Occlusion and Tooth Replacement1
Occlusion and TMJ + Tooth Replacement
By Dr Cheryl Fu
Learning Outcomes
Core Objectives2
- Recap on key concepts of occlusion: Centric Relation, Maximum Intercuspation Position (see 2025 occlusion lectures for full slides)
- Discuss clinical implications of pathological adaptations caused by malocclusion
- Recap the envelope of function
- Review the criteria for the ideal occlusion and how to assess clinically
- Tooth replacement options (including immediate replacement options)
Clinical Focus and Assessment
Whilst theoretical background knowledge is important, as this module focuses on the “clinical” aspects, we will try to keep the topic relevant.
As these lectures are given as a guest for “Clinical Practice 3”, these concepts will not be directly assessed for the FPD/RPD module, unless the content is also covered in the prosthodontic module. However, you are expected to retain knowledge from previous years.
Fundamentals of Occlusion
Definition of Occlusion3
*occlusion \ə-klō’ zhən* n (1645):
- The act or process of closure or of being closed or shut off.
- The static relationship between the incising or masticating surfaces of the maxillary or mandibular teeth or tooth analogues.
Related Components:
- Articulation
- Centric Occlusion
- Components of Occlusion
- Eccentric Occlusion
- Line of Occlusion
- Linear Occlusion
- Monoplane Occlusion
- Pathogenic Occlusion
- Spherical Form of Occlusion
 |  |
Definition and Ideal Occlusion4
An ideal occlusion is defined as “the maxillary and mandibular teeth contact simultaneously when the condylar processes are fully seated in the mandibular fossae, and the teeth do not interfere with harmonious movement of the mandible during function. Ideally, in the fully bilateral seated position of the condyle–articular disk assemblies, the maxillary and mandibular teeth exhibit maximum intercuspation. This means that the maxillary lingual and mandibular buccal cusps of the posterior teeth are evenly distributed and in stable contact with the opposing occlusal fossae. These functional cusps can then act as stops for vertical closure without excessively loading any one tooth, while left and right TMJs concurrently are in an unstrained position.”
Source: Contemporary Fixed Prosthodontics
Clinical Implications of Occlusal Disharmony5
Occlusal disharmony can cause a variety of issues:
- Attrition
- Splayed teeth
- Sore/sensitive teeth
- Mobility/occlusal fremitus
- Re-occurring failure of restorations/cracked teeth
Attrition and Wear6
Definition
Attrition is defined as wear due to “tooth-on-tooth” friction. It usually results from bruxism.
The University of Western Australia

Splayed Teeth and Posterior Support
The same type of forces that cause tooth wear can also force anterior teeth forwards.
Possible Causes
- Loss of posterior support: Posterior teeth are better at supporting occlusal forces.
- Excessive load: Anterior teeth take excessive occlusal load.
Sensitivity and Periodontal Tenderness
Clinical Presentation
- Periodontal Tenderness: Compression of the periodontal ligament can cause tenderness during percussion or pressure.
- Hypersensitivity: Occlusal overload can cause hypersensitivity of the pulp.
Etiology and Management
- May be due to occlusal interferences from restorations, or general occlusal overload/bruxism.
- If a restoration was recently placed on the tooth or opposing tooth, check the bite again.
- Patients may fail to perform their full envelope of motion during checks with articulating paper, especially when numb.
Hypermobility and Fremitus
Clinical Observations
- Occlusal fremitus resulting from occlusal overload.
- Radiographic evidence usually shows widening of the PDL, with an absence of apical radiolucency consistent with infections.
Management
- Check occlusal contacts for deflective contacts or occlusal overload.
- Adjust occlusion if required.
Cracked Teeth and Restorations
Clinical Characteristics
- Fracture of cusps or restorative material from heavy loading.
- Often occurs on the last teeth in the arch, which sustain considerable occlusal forces.
Research Findings (J Endod. 2016)
- Demographics: Most patients were aged 50–60 (32.0%) or over 60 (32.6%).
- Frequency: The lower second molar was the most frequently affected tooth (25.1%).
- Tooth Condition: Intact teeth (34.3%) or teeth with Class I restorations (32.0%) showed a higher incidence of cracks.
- Survival: The 2-year survival rate after Root Canal Treatment (RCT) was 90.0%.
- Prognosis: Probing depth >6 mm is a significant negative prognostic factor (74.1% survival vs. 96.8% for depths <6 mm).
Temporomandibular Joint and Mandibular Movement
Determinants of Occlusion7
The opening of the mouth involves both hinge and translatory movements. This explanation is based on Peter Dawson’s “Functional Occlusion.”
 |  |
 |
Anatomy and Mechanics of the Temporomandibular Joint
Components of the TMJ8
- Condyle head
- Articular disc (dense connective tissue)
- Glenoid fossa

