OPMDs and Oral Cancer II — OPMD nomenclature, classification, and key entities
Key paper (Warnakulasuriya 2007)1
Publication info2
- Journal: J Oral Pathol Med. 2007 Nov;36(10):575–80
- DOI: 10.1111/j.1600-0714.2007.00582.x
- Authors: S Warnakulasuriya, Newell W Johnson, I van der Waal
- Reference Standards: WHO Classification 2020/2021 updates
- Key Speaker: Participant in the WHO Collaborating Center for Oral Cancer workshop
- PMID: 17944749
Core takeaways (from abstract)
- Recommended term: “potentially malignant disorders (OPMDs)” (not all transform).
- Leukoplakia definition: “white plaques of questionable risk…” after excluding other no-risk disorders.
- Dx framework: suggested to reduce misclassification of “white lesions.”
- Terminology evolves with multi-step carcinogenesis understanding.
Clinical Context
The lecture highlights the transition from traditional terminology to evidence-based classifications established by the WHO in 2020, detailing specific entities such as leukoplakia, erythroplakia, and oral lichen planus, while emphasizing the role of risk factors like tobacco, alcohol, and areca nut.
Definitions & terminology
OPMD definition (WHO 2020)3
- OPMDs = lesions/conditions with increased risk of developing cancer of the lip and the oral cavity (C00, C02–C06).
Traditional terminology (older framework) 4
Consensus: “OPMD” umbrella term5
Includes (examples):
- Leukoplakia
- Erythroplakia
- Proliferative verrucous leukoplakia
WHO classification updates (2020/2021)
 |  |
Removed in 2021 (limited evidence)6
- Oral Epidermolysis Bullosa
- Chronic hyperplastic candidosis
- Exophytic verrucous hyperplasia / verrucous hyperplasia
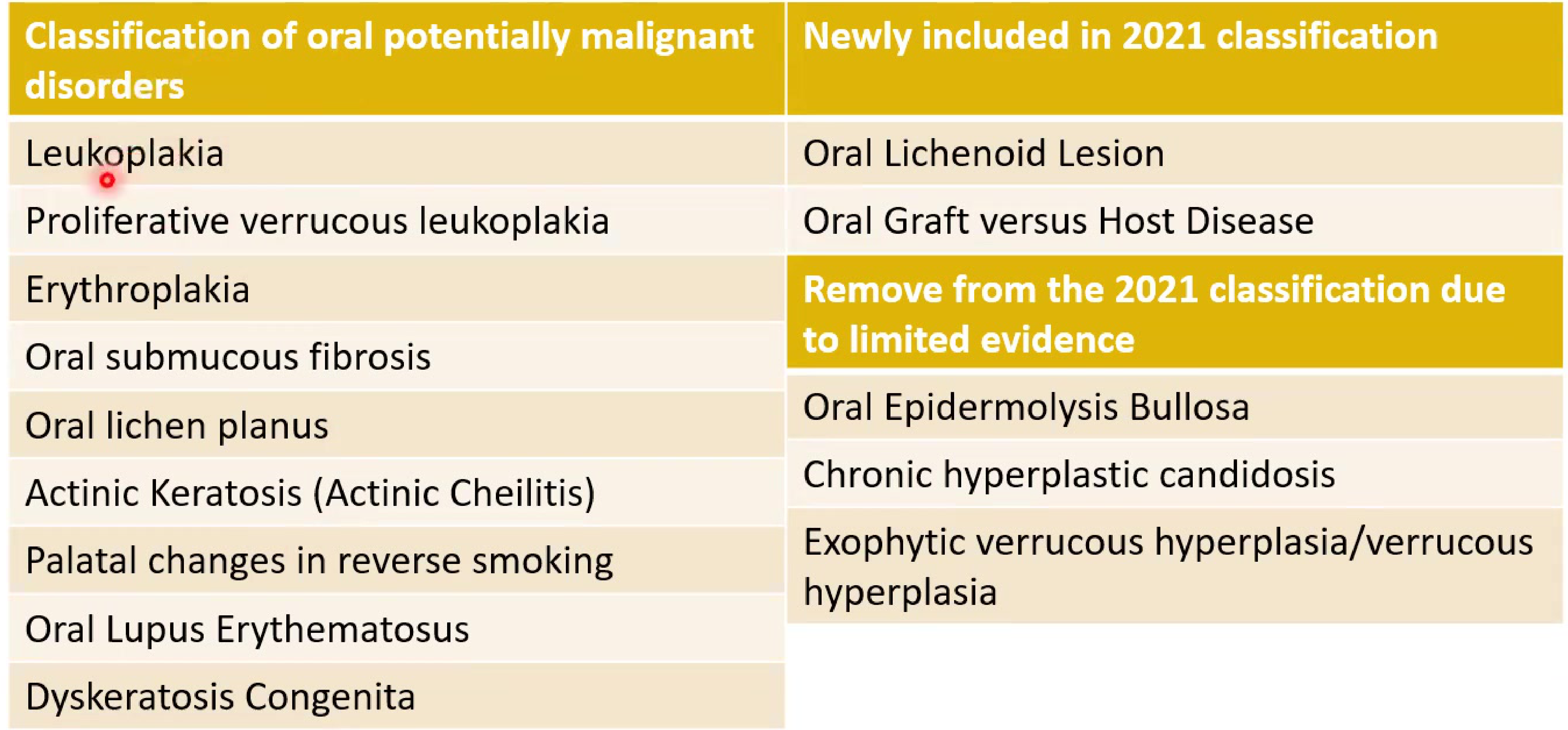
Current OPMDs (WHO 2021 list)7
- Leukoplakia
- Proliferative verrucous leukoplakia
- Now recognized as a specific, distinct entity.
- Erythroplakia
- Oral submucous fibrosis
- Oral lichen planus
- Actinic keratosis / actinic cheilitis
- Palatal changes in reverse smoking
- Oral lupus erythematosus
- Dyskeratosis congenita
Newly included (2021)7
- Oral lichenoid lesion
- Now a separate entity from Lichen Planus.
- Oral graft versus host disease
- Newly included (seen in transplant patients).
