The University of Western Australia1
Clinical Assessment Overview
This documentation outlines the fundamental procedures for clinical evaluation within the dental and oral health context, presented by Dr. Agnieszka Frydrych.
Core Components of Evaluation
- History Taking: Systematic collection of patient information and medical background.
- Patient Examination: Comprehensive physical assessment and clinical observation.
- Lesion Evaluation: Detailed analysis and diagnostic approach to oral abnormalities.
History Taking, Patient Examination and Lesion Evaluation
“Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice”, 2019, p. 139
The primary objective of this topic is to ensure clinicians can perform a thorough assessment to reach an accurate diagnosis for oral lesions.
The Importance of Diagnosis
Correct diagnosis enables clinicians to offer the most effective and safe treatment and provide an accurate prognosis. History taking is particularly crucial because a carefully obtained history will independently reveal the diagnosis in many instances.
Why This Topic2
History Taking
When evaluating the presenting complaint, the following details should be recorded: “Contemporary Oral Medicine: A Comprehensive Approach to Clinical Practice”, 2019, p. 140
Presenting Complaint3
- Date of onset and duration
- Non-healing ulcers of two months' duration warrant significantly greater concern than white patches of the same duration.
- Specific location(s)
- High-risk anatomical sites include the lateral borders of the tongue and the floor of the mouth, which are associated with a higher risk of oral cancer.
- Aggravating and relieving factors
- History of past investigations
- Prevents unnecessary repetition of costly tests and provides clues, such as nutritional deficiencies linked to oral ulceration.
- History of past treatments
- Response to treatment—whether favorable or not—provides valuable insight into pathogenesis.
A thorough medical history is critical as it directly influences:
Medical History456
- Diagnosis: Identifying systemic links to oral manifestations.
- Treatment: Determining safe clinical interventions.
- Prognosis: Understanding how systemic health affects healing and outcomes.
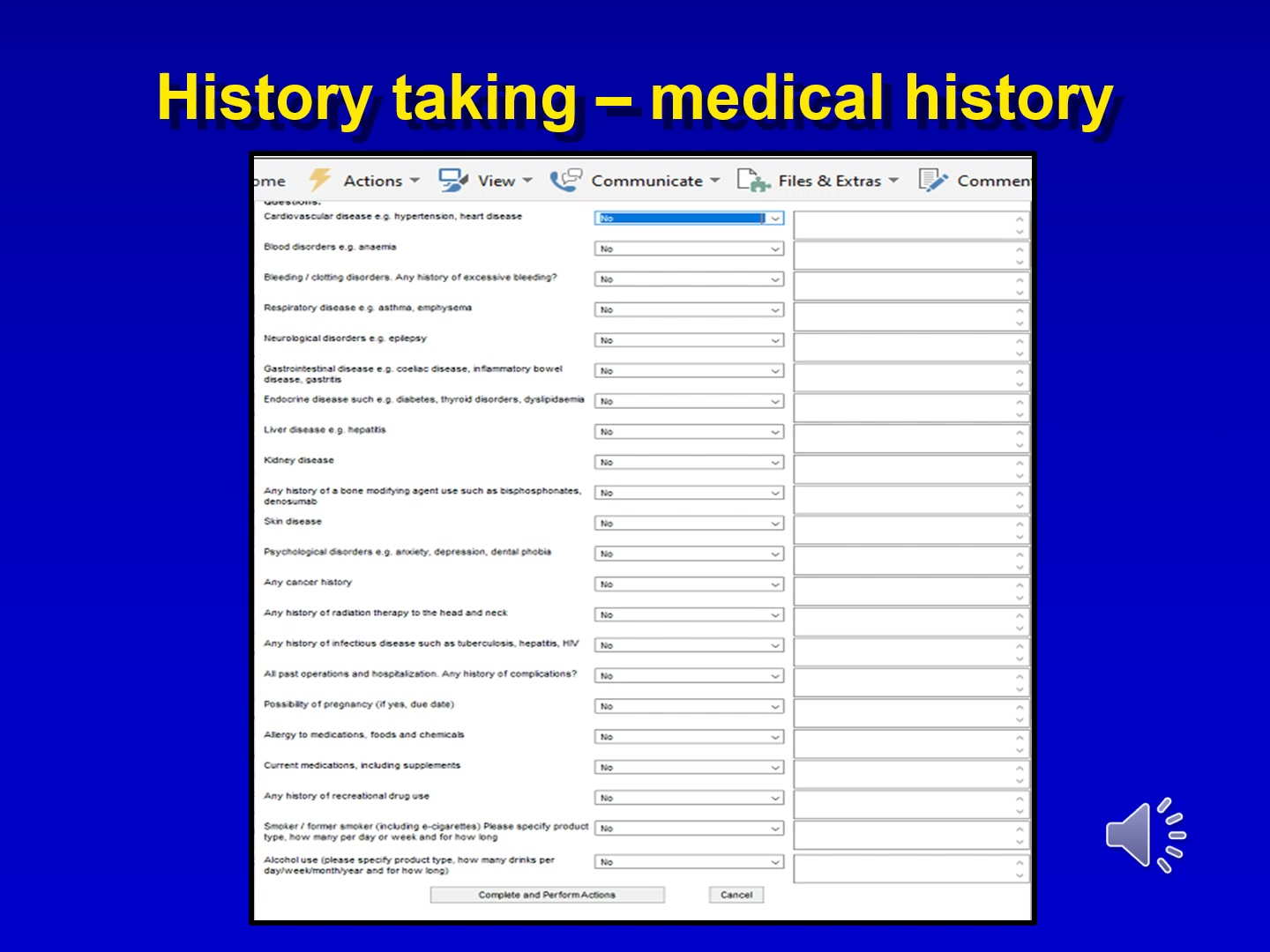
Recording Medical History
Do not simply record yes or no answers; elaborate on all positive responses. For example, for diabetes, record the type, duration, monitoring frequency, and typical glucose readings.
Systemic Review and Health Status
- Cardiovascular disease: e.g., hypertension, heart disease
- Identify patients predisposed to bacterial endocarditis or those on anticoagulants; calcium channel blockers may cause gingival hyperplasia.
- Blood disorders: e.g., anaemia, bleeding or clotting disorders (including history of excessive bleeding)
- Respiratory disease: e.g., asthma, emphysema
- Inhalers containing topical corticosteroids increase the risk of oral candidosis.
- Neurological disorders: e.g., epilepsy
- Use of phenytoin is associated with gingival hyperplasia.
- Gastrointestinal disease: e.g., coeliac disease, inflammatory bowel disease, gastritis
- Endocrine disease: e.g., diabetes, thyroid disorders, dyslipidaemia
- Liver and Kidney disease: e.g., hepatitis
- Bone modifying agents: History of bisphosphonates or denosumab use
- These place patients at risk for medication-related osteonecrosis of the jaw (MRONJ).
- Skin and Psychological disorders: e.g., anxiety, depression, dental phobia
- Oncology and Infectious disease:
- History of cancer
- History of radiation therapy to the head and neck
- Infectious diseases such as tuberculosis, hepatitis, or HIV
- Surgical and Hospital History: All past operations, hospitalizations, and complications
- Pregnancy: Current status and due date if applicable
- Allergies: Medications, foods, and chemicals
- Medications: Current prescriptions and supplements
- Substance Use:
- Recreational drug use
- Smoking/E-cigarettes: Specify product type, frequency, and duration
- Alcohol: Specify product type, frequency, and duration
Key Medical Considerations
Particular attention should be paid to the following systems during history taking:
- Cardiovascular disease
- Respiratory disease
- Central Nervous System (CNS) disease
- Skin disease
- Gastrointestinal (GIT) disease
- Liver disease
- Endocrine disorders
Key points to note regarding dental history:
Dental History7
- Regularity of dental attendance
- Compliance affects management; a compliant patient might be monitored for leukoplakia, whereas a non-compliant one may require excision.
- Recent dental problems or interventions
- A sudden increase in caries rate may signal changes in salivary function.
Relevant social factors include:
Social History8
- Marital status
- Indicates available support systems, which are crucial for outcomes in chronic disease or cancer treatment.
- Attitudes toward medical treatment
- Socioeconomic status
- History of overseas travel
- Sexual history
- Occupation
- Relevant for conditions like UV exposure and lip cancer.
- Life stressors
- Many orofacial pain complaints are stress-related or stress-modulated.
