Surgery in Oral Medicine Biopsy of Oral Lesions1
2024 UWA Dental Student Lecture
Presenter Information
- Dr Frank Chang
- Oral and Maxillofacial Surgeon
- BDS (Otago), MBChB (Auckland), FRACDS (OMS)
- Contact: Frank.chang@uwa.edu.au
Introduction to Biopsy
A biopsy is a clinical procedure involving the removal of cells or tissues from a living body for microscopic examination by a pathologist. This process is essential for several reasons:
What Is a Biopsy2
- Diagnostic Accuracy: To achieve a definitive diagnosis of a specific condition.
- Staging and Severity: To measure the severity of a disease or determine the stage of its progression.
- Treatment Planning: To facilitate and guide the required medical or surgical treatment.
Indications for Biopsy of Oral Tissue3
Biopsy of oral tissue is indicated in the following clinical scenarios:
Persistent Mucosal Abnormalities
- Any unexplained oral mucosal abnormality that persists despite conservative treatment or the removal of local irritants.
- Any lesion that remains persistent for more than 2 weeks with no obvious etiology.
Suspicion of Malignancy
- Persistent oral mucosal lesions that appear red and white (speckled), ulcerated, indurated, or fixated to deep underlying tissues.
- Lesions that bleed easily upon contact or exhibit rapid growth.
- Hemorrhagic or rapidly growing lesions: Lesions that bleed persistently or easily, or demonstrate rapid growth
Pigmented Lesions
- Unexplained pigmented oral mucosal lesions that are new or changing in appearance.
- Note: Biopsy may not be required if the pigmented lesion has been documented as stable and present for more than 5 years.
Functional Interference and Systemic Indicators
- Lesions interfering with local function, such as those causing trismus (restricted jaw opening).
- Sudden loosening of teeth without obvious periodontal cause (e.g., Langerhans cell histiocytosis).
- Sudden loosening of teeth in younger patients may specifically suggest Langerhans cell histiocytosis
- Persistent visible or palpable swelling with normal overlying tissue (e.g., suspected Lymphoma).
Hard Tissue Lesions
- Bone lesions that cannot be definitively diagnosed through clinical and radiological findings alone.
Contraindications for Biopsy4
While there are no absolute contraindications to biopsy, the decision to proceed depends on a thorough risk assessment of the following factors:
Patient Medical Status
Increased surgical risks may be present in patients with:
- Anticoagulation therapy (risk of hemorrhage).
- Immunocompromised status.
- Multiple systemic diseases or polypharmacy.
- Physical frailty or general malaise.
Clinical and Surgical Constraints
- Surgical Difficulty: Considerations regarding physical access to the site, availability of specialized surgical equipment, and the clinician’s specific skill level
- Considerations include lesions requiring general anesthesia due to location difficulty or vascularity requiring airway control.
- Clinician Factors: The dental clinician’s training, level of skill, interest, and experience in surgical pathology
- If uncomfortable with the procedure, refer to an oral and maxillofacial surgeon or oral medicine specialist.
High-Risk Lesion Characteristics
- Malignant Potential: If a high suspicion of malignancy exists, consider immediate referral to a specialist to avoid delays in definitive management.
- Vascular Lesions: Suspected vascular lesions (e.g., hemangiomas) carry a high risk of uncontrollable bleeding and should be managed with caution
- Suspected vascular lesions should be referred for management in a controlled setting, such as an operating theatre, due to bleeding risk.
Referral Considerations
If the clinician is unsure of the diagnosis or the surgical requirements, a referral to an Oral and Maxillofacial surgeon is recommended.