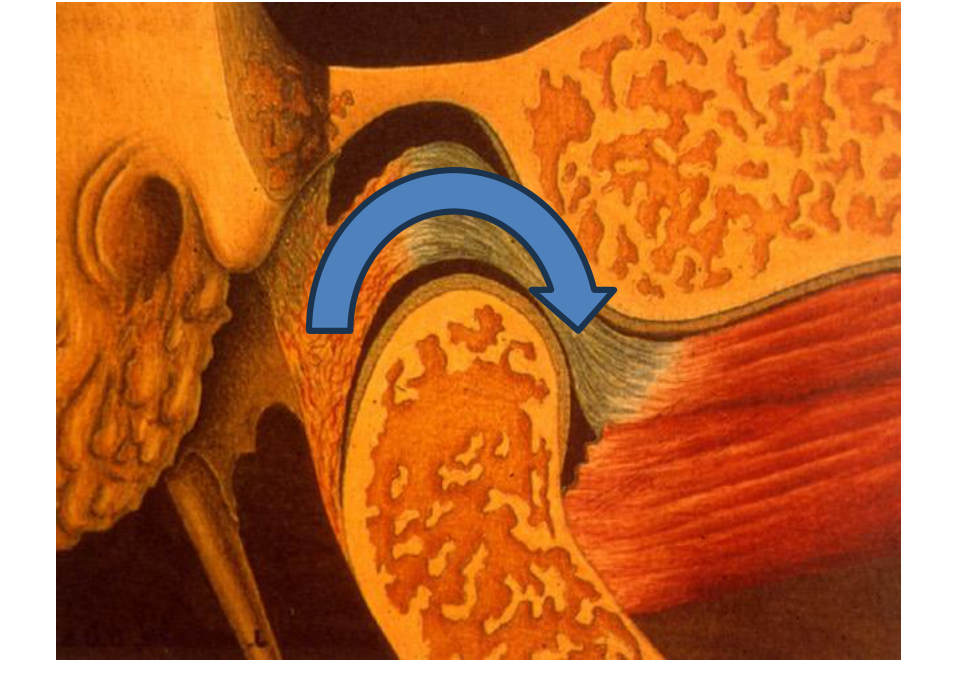
Ginglymoarthrodial Motion9
The joint is capable of both hinging and gliding motions.
- Initial Opening (<2cm): The condyle rotates within the glenoid fossa about the intra-condylar axis.
 |  |
 |
Translational Movement10
- Advanced Opening (>2cm): A translational movement occurs as the condyle glides against the articular eminence.
 |  |
 |
Excursive Movements and Condylar Guidance
Movement Types11
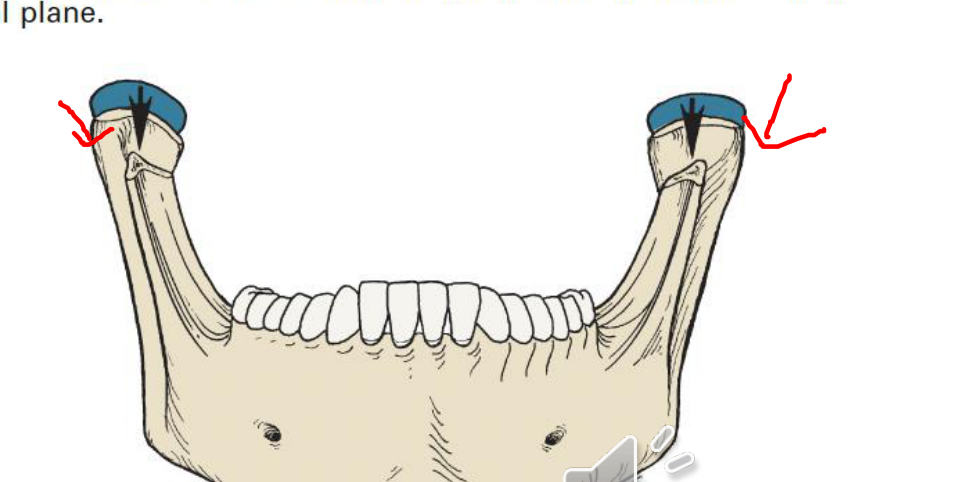
- Protrusive movements: Both condyles move in a forward gliding motion.
- Lateral movements:
- Working side: Rotates about the vertical axis without leaving the glenoid fossa.
- Non-working side: Follows a gliding path against the articular eminence.

Condylar Guidance12
The angle of downward movement is determined by the articular eminence. This is termed the “condylar angle” or “guidance inclination.”
- Protrusive mandibular movement occurs in both the horizontal and frontal planes.
 |  |
 |
Condylar Angle13
Condylar angle (guidance inclination) refers to the path established by the TMJ during excursive movements.

