Bone Diseases
Course Information1
**DENT 5322 Part II
Course Context
This lecture focuses on benign cemento-osseous lesions, odontogenic tumors, and malignant bone neoplasms. It serves as the second part of a series, following the study of reactive, inflammatory, and cystic disorders. **
Overview of Benign Cemento-Osseous Lesions
- These disorders represent a combination of cementum-like lesions and bone-like changes.
Fibrous Dysplasia2
Fibrous dysplasia represents a category of benign cemento-osseous lesions characterized by the replacement of normal bone with fibrous connective tissue and irregular bone trabeculae.
Cemento-Osseous Dysplasias
These lesions are classified into three distinct clinical and radiographic subtypes:
- Periapical cemental dysplasia: Typically involves the mandibular anterior teeth.
- Focal cemento-osseous dysplasia: Usually presents as a single site of involvement.
- Florid cemento-osseous dysplasia: Characterized by multifocal or symmetric involvement across multiple quadrants of the jaws.
Cemento-Ossifying Fibroma
This group includes neoplastic lesions categorized into two primary subtypes:
-
Conventional cemento-ossifying fibroma: The standard presentation of the neoplasm.
-
Juvenile active (ossifying) fibroma: A more aggressive variant typically seen in younger patients.
- Associated with café-au-lait skin pigmentations
Fibrous Dysplasia3
Fibrous Dysplasia is a benign, non-neoplastic bone disorder characterized by a developmental defect in bone formation.
Clinical Characteristics and Genetics
Pathological Overview4
- Benign disorder of bone
- Non-neoplastic tumor-like lesion
- Developmental defect in bone formation
- Fibrous proliferation
- Disorderly malformed woven bone
- Enlarged deformed bones
- Structurally weak
Clinical Presentation and Genetics5
- Common Sites: Ribs, femur, tibia, pelvis, and craniofacial bones
- Age of Onset: Typically occurs in childhood through adolescence
- Lesion Characteristics:
- Single or multiple bony lesions
- Slow growing
- Painless
- Often quiesces (stabilizes) at puberty
- Genetics: Associated with the GNAS I gene located on chromosome 20q13.1-2
Classification and Syndromes
Classification Types6
- Monostotic
- Accounts for 70% of cases
- Craniofacial involvement in 25% of cases
- Polyostotic
- Accounts for 25% of cases
- Craniofacial involvement in 50% of cases
- McCune-Albright Syndrome
- Accounts for 3% of cases
- Characterized by associated endocrine abnormalities
Oral and Maxillofacial Manifestations
Clinical Symptoms7
- Painless swelling
- Facial asymmetry
- Malocclusion and displaced teeth
- Headache
- Hearing loss
Laboratory Findings
- Clinical labs may show elevated alkaline phosphatase levels.
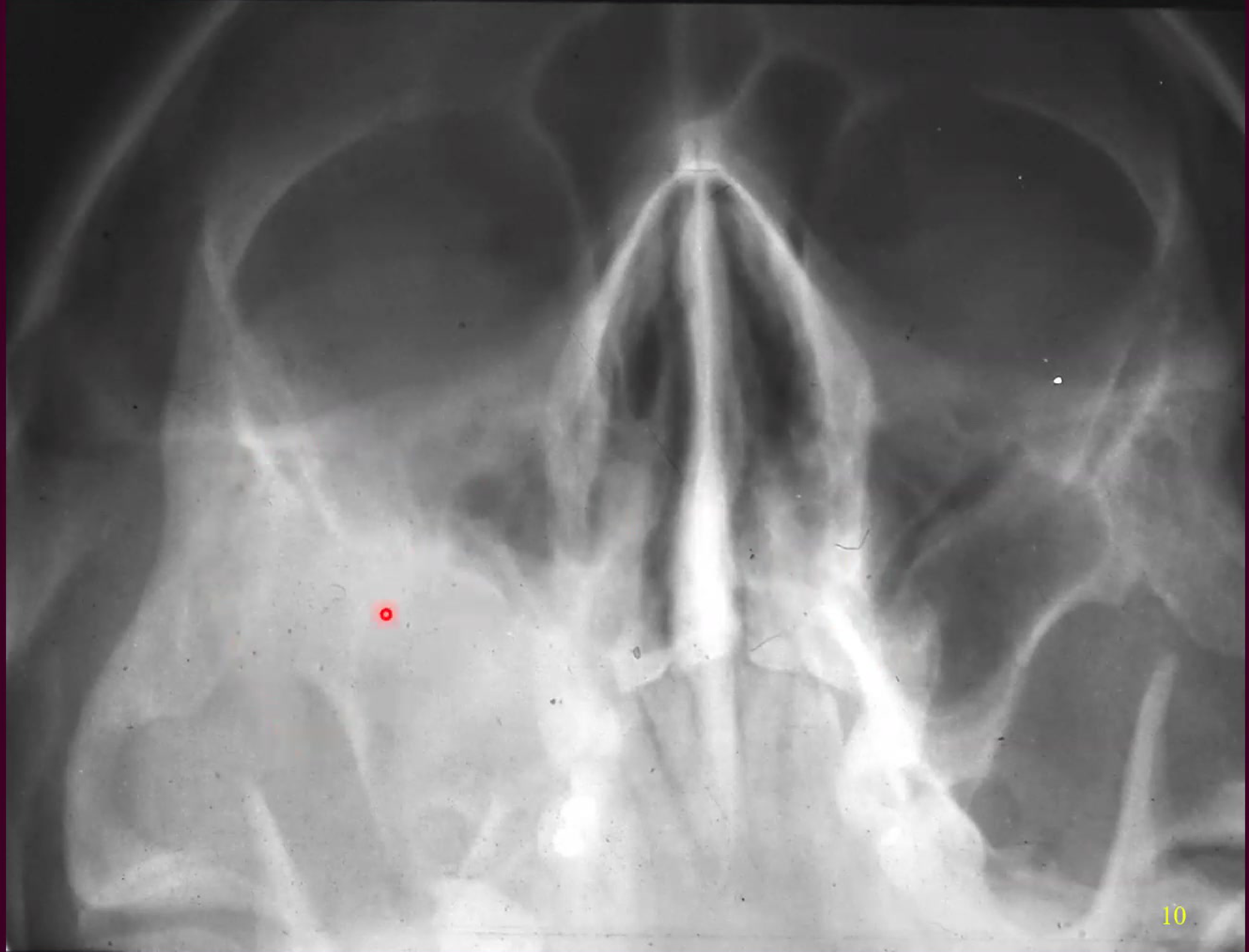
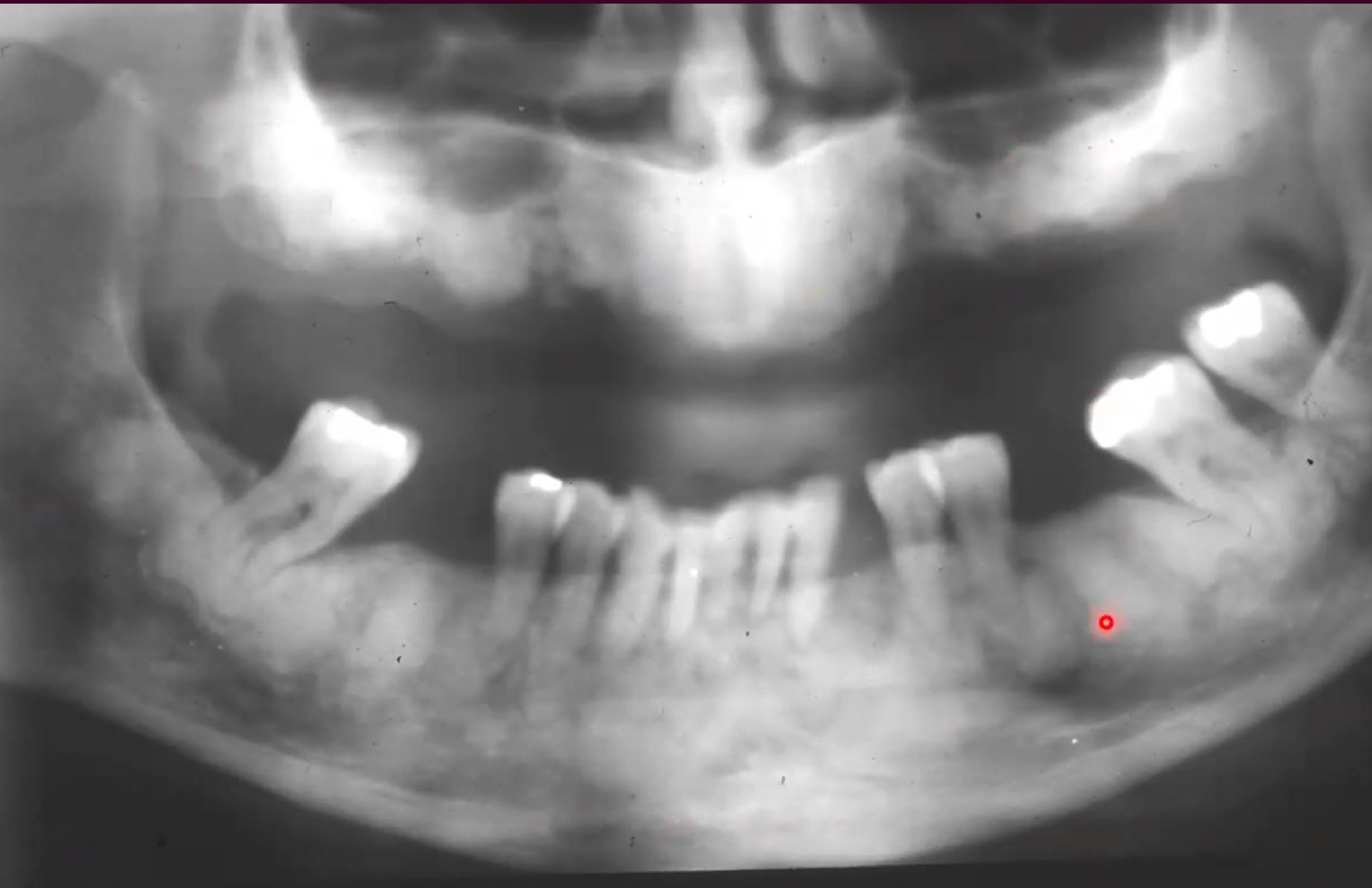
Radiographic Features8910
 |  |  Radioopaque area Radioopaque area |
 |  Condensed area in the mandible Condensed area in the mandible | |
Imaging Characteristics11
- Ground Glass Appearance: Classic opacification pattern
- Margins: Diffuse and poorly delineated
- Bone Changes: Cortical expansion resulting in fusiform enlargement
- Dental Implications:
- Narrow periodontal ligament
- Obscured lamina dura
- Early Progression: Early lesions may appear radiolucent or mottled - Lesions become mixed (radiolucent/radiopaque) and eventually dense/opaque over time
Radiographic evidence of fibrous dysplasia in the jawbone demonstrates characteristic changes in bone density and effects on the surrounding tooth structures.
S
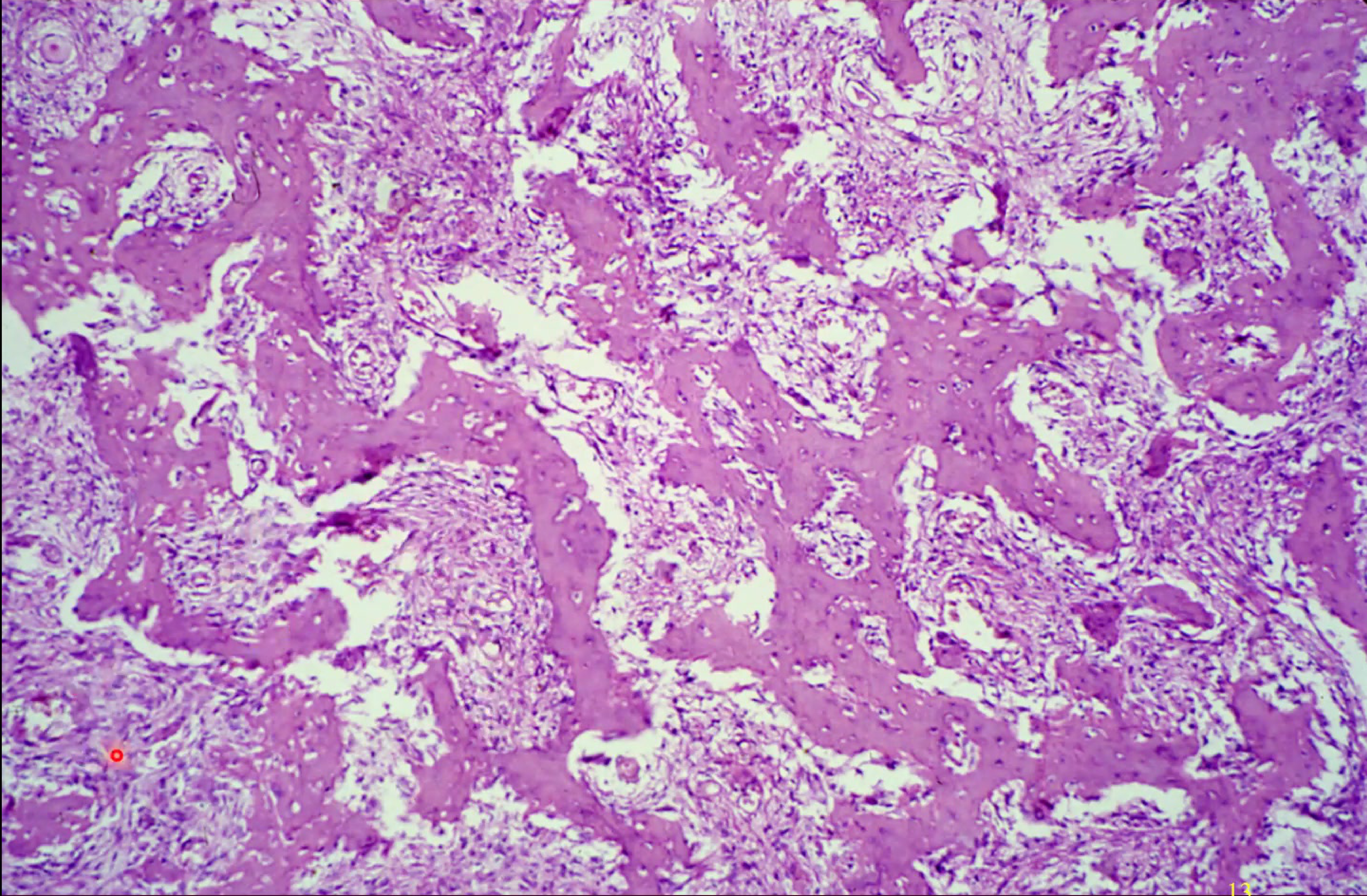
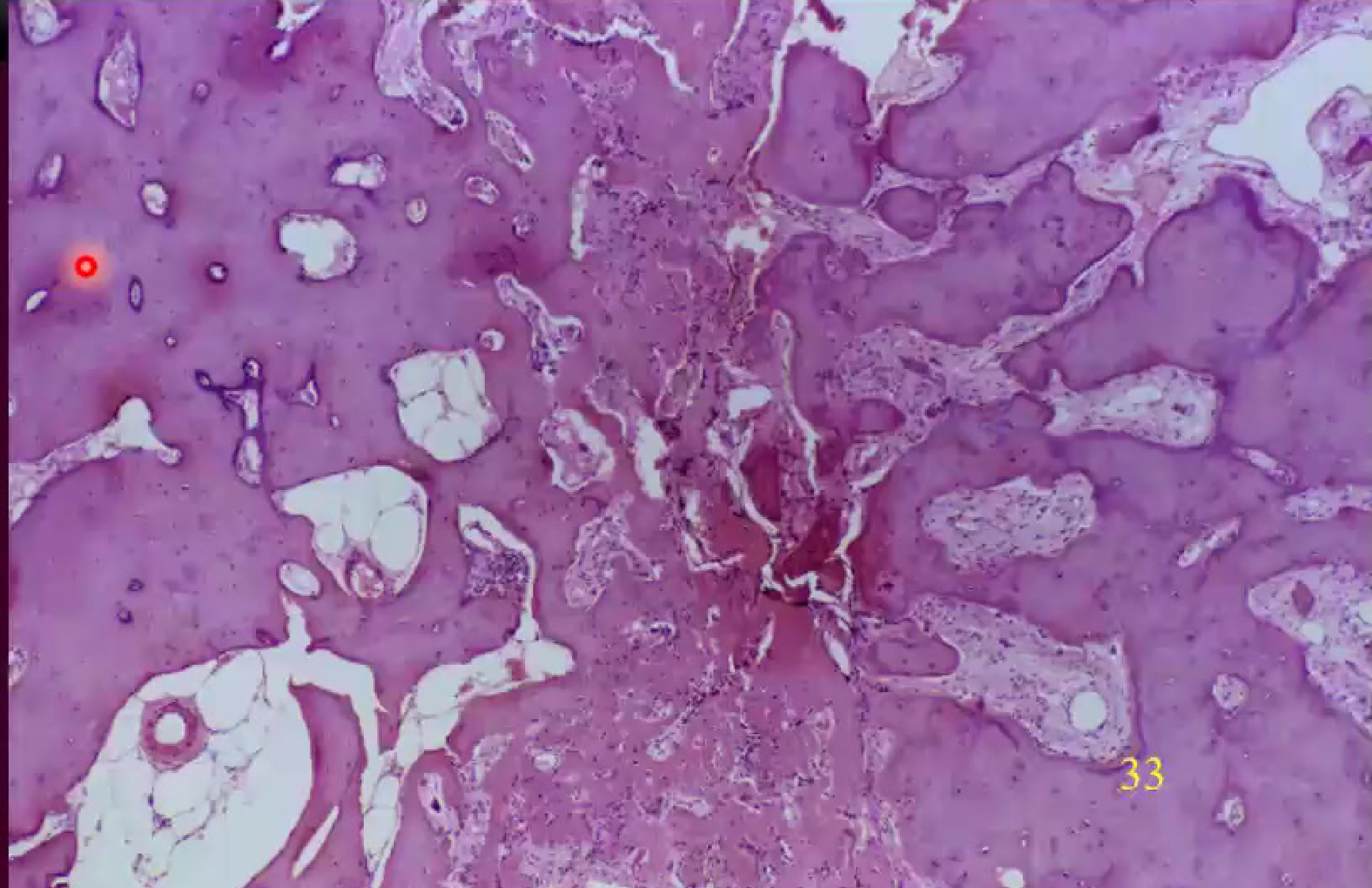
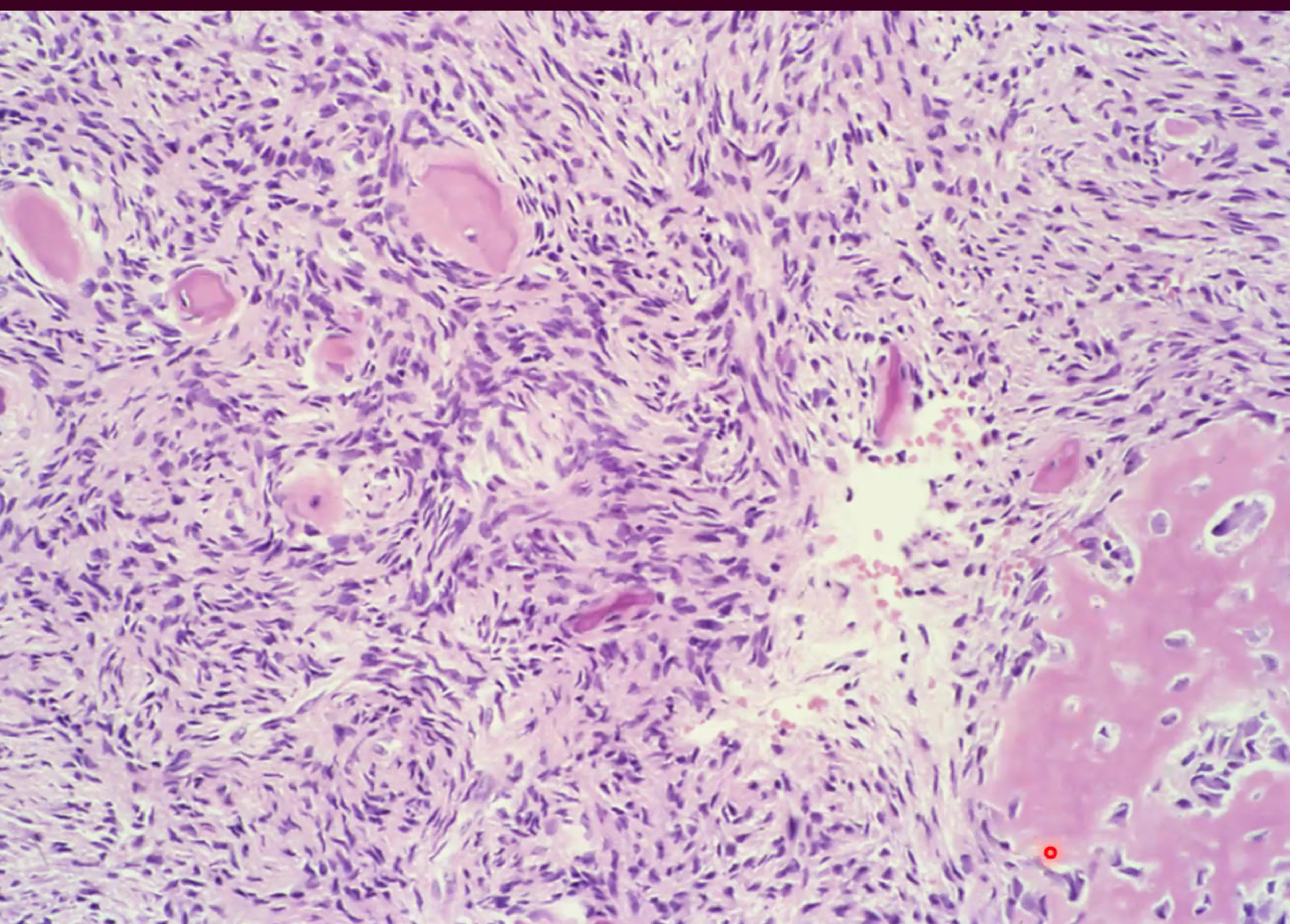
Histopathology1213
 Chinese character-like histology Chinese character-like histology | 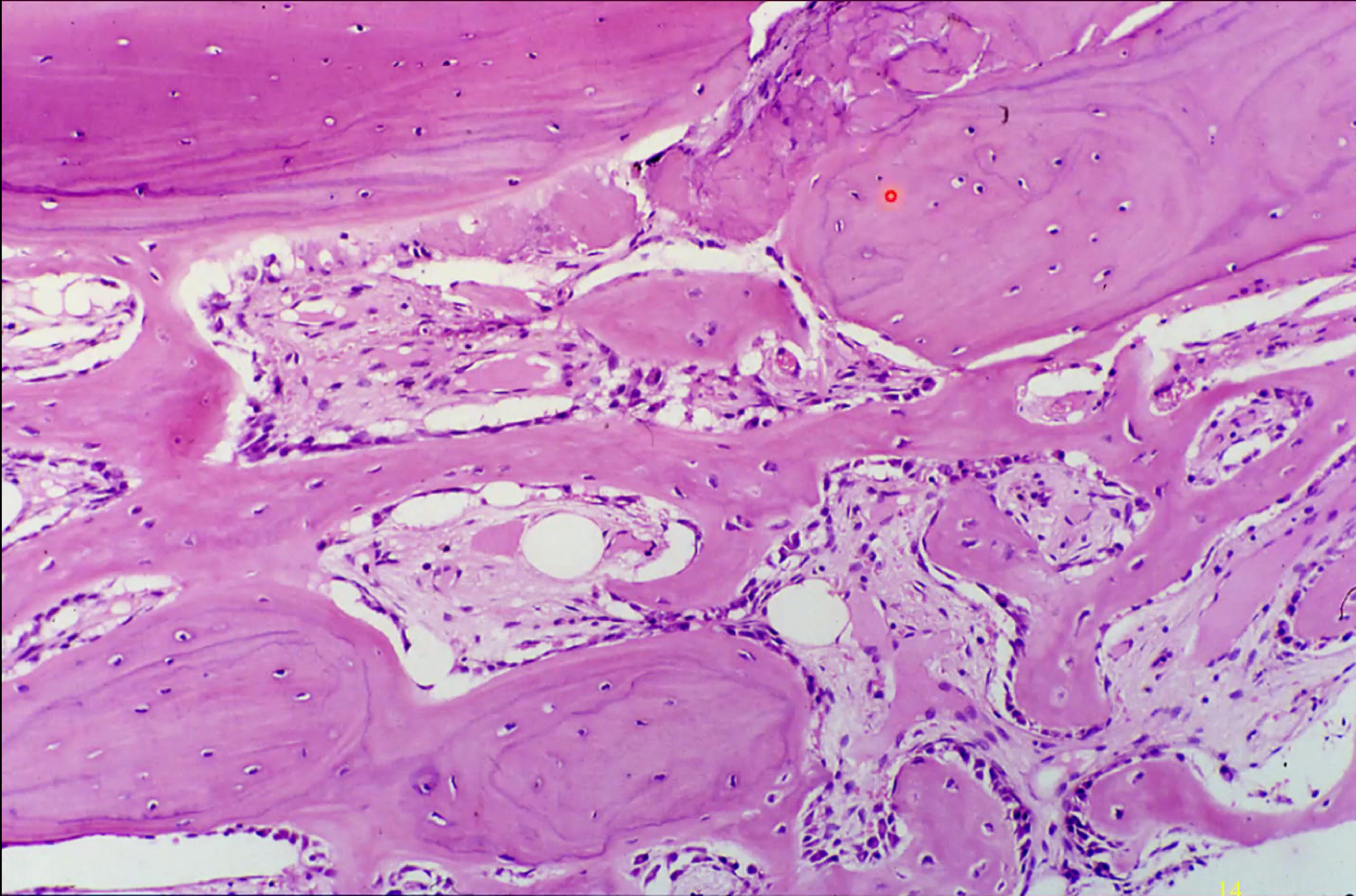 |
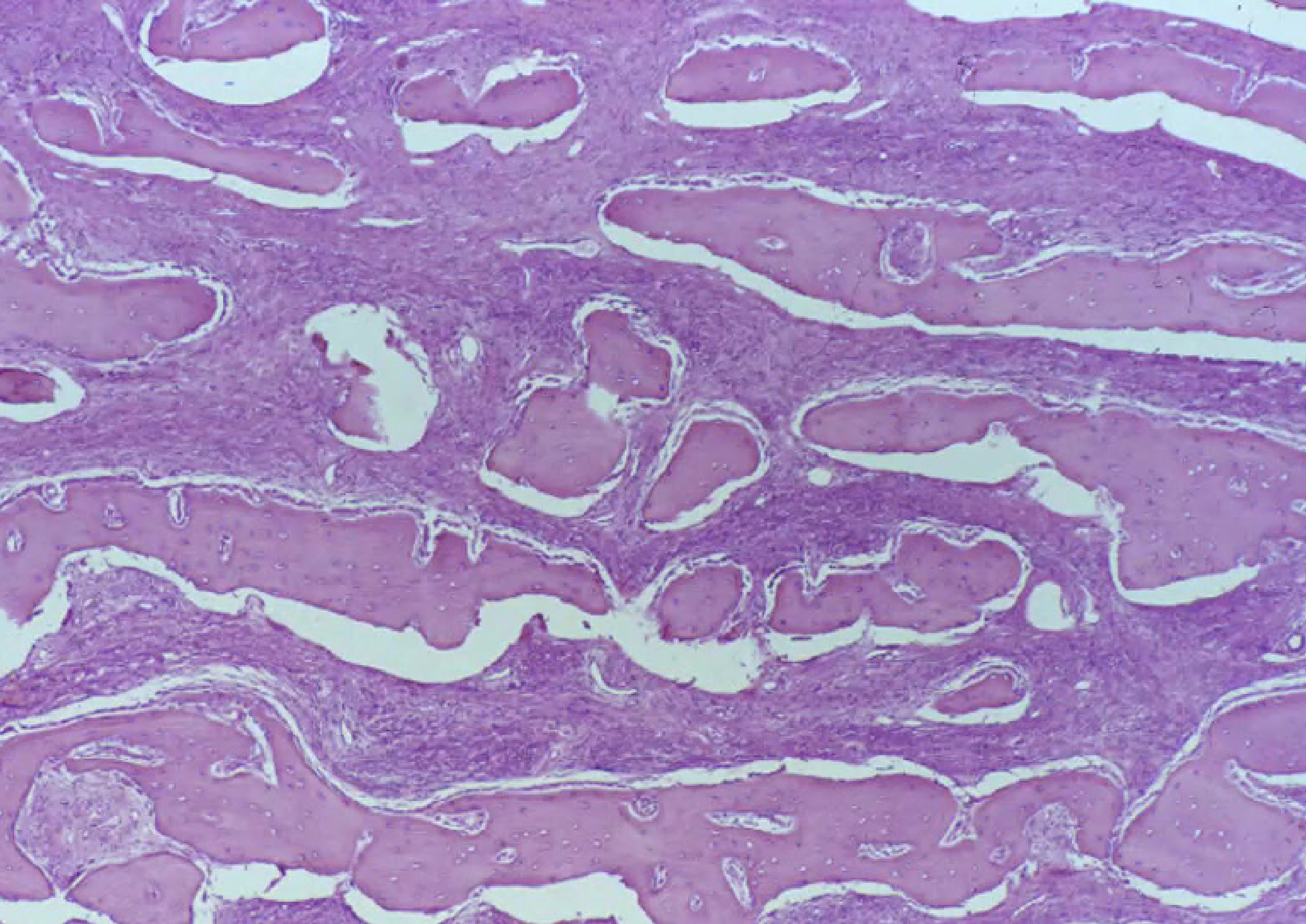
Microscopic Features14
- Bone Structure: Woven bone with irregular trabeculae often described as resembling “Chinese Characters”
- Stroma: Fibrous stroma present - The fibroblastic stroma is highly cellular
- Cellular Features: Absence of an osteoblastic lining
- Margins: Blends into normal bone without a capsule
- Progression: Potential maturation into lamellar bone - As the lesion matures, the amount of calcification increases and bone becomes more prominent
Microscopic tissue analysis using hematoxylin and eosin staining reveals the cellular structures and extracellular matrix characteristic of the lesion.