Lesion Detection and Diagnosis Pathway5
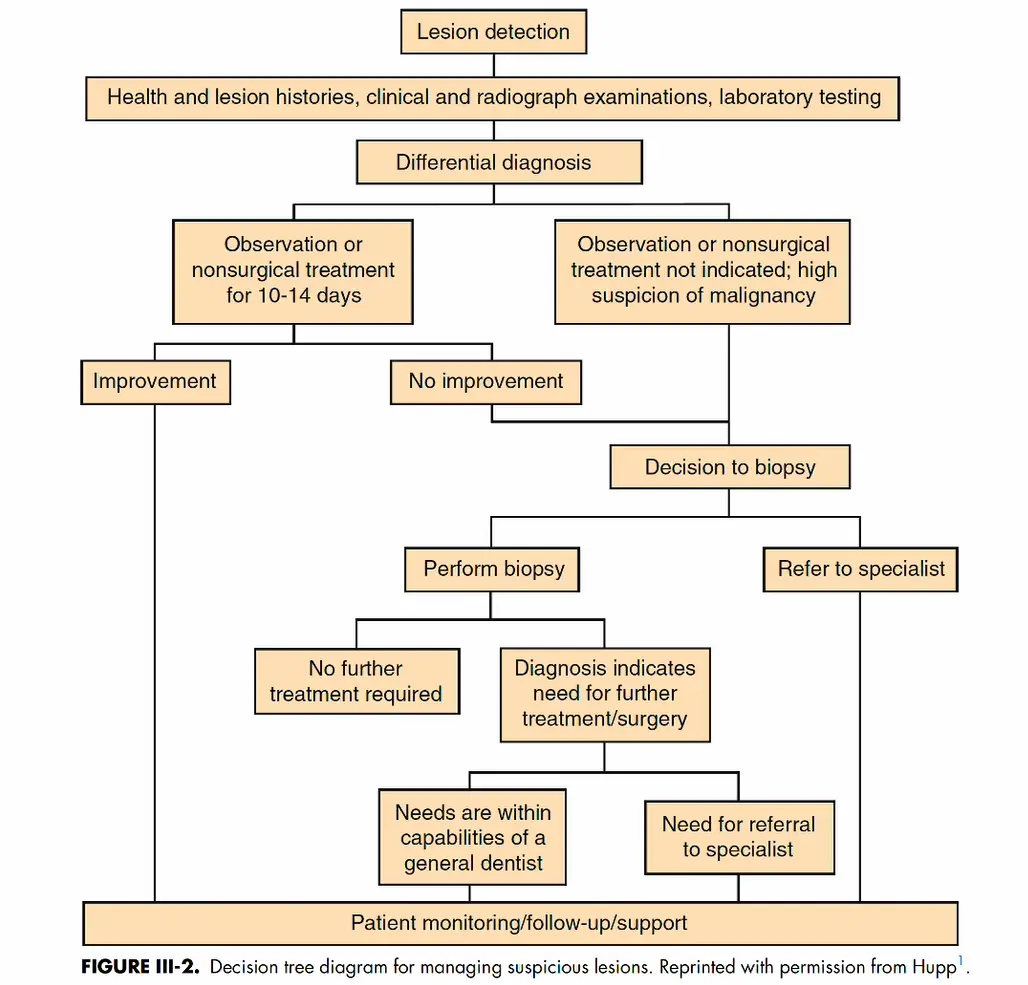 The management of suspicious oral lesions follows a structured decision-making process to ensure timely diagnosis and treatment.
The management of suspicious oral lesions follows a structured decision-making process to ensure timely diagnosis and treatment.
Initial Assessment and Differential Diagnosis
- Lesion Detection: Conduct a thorough review of health and lesion histories, clinical and radiographic examinations, and necessary laboratory testing
- Investigation includes obtaining a history of progression and conducting laboratory testing such as blood tests.
- Clinical Pathway Selection:
- If the lesion has a low suspicion of malignancy: Observation or nonsurgical treatment for 10–14 days.
- If observation is not indicated or there is a high suspicion of malignancy: Proceed directly toward biopsy or referral.
Immediate Action
Immediate biopsy is required for lesions highly suspicious for malignancy or specific diseases without waiting for an observation period.
Biopsy Decision Tree
- If no improvement is seen after the observation period:
- Option A: Perform Biopsy
- If the biopsy results indicate no further treatment is required, return to monitoring.
- If the diagnosis indicates a need for further treatment or surgery:
- Manage the case if within the capabilities of the general dentist.
- Refer to a specialist if the required treatment is complex.
- Option B: Refer to Specialist
- Direct referral for specialized diagnostic workup and management.
- Option A: Perform Biopsy
Long-term Management
- Continuous patient monitoring, follow-up, and support are required regardless of the initial biopsy outcome.
Patient Assessment and Examination
History of Presenting Complaints
-
Duration and Awareness
- Determine how long the lesion has been present.
- Distinguish between new lesions and those present for several years (the latter are more likely to be benign).
- Assess patient awareness of the lesion.
- Assess if the lesion was an incidental finding during a routine examination.
-
Changes in Size and Character
- Rapid enlargement may indicate an aggressive lesion or possible malignancy.
- Slow growth is often associated with benign lesions, though not exclusively.
- Observe changes in character, such as a mass starting to ulcerate or a vesicle turning into an ulcer.
-
Associated Symptoms
- Evaluate for pain, altered sensation, changes in taste, odor, dysphagia, or trismus.
-
Anatomical Location
- Identify the specific site, as certain lesions have a predilection for specific areas (e.g., keratinized vs. non-keratinized tissue).
-
Systemic Symptoms and Events
- Check for fever, malaise, or nausea.
Precipitating Factors
Identify if the onset was associated with recent dental treatments or exposure to specific chemicals.
Patient Management6
- Consider systemic conditions:
- Viral (measles, mumps, mononucleosis, herpes, AIDS).
- Autoimmune (pemphigus, lichen planus, erythema multiforme).
- Sexually Transmitted Infections (STIs).
- Identify surrounding events associated with onset, such as trauma, recent treatment, new medications, exposure to toxins, or recent travel.
Medical History
- Systemic illnesses can present with oral manifestations.
- In some cases, different diagnostic tests may be required instead of a biopsy.
