Dental Management of Oral Cancer Patients
Presentation Overview1
Presented by Dr. Agnieszka Frydrych, this document outlines the clinical protocols and considerations for the dental management of patients diagnosed with oral cancer.
Scope of Management
This lecture covers the specific dental protocols required before, during, and after radiation therapy to prevent debilitating complications and preserve quality of life.
Introduction and Clinical Significance2
Dental care forms an integral part of the multidisciplinary management of oral and oropharyngeal cancer patients and it significantly contributes to the preservation of life quality.
- Oral cancers are particularly devastating because they affect basic bodily functions—speaking, eating, and breathing—and can be profoundly disfiguring.
Epidemiology of Oral and Oropharyngeal Cancer
Australian Statistics34
In Australia, about 3,000 new cases of oral and oropharyngeal cancer are reported annually, representing approximately 2.5% of all cancer diagnoses.
Public Awareness
A West Australian study revealed that one-third of surveyed individuals had never heard of the condition, and less than 10% could correctly identify smoking and alcohol as primary risk factors.
 |  |
Psychosocial Impact5
Oral and oropharyngeal cancers have severe adverse impacts on quality of life, which is reflected in high suicide rates among this patient population.
- U.S. studies indicate that oral cancer patients are up to eight times more likely to commit suicide during the first year after diagnosis compared to the general population.
Histopathology6
Over 90% of cancers of the oral cavity and the oropharynx are Squamous Cell Carcinoma (SCC).
- While these share a common name, they are biologically diverse and require individualized treatment plans.

Demographic Trends789
The incidence of oral squamous cell carcinoma is increasing among young patients.
- Traditionally, SCC affects males in their 60s and 70s with histories of smoking and alcohol use.
- Younger patients pose unique challenges because they must manage treatment complications for many decades if they survive.
Young Patient Cases
- ==Rebecca (20): Large tongue cancer.==
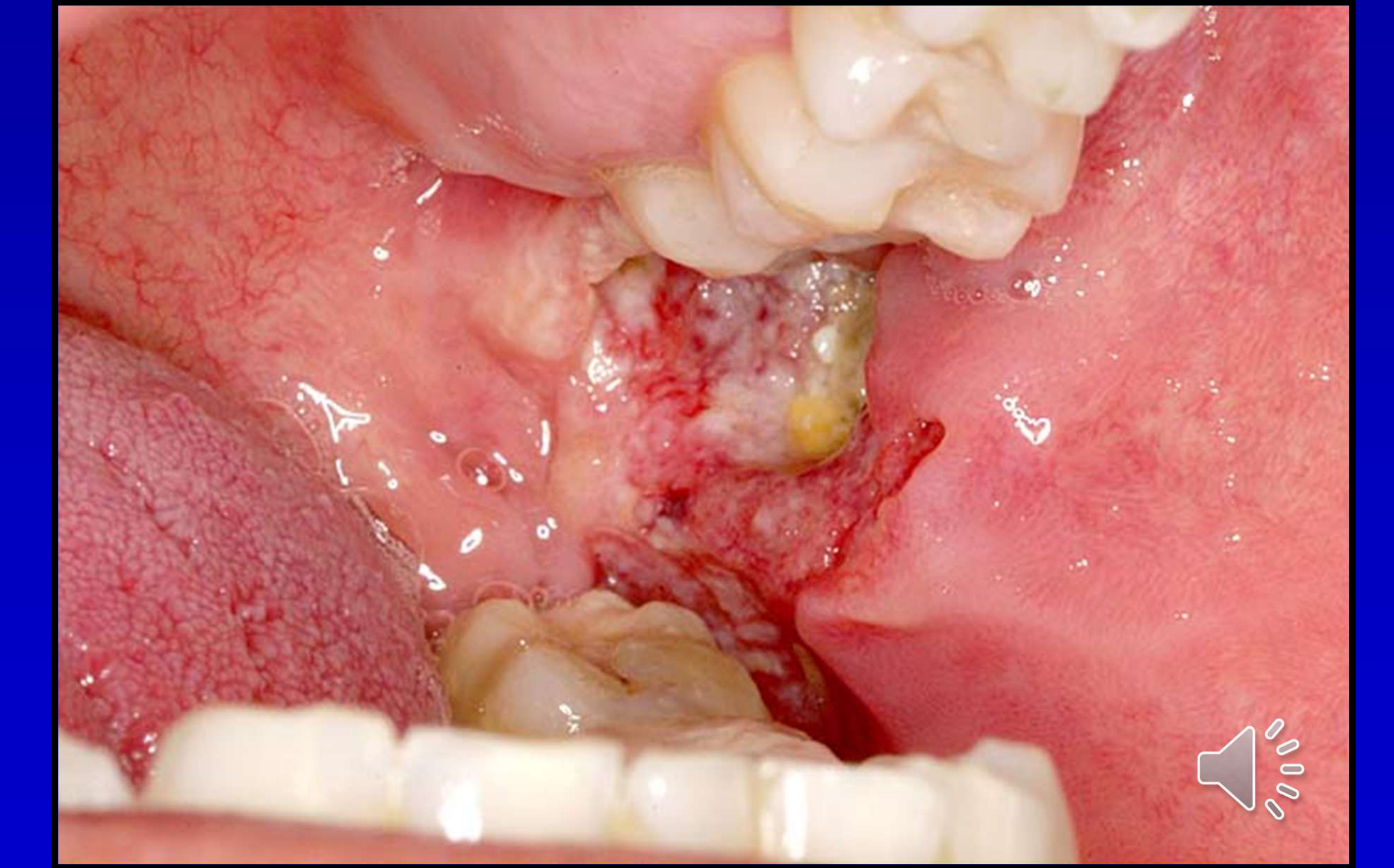
- ==Michael (36): Floor of mouth SCC.==
- ==Monika (28): Palatal SCC.==
| Rebecca (20) Large tongue cancer | Micheal 36: floor of mouth SCC |
|---|---|
 |  |
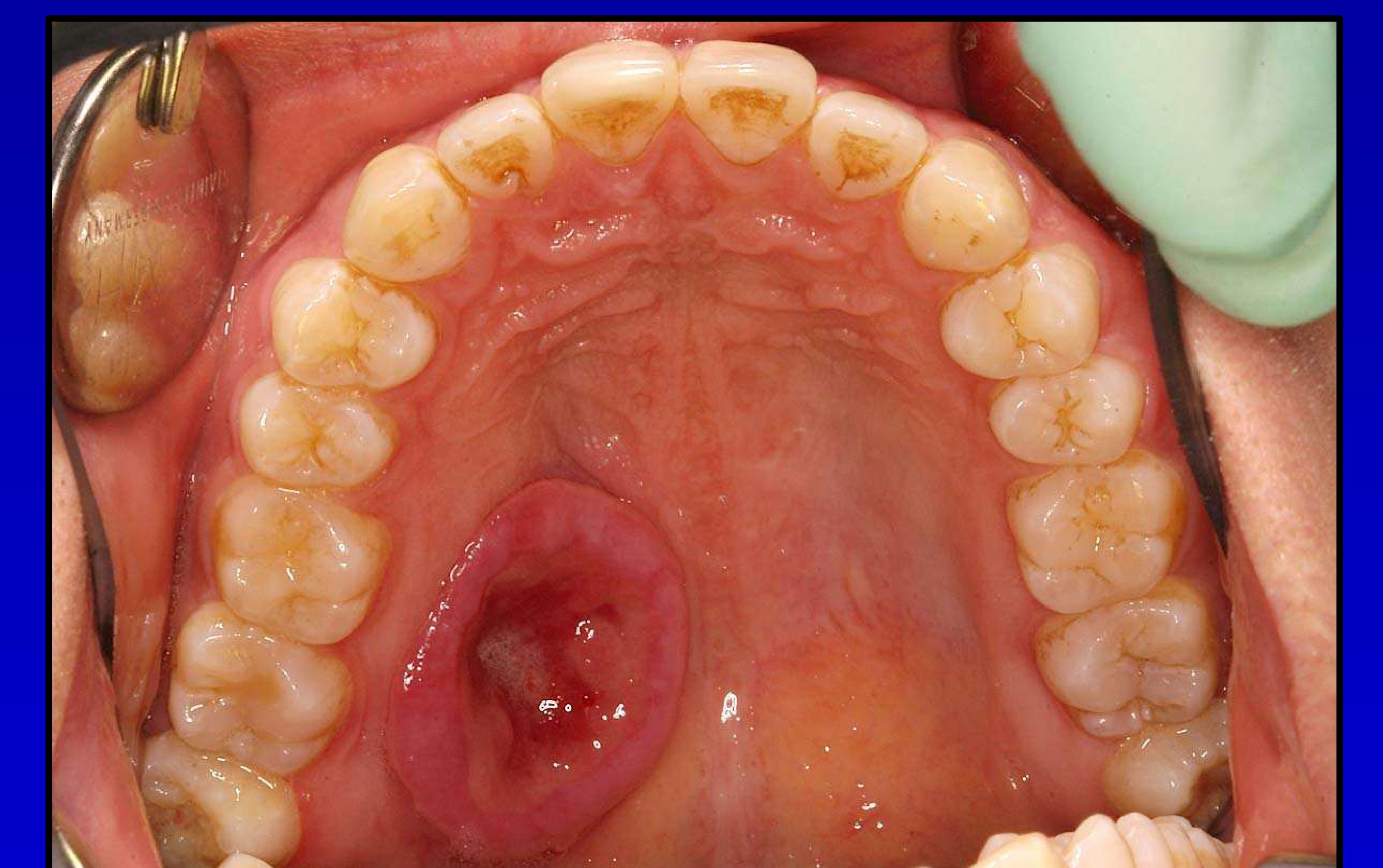 | |
| Monika 29 palatal oscc |
Treatment Modalities for Oral Cancer1011
Clinical presentation of oral cavity pathology, including visible redness and swelling on the tongue.
