Bone Diseases1
DENT 5322
Dr. Omar Kujan
Course Overview
This course provides a comprehensive examination of bone pathologies relevant to dental practice.
Lecture Focus
This lecture serves as the first part of a series on bone diseases, focusing on the fundamental biological principles and the radiographic classification of lesions.
Learning Objectives2
Upon completion of this section, students should be able to:
- Explain the aetiology, pathogenesis, clinical (including radiographic), and histopathological features of bone diseases.
- Discuss the diagnosis and treatment protocols for various bone conditions.
- Formulate a differential diagnosis using clinical and radiological information to reach a definitive diagnosis (often confirmed via biopsy).
For more details, please refer to the Unit Guide.
Recommended References3
Primary Textbook4
- Cawson’s Essentials of Oral Pathology and Oral Medicine
- Edition: 9th Edition
- Author: Edward Odell
- Recommended as an excellent undergraduate resource with comprehensive chapters on bone diseases.
Bone Biology and Physiology
Clinical Significance
A thorough understanding of bone biology is essential to comprehending how diseases develop and why they present with specific clinical and radiographic features.
Components of the Haversian System5
The microscopic structure of bone tissue is organized into the Haversian system, which includes the following key anatomical features:
- Bone is classified by its structure and composition into lamellar bone, compact bone, and spongy bone.
- Bone is a vascular tissue; however, it relies on nutrition from the surrounding connective tissue and bone marrow spaces.
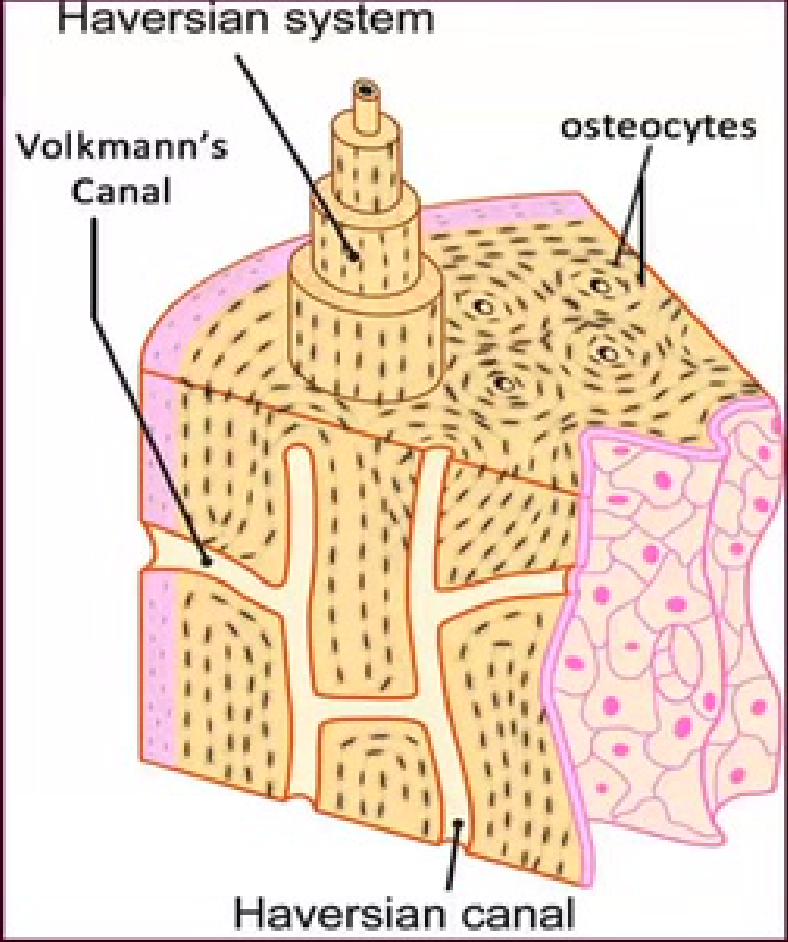
Microscopic Anatomy of Bone
- Haversian Canal: The central channel containing blood vessels and nerve fibers.
- These are vertical channels.
- Volkmann’s Canal: Channels that assist in transmitting blood vessels from the periosteum into the bone and communicate with the Haversian canals.
- These are horizontal channels that assist in communication between osteons.
- Osteocytes: Mature bone cells located within the bone matrix.
- Lamellae: Concentric layers of mineralized matrix surrounding the central canal.