Medication History7
Medication-Induced Conditions
- Assess for conditions triggered by medications, such as:
- Stevens-Johnson syndrome
- Aspirin burn
- Petechiae - Petechiae (particularly relevant for patients on anticoagulants)
Allergy History
- Document allergies to:
- Antibiotics
- NSAIDs
- Iodine
- Other substances - Food products that may trigger oral mucosal manifestations
Clinical Examination8
Clinical examination involves both inspection and palpation of the lesion.
Anatomical Location and Tissue Origin
A differential diagnosis can be developed based on the location. Pathologies may arise from various tissue types:
- Epithelium/mucosa
- Submucosal connective tissue
- Muscle or tendon
- Nerve
- Bone
- Blood vessels
- Lymphatic or salivary glands
Physical Characteristics
Identify the specific clinical presentation of the lesion:
- Bullae, vesicles, or pustules
- Crusts, scales, or erosion
- Ulcers or stomatitis
- Macules, papules, nodules, or plaques
- Hyperkeratosis, keratotic, or leukoplakia
- Hypertrophic or hyperplastic changes
- Dysplasia or malignancy
Single Versus Multiple Lesions9
Lesion Distribution
- Determine if the lesion is single or multiple (e.g., a single ulcer vs. multiple ulcers).
- Consider etiologies such as infection (viral, bacterial, fungal), trauma, or autoimmune disease.
Size, Shape, and Growth Pattern
- Margins: Regular vs. irregular.
- Growth: Exophytic vs. endophytic.
- Attachment: Sessile vs. pedunculated.
Surface Appearance
- Texture: Smooth, verruciform, or irregular.
- Ulcer Margins: Rolled, flat, raised, or everted.
- Ulcer Base: May be smooth, granulated, covered by a fibrin membrane, sloughing, or characterized by a hemorrhagic scab.
Coloration
- Dark Blue: May suggest a vascular lesion.
- Blue: May resemble a mucous retention cyst.
- Pigmented: Can range from a metallic tattoo to a melanotic tumor.
- Erythematous: Red lesions may represent more severe dysplastic changes compared to white lesions.
Mobility10
Tissue Attachment
- Determine if the lesion is fixed to surrounding deep tissues or is freely mobile.
- Assess whether the lack of mobility is due to the underlying structure of origin or infiltration into surrounding tissues.
Consistency and Palpation
- Soft/Compressible: Typical of lipoma, abscess, or mucous retention cyst.
- Firm/Indurated: Suggestive of fibroma or malignancy.
- Hard: Typical of bony exostosis.
- Fluctuant: Indicates a fluid-filled cavity, such as an abscess or mucous retention cyst.
Pulsation
- Presence of pulsation suggests a vascular lesion.
- Pulsation in a bluish lesion may specifically indicate an arteriovenous malformation.
Lymph Nodes
- Evaluate for lymphadenopathy; the location of involved nodes can indicate the spread of disease.
Documentation of Lesion11
- Ensure careful and detailed documentation of the lesion.
- Include a drawing or graphic schematic indicating:
- Location and orientation
- Shape and dimensions
- Maintain a digital photographic record.
- Sequential photography is recommended to enable comparison over time and detect progressive changes.
Features Suspicious of Malignancy12
- Bleeding: Occurs upon gentle manipulation.
- Duration: The lesion has persisted for more than two weeks.
- Erythroplasia: Presentation as a red lesion or a speckled red-and-white lesion.
- Fixation: The lesion is attached to adjacent structures.
- Growth Rate: Rapid increase in size.
- Induration: The lesion and surrounding tissues feel firm to the touch.
- Ulceration: The lesion is ulcerated or presents as a persistent ulcer
- Persistence: Any lesion exceeding two weeks without resolution or showing progressive worsening..
Biopsy Principles and Classification
Biopsy involves the removal of tissue from a living body for microscopic diagnostic examination. It stands as the most precise and accurate of all diagnostic tissue procedures.
General Principles of Biopsy13
Indications and Purpose
- Performed whenever a definitive diagnosis cannot be obtained using less invasive procedures, such as cytology, brush cytology, or Fine Needle Aspiration (FNA).
- The primary purpose is to determine a precise diagnosis to ensure the provision of proper treatment.
Handling
Gentle handling of the tissue is paramount; rough handling causes artifacts that compromise pathological interpretation.