Bennett Angle and Side Shift
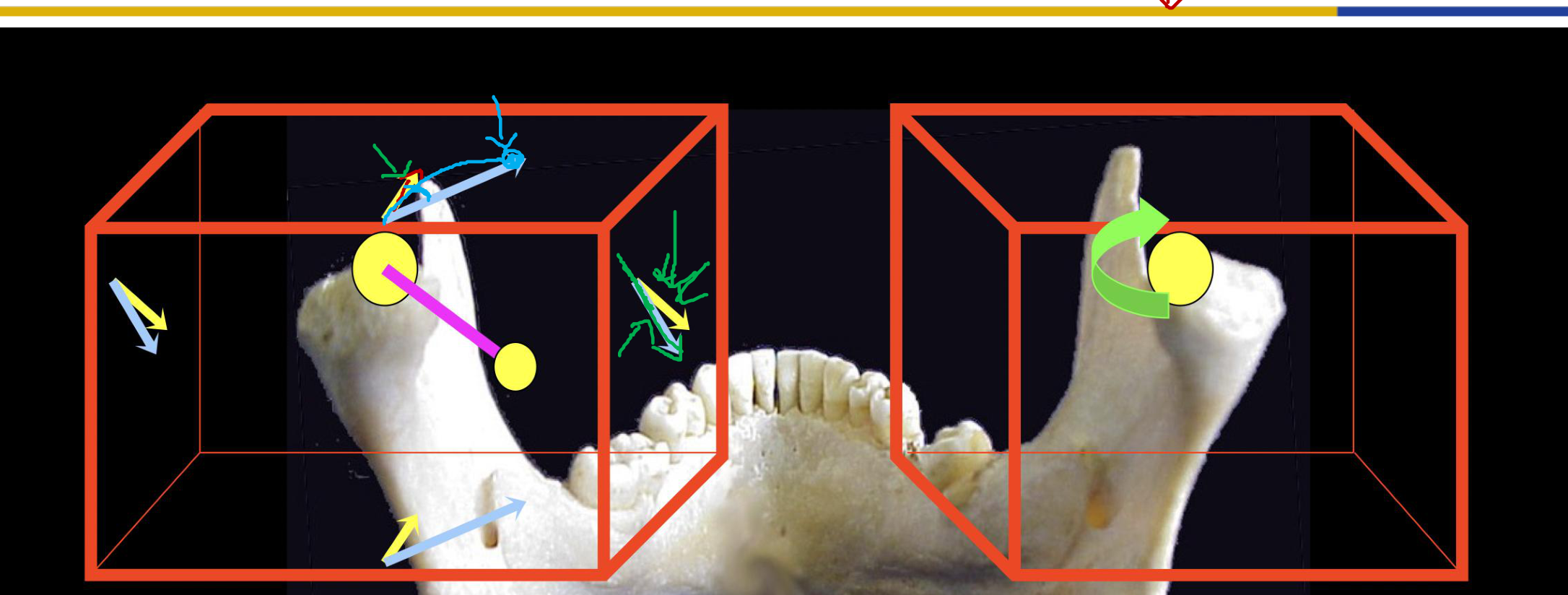
Lateral Excursive Dynamics14
During lateral movements, the principal movement occurs on the non-working side:
- Non-working condyle path: Moves forward, downward, and medially.
- Condylar Angle: The downward angle limited by the articular eminence.
- Bennett Angle: The angle formed between the sagittal plane and the average path of the advancing condyle as viewed in the horizontal plane.
- Fisher Angle: The angle between the protrusive path and the lateral excursive path of the non-working side. The lateral path is typically steeper than the protrusive path.
Angular Relationships15
- Bennett angle
- Fisher angle
Components of Side Shift16
The lateral movement of the non-working condyle is non-linear and consists of:
- Immediate side shift: The non-working condyle moves straight medially.
- Progressive side shift: The non-working condyle translates laterally in a curve from the end of the immediate side shift.

Bennett Side Shift Types17
- Progressive Bennett side shift
- Immediate Bennett side shift

Mandibular Movement Planes18
- Right lateral mandibular movement in the horizontal plane.
- Lateral movement in the frontal plane.
 |  |
Clinical Replication19
To accurately reflect patient jaw relationships, clinicians may replicate the condylar angle and the Bennett angle.

Average Values2021
- The Bennett angle averages approximately 15 degrees.
 |  |
Anterior Determinants and Envelope of Function
Determinants of Movement22
- Posterior Determinants: Shape of the articular eminence and configuration of the condyles (anatomical factors not affected by the dentist).
- Anterior Determinants: The palatal surface of maxillary anterior teeth and labial surfaces of mandibular incisors.

Anterior Tooth Morphology and Guidance
Incisal Morphology23
When placing restorations in the incisal area, the specific shape of the tooth is critical. Incisors are not simple rectangles; they possess curves and bends essential for anterior guidance.
Tooth Planes24
- The labial plane has multiple contours.
- The top half emerges with a prominent curve at the gingival embrasure, following the alveolar process contours.
- Proper contouring is necessary for direct restorations to maintain existing occlusion.

Labial Contours and Function25
- The lower half of the labial surface exists in a different plane than the gingival half.
- Contouring must allow the lower lip to slide comfortably by the incisal third to contact the top lip.
- Crown preparations for anterior teeth should reflect these two distinct planes.
- Adjustments to provisional restorations may be required to achieve an unstrained lip-closure path.

