Cardiovascular and Respiratory Disease1
Learning Outcomes2
- Gain an understanding of an overview of cardiovascular and respiratory disease
- To recognise the oral manifestations and management of patients with these conditions
- To develop an awareness when medically compromised patients should be referred to secondary care
Hypertension
Hypertension (HTN) is a significant health concern characterized by the following:
- In adults, hypertension is defined as a sustained systolic blood pressure (BP) of 130 mm Hg or greater or a sustained diastolic BP of 80 mm Hg or greater.
The Silent Killer
Hypertension is often referred to as the "silent killer" because patients are frequently unaware of their condition until significant damage has occurred.
- Many patients with high blood pressure are unaware of their disease.
- Early detection, followed by referral for diagnosis and treatment, can be lifesaving.
Definition and Classification
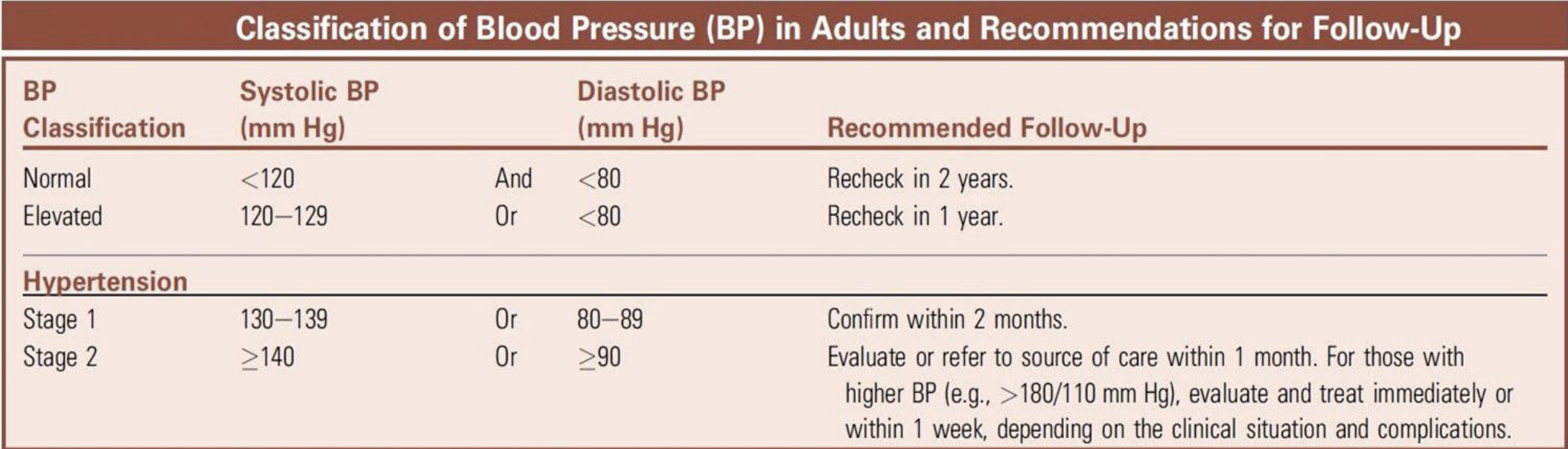
The American Cardiology Association and the American Heart Association define blood pressure in four stages. If there is a disparity between systolic and diastolic pressures, the higher value determines the stage.
Blood Pressure Classification Table3
| BP Classification | Systolic BP (mm Hg) | Diastolic BP (mm Hg) | Recommended Follow-Up |
|---|---|---|---|
| Normal | <120 | And <80 | Recheck in 2 years |
| Elevated | 120–129 | Or <80 | Recheck in 1 year |
| Hypertension Stage 1 | 130–139 | Or 80–89 | Confirm within 2 months |
| Hypertension Stage 2 | ≥140 | Or ≥90 | Evaluate or refer within 1 month. For BP >180/110 mm Hg, evaluate and treat immediately or within 1 week depending on clinical situation. |
- Hypertensive Crisis: > 180/110 mmHg (Requires immediate medical referral; no dental treatment).
Aetiology and Risk Factors
Primary (Essential) Hypertension4
- Accounts for 90% of cases.
- Patients have no readily identifiable cause.
- Risk factors include age, family history, genetic predisposition, and lifestyle factors.
- Obesity, excessive alcohol intake, smoking, high sodium diet, and physical inactivity.
Secondary Hypertension
- Accounts for 10% of cases and is secondary to underlying medical conditions.
- Causes include:
- Renal diseases (e.g., diabetic nephropathy)
- Endocrine conditions (e.g., Cushing syndrome, hyperthyroidism)
- Chronic steroid therapy
- Drug-related causes
- Obstructive sleep apnoea
Signs and Symptoms
Early Signs and Symptoms5
- Elevated blood pressure readings
- Narrowing and sclerosis of retinal arterioles
- Headache
- Dizziness
- Tinnitus
Advanced Signs and Symptoms
- Eye: Rupture and hemorrhage of retinal arterioles; papilledema
- Heart: Angina pectoris, left ventricular hypertrophy, congestive heart failure
- Kidney: Proteinuria, renal failure
- Brain: Dementia, encephalopathy, stroke
Complications of Prolonged Hypertension
Prolonged hypertension leads to several severe health consequences:
- Accelerates atherosclerosis.
- Increases the risk of cardiovascular, cerebrovascular, renal, and eye diseases, including:
- Left ventricular hypertrophy, myocardial infarction, heart failure, and stroke.
- Retinal damage, proteinuria, and renal failure.
- Malignant hypertension (BP >200/130 mmHg) causes retinal haemorrhage.
- Shortens life expectancy by 10–20 years.