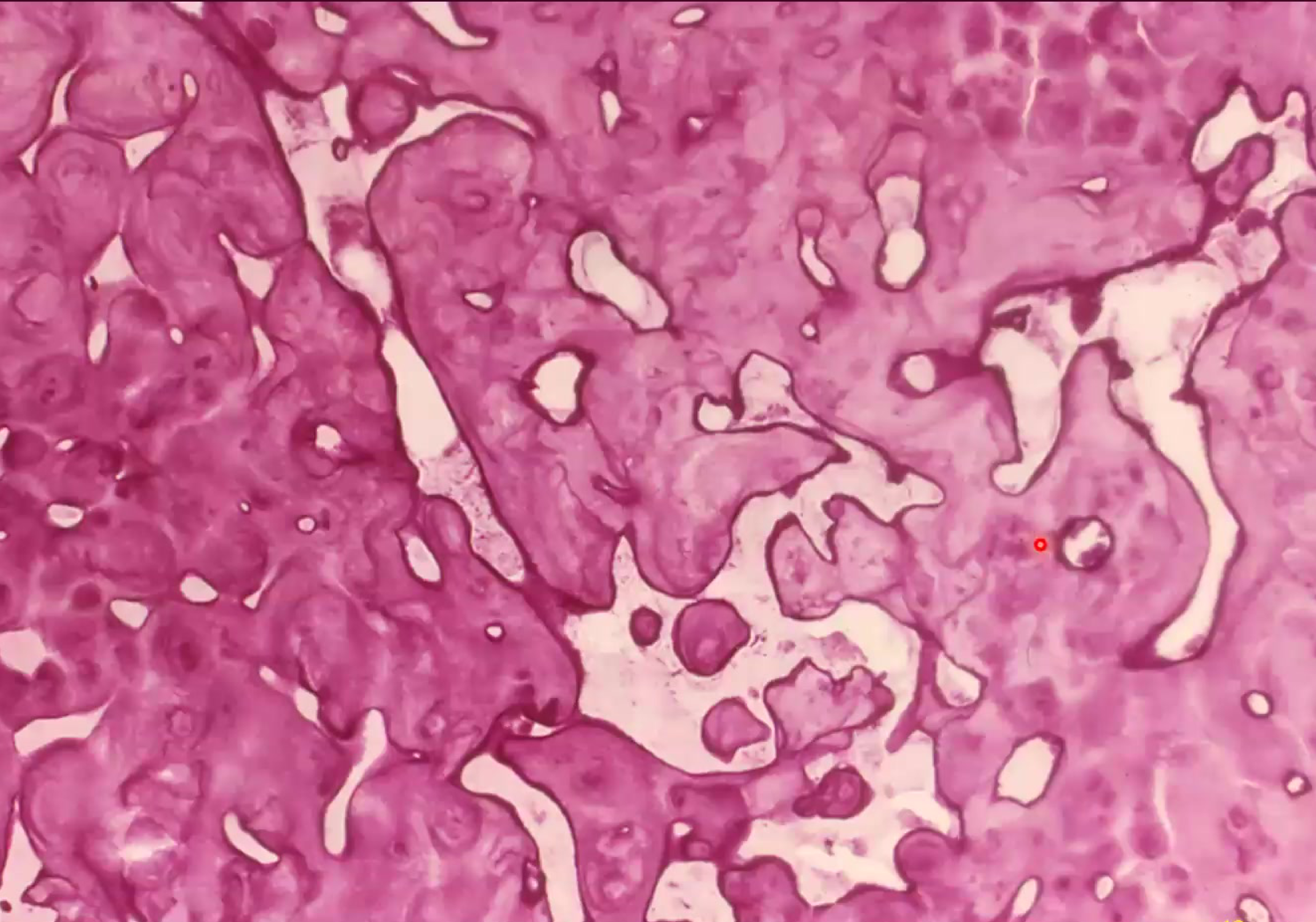
Growth Phase15
- Cellular - growing: Microscopic view showing active cellular proliferation within the tissue.
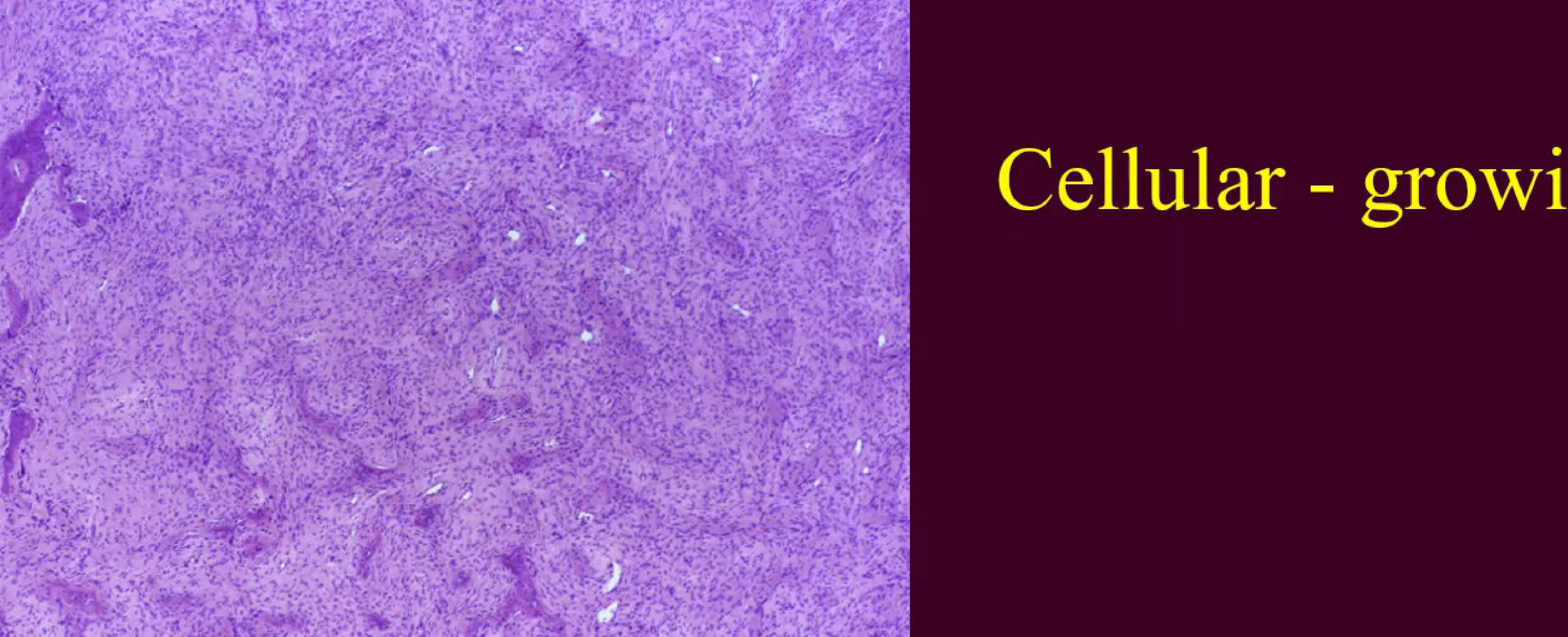 growth phase, radiolucent growth phase, radiolucent | 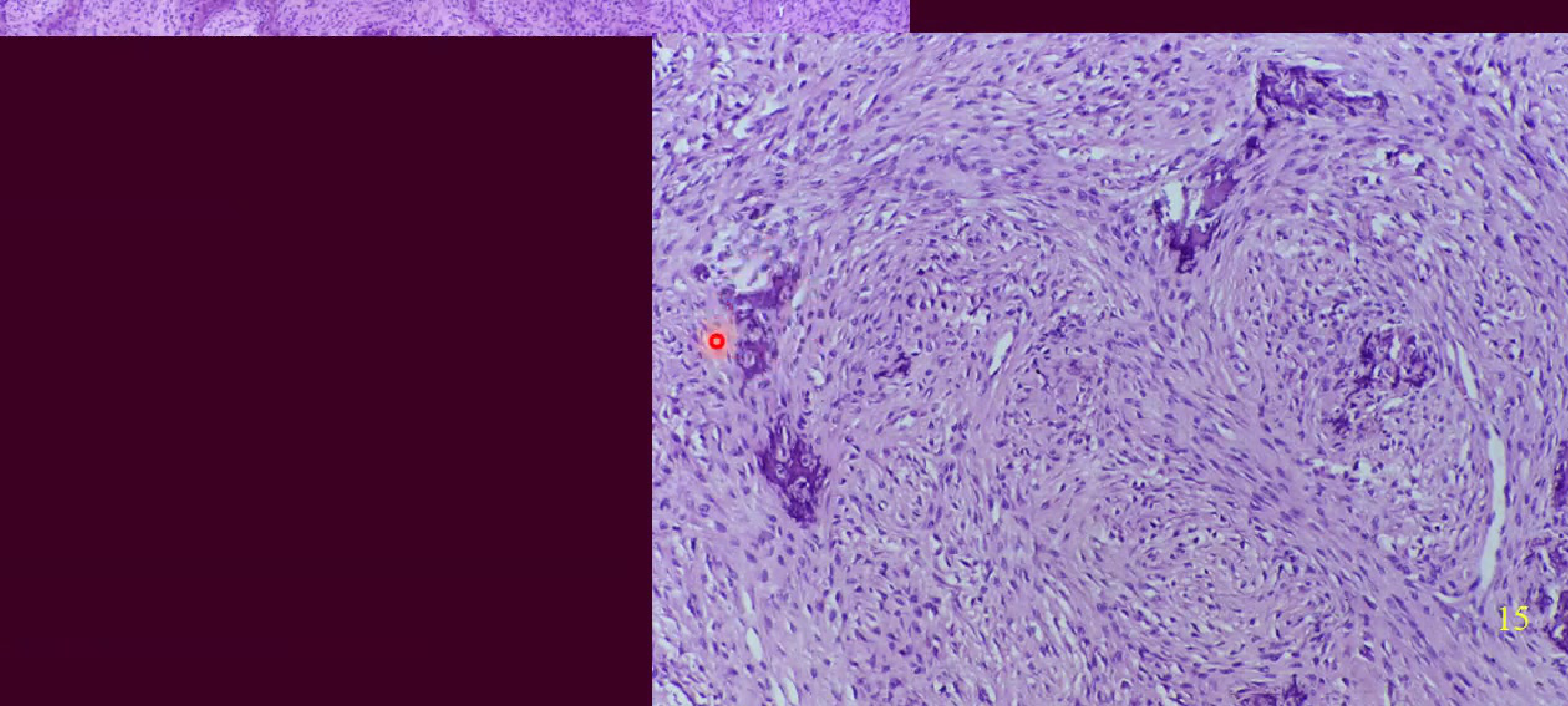 Mature - increased focal areas, woven bone and radioopque Mature - increased focal areas, woven bone and radioopque |
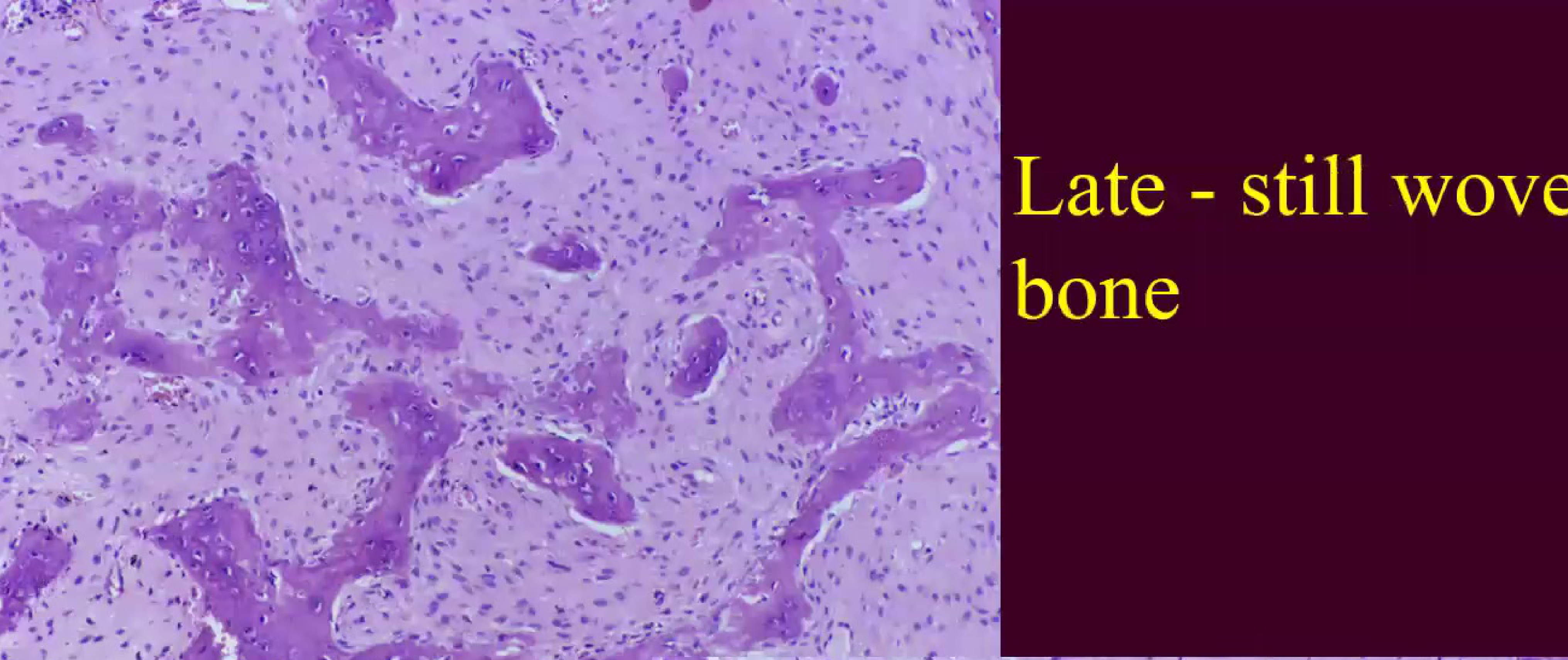
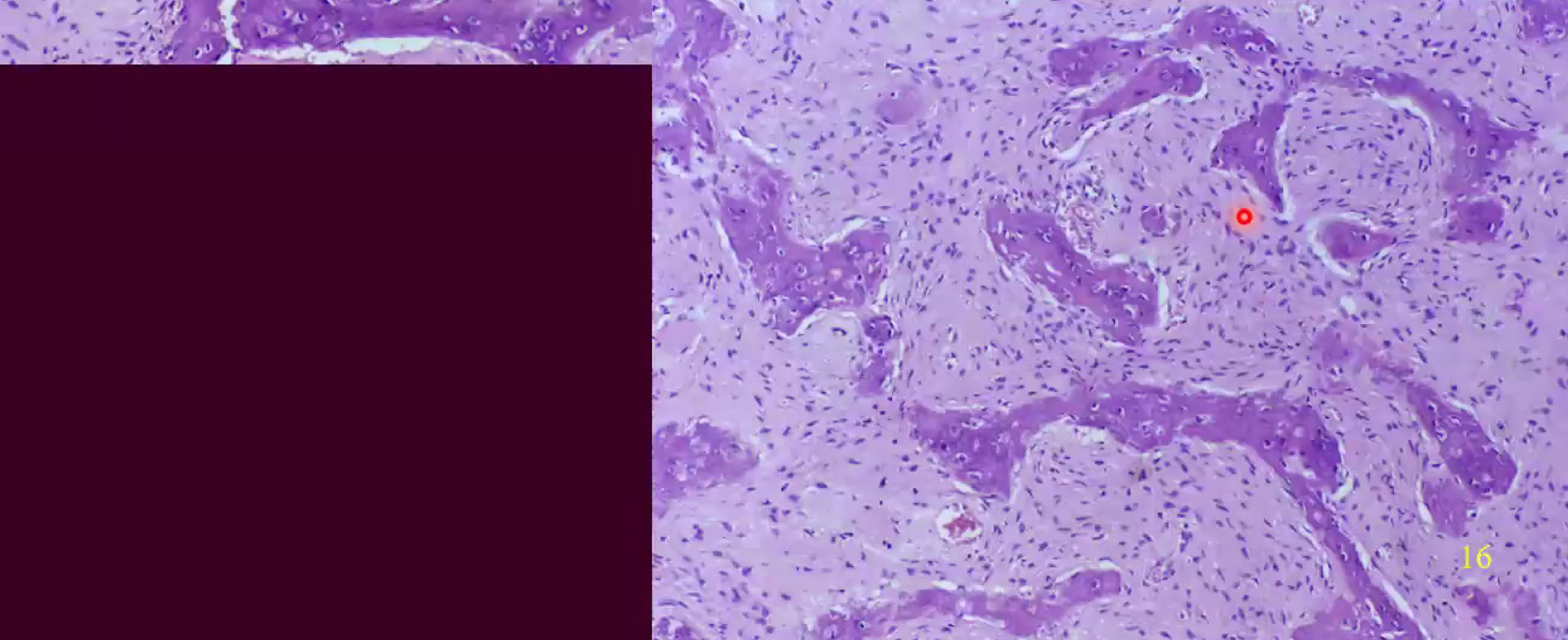
Late Stage Histology16
- Late - still woven bone: Histological evidence showing that even in later stages, the bone often retains its woven architecture.
 |  |
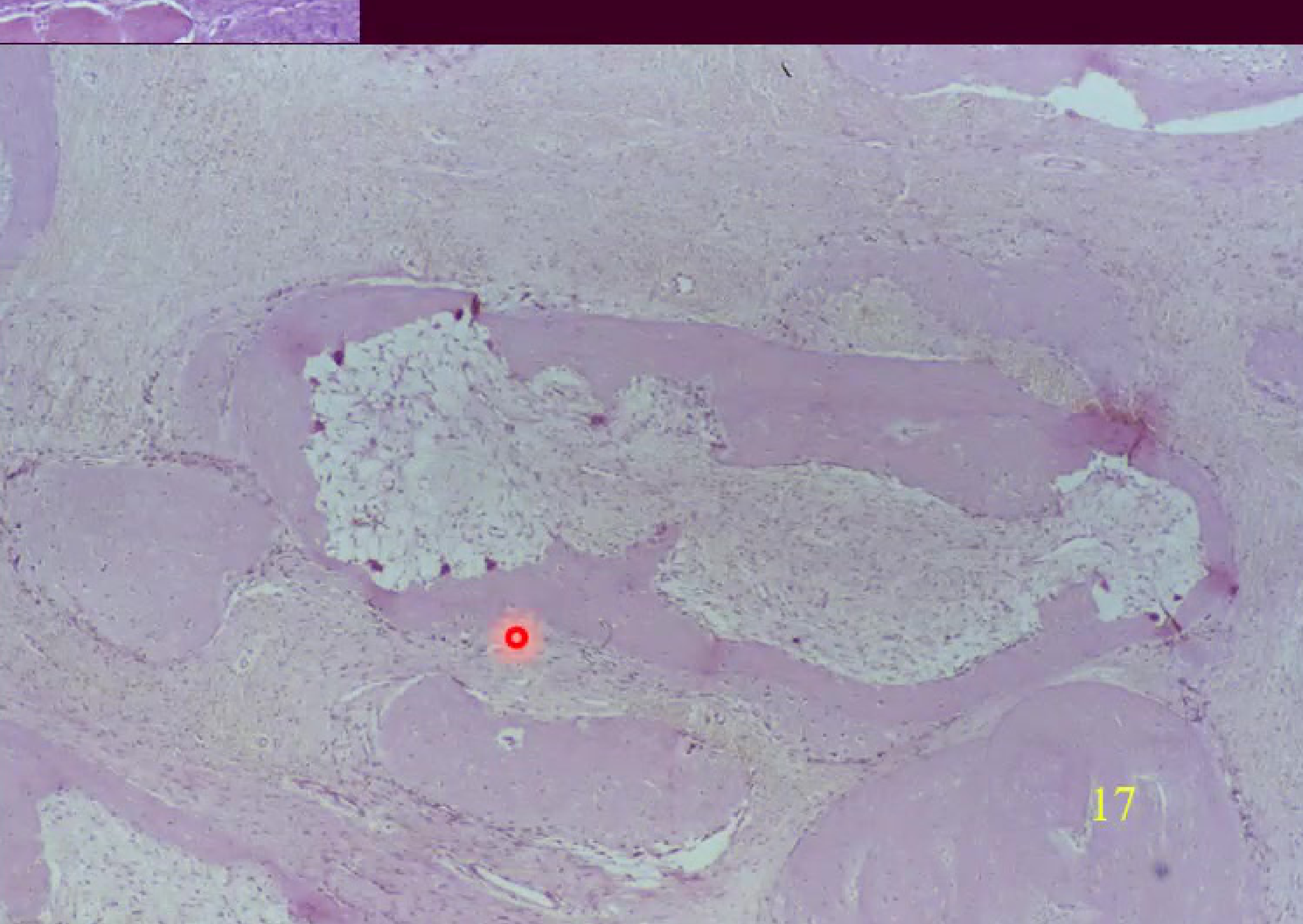
Tissue Variations17
- Old fibrous dysplasia: Characteristics of long-standing lesions.