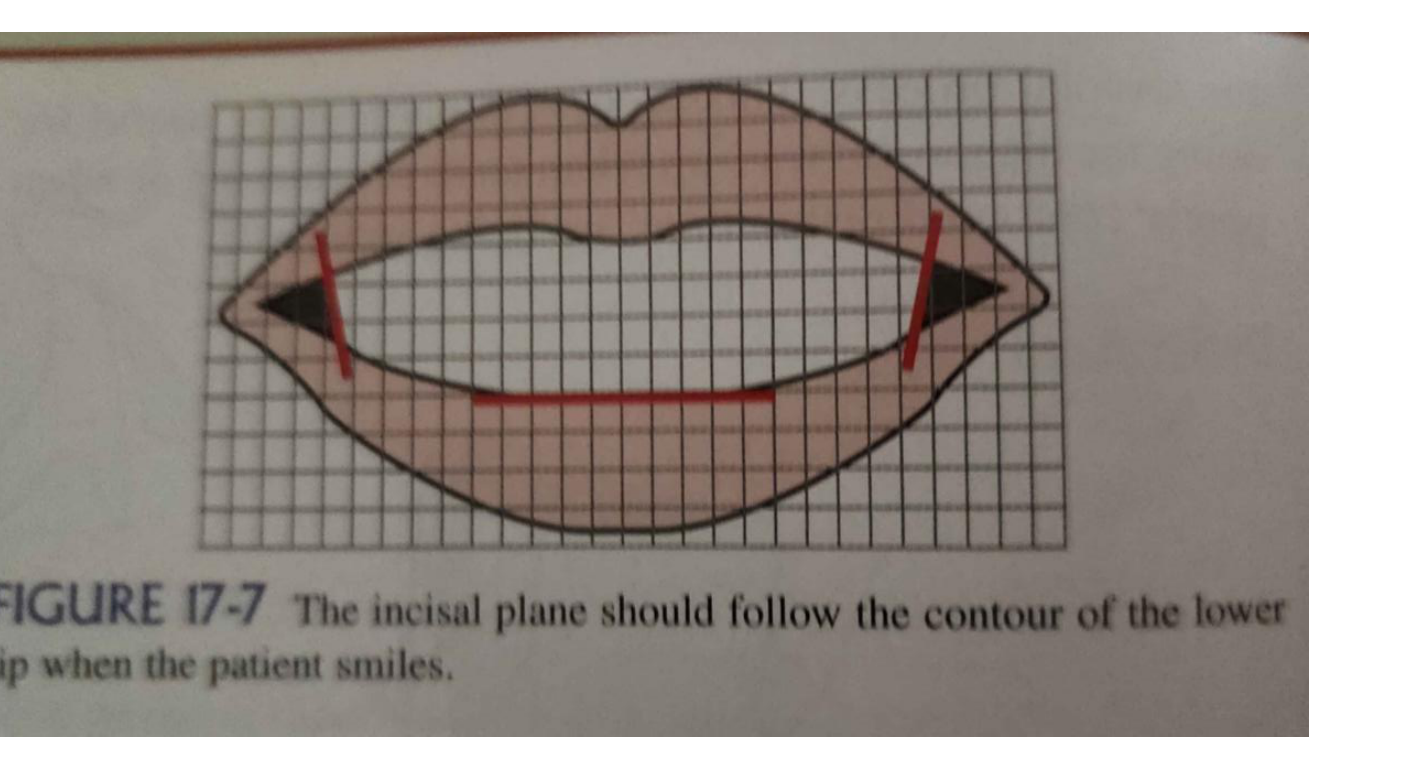
Esthetic Alignment26
The incisal plane should follow the contour of the lower lip when the patient smiles.
Clinical Occlusal Schemes
Centric Relation and Maximum Intercuspal Position
Key Definitions27
Maximal Intercuspal Position (MIP): The complete intercuspation of opposing teeth independent of condylar position. Also known as the “best fit” of teeth.
Centric Relation (CR): A maxillomandibular relationship, independent of tooth contact, where condyles articulate in the anterior-superior position against the posterior slopes of the articular eminences. It is a repeatable, unstrained reference position where the mandible is restricted to purely rotary movement.
Clinical Application28
Use Centric Relation (CR) when:
- Constructing complete dentures (no existing MIP).
- Changing the current occlusal scheme (e.g., due to attrition).
Use Maximal Intercuspal Position (MIP) when:
- Utilizing the existing occlusal scheme for restorative procedures.
Dynamic Occlusion and Ideal Criteria
Definition29
Dynamic occlusion refers to occlusal contacts during mandibular movement. It is powered by masticatory muscles and guided by both the TMJ (posterior determinant) and dentition (anterior determinant).
 |  |
 |
Ideal Occlusal State30
Ideal occlusion occurs when maxillary and mandibular teeth contact simultaneously while condyles are fully seated in the fossae. In this state, teeth do not interfere with harmonious mandibular movement. Functional cusps (maxillary lingual and mandibular buccal) should be evenly distributed in stable contact with opposing fossae to act as vertical stops.
Summary of Ideal Criteria31
- Simultaneous tooth contact in the seated condylar position.
- Maximum intercuspation coincides with the seated position.
- Functional cusps provide stable stops for vertical closure.
- No excessive loading on any single tooth.
- TMJs remain in an unstrained position.
Primary Goals3233
- Mandibular stability
- Axial load
- Absence of interferences
Axial Loading34
Occlusal forces should be distributed down the long axis of the teeth. This ensures even distribution of forces across the periodontal ligament fibers.
Occlusal Schemes35
- Canine guidance: Typical for dentate patients.
- Group function (Unilaterally balanced): Alternative for dentate patients.
- Balanced occlusion: Used for edentate patients.

Canine Guidance
Characteristics
- A form of mutually protective articulation.
- Vertical and horizontal overlap of canines disengages posterior teeth during excursive movements.
- Canines are well-designed as “guiding teeth” due to their length and root support.
- Contraindications: Not indicated if canines are endodontically or periodontally compromised.
Functional Formula
- Dots in back: Signify centric relation contact only on posterior teeth.
- Lines in front: Signify the role of anterior teeth in discluding posterior teeth during excursions.
- Primary Role: Anterior guidance protects the posterior occlusion.
Group Function
Characteristics
- Multiple contacts between maxillary and mandibular teeth on the working side during lateral movements.
- Simultaneous contacts of several teeth act as a group to distribute forces.
- Advantages: Avoids destructive non-working side interferences.
- Disadvantages: Difficult to establish; may place additional load on posterior teeth.
Bilateral Balanced Occlusion
Characteristics
- Bilateral, simultaneous anterior and posterior contact in both centric and eccentric positions.
- Requires at least three contact points (two posterior, one anterior).
- Clinical Use: Too destructive for natural teeth; primarily used in complete dentures to stabilize the prosthesis and prevent tipping.
Summary Checklist36
- Mandibular stability.
- Axial occlusal load.
- No interference on the working side during lateral excursions.
- Disocclusion on the non-working side during lateral excursions.
- Disocclusion of posterior teeth during protrusion.
Occlusal Interferences37
Interferences are undesirable contacts that produce mandibular deviation during closure or hinder smooth movement to and from the intercuspal position.

