Oral Potentially Malignant Disorders: Risk of Progression to Malignancy
Oral potentially malignant disorders (OPMDs) represent a group of conditions characterized by a statistically increased risk of progressing to cancer. However, this risk is not uniform and varies significantly based on a range of patient-specific and lesion-related factors. Predicting the exact risk of progression for an individual patient remains a clinical challenge, requiring a comprehensive judgment based on the assessment of each unique case.
Common Clinical Presentations1
The most frequently encountered OPMD is leukoplakia. Other conditions that may be observed in clinical practice include:
- Leukoplakia: Idiopathic white patches categorized as homogeneous (uniform) or non-homogeneous (irregular)
- Speckled/Nodular Leukoplakia: Mixed red and white areas, often fissured or cracked
- Sublingual Keratosis: Serious white lesions exclusive to the ventral tongue and floor of mouth
- Lichen planus
- Oral submucous fibrosis
- Erythroplakia
- Erythroplakia: Red lesions carrying a significantly higher risk; 90% show severe dysplasia or carcinoma in situ
Factors Influencing Malignant Transformation
Several key factors are associated with an increased likelihood of a lesion progressing to malignancy:
- Patient Demographics: Factors such as sex.
- Patients over age 50; female non-smokers with leukoplakia are a very high-risk group
- Lesion Characteristics: The specific site and clinical type of the lesion.
- High-risk sites: Lateral border of the tongue and floor of the mouth
- Morphology: Non-homogeneous lesions like Verrucous Proliferative Leukoplakia (VPL) have a ~45% transformation rate
- Lifestyle Habits: Behaviors including smoking and alcohol consumption.
- Long history of smoking or use of betel tobacco
- Histologic Findings: The presence and severity of epithelial dysplasia upon microscopic examination.
Risk Assessment and Clinical Evaluation
Identifying important risk factors is essential for effective patient management. A structured approach, such as a clinical algorithm, can serve as a guide for risk assessment at every stage of a patient’s evaluation to better determine the prognosis and necessary interventions.
Clinical Management Goals
Practitioners must estimate the timeframe of potential malignant events, identify and mitigate patient-specific risk factors, and distinguish between idiopathic patches and those with known causes like trauma or infection.
Clinical Assessment of Suspicious Oral Lesions
The clinical assessment of a suspicious oral lesion involves a multi-factorial approach considering patient history, clinical examination, and histological findings to determine the risk of malignancy.
Patient History and Risk Factors2
Certain demographic and behavioral factors influence the risk profile of an oral lesion:
- Demographics: Age >50, Male, or Female (noting specific risk variations).
- Habits: Persistent smokers vs. non-smokers
- Tobacco (type and consumption levels) and alcohol intake
- Symptoms: Rapid onset of a lesion, weight loss, or neurological signs like numbness or pain
- Dental History: Presence of ill-fitting dentures, sharp restorations, or missing opposing teeth causing chronic friction.
- Anatomical Site: High-risk locations include the tongue or floor of the mouth.
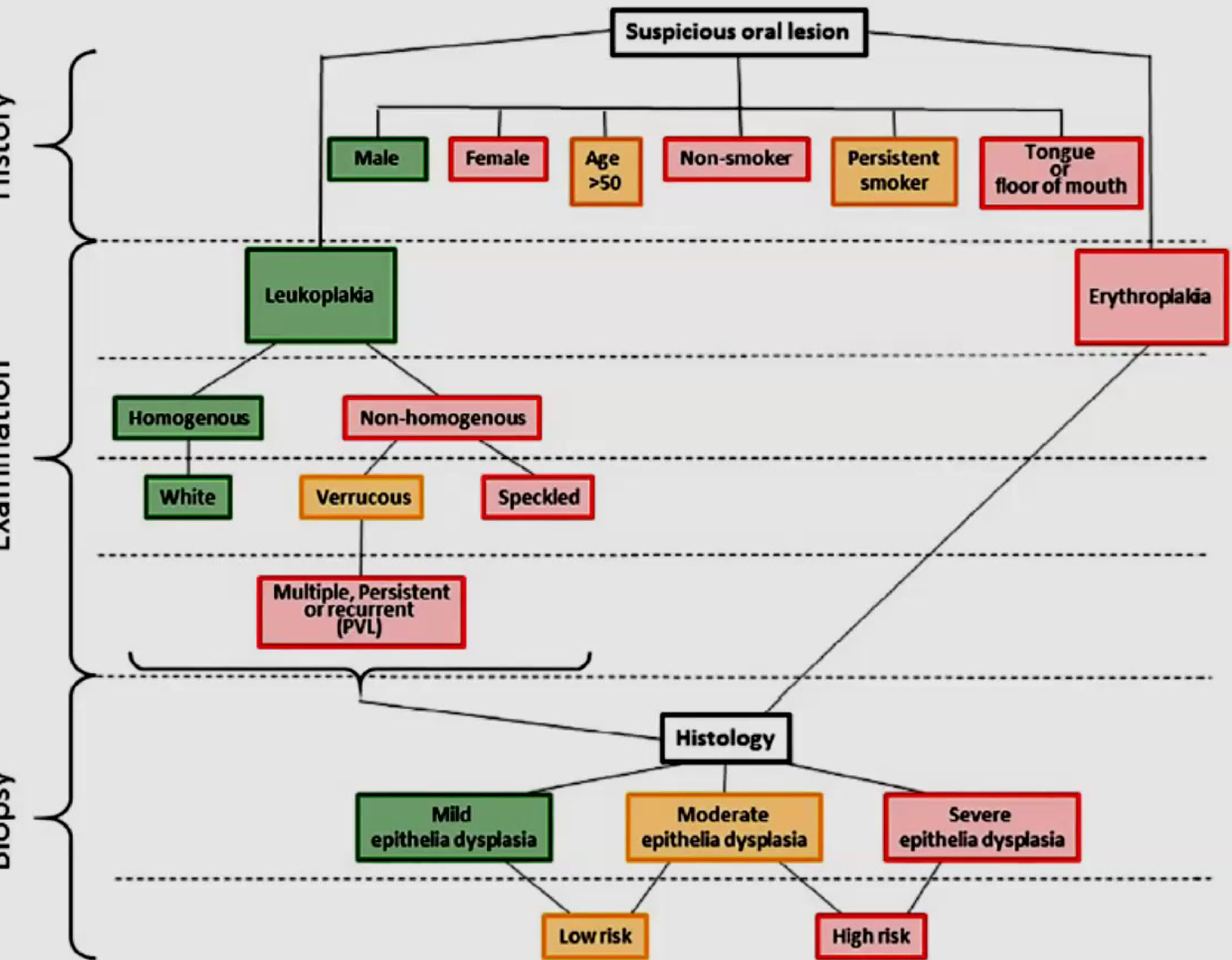
Clinical Examination and Morphology
Lesions are categorized based on their appearance and clinical behavior:
- Erythroplakia: Red patches (high risk).
- Leukoplakia: White patches, further divided into:
- Homogenous: Uniformly white appearance.
- Non-homogenous: Higher risk presentations including:
- Verrucous (wart-like)
- Speckled (mixed red and white)
- Proliferative Verrucous Leukoplakia (PVL): Characterized by multiple, persistent, or recurrent lesions; associated with high risk
Clinical Red Flags
- Induration: Palpation is critical; a firm or 'hard' feel suggests the lesion is infiltrating deeper tissues.
- Borders: Malignant lesions often have ill-defined or ragged borders.
- Healing: Any ulcer that does not heal within two weeks after removing potential irritants must be considered suspicious.
- Lymphadenopathy: Examination of the neck for swollen, fixed, or hard lymph nodes. .
Biopsy and Histological Grading
Histology is used to grade epithelial dysplasia and determine the overall risk level:
- Mild Epithelial Dysplasia: Generally categorized as low risk.
- Moderate Epithelial Dysplasia: May be categorized as low or high risk depending on clinical context.
- Severe Epithelial Dysplasia: Categorized as high risk
Biopsy Protocol
In principle, every persistent white patch should have a biopsy sample removed as histopathology is the 'gold standard' to check for invasive tumor islands.
Differential Diagnosis of White Lesions
Idiopathic White Patches and Leukoplakia345
Idiopathic white patches are clinically referred to as “leukoplakia.” These lesions may represent a range of histological changes from simple keratosis to malignancy.
Definition
Leukoplakia is a diagnosis of exclusion; it is idiopathic, meaning it remains only after excluding all other known pathologies.
