Case Portfolio1
[REDACTED]
DMD 4 [REDACTED]
Table Of Contents
Case 1: Multi-disciplinary (Page 4)2
- The patient (5)
- Examination and diagnostics (9)
- Diagnoses and problem list (19)
- Prognosis (20)
- Treatment options (22)
- Management plan (25)
- Treatment delivery (26)
Case 2: Fixed Aesthetic (Page 42)
- The patient (43)
- Examination and diagnostics (45)
- Diagnoses and problem list (56)
- Prognosis (58)
- Treatment options (60)
- Management plan (64)
- Treatment delivery (66)
Case 3: Removable Aesthetic (Page 76)
- The patient (77)
- Examination and diagnostics (45)
- Diagnoses and problem list (88)
- Prognosis (89)
- Treatment options (92)
- Management plan (95)
- Treatment delivery (96)
Case 4: Fixed Occlusal Rehabilitation (Page 100)
- The patient (101)
- Examination and diagnostics (105)
- Diagnoses and problem list (114)
- Prognosis (115)
- Treatment options (117)
Case 4: Fixed Occlusal Rehabilitation (Continued)3
- Management plan (120)
- Treatment delivery (121)
Case 5: Removable Occlusal Rehabilitation (Page 129)
- The patient (130)
- Examination and diagnostics (134)
- Diagnoses and problem list (143)
- Prognosis (144)
- Treatment options (146)
- Management plan (148)
- Treatment delivery (149)
References
- References (158)
Case 1: Multi-disciplinary
Case Overview4
- Case Type: Multi-disciplinary
The Patient
Patient Details5
- Age: 64-year-old male
Presenting Complaints (January 2019)
- Intermittent pain in teeth 37 and 47, and in the gums.
- Cavity in tooth 22 causing sensitivity and food impaction.
- Desire for dentures to replace missing teeth.
History of Presenting Complaints
- Lower Left: Dull, throbbing pain lingering with minor temperature changes.
- Lower Right: Recent spontaneous dull pain with minor temperature changes.
- Gingiva: Pain and bleeding during brushing.
Medical History and Dental Implications6
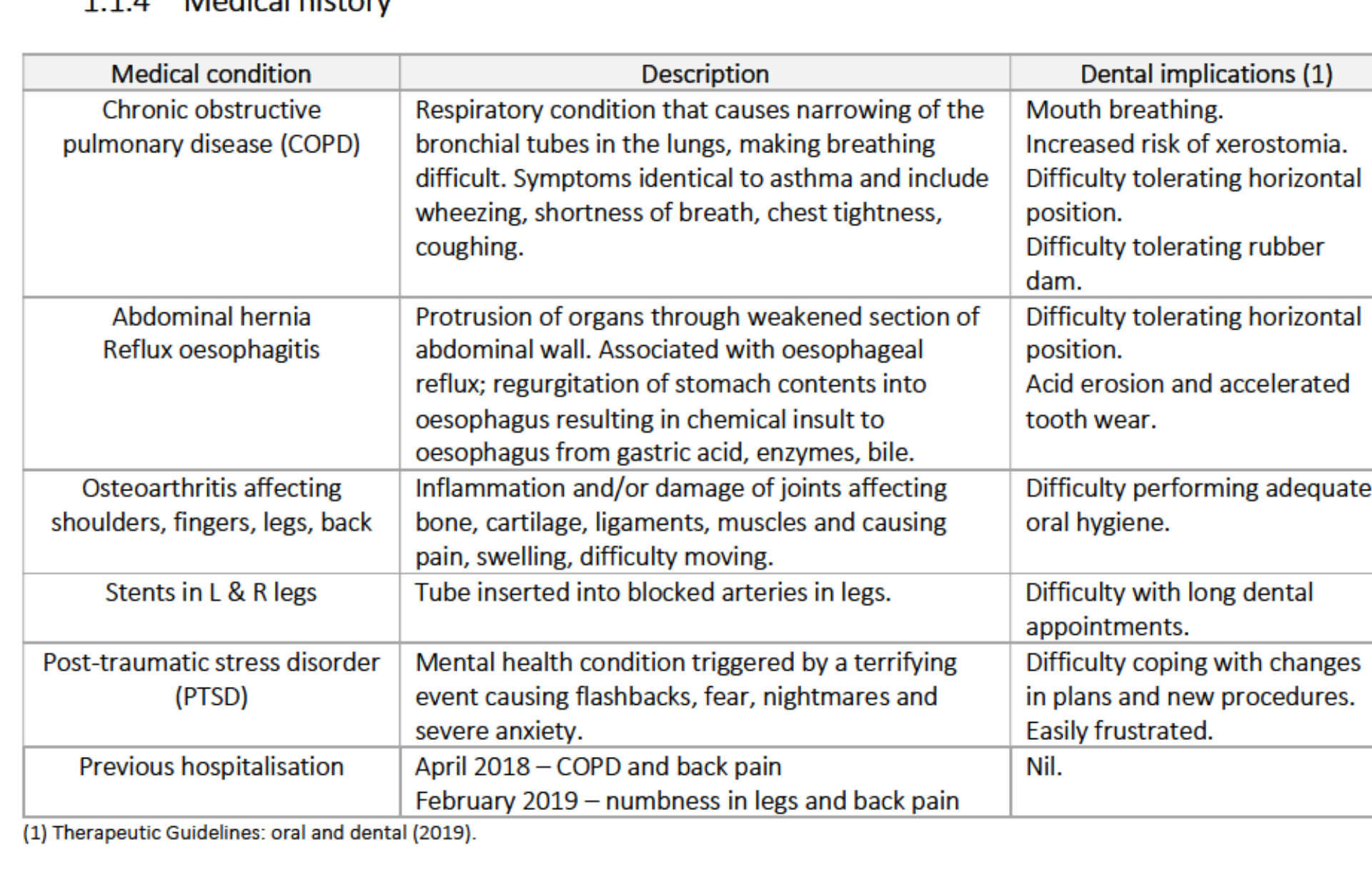
| Medical Condition | Description | Dental Implications |
|---|---|---|
| Chronic Obstructive Pulmonary Disease (COPD) | Respiratory narrowing causing wheezing and shortness of breath. | Mouth breathing; increased xerostomia risk; difficulty with horizontal positioning and rubber dam. |
| Abdominal Hernia / Reflux Oesophagitis | Protrusion of organs; associated with esophageal reflux and gastric acid insult. | Difficulty with horizontal positioning; acid erosion and accelerated tooth wear. |
| Osteoarthritis | Joint inflammation affecting shoulders, fingers, legs, and back. | Difficulty performing adequate oral hygiene. |
| Stents (L & R legs) | Inserted for blocked arteries. | Difficulty with long dental appointments. |
| Post-Traumatic Stress Disorder (PTSD) | Triggered by terrifying events; causes flashbacks and severe anxiety. | Difficulty coping with plan changes; easily frustrated. |
| Previous Hospitalization | April 2018 (COPD/back pain); Feb 2019 (leg numbness). | Nil. |
 |  |
Medications
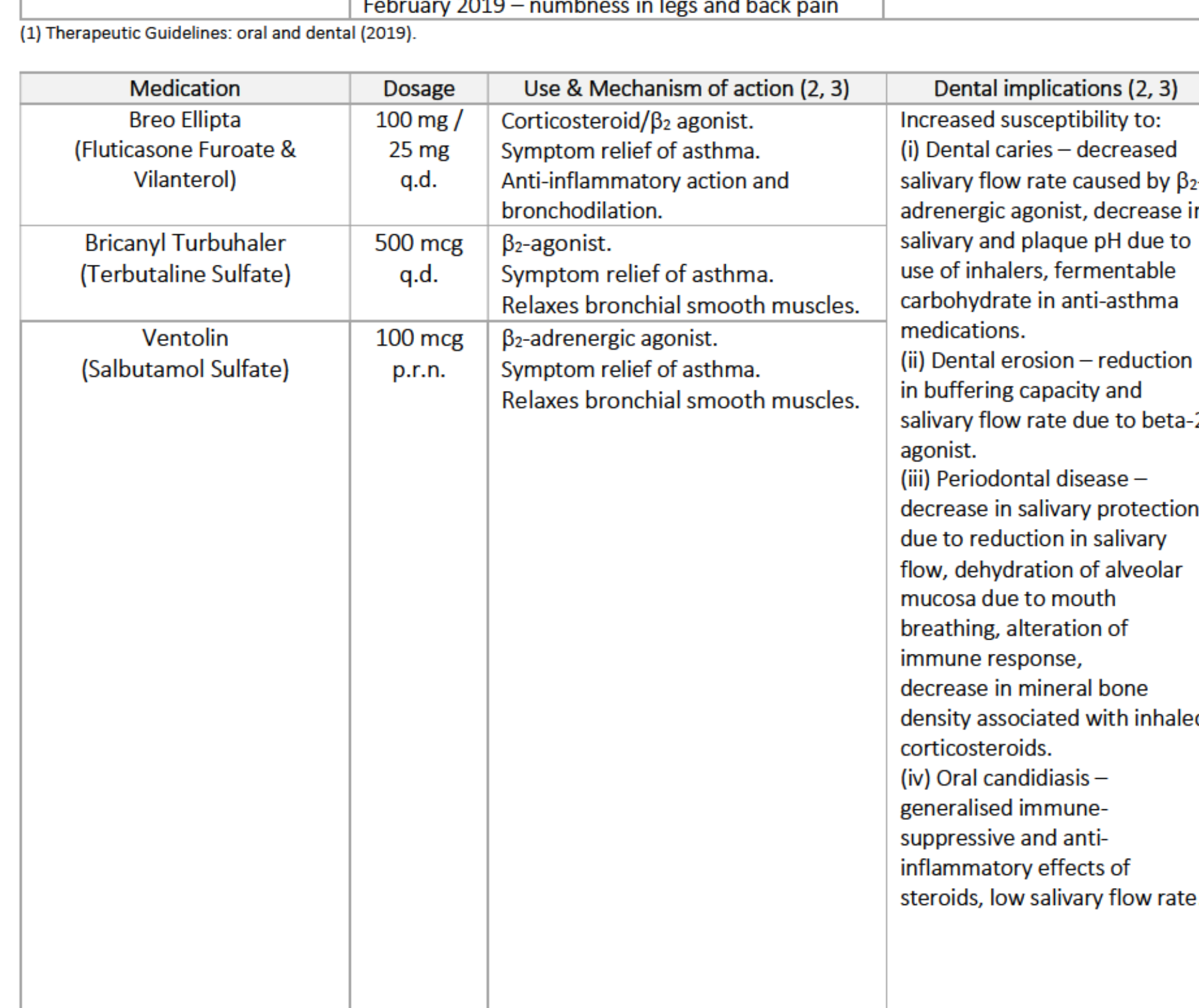
| Medication | Dosage | Mechanism of Action | Dental Implications |
|---|---|---|---|
| Breo Ellipta | 100 mg / 25 mg q.d. | Corticosteroid/β₂ agonist for asthma. | Increased susceptibility to dental caries, periodontal disease, and oral candidiasis. |
| Bricanyl Turbuhaler | 500 mcg q.d. | β₂-agonist for asthma. | Reduction in buffering capacity and salivary flow; dental erosion. |
| Ventolin | 100 mcg p.r.n. | β₂-adrenergic agonist for asthma. | Dehydration of mucosa; alteration of immune response; decreased mineral bone density. |
Medication Management and Allergies7
Additional Medications
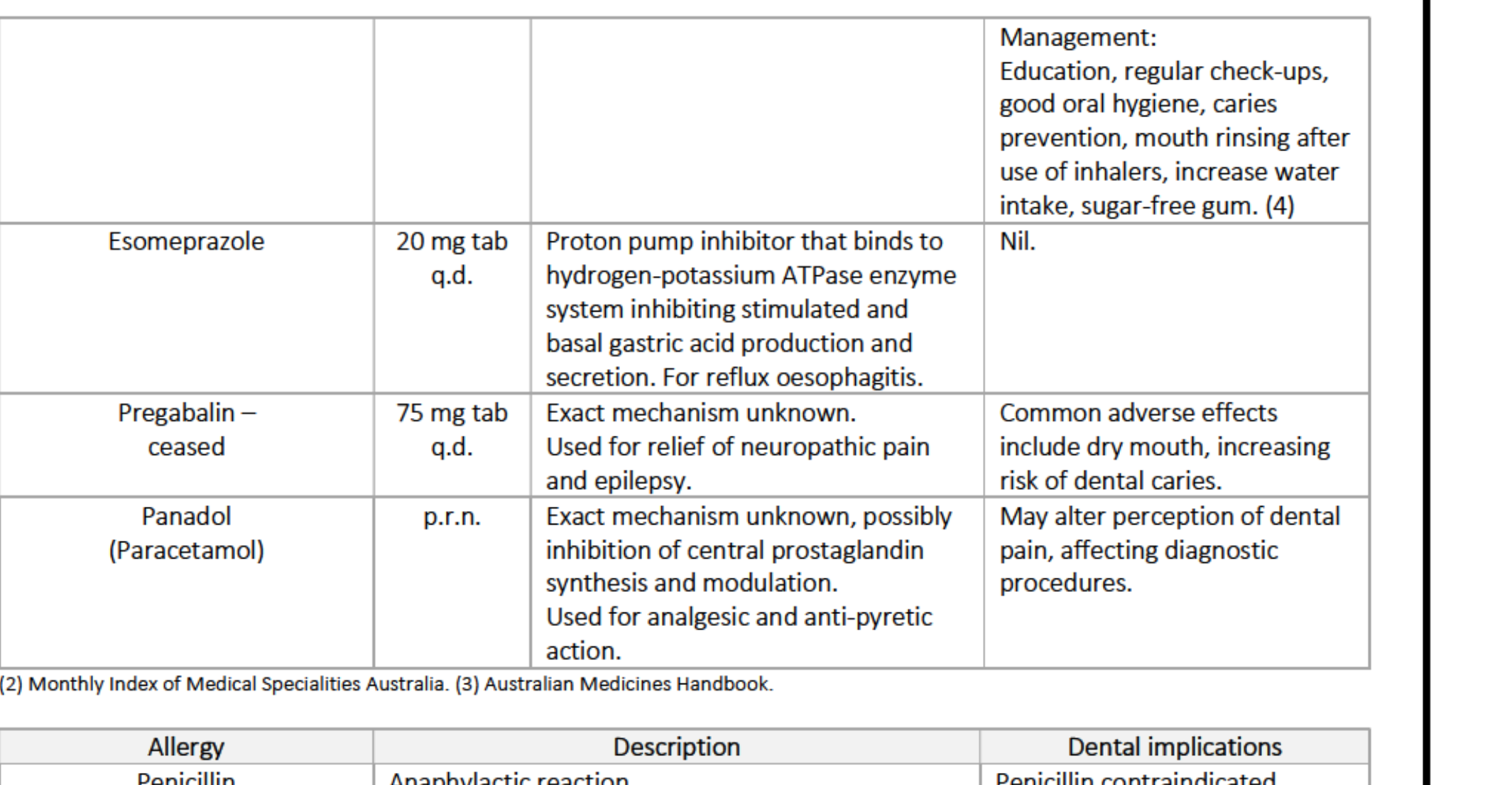
- Management Strategy: Education, regular check-ups, caries prevention, mouth rinsing after inhaler use, increased water intake, and sugar-free gum.
- Esomeprazole (20 mg q.d.): Proton pump inhibitor; nil dental implications.
- Pregabalin (75 mg q.d. - ceased): Used for neuropathic pain/epilepsy; adverse effect includes dry mouth (caries risk).
- Panadol (p.r.n.): Analgesic/anti-pyretic; may alter perception of dental pain during diagnostics.
Allergies
- Penicillin: Anaphylactic reaction. Penicillin is contraindicated; use alternatives like Clindamycin.
Social Habits
- Tobacco: Never smoker.
- Alcohol: Current drinker (1-2 standard drinks per month). Increases risk of oral cavity cancer.
 |  |
 |
Dental History and Attitude8
- History:
- Attended government clinics (2016) and free dental days (2017) for extractions, fillings, and cleans.
- History of extractions due to decay; never worn dentures.
- Long waitlists previously prevented regular care.
- Attitude:
- Functionally motivated; understands the link between oral and overall health.
- Highly motivated and compliant; perfect attendance record.
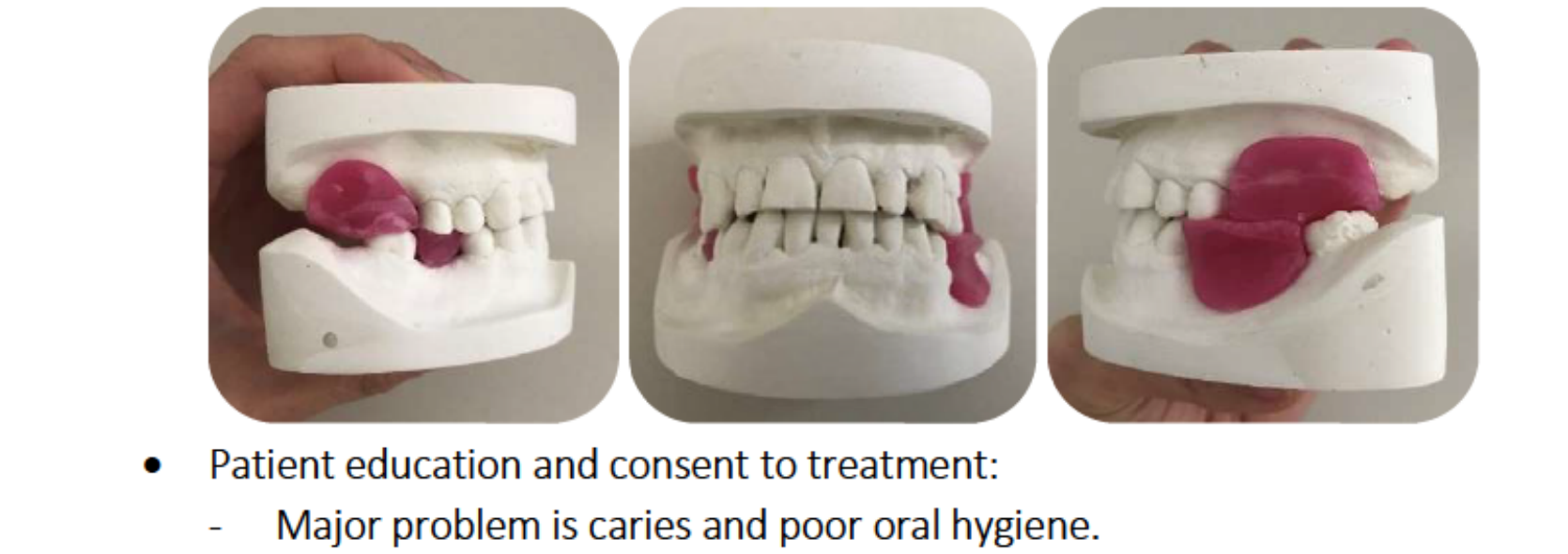
Oral Hygiene
- Status: Poor.
- Routine: Brushes 2-3 times daily (manual brush, fluoride toothpaste); occasional floss picks; daily salt-water rinses.
Social History
- Born in Melbourne, raised in Israel.
- Former Ultra-Orthodox Jewish Rabbi and UN Human Rights Commission worker; suffered physical/psychological injuries.
- Retired in Perth, living alone on a disability pension; active volunteer.
Examination And Diagnostics
Extra-oral Examination Findings9
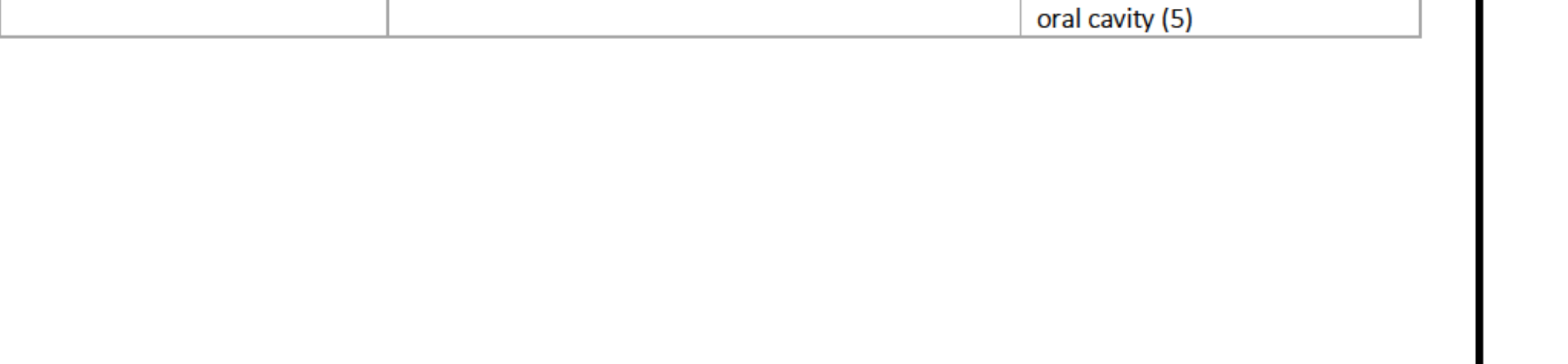
- Facial Symmetry/Skin: Symmetrical; skin, lips, and commissures are intact and healthy.
- TMJ: Bilateral clicking on closing and lateral excursion to the right; no pain or tenderness.
- Lymph Nodes/Muscles: No lymphadenopathy; muscles of mastication are non-tender.
- Thyroid: No abnormal enlargement.
Dentofacial Analysis
- Proportions: Proportional facial thirds and fifths.
- Symmetry: Parallel interpupillary/incisal lines. Mild facial asymmetry (mandible left of midline).
- Midlines: Facial and dental midlines coincide; however, mandibular dental midline is deviated 4-5 mm to the left.
- Smile Analysis: High smile line, average width, wide buccal corridors, flat occlusal curve.
- Profile: Indications of Class I skeletal relationship.
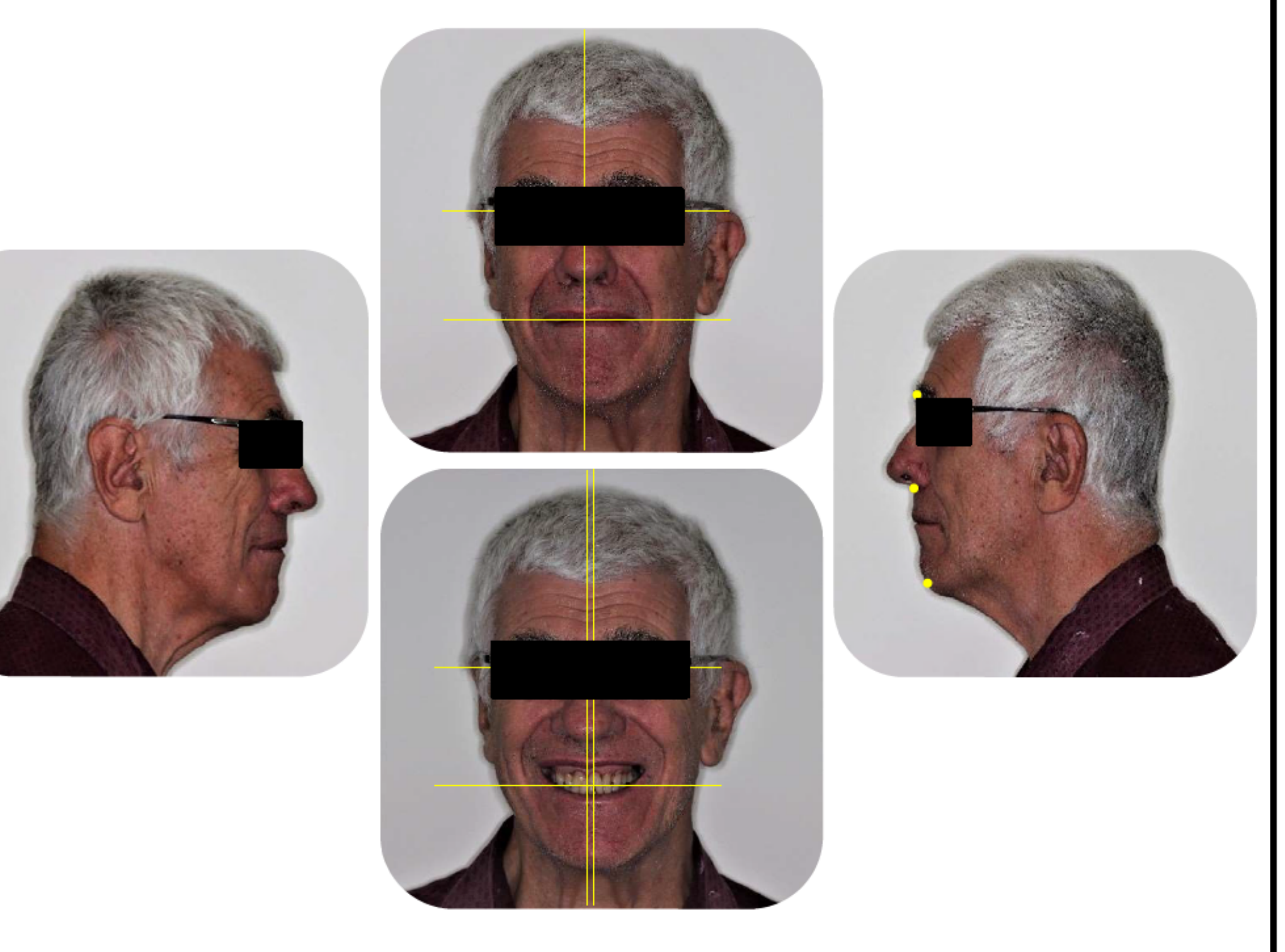
Intraoral Examination Findings10
- Mucosa/Sulci: Labial and buccal mucosa normal; adequate sulci depth.
- Frenal Attachments: Normal maxillary (labial/buccal) and mandibular (labial/lingual) attachments.
- Palate: Prominent rugae on hard palate; soft palate normal.
- Gingivae:
- Thick scalloped phenotype.
- Generalised inflammation.
- Generalised recession and blunted papillae.
- Tongue: Fissuring and plaque accumulation on the dorsum.
- Floor of Mouth: Nil abnormalities detected.
 |  |
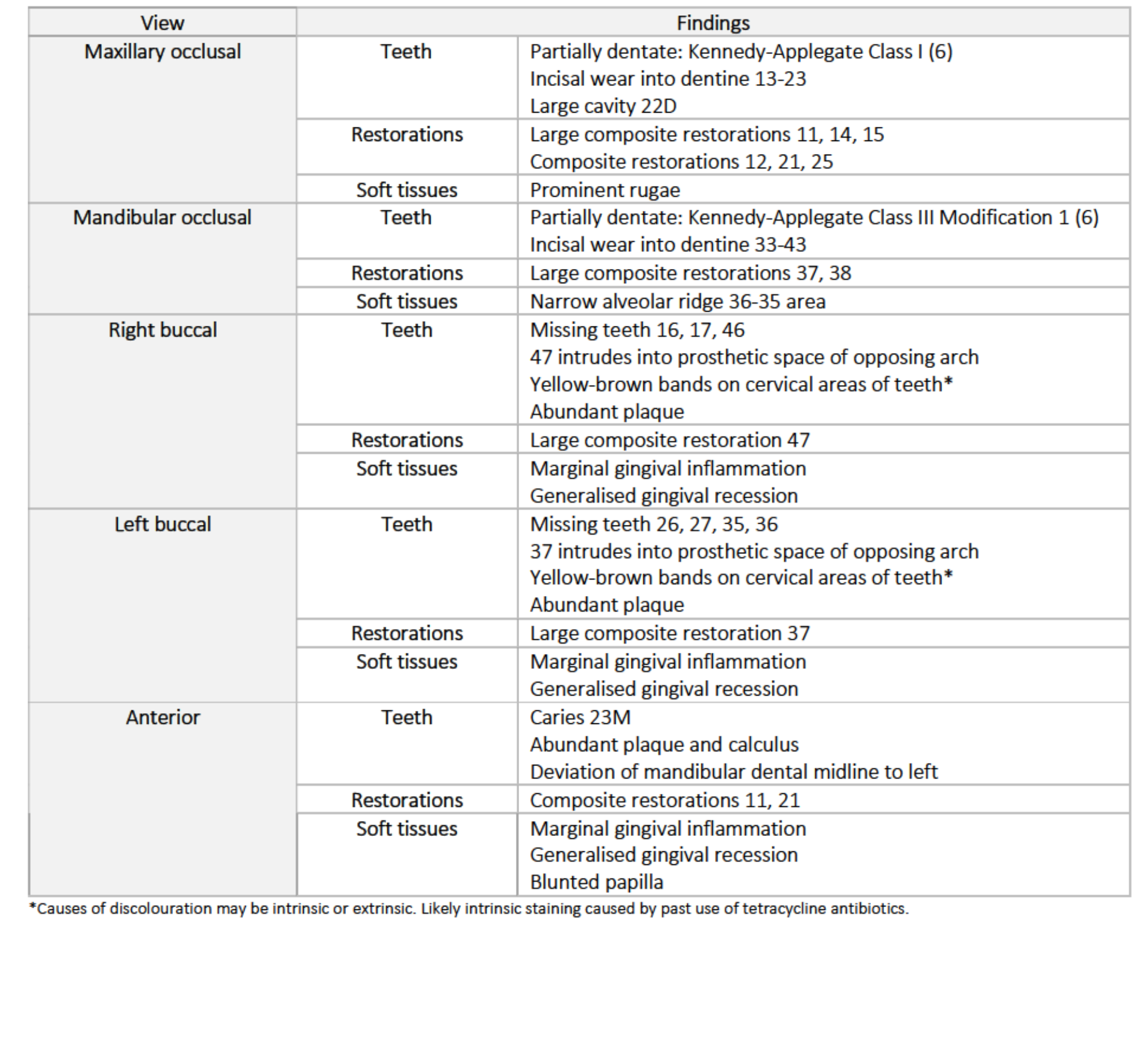
Intraoral Findings by View11
Maxillary Occlusal
- Teeth: Partially dentate (Kennedy-Applegate Class I); incisal wear into dentine (13-23); large cavity 22D.
- Restorations: Large composites (11, 14, 15); composites (12, 21, 25).
Mandibular Occlusal
- Teeth: Partially dentate (Kennedy-Applegate Class III Mod 1); incisal wear into dentine (33-43).
- Restorations: Large composites (37, 38).
- Soft Tissues: Narrow alveolar ridge in 36-35 area.
Right/Left Buccal
- Missing Teeth: 16, 17, 46 (Right); 26, 27, 35, 36 (Left).
- Occlusion: 47 and 37 intrude into opposing prosthetic spaces.
- Observations: Yellow-brown cervical bands (likely intrinsic tetracycline staining); abundant plaque; marginal gingival inflammation; generalised recession.
Anterior
- Teeth: Caries 23M; abundant plaque/calculus; mandibular midline deviation to the left.
- Soft Tissues: Blunted papillae and inflammation.
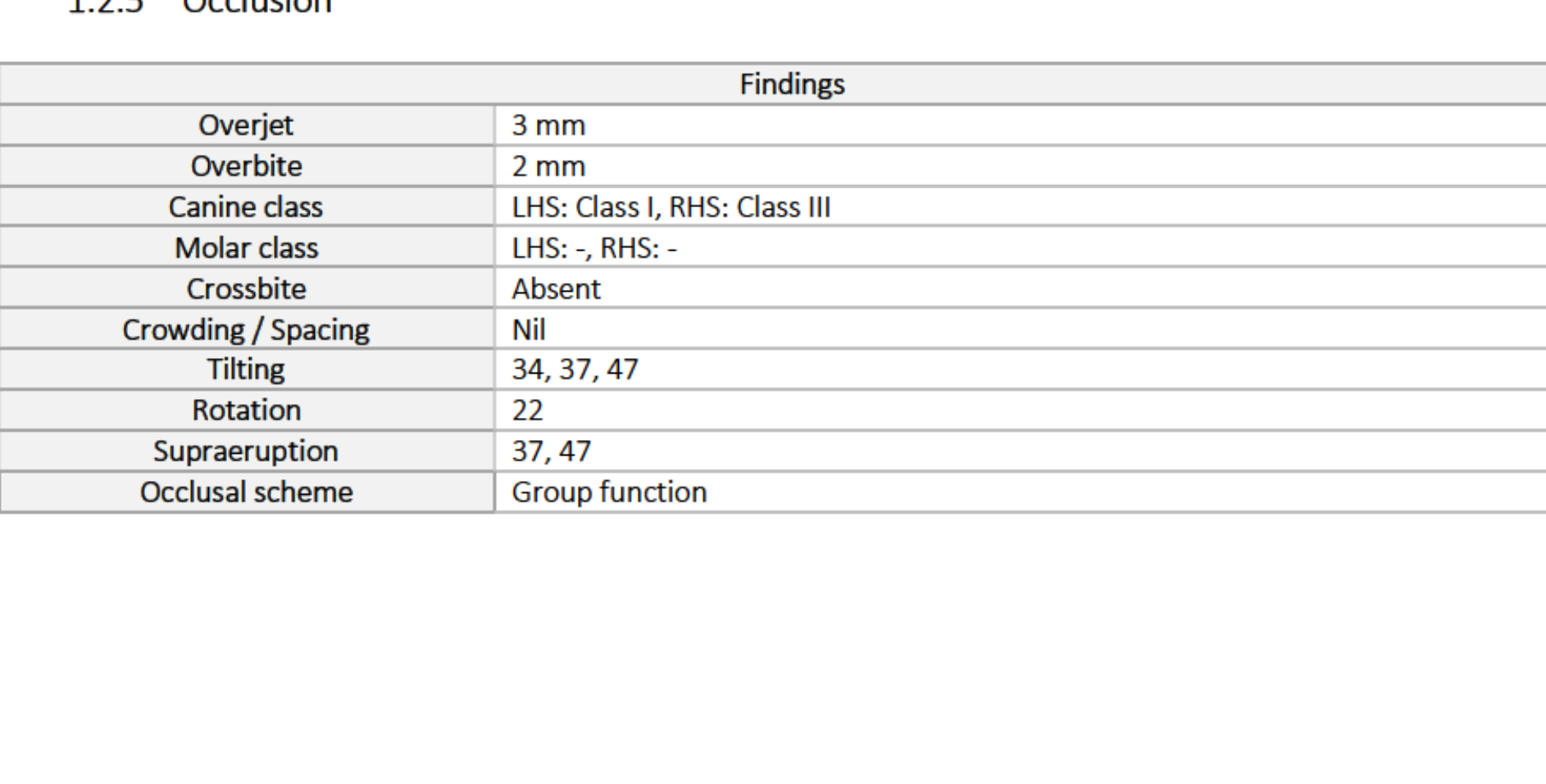
Occlusal Analysis12
- Overjet: 3 mm
- Overbite: 2 mm
- Canine Class: LHS Class I; RHS Class III
- Molar Class: Not applicable (missing teeth)
- Alignment: Tilting (34, 37, 47); Rotation (22); Supraeruption (37, 47).
- Occlusal Scheme: Group function.
- Other: Crossbite, crowding, and spacing are absent.
 |  |
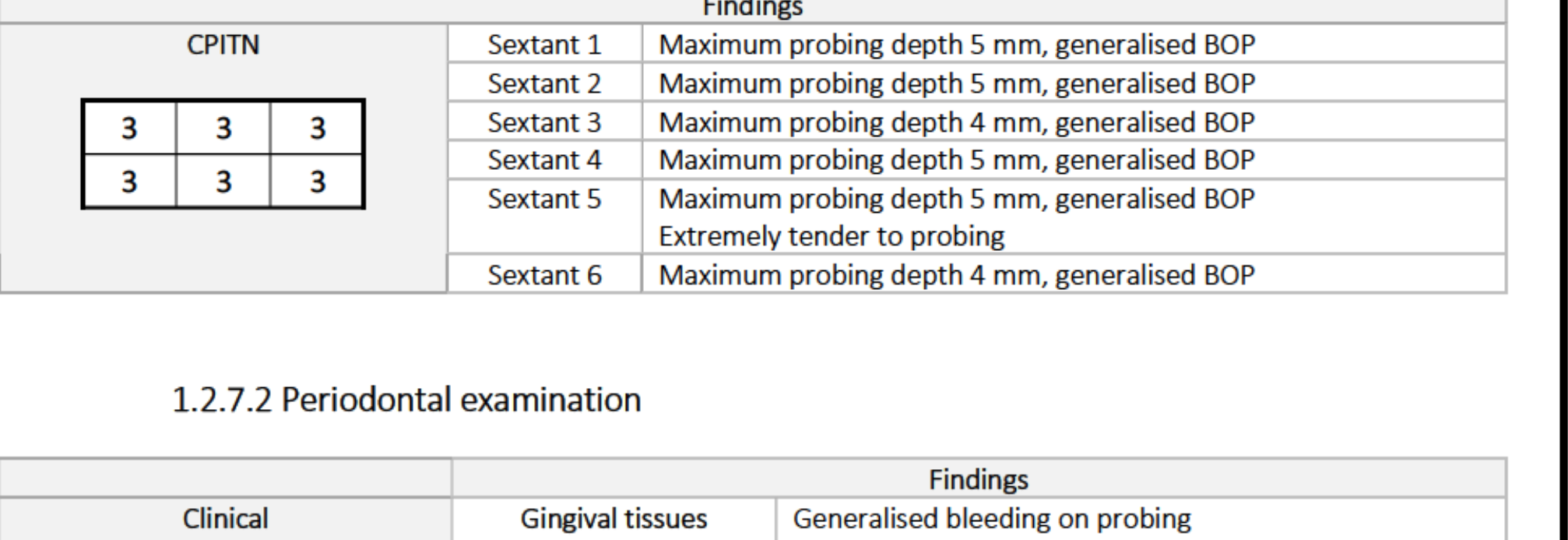
Periodontal Assessment13
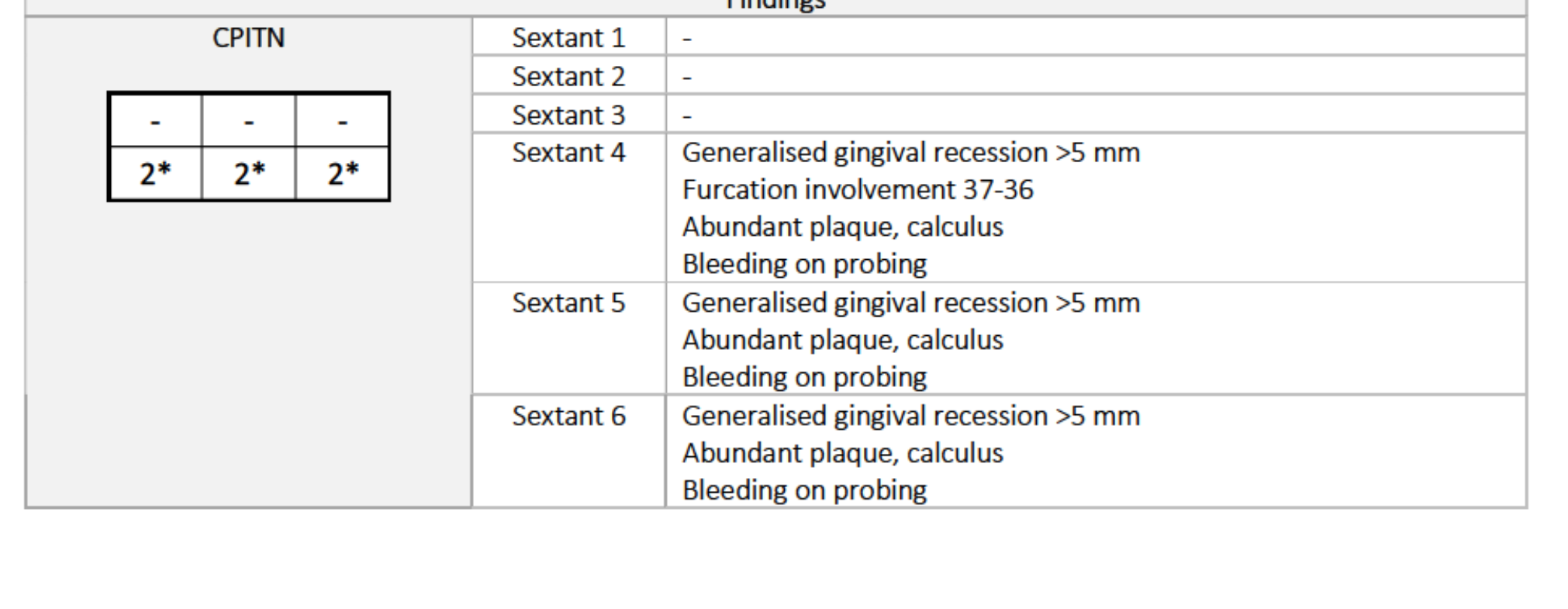
CPITN Scores
- Sextants 1, 2, 4, 5: Score 3 (Max probing depth 5mm, generalised BOP).
- Sextants 3, 6: Score 3 (Max probing depth 4mm, generalised BOP).
- Note: Sextant 5 was extremely tender to probing.
Clinical Findings
- Gingiva: Oedematous, pink/red marginal inflammation, thick biotype, generalised recession.
- Plaque/Calculus: 43% plaque score; abundant interproximal plaque; generalised supragingival and subgingival calculus (heavy on lower lingual anterior).
- Plaque-Retentive Factors: Overhangs (11), rotation (22), tilting (34, 37).
- Halitosis: Present.
Radiographic Findings
- Bone Levels: Generalised mild horizontal bone loss in both arches.
 |  |
 |
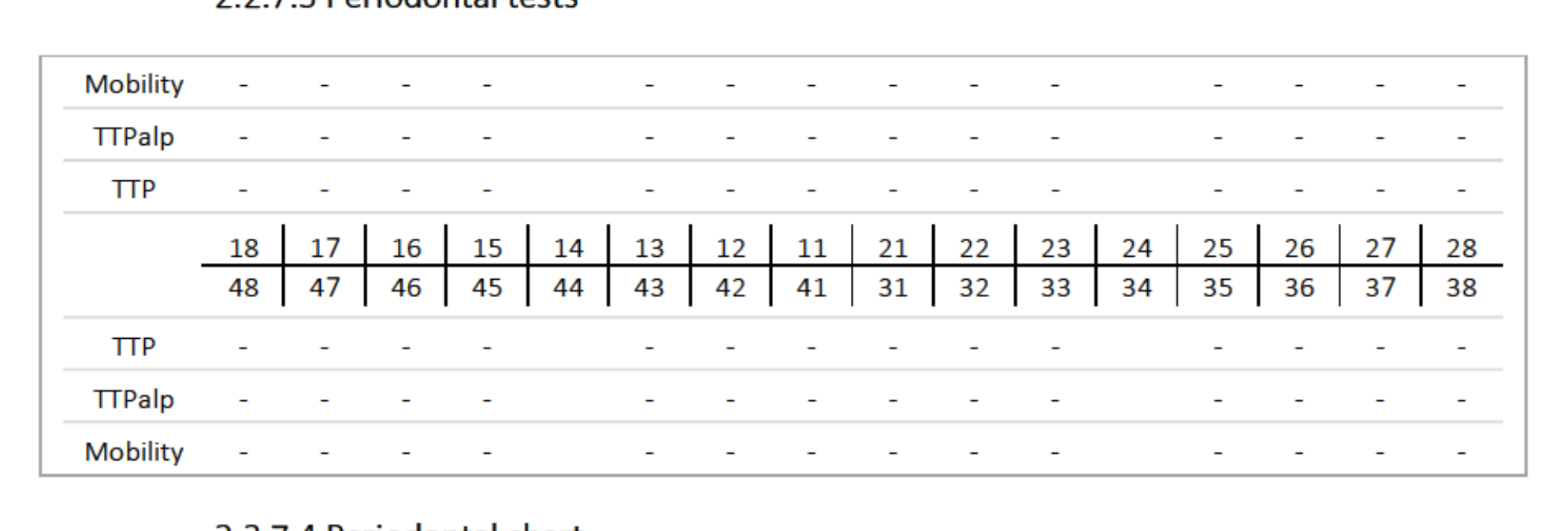
Periodontal and Pulp Testing14
Periodontal Tests
- TTP (Tenderness to Percussion): Positive (++) on 47; strongly positive (+++) on 37.
- Mobility: Grade I (GI) noted on teeth 31, 32, and 37.
- TTPalp (Tenderness to Palpation): Negative across all tested teeth.
Clinical Rationale
- CPITN results necessitated a full periodontal chart.
- Baseline data required to evaluate periodontal treatment success and suitability for removable prostheses.
 |  |
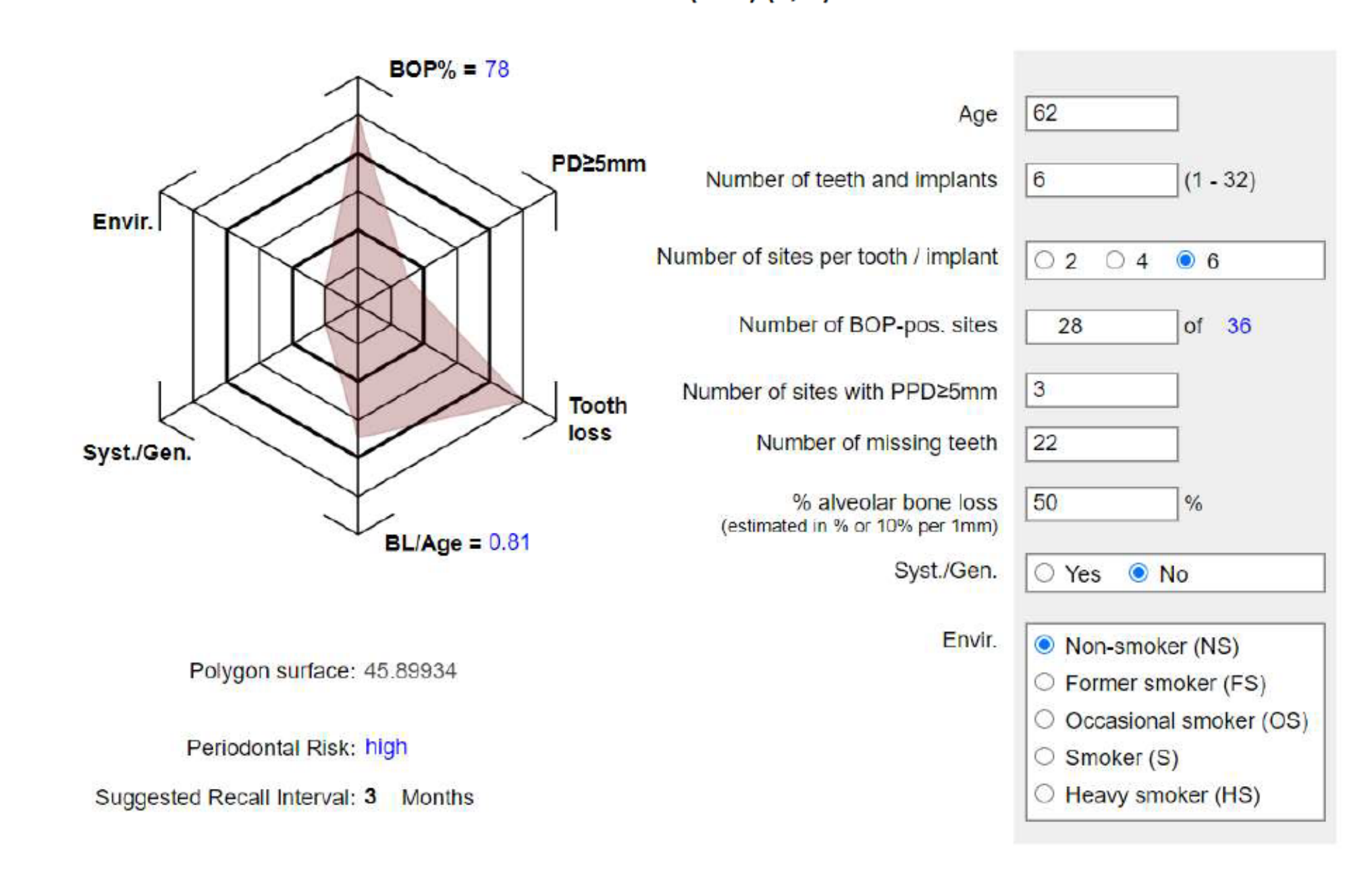
Periodontal Risk Assessment (PRA)15
- Patient Data: Age 64; 21 teeth present.
- BOP: 57% (72 of 126 sites).
- Probing Depths: 7 sites with PPD ≥ 5mm.