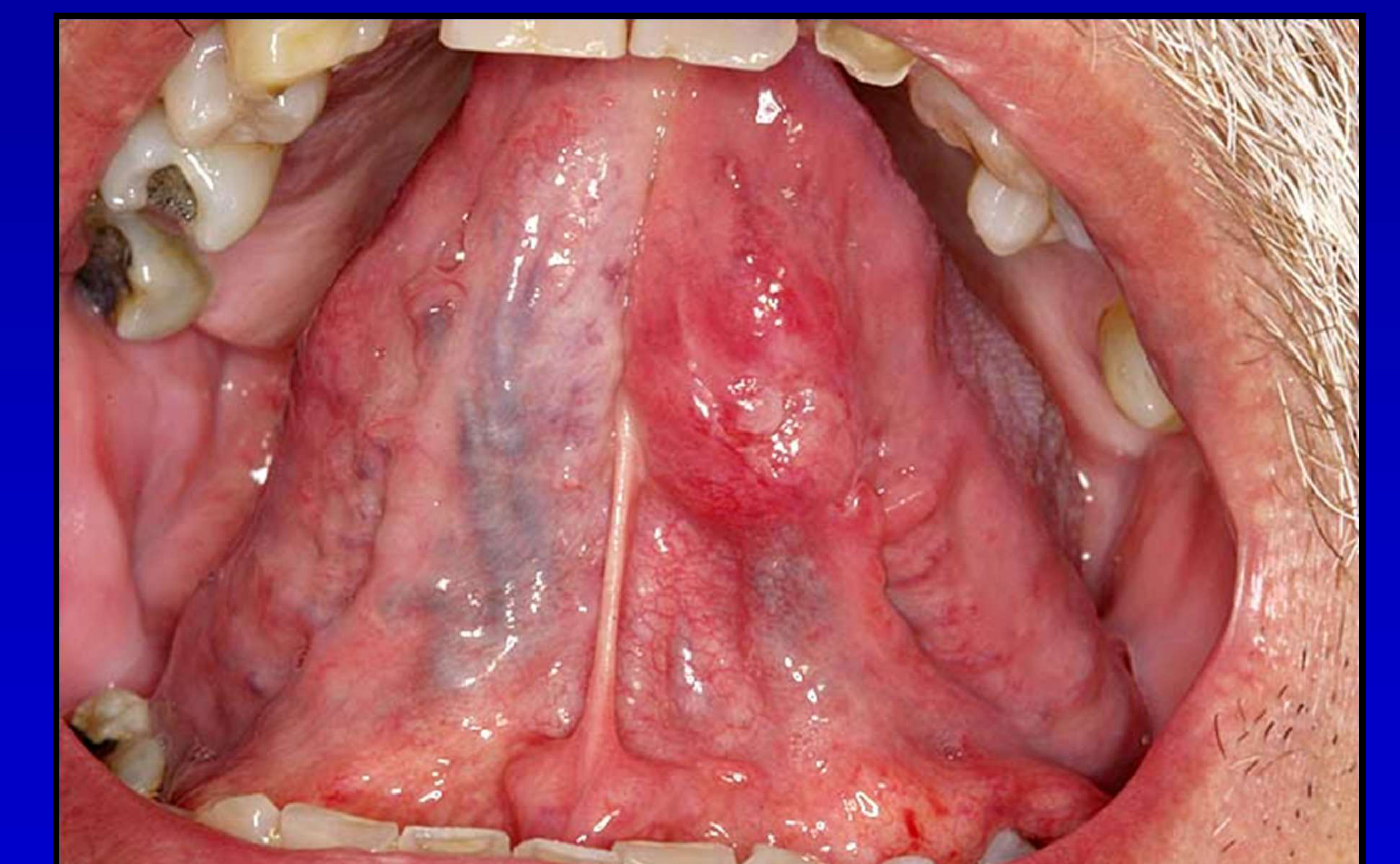 |  |
 |
Therapeutic Approaches12
- Surgery
- Radiation therapy
- Surgery + radiation therapy
- Radiation + chemotherapy
- Surgery + radiation + chemotherapy
- Early Stage: Surgery or radiation therapy as a single modality (surgery is the gold standard).
- Advanced Stage: Multimodality approach (surgery, radiation, and/or chemotherapy).
- No treatment (palliation)
Surgical Intervention13
Content related to surgical management of oral cancer.
- Surgery involves removing the primary tumor and often the regional lymph nodes in the neck.
Additional considerations regarding surgical procedures.
Case Study: Monika (28-year-old PhD Student)
Monika underwent extensive palatal resection for an SCC. This case illustrates the significant impact of surgery on cosmesis and function (speech and swallowing), particularly in young individuals.