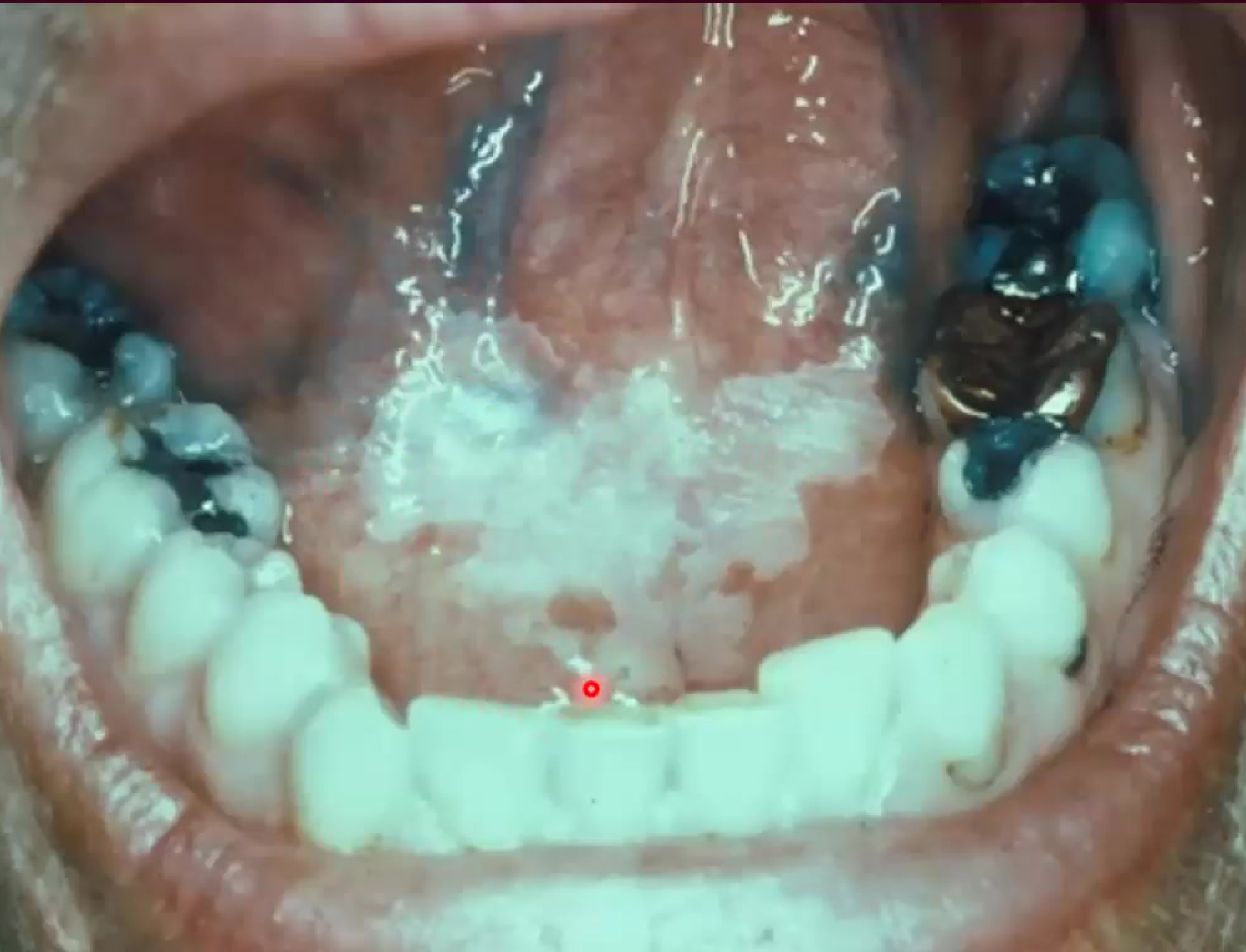
 Sublingual keratosis , where you have a white lesion exclusively on ventral surface of tongue and floor of the mouth Sublingual keratosis , where you have a white lesion exclusively on ventral surface of tongue and floor of the mouth | 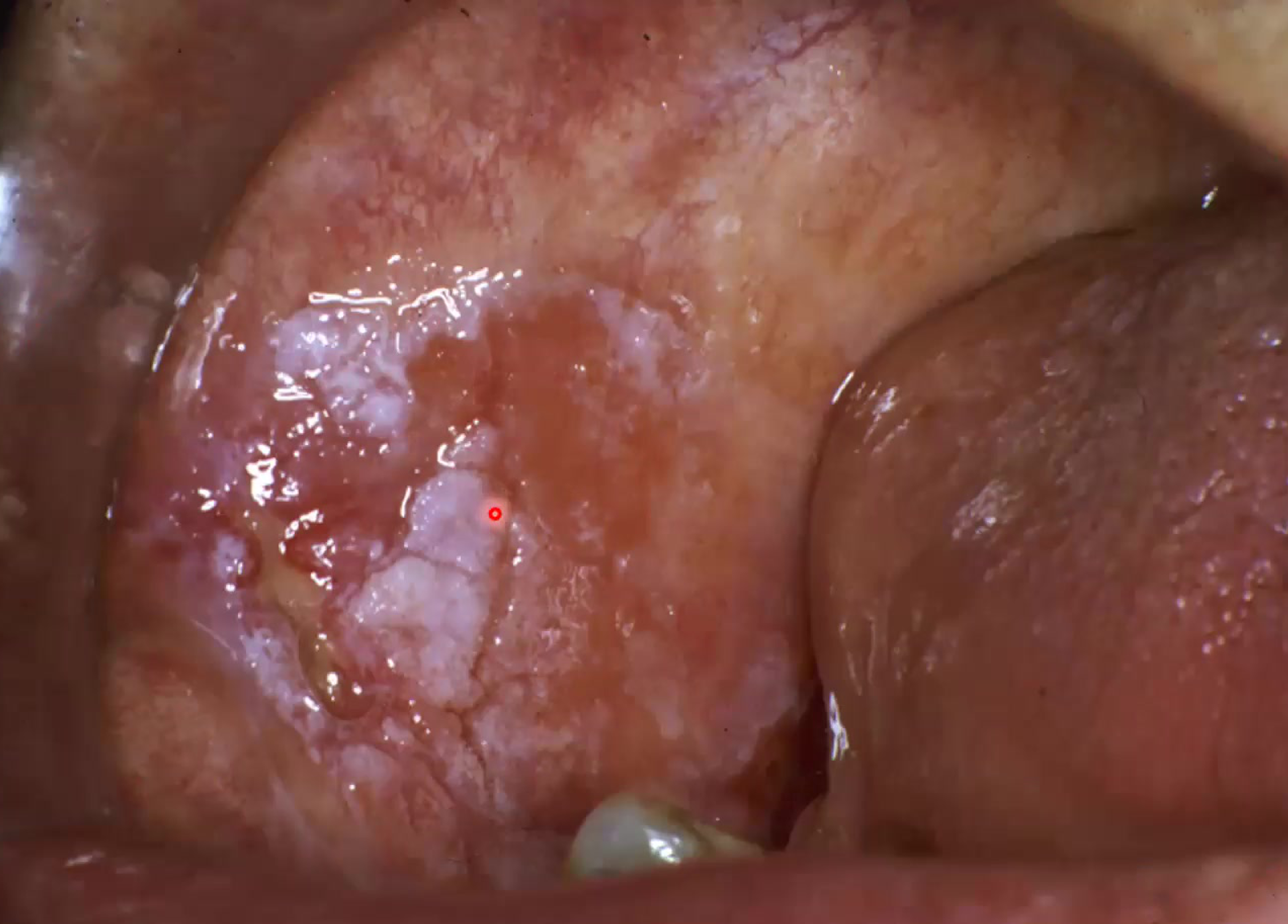 Speckeld and nodular leukoplakia, erythmatous and white areas too with fissures and cracks Speckeld and nodular leukoplakia, erythmatous and white areas too with fissures and cracks |
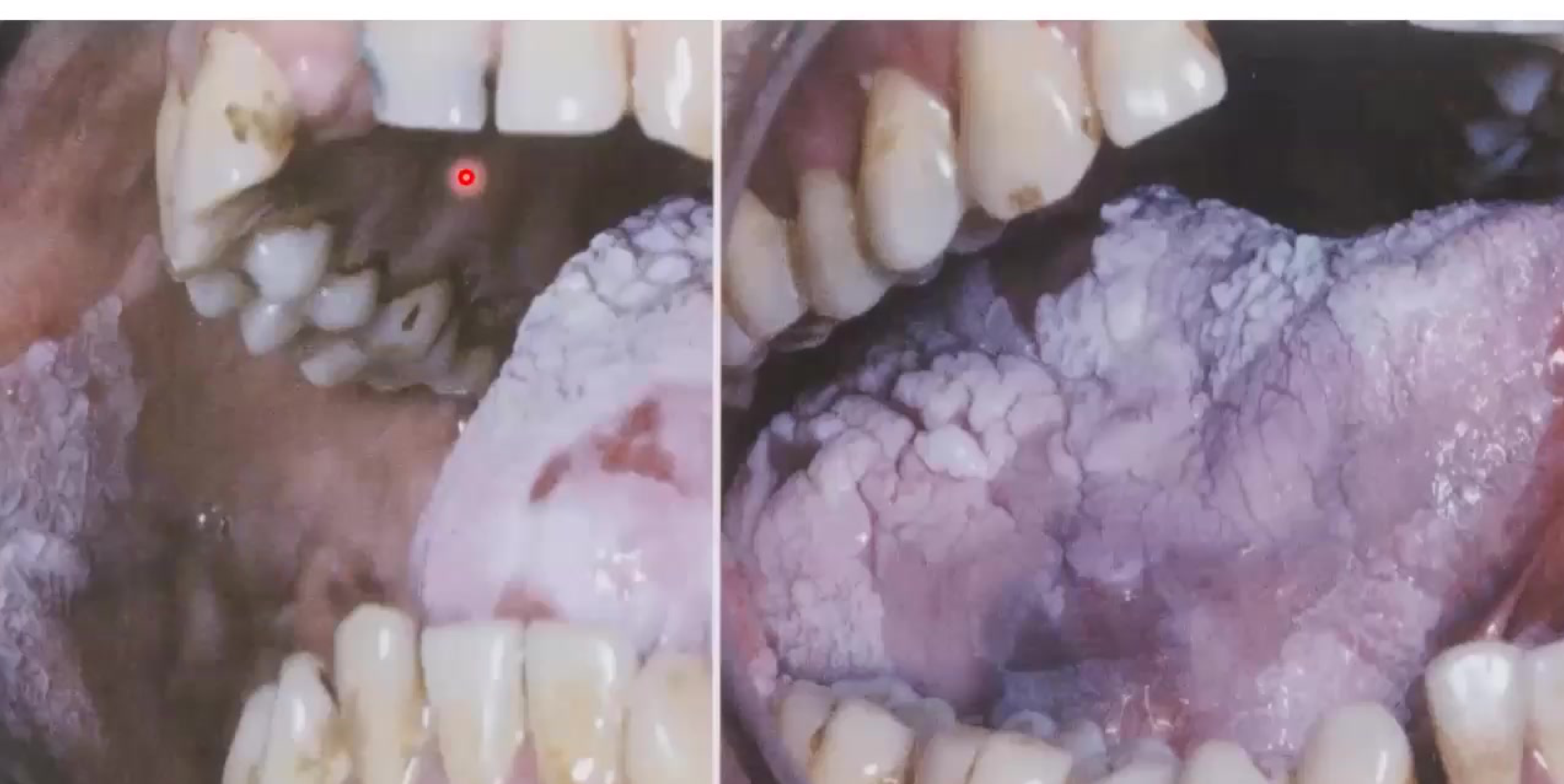 | |
| Significant white lesion |
Keratosis and Dysplasia6
- Clinical Presentations:
- Homogeneous
- Nodular
- Verrucous
- Speckled
- Specific Variants and Sites:
- Sublingual keratosis
- Proliferative verrucous leukoplakia
- Presumed Aetiology:
- Smokers’ keratosis
- Actinic keratoses
- Frictional keratosis (caused by trauma) must be differentiated from true leukoplakia
- If a biopsy shows dysplasia, the risk of progression is significantly higher
Malignancy
- Squamous cell carcinoma: Idiopathic white patches may also present as or progress to invasive squamous cell carcinoma.