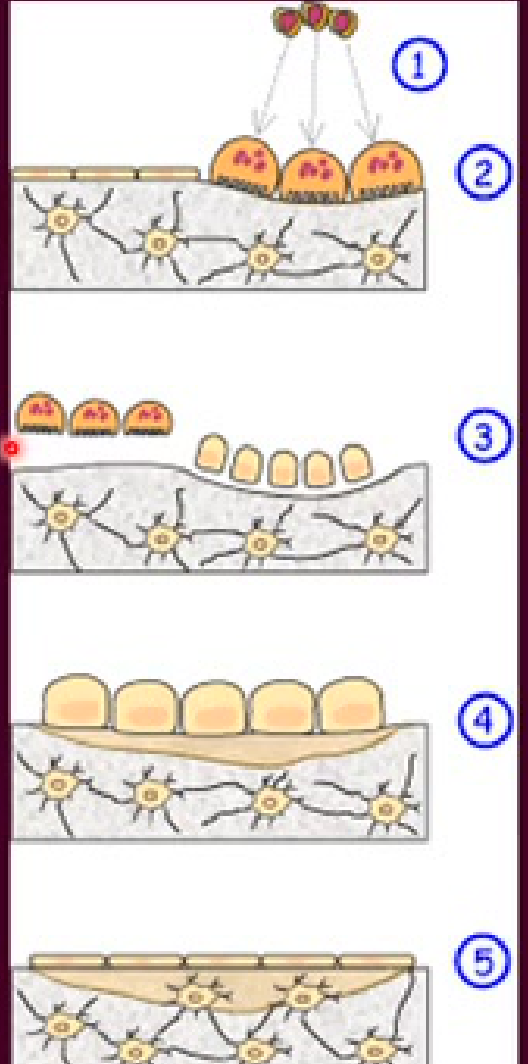
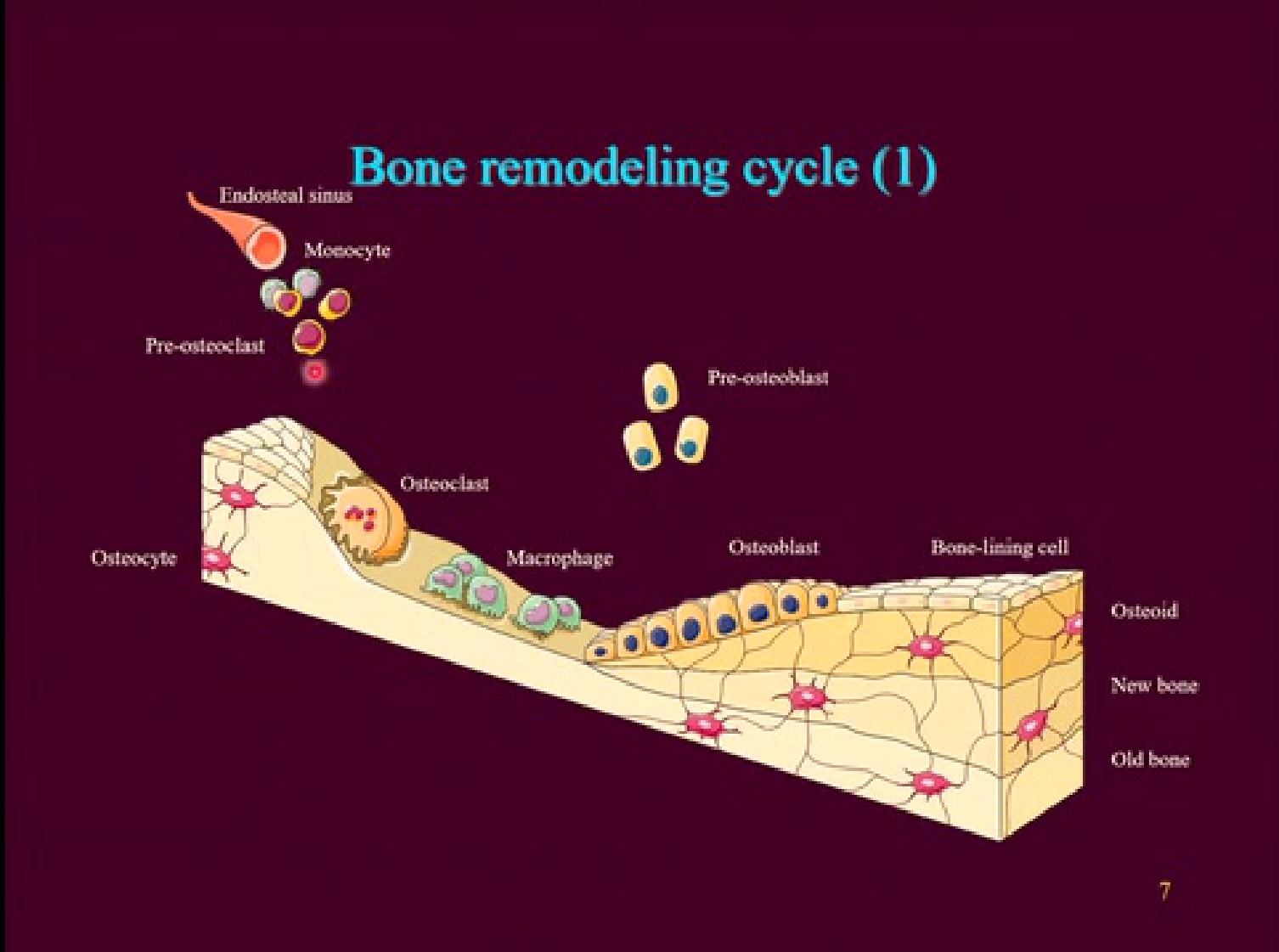
The Bone Remodeling Cycle67
Bone remodeling is the continuous process of replacing old tissue with new bone. This cycle consists of five distinct phases:
- Activation: Preosteoclasts are stimulated and differentiate into mature, active osteoclasts under the influence of cytokines and growth factors.
- Resorption: Active osteoclasts digest the mineral matrix of the old bone.
- Reversal: This phase marks the end of bone resorption.
- This is the transition point where resorption stops and formation begins, marked by a "reversal line".
- Formation: Osteoblasts synthesize new bone matrix.
- Quiescence: Osteoblasts transition into resting bone-lining cells on the newly formed bone surface.
 | 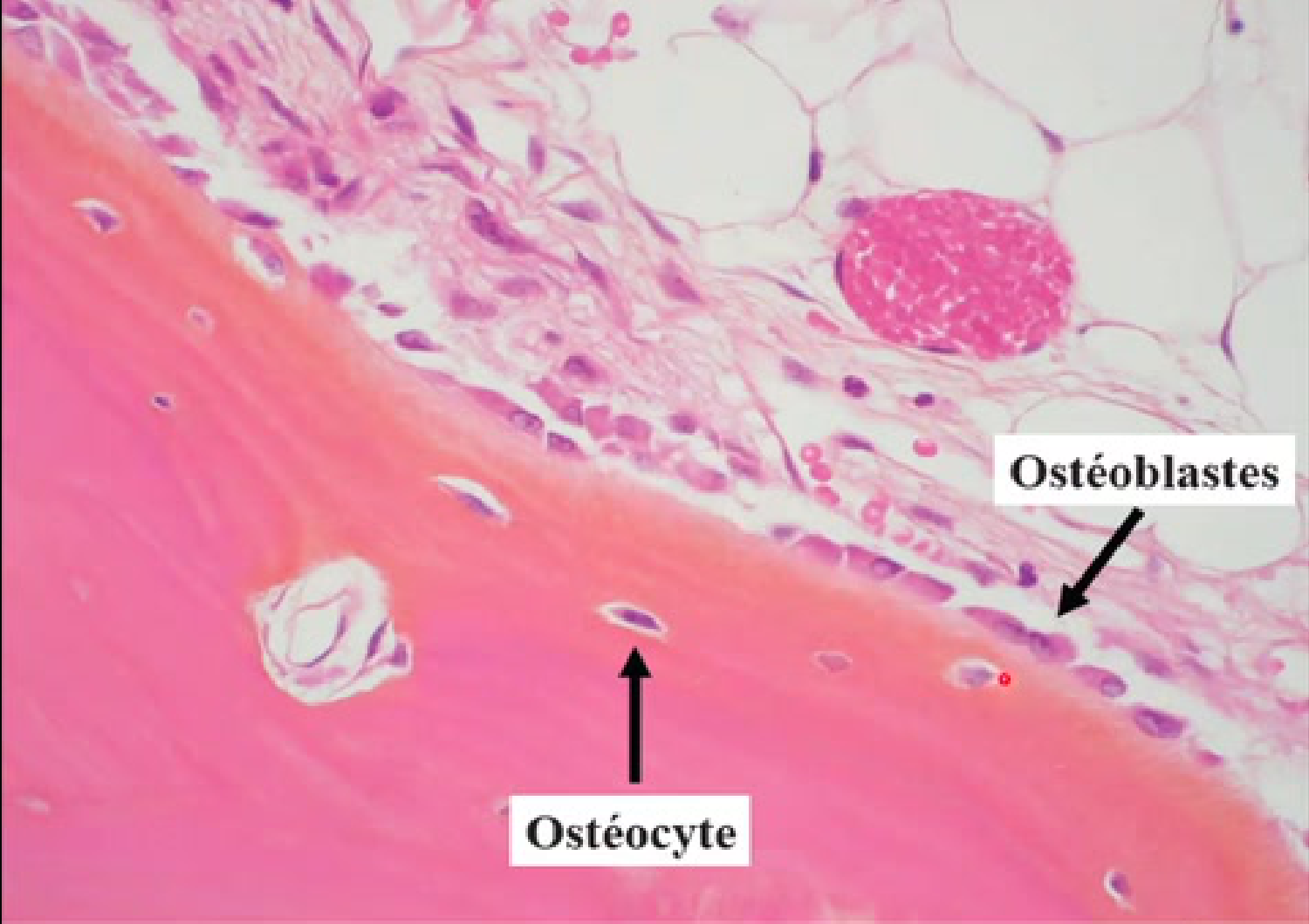 |
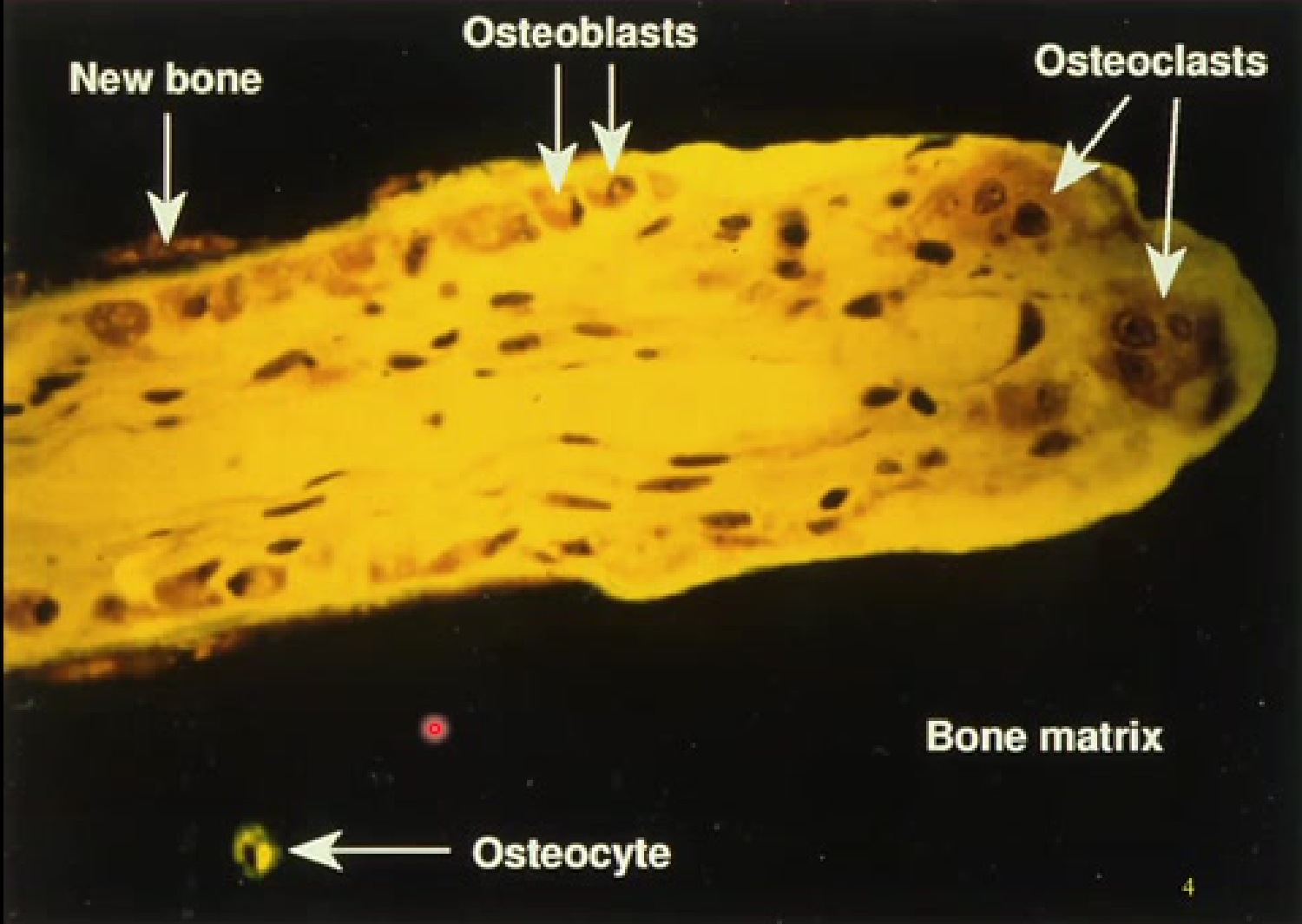
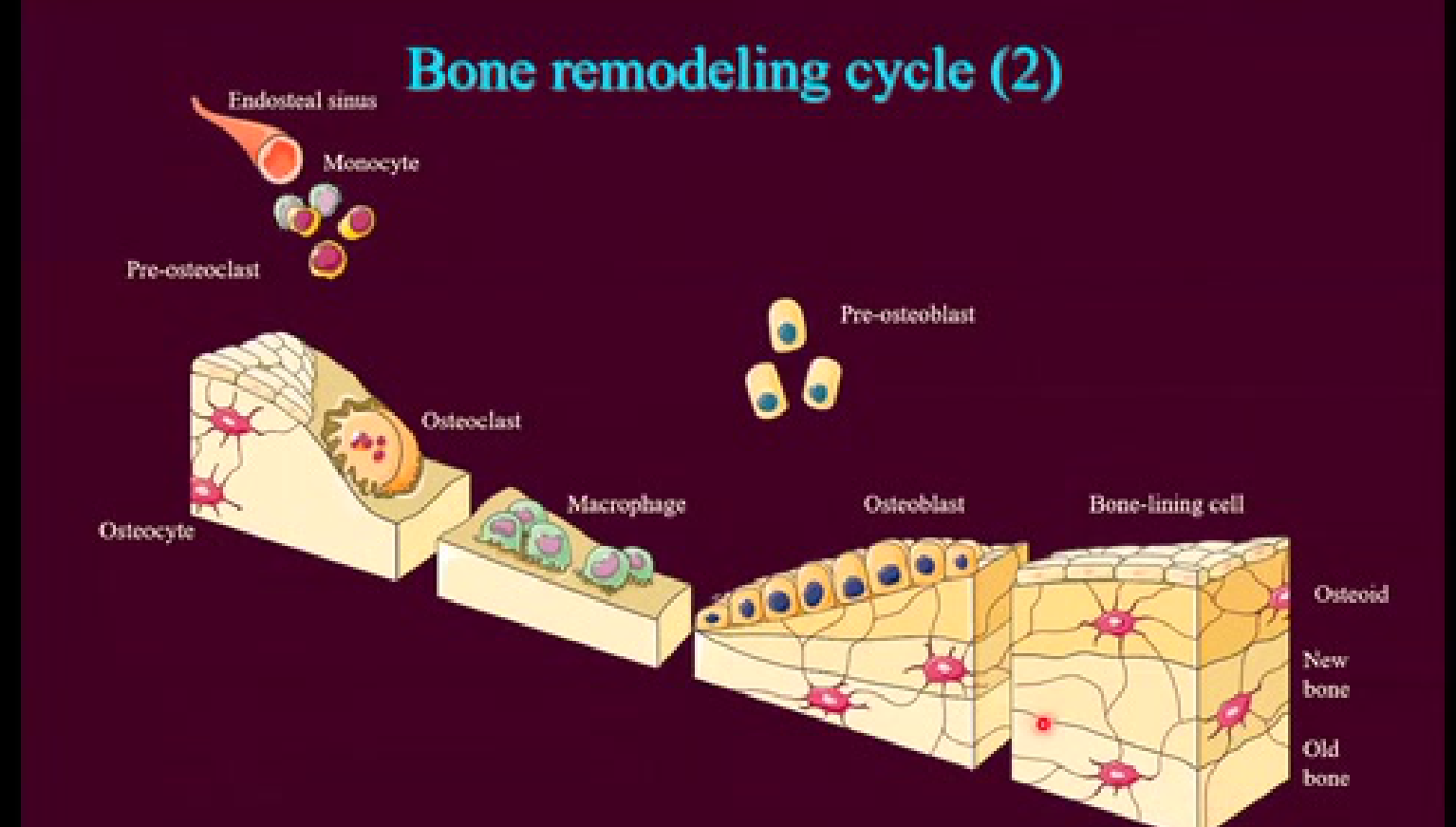
Cellular Components of the Remodeling Cycle8
The bone remodeling cycle involves a variety of specialized cells and structures working in coordination:
- Vascular and Precursor Elements: Endosteal sinus, monocytes, and pre-osteoclasts.
