Biomaterials: Dental Cements1
Lecture 8: Biomaterials (Cements)
By Dr Cheryl Fu
Learning Objectives and Introduction
Core Competencies2
- Different permanent and temporary cements and their uses
- Bonding/luting mechanisms
- Clinical steps for cementing a permanent crown (glassy vs crystalline vs metallic)
Lecture Focus
The lecture focuses on the different types of permanent and temporary dental cements, their bonding and luting mechanisms, and the specific clinical steps required for cementing permanent crowns made of various materials such as glassy ceramics, crystalline ceramics, or metals.

Recommended Reading
- Contemporary Fixed Prosthodontics, Chapter 30
- Dental Luting Cements: An Updated Comprehensive Review; Artak Hebayan, Anna Vardanian, Mohmed Isaqali Karobari, Anand Marya, Tavayk Avagyan, Hamid Tebyaniyan, Mohammed Mustafa, Dinesh Rokaya, and Anna Avetisyan
Classification of Cements
Dental cements are broadly categorized based on their intended duration of use and their chemical properties.
Duration of Use3
- Temporary Cements: These include zinc oxide eugenol and eugenol-free formulations, typically utilized during the temporization phase.
- Permanent Cements: These are intended for long-term restoration and are further classified by composition and bonding mechanism.
Classification of Permanent Cements
- By Composition:
- Resin-based cements
- Water-based cements (e.g., Glass Ionomer Cement [GIC], zinc polycarboxylate, and zinc phosphate)
- Hybrids: Compomers (half GIC, half resin)
- By Bonding Mechanism:
- Non-adhesive luting
- Micromechanical retention
- Molecular adhesion
Bonding and Luting Mechanisms
The term “lute” originates from the Latin lutum, meaning mud or clay. In a clinical context, a luting agent is a substance—such as cement, wax, or clay—applied to a joint area to create a tight seal. Historically, these agents were used to mechanically link restorations to a prepared tooth.
Mechanism of Action4
- Luting cements function primarily through mechanical friction.
- They are traditionally used for the final placement of cast restorations.
- During the setting process, the cement powder transforms into a hardened matrix.
Sandpaper Analogy
Luting is compared to two pieces of sandpaper pressed together; the grit (hardened cement matrix) creates mechanical friction that prevents sliding.

Clinical Considerations
- Luting cements often present solubility issues because their matrix consists of ionic salts.
- A parallel preparation is essential to ensure the crown cannot be removed without shearing the cement particles.
Micromechanical Bonding5
Micromechanical bonding is a primary retention mechanism for resin cements and involves specific surface treatments for different restorative materials:
- Dentin and Enamel: Prepared using phosphoric acid etching
- Etching removes minerals and exposes collagen fibrils, which are then infiltrated by resin monomers.
- Glassy Ceramics: Prepared using hydrofluoric acid etching.
- Metal and Zirconia Crowns: Prepared via sandblasting
- Sandblasting (airborne particle abrasion) uses aluminum oxide to increase surface area and roughness.
Molecular Adhesion
Molecular adhesion involves the use of physical forces or chemical interactions to secure a restoration.
Adhesion Principles
- Utilizes physical forces such as Van der Waals forces or chemical ionic bonding.
- Employs functional monomers such as 10-MDP.
- The 10-MDP molecule interacts chemically with metal oxides and tooth calcium.
Clinical Limitations
- Current cement technology cannot rely solely on molecular adhesion for retention.
- Supplemental methods of retention, such as maintaining parallel preparation walls, remain necessary.
Ideal Properties of Cements
Characteristics of an Ideal Luting Agent6
- Low film thickness
- Low film thickness (maximum 25 microns per ADA standards)
- Suitable working time and setting time
- High compressive strength
- Similar elastic modulus as dentin
- Biocompatible
- Plaque/caries inhibition
- Low solubility
- Low microleakage
- Easy removal of excess
- High retention
Biocompatibility and Antimicrobial Effects
Tissue Interaction and Sensitivity7
- Cements should ideally not interact with bodily tissues, and not cause sensitivity or allergic reactions.
Pulp Sensitivity
Zinc phosphate has a low initial pH (~2) which may cause sensitivity if the preparation is close to the pulp.
Antimicrobial Properties
- Antimicrobial effects are desired to prevent marginal caries.
- Evidence is inconclusive regarding whether low-level fluoride or other antimicrobial agents provide long-term inhibition (e.g., effectiveness over a 10-year period).
- While GICs release fluoride (acting as a "fluoride bank"), evidence is inconclusive if they can be effectively "recharged" by toothpaste.
Working and Setting Time
Clinical Handling8
- Ideally, there should be enough time to mix the cement, seat the restoration, and clean up excess in an appropriate timeframe.
- Ideal Time: Enough time to mix, seat, and clean up (typically >2 mins).
- Risks: If setting takes too long (>10 mins), it is inefficient. Moving the restoration during the setting phase can cause cracks.
- Tack cure resin cements offer clinical benefits for efficiency.
- Caution: If excess resin cement is not fully removed before the final cure, it becomes extremely difficult to remove.
Microleakage and Solubility
Impact of Solubility on Retention9
- Solubility of cements in the oral environment (water) can lead to microleakage at the marginal interface and possible loss of retention.
- Zinc phosphate and zinc polycarboxylate: High solubility.
- Resin cements: Low solubility.