- Behavioral habits
Examination
Visual Assessment
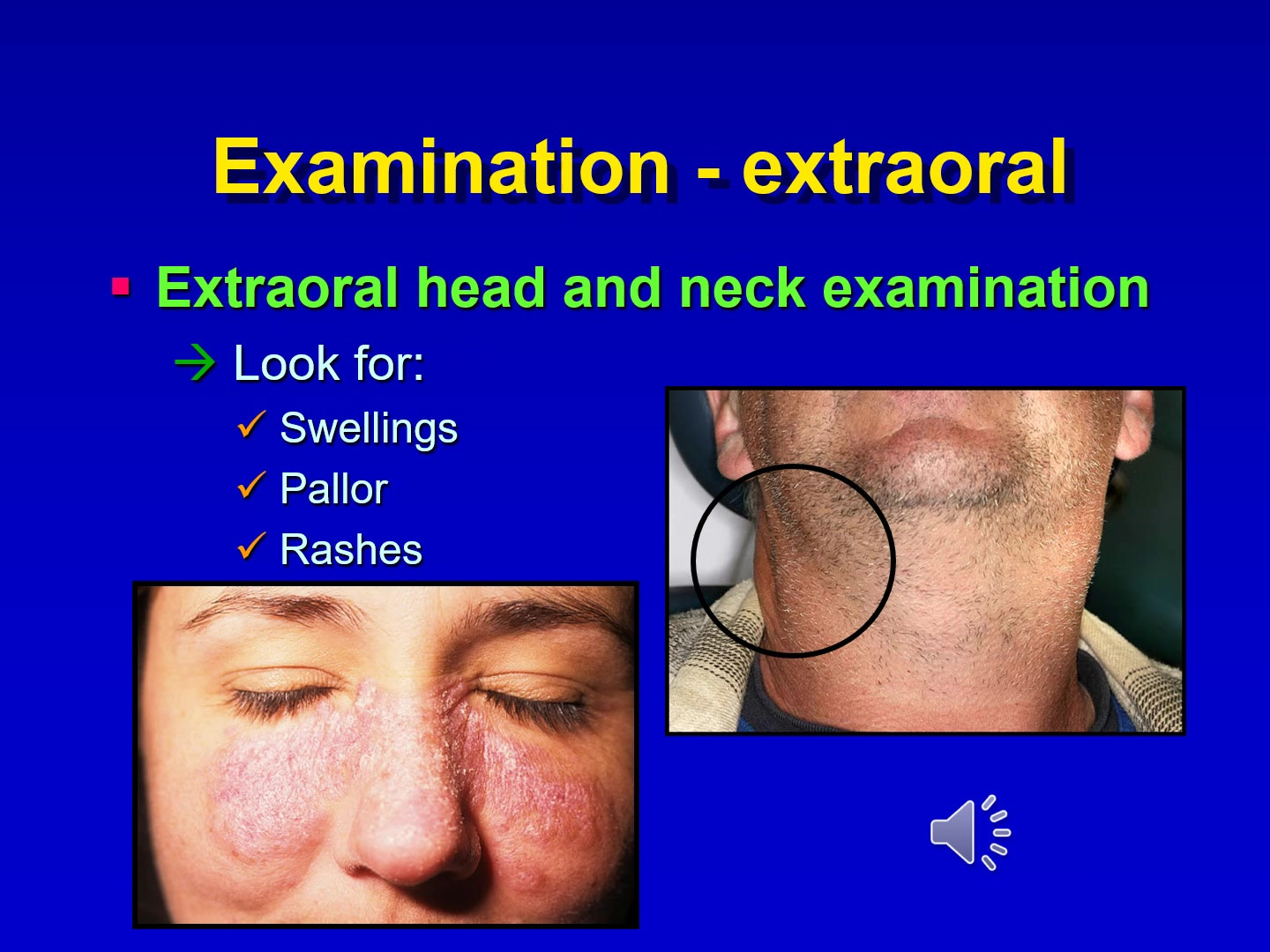
During the extraoral head and neck examination, observe the patient for:
- Vital Signs: Fever may indicate infection; high pulse may indicate anxiety or cardiac disorders.
- Weight Loss: May be associated with eating disorders, cancer, or HIV.
- Hands: Note deformities such as those from rheumatoid arthritis.
- Eye Color: Yellow discoloration indicates jaundice or liver disease.
Extraoral Examination9
- Swellings
- Pallor
- Rashes
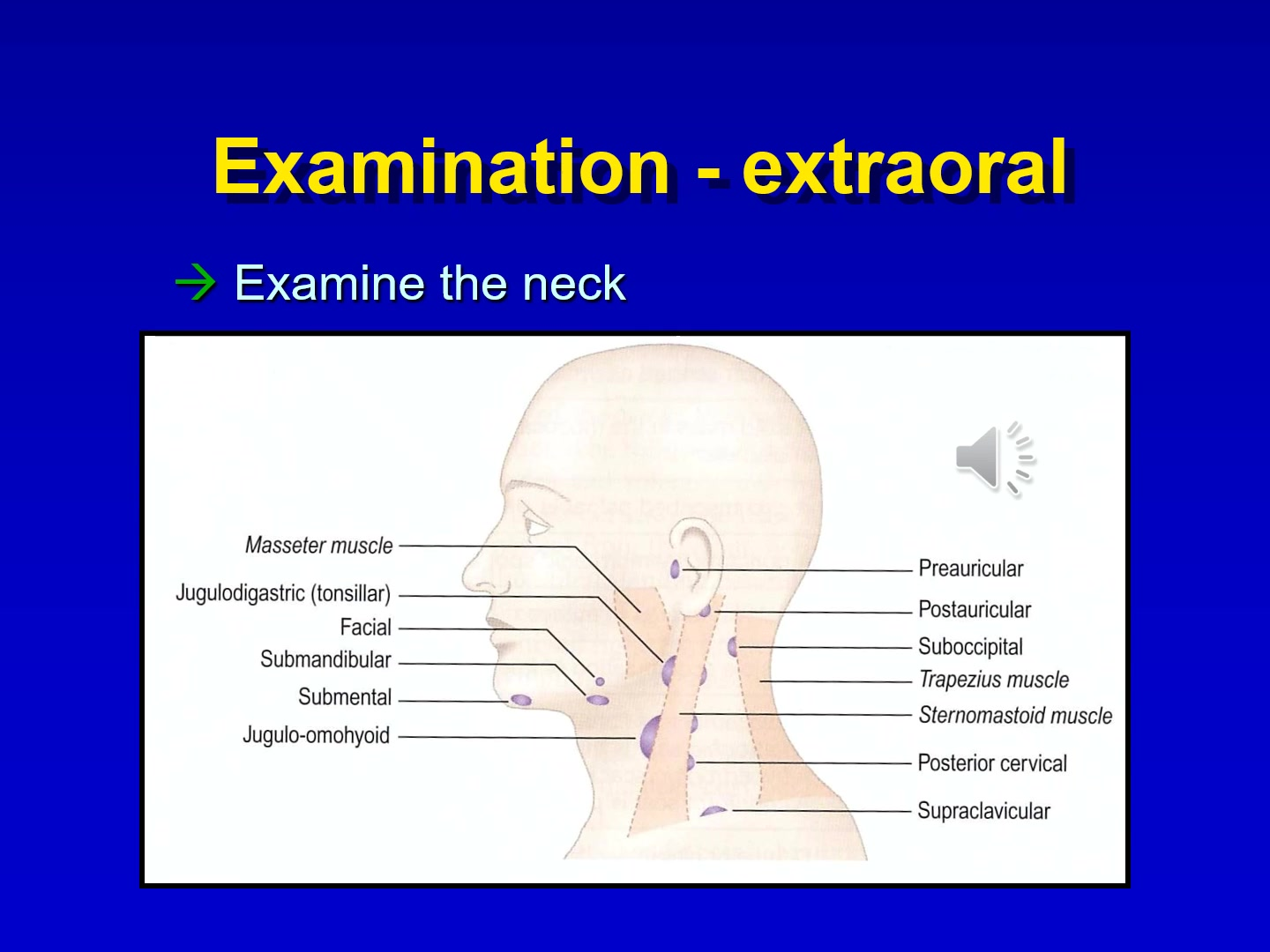
Lymph Node and Muscle Palpation
Systematically examine the following areas and structures:
Neck Examination1011
- Masseter muscle
- Jugulodigastric (tonsillar) nodes
- Facial nodes
- Submandibular nodes
- Submental nodes
- Jugulo-omohyoid nodes
- Preauricular and Postauricular nodes
- Suboccipital nodes
- Trapezius muscle
- Sternomastoid muscle
- Posterior cervical nodes
- Supraclavicular nodes
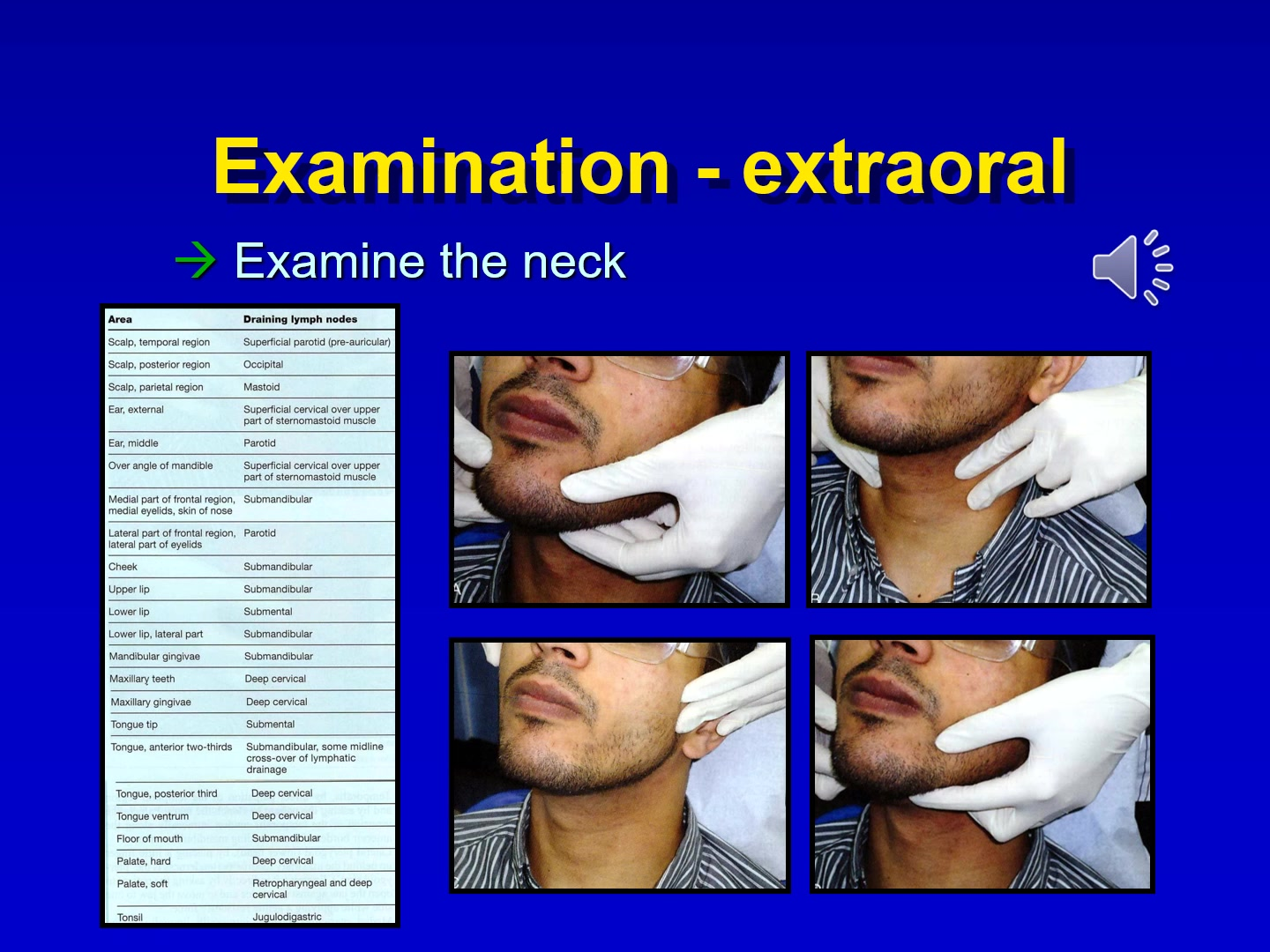
Examination Technique
Observe the patient from the front for asymmetry, then stand behind the patient to palpate lymph nodes. A thorough understanding of lymphatic drainage is required to identify the source of pathology.