Adverse Effects of Radiation Therapy
Radiation Dosage and Administration14
- Doses required to kill malignant cells range from 50-70Gy (High dose)
- Radiation is fractionated into daily doses of approximately 2Gy
- Delivered Monday to Friday, usually over a 6-7 week period
Acute Mucosal and Skin Reactions
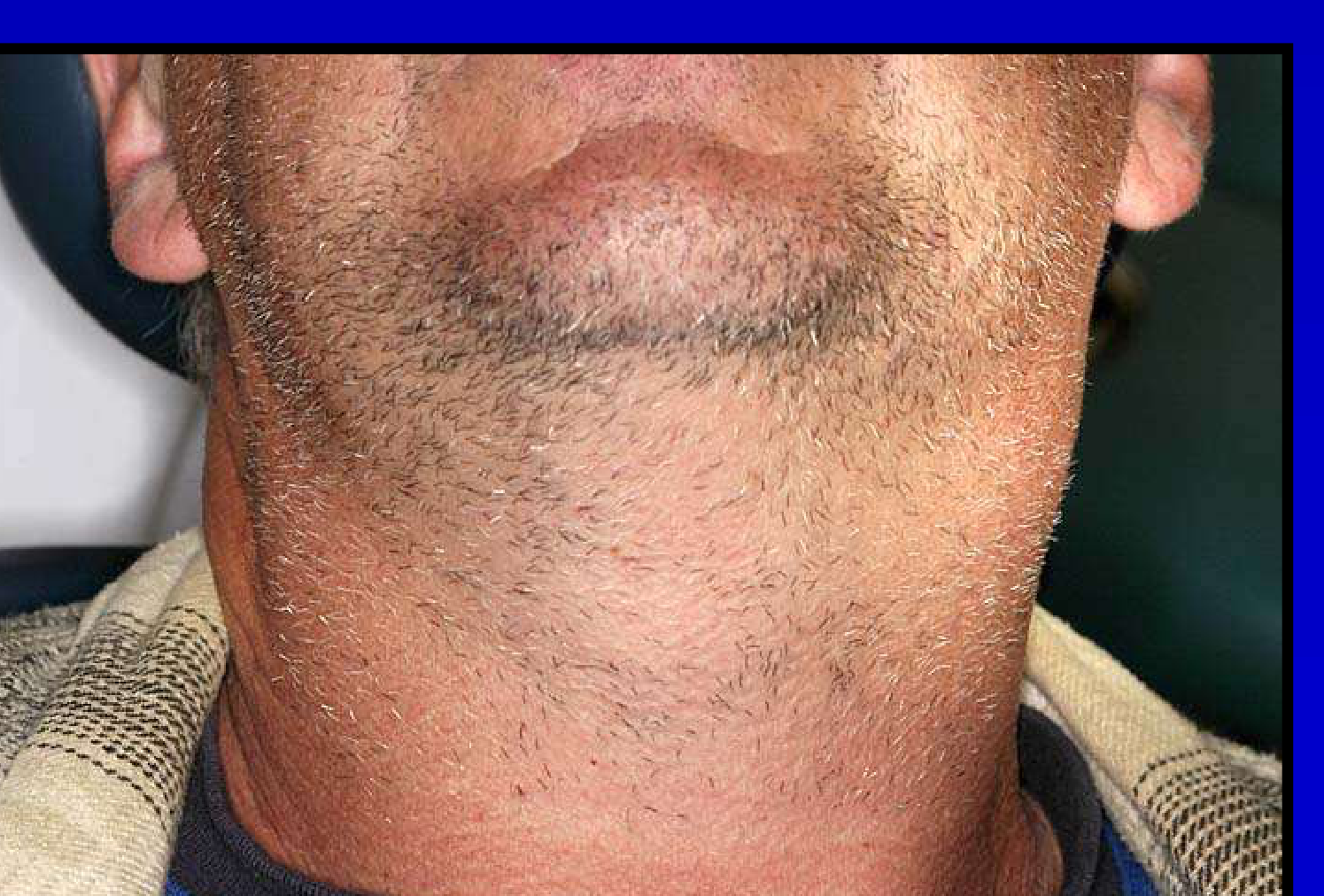
Dermatological Impact15
- Radiation dermatitis
- Resembles a severe sunburn and is precisely delineated to the treatment field
- Hair loss becomes permanent at doses exceeding 50 Gy
 |  |
Mucosal Impact16
- Radiation mucositis

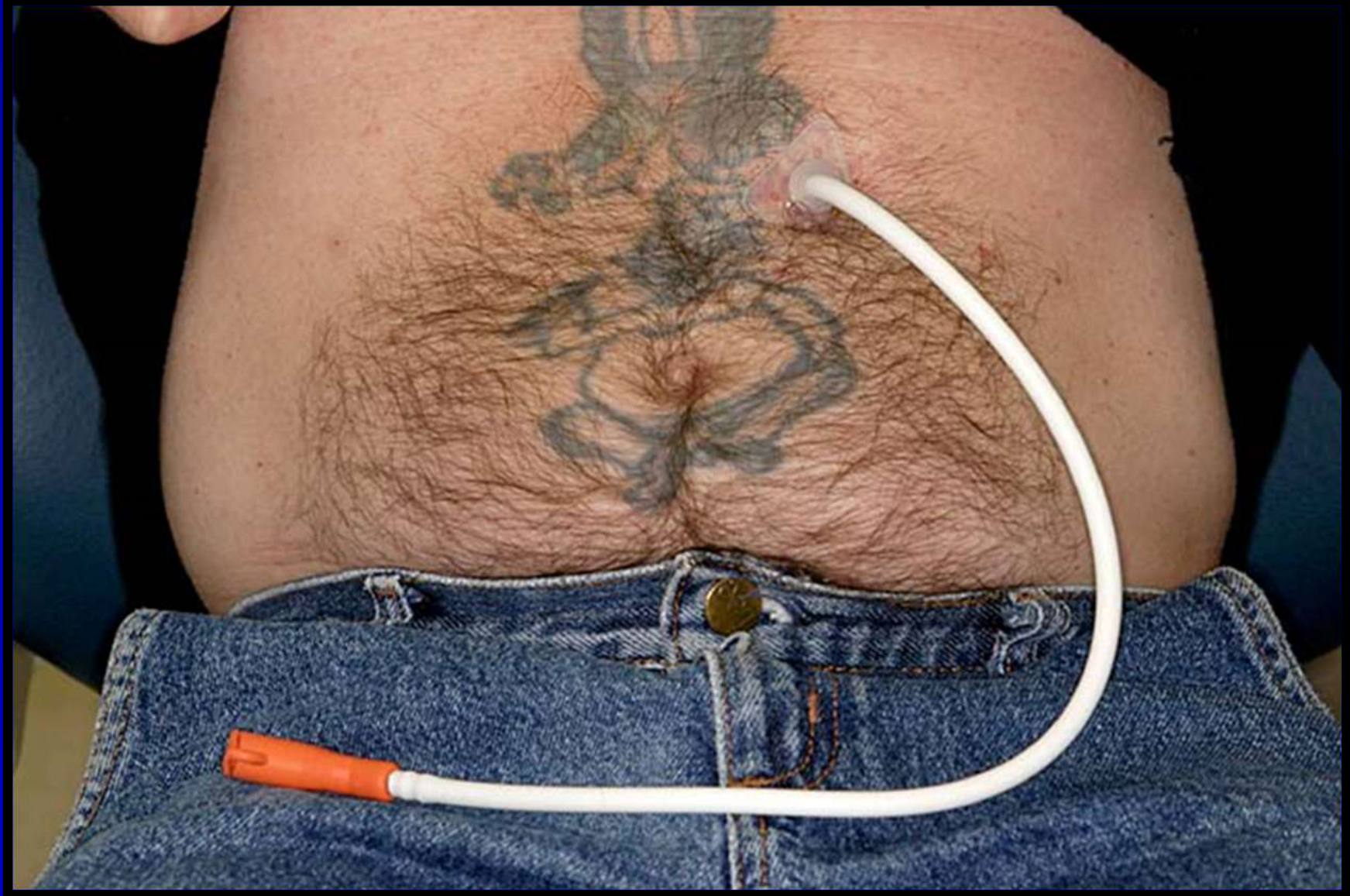
Clinical Manifestations of Mucositis17
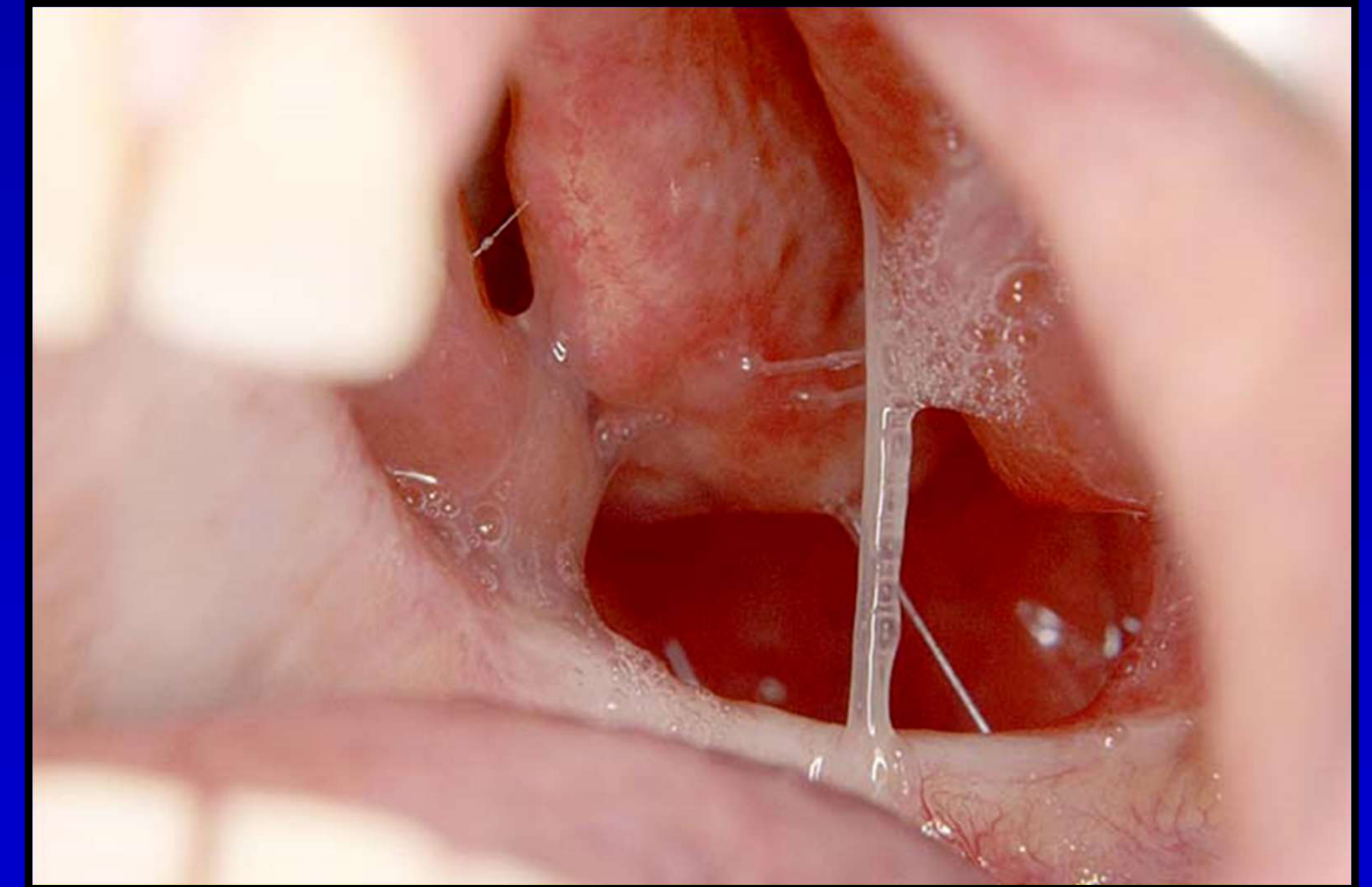
- Radiation mucositis presenting as inflamed oral mucosa
- Often requires opioids for pain management
- Can lead to the use of PEG (feeding) tubes if the patient cannot eat