Types of Biopsy14
Surgical Biopsy Methods (Main focus)
These techniques represent the main focus for dentists in general practice:
- Punch Biopsy
- Incisional Biopsy
- Excisional Biopsy
Specialized Diagnostic Techniques (Done by specialists)
- Fine Needle Aspiration Cytology (FNAC)
- Core Biopsy
- Cytology
- Brush Biopsy
- Frozen section Biopsy
Detailed Biopsy Techniques
The standard protocol for performing a biopsy includes the following clinical steps:
Biopsy Procedure Overview15
- Identify and mark the area for biopsy
- Marking: Outline the biopsy area and photograph for documentation
- Surgical preparation: Clean the field using chlorhexidine or iodine preparations to minimize post-operative infection
- Preparation of the surgical field
- Administration of local anesthesia
- Collection of the tissue sample
- Handling and preservation of the specimen
- Management of the surgical wound
Biopsy Techniques16171819
 Commonly utilized surgical biopsy techniques include:
Commonly utilized surgical biopsy techniques include:
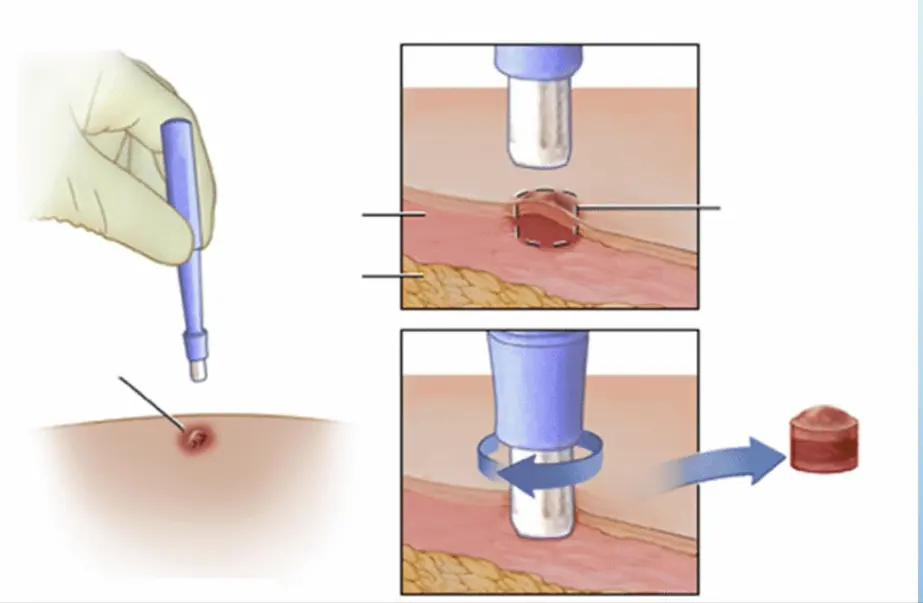
- Punch Biopsy: Utilizing a circular blade to remove a core of tissue.
- Instrumentation: Available in sizes 3mm, 4mm, and 6mm; the silver circular blade incises the tissue
- Technique: Apply twisting motion to punch through the lesion; use Adson's forceps to grasp the specimen; excise the basal attachment with scalpel or scissors
- Incisional Biopsy: Removal of a representative portion of a lesion for diagnostic purposes.
- Excisional Biopsy: Complete removal of the entire lesion, typically performed on smaller localized abnormalities.
Clinical Procedure Overview
The process of performing an oral biopsy, specifically on the lower lip, typically involves the following stages:
- Identification of the ulcerative lesion.
- Execution of the punch biopsy.
- Amputation of the tissue specimen using surgical scissors.
- Reapproximation of the tissue edges using sutures.
Punch Biopsy20
Clinical Considerations for Punch Biopsy
- Ease of Use: This is considered an easy technique.
- Suturing Requirements:
- Sutures may not be required if a small diameter punch is utilized.
- If sutures are necessary, a single suture is often sufficient.
- Site Suitability:
- Highly effective for soft tissues that are bound down, such as the gingiva, alveolar soft tissue, and hard palate.
- The procedure is more tedious when performed on mobile soft tissue.
- Mobile soft tissue examples include the cheek, tongue, and floor of mouth.
Incisional and Excisional Biopsy2122
Selection Criteria for Biopsy Types
- Instrument Setup: Standard surgical biopsy setup is required for both incisional and excisional procedures.
- Incisional Biopsy Indications:
- Large lesions.
- Lesions exhibiting multiple different characteristics in different areas.
- Suspected malignant lesions.
- Excisional Biopsy Indications:
- Small lesions that can be completely removed along with a surrounding margin of normal tissue.
Incisional Biopsy232425
Indications and Sampling Technique
- Primary Indications:
- Suspicion of malignancy.
- Large lesion area.
- Situations with location restrictions involving vessels, nerves, or ducts.
- Sampling Methodology:
- The specimen is taken as a wedge in an area representative of the lesion.
- Sampling should target the most suspicious or “worst looking” area.
- Multiple samples may be necessary.
- Biopsy must include normal margins and deep margins to provide adequate diagnostic information.
Case Study: Leukoplakia of the Left Buccal Mucosa
An incisional biopsy was performed on a leukoplakic lesion of the left buccal mucosa. The specimen was oriented with a suture marking the anterior aspect, placed adjacent to a ruler to document dimensions. This orientation facilitates precise localization for definitive treatment if margins are involved.
Disadvantages of Incisional Biopsy
- Tissue Artifacts: Due to small sampling sizes, handling of the tissue can cause crushing and hemorrhage, resulting in artifacts that may complicate diagnosis.
- Cell Seeding: There is a risk of seeding malignant cells into the surrounding normal tissue.