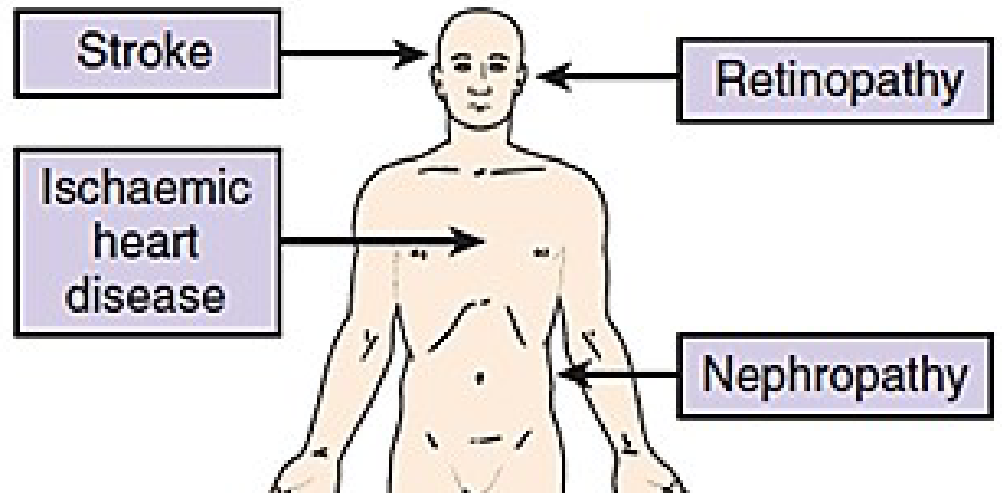
Systemic Effects6
- Stroke
- Retinopathy
- Ischaemic heart disease
- Nephropathy
Pharmacological Management7
Common classes of antihypertensive drugs include:
- Diuretics: Chlorothiazide (Diuril®)
- Angiotensin converting enzyme (ACE) inhibitors: Captopril (Capoten®)
- Angiotensin II receptor blockers: Candesartan (Atacand®)
- Calcium channel blockers: Amlodipine (Norvasc®)
- Beta-blockers: Atenolol (Tenormin®)
- Alpha-blockers: Prazosin (Minipres®)
Oral Manifestations and Side Effects8

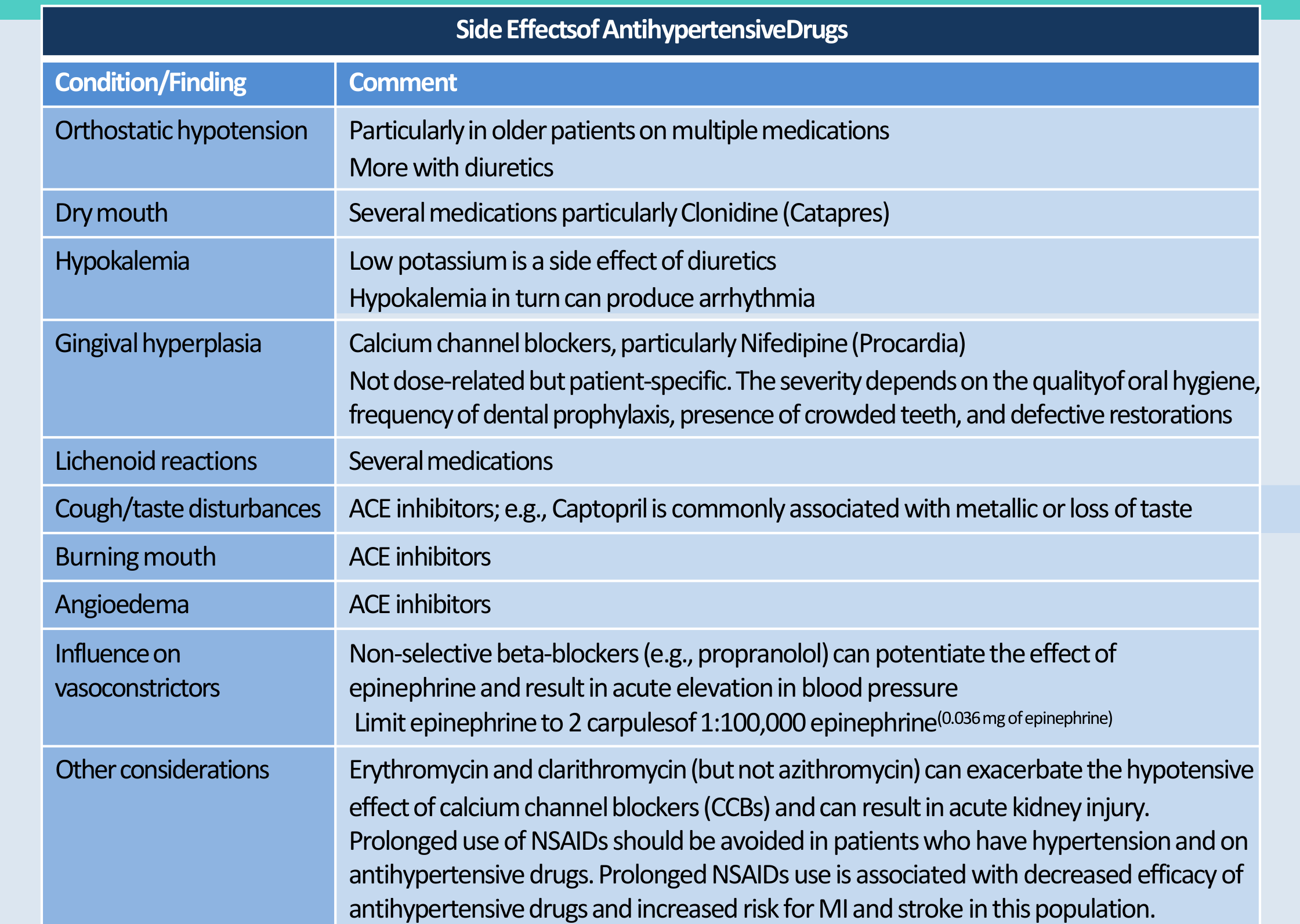
Clinical Findings and Drug Side Effects9
- Orthostatic hypotension: Particularly in older patients on multiple medications; more common with diuretics.
- Dry mouth: Associated with several medications, particularly Clonidine (Catapres).
- Hypokalemia: Low potassium is a side effect of diuretics, which can produce arrhythmia.
- Gingival hyperplasia: Associated with Calcium channel blockers, particularly Nifedipine (Procardia). It is patient-specific rather than dose-related; severity depends on oral hygiene, prophylaxis frequency, tooth crowding, and restorations.
- Lichenoid reactions: Associated with several medications
- Distinguished from idiopathic oral lichen planus..
- Cough and taste disturbances: Associated with ACE inhibitors; Captopril is commonly linked to metallic taste or loss of taste.
- Burning mouth and Angioedema: Associated with ACE inhibitors.
Drug Interactions and Precautions
- Influence on vasoconstrictors: Non-selective beta-blockers (e.g., propranolol) can potentiate epinephrine, resulting in acute BP elevation. Limit epinephrine to 2 carpules of 1:100,000 (0.036 mg).
- Antibiotic interactions: Erythromycin and clarithromycin (but not azithromycin) can exacerbate the hypotensive effect of calcium channel blockers (CCBs) and may result in acute kidney injury.
- NSAID use: Prolonged use should be avoided as it decreases the efficacy of antihypertensive drugs and increases the risk for MI and stroke in this population.
While there are no recognized primary oral manifestations of hypertension itself, antihypertensive medications can cause several secondary conditions:
- Dry mouth (e.g., clonidine)
- Gingival hyperplasia (e.g., calcium channel blockers)
- Lichenoid reactions
- Erythema multiforme
- Angioedema
- Burning mouth (e.g., ACE inhibitors)
- Parotid gland swelling (sialadenosis)
Dental Management Considerations for Hypertension
Patient Evaluation and Consultation10
- Review medical history and assess the severity of hypertension.
- Obtain a medical consultation if the patient has poorly controlled BP.
- Check BP before surgical treatments.
Management of Oral Side Effects
- Dry mouth: Improve oral hygiene, provide dietary counselling, recommend sugarless candy/gum, artificial saliva, or fluoride application
- Artificial saliva (methylcellulose)..
- Drug-induced gingival hyperplasia: Perform scaling and root planning, increase frequency of dental prophylaxis, and provide oral hygiene instructions. Consult with a physician regarding the possibility of changing the medication.
- Lichenoid reactions: Consult with a physician to replace the medication if possible.
Key Points for Hypertension11
- Hypertension is often undiagnosed or poorly controlled and frequently accompanied by co-morbidities.
- BP should be routinely assessed in the dental office along with signs, symptoms, and co-morbidities.
- BP may be elevated due to dental anxiety and pain but can be reduced with appropriate measures.
- Routine dental care is safe for most patients when anxiety and pain are controlled.
- Local anesthesia with 1:100,000 epinephrine should be limited to two carpules or fewer.
- Dental treatment must be deferred if BP is >180/110; these patients require immediate medical referral.