- Clinical observation of radiation therapy catheter insertion sites
 |  |
Salivary Gland Dysfunction and Xerostomia
Glandular Impact18
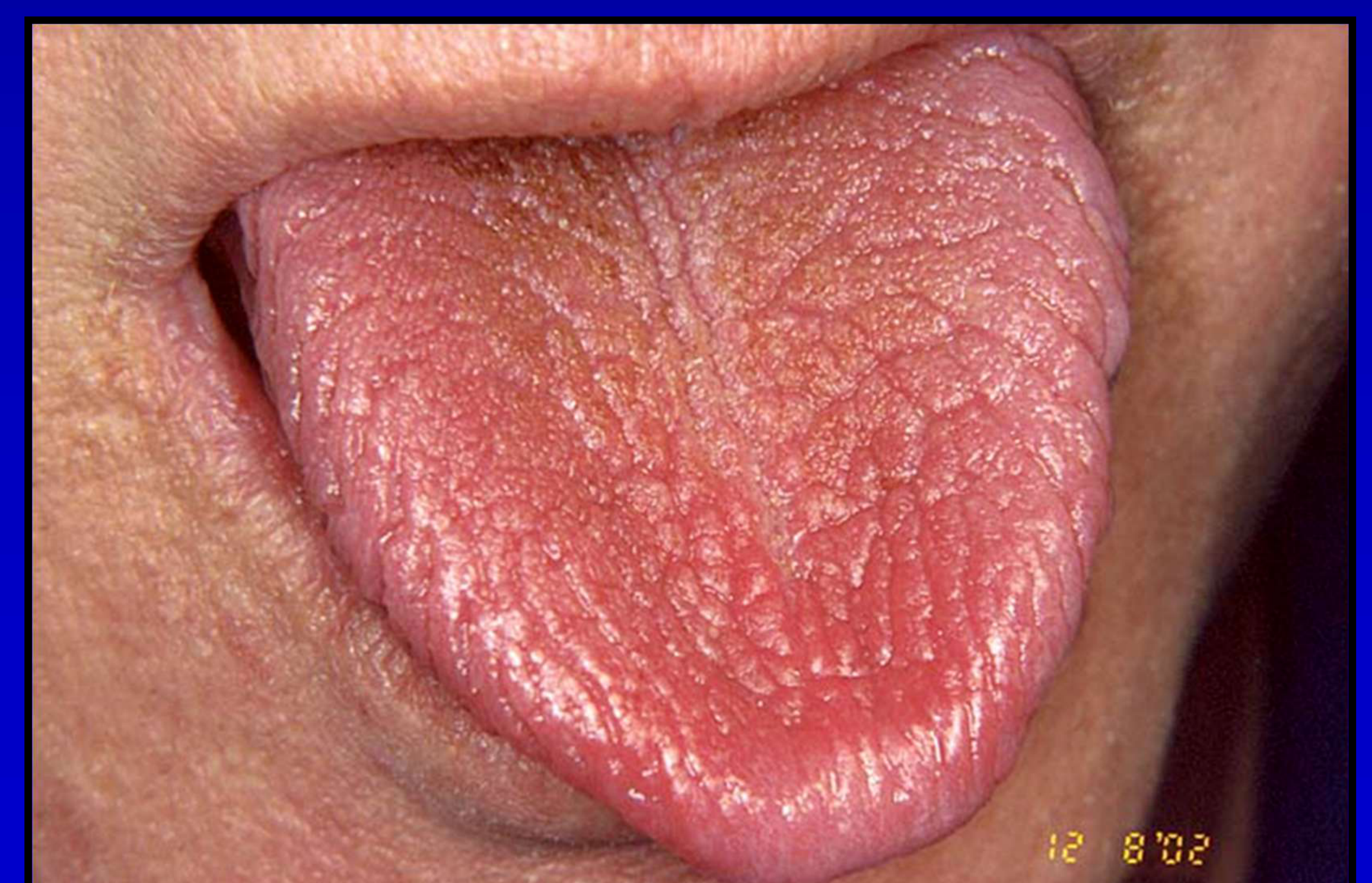
- Salivary gland dysfunction
- Glands are highly sensitive; doses over 30 Gy cause permanent dysfunction
- Saliva becomes thick and ropey before disappearing completely
Sensory and Secretory Changes19
- Xerostomia
- Loss of taste
- Known as dysgeusia; caused by direct damage to taste buds and lack of saliva to dissolve flavor chemicals
Radiation Induced Dental Caries
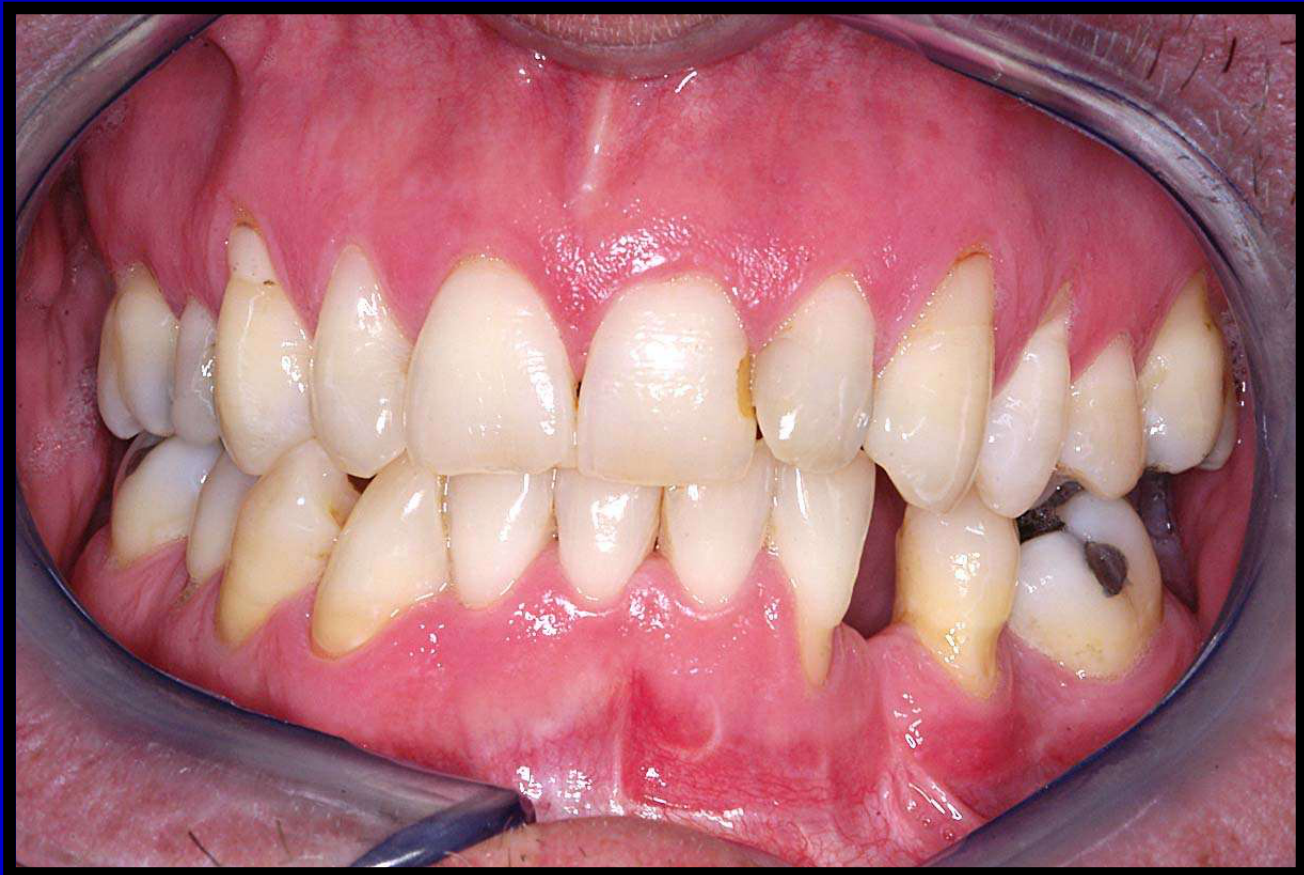
Radiation-Related Decay20
- Dental caries clinical presentations following radiation therapy
- Radiation caries are entirely preventable with proper education and compliance
- Occur secondary to the loss of the protective properties of saliva
 |  |
 |
Secondary Infections21
- Candidiosis