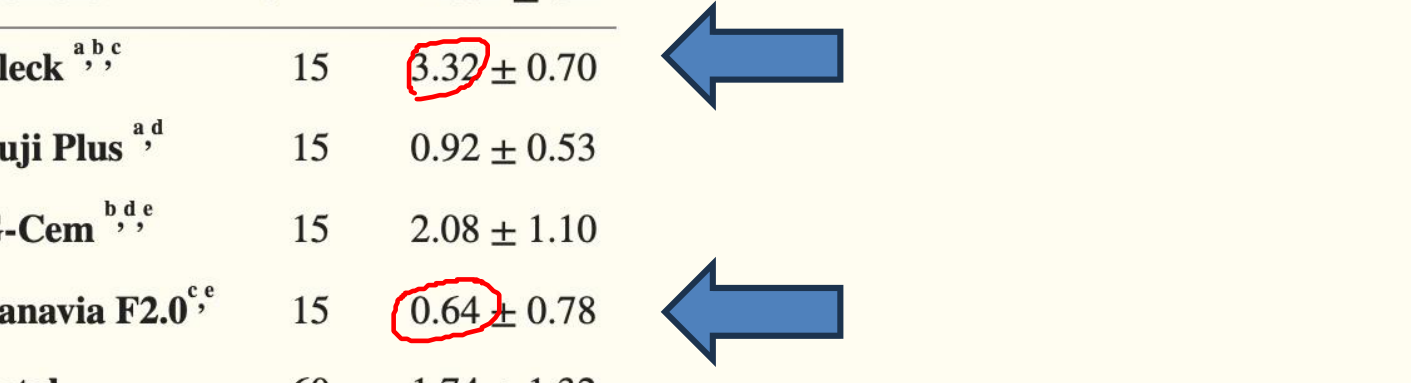
Comparative Microleakage Data10
Microleakage in Restorations with Open Margins (mm)
| Cement | N | Mean ± SD |
|---|---|---|
| Fleck (Zinc Phosphate) | 15 | 3.32 ± 0.70 |
| Fuji Plus | 15 | 0.92 ± 0.53 |
| G-Cem | 15 | 2.08 ± 1.10 |
| Panavia F2.0 | 15 | 0.64 ± 0.78 |
| Total | 60 | 1.74 ± 1.32 |
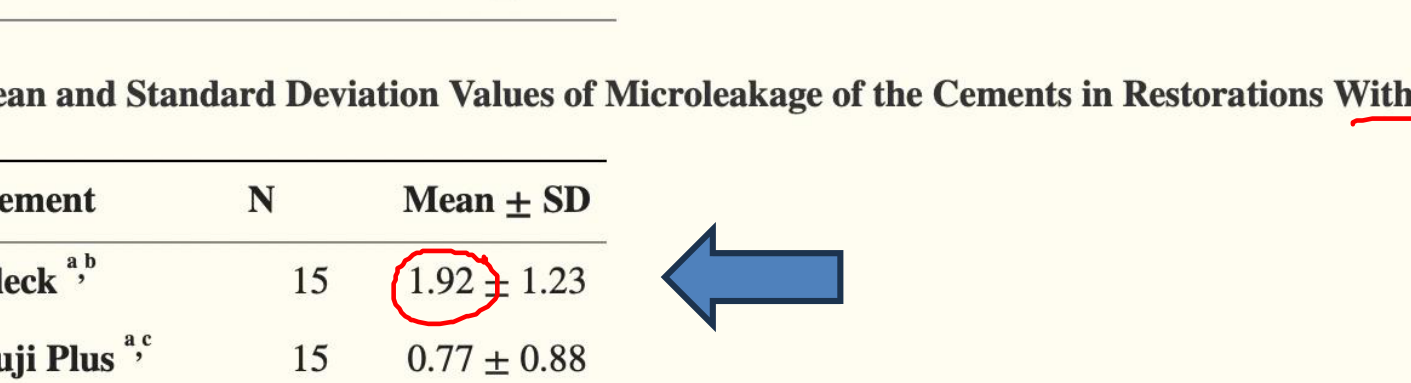
Microleakage in Restorations with Closed Margins (mm)
| Cement | N | Mean ± SD |
|---|---|---|
| Fleck (Zinc Phosphate) | 15 | 1.92 ± 1.23 |
| Fuji Plus | 15 | 0.77 ± 0.88 |
| G-Cem | 15 | 1.25 ± 1.07 |
| Panavia F2.0 | 15 | 0.18 ± 0.14 |
| Total | 60 | 1.03 ± 1.11 |
Note: While resin cements show lower microleakage, they are not considered perfect in all clinical scenarios.
 |  |
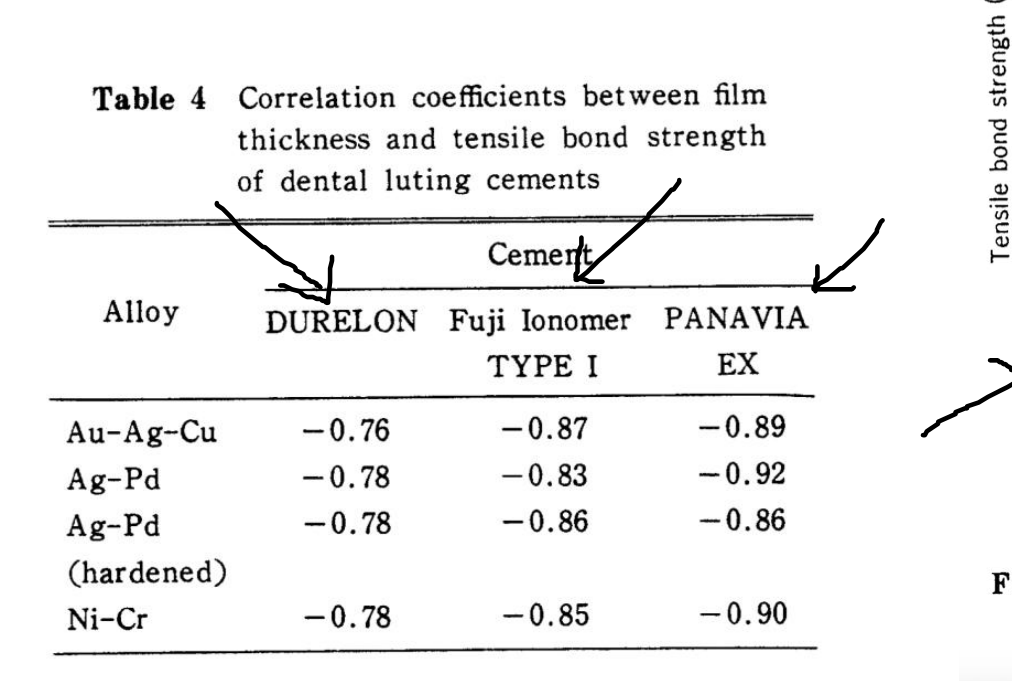
Film Thickness and Bond Strength
Correlation Between Film Thickness and Bond Strength11
Research indicates a strong negative correlation between film thickness and tensile bond strength across various dental alloys.
- Lower film thickness is associated with better seating and higher micro-tensile bond strength. ADA standards recommend a maximum of 25 microns for luting agents.
Correlation Coefficients (Film Thickness vs. Tensile Bond Strength)
| Alloy | DURELON | Fuji Ionomer TYPE I | PANAVIA EX |
|---|---|---|---|
| Au-Ag-Cu | -0.76 | -0.87 | -0.89 |
| Ag-Pd | -0.78 | -0.83 | -0.92 |
| Ag-Pd (hardened) | -0.78 | -0.86 | -0.86 |
| Ni-Cr | -0.78 | -0.85 | -0.90 |
 |  |
Elastic Modulus and Compressive Strength
Stress Distribution and Material Compatibility12
- If a cement has a similar elastic modulus to dentin, there is less stress concentration at the interface.
- Studies suggest that fractures in ceramic restorations may originate within the cement layer.