Lymphatic Drainage Patterns
| Anatomical Area | Primary Draining Lymph Nodes |
|---|---|
| Scalp (temporal), Lateral eyelids | Superficial parotid (pre-auricular) |
| Scalp (posterior) | Occipital |
| Scalp (parietal) | Mastoid |
| External ear, Mandibular angle | Superficial cervical (upper sternomastoid) |
| Middle ear, Lateral eyelids | Parotid |
| Frontal region (medial), Nose, Cheek, Upper lip | Submandibular |
| Lower lip (midline), Tongue tip | Submental |
| Lower lip (lateral), Mandibular gingivae, Floor of mouth | Submandibular |
| Maxillary teeth and gingivae | Deep cervical |
| Tongue (anterior two-thirds) | Submandibular (with midline cross-over) |
| Tongue (posterior third, ventrum), Hard palate | Deep cervical |
| Soft palate | Retropharyngeal and deep cervical |
| Tonsil | Jugulodigastric |
Clinical Evaluation of Function
Assess the Temporomandibular Joints (TMJs) and muscles of mastication for:
TMJ and Mastication Muscles12
- Facial asymmetry
- Mandibular opening and closing paths (deviations or deflections)
- Mandibular opening extent (Note: Restricted opening is defined as <40mm)
- Lateral excursions (Normal range approximately 8mm)
- Joint noises (clicking, crepitus)
Salivary Glands
- examine salivary glands for:
- Symmetry
- Evidence of enlargement
- Evidence of salivary flow
- Evidence of salivary pooling in the floor of the mouth
- Salivary appearance
- Evidence of oral dryness
Cranial Nerve Assessment Table
Cranial Nerve Exam13
- only undertaken when neurlogical abnormality is obvious
| Nerve | Major functions | Assessment Method |
|---|---|---|
| I Olfactory | Smell | Identify familiar scents (often deferred). |
| II Optic | Vision; pupil reactivity (afferent) | Read text; test visual fields in four quadrants. |
| III Oculomotor | Eyelid/Eye movement; pupil size (efferent) | Check pupillary light response, accommodation, and EOMs. |
| IV Trochlear | EOM (down and lateral) | Have patient look down and in. |
| V Trigeminal | Mastication; facial sensation | Test jaw strength/lateral movement; test facial touch sensation. |
| VI Abducens | EOM (lateral) | Have patient move eyes side to side. |
| VII Facial | Expression; taste; eyelid/lip closure | Smile, raise eyebrows, close eyes against resistance. |
| VIII Acoustic | Hearing; equilibrium | Tuning fork, finger rub, or whisper test. |
| IX Glossopharyngeal | Gagging; swallowing; taste | Test gag reflex and swallowing. |
| X Vagus | Gagging; swallowing; speech | Assess vocal quality and swallowing. |
| XI Spinal accessory | Shoulder/Head movement | Shrug shoulders; turn head against resistance. |
| XII Hypoglossal | Tongue movement; articulation | Stick out tongue; move cheek to cheek; assess speech. |
Intraoral Examination141516171819202122
Requirements for Examination
To perform a thorough intraoral examination, ensure the following are available:
- Proper lighting
- Dental mouth mirror
- Gauze squares (for tongue retraction and drying tissues)
- Personal Protective Equipment (PPE)
- Visual aids
Asymptomatic Dysplastic Lesion Masked by Prosthesis
A patient presented with an asymptomatic dysplastic lesion at high risk of malignant transformation. The lesion was completely invisible while her denture was in place. Lipstick can similarly mask early lip cancers.
Preparation for Exam
All removable prostheses must be removed and lipstick must be wiped off prior to examination. Examining with prostheses in place is considered negligent.
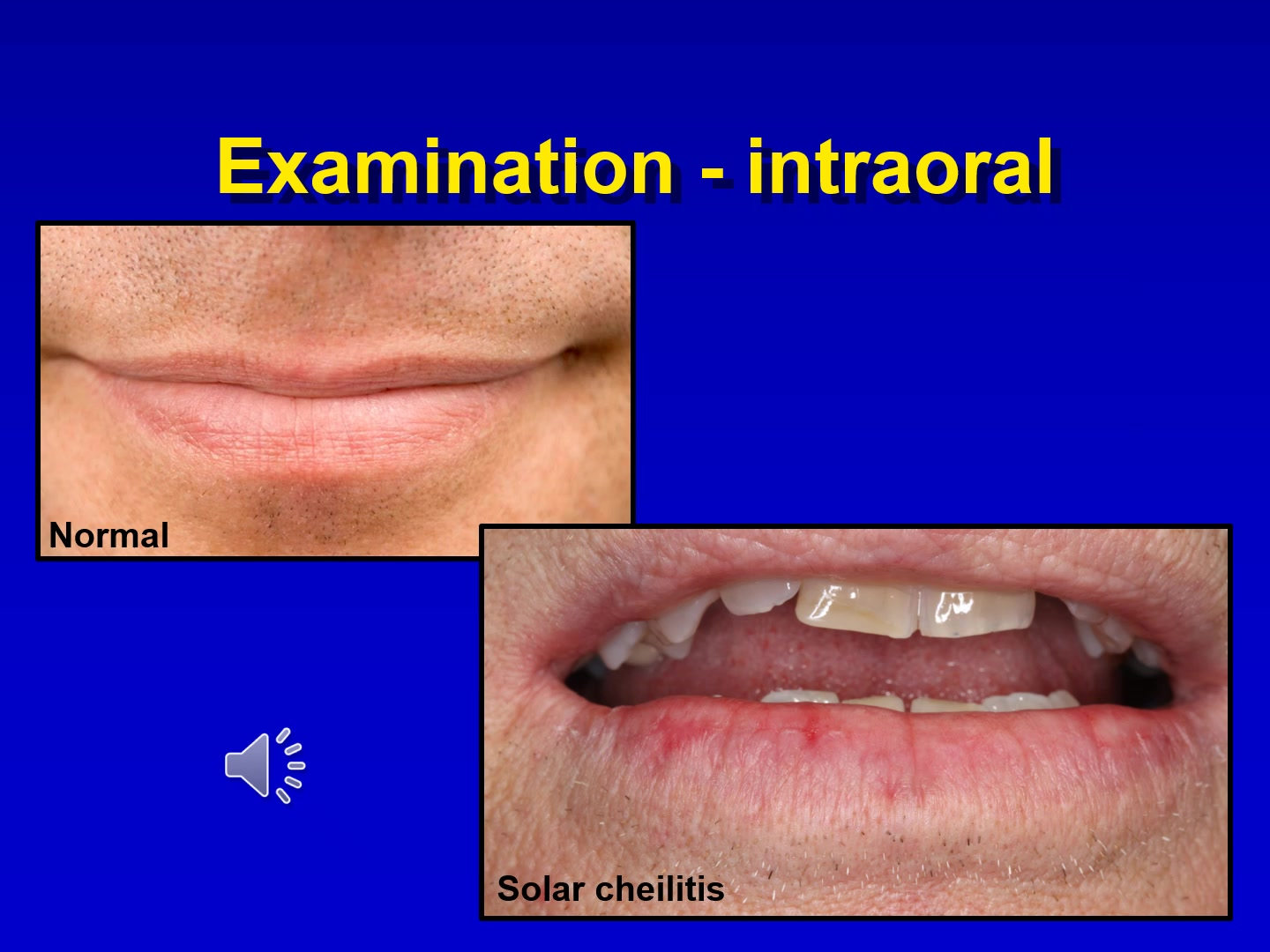
Lip Examination
Comparison of clinical appearances:
- Normal: Healthy vermilion border and mucosal integrity.
- Solar cheilitis: Evidence of sun damage, loss of vermilion border definition, or crusting.