Classification and Diagnostic Categories789
Establishing a differential diagnosis for white lesions in the mouth is essential for identifying potentially malignant disorders.
The diagnostic process is complicated by several factors:
- There are a high number of clinical possibilities for white lesions.
- There is a high frequency of insignificant or benign lesions that may mimic more serious conditions.
To aid in diagnosis, lesions can be organized into the following useful categories:
- Not really a white lesion (pseudo-membranes or debris)
- Normal anatomical variations
- Developmental conditions
- Traumatic lesions
- Infectious processes
- Candidosis (specifically "pseudomembranous" which rubs off, unlike leukoplakia)
- Lichen planus and similar lichenoid conditions
- Idiopathic lesions
Clinical Differentiation Strategies
Effective differentiation of oral lesions requires a systematic evaluation of clinical features and diagnostic testing.
Diagnostic Questions and Observations10
- Malignancy: Is there clinical evidence of carcinoma?
- Look for induration, rapid growth, and ill-defined borders
- Normalcy: Is the appearance within the range of normal anatomical variation?
- Developmental: Is there evidence for a long-standing developmental condition?
- Etiology: Are there specific habits or causes of friction (trauma) present?
- Site Specificity: Does the location help narrow the diagnosis (e.g., Chronic Hyperplastic Candidiasis [CHC], Oral Hairy Leukoplakia [OHL], or Stomatitis Nicotina [SN])?
- Morphology: Are there characteristic features like striae (Wickham striae)?
Risk Assessment and Investigation
-
Evaluate specific risk features for dysplasia or malignancy.
-
Utilize diagnostic aids such as a smear (cytology).
-
Perform a biopsy for definitive histological diagnosis.
-
Rub-off test: To exclude pseudomembranous candidiasis
-
Observation: Short-term monitoring after removing a suspected trauma source
-
Biopsy is essential if the lesion persists or if the patient has a history of previous oral cancer
Oral Malignant Neoplasms
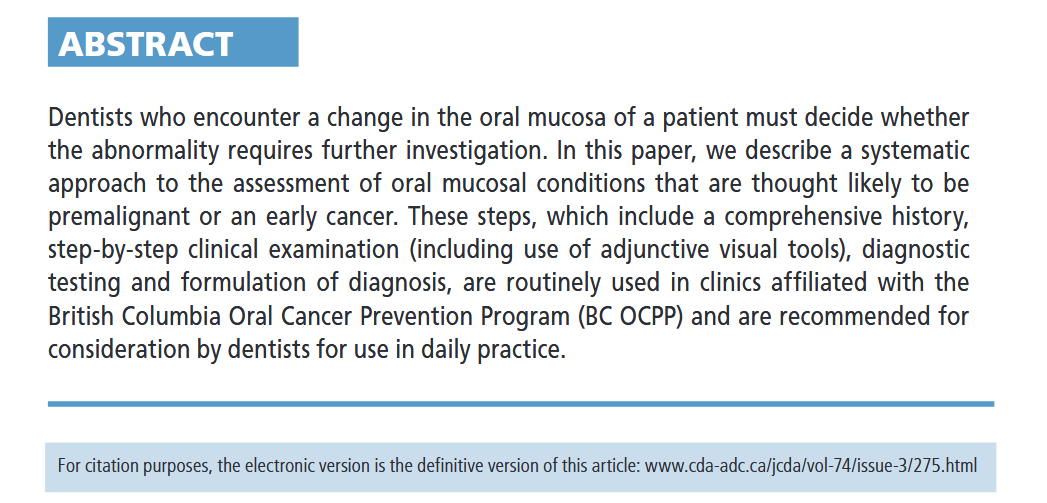
Evaluation of a Suspicious Oral Mucosal Lesion
Abstract
Link to original
Introduction to oral cancer and Global Burden
Global Incidence11
- More than 350,000 patients are diagnosed with oral cavity and lip cancer annually worldwide.
- The global incidence is rising, with nearly 400,000 new cases annually.
Types of Oral Malignancies
Common Malignancies12
- Oral Squamous Cell Carcinoma (OSCC)
- OSCC accounts for 90% of all oral malignancies.
Less Common Malignancies
- Salivary gland tumours
- Malignant melanoma
- Lymphoma
- Neoplasms of bone and connective tissue
- Specific odontogenic tumours
- Maxillary antral carcinoma
- Metastatic neoplasms
- Kaposi sarcoma
Molecular Alterations in Oral Squamous Cell Carcinoma
Genetic Basis of Oral Cancer13
Oral cancer is a genetic disease. Development typically requires approximately 6 to 7 specific mutations.
Molecular Transformation
Risk factors (carcinogens) cause permanent defects in the cellular genetic makeup, requiring six to seven permanent molecular changes for a normal cell to transform into a cancer cell.
Mechanisms of Genetic Defect
Genetic defects in Oral Squamous Cell Carcinoma (OSCC) can be induced by several mechanisms:
- Gene amplification
- Translocations
- Point mutations
- Rearrangements
- Deletions
Clinical and Histological Features14
Example of OPMD preceding OSCC:
Squamous Cell Carcinoma Overview15
Squamous cell carcinoma is the most common malignant epithelial neoplasm of the oral region.
Clinical Presentation
OSCC often presents as a non-healing ulcer, an exophytic mass, or an indurated white/red patch.
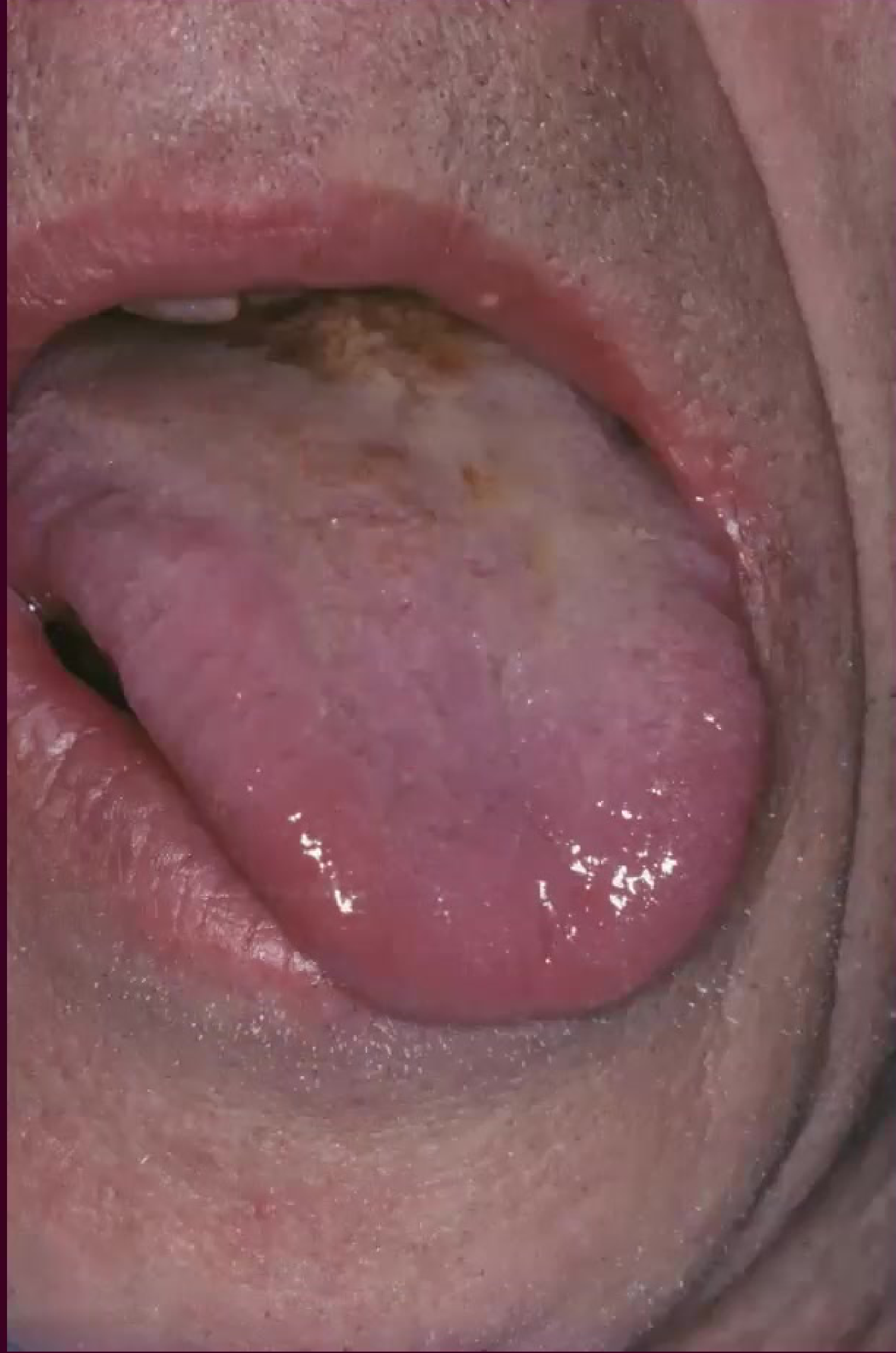
Common Clinical Sites16
Clinical presentations often include:
- White patches on the tongue
- Red, ulcerated lesions on the buccal mucosa (inner cheek) near the dentition
- Lateral border of the tongue
- Floor of the mouth
- Ventral tongue

Clinical and Diagnostic Indicators17
- History: Growth may be slow or fast; may present with or without pain or neurological signs; impaired function; presence of known risk factors.