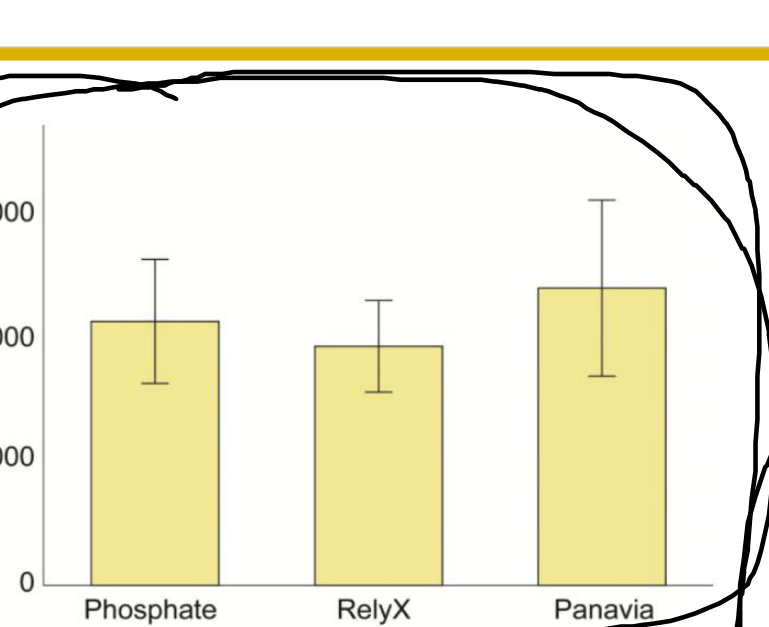 |  |
Material-Specific Considerations
- Zirconia: Fracture load of monolithic zirconia crowns may not be significantly affected by the type of cement used.
- Fracture strength is often independent of the cement's compressive strength.
- Lithium Disilicate: Chemical adhesion is essential for the fatigue behavior and load-bearing capacity of lithium disilicate glass-ceramic crowns. Weak adhesion increases stress concentration in the crown and cement, impairing performance.
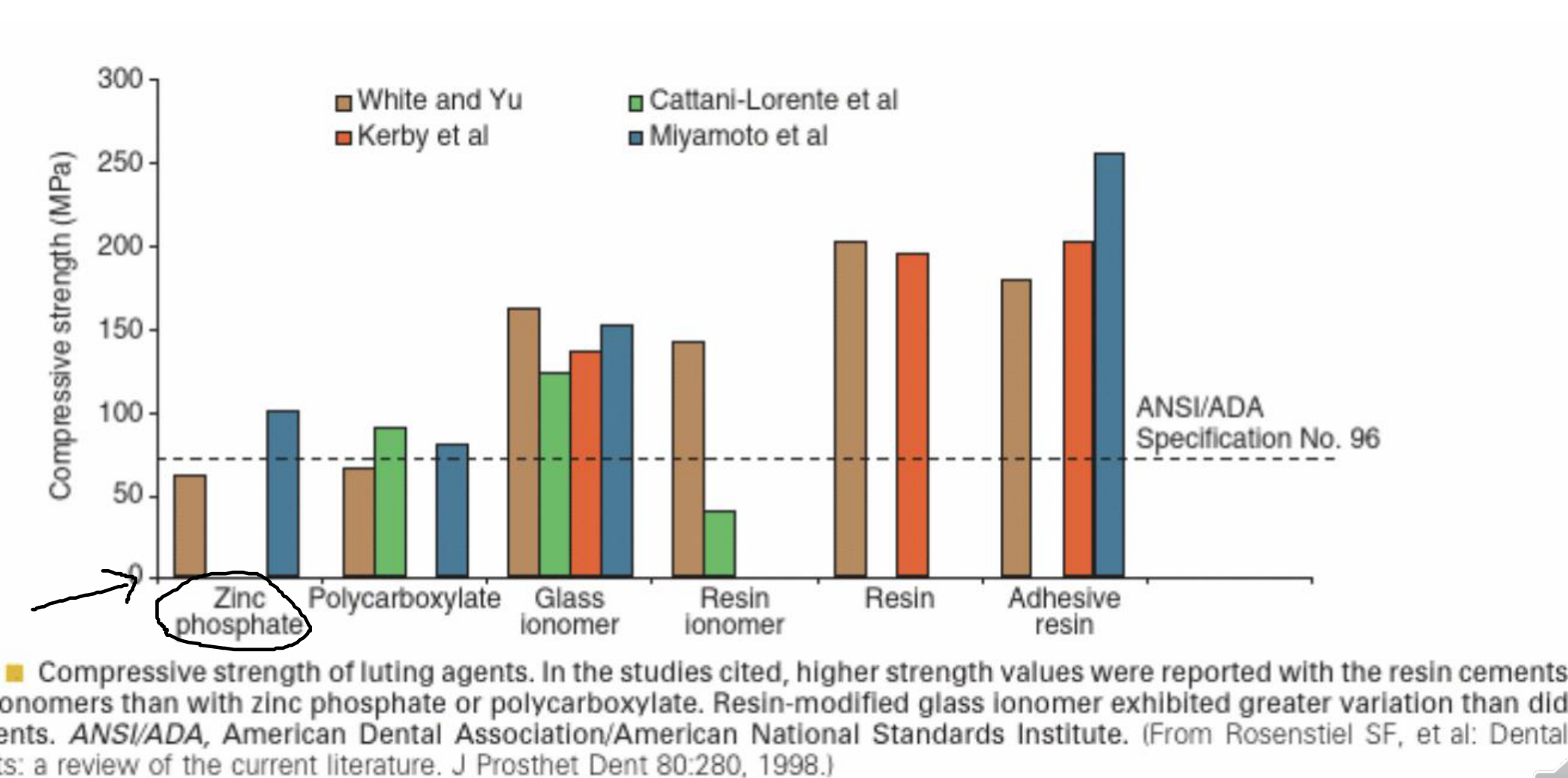
Comparative Compressive Strength13
According to ANSI/ADA Specification No. 96 and literature reviews (Rosenstiel et al.):
- Resin Cements: Highest reported strength values.
- Glass Ionomers: Higher strength than zinc phosphate or polycarboxylate.
- Resin-Modified Glass Ionomer (RMGI): Exhibits greater variation in strength compared to other categories.
- Zinc Phosphate and Polycarboxylate: Generally lower compressive strength values.
- Zinc phosphate generally has the lowest compressive strength compared to modern resin-based alternatives.
Retention and Failure Loads
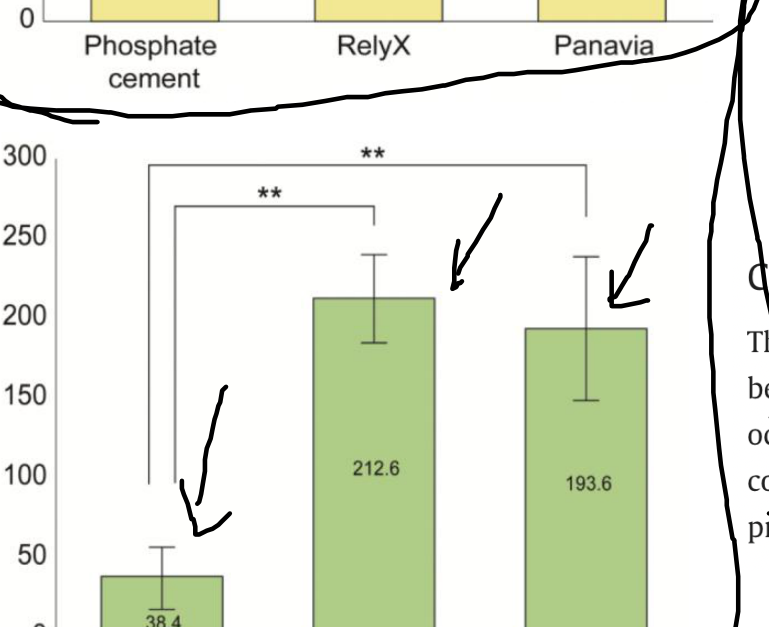
Failure Loads in Lithium Disilicate Crowns14
Lithium disilicate crowns cemented adhesively with resin cement demonstrate higher failure loads and fewer cases of debonding compared to Glass Ionomer Cement (GIC).