- Bone Loss: 25% alveolar bone loss (BL/Age = 0.39).
- Risk Level: Medium.
- Suggested Recall: 6 Months.
 | 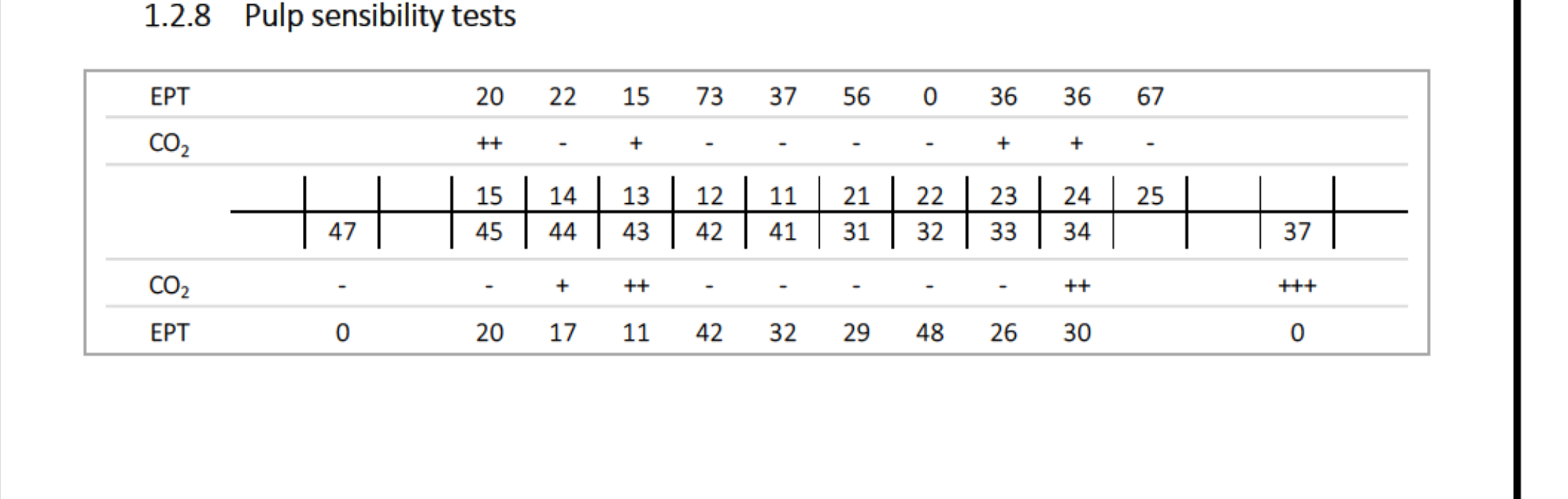 |
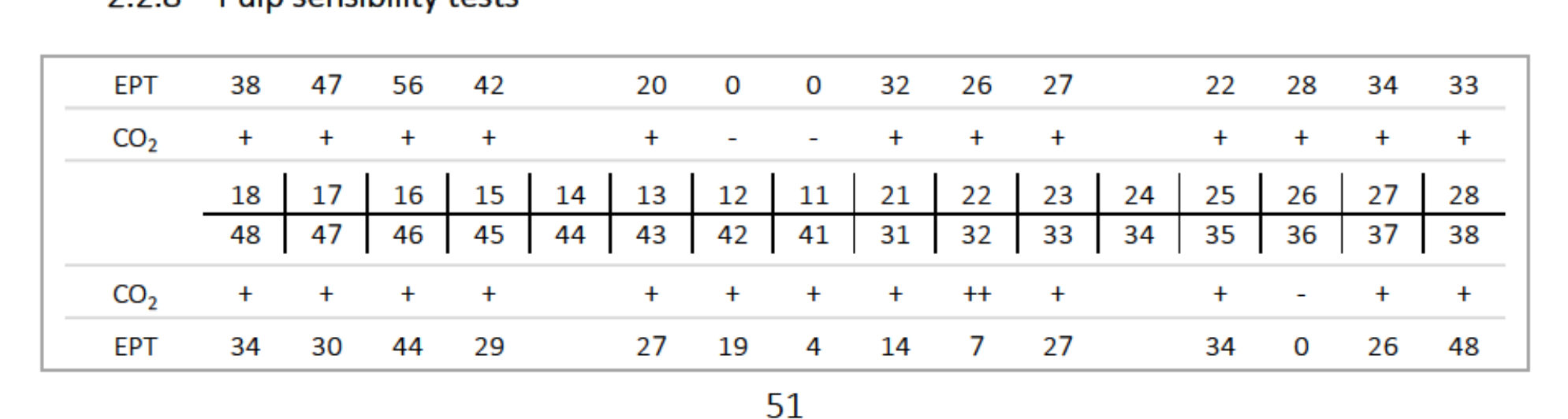
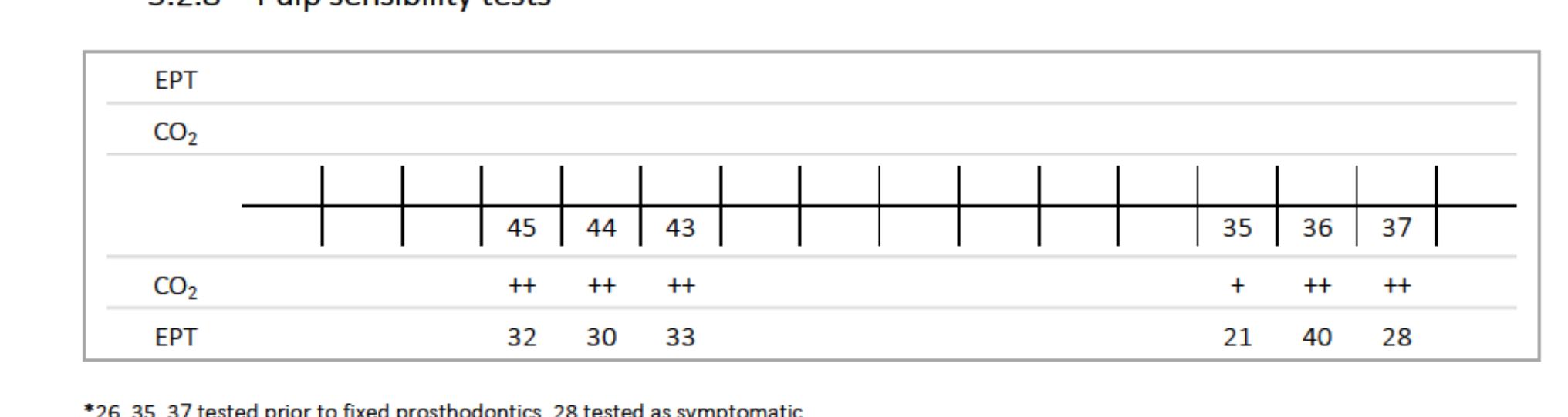
Pulp Sensibility Tests
| Tooth | EPT | CO2 | Clinical Status |
|---|---|---|---|
| 15 | 15 | + | Vital |
| 14 | 73 | ++ | Vital |
| 13 | 37 | ++ | Vital |
| 11 | 0 | - | Non-responsive |
| 21 | 36 | - | Non-responsive |
| 22 | 36 | - | Non-responsive |
| 23 | 67 | - | Non-responsive |
| 37 | 0 | + | Responsive |
| 47 | 0 | - | Non-responsive |
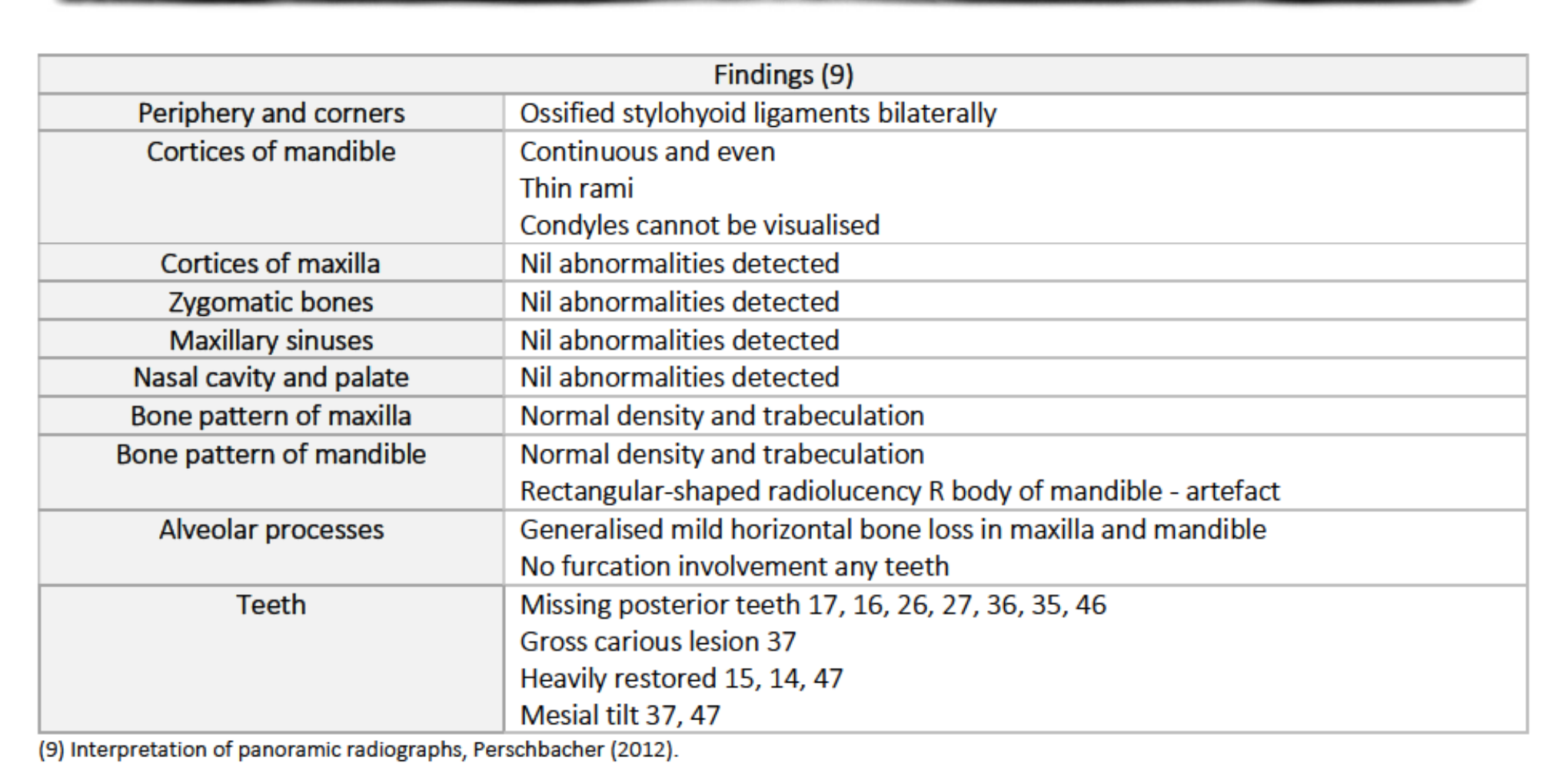
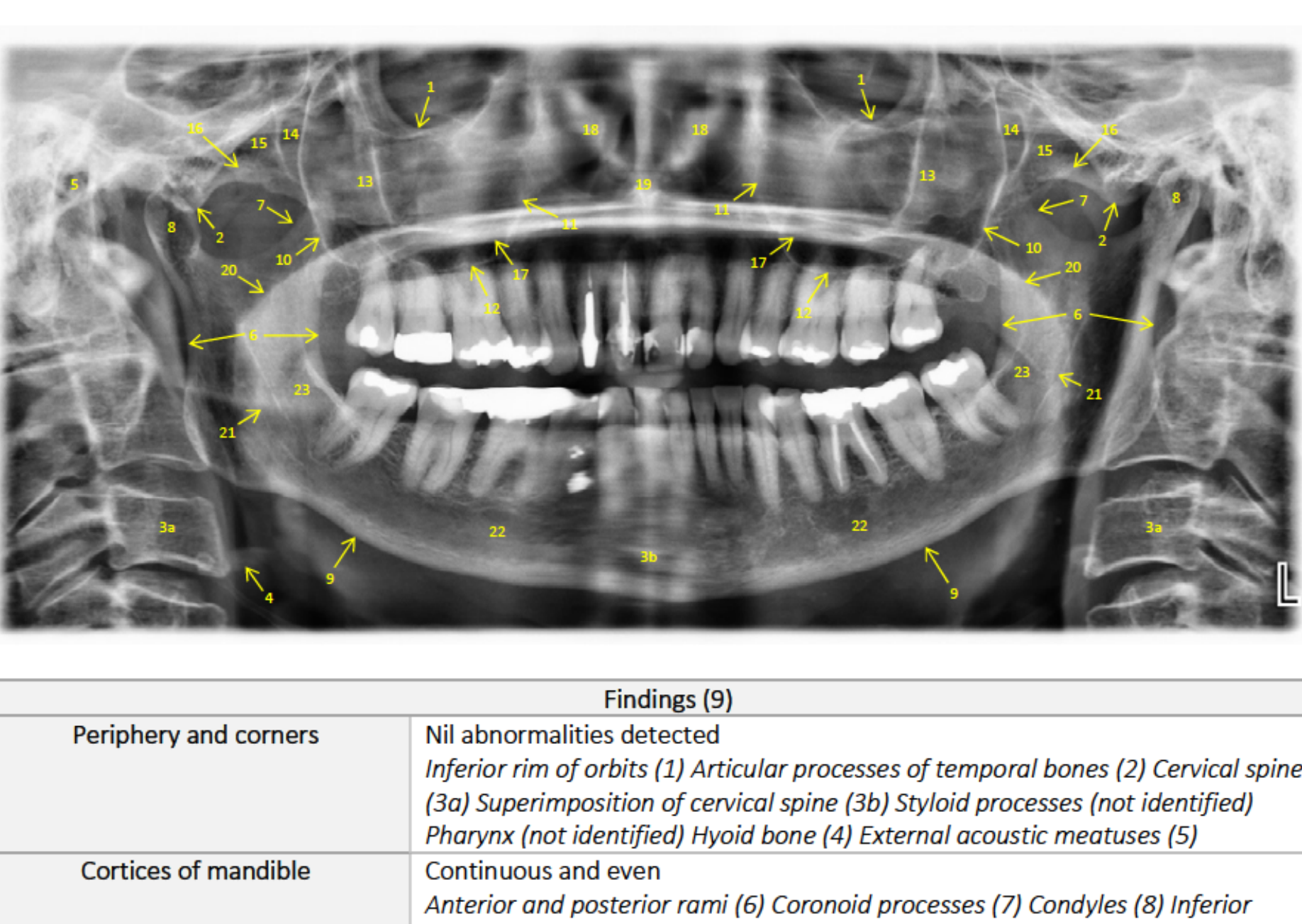
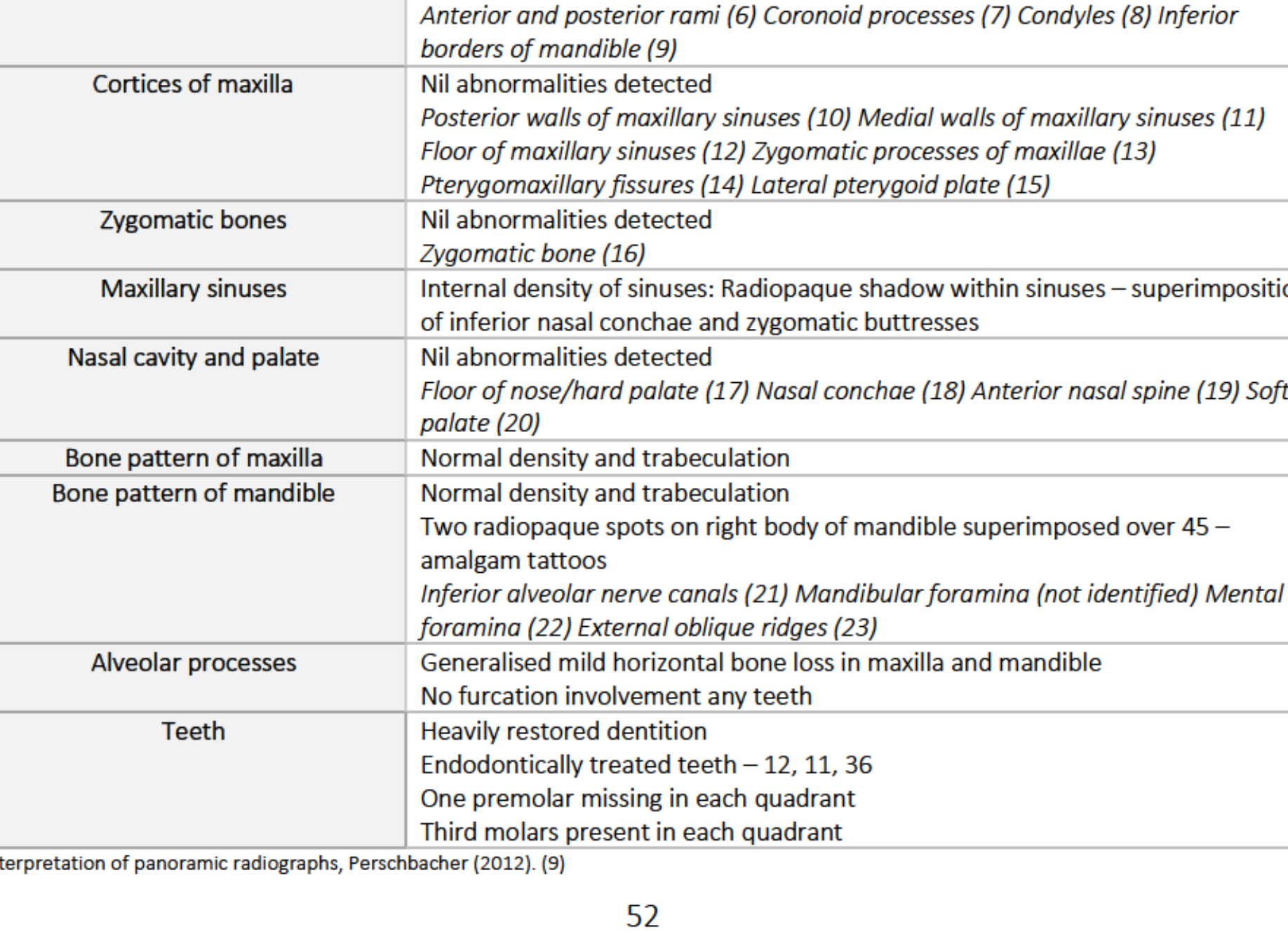
Radiographic Findings: Orthopantogram (OPG)16
- General Structures: Ossified stylohyoid ligaments; thin mandibular rami; normal maxillary sinus and nasal cavity.
- Bone Pattern: Normal density; generalised mild horizontal bone loss; no furcation involvement.
- Teeth Observations:
- Missing: 17, 16, 26, 27, 36, 35, 46.
- Gross caries: 37.
- Heavily restored: 15, 14, 47.
- Mesial tilt: 37, 47.
- Artefact: Rectangular radiolucency in right body of mandible.
 |  |
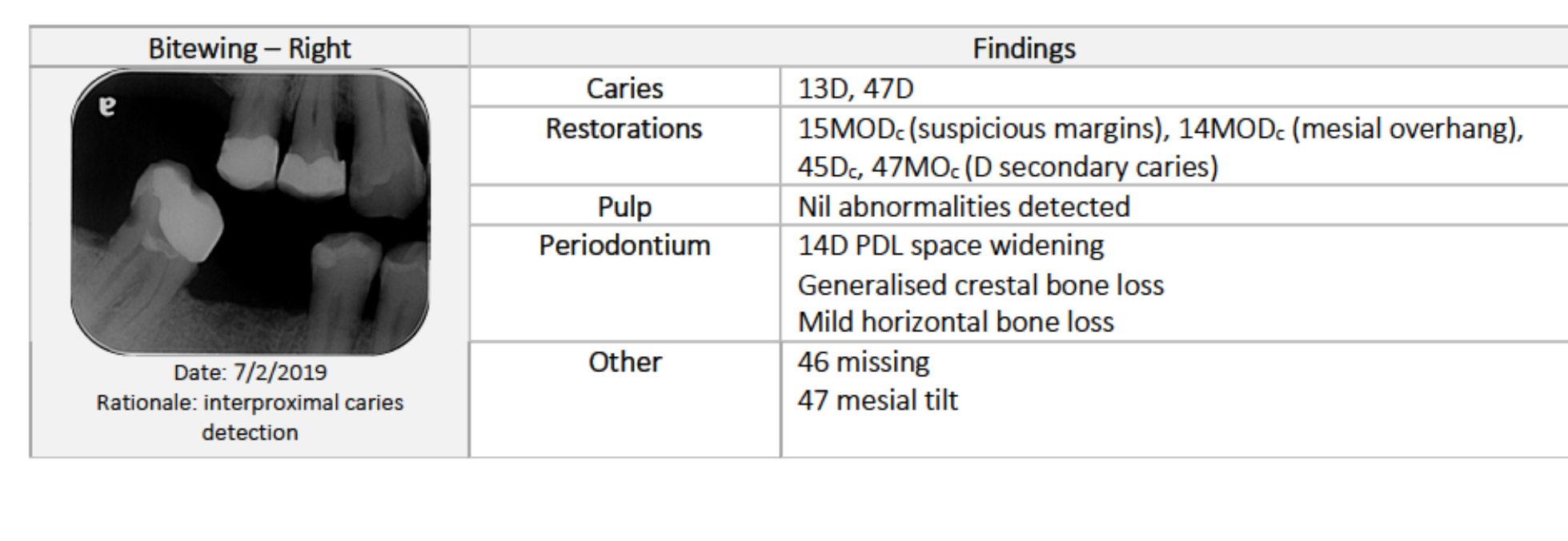
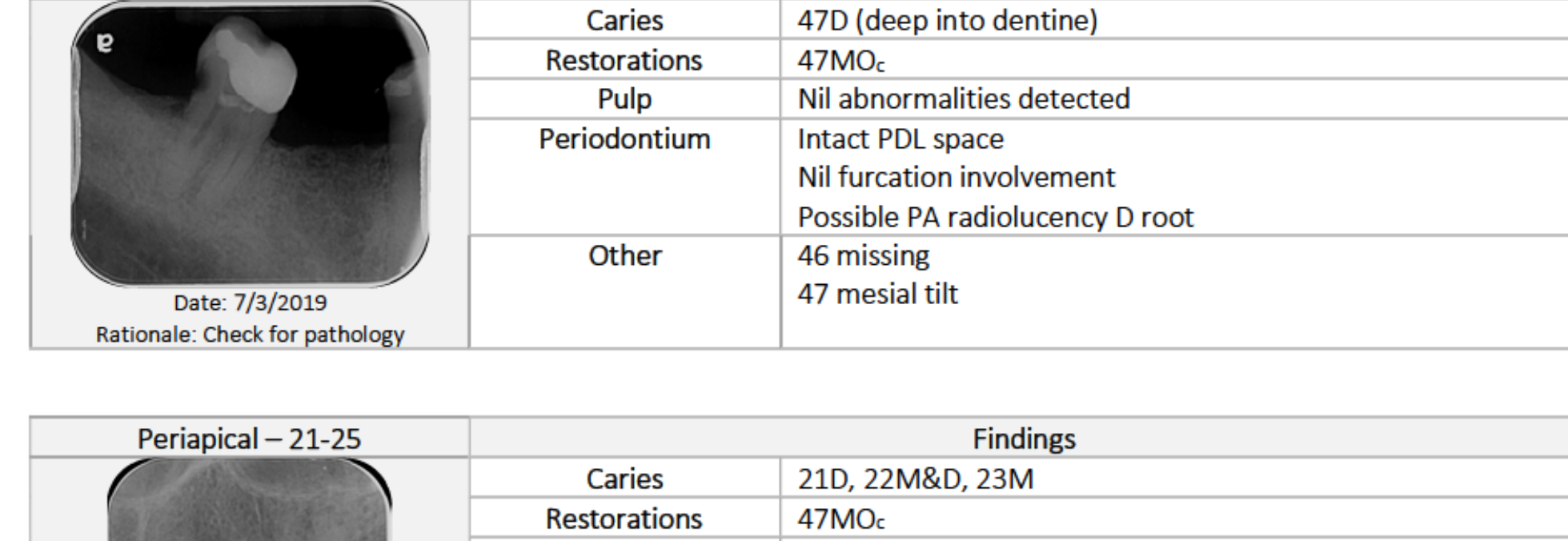
Radiographic Findings: Bitewings and Periapicals17
Bitewing - Right
- Caries: 13D, 47D, 47 secondary caries.
- Restorations: 15MODc (suspicious margins), 14MODc (overhang), 45Dc, 47MOc.
- Periodontium: 14D PDL widening; mild horizontal bone loss.
Periapical - 47
- Caries: Deep 47D into dentine.
- Periodontium: Possible periapical radiolucency at distal root; intact PDL space elsewhere.
- Other: 47 mesial tilt.
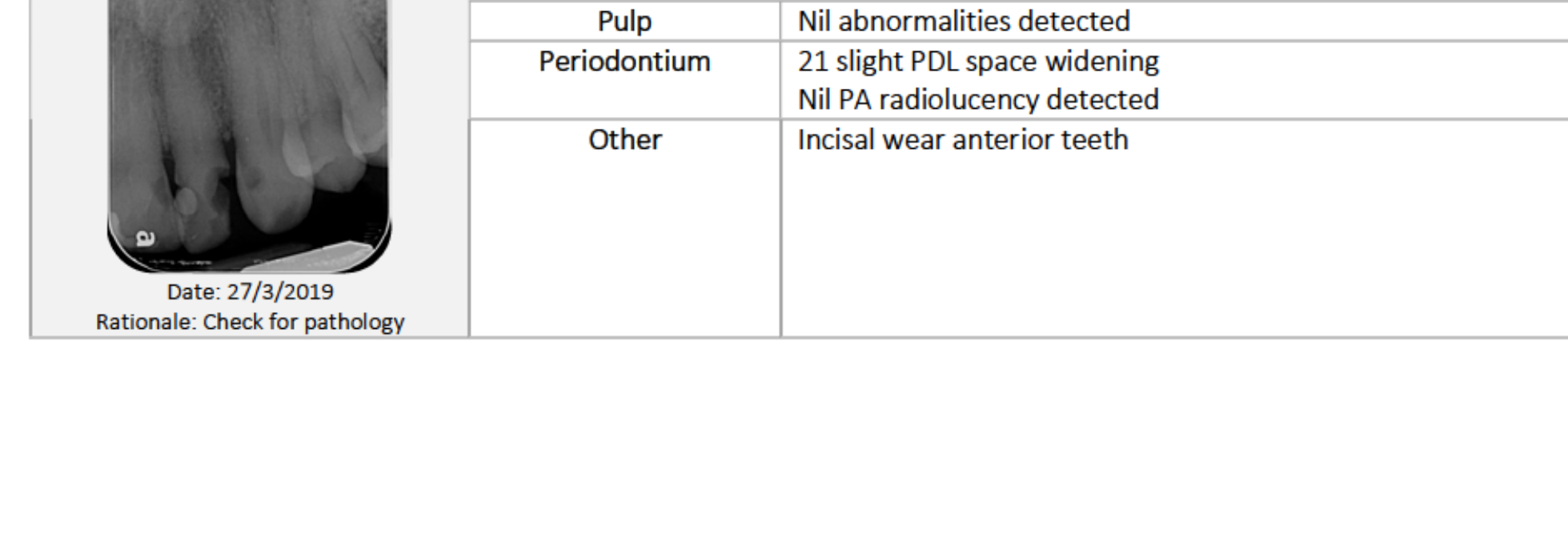
Periapical - 21-25
- Caries: 21D, 22M&D, 23M.
- Periodontium: 21 slight PDL space widening; no PA radiolucency detected.
- Other: Incisal wear on anterior teeth.
 |  |
 |
Caries Risk Assessment18
Dietary Factors
- High sugar/fermentable carbohydrate intake.
- Coffee with sugar (4-6x daily), fruit juice, bread, pasta, cakes, and ice cream.
- Frequent snacking (2-3x daily).
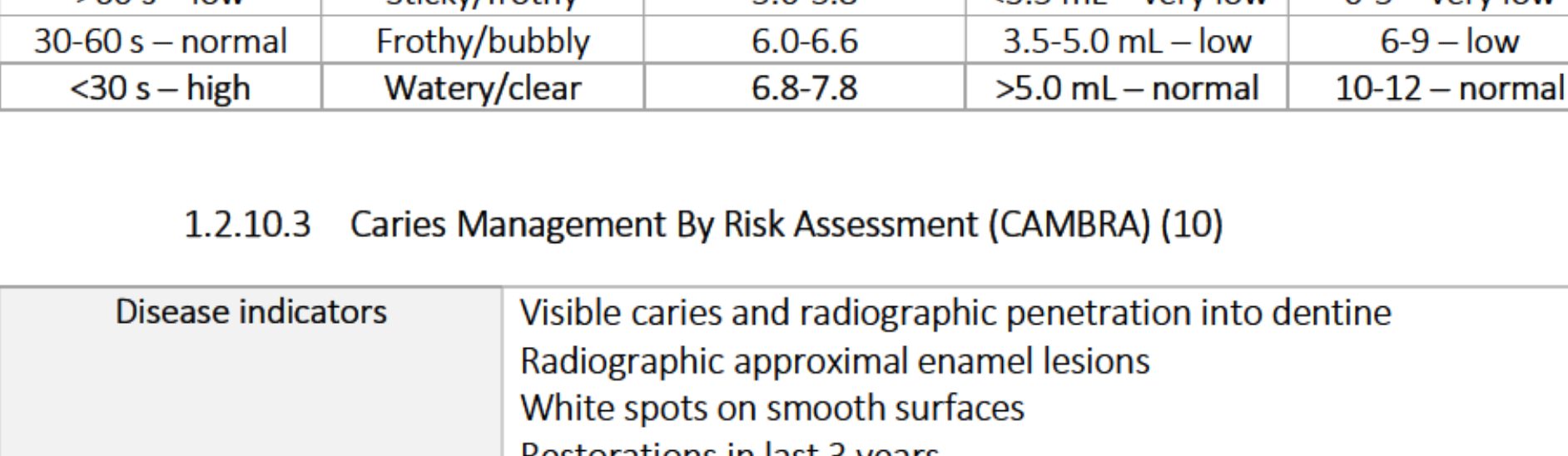
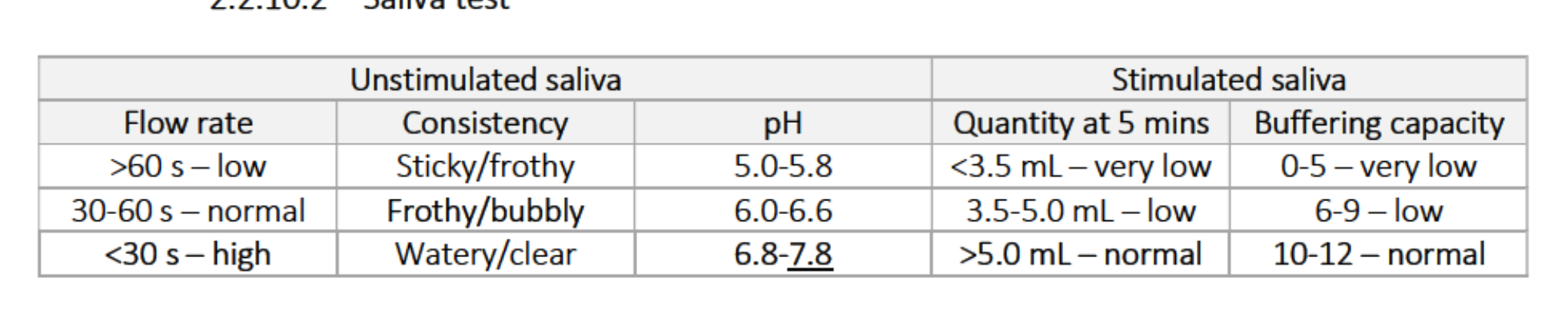
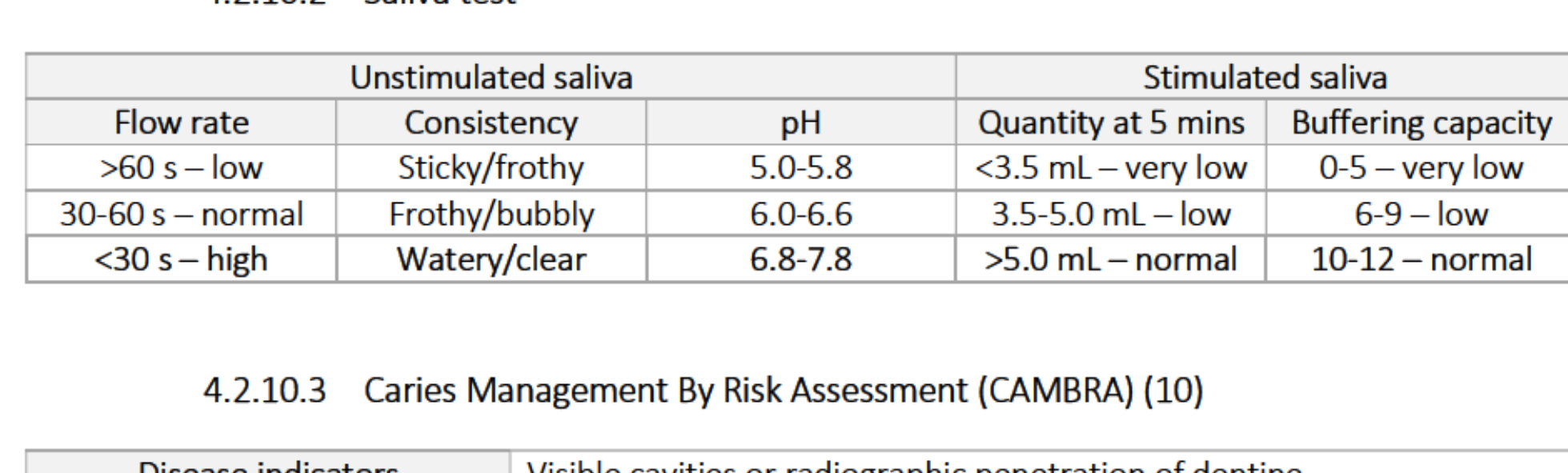
Saliva Testing
- Unstimulated: Low flow rate (<60s); sticky/frothy consistency; pH 5.0-5.8.
- Stimulated: Very low quantity (<3.5 mL at 5 mins); low buffering capacity.
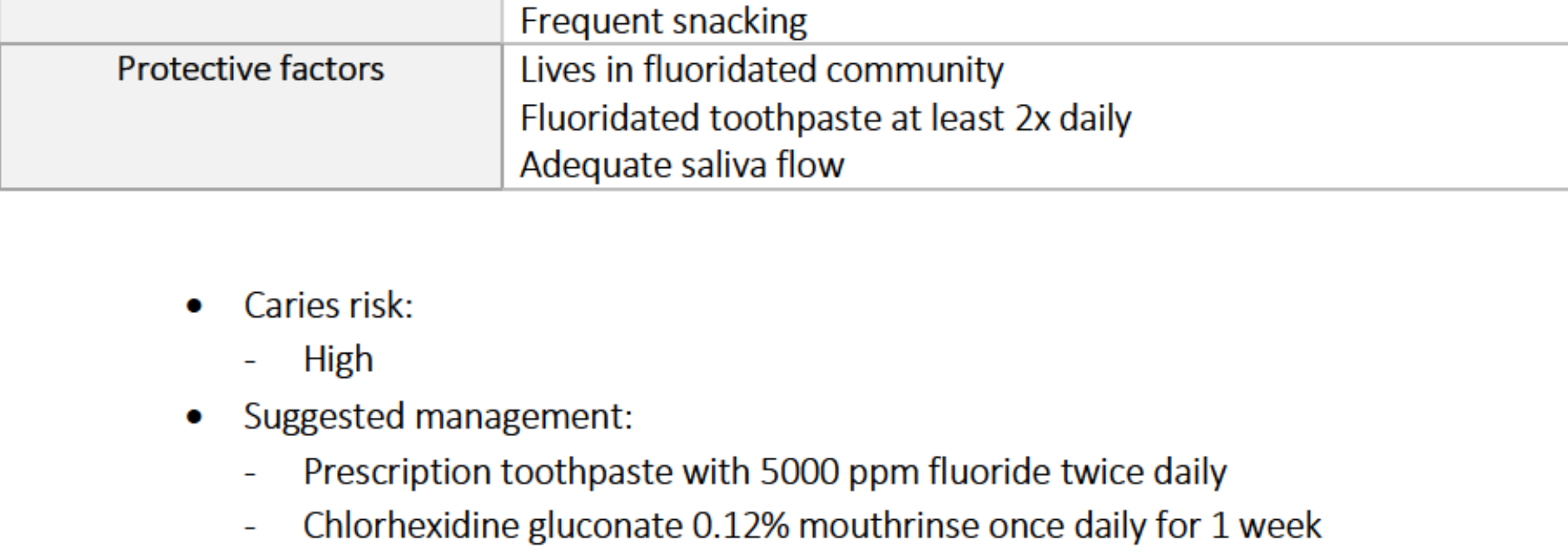
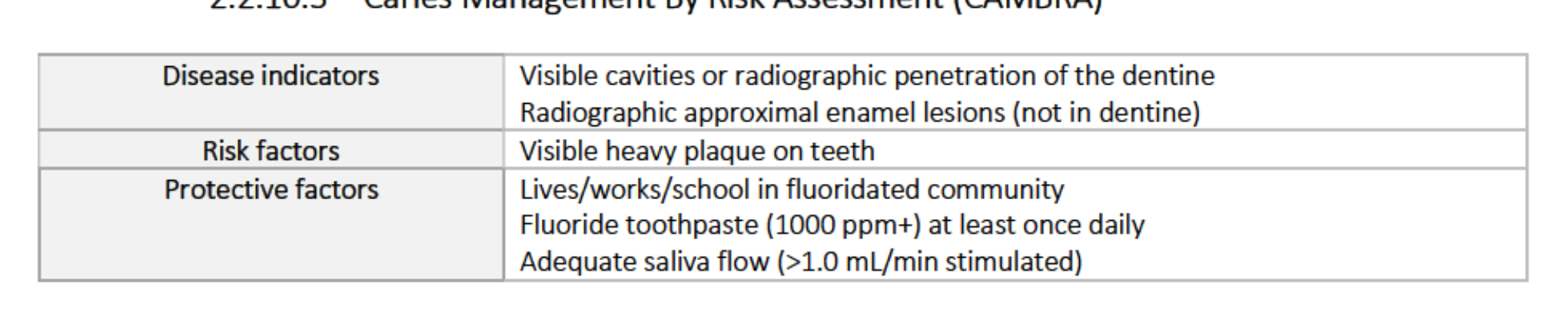
CAMBRA Summary
- Risk Level: High.
- Indicators: Visible caries, dentine penetration, heavy plaque, frequent snacking, and low salivary flow.
- Management: 5000 ppm fluoride toothpaste, Chlorhexidine rinse (1 week/month), Xylitol gum, fluoride varnish, and 3-month recall.
 |  |
Diagnoses And Problem List
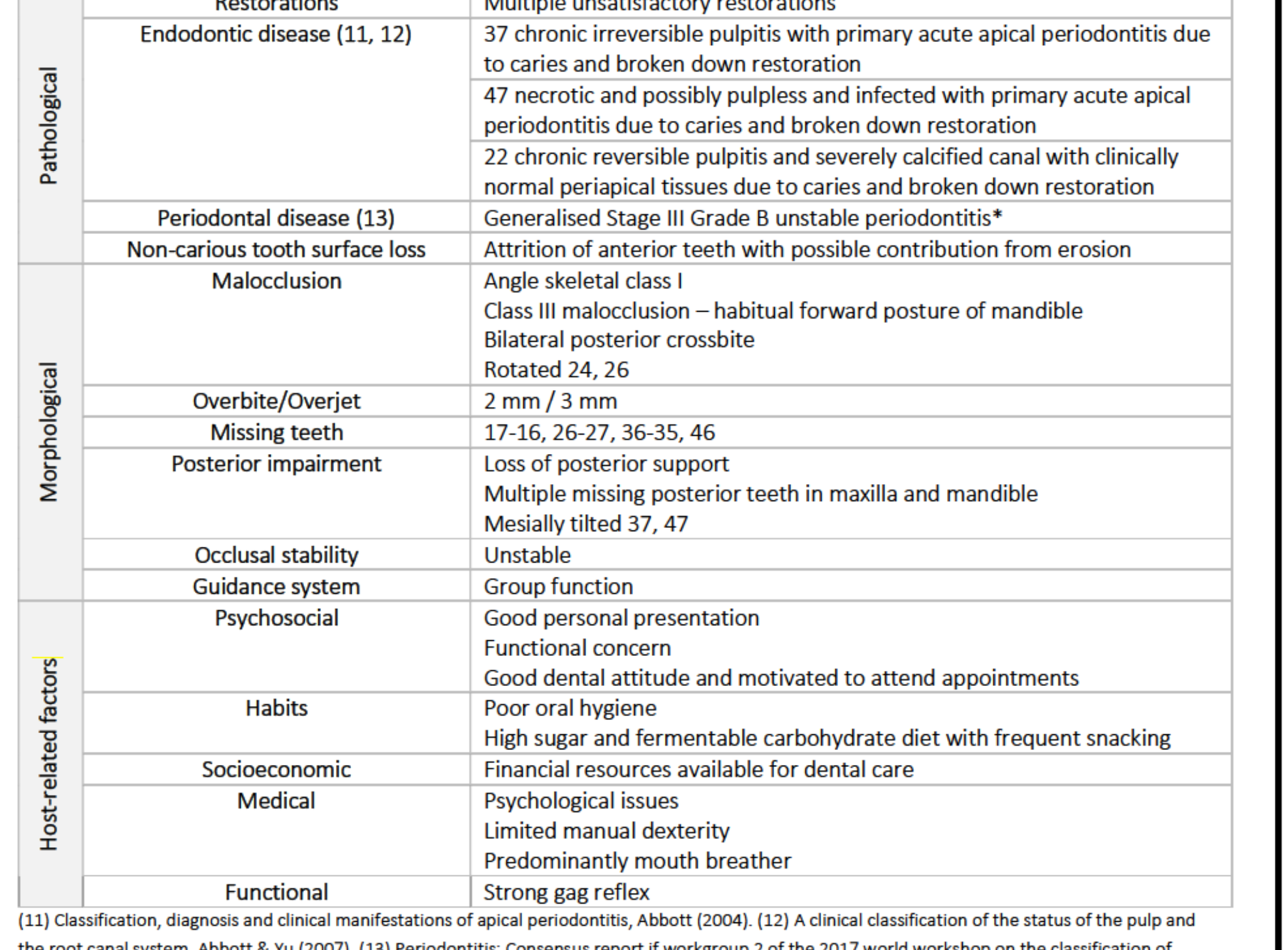
Diagnoses19
- Pathological:
- Multiple active caries and unsatisfactory restorations.
- Endodontic: 37 Chronic irreversible pulpitis; 47 Necrotic/infected; 22 Chronic reversible pulpitis (calcified).
- Periodontal: Generalised Stage III Grade B unstable periodontitis.
- TSL: Attrition and erosion of anterior teeth.
- Morphological:
- Angle Class I skeletal; Class III habitual posture.
- Bilateral posterior crossbite; multiple missing posterior teeth; unstable occlusion.
- Host Factors: Poor hygiene, high sugar diet, limited manual dexterity, mouth breathing, and strong gag reflex.
 |  |
Problem List
- Pulpal pathology (37, 47, 22).
- Extensive caries (multiple sites including 13, 12, 21, 22, 23, 24, 25, 37, 34, 42, 43, 47).
- Unsatisfactory restorations (15, 14, 12, 11, 22, 37, 45, 47).
- Lack of posterior support and occlusal instability.
Prognosis
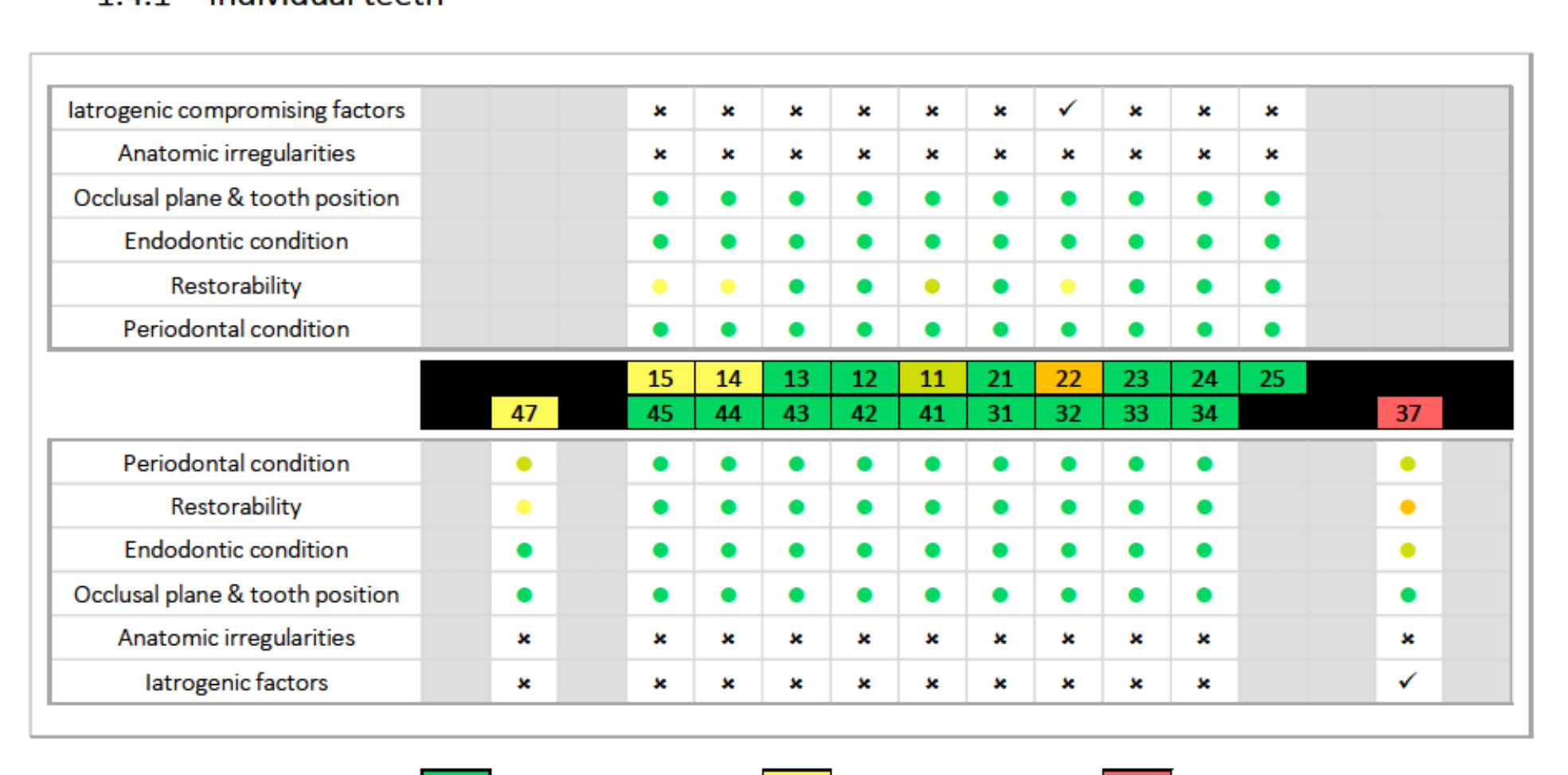
Individual Tooth Prognosis20
Prognosis Classification
- Good: 11, 12, 13, 21, 23, 24, 25, 31, 32, 33, 34, 41, 42, 43, 44, 45.
- Fair/Guarded: 14, 15, 47.
- Poor: 22 (minimal tooth structure, iatrogenic factors).
- Hopeless: 37 (gross destruction, unrestorable).