- Active Bone Cells: Osteoclasts (responsible for resorption) and osteoblasts (responsible for formation).
- Osteoblasts: Mononucleated cells that secrete osteoid (the initial organic, non-mineralized matrix).
- Osteoclasts: Large, multinucleated giant cells originating from the monocyte/macrophage lineage in the bone marrow.
- Osteoblasts: Mononucleated cells that secrete osteoid (the initial organic, non-mineralized matrix).
- Supportive and Regulatory Cells: Macrophages, pre-osteoblasts, and bone-lining cells.
- Matrix and Tissue States: Osteoid (unmineralized matrix), new bone, old bone, and embedded osteocytes.
 | 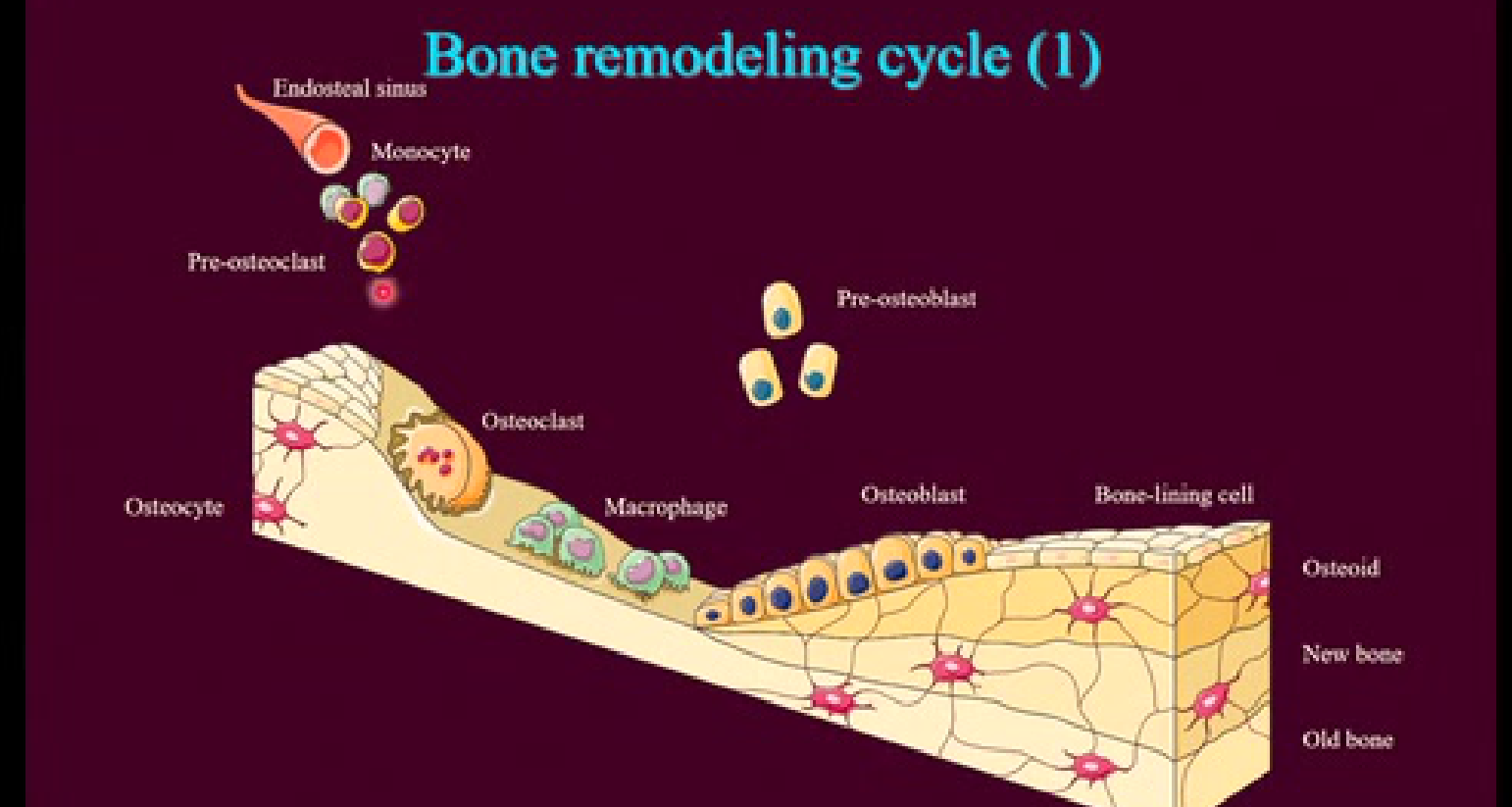 |
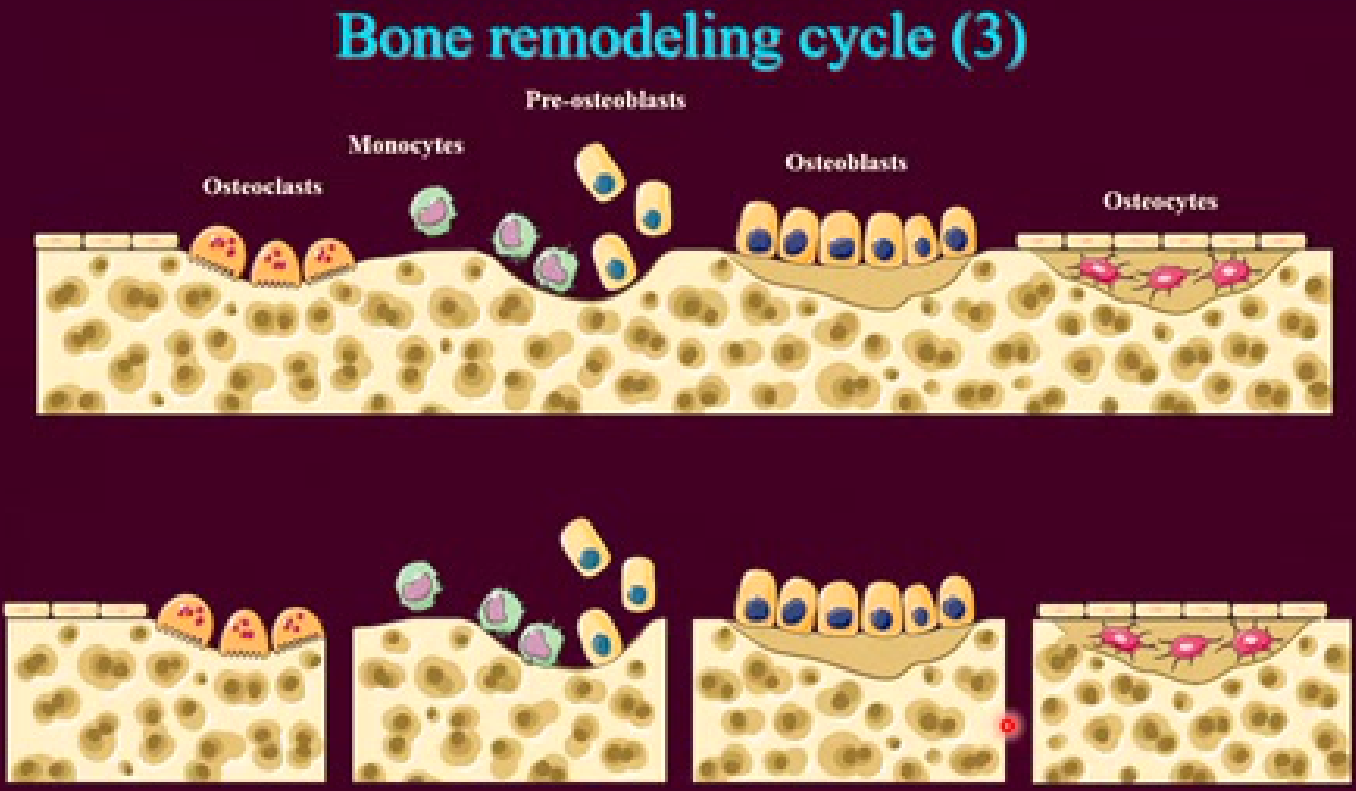
Stages of Bone Tissue Turnover9