Mean Failure Loads (N)
| Groups | Mean (SD) |
|---|---|
| Composite group | 306.6 (193.8) |
| GIC group | 94.7 (48.2) |
 |  |
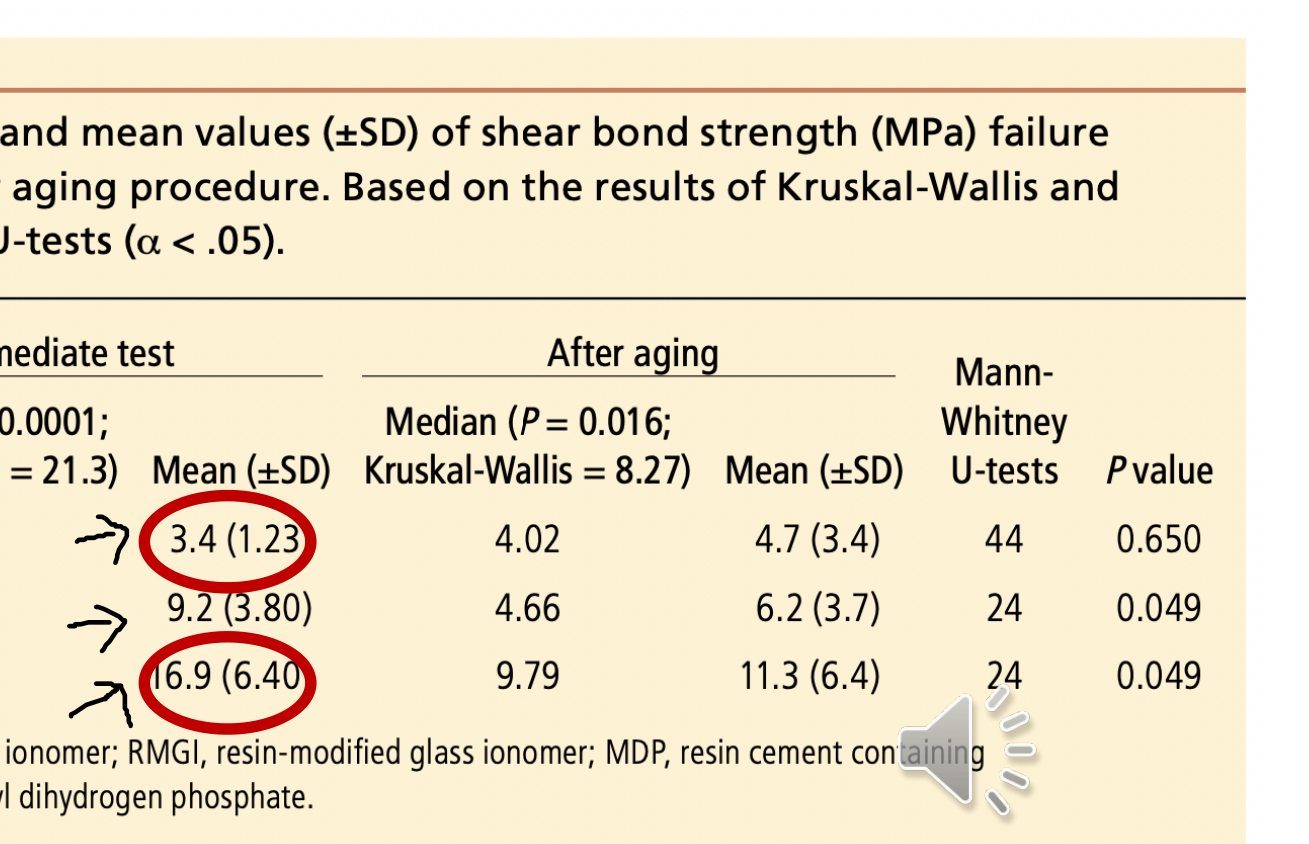
Zirconia-Dentin Complex Bond Strength15
Literature regarding zirconia crowns is mixed; some studies suggest MDP-containing cements promote better bond strength, while others find no significant difference.
- Cements containing 10-MDP show significantly higher immediate bond strength to zirconia compared to GIC.
