Crowning Teeth
Case 1 : Would you crown this tooth
- it has root surface caries but perhaps you can do crown lengthening
- You may be losing bone and cutting it down
- this is similar to emulating gum disease
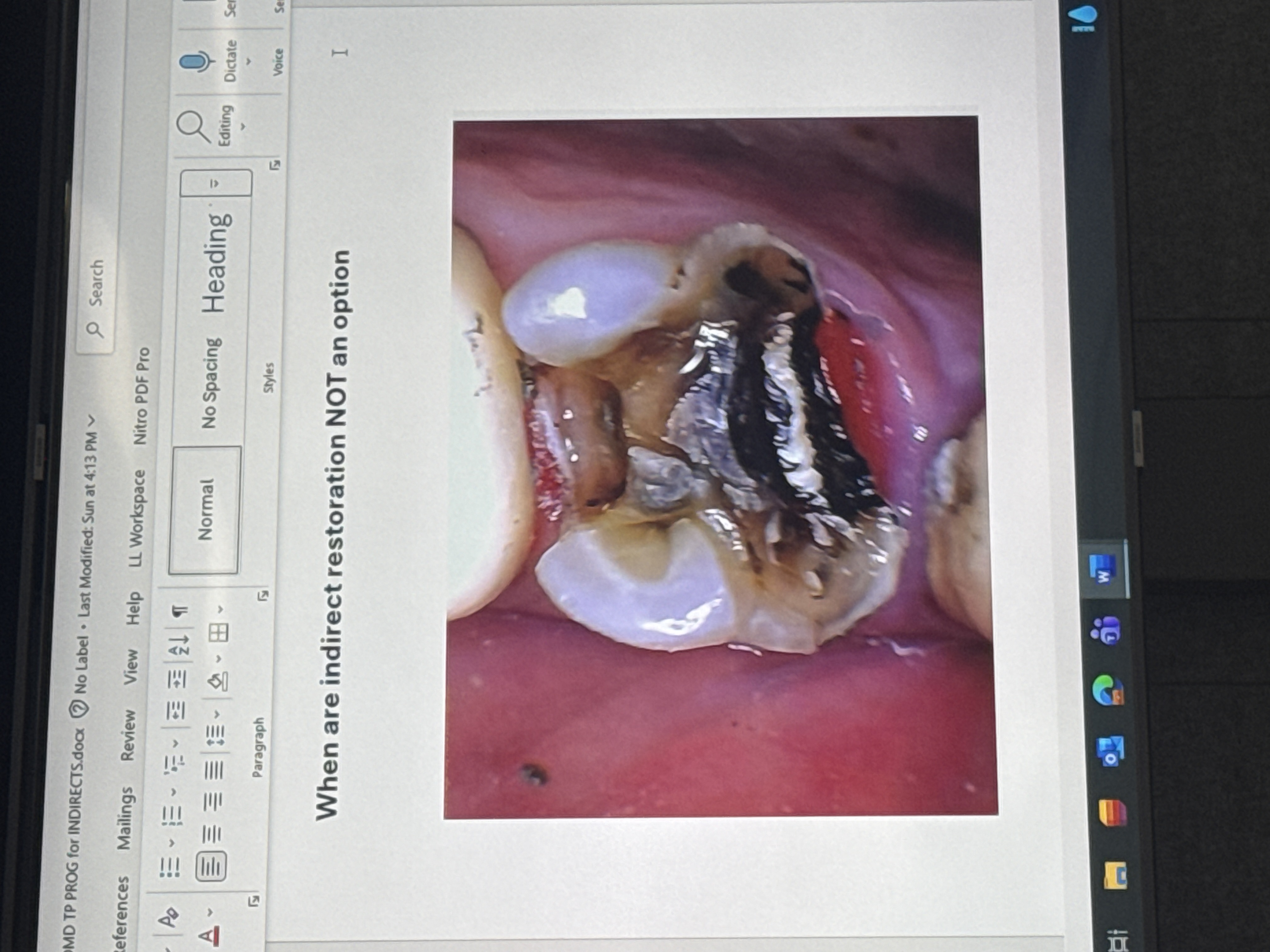
Case: No ferrule

Clinical Findings: No Ferrule
- Root-treated tooth that has become brittle with "nothing left" of the clinical crown
- Inability to establish a margin as everything is at or below the gingival level
- Severe gingival inflammation present around the site
- Iatrogenic damage noted where aggressive tissue removal has created a "dip" or concavity around the tooth - ==Treatment options include crown lengthening surgery (approx. 8,000) - Clinicians must weigh the biological cost against financial cost, as many patients prefer the predictability of an implant over a high-risk restoration==
fractured tooth - unrestorable
- Would need to do crown lengthening and a bunch of other stuff all for it to still be hopeless and very expensive
