Osteomyelitis and Related Bone Conditions123
Osteomyelitis is an infection of the bone that can be caused by a variety of microbial agents, typically resulting in inflammation and bone destruction.
Osteomyelitis
Osteomyelitis of the Jaws
Definition and Predisposing Factors
Definition of Osteomyelitis4
Osteomyelitis is an inflammatory condition of the bone that begins as an infection of the medullary cavity. It rapidly involves the Haversian systems and extends to involve the periosteum of the affected area.
-
It typically initiates as an infection of the bone marrow.
-
Prevalence: Approximately 2 out of every 10,000 people develop osteomyelitis.
Predisposing Factors5
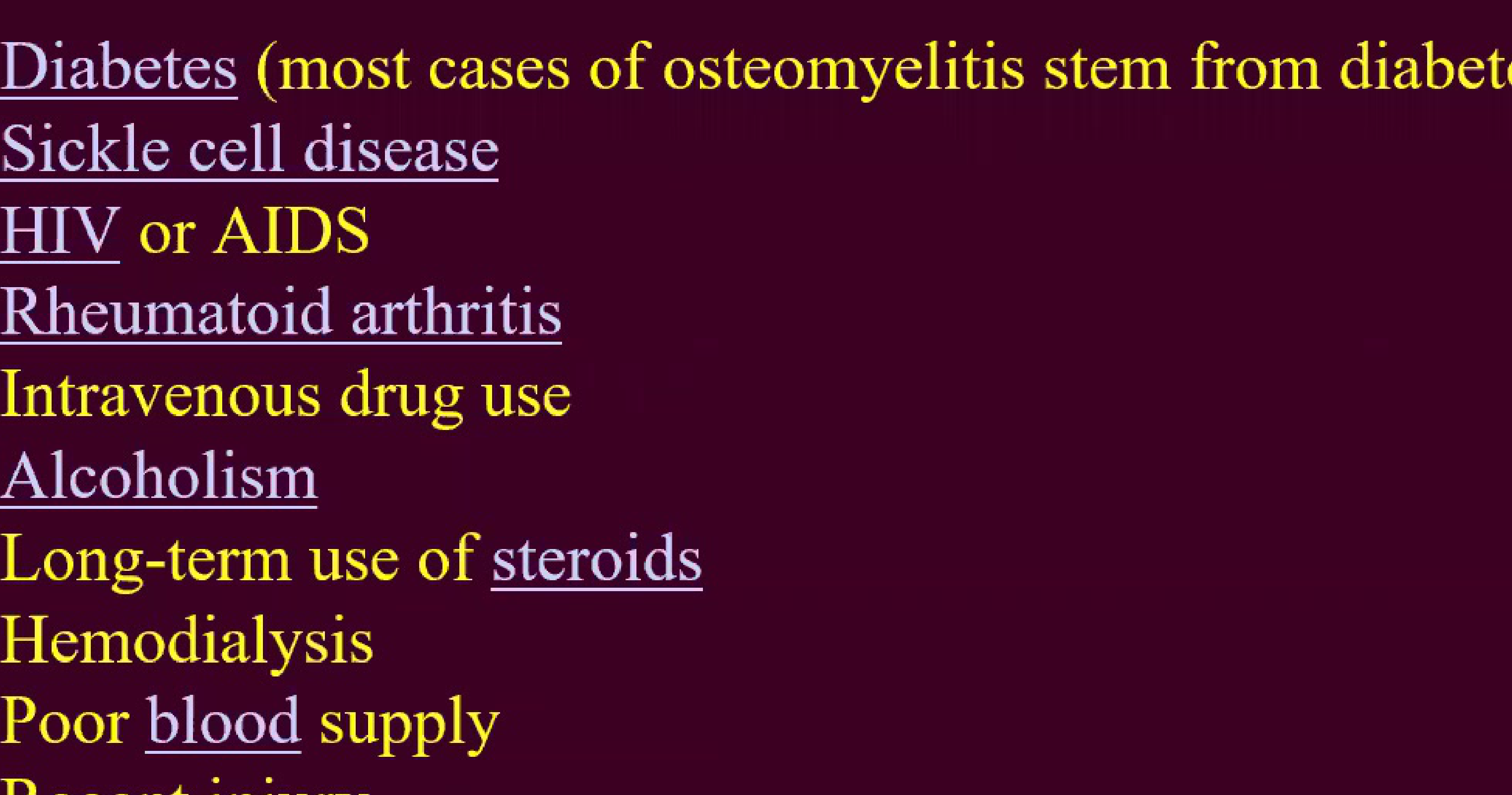
Various systemic conditions and lifestyle factors can increase the risk of developing osteomyelitis:
- Diabetes: The primary cause in most cases of osteomyelitis.
- Immune System Deficiencies: HIV or AIDS, and long-term use of steroids.
- Chronic Conditions: Rheumatoid arthritis, sickle cell disease, and hemodialysis.
- Lifestyle and Substance Use: Alcoholism and intravenous drug use.
- Local Factors: Poor blood supply and recent injury.
Etiology and Clinical Presentation
Potential Sources of Infection6
Infection in the jaws typically originates from the following sources:
- Periapical infection
- Periodontal pockets
- Acute gingivitis
- Penetrating and contaminated injuries
- Open mandibular fractures (penetrating or contaminated injuries).
- Tooth extraction
Signs and Symptoms7
Clinical presentation of osteomyelitis often includes:
- Systemic Symptoms: Fever, irritability, fatigue, and nausea.
- Local Inflammation: Tenderness, redness, and warmth in the area of infection.
- Physical Changes: Swelling around the affected bone and lost range of motion.
- Advanced signs: Presence of bone sequestra (dead bone) which may exhibit motion.
Classification and Pathogenesis
Clinical Classification8
Osteomyelitis is classified based on the duration and nature of the inflammatory process:
- Acute Osteomyelitis: Primarily affects children; the acute process occurs up to one month after the onset of symptoms.
- Chronic Osteomyelitis: Primarily affects adults and is subdivided into:
- Primary Chronic Osteomyelitis (PCO): Defined as chronic non-suppurative osteomyelitis. When occurring in children and adolescents, it is termed “Garré’s osteomyelitis.”
- Secondary Chronic Osteomyelitis (SCO): Chronic osteomyelitis characterized by suppuration, abscess or fistula formation, and sequestration, resulting from a defined infectious etiology.
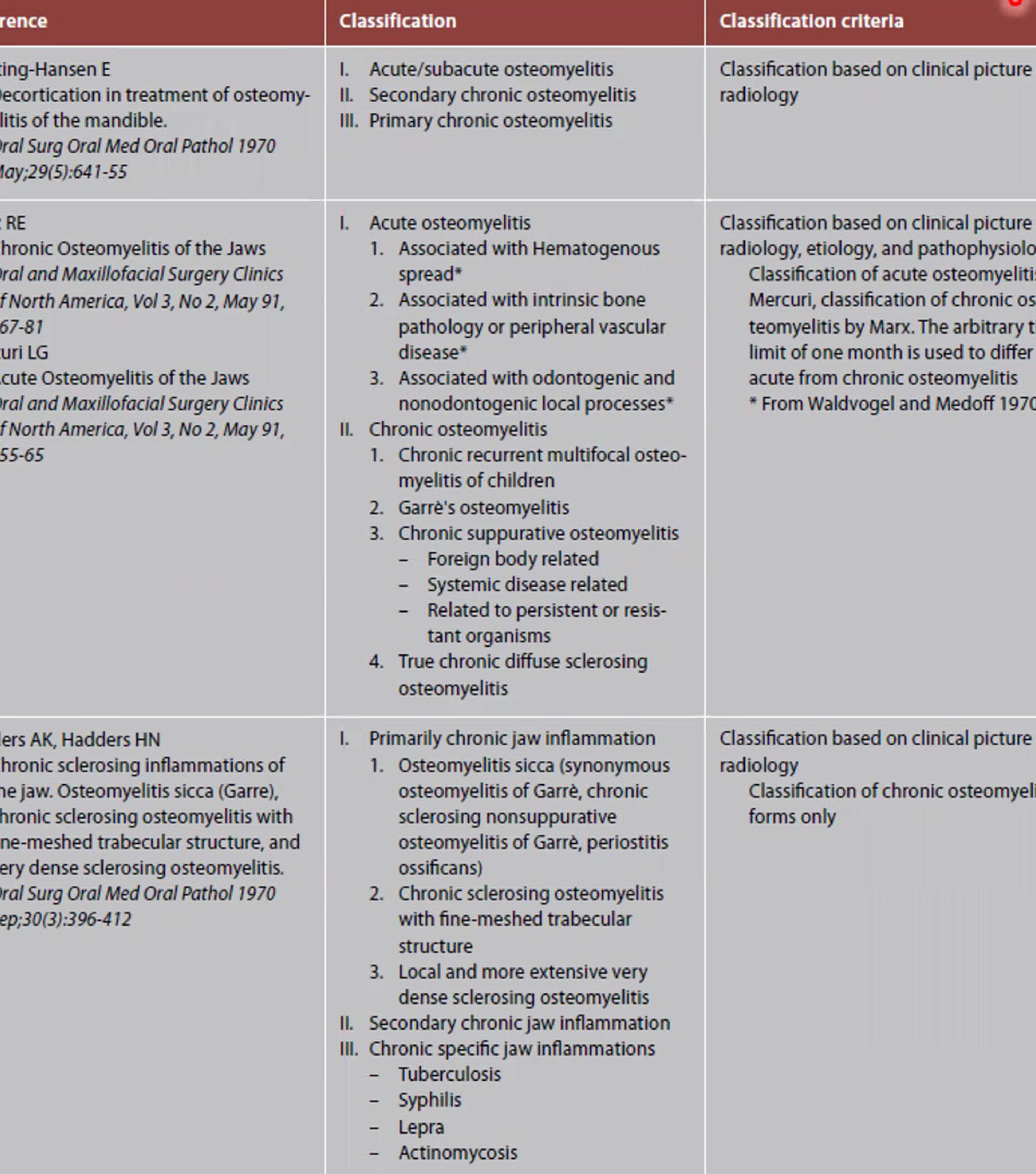
Historical Classification Systems9
| Reference | Classification Categories | Criteria and Notes |
|---|---|---|
| Hjorting-Hansen (1970) | I. Acute/subacute II. Secondary chronic III. Primary chronic | Based on clinical picture and radiology. |
| Marx & Mercuri (1991) | I. Acute: Hematogenous spread, intrinsic bone pathology/vascular disease, or odontogenic/nonodontogenic processes. II. Chronic: Recurrent multifocal (children), Garre’s, Suppurative (foreign body, systemic, or resistant organisms), and True chronic diffuse sclerosing. | Based on clinical picture, radiology, etiology, and pathophysiology. Uses a one-month threshold to differentiate acute from chronic. |
| Panders & Hadders (1970) | I. Primarily chronic: Osteomyelitis sicca (Garre’s), fine-meshed trabecular structure, or dense sclerosing. II. Secondary chronic. III. Chronic specific: Tuberculosis, Syphilis, Lepra, Actinomycosis. | Focuses on chronic forms based on clinical and radiological presentation. |
Disease Progression Timeline10
The progression of the condition follows a specific sequence:
- Onset of Disease: Deep bacterial invasion into the medullary and cortical bone.
- Acute Osteomyelitis: Clinical manifestation following the initial invasion.
Progression to Chronic
If the infection is not treated or fails to respond to treatment within four weeks, it transforms into the chronic type.

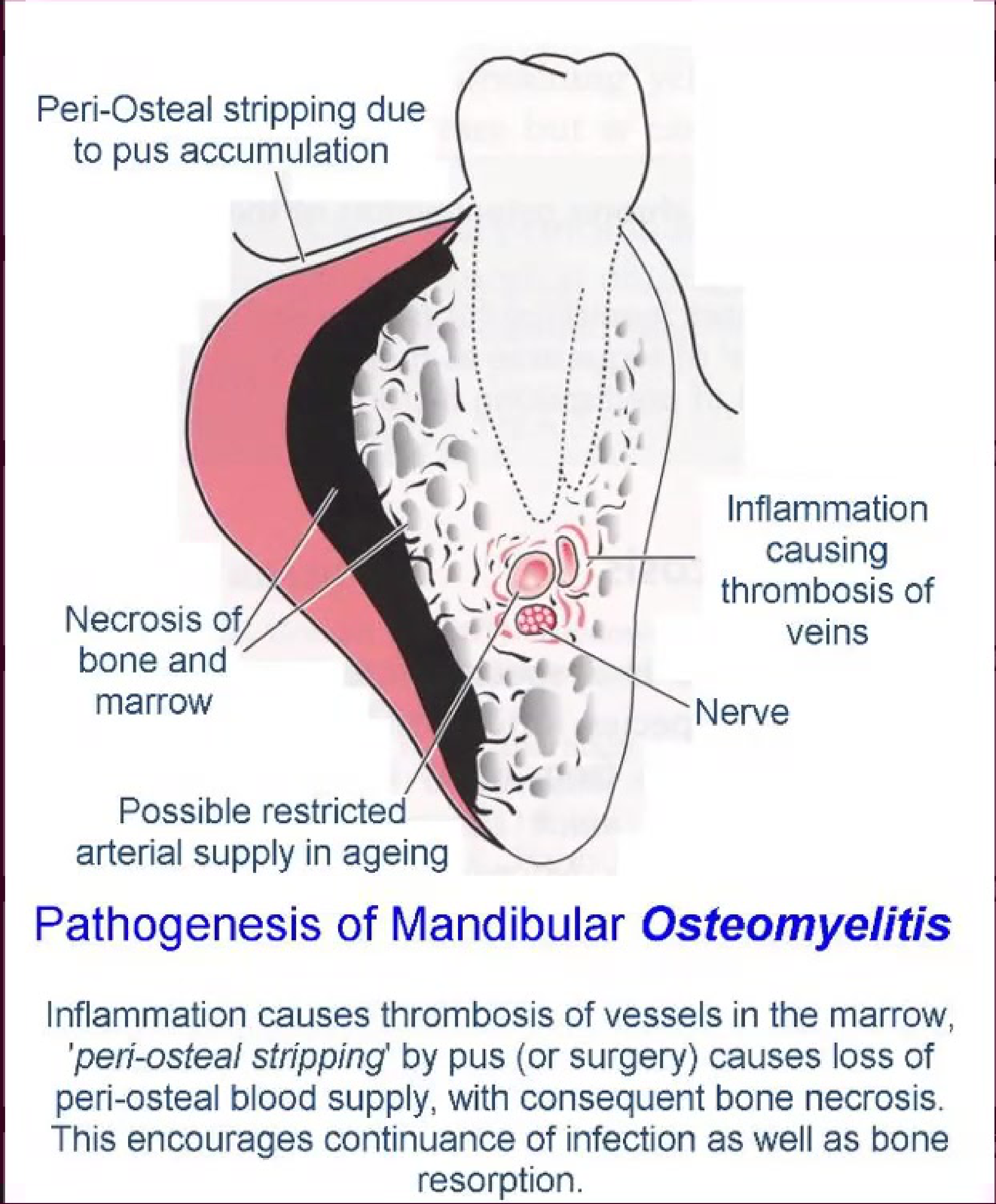
Pathogenesis of Mandibular Osteomyelitis11
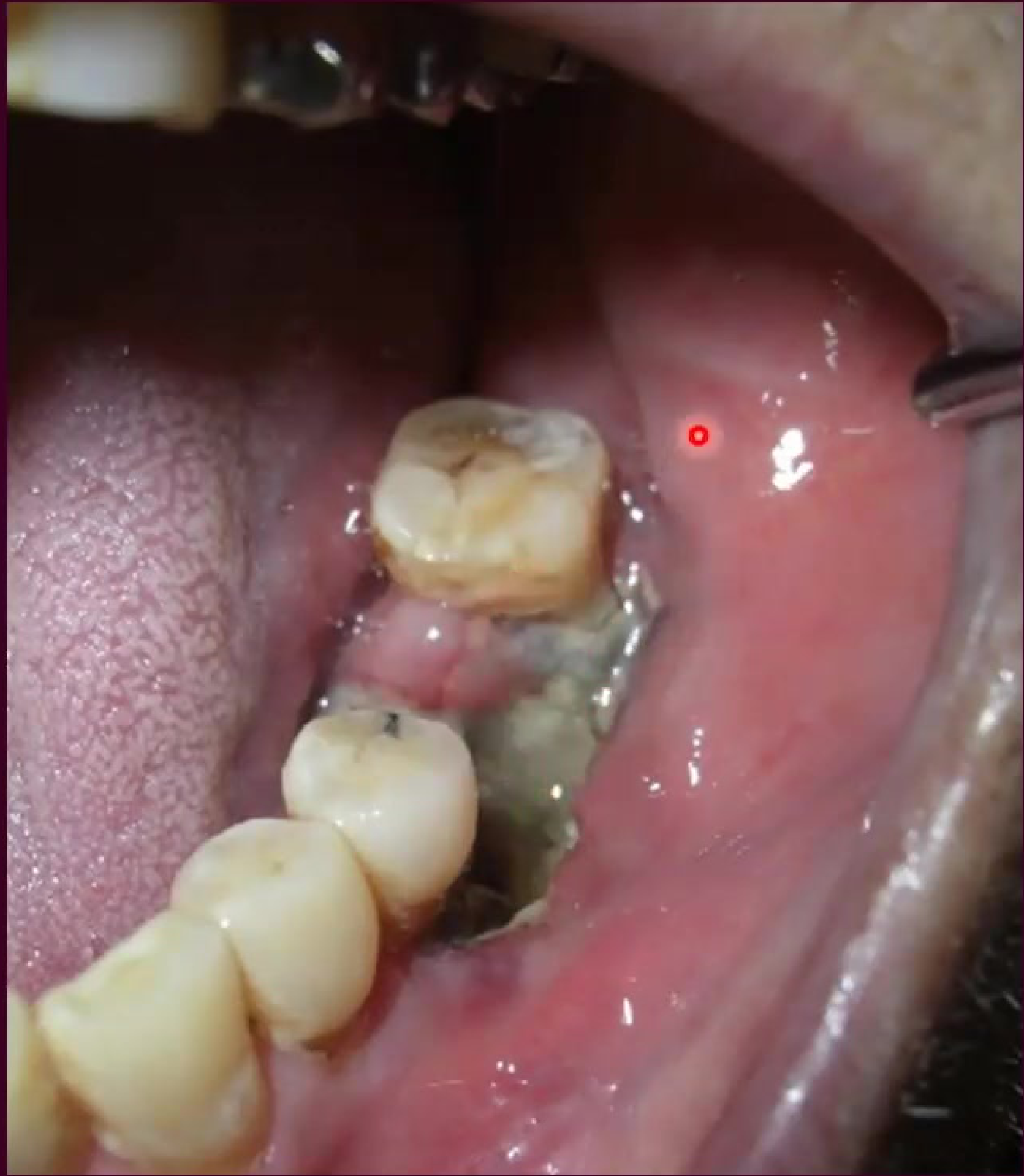
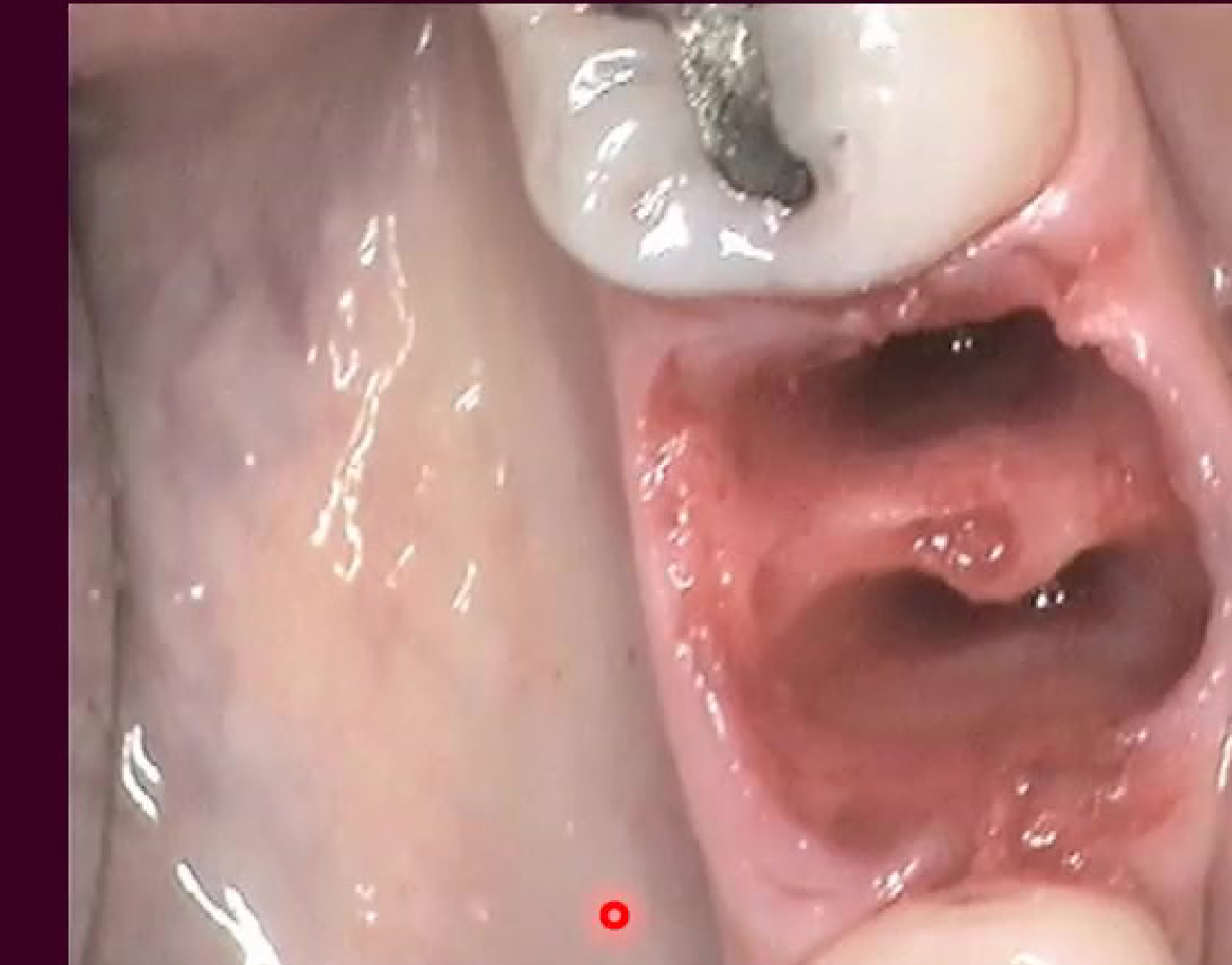
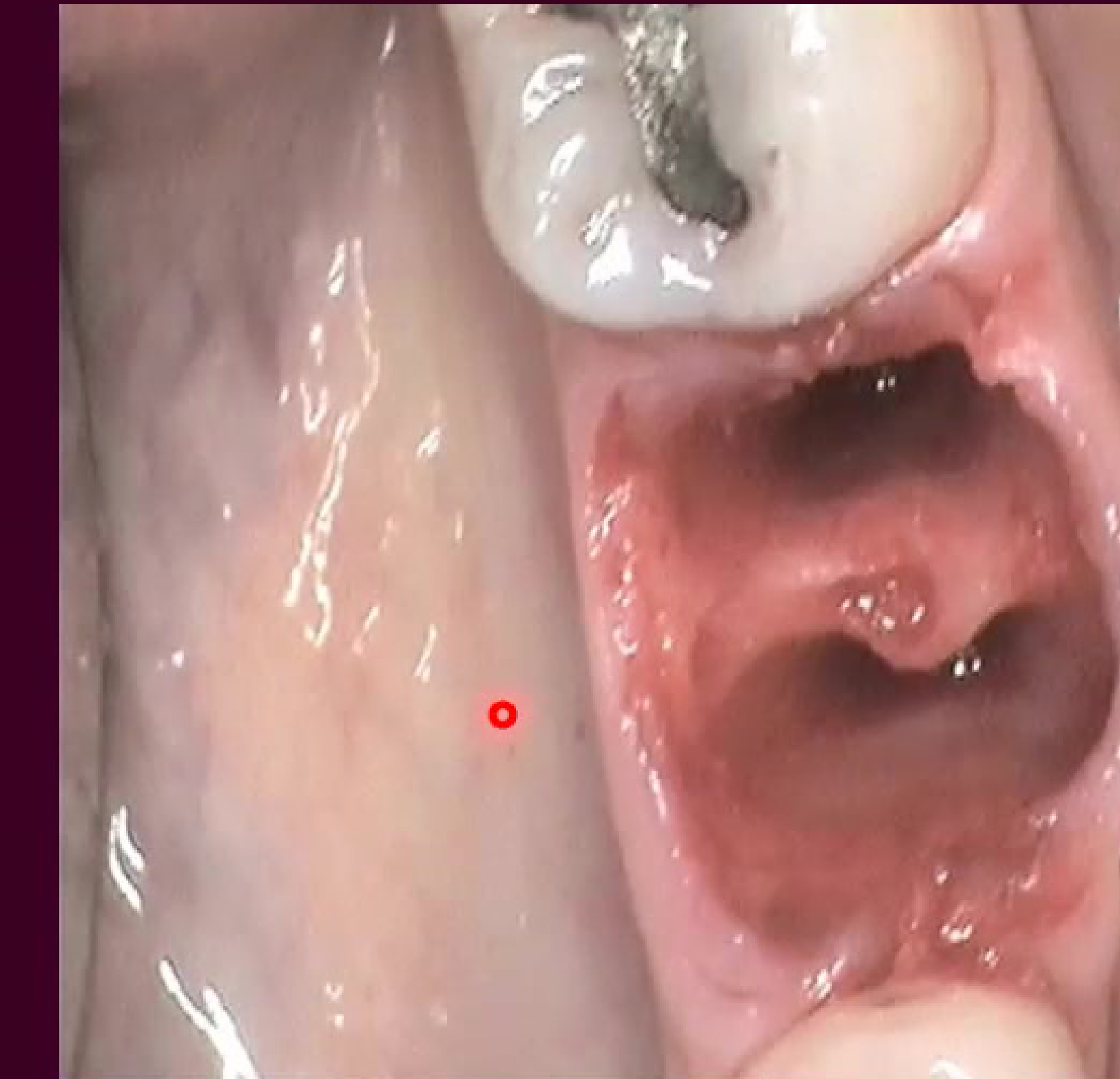
The pathogenesis involves the spread of infection through the medullary spaces of the mandible, leading to inflammation and potential bone necrosis. Clinical presentation often shows significant swelling and intraoral or extraoral involvement.
Mandibular vs. Maxillary Pathogenesis
The mandible is more susceptible to necrosis than the maxilla due to its denser bone structure, differences in marrow spaces, and a more limited, centrifugal blood supply. Clinical appearance often includes mucosal ulceration, exposed bone, necrotic tissue, and the formation of granulation tissue.
 |  |
Alveolar Osteitis
Definition and Overview12
Alveolar osteitis, commonly known as “Dry Socket,” is a localized inflammation of the bone. It occurs following the failure of a blood clot to form in the extraction socket, or the premature loss/disintegration of that clot.