Types of Interferences38
- Centric
- Working
- Non-working
- Protrusive
Occlusal analysis
Tooth Replacement39
Second lecture of the combined lecture
Impacts of Tooth Loss
Importance of Teeth40
- One of the components of the masticatory system
- Teeth are important for acquisition and chewing of food
- Loss of masticatory efficiency may impact diet
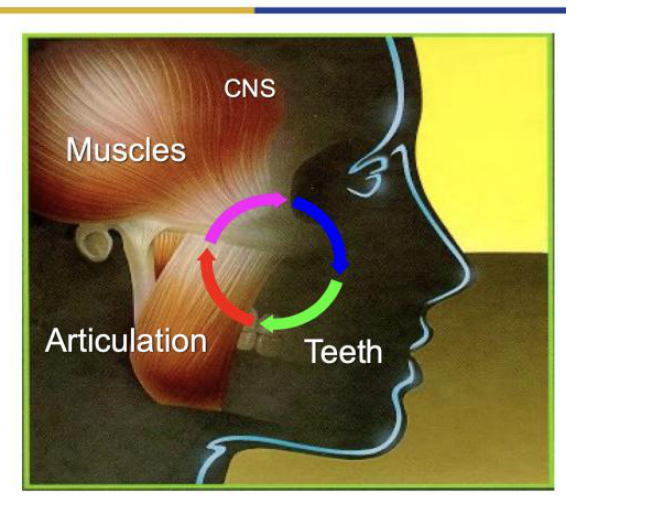
Masticatory System Components
- Teeth
- Periodontal tissues
- Articulatory apparatus
These components form an interconnected biomechanical system.
Dietary and Nutritional Impacts
There are inconsistent reports of dietary changes and nutritional deficiencies associated with tooth loss.
It is theorized that tooth loss reduces masticatory function and chewing ability, which in turn can limit food choices and variety in the diet. For these reasons, dietary intake has been regarded as an intermediate in the pathway between tooth retention and a number of diet-related chronic diseases.
Comparison of Review Articles
Study 1: The nutritional effects of tooth loss (Geissler & Bates, 1984)
- Mixed results: Reduced consumption linked to lower Hemoglobin and Vitamin C.
- No striking differences found in digestion or nutritional status.
- Noted that confounding factors were often missed.
Study 2: Systematic review of longitudinal studies (Gaewkhiew et al.)
- Conclusion: There is at present no strong evidence on the effect of tooth loss on diet and nutrition, with inconsistent results among the few studies identified.
- Additional high-quality longitudinal studies are required to address previous limitations.
Masticatory Performance and Swallowing
Because occlusal contact area is highly correlated with masticatory performance, the loss of molar teeth would be expected to have a greater impact on measures of performance in that the molar has a larger occlusal contact area.
This effect has been demonstrated in individuals with missing molars who reveal:
- A greater number of chewing strokes required.
- A greater mean particle size before swallowing.
Swallowing Threshold
The point at which an individual is prepared to swallow the food bolus is described as the swallowing threshold.
- Superior masticatory ability (correlated with occlusal contact area) achieves greater food reduction at the swallowing threshold.
- Diminished ability to chew is reflected in larger particles at the swallowing threshold.
Study Conclusions (Okamoto et al.)
- A low number of teeth was associated with low masticatory ability in both males and females.
- Low masticatory ability was associated with low plasma albumin levels and low BMI in females.
- Factors important for preventing undernutrition include not smoking, maintaining grip strength, preventing cancer, and maintaining masticatory ability.
Cognitive Impacts
Mechanisms of Cognitive Impact
- Hippocampal Function: Regular sensory stimulation of mastication is essential for maintaining the learning and memory functions of the aged hippocampus.
- Synaptic Density: A decrease in masticatory stimulation may reduce synaptic density in the cerebral cortex by decreasing sensory input.
- Cerebellar Activity: Cerebellar functions seem influenced by masticatory activity; increased activity during chewing may improve certain motor functions.
Study: Tooth loss, chewing efficiency and cognitive impairment in geriatric patients (Elsig et al.)
- Background: Patients with dementia often have poorer oral health and fewer teeth than peers without cognitive impairment.
- Methods: Cross-sectional study of patients aged 75+ (28 with dementia, 22 controls). Chewing efficiency was assessed with a two-colour mixing test.
- Results:
- Demented patients (4.9 teeth) and controls (6.5 teeth) showed no statistically significant difference in tooth number (p = 0.553).
- Chewing efficiency was significantly worse in participants with dementia (p = 0.011) and explained 9.3% of the variance in dementia diagnosis.
- Conclusion: Chewing functions seem more strongly related to cognitive impairment than the number of teeth. Dental examinations for geriatric assessment should be complemented by chewing efficiency tests.
Benefits of Prosthetic Rehabilitation
Partial dentures or other teeth replacement options may help mitigate cognitive decline.
Study Results (Qi et al., 10-year prospective cohort):
- Dentate Participants: Those using dentures had better baseline cognitive function and a slower annual decline in cognitive function (p < 0.01) compared to non-users.
- Edentulous Participants: Denture use was associated with higher baseline cognitive function but not with the rate of cognitive decline.
- Conclusion: Denture use may help protect against cognitive decline in older adults with partial tooth loss. This highlights the potential importance of prosthodontic rehabilitation in preserving cognitive health.
Confounding Variables and Life Course Approach
While tooth loss is a putative risk factor for dementia, systematic review findings are mixed. Three main proposed mechanisms include:
- Compromised nutrition leading to poorer Central Nervous System (CNS) function.
- Reduced somatosensory feedback to the CNS due to fewer interocclusal contacts.
- Chronic periodontitis causing systemic inflammation that affects the CNS.
Critical Examination (Thomson and Barak): Evidence from cohort studies suggests the association may arise from cognitive function earlier in life (childhood).
- Individuals with better childhood cognitive function tend to have better oral health and access to care throughout life, losing fewer teeth.
- Those with lower childhood cognitive ability experience higher disease rates and poorer access to care, resulting in greater incremental tooth loss.
- The observed correlation in old age may reflect a lifelong trajectory rather than a direct causal link between tooth loss and dementia.
Anatomical Changes and Bone Resorption41
Residual Ridge Resorption
After tooth loss occurs:
- The residual ridge no longer benefits from functional stimulus.
- There is a loss of ridge volume in both height and width.
- Ridge volume loss is not predictable for all individuals.
Patterns of Bone Loss
- Bone loss is generally greater in the mandible than in the maxilla.
- Loss is more pronounced posteriorly than anteriorly.
- Resorption produces a broader mandibular arch while constricting the maxillary arch.
The alveolar process is dependent on the presence of teeth and metabolic aspects. Its “rise and fall” dictates the available bone for future interventions, such as implant placement.