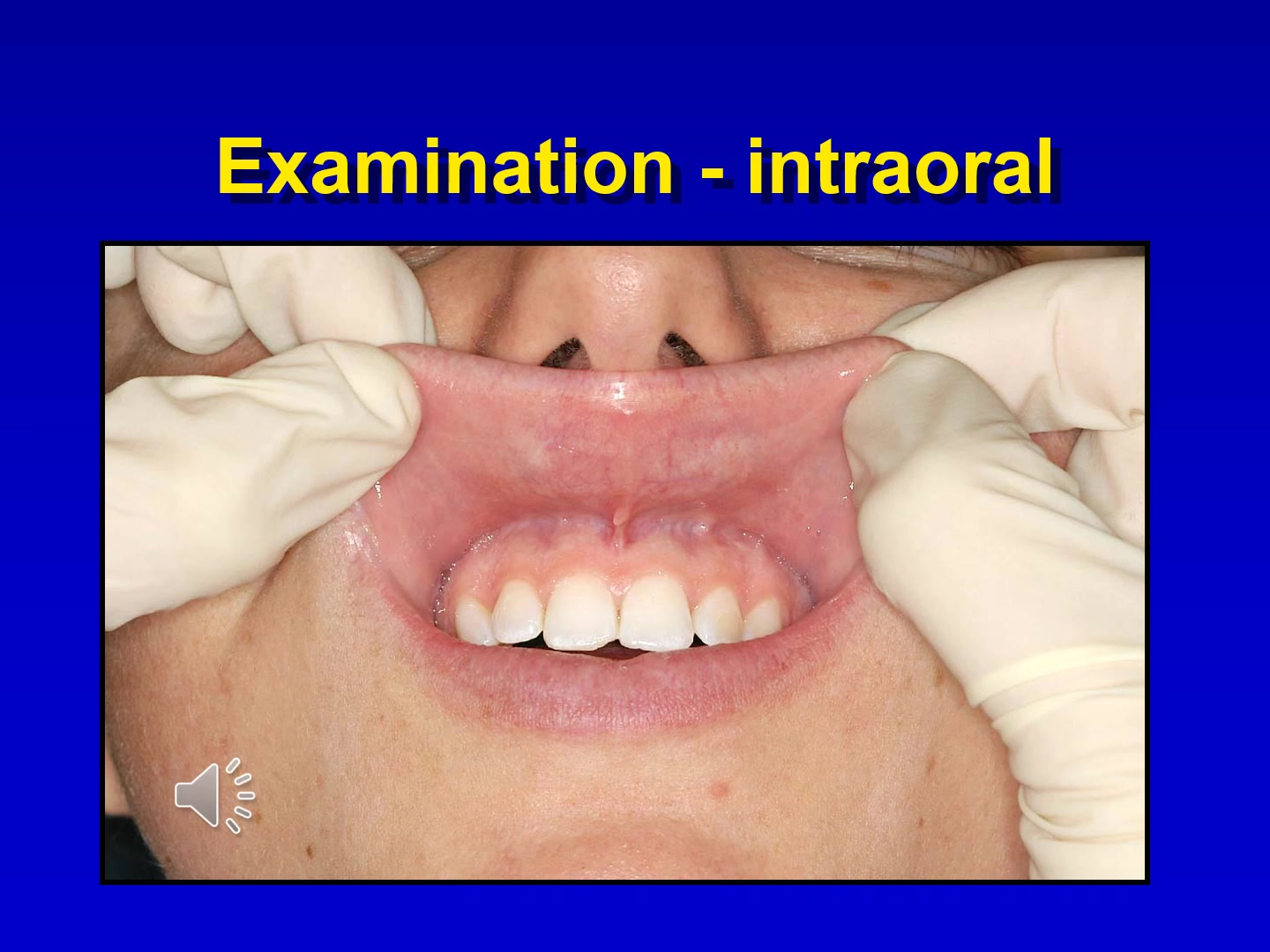
Systematic Intraoral Protocol
- Labial Mucosa: Examine maxillary and mandibular areas, including sulcus and frena.
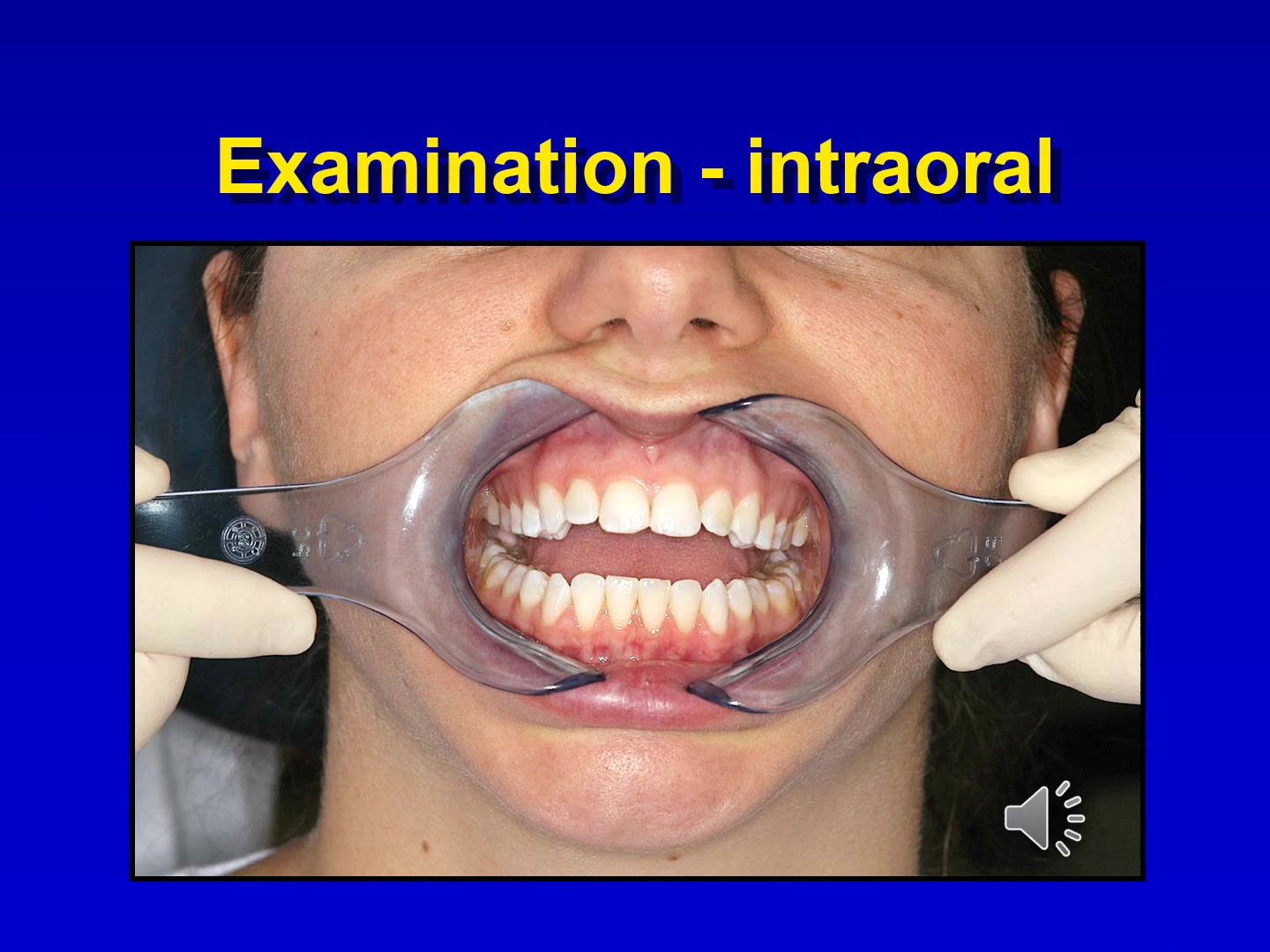
- Buccal Mucosa: Retract with two mirrors; examine from labial commissure to anterior tonsillar pillar.
- Gingiva and Alveolar Mucosa: Check all aspects for color, texture, and ulceration.