- Antihypertensive drugs are associated with hyposalivation, xerostomia, dental caries, and fungal infections.
Ischemic Heart Disease
Ischemic Heart Disease (IHD), also known as Coronary Artery Disease (CAD), is a condition marked by a progressive decrease in the blood supply (ischemia) to the heart muscles.
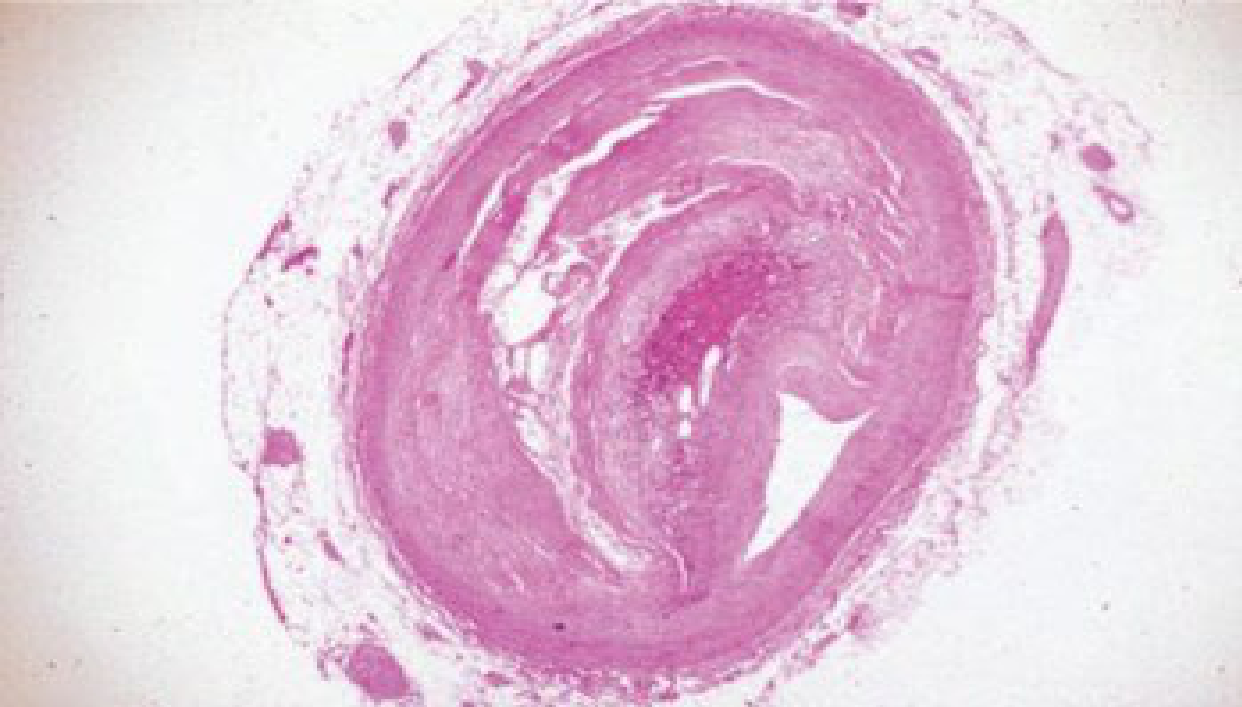
Pathophysiology and Outcomes12
- The primary cause is plaque accumulation (atherosclerosis) in the coronary artery wall.
- IHD can lead to clinical complications such as angina pectoris, myocardial infarction (MI), or sudden cardiac death.
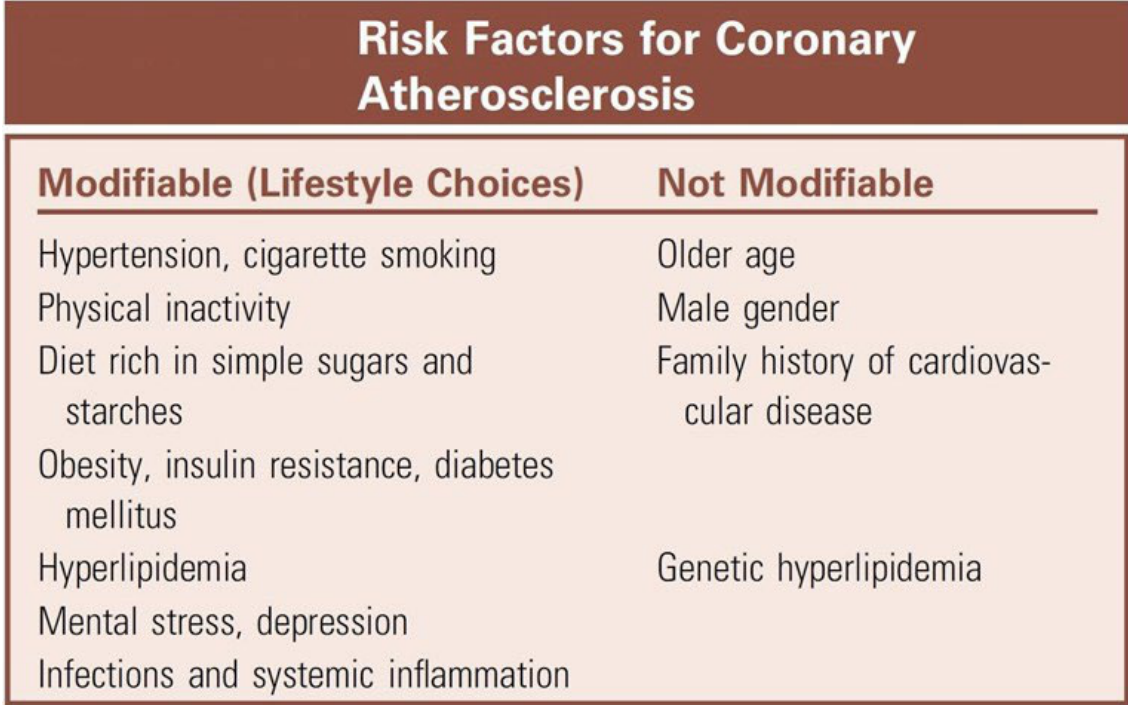 |  |
Risk Factors for Coronary Atherosclerosis
Modifiable (Lifestyle Choices)
- Hypertension
- Cigarette smoking
- Physical inactivity
- Diet rich in simple sugars and starches
- Obesity, insulin resistance, and diabetes mellitus
- Hyperlipidemia
- Mental stress and depression
- Infections and systemic inflammation
Non-Modifiable
- Older age
- Male gender
- Family history of cardiovascular disease
- Genetic hyperlipidemia
Clinical Presentation of Ischemic Heart Disease
Symptomatic Presentation13
- Chest pain or discomfort (angina)
- Weakness
- Shortness of breath
- Lightheadedness
- Nausea
- Cold sweat
 |  |
 |
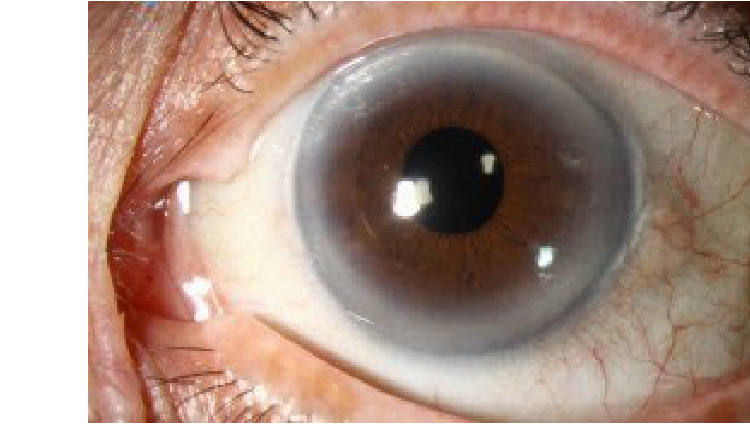
Clinical Warning Signs
- Corneal arcus
- Corneal Arcus: A whitish/bluish ring around the iris (linked to high cholesterol).