- Consistency: Indurated (hardened) and non-encapsulated.
- Size: Progressive increase in size; can present as large or small lesions.
- Ulceration: May or may not be present.
- Spread: Potential for metastasis to regional lymph nodes.
- Imaging: Radiographic evidence of irregular patterns of bone destruction or soft tissue invasion.
- Fixation: The lesion is attached to underlying structures.
- Sensory changes: Numbness or tingling due to nerve involvement.
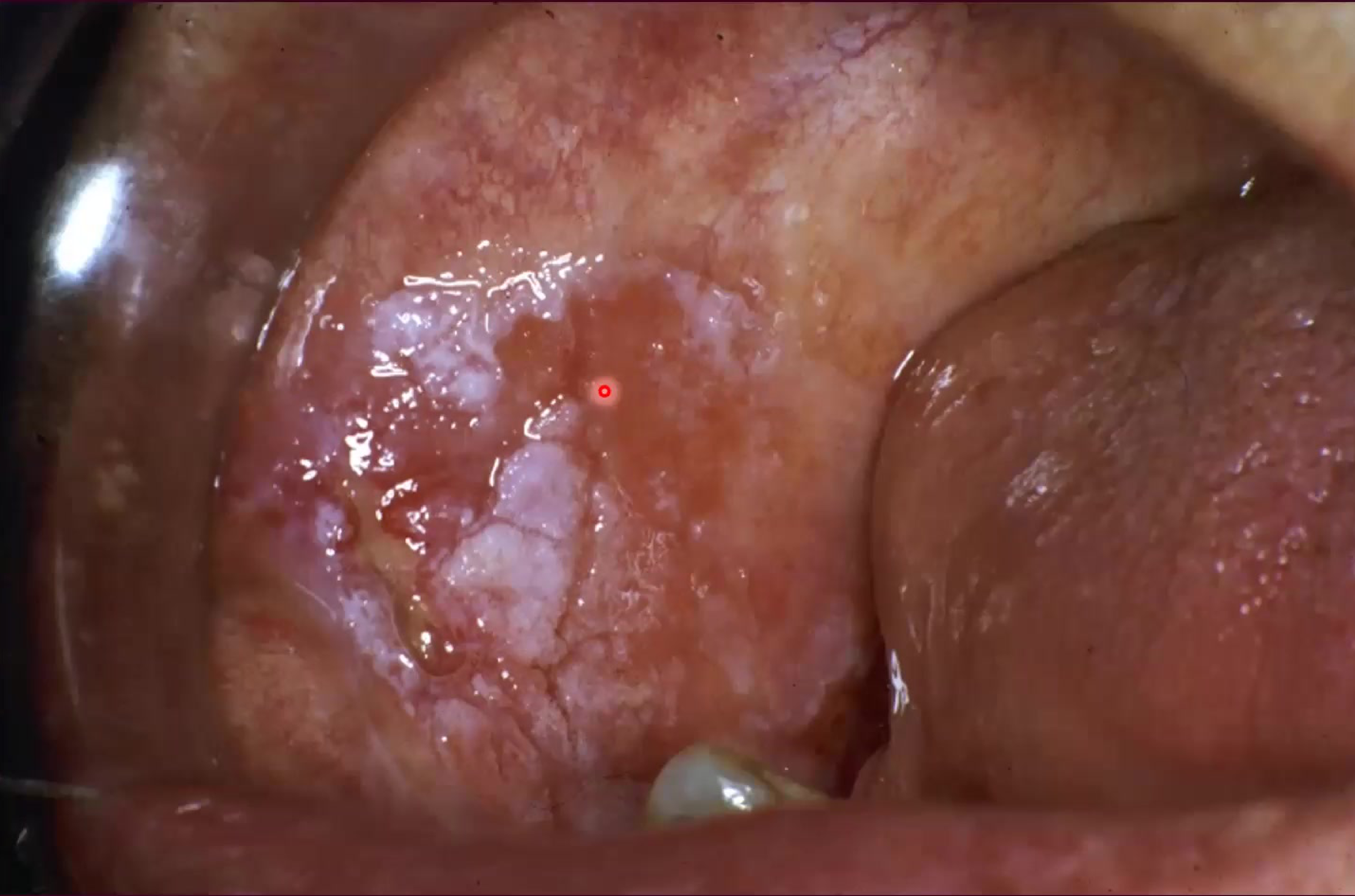
Histological Classification18
- Poorly differentiated squamous cell carcinoma: Characterized by highly atypical cellular features and a lack of normal maturation patterns.
- Also known as anaplastic; these tumors have a much worse prognosis.
| Examples of tumour islands | |
|---|---|
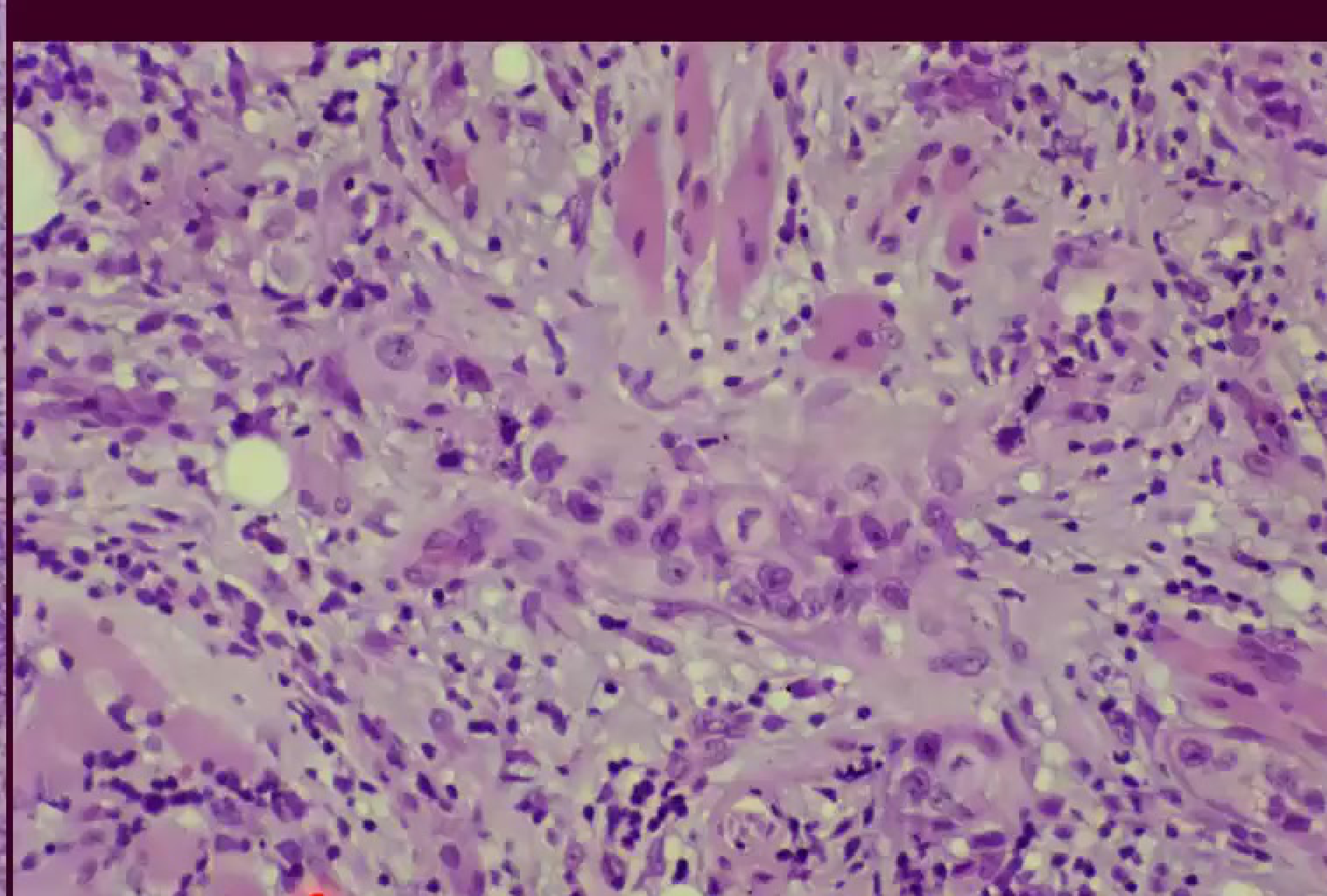 |  |
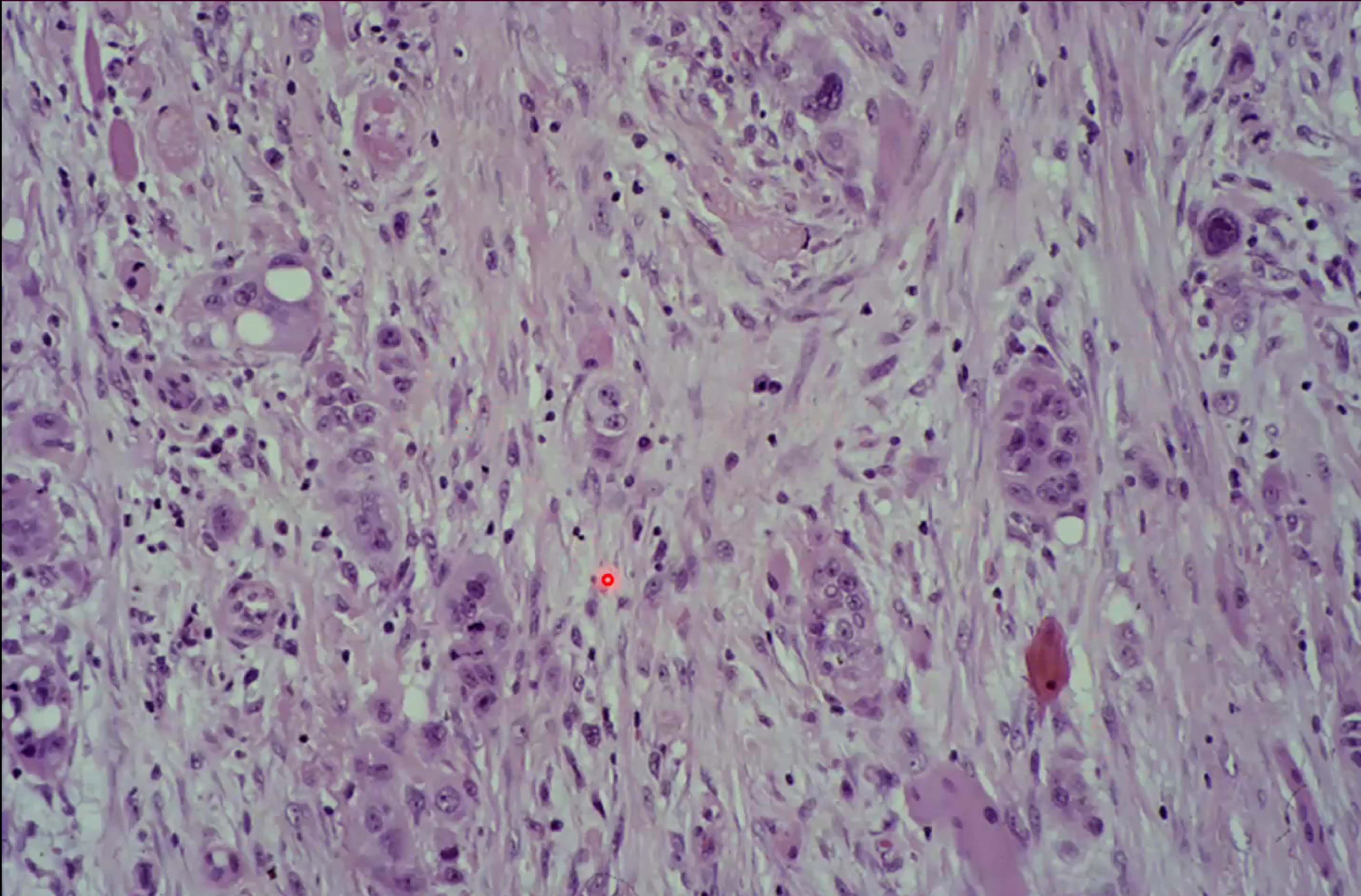
Microscopic Architecture19
- Poorly differentiated SCC: Displays irregular cell morphology and disorganized tissue architecture.
- Invasion: Tumor islands or isolated cells invading the connective tissue and destroying muscle fibers.
Epithelial Dysplasia
Severe Epithelial Dysplasia20
Severe dysplasia is characterized by significant abnormal cell growth and architectural changes within the epithelium.