- Reactivated area: Evidence of renewed activity or growth within an established lesion.
 |  |
Complications and Malignant Degeneration1819
Clinical Complications20
- Debilitating deformities
- Esthetic and psychosocial concerns
- Malocclusion
- Pathologic fractures
- Cranial nerve and orbital involvement
Malignant Transformation
- Rare occurrence (less than 1%)
- Most commonly transforms into osteosarcoma
Radiation Precaution
It is critical to avoid radiation therapy in these areas, as it significantly increases the risk of malignant transformation into osteosarcoma.
- Debilitating deformities
- Esthetic/psychosocial concerns
- Malocclusion
- Pathologic fractures
- Cranial nerve and orbital involvement
Malignant Degeneration21
-
Rare (< 1%)
-
Osteosarcoma
-
Avoid radiation therapy
-
Debilitating deformities
-
Esthetic/psychosocial concerns
-
Malocclusion
-
Pathologic fractures
-
Cranial nerve and orbital involvement
-
Rare (< 1%)
-
Osteosarcoma
-
Avoid radiation therapy
Management and Prognosis
Treatment Strategies22
- Treatment may not be required in all cases.
- Conservative Management: Often preferred as the condition typically stabilizes with skeletal maturity.
- Surgical Considerations:
- Diffuse involvement often precludes complete excision.
- Surgery is indicated for cosmetic and functional deformities.
- Procedures include surgical recontouring or decompression.
- Prognosis: Regrowth occurs in 25-50% of cases, primarily in younger patients.
Periapical Cemento-Osseous Dysplasia23
Periapical cemento-osseous dysplasia is a specific form of bone dysplasia that occurs in the periapical region of the jaws.
Clinical and Radiographic Findings242526
 |  |
 |
Clinical Presentation27
Periapical cemento-osseous dysplasia is a benign, non-neoplastic dysplastic process with the following clinical characteristics:
- Incidence: Relatively common.
- Demographics:
- Age: Typically affects middle-aged individuals (30–50 years).
- Gender: Strong female predilection (14:1 ratio).
- Race: More frequently observed in Black populations.
- Location: Primarily involves the mandibular anterior periapical area.
- Symptoms: The condition is asymptomatic; teeth remain vital, and there is no cortical expansion.
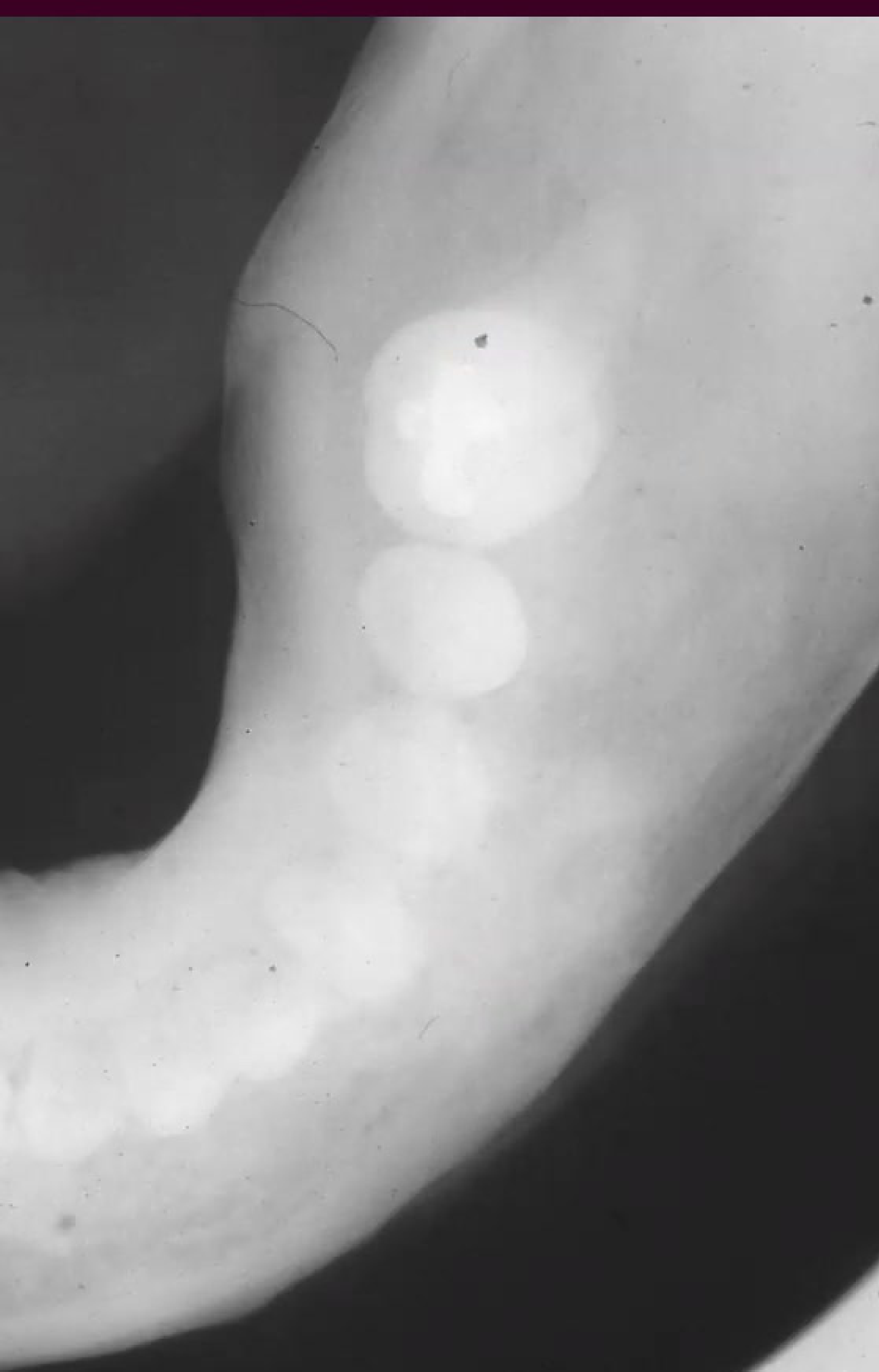
Radiographic Characteristics28
- Distribution: Often presents as multiple lesions.
- Appearance: Circumscribed apical radiolucencies with variable degrees of radiopacity depending on the stage of maturation.
- Size: Generally less than 1.0 cm in diameter.
- Intact Lamina Dura: The lamina dura remains visible around the root apex.
- Impact on Structures: Non-expansile nature; associated teeth remain vital.
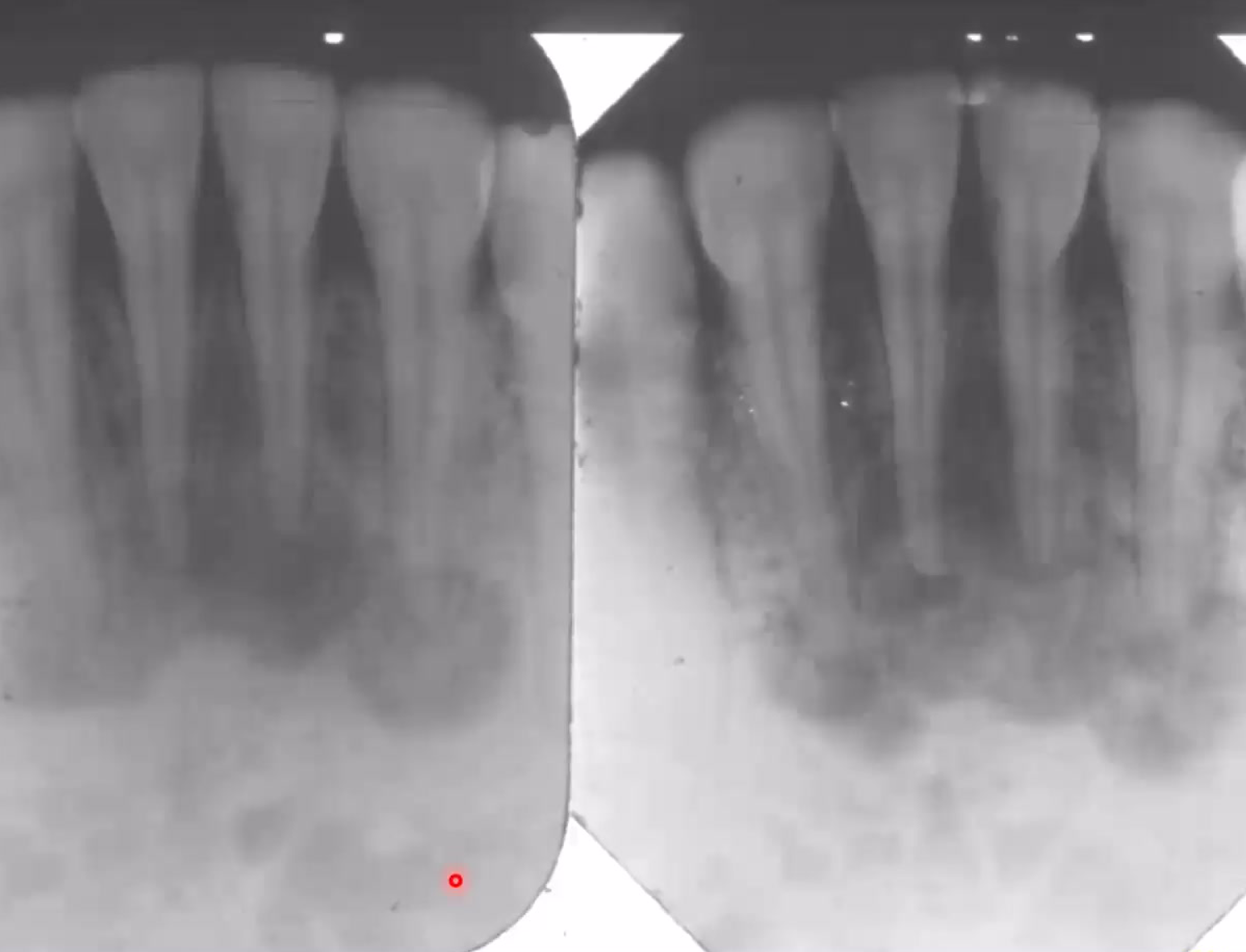
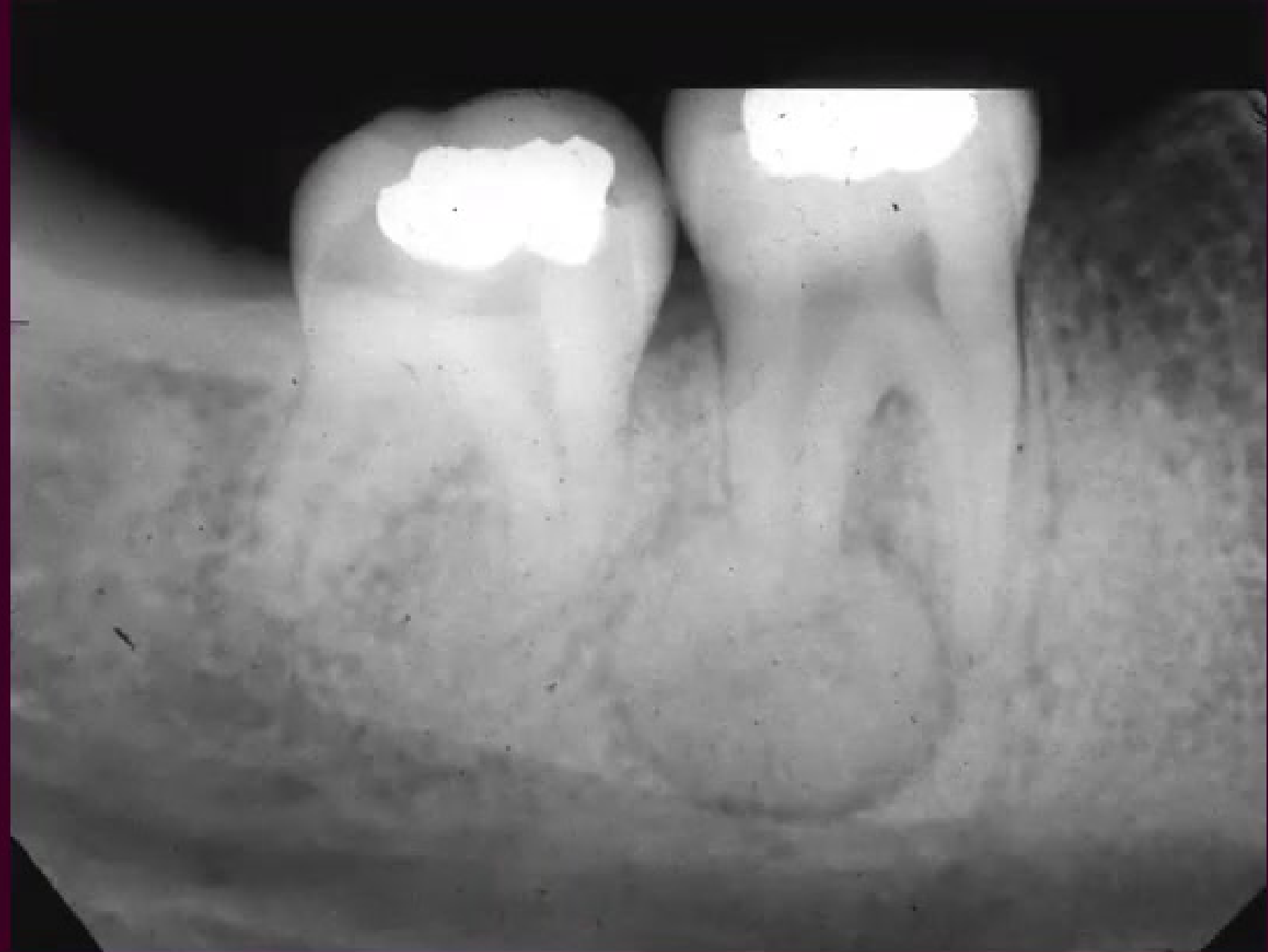
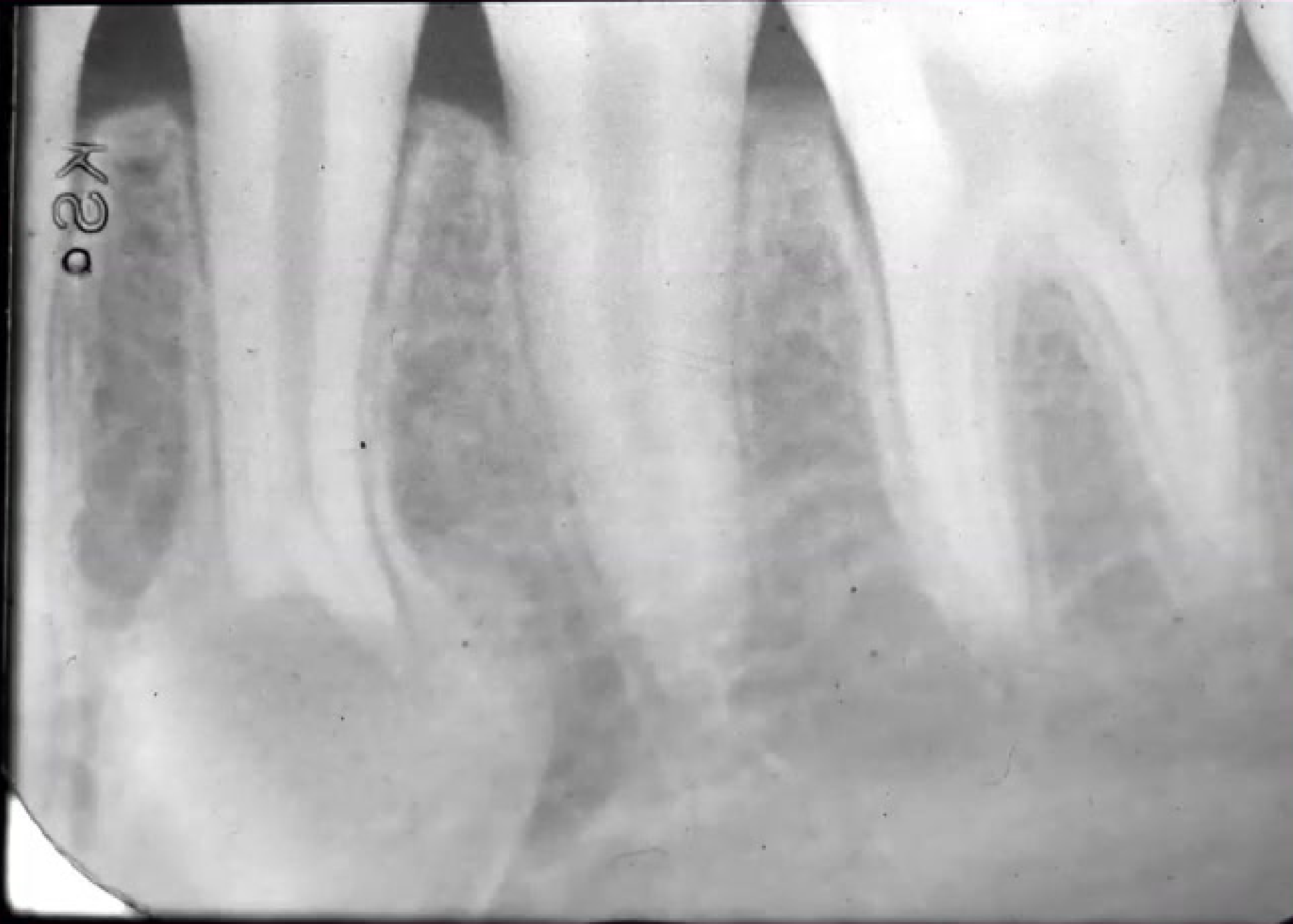
Radiographic Evidence29
Radiographic imaging of the mandibular anterior region demonstrates the characteristic periapical involvement associated with this condition.
- Starts as a radiolucency (mimicking periapical pathology) and matures into a radiopaque mass with a radiolucent rim.
 |  |
Management and Prognosis
Clinical Management30
- Diagnosis: Established through a combination of clinical and radiographic findings.
- Nature of Disease: Benign, self-limiting process with no progressive growth.
- Treatment Protocol: No treatment is required.
- Prognosis: Excellent.
Clinical Precautions
It is essential to avoid unnecessary dental interventions, including:
- Endodontic therapy
- Surgical intervention
- Extractions
Risk of Infection
Surgical intervention in these areas can trigger osteomyelitis.
Focal Cemento-Osseous Dysplasia
Demographic and Etiological Profile31
Clinical and Histological Features3233
- Etiology: Non-neoplastic; characterized by the disordered growth of cementum and bone.
- Incidence: Recognized as the most common benign fibro-osseous lesion.
- Age: Typically presents in the 4th to 5th decades of life.
- Gender: Predominantly affects females (approximately 80% of cases).
- Race: Most frequently observed in Caucasian populations.
 |  |
 |
Clinical Presentation and Radiographic Findings34
- Site: Most commonly located in the posterior mandible.
- Symptoms: Typically asymptomatic and discovered during routine examination.
- Presentation: Usually appears as a solitary lesion, often in edentulous areas.
- Size: Generally measures less than 1.5 cm.
- Radiographic Appearance:
- Mixed radiolucent-opaque presentation.
- Borders may be well-defined or irregular.
Focal Cemento-Osseous Dysplasia (FCOD) clinical and radiographic documentation.