- Commonly leads to pain, malnutrition, and potential esophageal infections
 |  |
 |
Trismus and Osteoradionecrosis2223
 |  |
 |
Functional Impairment24
- Trismus (myofibrotic contracture)
- Results from radiation to the TMJ, masseter, or pterygoid muscles, leading to fibrosis

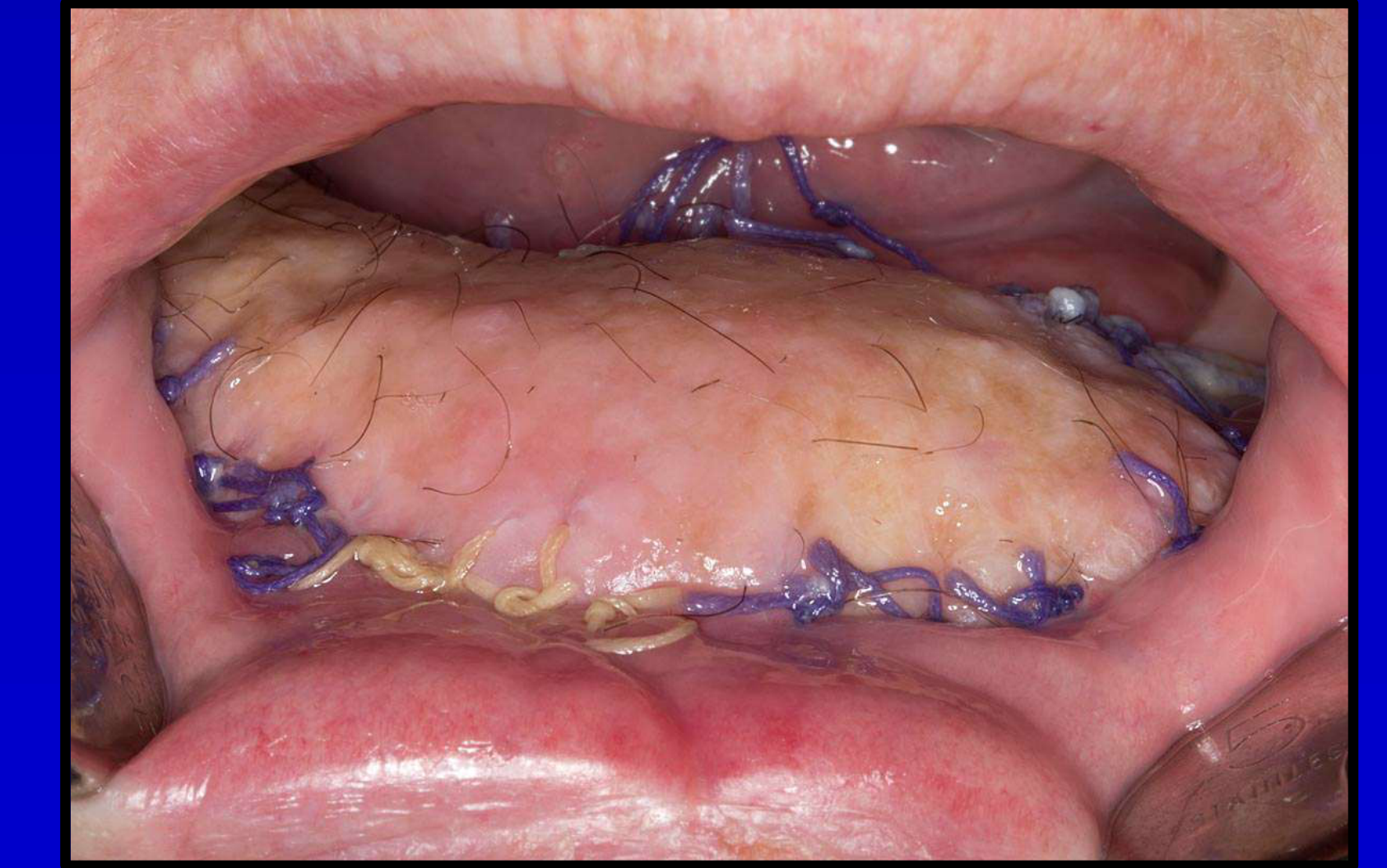
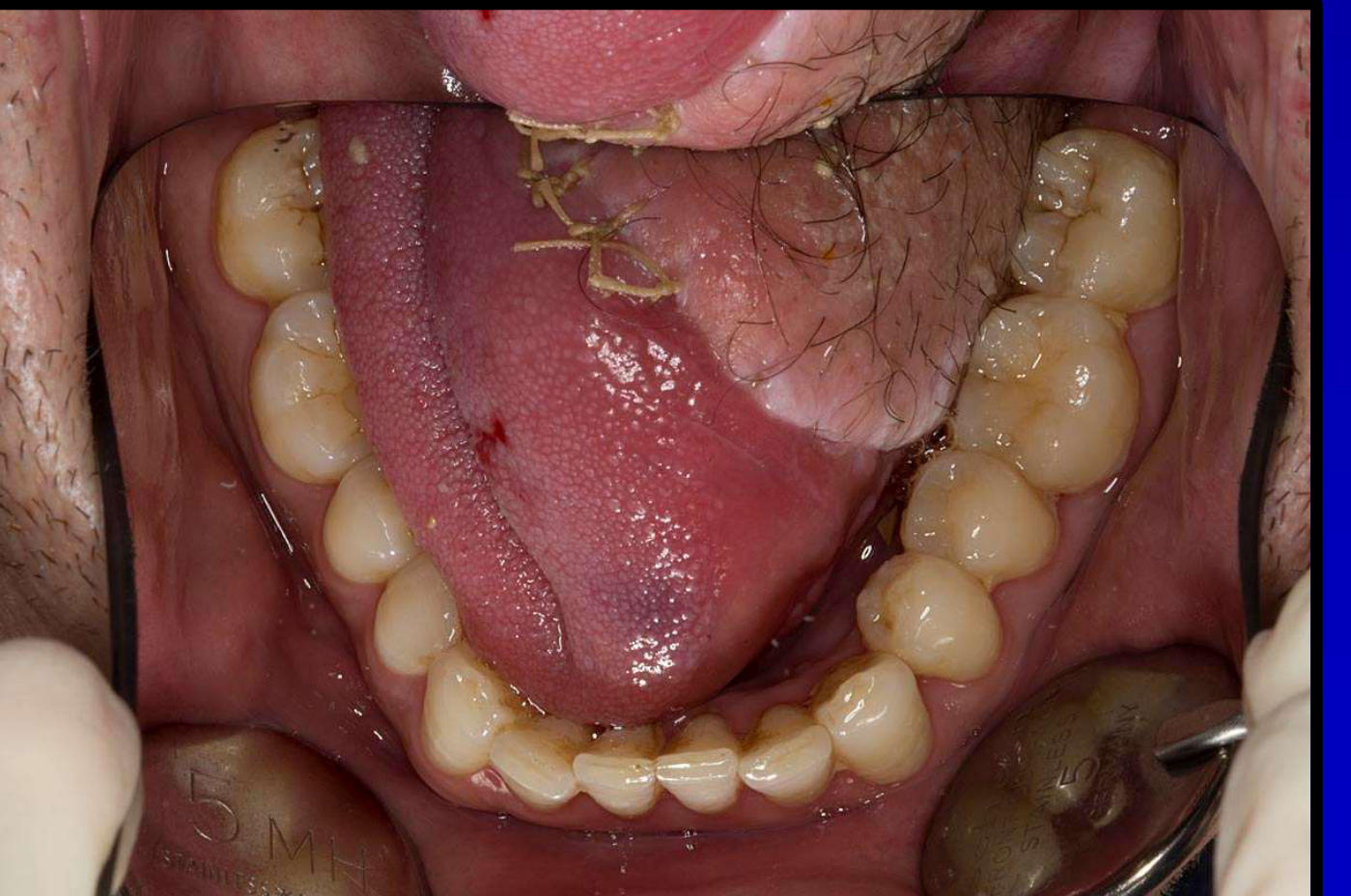
Bone Necrosis25
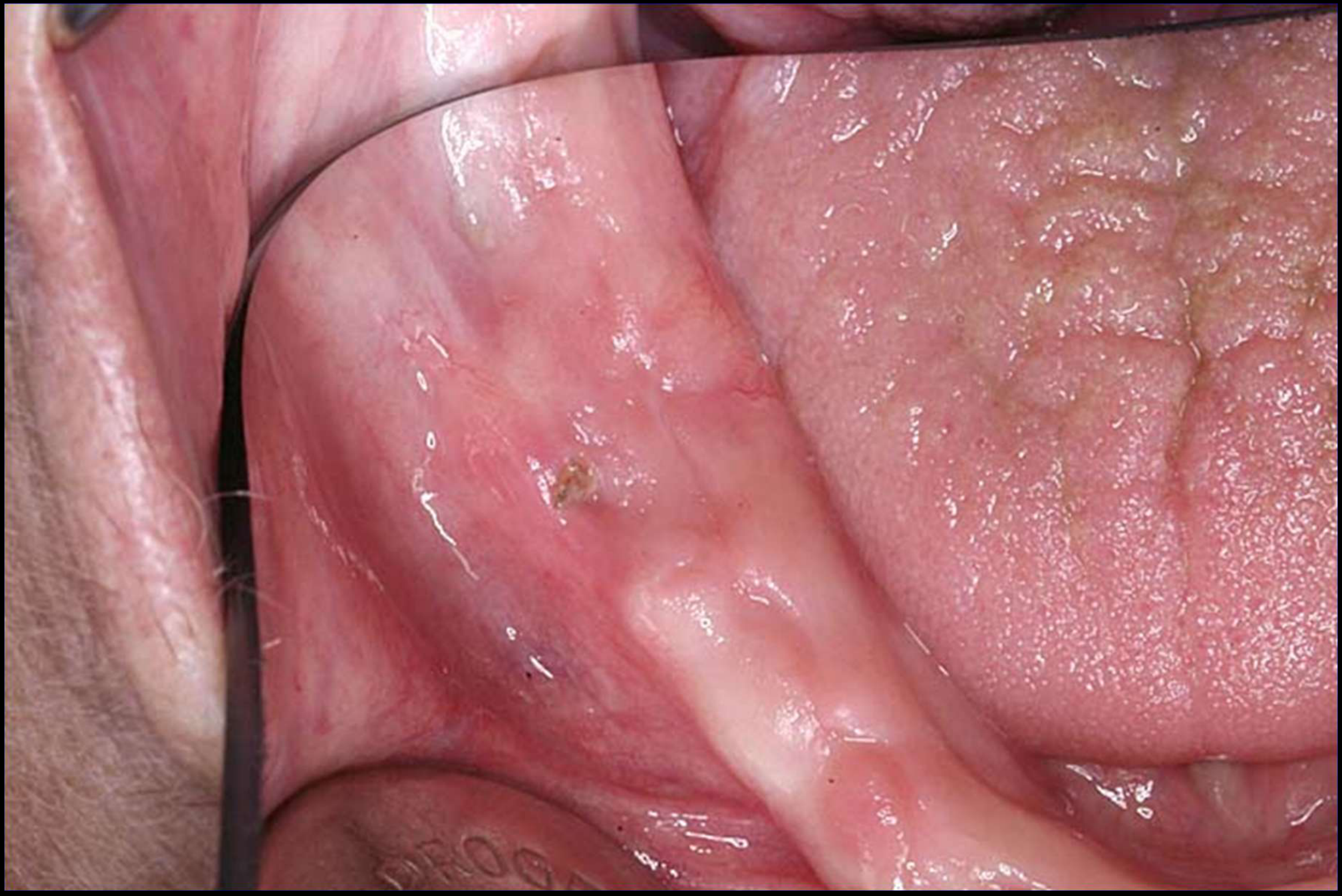
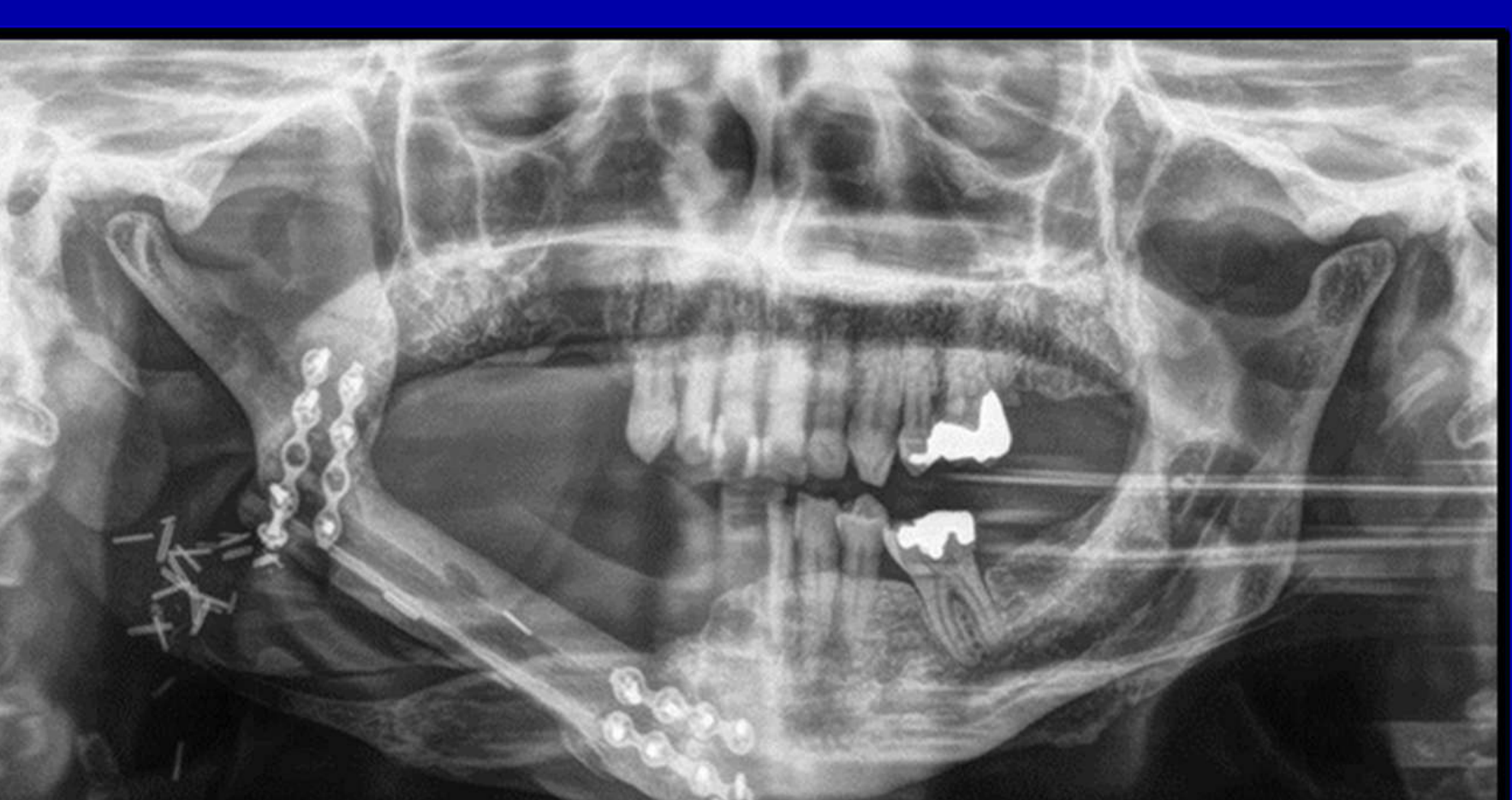
- Osteoradionecrosis
- Clinical presentation showing exposed bone and tissue damage
- Radiographic evidence (panoramic X-ray) showing bone density changes in the mandible
- Ischemic necrosis resulting from a failure of bone healing
- Often precipitated by dental infections, extractions, or trauma (e.g., from dentures)
 |  |
Radiation Therapy Complications26
Further clinical details regarding radiation-induced bone complications.