- No ferrule: No tooth structure remains above bone level to grip or retain a crown
- The tooth is already brittle due to being root-treated and having an active fracture
- Placement of a crown margin on sound tooth structure is impossible; extraction is the only viable option
Section 2: What Caries looks like
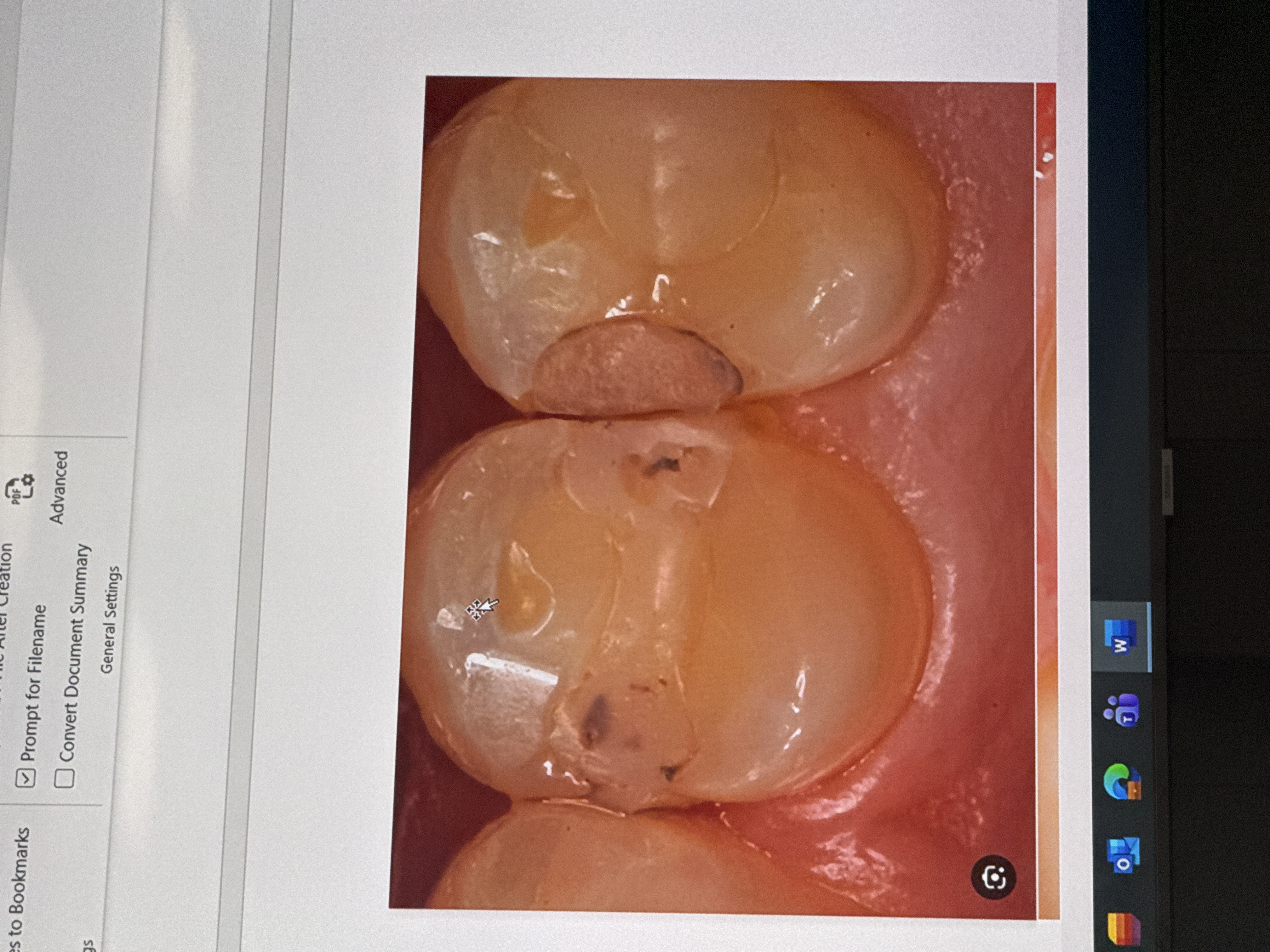
Redo DO above
secondary caries

- Secondary caries refers to recurrent decay occurring at the margins of existing restorations
- This often indicates a failure of the existing restoration or inadequate caries control by the patient
Identification and Diagnosis
- Look for a "halo" effect or white demineralization around cavity margins, which is distinct from simple staining
- Composite resins leak more readily than amalgam, often leading to more rapid or "catastrophic" decay patterns
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Fundamental Principles: Does Crowning Strengthen Teeth?