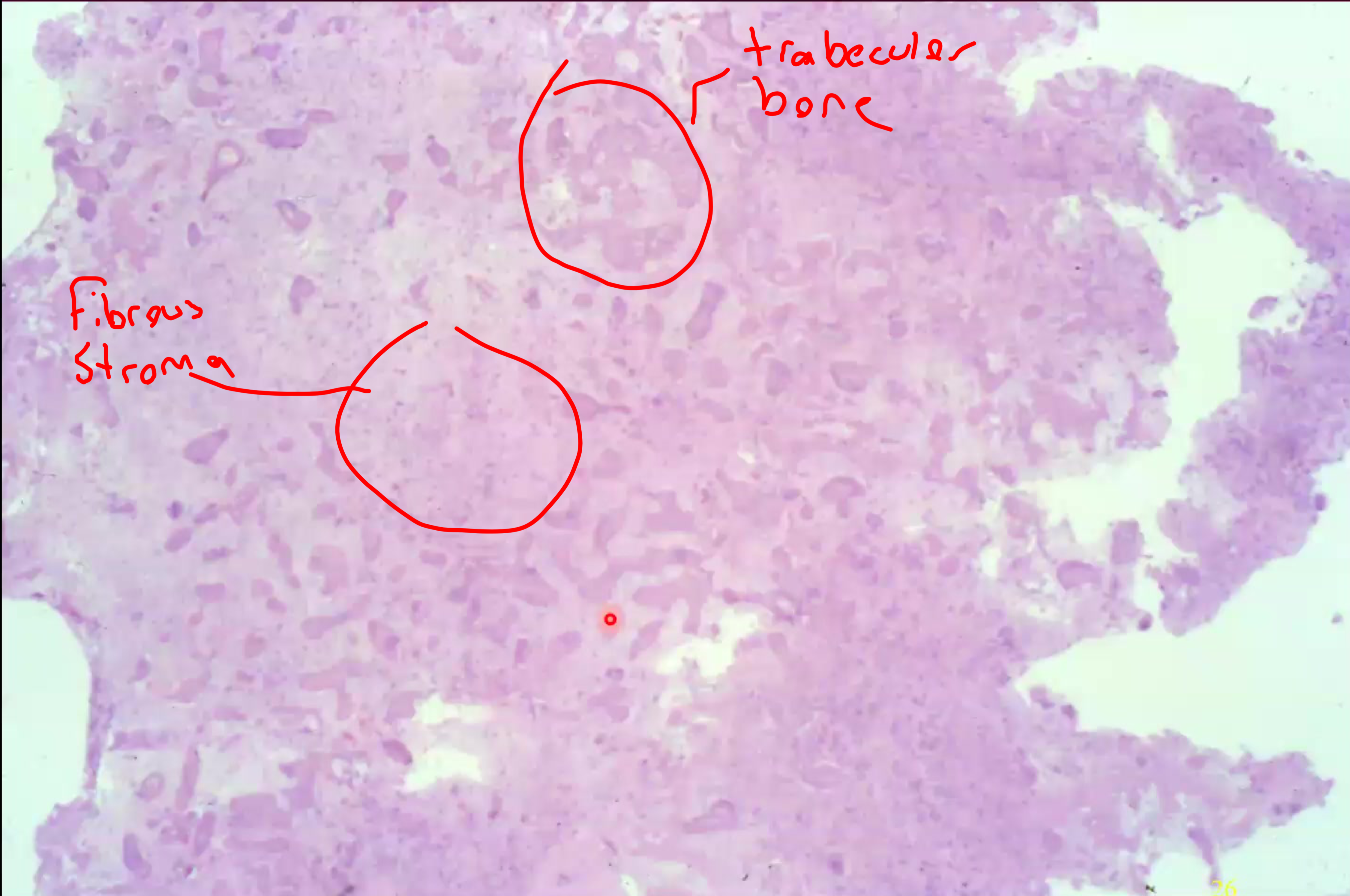
Histopathological Characteristics35
As a benign fibro-osseous lesion, the histology is characterized by:
- Cellular spindled fibroblasts.
- Dense collagen fibers.
- Globular cementum matrix material.
- Woven osseous matrix material.
- Presence of vascular channels.
Treatment and Prognosis
Management and Clinical Outlook36
- Intervention: Treatment typically involves curettage or biopsy for diagnostic confirmation.
- Prognosis: The outlook is excellent.
- Growth: The lesion exhibits limited growth potential.
- Follow-up: Periodic monitoring and follow-up are recommended.
Florid Cemento-Osseous Dysplasia37
Florid cemento-osseous dysplasia is a specific form of bone dysplasia that occurs within the tooth-bearing areas of the jaws.
Clinical and Radiographic Findings
Demographic and Clinical Characteristics38
Florid cemento-osseous dysplasia is a benign, non-neoplastic dysplastic process with the following clinical profile:
- Incidence: Relatively rare.
- Age: Primarily affects middle-aged adults.
- Gender: Significant female predilection (Female > Male).
- Race: Predominantly affects Black individuals (approximately 90% of cases).
- Site: Characterized by diffuse involvement of the jaws.
- Diffuse involvement often spans two or more quadrants.
Symptomatology
While often discovered incidentally, clinical presentations may include:
- Asymptomatic nature in many patients.
- Potential for jaw expansion.
- Risk of secondary infection.
Imaging Characteristics39
The radiographic appearance of this condition is distinct and typically involves:
- Irregular lobular dense radiopacities.
- Radiopacities often present with a distinct "cloud-like" appearance.
- Mixed radiolucent and radiopaque areas (maturing stages).
- Diffuse involvement of both the maxilla and mandible.
- Bilateral and symmetrical distribution.
Radiographic Presentation40
Clinical imaging (such as dental X-rays) demonstrates the characteristic dense, lobulated radiopaque masses within the alveolar bone, often localized or diffuse along the mandibular or maxillary arches.
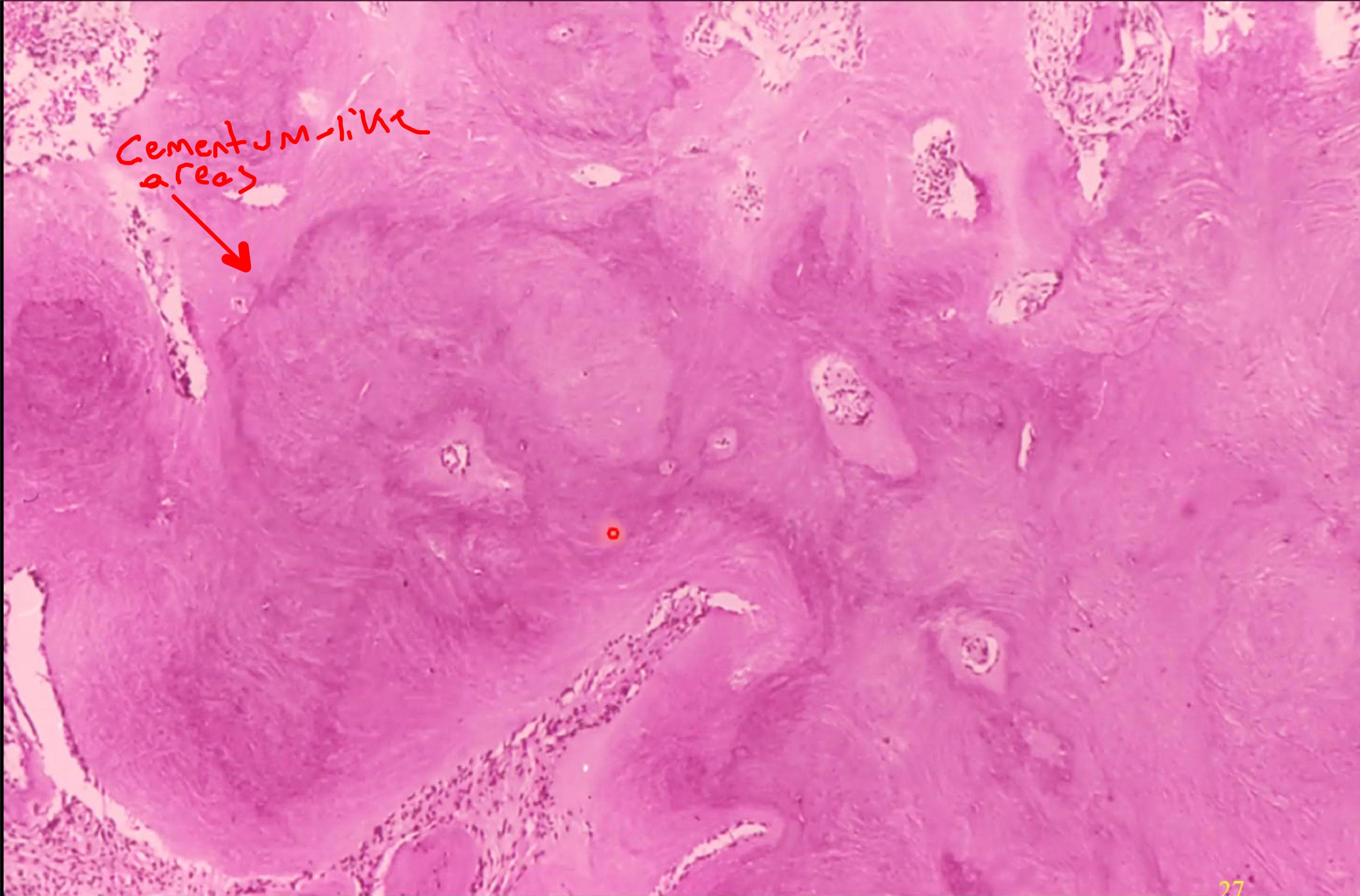
Histopathological Features41
Microscopic examination typically reveals a mixture of fibrous connective tissue, woven bone, and cementum-like calcifications. The tissue shows varying degrees of mineralization depending on the stage of the lesion.
Late-Stage Histopathology
In the late stages of the disease, microscopic examination reveals large, dense masses of cementum and osseous material with minimal stroma.
Management and Complications42
Clinical Management Guidelines43
As a benign and often self-limiting process, the management strategy focuses on observation and prevention:
- No active treatment is required for asymptomatic cases.
- Emphasis is placed on the maintenance of dentition to avoid the need for extractions.
- Rigorous oral hygiene is the primary management focus to prevent tooth loss and subsequent bone exposure.
- Avoid surgical exposure of the calcific masses, as these areas have poor vascularity and are prone to infection.
Potential Complications
Despite its benign nature, significant complications can arise, particularly if the bone is compromised:
- Chronic Osteomyelitis: May present with pain, fistulae, dehiscence, and sequestration.
- The dense, hypocellular bone is highly susceptible to infection and sequestration if exposed to the oral cavity, which can occur through extractions or even simple denture sores.
- Traumatic Bone Cysts: These secondary lesions may occasionally develop within the dysplastic bone.
Benign Cementoblastoma4445
Benign cementoblastoma is a rare odontogenic neoplasm characterized by the formation of cementum-like tissue.
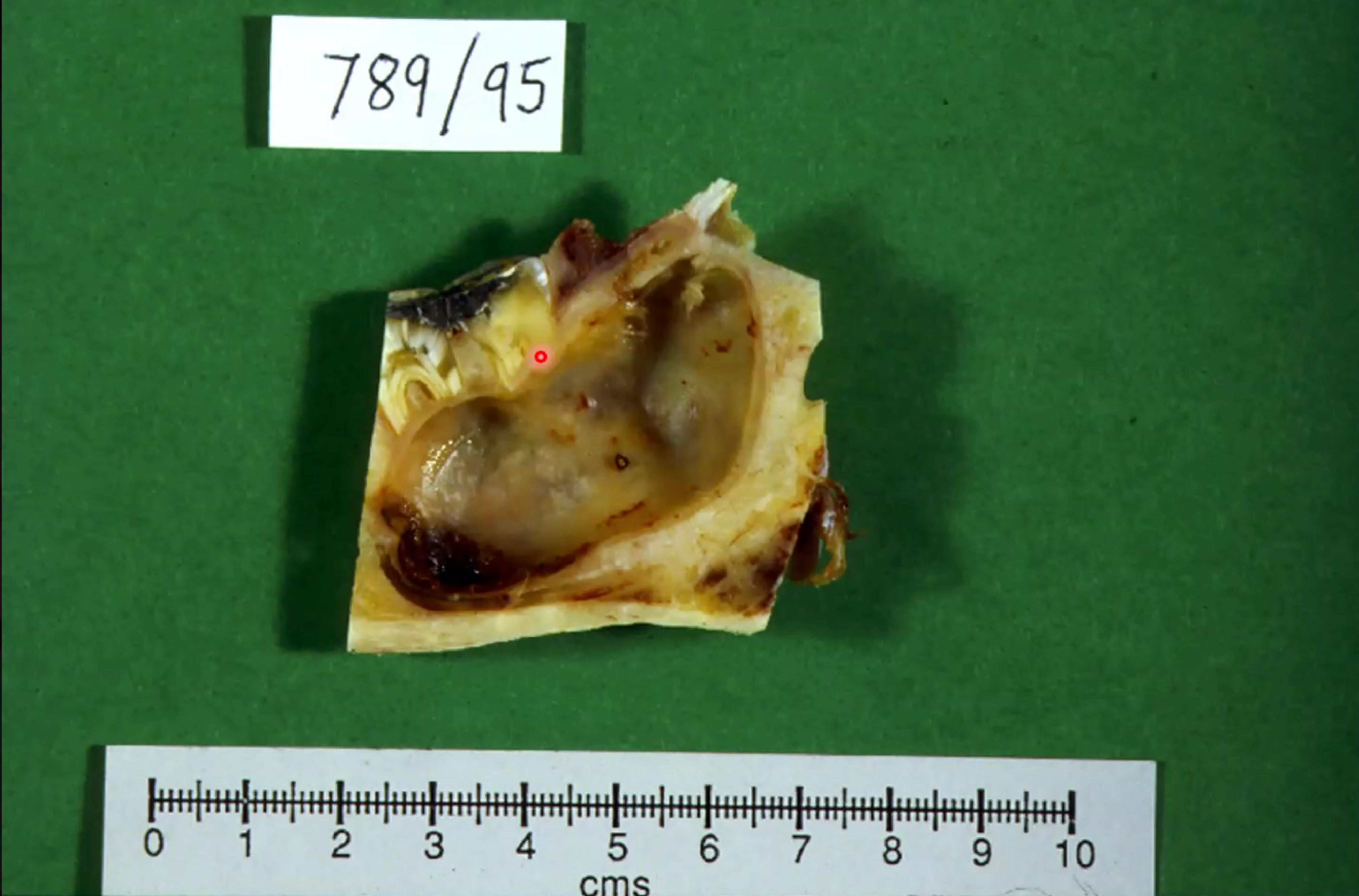
Definition and Nature46
Cementoblastoma is a benign ectomesenchymal odontogenic neoplasm that forms a mass of cementum or cementum-like tissue continuous with the tooth root. It is considered analogous to osteoblastoma and can be destructive to surrounding tissue.
 |  |  |
 |  |  |
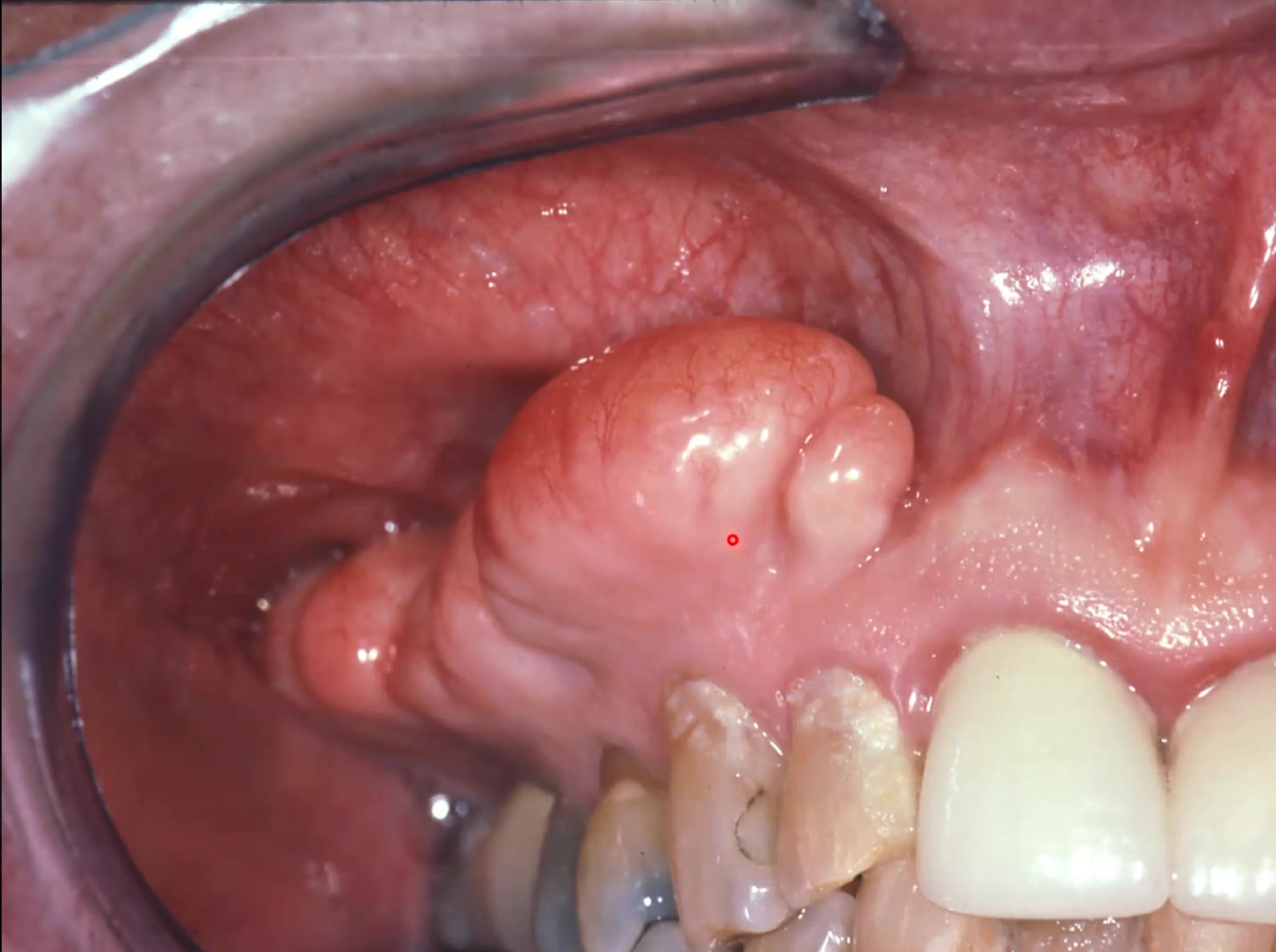
Clinical Presentation
- Typically presents as a tender, sometimes painful swelling at the buccal and lingual/palatal aspect of the alveolus.
- Generally affects individuals under the age of 30.
- Higher prevalence in males (1.2:1).
- Usually involves a mandibular premolar or first molar.
- Typically associated with the permanent first molar.