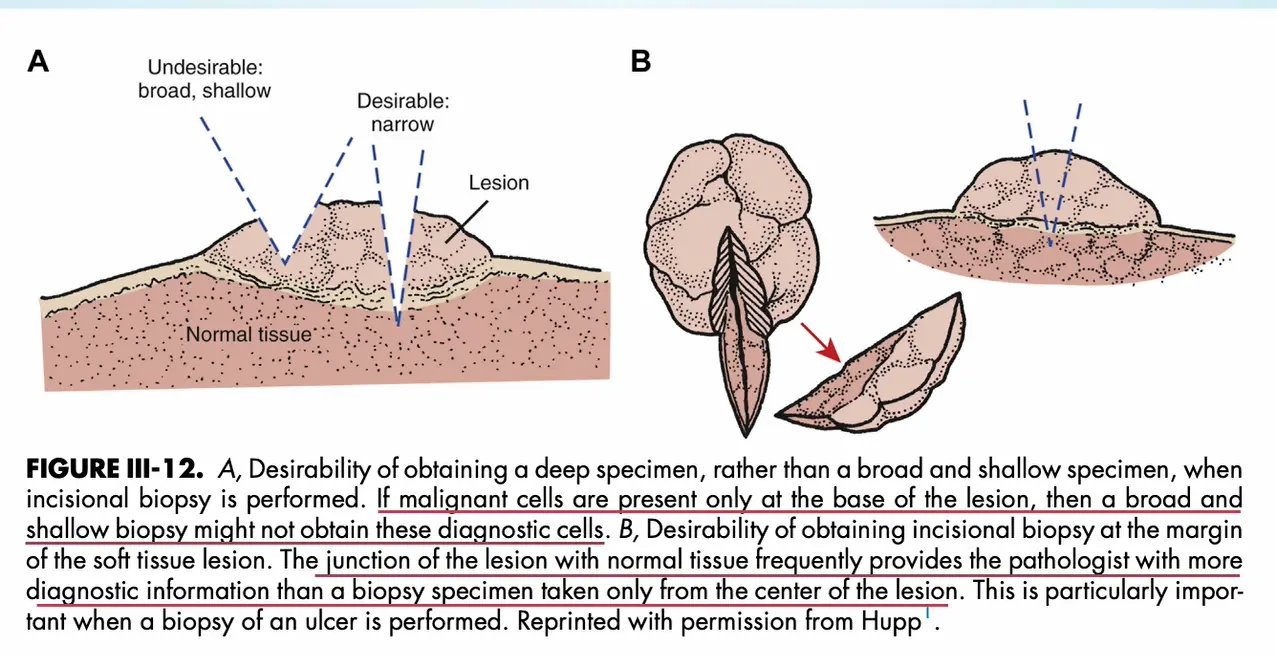
Specimen Depth and Margin Selection
- Specimen Depth: It is desirable to obtain a deep specimen rather than a broad and shallow one. If malignant cells are present only at the base of the lesion, a shallow biopsy may fail to capture diagnostic cells.
- Margin Inclusion: Obtaining the biopsy at the margin of the soft tissue lesion is preferred. The junction of the lesion with normal tissue frequently provides more diagnostic information than a specimen taken only from the center. This is particularly critical when performing a biopsy of an ulcer.
Excisional Biopsy2627
Indications and Procedure for Excisional Biopsy
- Definition: Complete removal of the entire lesion.
- Indications:
- Smaller lesions that can be removed with a normal margin without causing wound distortion.
- Lesions that appear clinically benign.
- Surgical Technique:
- Removal of the entire lesion with a 2-5mm margin of normal-appearing tissue.
- The biopsy sample should be marked to orient the specimen for the pathologist.
- For infiltrative lesions, marking facilitates the removal of further soft tissue if necessary.
- Orientation: Mark the specimen with a suture at one corner, documenting whether this represents the anterior, posterior, or other specific aspect to guide future re-excision if margins are positive.
Surgical Approach for Excision
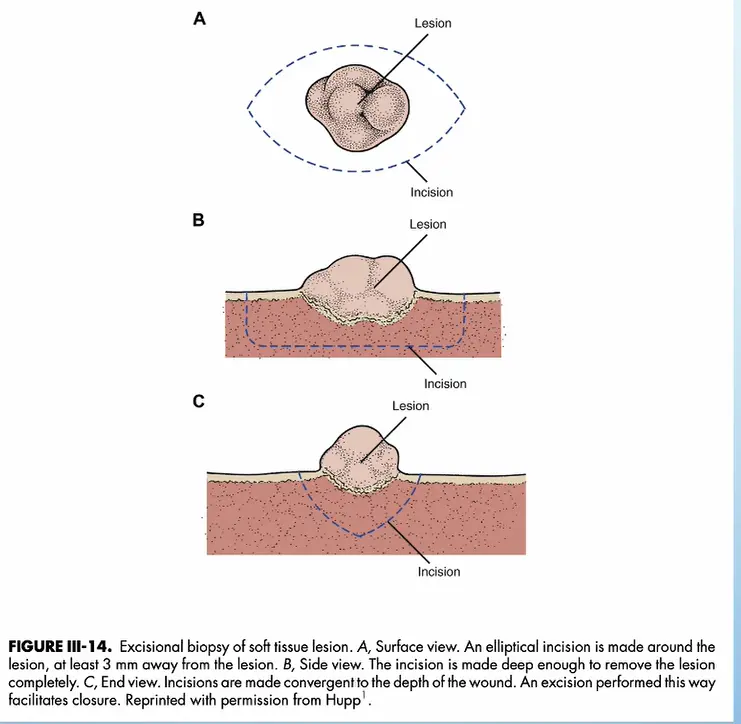
- Incision Geometry: An elliptical incision is made around the lesion, maintaining a distance of at least 3 mm from the lesion borders.