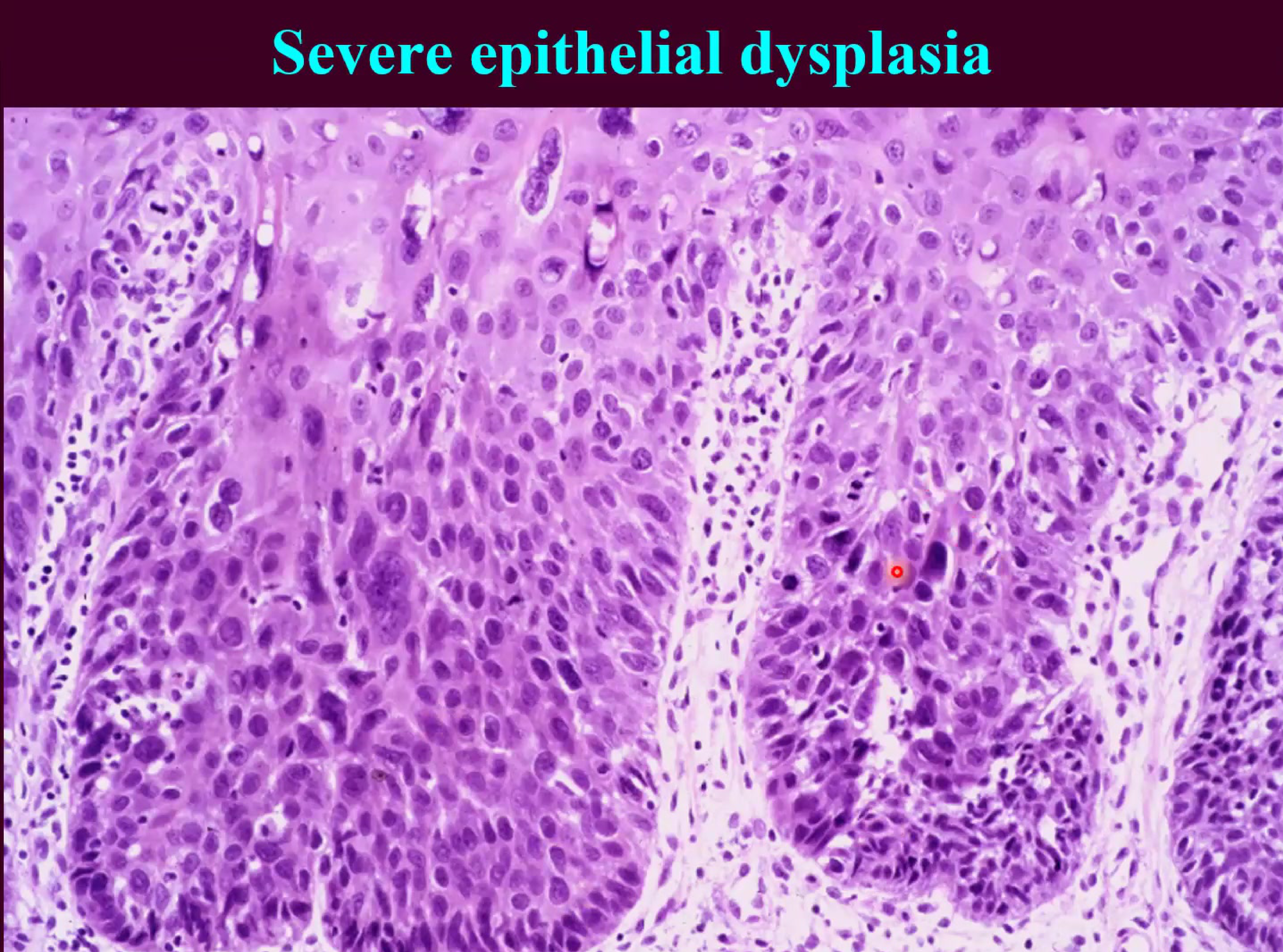
Characteristics of Dysplasia21
Dysplasia involves disturbed differentiation and proliferation, marked by the following features:
- Disordered tissue architecture
- Deep cell keratinisation
- Cell and nuclear pleomorphism (variation in size and shape)
- Nuclear hyperchromatism
- Increased nuclear/cytoplasmic ratio
- Abnormal mitotic figures
Oral Cancer by Anatomical Site
Lip Carcinoma2223
 |  |
Epidemiology and Risk Factors24
- Most commonly affected site.
- Geographical variation often related to UV light exposure.
- Susceptibility factors include race and immunosuppression.
- Incidence in Australia dropped significantly after the 1980s due to the increased use of sunscreen.
Clinical Presentation25
- Typically presents as a non-healing ulcer.
- Characteristically painless.
- Easily overlooked during clinical examination.
- May be preceded by Actinic Cheilitis (blurred vermilion border).
Intraoral Carcinoma
Common Presentations and Sites26272829
- The typical presentation is a painless indurated ulcer.
- The floor of the mouth and the ventral tongue are the most common intraoral sites for carcinoma.
Gingival Presentation
Carcinoma of the gingiva can mimic inflammatory conditions like gingivitis, leading to diagnostic delays.