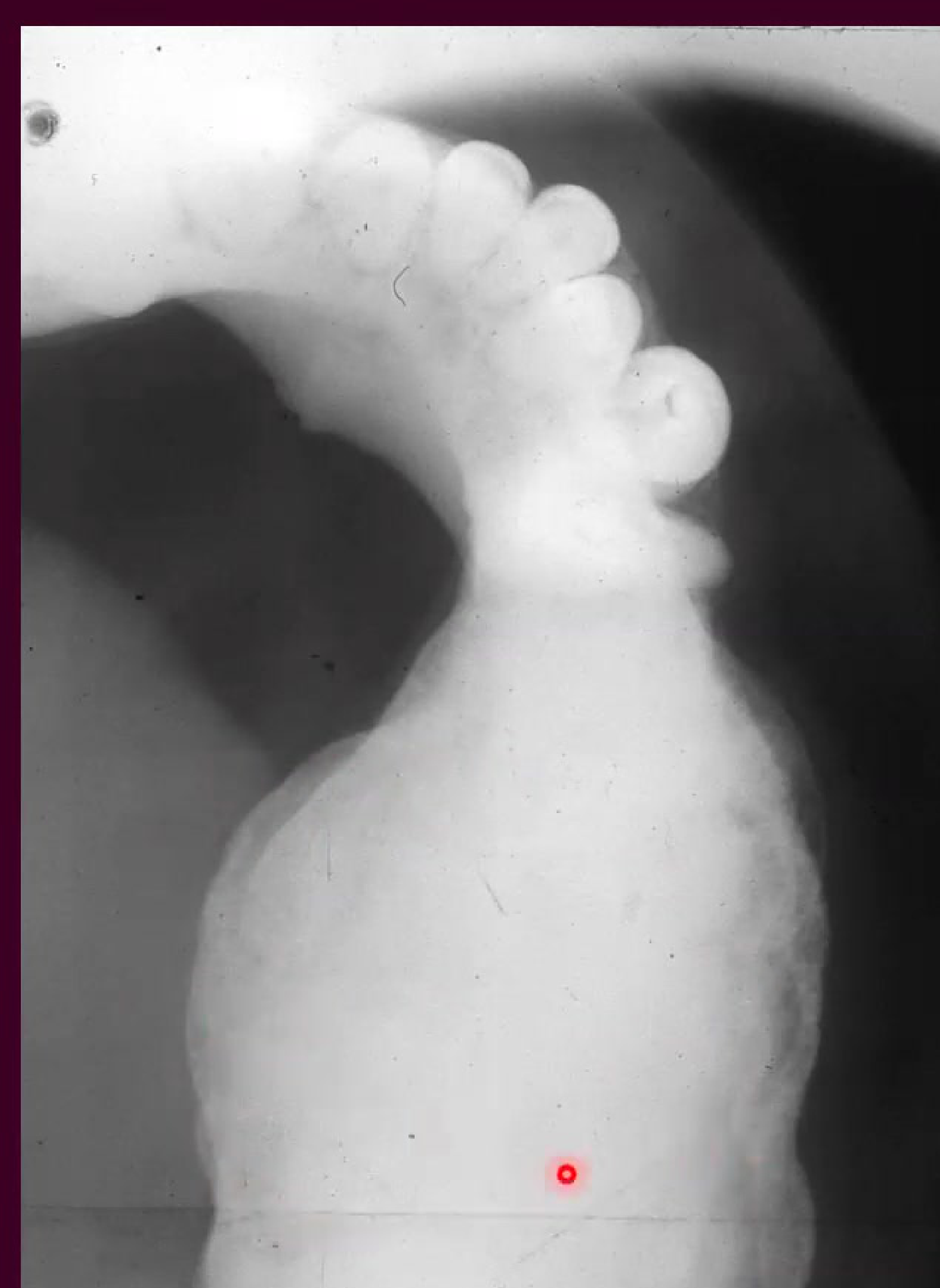
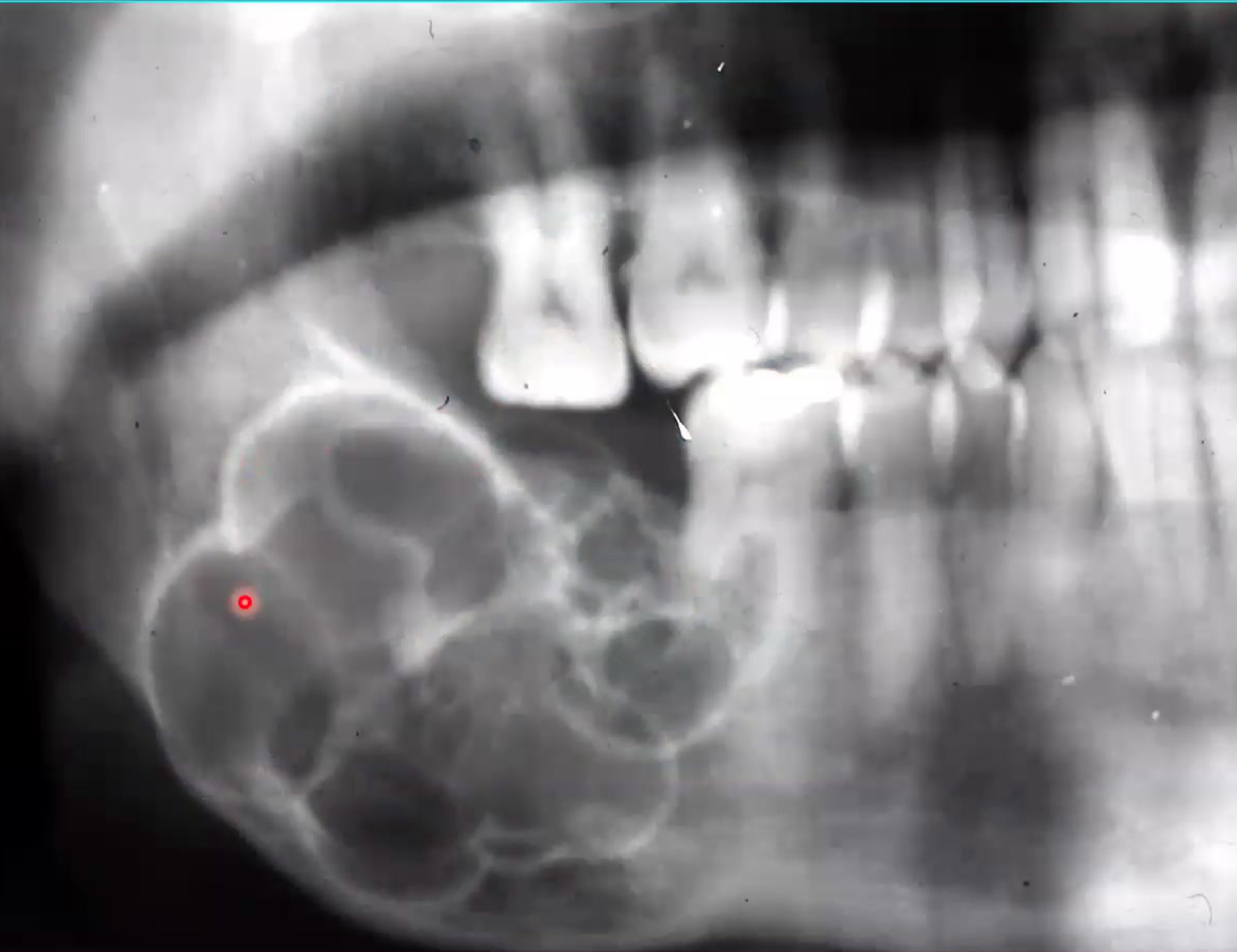
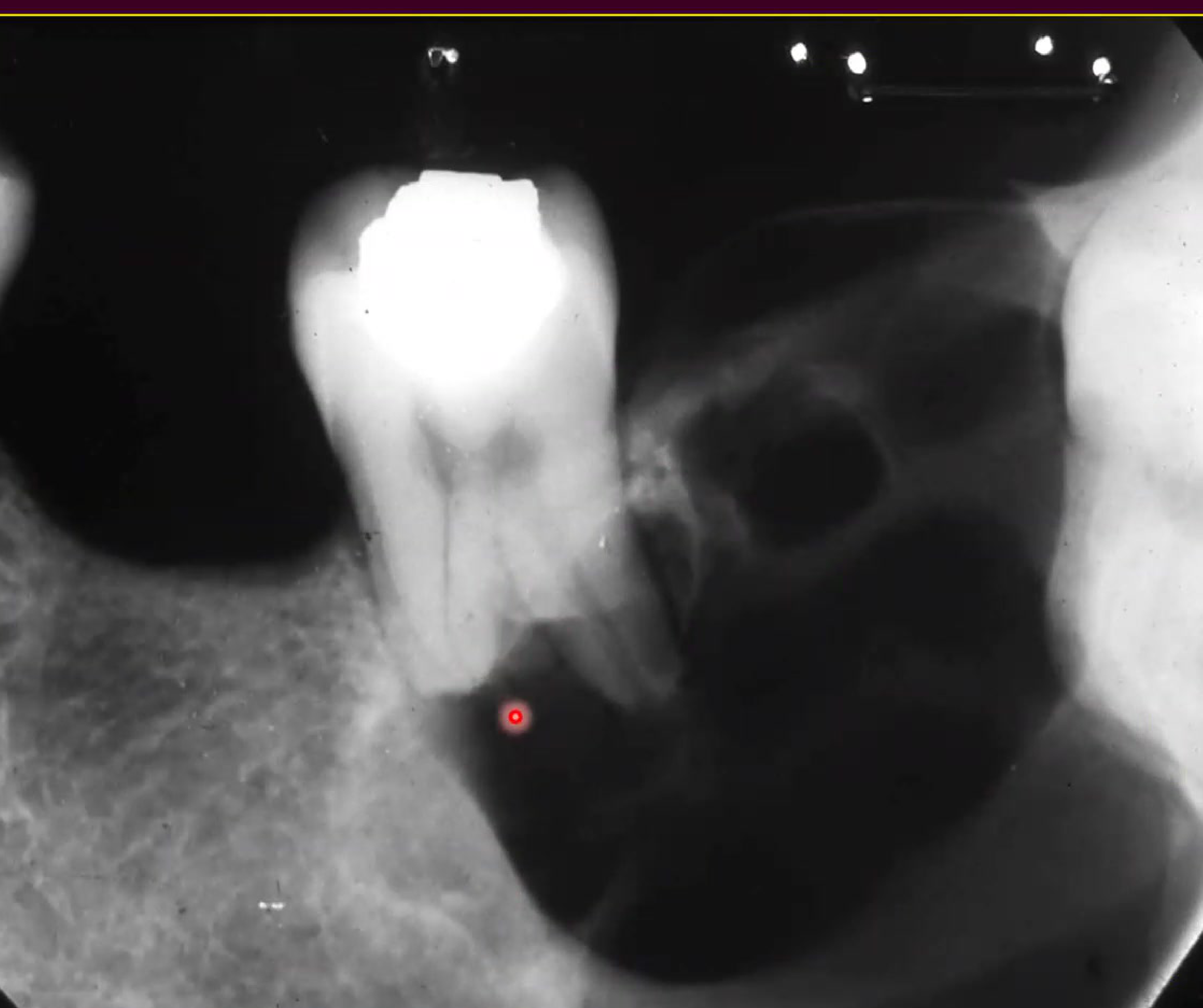
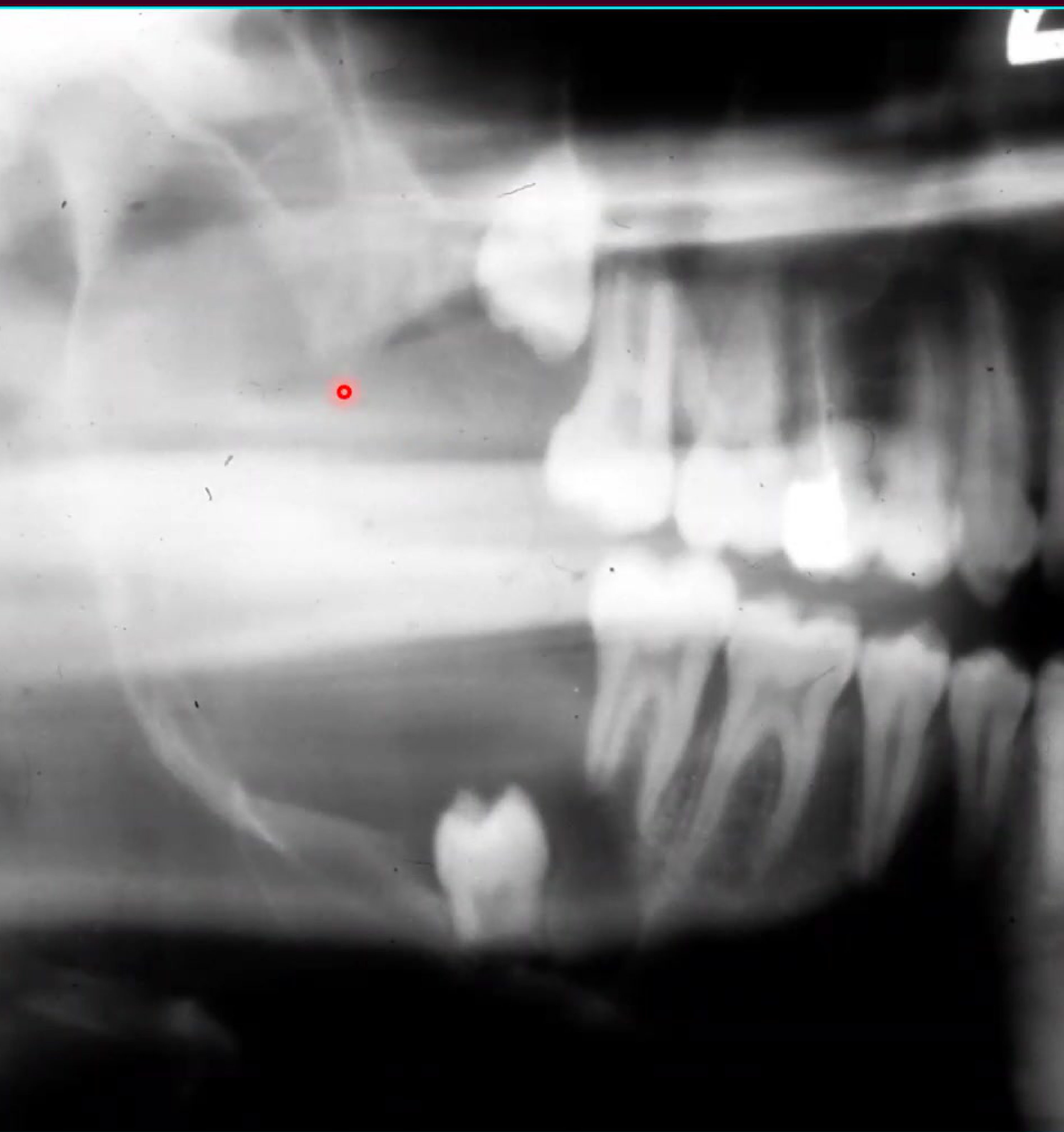
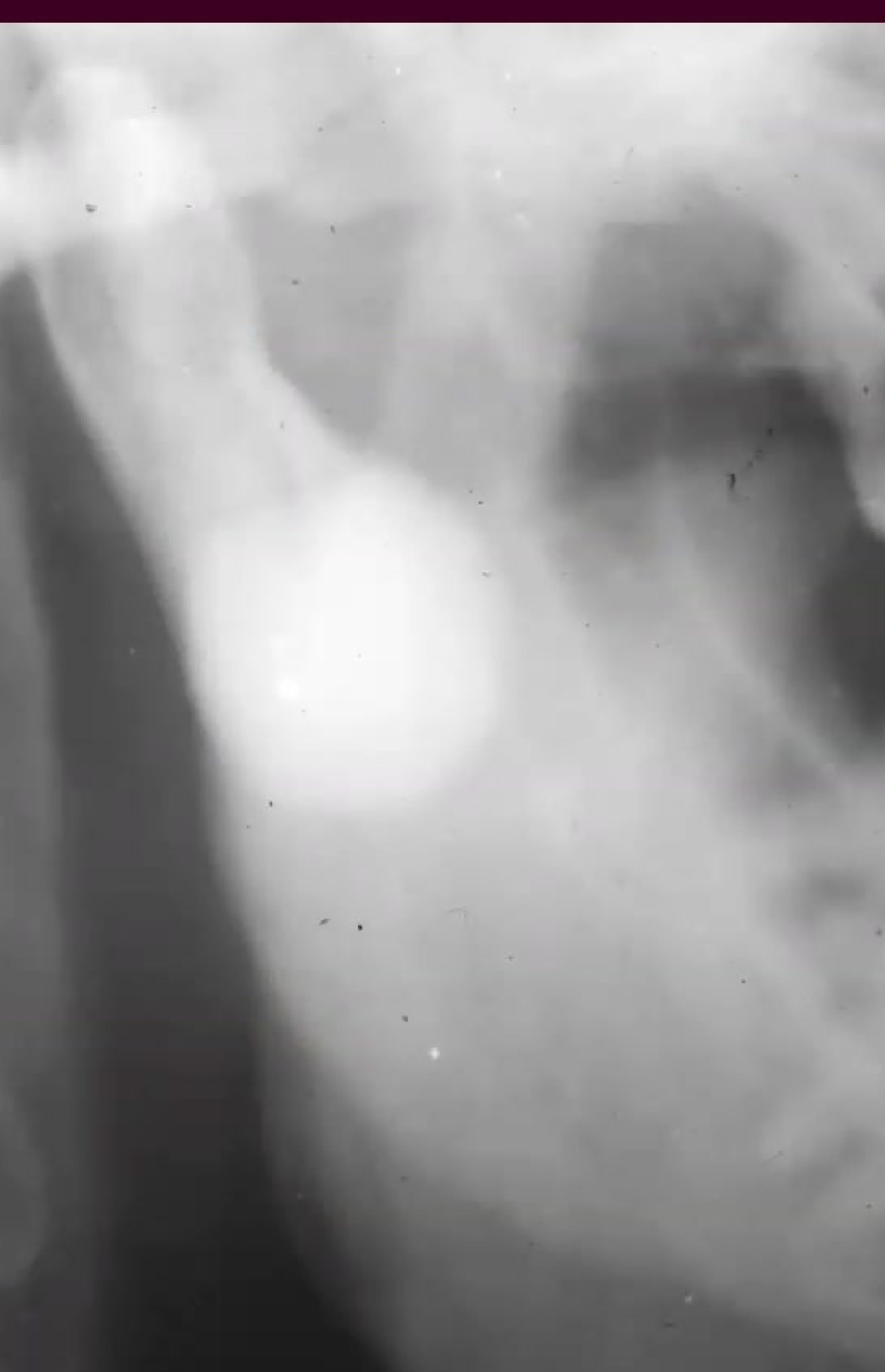
Radiographic Appearance
- Appears as a radiopaque mass with a thin radiolucent rim attached to the roots of a tooth.
- The mass may be rounded or irregular in shape and mottled in texture.
- Common features include tooth resorption, loss of root outline, and obliteration of the periodontal ligament space.
Management and Prognosis
Previously thought to be an innocuous entity due to limited follow-up data, it is usually managed by conservative surgical enucleation. However, cases of rapid growth and recurrence have been documented.
Clinical and Radiological Features47
 |  |
 |
Clinical Presentation48
- Tender, sometimes painful swelling.
- Located at the buccal and lingual/palatal aspect of the alveolus.
- Predominantly affects patients under age 30 years.
- Male prevalence (1.2:1).
- Most common site: Mandible (80%), specifically the 1st molar.
- May cause localized pain and cortical expansion.
Radiographic Features49
- Radiopaque mass with a thin radiolucent rim attached to the roots of a tooth.
- The mass is fused to the root and surrounded by a thin, well-defined radiolucent rim (capsule).
- Associated with tooth resorption, loss of root outline, and obliteration of the periodontal ligament space.
Radiological imaging of cementoblastoma demonstrates the characteristic attachment to the tooth root and the surrounding radiolucent rim.
Histological Features and Treatment5051
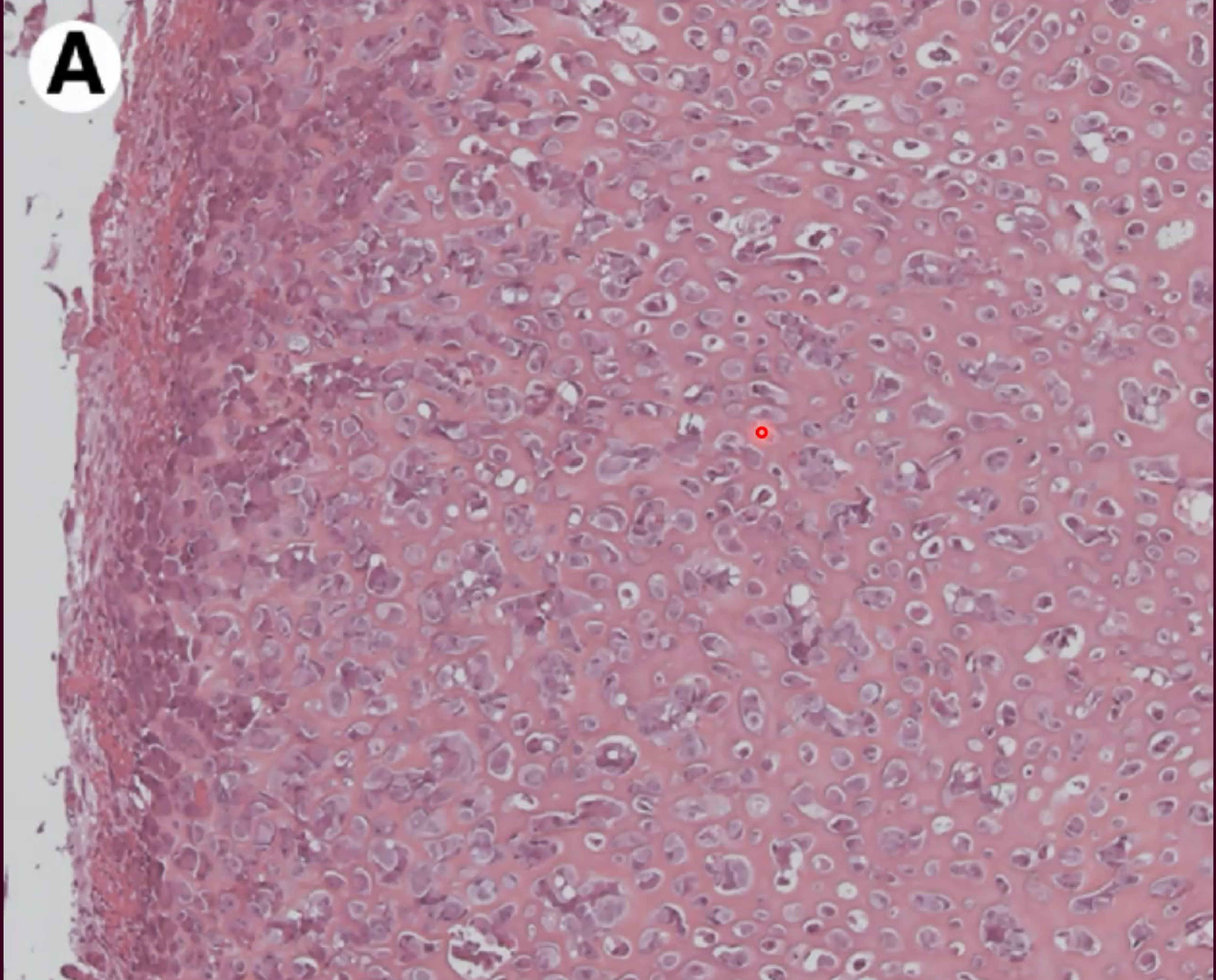 |  |
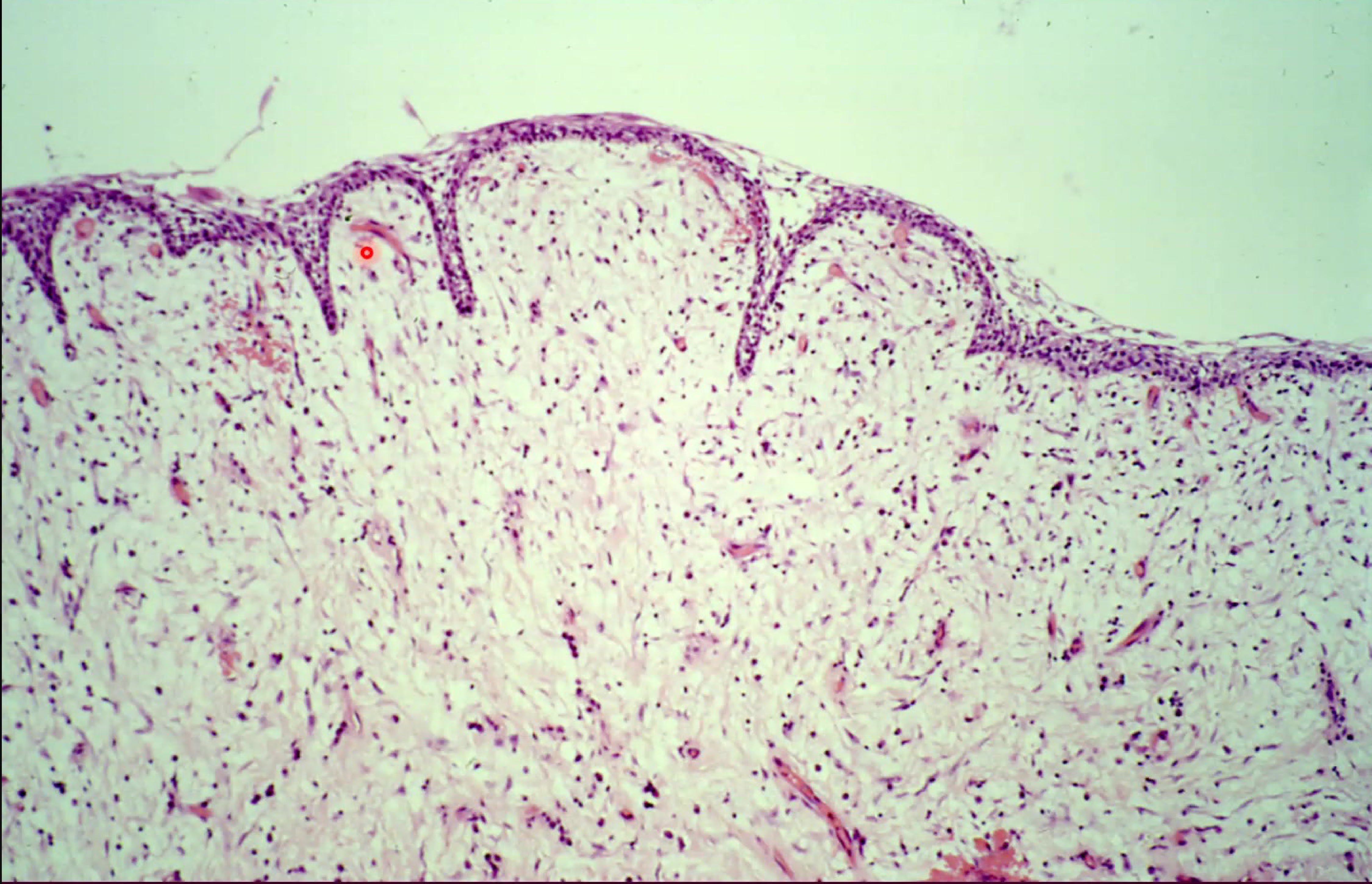
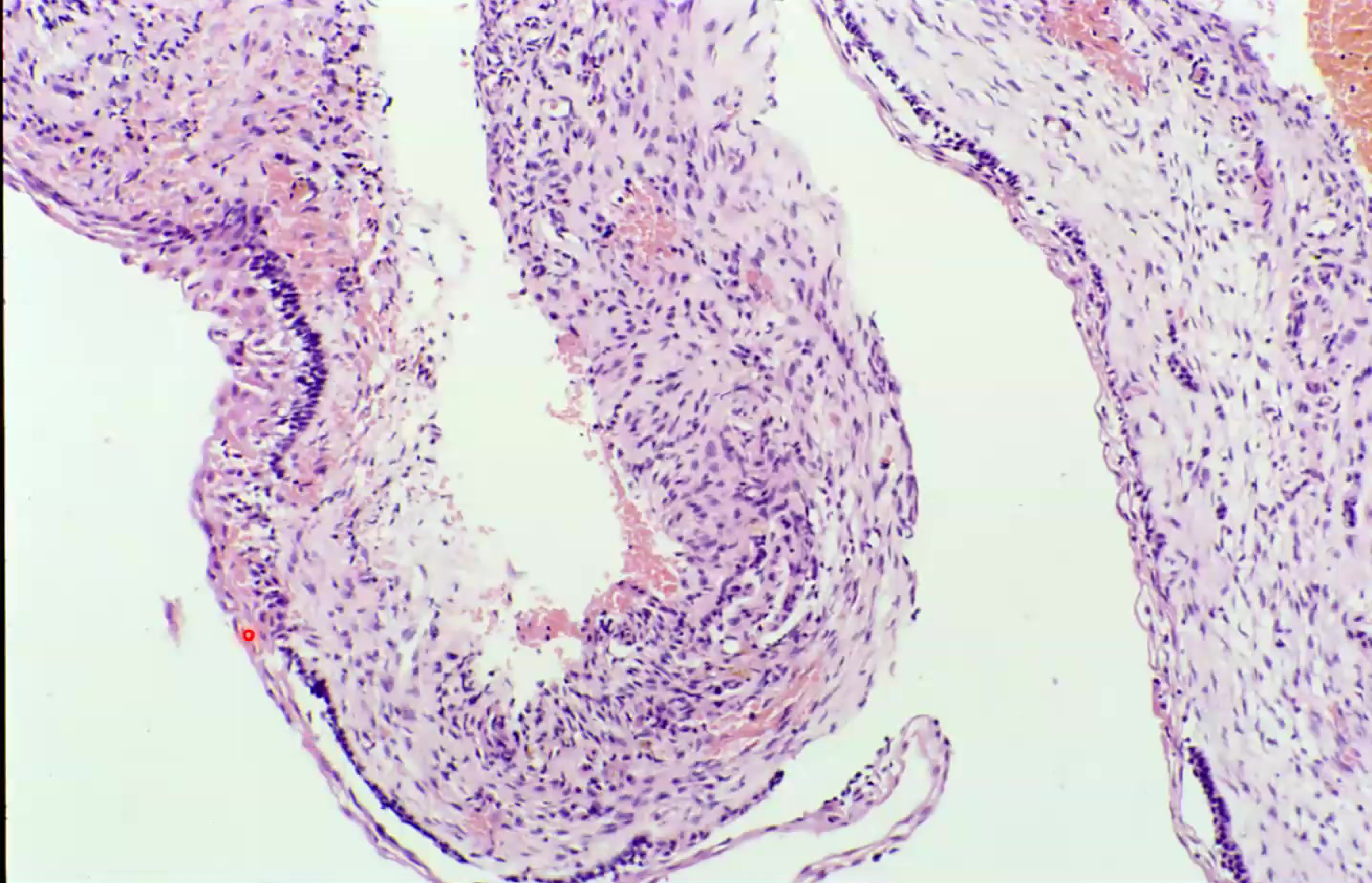
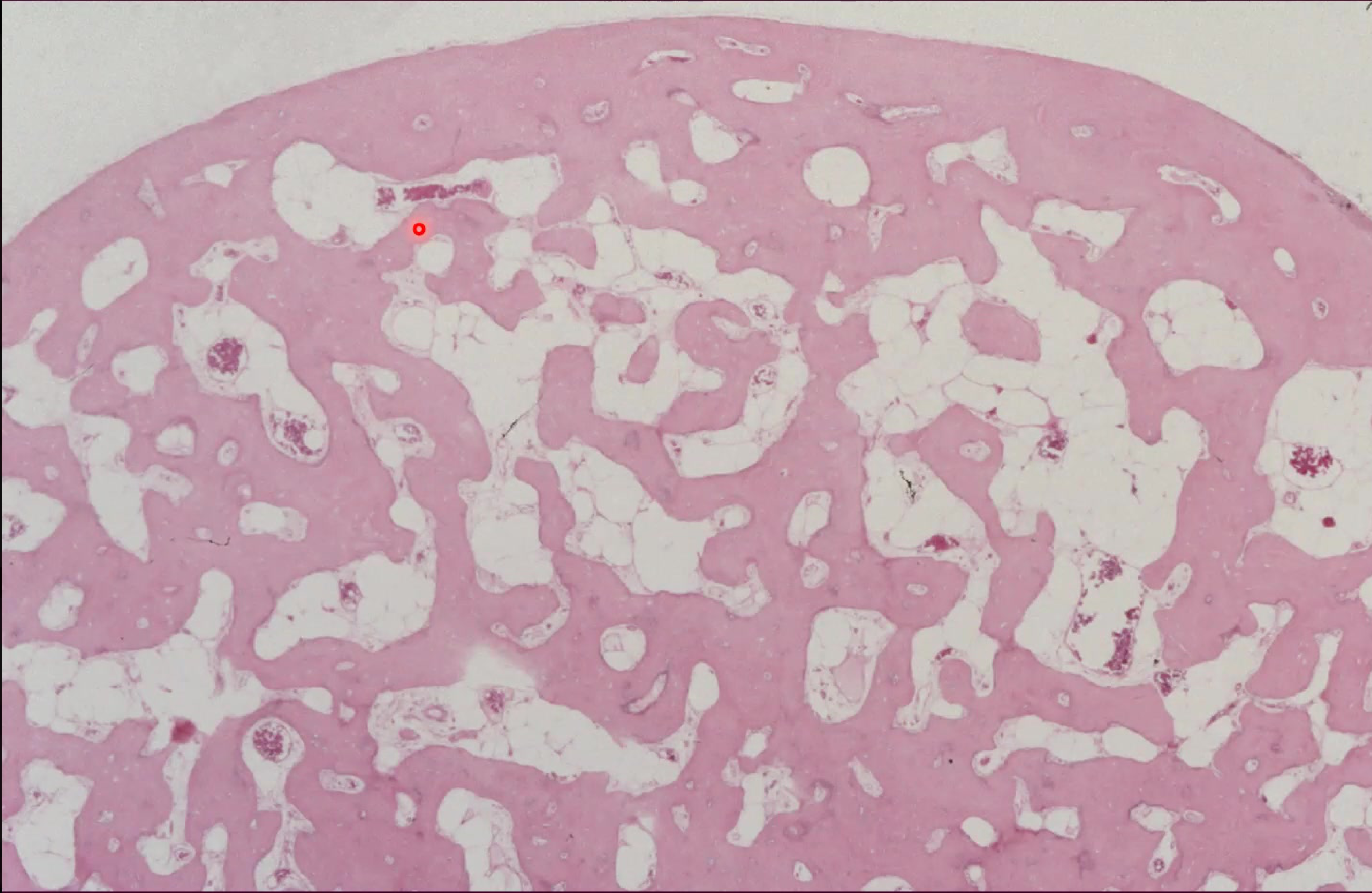
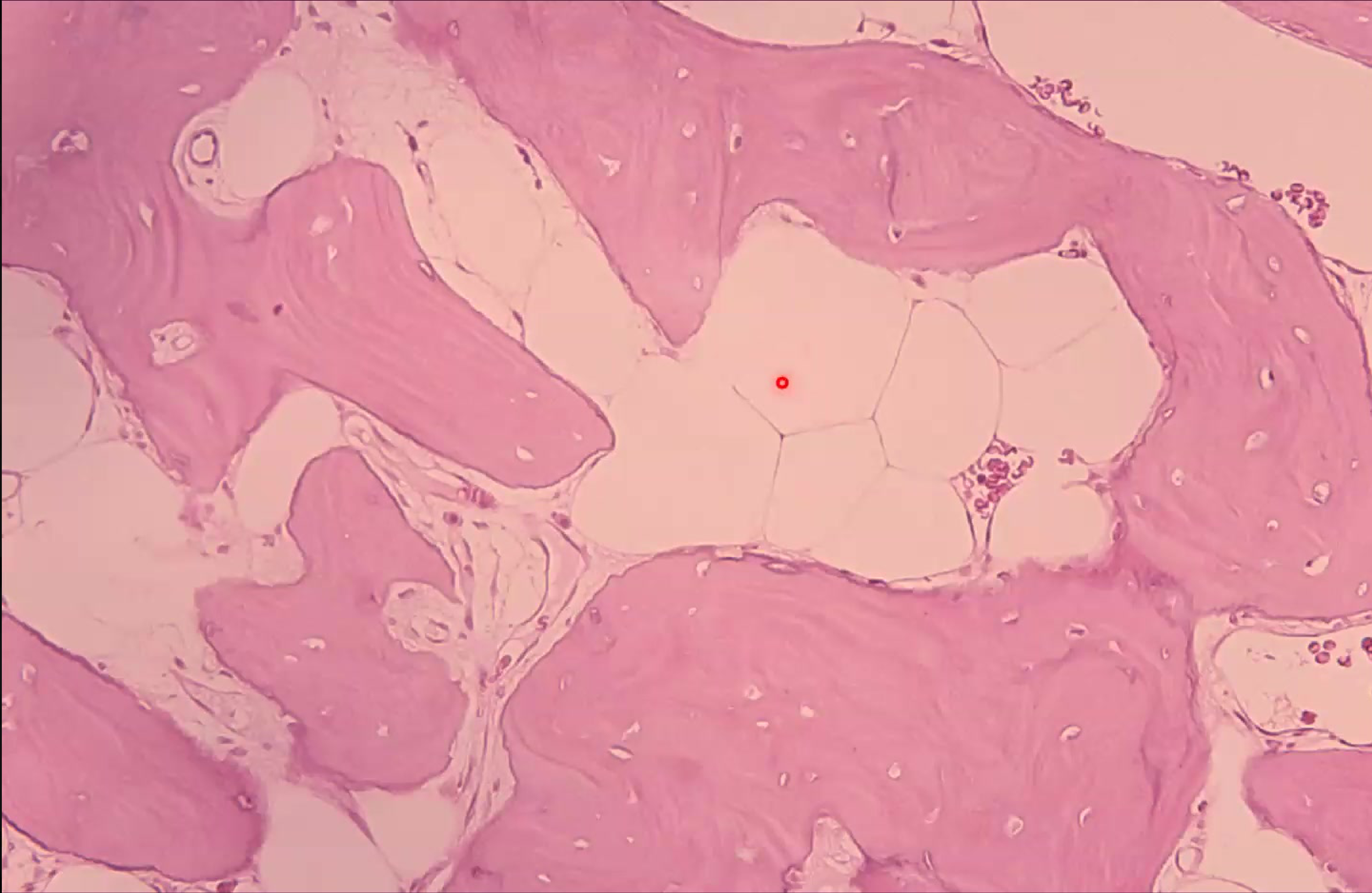
Histological Characteristics
- Composed predominantly of sheets or trabeculae of cementum-like calcified tissue.
- Features variably prominent reversal lines, sometimes exhibiting a pagetoid appearance.
- Cementoblasts and cementoclasts are found enclosed within the hard tissue or around the periphery of the trabeculae.
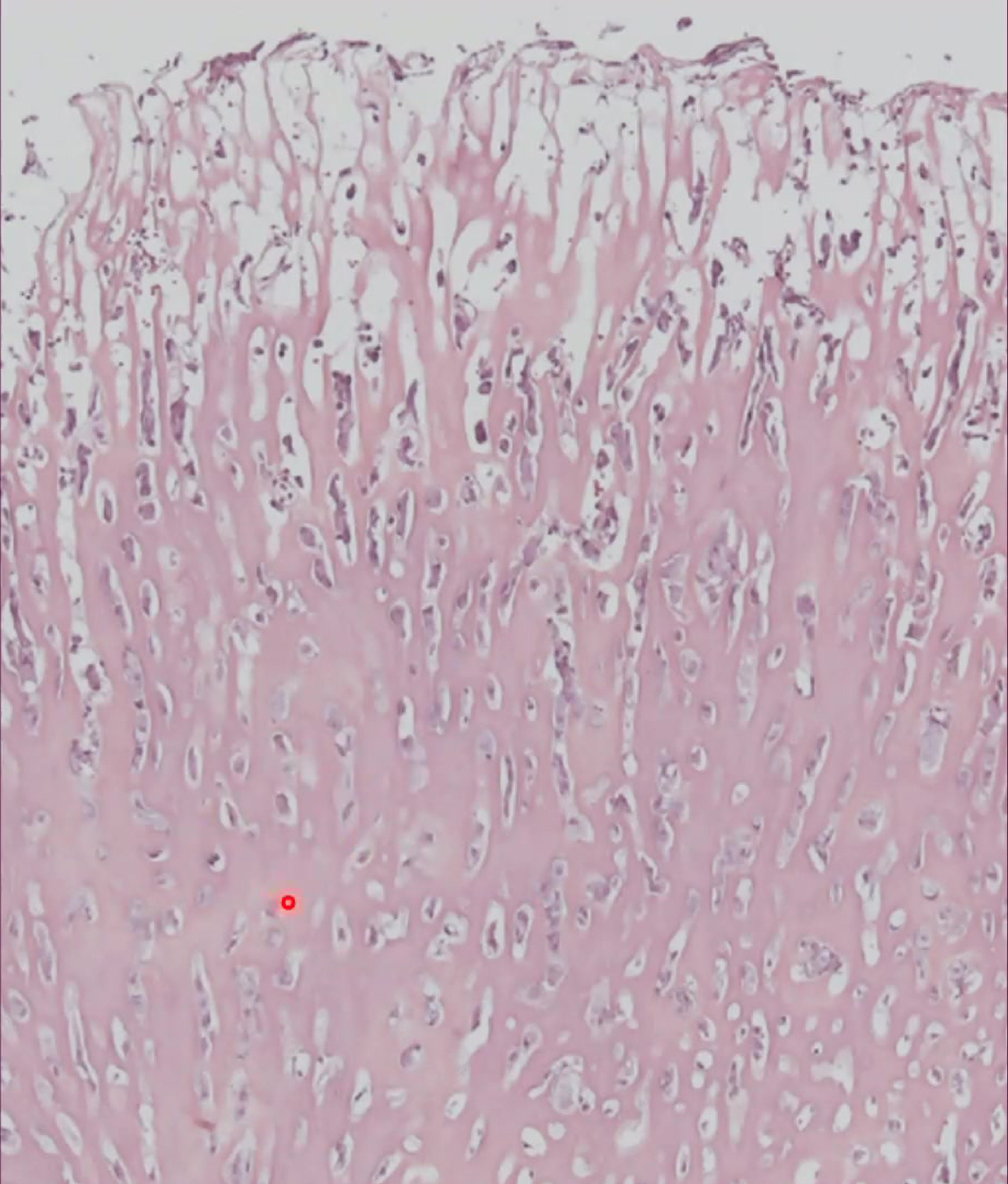
Microscopic Findings52
- Presence of sheets or trabeculae of cementum-like calcified tissue.
- Prominent reversal lines are variably present, occasionally showing a pagetoid appearance.
Histological Comparison
Resembles osteoblastoma histologically and features prominent reversal lines with a pagetoid appearance.
Treatment and Prognosis
- Primary treatment: Surgery.
- Treatment specifically involves surgical extraction of the tooth along with the attached tumor.
- Recurrence rate: 35-60%.
Classification of Odontogenic Tumors
The classification of benign odontogenic tumors is categorized into three primary groups based on the tissue of origin and the presence of dental hard tissue formation:
Historical Context