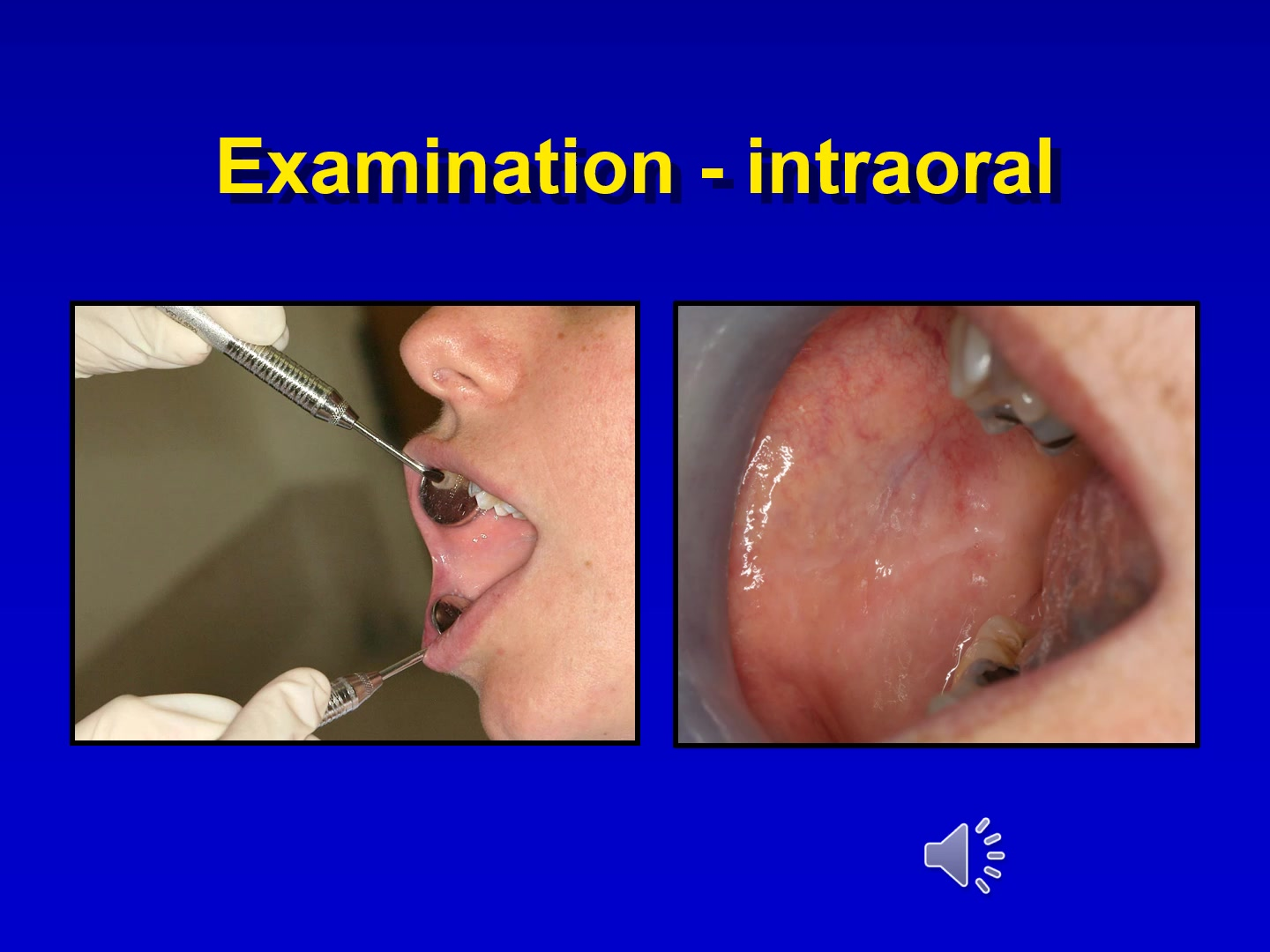
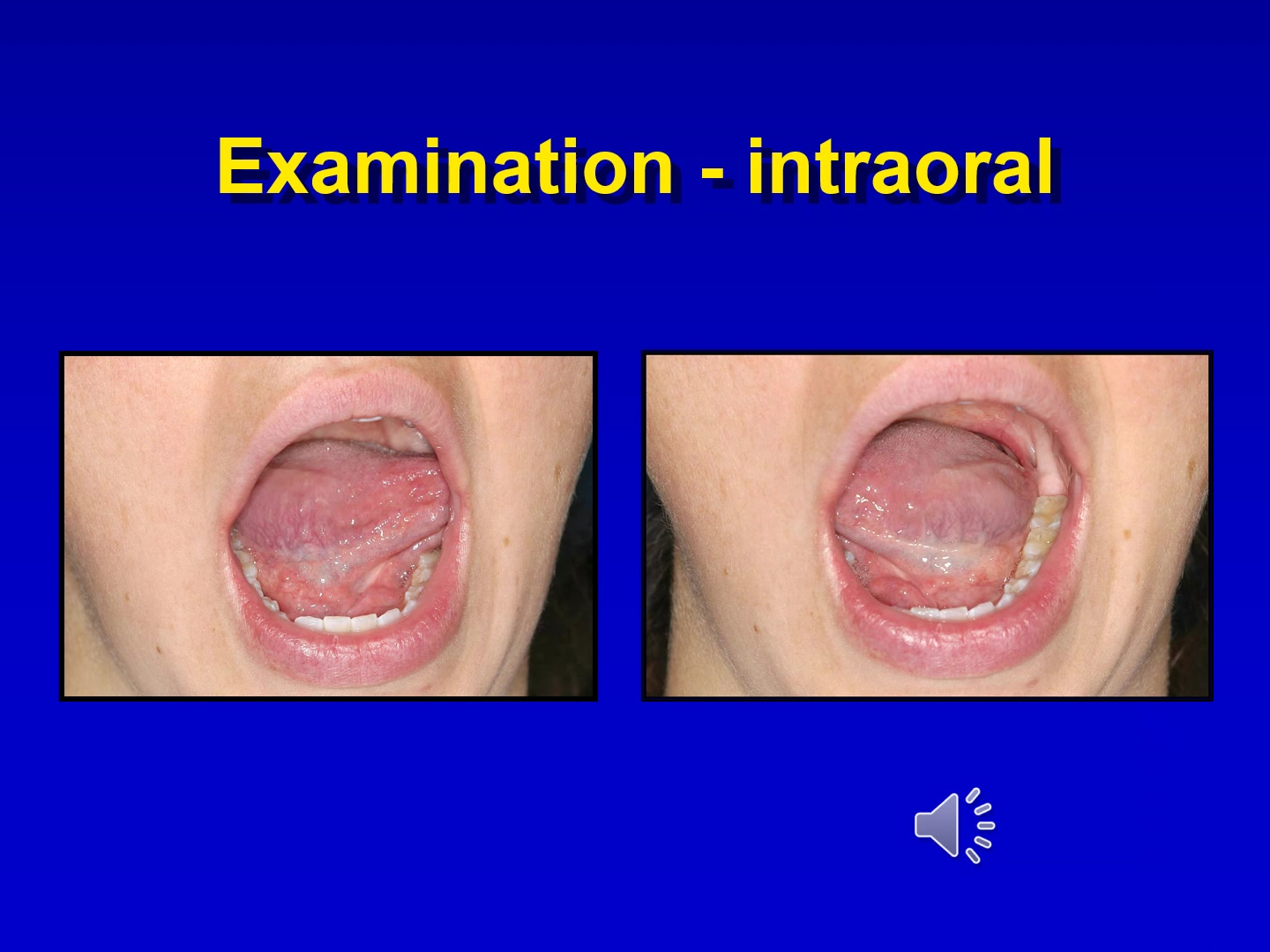
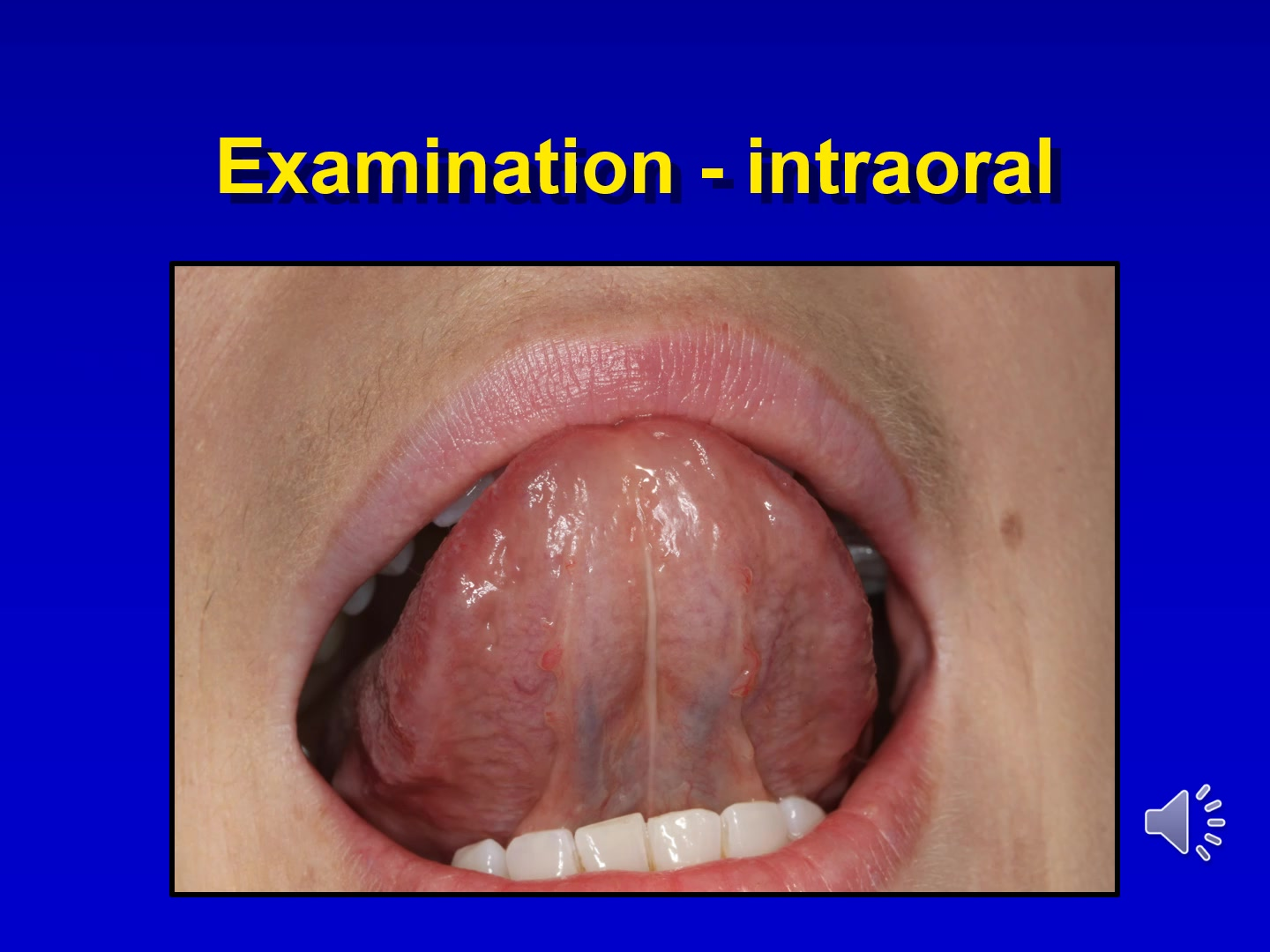
- Tongue and Floor of Mouth:
- Inspect dorsal surface at rest.
- Note protrusion deviation.
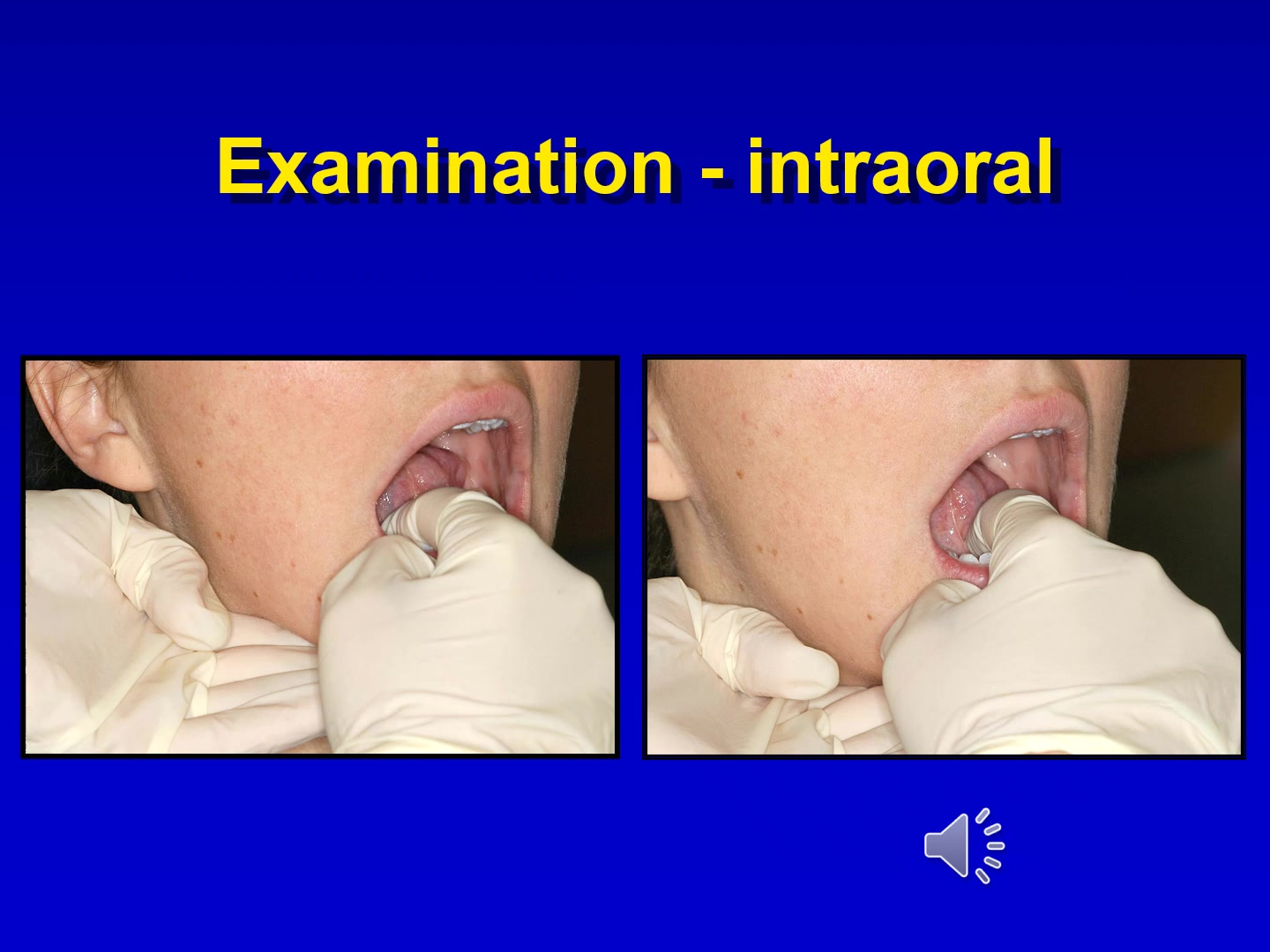
- Grasp with gauze to examine entire lateral surface from tip to base.