- Incidence: It is an unpredictable complication occurring in approximately 1–3% of tooth extractions.
 |  |
Etiology and Clinical Features
Etiological Factors13
-
Failure of Blood Clot Formation: Often due to poor blood supply associated with:
- Paget’s disease
- Osteopetrosis
- History of radiotherapy
- Excessive use of vasoconstrictors in local anesthesia
-
Premature Loss of Blood Clot: May be caused by:
- Excessive mouth rinsing
- Fibrinolysis triggered by proteolytic bacteria
- Spitting or smoking within 24 hours post-op
- Bacterial enzymes leading to fibrinolysis
Clinical Features14
- Pain: Intense, localized pain.
- Pain typically appears a few days post-extraction
- Most common in mandibular third molars
- Risk Groups: Most frequently observed in 3rd molar extractions, difficult/traumatic extractions, and smokers.
- Physical Appearance: The tooth socket appears empty and dry; the underlying jaw bone is often visible.
- Associated Symptoms: Bad breath (halitosis), unpleasant taste, and swelling of regional lymph nodes.
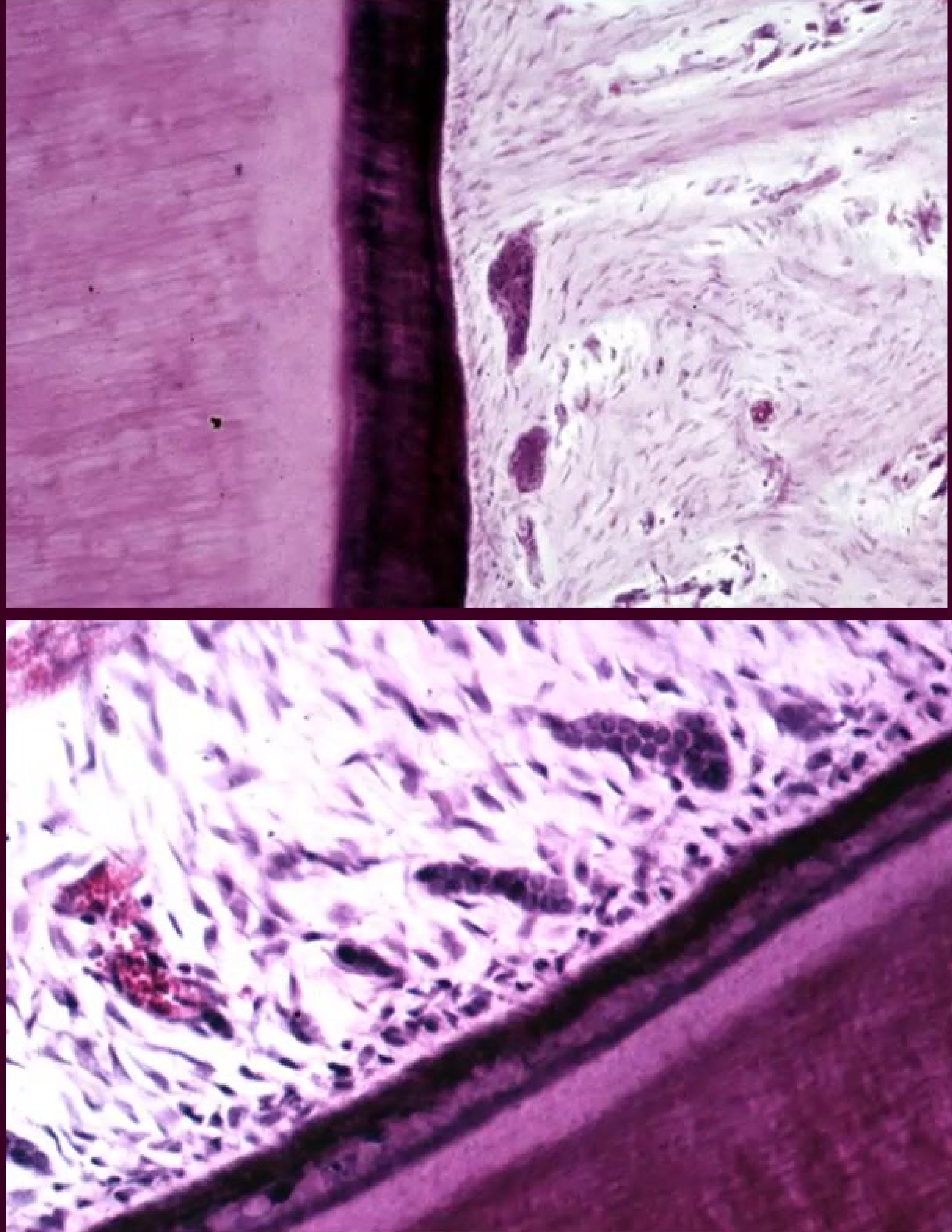
Histopathology of Dry Socket
Histological Characteristics15
Histological sections of the socket wall in alveolar osteitis reveal the formation of necrotic bone. A key diagnostic feature is the presence of empty lacunae within the bone tissue.
Diagnostic Note
The empty lacunae observed in histological sections indicate an absence of osteocytes, confirming the presence of necrotic bone.
Osteonecrosis
Types of Osteonecrosis16
- Osteoradionecrosis: Bone death resulting from radiation therapy.
- Osteochemonecrosis: Induced by corticosteroids and other antineoplastic drugs.
- MRONJ: Medication-related osteonecrosis of the jaw.
- BRONJ: Bisphosphonate-induced osteonecrosis of the jaw.
- Phosphorous Necrosis: Also known as “phossy jaw,” caused by exposure to white phosphorous.
Osteoradionecrosis
Pathological Concepts17
- Radiation Context: Primarily associated with radiotherapy for Head and Neck Squamous Cell Carcinoma (HNSCC).
- Historical View: Historically viewed as an infection initiated by bacteria invading radiation-damaged bone.
- Terminology: The term “radiation-induced osteomyelitis” or “radioosteomyelitis” was commonly utilized (Marx, 1983).
Pathogenesis Factors18
- HNSCC Treatment: Radiation exposure.
- Bone Changes: Development of hypoxia, hypocellularity, and hypovascularity.
-
- Trauma: Leads to chronic non-healing wounds that are highly susceptible to superinfection.
The 3-H Environment
This "3-H" environment results in low-quality bone that cannot heal following trauma, leading to superinfection and necrosis.
Medication-Related Osteonecrosis of the Jaw
Bisphosphonate-Related Osteonecrosis (BRONJ)19
Bisphosphonates are commonly prescribed for the management of:
- Osteoporosis
- Multiple myeloma
- Metastatic cancer
Biologic Action of Bisphosphonates
Mechanisms of Action
Bisphosphonates exert their effects through osteoclastic toxicity and altered bone dynamics:
- Osteoclast Impact: Induction of apoptosis and inhibition of the release of bone induction proteins (BMP, ILG1, ILG2).
- Bone Turnover: Reduced resorption and overall turnover.
- Mineralization Effects:
- Reduced serum calcium (therapeutic goal).
- Hypermineralization, leading to “sclerotic” changes in the lamina dura of alveolar bone.
- Hyper-mineralization and sclerosis of bone significantly reduces blood supply.
Cellular Interaction
The biological action involves the inhibition of osteoclasts (affecting proton pumps and HCl release), which disrupts the normal chemo-attraction of mesenchymal stem cells and their differentiation into osteoblasts.
Clinical Manifestations
Severe cases may present with gingival necrosis and significant tissue discoloration.
Radiographic Presentation
Panoramic imaging may reveal localized areas of bone density changes or sequestration in the affected jaw regions.
Microscopic Findings
Histological examination typically shows dense bone tissue with irregular cellular regions, consistent with the suppression of normal bone remodeling.
Clinical Guidelines and Management
AAOMS Position Paper Update readings
In the 2014 update, the American Association of Oral and Maxillofacial Surgeons (AAOMS) Special Committee recommended a change in nomenclature from Bisphosphonate-Related Osteonecrosis of the Jaw (BRONJ) to Medication-Related Osteonecrosis of the Jaw (MRONJ).
- Rationale: The change accounts for the increasing number of cases associated with other antiresorptive therapies (such as denosumab) and antiangiogenic therapies.
- Impact: MRONJ significantly affects quality of life and produces substantial morbidity.
- Guidelines: The update reflects expanded knowledge and refinements to the 2009 guidelines for managing patients at risk.
World Workshop on Oral Medicine VI readings
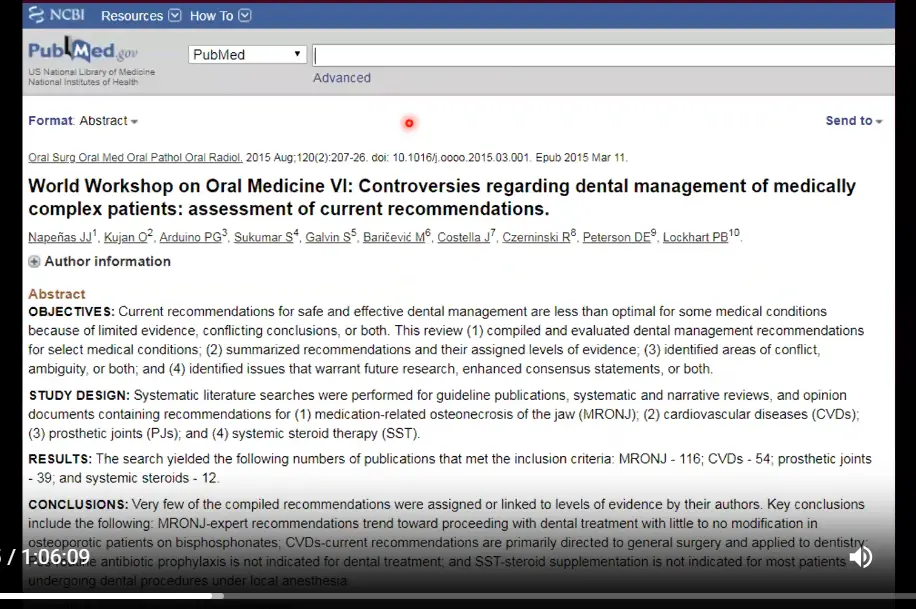
A systematic review was conducted to assess dental management recommendations for medically complex patients, specifically focusing on MRONJ, cardiovascular diseases, prosthetic joints, and systemic steroid therapy.
- MRONJ Findings: Expert recommendations generally trend toward proceeding with dental treatment with little to no modification for osteoporotic patients taking bisphosphonates.
- General Conclusions:
- Routine antibiotic prophylaxis is not indicated for dental treatment in patients with prosthetic joints.
- Steroid supplementation is not required for most patients on systemic steroids undergoing procedures under local anesthesia.
Management Recommendations for Osteoporotic Patients
General Patient Communication:
- Emphasize the importance of maintaining excellent oral hygiene.
- Discuss lifestyle modifications, such as smoking cessation.
- Inform patients of the very rare occurrence of MRONJ.
Risk Factors for MRONJ:
-
Oral Risk Factors:
- Recent dentoalveolar trauma
- Dental extractions or surgery
- Poor oral hygiene and oral infections
- Periodontal disease
-
Systemic Risk Factors:
- High frequency of drug administration and larger doses
- Longer duration of treatment regimens
- History of radiation therapy
- Concomitant corticosteroid therapy
- Immunodeficiency or compromised immune status
- Advanced age and chronic systemic diseases
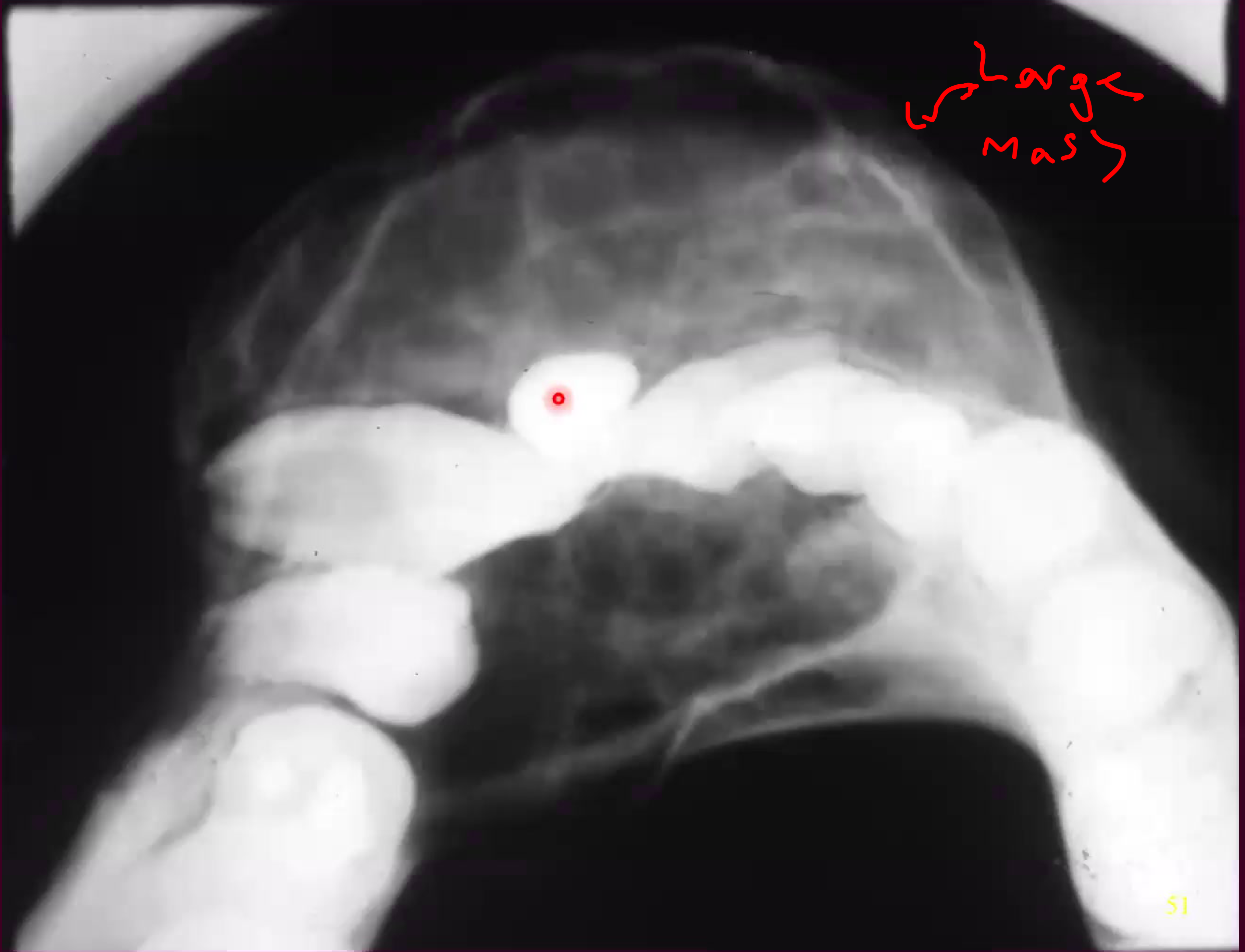
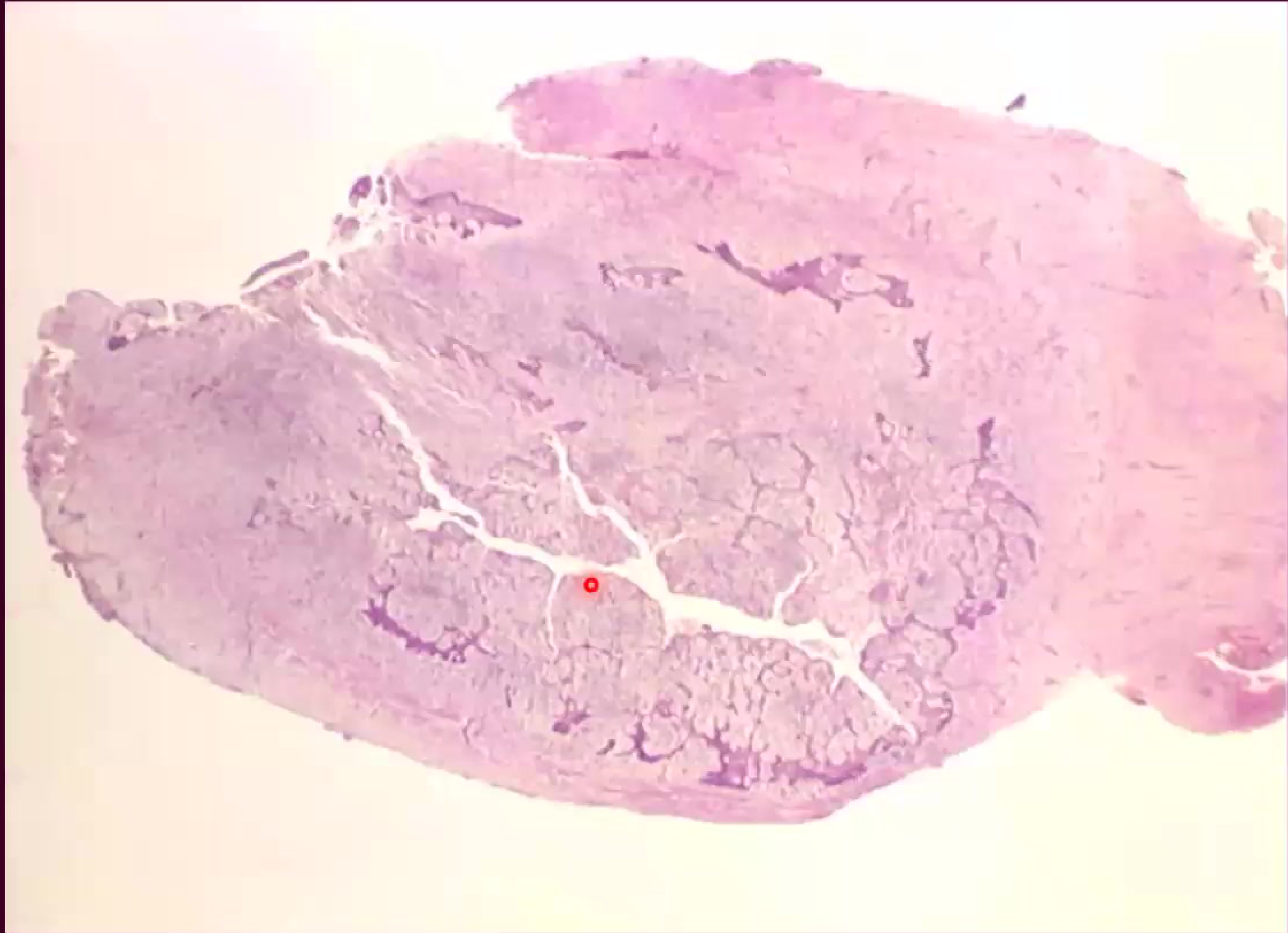
Central Giant Cell Granuloma2021222324
Central Giant Cell Granuloma is a localized benign, but sometimes aggressive, osteolytic proliferation of the jaws.
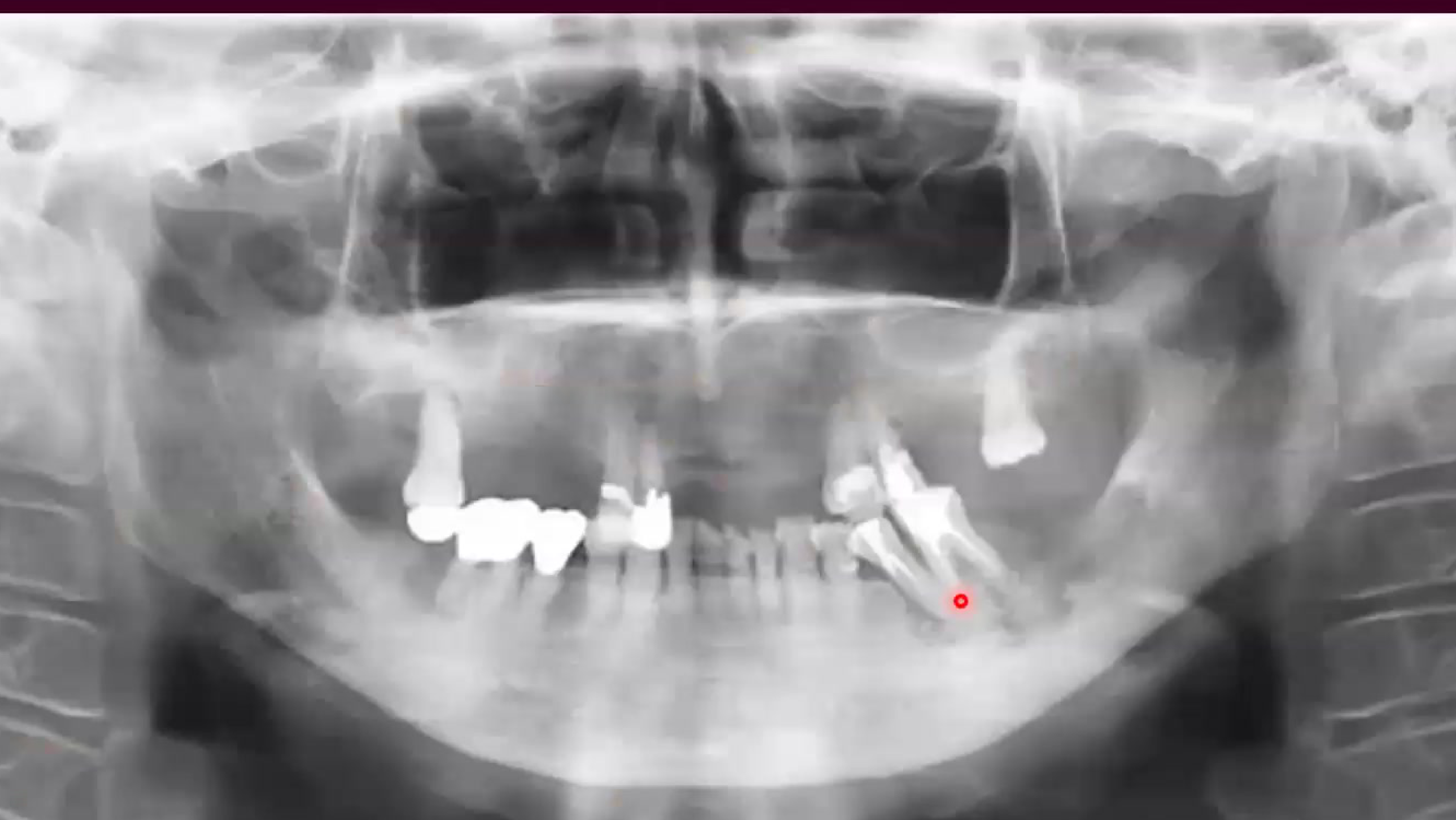
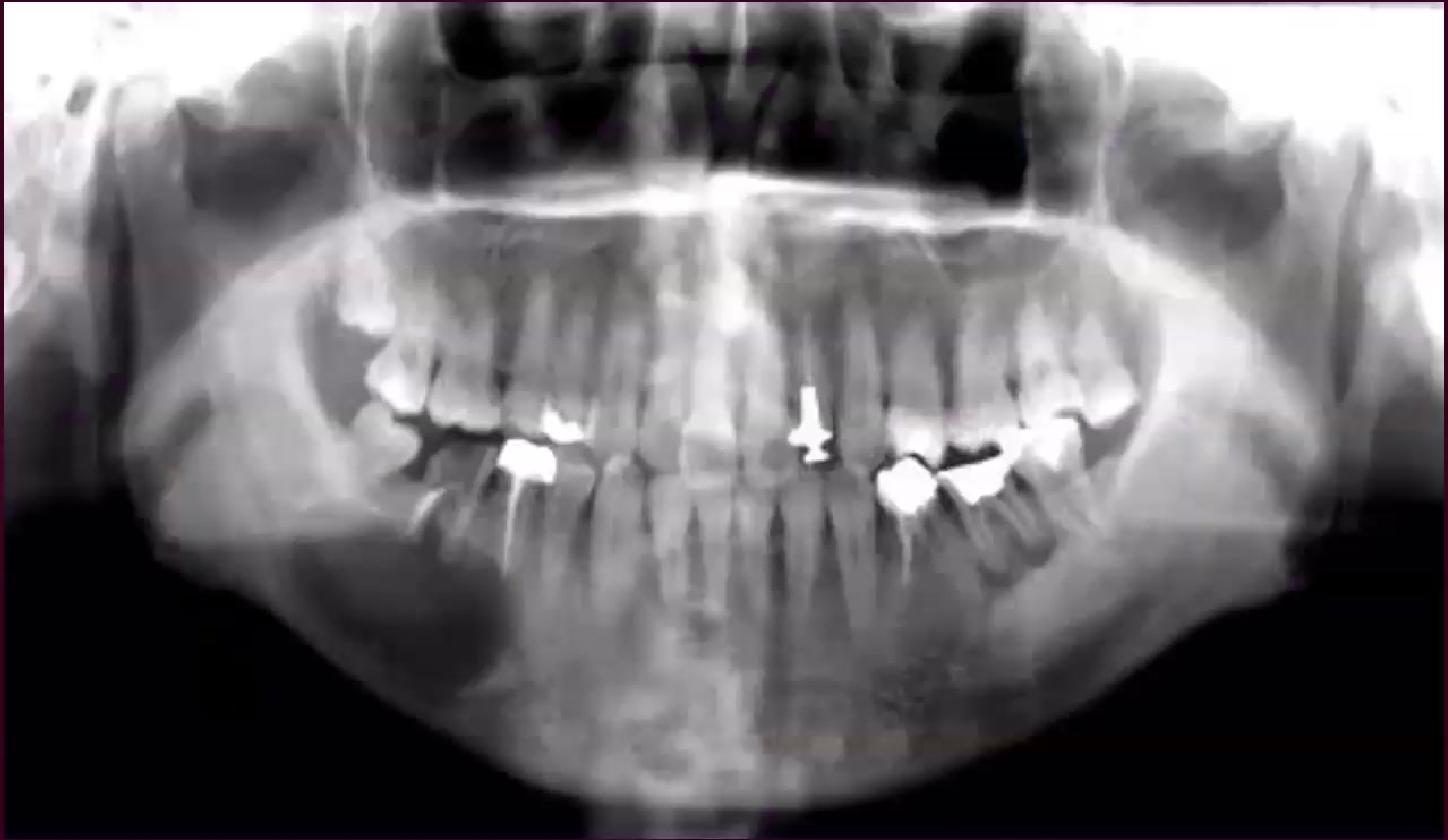
Radiographic examination of the affected dental arches often reveals localized areas of bone alteration, frequently appearing as radiolucent lesions in the mandible or maxilla.
The lesion is characterized by its unique cellular composition and its tendency to occur in specific demographic groups, often presenting as an asymptomatic swelling.
Clinical evaluation is essential to distinguish this reactive process from other more aggressive neoplastic conditions of the bone.