The classification is based on the 1990 WHO/Kramer classification, which relates these tumors to specific stages of tooth development.
Benign Odontogenic Tumors5354
- Odontogenic epithelium without odontogenic ectomesenchyme
- Odontogenic epithelium with odontogenic ectomesenchyme, with or without dental hard tissue formation
- Odontogenic ectomesenchyme with or without included odontogenic epithelium
 |  |
Histological Components5556
- Layers of the enamel organ
 |  |
Epithelial Tumors without Ectomesenchyme57
This category includes tumors derived solely from odontogenic epithelium:
- Ameloblastoma
- Squamous odontogenic tumour
- Calcifying epithelial odontogenic tumour (Pindborg Tumour)
Mixed Epithelial and Ectomesenchymal Tumors58
These tumors involve both odontogenic epithelium and ectomesenchyme, and may or may not exhibit dental hard tissue formation:
- Ameloblastic fibroma
- Ameloblastic fibro-dentinoma
- Ameloblastic fibro-odontome
- Adenomatoid odontogenic tumour
- Calcifying odontogenic cyst
- Complex odontome
- Compound odontome
Ectomesenchymal Tumors59
These tumors are primarily composed of odontogenic ectomesenchyme, which may or may not contain included odontogenic epithelium:
- Odontogenic fibroma
- Myxoma (myxofibroma)
- Benign cementoblastoma (‘true’ cementoma)
Malignant Odontogenic Tumors60
Malignant odontogenic tumors are classified as follows:
- Malignant odontogenic tumors are considered extremely rare in clinical practice.
- Clear cell odontogenic carcinoma
- Malignant ameloblastoma
- Primary intra-osseous carcinoma
- Malignant variants of other odontogenic epithelial tumours
- Malignant changes in odontogenic cysts
Ameloblastoma6162
Ameloblastoma is a benign but locally aggressive odontogenic tumor. It is the most common clinically significant odontogenic tumor, characterized by its slow growth and potential for extensive bone destruction.

Clinical Presentation63646566676869
Clinical examination may reveal oral lesions. In some cases, these present as swelling or abnormalities within the oral cavity, including the tongue or alveolar ridges, which require careful diagnostic evaluation.
- Most common in the posterior mandible; often seen in the 4th decade of life.
- Can cause significant "bucco-lingual" expansion.
 |  example of multi-cystic lesion example of multi-cystic lesion |  |
 |  |  |
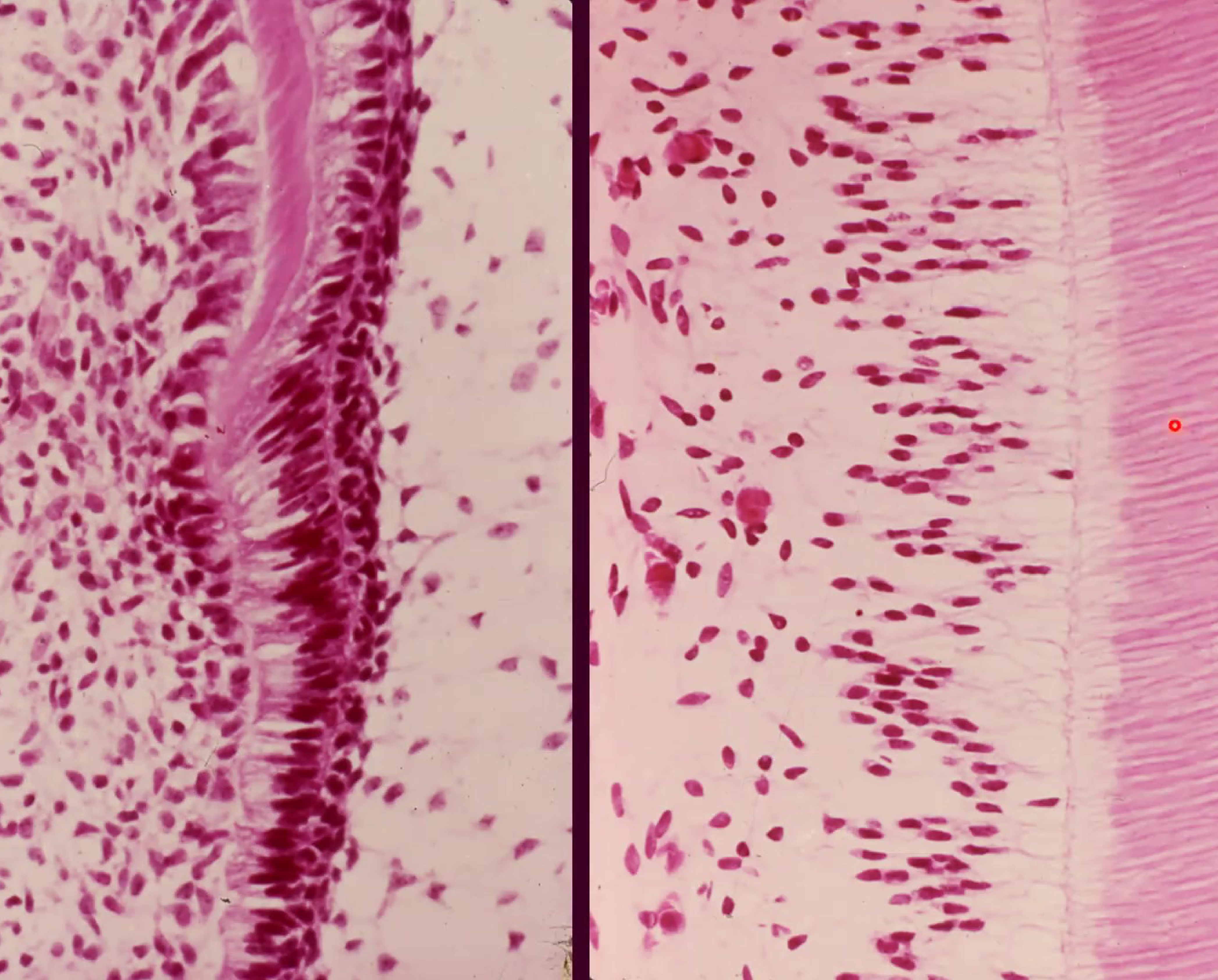
 islands of epithelial cells , reverse polarization of columantar cells islands of epithelial cells , reverse polarization of columantar cells | ||
| - |
Radiographic Features7071
Dental imaging and X-rays are essential for identifying the extent of the tumor. Radiographically, these lesions often appear as well-defined radiolucencies, which may be unilocular or multilocular (soap-bubble or honeycombed appearance), frequently associated with the jawbone and surrounding teeth.
- Often associated with root resorption of adjacent teeth.