- Eyelid xanthomas
- Eyelid Xanthomas: Yellowish cholesterol deposits.
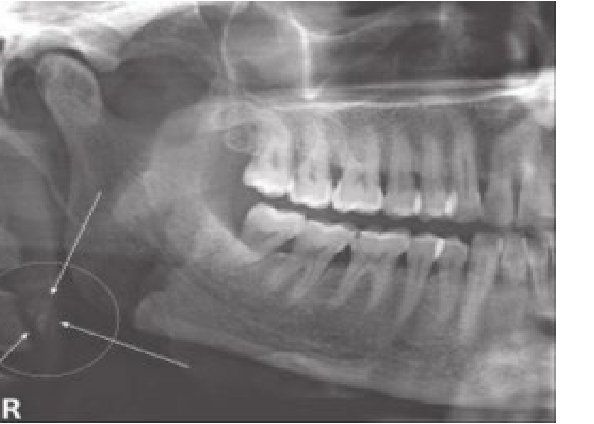
- Carotid artery calcifications: These may be visible on panoramic radiographs, typically located in the areas of the C3 and C4 vertebrae.
Dental Management of Ischemic Heart Disease
Patient Assessment14
- Determine the severity, onset, and specific symptoms of the patient’s Ischemic Heart Disease.
Treatment Protocols by Stability
- Stable Patients (Stable Angina): These patients can receive routine dental care.
- Unstable Patients: This includes those with unstable angina or patients who have experienced a Myocardial Infarction (MI) within the previous 30 days.
- Elective dental care should not be provided.
- If urgent treatment is required, it must be kept minimal and conservative.
- A physician consultation is necessary to develop an appropriate treatment plan.
- These patients are best treated at a hospital-based clinic or special care facility that offers continuous vital sign monitoring.
Oral Manifestations of Ischemic Heart Disease
Direct and Radiographic Findings15
- Referred Pain: Angina is a rare cause of pain localized in the mandible, teeth, or oral tissues.
- Radiographic Indicators: Carotid calcifications can be detected on panoramic images in approximately one-third of patients with atherosclerosis.

Medication-Related Manifestations
Several drugs used to manage IHD have reported oral side effects:
- General Side Effects: Dry mouth, taste changes, lichenoid lesions, and gingival hyperplasia.
- Nicorandil: Specifically associated with oral ulcers
Nicorandil Ulcers
Nicorandil can cause large, painful oral ulcers (often on the palate) that mimic malignancy. .
- Antiplatelet/Anticoagulant Drugs: Increased risk of bleeding may occur with medications such as aspirin or warfarin.
Key Points for Ischemic Heart Disease
Disease Progression and Risks16
- Atherosclerosis and IHD may be either asymptomatic or symptomatic.
- Features suggestive of the disease may be identified on panoramic dental images.
- Patients with atherosclerosis are at risk for angina, MI, and stroke before, during, or after dental treatment.
Clinical Management Strategies
- Adverse outcomes during dental treatment can be reduced by managing blood pressure, anxiety, and pain, and by limiting the amount of local anesthetic containing epinephrine.
- Routine dental care must be deferred for patients who have had an MI within the last 30 days, as well as those who are unstable or symptomatic.
Provider Responsibilities
- Dental providers must be aware of potential drug interactions in patients with IHD and avoid prescribing medications that may cause adverse reactions.
- Patients with IHD must be evaluated by their physician on a regular basis.
Infective Endocarditis
Infective endocarditis (IE) is a serious condition characterized by the following:
Pathophysiology and Etiology17
- Infection caused by microbes that settle on the endothelial surface of the heart valves.
- Primary causative agents include Staphylococci aureus and viridans group streptococci (alpha-haemolytic streptococci).
- The condition occurs near congenital or acquired cardiac defects.
- It results when microbes enter the bloodstream and colonize damaged or artificial cardiac valves.
Clinical Significance and Risk Factors
- Associated with significant morbidity and mortality.
- Most IE cases related to oral microflora are attributed to random bacteraemia resulting from routine daily activities.
- Daily activities contributing to random bacteremia include brushing and chewing.
- A very small number of cases are believed to result specifically from dental procedures.
Signs and Symptoms of Infective Endocarditis
Signs and symptoms typically appear within 2 weeks after the initiating bacteraemia.
Common Clinical Findings18
- Fever: The most common sign of infection.
- Heart Murmurs: Present in 85% of patients.
 |  |
 |  |
Immune-Complex Mediated Manifestations
These conditions involve vasculitis, arthritis, and renal damage:
- Petechiae: Found on the skin, conjunctiva, and oral mucosa.
- Osler nodes: Tender red nodules located on the pulp of fingers.
- Janeway lesions: Painless red haemorrhagic macules on the palms and soles.
- Splinter haemorrhages: Dark-red linear lesions found in the nail beds.
- Roth spots: Oval retinal haemorrhages characterized by small clear centres.
- Glomerulonephritis: Inflammation of the kidney filters.
Antibiotic Prophylaxis Regimens
Administration Guidelines19
- Antibiotic prophylaxis should be administered in a single dose 30–60 minutes before the procedure.
- If not administered before the procedure, the dosage may be administered up to 2 hours after the procedure.