Management strategies vary based on the clinical behavior of the lesion, ranging from conservative surgical intervention to medical therapies.
 |  |
 |  |
Clinical and Radiographic Features
Clinical Characteristics25
- Etiology: Non-neoplastic – reactive lesion
- Age: Wide range (60% occur in patients under 30 years of age)
- Gender: Higher prevalence in females than males
- Site: Predominantly found in the anterior mandible (70% of cases)
- Symptoms: Typically presents as a painless expansion of the bone
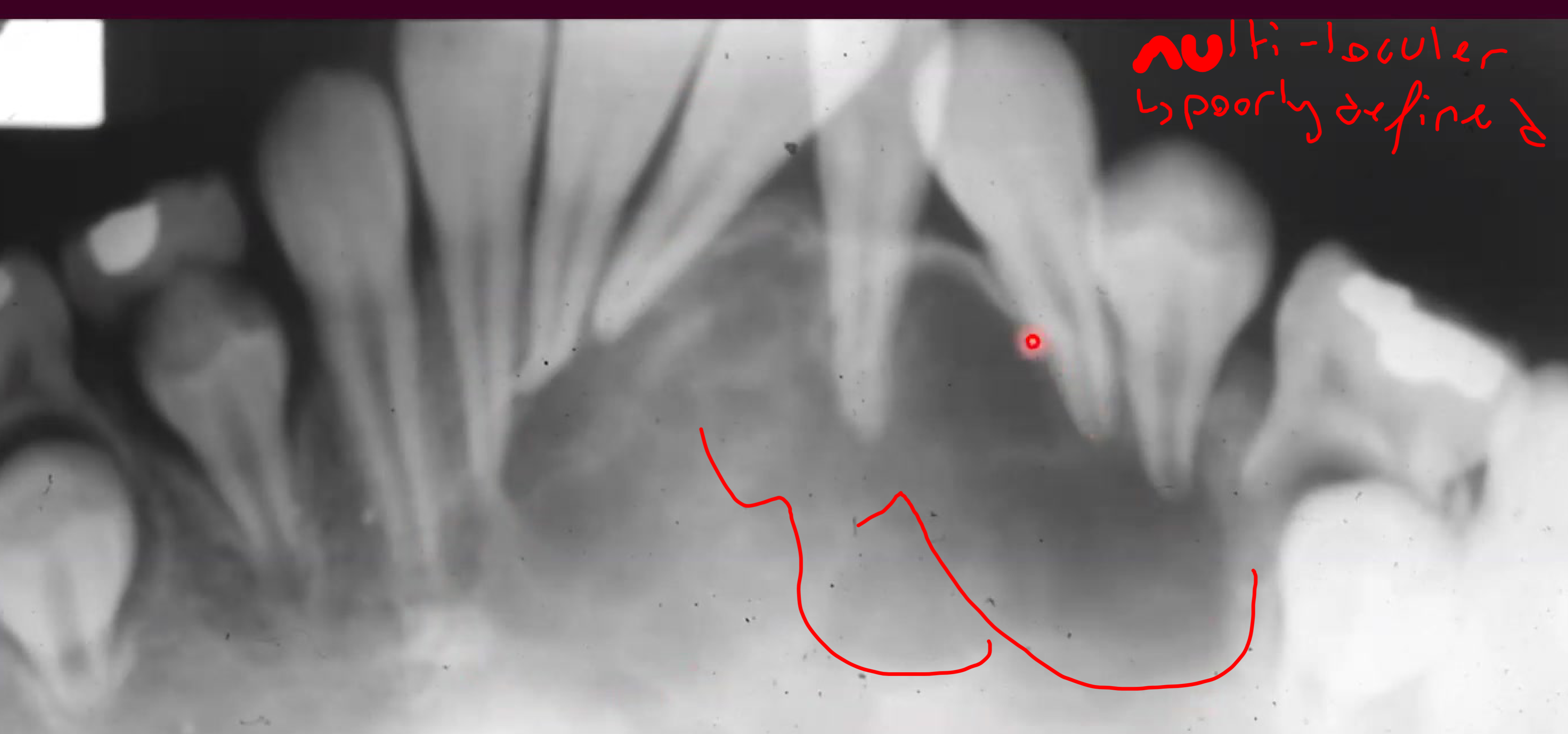
Radiographic Presentation26
- Appearance ranges from unilocular to multilocular radiolucency
- Size varies significantly, typically between 0.5 cm and 10.0 cm
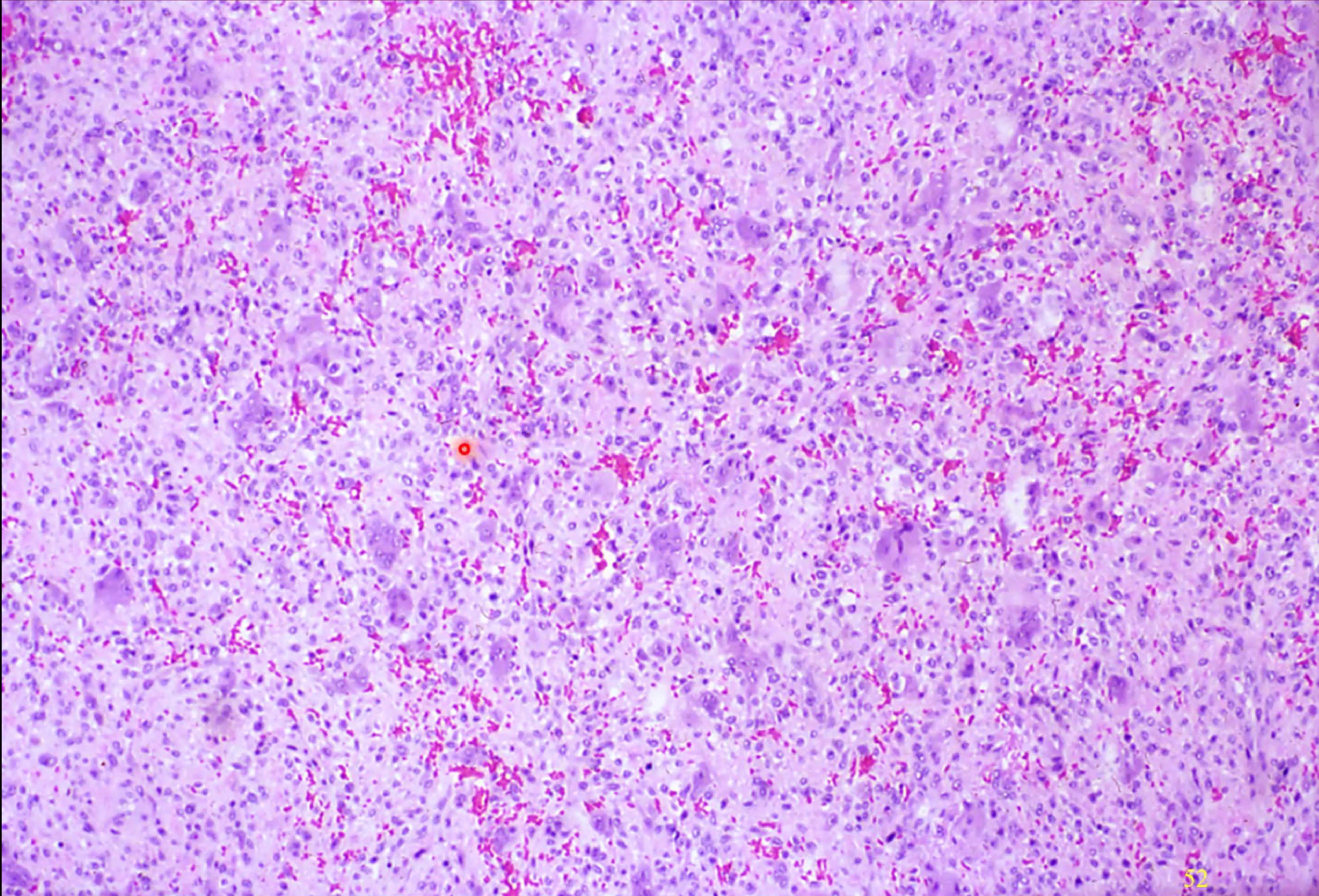
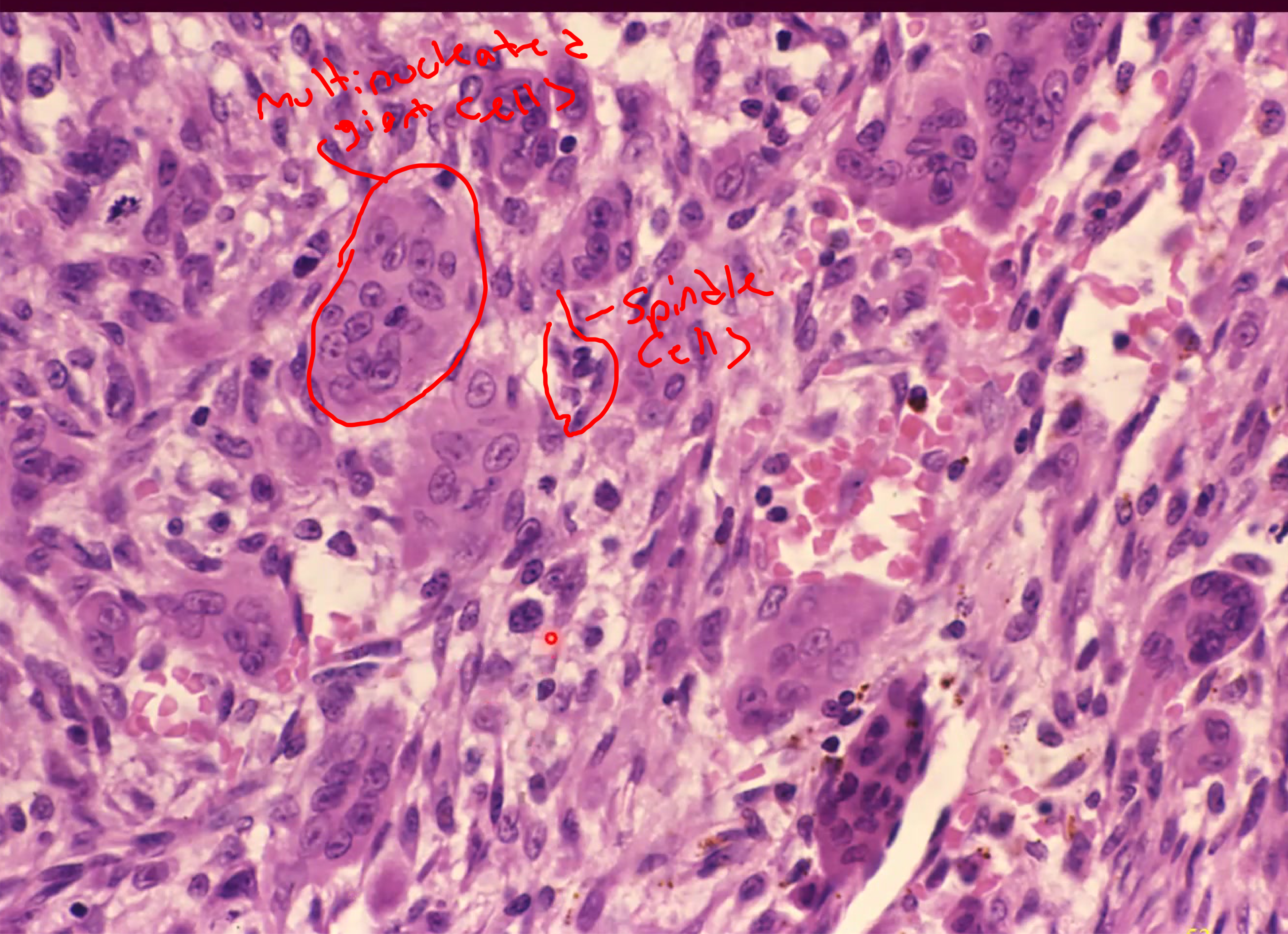
Histology and Treatment
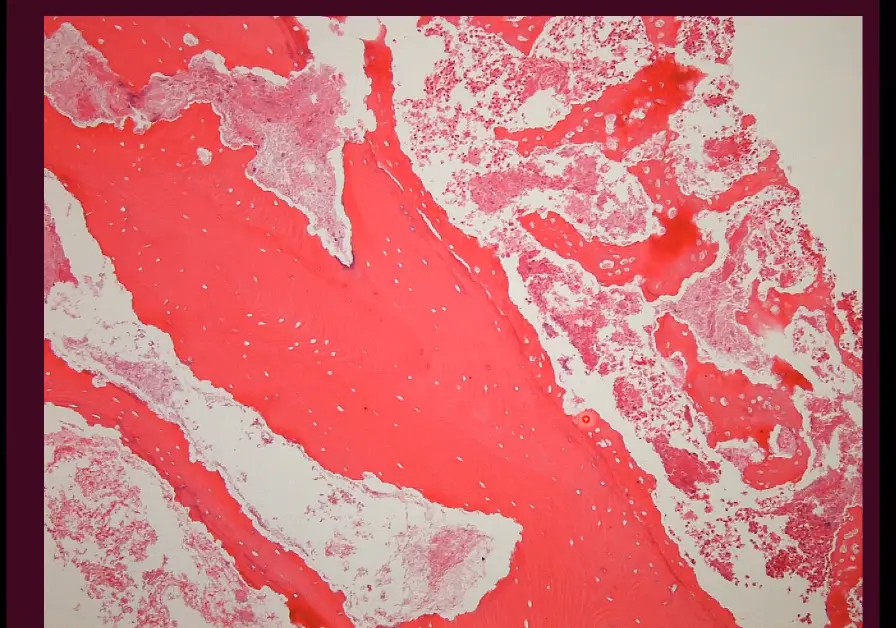
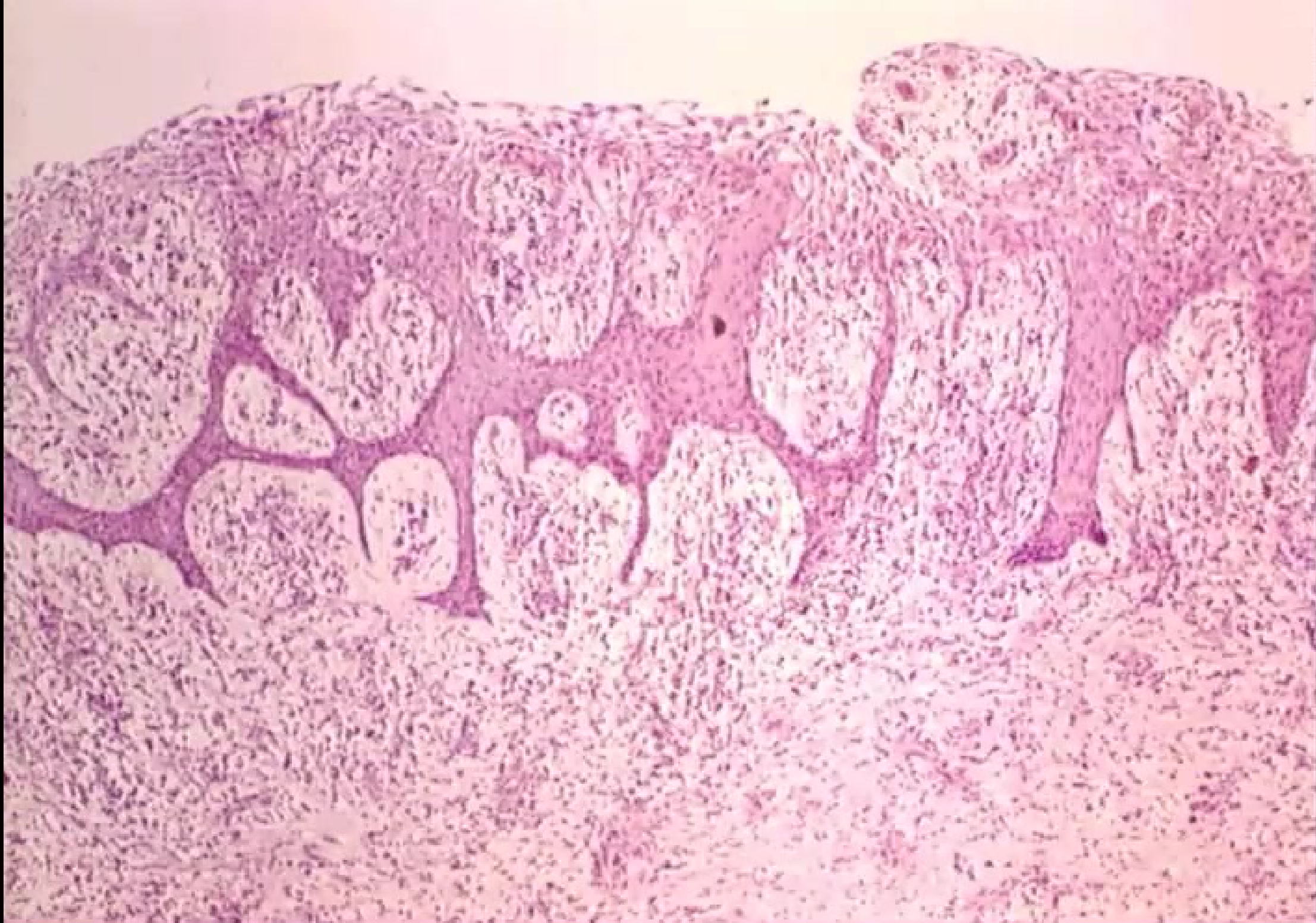
Microscopic Findings27
- Presence of multinucleated giant cells
- Spindled mesenchymal stroma
- Erythrocyte extravasation (bleeding into the tissue)
- Hemosiderin deposits
- Areas of fibrosis
- Evidence of osteoid formation
Treatment Modalities28
- Surgical curettage
- Intra-lesional steroid injections
- Calcitonin therapy
- Interferon alpha 2a
- Surgical resection for more extensive cases
Prognosis and Behavior
- Clinical Behavior: Categorized as either non-aggressive or aggressive
- Recurrence: Observed in approximately 15-20% of cases
Differential Diagnosis and Hyperparathyroidism29
Differential Diagnosis for Giant Cell Lesions30
- Central giant cell granuloma
- Brown tumor associated with hyperparathyroidism
- Aneurysmal bone cyst
- Cherubism
- Giant cell tumor
- Benign fibro-osseous lesion
Hyperparathyroidism and Bone Involvement31
- Brown Tumor: Also known as osteitis fibrosa cystica, this lesion is a bone manifestation of hyperparathyroidism and is histologically indistinguishable from central giant cell granuloma.
Case Study - treating a brown tumour by supplementation
Cysts of the Jaws32
Definition of a cyst: ” A pathological cavity filled with fluid, semi-fluid or gaseious contents and is not created by an accumulation of pus.”
Cysts of the jaws represent a significant category of oral and maxillofacial pathology, often requiring detailed clinical and radiographic assessment for proper diagnosis and management.
General Principles of Cysts
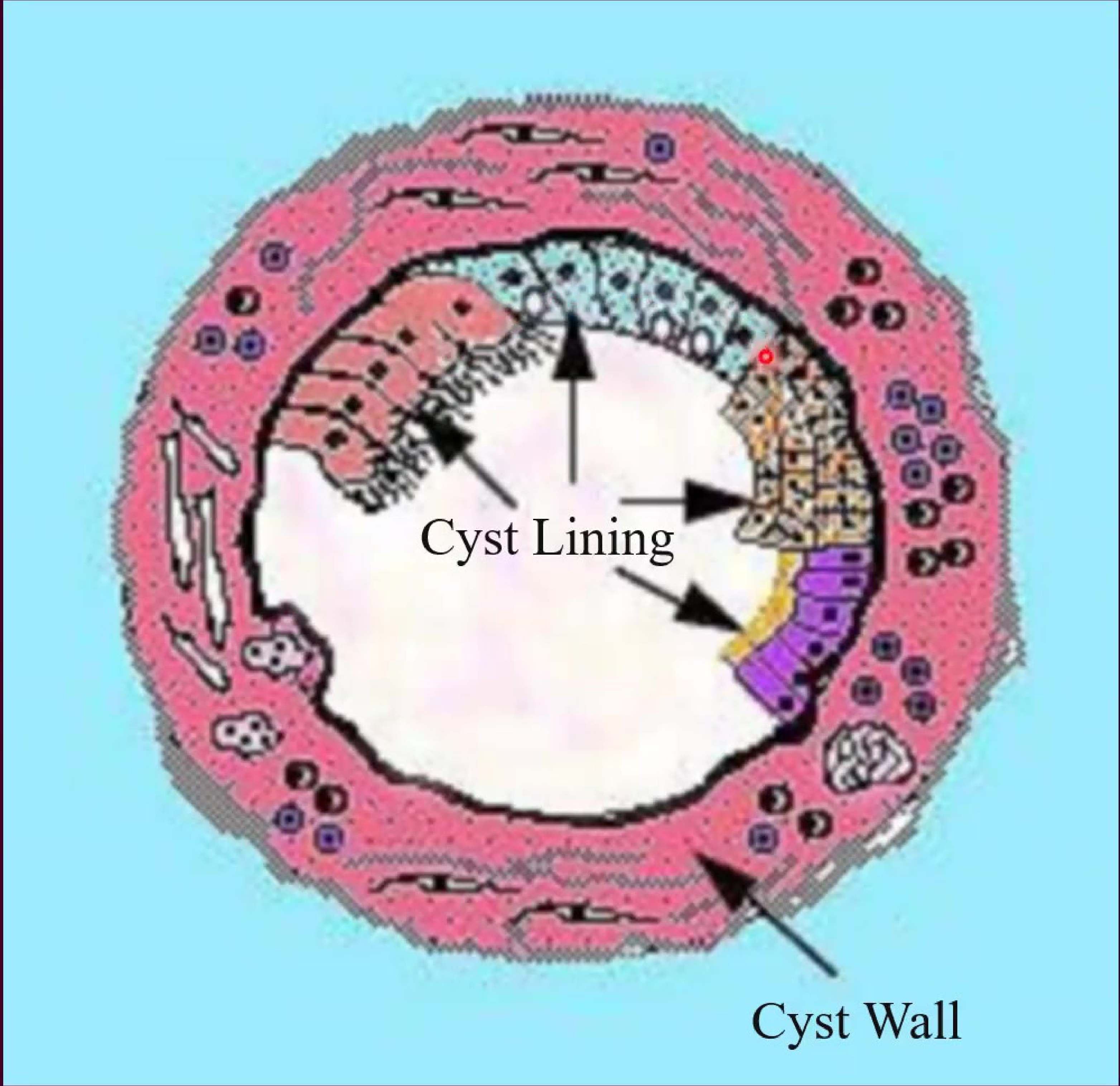
Structural Components of a Cyst33
- Cyst Lining: The inner epithelial layer that characterizes the type of cyst and regulates the passage of fluids.
- Cyst Wall: The outer connective tissue capsule that provides structural integrity and contains the blood supply.
Definition and Distinction
A cyst is a pathological cavity filled with fluid, semi-fluid, or gas (not pus). A true cyst must be lined by epithelium; if no lining is present, it is classified as a pseudocyst.
Aetiology and Classification
Mechanisms of Development34
The growth and expansion of jaw cysts involve several integrated processes:
- Epithelial proliferation: The active multiplication of the epithelial lining.
- Hydrostatic or osmotic factors: Pressure gradients that contribute to the expansion of the cyst lumen.
- Keratin formation: Accumulation of keratinized debris in specific cyst types.
- Bone resorbing factors: The release of substances such as prostaglandins and collagenase that facilitate bone destruction to accommodate cyst growth.
- Degeneration: The center of the epithelial mass loses nutrient supply and undergoes necrosis, forming the initial cavity.
Presentation and Symptoms35
Cysts of the jaws may present with various clinical signs, including:
- Noticeable swelling of the jaw or soft tissues.
- "Eggshell crackling" may be felt on palpation as the overlying bone thins.
- Discharge of cystic contents into the oral cavity.
- Pain, typically occurring as a result of secondary infection.
Diagnosis
- diagnosis of cysts is done through a combination of adequate history, clinical examination and selected investigation (radiographs)
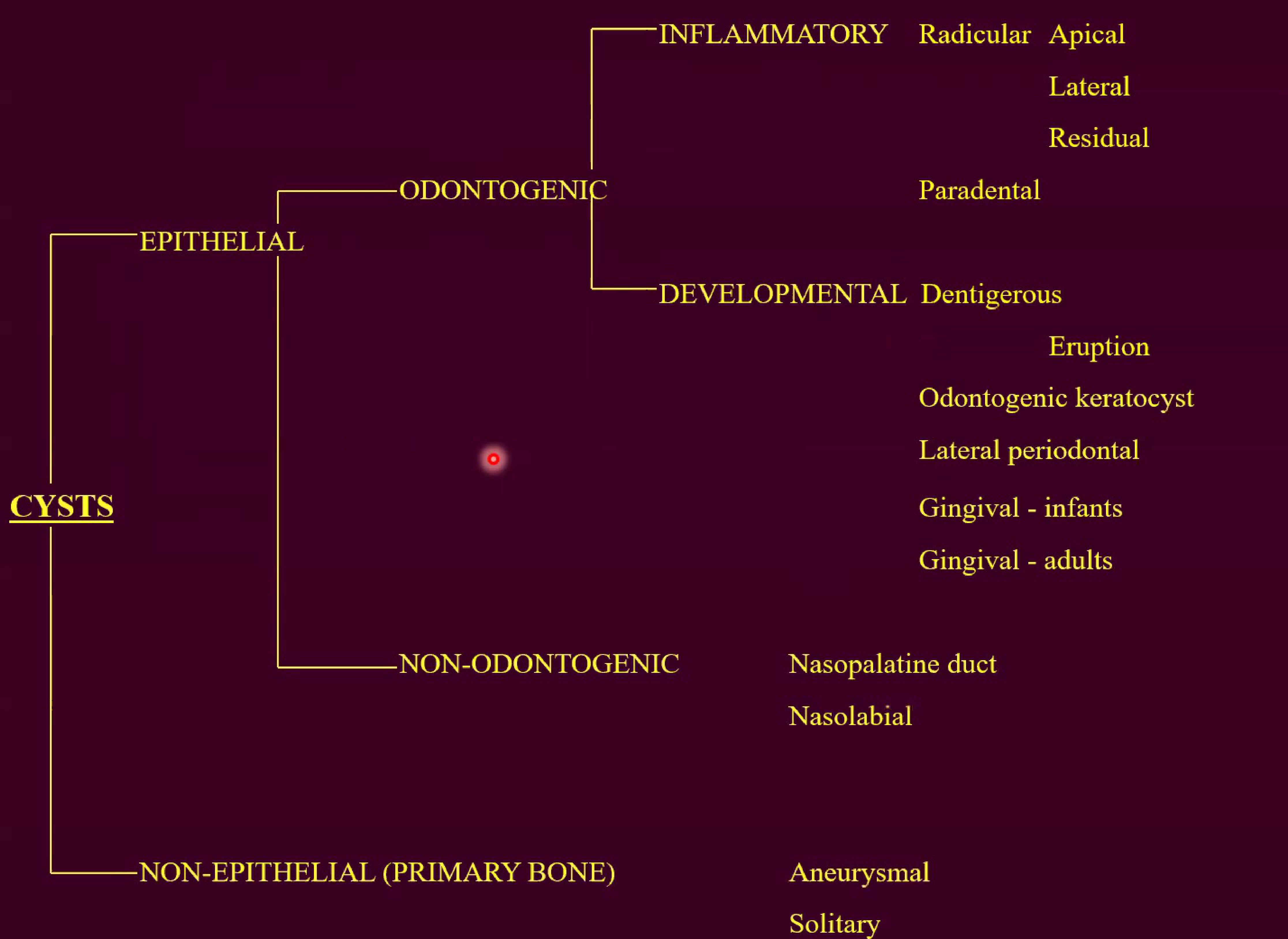
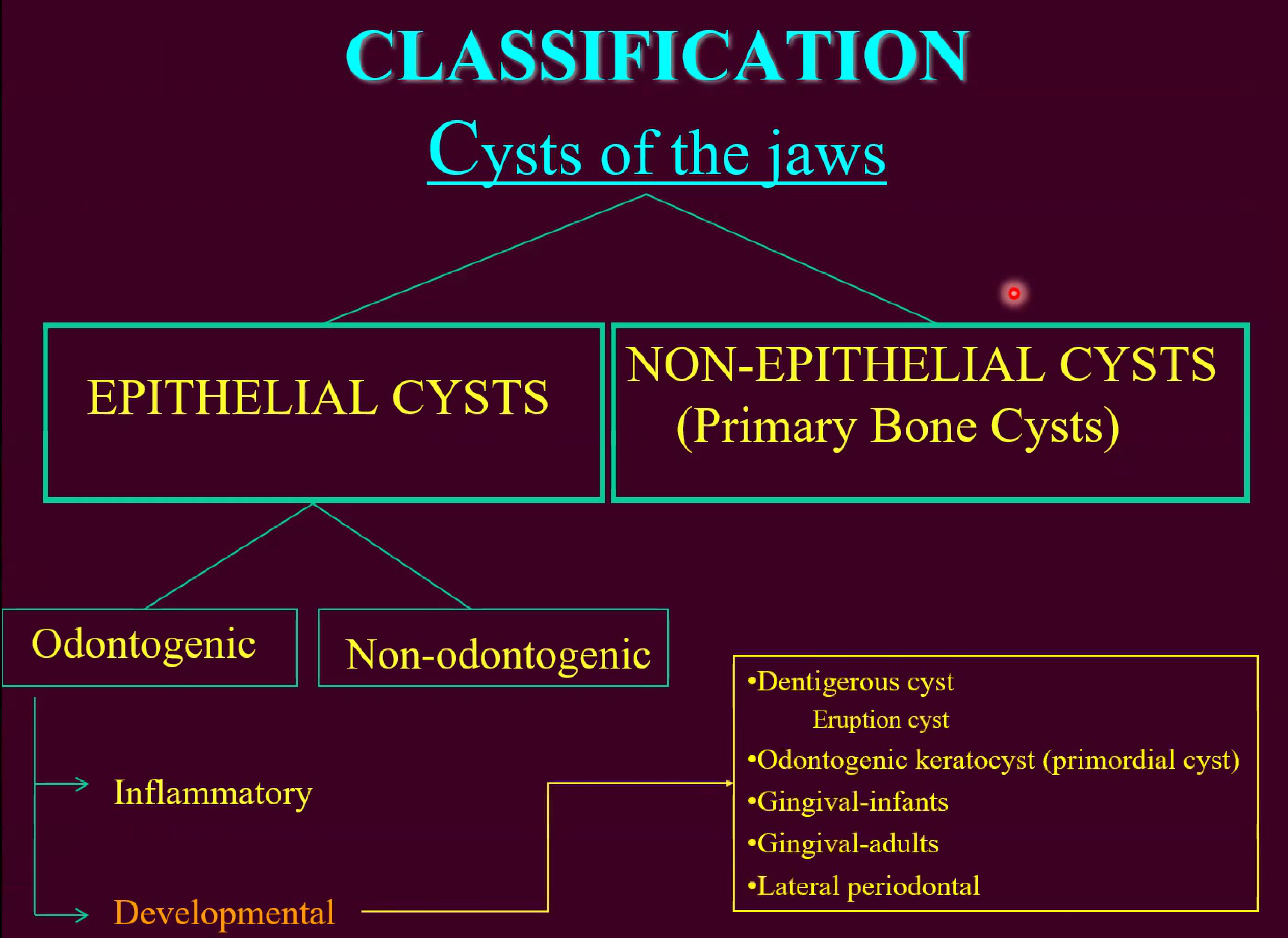
Classification Hierarchy36
-
Epithelial Cysts
- Odontogenic Cysts
- Inflammatory
- Radicular (Apical, Lateral, Residual)
- Paradental
- Paradental cyst
- Developmental
- Dentigerous
- Eruption
- Odontogenic keratocyst
- Lateral periodontal
- Gingival (infants and adults)
- Inflammatory
- Non-Odontogenic Cysts
- Nasopalatine duct
- Nasolabial
- Odontogenic Cysts
-
Non-Epithelial (Primary Bone) Cysts
- Pseudocysts: These lack an epithelial lining and include simple and aneurysmal bone cysts.