- Resorption Phase: Involves the transition from the endosteal sinus to monocytes and pre-osteoclasts, culminating in osteoclasts resorbing old bone.
- Clearance Phase: Osteoclasts and macrophages work to clear cellular and matrix debris from the site.
- Formation Phase: Pre-osteoblasts differentiate into osteoblasts, which eventually become bone-lining cells as they form new bone.
- Maturation Phase: Osteoblasts produce osteoid, which undergoes mineralization to become functional new bone.
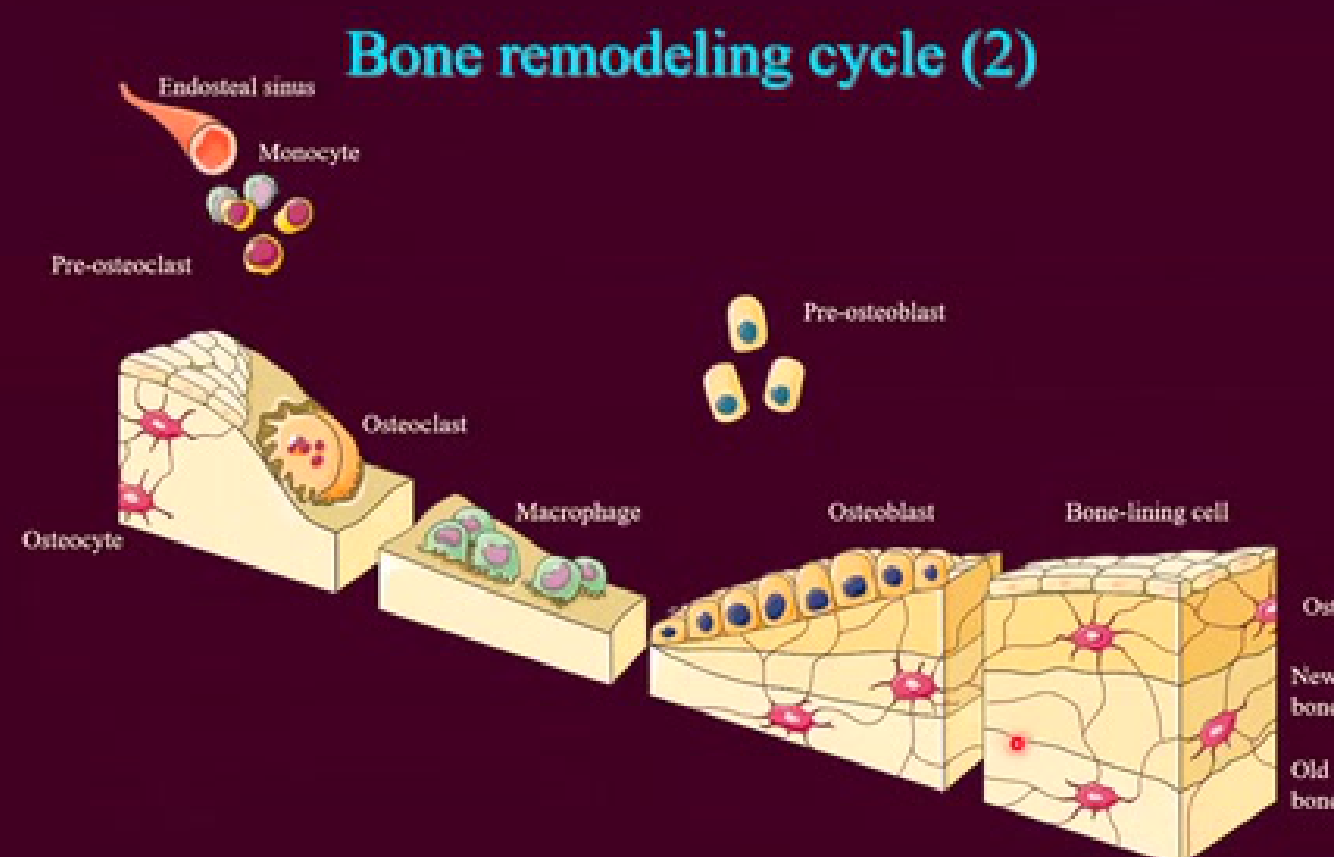 |  |
Cellular Interaction in the Remodeling Site10
The spatial organization of the remodeling cycle demonstrates the interaction between different cell lineages within the bone tissue:
- Osteoclast Lineage: Monocytes and pre-osteoclasts migrating to the resorption site.