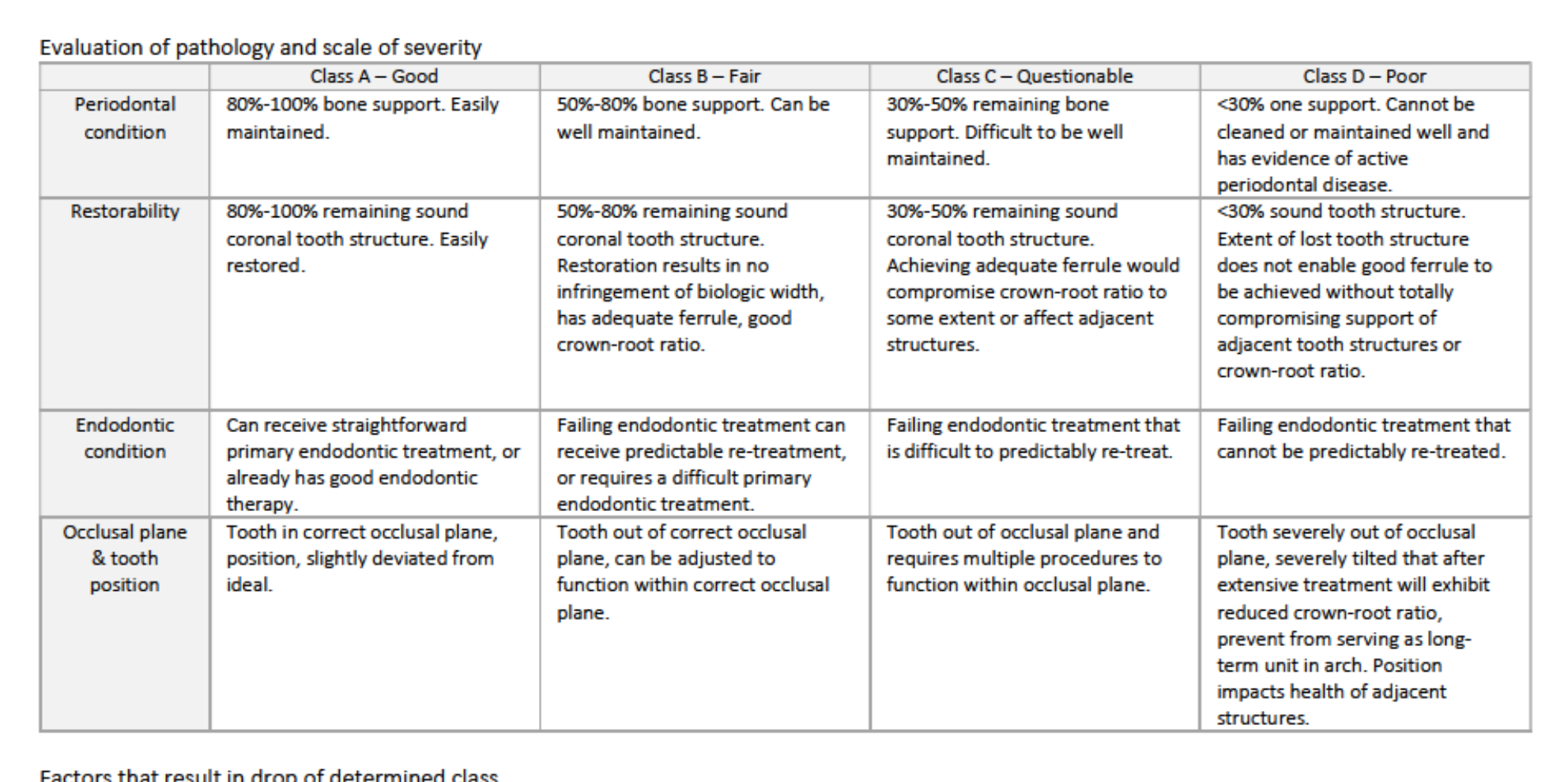
Evaluation Criteria
- Periodontal: Based on bone support (80-100% for Good).
- Restorability: Based on remaining sound coronal structure and ferrule.
- Endodontic: Based on predictability of primary or re-treatment.
- Occlusal: Based on tooth position and plane alignment.
 |  |
 |
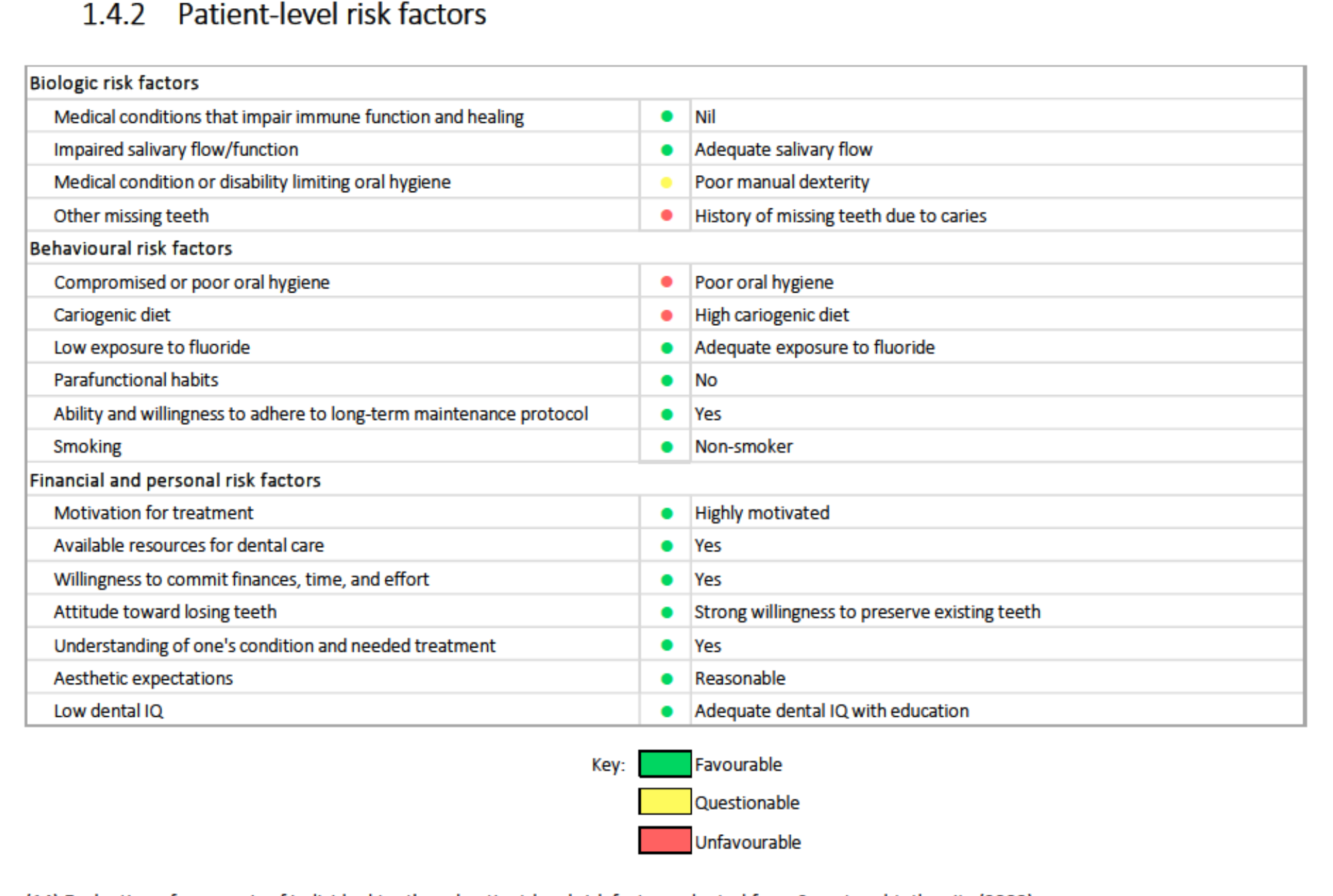
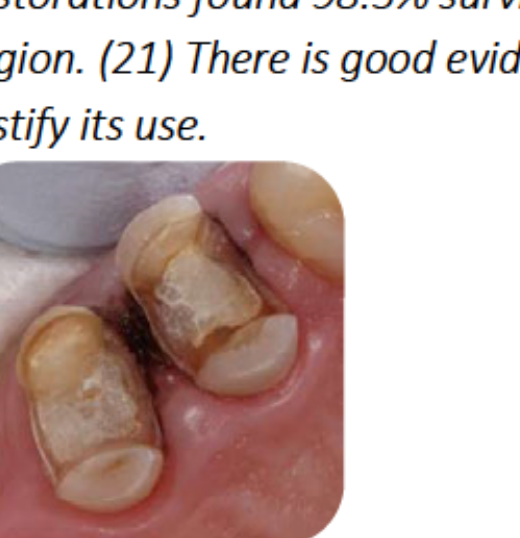
Patient-Level Risk Factors21
- Favourable: High motivation, available resources, willingness to commit to treatment, reasonable aesthetic expectations.
- Questionable: Poor manual dexterity, history of caries-related tooth loss.
- Unfavourable: Poor oral hygiene, high cariogenic diet.
 |  |
Overall Prognosis Summary
- Current Status: Guarded for 14, 15, 47; Poor for 22; Hopeless for 37.
- Risk of No Treatment: Progression of caries and pulpal/periodontal disease, leading to total edentulism and reduced quality of life.
- Mitigating Factors: Patient is highly compliant and open to education, which improves the long-term outlook if dietary and hygiene habits are modified.
Treatment Options
Pulpal and Carious Pathology
Tooth 37
- Option: Extraction.
- Rationale: Hopeless prognosis; addresses pain and infection with minimal commitment.
Tooth 47
- Option: Endodontic treatment followed by restoration.
- Rationale: High strategic value; patient wishes to save the tooth despite difficult access and questionable longevity.
Tooth 22
- Option: Endodontic treatment, post/core, and crown.
- Rationale: Patient wishes to save the anterior tooth; extraction would cause aesthetic concerns in a visible region.
Caries (Multiple Teeth)
- Option: Direct restorations.
- Rationale: Prevent further breakdown and pulpal involvement; aligns with patient’s goal to keep natural teeth.
Restorations, Periodontics, and Maxillary Edentulism
Unsatisfactory Restorations (14, 15)
- Option: Remove caries/old restorations and restore (Onlays).
- Rationale: Maximise longevity of teeth intended as denture abutments.
Periodontal Disease (Stage III Grade B)
- Option: Non-surgical periodontal therapy and OHI.
- Rationale: Reduce disease progression and create a healthy environment for indirect prostheses.
Missing Maxillary Posterior Teeth (17-16, 26-27)
- Option: Cobalt-Chrome (Co-Cr) Partial Denture.
- Rationale: Addresses lack of posterior support and stability; patient desires occlusal rehabilitation.
Mandibular Edentulism
Missing Mandibular Posterior Teeth (37-36, 46)
- Option 1: No treatment (Shortened Dental Arch).
- Option 2: Co-Cr Partial Denture.
- Decision: Option 2.
- Rationale: Patient specifically requested dentures to improve function and stability. Success depends on long-term hygiene maintenance.
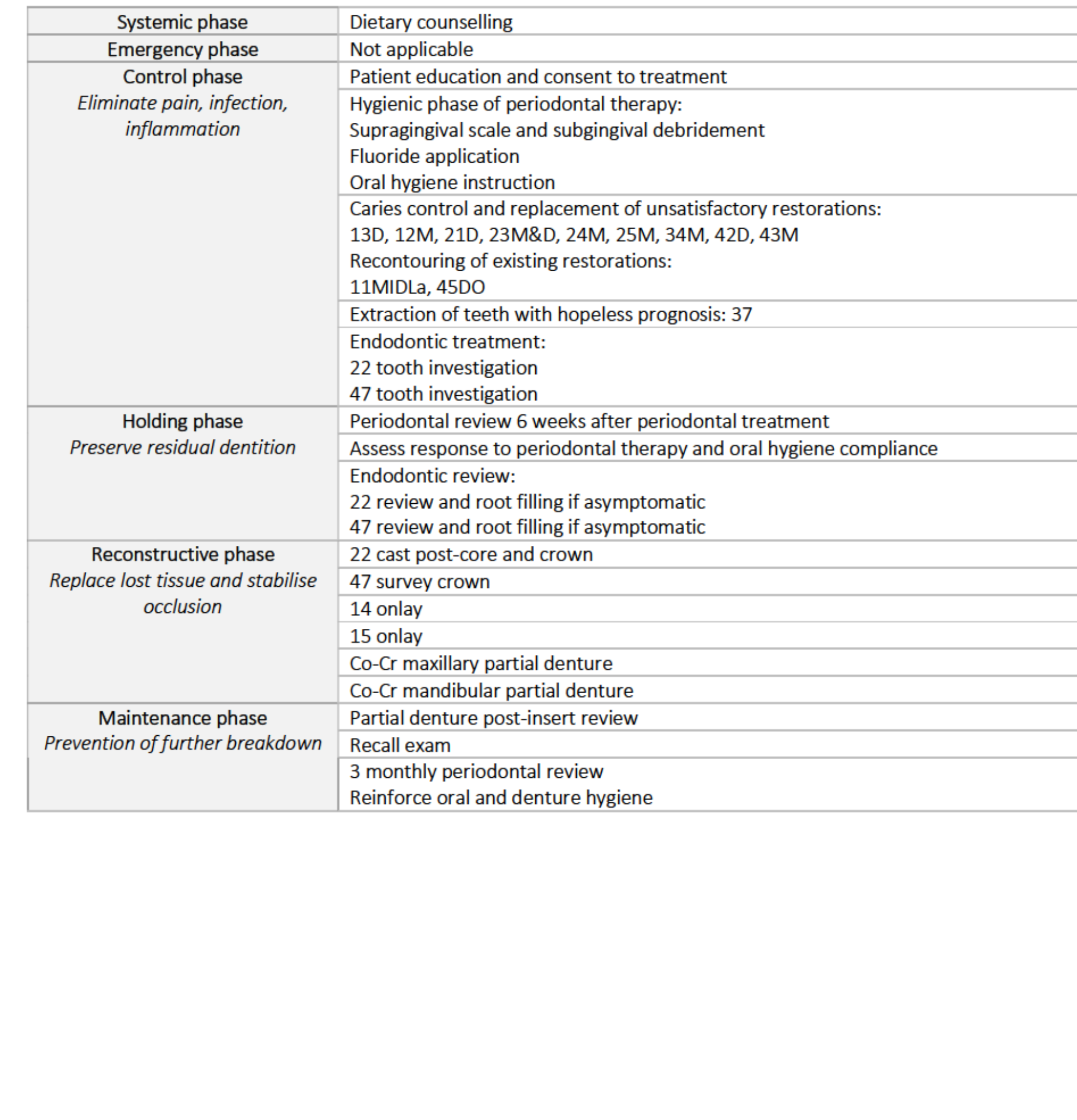
Management Plan
Management Plan Phases22
Control Phase
- Periodontal debridement, OHI, and fluoride application.
- Caries control and replacement of restorations (13, 12, 21, 23, 24, 25, 34, 42, 43).
- Extraction of 37.
- Endodontic investigation/treatment of 22 and 47.
Holding Phase
- 6-week periodontal review.
- Completion of root fillings for 22 and 47 if asymptomatic.
Reconstructive Phase
- 22: Cast post-core and crown.
- 47: Survey crown.
- 14 & 15: Onlays.
- Maxillary and Mandibular Co-Cr partial dentures.
Maintenance Phase
- 3-monthly periodontal reviews and denture hygiene reinforcement.
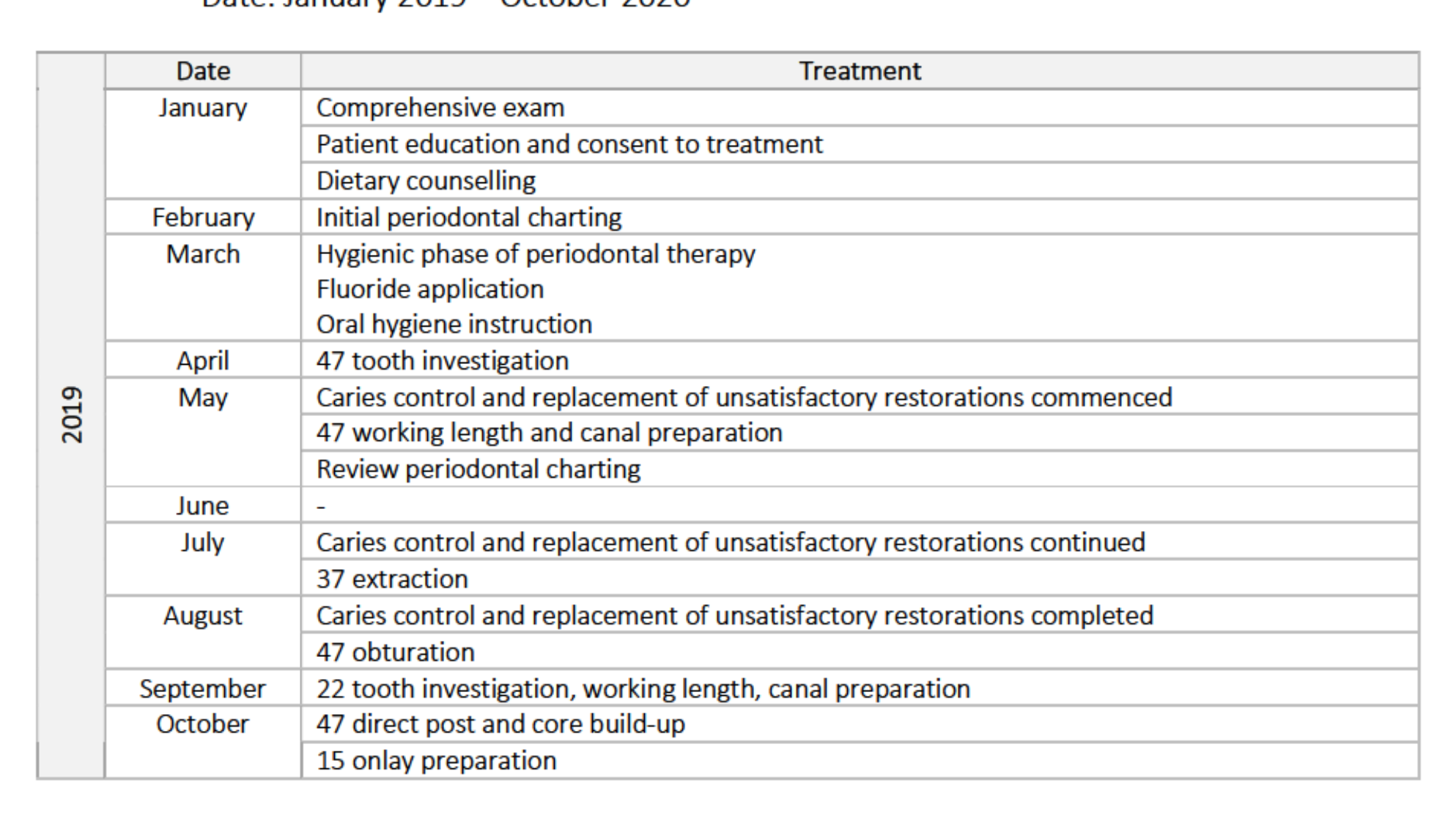
Treatment Delivery
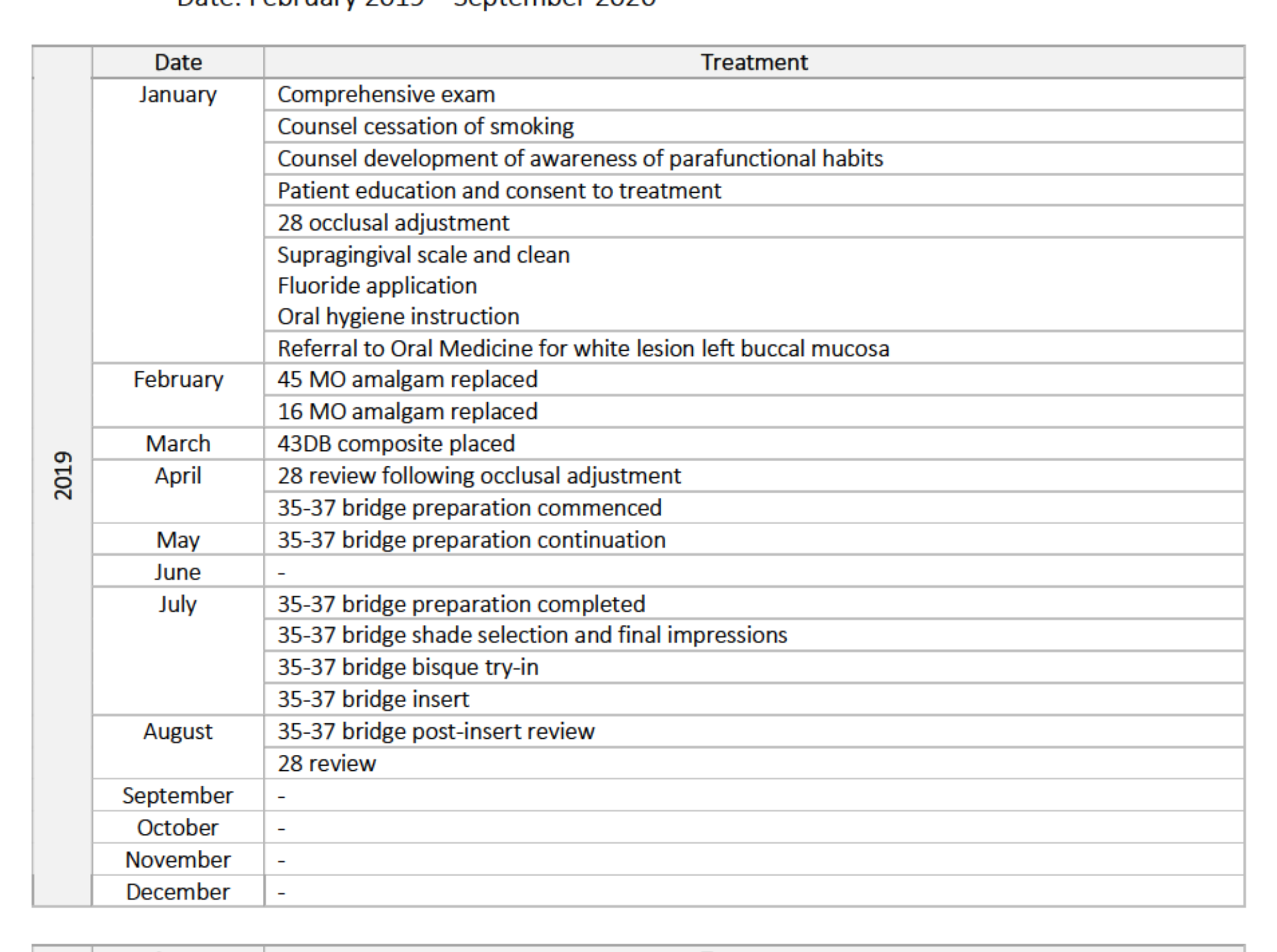
Treatment Timeline (2019-2020)23
2019 Highlights
- Jan-Mar: Exam, education, and hygienic periodontal phase.
- Apr-Aug: 47 endodontic treatment and obturation; 37 extraction.
- May-Aug: Caries control and restoration replacement.
- Sep-Oct: 22 endodontic start; 15 onlay preparation.
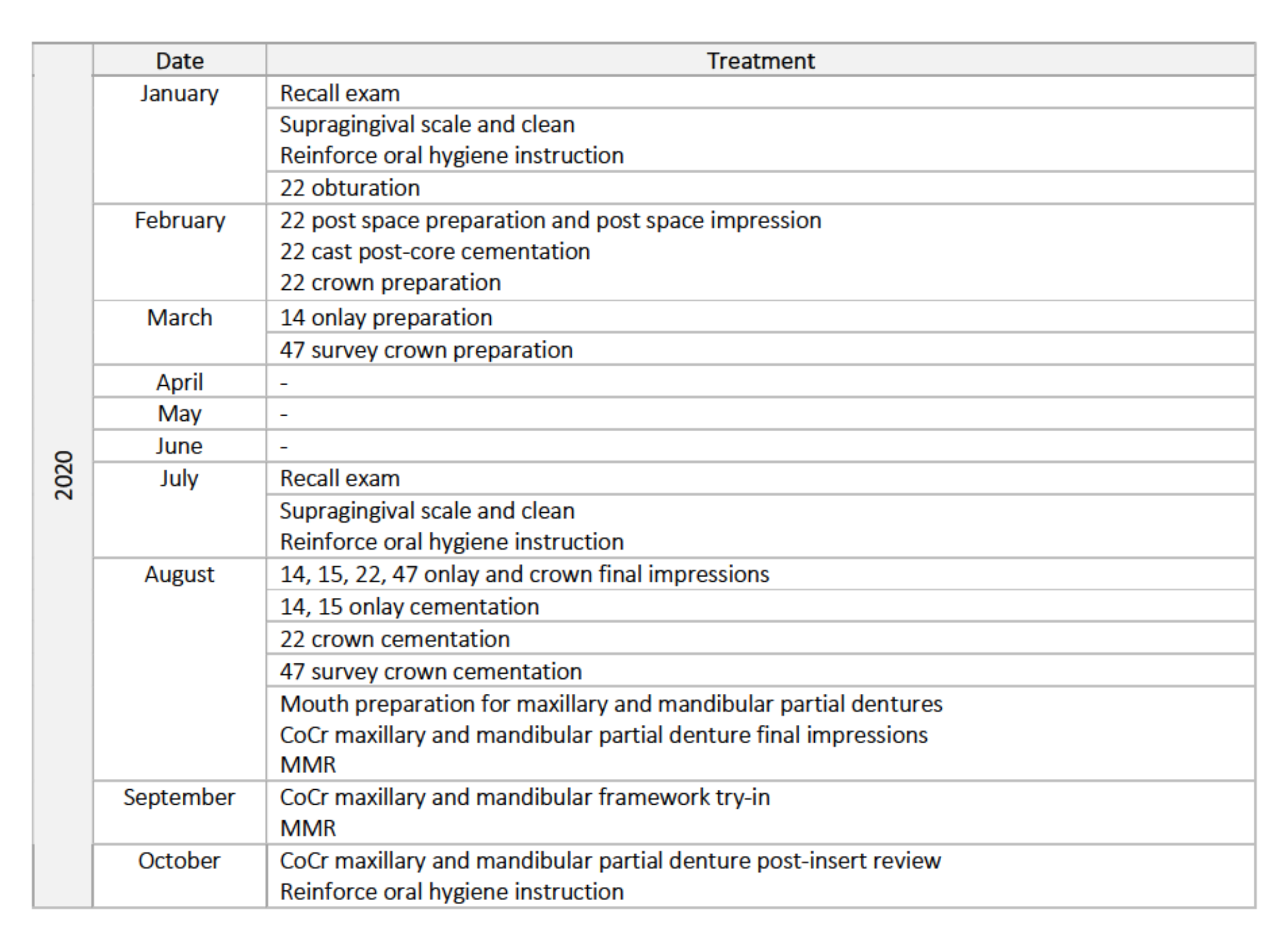
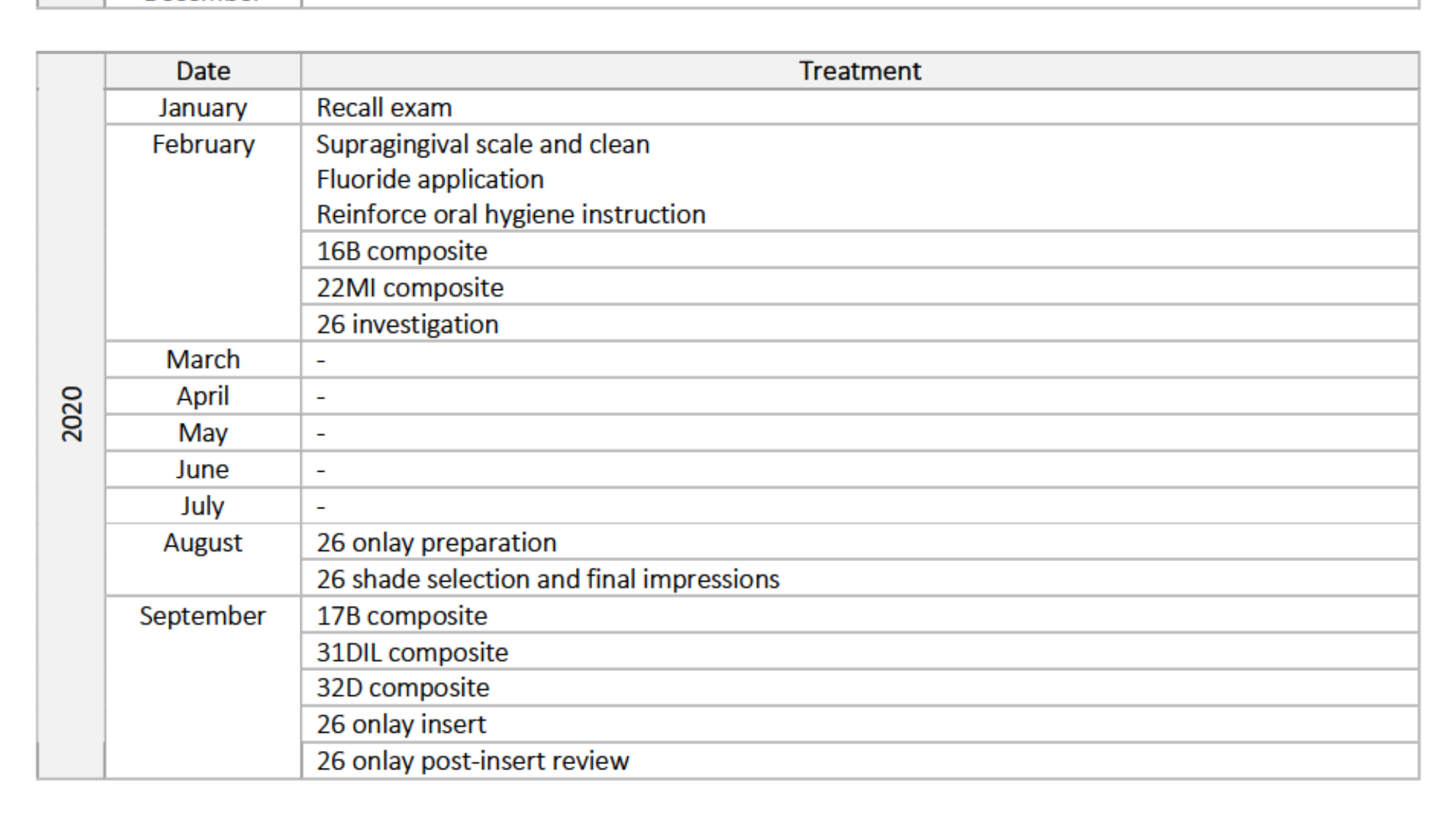
2020 Highlights
- Jan-Feb: 22 obturation and cast post-core cementation.
- Mar-Aug: Preparations for 14, 47 (survey crown), and final impressions for all indirect restorations.
- Aug-Oct: Cementation of crowns/onlays; fabrication and insertion of Co-Cr partial dentures; post-insert reviews.
 |  |
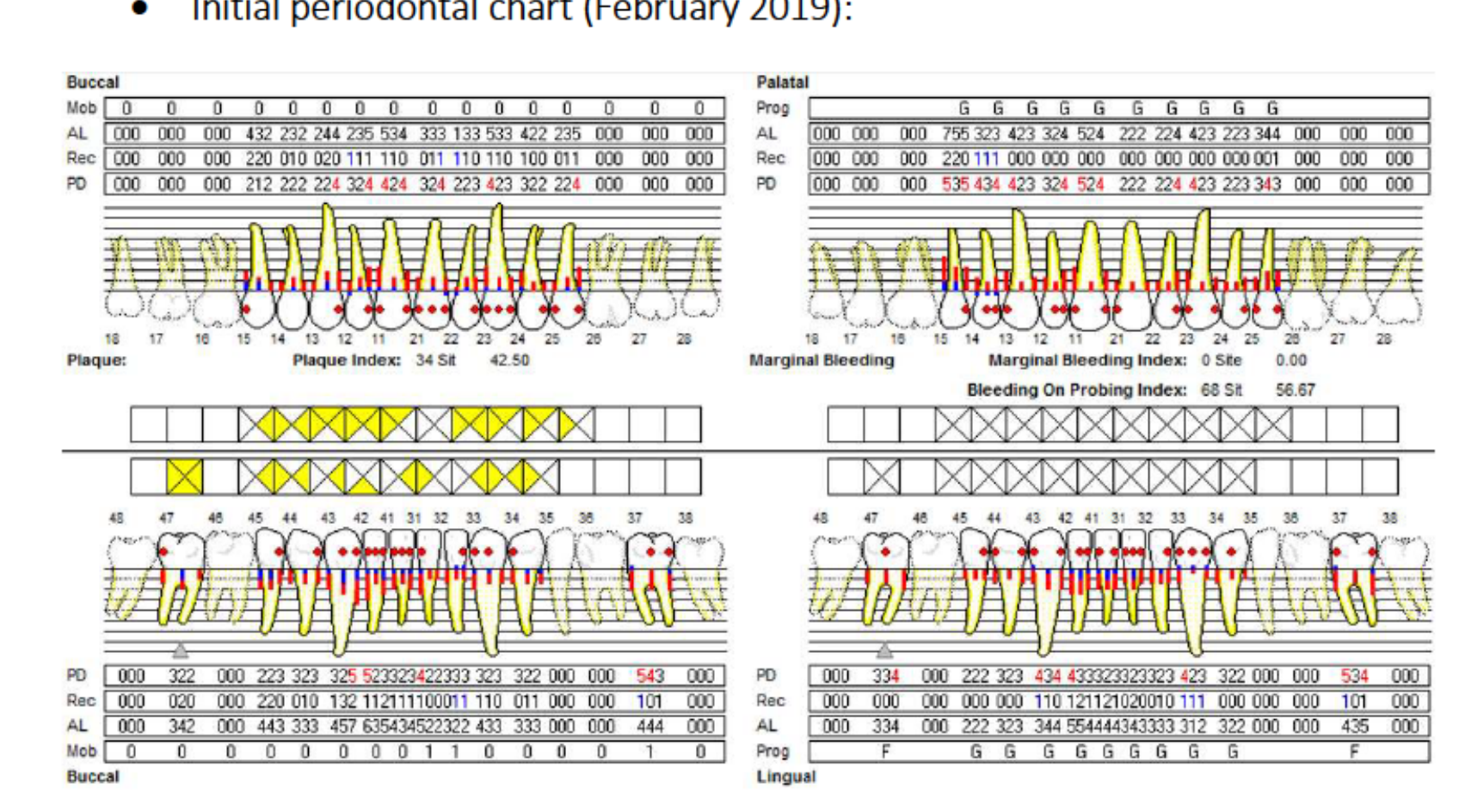
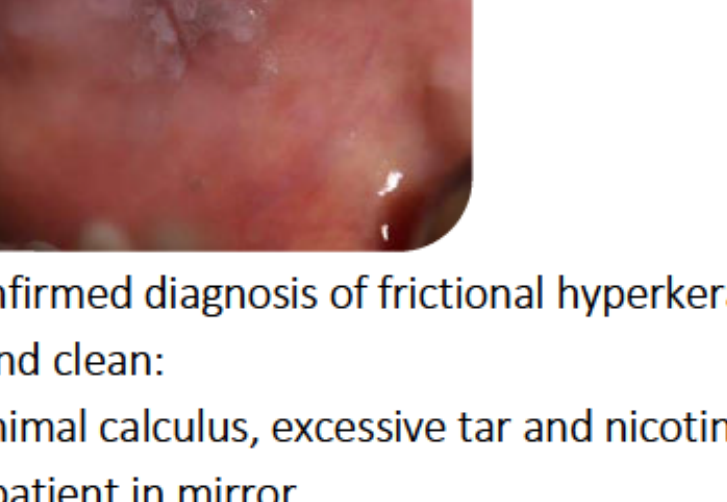
Initial Periodontal Therapy (Feb 2019)24
- Baseline Data:
- Plaque Score: 100%.
- Bleeding on Probing (BOP): 57%.
- PPD ≥ 4mm: 24% of sites.
- Mobility: Grade I on 31, 32, 37.
- Clinical Notes: Extreme gingival pain during probing. Patient instructed on electric toothbrush use and interproximal brushes.
- Education: Patient educated on caries aetiology (diet, bacteria, time) and encouraged to keep a food diary.
 |  |
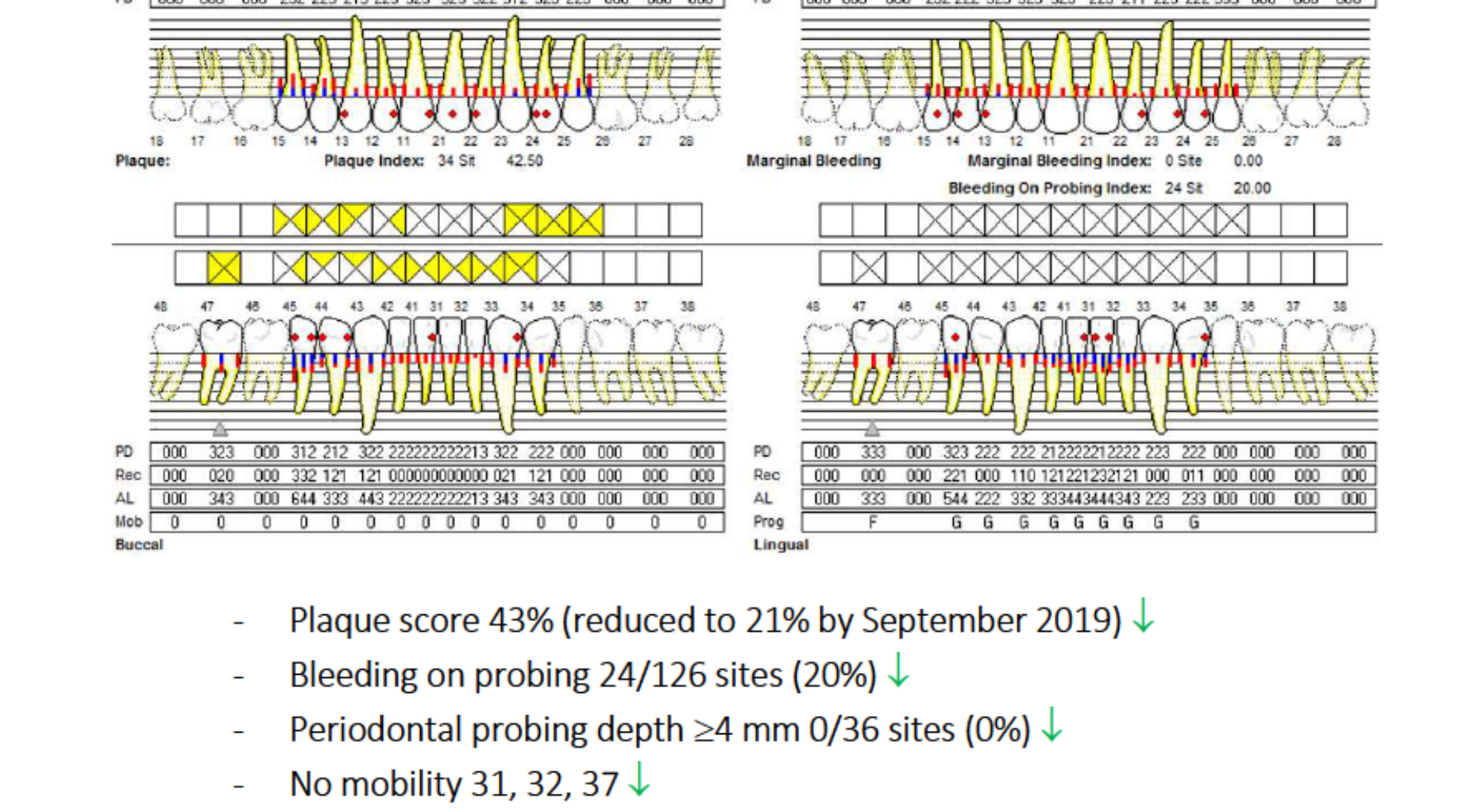
Periodontal Review and Caries Control25
- Periodontal Progress (May-Sep 2019):
- Plaque score reduced from 43% to 21%.
- BOP reduced to 20%.
- PPD ≥ 4mm reduced to 0%.
- Diagnosis revised to “Periodontitis in remission.”
- Dietary Changes: Substituted sugar with Stevia; reduced coffee and snacking; increased dairy and vegetable intake.
- Surgical: 37 extracted due to symptomatic, extensive subgingival caries.
 |  |
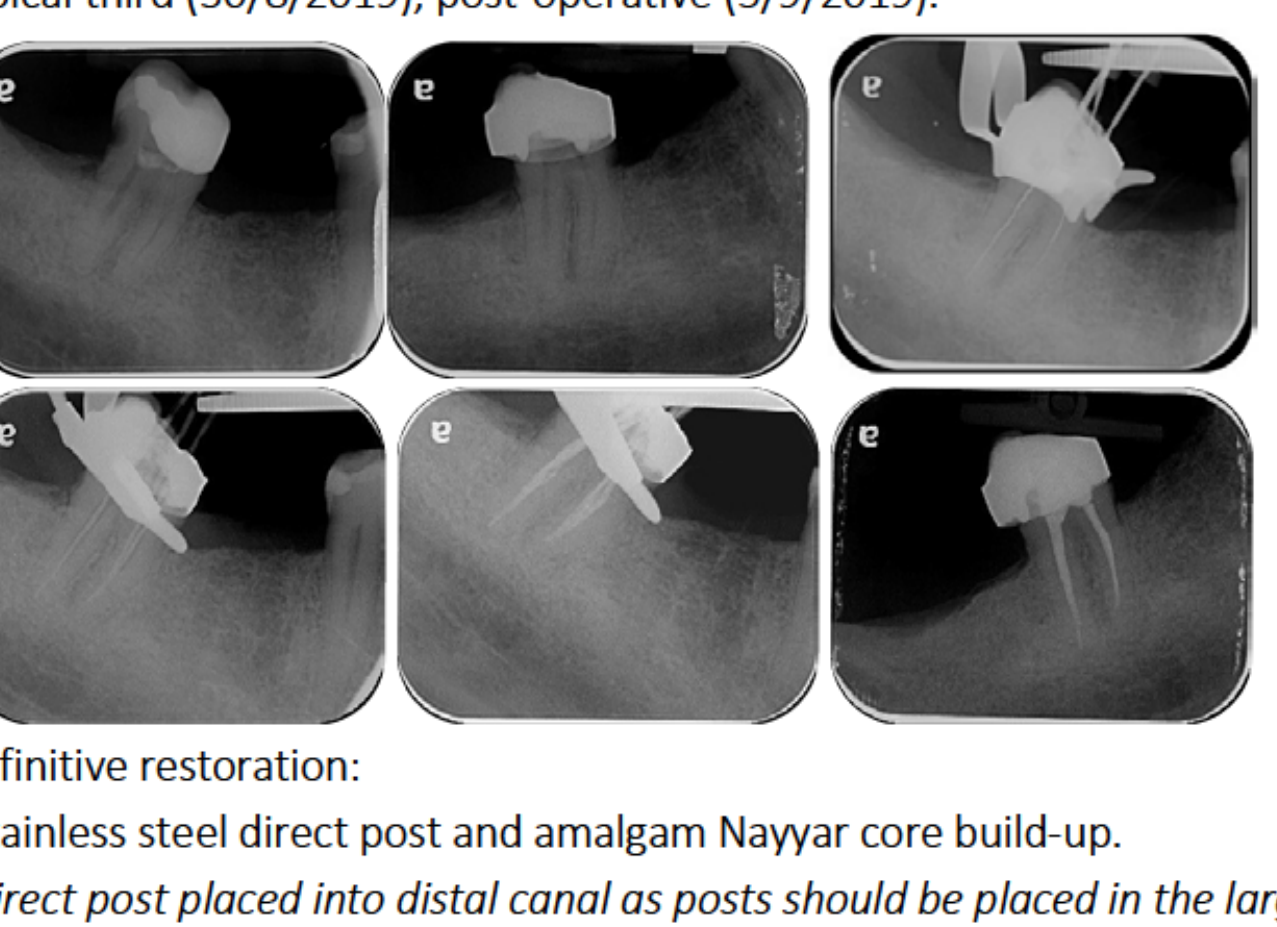
Tooth 47: Endodontics and Core Build-up26
- Endodontic Treatment: Completed between April and September 2019.
- Definitive Restoration:
- Stainless steel direct post placed in the distal canal (largest/straightest).
- Amalgam Nayyar core technique utilized.
- Rationale: Amalgam provides high strength and low solubility, though it requires setting time before preparation.
 |  |
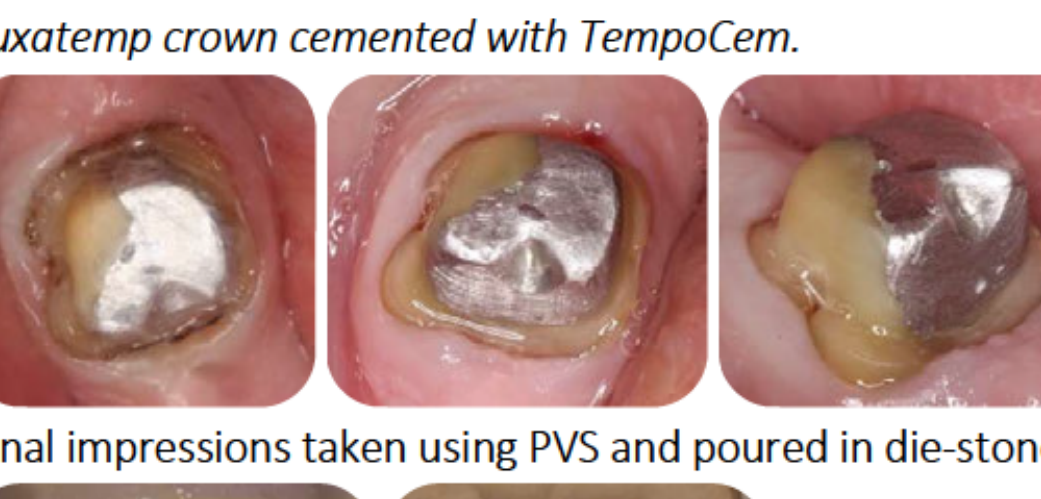
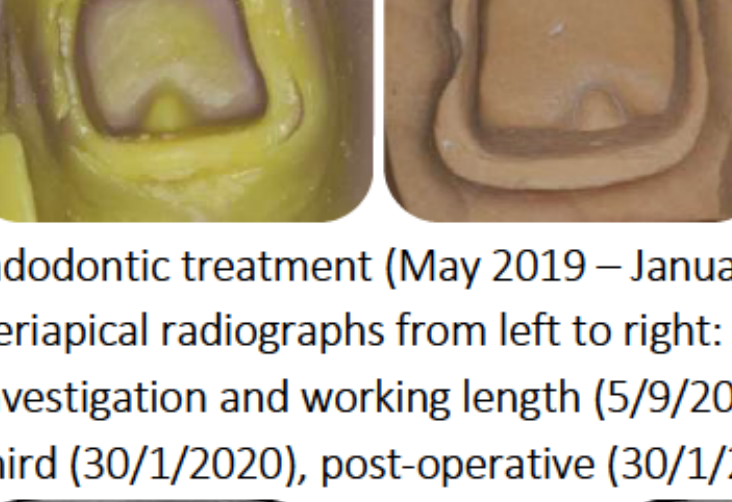
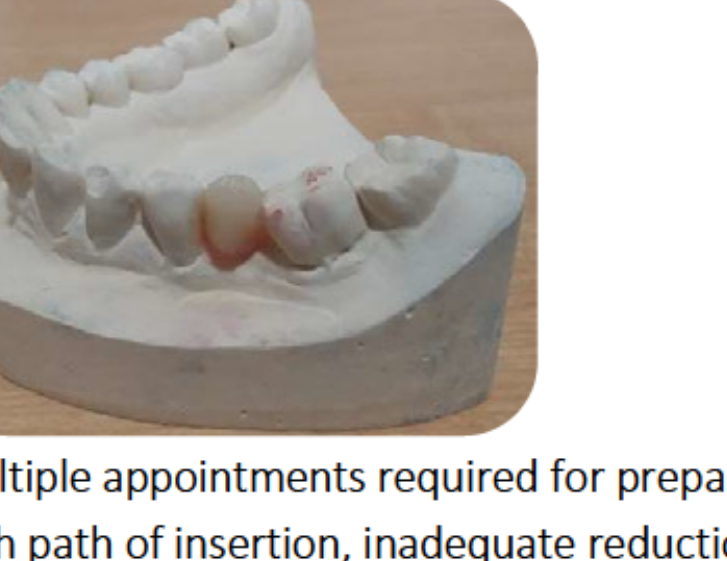
Tooth 47 Survey Crown and Tooth 22 Endodontics27
- 47 Survey Crown: Prepared for a Zirconia crown to serve as a posterior denture abutment. Zirconia selected for superior mechanical strength.