- Aneurysmal bone cyst
- Solitary bone cyst
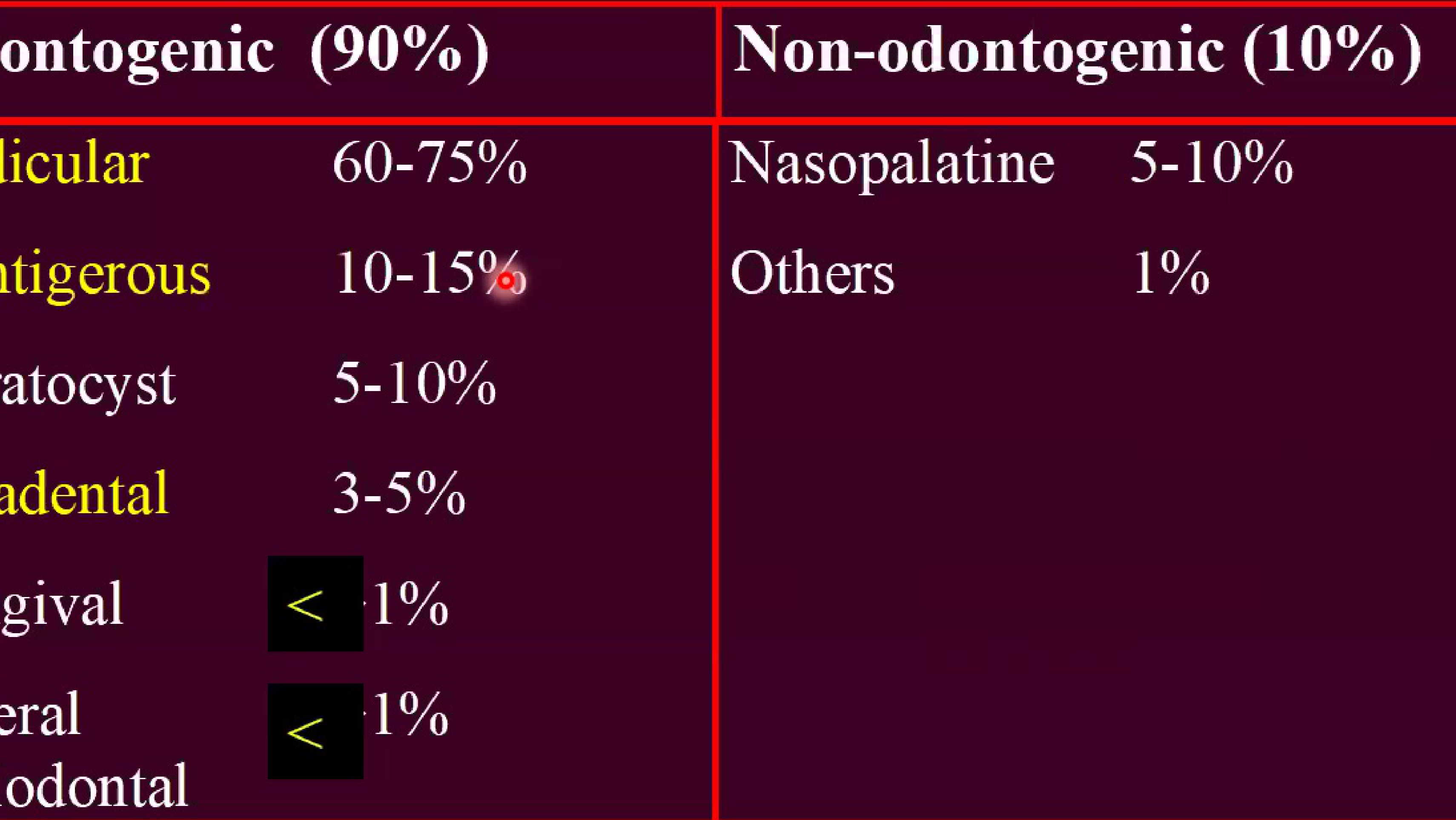
Relative Incidence and Frequency37
Odontogenic Cysts (90% of total)
- Radicular: 60–75%
- Dentigerous: 10–15%
- Keratocyst: 5–10%
- Paradental: 3–5%
- Gingival: < 1%
- Lateral periodontal: < 1%
Non-odontogenic Cysts (10% of total)
- Nasopalatine: 5–10%
- Others: 1%
Diagnostic Clue
The association with a non-vital tooth is the primary diagnostic clue for a radicular cyst.
Radicular Cysts
Classification of Inflammatory Odontogenic Cysts38
- Radicular (dental) cyst
- Periapical
- Lateral
- Residual
- Paradental cyst
Clinical and Radiographic Presentation
Clinical Features39
- Prevalence: Accounts for 60-75% of all jaw cysts (the most common type).
- Demographics: Peak incidence occurs in the 4th and 5th decades of life.
- Associated Tooth:
- Always associated with a non-vital tooth.
- The upper lateral incisor is the most commonly affected tooth.
- Rare in deciduous teeth.
- Symptoms and Progression:
- Often asymptomatic.
- Expansion can lead to a “springy” sensation, followed by egg-shell crackling, and eventually fluctuation.
- Secondary infection will result in pain.
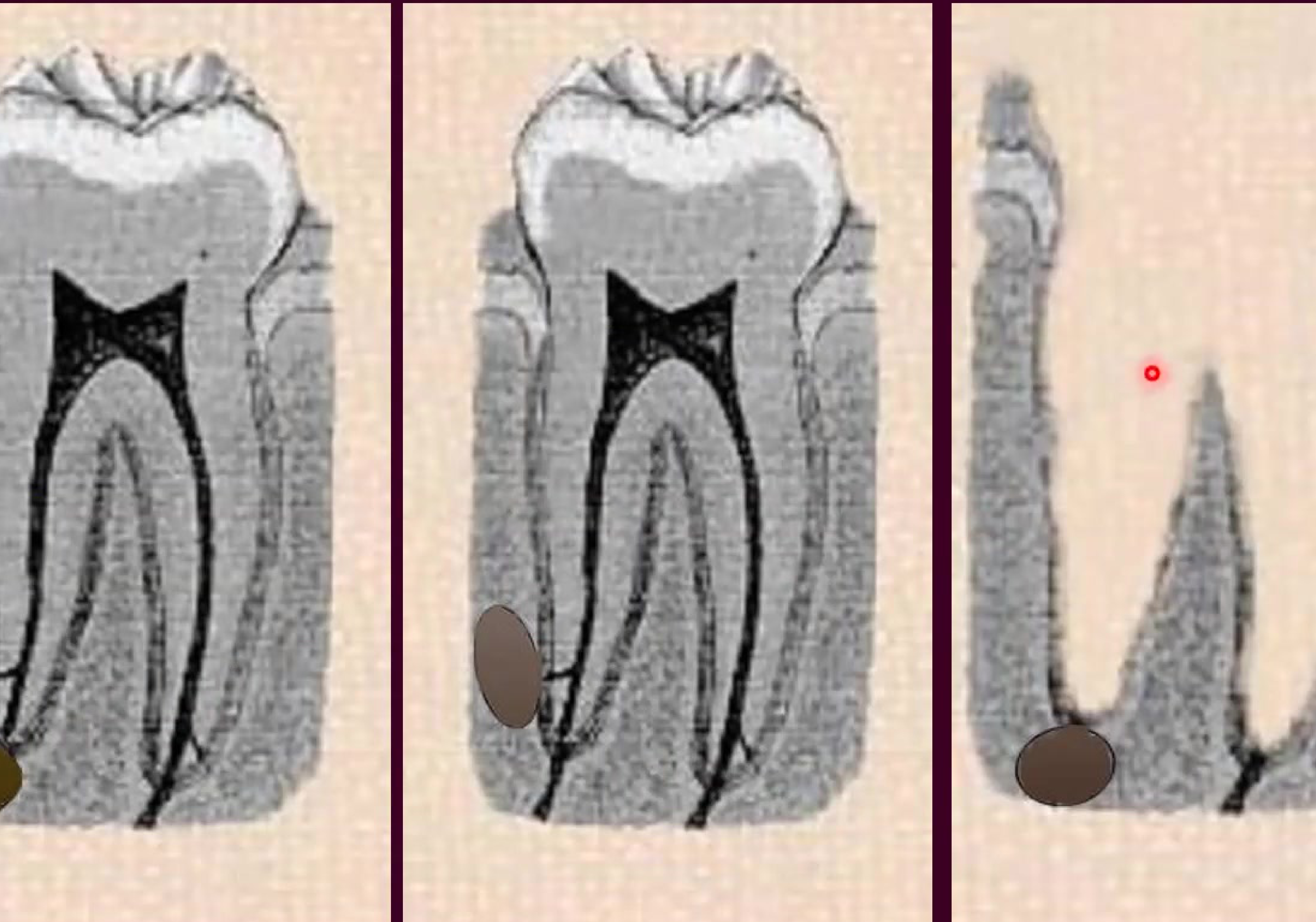
Anatomical Variations404142
- Apical: A cyst located at the root apex of the tooth.
- Lateral: A cyst developing on the side of the root.
- Residual: A cyst that remains in the jaw after the removal of the associated tooth.
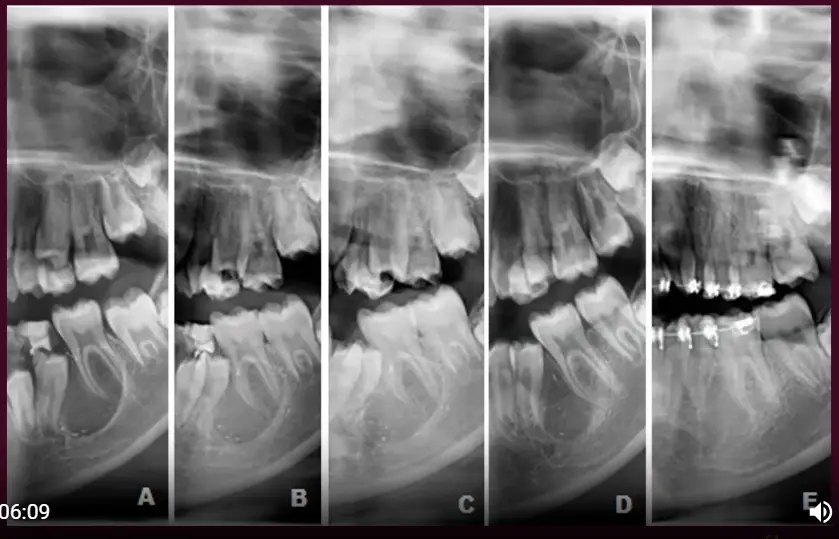
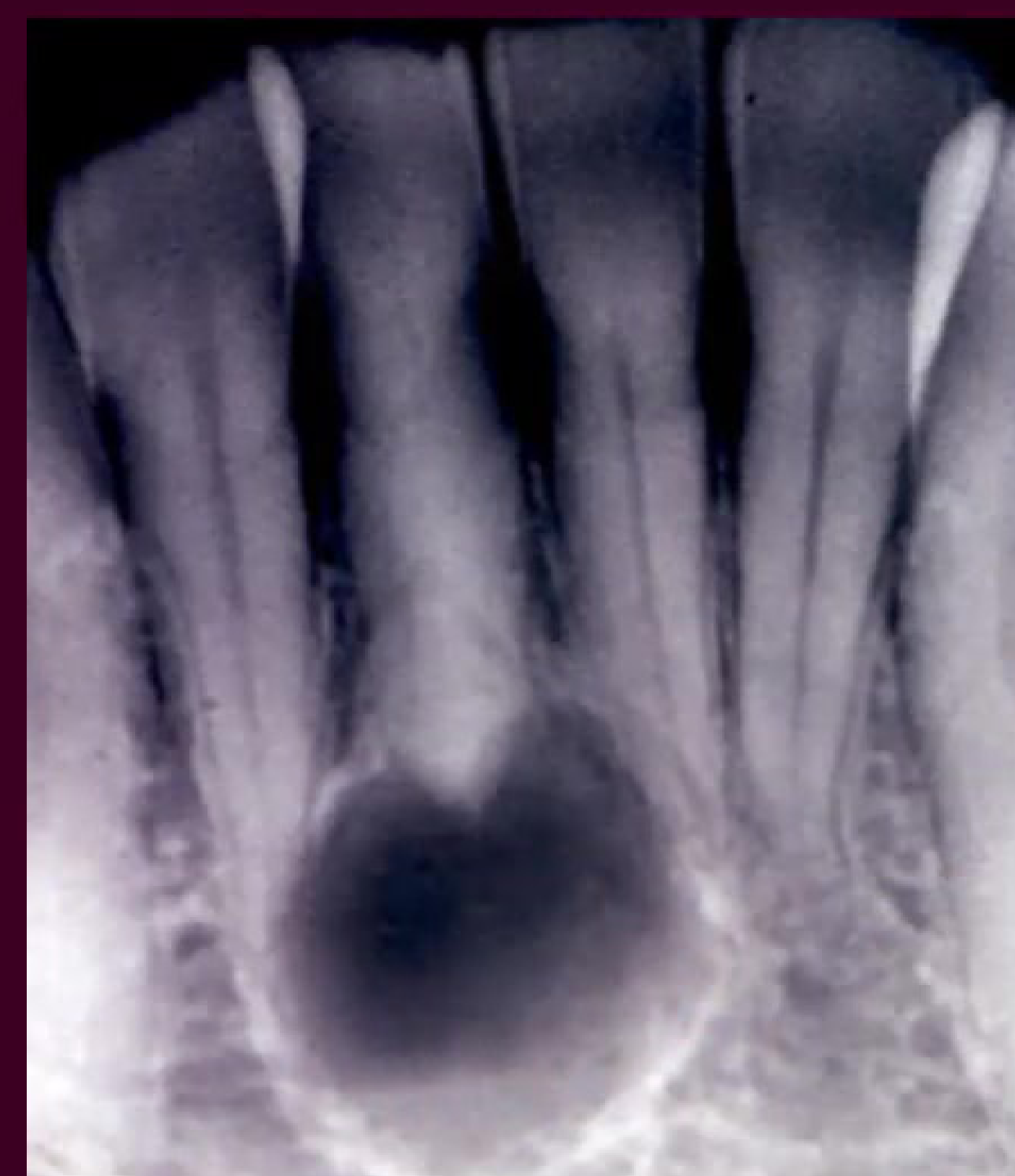
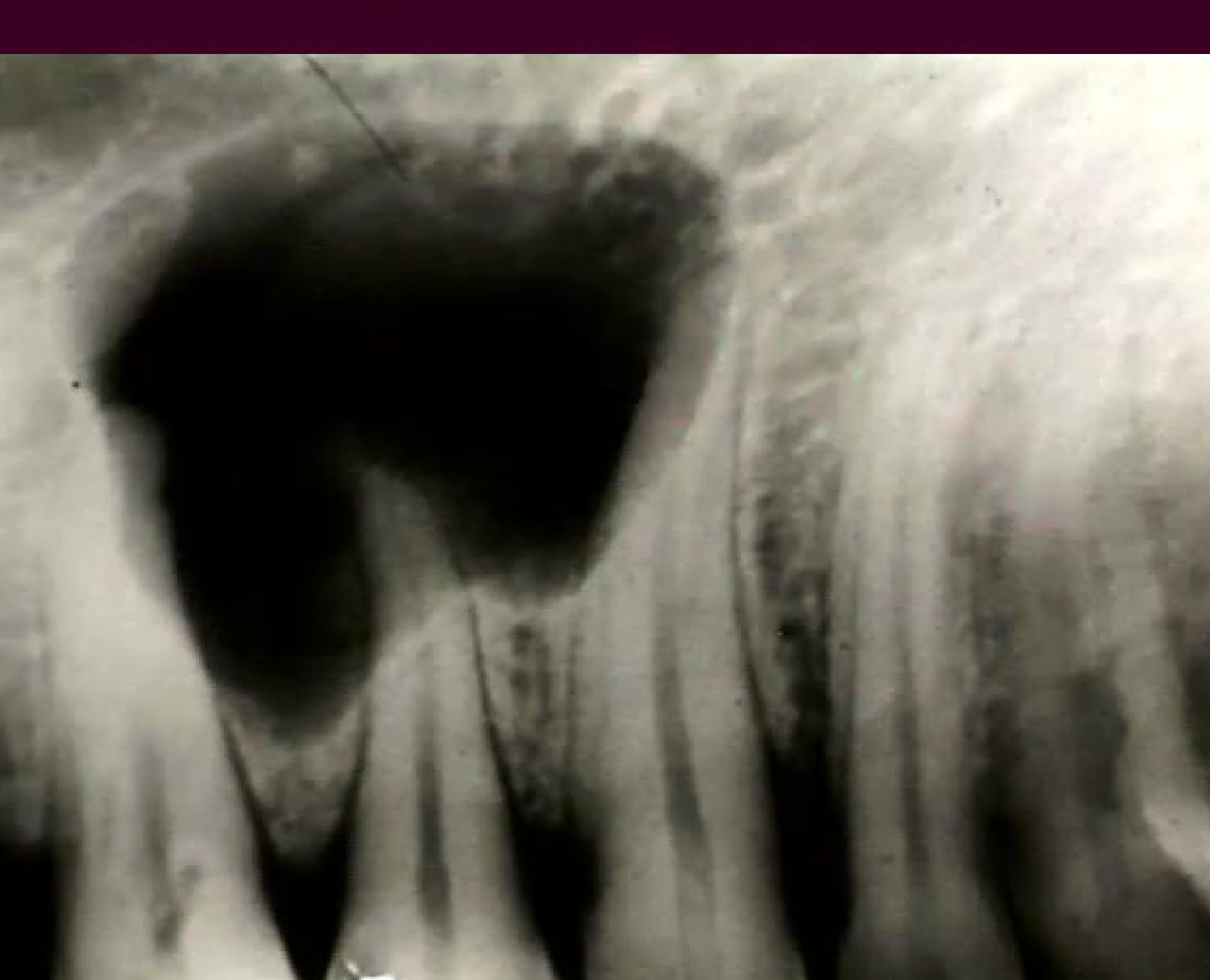
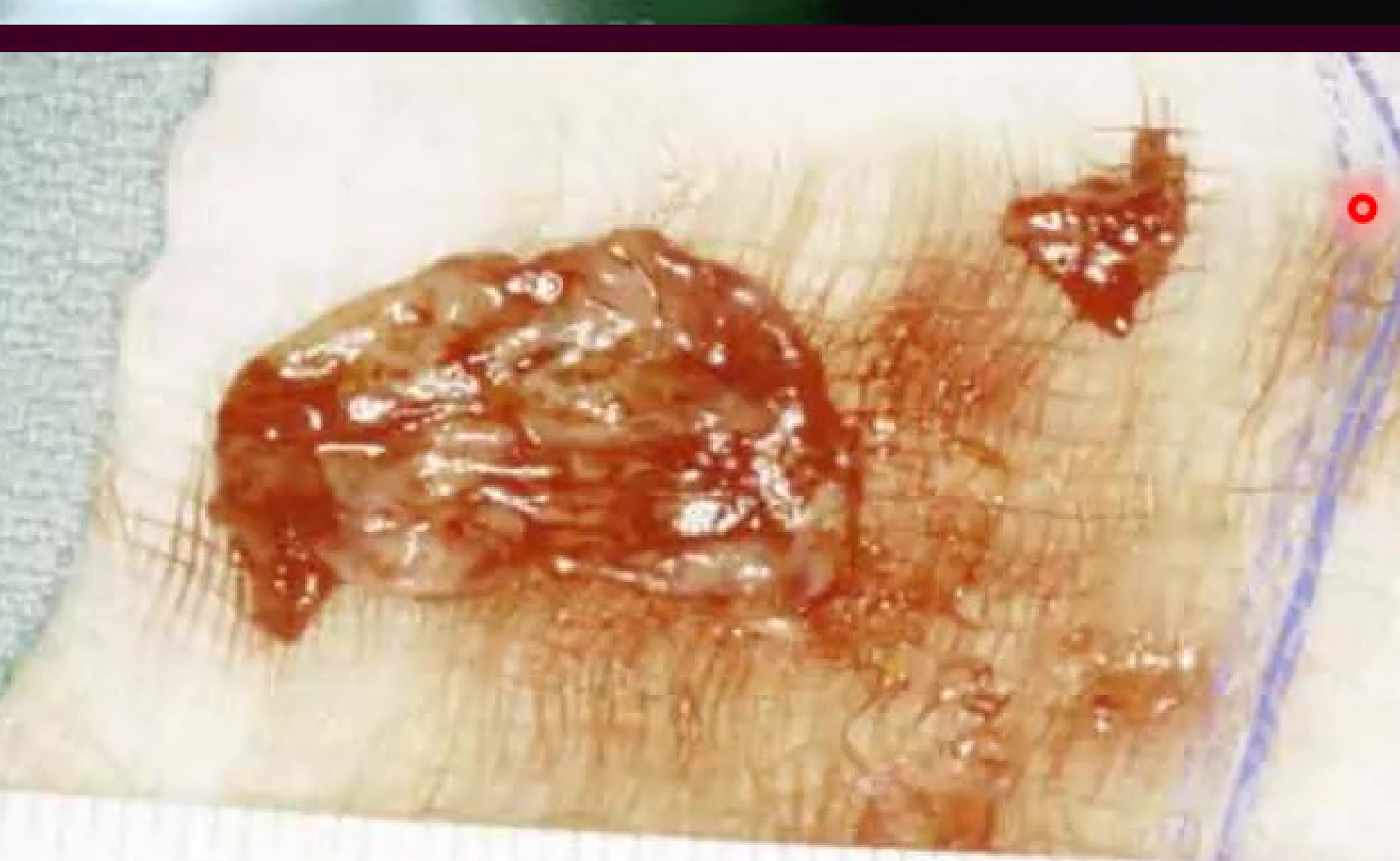
Radicular cysts typically present near the root of the involved tooth.