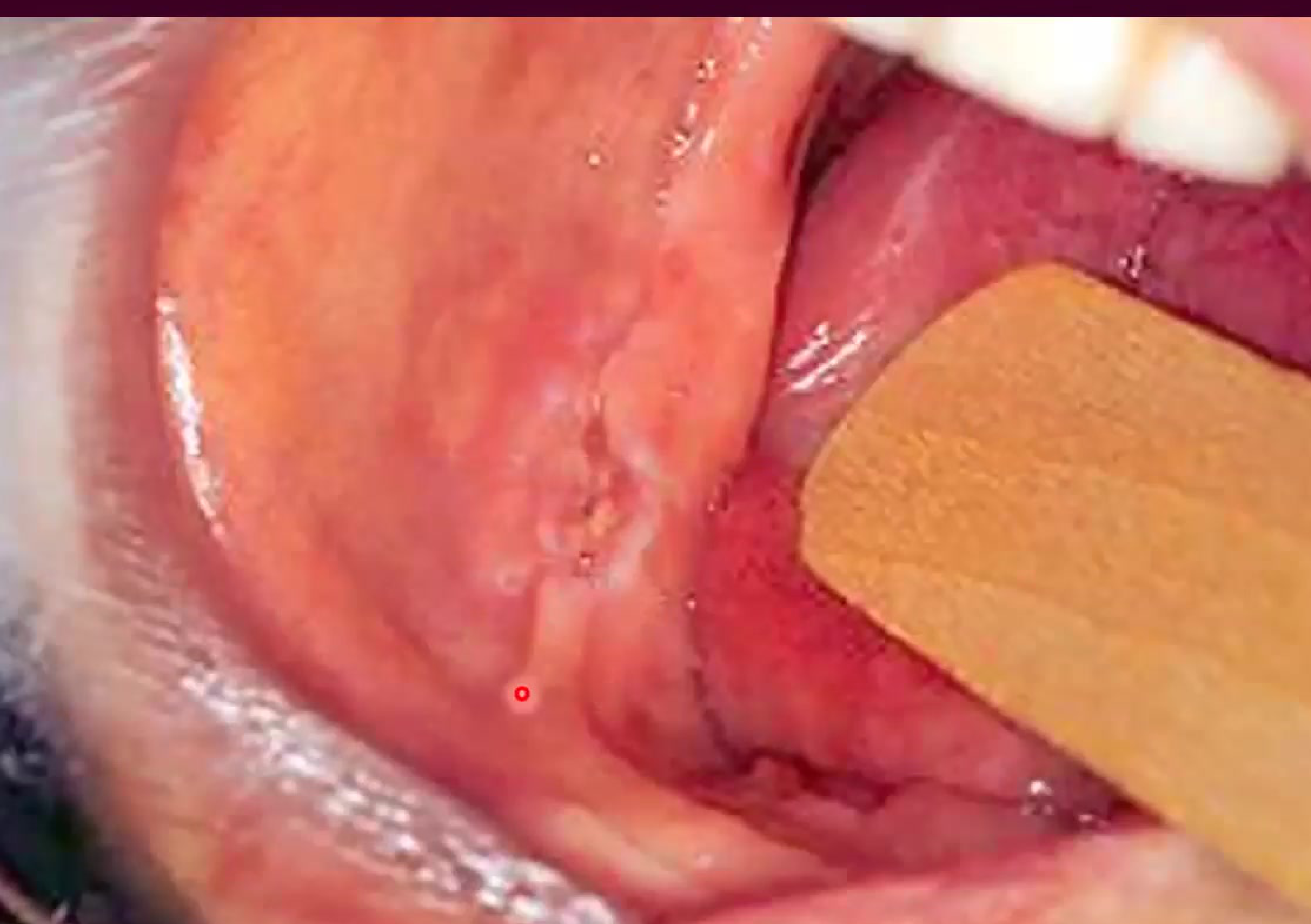
 |  |
 white lesion associated with the tongue white lesion associated with the tongue |
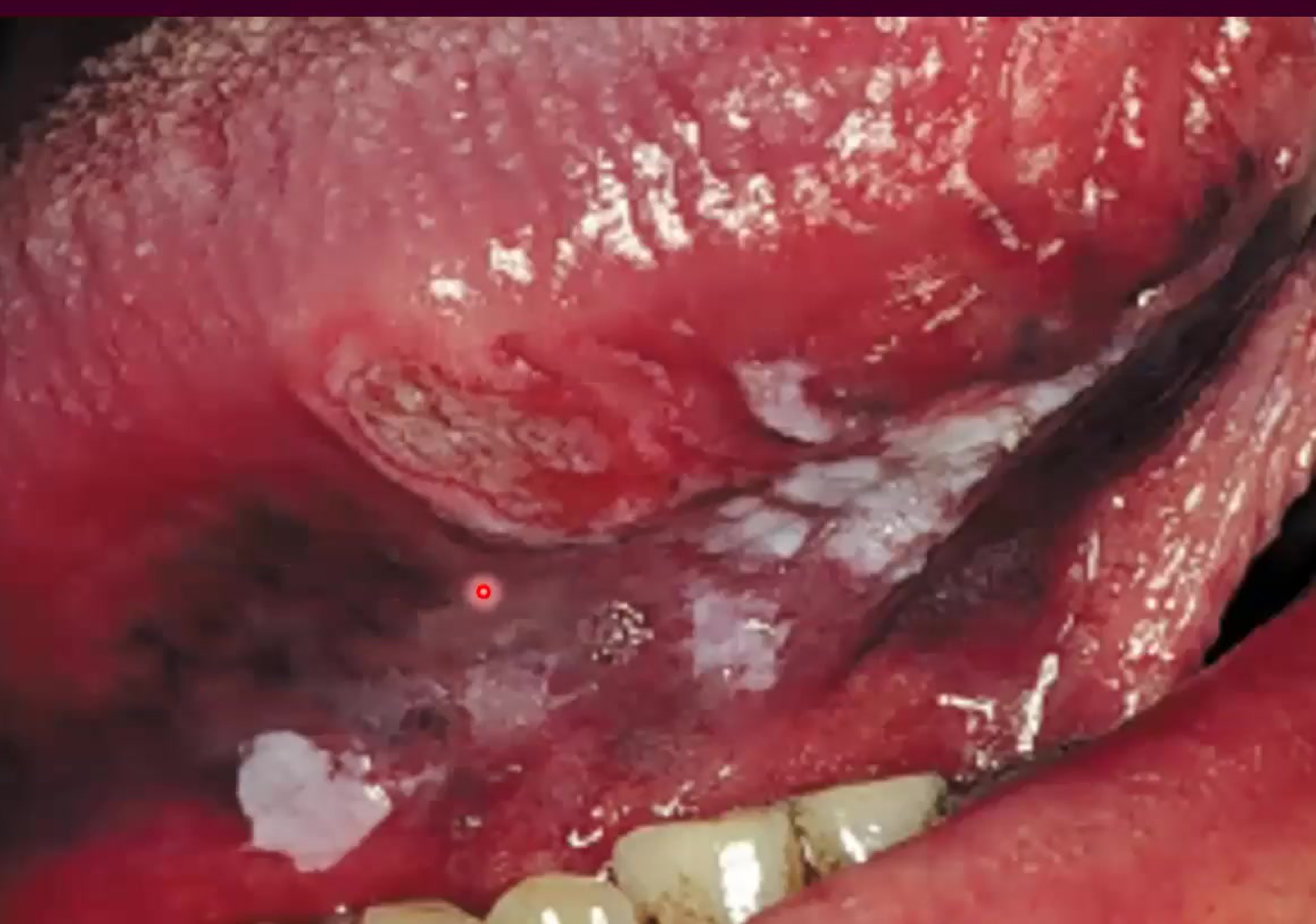
Erythematous Presentation30
- A less common clinical presentation.
- Appears as a red, soft, and raised lesion.
- Often presents as red, soft, velvety patches known as Erythroplakia.
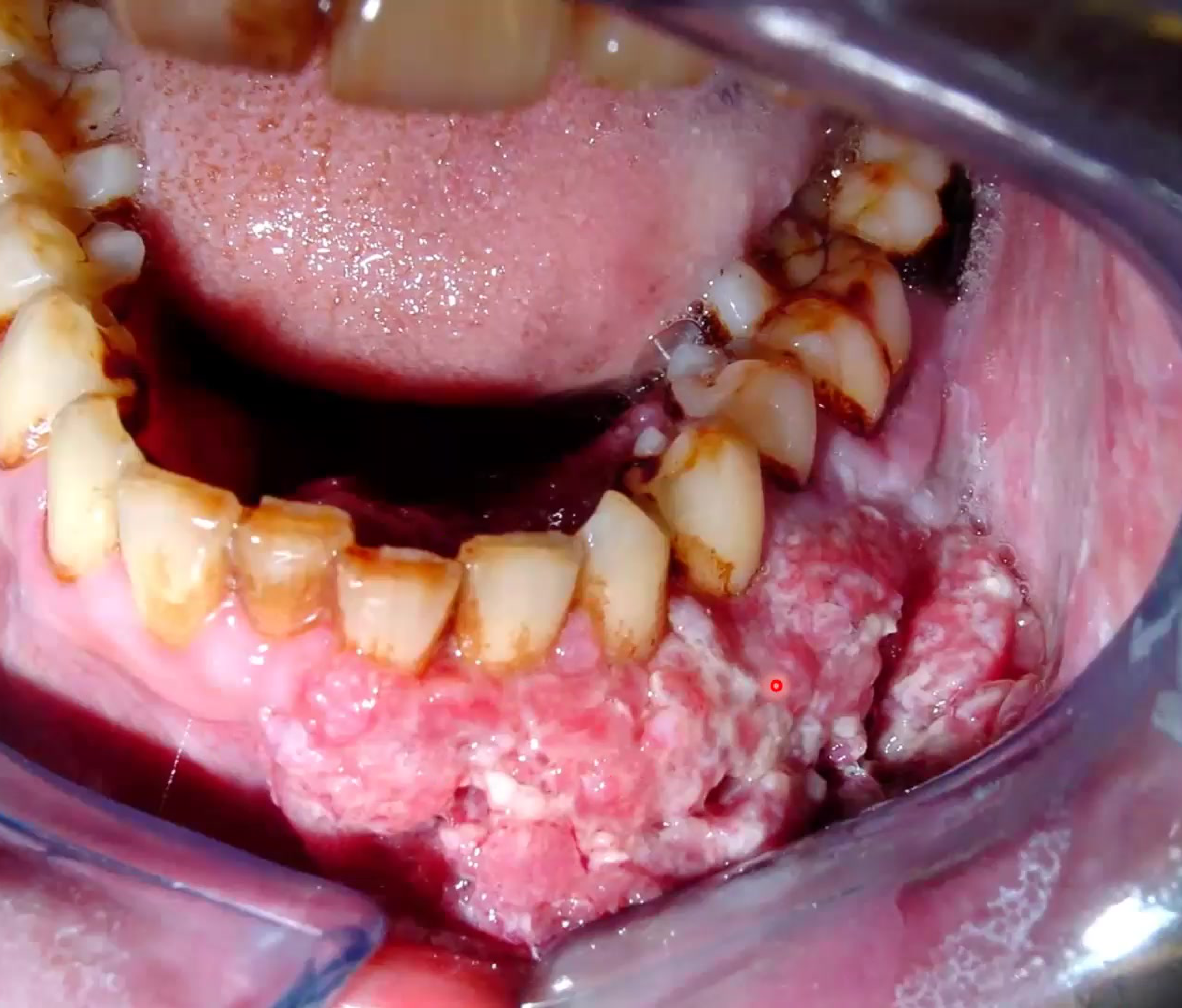
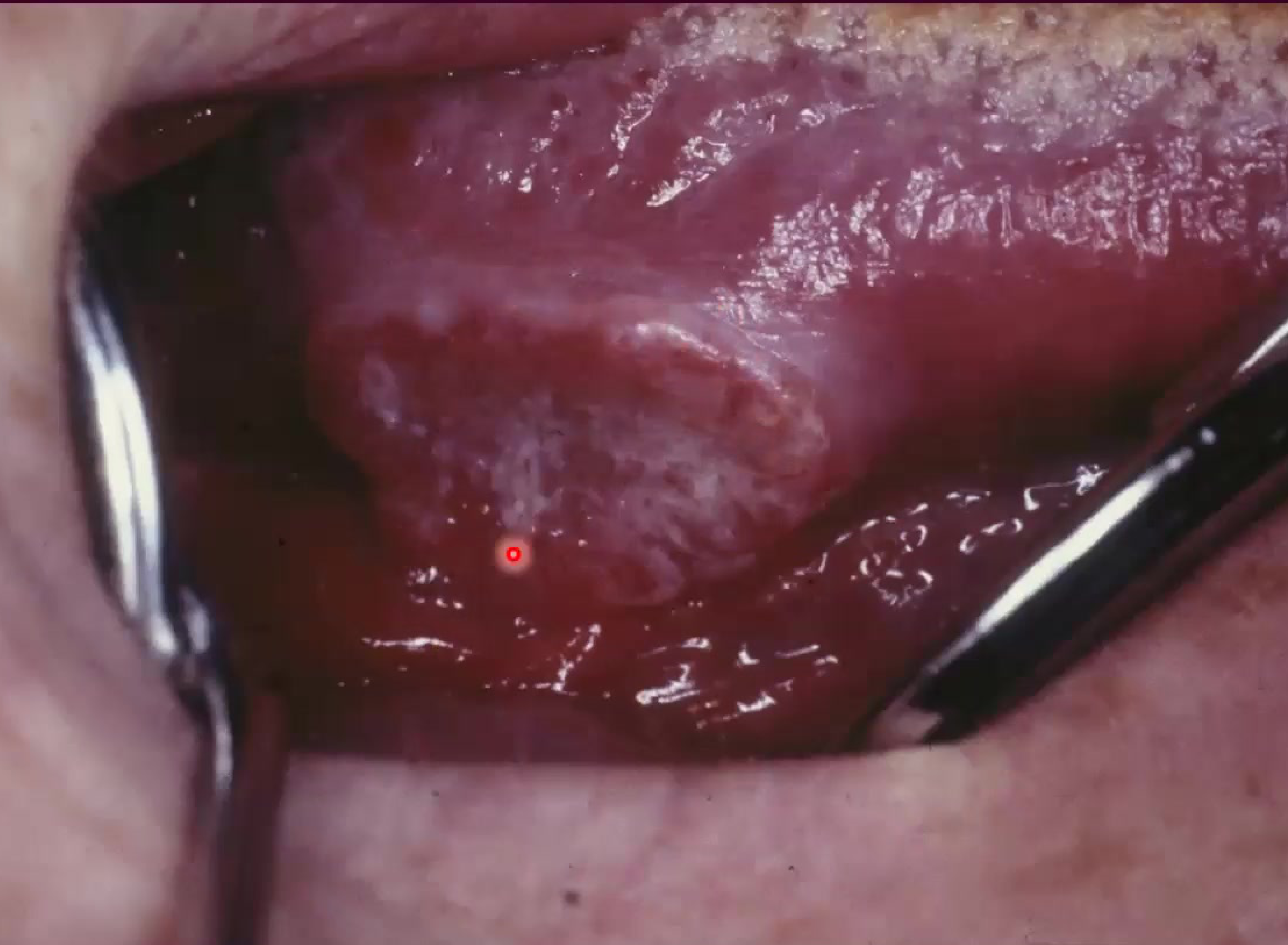
Leukoplakic Presentation31323334
- A less common clinical presentation.
- Appears as an indurated white patch.
 |  |
 |
Oropharyngeal Carcinoma3536373839
 |  |  |
 |  |  clinically looks like gingivitis but its OSCC clinically looks like gingivitis but its OSCC |
Clinical Symptoms and Signs40
- Pain localized to the face and the ear.
- Physical signs may include tongue deviation.
- Tongue deviation indicates nerve involvement.
- May present as a "volcano-like" ulcer in the tonsillar region or buccal mucosa.
Staging and Clinical Evaluation
Standard Clinical Evaluation41