Management considerations for radiation-induced bone complications.
Additional observations on radiation-induced bone complications.
Case Study: Mandibular SCC Patient
A patient treated for a right mandibular SCC survived 10 years post-op, only to develop ORN in the maxilla, eventually losing a significant portion of the jaw.
 |  |
Other Adverse Effects of Treatment
Pain Management27
- Pain associated with dental procedures and inflamed gum tissue
 |  |
Functional and Psychological Impact28
- Dysphagia
- Dysarthria
- Psychological problems
 |  |
Miscellaneous Considerations29
Other clinical considerations in the management of oral cancer patients.
Risk of Second Primary Cancer
There is a 20% risk of a second primary cancer in the upper aerodigestive tract; vigilance is required during all follow-up appointments.
Dental Management Protocols3031
Dental management involves comprehensive care for oral cancer patients throughout their treatment journey.
The dental management protocol is divided into three primary phases:
- Pre-radiation therapy work-up
- Follow-up during radiation therapy
- Long term, post radiation therapy care
 |  |
Pre-Radiation Therapy Work-Up32
Initial assessment and preparation of the patient prior to the commencement of radiation therapy.
Objectives of Pre-Radiation Work-Up33
- Ensure that a patient is dentally fit
- Ensure that a patient understands the implication of radiation therapy from the dental point of view
- Ensure that a patient understands the required life style changes to maintain dentition post radiation therapy

Clinical Examination and Treatment Planning
Initial Assessment
- Medical, dental, and social history
- Establishment of proposed radiation therapy fields
- Dentists must obtain specific radiation fields and dosage information from the oncologist, as teeth in high-dose fields require stricter assessment.
Diagnostic Procedures
- Comprehensive dental examination, including radiographic examination
- Dietary counselling
Factors for Special Consideration
Special consideration must be given to teeth located within the irradiated field, focusing on:
- Condition of dentition
- Patient’s dental awareness
- Immediacy of treatment
- Prognosis for tumour control
Criteria for Pre-Treatment Extractions
Clinical Indications for Extraction
Teeth generally recommended for extraction include:
- Non-restorable teeth
- Root caries
- Periodontal disease
- Peri-apical disease
- Third molars
- Non-functional teeth
- Impacted teeth
Patient-Related Factors for Extraction
Extractions may also be indicated based on:
- Poor oral hygiene
- Lack of dental awareness
- Lack of cooperation
Clinical and radiographic evaluation is essential to identify teeth requiring extraction before radiation begins.
Pre-treatment dental clearance is a critical step in preventing future complications such as osteoradionecrosis.
The timing of extractions must allow for adequate healing before the start of radiation therapy.
Surgical Technique for Pre-Radiation Extractions
Extractions must include alveolectomies to ensure the ridge is perfectly smooth, as bone remodeling is significantly impaired following radiation therapy.
Protective Appliances
Use of dental models and transparent appliances may be required for planning or protecting tissues during treatment. To prevent Radiation Backscatter (which can double the dose to soft tissues near metal), use 5mm EVA (ethyl vinyl acetate) stents to separate the cheeks and tongue from metal restorations. Final review of the oral cavity and dental stability prior to the initiation of oncology protocols.
Management During Radiation Therapy34
Active dental monitoring and supportive care while the patient is undergoing radiation treatment.
Acute Side Effect Management35
Symptomatic management of the following conditions is required:
- Mucositis
- Loss of taste
- Dry mouth

Oral Hygiene and Therapeutic Agents36
- Maintenance of good oral hygiene (OH)
- Use of Benzydamine hydrochloride (e.g., Difflam Anti-Inflammatory Solution)
- Use of specialized oral care products (e.g., soft surgical toothbrushes and moisturizing toothpaste like Oral 7)
 |  |
 |
Long Term Post-Radiation Therapy Care37
Ongoing surveillance and management of late-onset effects following the completion of radiation therapy.
Post-Radiation Complications38
Long-term care involves dealing with:
- Dry mouth
- Caries
- Increased periodontal attachment loss
- Infections
- Trismus
- Osteoradionecrosis (ORN)
- Chronic pain
Management of Dry Mouth3940
Xerostomia Management Products
Various commercial products are available for managing dry mouth, including:
- Biotene
- OralSeven
- Hamilton Aquae
- GC Dry Mouth Gel
- Denta-Med
Management of dry mouth is essential for patient comfort and the prevention of radiation-induced dental decay.
Salivary Stimulants
- Sugar-free chewing gum
- Sugar-free candies and mints
- Xylitol-based gum is preferred; avoid acidic "sugar-free" candies as they can cause dental erosion.
Secretogogues
Pharmacological intervention to stimulate saliva production:
- Pilocarpine
- Other systemic agents
Mechanical Stimulation
- Electro-stimulating devices (e.g., GenNarino)
 |  |
Management of Caries and Infections4142
Preventive Strategies
- DIET (Sugar control)
- Oral Hygiene (OH)
- Daily Fluoride (F) application
- Regular dental visits
- High-fluoride toothpaste (5000ppm) is often recommended over fluoride trays to improve patient compliance.
- Dietary monitoring should specifically include avoiding high-sugar meal supplements or milkshakes.
Radiation-related caries can progress rapidly and require aggressive preventive measures.
Early detection of carious lesions is vital to prevent the need for extractions in irradiated bone.
Clinical Presentation of Caries
Monitoring for various stages of dental caries and implementing appropriate restorative treatments.
 |  |  |
 |  |  |
Management of Oral Infections
Treatment of fungal infections (e.g., Candidiasis) using antifungal agents such as Nilstat Oral drops.
Antifungal Selection
Miconazole gel is preferred for oral infections; avoid Nystatin (Nilstat) if possible due to its high sugar content, which can exacerbate radiation-related caries.
Management of Trismus and Osteoradionecrosis43
Trismus
Management of myofibrotic contracture and restricted jaw opening resulting from radiation therapy.
- Patients should perform jaw-opening exercises consisting of 20 repetitions, three times daily.
Osteoradionecrosis (ORN) Management
- Prevention (Primary focus)
- Hyperbaric oxygen treatment (HBO):
- Breathing 100% O₂ at pressure greater than 1 atmosphere absolute (Usually 2-3 ATA)
- Surgery
- Medical treatment
Osteoradionecrosis represents a severe late complication requiring multidisciplinary management.

Patient Information and Support
Radiation Therapy to the Head and Neck44
Professional Guidance
Patients must be warned against erroneous advice regarding oral care during treatment. >- Caution: For dentate patients, sucking on boiled sweets and lemons is a "recipe for dental caries" and should be avoided.
Clinical Case Studies
Patient Profile and Diagnosis45
Case 1: Metastatic Neck Squamous Cell Carcinoma
- Age: 46 years old
- Diagnosis: Metastatic neck Squamous Cell Carcinoma (SCC) – unknown primary
- Planned Treatment: Surgery and radiation therapy
Radiation Therapy Planning4647
- Proposed radiation therapy fields: All molars are located within the irradiated field.
 |  |
 |
Radiographic Assessment48
Radiographic evaluation via panoramic X-ray (OPG) was performed to assess the dentition and bone structure prior to the commencement of oncology treatment.
- Radiographic assessment identified impacted and heavily restored teeth.