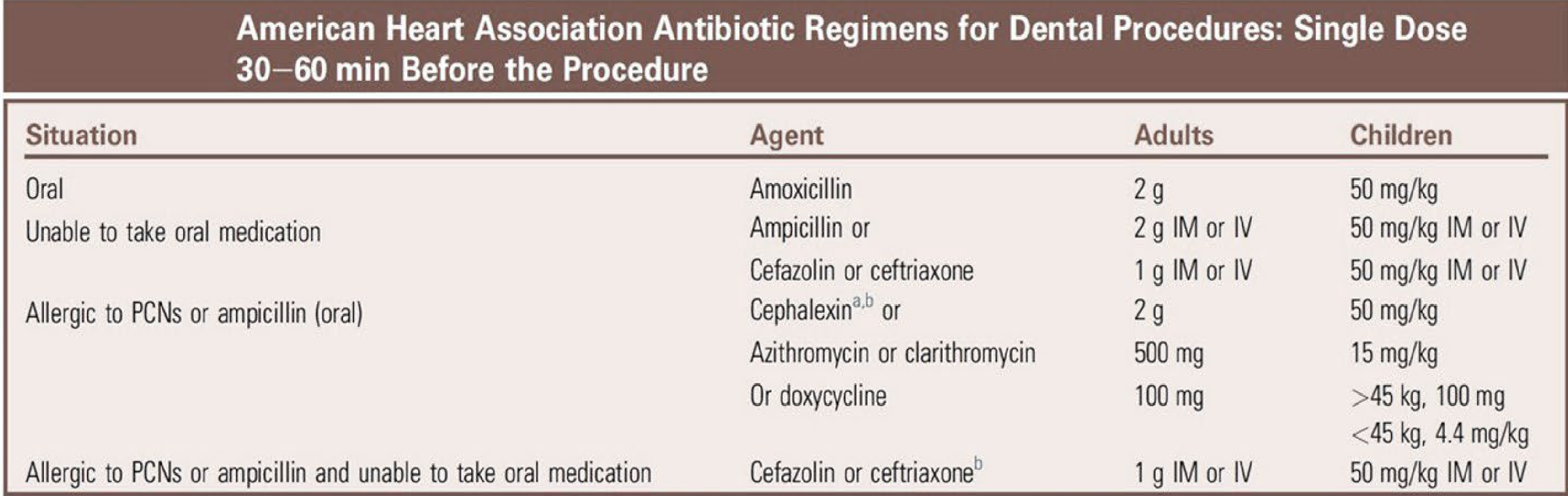
American Heart Association Antibiotic Regimens for Dental Procedures
| Situation | Agent | Adults | Children |
|---|---|---|---|
| Oral | Amoxicillin | 2 g | 50 mg/kg |
| Unable to take oral medication | Ampicillin OR Cefazolin OR Ceftriaxone | 2 g IM or IV | 50 mg/kg IM or IV |
| Allergic to Penicillins or Ampicillin (Oral) | Cephalexin* OR Azithromycin OR Clarithromycin OR Doxycycline | 2 g (Cephalexin/Azithromycin/Clarithromycin) OR 100 mg (Doxycycline) | 50 mg/kg (Cephalexin/Azithromycin/Clarithromycin) OR 15 mg/kg (Clarithromycin) OR >45 kg: 100 mg; <45 kg: 4.4 mg/kg (Doxycycline) |
| Allergic to Penicillins or Ampicillin AND unable to take oral medication | Cefazolin OR Ceftriaxone* | 1 g IM or IV | 50 mg/kg IM or IV |
Important Considerations
- *Or other first- or second-generation oral cephalosporin in equivalent adult or pediatric dosing.
- *Cephalosporins should not be used in an individual with a history of anaphylaxis, angioedema, or urticaria with penicillin or ampicillin.
- Clindamycin is no longer recommended for antibiotic prophylaxis for dental procedures.
Abbreviations: IM, Intramuscular; IV, intravenous; PCN, penicillin.
Key Points for Infective Endocarditis
Disease Overview20
- IE is associated with significant morbidity and mortality.
- IE results when microbes enter the bloodstream and colonize damaged or artificial valves.
- Viridans group streptococci (VGS) in the oral cavity can cause IE because of transient bacteraemia from daily mouth activities and, less commonly, after dental procedures.
Prevention and Clinical Responsibility
- Good oral health and regular dental care are important to prevent VGS IE.
- AHA guidelines recommend antibiotic prophylaxis based on three risk factors:
- Underlying cardiac conditions.
- The specific dental procedure being performed.
- Oral microbes (VGS) likely to cause bacteraemia.
- Dental providers must be aware of and follow recommended guidelines for antibiotic prophylaxis.
Guideline Variations
Dental providers should be aware of differences between international guidelines, such as the American Heart Association (AHA) versus the British Heart Association, when determining prophylaxis based on patient risk and procedure invasiveness.
Asthma21
Respiratory Diseases
Classification and Triggers
Asthma is a chronic inflammatory disease of the airways marked by reversible episodes of enhanced airway hyperresponsiveness, resulting in recurrent bouts of dyspnea, coughing, and wheezing. It is a multifactorial and heterogeneous disease.
Categories of Exacerbation Factors22
Factors that can exacerbate asthma are grouped into one of four categories:
- Extrinsic (allergic or atopic)
- Intrinsic (idiosyncratic, non-allergic or non-atopic)
- Drug induced
- Exercise induced
Allergic or Extrinsic Asthma23
- The most common form; accounts for 35% of all adult cases.
- Triggered by inhaled seasonal allergens such as pollens, dust, house mites, animal dander, and irritating fumes (seasonal variations).
- Usually seen in children and young adults.
- Patients frequently have a well-defined allergy history, high IgE levels upon allergen exposure, positive skin tests to numerous allergens, and a family history of allergic conditions.
- When exposed to an allergen, several inflammatory mediators are secreted resulting in:
- Bronchial smooth muscle contraction (bronchoconstriction) and spasm (bronchospasm)
- Increased vascular permeability
- Tissue oedema
- Mucous secretion
Intrinsic Asthma24
- Accounts for about 30% of asthma cases and seldom is associated with a family history of allergy or with a known cause.
- Most common in middle-aged adults (adult onset, over the age of 30).
- Patients often have normal IgE levels, negative skin testing, and no history of allergies.
- Onset is linked to endogenous factors like emotional stress or GERD.
- Patients are more likely to develop status asthmaticus.
- Note: Some patients may have both extrinsic and intrinsic asthma.
Drug-Induced Asthma25
- Triggered by drugs such as aspirin, NSAIDs, beta-blockers, ACE inhibitors, and metabisulphite preservatives.
- Aspirin causes bronchoconstriction in 10% of asthma patients; aspirin sensitivity affects 30% of asthmatic patients.
- Metabisulphite preservatives are found in epinephrine-containing local anaesthetics.
Exercise-Induced Asthma
- Triggered by physical exertion.
Infection-Related Asthma
- Caused or triggered by respiratory infections.
- Controlled by antimicrobial treatment (bacterial) and supportive care (viral).
Clinical Presentation and Complications
Clinical Symptoms26
- Recurrent episodes of wheezing, dyspnea, cough, and chest tightness.
- Symptoms are frequently worse at night, early morning, or after exposure to a stimulus.
- Onset is abrupt, with the peak of symptoms happening within 10-15 minutes.
- Most episodes are self-limiting; severe attacks need medical attention.
- Favourable prognosis when diagnosed in childhood; condition often resolves spontaneously after puberty.
Complications
- Acute asthmatic attacks can happen in the dental office; usually self-limiting or respond to an inhaler.
Status Asthmaticus
- Serious manifestation of asthma; potentially fatal.
- Severe and prolonged attack that persists for hours despite therapy.
- Characterized by increased and progressive dyspnea, jugular venous pulsation, cyanosis, and pulsus paradoxus (fall in systolic pressure with inspiration).
Diagnosis of Asthma
Diagnosis is based on clinical symptoms and response to therapy.
Spirometry27
- Widely applied in diagnosing asthma and considered the single best test.
- Performed before and after administration of a short-acting bronchodilator.
- If pulmonary function improves more than 12% following administration, this is supportive of the diagnosis.
Other Diagnostic Tools
- Bronchial provocation (by histamine or methacholine chloride challenge)
- Allergy blood and skin tests
- Cell counts (to detect neutrophilia or eosinophilia)
- Chest radiographs (to exclude other lung diseases)
Oral Findings in Asthma
Dry Mouth28
- β2-agonists and anticholinergics can cause dry mouth.

Oral Candidiasis
- Occurs in 5% of patients who use inhalation steroids for long periods at high dose or frequency.
- Presents as pseudomembranous (white patches) or erythematous candidiasis.
- Condition is rare if a “spacer” or aerosol-holding chamber is used and the mouth is rinsed with water after each use.