Epidemiology (OPMDs)
Prevalence overview8
- Global prevalence: 4.47% (95% CI 2.43–7.08)
- Higher prevalence in:
- Asian populations
- Male individuals
Risk factors (major carcinogenic exposures)
Tobacco / nicotine products
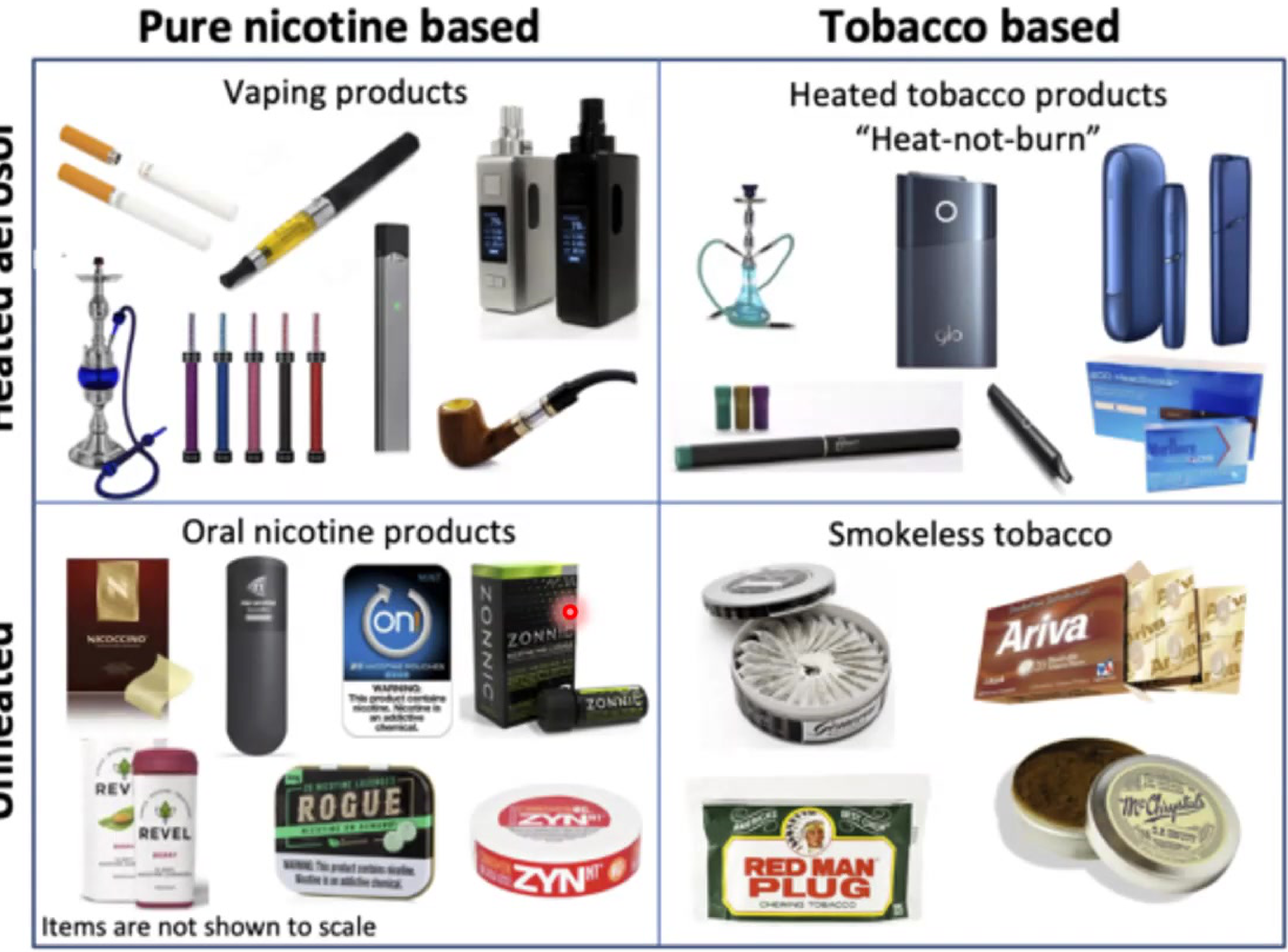 |  |
Delivery systems9
- Pure nicotine-based
- Vaping products
- Tobacco-based
- Heated tobacco products (“heat-not-burn”)
- Hubble Bubble (Shisha/Hookah) and traditional cigarettes
- Powders and unheated tobacco products (Smokeless)
- Oral nicotine products
- Smokeless tobacco
Risk statements1011
- Smokers: ~10× higher risk of oral cancer vs non-smokers.
- Tobacco contains numerous carcinogenic chemical compounds.
- Nicotine is the primary addictive substance, necessitating smoking cessation counseling by dentists.
- “Nicotine potency vs heroin” statement retained as written in your notes (verify if needed):
- Nicotine is 10 times more potent than heroin on a milligram-for-milligram basis.
Alcohol1213
- Moderate drinking: ↑ risk (oral/pharynx 1.8×; larynx 1.4×)
- Heavy drinking: ↑ risk (oral/pharynx 5×; larynx 2.6×)