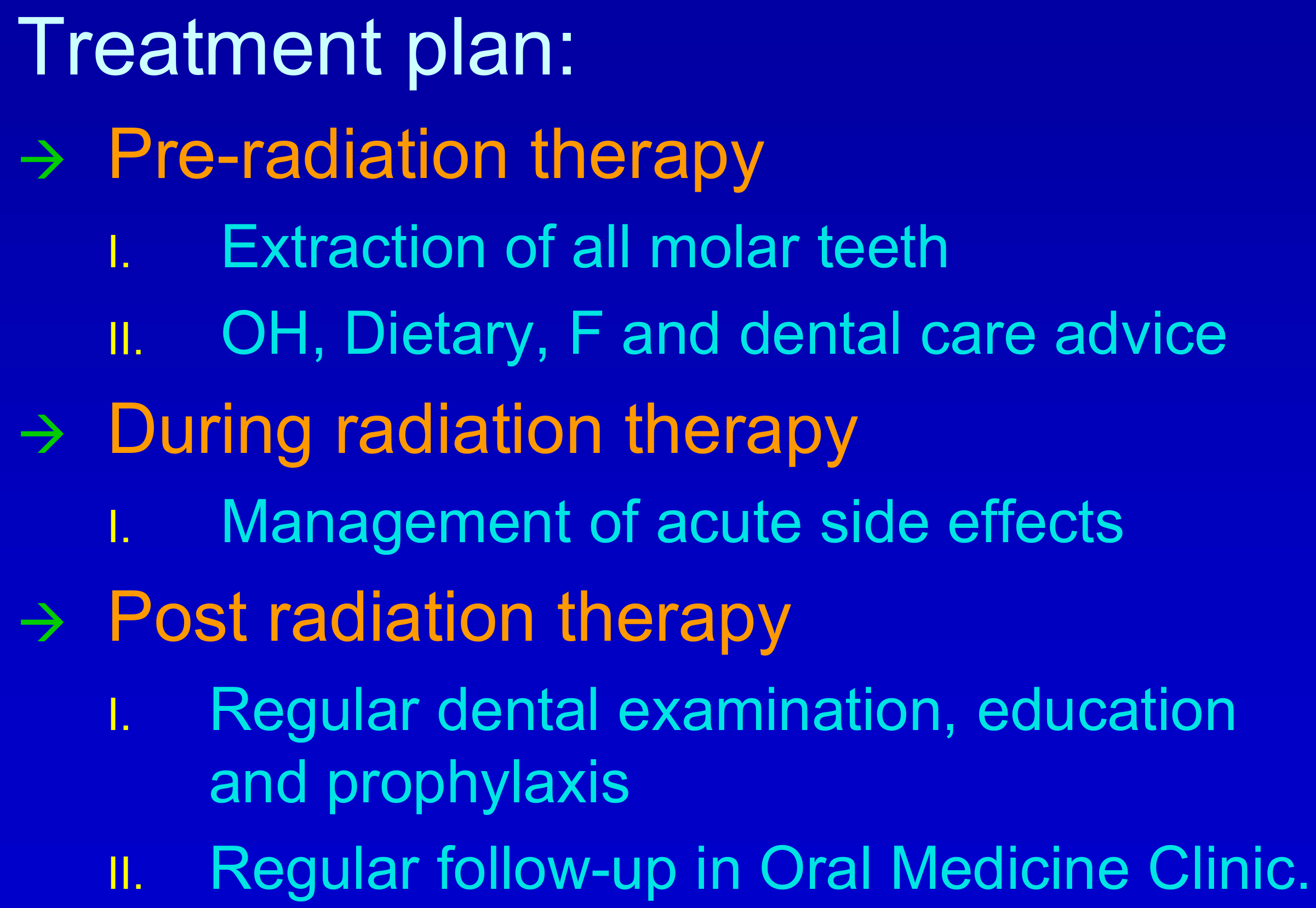
Comprehensive Treatment Plan495051
- Pre-radiation Therapy Phase
- Extraction of all molar teeth located within the radiation field.
- Provision of Oral Hygiene (OH), dietary counseling, fluoride (F) therapy, and general dental care advice.
- During Radiation Therapy Phase
- Active management of acute side effects.
- Post-radiation Therapy Phase
- Regular dental examinations, ongoing patient education, and professional prophylaxis.
- Regular follow-up appointments in the Oral Medicine Clinic.
- Outcome: The patient was highly compliant with fluoride and hygiene, resulting in perfect dentition maintained 3 years post-treatment.
 |  |  |
 |
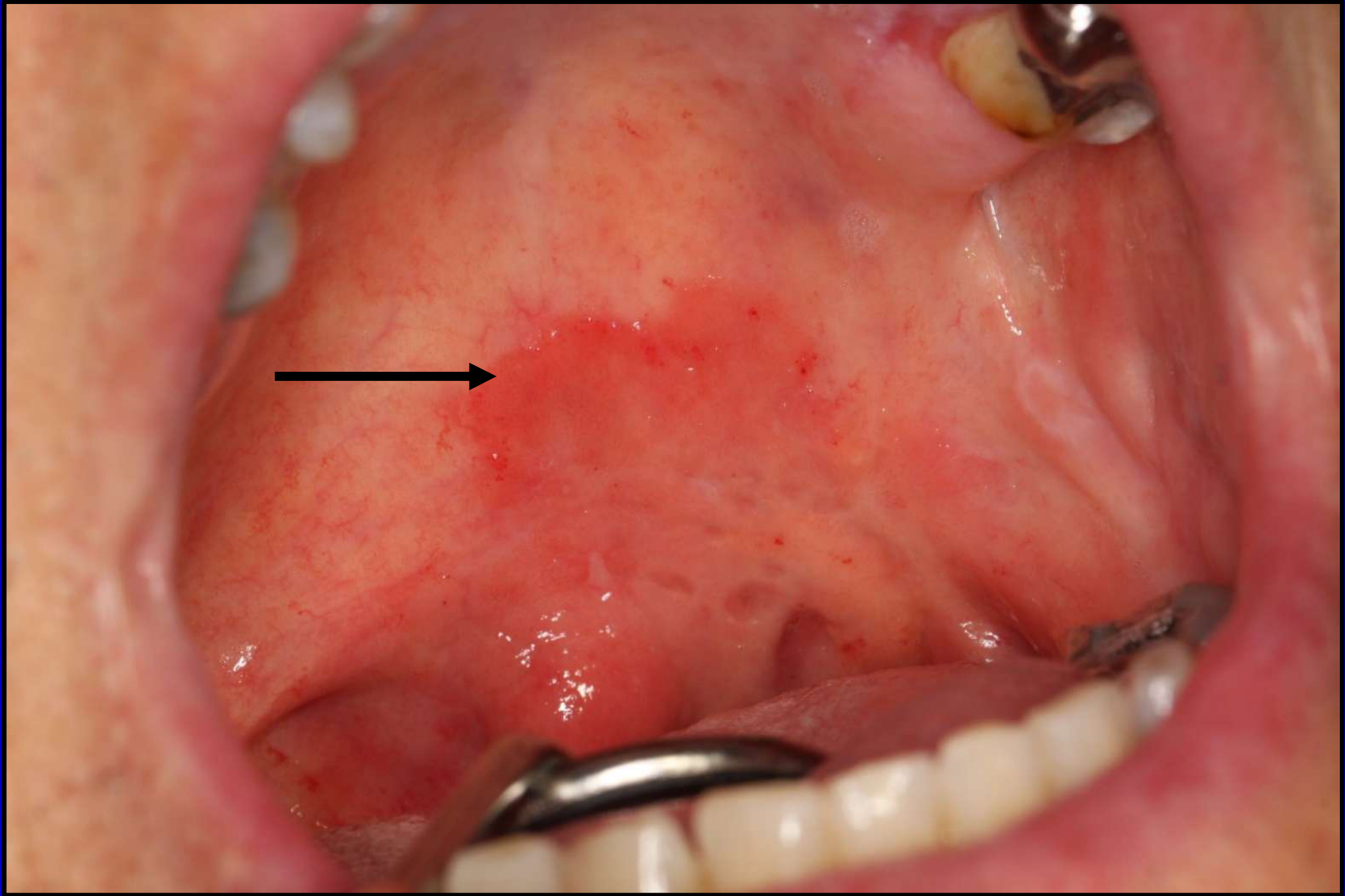
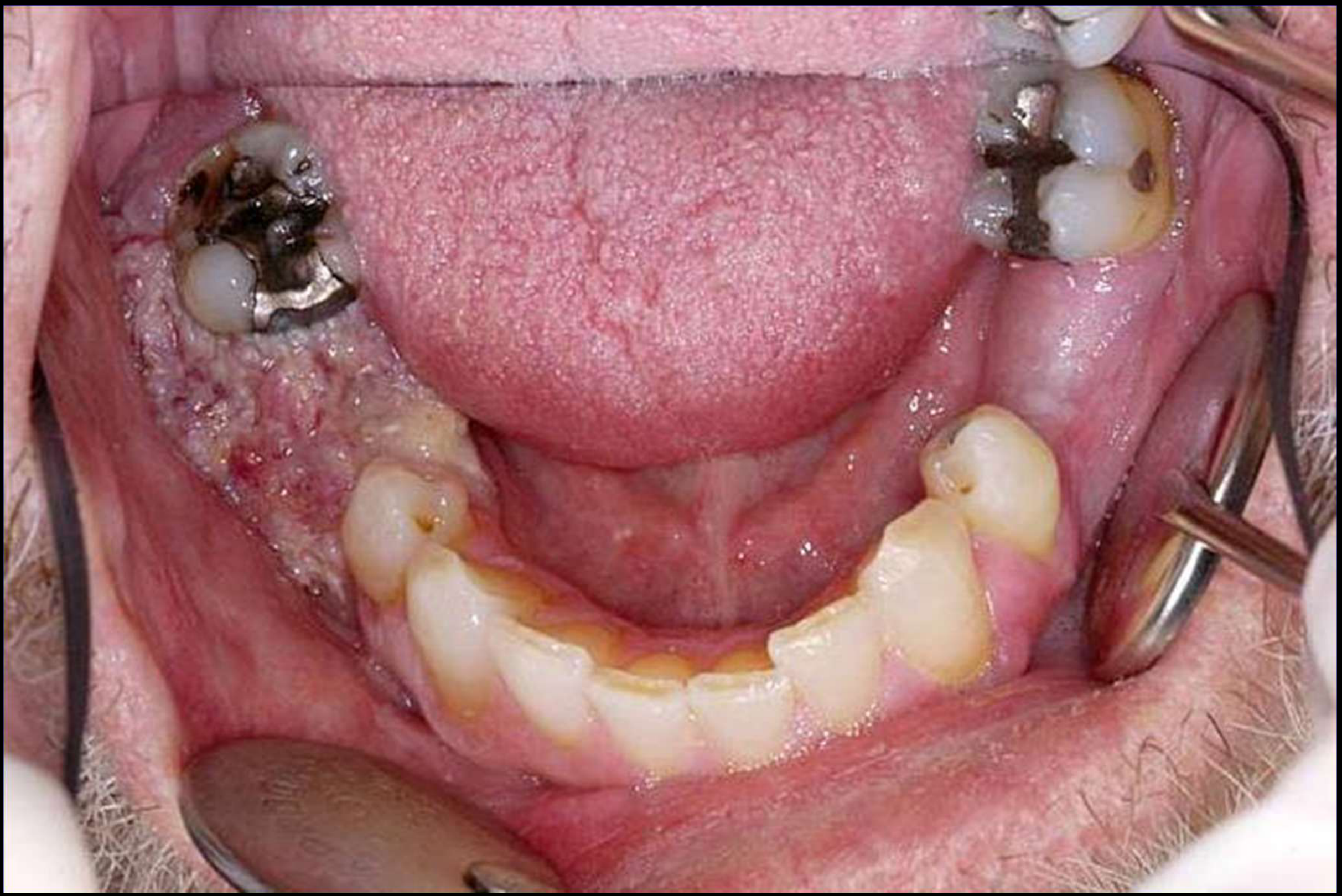
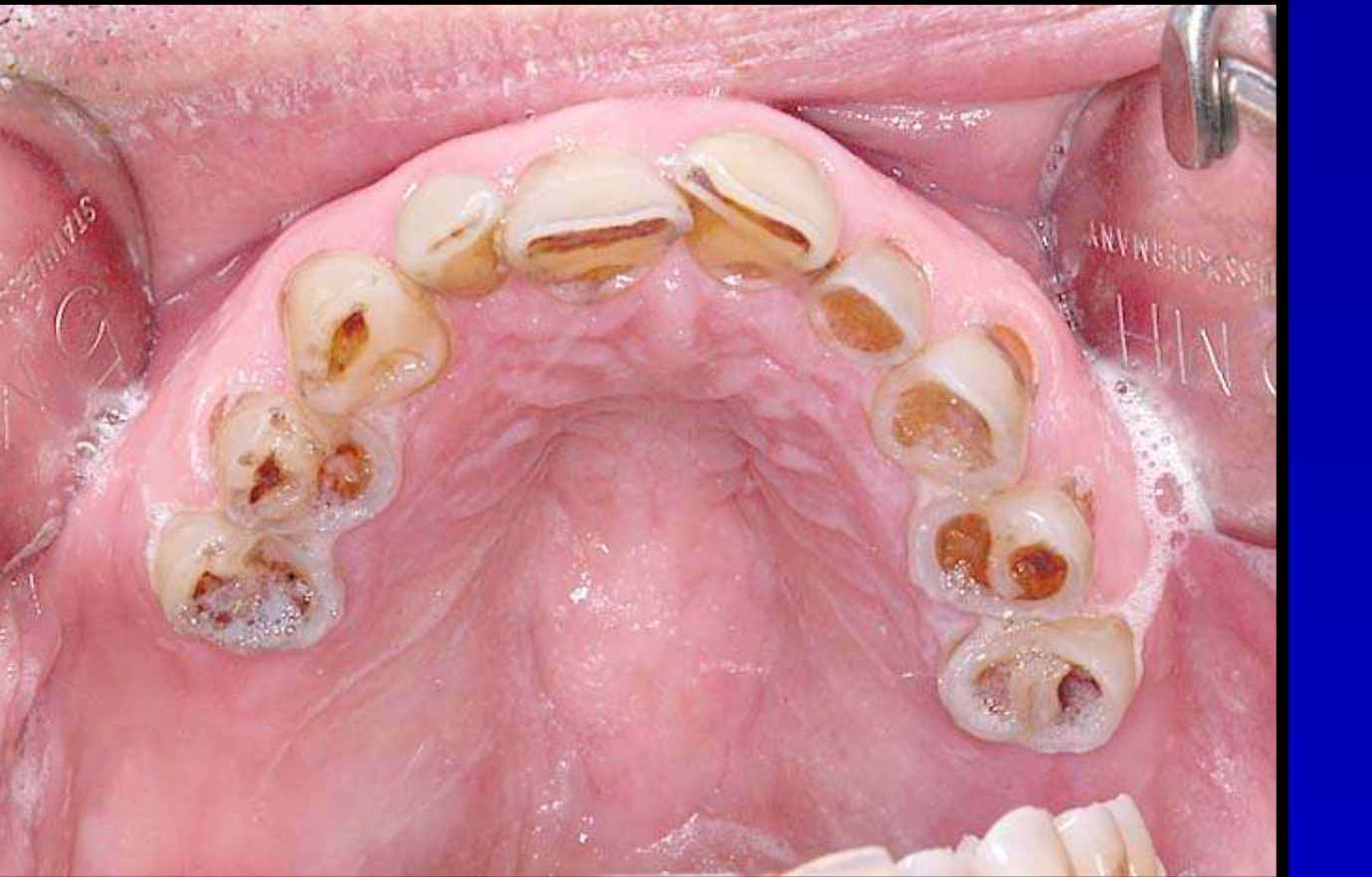
Case 2: Clinical Presentation52
Case 2: The "Sad Case"
- Patient Profile: Male in early 40s with base of tongue cancer.
- Diagnosis: Reasonable initial dentition, but identified as high risk for non-compliance.
- Outcome: The patient did not return for follow-up. One year later, he presented with "radiation caries" in every tooth due to a high-sugar diet (iced coffee/supplements) and dry mouth. He required full dental clearance.

 |  |
 |
Conclusion53
Dental care forms an integral part of the multidisciplinary management of oral cancer patients and it significantly contributes to the preservation of life quality.
Dental management is not merely about treating complications but about prevention. Through careful pre-radiation planning, patient education, and lifelong vigilance, dentists can prevent catastrophic outcomes like ORN and radiation caries.
 |  |
Footnotes
-
Original PDF page 1: L13 Dental management of oral cancer patients, p.1 ↩
-
Original PDF page 2: L13 Dental management of oral cancer patients, p.2 ↩
-
Original PDF page 3: L13 Dental management of oral cancer patients, p.3 ↩
-
Original PDF page 4: L13 Dental management of oral cancer patients, p.4 ↩
-
Original PDF page 6: L13 Dental management of oral cancer patients, p.6 ↩
-
Original PDF page 7: L13 Dental management of oral cancer patients, p.7 ↩
-
Original PDF page 8: L13 Dental management of oral cancer patients, p.8 ↩
-
Original PDF page 9: L13 Dental management of oral cancer patients, p.9 ↩
-
Original PDF page 10: L13 Dental management of oral cancer patients, p.10 ↩
-
Original PDF page 11: L13 Dental management of oral cancer patients, p.11 ↩
-
Original PDF page 14: L13 Dental management of oral cancer patients, p.14 ↩
-
Original PDF page 12: L13 Dental management of oral cancer patients, p.12 ↩
-
Original PDF page 13: L13 Dental management of oral cancer patients, p.13 ↩
-
Original PDF page 15: L13 Dental management of oral cancer patients, p.15 ↩
-
Original PDF page 16: L13 Dental management of oral cancer patients, p.16 ↩
-
Original PDF page 17: L13 Dental management of oral cancer patients, p.17 ↩