A critical misconception in restorative dentistry is that crowning a tooth makes it stronger. In reality, crowning does not strengthen a tooth—it merely gathers whatever structural weakness exists and holds it together temporarily.
The Structural Paradox of Crown Preparation
When preparing a tooth for a crown:
- You must cut away significant remaining tooth structure
- A tooth with a massive filling (described as a “big hole” with only a thin “sliver of a wall” remaining, like an empty can) presents particular risk
- During crown preparation, you cut away that remaining thin wall
- What remains to hold the crown? Only whatever ferrule (tooth structure above the gum line) exists—no more surrounding tooth structure remains because it was removed during preparation
The Splinting Effect
The benefit of a crown comes from it acting as a full-coverage splint—similar to placing a hat over a jigsaw puzzle to hold the remaining pieces together as a single functional unit. This is especially critical for strategic abutment teeth supporting removable prostheses.
Crowning as a Last Resort
Crowning is a last resort, not a routine procedure. You should only crown a tooth when it provides a clear advantage to the patient. Critically, you must know when NOT to crown because when a crown fails, the responsibility falls on the clinician. Crown preparation involves constant cutting of tooth structure, which is irreversible.
- Crowns should not be placed solely to adjust occlusion, as this falls under complex prosthodontics.
- Indications for crowning include when a tooth cannot be restored directly without compromising contact points or when fracture is inevitable without full coverage protection.
Case: No Ferrule / Fractured Tooth - Unrestorable
Clinical Presentation
The lecture presents a terminal case illustrating when crowning is impossible:
Findings:
- Tooth condition: Root-treated tooth (brittle), fractured, with “nothing left”
- Structural compromise: Cannot establish a margin; everything is at or below gingival level
- Subgingival fracture extends below the alveolar bone level
- Insufficient clinical crown height to achieve a ferrule effect (360-degree encirclement of sound tooth structure)
- Gingival status: Severe inflammation present
- Iatrogenic damage: The patient has had aggressive tissue removal (“every single gum tissue” removed), creating a “dip” or concavity around the tooth
Prognosis
This represents an unrestorable tooth:
- No ferrule: No tooth structure above bone level to grip or retain a crown
- Root-treated: Already brittle with fracture present
- No margin possible: Cannot place a crown margin on sound tooth structure
- The tooth is hopeless and requires extraction rather than heroic restorative attempts
Financial & Biological Considerations
Saving the tooth via crown lengthening requires significant investment (approx. ==8,000) may offer better long-term value and predictability. Clinicians must transparently present the biological cost== of heroic attempts versus the benefit.
Root Caries
Also discussed in the context of crowning decisions:
- Appearance: Decay on root surfaces, often appearing as subgingival lesions
- Risk factors: Patients prone to root caries present specific contraindications for crowning because decay progresses beneath crown margins (described as going under the “bulging” of the crown)
- Implications: Crown margins on teeth susceptible to root caries will likely fail as decay continues underneath. This makes the patient a poor candidate for crowns regardless of other structural factors.