- Tobacco + alcohol:
- major combined aetiological factor
- up to 75% of OPMD cases (as per slide note)
Betel quid / areca nut14
- Areca nut: copper/flavonoids → collagen cross-linking → fibrosis
- Alkaloids (arecoline) → ↑ collagen synthesis, ↓ degradation; nitrosamine formation
- Gutka: tobacco + lime + spices in betel leaf → more rapid lesion development
HPV15
- HPV estimated responsible for ~70% of oropharyngeal cancers (US).
- High-risk subtypes include HPV-16 and HPV-18.
- Transmission is often related to oral sex.
Leukoplakia
Clinical types / appearance
 |  |
 |  |
Core facts16
- Persistent white patch, cannot be rubbed off, usually asymptomatic
- Prevalence:
- global 2–3%
- Western countries 1–4%
- SE Asia higher
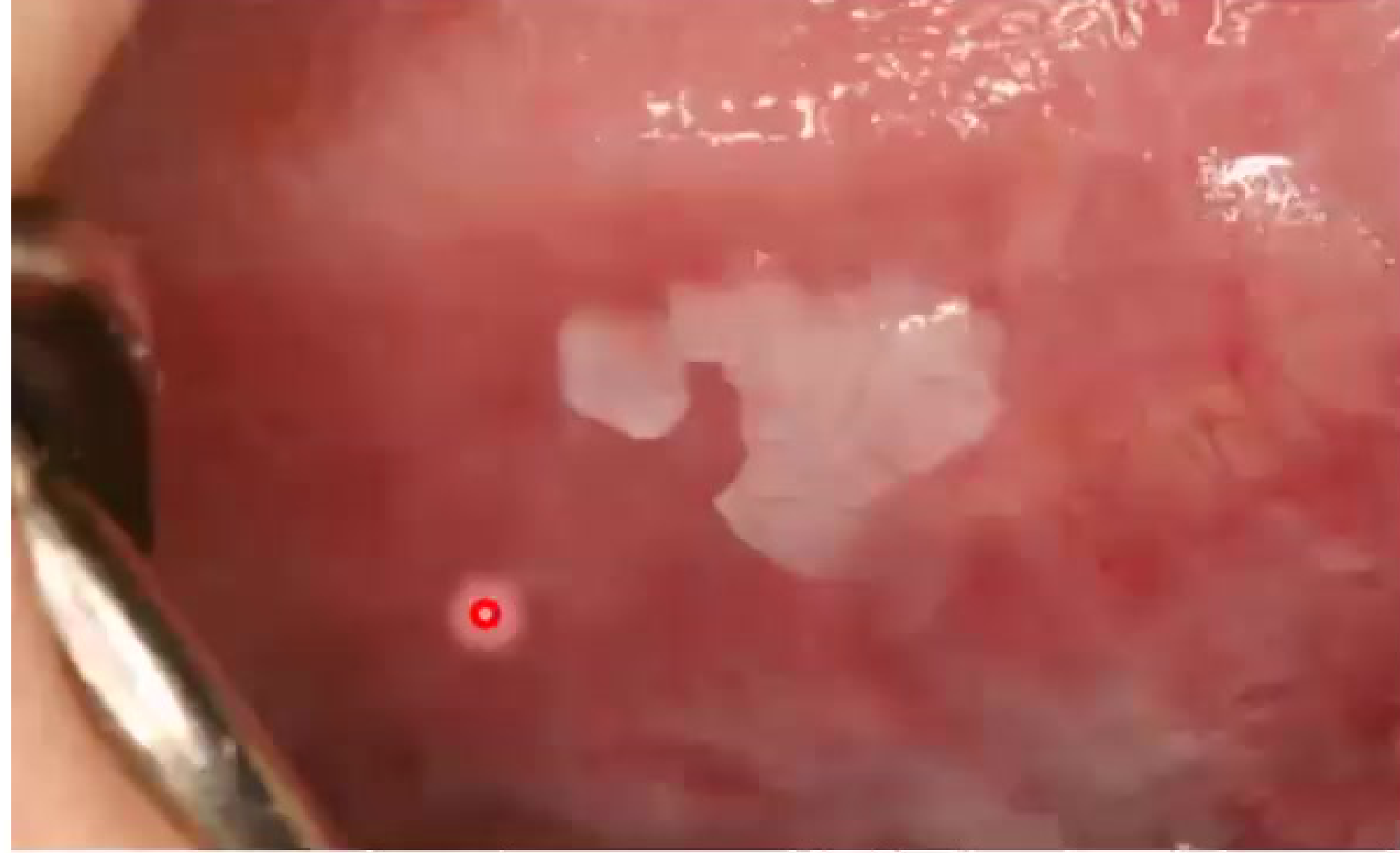
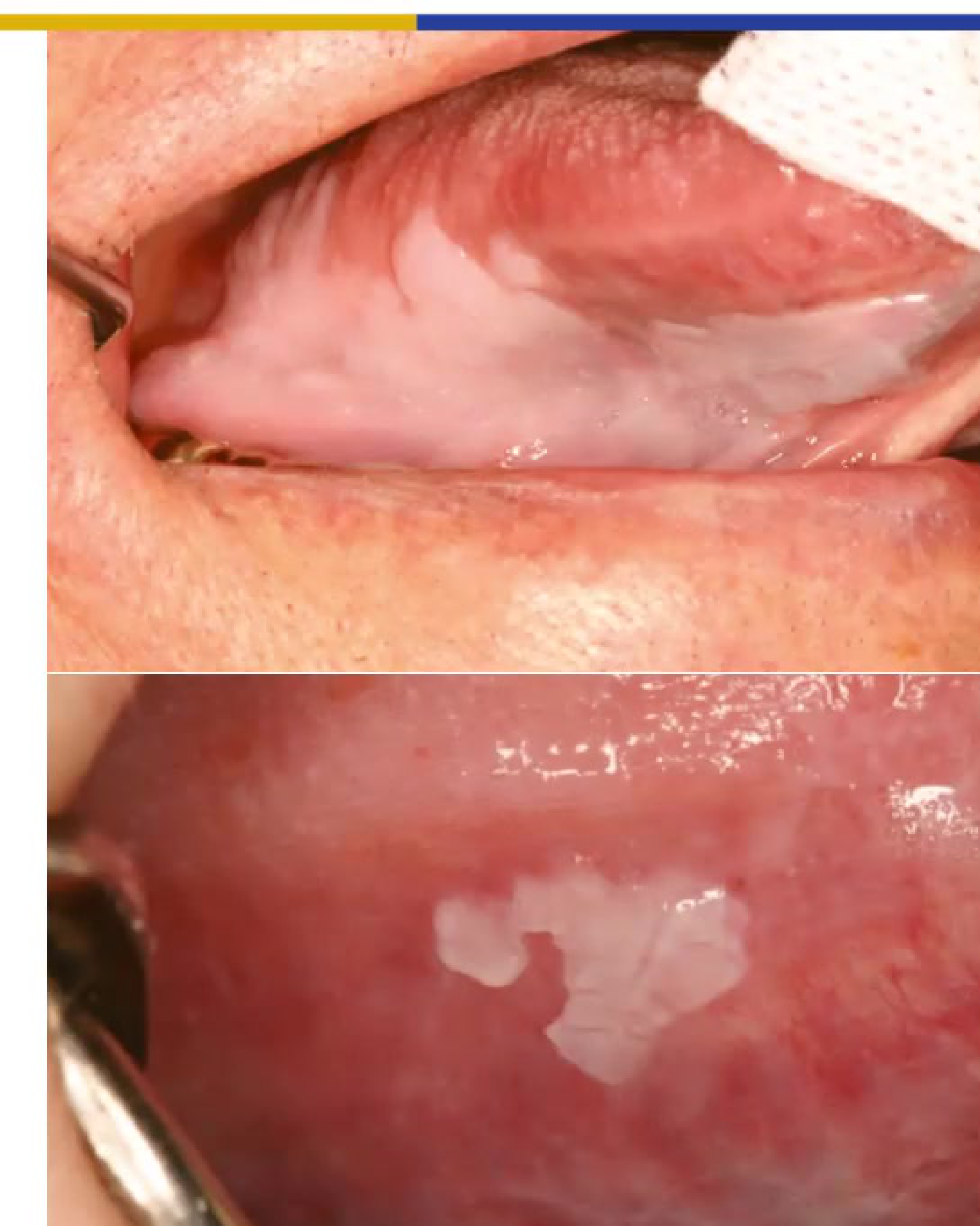
Morphology (memorize)
- Homogeneous: uniform white, flat/thin, smooth ± shallow cracks
- Nodular: small polypoid/rounded outgrowths (red/white excrescences)
- Verrucous: raised/exophytic, wrinkled/corrugated
- Speckled (erythroleukoplakia): mixed red + white
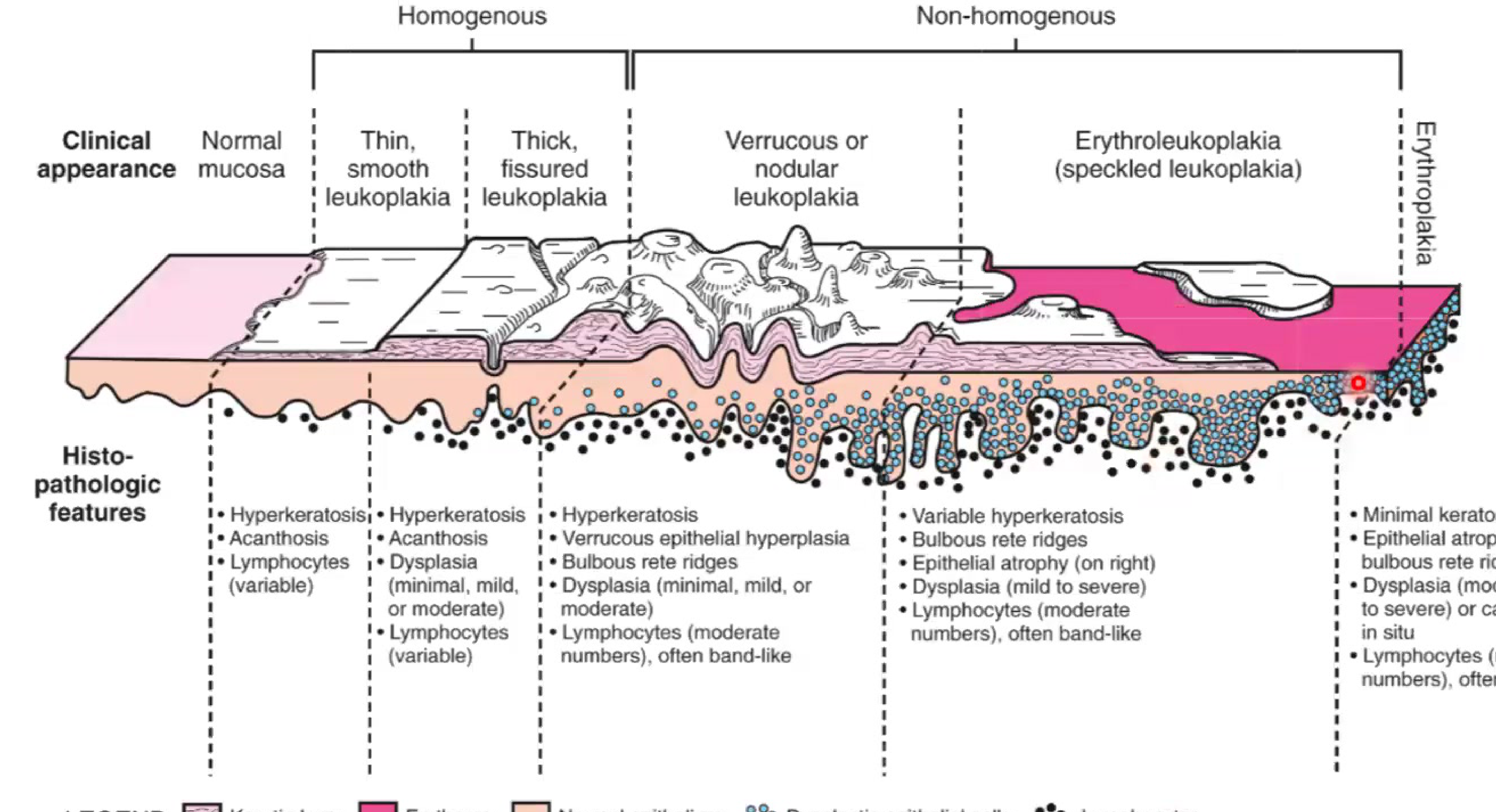