Visual documentation of radicular cyst presentations.
 |  |
 |  |
 |  |  |
 |  |  |
 |  |  |
 |  |
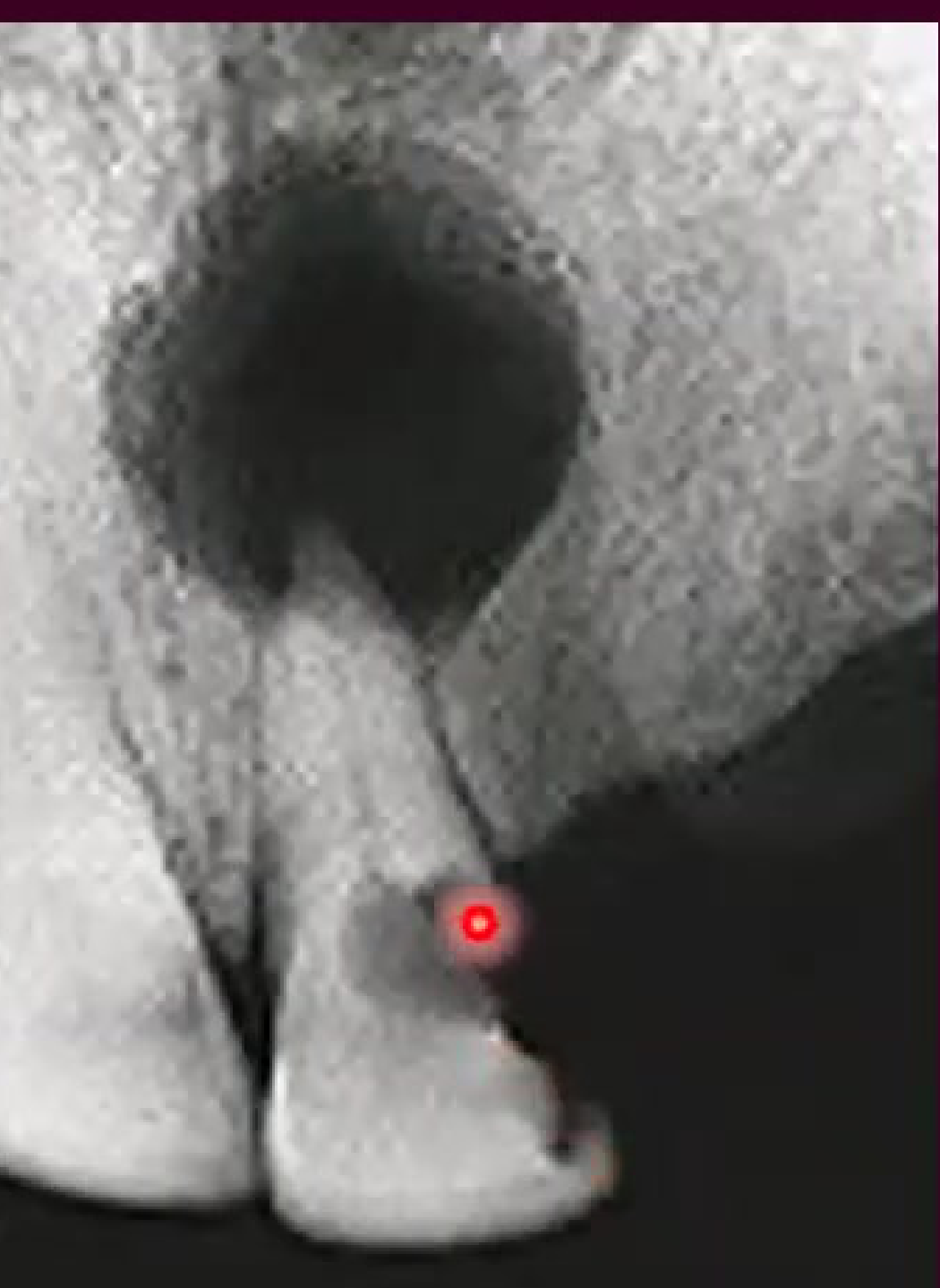
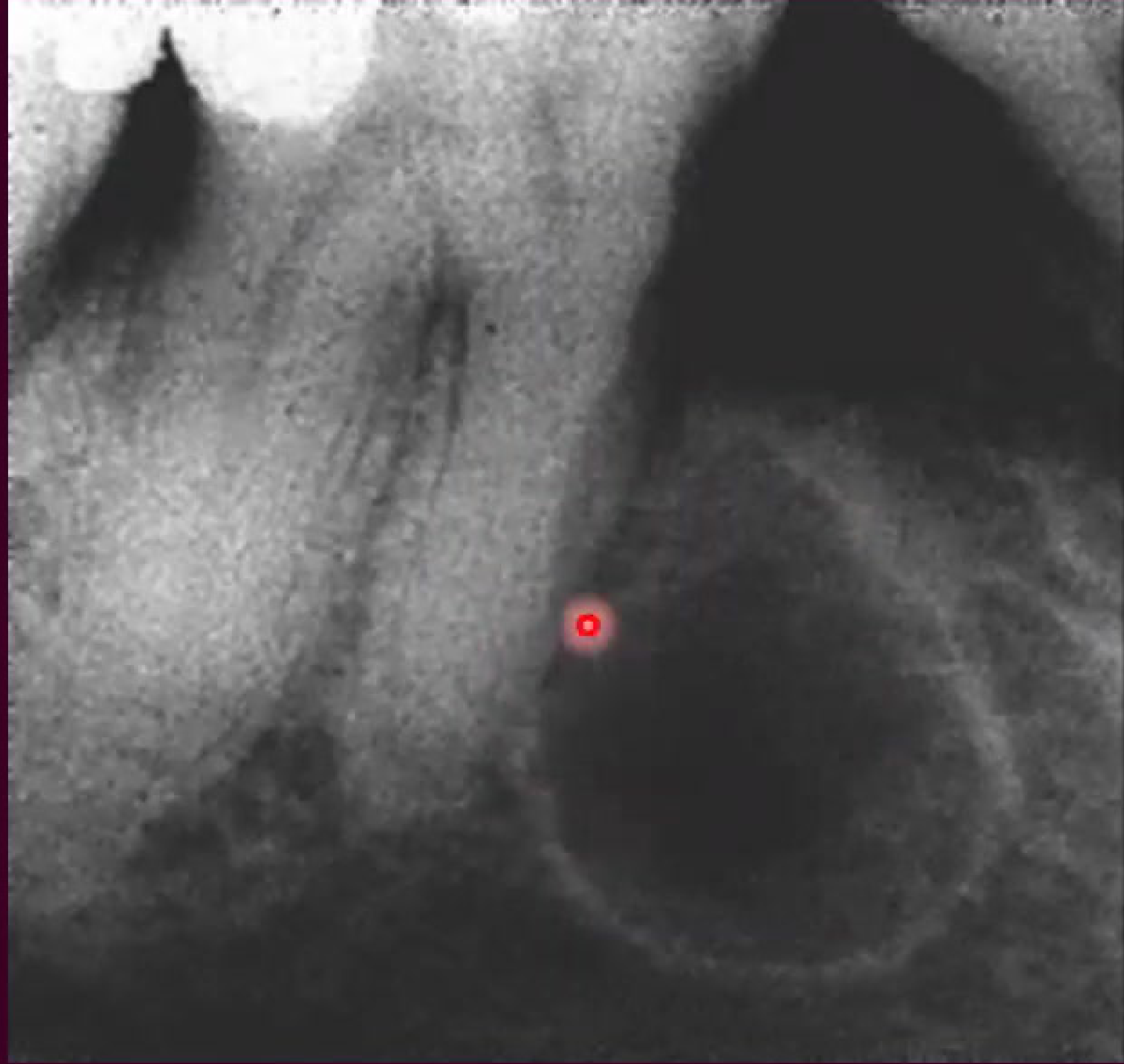
Radiographic Characteristics43
- Shape: Monolocular
- Outline: Well defined and well corticated
- Radiodensity: Uniformly radiolucent
 |  |
- Shape: Monolocular
- Outline: Well defined and well corticated
- Radiodensity: Uniformly radiolucent
 |  |
 |
Radiographic Presentation
- Shape: Monolocular
- Outline: Well defined and well corticated
- Radiodensity: Uniformly radiolucent
Radiographs often show a large radiolucent lesion involving one or multiple teeth.
Clinical imaging of a radicular cyst.
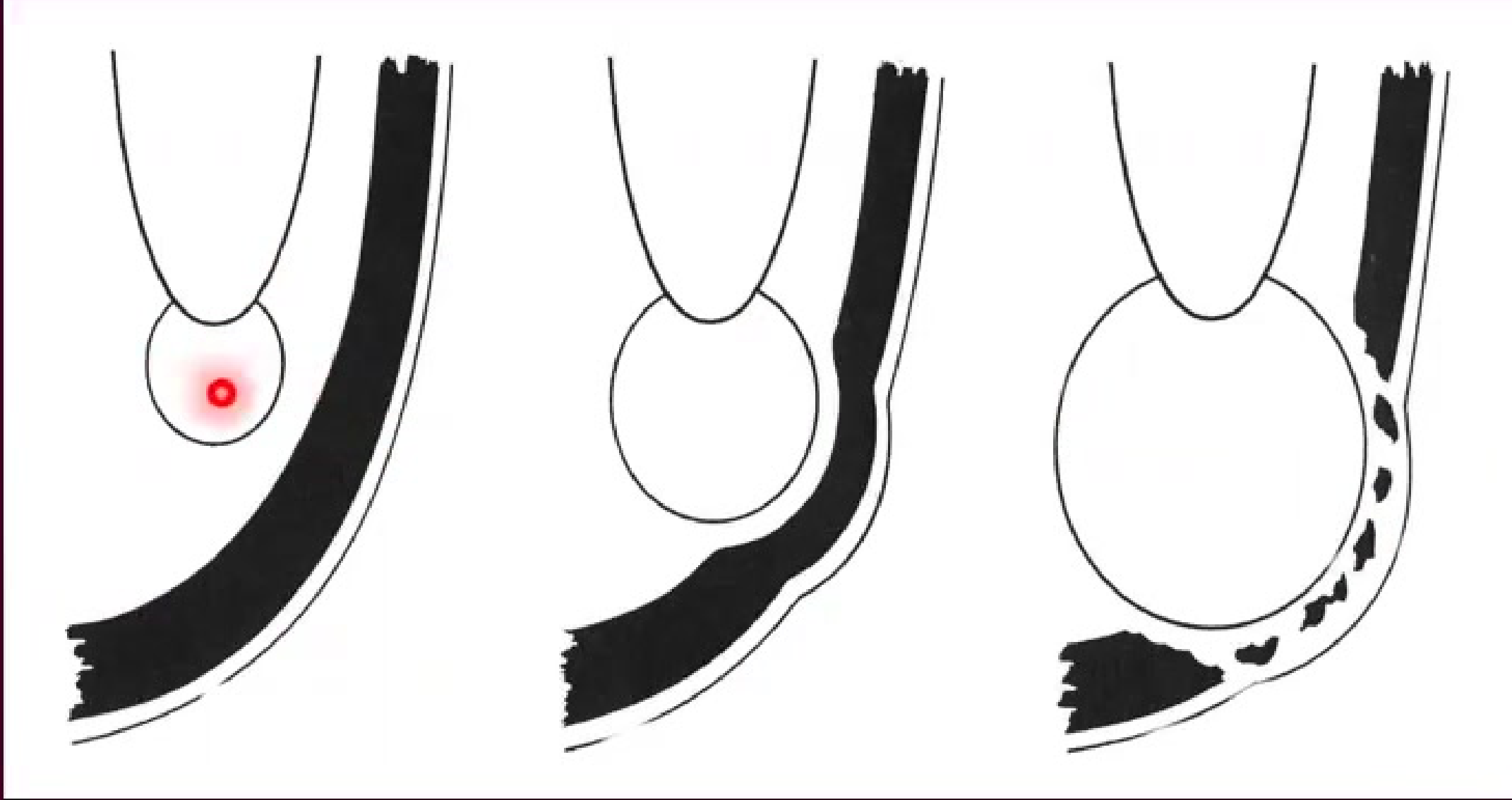
Pathogenesis and Contents
Initiation and Formation44
-
Initiation
- Cell rests of Malassez are activated.
- Activation is triggered by products of necrotic pulp.
- Rest Cells of Malassez are remnants of Hertwig’s Epithelial Root Sheath.
-
Cyst Formation
- Degeneration and death of central cells leads to cavitation.
Cyst Enlargement45
- Osmotic Pressure: Enlargement is driven by increased osmolality. This occurs because breakdown products become smaller and more osmotically active.
- Mechanism: The cyst wall acts as a semi-permeable membrane.
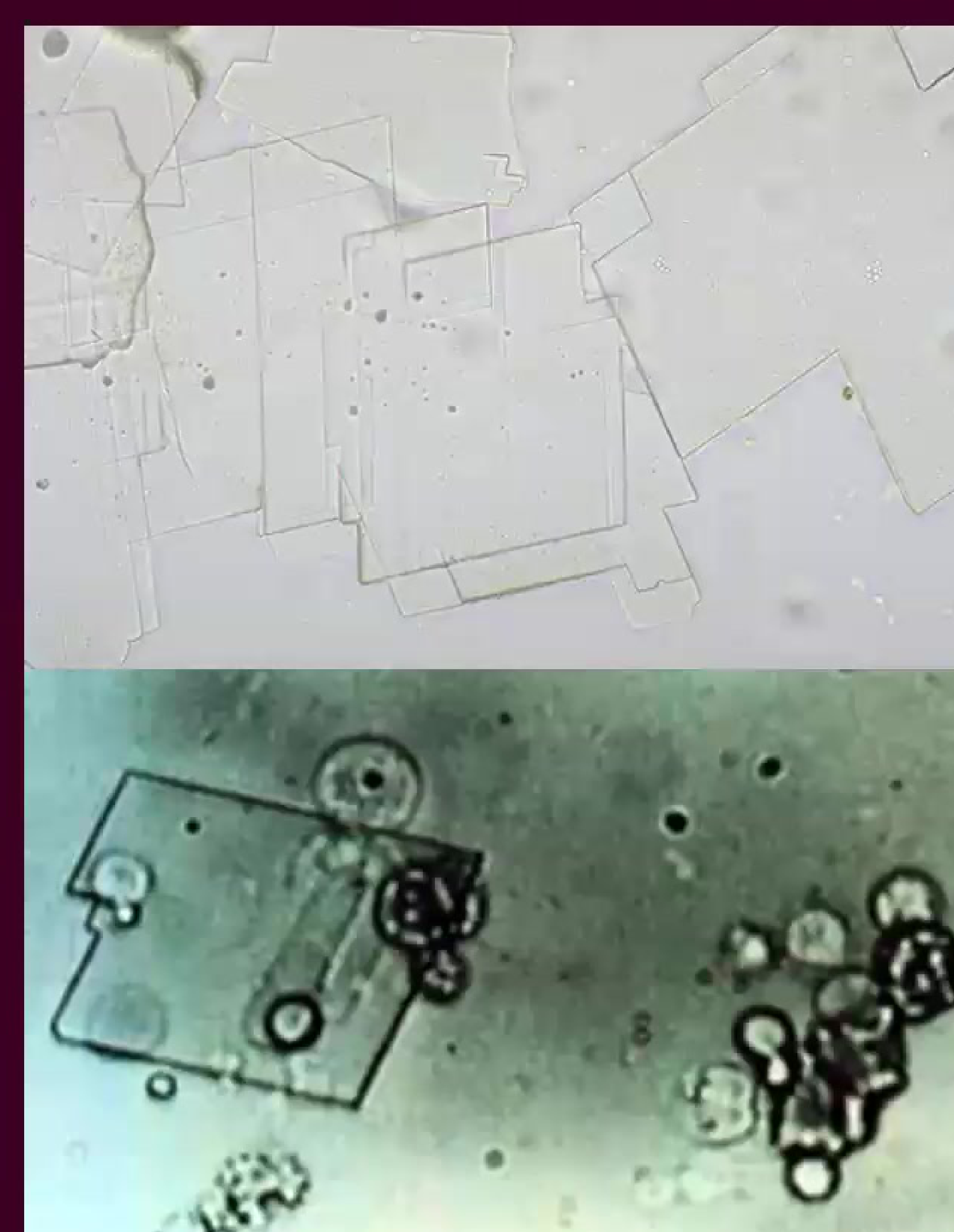
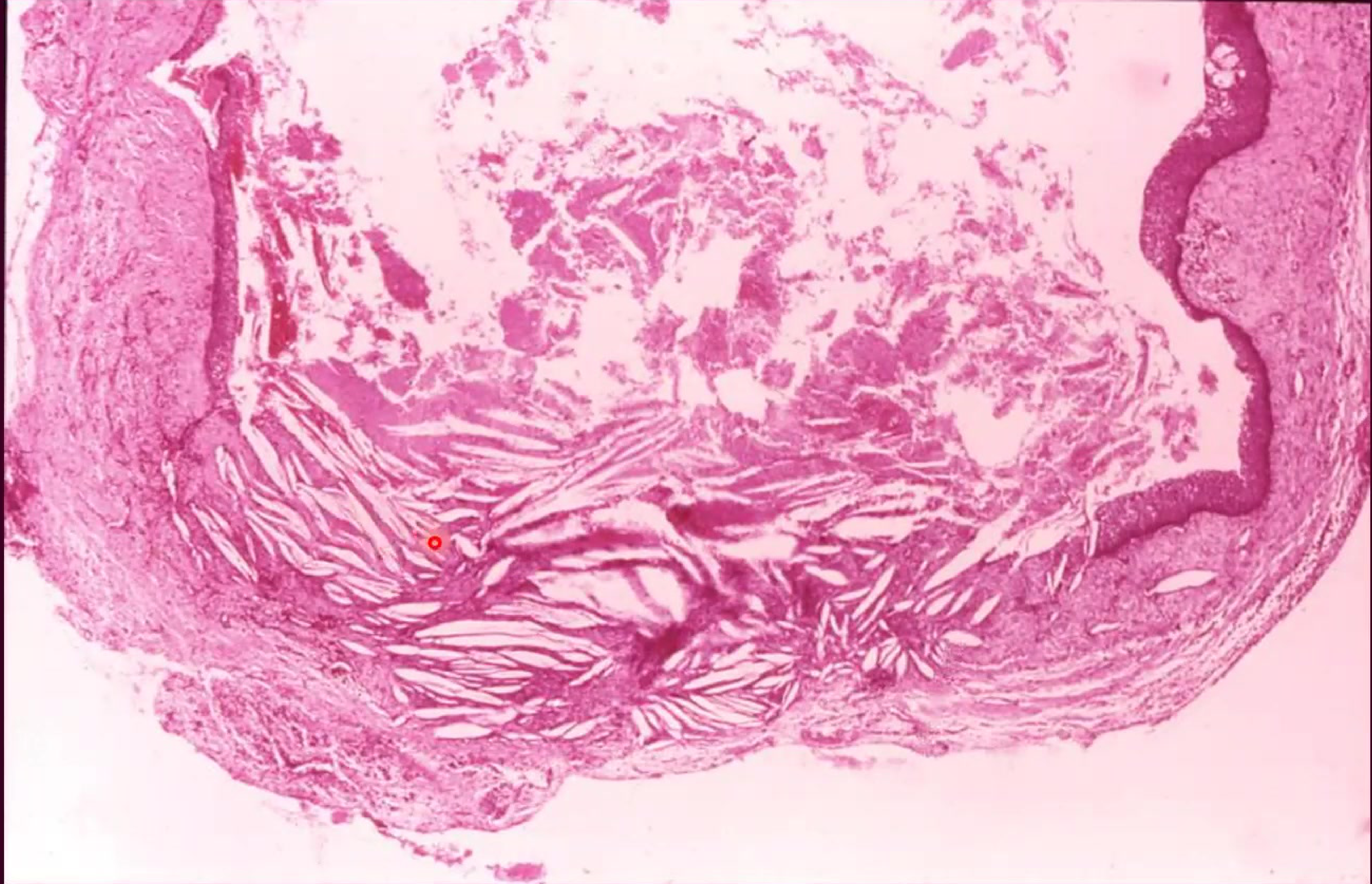
Cystic Contents46
- Breakdown products of cells
- Serum proteins
- Water and electrolytes
- Cholesterol crystals
- Cholesterol crystals appear as "cholesterol clefts" under a microscope.
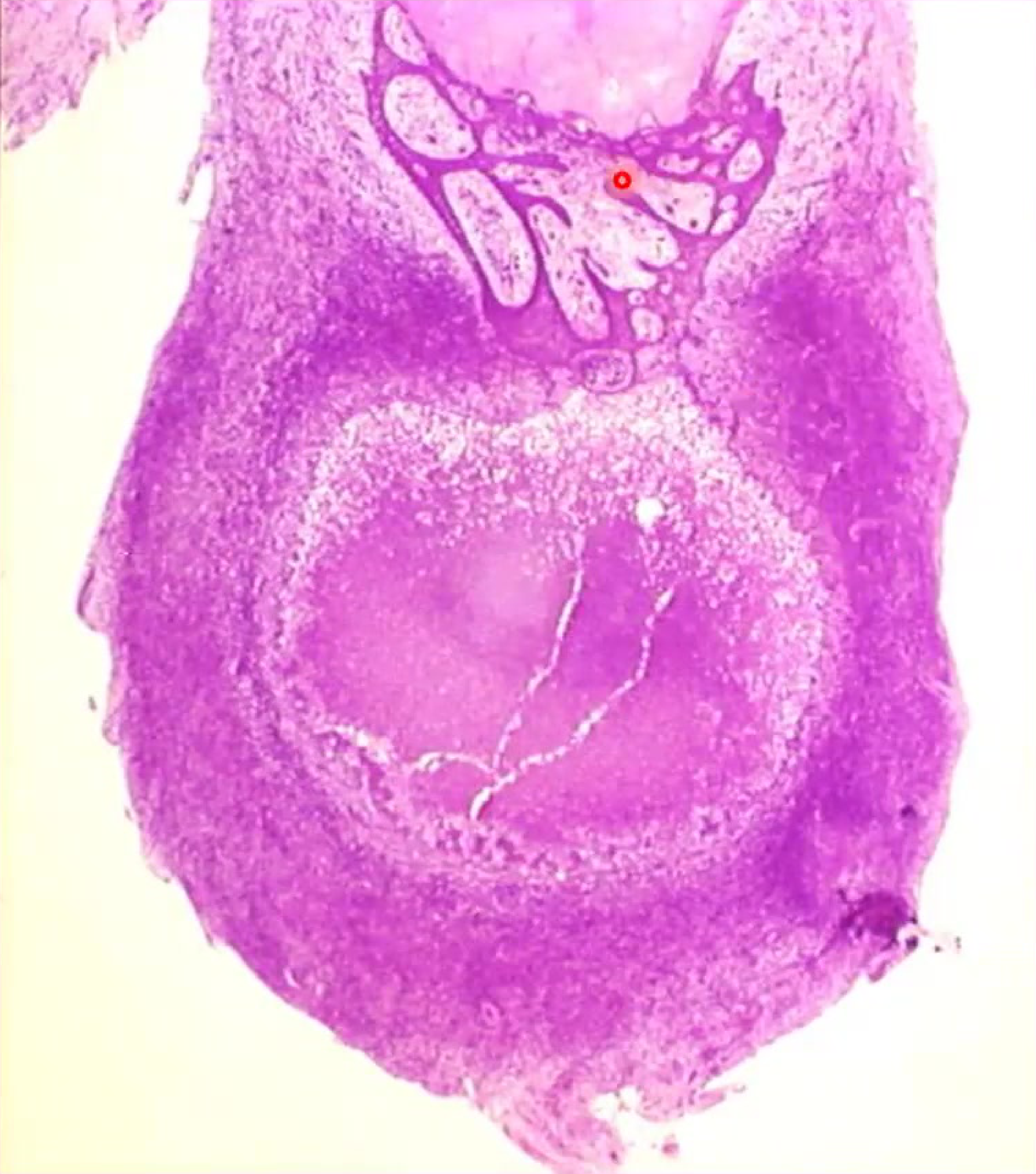
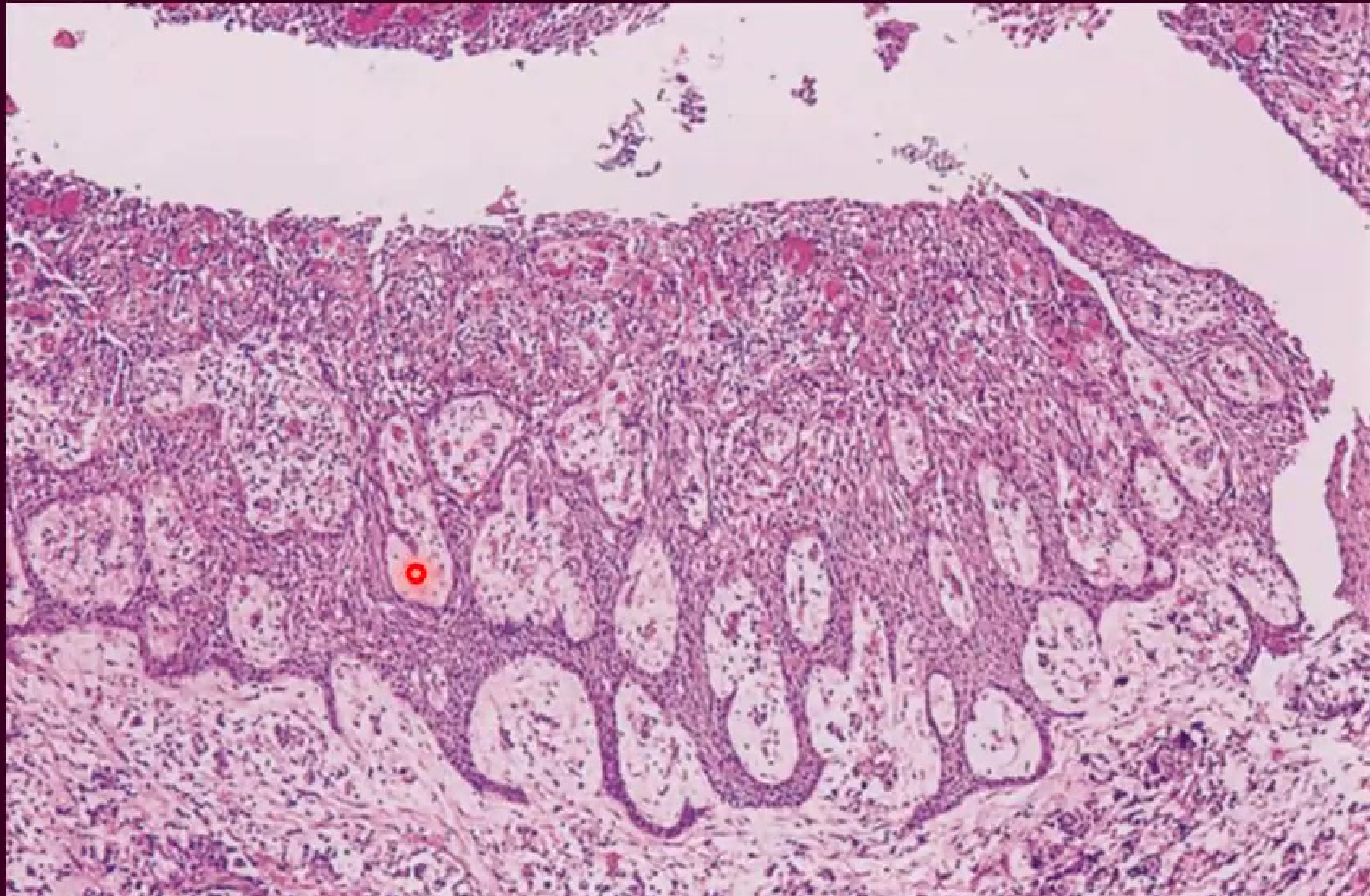
Histopathology of Radicular Cysts
Microscopic Features47484950515253
- Epithelium:
- The cyst is lined by irregular, non-keratinized stratified squamous epithelium.
- The epithelium often shows an "arcading" pattern.
- Epithelial proliferation is often seen in association with periapical granuloma.
- Polymorphs may be present within the epithelium.
- The cyst is lined by irregular, non-keratinized stratified squamous epithelium.
- Cyst Wall and Lining:
- The lining may become thinner and less inflamed over time.
- Approximately 10% of cases contain hyaline (Rushton) bodies.
- Connective Tissue Features:
- Presence of foam cells, lymphocytes, and plasma cells.