Angina Bullosa Haemorrhagica
- Related to the use of corticosteroid inhalers and trauma.
- Presents as blood-filled blisters on the palate.
Enamel Erosion
- β-agonists and theophylline can exacerbate GORD (GERD), which contributes to erosion of enamel.
- Erosion typically affects the palatal surfaces of the teeth.
Dental Management of Asthma Patients29
- Take a thorough history to determine the severity and stability of the disease.
- Ask about the type of asthma, adherence to medication, precipitating factors, timing, frequency, and severity of attacks.
- Remind the patient to bring their rescue inhaler to the appointment.
- Encourage smokers to stop smoking.
- Obtain medical consultation if asthma is poorly controlled (e.g., wheezing, coughing, or recent hospitalization).
- For severe and unstable asthma, consult with the patient’s physician; routine dental treatment should be postponed.
Prevention of Acute Asthmatic Attacks
Anxiety Management
- Provide a stress-free environment through the establishment of rapport and openness to reduce the risk of anxiety-induced asthma attacks.
- If sedation is required, use of nitrous oxide-oxygen inhalation sedation or small doses of a short-acting benzodiazepine (oral diazepam) (or both) is recommended.
- Avoid barbiturates and narcotics because they can provoke asthmatic attacks in some patients (histamine-releasing drugs) and can depress respiration.
Anaesthesia
- Epinephrine-containing local anesthetics are generally not contraindicated.
- Sodium metabisulfite preservative may elicit asthmatic attacks in susceptible individuals.
Antibiotics
- Avoid prescribing macrolide antibiotics (e.g., erythromycin, azithromycin) or ciprofloxacin to patients who are taking theophylline, as they can raise blood levels.
Analgesics
- The administration of aspirin to patients with asthma is not advisable because it can provoke asthma attacks in some patients.
- Avoid aspirin and other NSAIDs in susceptible individuals.
Medication Adherence and Prophylaxis
- Make sure that the patient has taken their most recent scheduled dose of medication.
- Check the availability of the rescue inhaler; use it prophylactically in moderate to severe disease.
- For patients on systemic steroids, provide corticosteroid on the morning of a surgical procedure.
Environmental and Procedural Measures
- Patients who have nocturnal asthma should be scheduled for late-morning appointments, when attacks are less likely.
- Keep away materials with irritating odors (e.g., surface disinfectants, methyl methacrylate, fissure sealants).
- Use a dental dam to reduce exposure to irritating particles like tooth-enamel dust and prophy paste.
- Non-latex gloves and dental dams should be used for latex-sensitive patients.
- Cold-temperature clinics and surgical rooms should be avoided.
- Patients who experience respiratory discomfort when fully reclined should be treated in a semi-supine position.
Chronic Obstructive Pulmonary Disease
Chronic obstructive pulmonary disease (COPD) is a general term for pulmonary disorders characterized by chronic and progressive air flow limitation that is irreversible. It is primarily linked to exposure to harmful environmental stimuli, most notably cigarette smoke.
Primary Disease Classifications30
- Chronic Bronchitis: Defined as a condition associated with chronic inflammation of the bronchi that produces excessive tracheobronchial mucous production.
- Emphysema: Defined as a permanent enlargement of the air spaces in the lung (distal to the terminal bronchioles) followed by the destruction of the air space (alveolar) walls.

Aetiology and Pathogenesis of COPD
Etiological Factors31
- Tobacco smoking is the most important cause of COPD; approximately one in five chronic smokers develops the condition.
- Long-term exposure to occupational and environmental pollutants.
- Hereditary absence or deficiency of alpha-1 antitrypsin.
Pathogenesis
Chronic exposure to cigarette smoke leads to:
- Persistent inflammation.
- Narrowing of small airways.
- Damage to the alveolar walls.
- Airflow limitation and obstruction.
Clinical Presentation of COPD
Symptoms of COPD typically develop slowly and include a chronic cough with sputum (more frequent in chronic bronchitis) and dyspnoea that is persistent, progressive, or worsens with exercise.
Clinical Phenotypes32
- Blue Bloaters (Chronic Bronchitis): Patients are often sedentary, overweight, cyanotic, oedematous, and breathless.
- Pink Puffers (Emphysema): Patients exhibit enlarged chest walls (barrel-chested appearance), weight loss, and severe exertional dyspnoea.
Many patients with COPD may exhibit features of both diseases simultaneously.
Oral Manifestations of COPD
Smoking-Related Manifestations33
- Halitosis
- Extrinsic tooth stains
- Nicotine stomatitis
- Periodontal disease
- Cancerous and precancerous lesions
 |  |
 |
Drug-Related Manifestations
- Dry mouth (xerostomia)
- Dental caries
- Oral candidiasis
Dental Management of COPD Patients
Patient Assessment and History34
- Assess the severity of the respiratory disease and the degree of control.
- Take a thorough history and review systems to determine onset, stage, symptoms, medications, and coexisting conditions (e.g., hypertension, congestive cardiac failure, respiratory infections).
- Assess vital signs including blood pressure, pulse, and respiratory rate.
- Determine smoking status and advise smokers to cease smoking.
- Remind the patient to bring their short-acting inhaler to every dental appointment.
Medical Consultation and Stability
Obtain a medical consultation if the condition is undiagnosed (indicated by a history of smoking, coughing, exertional dyspnoea, cyanosis, or frequent respiratory infections).
- Unstable Patient: Characterized by shortness of breath at rest, productive cough, upper respiratory infection (URI), or oxygen saturation less than 91%.
- Stable Patient: Characterized by no dyspnoea, oxygen saturation greater than 95%, and no active URI.
Clinical Precautions and Contraindications35
- Positioning: If orthopnoea is present, treat the patient in a semi-supine or upright chair position.
- Local Anaesthesia: Limit epinephrine if significant cardiovascular disease is present. Avoid bilateral mandibular blocks, as they can cause an unpleasant sensation of airway constriction.
- Equipment: Avoid the use of rubber dams in patients with severe disease or those who are mouth-breathers.
- Pharmacological Considerations:
- Avoid macrolide antibiotics (they reduce the metabolism of theophylline).
- Avoid narcotics and barbiturates (they depress respiration).
- Use anticholinergics and antihistamines with caution due to drying properties and increased mucous tenacity.
- Sedation and General Anaesthesia:
- If sedation is required, low-dose oral diazepam may be used.
- Outpatient general anaesthesia (GA) is contraindicated for most patients with COPD.
Tuberculosis
Tuberculosis is a chronic infectious disease caused primarily by Mycobacterium tuberculosis, an acid-fast aerobic, non-motile bacillus. Transmission occurs through the inhalation of infected airborne droplets from a person with active pulmonary disease.