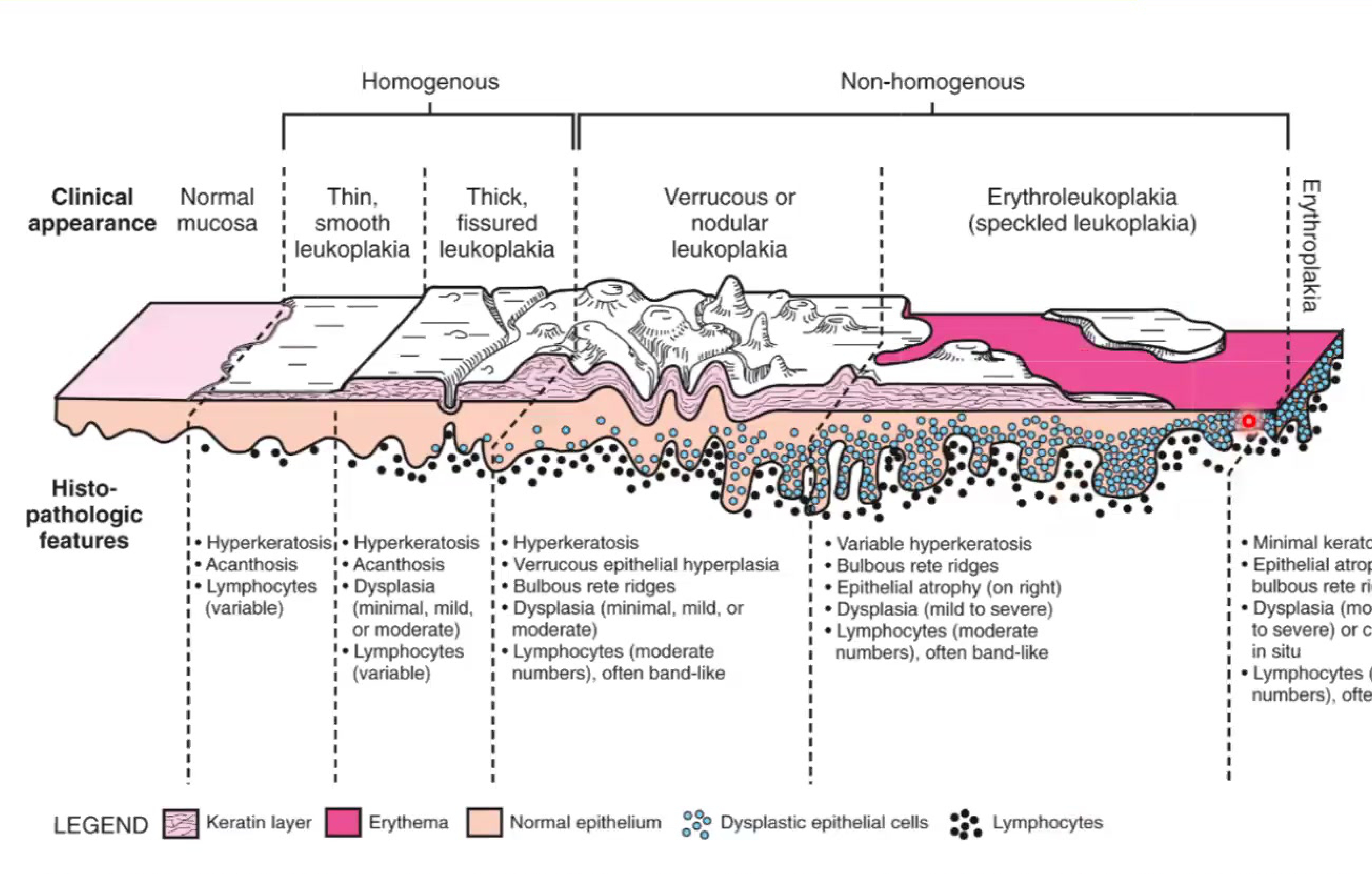
Clinical ↔ histology correlation17
| Clinical Type | Histopathologic Features |
|---|---|
| Thin, smooth leukoplakia (Homogenous) | • Hyperkeratosis • Acanthosis • Lymphocytes (variable) |
| Thick, fissured leukoplakia (Homogenous) | • Hyperkeratosis • Acanthosis • Dysplasia (minimal, mild, or moderate) • Lymphocytes (variable) |
| Verrucous or nodular leukoplakia (Non-homogenous) | • Hyperkeratosis • Verrucous epithelial hyperplasia • Bulbous rete ridges • Dysplasia (minimal, mild, or moderate) • Lymphocytes (moderate numbers), often band-like |
| Erythroleukoplakia / Speckled leukoplakia (Non-homogenous) | • Variable hyperkeratosis • Bulbous rete ridges • Epithelial atrophy • Dysplasia (mild to severe) • Lymphocytes (moderate numbers), often band-like |
| Erythroplakia | • Minimal keratosis • Epithelial atrophy or bulbous rete ridges • Dysplasia (moderate to severe) or carcinoma in situ • Lymphocytes (moderate numbers), often band-like |
Definition18
- “A predominantly white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer.”