- Cholesterol clefts and surrounding fibrosis are common.
 |  |  |
 |  |  Residual cysts Residual cysts |
 residual cysts residual cysts | 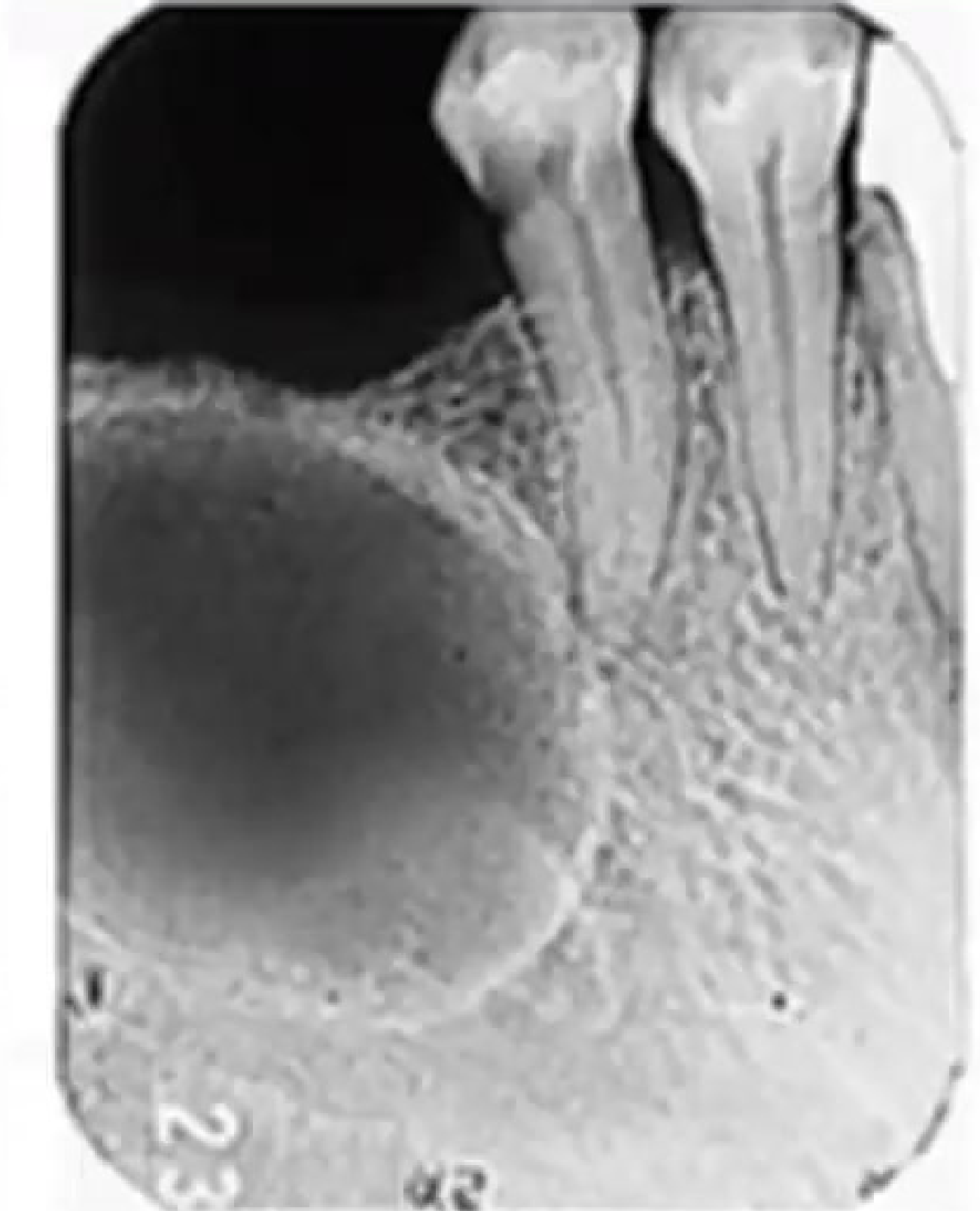 | 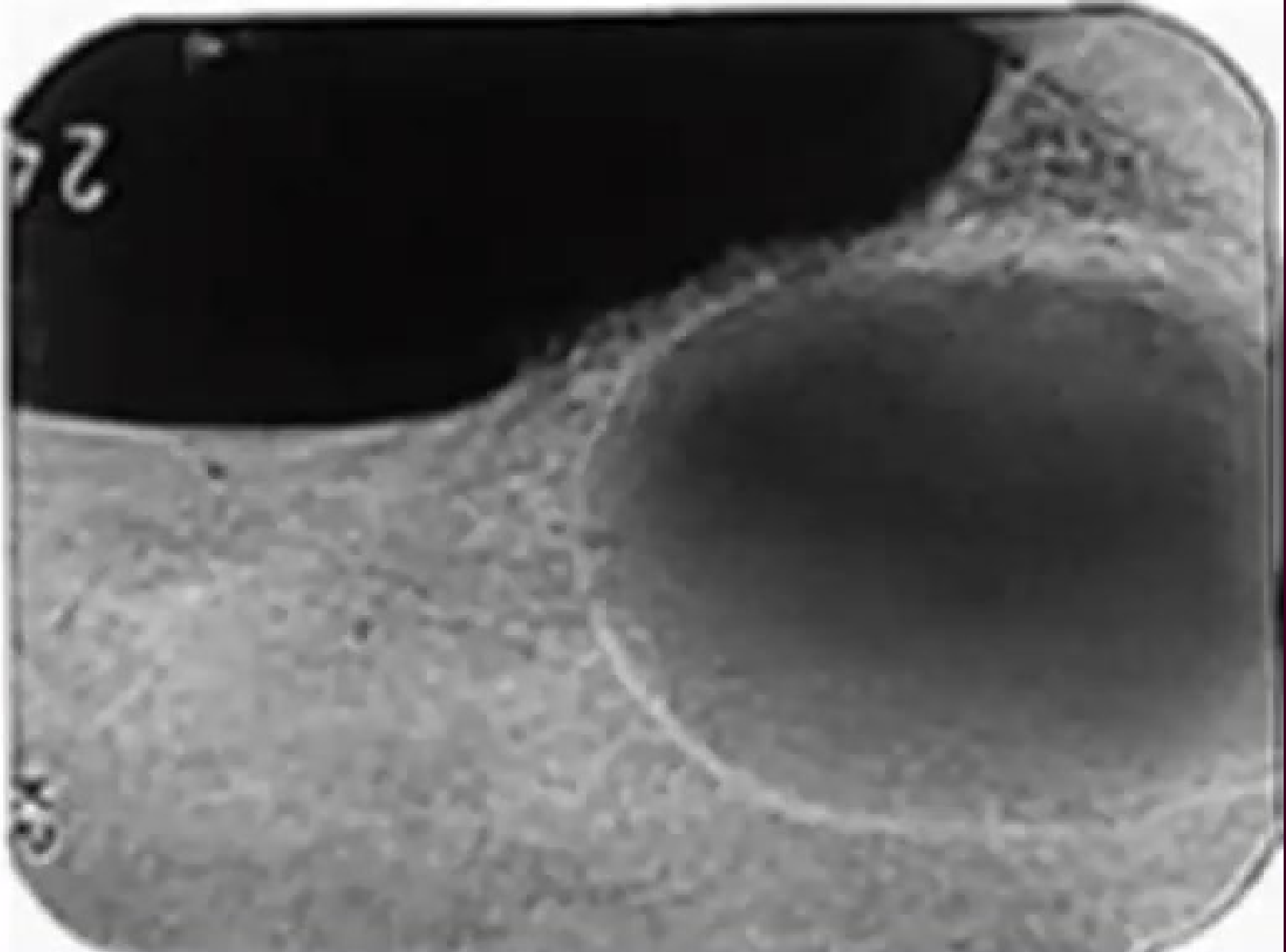 |
Dentigerous and Eruption Cysts
Classification of Jaw Cysts54
Epithelial Cysts
-
Odontogenic
- Inflammatory
- Developmental
- Dentigerous cyst
- Eruption cyst
- Odontogenic keratocyst (primordial cyst)
- Gingival cyst of infants
- Gingival cyst of adults
- Lateral periodontal cyst
-
Non-odontogenic
Non-Epithelial Cysts (Primary Bone Cysts)
Dentigerous Cyst Pathogenesis and Clinical Features5556
 |  |
 |
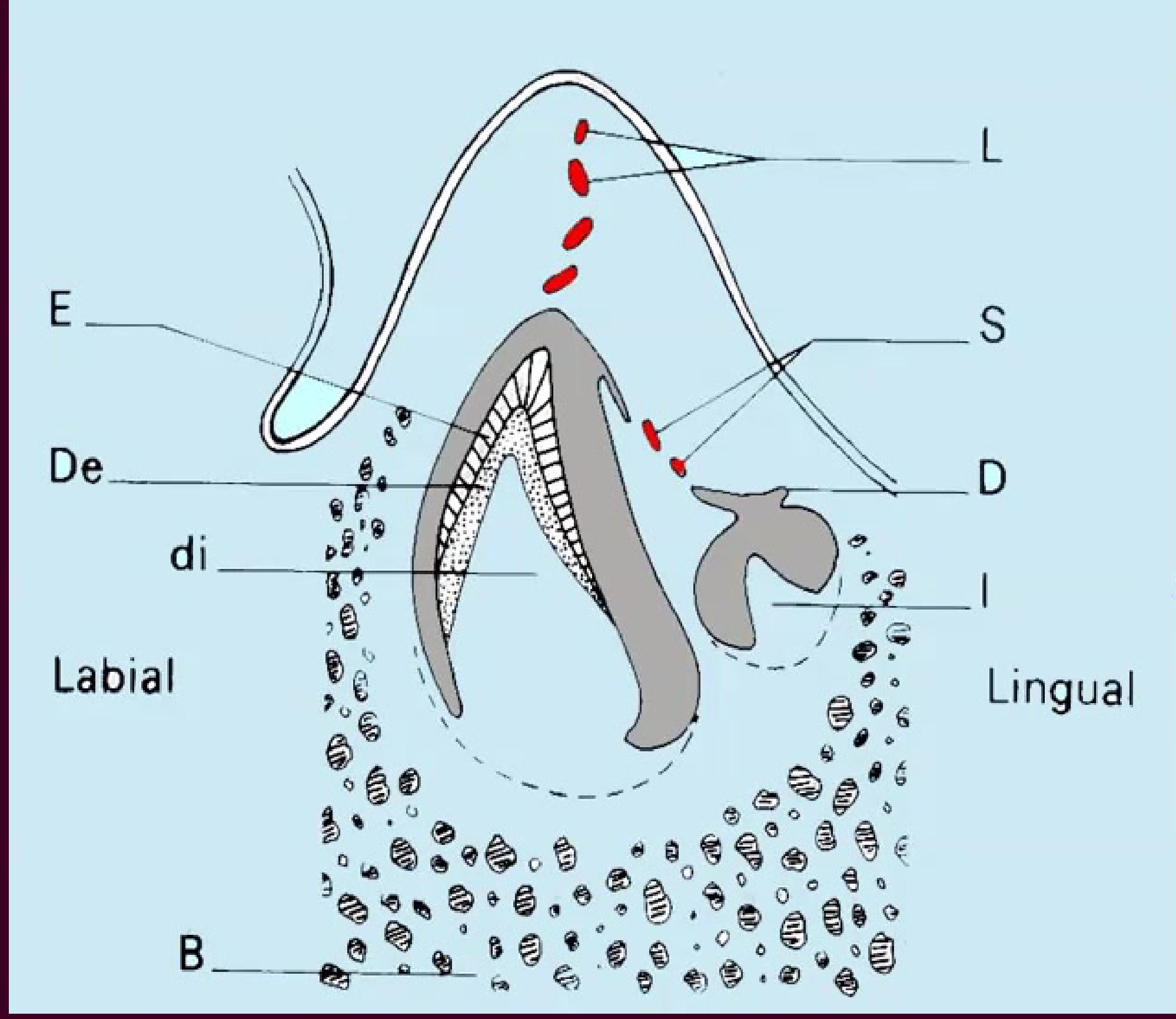
Definition and Terminology57
- A cyst enclosing the crown of an unerupted tooth.
- Attached to the cemento-enamel junction.
- Also known as a follicular cyst.
Pathogenesis Mechanisms58
- Intrafollicular fluid accumulates between the reduced enamel epithelium (REE) and the enamel.
- Pressure of the tooth on the impacted follicle leads to:
- Obstruction of venous outflow
- Serum transudation
- Exudation
Clinical Presentation59
- Accounts for 10-15% of all jaw cysts.
- Primarily affects children and young adults.
- Associated with permanent teeth.
- Most common sites involve teeth likely to be impacted:
- Upper canine
- Lower 3rd molar
- Gender distribution: M:F ratio of 1.6:1.
- Clinical signs include:
- Painless enlargement
- Missing tooth
- Tilting of adjacent teeth
- Root resorption
Radiographic Presentation6061626364
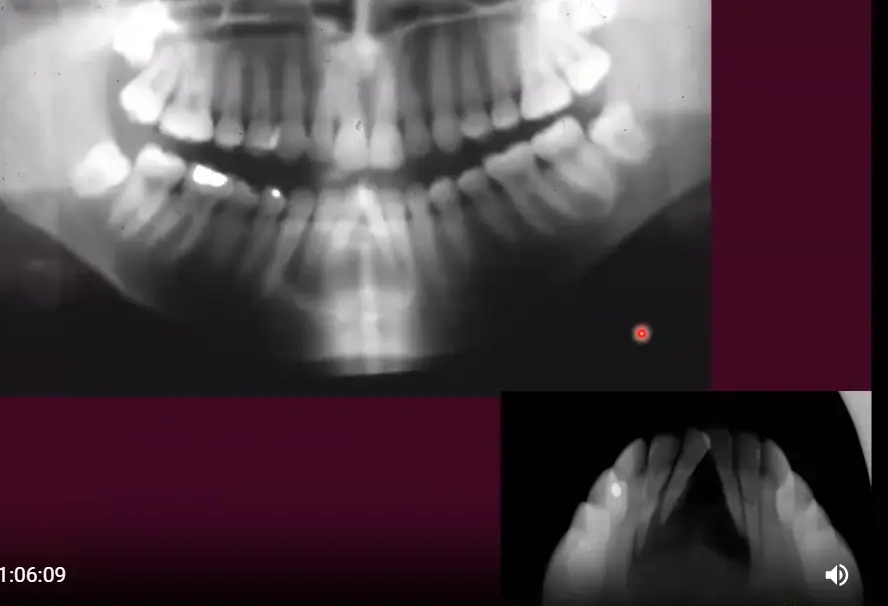
Radiographic examination typically reveals radiolucent lesions associated with unerupted teeth. Key features include:
- Radiolucency surrounding the crown of an unerupted tooth.
- Unilocular radiolucency engulfing the crown of an impacted tooth.
- Potential displacement of adjacent roots.
- Clear demarcation of the lesion around the tooth crown.
Dentigerous Cyst Pathology65
Gross and Microscopic Features66
- Cyst Contents: Clear yellow fluid containing cholesterol; may become purulent if infected.
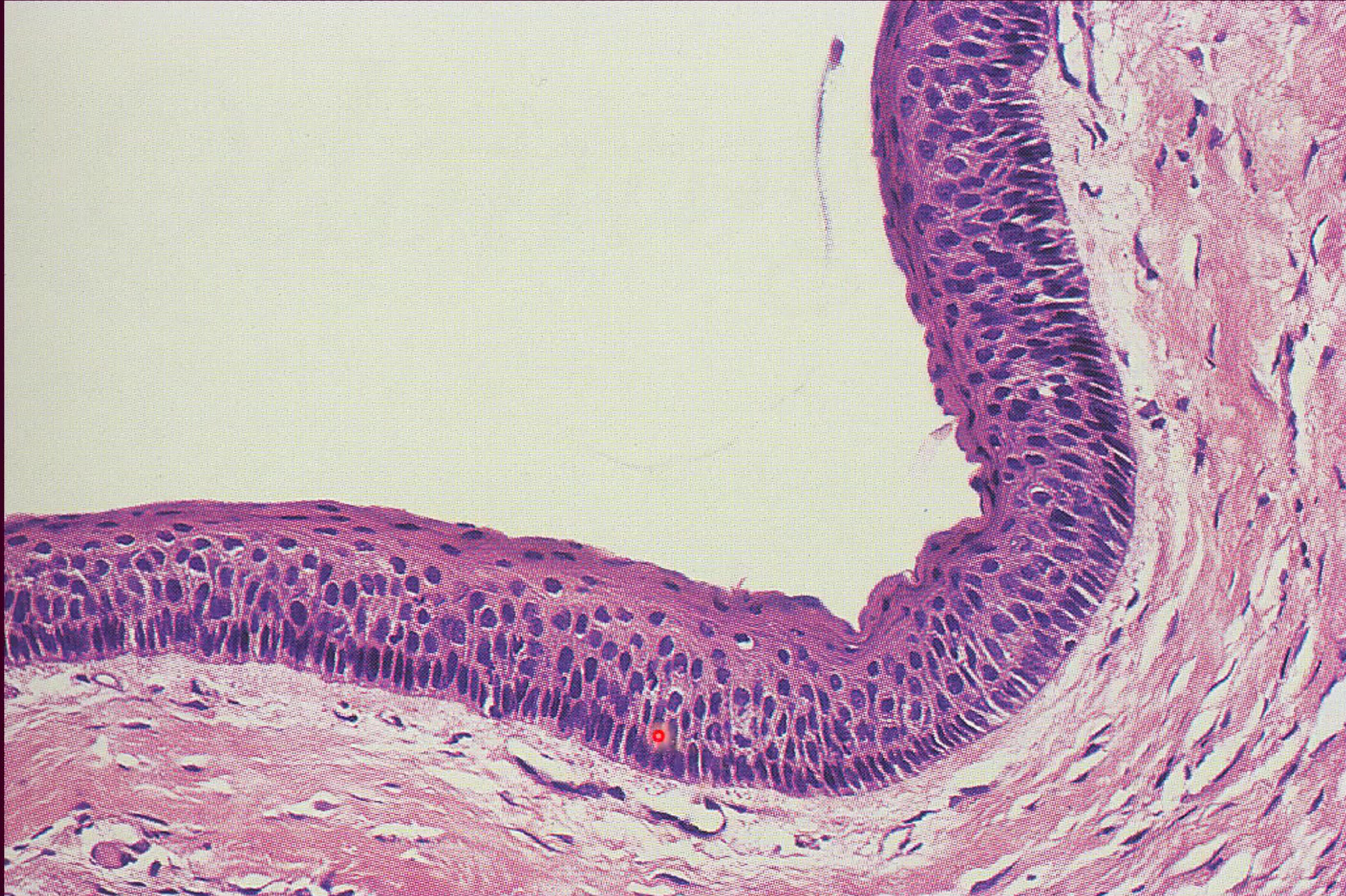
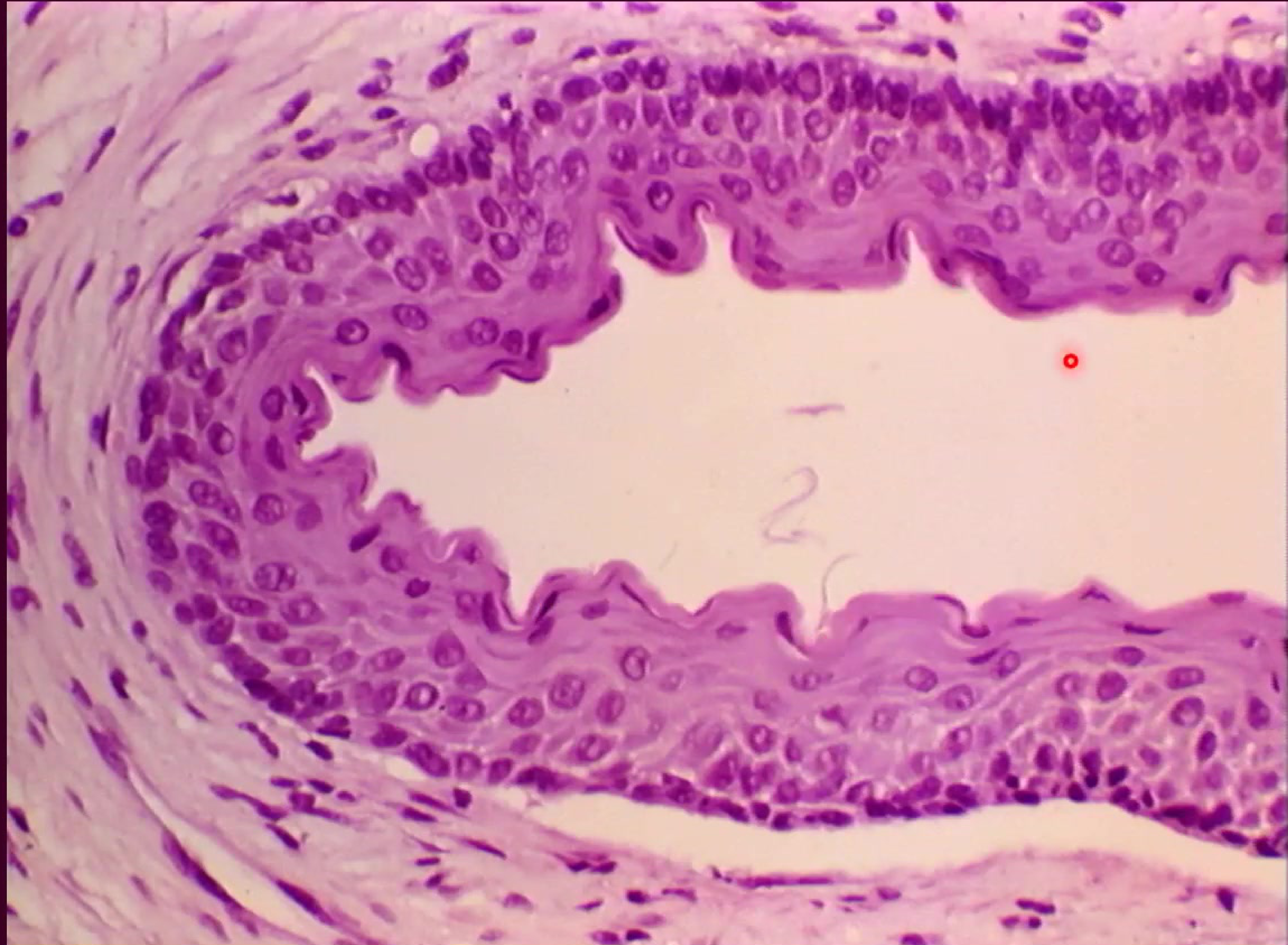
- Epithelial Lining:
- Lined by flattened, non-keratinised stratified squamous epithelium.
- Thin lining consisting of only 2–4 layers of flattened epithelium.
- The lining is continuous with the reduced enamel epithelium.
- May exhibit mucous and ciliated columnar metaplasia.
- Lined by flattened, non-keratinised stratified squamous epithelium.
- Cyst Wall: Composed of a fibrous wall with variable degrees of inflammation.
- The wall is typically non-inflamed unless a secondary infection occurs.
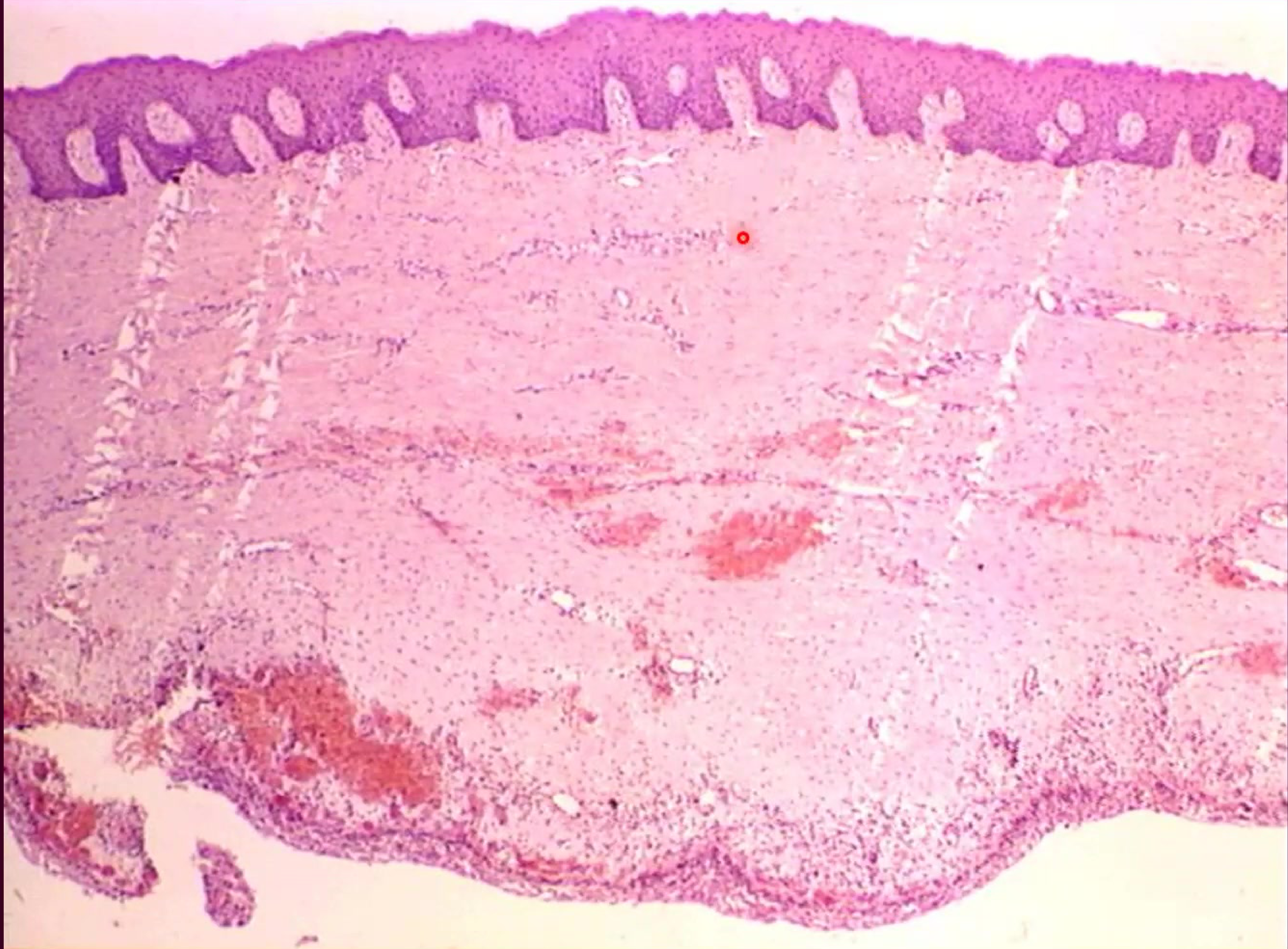
Histological Characteristics67
Histological sections typically demonstrate a cystic structure with a tooth crown embedded within the lumen. The cyst wall is attached at the cemento-enamel junction, showing the relationship between the dental follicle and the developing tooth.