- Bimanual palpation of the floor of the mouth is essential as many swellings are not visible.
- Palpation of tongue is also important
- Look for any deviation in patient otngue protrusion
- Blurring of the cutaneous-vermilion border is associated with an increased risk of lip squamous cell carcinoma.
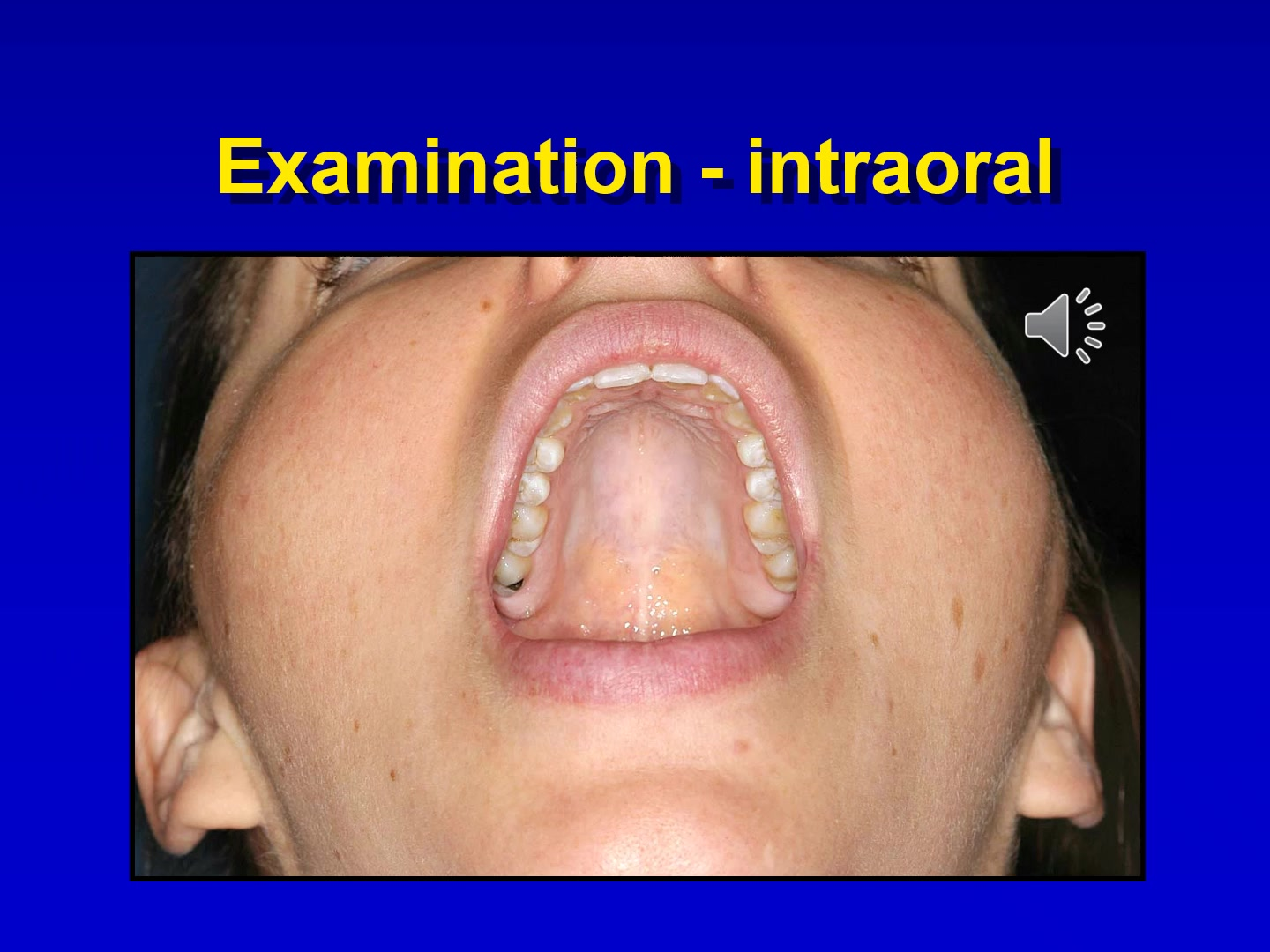
- Soft palate mucosa
- Oropharynx
Lesion Evaluation2324252627
Evaluation of oral lesions requires a systematic approach to ensure all clinical features and patient factors are considered.
Clinical Workflow
Problem History28
- Problem history
- Medical and social history
- Clinical examination
- Differential diagnosis
- Diagnostic tests
- Definitive diagnosis
- Management
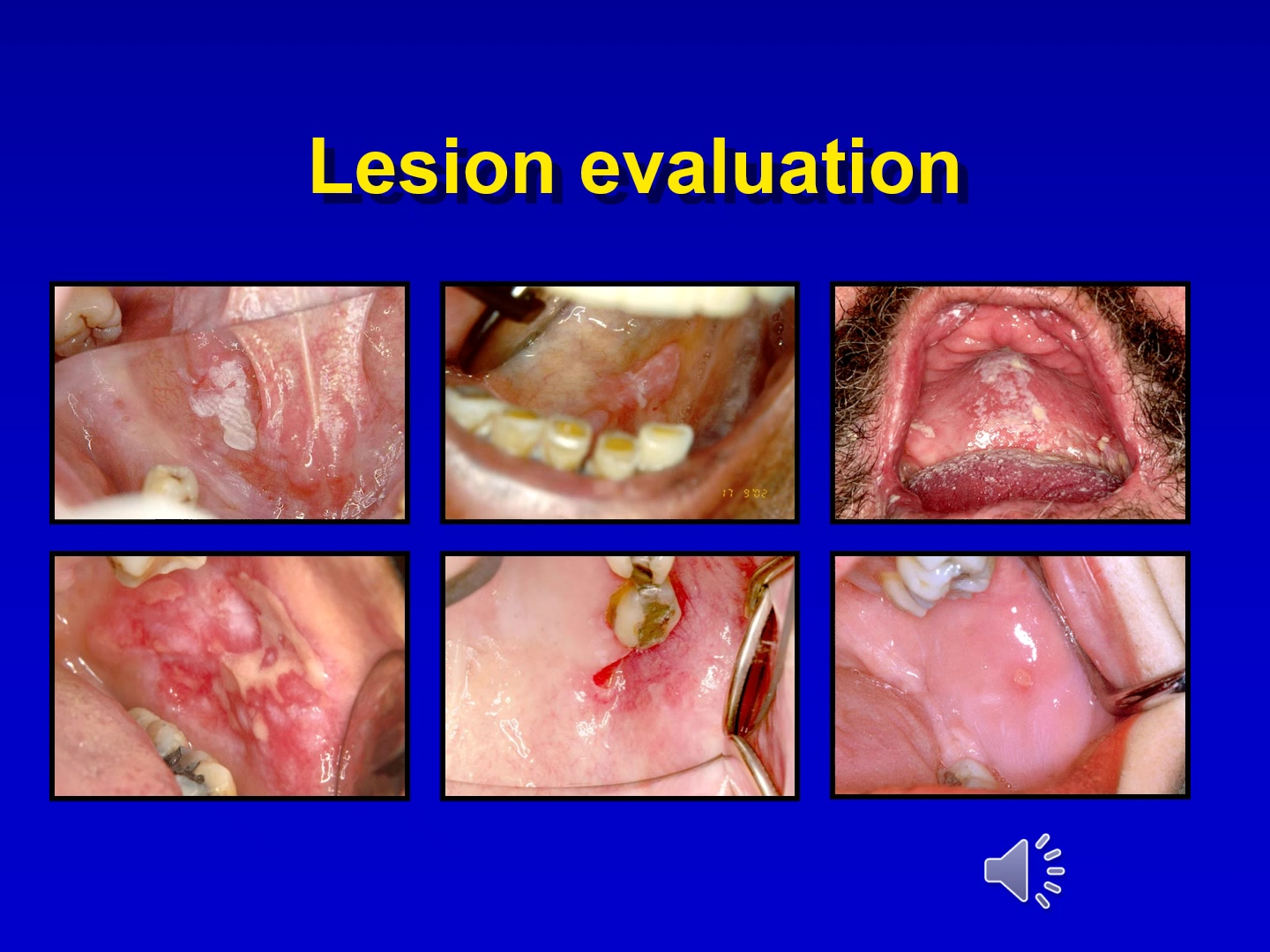
Case Study: The Six Patient Challenge
In a test of six patients, five had benign lesions and one had cancer. Only one clinician correctly identified the malignancy, illustrating that visual examination alone gives limited information and can lead to wrong perceptions.