Clinical diagnostic criteria (Dx of exclusion)
- White patch/plaque cannot be rubbed off
- Borders: homogeneous = often well-demarcated; non-homogeneous = more diffuse ± red/nodular
- Exclude trauma/friction (sharp tooth, masticatory friction, toothbrushing)
- Persistence after eliminating suspected cause
- Stretch test: does not fade/disappear on stretching
- If disappears on stretching → leukoedema
- If rubs off → likely candidiasis
- Exclude other white/white-red lesions
Aetiology / pathogenesis (risk factors)
- Tobacco, alcohol, areca nut/betel quid
- High-risk HPV: very rare in OPMDs (per note)
Erythroplakia
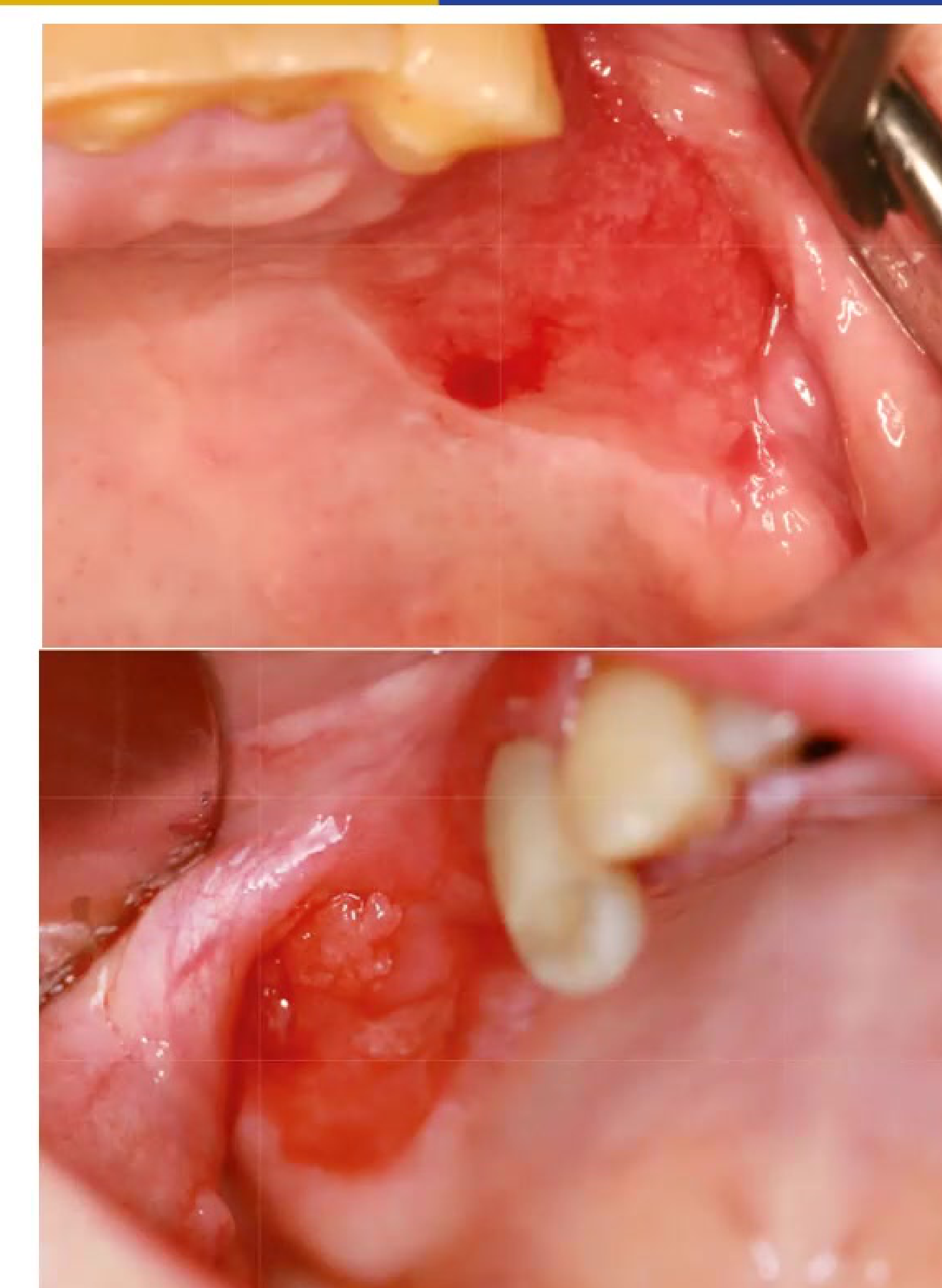
Definition19
- “A predominantly fiery red patch that cannot be characterized clinically or pathologically as any other definable disease.”