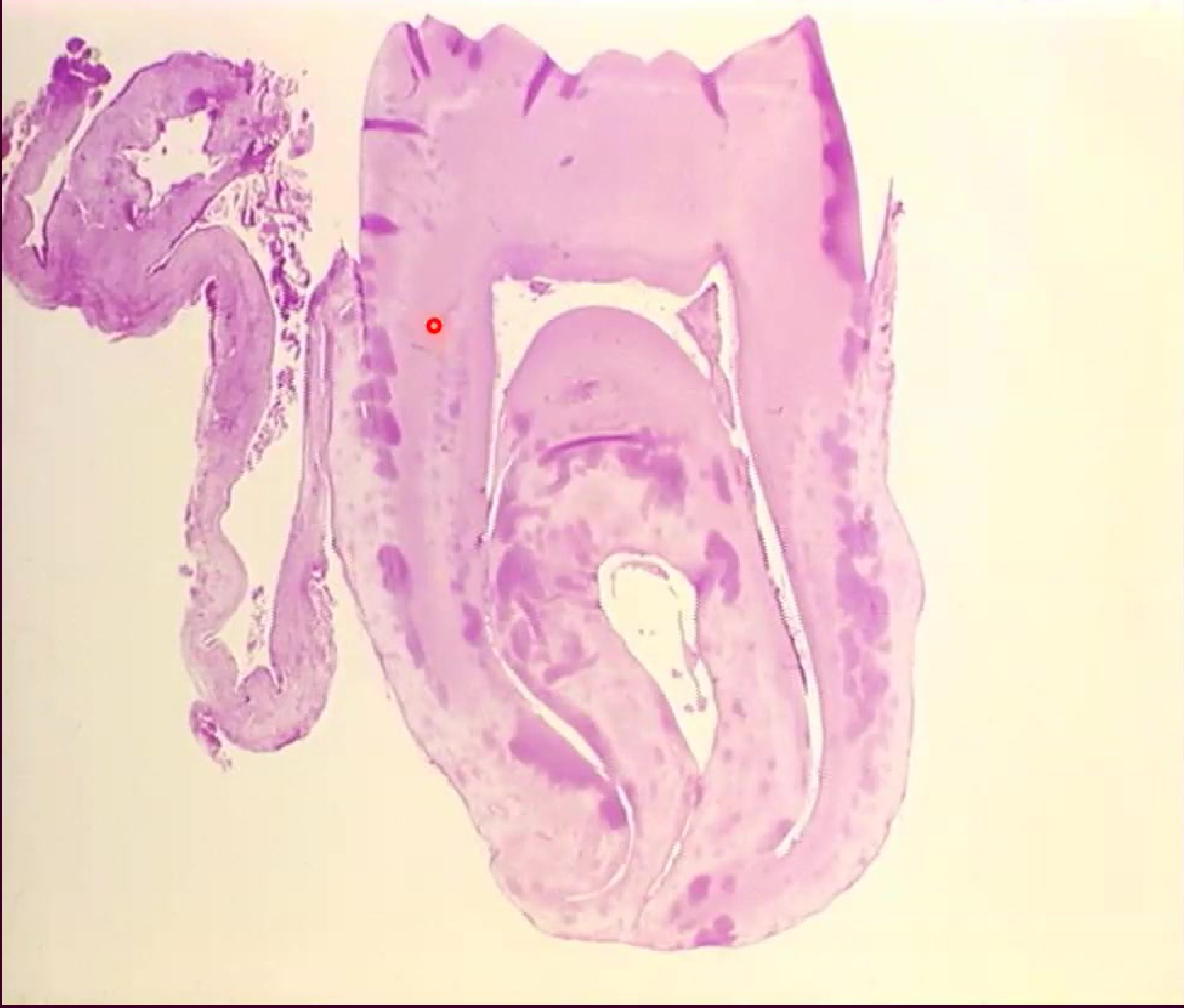
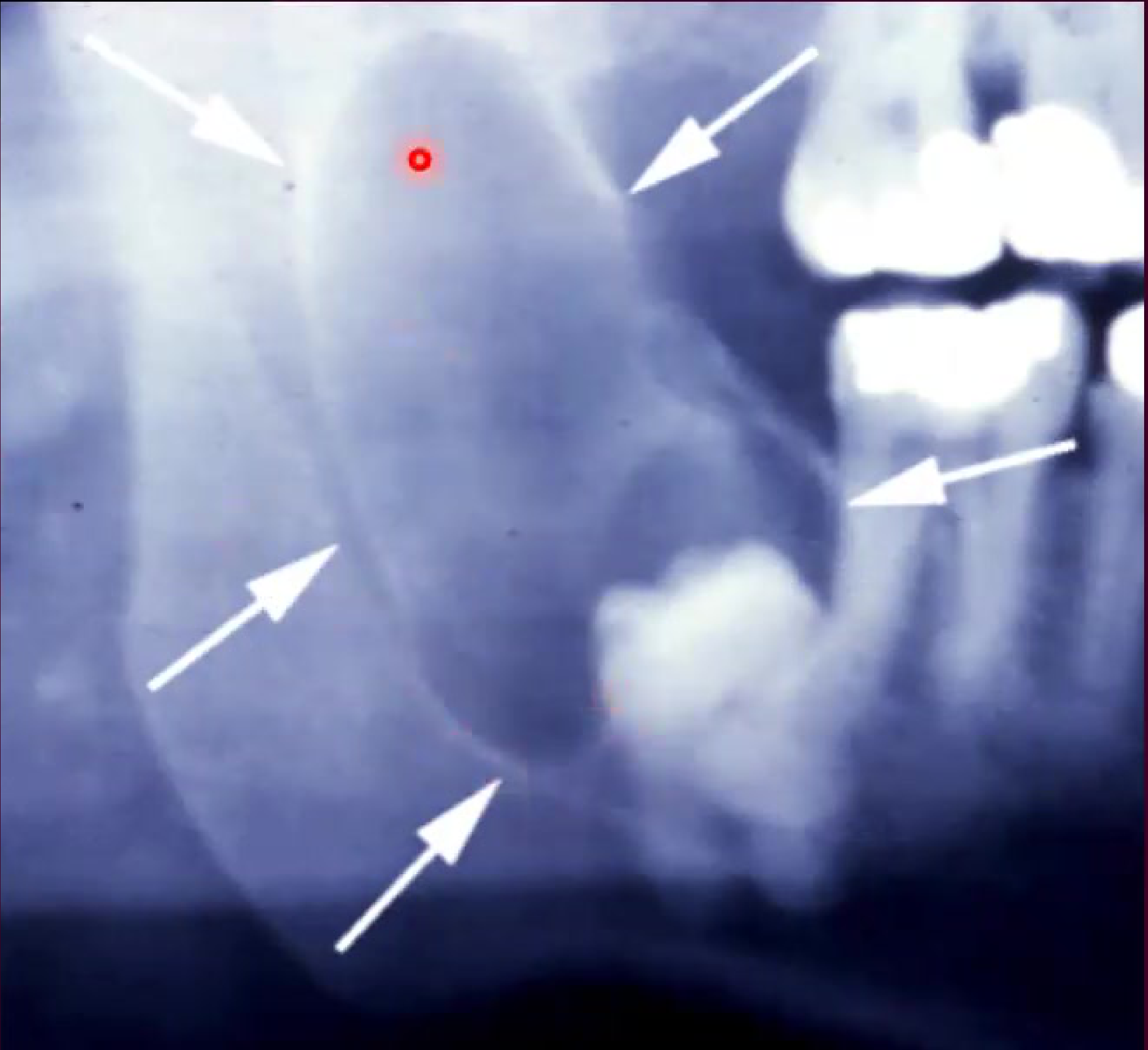
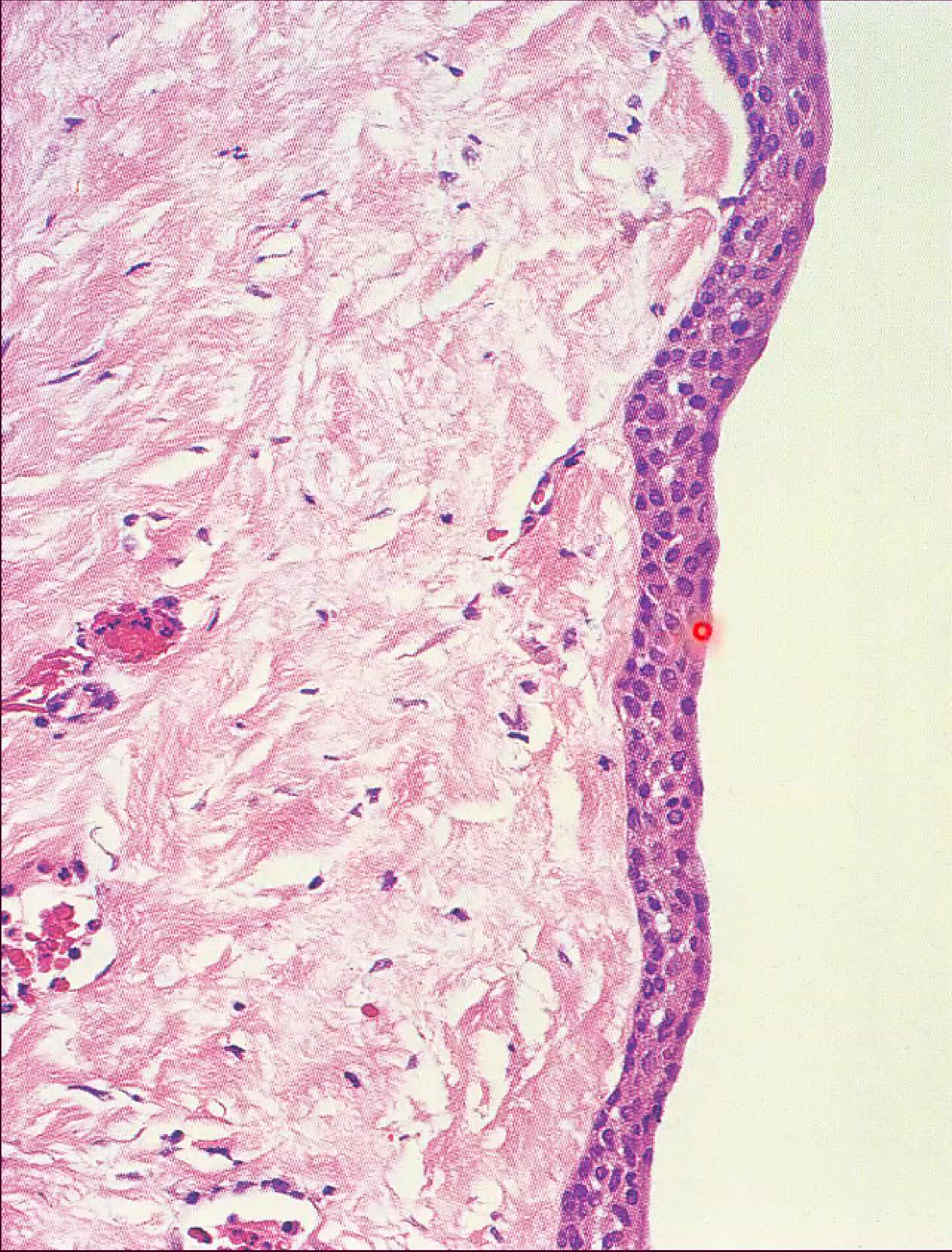
Eruption Cyst686970
 |  |
 |  |
Clinical Characteristics and Management71
- Considered an extra-alveolar dentigerous cyst.
- Associated with deciduous teeth or permanent molars.
- Presents as a fluctuant, often bluish swelling on the alveolar ridge.
Soft Tissue Presentation
The eruption cyst is essentially an extra-alveolar version of a dentigerous cyst that occurs specifically within the soft tissue over an erupting tooth.
- Hemorrhage into the cyst is common (sometimes called an eruption hematoma).
- Management:
- Most cases resolve spontaneously as the tooth erupts.
- Surgical intervention via marsupialization may be required if eruption is impeded.

Odontogenic Keratocyst
Clinical and Radiological Appearance727374
 |  |  |
 |  |  |
Clinical Presentation75
- Comprises 5-10% of all jaw cysts
- Gender predilection: Males > Females
- Often asymptomatic
- Common symptoms include:
- Swelling
- Discharge
- Pain
- Pathological fracture
- Tooth displacement
- Rarely buccal expansion
- 10% of cases present as multiple cysts
- Characterized by a high recurrence rate
Common Sites
- 70-80% occur in the mandible
- 50% are located in the angle or ramus
Pathogenesis76
- Derived from the dental lamina or its remnants (cell rests of Serres)
- Originate from the enamel organ (tooth primordium) of a tooth before hard tissues develop, involving:
- Normal teeth
- Supernumerary teeth
Radiographic Features77
- Well-demarcated radiolucency
- Appearance may be pseudolocular or multilocular
- Often exhibits a scalloped periphery
- Associated with root or tooth displacement
Histopathology and Recurrence7879
 |  |
Histological Features80
- Regular stratified squamous epithelium
- Thin epithelial layer (typically 5-8 cells thick)
- Palisaded basal layer
- Corrugated surface which can be parakeratinised or orthokeratinised
- Thin, friable fibrous capsule with little inflammation
- Presence of satellite (daughter) cysts
Patterns of Enlargement81
- Cancellous enlargement occurs in an antero-posterior direction
- Characterized by little or no bucco-lingual expansion
- Can become quite large, especially when located in the angle and ramus of the mandible
Factors Influencing Recurrence82
Recurrence rates are reported up to 60%. Contributing factors include:
- Large size and infiltrative nature
- Tendency toward multiplicity and the formation of satellite cysts
- Intrinsic growth potential
- Thin, friable capsule which is difficult to remove intact
- Genetic predisposition, such as multiple basal cell naevus syndrome (Gorlin-Goltz)
Gorlin-Goltz Syndrome8384
 |  |
 |
Clinical and Systemic Features85
- Multiple keratocysts of the jaws
- Multiple basal cell naevi, which may progress to carcinomas
- Skeletal abnormalities:
- Bifid ribs
- Spine defects
- Facial features including frontal bossing and hypertelorism
- Calcification of the falx cerebri
 |  |
Non-Odontogenic and Bone Lesions
Non-Odontogenic Developmental Cysts86
- Nasopalatine duct cyst
- Nasolabial (naso-alveolar) cyst
Nasopalatine Duct and Nasolabial Cysts87

Nasopalatine Duct Cyst (Incisive Canal Cyst)88
- Etiology: Derived from remnants of the nasopalatine duct.
- Demographics:
- Gender: Male to Female ratio of 4:1.
- Age: Typically occurs between 30–60 years.
- Clinical Presentation:
- Swelling of the midline of the palate.
- Pain and discharge (often described as mucoid and salty).
- Anterior teeth remain vital.
- Radiographically: Heart-shaped or oval radiolucency between central incisors.

Clinical Presentation89
Visual evidence of a nasopalatine duct cyst presenting as a visible cystic lesion in the oral cavity near the hard palate.

Diagnostic Imaging90
Radiographic and clinical documentation of a nasopalatine duct cyst.
Nasolabial Cyst91
- Clinical Features:
- Swelling in the nasolabial fold below the alae, leading to the loss of the fold.
- Can occasionally be bilateral.
- Symptoms include swelling, pain, and difficulty in nasal breathing.
- A soft tissue cyst with no bone involvement.
Simple Bone Cyst
Clinical Features92
- Description: An empty intra-osseous bone cavity.
- Etiology: Uncertain; possibly related to trauma causing intra-medullary hemorrhage.
- Demographics:
- Age: 10–20 years.
- Gender: Predominantly male (60%).
- Location: Mandibular body (molar-premolar region).
- Symptoms: Asymptomatic; may present as a painless swelling.
Pseudocyst Classification
Also called "Traumatic Bone Cyst," it is a pseudocyst because it lacks an epithelial lining.
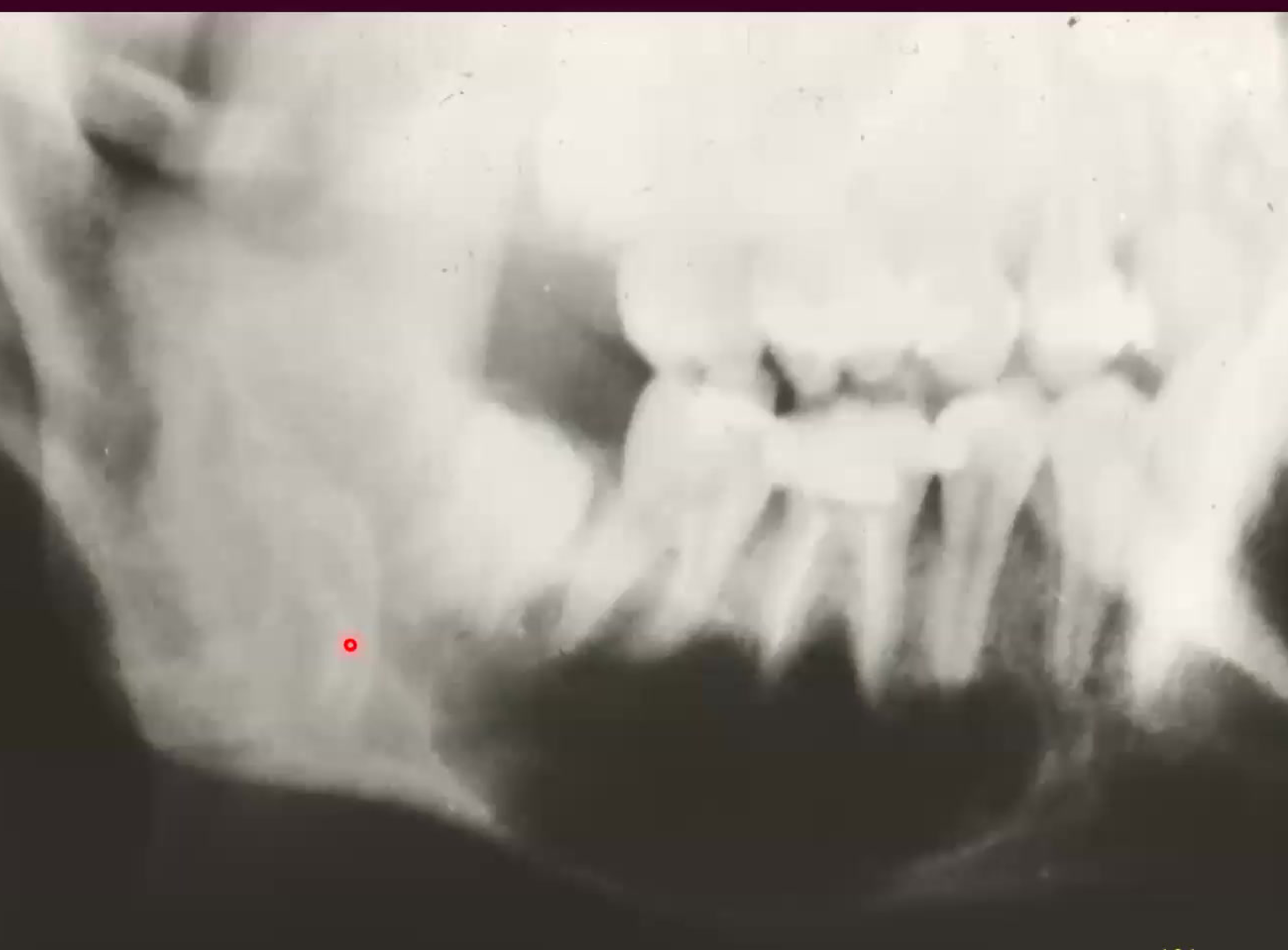
Radiographic Findings93
- Often an incidental finding.
- Appears as a radiolucency, ranging from well-defined to ill-defined.
- Size: 1–10 cm.
- Characteristics:
- Scalloping between the roots of the teeth.
- Associated teeth remain vital.
- No evidence of root resorption.
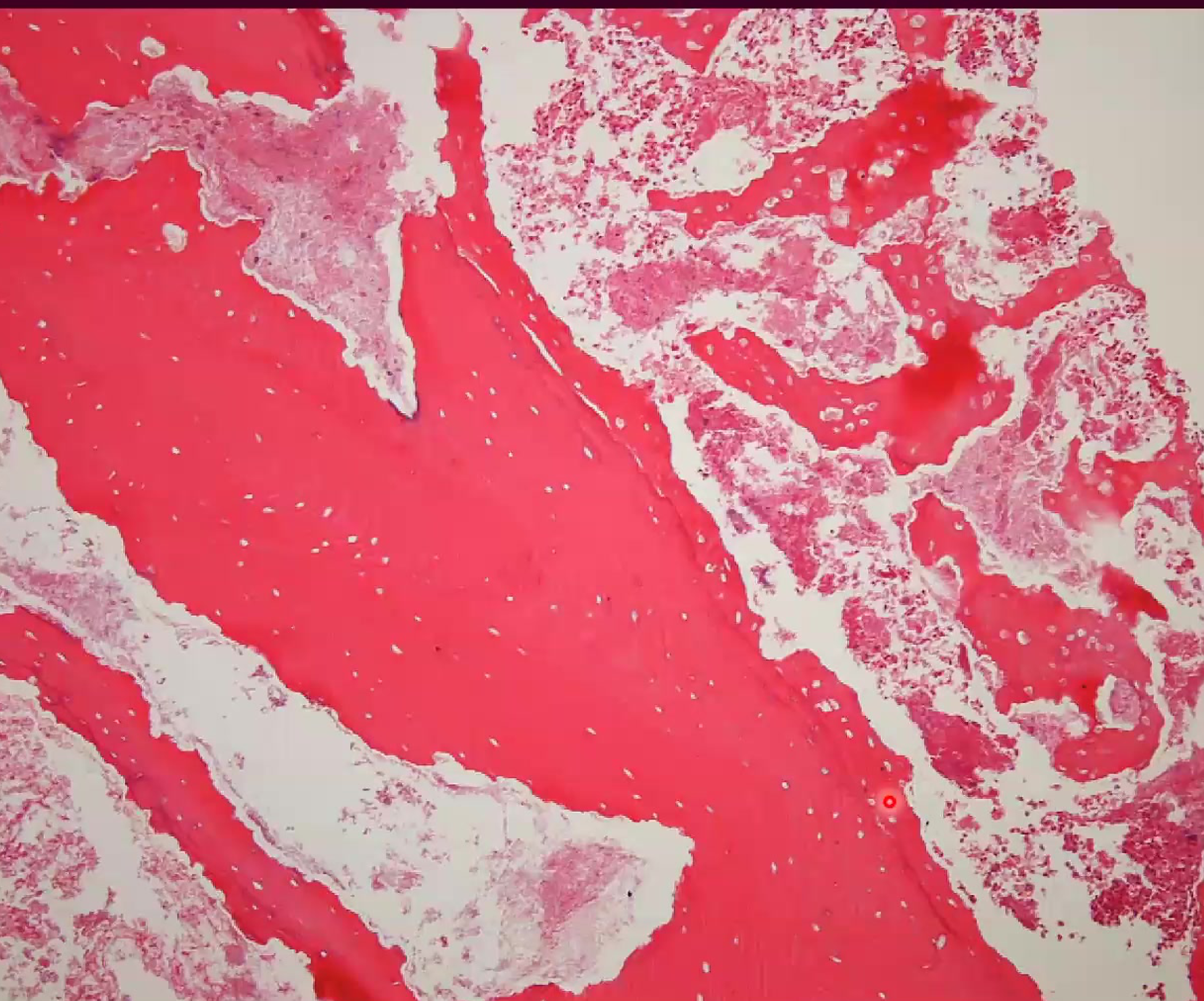
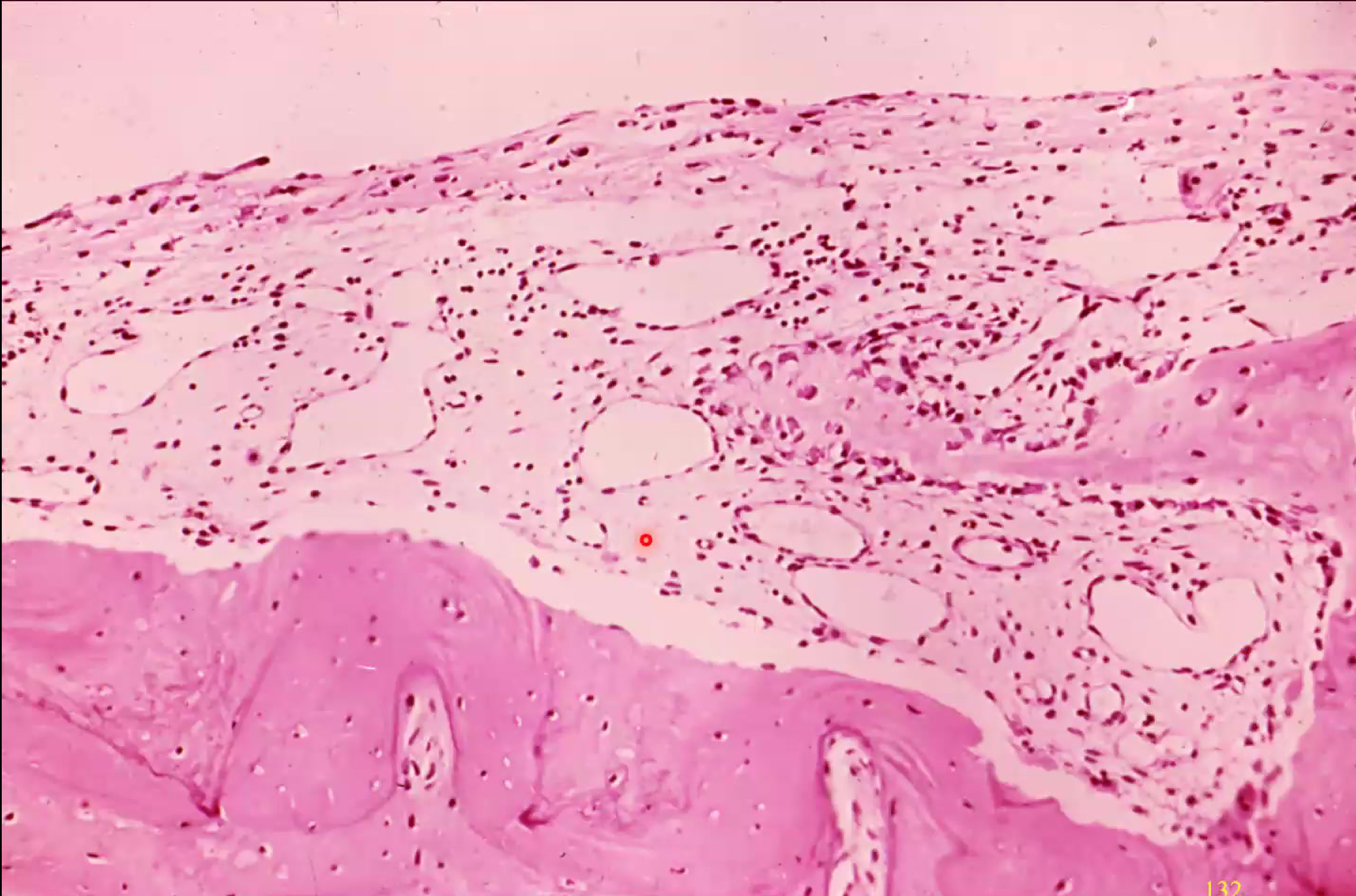
Histopathology9495
- Presence of a cortical bone cap.
- Evidence of bone resorption and remodeling.
- Membranous fibrovascular tissue.
- Presence of fibrin and hemorrhage.
- Characterized by the absence of an epithelial lining.