 |  |
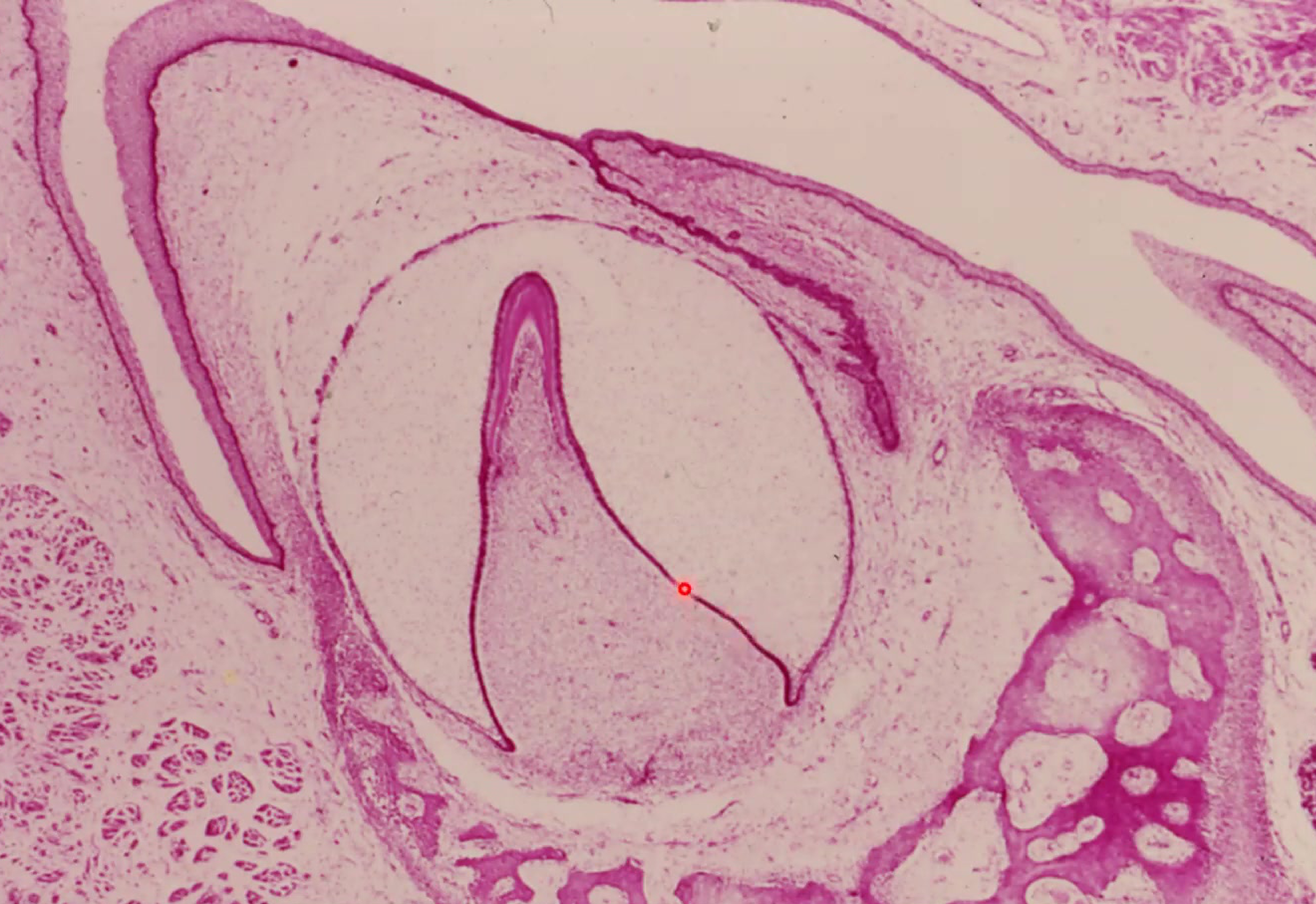
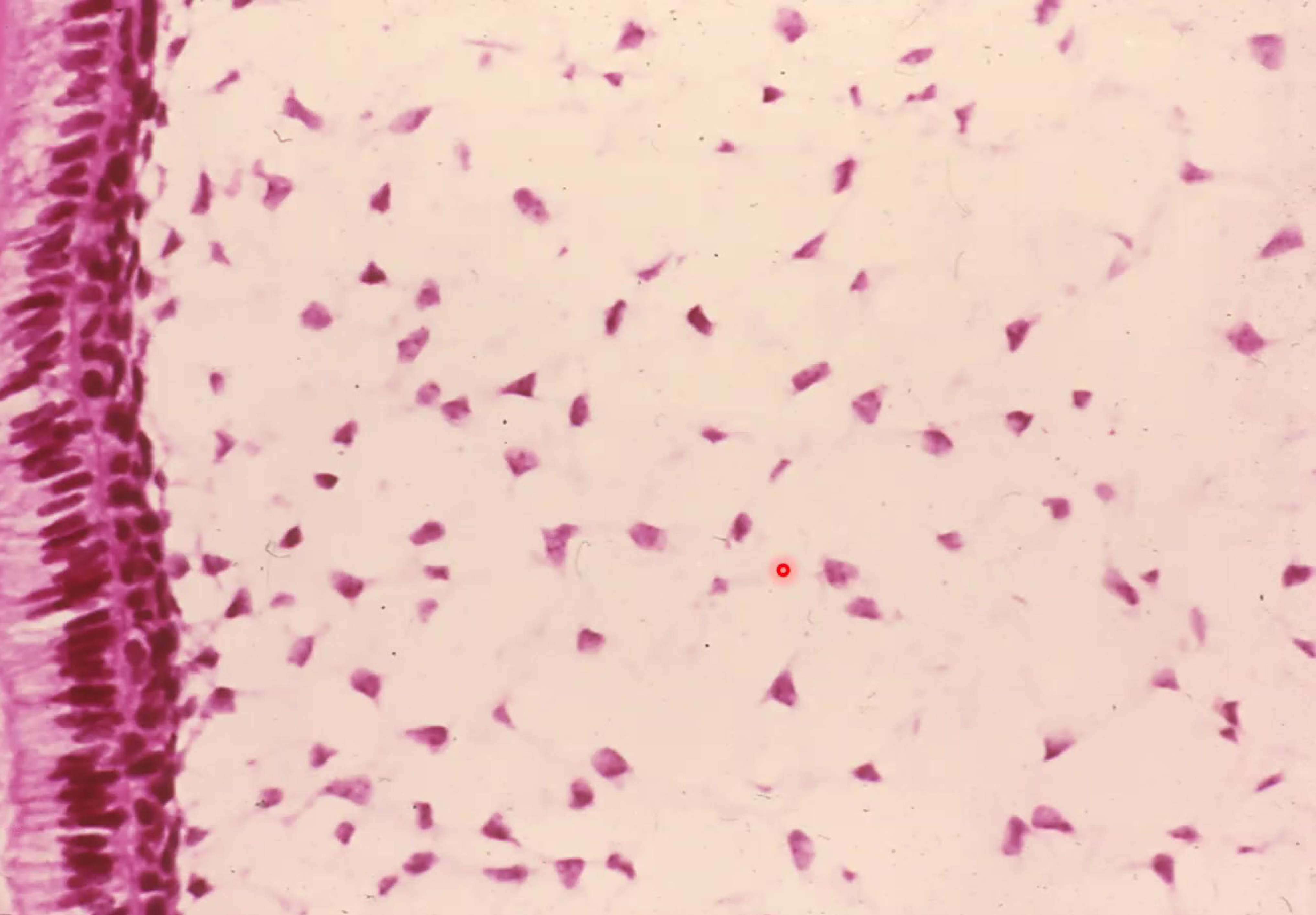
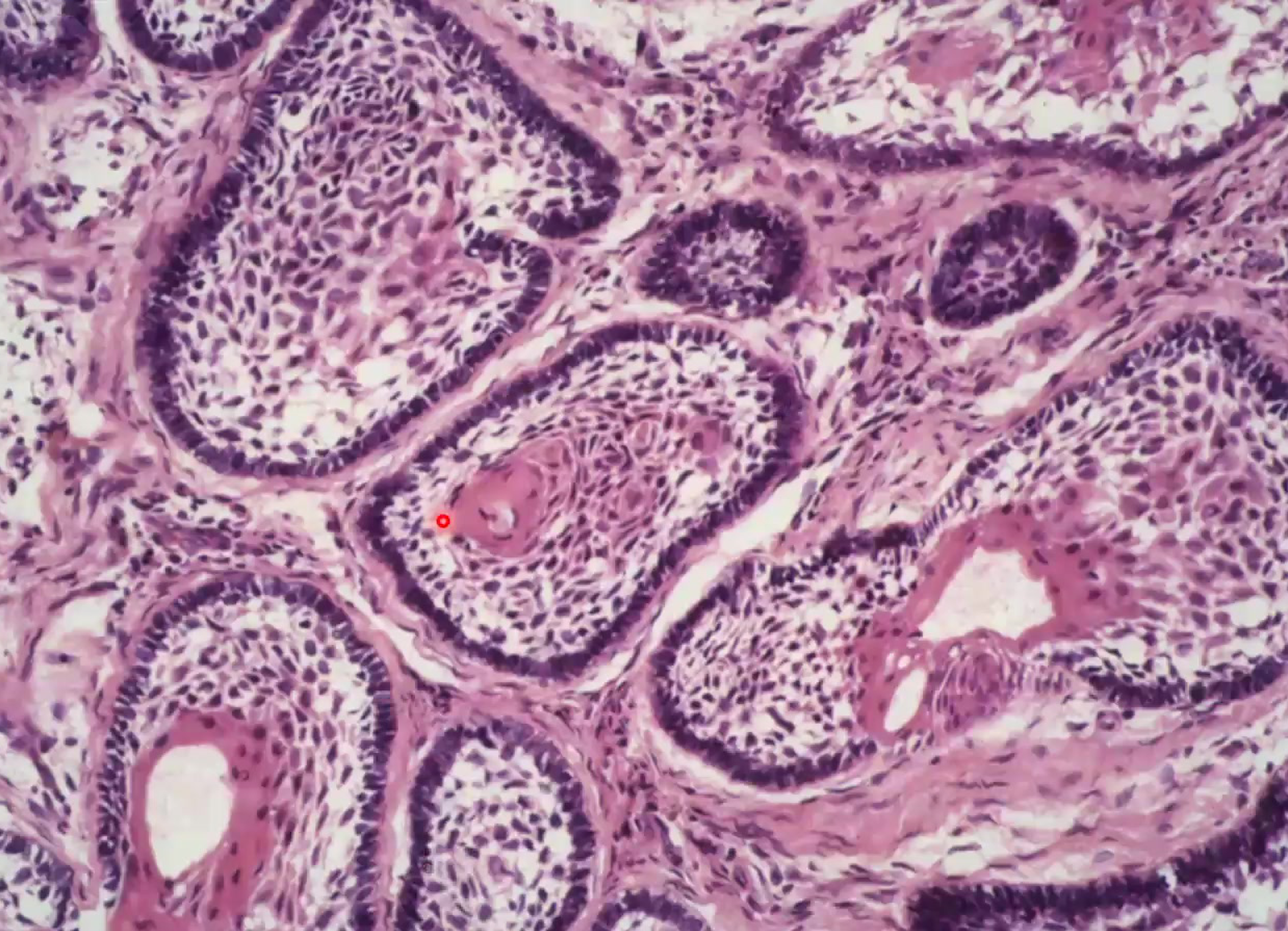
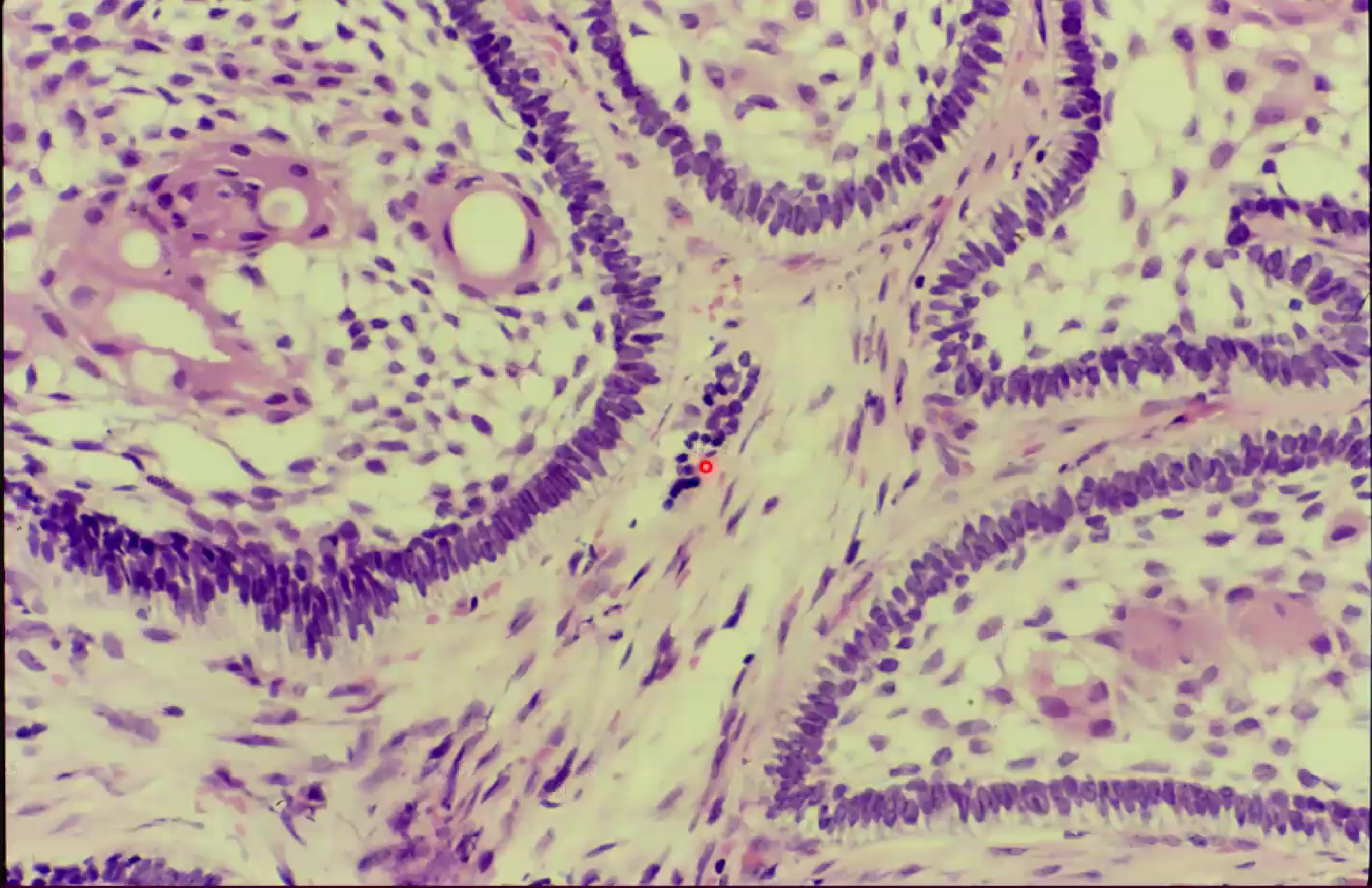
Histopathological Characteristics7273
Microscopic analysis of a unicystic ameloblastoma typically reveals:
- Cystic Lesion Structure: A central cystic cavity.
- Epithelial Lining: The lesion is lined by odontogenic epithelium.
- Stroma Composition: The supporting stroma is composed of spindle cells and may contain inflammatory cells.
- Cellular Features: Islands of epithelium with columnar cells showing reverse polarity (nuclei away from the basement membrane), resembling ameloblasts.
- Internal Structure: Central areas of the islands resemble stellate reticulum.
 |  |
Osteoma7475767778
 |  |  |
 |  |  |
Clinical Overview79
An osteoma is a benign bone-forming tumor, often considered reactive or developmental rather than truly neoplastic. These lesions typically present as a solitary exophytic mass composed of dense bone.
Location and Presentation
- Primary Sites: Craniofacial bones, including the skull and paranasal sinuses.
- Origin: Arises from either the periosteal or endosteal surface.
- Symptoms: Generally asymptomatic.
- ==Gardner’s Syndrome: If multiple osteomas are present, the patient must be evaluated for this syndrome (which includes intestinal polyps and skin tumors).==
Behavior and Prognosis
- Growth Pattern: Non-aggressive.
- Malignancy: There is no risk of malignant transformation.
- ==Differential Diagnosis: Distinguished from exostoses by the lack of a clear triggering factor (like trauma).==
Osteosarcoma80
Osteosarcoma is a primary malignancy of the bone characterized by the production of osteoid by neoplastic cells.
General Characteristics and Secondary Types
Clinical Features and Demographics81
- Nature: Malignant mesenchymal neoplasm
- Diagnostic Hallmark: Osteoid production by tumor cells
- Prevalence: Most common primary bone malignancy
- Age Predilection: 2nd decade of life
- Bimodal age distribution, but often affects the 2nd and 3rd decades
- Gender Predilection: Male > female (1.6:1 ratio)
Common Anatomical Sites
- Metaphysis of long bones
- Distal femur
- Proximal tibia
- Humerus
Predisposing Conditions and Etiology82
Secondary osteosarcoma may arise in the context of:
- Paget’s disease of bone
- Fibrous dysplasia
- Prior irradiation
- Retinoblastoma
- Associated with tumor suppressor gene (13q14)
- Osteochondromatosis
- Chronic osteomyelitis
Osteosarcoma of the Head and Neck83848586
 |  |
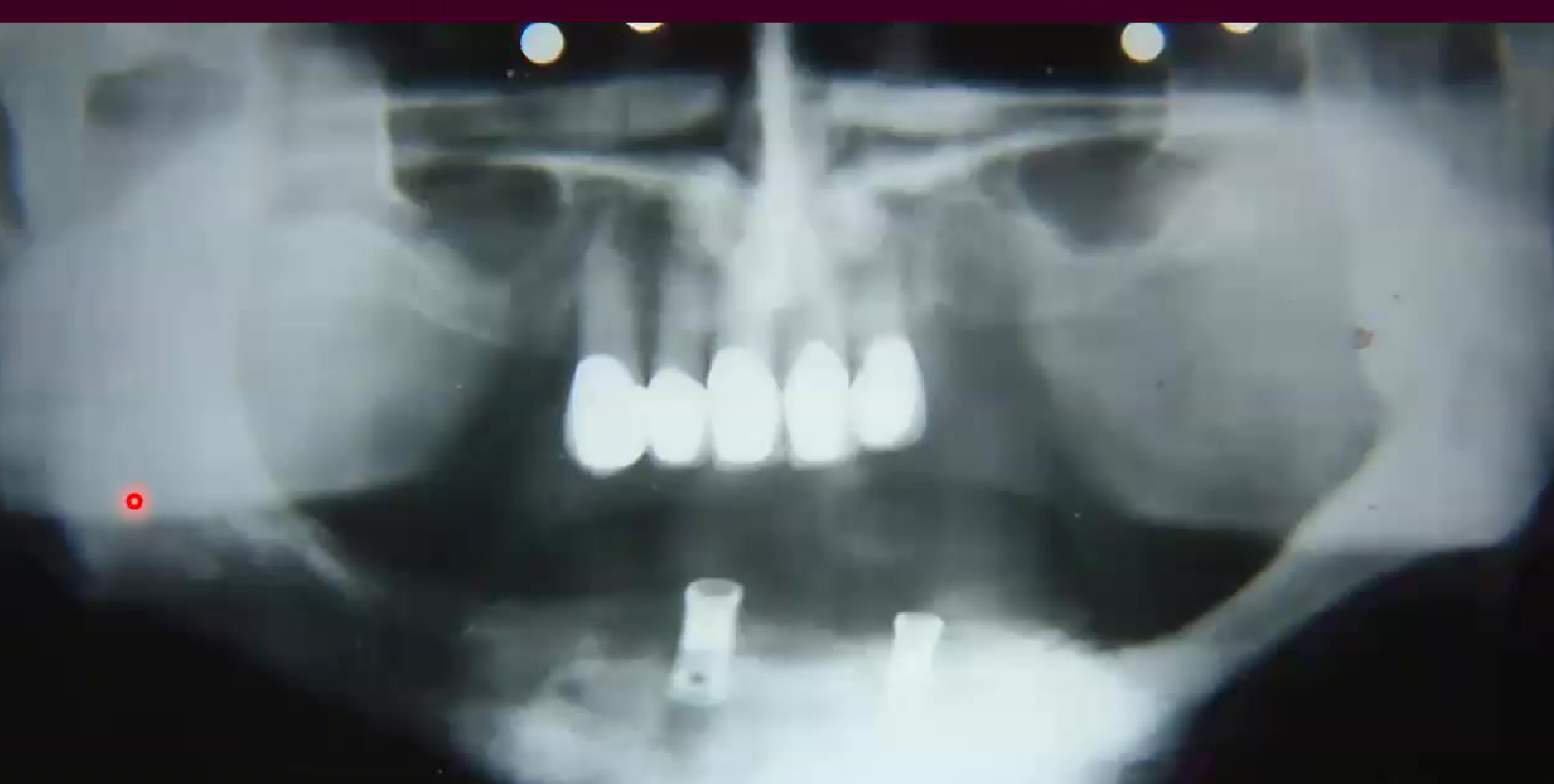 |  |
Clinical Presentation87
- Incidence: Rare in the jaws; approximately 6-8% occur in the gnathic skeleton
- Age: 3rd to 4th decade (mean age 33 years)
- Gender: Male > female
- Site Distribution:
- Mandible
- Maxilla
- Paranasal sinuses
- Skull
- Symptoms:
- Painful swelling
- Paresthesia
- Loose teeth
Radiographic Findings88
- Appearance: Mixed radiolucent – radiopaque
- Growth Pattern: Destructive with poorly defined, infiltrative borders
- Classic Patterns:
- Sunburst pattern (observed in 25% of cases)
- "Sunray" pattern: Radiating spicules of bone
- Symmetric widening of the periodontal ligament
- Calcification occurring above the level of the alveolar crest
- Spiking root resorption
- Sunburst pattern (observed in 25% of cases)
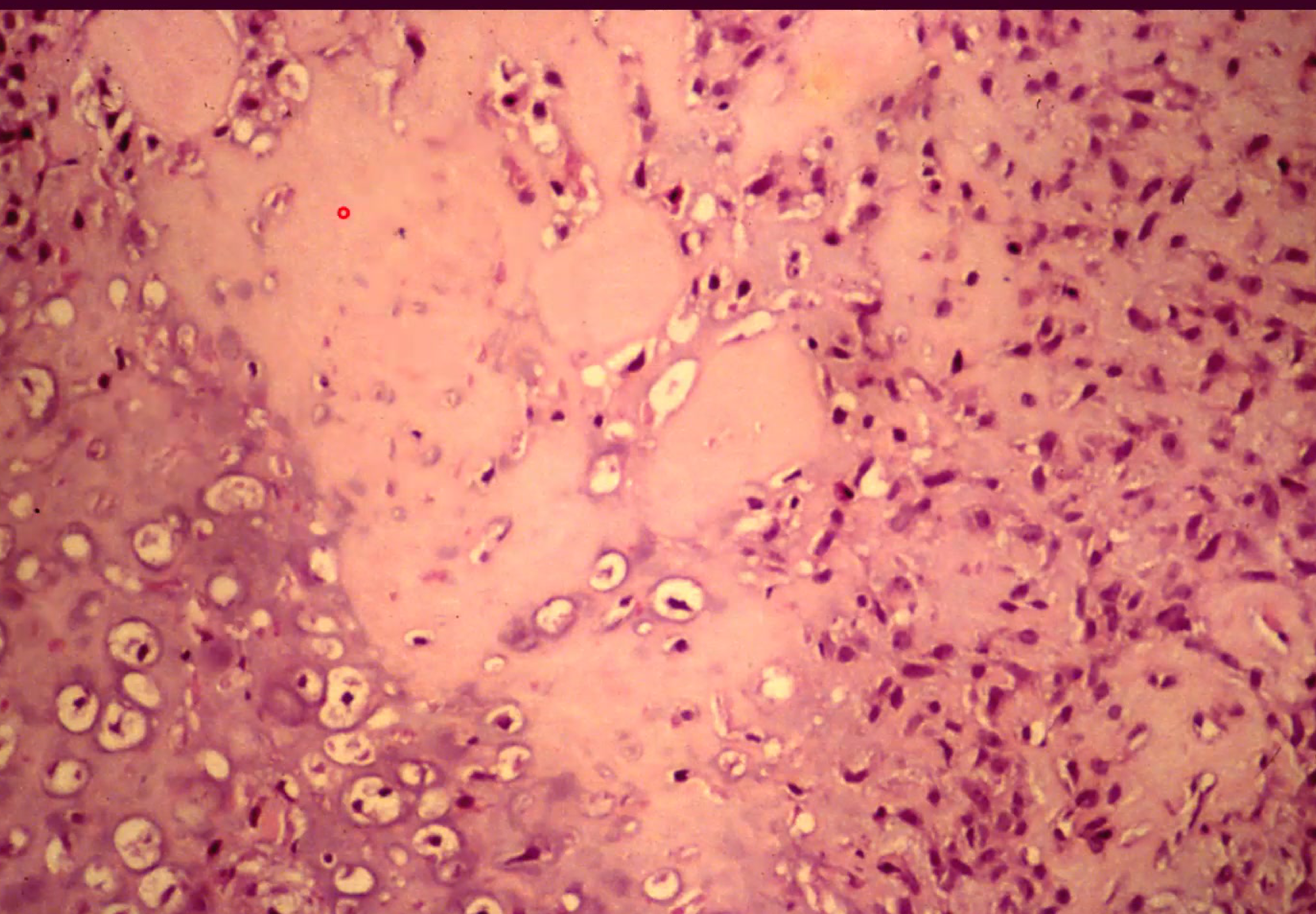
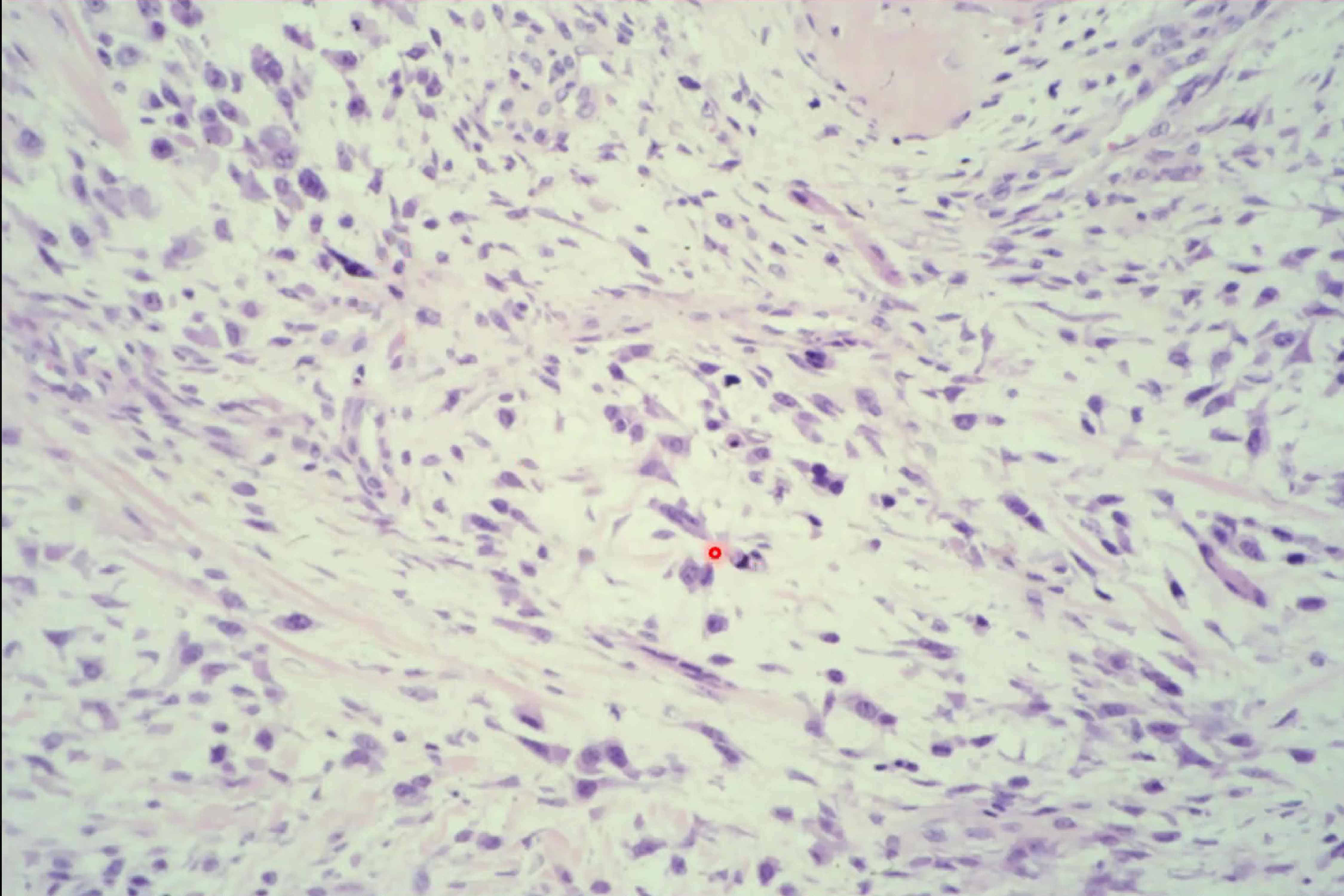
Histology and Clinical Labs89909192
 |  |
 |  |
Microscopic Features93
- Cellular Morphology: Pleomorphic malignant mesenchymal cells ranging from spindled to polygonal shapes
- Matrix Production: Evidence of osteoid production
- Histologic Variants:
- Osteoblastic
- Chondroblastic
- Fibroblastic
- **Malignancy Indicators:
- High mitotic activity and hyperchromatism**
- Atypical mitotic figures
- Necrosis
- Gnathic Specificity: Tumors of the jaws tend to be better differentiated than those in long bones
Treatment and Prognosis94

Clinical Laboratory Findings95
- Elevated alkaline phosphatase levels
Therapeutic Interventions
- Radical surgery
- Chemotherapy
- Radiation therapy
- Monoclonal antibody therapy
Clinical Outlook96
- Nature: Aggressive neoplasm
- Survival Rate: 30-50%
- Recurrence: Local recurrence occurs in approximately 70% of cases
- Metastasis: Occurs in 6-50% of cases
- Common sites: Lung, brain, and lymph nodes
- Mortality: Primarily driven by persistent local or regional disease
Metastatic Tumors to the Jaws979899
Metastases to the jaws represent a significant clinical concern in oral oncology, involving the spread of malignant cells from distant primary sites to the gnathic bones.
 |  |
 |  |
General Characteristics of Bone Metastasis100
Metastatic disease is the most common form of cancer involving the skeletal system. These lesions typically originate from carcinomas, with the most frequent primary sites being:
- Breast
- Prostate
- Lung
- Kidney
- Thyroid
Common Skeletal Sites and Pathogenesis
Metastatic spread frequently involves the vertebral column, pelvis, ribs, and skull. The spread is primarily hematogenous, often occurring via Batson’s venous plexus.