Clinical features
- Velvety red, granular appearance
- Usually painless and flat
- May be indurated (firm on palpation)
Diagnostic aids (adjuncts, not replacements)
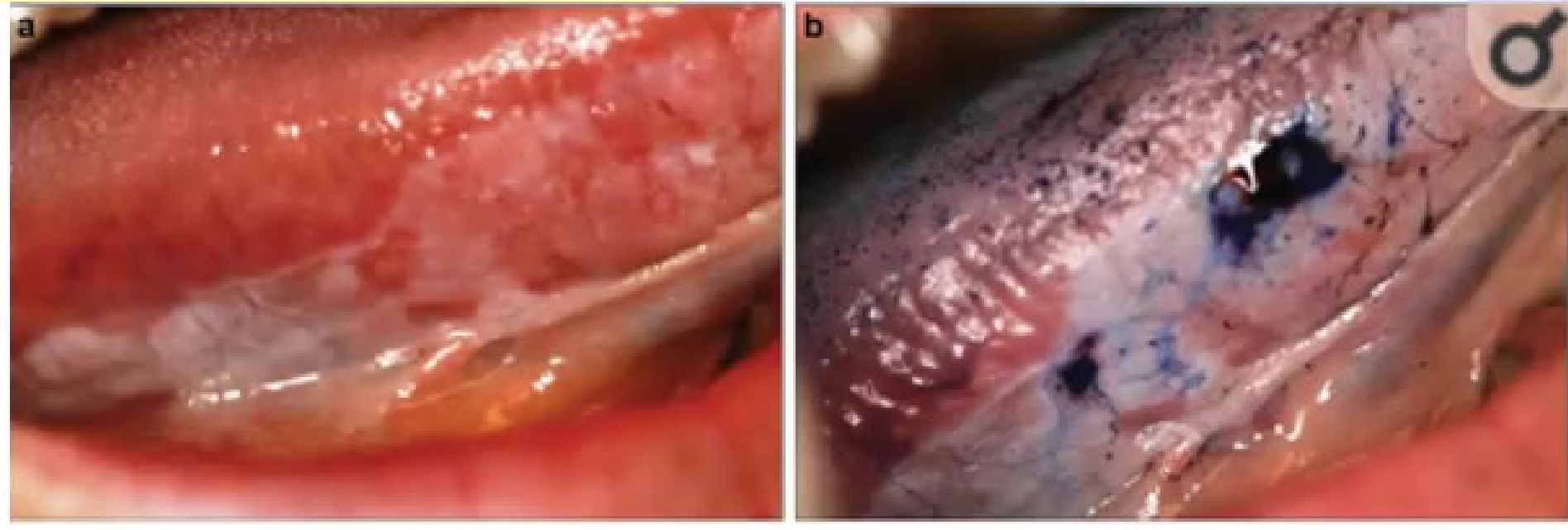 |  |
Approach20
- Leukoplakia/erythroplakia: diagnosis of exclusion
Adjunctive tools
- Toluidine blue / tolinium chloride stain
- Oral CDx brush biopsy kits
- Optical devices: autofluorescence (e.g., VELscope) and reflection devices
- Saliva testing: protein biomarkers
Diagnostic Aid Limitation
While these aids help visualization, they do not replace the gold standard of biopsy and histopathological examination.
Oral submucous fibrosis (OSF)
Aetiology / pathogenesis2122
- Areca nut (copper/flavonoids; arecoline) → fibrosis; nitrosamines
- Gutka → faster lesion development
Clinical features2324
- Diffuse pale, marble-like, keratotic areas
- Sites: buccal mucosa, soft palate, tongue
- Burning sensation
- Trismus (limited mouth opening)
- Often bilateral (buccal mucosa)
Diagnosis & management (overview)25
- Document history + high-quality photos + detailed notes
- Biopsy when indicated; ongoing monitoring
- Staged Stage 1–4
- Monitor for leukoplakia within fibrotic areas
- Pentoxifylline may be used
- Manage associated TMD if present