-
Original PDF page 18: L13 Dental management of oral cancer patients, p.18 ↩
-
Original PDF page 19: L13 Dental management of oral cancer patients, p.19 ↩
-
Original PDF page 20: L13 Dental management of oral cancer patients, p.20 ↩
-
Original PDF page 21: L13 Dental management of oral cancer patients, p.21 ↩
-
Original PDF page 22: L13 Dental management of oral cancer patients, p.22 ↩
-
Original PDF page 26: L13 Dental management of oral cancer patients, p.26 ↩
-
Original PDF page 27: L13 Dental management of oral cancer patients, p.27 ↩
-
Original PDF page 23: L13 Dental management of oral cancer patients, p.23 ↩
-
Original PDF page 24: L13 Dental management of oral cancer patients, p.24 ↩
-
Original PDF page 25: L13 Dental management of oral cancer patients, p.25 ↩
-
Original PDF page 28: L13 Dental management of oral cancer patients, p.28 ↩
-
Original PDF page 29: L13 Dental management of oral cancer patients, p.29 ↩
-
Original PDF page 30: L13 Dental management of oral cancer patients, p.30 ↩
-
Original PDF page 31: L13 Dental management of oral cancer patients, p.31 ↩
-
Original PDF page 32: L13 Dental management of oral cancer patients, p.32 ↩
-
Original PDF page 33: L13 Dental management of oral cancer patients, p.33 ↩
-
Original PDF page 34: L13 Dental management of oral cancer patients, p.34 ↩
-
Original PDF page 45: L13 Dental management of oral cancer patients, p.45 ↩
-
Original PDF page 46: L13 Dental management of oral cancer patients, p.46 ↩
-
Original PDF page 47: L13 Dental management of oral cancer patients, p.47 ↩
-
Original PDF page 48: L13 Dental management of oral cancer patients, p.48 ↩
-
Original PDF page 49: L13 Dental management of oral cancer patients, p.49 ↩
-
Original PDF page 51: L13 Dental management of oral cancer patients, p.51 ↩
-
Original PDF page 55: L13 Dental management of oral cancer patients, p.55 ↩
-
Original PDF page 57: L13 Dental management of oral cancer patients, p.57 ↩
-
Original PDF page 58: L13 Dental management of oral cancer patients, p.58 ↩
-
Original PDF page 63: L13 Dental management of oral cancer patients, p.63 ↩
-
Original PDF page 64: L13 Dental management of oral cancer patients, p.64 ↩
-
Original PDF page 66: L13 Dental management of oral cancer patients, p.66 ↩
-
Original PDF page 67: L13 Dental management of oral cancer patients, p.67 ↩
-
Original PDF page 68: L13 Dental management of oral cancer patients, p.68 ↩
-
Original PDF page 69: L13 Dental management of oral cancer patients, p.69 ↩
-
Original PDF page 70: L13 Dental management of oral cancer patients, p.70 ↩
-
Original PDF page 71: L13 Dental management of oral cancer patients, p.71 ↩
-
Original PDF page 72: L13 Dental management of oral cancer patients, p.72 ↩
-
Original PDF page 73: L13 Dental management of oral cancer patients, p.73 ↩
-
Original PDF page 74: L13 Dental management of oral cancer patients, p.74 ↩