- Depth and Angulation:
- The incision must be deep enough to remove the lesion completely.
- Incisions should converge toward the depth of the wound (forming a V-shape in cross-section) to facilitate easier closure.
Case Study: Submental Region Lymphoma
A growth in the submental region was completely excised as an excisional biopsy for diagnostic analysis. The pathology report confirmed lymphoma, demonstrating the utility of excisional biopsy for diagnostic purposes in accessible swellings.
Case Study: Tongue Lesion with Atrophic Papilla
An excisional biopsy of the left lateral tongue demonstrated an area of atrophic papilla. The procedure required careful dissection down to the muscle of the tongue, avoiding "buttonholing" (perforation) of the musculature. The specimen was marked with a suture at the anterior aspect and photographed with a ruler. Due to the tongue's vascularity and the need for patient immobility, sedation or general anesthesia may be necessary.
Case Study: Right Soft Palate/Hard Palate Lesion
A lesion of the right soft palate/hard palate was completely excised. The specimen was divided: one half sent for immunohistochemistry and one half for routine histopathology, with the entire specimen labeled against a ruler for margin assessment.
Case Study: Left Hard Palate Lesion
This excisional biopsy involved initial marking with dots around the lesion, followed by a firm line delineating the margins. The wound was left to heal by secondary intention (no suturing possible on hard palate). Preoperative assessment ensured no adjacent blood vessels were present; any encountered vessels required cauterization.
Fine Needle Aspiration28
Applications and Benefits of Fine Needle Aspiration (FNA)
- Procedure: Involves the aspiration of fluid, cells, or tissue products using a fine needle for microscopic examination.
- Clinical Applications:
- Biopsy of fluctuant lesions.
- Collection of cellular samples from lymph nodes.
- Evaluation of deep lesions found incidentally on CT scans (often ultrasound-guided).
- Used to rule out vascular lesions.
- Diagnostic utility: Rules out vascular lesions (significant blood backflush indicates vascularity); useful for cystic lesions.
- Advantages:
- Simple technique with minimal patient pain.
- Cost-effective.
- Results in a minimal wound.
Specimen Handling and Transport
To ensure an accurate diagnosis, the pathology request must be completed with comprehensive information:
Patient and Test Identification
- Accurate patient details
- Specific test required:
- Histopathology
- Cytology
Pathology Request29
Clinical Documentation
Detailed clinical notes are essential to assist the pathologist. Include the following data points:
- Precise location of the lesion
- Duration (how long the lesion has been present)
- Size of the lesion and any recorded changes in dimensions
- Physical characteristics and morphological features of the lesion
- Any associated symptoms reported by the patient
- Clinician’s differential diagnosis
Importance of Clinical Notes
Pathologists examine only the submitted specimen without seeing the patient; therefore, comprehensive clinical notes are essential for accurate diagnosis.
Transport of Specimen30
Media for Histological and Immunofluorescence Analysis
- Routine Light Microscopy: For standard Haematoxylin and eosin (H&E) testing, specimens should be transported in a 10% buffered formalin solution.
- Direct Immunofluorescence (DIF):
- Tissue can be submitted in a sterile pot containing saline-soaked gauze. Note that delays in collection and processing may reduce diagnostic accuracy.
- Alternatively, Michel’s medium can be used as a transport medium when immediate processing is not possible.
- Microbiological Culture: Tissue should be submitted fresh in a sterile container. Consult the pathology provider if specific requirements are unclear.
- Submit in fresh sterile container without fixative
- Contact the laboratory if uncertain about transport media
Labeling and Verification
Sample containers must be clearly labeled to prevent errors. Ensure the following details are present and consistent with the request form:
- Patient identification details
- Precise anatomical body site of the biopsy
- Time and date of the procedure --- Lecture stopped here
Practical Templates
Procedure Overview
Incisional Biopsy Template313233
An incisional biopsy is a diagnostic procedure used to remove a representative portion of a lesion for histopathological examination. This technique is typically indicated for large lesions, suspected malignancies, or when a definitive diagnosis is required before definitive treatment can be planned.
Documentation Essentials
- Patient identification: Name, date of birth, medical record number
- Orientation marking: Documentation of suture placement (e.g., "suture marks anterior margin") and use of measurement scales (rulers) in photographs
- Special instructions: Indicate if portion of specimen is for immunohistochemistry vs. routine histopathology
Clinical Documentation and Steps
- Site Selection: Identify the most representative area of the lesion, avoiding necrotic or heavily traumatized tissue.