Common Etiologies42
- Congenitally missing teeth
- Periodontal disease
- Caries
- Trauma
- Resection (e.g., due to oral cancers)

Prosthetic Options and Management43

Prosthetic Categories44
Fixed Prosthodontics
- Replace the coronal portion of teeth.
- Rigidly fixed to remaining teeth or implants.
- Examples: Bridges (FPD), Implants.
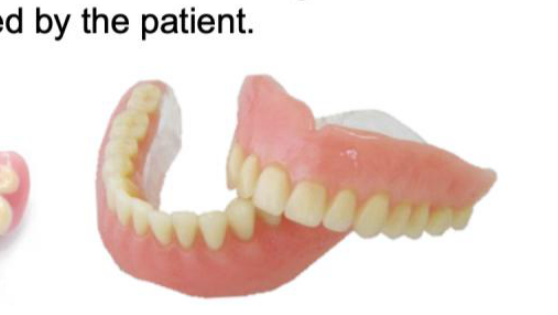
Removable Prosthodontics
- Replacement of missing teeth and supporting tissues.
- Designed to be removed by the patient.
- Example: Dentures (RPD).
 |  |
 |
Managing Patient Expectations45
Loss of teeth represents a non-reversible medical condition. Managing patient expectations is often more challenging than the technical skills required for the procedure. If a patient has never had replacements, their only experience is with natural teeth.

Hierarchy of Similarity to Natural Teeth
- Fixed (Implants): Most similar to a “real” tooth.
- Fixed (Tooth supported): Intermediate similarity.
- Removable: Least similar to a “real” tooth.
Loss of teeth is a non-reversible condition. Managing expectations is a critical component of treatment, as patients often compare prostheses to their natural teeth.
Continuum of Treatment Options: Fixed (implants) Fixed (tooth supported) Removable
This progression moves from the option most similar to a natural tooth to the option least similar.
Shared Decision Making4647
Treatment decisions must be made collaboratively between the clinician and the patient. Involve the patient by providing information on the following differences:
- Technical and Physical Outcomes: Durability and function.
- Esthetic Outcomes: Visual appearance.
- Maintenance: Initial and future costs, plus cleaning requirements.
- Physiologic Outcomes: To what extent the prosthesis “feels” like natural teeth.
Shared decision making involves outlining crucial differences to the patient:
- Technical outcomes
- Physical outcomes
- Esthetic outcomes
- Various maintenance needs
- Initial and future costs
- Physiologic outcomes (proprioception and “feel”)
Immediate Tooth Replacement
Immediate replacement usually refers to restoration immediately after extraction, or temporary prostheses used while awaiting definitive treatment.
Rationale for Immediate Replacement48
- Aesthetics: Preventing self-consciousness regarding missing teeth.
- Function: Maintaining masticatory ability (especially in full clearance cases).
- Soft Tissue Preservation: Maintaining architecture (to be discussed further in FPDs).
Note: Ensure patients are aware of any additional costs associated with immediate replacement.