Shear Bond Strength (MPa) and Stability
| Cement Type | Immediate (Mean ± SD) | After Aging (Mean ± SD) | P value |
|---|---|---|---|
| GI (Glass Ionomer) | 3.4 (1.23) | 4.7 (3.4) | 0.650 |
| RMGI | 9.2 (3.80) | 6.2 (3.7) | 0.049 |
| MDP (Resin with MDP) | 16.9 (6.40) | 11.3 (6.4) | 0.049 |
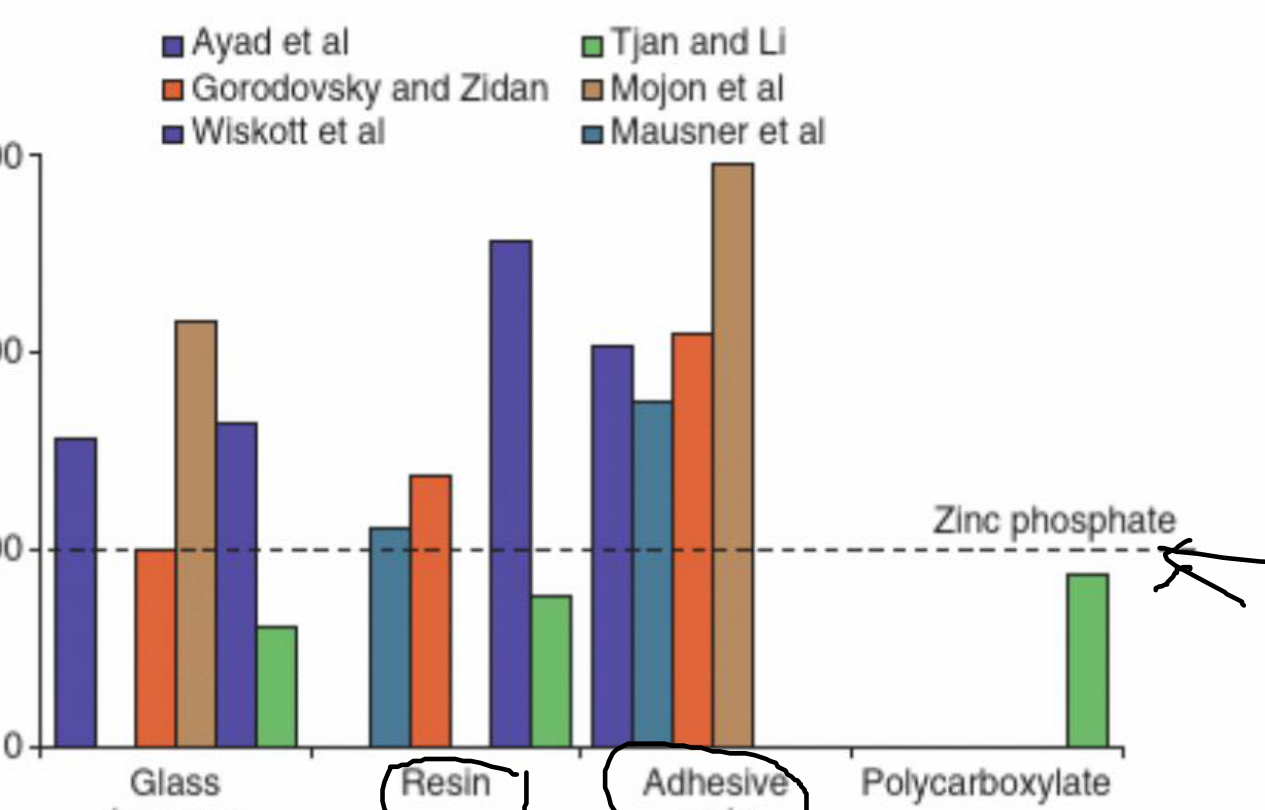
Comparative Crown Retention16
In vitro studies evaluating the effect of luting agents on crown retention (normalized against zinc phosphate) show:
- Adhesive Resins: Consistently higher retention than zinc phosphate.
- Conventional Resins and Glass Ionomers: Yielded less consistent results across different studies.
Types of Dental Cements
Composition and Properties17
- Basic composition: Zinc oxide + Eugenol + Rosin + Zinc Acetate
- Strength: Low strength and high solubility in the oral environment.
- Biocompatibility: Provides a potential “sedative” effect for the pulp and is otherwise biocompatible.

Zinc Oxide Eugenol
Clinical Considerations
- Resin Inhibition: Eugenol can inhibit resin polymerization.
- Primary Use: Indicated as a temporary cement.
Zinc Phosphate
Composition and History18
- Basic composition: Zinc oxide + magnesium oxide + phosphoric acid + water + buffers
- Background: Popular cement for use in traditional cast restorations; has been in use since the 1800s.
 |  |
Clinical Performance
- Film Thickness: Acceptable film thickness of 25μm.
- Handling: Ease of removal of excess material after setting.
- Working Time: Acceptable working time of approximately 5 minutes.
Biocompatibility
- Potential issues due to the inclusion of phosphoric acid (pH 2 at the time of cementing).
- Generally well tolerated if the preparation is not too close to the pulp.
Zinc Polycarboxylate
Composition and Adhesion19
- Basic composition: Zinc oxide + polyacrylic acid
- Development: Attempts to address biocompatibility issues of zinc phosphate by utilizing polyacrylic acid
- Large molecules in polyacrylic acid prevent penetration into dentine tubules, further improving biocompatibility.
- Adhesion: Exhibits some adhesion to the tooth surface through chelation of calcium (note: does not adhere to cast metal surfaces).
 |  |
Handling and Indications
- Technique Sensitivity: Potentially sensitive due to the mixing of viscous powder and liquid (mitigated via capsules).
- Working Time: Very short working time of under 3 minutes.
- Indications: Recommended for high retention preparations or preparations close to pulp horns.
Glass Ionomer Cement
Composition and Bonding20
- Basic composition: Polycarboxylate + fluorialuminosilicate glass + water + tartaric acid
- Bonding: Ionic bonding to tooth structure.

Clinical Advantages
- Biocompatibility: Good biocompatibility and theoretically anticariogenic.
- Aesthetics: Translucent properties provide good aesthetic results.
Considerations
- Moisture Sensitivity: Potential for water absorption during early setting, which can lead to erosion of the weakened material.
- Post-operative Sensitivity: Concerns regarding sensitivity are not supported by literature when manufacturer guidelines are followed.
Resin Modified Glass Ionomer
Composition and Improvements21
- Basic composition: GIC + resin
- Enhancements: Inclusion of resin and photoactivators improves upon standard GIC issues.
- Mechanical Properties: Resin matrix improves compressive and fracture strength; suggests improved retention and bond strength.

Clinical Handling
- Cleanup: Can be harder to remove excess; tack curing is recommended.
- Latest Generation Features:
- Excellent handling, consistency, and bond strength.
- Easy clean-up and one-step application.
- Moisture tolerant; no isolation required.
- High fluoride release.
Indications and Contraindications
- Indications: Ideal for cementation of zirconia, PFM, and lithium disilicate restorations.
- Contraindications: Some studies suggest it is contraindicated for all-ceramic crowns due to the risk of fracture after water absorption.
Resin Based Cements
Composition and Characteristics22
- Basic composition: Resin + filler (lower filler ratio utilized for lower film thickness).
- Retention: Offers micromechanical retention.
- Physical Properties: Very high compressive strength and the least soluble of the cement types.

Clinical Application
- Procedure: Similar to restorative composite; requires the exact same steps
- The procedure specifically requires etching and bonding steps.
- Curing Options: Available in self-cure, dual-cure, or light-cure options.
- Technique Sensitivity: Highly sensitive to moisture control.
- Cleanup: Removal of excess may be difficult if not performed at the tack cure stage.
- Cost: May be more expensive than other options.
Adhesive Monomers and Panavia
Panavia and 10-MDP
Panavia is a resin cement featuring the bifunctional monomer 10-methacryloyloxydecyldihydrogen-phosphate (MDP).
- Metal Bonding: 10-MDP interacts with metal oxides via the hydrophilic phosphoric acid end group.
- Dentin Bonding: 10-MDP facilitates a chemical bond with dentin through the formation of MDP-Ca insoluble salts.
Chemical Bonding of 10-MDP
10-MDP is a notable monomer that allows for chemical bonding to both metal oxides (such as zirconia and metal) and tooth calcium.