- 22 Endodontic Treatment:
- Treatment spanned May 2019 to January 2020.
- Challenge: Canal was severely calcified; required specialist endodontic assistance for access.
- Temporized with a GIC dome restoration during the process.
 |  |
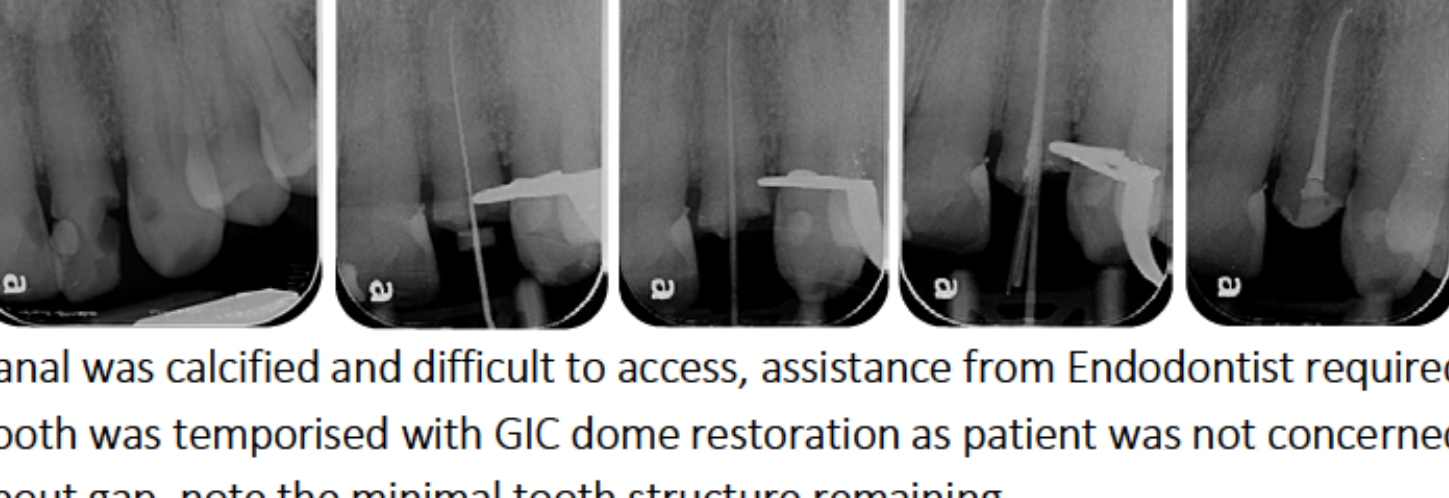 |  |
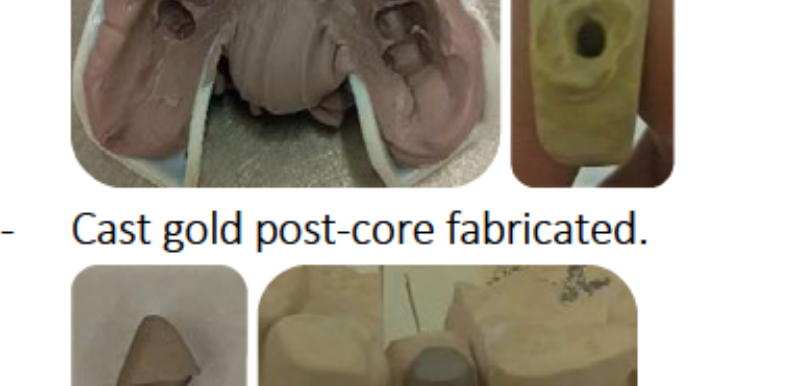
Tooth 22: Cast Post-Core28
- Rationale: Post required due to insufficient tooth substance to support a crown.
- Design: Cast gold alloy (Type III/IV) used for its modulus of elasticity similar to enamel and high compressive strength.
- Specifications: Parallel, passive post design; length extended to half the root supported by bone; 3-6 mm apical gutta-percha preserved.
- Procedure: Post space prepared and impression taken with PVS.
 |  |
 |
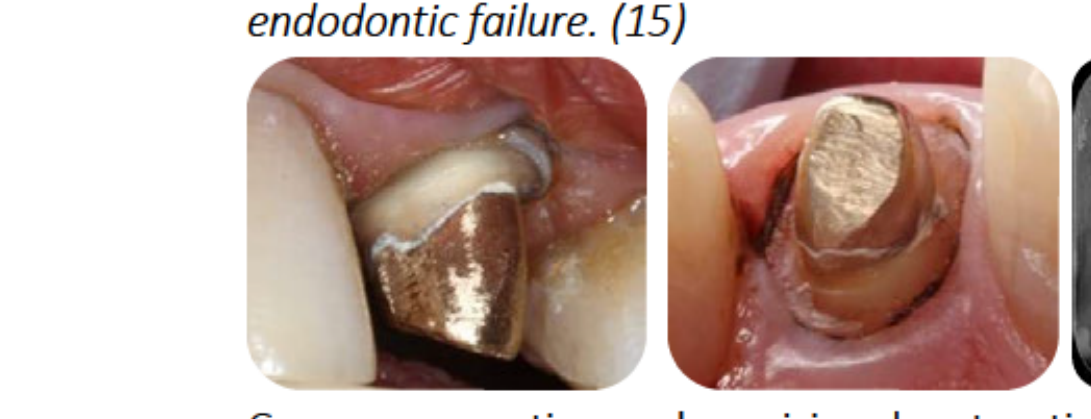
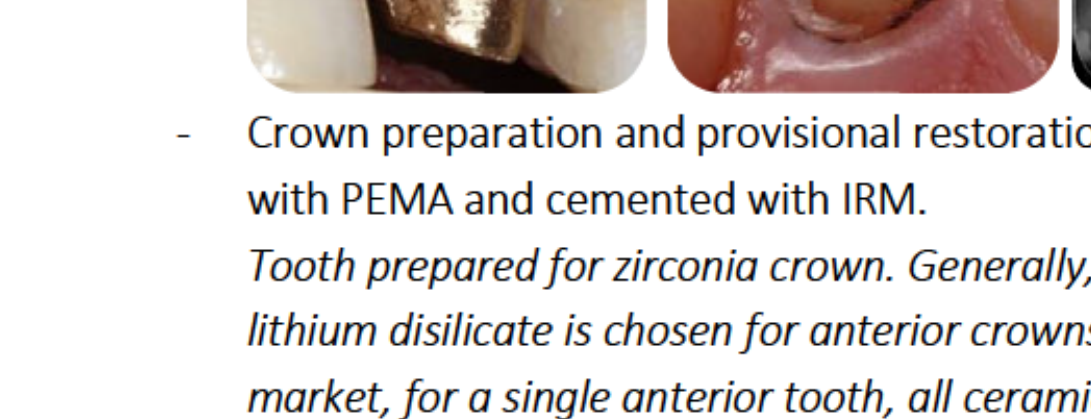
Tooth 22: Crown Preparation29
- Cementation: Cast post-core cemented with Panavia.
- Crown Selection: Zirconia crown chosen.
- Rationale: While lithium disilicate is often used for anterior teeth, Zirconia was selected here to mask the dark metallic shade of the cast gold post-core. Opaque cement was also utilized for masking.
 |  |
 |
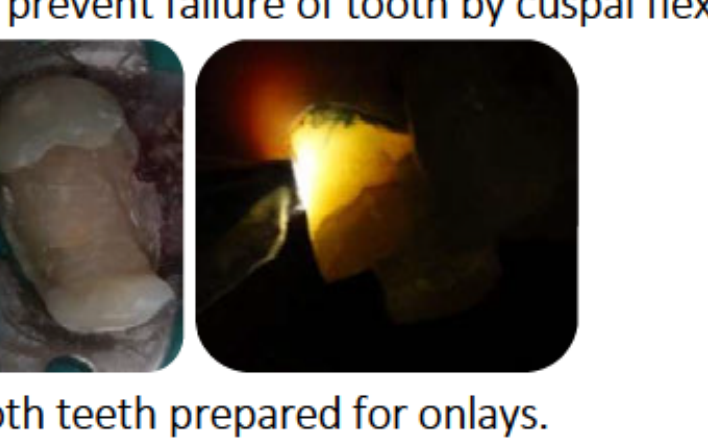
Teeth 14 and 15: Onlay Preparations30
- Findings: Removal of old MOD composites revealed cracks in tooth 15.
- Design: Buccal and palatal walls reduced for cuspal coverage to prevent tooth failure from flexure.
- Temporization: Stainless steel bands and IRM used while onlays were fabricated.
 |  |
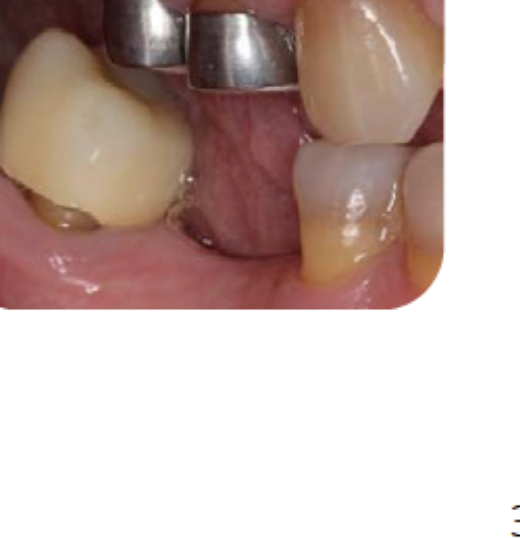 |
Final Cementation of Indirect Restorations31
- 14 & 15 Onlays: Cemented with Variolink.
- 22 Crown: Cemented with Panavia.
- 47 Survey Crown: Cemented with Permacem.
 |  |  |
 | 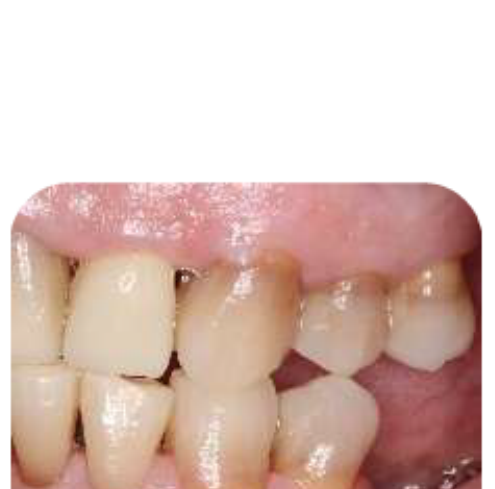 |
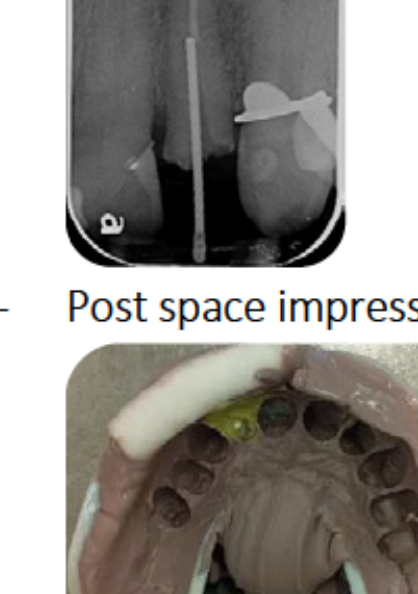
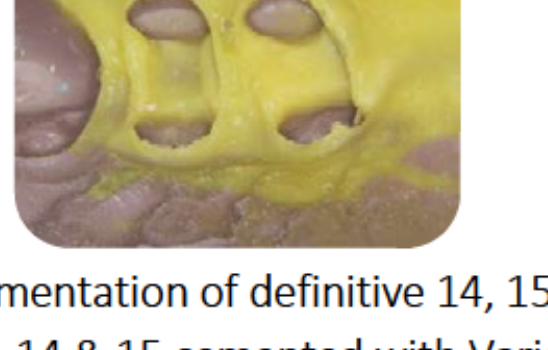
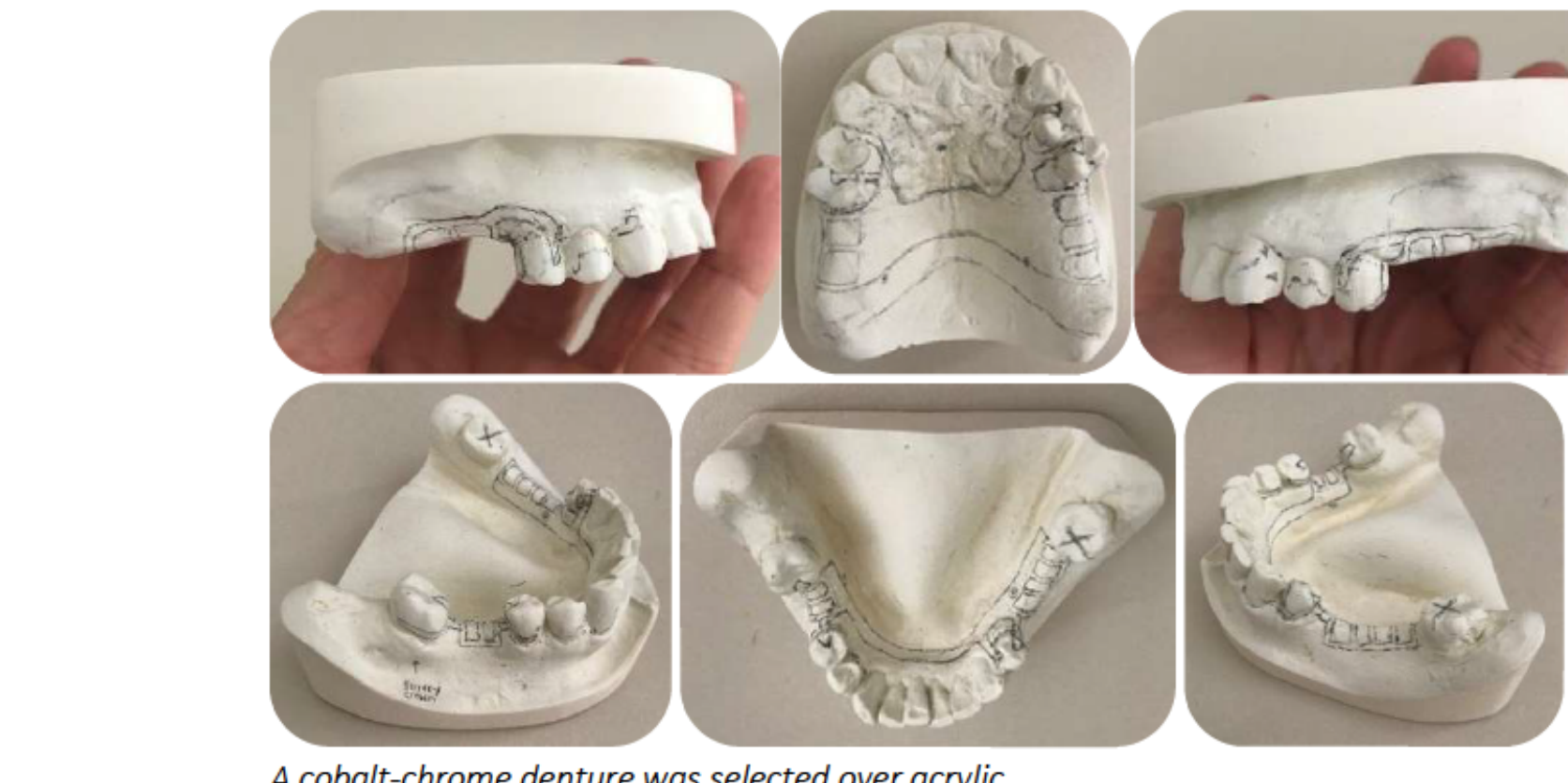
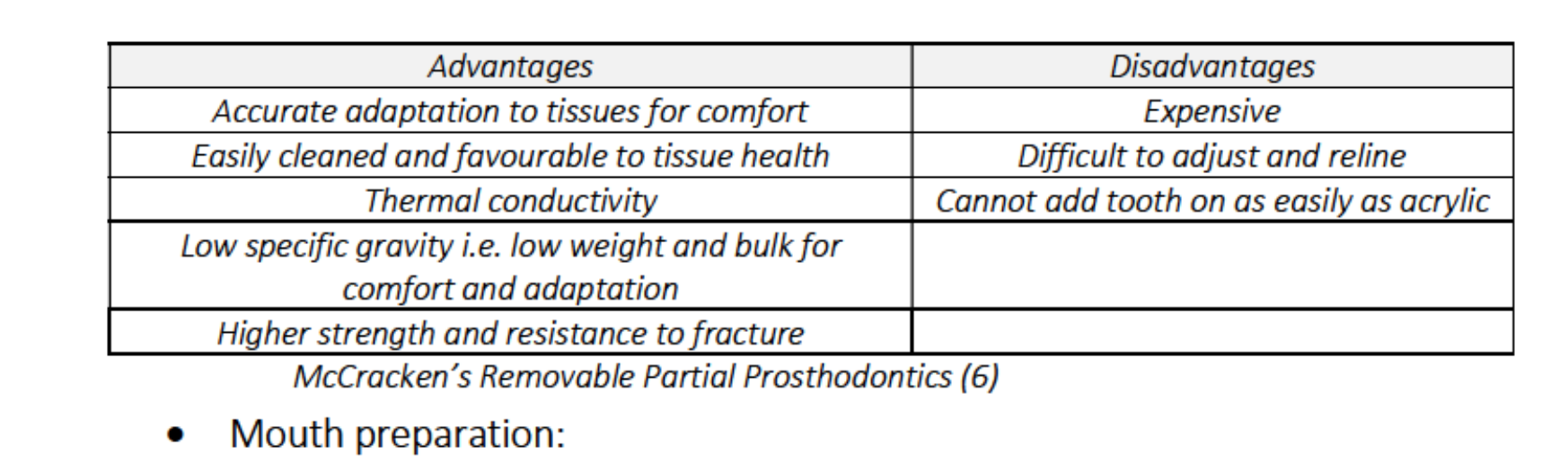
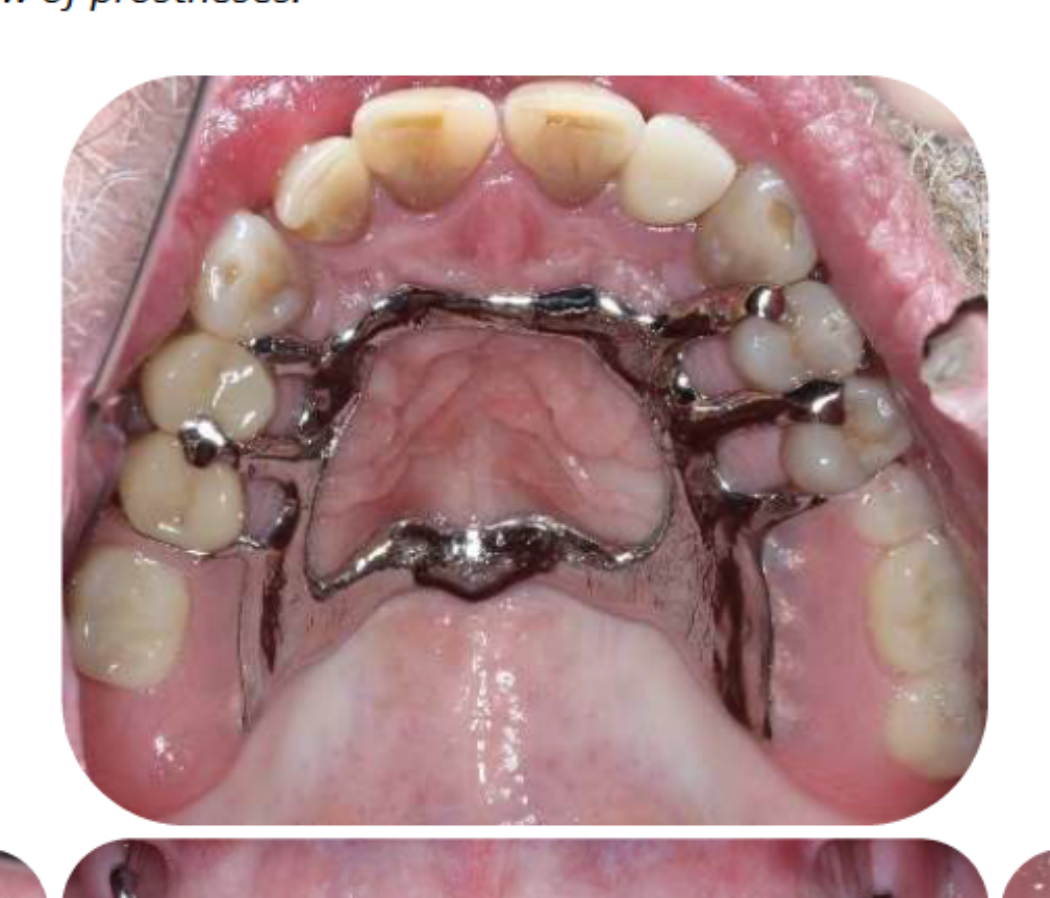
Removable Partial Denture (RPD) Design32
- Material: Cobalt-Chrome (Co-Cr) selected over acrylic for better adaptation, thermal conductivity, and strength.
- Mouth Preparation:
- Rest seats: 15M, 14M, 47M (in restorations); 24M, 25M, 33P, 45D.
- Guide planes: 15D, 47M (in restorations); 25D, 34D.
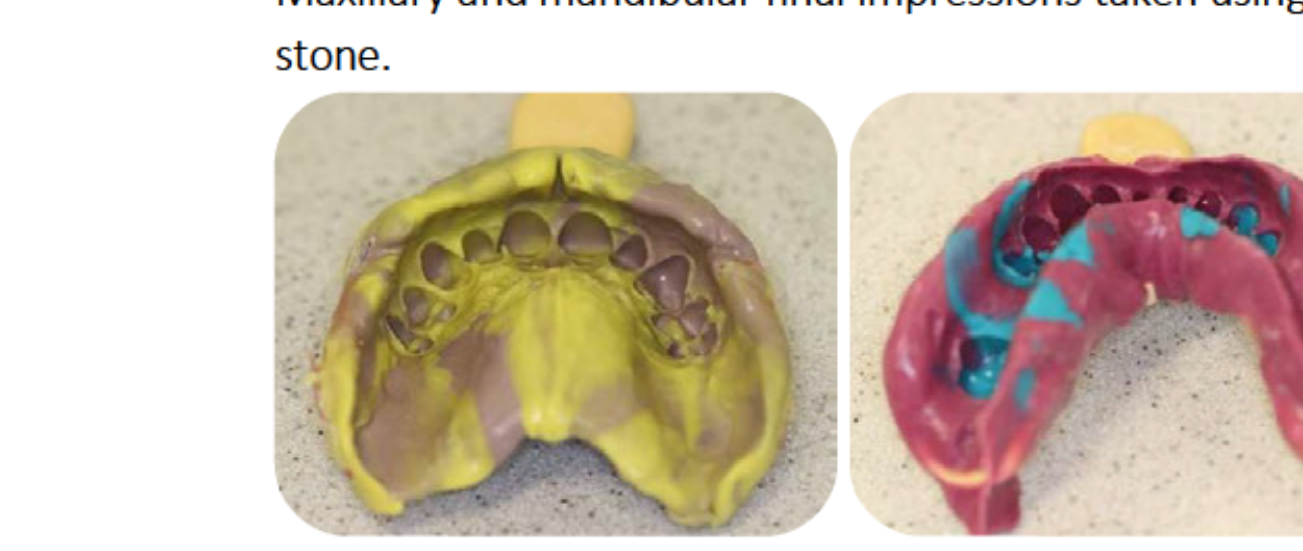
- Impressions: Final maxillary and mandibular impressions taken using PVS.
 |  |
 |
RPD Framework Try-in and Insertion33
- Framework Try-in: Maxillary framework required a re-impression due to non-passive fit. Second framework was acceptable. Mandibular framework fit correctly.
- Try-in with Teeth: Satisfactory aesthetics, phonetics, and occlusion.
- Insertion: Maxillary denture required clasp adjustment for stability. Patient reported high satisfaction.
- Clinical Rationale: Although the patient has 21 teeth (Shortened Dental Arch), dentures were provided to meet functional and psychological needs.
Patient Choice and Long-term Success34
- The patient elected for removable partial dentures despite having 21 teeth.
- Success is contingent upon the patient’s adaptation to the prostheses and strict adherence to oral/denture hygiene and regular periodontal maintenance.
 |  |  |
 |  |
Treatment Progress Summary (2019)35
- Jan 2019: Diagnostic phase.
- May 2019: Initial periodontal therapy complete; caries control and 47 endodontics in progress.
- Aug 2019: 37 extracted; 22 and 47 endodontics in progress; periodontal status stable.
- Sep 2019: Caries control complete; 47 endodontics complete; 22 endodontics in progress.
Treatment Progress Summary (2019-2020)36
- Oct 2019: 47 post/core complete; 15 preparation in progress.
- Mar 2020: 22 endodontics and cast post-core complete; crown preparations for 14, 15, 22, 47 in progress.
- Aug 2020: All indirect fixed restorations (14, 15, 22, 47) completed.
- Oct 2020: Removable prostheses inserted; periodontal status maintained.
Clinical Outcomes And Reflection
Clinical Outcomes37
- Patient Satisfaction: Very satisfied; reported improved bite stability.
- Complaint Resolution:
- Pain in 37, 47, and gums resolved.
- Sensitivity in 22 resolved.
- Missing teeth replaced with Co-Cr dentures.
- Compliance: Patient successfully modified diet and hygiene habits. Highly compliant with appointments and maintenance.
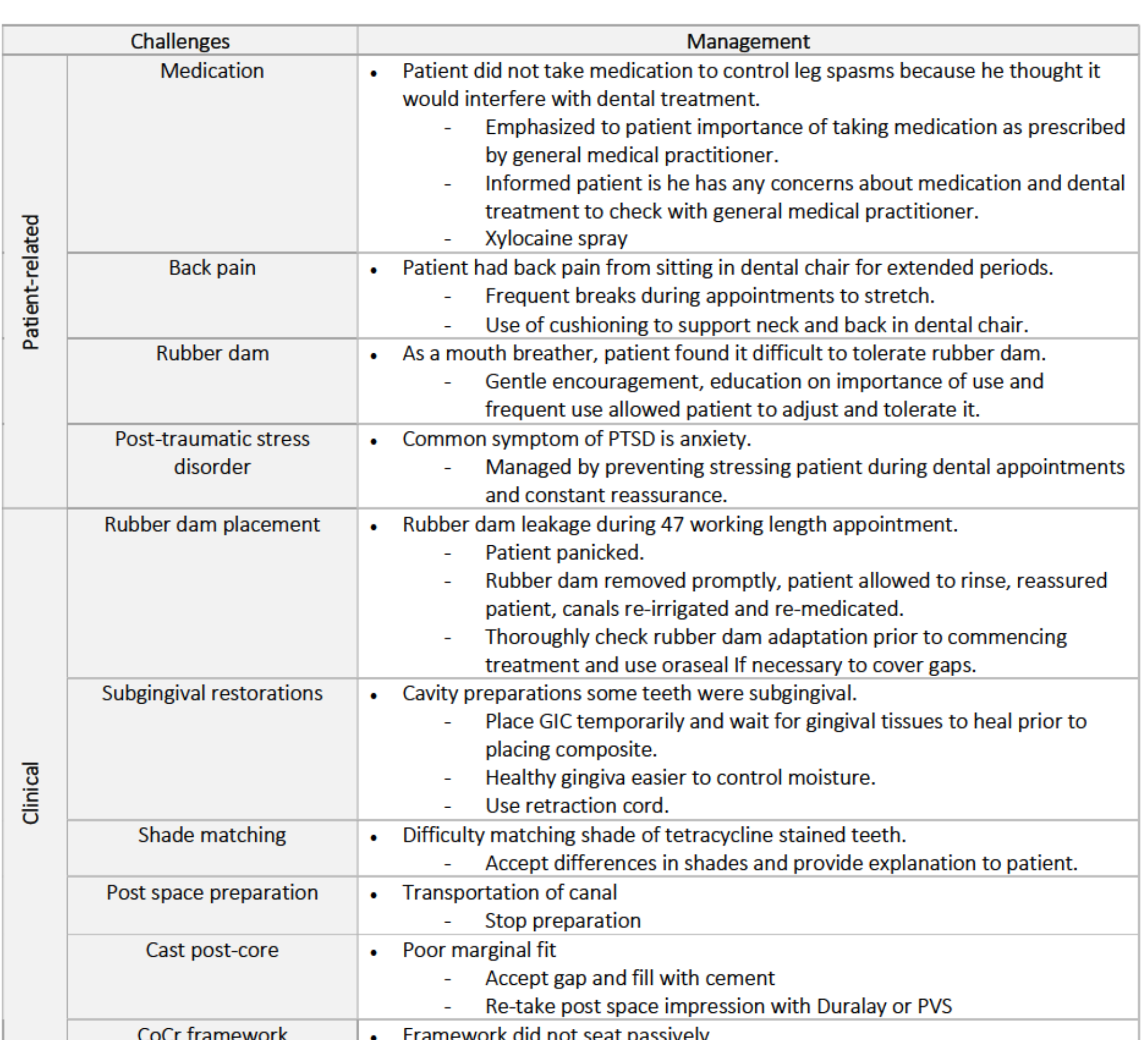
Reflection on Challenges38
Patient-Related Challenges
- Medical: Managed leg spasms by reinforcing medication adherence; managed back pain with frequent breaks and cushioning.
- Anxiety/PTSD: Managed with constant reassurance and preventing stressful situations.
- Mouth Breathing: Managed rubber dam intolerance through education and gradual adjustment.
Clinical Challenges
- Rubber Dam Leakage: Occurred during 47 treatment; managed by prompt removal, rinsing, and re-medication.
- Subgingival Margins: Managed with temporary GIC and retraction cords to allow tissue healing.
- Shade Matching: Difficult due to tetracycline staining; managed by patient education on aesthetic limitations.
- Technical Issues: Managed canal transportation by stopping preparation; managed non-passive Co-Cr framework with re-impressions.
Case 2: Fixed Aesthetic39
Fixed Aesthetic
The Patient
Patient Details40
- 61 year-old female

Presenting Complaints
Patient presented to student clinic in May 2019 with the following complaints:
- “I don’t smile anymore because my front teeth are so bad. The front tooth (21) is brown, they’re all mismatched. I want the teeth (13-21) to look the same colour because when I smile, I’m self-conscious.”
- “My crown (11) has fallen off and been stuck on again – I’m afraid it will fall off again.”
- “I had some sensitivity last week when eating sweet foods (47).”
History of Presenting Complaints
- Upper anterior crowns (11, 12) were inserted 20-30 years ago. 11 crown de-bonded and was re-cemented 7 years ago.
- Noticed occasional sensitivity on lower right-hand side after eating sweet foods. Happened about a week ago. No sensitivity to thermal stimuli. Did not cause patient to wake at night. Relieved by ibuprofen.
Medical History41
| Medical condition | Description | Dental implications |
|---|---|---|
| History of asthma attack | Wheezing, coughing, chest tightness or shortness of breath. | Asthma attack in dental chair. Sit person upright, reassure. Give 4 puffs blue/grey reliever every 4 minutes. |
Medications: Not currently taking any medication/s.
Allergies: No known allergies.
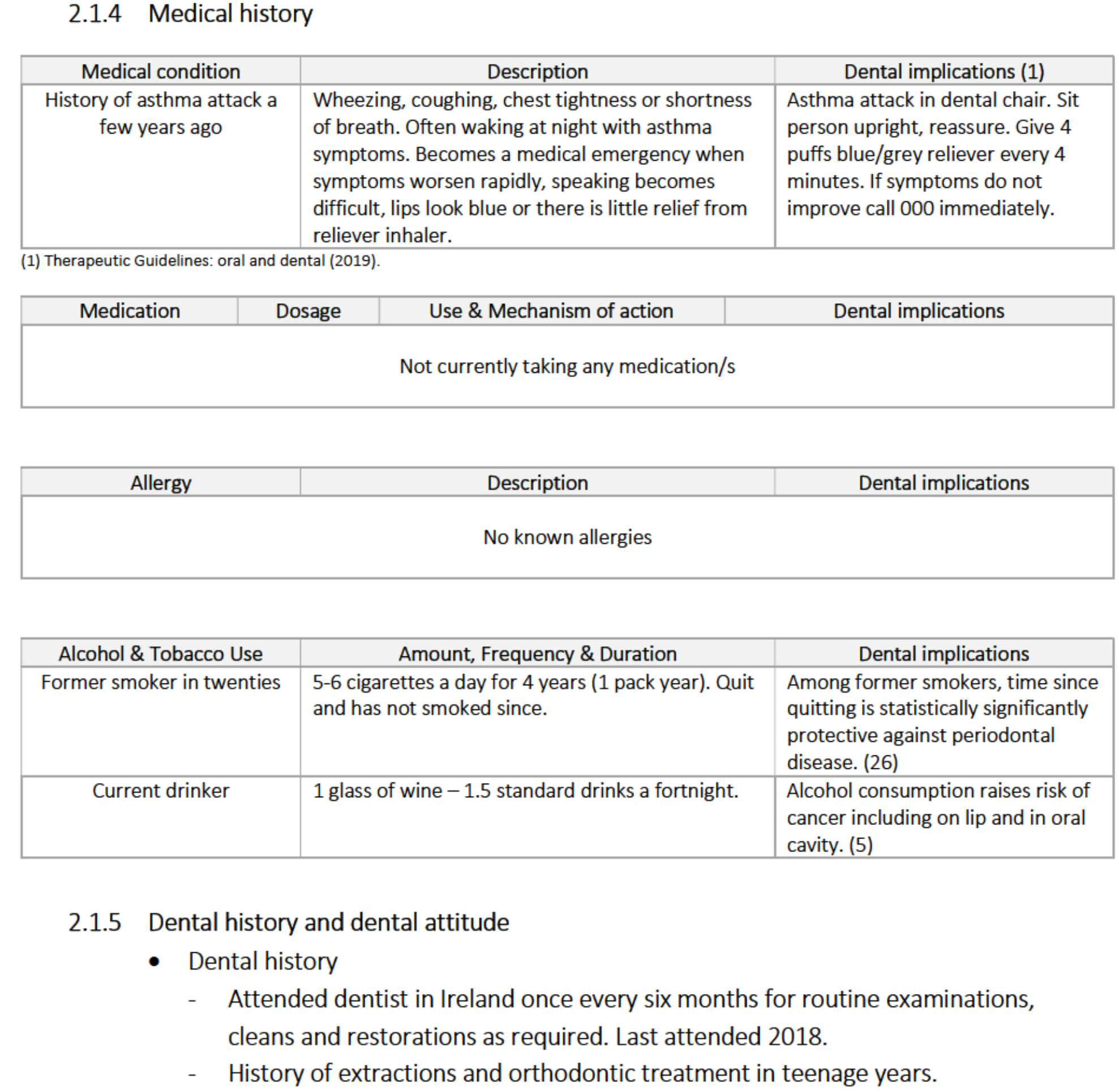
Alcohol & Tobacco Use
- Former smoker: Smoked in twenties (5-6 cigarettes a day for 4 years; 1 pack year). Quit and has not smoked since. Time since quitting is statistically protective against periodontal disease.
- Current drinker: 1 glass of wine (1.5 standard drinks) a fortnight. Alcohol consumption raises risk of oral cavity cancer.
Dental History
- Attended dentist in Ireland every six months for routine examinations, cleans, and restorations. Last attended 2018.
- History of extractions and orthodontic treatment in teenage years.
- History of endodontic treatment (11, 12) due to dental infection.
- No history of trauma.
- Attended OHCWA screening clinic February 2019; initial examination May 2019.
Dental Attitude
- Aesthetic motivation.
- Apprehensive to radiation exposure.
- Strong gag reflex.
- Lack of trust in student clinicians.
- Never missed an appointment.
Oral Hygiene42
- Status: Fair oral hygiene.
- Routine: Brushes twice daily with electric toothbrush and fluoride toothpaste.
- Adjuncts: Uses floss once a week; no other cleaning adjuncts.
 |  |
Social History
- Born and raised in Ireland; moved to Australia in November 2018.
- Lives alone; works in aged care.
- Two children (son in Sydney, daughter in Perth).
- Enjoys playing competitive golf.
- Considering moving to Sydney in the future.
Examination And Diagnostics
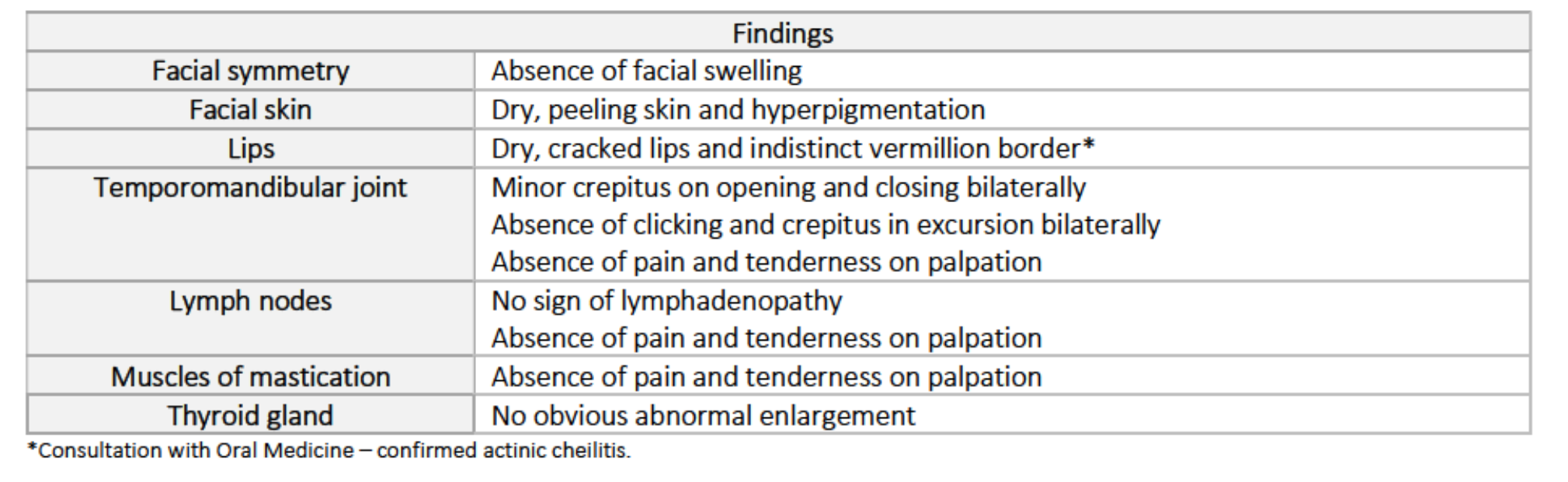
Extra-oral Examination (May 2019)43
| Feature | Findings |
|---|---|
| Facial symmetry | Absence of facial swelling; relatively symmetrical |
| Facial skin | Dry, peeling skin and hyperpigmentation |
| Lips | Dry, cracked lips and indistinct vermilion border (Confirmed actinic cheilitis) |
| TMJ | Minor crepitus on opening/closing bilaterally; no pain or tenderness |
| Lymph nodes | No lymphadenopathy; no pain or tenderness |
| Muscles of mastication | Absence of pain and tenderness on palpation |
| Thyroid gland | No obvious abnormal enlargement |
 |  |
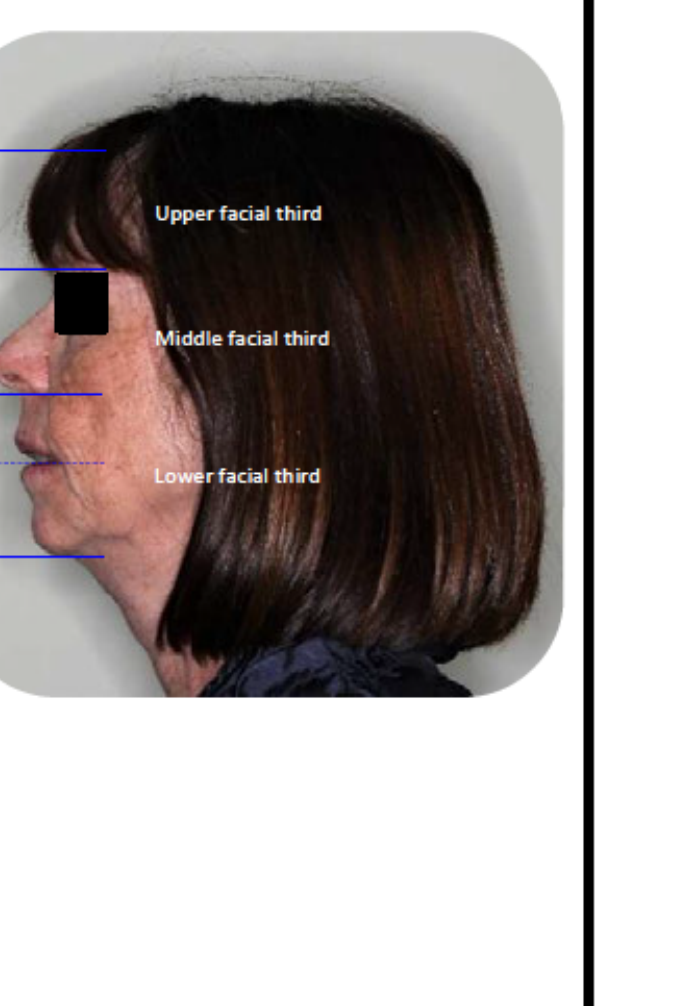 |  |
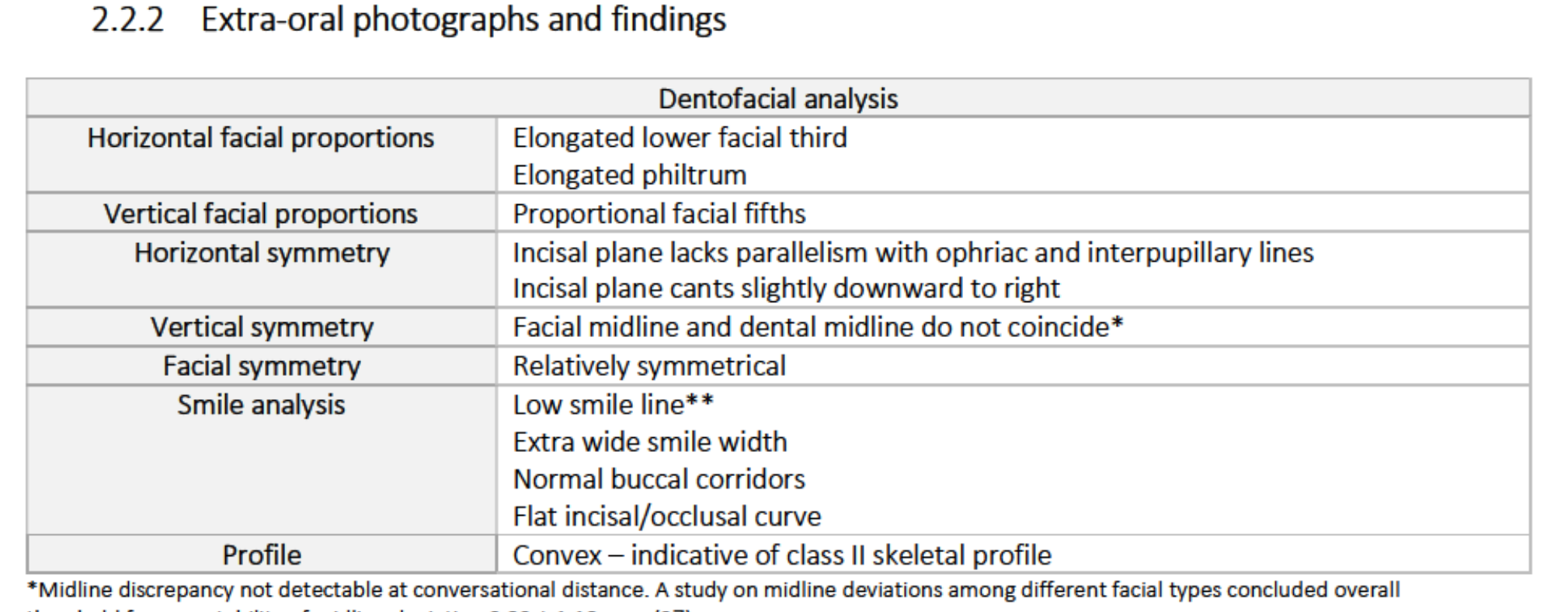
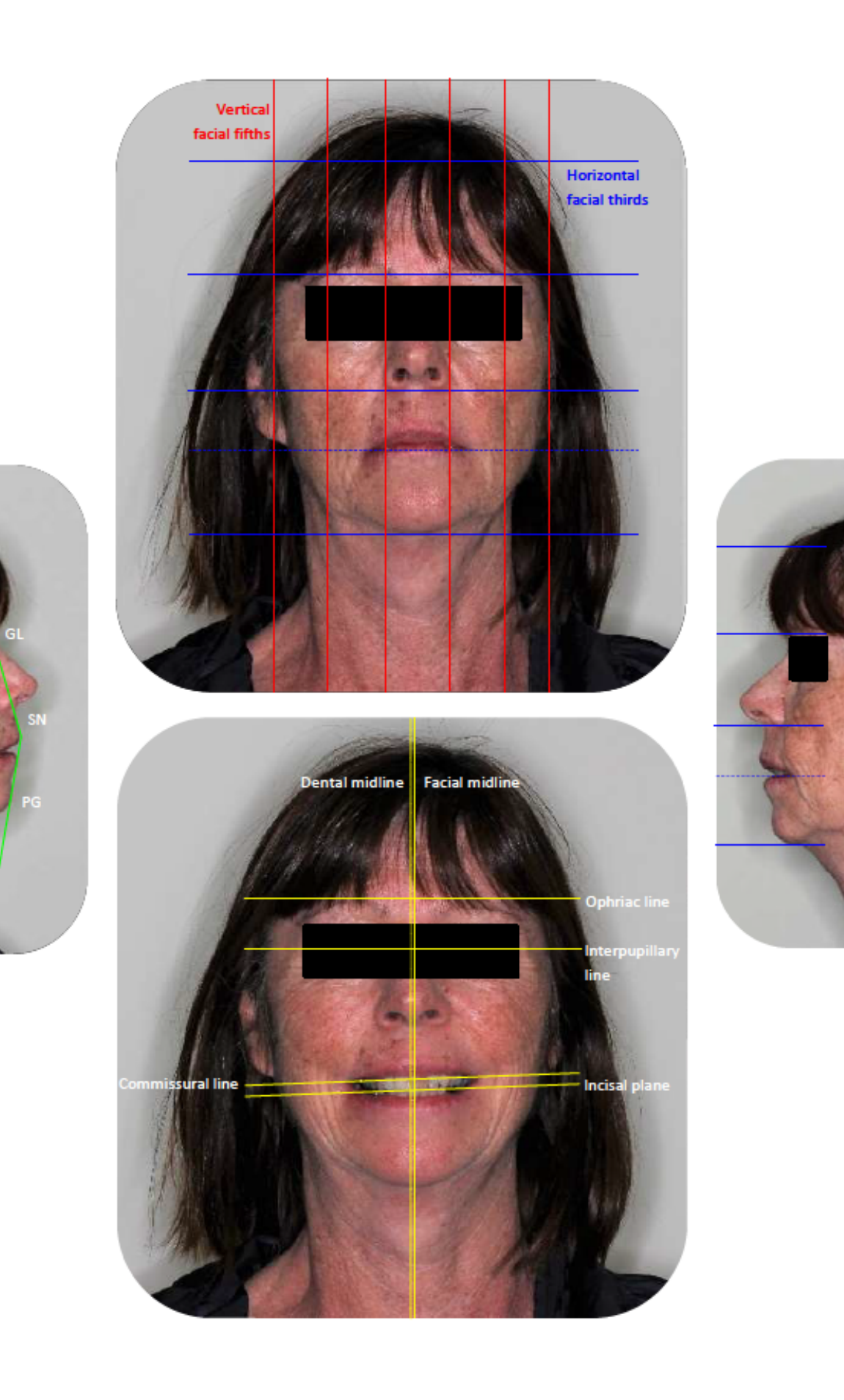
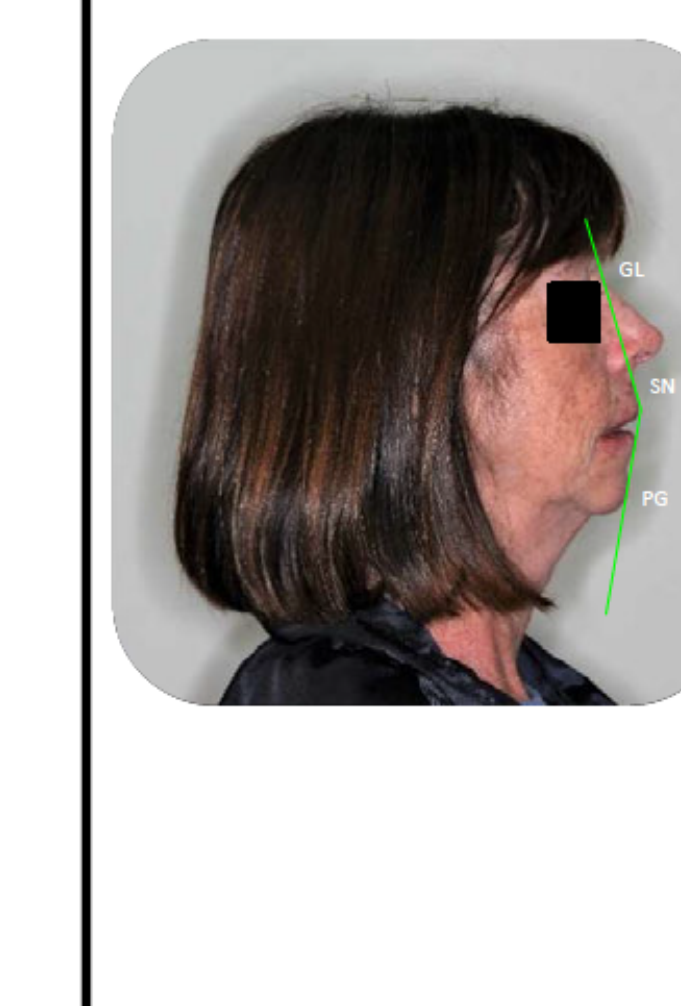
Dentofacial Analysis
- Horizontal facial proportions: Elongated lower facial third; elongated philtrum.