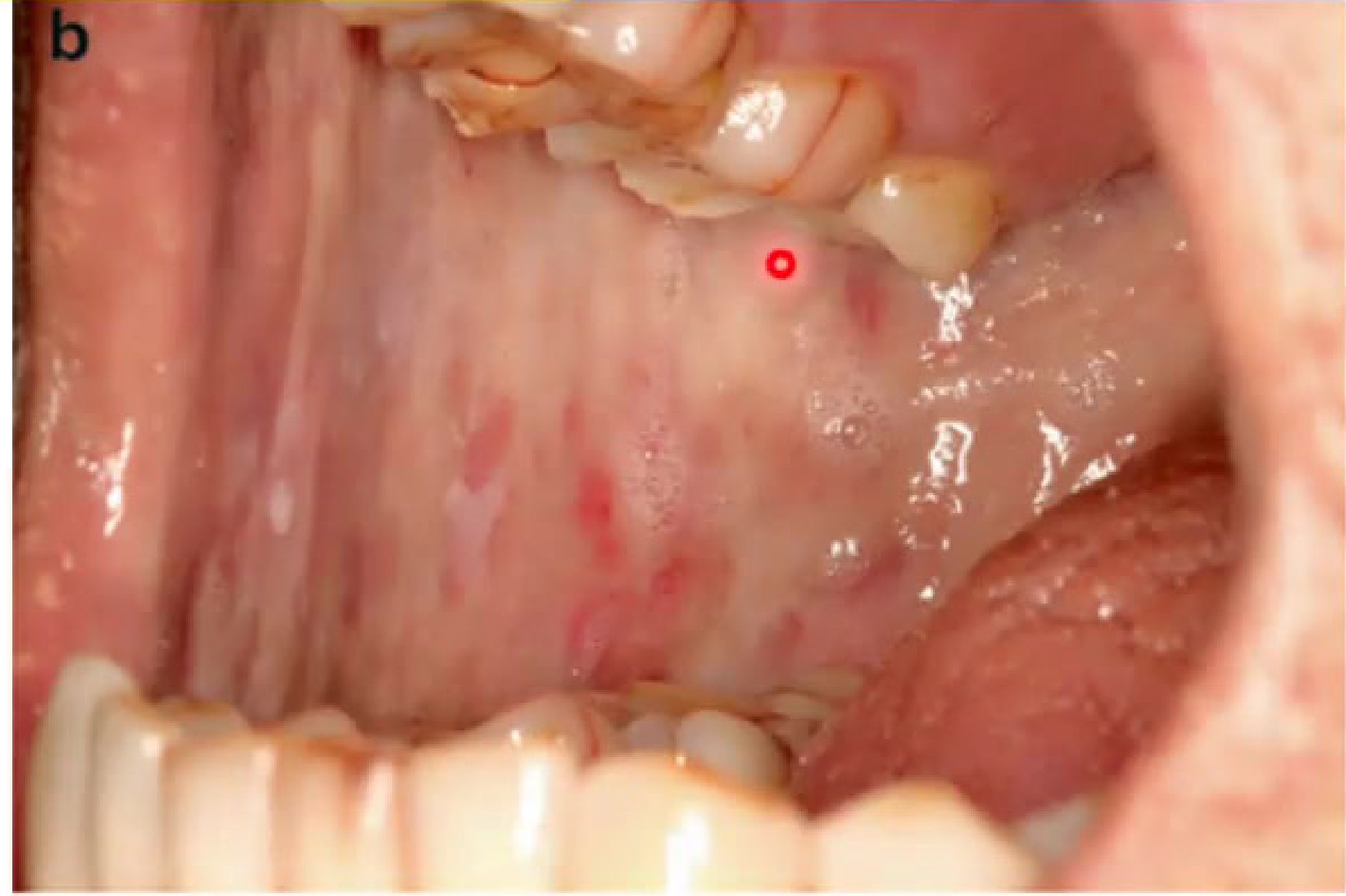
Palatal lesions in reverse smoking
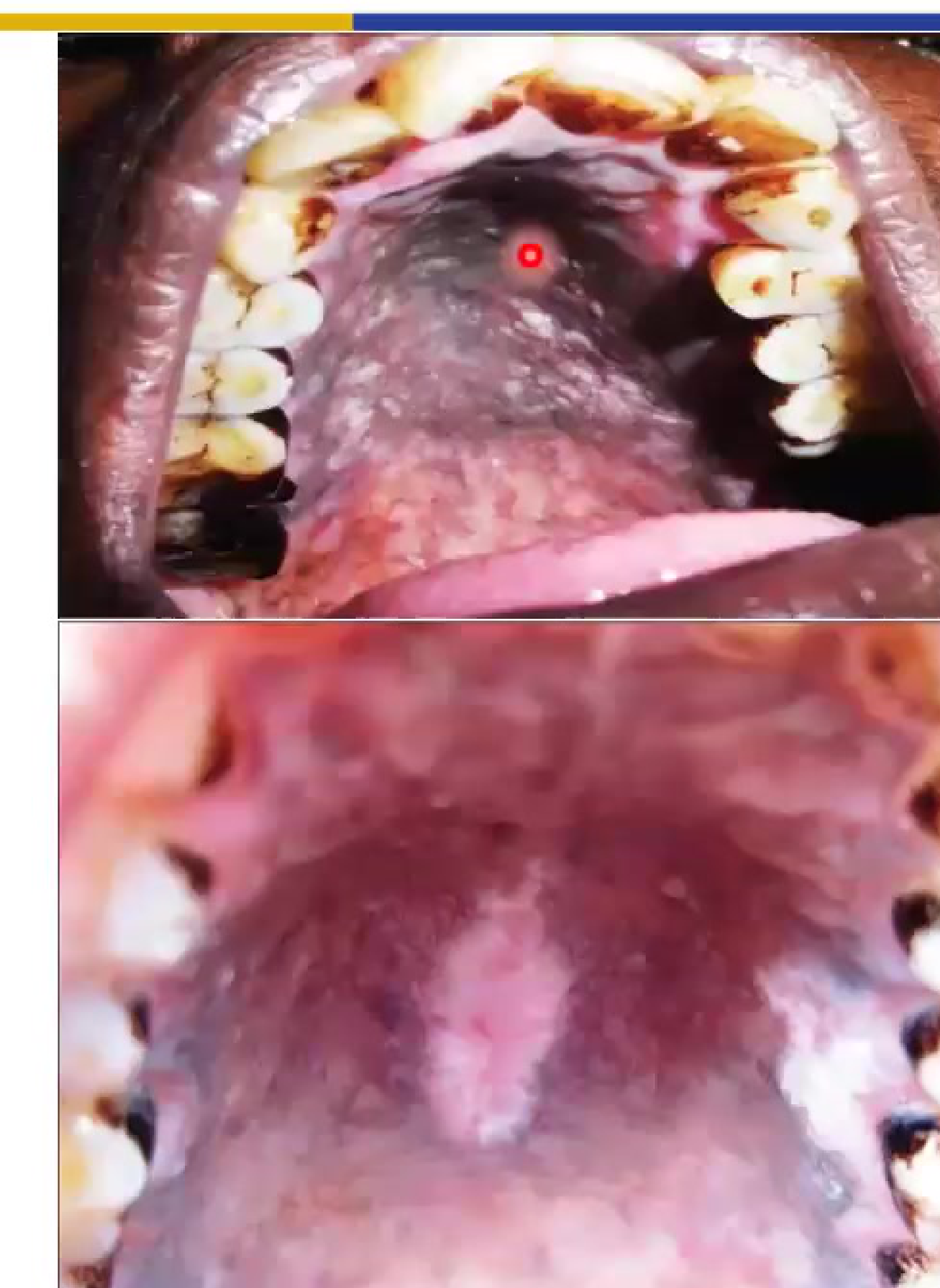
Clinical presentation26
- Hard palate: red dots (inflamed duct orifices), raised keratotic areas, diffuse whitening/thickening
- More common in females in some cultures (heated end inside mouth)
- Hyperpigmentation + high risk for frank malignancy
Actinic cheilitis (actinic keratosis of lip)
 |  |
Cause27
- Chronic UV exposure (similar pathogenesis to skin actinic keratosis)
Clinical pointers (memorize)28
- Usually lower lip > upper lip
- Vermilion border blurring/effacement; dry/scaly; white/gray patches ± erythema
- Concerning: crusting, ulceration, induration
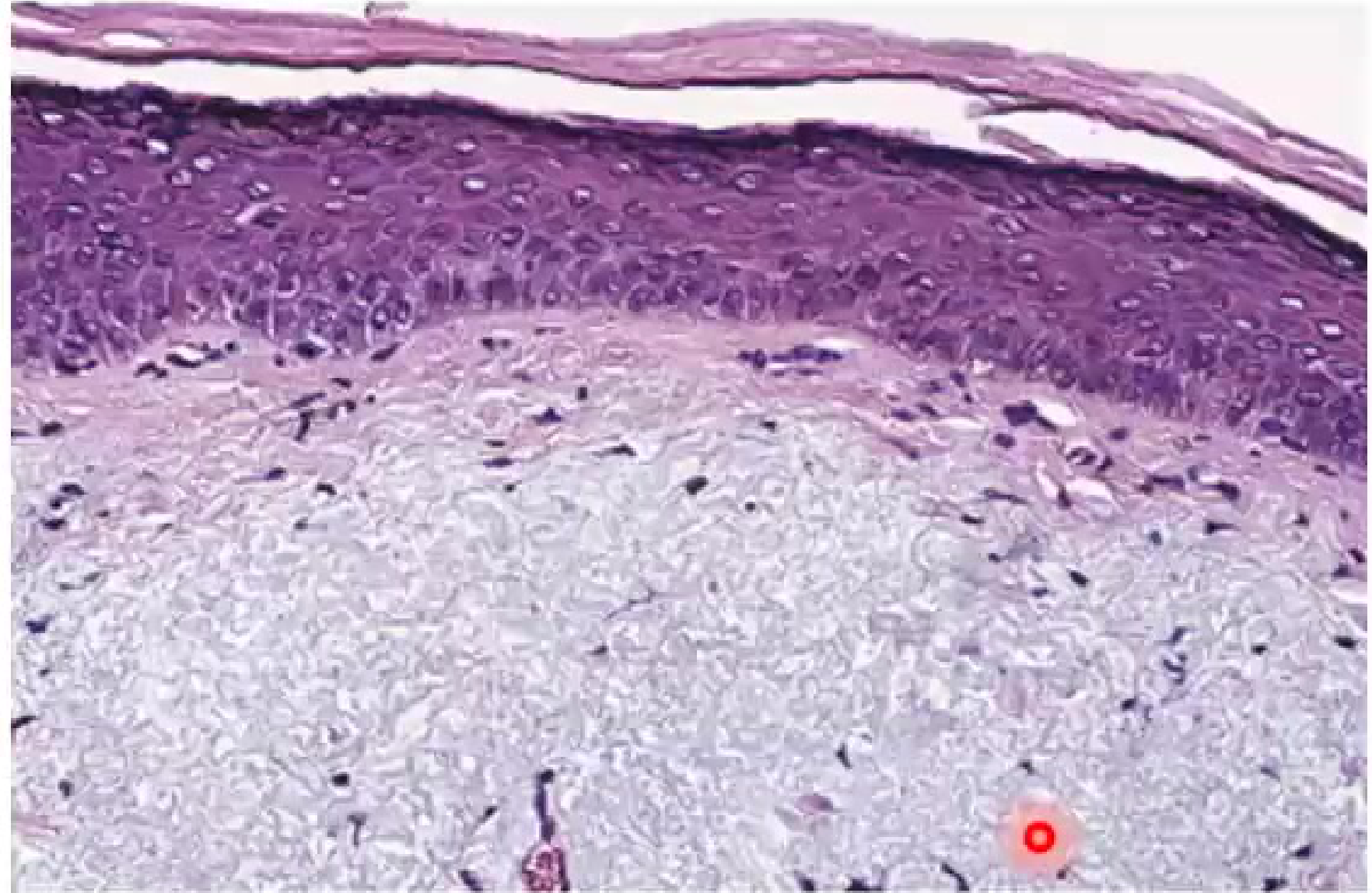
Histology29
- Dysplasia variable; solar elastosis; chronic inflammation
Management (options)29
- Sun protection (SPF lip balm)
- Topicals (5-FU, imiquimod)
- Cryotherapy / laser / PDT
- Vermilionectomy for extensive/refractory significant dysplasia
Oral lichen planus (OLP)
Pathogenesis30
- Immune mediated (T lymphocytes); idiopathic or drug-induced
Epidemiology31-32
- Prevalence 0.22–5%
- Age 30–80
- Female > male
- ~15% also cutaneous disease
Clinical Presentation of OLP
- Key Feature: Lesions are typically bilateral and symmetrical.