Structure of Adhesive Monomer MDP
| Part | Group |
|---|---|
| Polymerisable group | Polymerisable group |
| Hydrophobic group | Aliphatic chain (CH2)10 |
| Hydrophilic group | Phosphate group (P-OH) |
Indications and Contraindications Summary
Clinical Indications Table23
| Restoration | Indication | Contraindication |
|---|---|---|
| Cast crown, metal-ceramic crown, partial FDP | 1, 2, 3, 4, 5, 6, 7 | — |
| Crown or partial FDP with poor retention | 1, 2 | 3, 4, 5, 6, 7 |
| MCC with porcelain margin | 1, 2, 3, 4, 5, 6, 7 | — |
| Casting on patient with history of sensitivity | Consider 4 or 7 | 2 |
| Pressed, high-leucite, ceramic crown | 1, 2 | 3, 4, 5, 6, 7 |
| Slip-cast alumina crown | 1, 2, 3, 4, 6, 7 | 5 |
| Ceramic inlay | 1, 2 | 3, 4, 5, 6, 7 |
| Ceramic veneer | 1, 2 | 3, 4, 5, 6, 7 |
| Resin-retained partial FDP | 1, 2 | 3, 4, 5, 6, 7 |
| Cast post-and-core | 1, 2, 3, 5, 6 | 4, 7 |
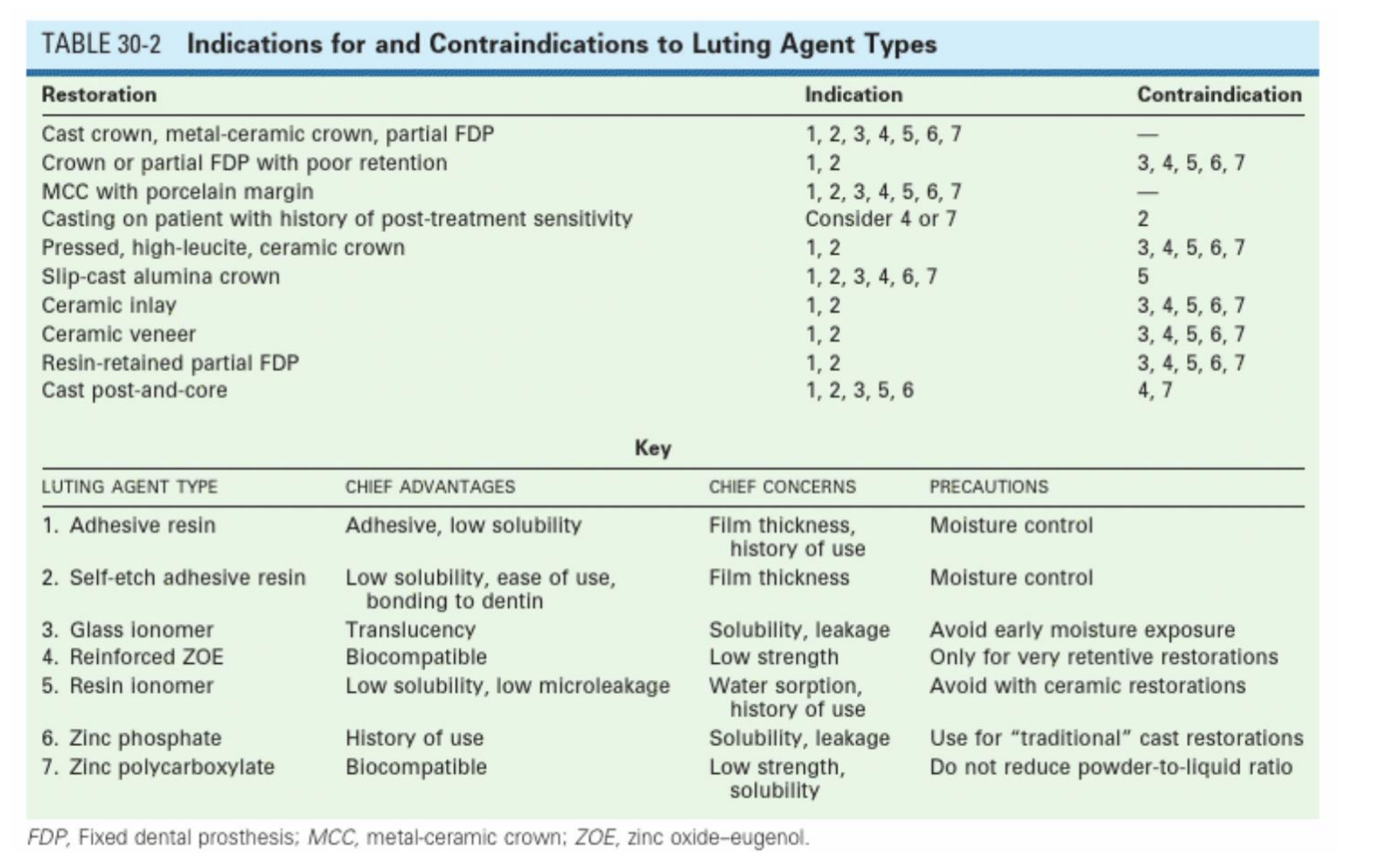
Luting Agent Key
- Adhesive resin: Adhesive, low solubility. (Precaution: Moisture control)
- Self-etch adhesive resin: Low solubility, ease of use, bonding to dentin. (Precaution: Moisture control)
- Glass ionomer: Translucency. (Precaution: Avoid early moisture exposure)
- Reinforced ZOE: Biocompatible. (Concern: Low strength; Use only for very retentive restorations)
- Resin ionomer: Low solubility, low microleakage. (Precaution: Avoid with ceramic restorations)
- Zinc phosphate: History of use. (Concern: Solubility, leakage)
- Zinc polycarboxylate: Biocompatible. (Concern: Low strength, solubility; Do not reduce powder-to-liquid ratio)
Abbreviations: FDP (Fixed dental prosthesis); MCC (Metal-ceramic crown); ZOE (Zinc oxide–eugenol).
Clinical Cementation Procedures
Pre-Cementation Requirements24
- Ensure the permanent crown seats fully.
- Obtain patient consent for cementation.
- Determine material type: Zirconia vs. Lithium Disilicate crowns.
Glassy Ceramic Crowns
Hydrofluoric Acid Etching25
Prior to returning the crown, the laboratory may have already etched the internal fitting surface with hydrofluoric acid (e.g., Ceram Etch 9% hydrofluoric gel).
 |  |
Laboratory and Surface Preparation
Chemical Reactions:
- SiO₂(s) + 4 HF(aq) → SiF₄(g) + 2 H₂O(l)
- 4 SiF₄(g) + 3 H₂O(l) + 2 HF(aq) → 3 H₂SiF₆(aq) + H₂SiO₃(aq)
Etching Time Comparisons:
- 1% HF for 20 seconds (10 µm surface change at x2,000 magnification).
- 1% HF for 120 seconds (Significant surface change at x2,808 magnification).
Laboratory Surface Conditioning
- Hydrofluoric Acid Etching: The lab may etch the internal fitting surface with hydrofluoric acid (e.g., 9% HF gel) before delivery.
- Silane Coupling Agent: Application of agents such as 3-methacryloxypropyltrimethoxysilane (MPS).