- Vertical facial proportions: Proportional facial fifths.
- Horizontal symmetry: Incisal plane lacks parallelism with interpupillary lines; cants downward to right.
- Vertical symmetry: Facial and dental midlines do not coincide (discrepancy not detectable at conversational distance).
- Smile analysis: Low smile line; extra wide smile width; normal buccal corridors; flat incisal/occlusal curve.
- Profile: Convex (indicative of Class II skeletal profile).
Intraoral Soft Tissue Findings
- Labial mucosa: No abnormalities detected.
- Buccal mucosa: Bilateral, symmetrical horizontal white lines (frictional hyperkeratosis).
- Gingivae: 5 mm x 3 mm soft, slate grey macule buccal of 45 (amalgam tattoo).
- Floor of mouth: Bilateral lingual tori.
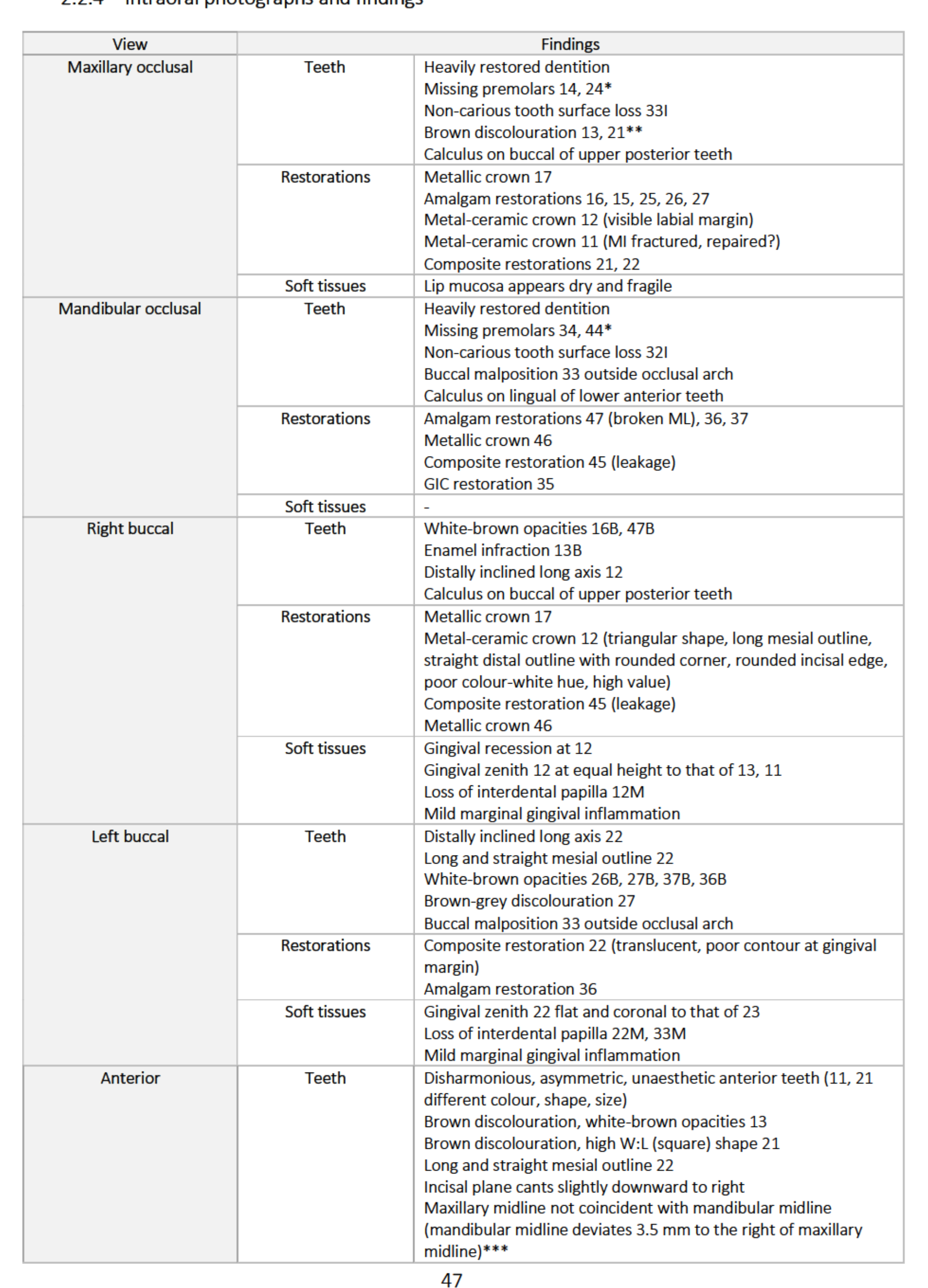
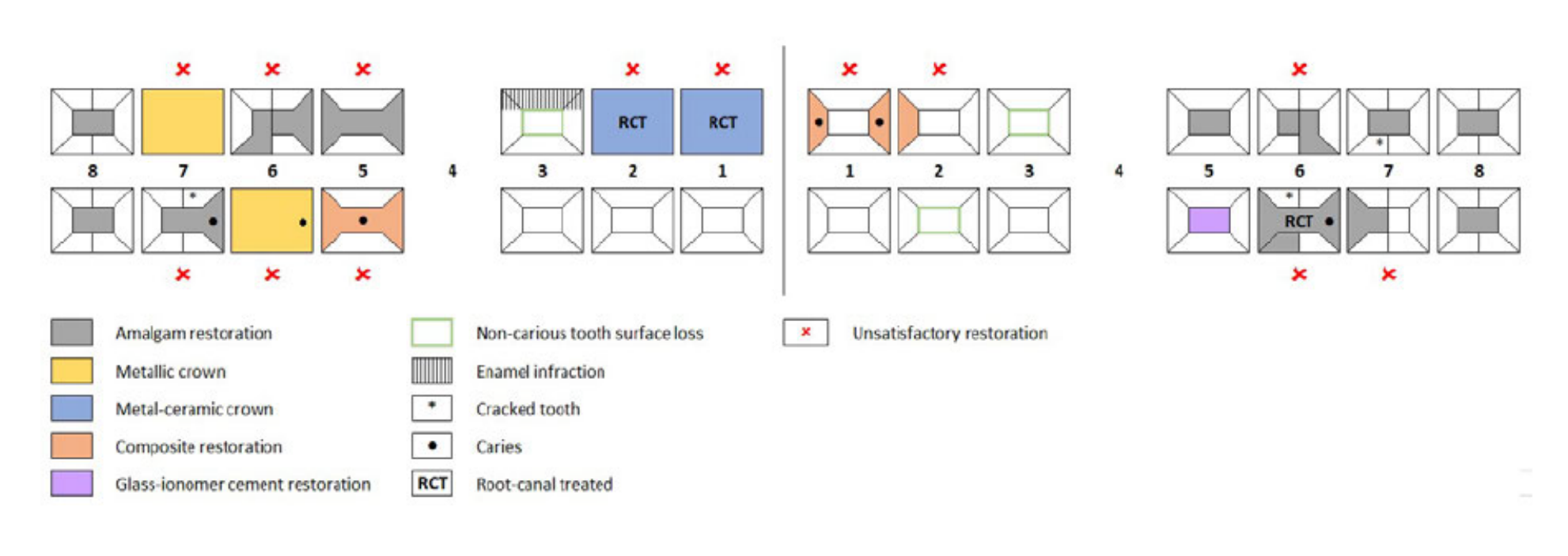
Intraoral Findings by Region44
Maxillary Occlusal
- Teeth: Heavily restored; missing 14, 24; tooth surface loss 33I; brown discolouration 13, 21; calculus on posterior buccal.
- Restorations: Metallic crown 17; Amalgams 16, 15, 25, 26, 27; Metal-ceramic crown 12 (visible margin) and 11 (fractured/repaired); Composites 21, 22.
Mandibular Occlusal
- Teeth: Heavily restored; missing 34, 44; tooth surface loss 32I; 33 buccally malposed; calculus on anterior lingual.
- Restorations: Amalgams 47 (broken ML), 36, 37; Metallic crown 46; Composite 45 (leakage); GIC 35.
Right Buccal
- Teeth: White-brown opacities 16B, 47B; Enamel infraction 13B; 12 distally inclined.
- Soft Tissues: Gingival recession at 12; mild marginal inflammation.
Left Buccal
- Teeth: 22 distally inclined; white-brown opacities 26B, 27B, 37B, 36B; 33 buccally malposed.
- Soft Tissues: Gingival zenith 22 flat and coronal to 23; loss of interdental papilla 22M, 33M.
Anterior
- Teeth: Disharmonious/asymmetric (11, 21 differ in colour, shape, size); 21 square shape; incisal plane cants downward to right.
- Midline: Mandibular midline deviates 3.5 mm to the right of maxillary midline.
Anterior Restorative and Soft Tissue Details45
Restorations
- 12 Crown: Metal-ceramic; visible margins; poor colour (white hue, high value).
- 11 Crown: Metal-ceramic; square shape; poor colour (white hue, high value).
- 21/22 Composites: Poor contour at gingival margins; 22 is translucent.
- Embrasures: Asymmetric (larger on left than right).
Soft Tissues
- Gingiva: Recession at 12; non-ideal gingival zenith 13-23; loss of interdental papilla 12-22.
- Discolouration: Gingival discolouration 12-11; mild marginal inflammation.
Clinical Notes
- Missing premolars suggest history of orthodontic extractions.
- Discolouration on 13/21 may be intrinsic or extrinsic (tea/coffee).
- Midline discrepancies are common post-orthodontics; thresholds for acceptability are approximately 2.92mm.
- Aesthetic gingival zenith for central incisors and canines should be apical to lateral incisors.
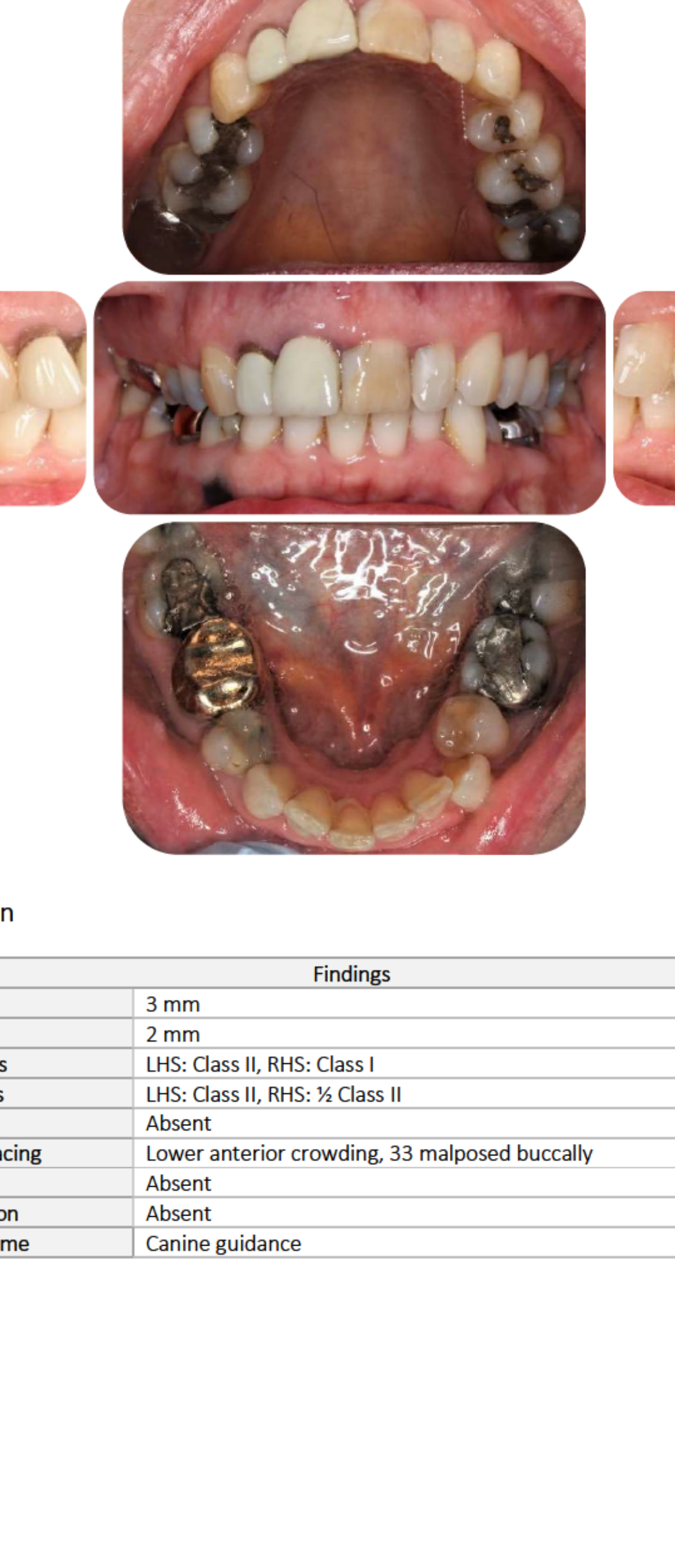
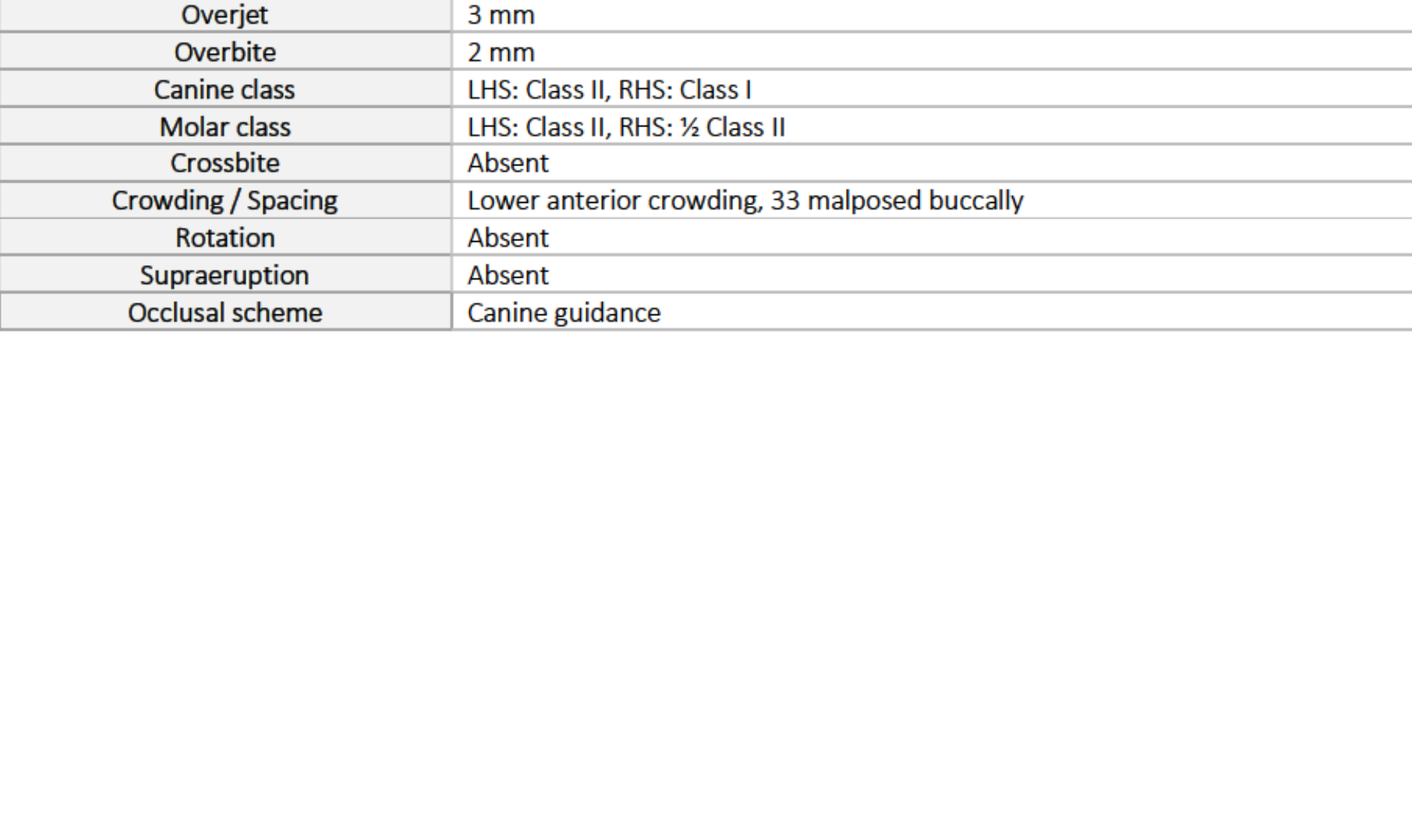
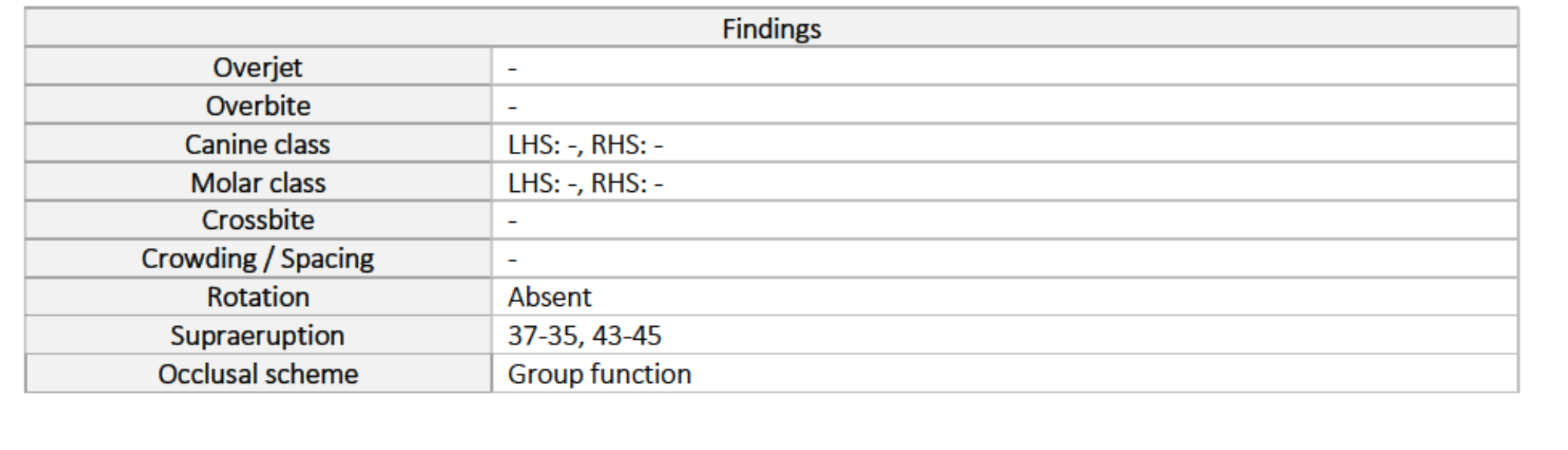
Occlusal Analysis46
| Parameter | Findings |
|---|---|
| Overjet | 3 mm |
| Overbite | 2 mm |
| Canine Class | LHS: Class II; RHS: Class I |
| Molar Class | LHS: Class II; RHS: ½ Class II |
| Crossbite | Absent |
| Crowding / Spacing | Lower anterior crowding; 33 malposed buccally |
| Occlusal Scheme | Canine guidance |
| Rotation / Supraeruption | Absent |
 |  |
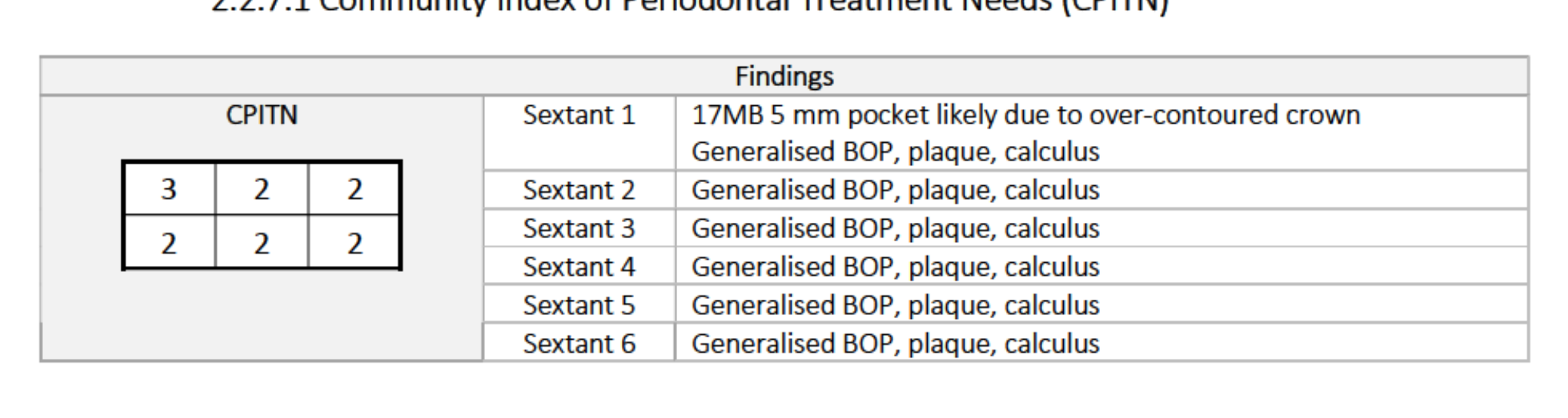
Periodontal Assessment47
CPITN Scores
- Sextant 1: 3 (17MB 5mm pocket due to over-contoured crown)
- Sextant 2: 2
- Sextant 3: 2
- Sextant 4: 2
- Sextant 5: 2
- Sextant 6: 2
- Generalised BOP, plaque, and calculus.
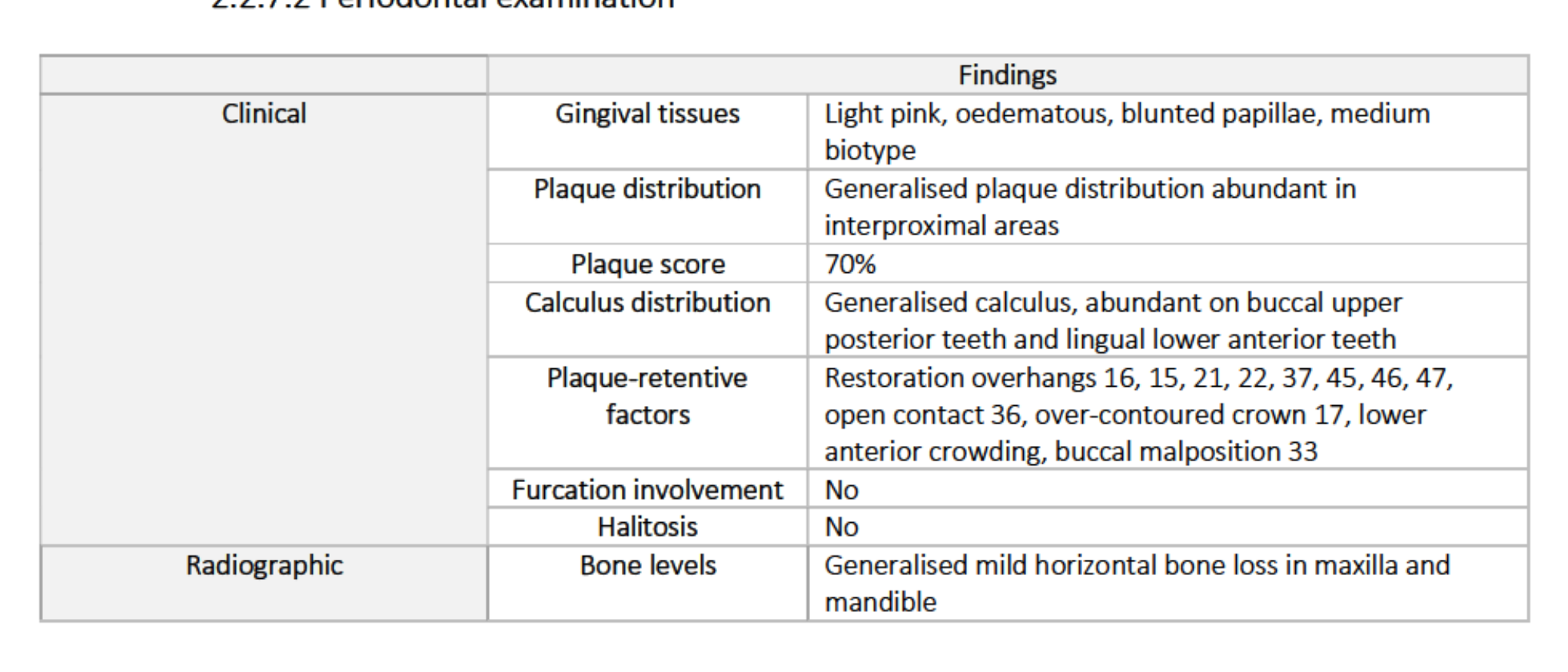
Clinical Findings
- Gingiva: Light pink, oedematous, blunted papillae, medium biotype.
- Plaque Score: 70% (abundant interproximally).
- Calculus: Generalised; abundant on upper posterior buccal and lower anterior lingual.
- Plaque-retentive factors: Overhangs (16, 15, 21, 22, 37, 45, 46, 47), open contact (36), over-contoured crown (17), crowding, and malposition (33).
- Radiographic: Generalised mild horizontal bone loss.
 |  |
 |
Periodontal Risk Assessment (PRA)48
- BOP%: 69%
- Sites with PPD ≥ 5mm: 1
- Bone Loss: Estimated 25% alveolar bone loss.
- Environmental: Former smoker.
- Overall Risk: Medium.
- Recall Interval: 6 Months.
 |  |
Pulp Sensibility Tests
- CO2 (Cold Test): Positive response for all teeth tested except 24 (missing) and 12/11 (RCT).
- EPT (Electric Pulp Test): Positive responses across dentition; 12 and 11 showed no response (consistent with RCT status).
Radiographic Findings: OPG49
- Mandible: Continuous cortices; two radiopaque spots on right body (amalgam tattoos).
- Maxilla: Normal density; radiopaque shadows in sinuses (superimposition of nasal conchae).
- Alveolar Processes: Generalised mild horizontal bone loss; no furcation involvement.
- Teeth: Heavily restored; endodontically treated (12, 11, 36); missing one premolar per quadrant; third molars present.
 |  |
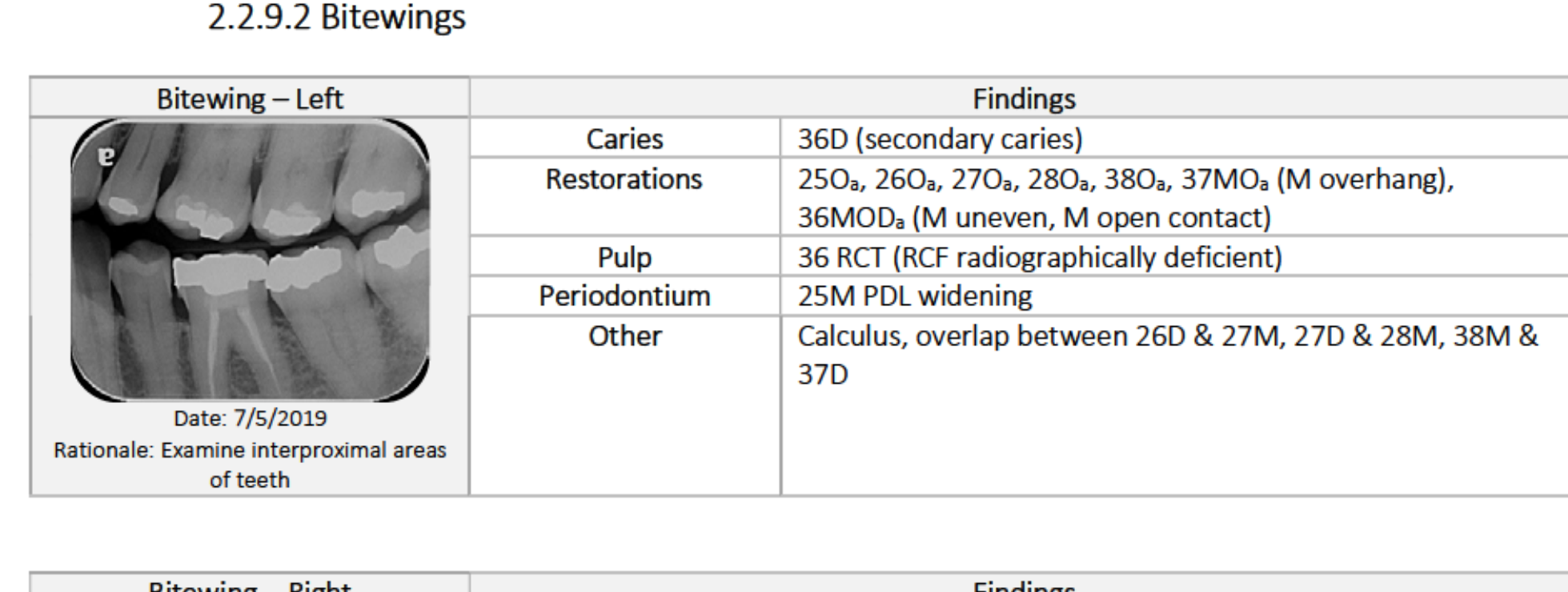
Bitewing Radiographs50
Left Side
- Caries: 36D (secondary).
- Restorations: Multiple amalgams; 37MO overhang; 36MOD open contact.
- Pulp: 36 RCT (radiographically deficient RCF).
- Periodontium: 25M PDL widening.
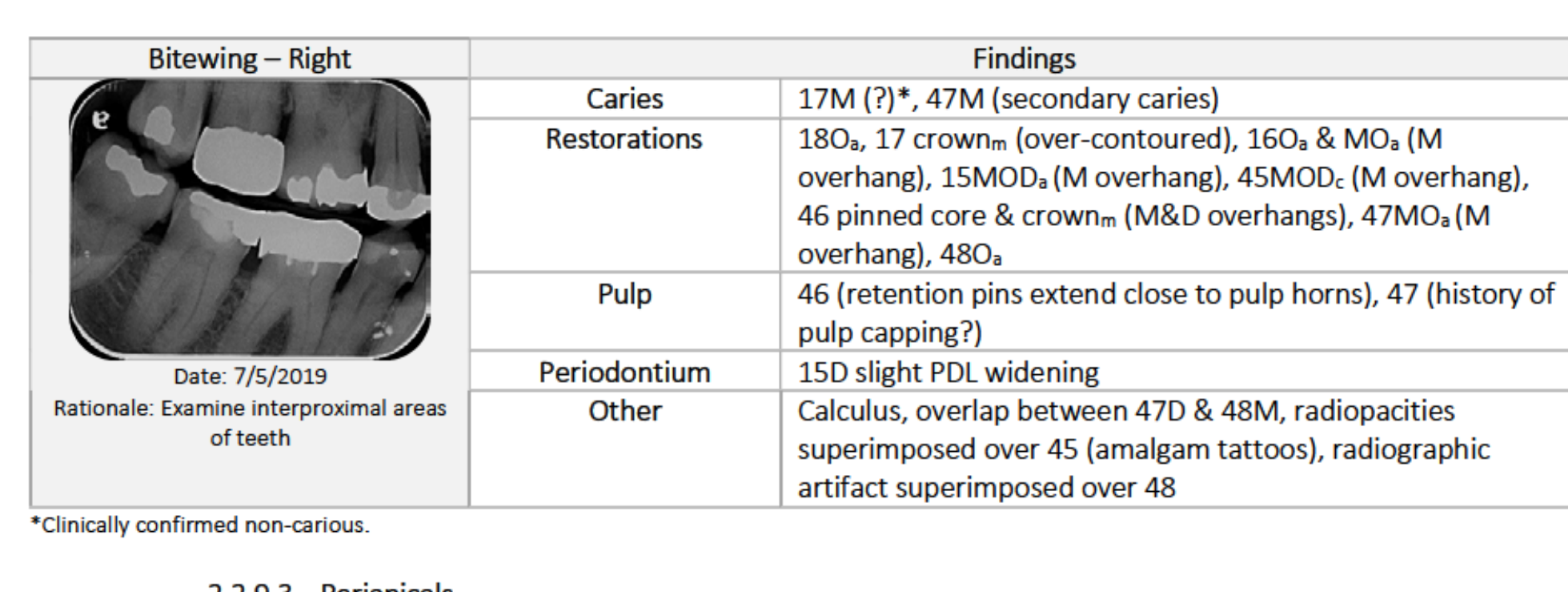
Right Side
- Caries: 47M (secondary).
- Restorations: 17 crown over-contoured; 16, 15, 45, 46, 47 all show overhangs.
- Pulp: 46 retention pins near pulp; 47 history of pulp capping.
 |  |
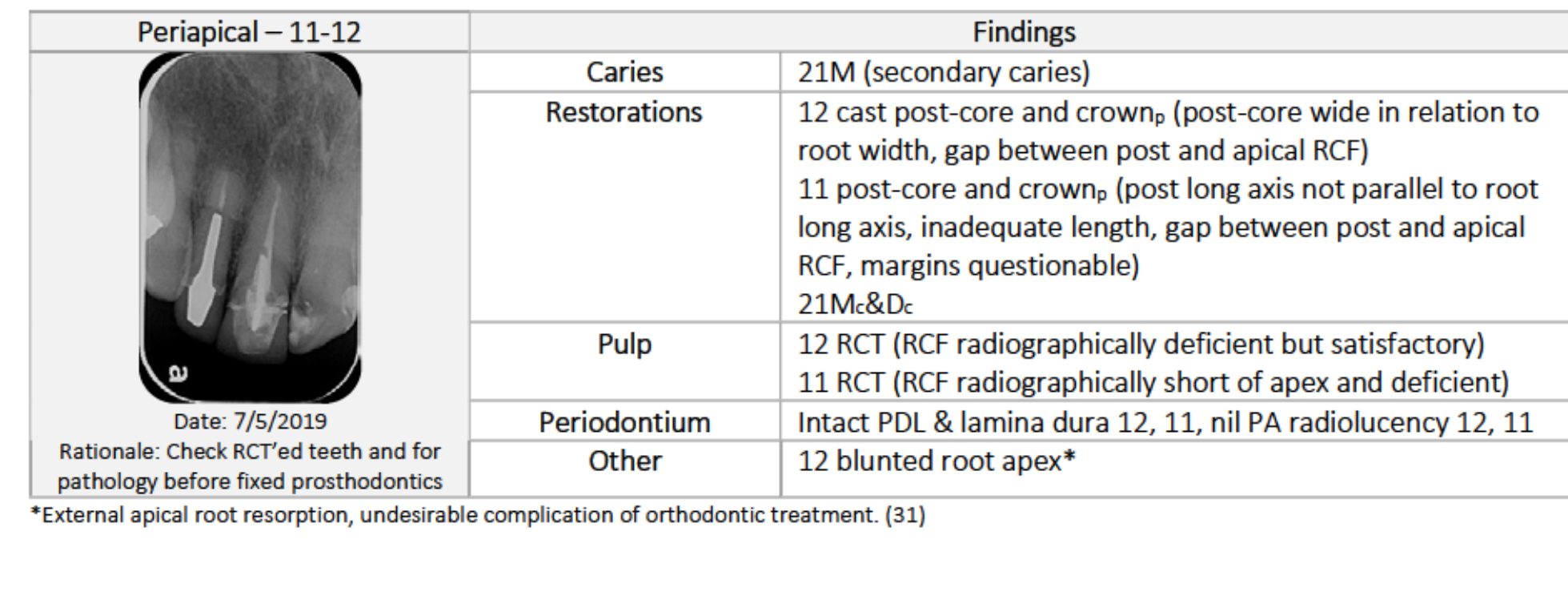 |
Periapical Radiographs: 11-12
- Caries: 21M (secondary).
- Restorations: 12 cast post-core (wide post); 11 post-core (short, non-parallel, gap to RCF).
- Pulp: 12 RCT (satisfactory); 11 RCT (short and deficient).
- Other: 12 shows blunted root apex (external apical root resorption from orthodontics).
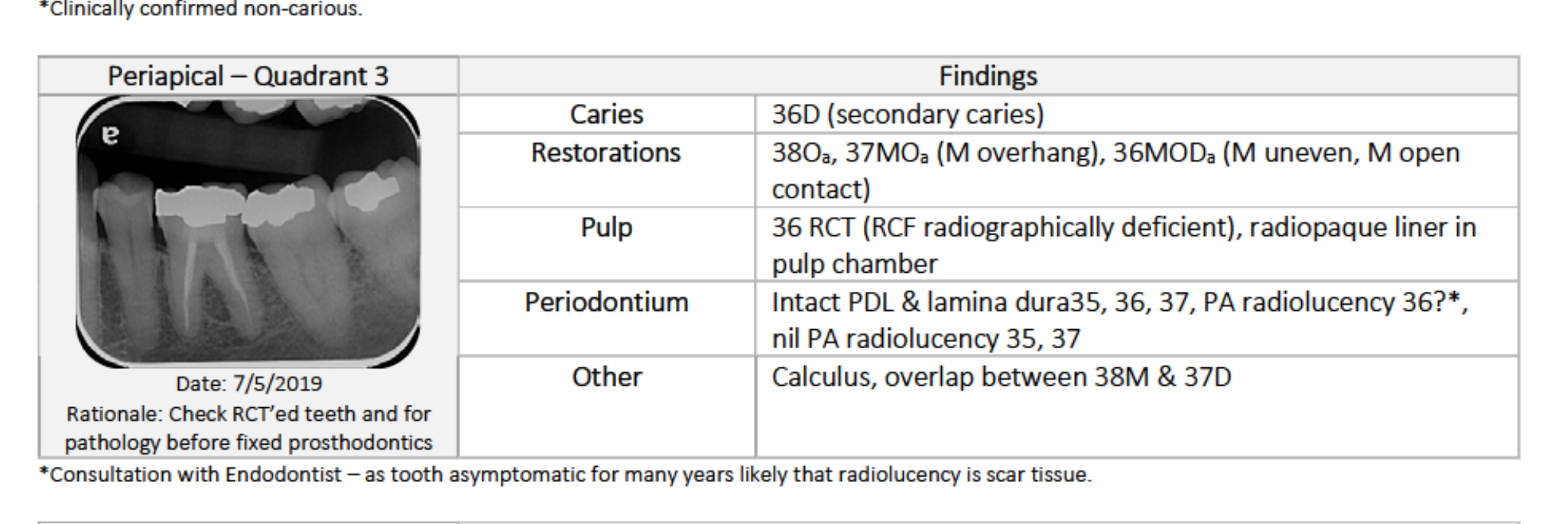
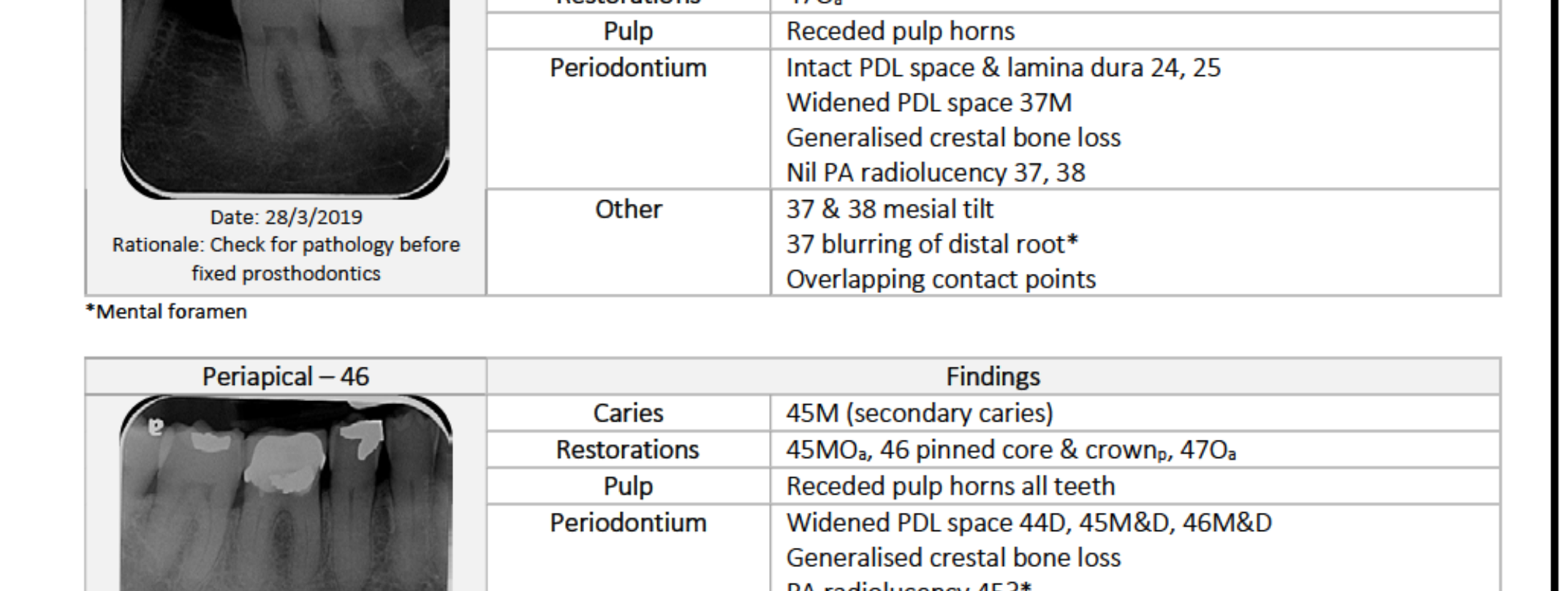
Periapical Radiographs: Quadrants 3 & 451
Quadrant 3 (35, 36, 37)
- Caries: 36D (secondary).
- Restorations: 37MO overhang; 36MOD open contact.
- Pulp: 36 RCT (deficient RCF); radiopaque liner present.
- Periodontium: Possible PA radiolucency at 36.
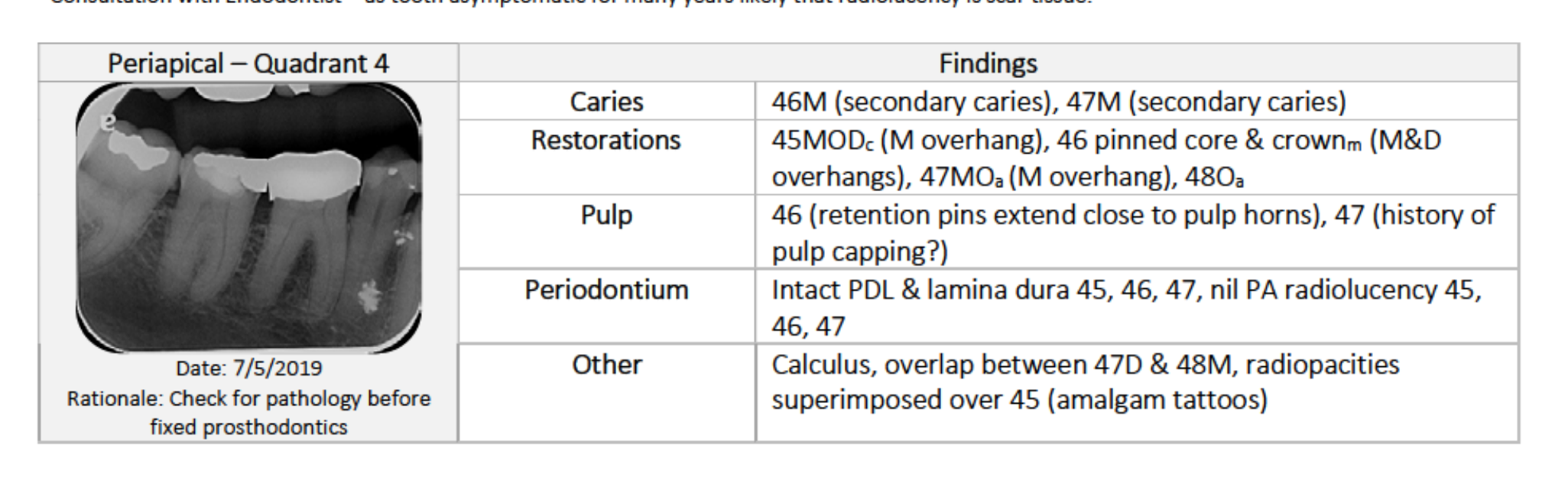
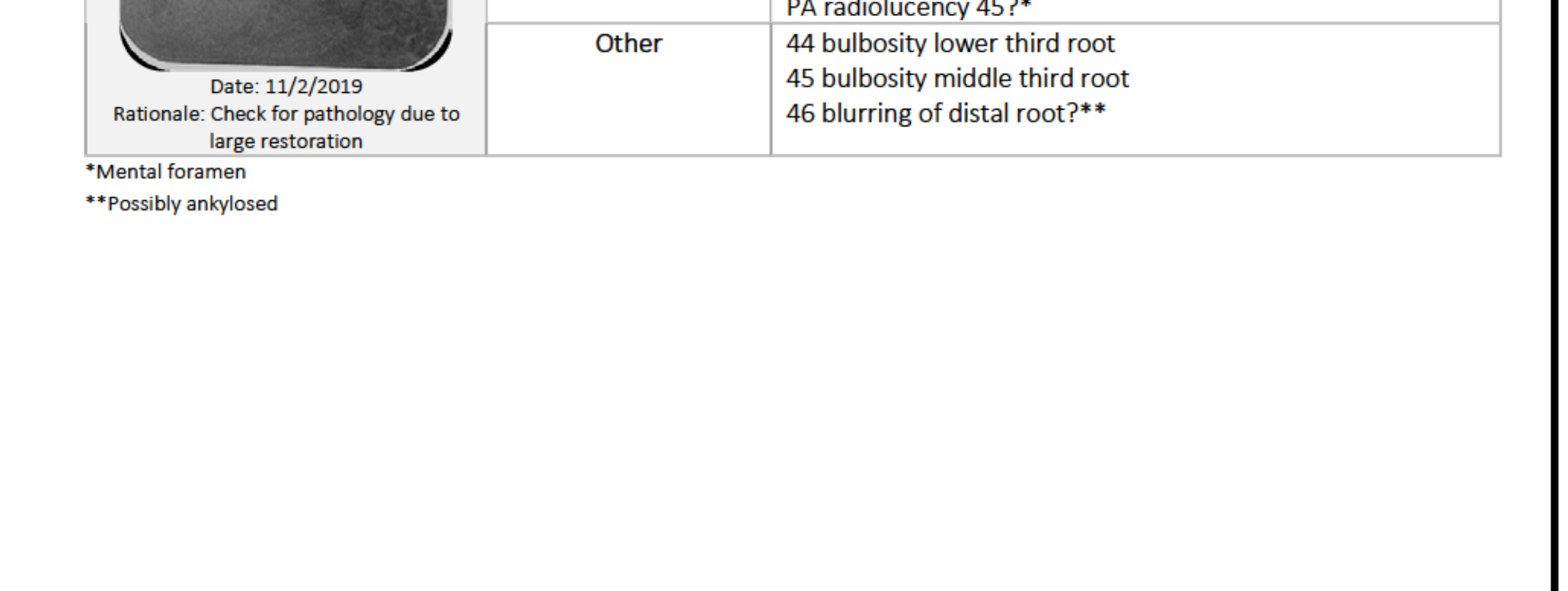
Quadrant 4 (45, 46, 47)
- Caries: 46M, 47M (secondary).