A thorough clinical assessment is essential for the evaluation of oral potentially malignant disorders and the risk of progression. This evaluation includes:
-
Cranial nerve examination
-
Neck palpation
-
Clinical photographs
-
Complete history of the disease
-
Assessment of alcohol and tobacco consumption
-
Monitoring of weight and documentation of any weight loss
TNM Staging Classification4243
The staging process utilizes standardized international systems to ensure accurate classification and communication of findings:
Importance of Staging
Staging is vital for determining the appropriate treatment plan and establishing a prognosis for the patient.
- TNM classification system
- International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3)
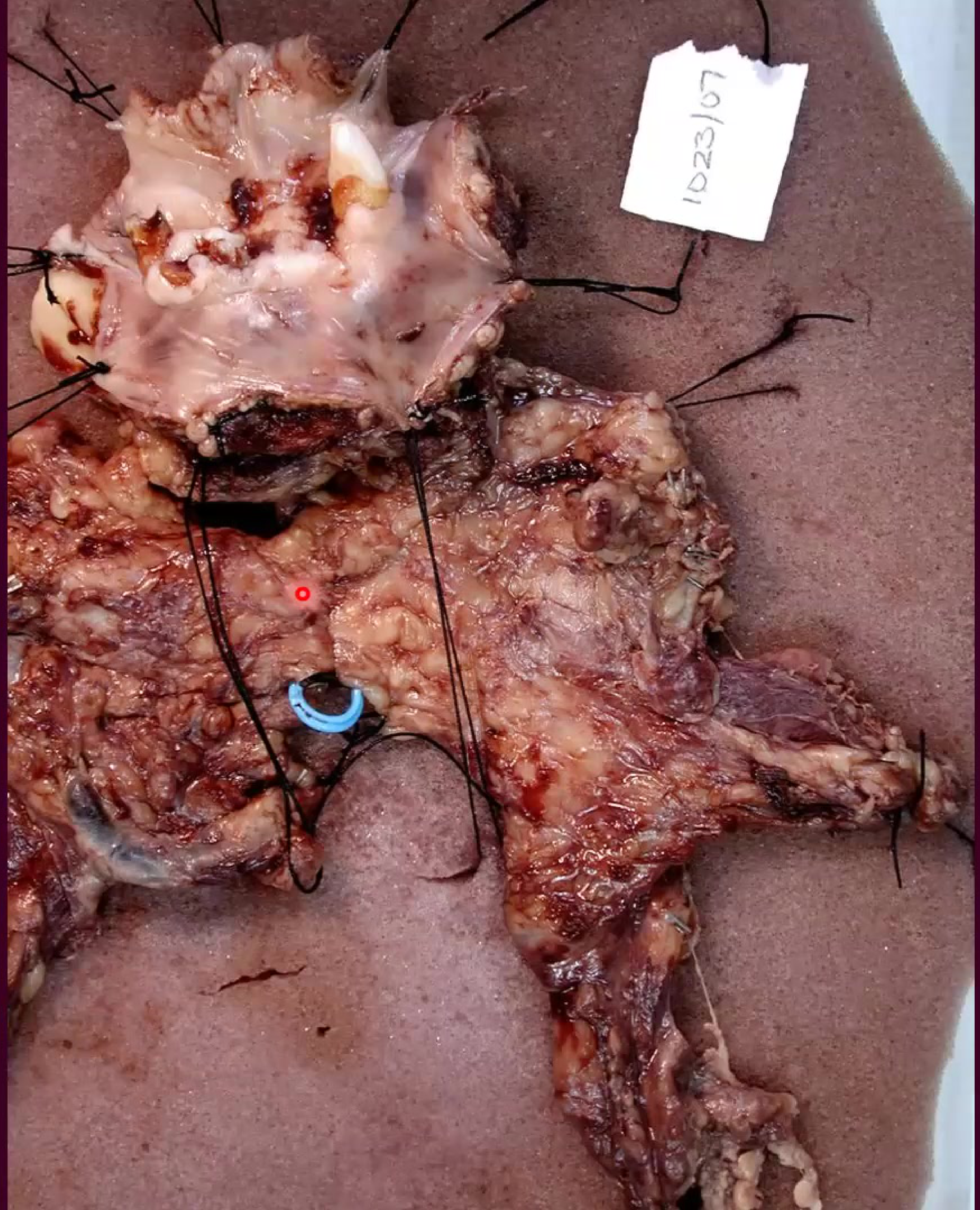
Pathological Specimen Documentation44
Clinical evaluation involves the detailed examination of specimens (e.g., specimen 1023/07). Documentation includes:
- Visual inspection of the specimen with a scale for measurement.