Temporary Options and Suspension Bridges49
Examples of Immediate Replacement Prostheses
- Vacuform Stent: Essix retainer with a tooth (also known as a “suspension bridge”).
- Immediate FPD: Temporary fixed partial denture.
- Immediate Denture: Removable option inserted at extraction.
- Immediate Implant: Placement and temporary abutment/crown at the time of extraction.
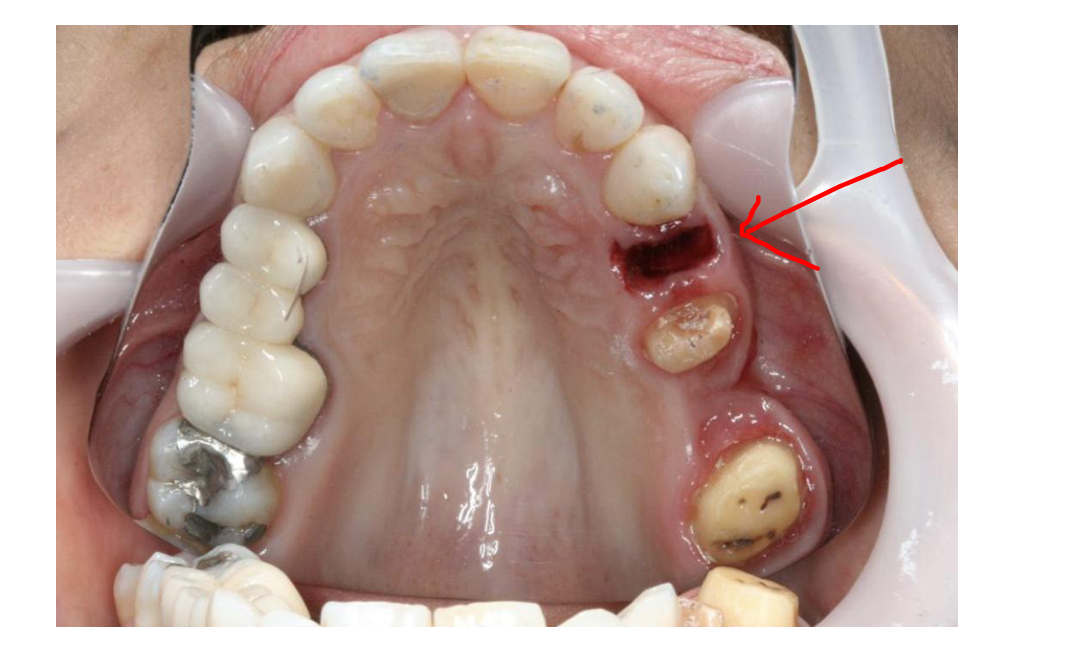
Case Study: Suspension Bridge
- Patient Presentation: Missing lower teeth, gingival bleeding, and halitosis.
- Clinical Context: Unable to proceed to definitive treatment before year-end due to timing.
- Solution: Patient was offered an Essix retainer (suspension bridge) as a temporary solution.
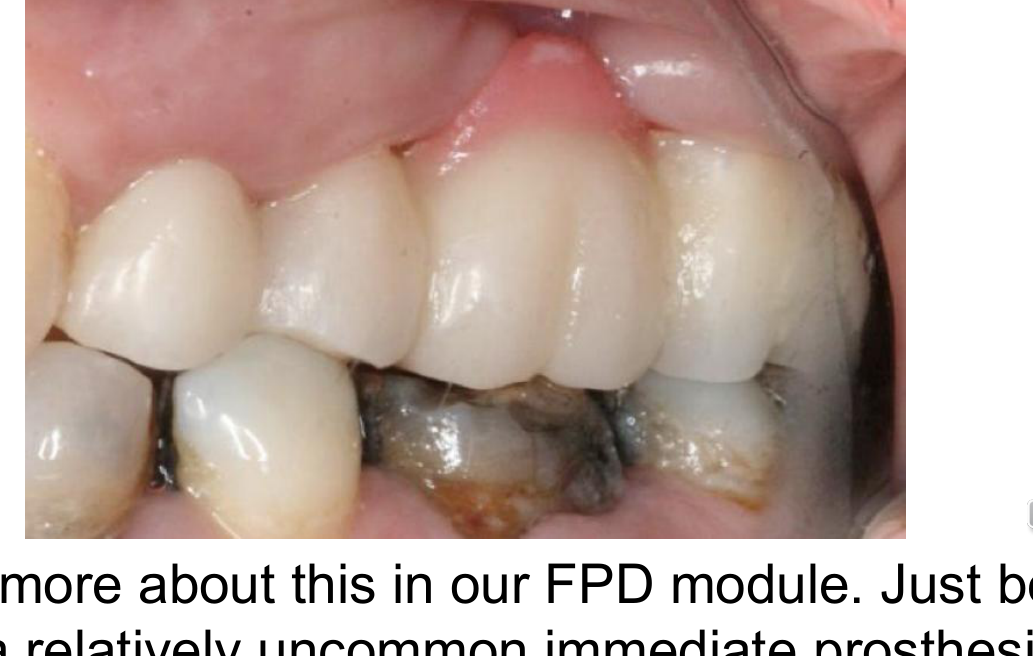
Characteristics of Suspension Bridges
- Indications: Good for short-term replacement of a few teeth (e.g., front tooth replacement while an implant heals).
- Advantages: Very inexpensive and quick to fabricate.
- Disadvantages: Not strong; the patient cannot eat on the prosthesis.
Immediate temporary bridges are a relatively uncommon form of immediate prosthesis. They serve as a fixed interim solution during the healing phase.
 |  |
 |  |
Immediate Dentures
Clinical Considerations
- Can be a Removable Partial Denture (RPD) or a Complete Denture.
- Inserted on the same day as extractions.
- Requires pre-planning and accommodations for tissue inflammation during healing.
Advantages and Challenges
- Maintenance: Easy to modify with relines.
- Technical Limitations: Fit is unpredictable as there is no “try-in” phase; the lab estimates the extraction site contour.
- Patient Management: Requires setting realistic (low) expectations.
- Clinical Time: Significant chairside time is required for adjustments.
Key Features of Immediate Dentures
- Inserted at the date of extraction.
- Requires pre-planning for tissue changes.
- Modification: Easy to maintain and modify via relines.
- Technician Dependence: Fit is unpredictable because a real “try-in” is impossible.
- Chairside Time: Requires significant time for adjustments post-insertion.
Treatment Planning Options
Option 1: Immediate Denture
- Benefit: Immediate replacement; no period without teeth.
- Drawback: The denture will not fit well initially.
- Follow-up: Requires subsequent relines or the fabrication of a new definitive denture.
Option 2: Denture Fabrication After Healing
- Benefit: Potentially lower cost (no immediate relines needed).
- Drawback: Delayed replacement; patient remains edentulous during healing (non-aesthetic).
Case Study: Maxillary Complete Conventional Immediate Denture
Reference: Prosthodontic Rehabilitation and Follow-Up (Yeung et al.).
Clinical Workflow
- Discussion and agreement on full maxillary clearance and immediate denture.
- Maxillary irreversible hydrocolloid impression.
- Fabrication of maxillary occlusal rim.
- Wax-up denture try-in (for aesthetics/records).
- Trimming of the maxillary cast to simulate extractions.
Post-Extraction Instructions
- The denture should be kept in the mouth for the first 24 hours (or overnight) if possible.
- This helps manage initial swelling.
Reline Protocols
- Direct Relines: Required periodically until healing is complete (approx. 3 months for bone remodeling).
- Indirect Reline: Performed once healing is finalized.
Procedure for Relining
- Roughen the denture surface.
- Mix and apply relining material to the tissue surface of the denture.
- Insert denture; patient bites down in Maximum Intercuspation (MIP).
- Perform border molding.
- Remove excess material after the set.
Immediate Implants
Immediate Restoration of Single Implants
This involves placing an implant immediately after tooth extraction. Clinical assessment includes evaluating the compromised tooth (e.g., left central incisor) via visual inspection and periapical radiographs before proceeding with extraction and immediate placement.
Clinical Stages of Immediate Implants