- Restorations: 45MOD, 46 crown, 47MO all show overhangs.
- Pulp: 46 retention pins near pulp horns.
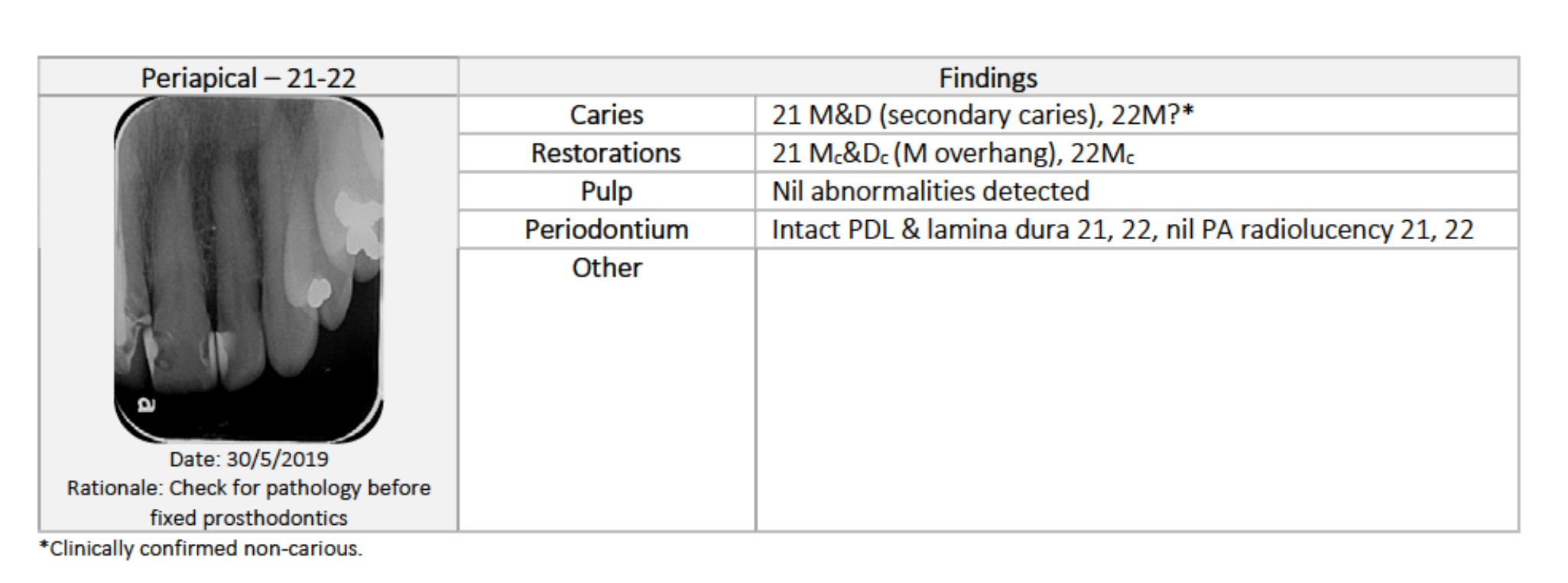
Teeth 21-22
- Caries: 21 M&D (secondary), 22M?.
- Restorations: 21 M overhang.
 |  |
 |
Caries Risk Assessment52
Dietary Assessment
- Low sugar and acid intake.
- Moderate fermentable carbohydrates.
- Limited snacking; lacking dairy.
Saliva Test
- Unstimulated: Low flow rate; sticky/frothy consistency; pH 5.0-5.8 (Low).
- Stimulated: Very low quantity (<3.5 mL at 5 mins); very low buffering capacity.
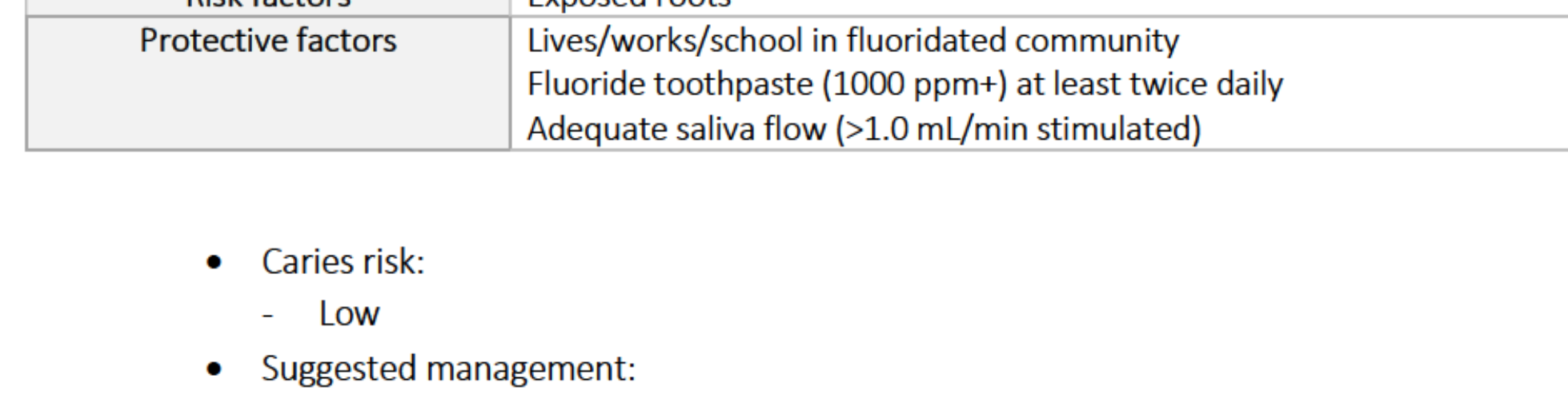
CAMBRA Analysis
- Indicators: Visible cavities and radiographic dentine penetration.
- Risk Factors: Visible heavy plaque.
- Protective Factors: Fluoridated community; fluoride toothpaste use; adequate stimulated flow (noted as factor despite test results).
Suggested Management (Moderate Risk)
- 1000 ppm fluoride toothpaste 2x daily.
- 0.05% NaF rinse 1x daily.
- Xylitol gum/candies 4x daily.
 |  |
Diagnoses And Problem List
Pathological Diagnoses53
- Caries: Multiple teeth with secondary caries.
- Restorations: Heavily restored; several unsatisfactory.
- Endodontic:
- 47: Chronic reversible pulpitis.
- 11, 12, 36: Previous RCT; no current signs of infection.
- Periodontal: Generalised Stage II Grade B unstable periodontitis.
- Oral Medicine: Actinic cheilitis; bilateral frictional keratosis; amalgam tattoo (45).
- Other: Tooth surface loss (13I, 23I, 32I); cracked teeth (27, 36, 47).
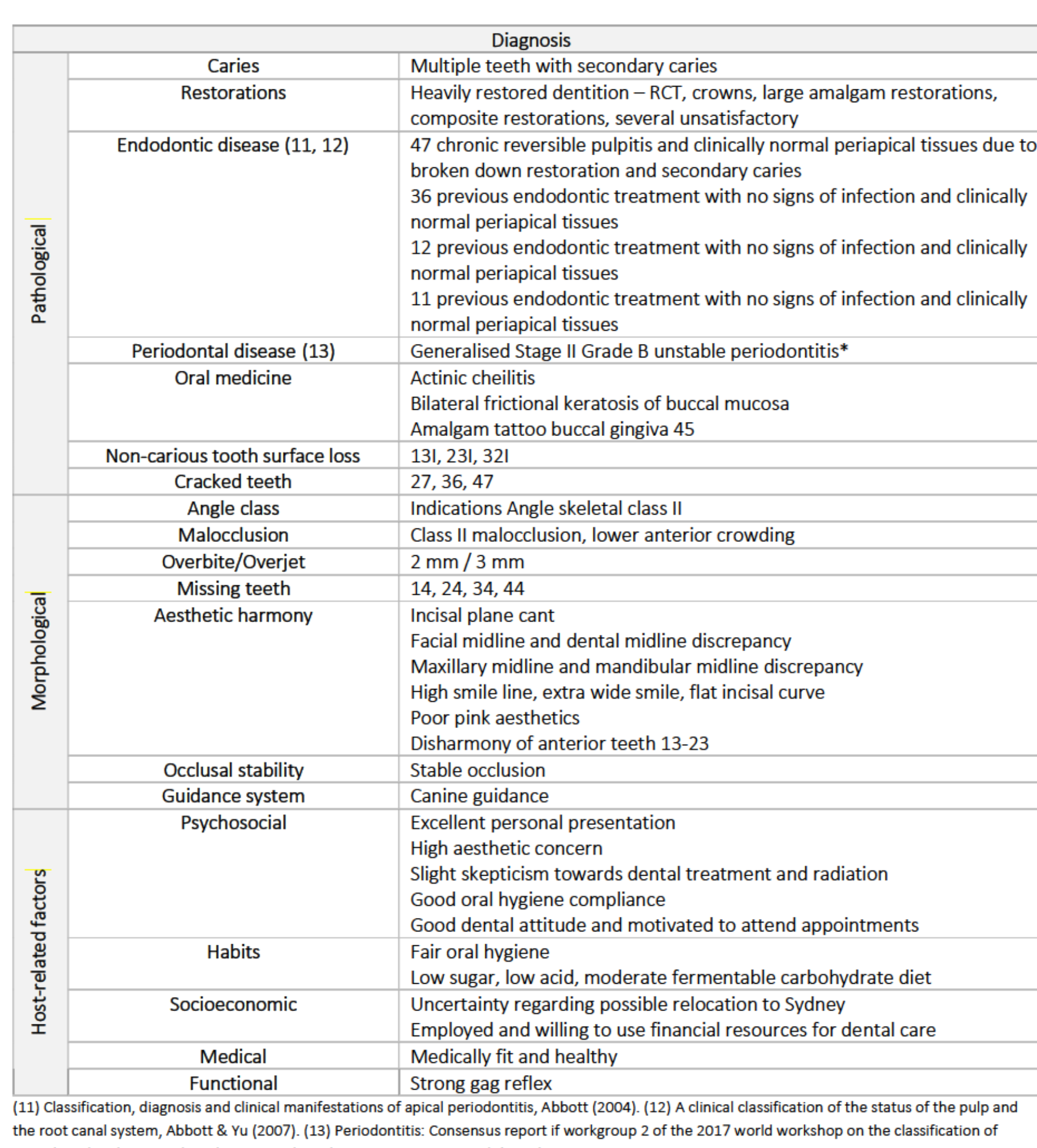
Morphological & Aesthetic Diagnoses
- Malocclusion: Class II skeletal/dental profile; lower anterior crowding.
- Aesthetics: Incisal plane cant; midline discrepancies; high smile line; poor pink aesthetics; disharmony of 13-23.
- Stability: Stable occlusion; canine guidance.
Host-Related Factors
- Psychosocial: High aesthetic concern; slight skepticism/apprehension; good compliance.
- Socioeconomic: Potential relocation to Sydney; employed.
- Functional: Strong gag reflex.
Problem List54
- Pulpal: Reversible pulpitis 47.
- Periodontal: Generalised Stage II Grade B unstable periodontitis.
- Aesthetic:
- Asymmetrical anterior teeth 13-23.
- Discoloured teeth 13, 21; non-ideal colour 11, 12, 21, 22.
- Non-ideal size/shape/contours 12, 21, 22.
- Asymmetric incisal embrasures.
- Pink aesthetics: High smile line, recession, loss of papillae, gingival discolouration 12-11.
- Restorative/Endodontic:
- Questionable RCF: 11, 12, 36.
- Multiple furcation involvements (26, 16, 36, 46).
- Patient Factors: Strong gag reflex; uncertainty regarding relocation to Sydney.
Prognosis
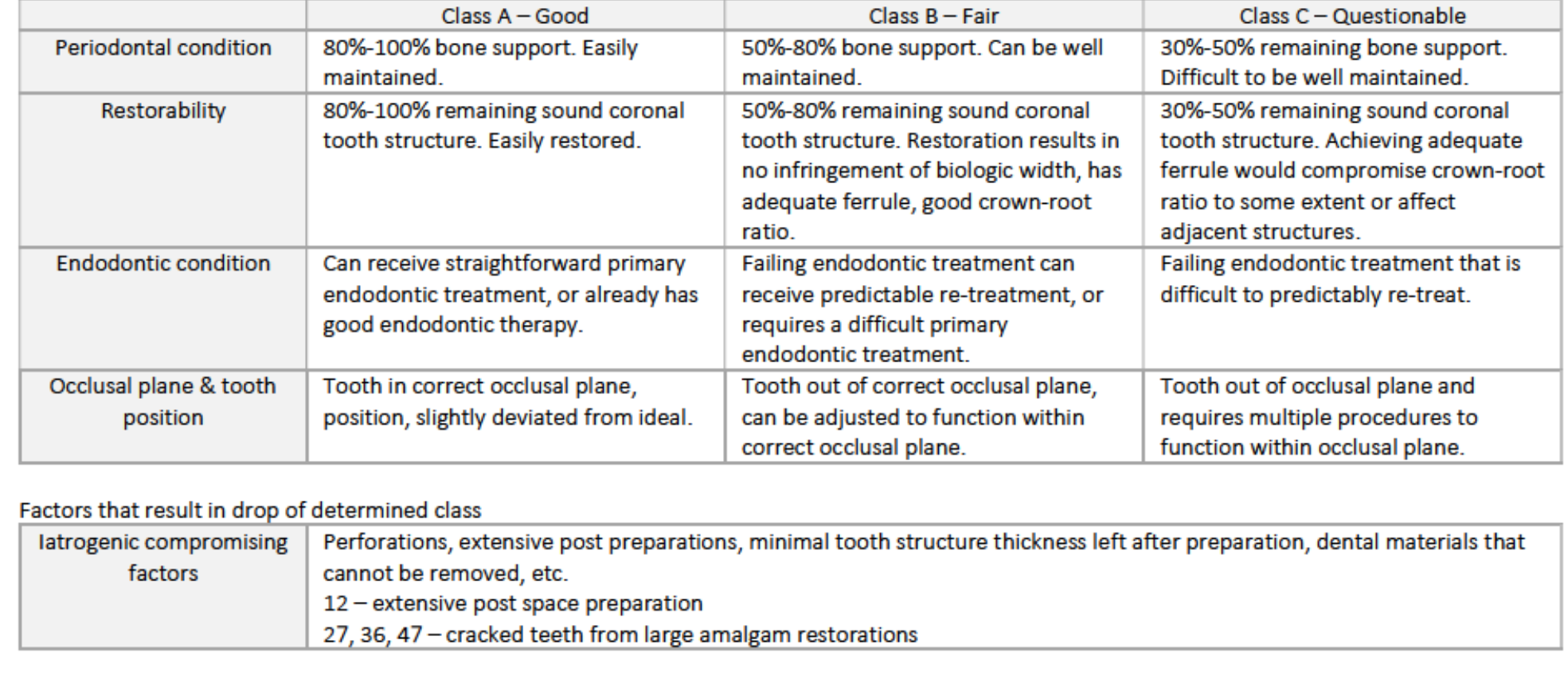
Individual Tooth Prognosis Criteria55
- Class A (Good): 80-100% bone support; 80-100% sound structure; straightforward endodontics; correct position.
- Class B (Fair): 50-80% bone support; 50-80% sound structure (adequate ferrule); predictable re-treatment.
- Class C (Questionable): 30-50% bone support; 30-50% sound structure (compromised ferrule/ratio); difficult re-treatment.
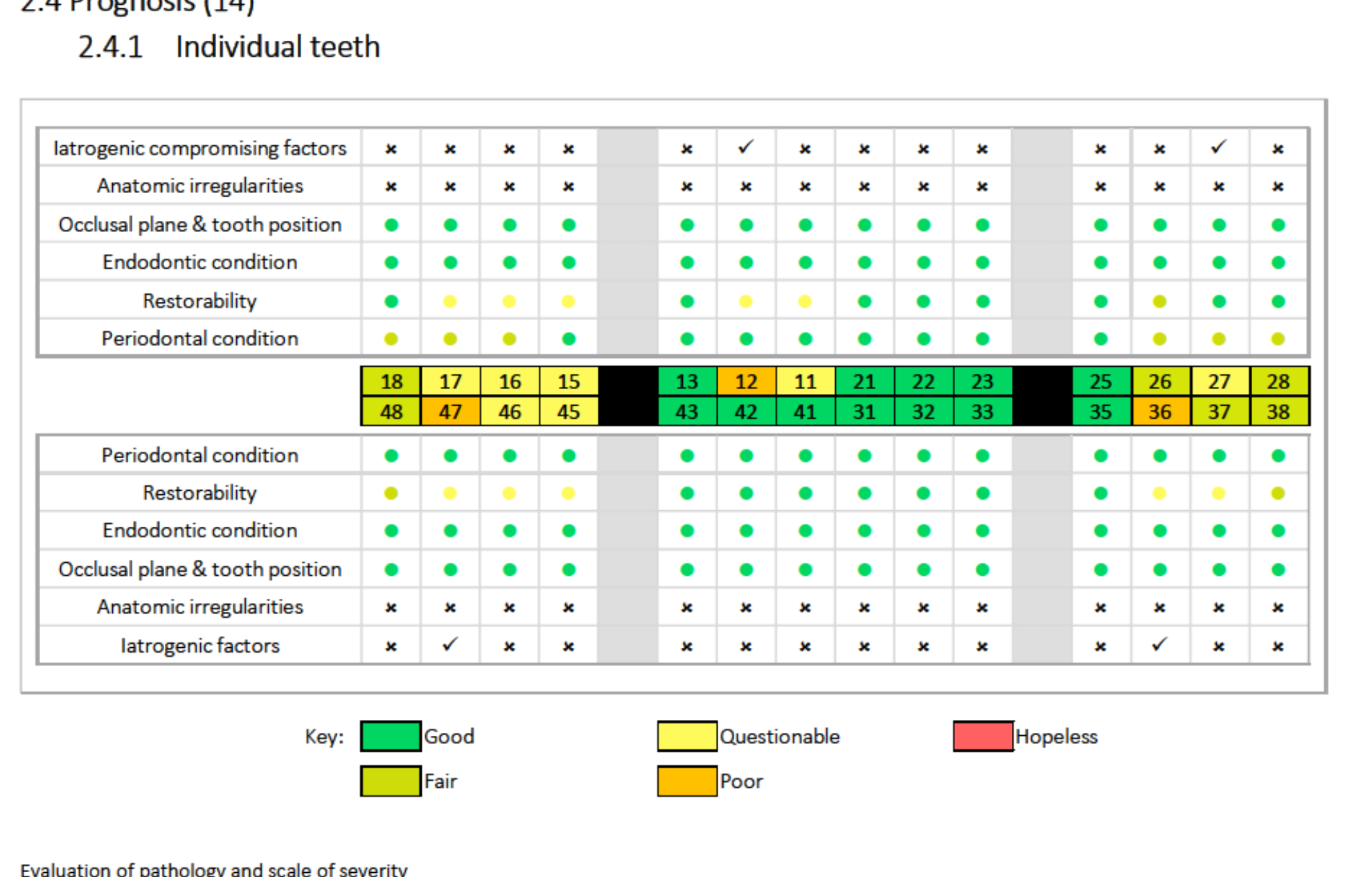 |  |
 |
Compromising Factors
- 12: Extensive post space preparation (lowers prognosis).
- 27, 36, 47: Cracked teeth from large amalgams (lowers prognosis).
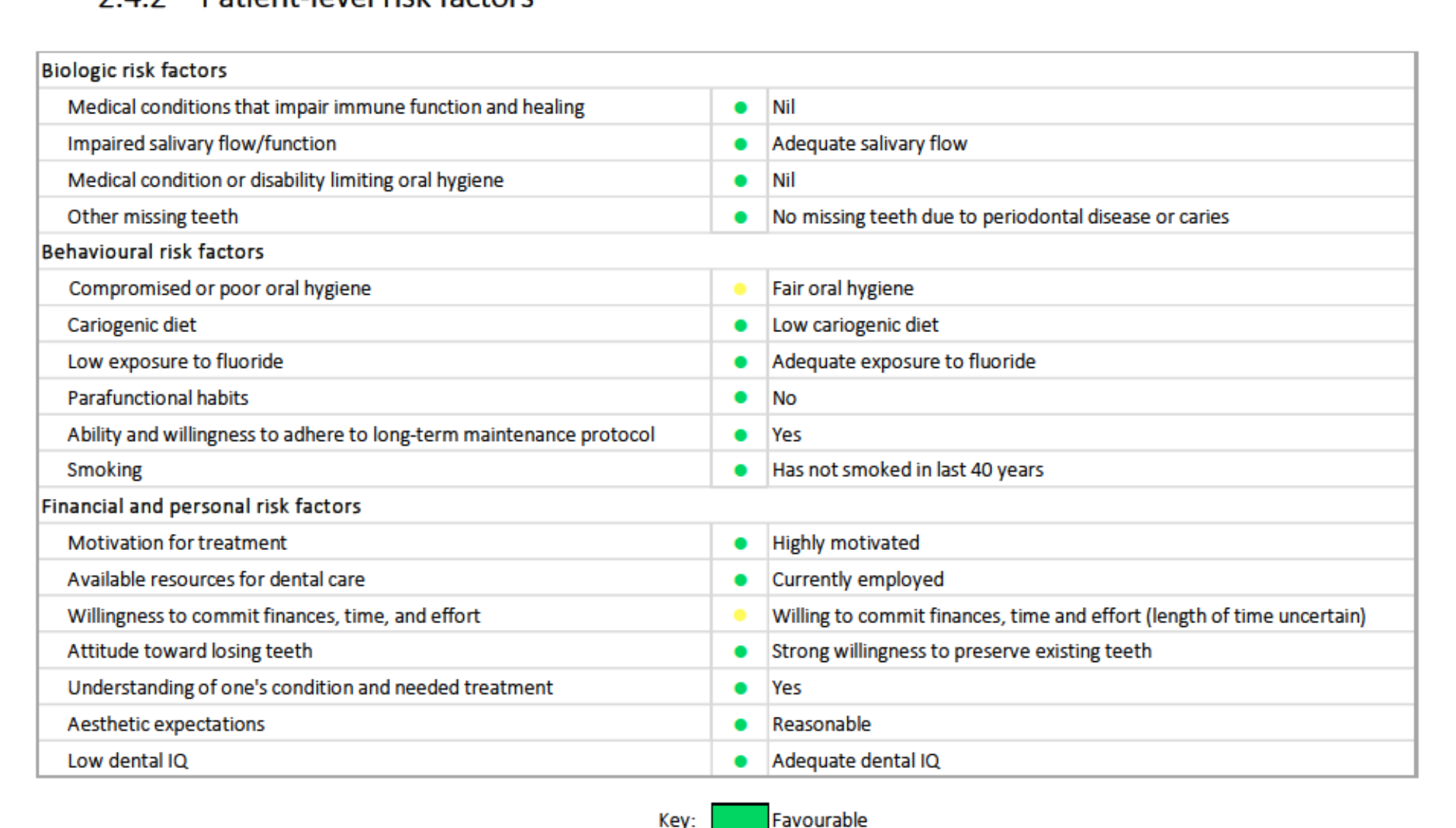
Patient-Level Risk Factors56
- Biologic: Favourable (adequate flow, no systemic impairment).
- Behavioural: Favourable (low cariogenic diet, motivated, non-smoker for 40 years).
- Financial/Personal: Questionable (uncertainty regarding relocation timeframes).
Overall Dentition Prognosis
- Favourable factors: Stable occlusal plane; sound periodontal health for most teeth; unremarkable medical history; high motivation.
- Unfavourable factors: History of extensive posterior restorations; skepticism/apprehension; relocation uncertainty.
- Risk of No Treatment: Progression of caries to pulpal infection; further deterioration of aesthetics leading to decreased quality of life.
Treatment Options57
Posterior Teeth
Tooth 47 (Pulpitis/Crack/Unsat. Restoration)
- Option 1: No treatment. (Risk: Ongoing pain, caries progression, tooth loss).
- Option 2 (Selected): Remove caries/restoration, endodontic assessment, assess restorability, temporise, and restore. (Rationale: Addresses complaint, prevents further breakdown).
Tooth 46 & 45 (Unsat. Restorations/Caries)
- Option 1: No treatment. (Risk: Plaque trap, infection).
- Option 2 (Selected): Remove caries and restore. (Rationale: Eliminate plaque trap, preserve tooth).
Tooth 36 (Unsat. Restoration/Crack/Questionable RCT)
- Option 1: No treatment. (Risk: Extraction eventually).
- Option 3 (Selected): Endodontic assessment, restorability assessment, endodontic re-treatment, and restore. (Rationale: More predictable outcome than just restoring).
Posterior & Lower Anterior
Tooth 37 (Unsat. Restoration/Overhang)
- Option 2 (Selected): Polish restoration. (Rationale: Conservative; eliminates plaque trap).
Tooth 27 (Cracked Tooth - Asymptomatic)
- Option 1 (Selected): No treatment and monitor. (Rationale: Investigation could render tooth unrestorable; currently asymptomatic).
Tooth 22 (Unsat. Restoration/Poor Aesthetics)
- Option 3 (Selected): Restore. (Rationale: Addresses presenting complaint; recontouring alone insufficient).
Upper Anterior
Tooth 21 (Unsat. Restoration/Caries/Aesthetics)
- Option 2 (Selected): Composite veneer. (Rationale: Conservative attempt before invasive crown; serves as a mock-up).
Tooth 11 (Unsat. Crown/Post/Questionable RCT)
- Option 3 (Selected): Endodontic re-treatment and full coverage crown. (Rationale: Controls RCT quality; provides satisfactory support for restoration).
Tooth 12 (Unsat. Crown/Wide Post/Questionable RCT)
- Option 2 (Selected): Full coverage crown without endodontic re-treatment. (Rationale: Post is biomechanically sound; removal carries high risk of catastrophic root fracture).
Tooth 13 (Extrinsic Staining)
- Option 2 (Selected): External bleaching. (Rationale: Addresses aesthetic complaint).
63
Management Plan5859
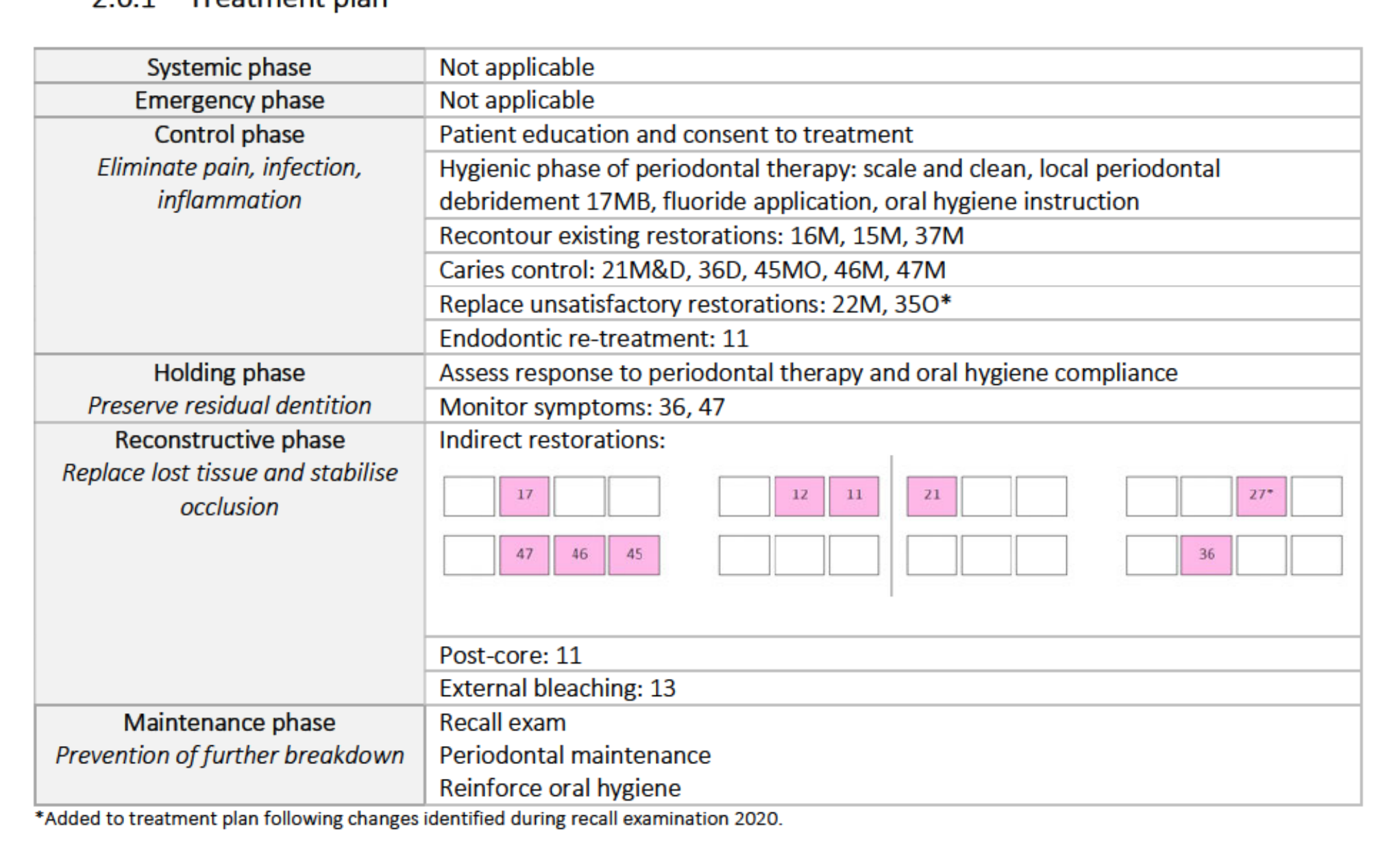
Management Plan Phases60
Control Phase
- Patient education and consent.
- Periodontal therapy: Scale and clean, local debridement (17MB), fluoride, OHI.
- Recontouring: 16M, 15M, 37M.
- Caries control: 21M&D, 36D, 45MO, 46M, 47M.
- Replace restorations: 22M, 35O.
- Endodontic re-treatment: 11.
Holding Phase
- Assess periodontal response and OHI compliance.
- Monitor symptoms: 36, 47.
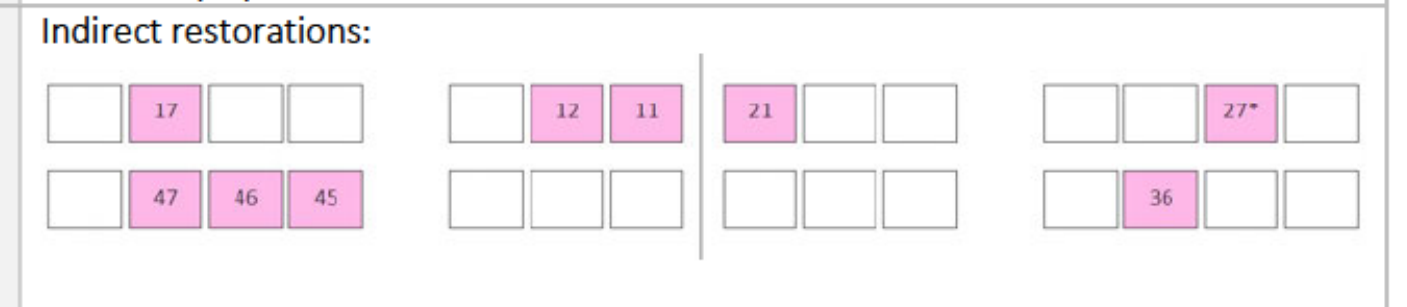
Reconstructive Phase
- Indirect restorations (crowns/onlays).
- Post-core: 11.
- External bleaching: 13.
Maintenance Phase
- Recall exams, periodontal maintenance, and OHI reinforcement.
 |  |
Treatment Sequencing and Constraints61
- Relocation Risk: Discussed risks of incomplete complex treatment (e.g., dislodged interim restorations, root canal infection) due to potential move to Sydney.
- Sequence Strategy:
- Quadrant 4 then Quadrant 3 (Lower arch first).
- Upper anterior then upper posterior.
- Aesthetic Timing: Treatment of the aesthetic region was delayed until adequate rapport was established.
66
67
Treatment Delivery62636465
January 2020 Review
- Recall Findings: Restored teeth asymptomatic; 27B crack noted; 35O GIC crumbling. Plan amended to include 27 investigation and 35 composite restoration.
- Timeline Update: Patient confirmed potential relocation for May 2020. Goal set to finish upper anterior reconstructive phase by March.
- Tooth 21: Caries/restoration removed; replaced with composite. Decision made to eventually use a zirconia crown for definitive aesthetics.
- Tooth 22: Subgingival caries removed; temporised with GIC for 6 weeks to allow gingival healing before composite replacement.
69
70
71
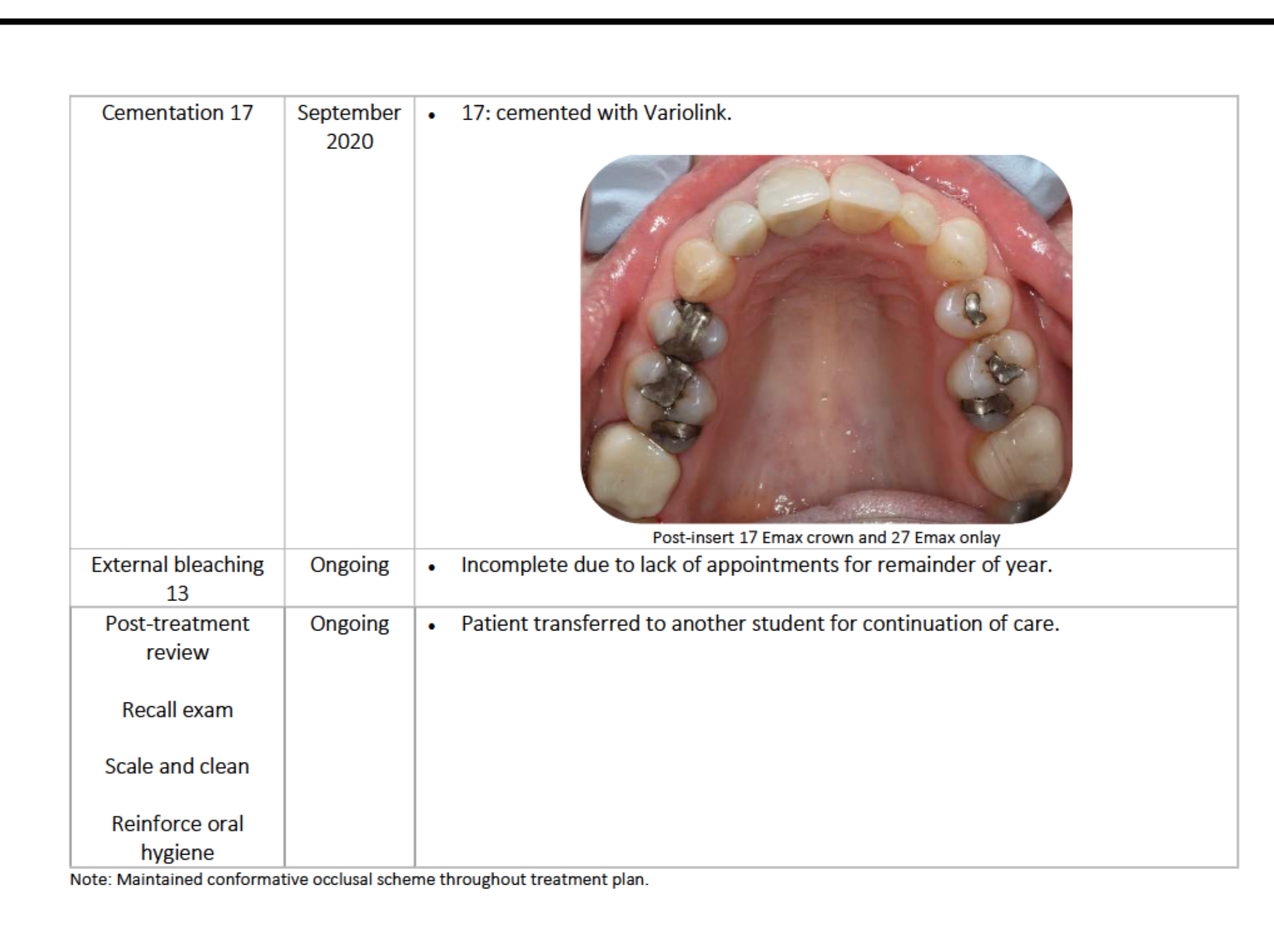
Final Procedures and Status66
- September 2020: 17 cemented with Variolink.
- Indirect Restorations: Post-insert review for 17 Emax crown and 27 Emax onlay.
- Incomplete Treatment: External bleaching of 13 was not completed due to lack of appointments.
- Transfer of Care: Patient transferred to another student for ongoing maintenance and recall exams.
- Occlusion: Maintained conformative occlusal scheme throughout.
73
 |  |
Clinical Outcomes And Reflection
Patient Response to Treatment67
- Satisfaction: Patient very satisfied; stated, “I can smile again – I can’t stop smiling!”
- Resolution of Complaints:
- 12-21 indirect restorations addressed aesthetic concerns (13 incomplete).
- 11 endodontic re-treatment and new crown addressed fear of crown falling off.
- 47 investigation and restoration resolved sensitivity to sweets.
- Compliance: Patient became highly compliant despite initial apprehension; never missed an appointment.
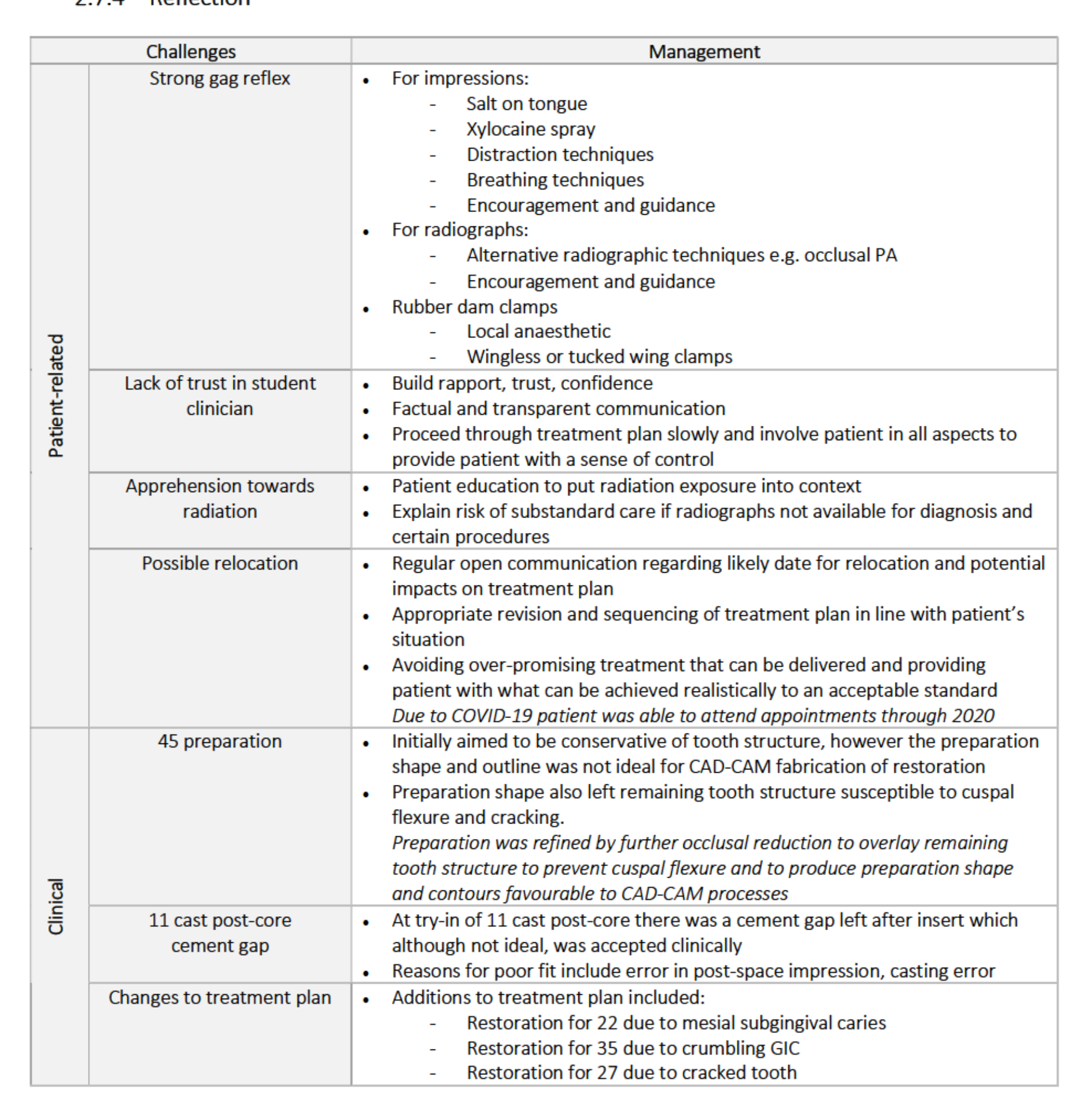
Clinical Reflection68
Patient Management Challenges
- Strong Gag Reflex: Managed with salt on tongue, Xylocaine spray, distraction, and specific rubber dam clamping techniques.
- Lack of Trust: Addressed by building rapport through transparent communication and proceeding slowly.
- Radiation Apprehension: Managed through patient education on risk vs. benefit.
- Relocation: Sequencing was adjusted; COVID-19 ultimately allowed the patient to stay for the full 2020 treatment period.
Clinical Challenges
- 45 Preparation: Refined to overlay tooth structure to prevent cuspal flexure and suit CAD-CAM fabrication.
- 11 Cast Post-Core: A cement gap was accepted clinically; likely due to impression or casting error.
- Plan Changes: Added 22 (subgingival caries), 35 (crumbling GIC), and 27 (crack) to the active plan.
Case 3: Removable Aesthetic69
The Patient7071
Patient Details72
- 82-year-old male

Presenting Complaints
Presented in July 2020 for initial examination with the following complaints:
- “My fillings (21, 22) have broken off.”
- “I have a missing tooth (11) that bothers me.”
History of Presenting Complaints
- Tooth 22 restored with pinned composite in July 2020.
- Tooth 21 restored with pinned composite twice (July and August 2020).
- Tooth 11 has been missing for some time.
Medical History and Medications73
| Medication/Supplementation | Dose | Mechanism of Action / Indication | Dental Implications |
|---|---|---|---|
| Uremide (Furosemide) | 40 mg q.d. | Loop diuretic; inhibits sodium/chloride reabsorption. For oedema and hypertension. | May increase ototoxic/nephrotoxic potential of aminoglycosides/cephalosporins. NSAIDs may reduce antihypertensive effect. |
| Multivitamin | - | Dietary supplement. | Nil. |
| Garlic | - | Dietary supplement. | May inhibit platelet aggregation and increase bleeding risk. |
| Horseradish | - | Dietary supplement. | Nil. |
| Vitamin C complex | - | Dietary supplement. | Nil. |
 |  |
 |
Allergies and Social Habits
- Allergies: No known allergies.
- Alcohol: 1 standard drink per week. (Raises risk of oral cavity cancer).
- Tobacco: N/A.
Dental History and Attitude
- History:
- Regular attendance at OHCWA.
- Previous Co-Cr partial upper dentures were made but not worn due to poor fit.
- Transferred from another DMD student in July 2020.
- Attitude:
- High aesthetic motivation; concerned about broken front teeth.
- No functional issues reported; chews slowly on posterior teeth.
- Motivated; uses public transport for all appointments.
Oral Hygiene
- Status: Poor.
- Routine: Manual toothbrush and fluoride toothpaste twice daily.
- Adjuncts: No interproximal cleaning aids or other adjuncts used.
Social History
- Retired.
- Spends time reading poetry, farming, and maintaining light aircraft.