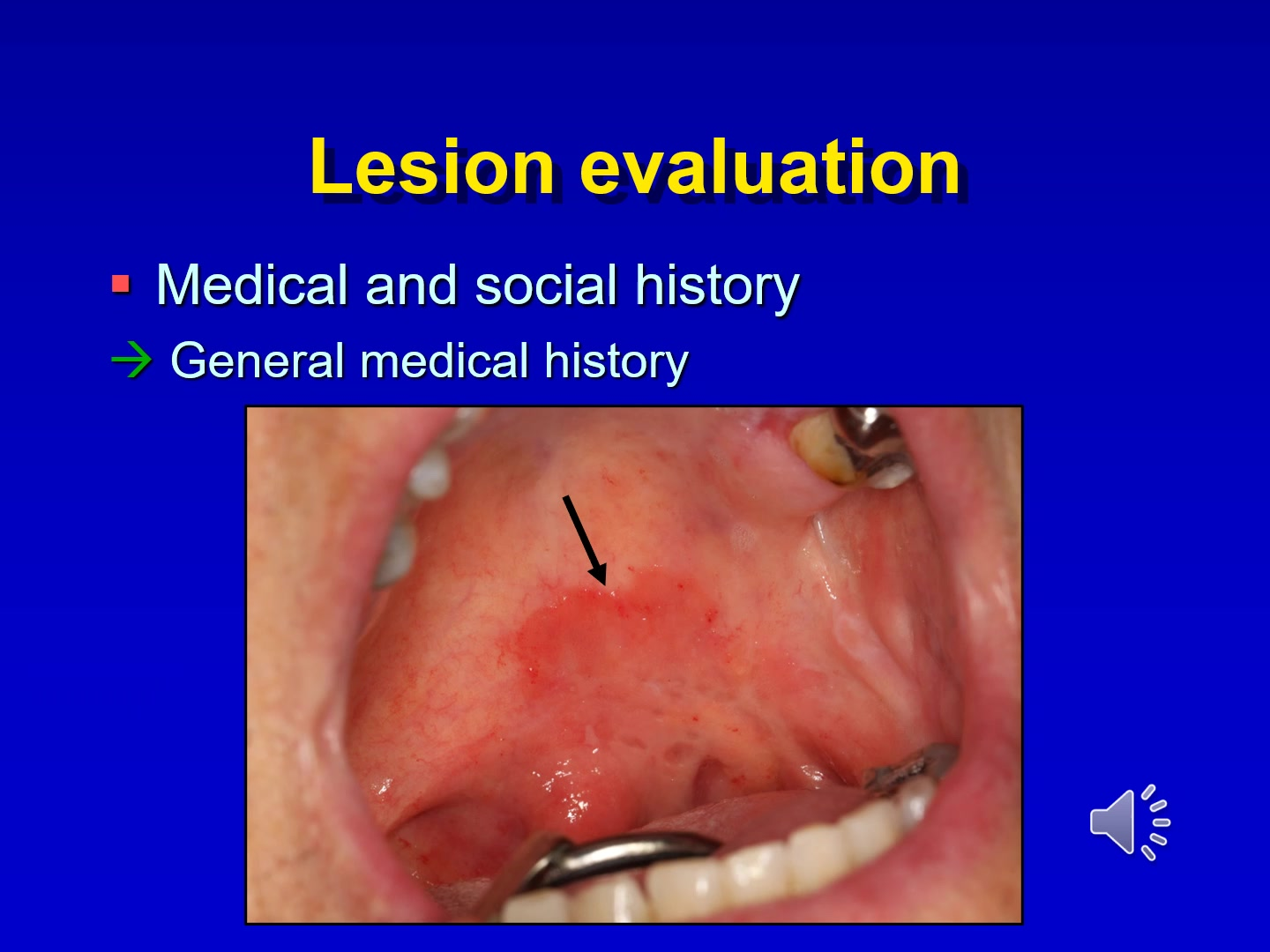
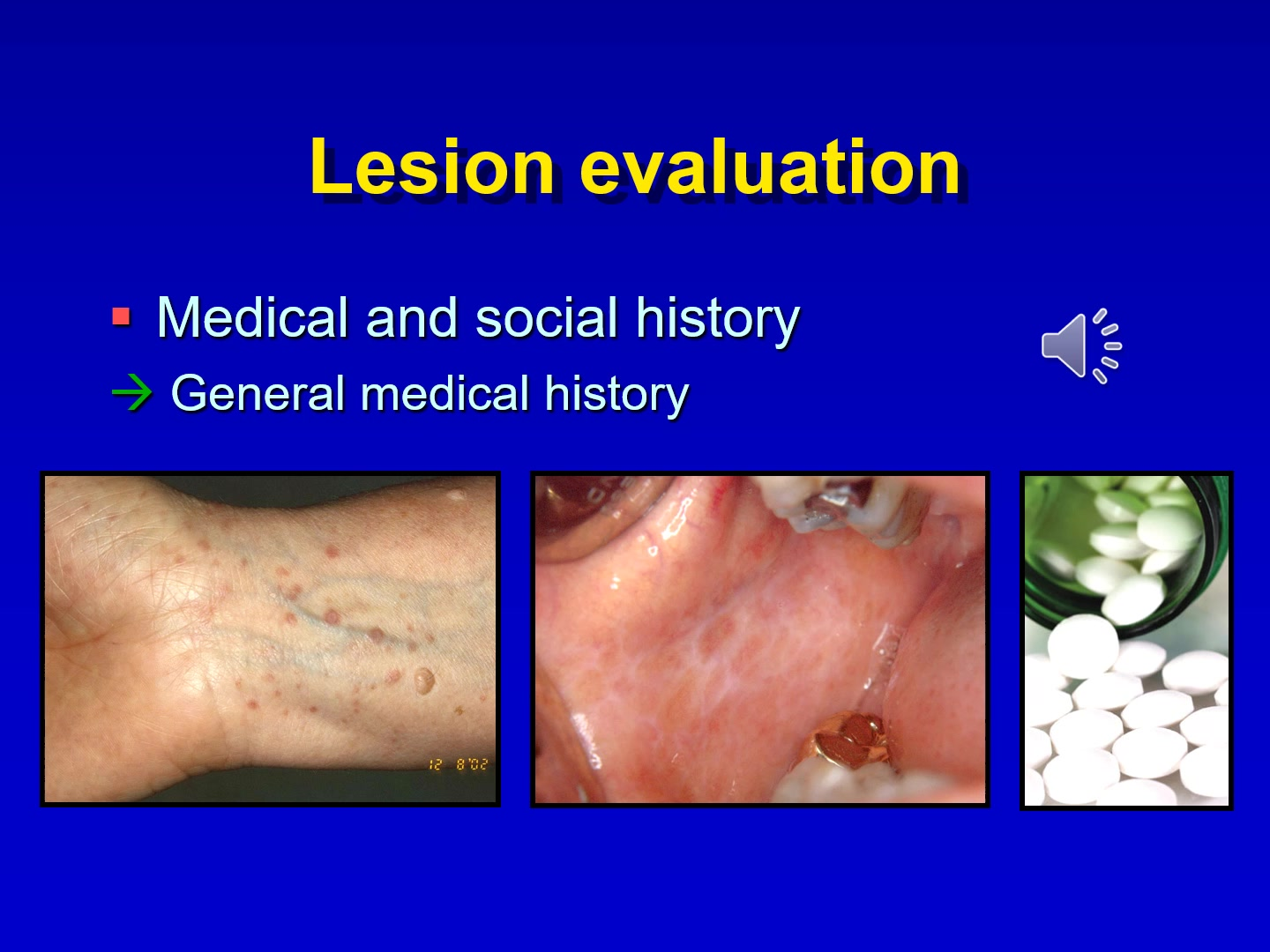
The general medical history is a foundational component of lesion evaluation, providing context for potential systemic causes or contraindications for treatment.
Problem History
- asymptomatic
- symptomatic
- onset
- Location
- Intensity Frequency
- duration
Medical and Social History2930
The general medical history must be reviewed to identify any underlying conditions that may manifest as oral lesions.
- previous cancer history
- Tobacco and alcohol use
- frequency
- Duration
Second Primary Cancer Detection
A tonsillar cancer survivor presented with a red lesion during a routine exam. It was diagnosed as carcinoma in situ. Early detection was critical as treatment options for a second primary cancer at that site are limited.
Lesion evaluation
- Location
- size
- colour
- outline
- Texture
Focus: Differential Diagnosis
After gathering history and performing a clinical examination, the clinician must develop a differential diagnosis before proceeding to diagnostic tests.
Consider the following categories when developing a differential diagnosis:
Differential Diagnosis31
- Inherited
- Inflammatory
- Infection
- Iatrogenic
- Idiopathic
- Neoplastic
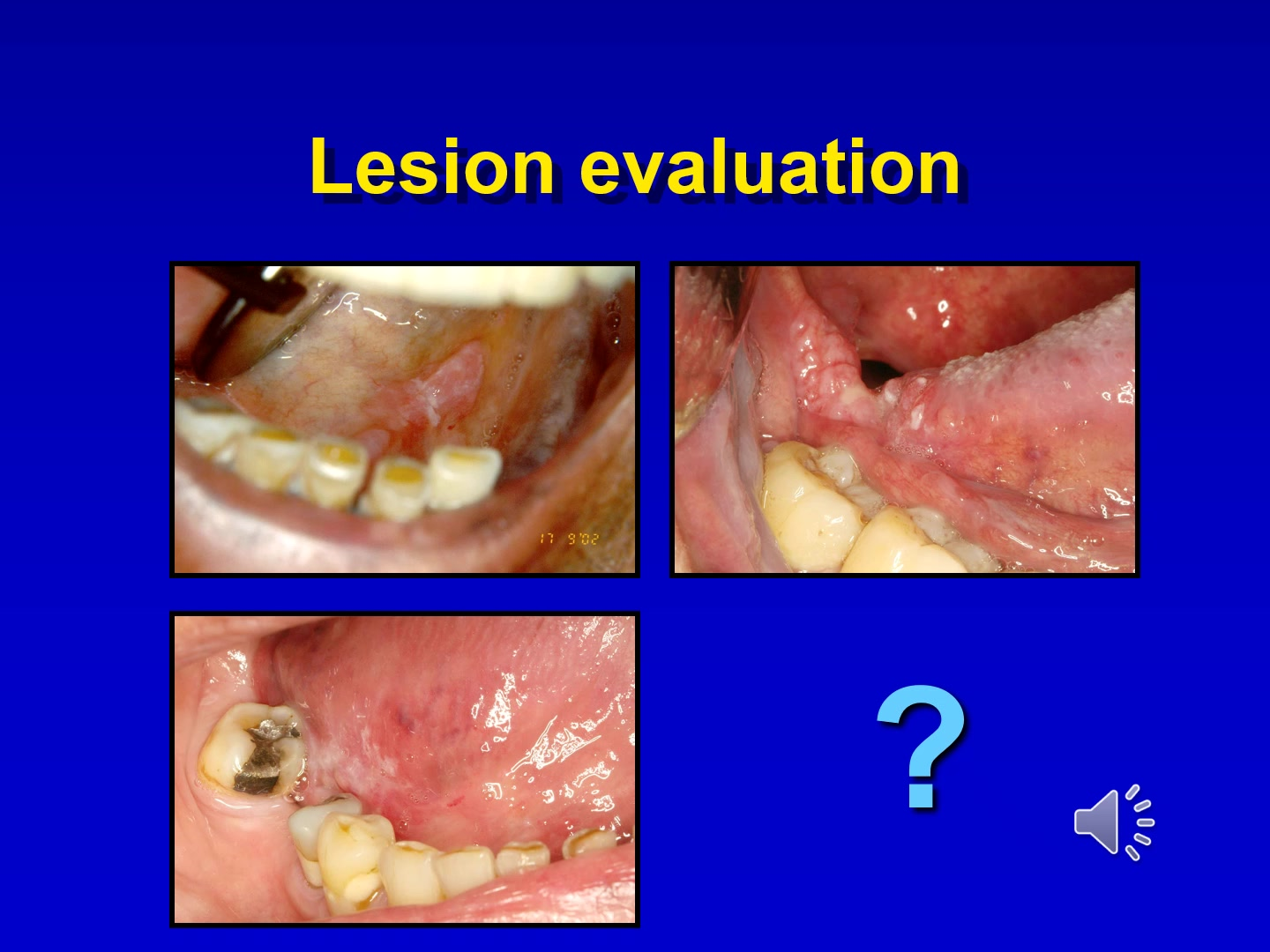
Three Patients, Three Lesions
- Patient 1: Red/white lesion on lateral tongue; soft with some induration. Diagnosis: Severely dysplastic leukoplakia.
