Caries
- Restoration breakdown
- NCTSL
Footnotes
-
Original PDF page 1: Sample portfolio 1, p.1 ↩
-
Original PDF page 2: Sample portfolio 1, p.2 ↩
-
Original PDF page 3: Sample portfolio 1, p.3 ↩
-
Original PDF page 4: Sample portfolio 1, p.4 ↩
-
Original PDF page 7: Sample portfolio 1, p.7 ↩
-
Original PDF page 5: Sample portfolio 1, p.5 ↩
-
Original PDF page 6: Sample portfolio 1, p.6 ↩
-
Original PDF page 9: Sample portfolio 1, p.9 ↩
-
Original PDF page 8: Sample portfolio 1, p.8 ↩
-
Original PDF page 10: Sample portfolio 1, p.10 ↩
-
Original PDF page 11: Sample portfolio 1, p.11 ↩
-
Original PDF page 12: Sample portfolio 1, p.12 ↩
-
Original PDF page 13: Sample portfolio 1, p.13 ↩
-
Original PDF page 14: Sample portfolio 1, p.14 ↩
-
Original PDF page 15: Sample portfolio 1, p.15 ↩
-
Original PDF page 18: Sample portfolio 1, p.18 ↩
-
Original PDF page 19: Sample portfolio 1, p.19 ↩
-
Original PDF page 16: Sample portfolio 1, p.16 ↩
-
Original PDF page 17: Sample portfolio 1, p.17 ↩
-
Original PDF page 20: Sample portfolio 1, p.20 ↩
-
Original PDF page 21: Sample portfolio 1, p.21 ↩
-
Original PDF page 22: Sample portfolio 1, p.22 ↩
-
Original PDF page 23: Sample portfolio 1, p.23 ↩
-
Original PDF page 24: Sample portfolio 1, p.24 ↩
-
Original PDF page 25: Sample portfolio 1, p.25 ↩
-
Original PDF page 26: Sample portfolio 1, p.26 ↩
-
Original PDF page 27: Sample portfolio 1, p.27 ↩
-
Original PDF page 29: Sample portfolio 1, p.29 ↩
-
Original PDF page 28: Sample portfolio 1, p.28 ↩
-
Original PDF page 31: Sample portfolio 1, p.31 ↩
-
Original PDF page 30: Sample portfolio 1, p.30 ↩
-
Original PDF page 32: Sample portfolio 1, p.32 ↩
-
Original PDF page 34: Sample portfolio 1, p.34 ↩
-
Original PDF page 33: Sample portfolio 1, p.33 ↩
-
Original PDF page 35: Sample portfolio 1, p.35 ↩
-
Original PDF page 36: Sample portfolio 1, p.36 ↩
-
Original PDF page 37: Sample portfolio 1, p.37 ↩
-
Original PDF page 38: Sample portfolio 1, p.38 ↩
-
Original PDF page 39: Sample portfolio 1, p.39 ↩
-
Original PDF page 40: Sample portfolio 1, p.40 ↩
-
Original PDF page 41: Sample portfolio 1, p.41 ↩
-
Original PDF page 42: Sample portfolio 1, p.42 ↩
-
Original PDF page 43: Sample portfolio 1, p.43 ↩
-
Original PDF page 44: Sample portfolio 1, p.44 ↩
-
Original PDF page 46: Sample portfolio 1, p.46 ↩
-
Original PDF page 49: Sample portfolio 1, p.49 ↩
-
Original PDF page 50: Sample portfolio 1, p.50 ↩
-
Original PDF page 45: Sample portfolio 1, p.45 ↩
-
Original PDF page 47: Sample portfolio 1, p.47 ↩
-
Original PDF page 48: Sample portfolio 1, p.48 ↩
-
Original PDF page 52: Sample portfolio 1, p.52 ↩
-
Original PDF page 53: Sample portfolio 1, p.53 ↩
-
Original PDF page 51: Sample portfolio 1, p.51 ↩