- Identification and marking of specific anatomical features and margins.
 |  |
Primary Tumor (T) Classification45
According to the TNM/AJCC guidelines, the primary tumor is categorized as follows:
- Tis: Carcinoma in situ
- T1: Tumor 2 cm or less in greatest dimension
- T2: Tumor > 2 cm but ≤ 4 cm in greatest dimension
- T3: Tumor > 4 cm in greatest dimension
- T4 (Lip): Tumor invades adjacent structures (through cortical bone, inferior alveolar nerve, floor of mouth, skin of face)
- T4 (Oral Cavity): Tumor invades adjacent structures (through cortical bone, into deep muscle of tongue, maxillary sinus, skin)
Regional Lymph Nodes (N) Classification46
- N0: No regional node metastasis
- Nx: Regional nodes cannot be assessed
- N1: Single ipsilateral node, ≤ 3 cm
- N2a: Single ipsilateral node, > 3 cm and ≤ 6 cm
- N2b: Multiple ipsilateral nodes, ≤ 6 cm
- N2c: Contralateral or bilateral nodes, ≤ 6 cm
- N3: Node > 6 cm
Distant Metastasis (M) Classification47
- Mx: Distant metastasis cannot be assessed
- M0: No distant metastasis
- M1: Distant metastasis
Treatment and Management
Surgical and Radiotherapy Protocols48
Treatment strategies for oral carcinoma are determined by the TNM stage:
-
T1-T2 N0:
- Surgery of the primary tumor (T) only
- Brachytherapy (indicated if T < 3cm, no ulceration, no infiltration, and located on dry vermilion)
-
T3-T4 N0:
- Surgery of the primary tumor (T) + Supraomohyoid Neck Dissection (SOH ND) ± post-operative Radiotherapy
-
T1-T4 N1:
- Surgery of the primary tumor (T) + SOH or radical modified Neck Dissection ± post-operative Radiotherapy
-
T1-T4 N2a-N3:
- Surgery of the primary tumor (T) + radical modified Neck Dissection ± post-operative treatment
-
Advanced Stage treatment may also involve chemotherapy and, increasingly, immunotherapy.
Follow-up and Surveillance
Clinical and Mucosal Surveillance49
- Clinical examination of head and neck mucosa (including fiberoptic) and neck palpation, performance status, and nutritional assessment:
- Every 2 months for the first 2 years
- Every 6 months for years 3 to 5
- Once a year after 5 years
- Dental and Imaging:
- Dental examination and orthopantomogram every 6 months
- Chest X-ray every year
- Chest spiral CT every year
- Laboratory Tests:
- TSH levels every year (required if Radiotherapy was delivered)
Prognosis and Prevention
Survival Rates and Field Cancerization
Five-Year Survival Rates50
Survival outcomes for oral cancer are highly dependent on the stage at diagnosis:
- Stage I: > 80%
- Stage II: ~60%
- Stage III: ~35%
- Stage IV: < 15%
Second Primary Head and Neck Cancer51
- Second primary cancers of the aerodigestive pathway occur synchronously or metachronously in 20% of patients with an index cancer of the head and neck.
- This phenomenon is associated with the concept of “field cancerization.”
Field Cancerization
This occurs because the entire mucosal lining is "primed" for cancer due to chronic exposure to carcinogens like smoking and alcohol, making the whole area susceptible to multiple primary tumors.
Post-Treatment Care52
Post-treatment care focuses on rehabilitation and early detection of recurrence:
- Speech and Swallowing Therapy
- Dietitians for nutritional support
- Dentists for oral rehabilitation
- Routine follow-up tests
- Chemoprevention strategies
- Vigilance for new symptoms
- Management of general health considerations
Prevention Strategies in Primary Care53
Primary care providers play a critical role in the early detection and prevention of head and neck cancer through the following actions:
- Identify patients who use tobacco and alcohol products.
- Counsel patients to stop using tobacco and alcohol products.
- Maintain a high index of suspicion.
- Conduct comprehensive examinations.
- Dentists are the first line of defense in detecting early mucosal changes.
- Attend to common symptoms.
- Evaluate symptomatic patients.
- Maintain close medical surveillance of patients in high-risk occupations.
- Refer high-risk patients with persistent symptoms and no findings to a head and neck surgeon.
Factors Delaying Diagnosis54
Several factors can lead to a delay in the diagnosis of head and neck cancers:
- Patient procrastination in seeking medical attention
- Often due to the lesion being painless in early stages
- Physician delay in diagnosis
- Clinicians may misdiagnose a malignancy as a simple infection or trauma
- The patient remaining asymptomatic for a prolonged period
Clinical Guidelines for White Lesions
- Idiopathic White Patches (Leukoplakia):
- May present as keratosis with or without dysplasia.
- Clinical presentations: Homogeneous, nodular, verrucous, or speckled.
- Specific types/sites: Sublingual keratosis, actinic keratosis, and proliferative verrucous leukoplakia.
- Presumed aetiology often includes smoking or actinic damage.
- Differential diagnosis must include squamous cell carcinoma.
- Biopsy Protocol: In principle, every white patch in the mouth should have a biopsy sample removed for definitive diagnosis.
Footnotes
-
Original PDF page 1: L12 OPMD Oral cancer Part III slides, p.1 ↩
-
Original PDF page 2: L12 OPMD Oral cancer Part III slides, p.2 ↩
-
Original PDF page 4: L12 OPMD Oral cancer Part III slides, p.4 ↩
-
Original PDF page 5: L12 OPMD Oral cancer Part III slides, p.5 ↩
-
Original PDF page 6: L12 OPMD Oral cancer Part III slides, p.6 ↩
-
Original PDF page 3: L12 OPMD Oral cancer Part III slides, p.3 ↩
-
Original PDF page 7: L12 OPMD Oral cancer Part III slides, p.7 ↩
-
Original PDF page 8: L12 OPMD Oral cancer Part III slides, p.8 ↩
-
Original PDF page 9: L12 OPMD Oral cancer Part III slides, p.9 ↩
-
Original PDF page 10: L12 OPMD Oral cancer Part III slides, p.10 ↩
-
Original PDF page 12: L12 OPMD Oral cancer Part III slides, p.12 ↩
-
Original PDF page 13: L12 OPMD Oral cancer Part III slides, p.13 ↩
-
Original PDF page 14: L12 OPMD Oral cancer Part III slides, p.14 ↩
-
Original PDF page 20: L12 OPMD Oral cancer Part III slides, p.20 ↩
-
Original PDF page 15: L12 OPMD Oral cancer Part III slides, p.15 ↩
-
Original PDF page 16: L12 OPMD Oral cancer Part III slides, p.16 ↩
-
Original PDF page 17: L12 OPMD Oral cancer Part III slides, p.17 ↩
-
Original PDF page 18: L12 OPMD Oral cancer Part III slides, p.18 ↩
-
Original PDF page 19: L12 OPMD Oral cancer Part III slides, p.19 ↩
-
Original PDF page 21: L12 OPMD Oral cancer Part III slides, p.21 ↩
-
Original PDF page 22: L12 OPMD Oral cancer Part III slides, p.22 ↩
-
Original PDF page 25: L12 OPMD Oral cancer Part III slides, p.25 ↩
-
Original PDF page 26: L12 OPMD Oral cancer Part III slides, p.26 ↩
-
Original PDF page 23: L12 OPMD Oral cancer Part III slides, p.23 ↩
-
Original PDF page 24: L12 OPMD Oral cancer Part III slides, p.24 ↩
-
Original PDF page 27: L12 OPMD Oral cancer Part III slides, p.27 ↩
-
Original PDF page 28: L12 OPMD Oral cancer Part III slides, p.28 ↩
-
Original PDF page 29: L12 OPMD Oral cancer Part III slides, p.29 ↩
-
Original PDF page 30: L12 OPMD Oral cancer Part III slides, p.30 ↩
-
Original PDF page 31: L12 OPMD Oral cancer Part III slides, p.31 ↩
-
Original PDF page 32: L12 OPMD Oral cancer Part III slides, p.32 ↩
-
Original PDF page 33: L12 OPMD Oral cancer Part III slides, p.33 ↩
-
Original PDF page 34: L12 OPMD Oral cancer Part III slides, p.34 ↩
-
Original PDF page 35: L12 OPMD Oral cancer Part III slides, p.35 ↩
-
Original PDF page 37: L12 OPMD Oral cancer Part III slides, p.37 ↩
-
Original PDF page 38: L12 OPMD Oral cancer Part III slides, p.38 ↩
-
Original PDF page 39: L12 OPMD Oral cancer Part III slides, p.39 ↩
-
Original PDF page 40: L12 OPMD Oral cancer Part III slides, p.40 ↩
-
Original PDF page 41: L12 OPMD Oral cancer Part III slides, p.41 ↩
-
Original PDF page 36: L12 OPMD Oral cancer Part III slides, p.36 ↩
-
Original PDF page 42: L12 OPMD Oral cancer Part III slides, p.42 ↩
-
Original PDF page 43: L12 OPMD Oral cancer Part III slides, p.43 ↩
-
Original PDF page 47: L12 OPMD Oral cancer Part III slides, p.47 ↩
-
Original PDF page 44: L12 OPMD Oral cancer Part III slides, p.44 ↩
-
Original PDF page 45: L12 OPMD Oral cancer Part III slides, p.45 ↩
-
Original PDF page 46: L12 OPMD Oral cancer Part III slides, p.46 ↩
-
Original PDF page 48: L12 OPMD Oral cancer Part III slides, p.48 ↩
-
Original PDF page 49: L12 OPMD Oral cancer Part III slides, p.49 ↩
-
Original PDF page 50: L12 OPMD Oral cancer Part III slides, p.50 ↩
-
Original PDF page 51: L12 OPMD Oral cancer Part III slides, p.51 ↩
-
Original PDF page 52: L12 OPMD Oral cancer Part III slides, p.52 ↩
-
Original PDF page 53: L12 OPMD Oral cancer Part III slides, p.53 ↩
-
Original PDF page 54: L12 OPMD Oral cancer Part III slides, p.54 ↩
-
Original PDF page 55: L12 OPMD Oral cancer Part III slides, p.55 ↩