- Osteoblast Lineage: Pre-osteoblasts and active osteoblasts lining the areas of new bone formation.
- Integration: Mature osteocytes remain embedded within the bone matrix to monitor mechanical strain and direct remodeling activity.
The bone remodeling cycle is a continuous physiological process involving the coordinated actions of osteoclasts and osteoblasts to maintain skeletal integrity and mineral homeostasis.
Radiographic Interpretation of Bone Lesions
Radiographic interpretation is essential for diagnosing bone lesions, requiring a systematic approach to evaluate changes in bone density and structure.
Info
Radiolucency indicates a loss of bone density, appearing as dark areas on an X-ray, whereas radiopacity indicates an increase in bone density, appearing white or light.
Imaging Modalities
Common Radiographic Techniques11
- Periapical
- OPG (Orthopantomogram)
- CBCT (Cone Beam Computed Tomography)
- CT Scan
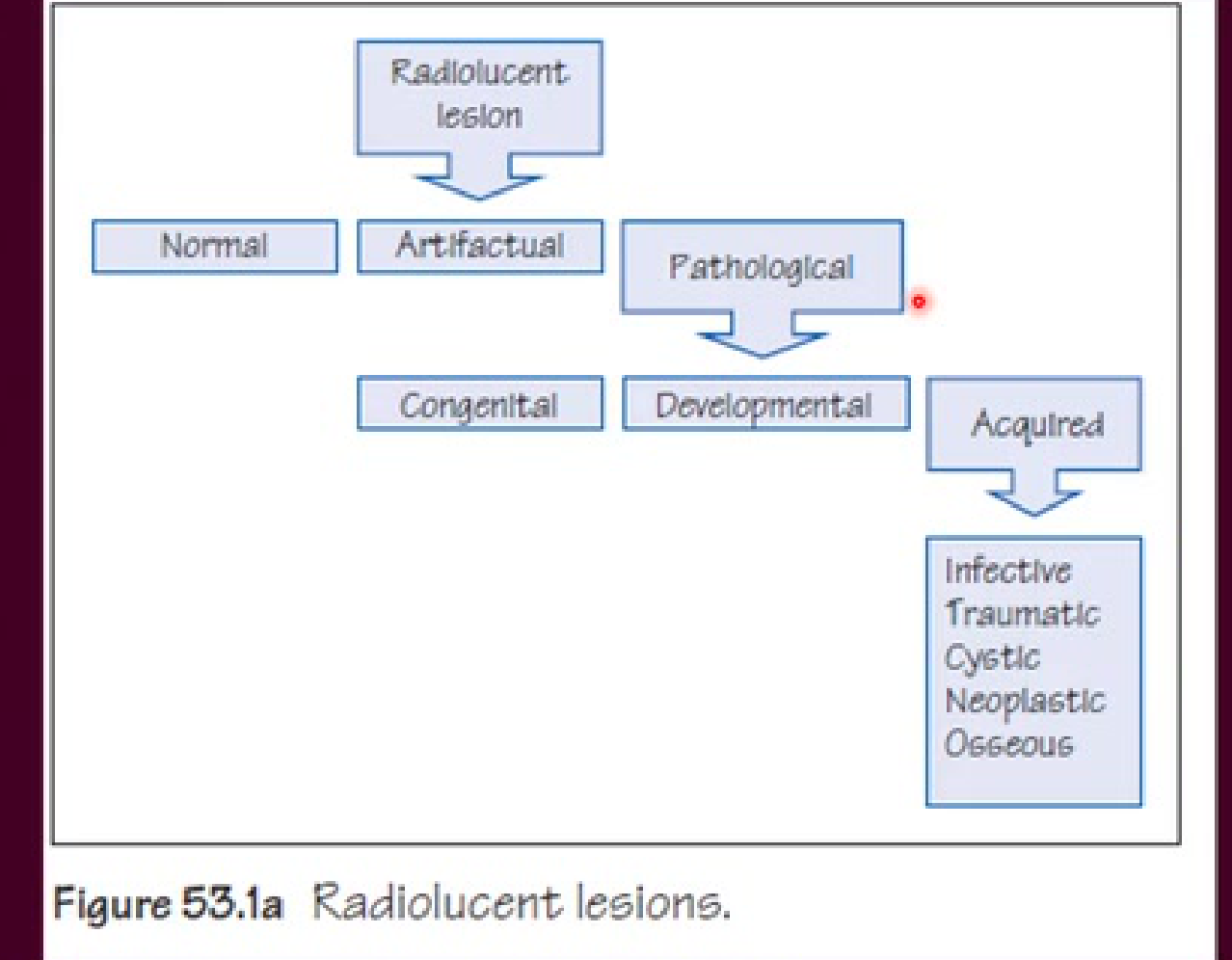
Classification of Radiolucent Lesions
Categorization of Radiolucent Lesions12
Radiolucent lesions can be classified based on their nature and origin:
- Normal anatomical variations
- Artifactual findings
- Pathological conditions
- Congenital
- Developmental
- Acquired:
- Infective
- Traumatic
- Cystic
- Neoplastic
- Osseous
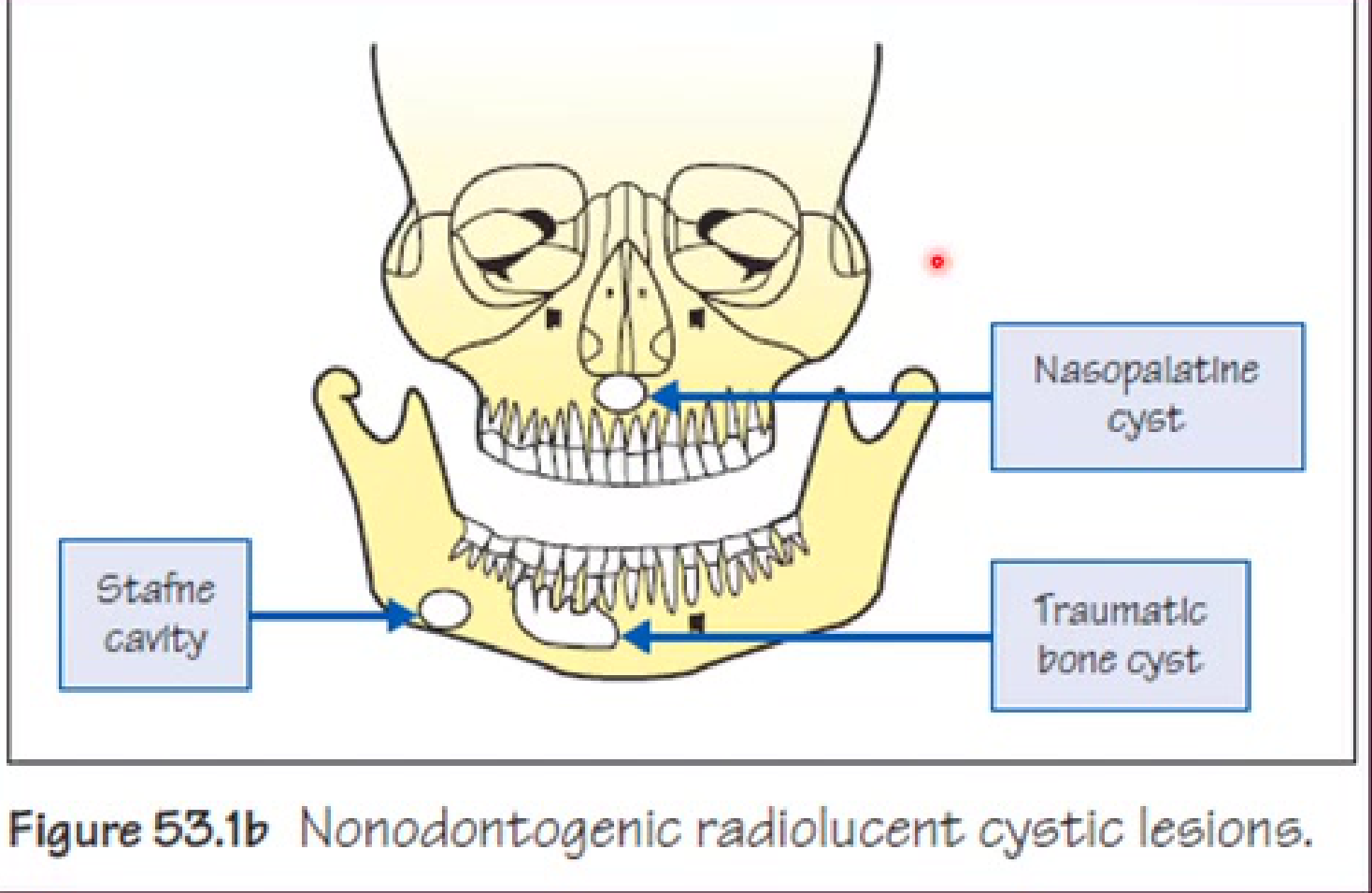
Nonodontogenic Radiolucent Cystic Lesions13
This category includes various cystic presentations within the bone that do not originate from tooth-forming tissues.