- Presence of serosangeous fluid upon asporactoin with needle
Microscopic Analysis9697
Microscopic view of tissue stained with hematoxylin and eosin (H&E) showing cellular structures associated with the lesion.
 |  |
 |
Simple Bone Cyst Treatment:
- surgical exploration
- Stimulate hemorrhage into defect
- Rapid spontaneous healing (6 months)
- Prognosis: excellent
- Recurrence: rare
- Follow up is important
- Assocaition with fibro-osseous lesions
Radiographic Case Study98
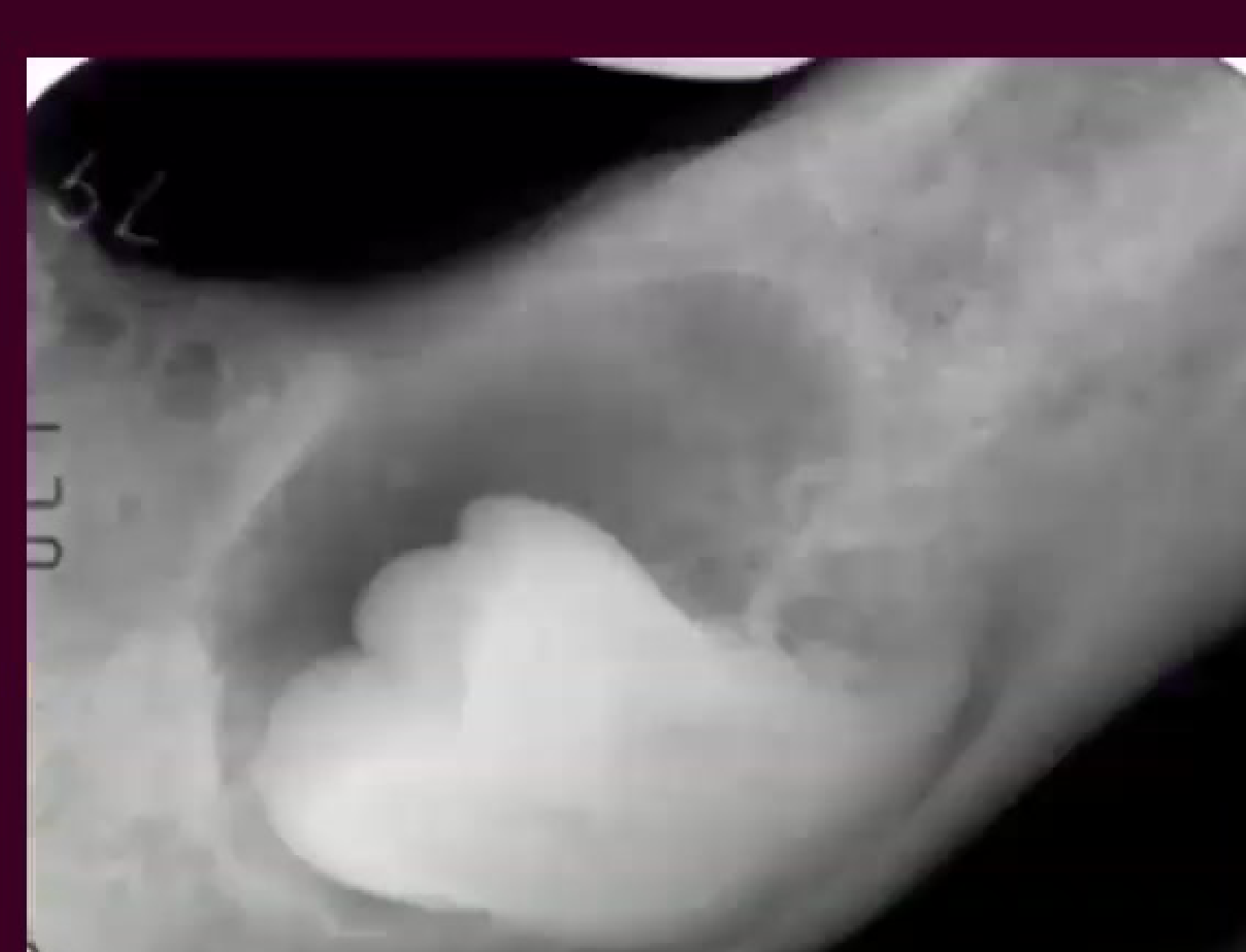
Stafne Cysts
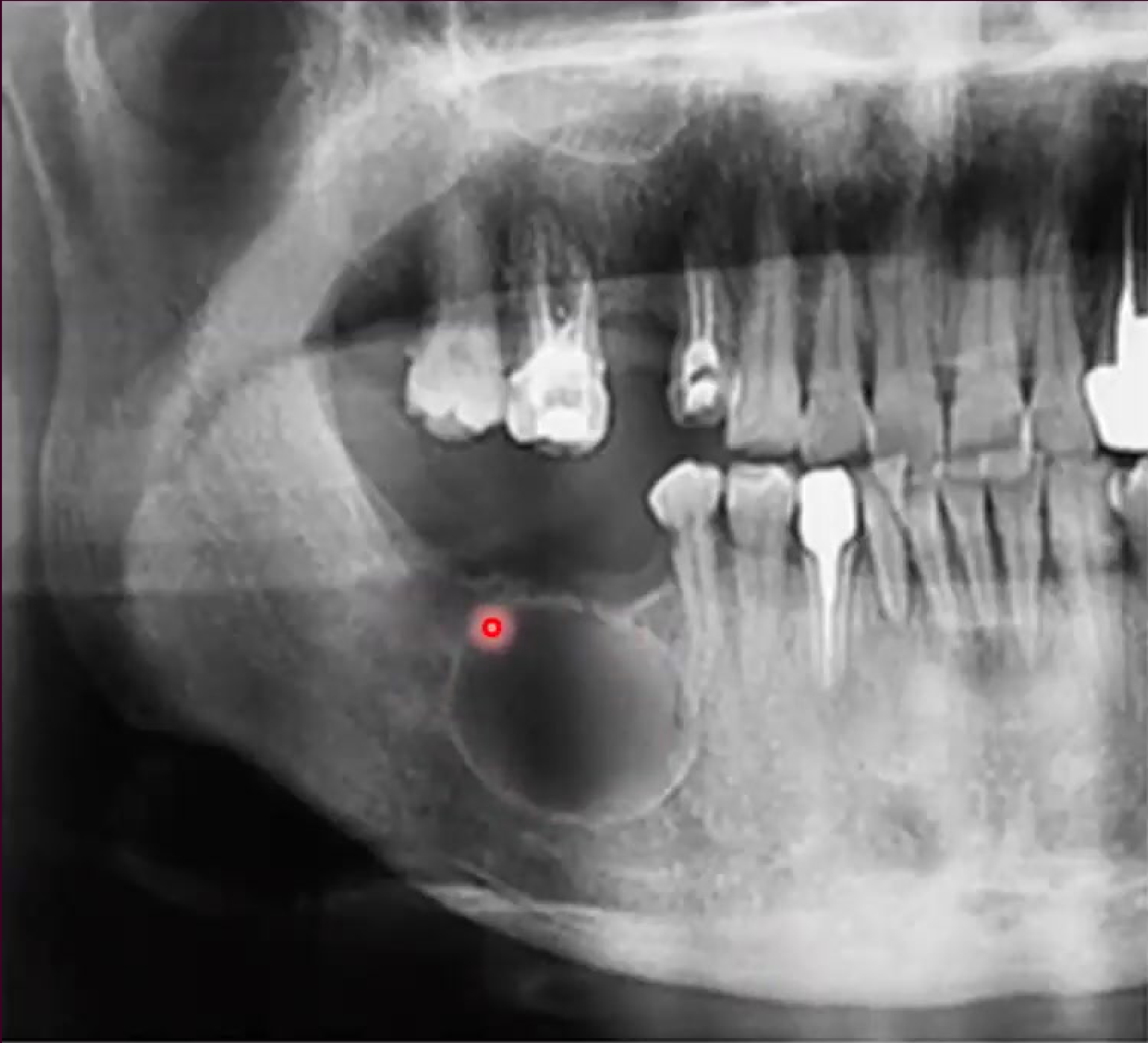
Clinical Overview99
- Synonyms: Static bone cavity of the mandible or lingual salivary gland inclusion defect.
- Demographics: Most commonly found in middle-aged men.
- Prevalence: Estimated to be approximately 0.10–0.48%
- Not a true cyst, but a developmental inclusion defect where the submandibular salivary gland creates a depression on the lingual aspect of the mandible.
- Located below the inferior alveolar nerve canal.
- Asymptomatic and requires no treatment.
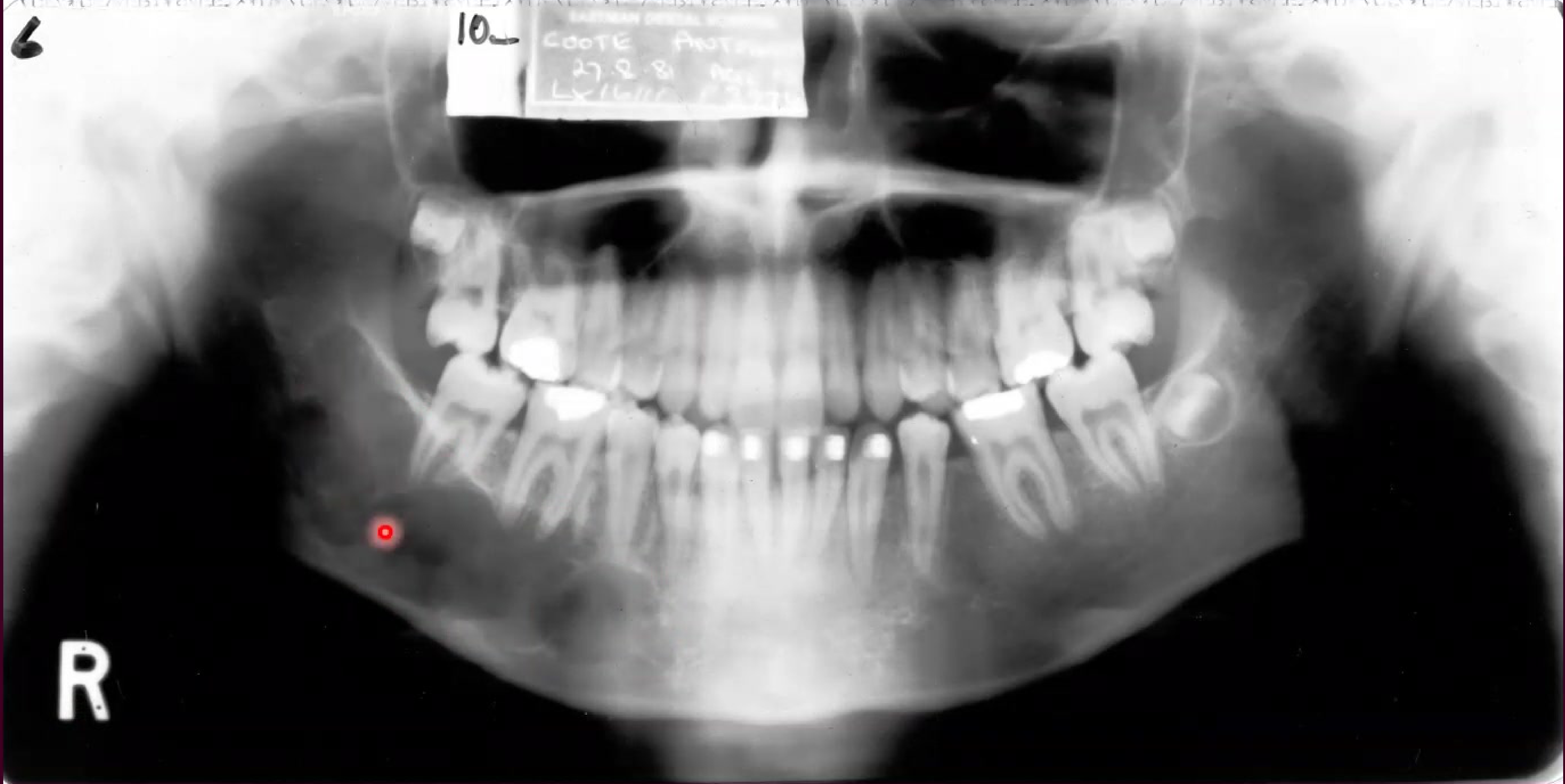
Radiographic Presentation100
Oral radiograph showing a highlighted region of interest in the mandible, characteristic of a Stafne cyst.
 |  |
 |
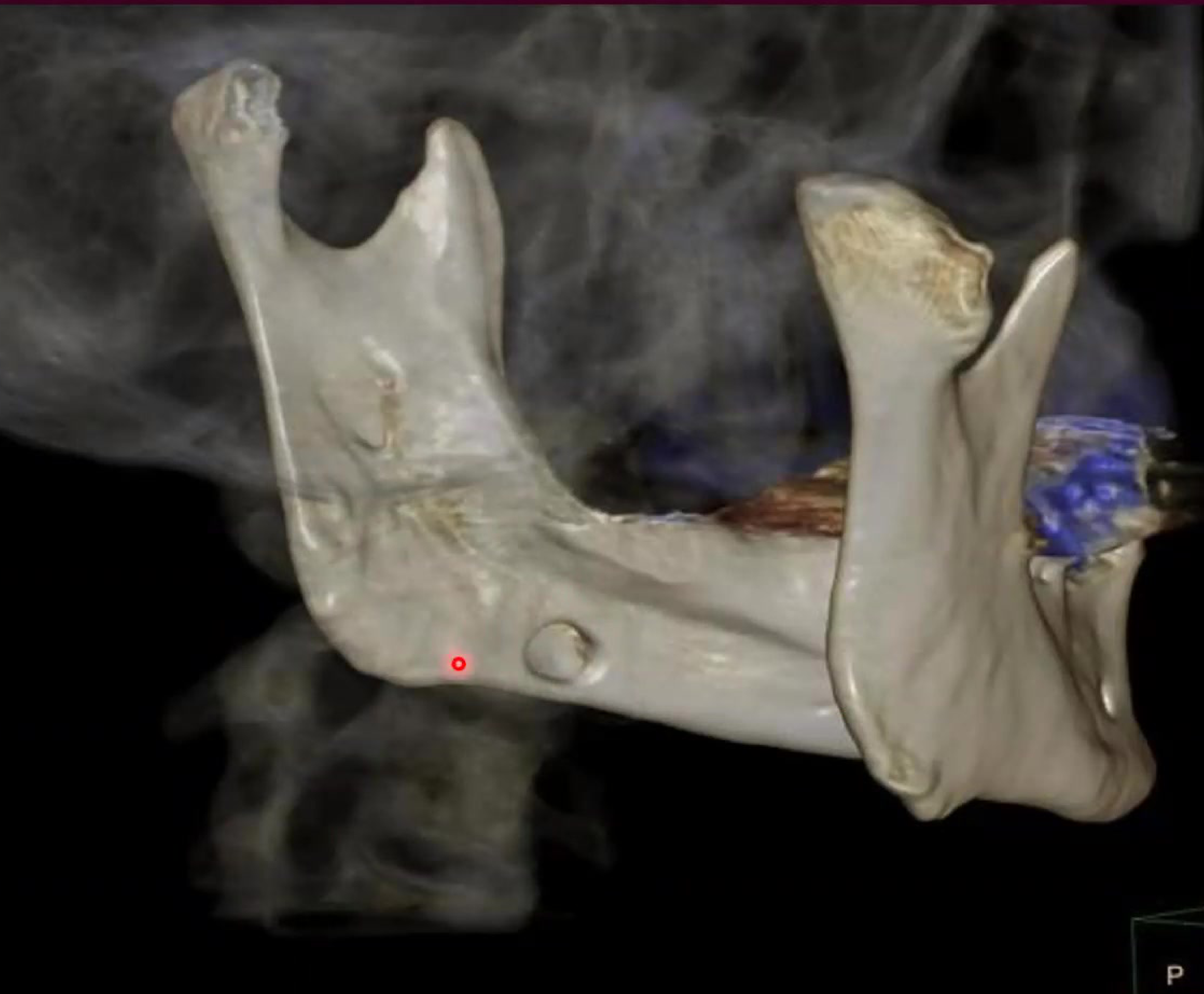
Advanced Imaging101
3D CT scan of the mandible indicating the location and scale of a mandibular lesion.
Conclusion
Summary of Findings102
This concluding section summarizes the clinical and radiographic characteristics of jaw cysts discussed throughout the presentation. Proper identification and classification remain essential for effective diagnosis and treatment planning.
Key Diagnostic Differentiators
Key diagnostic differentiators include tooth vitality, radiographic borders, and specific histological markers like keratinization or giant cells.
Presentation Closure103
End of slide show. Click to exit.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Central Giant Cell Granuloma (CGCG)
Clinical and Radiographic Features
Clinical Characteristics
- Demographics: Typically affects patients aged 30–60; more common in females.
- Location: 70% of cases occur in the anterior mandible.
- Presentation: Starts as a painless expansion but can grow to large sizes (0.5 cm to 10 cm), displacing teeth and disrupting occlusion.
Radiographic Presentation104
- Appears as a multilocular radiolucency with a “bubble-like” appearance.
- Borders are often ill-defined.
Histology and Treatment

Microscopic Findings105
- Two Cell Populations: Mononuclear spindle cells and multinucleated giant cells.
- Vascularity: Highly vascular with frequent hemorrhage.
- Pigmentation: Presence of hemosiderin (brownish pigment from red blood cell breakdown).
- Osteoid: Some areas may show osteoid formation.
Treatment Modalities
- Primary treatment is surgical (curettage).
- Aggressive or recurrent cases may require block resection.
Prognosis and Behavior
Recurrence rates are approximately 15–20%. While most are non-aggressive, some exhibit aggressive destructive behavior.
Differential Diagnosis and Hyperparathyroidism
Differential Diagnosis for Giant Cell Lesions
- Brown Tumor of Hyperparathyroidism: Histologically identical to CGCG.
- Aneurysmal Bone Cyst.
- Cherubism.
- Giant Cell Tumor: The aggressive long-bone equivalent.
Hyperparathyroidism and Bone Involvement
If a giant cell lesion is found, clinicians must check Parathyroid Hormone (PTH) levels.
Case Study: Vitamin D and PTH
A young patient presented with a well-defined cystic-looking radiolucent lesion. Blood chemistry revealed elevated PTH and severely low Vitamin D. Treating the Vitamin D deficiency led to the resolution of the bone lesion without surgery.
Odontogenic Keratocyst (OKC)
Clinical and Radiological Appearance
Clinical Presentation
- High recurrence rate.
- Arises from the Dental Lamina (Rests of Serres).
- 70–80% occur in the posterior mandible/ramus.
Radiographic Features
- Well-defined radiolucency, often multilocular with scalloped margins.
- Grows primarily in an anteroposterior direction within the medullary bone without causing significant buccal-lingual expansion.
Histopathology and Recurrence
Histological Features
- Uniform lining (8–12 cells thick).
- Palisaded basal layer (nuclei lined up like a fence).
- Corrugated (wavy) parakeratin surface.
- Presence of “Daughter Cysts” in the capsule contributes to high recurrence.
Gorlin-Goltz Syndrome
Clinical and Systemic Features
A genetic condition characterized by:
- Multiple OKCs.
- Multiple Basal Cell Carcinomas of the skin.
- Skeletal anomalies (bifid ribs, calcified falx cerebri).
- Frontal bossing.
Footnotes
-
Original PDF page 1: L18 Bone disease 2 slides, p.1 ↩
-
Original PDF page 2: L18 Bone disease 2 slides, p.2 ↩
-
Original PDF page 3: L18 Bone disease 2 slides, p.3 ↩
-
Original PDF page 4: L18 Bone disease 2 slides, p.4 ↩
-
Original PDF page 5: L18 Bone disease 2 slides, p.5 ↩
-
Original PDF page 6: L18 Bone disease 2 slides, p.6 ↩
-
Original PDF page 7: L18 Bone disease 2 slides, p.7 ↩
-
Original PDF page 8: L18 Bone disease 2 slides, p.8 ↩
-
Original PDF page 9: L18 Bone disease 2 slides, p.9 ↩
-
Original PDF page 10: L18 Bone disease 2 slides, p.10 ↩
-
Original PDF page 11: L18 Bone disease 2 slides, p.11 ↩
-
Original PDF page 12: L18 Bone disease 2 slides, p.12 ↩
-
Original PDF page 13: L18 Bone disease 2 slides, p.13 ↩
-
Original PDF page 14: L18 Bone disease 2 slides, p.14 ↩
-
Original PDF page 15: L18 Bone disease 2 slides, p.15 ↩
-
Original PDF page 16: L18 Bone disease 2 slides, p.16 ↩
-
Original PDF page 17: L18 Bone disease 2 slides, p.17 ↩
-
Original PDF page 18: L18 Bone disease 2 slides, p.18 ↩
-
Original PDF page 19: L18 Bone disease 2 slides, p.19 ↩
-
Original PDF page 27: L18 Bone disease 2 slides, p.27 ↩
-
Original PDF page 28: L18 Bone disease 2 slides, p.28 ↩
-
Original PDF page 29: L18 Bone disease 2 slides, p.29 ↩
-
Original PDF page 30: L18 Bone disease 2 slides, p.30 ↩
-
Original PDF page 31: L18 Bone disease 2 slides, p.31 ↩
-
Original PDF page 32: L18 Bone disease 2 slides, p.32 ↩
-
Original PDF page 22: L18 Bone disease 2 slides, p.22 ↩
-
Original PDF page 23: L18 Bone disease 2 slides, p.23 ↩
-
Original PDF page 34: L18 Bone disease 2 slides, p.34 ↩
-
Original PDF page 37: L18 Bone disease 2 slides, p.37 ↩
-
Original PDF page 35: L18 Bone disease 2 slides, p.35 ↩
-
Original PDF page 36: L18 Bone disease 2 slides, p.36 ↩
-
Original PDF page 38: L18 Bone disease 2 slides, p.38 ↩
-
Original PDF page 39: L18 Bone disease 2 slides, p.39 ↩
-
Original PDF page 40: L18 Bone disease 2 slides, p.40 ↩
-
Original PDF page 41: L18 Bone disease 2 slides, p.41 ↩
-
Original PDF page 42: L18 Bone disease 2 slides, p.42 ↩
-
Original PDF page 43: L18 Bone disease 2 slides, p.43 ↩
-
Original PDF page 44: L18 Bone disease 2 slides, p.44 ↩
-
Original PDF page 45: L18 Bone disease 2 slides, p.45 ↩
-
Original PDF page 46: L18 Bone disease 2 slides, p.46 ↩
-
Original PDF page 47: L18 Bone disease 2 slides, p.47 ↩
-
Original PDF page 48: L18 Bone disease 2 slides, p.48 ↩
-
Original PDF page 49: L18 Bone disease 2 slides, p.49 ↩
-
Original PDF page 56: L18 Bone disease 2 slides, p.56 ↩
-
Original PDF page 57: L18 Bone disease 2 slides, p.57 ↩
-
Original PDF page 58: L18 Bone disease 2 slides, p.58 ↩
-
Original PDF page 59: L18 Bone disease 2 slides, p.59 ↩
-
Original PDF page 60: L18 Bone disease 2 slides, p.60 ↩
-
Original PDF page 61: L18 Bone disease 2 slides, p.61 ↩
-
Original PDF page 62: L18 Bone disease 2 slides, p.62 ↩
-
Original PDF page 63: L18 Bone disease 2 slides, p.63 ↩
-
Original PDF page 64: L18 Bone disease 2 slides, p.64 ↩
-
Original PDF page 65: L18 Bone disease 2 slides, p.65 ↩
-
Original PDF page 66: L18 Bone disease 2 slides, p.66 ↩
-
Original PDF page 71: L18 Bone disease 2 slides, p.71 ↩
-
Original PDF page 72: L18 Bone disease 2 slides, p.72 ↩
-
Original PDF page 67: L18 Bone disease 2 slides, p.67 ↩
-
Original PDF page 68: L18 Bone disease 2 slides, p.68 ↩
-
Original PDF page 69: L18 Bone disease 2 slides, p.69 ↩
-
Original PDF page 51: L18 Bone disease 2 slides, p.51 ↩
-
Original PDF page 52: L18 Bone disease 2 slides, p.52 ↩
-
Original PDF page 53: L18 Bone disease 2 slides, p.53 ↩
-
Original PDF page 54: L18 Bone disease 2 slides, p.54 ↩
-
Original PDF page 55: L18 Bone disease 2 slides, p.55 ↩
-
Original PDF page 75: L18 Bone disease 2 slides, p.75 ↩
-
Original PDF page 73: L18 Bone disease 2 slides, p.73 ↩
-
Original PDF page 74: L18 Bone disease 2 slides, p.74 ↩
-
Original PDF page 76: L18 Bone disease 2 slides, p.76 ↩
-
Original PDF page 78: L18 Bone disease 2 slides, p.78 ↩
-
Original PDF page 79: L18 Bone disease 2 slides, p.79 ↩
-
Original PDF page 77: L18 Bone disease 2 slides, p.77 ↩
-
Original PDF page 83: L18 Bone disease 2 slides, p.83 ↩
-
Original PDF page 84: L18 Bone disease 2 slides, p.84 ↩
-
Original PDF page 85: L18 Bone disease 2 slides, p.85 ↩
-
Original PDF page 80: L18 Bone disease 2 slides, p.80 ↩
-
Original PDF page 81: L18 Bone disease 2 slides, p.81 ↩
-
Original PDF page 82: L18 Bone disease 2 slides, p.82 ↩
-
Original PDF page 87: L18 Bone disease 2 slides, p.87 ↩
-
Original PDF page 88: L18 Bone disease 2 slides, p.88 ↩
-
Original PDF page 86: L18 Bone disease 2 slides, p.86 ↩
-
Original PDF page 89: L18 Bone disease 2 slides, p.89 ↩
-
Original PDF page 90: L18 Bone disease 2 slides, p.90 ↩
-
Original PDF page 92: L18 Bone disease 2 slides, p.92 ↩
-
Original PDF page 93: L18 Bone disease 2 slides, p.93 ↩
-
Original PDF page 91: L18 Bone disease 2 slides, p.91 ↩
-
Original PDF page 94: L18 Bone disease 2 slides, p.94 ↩
-
Original PDF page 98: L18 Bone disease 2 slides, p.98 ↩
-
Original PDF page 95: L18 Bone disease 2 slides, p.95 ↩
-
Original PDF page 96: L18 Bone disease 2 slides, p.96 ↩
-
Original PDF page 97: L18 Bone disease 2 slides, p.97 ↩
-
Original PDF page 99: L18 Bone disease 2 slides, p.99 ↩
-
Original PDF page 100: L18 Bone disease 2 slides, p.100 ↩
-
Original PDF page 101: L18 Bone disease 2 slides, p.101 ↩
-
Original PDF page 102: L18 Bone disease 2 slides, p.102 ↩
-
Original PDF page 103: L18 Bone disease 2 slides, p.103 ↩
-
Original PDF page 104: L18 Bone disease 2 slides, p.104 ↩
-
Original PDF page 105: L18 Bone disease 2 slides, p.105 ↩
-
Original PDF page 106: L18 Bone disease 2 slides, p.106 ↩
-
Original PDF page 107: L18 Bone disease 2 slides, p.107 ↩
-
Original PDF page 70: L18 Bone disease 2 slides, p.70 ↩
-
Original PDF page 109: L18 Bone disease 2 slides, p.109 ↩
-
Original PDF page 110: L18 Bone disease 2 slides, p.110 ↩
-
Original PDF page 111: L18 Bone disease 2 slides, p.111 ↩
-
Original PDF page 108: L18 Bone disease 2 slides, p.108 ↩
-
Original PDF page 33: L18 Bone disease 2 slides, p.33 ↩