- Patient 2: Painful, ulcerated, indurated lesion. Diagnosis: Advanced Squamous Cell Carcinoma (SCC).
- Patient 3: Asymptomatic floor of mouth lesion; soft and non-ulcerated. Diagnosis: SCC. Conclusion: All three patients required urgent concern due to high-risk sites and lesion characteristics.
Summary of Evaluation Steps
- Problem history
- Medical and social history
- Clinical examination
- Differential diagnosis
- Diagnostic tests
- Definitive diagnosis
- Management
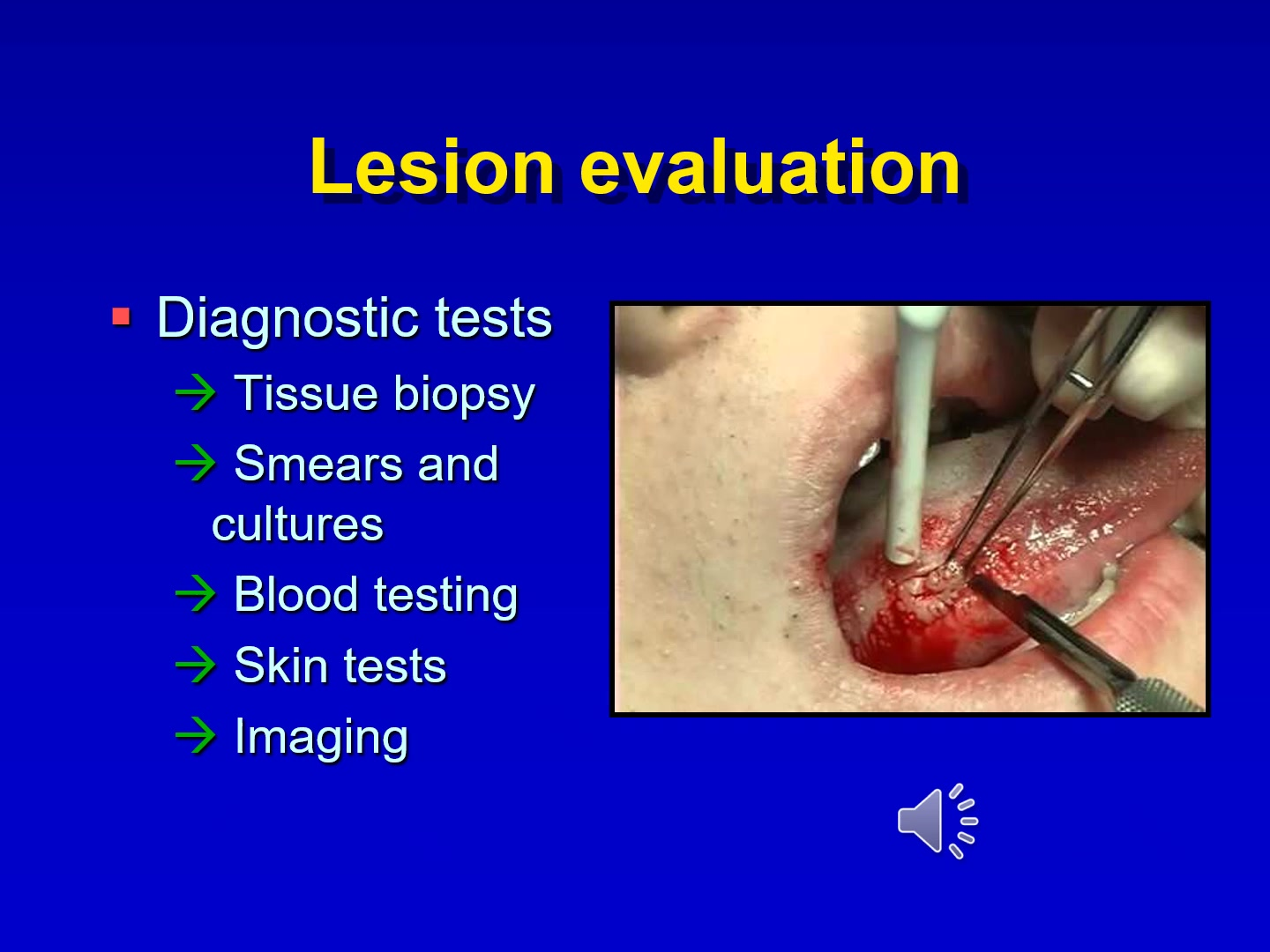
The following tests may be required to reach a definitive diagnosis:
Diagnostic Tests32
- Tissue biopsy
- Smears and cultures
- Blood testing
- Skin tests
- Imaging
Integration and Re-evaluation
After diagnosis and treatment, the patient must be re-evaluated. If they do not respond as expected, the clinician must reconsider the diagnosis and repeat the evaluation process.
Footnotes
-
Original PDF page 1: L1 Oral soft tissue examination and lesion evaluation slides, p.1 ↩
-
Original PDF page 2: L1 Oral soft tissue examination and lesion evaluation slides, p.2 ↩
-
Original PDF page 3: L1 Oral soft tissue examination and lesion evaluation slides, p.3 ↩
-
Original PDF page 4: L1 Oral soft tissue examination and lesion evaluation slides, p.4 ↩
-
Original PDF page 5: L1 Oral soft tissue examination and lesion evaluation slides, p.5 ↩
-
Original PDF page 6: L1 Oral soft tissue examination and lesion evaluation slides, p.6 ↩
-
Original PDF page 7: L1 Oral soft tissue examination and lesion evaluation slides, p.7 ↩
-
Original PDF page 8: L1 Oral soft tissue examination and lesion evaluation slides, p.8 ↩
-
Original PDF page 9: L1 Oral soft tissue examination and lesion evaluation slides, p.9 ↩
-
Original PDF page 10: L1 Oral soft tissue examination and lesion evaluation slides, p.10 ↩
-
Original PDF page 11: L1 Oral soft tissue examination and lesion evaluation slides, p.11 ↩
-
Original PDF page 12: L1 Oral soft tissue examination and lesion evaluation slides, p.12 ↩
-
Original PDF page 13: L1 Oral soft tissue examination and lesion evaluation slides, p.13 ↩
-
Original PDF page 14: L1 Oral soft tissue examination and lesion evaluation slides, p.14 ↩
-
Original PDF page 15: L1 Oral soft tissue examination and lesion evaluation slides, p.15 ↩
-
Original PDF page 16: L1 Oral soft tissue examination and lesion evaluation slides, p.16 ↩
-
Original PDF page 17: L1 Oral soft tissue examination and lesion evaluation slides, p.17 ↩
-
Original PDF page 18: L1 Oral soft tissue examination and lesion evaluation slides, p.18 ↩
-
Original PDF page 19: L1 Oral soft tissue examination and lesion evaluation slides, p.19 ↩
-
Original PDF page 20: L1 Oral soft tissue examination and lesion evaluation slides, p.20 ↩
-
Original PDF page 21: L1 Oral soft tissue examination and lesion evaluation slides, p.21 ↩
-
Original PDF page 22: L1 Oral soft tissue examination and lesion evaluation slides, p.22 ↩
-
Original PDF page 23: L1 Oral soft tissue examination and lesion evaluation slides, p.23 ↩
-
Original PDF page 24: L1 Oral soft tissue examination and lesion evaluation slides, p.24 ↩
-
Original PDF page 28: L1 Oral soft tissue examination and lesion evaluation slides, p.28 ↩
-
Original PDF page 29: L1 Oral soft tissue examination and lesion evaluation slides, p.29 ↩
-
Original PDF page 31: L1 Oral soft tissue examination and lesion evaluation slides, p.31 ↩
-
Original PDF page 25: L1 Oral soft tissue examination and lesion evaluation slides, p.25 ↩
-
Original PDF page 26: L1 Oral soft tissue examination and lesion evaluation slides, p.26 ↩
-
Original PDF page 27: L1 Oral soft tissue examination and lesion evaluation slides, p.27 ↩
-
Original PDF page 30: L1 Oral soft tissue examination and lesion evaluation slides, p.30 ↩
-
Original PDF page 32: L1 Oral soft tissue examination and lesion evaluation slides, p.32 ↩