Disease Progression and Classification36
-
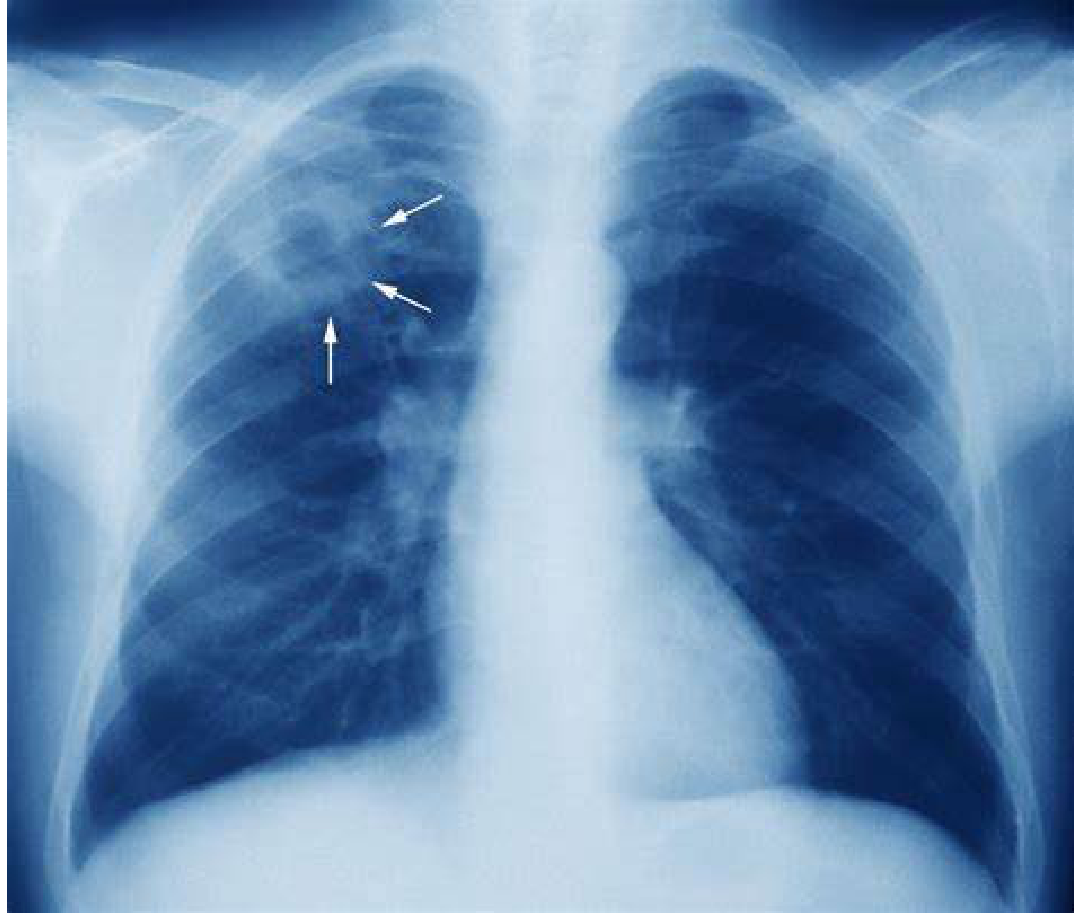
Primary TB
- The primary site of infection is the lung, with potential spread to other parts of the body.
-
Latent TB
- Develops in 90-95% of patients.
- Healed primary lesions leave a calcified nodule, which may include a hilar lymph node.
- Bacteria can remain dormant in these nodules for years.
- Patients are asymptomatic and cannot infect others.
-
Secondary TB
- Occurs when latent infections progress to active disease (5-10% of cases).
- Common in immunocompromised persons.
- HIV infection is the most significant risk factor for developing active TB.
Diagnosis of Tuberculosis
Diagnostic Testing Methods37
-
Tuberculin Skin Test (TST)
- Also known as the Mantoux test or purified protein derivative (PPD) test.
- PPD is injected under the skin of the forearm.
- After 72 hours, the circumference of induration is measured; a 15mm induration is considered positive.
-
Interferon-Gamma Release Assay (IGRA)
- A blood test used to determine exposure to M. tuberculosis.
- Can detect recent infections with results available within 24 hours.
- Cannot differentiate between latent TB and active TB.
Dental Management of Tuberculosis38
Clinical Management Protocols39
-
Patients are categorized into four infectivity groups:
- Active TB
- History of TB
- Positive TST or IGRA
- Signs or symptoms suggestive of TB
-
Consult with a physician before commencing treatment.
-
Emergency care must be provided in a hospital setting utilizing:
- Isolation protocols
- Sterilization
- Specialized ventilation
- Filtration masks (N95, N99, or N100)
-
Use rubber dams and high-speed suction during procedures to minimize the aerosolization of oropharyngeal microbes.
-
Patients are categorized into four infectivity groups:
- Active TB
- History of TB
- Positive TST or IGRA
- Signs or symptoms suggestive of TB
-
Consult with a physician before commencing treatment.
-
Emergency care must be provided in a hospital setting utilizing:
- Isolation protocols
- Sterilization
- Specialized ventilation
- Filtration masks (N95, N99, or N100)
-
Use rubber dams and high-speed suction during procedures to minimize the aerosolization of oropharyngeal microbes.
Pharmacological Side Effects
Antituberculosis Medication Interactions40
-
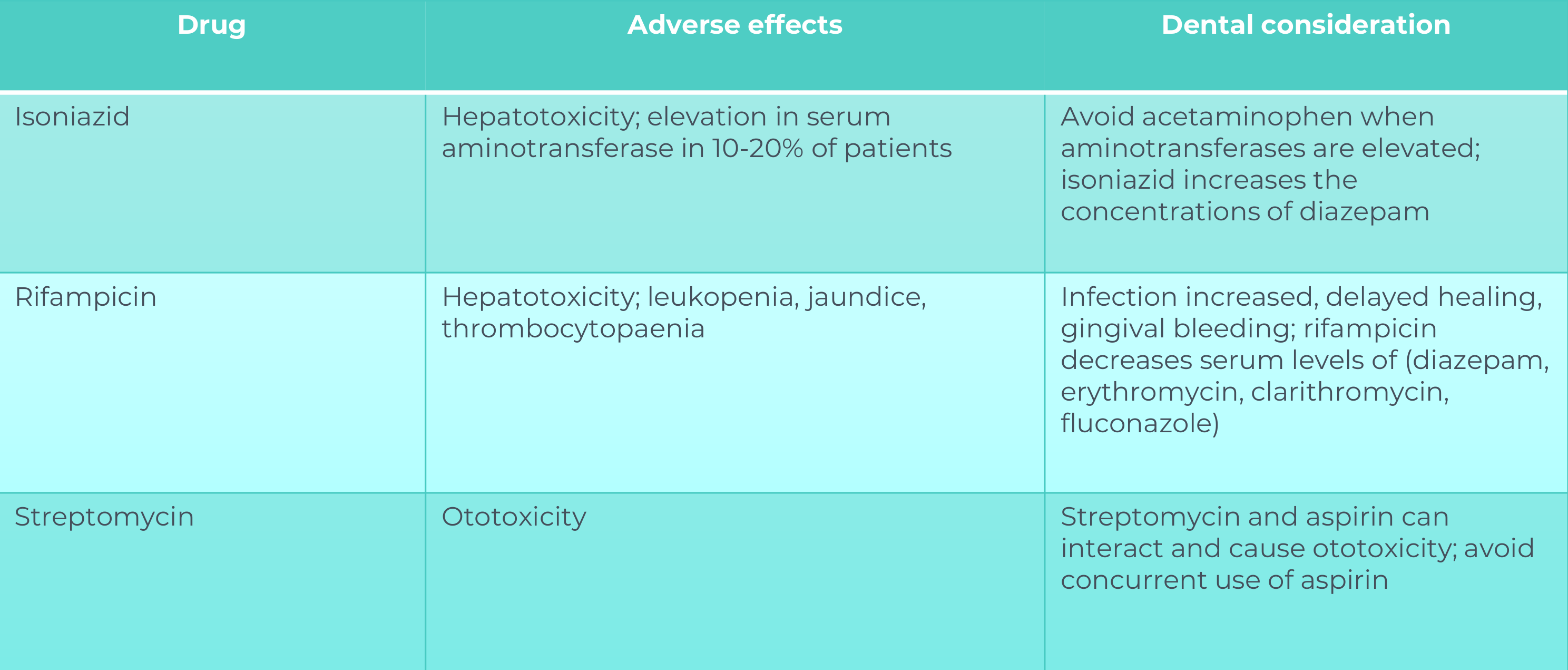
Isoniazid
- Adverse Effects: Hepatotoxicity; elevation in serum aminotransferase in 10-20% of patients.