- Significant risk in elderly patients (70s-80s) due to arthritis and reduced manual dexterity
- Difficulty flossing under pontics leads to plaque accumulation and recurrent caries
- The biological cost of bridges must be weighed against long-term hygiene maintenance capabilities
Summary of Key Clinical Principles:
- Crowning weakens, not strengthens - it gathers existing weakness; preparation removes the very walls that might be holding the tooth together
- Ferrule is essential - without adequate tooth structure above the gum line (ferrule), crowning is contraindicated and the tooth may be unrestorable
- Investigate thoroughly - always remove old restorations, check margins, verify restorability with transillumination, and confirm pulp vitality before preparing for a crown
- Biological cost matters - crown lengthening and heroic measures often sacrifice neighboring teeth (interproximal bone loss) or create periodontal problems; the cost is often too high
- Know when not to crown - unrestorable teeth (no ferrule, fractured, root caries) should be extracted rather than subjected to complex, doomed restorative attempts
- Patient factors - patients prone to root caries are poor candidates for crowns because decay will progress submarginally regardless of the crown’s quality# Crowning Teeth
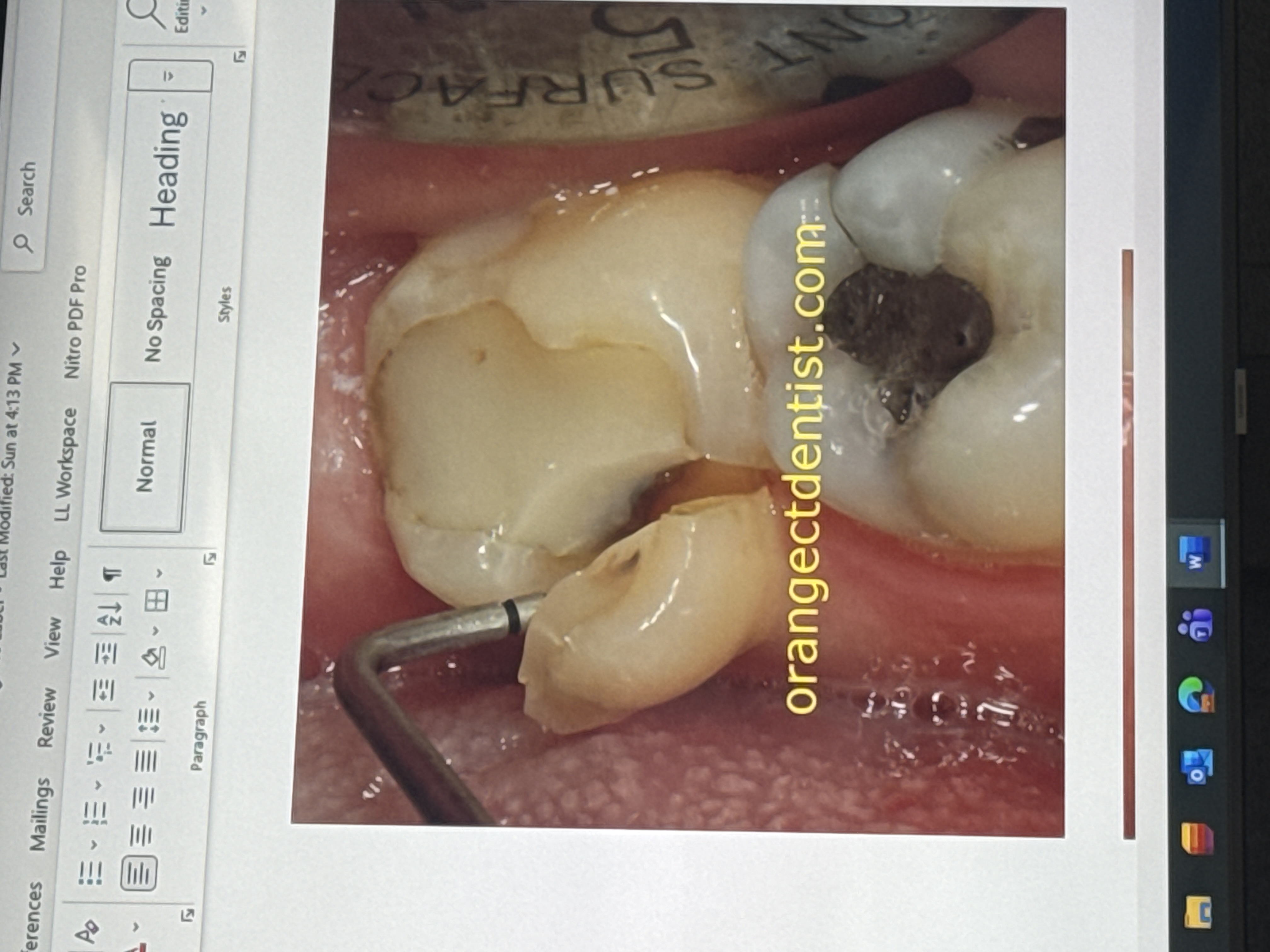
Case 1: Would you crown this tooth?