- Reticular: Most common; white Wickham’s striae.
- Erosive/Atrophic: Erythema; can present as desquamative gingivitis.
- Plaque-like: Can mimic leukoplakia or Proliferative Verrucous Leukoplakia.
Histopathology
- Hyperkeratosis (reticular/papular/plaque-like)
- Ulceration (atrophic variants)
Diagnostic criteria33
- Basal cell degeneration/loss (squamatization)
- Band-like lymphocytic infiltrate (variable thickness)
- Recommendation: biopsy all suspected cases (AAOMP position paper, per note)
Treatment
- Symptomatic: topical anti-inflammatory first-line
- Systemic therapy sometimes for severe/refractory disease
Oral lupus erythematosus / Discoid lupus (DLE)
LE classification34
- SLE
- Cutaneous LE:
- ACLE
- SCLE
- CCLE → classic DLE
DLE facts
- Most common chronic cutaneous LE
- 15–30% of SLE patients also have DLE
Clinical features3536
- Red-purple macules/plaques → hyperkeratotic surface → sharply demarcated discoid plaques
- Oral: sharp margins, scalloped white borders with radiating striae + telangiectasia
- Honeycomb appearance (palate)
- Painful ulceration common
Histology & diagnosis3738
- Acanthosis + atrophy; basal vacuolar degeneration
- Bandlike + deep perivascular/paravascular lymphocytes
- Biopsy-based diagnosis
- DIF: “Lupus band test” positive
Management
- Relapsing/remitting; immunosuppression mainstay (per note)
Footnotes
-
Original PDF page 3: L11 OPMDs and Oral Cancer II slides, p.3 ↩
-
Original PDF page 1: L11 OPMDs and Oral Cancer II slides, p.1 ↩
-
Original PDF page 2: L11 OPMDs and Oral Cancer II slides, p.2 ↩
-
Original PDF page 4: L11 OPMDs and Oral Cancer II slides, p.4 ↩
-
Original PDF page 5: L11 OPMDs and Oral Cancer II slides, p.5 ↩
-
Original PDF page 6: L11 OPMDs and Oral Cancer II slides, p.6 ↩
-
Original PDF page 7: L11 OPMDs and Oral Cancer II slides, p.7 ↩ ↩2
-
Original PDF page 8: L11 OPMDs and Oral Cancer II slides, p.8 ↩
-
Original PDF page 9: L11 OPMDs and Oral Cancer II slides, p.9 ↩
-
Original PDF page 10: L11 OPMDs and Oral Cancer II slides, p.10 ↩
-
Original PDF page 11: L11 OPMDs and Oral Cancer II slides, p.11 ↩
-
Original PDF page 12: L11 OPMDs and Oral Cancer II slides, p.12 ↩
-
Original PDF page 13: L11 OPMDs and Oral Cancer II slides, p.13 ↩
-
Original PDF page 14: L11 OPMDs and Oral Cancer II slides, p.14 ↩
-
Original PDF page 15: L11 OPMDs and Oral Cancer II slides, p.15 ↩
-
Original PDF page 16: L11 OPMDs and Oral Cancer II slides, p.16 ↩
-
Original PDF page 17: L11 OPMDs and Oral Cancer II slides, p.17 ↩
-
Original PDF page 18: L11 OPMDs and Oral Cancer II slides, p.18 ↩
-
Original PDF page 21: L11 OPMDs and Oral Cancer II slides, p.21 ↩
-
Original PDF page 22: L11 OPMDs and Oral Cancer II slides, p.22 ↩
-
Original PDF page 23: L11 OPMDs and Oral Cancer II slides, p.23 ↩
-
Original PDF page 24: L11 OPMDs and Oral Cancer II slides, p.24 ↩
-
Original PDF page 25: L11 OPMDs and Oral Cancer II slides, p.25 ↩
-
Original PDF page 26: L11 OPMDs and Oral Cancer II slides, p.26 ↩
-
Original PDF page 27: L11 OPMDs and Oral Cancer II slides, p.27 ↩
-
Original PDF page 28: L11 OPMDs and Oral Cancer II slides, p.28 ↩
-
Original PDF page 29: L11 OPMDs and Oral Cancer II slides, p.29 ↩
-
Original PDF page 30: L11 OPMDs and Oral Cancer II slides, p.30 ↩
-
Original PDF page 31: L11 OPMDs and Oral Cancer II slides, p.31 ↩ ↩2
-
Original PDF page 32: L11 OPMDs and Oral Cancer II slides, p.32 ↩
-
Original PDF page 33: L11 OPMDs and Oral Cancer II slides, p.33 ↩
-
Original PDF page 40: L11 OPMDs and Oral Cancer II slides, p.40 ↩
-
Original PDF page 42: L11 OPMDs and Oral Cancer II slides, p.42 ↩
-
Original PDF page 44: L11 OPMDs and Oral Cancer II slides, p.44 ↩
-
Original PDF page 45: L11 OPMDs and Oral Cancer II slides, p.45 ↩
-
Original PDF page 46: L11 OPMDs and Oral Cancer II slides, p.46 ↩
-
Original PDF page 47: L11 OPMDs and Oral Cancer II slides, p.47 ↩
-
Original PDF page 48: L11 OPMDs and Oral Cancer II slides, p.48 ↩