- Stafne Defect (Stafne Cavity): A developmental variation (not a true cyst) often containing salivary gland tissue.
- Traumatic Bone Cyst: A radiolucent void in the bone.
- Nasopalatine Duct Cyst: A well-demarcated radiolucency in the midline of the anterior maxilla.
Morphological Classification of Radiolucencies14
Radiolucent lesions are often categorized by their internal architecture as either unilocular or multilocular.
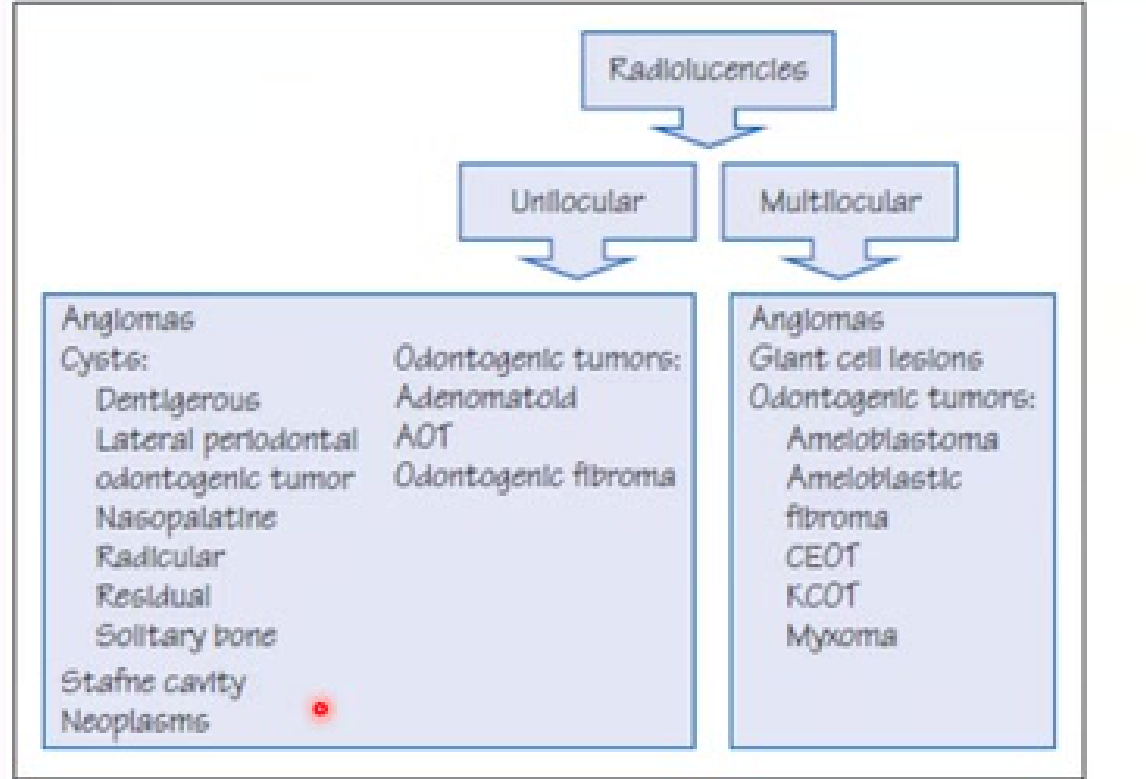 |  |
Unilocular Radiolucencies
- Angiomas
- Cysts:
- Dentigerous
- Lateral periodontal
- Odontogenic tumor (e.g., AOT)
- Nasopalatine
- Radicular
- Residual
- Solitary bone
- Stafne cavity - Odontogenic Fibroma
- Neoplasms
Multilocular Radiolucencies
- Angiomas
- Giant cell lesions
- Odontogenic tumors:
- Ameloblastoma
- Ameloblastic fibroma
- CEOT (Calcifying epithelial odontogenic tumor)
- KCOT (Keratocystic odontogenic tumor)
- Myxoma
Terminology Reference
-
AOT: Adenomatoid odontogenic tumor
-
CEOT: Calcifying epithelial odontogenic tumor
-
KCOT: Keratocystic odontogenic tumor
-
Well-demarcated: Clearly defined margins (common in cysts).
-
Ill-defined: Ragged borders (often suggestive of aggressive or malignant processes).