- Anesthesia: Administer local anesthesia, ensuring the injection is peripheral to the biopsy site to avoid tissue distortion or artifact.
- Incision: Perform a wedge-shaped or deep elliptical incision to include both the lesion and a small margin of adjacent normal-appearing tissue.
- Tissue Handling: Carefully remove the specimen using fine forceps or a traction suture to minimize crush injury.
- Hemostasis and Closure: Achieve primary closure using sutures if necessary, or apply local measures to control bleeding.
Clinical Presentation and Assessment
- Clinical Appearance: Describe the lesion’s color, size, shape, and texture.
- Surface characteristics (smooth, verrucous, ulcerated)
- Location: Specify the exact anatomical site.
- Duration: Note how long the lesion has been present.
- Rate of growth and associated systemic factors
- Symptoms: Record any pain, numbness, or functional interference.
- Differential Diagnosis: List the most likely clinical possibilities.
Procedural Details
- Anesthesia: Type and amount of local anesthetic used (e.g., 2% Lidocaine with 1:100,000 epinephrine).
- Incision Site Selection:
- Target the most representative area of the lesion.
- Include a margin of normal-appearing tissue if possible to show the interface.
- Avoid necrotic or heavily traumatized areas.
- Technique:
- Use a scalpel (typically #15 blade) to perform a wedge-shaped incision.
- Ensure adequate depth to include the underlying connective tissue.
- Tissue Handling: Use fine-toothed forceps or a traction suture to avoid crush artifacts.
Closure and Post-Operative Care
- Hemostasis: Achieved via pressure, electrocautery, or chemical agents.
- Suturing: Specify the type of suture material (e.g., 4-0 Silk, Chromic Gut) and the number of sutures placed.
- Specimen Management: Immediate immersion in 10% neutral buffered formalin.
- Instructions to Patient: Provide verbal and written post-operative care instructions, including management of swelling and pain.
- Follow-up: Schedule an appointment for suture removal and review of the pathology report.
Biopsy Site Diagrams3435363738
Right Lateral Tongue Biopsy Site
- Location: Right lateral tongue
- Orientation: Anterior to Posterior
Anterior Left Lateral Tongue Biopsy Site
- Location: Anterior left lateral tongue
- Orientation: Anterior to Posterior
Anatomical Mapping for Biopsy Sites
To ensure accurate clinical records and pathology correlation, the following anatomical diagrams are utilized to mark the precise location of oral lesions. Proper documentation of the biopsy site is critical for follow-up care and potential surgical re-resection.
Photographic and Schematic Standards
To ensure high-quality documentation, clinicians should utilize:
- Schematic drawings: Graphic documentation showing lesion location relative to anatomical landmarks like teeth, frenula, and the palate
- Photographic standards: Images including pre-operative marking (dots or lines outlining margins), measurement scales (rulers), post-excision views of the wound bed, and specimen photographs with orientation sutures
Maxillary and Palatal Landmarks
- Hard Palate: Central and lateral regions.
- Soft Palate: Posterior to the hard palate, including the uvula.
- Maxillary Alveolar Ridge: Divided by quadrants (Right and Left).
- Maxillary Vestibule: Labial and buccal aspects.
Mandibular and Floor of Mouth Landmarks
- Mandibular Alveolar Ridge: Divided by quadrants (Right and Left).
- Mandibular Vestibule: Labial and buccal aspects.
- Floor of the Mouth: Sublingual regions, divided by the midline frenum.
- Retromolar Trigone: Posterior to the last mandibular molar.
Tongue and Buccal Mucosa
- Dorsum of the Tongue: Anterior two-thirds and posterior one-third.
- Lateral Borders of the Tongue: Right and left margins (high-risk areas).
- Ventral Surface of the Tongue: Underside of the tongue.
- Buccal Mucosa: Internal cheek lining from the commissure to the pterygomandibular raphe.
Labial and Facial Landmarks
- Upper and Lower Lips:
- Vermilion border
- Labial mucosa
- Commissures (corners of the mouth)
Example Pathology Report and Closing39
Patient and Provider Information
- Patient Name: John Atkinson
- DOB: 31/05/1951 (70 Yrs Male)
- Lab ID: 434829626
- Specimen Number: 162071-21CL
- Referrer: Dr Frank Chang
- Requested/Collected: 01/12/2021
Histopathology Report
Clinical Details
- 70-year-old male.
- Right lateral tongue raised lesion with rough surface and healing ulcer posteriorly.
- Photos available on request.
Macroscopic Description
- Specimen: Right side tongue lateral; an orientated irregular mucosal fragment measuring 14 x 9 x 3mm.
- Orientation:
- Marking suture at the anterior pole (12 o’clock).
- 3 o’clock margin inked green.
- 9 o’clock margin inked black.
- Processing: Transversely sectioned into five pieces and processed in two blocks (5-2A TPM).