- Forms a bridge between organic compounds in resin cements and inorganic ceramic molecules.
- Improves bond strength.
- Increases surface energy and decreases contact angle for better resin/adhesive contact.
Research Reference
Influence of the Multiple Layers Application and the Heating of Silane on the Bond Strength between Lithium Disilicate Ceramics and Resinous Cement — Silva et al.
Laboratory Preparation Steps
- Etching: Internal fitting surface etching with hydrofluoric acid (e.g., 9% HF gel).
- Silanization: Use of 3-methacryloxypropyltrimethoxysilane (MPS) to create a chemical bridge between the resin cement and the ceramic, enhancing bond strength and surface wettability.
Research Reference
Influence of the Multiple Layers Application and the Heating of Silane on the Bond Strength between Lithium Disilicate Ceramics and Resinous Cement — Silva, Maia, Silva, Miranda, and Brandt.
Zirconia Crowns
Laboratory Surface Treatments26
Zirconia cannot be etched with traditional acids. Preparation requires:
- Micromechanical Treatments:
- Airborne particle abrasion (sandblasting) to increase surface roughness (Pressure ~1 bar).
- Risk: High pressure can cause micro-cracks in the zirconia structure.
- Chemical Treatments:
- Hot acid treatment (e.g., sulfuric acid and hydrogen peroxide).
- Silica coating (aluminum oxide particles coated with silica).
- Silica Coating: Blasting silica-coated alumina to "lock" silica into the surface for better chemical adhesion.
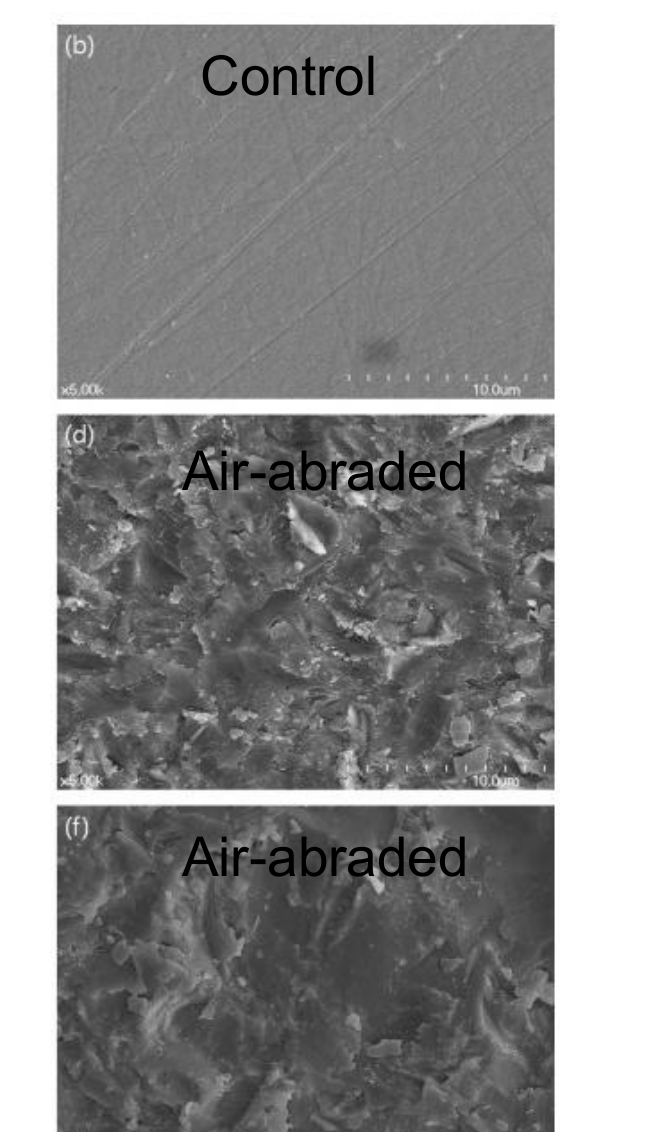
Surface Treatments and Cleaning
Research Reference
Effects of airborne-particle abrasion protocol choice on the surface characteristics of monolithic zirconia materials and the shear bond strength of resin cement — Moon et al.
Clinical Cleaning and Application27
Post-Try-In Cleaning
Once the try-in procedure is completed, the fitting surface must be cleaned:
- Specialized Cleansers: Use Katana Cleaner or Ivoclean.
- Alternative: Phosphoric acid can be used to remove saliva contaminants from the glassy ceramic surface
Phosphoric Acid Use
Phosphoric acid shows mixed results for cleaning; some studies suggest it may weaken the bond on certain ceramics. .
(Page contains no unique text beyond the header context provided in the assignment; content is identical to the cleaning protocols for glassy ceramics.)
Zirconia Surface Decontamination
Cleaning Zirconia Surface Prior To Bonding: A Comparative Study of Different Methods and Solutions — Sulaiman et al.
Study Conclusions:
- Airborne particle abrasion, zirconia cleaning solutions, and hydrofluoric acid are all feasible for removing saliva contamination.
- Airborne particle abrasion provided the best outcome for restoring bond strengths to uncontaminated levels.
- This is followed in effectiveness by HF acid or specialized intaglio cleaners.
Variolink Esthetic LC Protocol (Inlays < 2mm)
1. Try-In Phase
- Apply Try-In paste.
- Seat restoration for evaluation.
- Clean restoration after try-in.
- Ensure isolation/dryness.
2. Restoration Preparation
- Rinse with water and air dry.
- Apply Monobond Etch & Prime (20s scrub, 40s reaction time).
- Rinse with water and air dry.
3. Tooth Preparation
- Clean with water and air dry.
- Optional: Total Etch (15-30s enamel, 15s dentin).
- Rinse and air dry.
- Apply Adhese Universal (20s scrub).
- Air thin to a film and light cure (10s).
4. Cementation and Finishing
- Apply Variolink Esthetic LC and seat restoration.
- Tack cure margins (2s).
- Remove excess cement.
- Apply Liquid Strip (glycerin gel).
- Final light cure (10s per segment).
- Polish and apply Fluor Protector.
Clinical Cementation Protocol
Panavia F 2.0 Protocol for Zirconia
- Tooth Priming: Mix equal amounts of ED PRIMER II A & B. Apply to the tooth and wait 30 seconds. (Note: This primer initiates the cement set).
- Drying: Gently air dry the tooth surface.
- Dispensing: Dispense equal amounts of Paste A & B.
- Mixing: Mix Paste A & B for 20 seconds.
- Application: Apply the mixed paste to the internal surface of the sandblasted zirconia crown.
Panavia F 2.0 Finishing Procedures
6. Excess Removal:
- Remove excess cement.
- For easier cleanup, tack-cure excess for 2-3 seconds before removal.
7. Final Polymerization (Choose A or B):
- Option A (Light Cure): Cure margins for 20 seconds per surface (Conventional/LED) or 5 seconds per surface (Plasma arc/Fast halogen).