Clinical Presentation
The lecture presents a challenging case for consideration: a tooth with subgingival margins and root caries extending below the gum line. The question posed is whether this tooth is hopeless or salvageable.
Case: Massive MOD Restoration
A patient presents with tooth 25 featuring a massive MOD restoration where the buccal and palatal walls are significantly compromised. During treatment, a V3 ring clamp compresses the tooth due to lack of support, resulting in open contacts and improper axial contours that create a biological risk for food trapping and caries.
Key observations:
- Subgingival caries (decay below gum level)
- Compromised marginal placement options
- Inflammation present in the gingival tissues
Investigation and Treatment Planning
Is it unsavable? Probably not completely. Several heroic options exist, but each carries significant biological cost:
Crown Lengthening Considerations
Crown lengthening involves surgically removing gum tissue and bone to expose more tooth structure. However, this presents major concerns:
-
Interproximal risk: If the decay involves the interproximal (between teeth) walls, periodontists are hesitant to perform crown lengthening because:
- You lose supporting bone on both the tooth being treated and the neighboring tooth
- You essentially create or emulate gum disease by reducing support for the adjacent tooth
- The neighboring tooth may develop sensitivity and mobility
- Financial Cost: The combined cost of surgery and definitive restoration can reach approximately $6,000.
- You are sacrificing one tooth for the other
-
Biological cost: Crown lengthening is possible but rarely the safest choice. The biological cost is considered **very high
- Biological Width: Placing a margin too subgingivally without surgical intervention results in an invasion of the biological width.**.
Extrusion (Orthodontic Extrusion)
- Possibility: Extruding the tooth (pulling it out slowly using orthodontics) to bring root caries above the gum line
- Limitations:
- Expensive
- Difficult with multi-rooted teeth (e.g., molars with three roots anchored into bone)
- Not normally indicated for molars
Patient Risk Factors: Root Caries
Before considering crowning, assess the patient’s caries risk:
- Root caries susceptibility: If a patient is prone to root caries, crowning may be contraindicated because decay will simply progress underneath the crown margin (described as going under the “bulging”)
- Oral hygiene capability: Can the patient maintain adequate oral hygiene around the crowned tooth?
- Manual Dexterity: For patients in their 70s-90s, conditions like arthritis or tremors can prevent effective flossing, especially under bridges.
- Fixed Partial Dentures: Bridges can create inaccessible areas where plaque accumulates, leading to recurrent caries.
- Bone levels: If bone has receded significantly on the distal, alternative treatments like gingivectomy might be considered, but heroics are generally discouraged
Conclusion for Case 1: Generally, with subgingival margins and significant biological costs for crown lengthening, the prognosis for crowning is poor. A poor margin on a crown creates more trouble than benefit.
Pre-Crowning Investigation Protocols
Before committing to crown preparation, a thorough investigation is mandatory:
Essential Diagnostic Steps
- Pulp Vitality Testing: Confirm pulp status (vital vs. non-vital)
- Radiographic Assessment: Evaluate bone levels, root morphology, and caries extent
- Remove Existing Restorations:
- Take out old fillings completely to visualize the “negative tooth” (remaining tooth structure)
- Warn the patient that investigation may reveal the tooth is unrestorable, necessitating extraction
- Obtain informed consent documenting that the patient understands the worst-case scenario before dismantling restorations
- Critical: One student prepared a beautiful crown prep but forgot to remove the palatal filling, discovering only during preparation that the palatal margin was 2-3mm subgingival once the GIC was removed
Assessing Restorability
Once old restorations are removed:
- Quantify remaining structure: How much tooth is left? How many cusps remain?
- Transillumination: Use a transilluminator to check for cracks or fractures in remaining cusps
- Integrity assessment: Verify the structural integrity of whatever tooth remains
- Margin visualization: Determine exactly where margins will be placed
- Establish strategic value: Is it a key abutment or the last standing tooth in the quadrant?
- Financial assessment: Can the patient afford the full sequence (crown lengthening, post/core, crown) versus alternatives like implants?
Margin Placement Rules:
- Avoid ending margins on composite or GIC (glass ionomer cement)
- Margins must be on sound tooth structure
- Visualize all margins before preparation to avoid surprises
Case Study: The Missed Palatal Margin
A clinical example illustrates the importance of complete investigation:
Scenario: A student performed a “beautiful, beautiful crown prep” but failed to remove the existing palatal restoration first. During preparation, he realized the palatal surface was hitting on GIC (glass ionomer cement). Upon removing the GIC, he discovered the margin was 2-3mm subgingival.