Microscopic Description
- Examination: Six levels of blocks 1A and 1B were examined.
- Observations:
- Mature fibrous connective tissue covered by parakeratinised stratified squamous epithelium with a papillary surface configuration.
- No ulceration seen at these levels.
- Features of epithelial dysplasia present, including nuclear pleomorphism, hyperchromatism, and irregular stratification.
- Dysplastic features are confined to the lower half of the epithelium.
- Eosinophilic coagulum observed in the basement membrane zone.
- Moderately intense chronic inflammatory cell infiltrate (predominantly lymphocytes and macrophages) in the connective tissue, disrupting the epithelium.
- No PAS-D positive fungal elements identified.
Conclusion
- Diagnosis: Right lateral tongue showing parakeratosis with moderate epithelial dysplasia, possibly on a background of oral mucosal lichen planus
- The conclusion or diagnosis provides a definitive pathological diagnosis, such as squamous cell carcinoma, fibroma, or lymphoma, and includes margin status where applicable..
- Margins: Mild dysplasia extends to peripheral margins.
- Recommendation: Clinical correlation is required.
Review and Authentication
- Case Review: Reviewed with Dr Norman Firth using remote digital microscopy.
- Pathologist: Dr Jason Lau (Clinipath Specialist Oral Pathology Service).
- Accreditation: Accredited for compliance with NPAAC standards and ISO 15189.
Closing Remarks
Biopsy of oral lesions requires careful patient selection, meticulous technique, and thorough documentation. When uncertainty exists regarding approach, technique, or management, consultation with oral and maxillofacial surgery or oral medicine specialists is appropriate to ensure optimal patient outcomes.
Footnotes
-
Original PDF page 1: L2 Surgery in Oral medicine, p.1 ↩
-
Original PDF page 2: L2 Surgery in Oral medicine, p.2 ↩
-
Original PDF page 3: L2 Surgery in Oral medicine, p.3 ↩
-
Original PDF page 4: L2 Surgery in Oral medicine, p.4 ↩
-
Original PDF page 5: L2 Surgery in Oral medicine, p.5 ↩
-
Original PDF page 6: L2 Surgery in Oral medicine, p.6 ↩
-
Original PDF page 7: L2 Surgery in Oral medicine, p.7 ↩
-
Original PDF page 8: L2 Surgery in Oral medicine, p.8 ↩
-
Original PDF page 9: L2 Surgery in Oral medicine, p.9 ↩
-
Original PDF page 10: L2 Surgery in Oral medicine, p.10 ↩
-
Original PDF page 11: L2 Surgery in Oral medicine, p.11 ↩
-
Original PDF page 12: L2 Surgery in Oral medicine, p.12 ↩
-
Original PDF page 13: L2 Surgery in Oral medicine, p.13 ↩
-
Original PDF page 14: L2 Surgery in Oral medicine, p.14 ↩
-
Original PDF page 15: L2 Surgery in Oral medicine, p.15 ↩
-
Original PDF page 16: L2 Surgery in Oral medicine, p.16 ↩
-
Original PDF page 17: L2 Surgery in Oral medicine, p.17 ↩
-
Original PDF page 18: L2 Surgery in Oral medicine, p.18 ↩
-
Original PDF page 19: L2 Surgery in Oral medicine, p.19 ↩
-
Original PDF page 20: L2 Surgery in Oral medicine, p.20 ↩
-
Original PDF page 21: L2 Surgery in Oral medicine, p.21 ↩
-
Original PDF page 22: L2 Surgery in Oral medicine, p.22 ↩
-
Original PDF page 23: L2 Surgery in Oral medicine, p.23 ↩
-
Original PDF page 24: L2 Surgery in Oral medicine, p.24 ↩
-
Original PDF page 25: L2 Surgery in Oral medicine, p.25 ↩
-
Original PDF page 26: L2 Surgery in Oral medicine, p.26 ↩
-
Original PDF page 27: L2 Surgery in Oral medicine, p.27 ↩
-
Original PDF page 28: L2 Surgery in Oral medicine, p.28 ↩
-
Original PDF page 29: L2 Surgery in Oral medicine, p.29 ↩
-
Original PDF page 30: L2 Surgery in Oral medicine, p.30 ↩
-
Original PDF page 31: L2 Surgery in Oral medicine, p.31 ↩
-
Original PDF page 32: L2 Surgery in Oral medicine, p.32 ↩
-
Original PDF page 33: L2 Surgery in Oral medicine, p.33 ↩
-
Original PDF page 34: L2 Surgery in Oral medicine, p.34 ↩
-
Original PDF page 35: L2 Surgery in Oral medicine, p.35 ↩
-
Original PDF page 36: L2 Surgery in Oral medicine, p.36 ↩
-
Original PDF page 37: L2 Surgery in Oral medicine, p.37 ↩
-
Original PDF page 38: L2 Surgery in Oral medicine, p.38 ↩
-
Original PDF page 39: L2 Surgery in Oral medicine, p.39 ↩