- Option B (Self Cure): Apply OXYGUARD II to the margins and wait 3 minutes to ensure anaerobic cure.
Metal and PFM Crowns
Panavia F 2.0 Protocol for Metal Restorations28
- Surface Prep: Sandblast the internal surface, wash, and dry.
- Metal Priming: Apply ALLOY PRIMER to the internal surface of precious metal restorations.
- Tooth Priming: Mix ED PRIMER II A & B, apply to tooth, and wait 30 seconds.
- Drying: Gently air dry the tooth.
- Dispensing: Dispense equal amounts of Paste A & B.
- Mixing: Mix Paste A & B for 20 seconds.
Panavia F 2.0 Final Steps for Metal/PFM29
- Application: Apply the mixed paste to the restoration.
- Cleanup: Remove excess cement (optional 2-3 second tack cure for easier removal).
9. Final Polymerization (Choose A or B):
- Option A (Light Cure): 20 seconds per surface (Conventional/LED) or 5 seconds (Plasma/Fast halogen).
- Option B (Self Cure): Apply OXYGUARD II to margins and wait 3 minutes.
Clinical Guidelines and Summary
- Always follow manufacturer-specific technique cards.
- Use 10-MDP containing cements for zirconia and metal for better chemical bonding.
- Always take a bitewing radiograph after cementation to check for subgingival cement remnants.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Metal and PFM Crowns (Panavia F 2.0 Protocol)
- Tooth Prep: Apply ED Primer II (Note: this initiates the cement set; do not put cement on the tooth first).
- Restoration Prep: Apply Alloy Primer to the sandblasted metal surface.
- Application: Mix Panavia paste, apply inside the crown, and seat.
- Cleanup: Tack cure (1 second) and remove excess.
- Final Steps: Light cure margins. Oxyguard can be used for self-cure areas.
Clinical Cementation Protocol (Variolink Esthetic Example)
- Try-in: Use try-in gel to check shade/fit.
- Clean Restoration: Wash off try-in gel, apply Ivoclean (rub, rinse, dry), then apply Silane (Monobond Plus) for 20 seconds and air dry.
- Prepare Tooth: Etch (total or selective) and apply adhesive (e.g., Adhese Universal). Light cure.
- Seat: Apply dual-cure resin cement to the crown, seat it, and have the patient bite on a cotton roll.
- Cleanup: Tack cure for 1 second per surface. Scrape excess and floss through interproximal contacts (pulling floss out the side).
- Final Cure: Apply liquid strip (glycerin) to margins to prevent the oxygen inhibition layer. Light cure each surface for 10+ seconds.
Glassy Ceramic Crowns (e.g., Lithium Disilicate)
Hydrofluoric Acid Etching
- Mechanism: Reacts with glassy phases to create microporosities and improve wettability.
- Laboratory and Surface Preparation: Usually performed by the lab (e.g., 9% HF gel). Over-etching can change surface texture significantly.
Silane Coupling Agent
- Function: Forms a chemical bridge between the inorganic ceramic (silica) and organic resin cement.
- Application: Rub vigorously for 20 seconds and air dry. It requires hydrolysis to form covalent bonds with the ceramic.
Resin Modified Glass Ionomer (RMGI)
- Composition and Improvements: Adds resin and photo-activators to GIC.
- Clinical Handling: Improved strength and lower solubility than GIC. Can be tack-cured for easier cleanup.
- Indications and Contraindications: Some older literature suggests a risk of fracture in all-ceramic crowns due to water absorption/expansion, but modern versions are often indicated for zirconia and lithium disilicate.
Zinc Oxide Eugenol (ZOE)
- Composition: Zinc oxide, eugenol, rosin, and zinc acetate.
- Clinical Considerations: Used primarily as a temporary cement due to low strength and high solubility. It has a sedative effect on the pulp. Warning: Eugenol can inhibit resin polymerization; eugenol-free versions should be used if resin cement is planned for the permanent restoration.
Glass Ionomer Cement (GIC)
- Composition and Bonding: Polycarboxylate, glass fillers, and water. Bonds ionically to the tooth.
- Clinical Advantages: Aesthetic (translucent) and releases fluoride.
- Considerations: Sensitive to water during early setting; requires a protective coat.

Footnotes
-
Original PDF page 1: DMD2 L3 Biomaterials (Cements), p.1 ↩
-
Original PDF page 2: DMD2 L3 Biomaterials (Cements), p.2 ↩
-
Original PDF page 3: DMD2 L3 Biomaterials (Cements), p.3 ↩
-
Original PDF page 4: DMD2 L3 Biomaterials (Cements), p.4 ↩
-
Original PDF page 5: DMD2 L3 Biomaterials (Cements), p.5 ↩
-
Original PDF page 7: DMD2 L3 Biomaterials (Cements), p.7 ↩
-
Original PDF page 8: DMD2 L3 Biomaterials (Cements), p.8 ↩
-
Original PDF page 9: DMD2 L3 Biomaterials (Cements), p.9 ↩
-
Original PDF page 10: DMD2 L3 Biomaterials (Cements), p.10 ↩
-
Original PDF page 11: DMD2 L3 Biomaterials (Cements), p.11 ↩
-
Original PDF page 12: DMD2 L3 Biomaterials (Cements), p.12 ↩
-
Original PDF page 13: DMD2 L3 Biomaterials (Cements), p.13 ↩
-
Original PDF page 14: DMD2 L3 Biomaterials (Cements), p.14 ↩
-
Original PDF page 15: DMD2 L3 Biomaterials (Cements), p.15 ↩
-
Original PDF page 16: DMD2 L3 Biomaterials (Cements), p.16 ↩
-
Original PDF page 17: DMD2 L3 Biomaterials (Cements), p.17 ↩
-
Original PDF page 18: DMD2 L3 Biomaterials (Cements), p.18 ↩
-
Original PDF page 19: DMD2 L3 Biomaterials (Cements), p.19 ↩
-
Original PDF page 20: DMD2 L3 Biomaterials (Cements), p.20 ↩
-
Original PDF page 21: DMD2 L3 Biomaterials (Cements), p.21 ↩
-
Original PDF page 22: DMD2 L3 Biomaterials (Cements), p.22 ↩
-
Original PDF page 23: DMD2 L3 Biomaterials (Cements), p.23 ↩
-
Original PDF page 25: DMD2 L3 Biomaterials (Cements), p.25 ↩
-
Original PDF page 26: DMD2 L3 Biomaterials (Cements), p.26 ↩
-
Original PDF page 27: DMD2 L3 Biomaterials (Cements), p.27 ↩
-
Original PDF page 30: DMD2 L3 Biomaterials (Cements), p.30 ↩
-
Original PDF page 35: DMD2 L3 Biomaterials (Cements), p.35 ↩
-
Original PDF page 38: DMD2 L3 Biomaterials (Cements), p.38 ↩
-
Original PDF page 39: DMD2 L3 Biomaterials (Cements), p.39 ↩