Clinical Presentation and Prognosis
- Lesion Types: Depending on cytokine mediation, lesions may appear as osteolytic (bone-destroying) or osteoblastic (bone-forming).
- Prognosis: Generally poor, indicating advanced systemic disease.
Clinical Features of Jaw Metastasis101
Metastatic tumors to the jaws are relatively uncommon, representing approximately 1% of oral malignancies. They primarily affect older adults.
- Primary Locations: The mandible is the most frequent site, accounting for 80% of cases.
- The lesions are most commonly found in the posterior mandible.
- Initial Presentation: In 50% of cases, the jaw metastasis is the first clinical evidence of an underlying malignancy.
Common Symptoms
Patients often present with the following clinical signs:
- Painful mass or swelling
- Unexplained loosening of teeth
- Paresthesia (numbness), particularly of the lower lip and chin
- Paresthesia is considered a major red flag for malignancy.
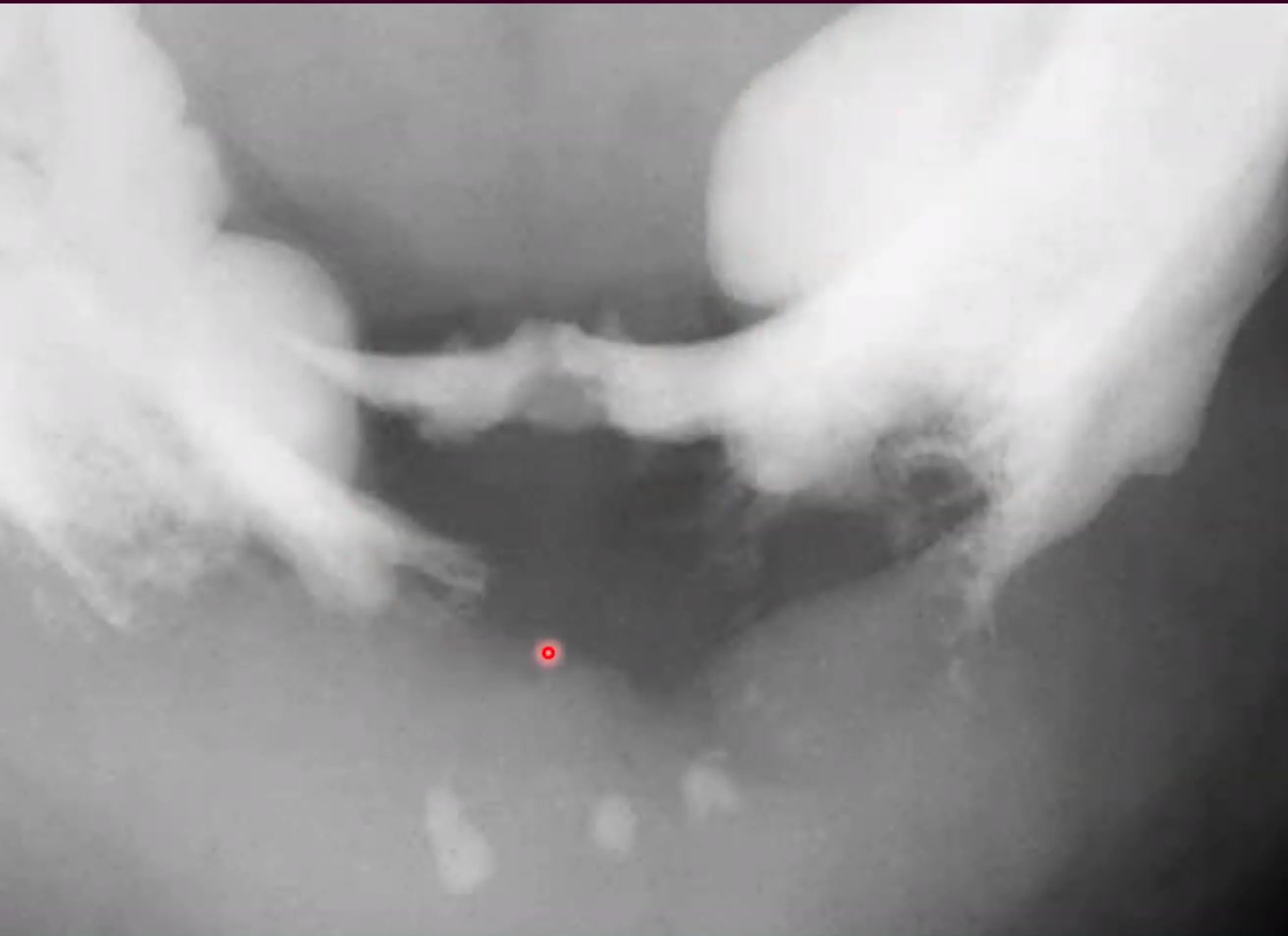
Radiographic Presentation102
The radiographic appearance of metastatic lesions varies based on the nature of the tumor:
- Osteolytic lesions: Present as ill-defined, destructive radiolucencies
- These often present with a "moth-eaten" appearance.
- Osteoblastic lesions: Present as radiopaque or mixed radiolucent-radiopaque lesions
- Prostate metastasis is a classic example of a primary site that produces osteoblastic (opaque) lesions.
- Diagnostic Pitfalls: These lesions may simulate common dental conditions, such as periapical or periodontal disease.
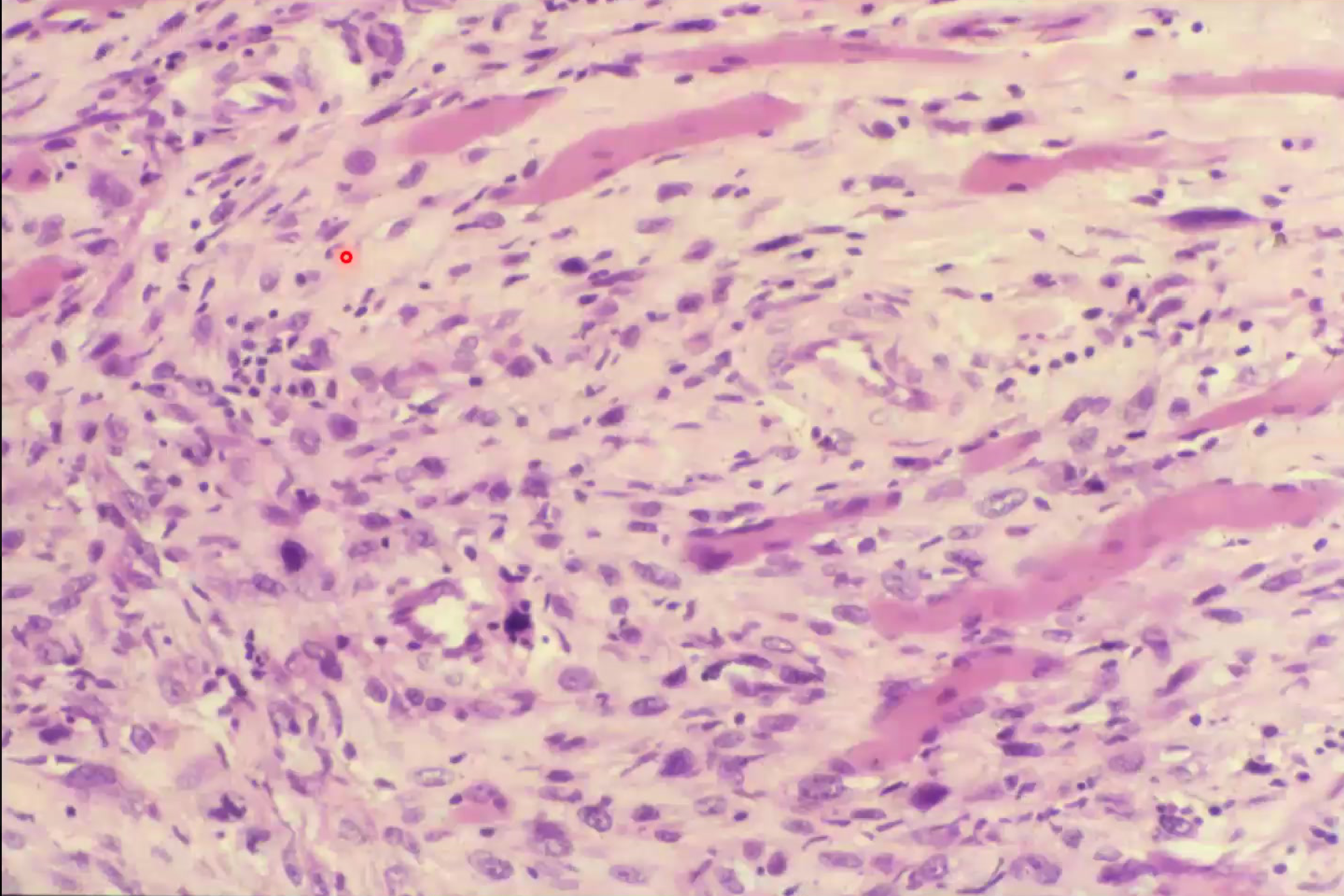
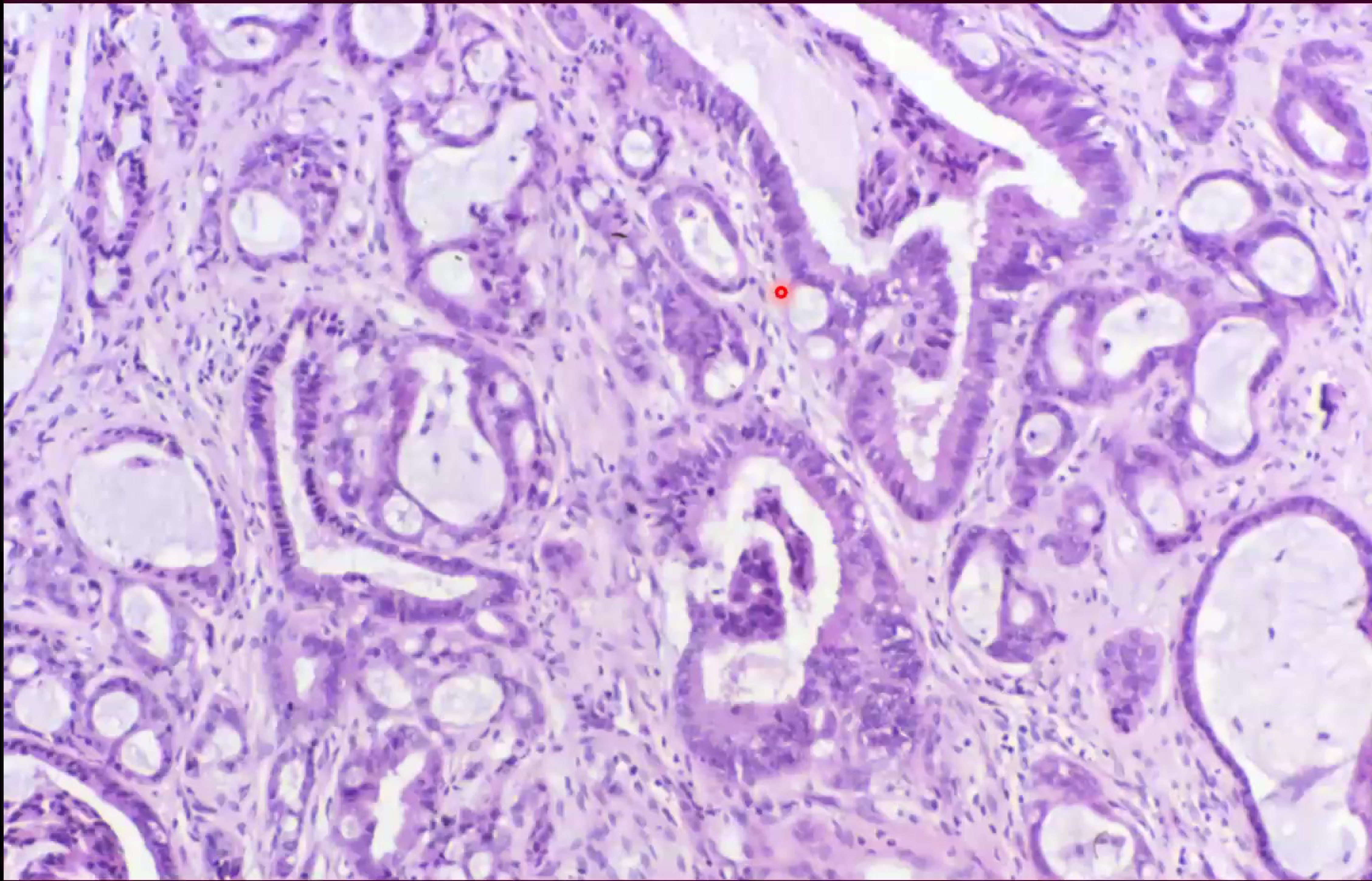
Histopathology and Outcomes
- Histology: Characterized by infiltrating nests and cords of pleomorphic epithelial cells supported by a fibrous stroma.
- Prognosis: The outlook is poor, as jaw involvement usually signifies widely disseminated disease.
- Survival Rate: Typically less than one year following diagnosis
Case Study: Prostate Metastasis
A patient presented with a dense, radiopaque (osteoblastic) area in the mandible and ulceration of the mucosa. The lesion was identified as a metastatic deposit from a primary prostate carcinoma, illustrating how metastatic disease can mimic primary bone tumors or periodontal disease.
Footnotes
-
Original PDF page 1: L19 Bone disease 3 slides, p.1 ↩
-
Original PDF page 3: L19 Bone disease 3 slides, p.3 ↩
-
Original PDF page 2: L19 Bone disease 3 slides, p.2 ↩
-
Original PDF page 4: L19 Bone disease 3 slides, p.4 ↩
-
Original PDF page 5: L19 Bone disease 3 slides, p.5 ↩
-
Original PDF page 6: L19 Bone disease 3 slides, p.6 ↩
-
Original PDF page 7: L19 Bone disease 3 slides, p.7 ↩
-
Original PDF page 9: L19 Bone disease 3 slides, p.9 ↩
-
Original PDF page 10: L19 Bone disease 3 slides, p.10 ↩
-
Original PDF page 11: L19 Bone disease 3 slides, p.11 ↩
-
Original PDF page 8: L19 Bone disease 3 slides, p.8 ↩
-
Original PDF page 13: L19 Bone disease 3 slides, p.13 ↩
-
Original PDF page 14: L19 Bone disease 3 slides, p.14 ↩
-
Original PDF page 12: L19 Bone disease 3 slides, p.12 ↩
-
Original PDF page 15: L19 Bone disease 3 slides, p.15 ↩
-
Original PDF page 16: L19 Bone disease 3 slides, p.16 ↩
-
Original PDF page 17: L19 Bone disease 3 slides, p.17 ↩
-
Original PDF page 19: L19 Bone disease 3 slides, p.19 ↩
-
Original PDF page 21: L19 Bone disease 3 slides, p.21 ↩
-
Original PDF page 18: L19 Bone disease 3 slides, p.18 ↩
-
Original PDF page 20: L19 Bone disease 3 slides, p.20 ↩
-
Original PDF page 22: L19 Bone disease 3 slides, p.22 ↩
-
Original PDF page 23: L19 Bone disease 3 slides, p.23 ↩
-
Original PDF page 26: L19 Bone disease 3 slides, p.26 ↩
-
Original PDF page 28: L19 Bone disease 3 slides, p.28 ↩
-
Original PDF page 29: L19 Bone disease 3 slides, p.29 ↩
-
Original PDF page 24: L19 Bone disease 3 slides, p.24 ↩
-
Original PDF page 25: L19 Bone disease 3 slides, p.25 ↩
-
Original PDF page 27: L19 Bone disease 3 slides, p.27 ↩
-
Original PDF page 30: L19 Bone disease 3 slides, p.30 ↩
-
Original PDF page 31: L19 Bone disease 3 slides, p.31 ↩
-
Original PDF page 33: L19 Bone disease 3 slides, p.33 ↩
-
Original PDF page 35: L19 Bone disease 3 slides, p.35 ↩
-
Original PDF page 32: L19 Bone disease 3 slides, p.32 ↩
-
Original PDF page 34: L19 Bone disease 3 slides, p.34 ↩
-
Original PDF page 36: L19 Bone disease 3 slides, p.36 ↩
-
Original PDF page 37: L19 Bone disease 3 slides, p.37 ↩
-
Original PDF page 38: L19 Bone disease 3 slides, p.38 ↩
-
Original PDF page 39: L19 Bone disease 3 slides, p.39 ↩
-
Original PDF page 40: L19 Bone disease 3 slides, p.40 ↩
-
Original PDF page 41: L19 Bone disease 3 slides, p.41 ↩
-
Original PDF page 43: L19 Bone disease 3 slides, p.43 ↩
-
Original PDF page 42: L19 Bone disease 3 slides, p.42 ↩
-
Original PDF page 44: L19 Bone disease 3 slides, p.44 ↩
-
Original PDF page 45: L19 Bone disease 3 slides, p.45 ↩
-
Original PDF page 46: L19 Bone disease 3 slides, p.46 ↩
-
Original PDF page 49: L19 Bone disease 3 slides, p.49 ↩
-
Original PDF page 47: L19 Bone disease 3 slides, p.47 ↩
-
Original PDF page 48: L19 Bone disease 3 slides, p.48 ↩
-
Original PDF page 51: L19 Bone disease 3 slides, p.51 ↩
-
Original PDF page 52: L19 Bone disease 3 slides, p.52 ↩
-
Original PDF page 50: L19 Bone disease 3 slides, p.50 ↩
-
Original PDF page 54: L19 Bone disease 3 slides, p.54 ↩
-
Original PDF page 55: L19 Bone disease 3 slides, p.55 ↩
-
Original PDF page 56: L19 Bone disease 3 slides, p.56 ↩
-
Original PDF page 57: L19 Bone disease 3 slides, p.57 ↩
-
Original PDF page 58: L19 Bone disease 3 slides, p.58 ↩
-
Original PDF page 59: L19 Bone disease 3 slides, p.59 ↩
-
Original PDF page 60: L19 Bone disease 3 slides, p.60 ↩
-
Original PDF page 61: L19 Bone disease 3 slides, p.61 ↩
-
Original PDF page 62: L19 Bone disease 3 slides, p.62 ↩
-
Original PDF page 63: L19 Bone disease 3 slides, p.63 ↩
-
Original PDF page 64: L19 Bone disease 3 slides, p.64 ↩
-
Original PDF page 65: L19 Bone disease 3 slides, p.65 ↩
-
Original PDF page 66: L19 Bone disease 3 slides, p.66 ↩
-
Original PDF page 67: L19 Bone disease 3 slides, p.67 ↩
-
Original PDF page 68: L19 Bone disease 3 slides, p.68 ↩
-
Original PDF page 69: L19 Bone disease 3 slides, p.69 ↩
-
Original PDF page 70: L19 Bone disease 3 slides, p.70 ↩
-
Original PDF page 71: L19 Bone disease 3 slides, p.71 ↩
-
Original PDF page 72: L19 Bone disease 3 slides, p.72 ↩
-
Original PDF page 73: L19 Bone disease 3 slides, p.73 ↩
-
Original PDF page 74: L19 Bone disease 3 slides, p.74 ↩
-
Original PDF page 76: L19 Bone disease 3 slides, p.76 ↩
-
Original PDF page 77: L19 Bone disease 3 slides, p.77 ↩
-
Original PDF page 78: L19 Bone disease 3 slides, p.78 ↩
-
Original PDF page 79: L19 Bone disease 3 slides, p.79 ↩
-
Original PDF page 80: L19 Bone disease 3 slides, p.80 ↩
-
Original PDF page 75: L19 Bone disease 3 slides, p.75 ↩
-
Original PDF page 81: L19 Bone disease 3 slides, p.81 ↩
-
Original PDF page 82: L19 Bone disease 3 slides, p.82 ↩
-
Original PDF page 83: L19 Bone disease 3 slides, p.83 ↩
-
Original PDF page 85: L19 Bone disease 3 slides, p.85 ↩
-
Original PDF page 86: L19 Bone disease 3 slides, p.86 ↩
-
Original PDF page 88: L19 Bone disease 3 slides, p.88 ↩
-
Original PDF page 89: L19 Bone disease 3 slides, p.89 ↩
-
Original PDF page 84: L19 Bone disease 3 slides, p.84 ↩
-
Original PDF page 87: L19 Bone disease 3 slides, p.87 ↩
-
Original PDF page 91: L19 Bone disease 3 slides, p.91 ↩
-
Original PDF page 92: L19 Bone disease 3 slides, p.92 ↩
-
Original PDF page 93: L19 Bone disease 3 slides, p.93 ↩
-
Original PDF page 94: L19 Bone disease 3 slides, p.94 ↩
-
Original PDF page 90: L19 Bone disease 3 slides, p.90 ↩
-
Original PDF page 53: L19 Bone disease 3 slides, p.53 ↩
-
Original PDF page 95: L19 Bone disease 3 slides, p.95 ↩
-
Original PDF page 96: L19 Bone disease 3 slides, p.96 ↩
-
Original PDF page 97: L19 Bone disease 3 slides, p.97 ↩
-
Original PDF page 101: L19 Bone disease 3 slides, p.101 ↩
-
Original PDF page 102: L19 Bone disease 3 slides, p.102 ↩
-
Original PDF page 98: L19 Bone disease 3 slides, p.98 ↩
-
Original PDF page 99: L19 Bone disease 3 slides, p.99 ↩
-
Original PDF page 100: L19 Bone disease 3 slides, p.100 ↩