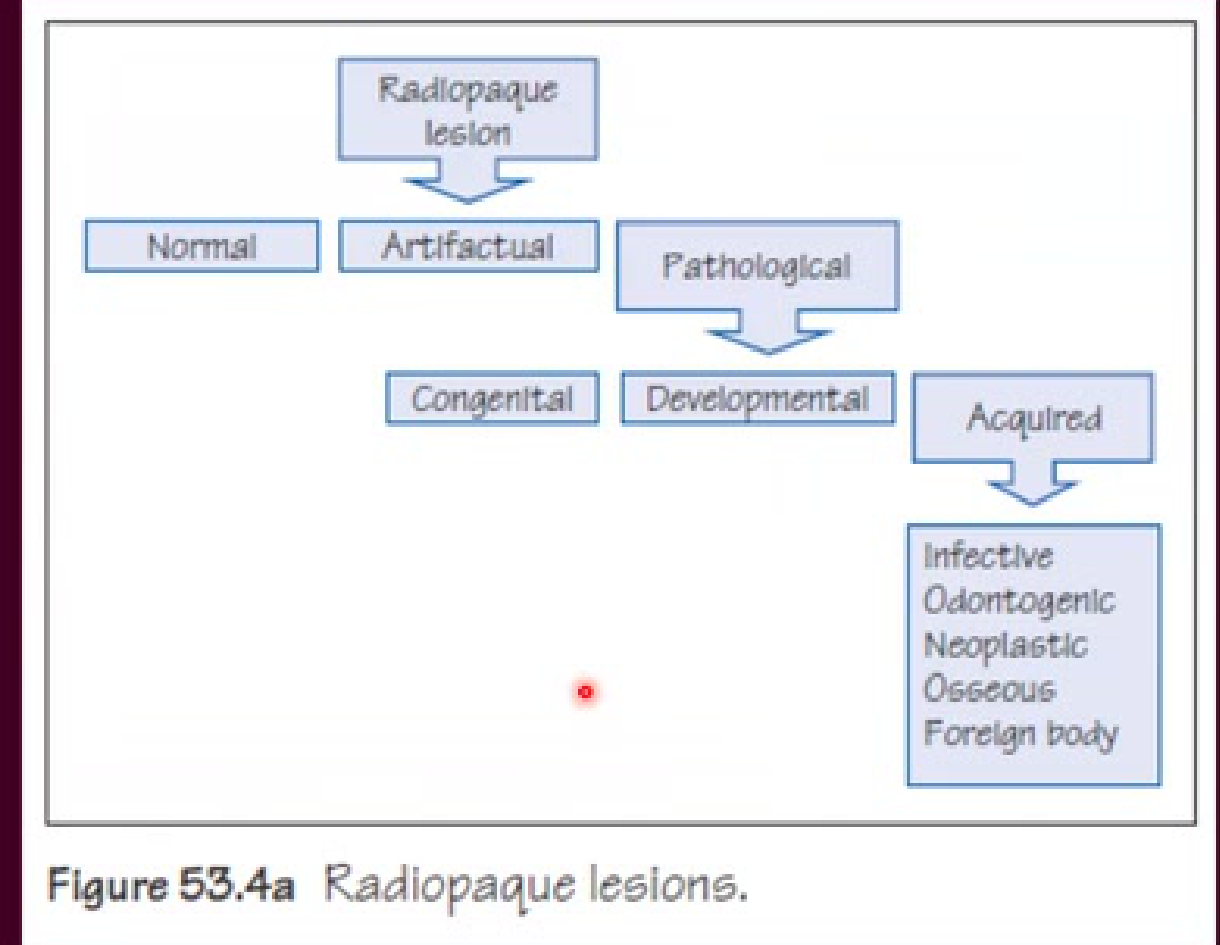
Classification of Radiopaque Lesions
Categorization of Radiopaque Lesions15
Radiopaque lesions are classified according to their etiology and clinical presentation:
- Normal anatomical structures
- Artifactual findings
- Pathological conditions
- Congenital
- Developmental
- Acquired:
- Congenital: Present at birth
- Developmental: Appearing at a young age (often genetic)
- Acquired: Resulting from infection, trauma, cysts, or neoplasia (benign/malignant)
- Infective
- Odontogenic
- Neoplastic
- Osseous
- Acquired causes include infections (e.g., condensing osteitis), tumors, or the presence of foreign bodies.
- Foreign body
Tori and Exostosis
These are localized, non-neoplastic overgrowths of mature lamellar bone.
Prevalence and Presentation16
- Tori affect approximately 2-10% of the adult population.
- Clinically, they present as exophytic, hard, bony masses.
- These masses can be uninodular or multinodular.
- They are covered by mucosa, which may show signs of ulceration resulting from trauma.
Common Locations
- Torus Palatinus: Located on the midline of the palate.
- Torus Mandibularis: Located on the lingual aspect of the mandible, usually presenting bilaterally and symmetrically.
- they are often sites of bisphosphonate-associated osteonecrosis
Clinical Features of Tori17
 |  |
 |
Clinical Considerations
- Tori are often identified as sites for the development of bisphosphonate-associated osteonecrosis.
- Prosthetics: Tori can interfere with the seating of complete dentures, requiring surgical removal or denture modification.
- Medication Risks: Tori are specifically identified as high-risk sites for Bisphosphonate-Related Osteonecrosis of the Jaw (BRONJ).
Clinical Features and Etiology of Exostoses18
 |  |
Prevalence and Clinical Presentation19
- Exostoses affect approximately 27% of adults.
- There is a significant male predilection, with a ratio of 5:1.
- Clinically, they appear as nodular or sessile outgrowths of bone.
- They occur frequently on the buccal aspects of the mandible and maxilla, or along the ascending arch of the palate.
- More than 90% of cases occur concurrently with tori.
Possible Etiology
- Chronic irritation
- Periosteal proliferation
- Bone formation
Extreme Exostosis
The lecturer presented a case of an unusual exostosis that had grown to an extremely large size, far exceeding the typical small nodules seen in general practice, illustrating the potential for significant growth under certain stimuli.
- Unlike tori (which are primarily developmental), exostoses are often attributed to external stimuli, such as trauma.
Footnotes
-
Original PDF page 1: L17 Bone disease 1 slides, p.1 ↩
-
Original PDF page 2: L17 Bone disease 1 slides, p.2 ↩
-
Original PDF page 4: L17 Bone disease 1 slides, p.4 ↩
-
Original PDF page 3: L17 Bone disease 1 slides, p.3 ↩
-
Original PDF page 5: L17 Bone disease 1 slides, p.5 ↩
-
Original PDF page 6: L17 Bone disease 1 slides, p.6 ↩
-
Original PDF page 10: L17 Bone disease 1 slides, p.10 ↩
-
Original PDF page 7: L17 Bone disease 1 slides, p.7 ↩
-
Original PDF page 8: L17 Bone disease 1 slides, p.8 ↩
-
Original PDF page 9: L17 Bone disease 1 slides, p.9 ↩
-
Original PDF page 11: L17 Bone disease 1 slides, p.11 ↩
-
Original PDF page 12: L17 Bone disease 1 slides, p.12 ↩
-
Original PDF page 13: L17 Bone disease 1 slides, p.13 ↩
-
Original PDF page 14: L17 Bone disease 1 slides, p.14 ↩
-
Original PDF page 15: L17 Bone disease 1 slides, p.15 ↩
-
Original PDF page 16: L17 Bone disease 1 slides, p.16 ↩
-
Original PDF page 17: L17 Bone disease 1 slides, p.17 ↩
-
Original PDF page 19: L17 Bone disease 1 slides, p.19 ↩
-
Original PDF page 18: L17 Bone disease 1 slides, p.18 ↩