Consequences:
- The case became a crown lengthening case unnecessarily
- The palatal margin location made surgical intervention complex
- While palatal crown lengthening has lower biological cost than interproximal (not destroying bone on the neighboring tooth), it is still undesirable
Clinical Lesson: Always visualize where margins will be before preparation. If a restoration exists on the palatal of a tooth (e.g., upper first molar), and you have enough tooth substance to place the margin above that restoration, you may proceed. However, you must decide and see these factors before preparation, not after. Never tell a patient, “Oops, sorry, we need surgery to cut your gums to lower the margin.”
Case Study: The Hollowed-Out Amalgam
A student investigated a tooth with a 20-year-old amalgam crown. Upon removal of the existing restoration, there was no remaining tooth structure—the tooth was completely hollowed out beneath the crown. Despite being asymptomatic, the tooth required extraction. This highlights the need for risk communication and documenting that investigation could lead to tooth loss before proceeding.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Administrative Procedures (Titanium Software)
Referral Protocols:
- Oral Medicine (Oral Med) and Orofacial Pain (OFP): Students write notes in Titanium under “Referral to Specialist,” which tutors must sign. The actual referral is handled by faculty to ensure proper triage (weekly triage occurs for these specialties).
- Oral Surgery and Periodontics: Students can place these referrals directly in the waitlist system (though waits may be 3-4 years for some services).
- Documentation: Upload photos to Sedexis and provide detailed clinical notes for all referrals.
Worksheet Management:
- Only place items on worksheets that the tutor is comfortable signing.
- Items requiring monitoring but not immediate treatment should be documented in notes rather than worksheets.
- If a procedure is partially completed (e.g., one of two restorations), leave the worksheet item for the next appointment rather than creating new entries.
Estimates:
- Use the estimate calculator to provide patients with comprehensive treatment cost projections.
General Principles and Strategic Considerations
Crowning teeth should not be approached merely as an aesthetic solution or a routine procedure for occlusal adjustment. As general practitioners, the decision to crown must be grounded in biological and strategic necessity rather than convenience.
Key Indications for Crowning:
- Loss of Structural Integrity: When a tooth (e.g., tooth 25 with a large MOD restoration) has lost significant wall structure such that matrix systems (like the V3 ring) compress the tooth excessively and cannot provide adequate molding support.
- Inability to Achieve Biological Goals: When direct restorations cannot establish proper contours or contacts, resulting in open contacts that lead to food impaction and subsequent decay risk.
- Strategic Abutment Support: Teeth supporting removable partial dentures require protection. A tooth with four-surface restorations serving as a denture abutment is vulnerable to fracture under functional load. A survey crown acts like a “hat” holding the tooth together as a single unit, offering better survival chances than unsupported, heavily restored teeth.
Strategic Tooth Assessment: Not every tooth warrants heroic preservation. The strategic value of a tooth must be weighed against the biological and financial costs:
- High Value: Teeth like 36 or 46 (mandibular first molars) that serve as the sole standing teeth in an arch.
- Low Value: Third molars (18/28) that are not strategically positioned; these may be better extracted than subjected to complex root canal therapy and crowning.
- Denture Considerations: For upper full dentures, a single remaining central incisor may compromise vacuum retention and is often not strategic. However, for lower dentures, any retained tooth (even a single incisor) aids stability and is worth preserving with a coping or survey crown.
Additional Clinical Topics
Bridges vs. Implants: Biological Cost Analysis
The lecturer noted having placed no bridges in the last 10 years due to the biological cost:
- Bridges ($6,000): Require reduction of healthy adjacent teeth; difficult for elderly patients to clean; high risk of caries and endodontic complications in abutments.
- Implants ($8,000): Preserve adjacent tooth structure; easier maintenance; more predictable long-term outcome for patients with adequate bone.
Patient Communication and Consent
Effective dental practice requires:
- Honesty: Presenting all options including the worst-case scenario (extraction).
- Contextual Decision Making: Recognizing when “sleeping dogs lie”—leaving asymptomatic, functioning restorations alone rather than risking iatrogenic damage.
- Documentation: Thorough documentation of warnings, patient refusals, and clinical findings protects against complaints.
- Strategic Patience: Building trust over time may allow for more complex treatment later; immediate aggressive treatment in a new patient relationship can lead to conflict if outcomes are poor.