Examination And Diagnostics
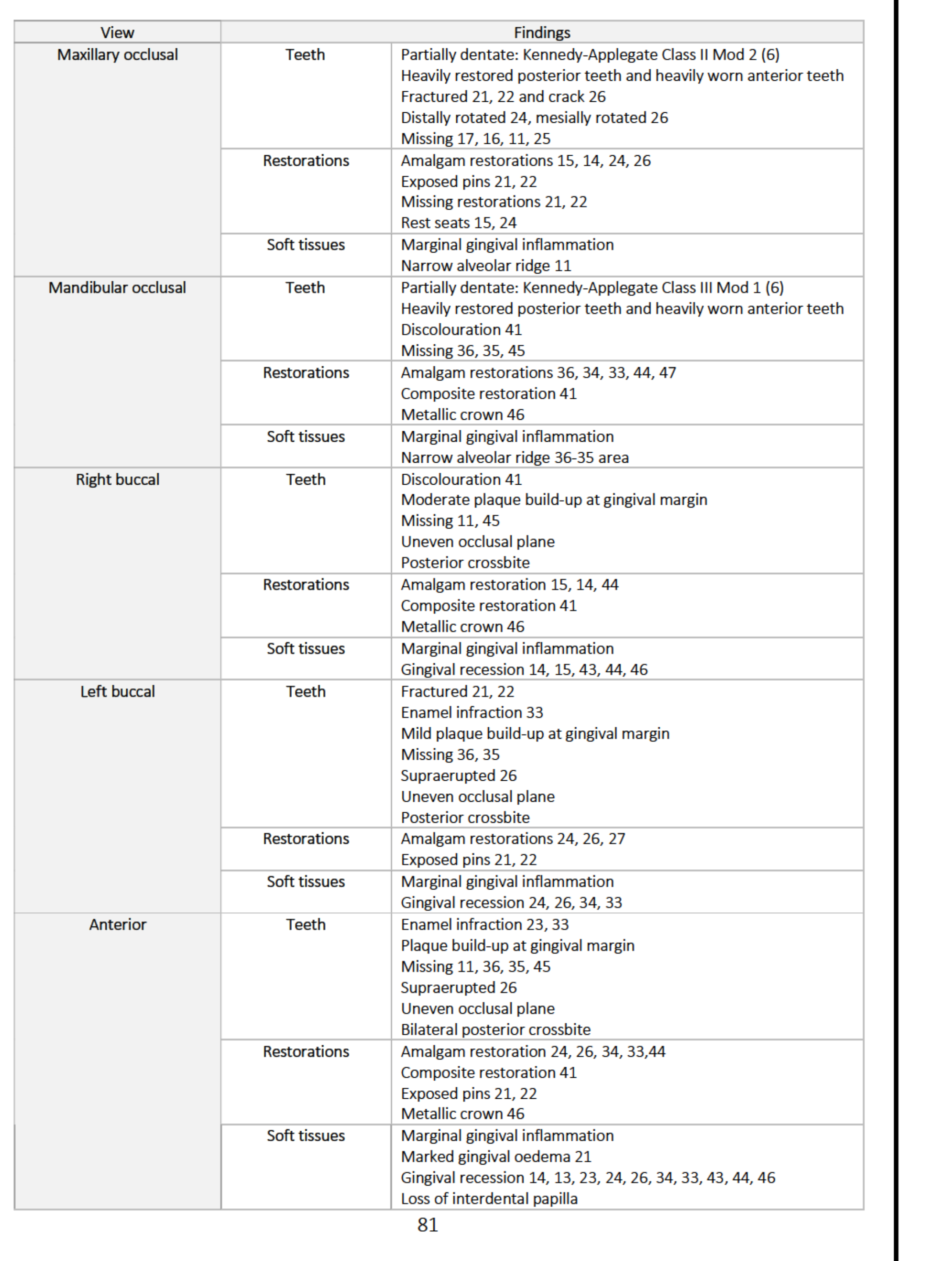
Intraoral Findings7475
| View | Category | Findings |
|---|---|---|
| Maxillary Occlusal | Teeth | Kennedy-Applegate Class II Mod 2. Heavily restored posterior/worn anterior teeth. Fractured 21, 22; crack 26. Rotated 24, 26. Missing 17, 16, 11, 25. |
| Restorations | Amalgam 15, 14, 24, 26. Exposed pins and missing restorations 21, 22. Rest seats 15, 24. | |
| Soft Tissues | Marginal gingival inflammation. Narrow alveolar ridge 11. | |
| Mandibular Occlusal | Teeth | Kennedy-Applegate Class III Mod 1. Heavily restored/worn teeth. Discolouration 41. Missing 36, 35, 45. |
| Restorations | Amalgam 36, 34, 33, 44, 47. Composite 41. Metallic crown 46. | |
| Soft Tissues | Marginal gingival inflammation. Narrow alveolar ridge 36-35. | |
| Right Buccal | Teeth | Discolouration 41. Moderate plaque. Missing 11, 45. Uneven occlusal plane. Posterior crossbite. |
| Restorations | Amalgam 15, 14, 44. Composite 41. Metallic crown 46. | |
| Soft Tissues | Marginal gingival inflammation. Recession 14, 15, 43, 44, 46. | |
| Left Buccal | Teeth | Fractured 21, 22. Enamel infraction 33. Mild plaque. Missing 36, 35. Supraerupted 26. Uneven occlusal plane. Posterior crossbite. |
| Restorations | Amalgam 24, 26, 27. Exposed pins 21, 22. | |
| Soft Tissues | Marginal gingival inflammation. Recession 24, 26, 34, 33. | |
| Anterior | Teeth | Enamel infraction 23, 33. Plaque at margin. Missing 11, 36, 35, 45. Supraerupted 26. Uneven occlusal plane. Bilateral posterior crossbite. |
| Restorations | Amalgam 24, 26, 34, 33, 44. Composite 41. Exposed pins 21, 22. Metallic crown 46. | |
| Soft Tissues | Marginal gingival inflammation. Marked oedema 21. Recession 14, 13, 23, 24, 26, 34, 33, 43, 44, 46. Loss of interdental papilla. |
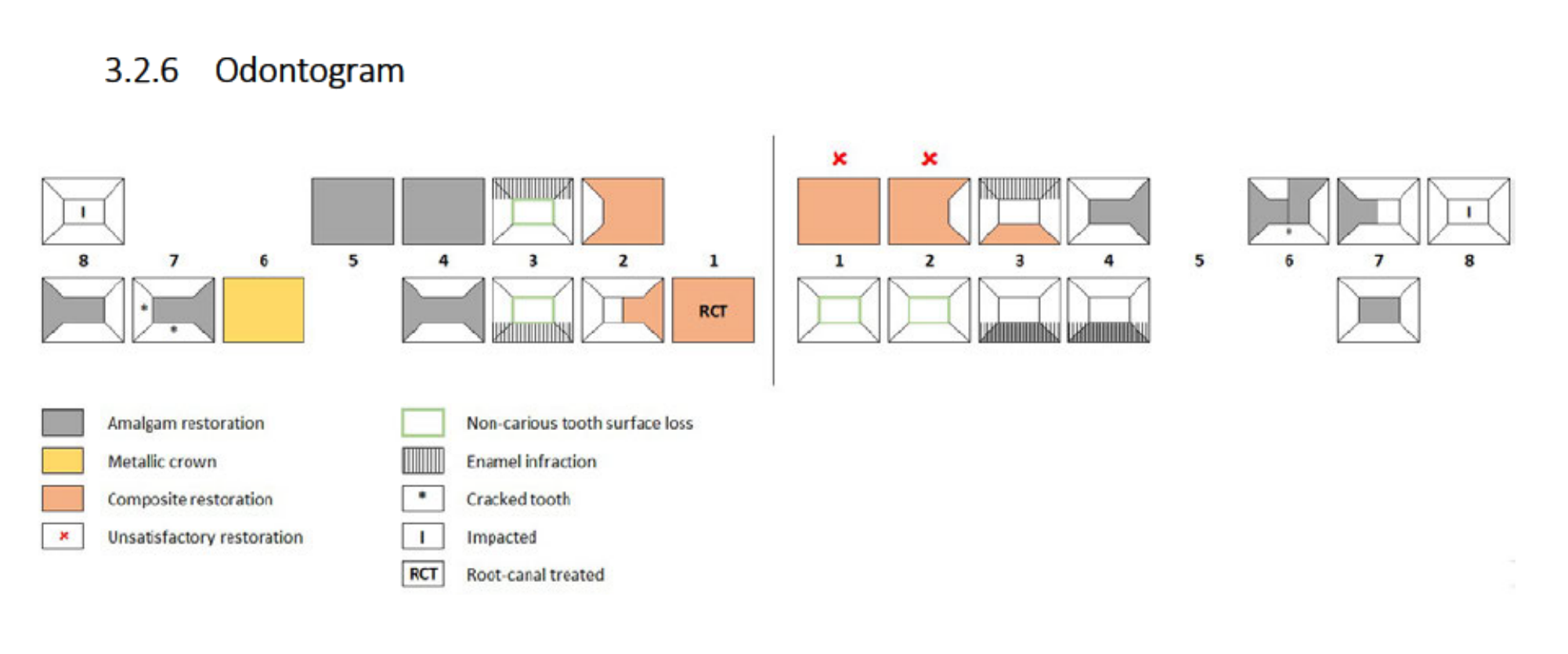
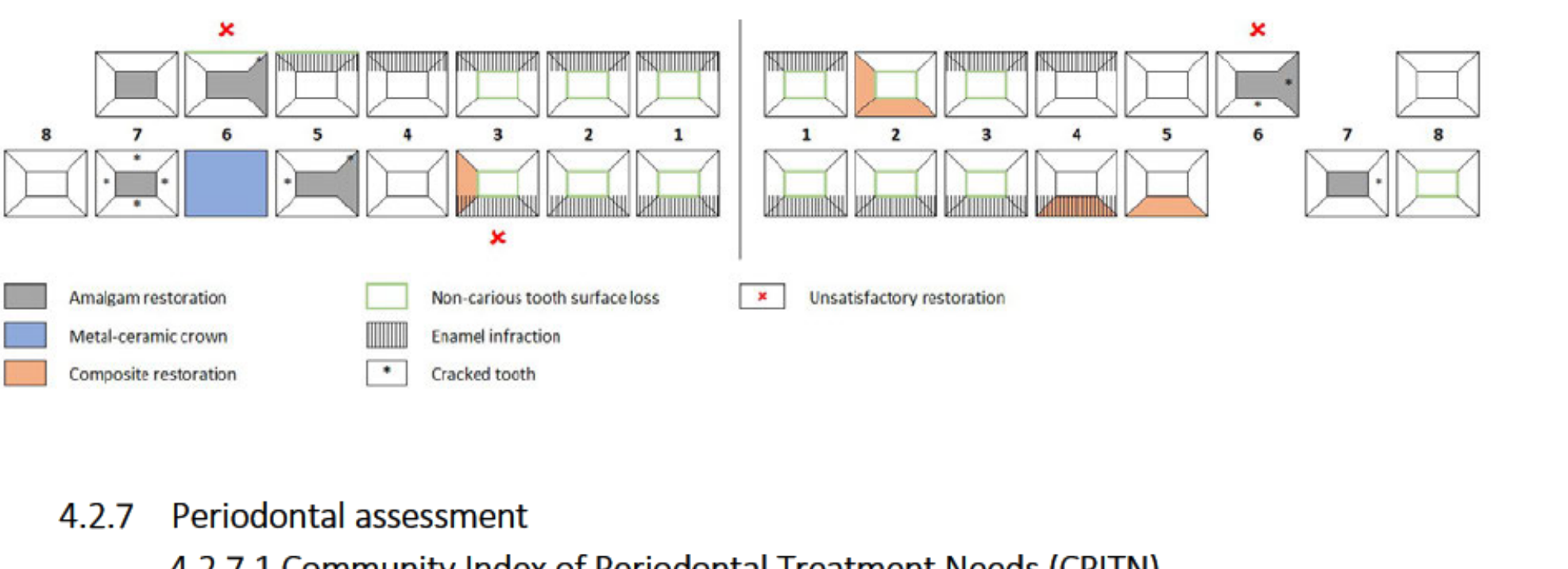
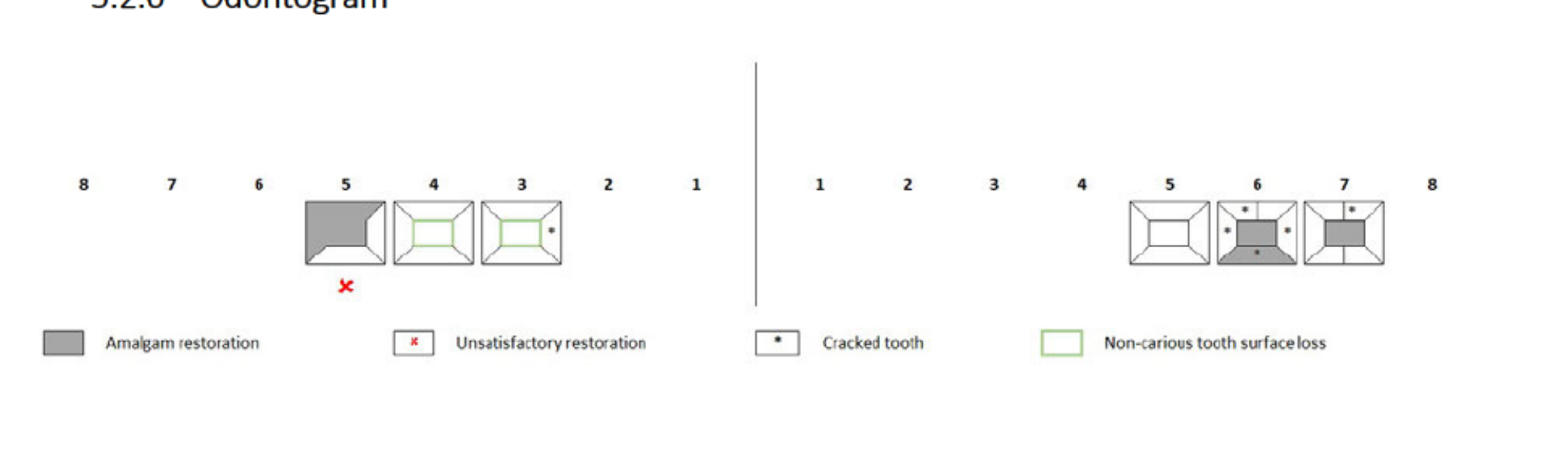
Odontogram Legend76
- Amalgam restoration
- Metallic crown
- Composite restoration
- Unsatisfactory restoration
- Non-carious tooth surface loss
- Enamel infraction
- Cracked tooth
- Impacted
- Root-canal treated (RCT)
 |  |
 |
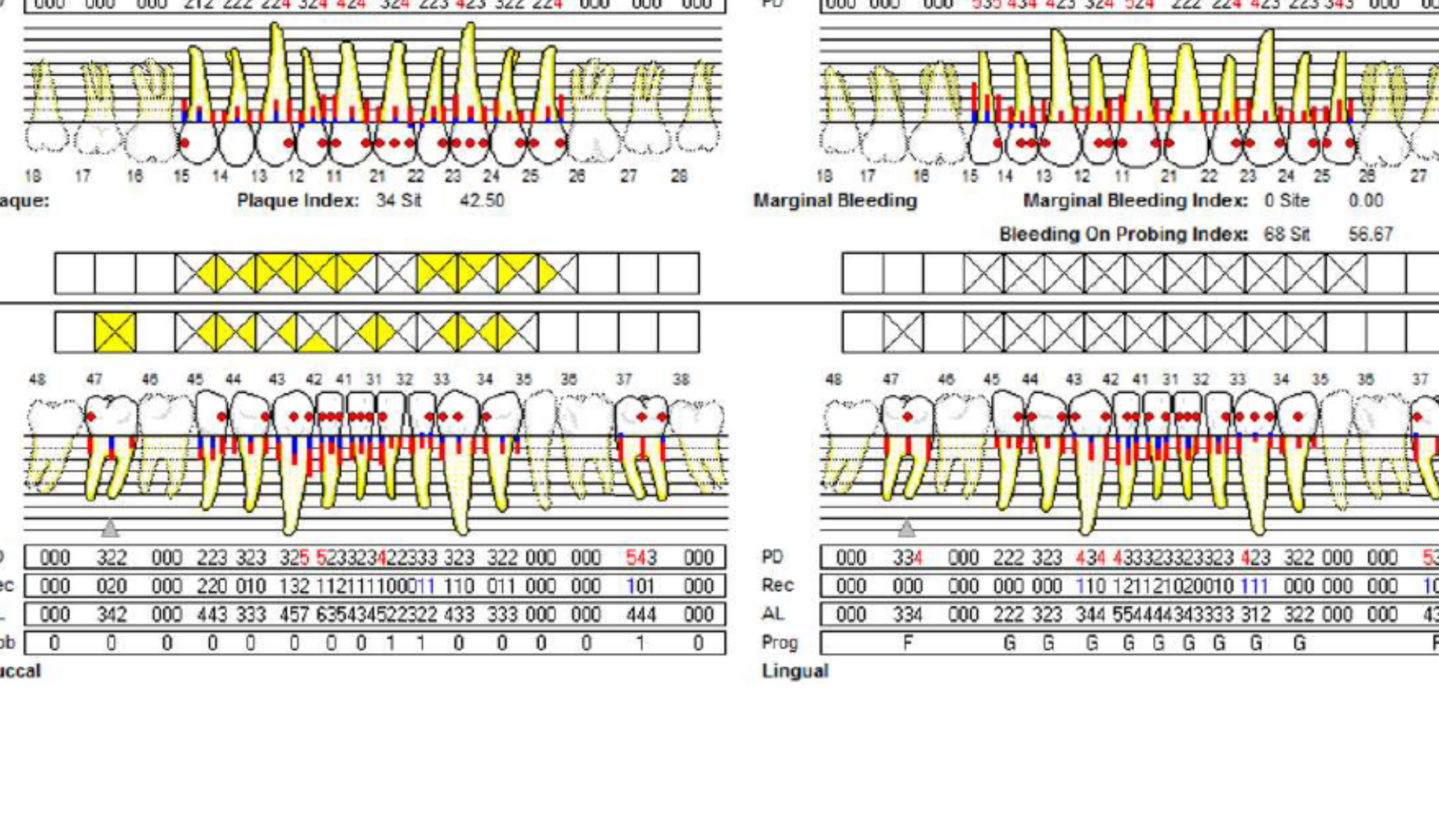
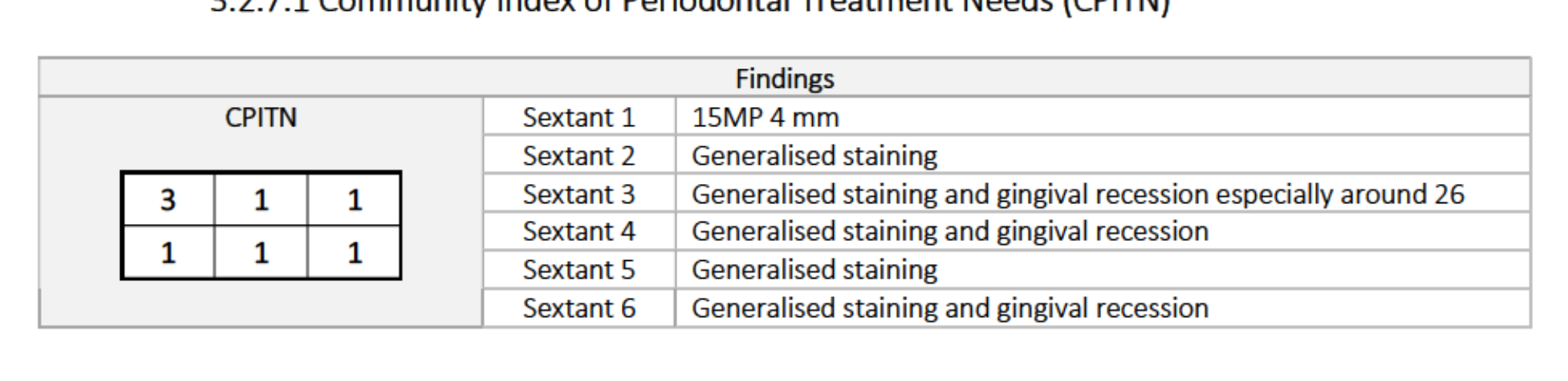
Periodontal Assessment
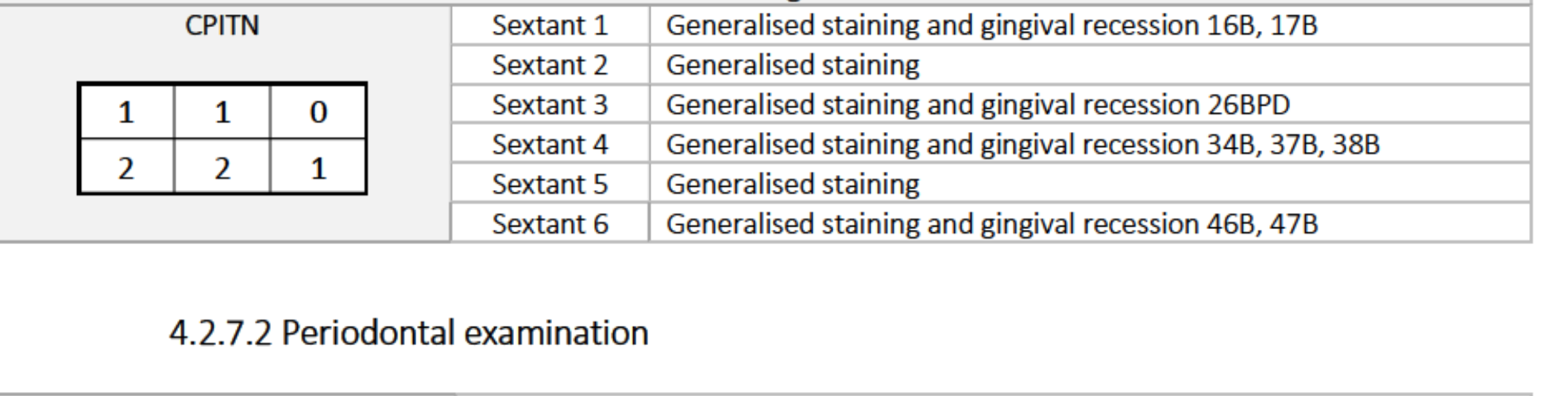
Community Index of Periodontal Treatment Needs (CPITN)
- Sextant 1: 15MP 4 mm
- Sextant 2: Generalised staining
- Sextant 3: Generalised staining and recession (especially 26)
- Sextant 4: Generalised staining and recession
- Sextant 5: Generalised staining
- Sextant 6: Generalised staining and recession
CPITN Scores:
| 3 | 1 | 1 |
|---|---|---|
| 1 | 1 | 1 |
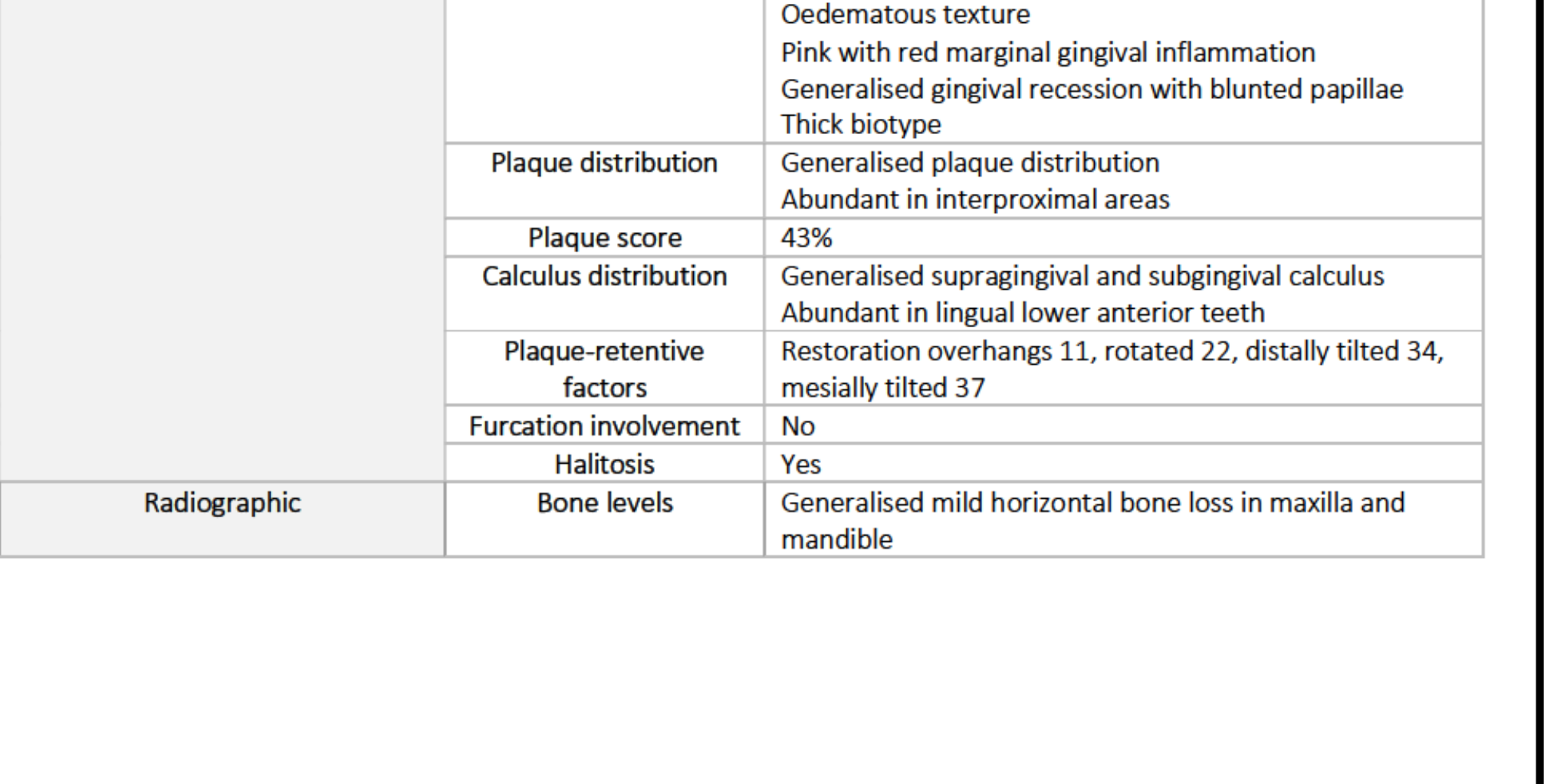
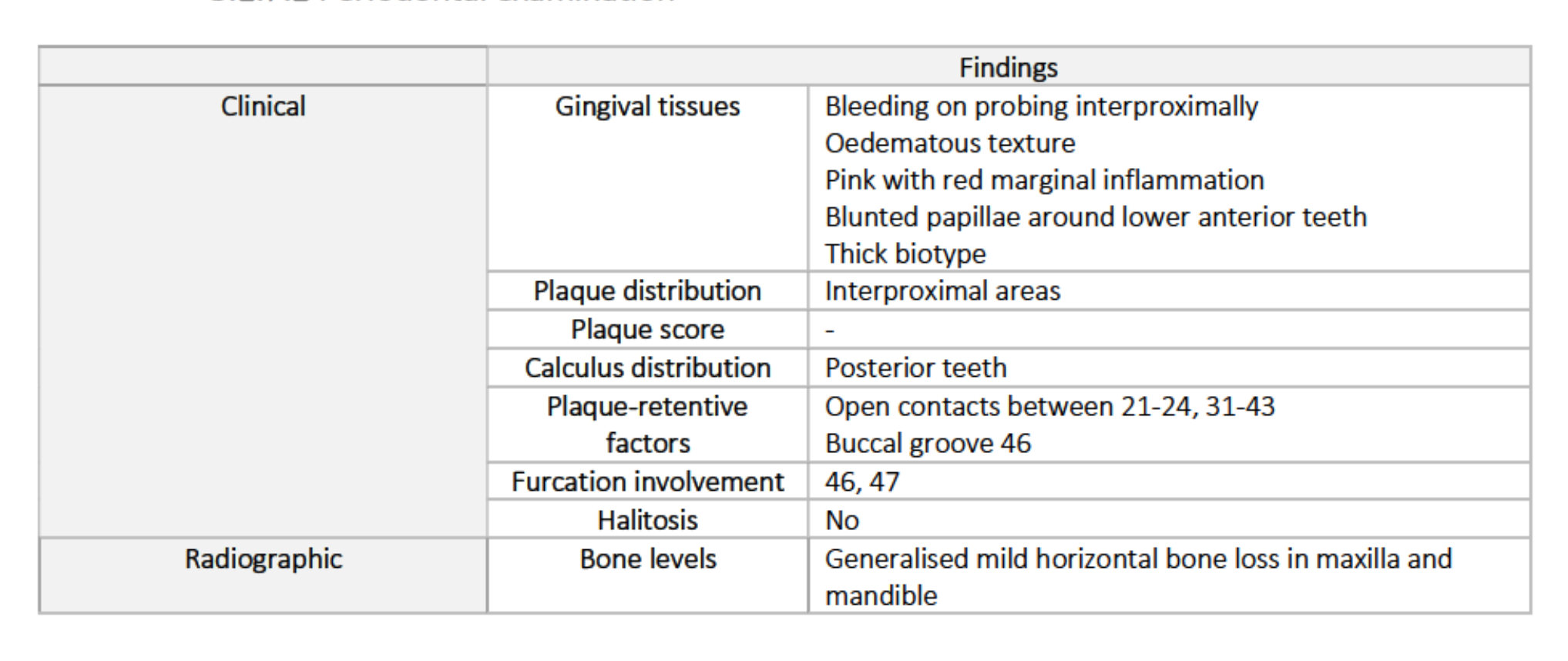
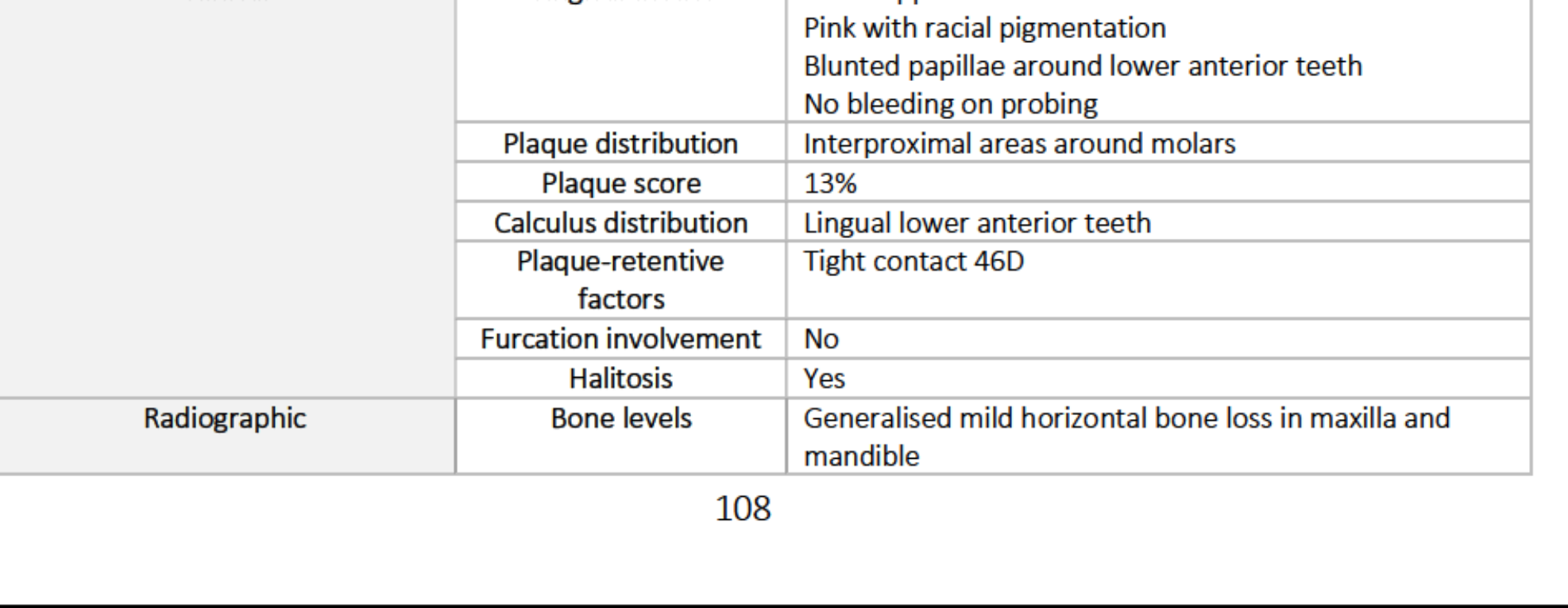
Clinical Periodontal Findings
- Gingival Tissues:
- Bleeding on probing (interproximal)
- Oedematous texture; pink with red marginal inflammation
- Blunted papillae (lower anterior)
- Thick biotype
- Plaque/Calculus:
- Plaque in interproximal areas
- Calculus on posterior teeth
- Plaque-retentive factors: Open contacts (21-24, 31-43), buccal groove 46
- Furcation: 46, 47
- Halitosis: No
Radiographic Periodontal Findings
- Bone levels: Generalised mild horizontal bone loss in maxilla and mandible.
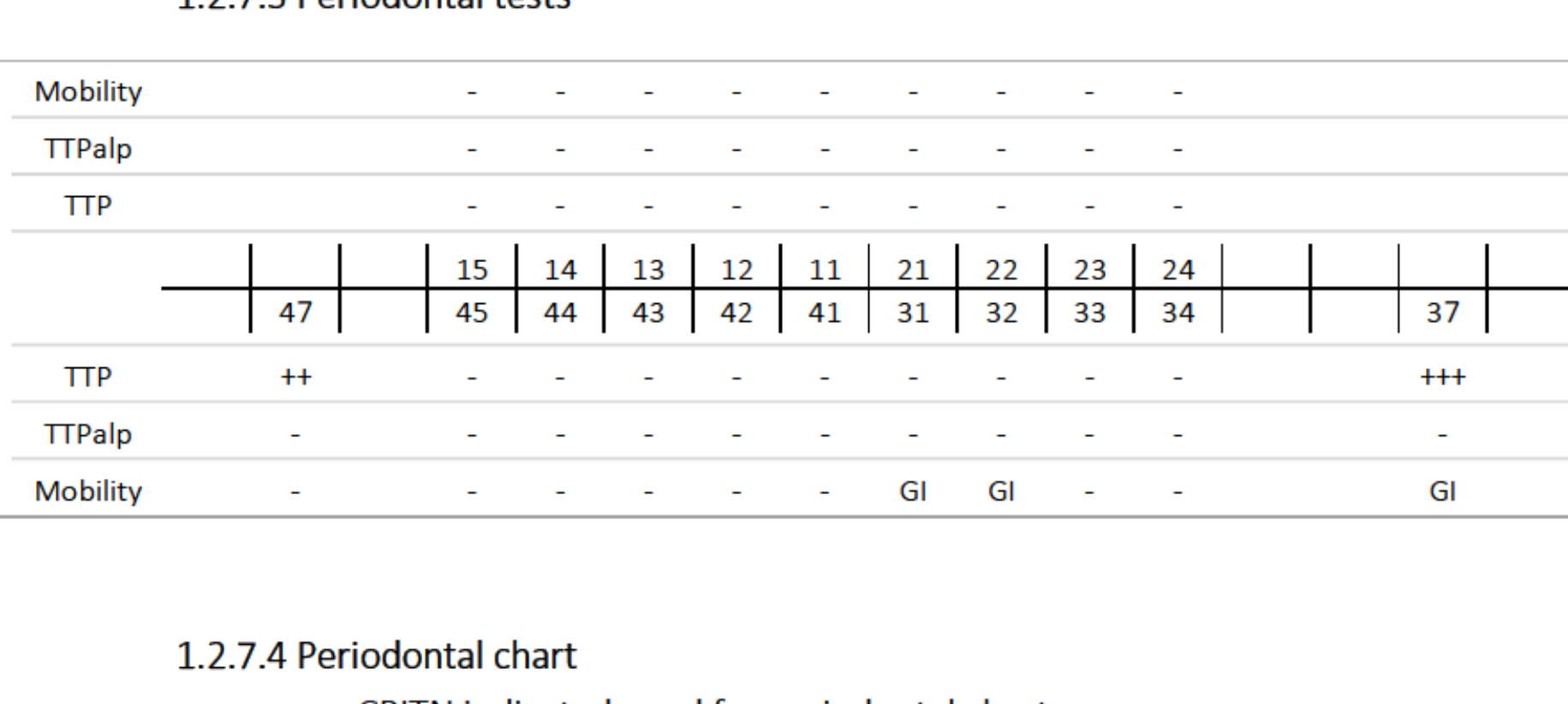
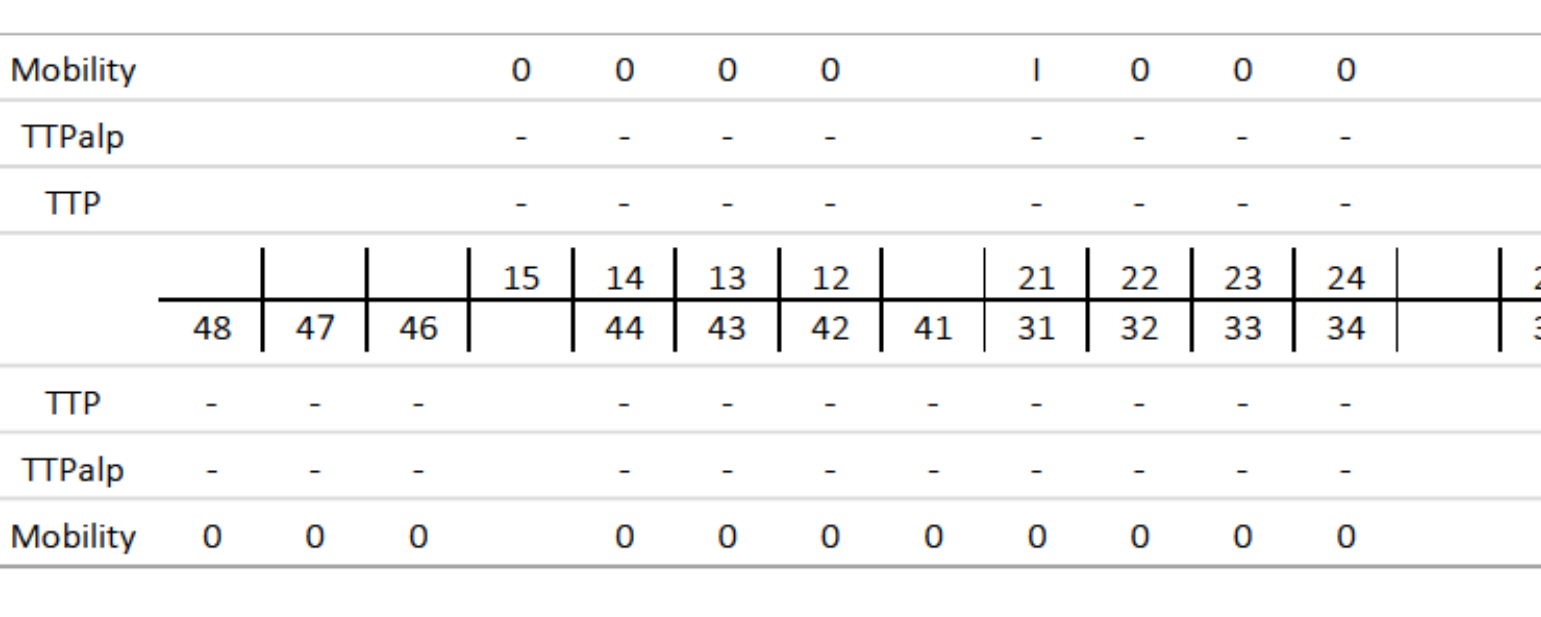
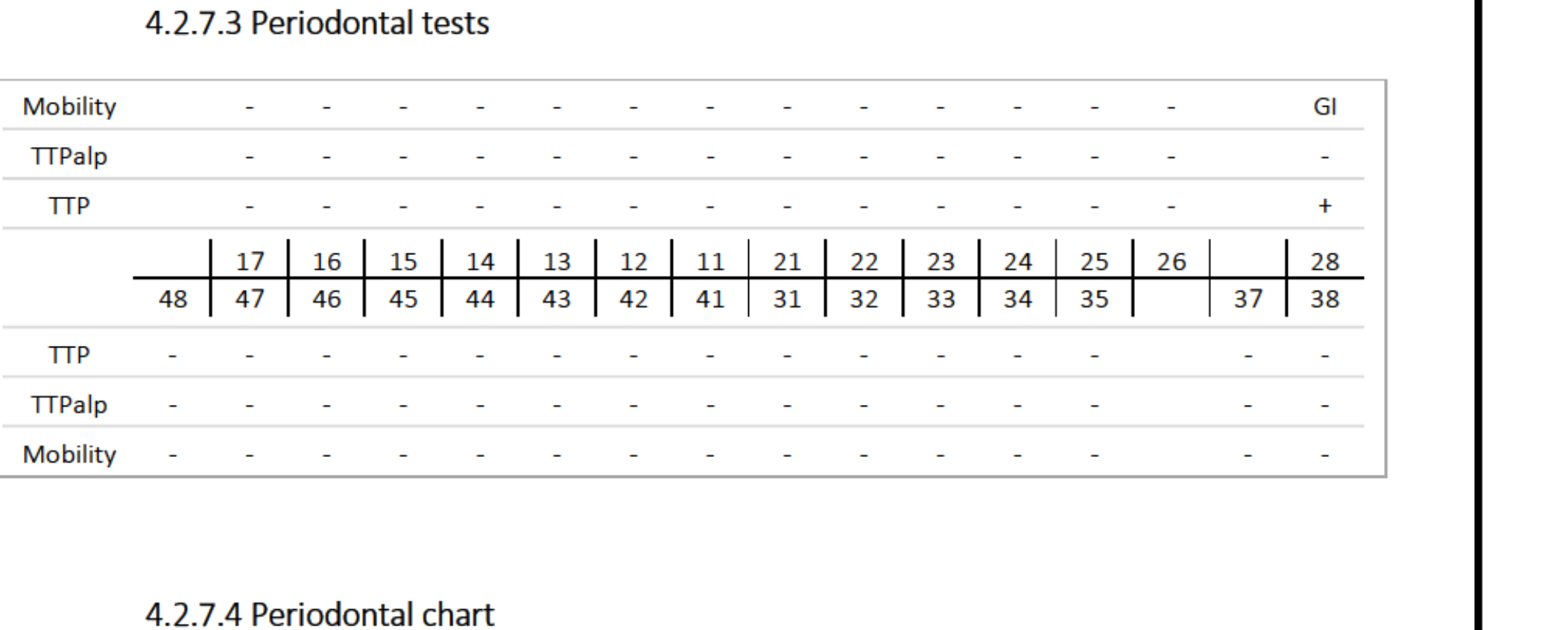
Periodontal Tests7778
| Tooth | 48 | 47 | 46 | 15 | 14 | 13 | 12 | 41 | 21 | 22 | 23 | 24 | 36 | 27 | 37 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mobility | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| TTPalp | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
| TTP | - | - | - | - | - | - | - | - | - | - | - | - | - | - | - |
 | 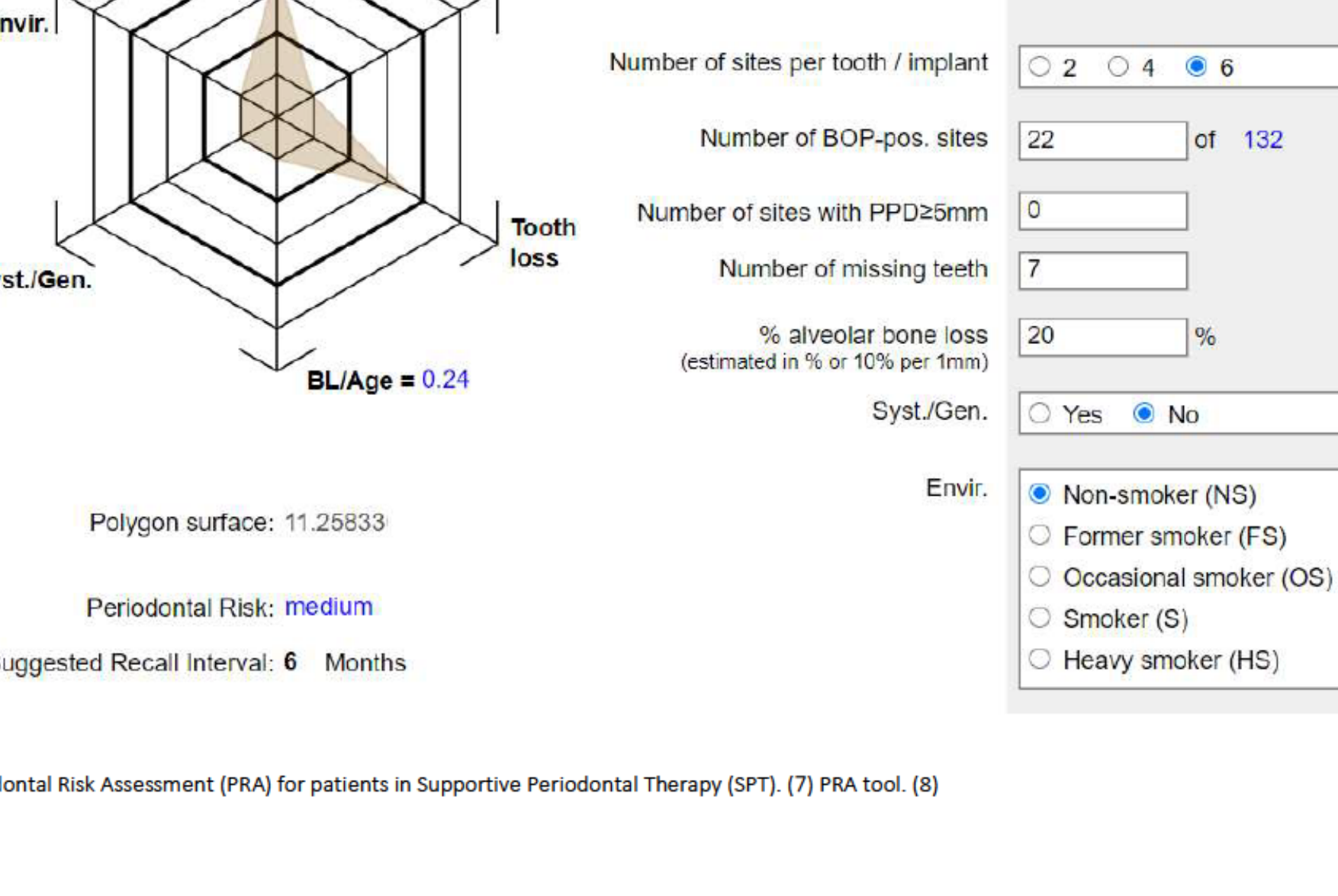 |
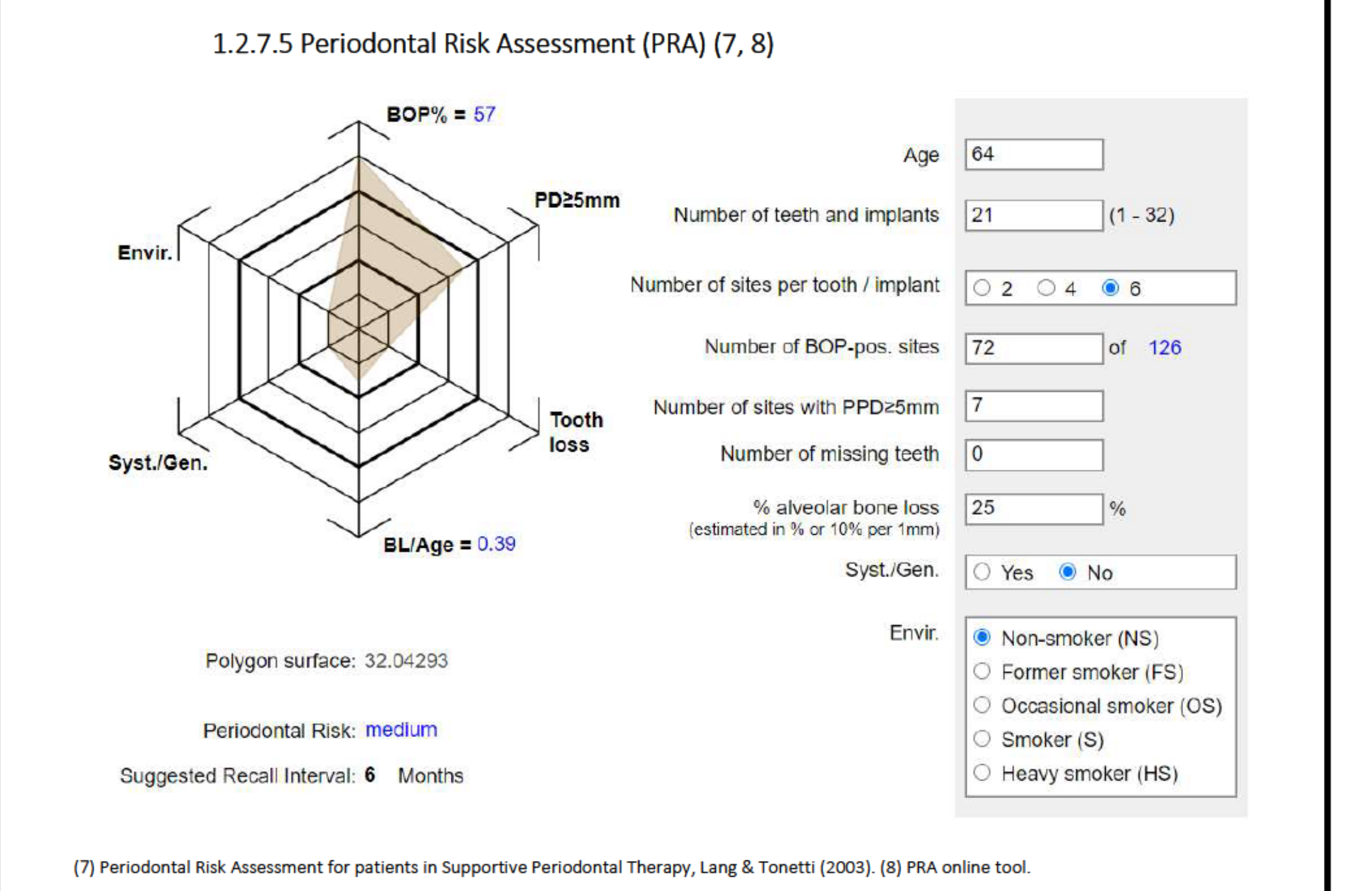
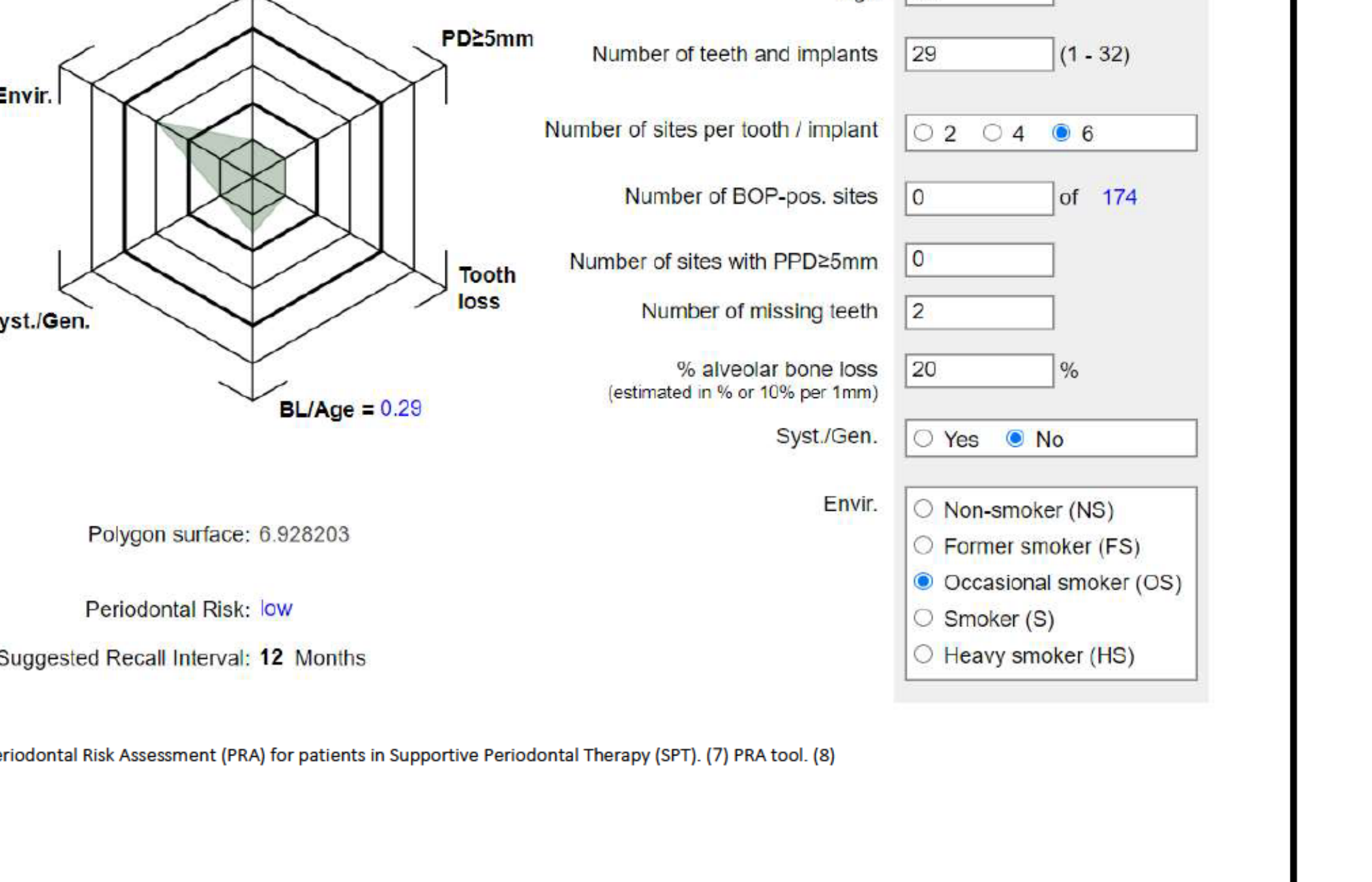
Periodontal Risk Assessment (PRA)
- BOP%: 17% (22 of 132 sites)
- PPD ≥5mm: 0 sites
- Bone Loss/Age: 0.24
- Missing Teeth: 7
- Alveolar Bone Loss: Estimated 20%
- Systemic/Genetic Factors: Yes
- Environmental: Non-smoker
- Overall Periodontal Risk: Medium
- Suggested Recall: 6 Months
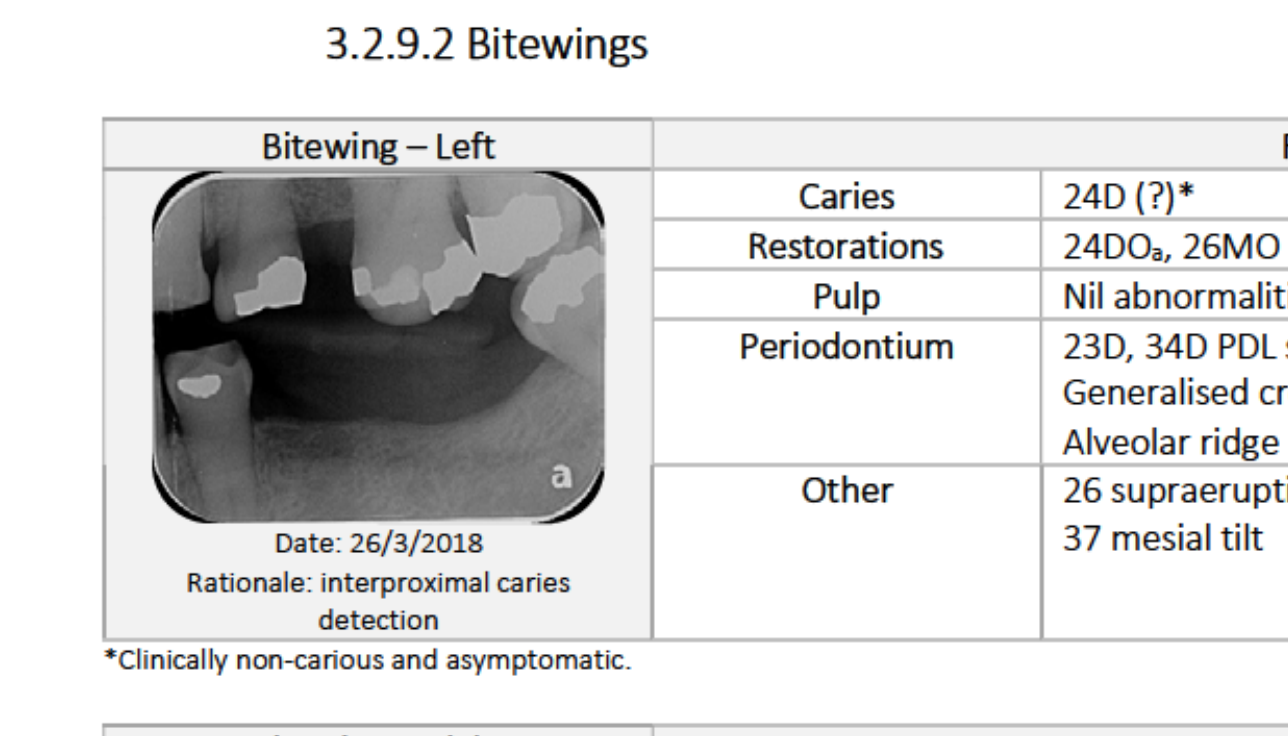
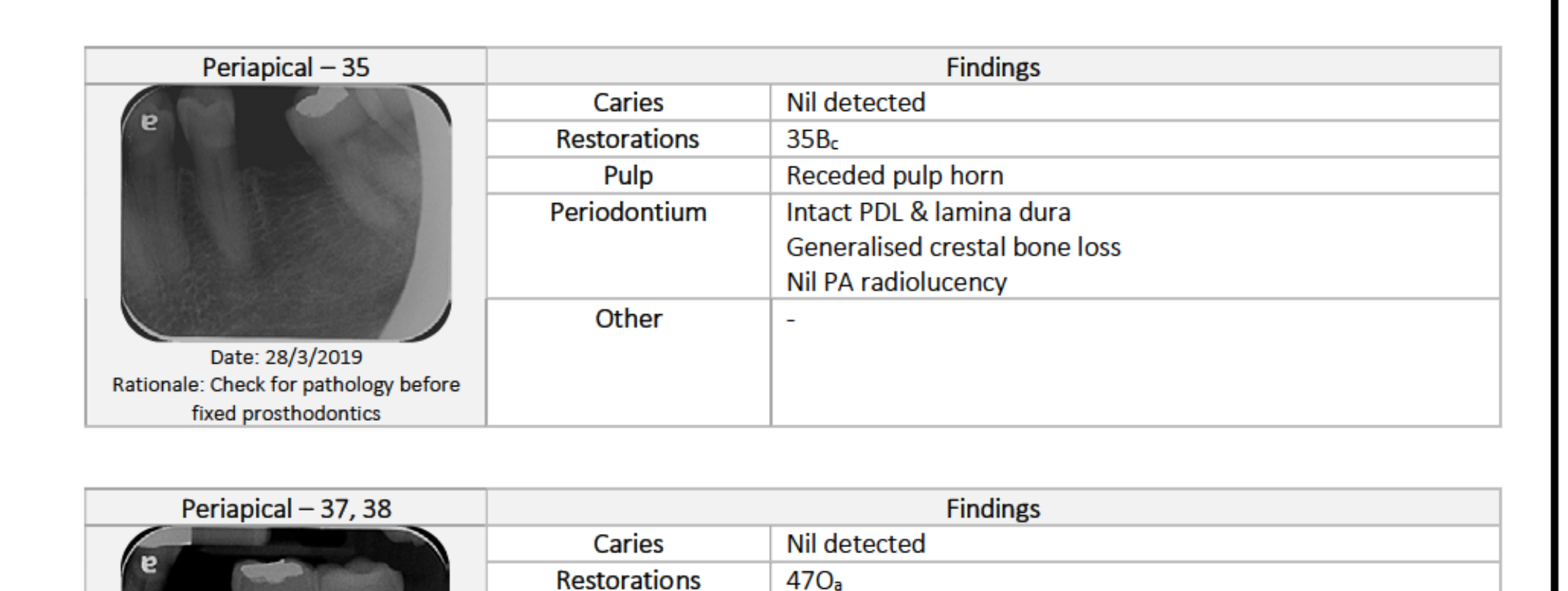
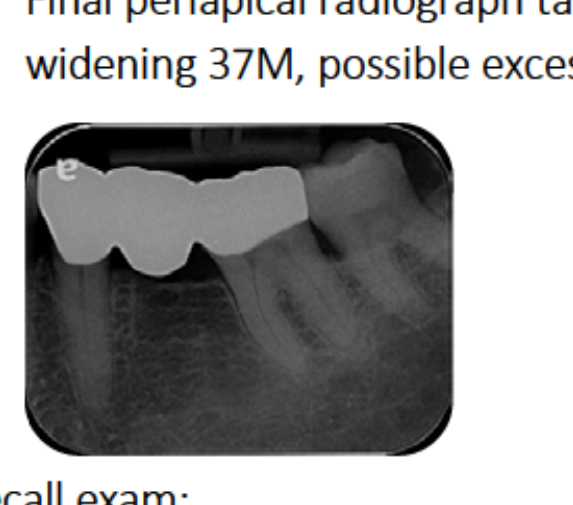
Radiographic Findings79
Bitewing – Left
- Restorations: 24DO, 26MO & OP, 27MOr (mesial overhang), 37Or, 34Ba.