- Fresh extraction site preparation.
- Immediate implant placement.
- Insertion of a temporary abutment.
- Placement of a temporary crown at the time of insertion.
- Evaluation of soft tissue healing (typically reviewed at 6 months post-placement).
Footnotes
-
Original PDF page 1: L4 Occlusion and TMJ and tooth replacement, p.1 ↩
-
Original PDF page 2: L4 Occlusion and TMJ and tooth replacement, p.2 ↩
-
Original PDF page 3: L4 Occlusion and TMJ and tooth replacement, p.3 ↩
-
Original PDF page 4: L4 Occlusion and TMJ and tooth replacement, p.4 ↩
-
Original PDF page 5: L4 Occlusion and TMJ and tooth replacement, p.5 ↩
-
Original PDF page 7: L4 Occlusion and TMJ and tooth replacement, p.7 ↩
-
Original PDF page 12: L4 Occlusion and TMJ and tooth replacement, p.12 ↩
-
Original PDF page 13: L4 Occlusion and TMJ and tooth replacement, p.13 ↩
-
Original PDF page 14: L4 Occlusion and TMJ and tooth replacement, p.14 ↩
-
Original PDF page 15: L4 Occlusion and TMJ and tooth replacement, p.15 ↩
-
Original PDF page 16: L4 Occlusion and TMJ and tooth replacement, p.16 ↩
-
Original PDF page 17: L4 Occlusion and TMJ and tooth replacement, p.17 ↩
-
Original PDF page 18: L4 Occlusion and TMJ and tooth replacement, p.18 ↩
-
Original PDF page 19: L4 Occlusion and TMJ and tooth replacement, p.19 ↩
-
Original PDF page 20: L4 Occlusion and TMJ and tooth replacement, p.20 ↩
-
Original PDF page 21: L4 Occlusion and TMJ and tooth replacement, p.21 ↩
-
Original PDF page 22: L4 Occlusion and TMJ and tooth replacement, p.22 ↩
-
Original PDF page 23: L4 Occlusion and TMJ and tooth replacement, p.23 ↩
-
Original PDF page 24: L4 Occlusion and TMJ and tooth replacement, p.24 ↩
-
Original PDF page 25: L4 Occlusion and TMJ and tooth replacement, p.25 ↩
-
Original PDF page 26: L4 Occlusion and TMJ and tooth replacement, p.26 ↩
-
Original PDF page 27: L4 Occlusion and TMJ and tooth replacement, p.27 ↩
-
Original PDF page 28: L4 Occlusion and TMJ and tooth replacement, p.28 ↩
-
Original PDF page 29: L4 Occlusion and TMJ and tooth replacement, p.29 ↩
-
Original PDF page 30: L4 Occlusion and TMJ and tooth replacement, p.30 ↩
-
Original PDF page 31: L4 Occlusion and TMJ and tooth replacement, p.31 ↩
-
Original PDF page 32: L4 Occlusion and TMJ and tooth replacement, p.32 ↩
-
Original PDF page 33: L4 Occlusion and TMJ and tooth replacement, p.33 ↩
-
Original PDF page 6: L4 Occlusion and TMJ and tooth replacement, p.6 ↩
-
Original PDF page 35: L4 Occlusion and TMJ and tooth replacement, p.35 ↩
-
Original PDF page 36: L4 Occlusion and TMJ and tooth replacement, p.36 ↩
-
Original PDF page 37: L4 Occlusion and TMJ and tooth replacement, p.37 ↩
-
Original PDF page 38: L4 Occlusion and TMJ and tooth replacement, p.38 ↩
-
Original PDF page 39: L4 Occlusion and TMJ and tooth replacement, p.39 ↩
-
Original PDF page 40: L4 Occlusion and TMJ and tooth replacement, p.40 ↩
-
Original PDF page 45: L4 Occlusion and TMJ and tooth replacement, p.45 ↩
-
Original PDF page 47: L4 Occlusion and TMJ and tooth replacement, p.47 ↩
-
Original PDF page 46: L4 Occlusion and TMJ and tooth replacement, p.46 ↩
-
Original PDF page 48: L4 Occlusion and TMJ and tooth replacement, p.48 ↩
-
Original PDF page 49: L4 Occlusion and TMJ and tooth replacement, p.49 ↩
-
Original PDF page 56: L4 Occlusion and TMJ and tooth replacement, p.56 ↩
-
Original PDF page 57: L4 Occlusion and TMJ and tooth replacement, p.57 ↩
-
Original PDF page 60: L4 Occlusion and TMJ and tooth replacement, p.60 ↩
-
Original PDF page 58: L4 Occlusion and TMJ and tooth replacement, p.58 ↩
-
Original PDF page 59: L4 Occlusion and TMJ and tooth replacement, p.59 ↩
-
Original PDF page 61: L4 Occlusion and TMJ and tooth replacement, p.61 ↩
-
Original PDF page 62: L4 Occlusion and TMJ and tooth replacement, p.62 ↩
-
Original PDF page 63: L4 Occlusion and TMJ and tooth replacement, p.63 ↩
-
Original PDF page 67: L4 Occlusion and TMJ and tooth replacement, p.67 ↩