- Periodontal: Generalised crestal bone loss; ridge resorption 36 region.
- Other: 23D/34D PDL space widening; 26 supraeruption; 37 mesial tilt.
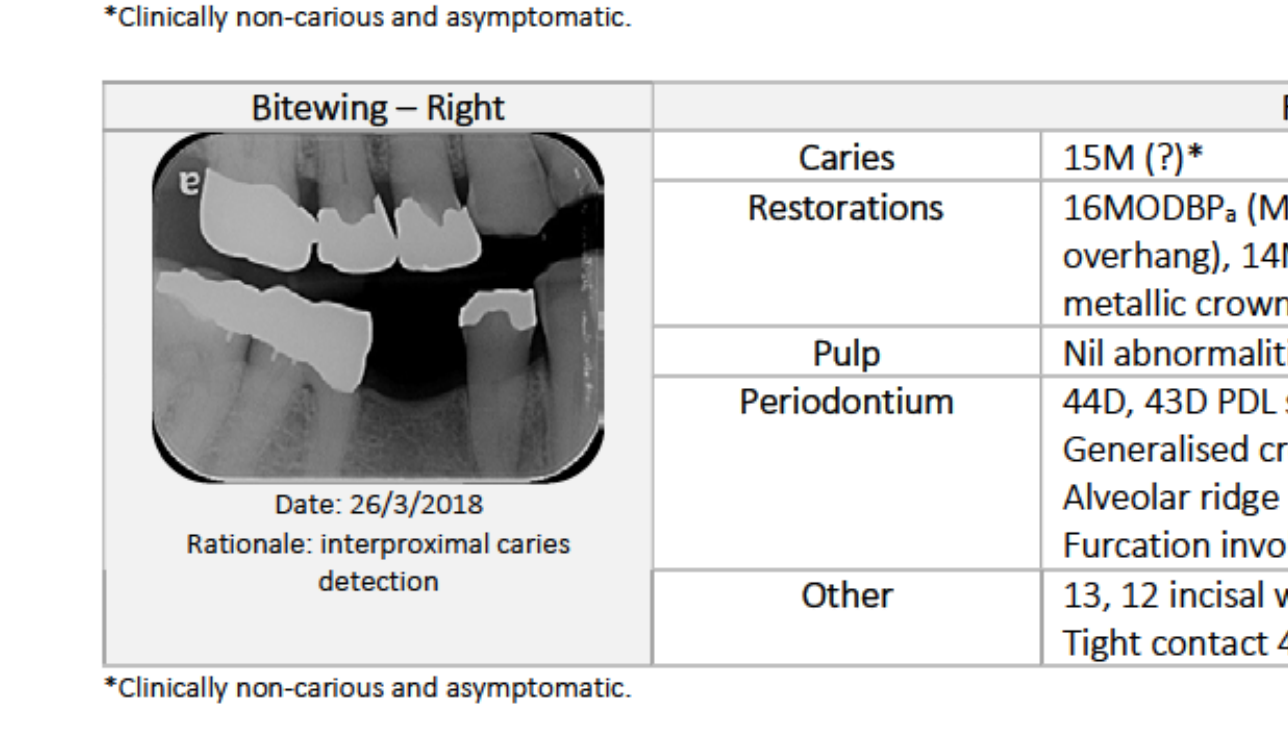
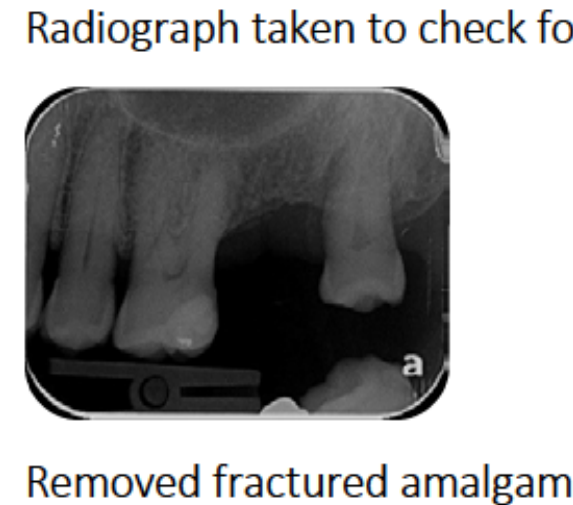
Bitewing – Right
- Restorations: 16MODBPa (overhang), 15MODBPa (overhang), 14MODBPa, 44MODa, 47Ma (pinned), 46 metallic crown (pinned core).
- Periodontal: Generalised crestal bone loss; ridge resorption 45 region; furcation involvement 46.
- Other: 44D/43D PDL space widening; 13, 12 incisal wear; tight contact 46D & 47M.
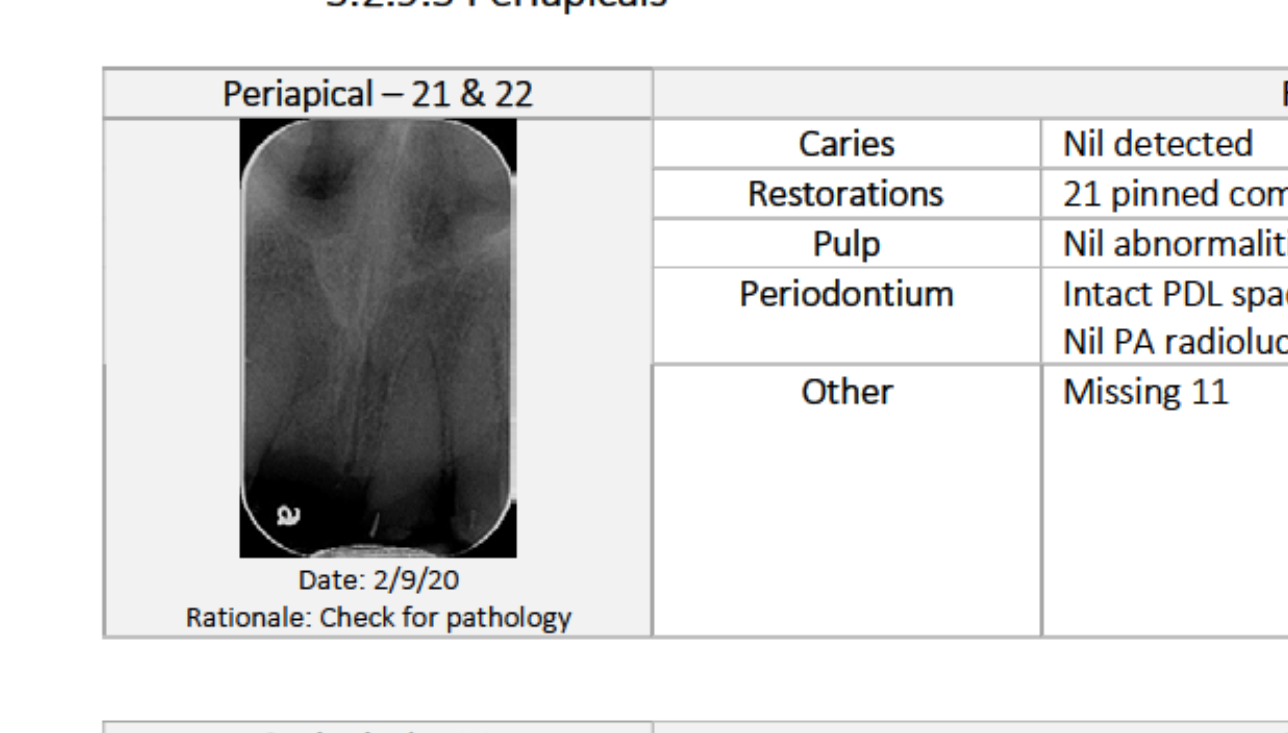
Periapical – 21 & 22
- Restorations: 21 pinned composite (failed), 22 pinned composite (failed).
- Findings: Intact PDL space and lamina dura; no periapical radiolucency; missing 11.
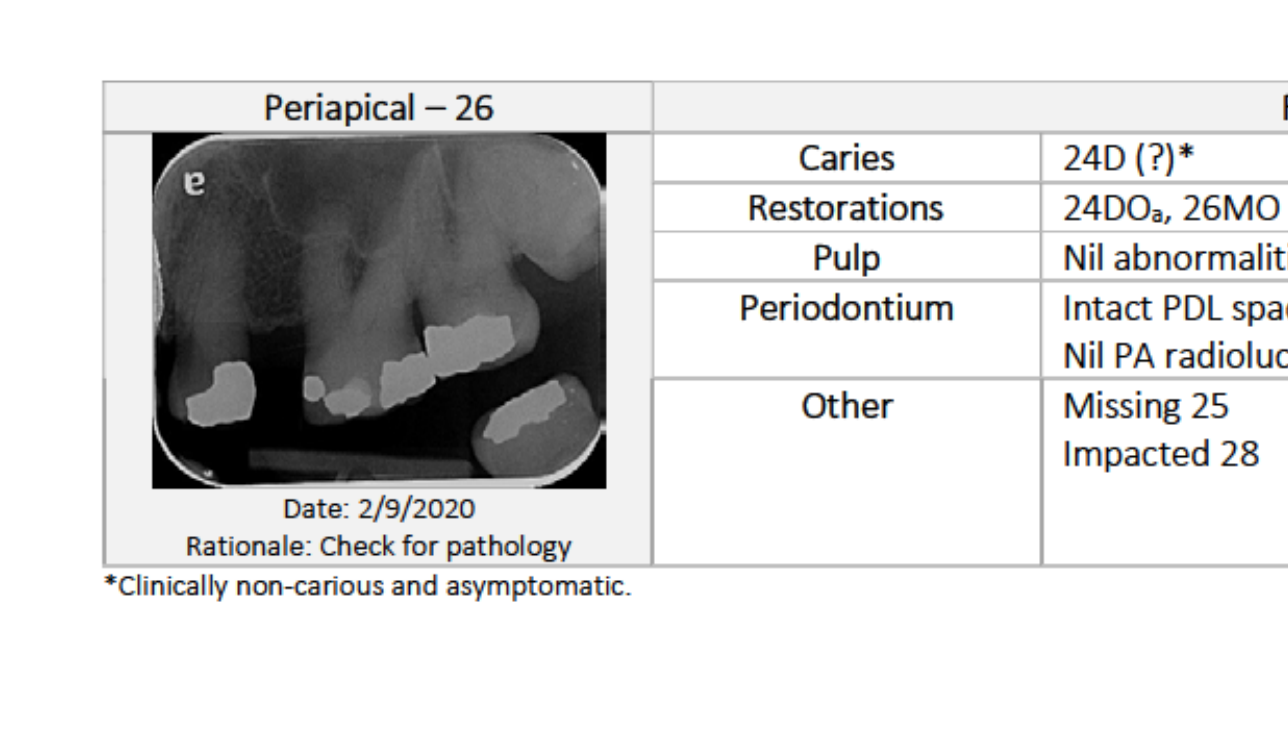
Periapical – 26
- Restorations: 24D Or, 26MO & OP, 27MOr, 37Or.
- Findings: Intact PDL space and lamina dura 24, 26, 27; no periapical radiolucency; missing 25; impacted 28.
 |  |
 |  |
Caries Risk Assessment80
Dietary Assessment
- High fermentable carbohydrates.
- Low sugar and low acid.
- Limited snacking frequency.
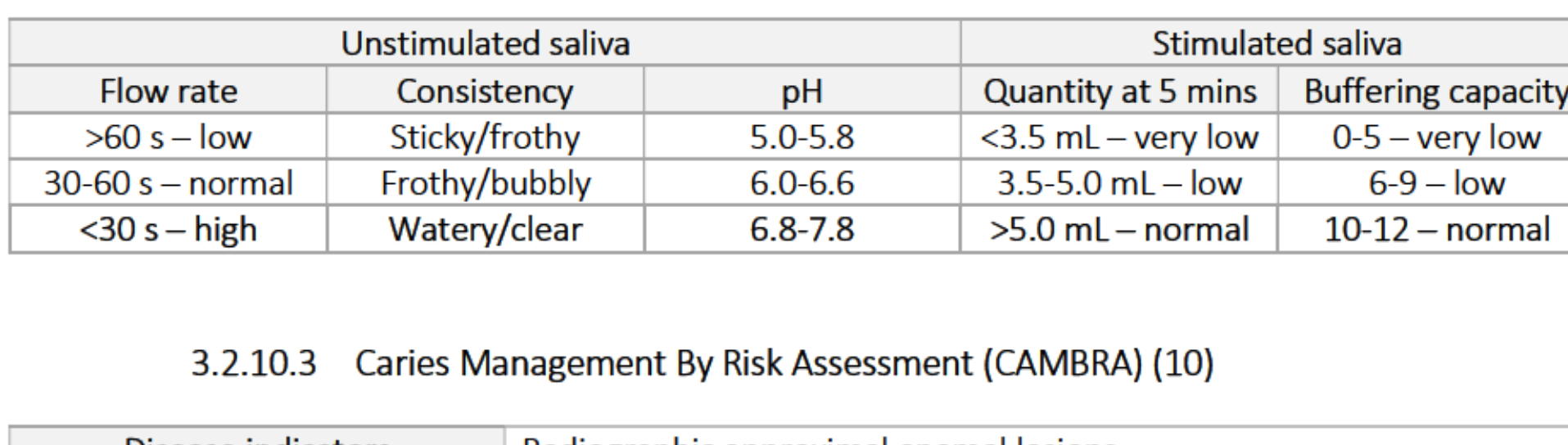
Saliva Test Results
- Unstimulated Flow Rate: Low (>60 s)
- Consistency: Sticky/frothy
- pH: 5.0-5.8 (Low)
- Stimulated Quantity (5 mins): Very low (<3.5 mL)
- Buffering Capacity: Very low (0-5)
CAMBRA Assessment
- Disease Indicators: Radiographic approximal enamel lesions.
- Risk Factors: Visible heavy plaque; exposed roots.
- Protective Factors: Fluoridated community; fluoride toothpaste twice daily; fluoride varnish (last 6 months); adequate stimulated flow.
- Overall Caries Risk: Low.
Suggested Management
- OTC toothpaste (1000 ppm fluoride) twice daily.
- 12-month recall.
 |  |
Diagnoses And Problem List81
Pathological Diagnoses82
- Restorations: Heavily restored dentition; history of multiple composite failures; metallic crown.
- Endodontic: 41 clinically/radiographically satisfactory RCT.
- Periodontal: Generalised Stage II Grade A stable periodontitis.
- Tooth Surface Loss: Attrition 13-12, 21-23, 34-43.
- Cracked Teeth: 13, 23, 26, 34, 33, 43, 47.
- Traumatic Occlusion: 21.
- Medical: Bilateral atherosclerotic carotid arteries; tonsilloliths.
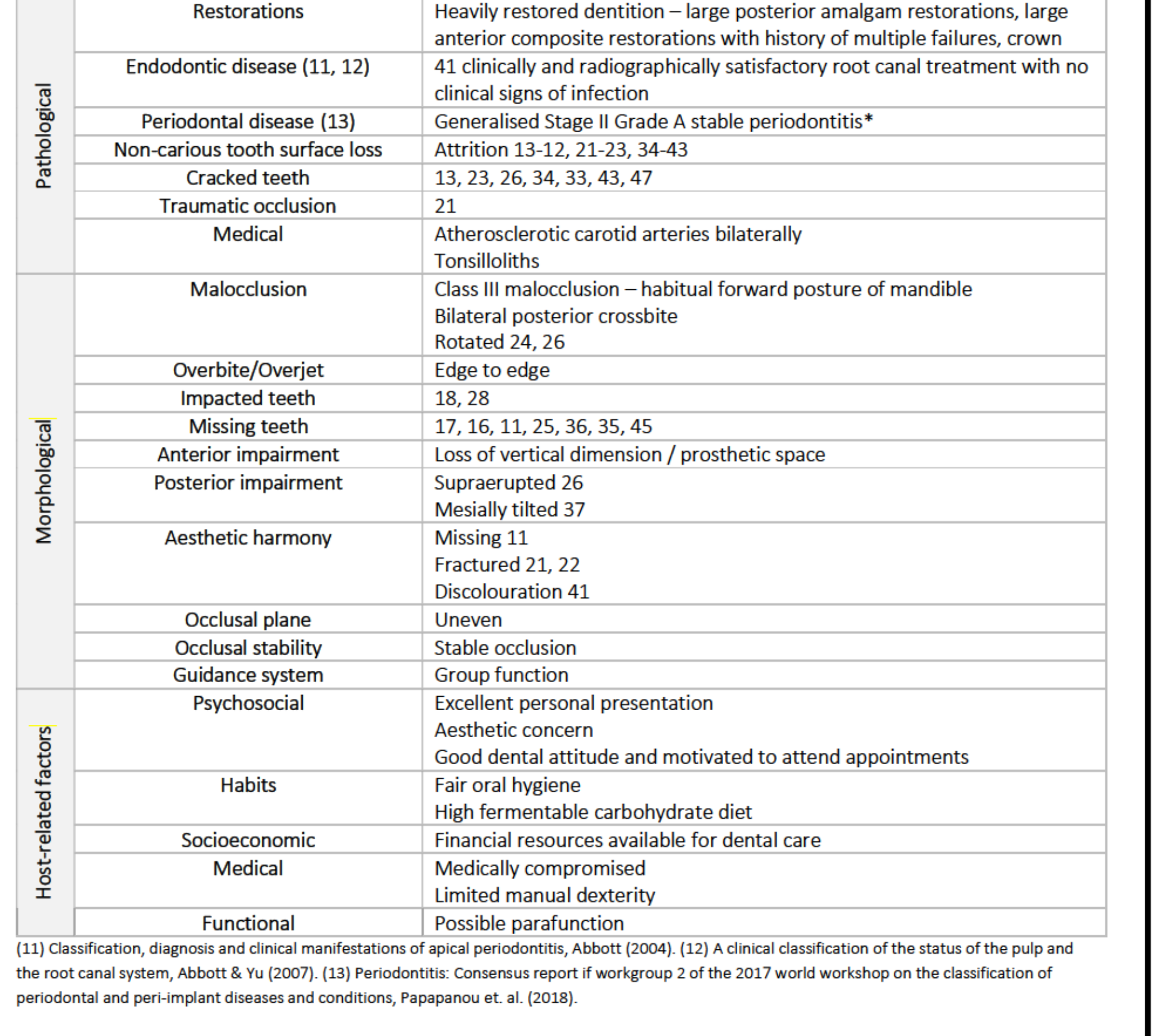
Morphological Diagnoses
- Malocclusion: Class III (habitual forward posture); bilateral posterior crossbite; rotated 24, 26.
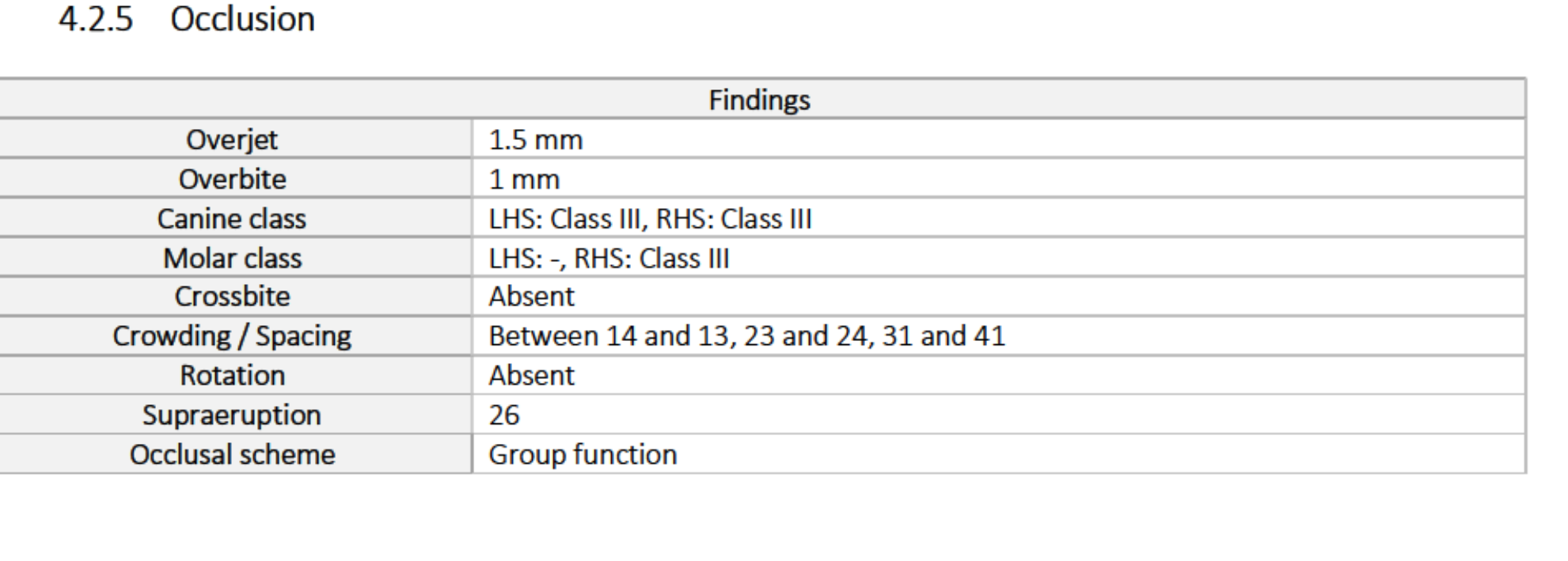
- Overbite/Overjet: Edge to edge.
- Missing/Impacted: Missing 17, 16, 11, 25, 36, 35, 45; impacted 18, 28.
- Impairment: Loss of vertical dimension/prosthetic space; supraerupted 26; tilted 37.
- Aesthetics: Missing 11; fractured 21, 22; discoloured 41.
- Occlusion: Stable; group function guidance; uneven occlusal plane.
Host-Related Factors
- Psychosocial: Excellent presentation; aesthetic concern; motivated.
- Habits: Fair oral hygiene; high fermentable carbohydrate diet.
- Socioeconomic: Financial resources available.
- Medical: Medically compromised; limited manual dexterity.
- Functional: Possible parafunction.
Problem List83
- Carotid artery disease.
- Poor aesthetics (Missing 11, failed restorations 21/22, discoloured 41).
- Tight contact: 46D & 47M.
- Generalised Stage II Grade A stable periodontitis (furcation 46, 47).
- Generalised anterior tooth wear (loss of VDO, uneven plane, group function).
- Missing posterior teeth: 17, 16, 25, 36, 35, 45.
- Impacted 18, 28.
- Tonsilloliths.
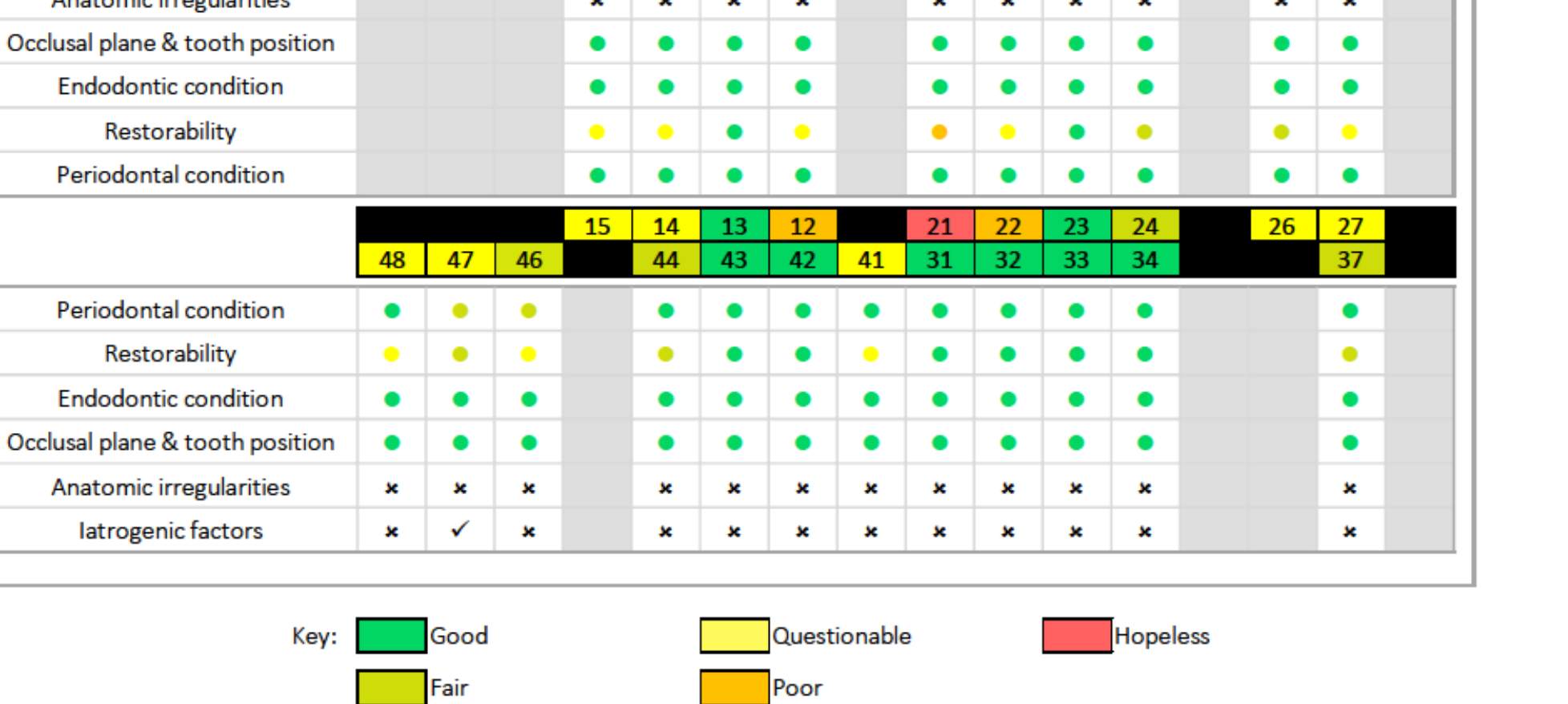
Prognosis84
Overall Dentition Prognosis85
- Periodontal: Sound health except 46, 47 (furcation involvement).
- Pulpal: Sound health except 41 (questionable RCT).
- Restorability: History of extensive posterior restorations and little remaining structure on 12, 21, 22 results in poor to hopeless prognosis for those specific teeth.
- Medical Priority: High risk for stroke (carotid artery disease) makes dental issues a lower systemic priority.
- Favourable Factors: Low cariogenic/acid diet and patient motivation/finances.
- Risks of No Treatment:
- High risk of stroke.
- Detrimental psychosocial impact due to aesthetics.
- Continued tooth loss via wear.
Treatment Options868788
Anterior Aesthetics and Posterior Contacts
Failed Composite 22
- No treatment: Does not address complaint.
- Restore tooth: Addresses complaint but high risk of failure due to minimal tooth structure and history of failure.
- Extraction and Immediate Partial Denture: Addresses complaint; patient wants to keep tooth as long as possible despite poor prognosis. (Selected Option: 3)
Discolouration 41
- No treatment: Patient not bothered by discolouration. (Selected Option: 1)
- Restore tooth: Risk of restoration failure due to little remaining structure.
Tight Contact 46D & 47M
- No treatment/Monitor: Risk of plaque trapping, caries, and infection. (Selected Option: 1 - Patient declined treatment)
- Restore tooth: Eliminates food trap but requires extensive work; margins likely subgingival.
Impacted Teeth and Tonsilloliths
Impacted 18, 28
- No treatment: Asymptomatic; present for long time. (Selected Option: 1)
- Surgical extraction: Risks of surgery outweigh benefits given medical history.
Tonsilloliths
- Self-management: Oral hygiene and warm salt water rinses. (Selected Option: 1)
- GP Referral: For symptomatic/large deposits.
Management Plan
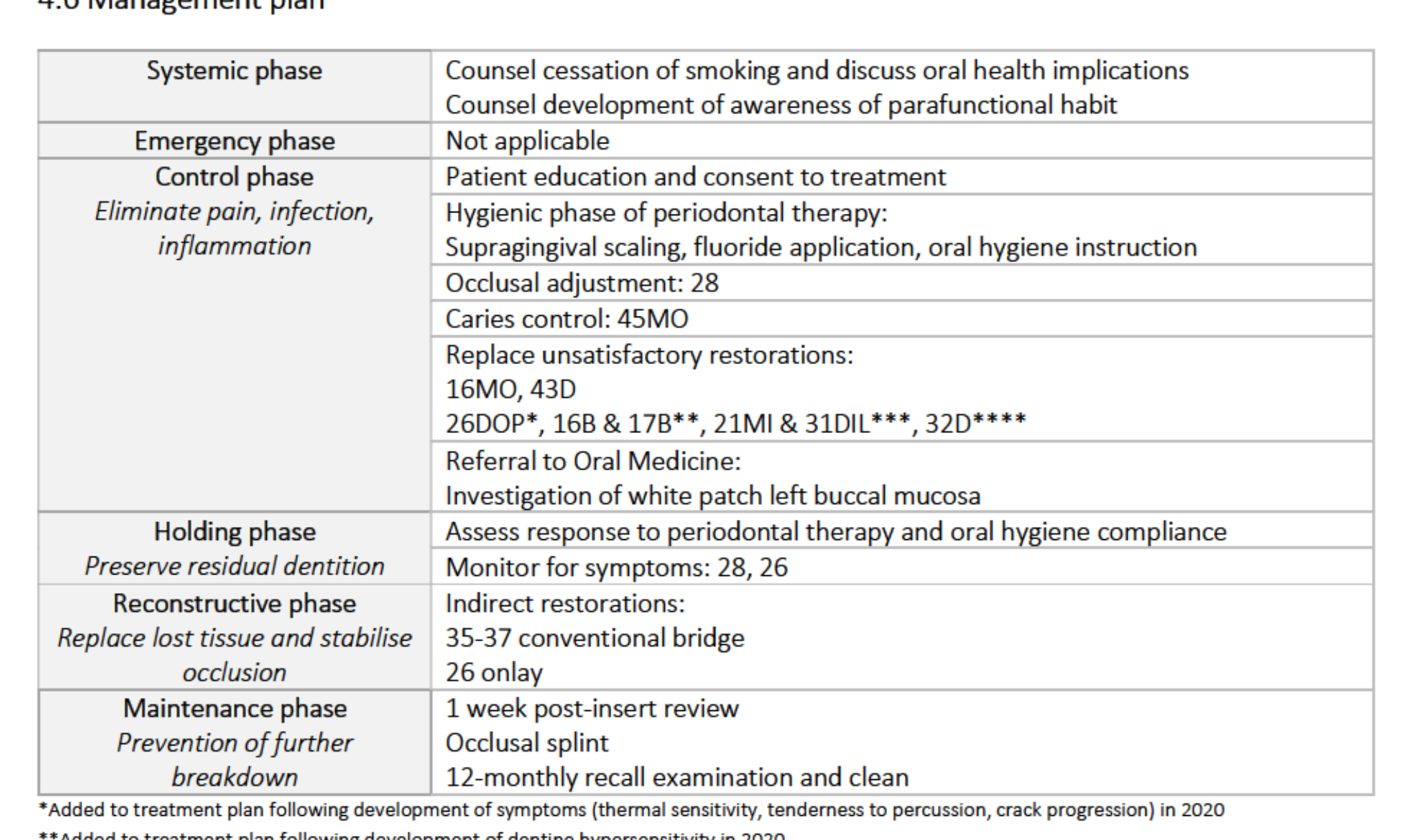
Systemic Phase
- Referral to GP for management of carotid artery disease.
Control Phase (Pain, Infection, Inflammation)
- Patient education and consent.
- Periodontal therapy: Scale and clean, debridement 46 & 47, fluoride, OHI.
- Replace unsatisfactory restoration: 22MDLa.
- Extraction: 21.
Holding Phase
- Assess periodontal response and OH compliance.
- Monitor cracked teeth: 26, 47.
Reconstructive Phase
- Indirect prosthesis: Immediate acrylic upper partial denture replacing 16, 11, 21.
Maintenance Phase
- 1-week post-insert review.
- 6-monthly recall: Periodontal maintenance, reinforce OHI, monitor cracked teeth.
- Review acrylic denture; consider Co-Cr replacement if appropriate.
Clinical Outcomes And Reflection
Case 4: Fixed Occlusal Rehabilitation
The Patient
Examination And Diagnostics
 |  |  |
 |  |  |
 |  |  |
 |  |
Management Plan
Treatment Delivery
 |  |  |
 |  |  |
 |
Case 5: Removable Occlusal Rehabilitation
The Patient

Examination And Diagnostics
 |  |  |
 |  |
Footnotes
-
Original PDF page 1: Sample portfolio 2, p.1 ↩
-
Original PDF page 2: Sample portfolio 2, p.2 ↩
-
Original PDF page 3: Sample portfolio 2, p.3 ↩
-
Original PDF page 4: Sample portfolio 2, p.4 ↩
-
Original PDF page 5: Sample portfolio 2, p.5 ↩
-
Original PDF page 6: Sample portfolio 2, p.6 ↩
-
Original PDF page 7: Sample portfolio 2, p.7 ↩
-
Original PDF page 8: Sample portfolio 2, p.8 ↩
-
Original PDF page 9: Sample portfolio 2, p.9 ↩
-
Original PDF page 10: Sample portfolio 2, p.10 ↩
-
Original PDF page 11: Sample portfolio 2, p.11 ↩
-
Original PDF page 12: Sample portfolio 2, p.12 ↩
-
Original PDF page 13: Sample portfolio 2, p.13 ↩
-
Original PDF page 14: Sample portfolio 2, p.14 ↩
-
Original PDF page 15: Sample portfolio 2, p.15 ↩
-
Original PDF page 16: Sample portfolio 2, p.16 ↩
-
Original PDF page 17: Sample portfolio 2, p.17 ↩
-
Original PDF page 18: Sample portfolio 2, p.18 ↩
-
Original PDF page 19: Sample portfolio 2, p.19 ↩
-
Original PDF page 20: Sample portfolio 2, p.20 ↩
-
Original PDF page 21: Sample portfolio 2, p.21 ↩
-
Original PDF page 25: Sample portfolio 2, p.25 ↩
-
Original PDF page 26: Sample portfolio 2, p.26 ↩
-
Original PDF page 27: Sample portfolio 2, p.27 ↩
-
Original PDF page 28: Sample portfolio 2, p.28 ↩
-
Original PDF page 29: Sample portfolio 2, p.29 ↩
-
Original PDF page 30: Sample portfolio 2, p.30 ↩
-
Original PDF page 31: Sample portfolio 2, p.31 ↩
-
Original PDF page 32: Sample portfolio 2, p.32 ↩
-
Original PDF page 33: Sample portfolio 2, p.33 ↩
-
Original PDF page 34: Sample portfolio 2, p.34 ↩
-
Original PDF page 35: Sample portfolio 2, p.35 ↩
-
Original PDF page 36: Sample portfolio 2, p.36 ↩
-
Original PDF page 37: Sample portfolio 2, p.37 ↩
-
Original PDF page 38: Sample portfolio 2, p.38 ↩
-
Original PDF page 39: Sample portfolio 2, p.39 ↩
-
Original PDF page 40: Sample portfolio 2, p.40 ↩
-
Original PDF page 41: Sample portfolio 2, p.41 ↩
-
Original PDF page 42: Sample portfolio 2, p.42 ↩
-
Original PDF page 43: Sample portfolio 2, p.43 ↩
-
Original PDF page 44: Sample portfolio 2, p.44 ↩
-
Original PDF page 45: Sample portfolio 2, p.45 ↩
-
Original PDF page 46: Sample portfolio 2, p.46 ↩
-
Original PDF page 47: Sample portfolio 2, p.47 ↩
-
Original PDF page 48: Sample portfolio 2, p.48 ↩
-
Original PDF page 49: Sample portfolio 2, p.49 ↩
-
Original PDF page 50: Sample portfolio 2, p.50 ↩
-
Original PDF page 51: Sample portfolio 2, p.51 ↩
-
Original PDF page 52: Sample portfolio 2, p.52 ↩
-
Original PDF page 53: Sample portfolio 2, p.53 ↩
-
Original PDF page 54: Sample portfolio 2, p.54 ↩
-
Original PDF page 55: Sample portfolio 2, p.55 ↩
-
Original PDF page 56: Sample portfolio 2, p.56 ↩
-
Original PDF page 57: Sample portfolio 2, p.57 ↩
-
Original PDF page 58: Sample portfolio 2, p.58 ↩
-
Original PDF page 59: Sample portfolio 2, p.59 ↩
-
Original PDF page 63: Sample portfolio 2, p.63 ↩
-
Original PDF page 66: Sample portfolio 2, p.66 ↩
-
Original PDF page 67: Sample portfolio 2, p.67 ↩
-
Original PDF page 64: Sample portfolio 2, p.64 ↩
-
Original PDF page 65: Sample portfolio 2, p.65 ↩
-
Original PDF page 69: Sample portfolio 2, p.69 ↩
-
Original PDF page 70: Sample portfolio 2, p.70 ↩
-
Original PDF page 71: Sample portfolio 2, p.71 ↩
-
Original PDF page 73: Sample portfolio 2, p.73 ↩
-
Original PDF page 72: Sample portfolio 2, p.72 ↩
-
Original PDF page 74: Sample portfolio 2, p.74 ↩
-
Original PDF page 75: Sample portfolio 2, p.75 ↩
-
Original PDF page 76: Sample portfolio 2, p.76 ↩
-
Original PDF page 78: Sample portfolio 2, p.78 ↩
-
Original PDF page 80: Sample portfolio 2, p.80 ↩
-
Original PDF page 77: Sample portfolio 2, p.77 ↩
-
Original PDF page 79: Sample portfolio 2, p.79 ↩
-
Original PDF page 81: Sample portfolio 2, p.81 ↩
-
Original PDF page 82: Sample portfolio 2, p.82 ↩
-
Original PDF page 83: Sample portfolio 2, p.83 ↩
-
Original PDF page 84: Sample portfolio 2, p.84 ↩
-
Original PDF page 85: Sample portfolio 2, p.85 ↩
-
Original PDF page 86: Sample portfolio 2, p.86 ↩
-
Original PDF page 87: Sample portfolio 2, p.87 ↩
-
Original PDF page 90: Sample portfolio 2, p.90 ↩
-
Original PDF page 88: Sample portfolio 2, p.88 ↩
-
Original PDF page 89: Sample portfolio 2, p.89 ↩
-
Original PDF page 92: Sample portfolio 2, p.92 ↩
-
Original PDF page 91: Sample portfolio 2, p.91 ↩
-
Original PDF page 94: Sample portfolio 2, p.94 ↩
-
Original PDF page 96: Sample portfolio 2, p.96 ↩
-
Original PDF page 97: Sample portfolio 2, p.97 ↩