- Dental Considerations: Avoid acetaminophen when aminotransferases are elevated. Isoniazid increases the concentrations of diazepam.
-
Rifampicin
- Adverse Effects: Hepatotoxicity, leukopenia, jaundice, and thrombocytopaenia.
- Dental Considerations: Risk of increased infection, delayed healing, and gingival bleeding. Rifampicin decreases serum levels of diazepam, erythromycin, clarithromycin, and fluconazole.
-
Streptomycin
- Adverse Effects: Ototoxicity.
- Dental Considerations: Streptomycin and aspirin can interact to cause ototoxicity; avoid concurrent use of aspirin.
Oral Findings in Tuberculosis
Clinical Presentation and Diagnosis41
-
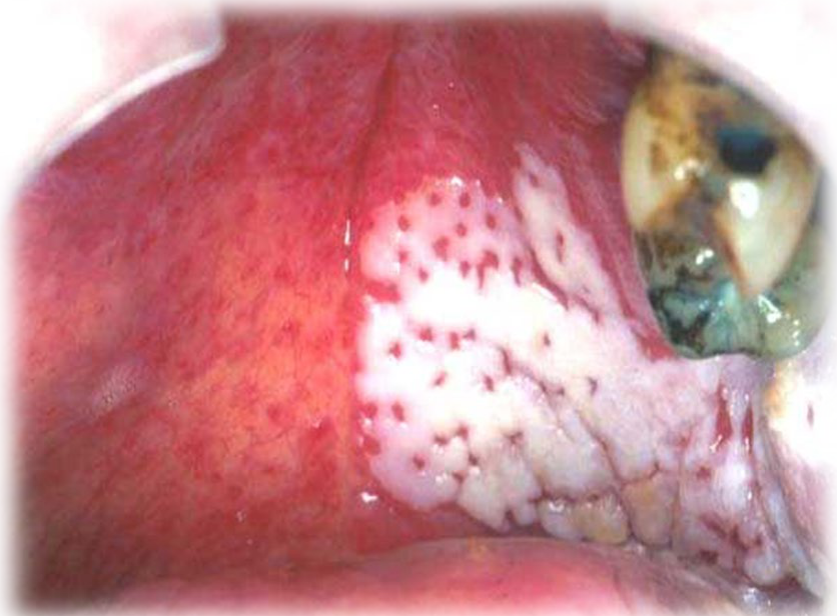
Oral Lesions
- Mouth ulceration is rare.
- When present, it typically appears as a chronic, painless, undermined ulcer on the dorsum of the tongue (may be indurated with raised margins).
- These lesions are caused by infected sputum.
- Granulating gingival lesions have also been reported.
-
Systemic and Lymphatic Involvement
- Cervical lymphadenitis.
- Sinus tracts extending from necrotic lymph nodes to the skin surface (known as a ‘collar stud’ abscess).
-
Diagnostic Identification
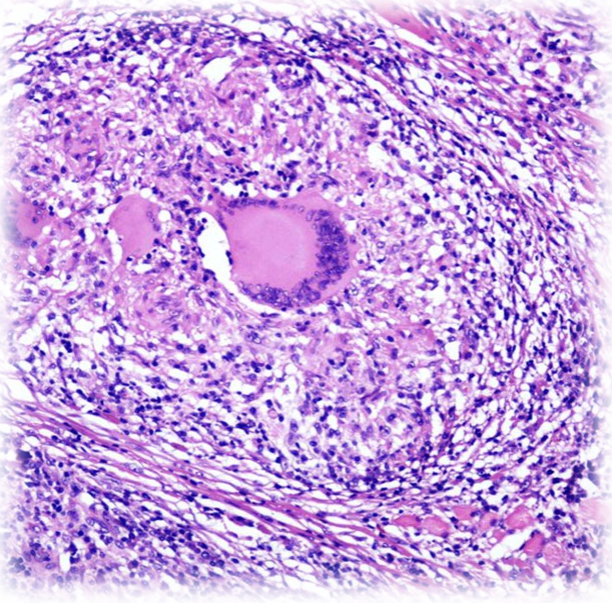
- Biopsy typically reveals caseating epithelioid granulomas.
- Identified via Ziehl-Neelsen stained sections, culture, or PCR.
-
Treatment
- Prolonged antibiotic therapy is required to clear the infection (e.g., isoniazid, rifampicin).
 |  |
 |
Cystic Fibrosis
Cystic fibrosis is an autosomal disorder characterized by the build-up of thick, viscous secretions that can damage many organs. It is caused by mutations in the cystic fibrosis transmembrane conductance regulator (CFTR) gene.
Clinical Presentation and Systemic Effects42
- Primary impact on the lungs and pancreas.
- Also affects the liver, kidneys, testicles, and salivary glands.
- End-stage lung disease is the main cause of death.
- Respiratory symptoms include difficulty in breathing and coughing up mucous.
- Other systemic signs include frequent lung infections, fatty stool, poor growth, nasal polyps, and recurrent sinusitis.
Medical Management
- Pharmacological interventions: Antibiotics, bronchodilators, and mucolytic agents.
- Respiratory support: Oxygen therapy as needed and chest physiotherapy to loosen mucous.
- Nutritional support: Diet high in protein supplemented with pancreatic enzymes and fat-soluble vitamins.
Oral Manifestations of Cystic Fibrosis
Salivary and Developmental Changes43
- Major salivary glands may enlarge.
- Hyposalivation can occur.
- Delayed dental eruption, often associated with poor systemic growth.
Hard Tissue and Oral Health Findings
- Higher incidence of enamel defects due to repeated infections.
- Increased calculus formation resulting from higher concentrations of calcium in the saliva.
- Potential predisposition to dental caries due to a combination of dry mouth and a low-fat, high-carbohydrate diet.
Dental Considerations for Cystic Fibrosis
Clinical Management and Appointment Planning44
- Treatment may be complicated by reduced respiratory function, liver disease (which may cause a bleeding tendency), and diabetes.
- Short appointments are recommended to accommodate patient limitations.
- Avoid early morning appointments due to increased mucous production during those times.
- Mucus production is highest in the morning, making early appointments particularly challenging for patient comfort and safety.
- Patients are best treated in an upright position to assist with respiratory comfort.
Pharmacological Precautions
- Antimicrobials for oral infections must be selected carefully, as these patients are often on long-term antibiotic therapy.
Pharmacological Considerations
Clinicians must be mindful of potential bleeding tendencies due to liver involvement and the implications of long-term antibiotic use on drug selection and resistance.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Tuberculosis (TB)
Infectious disease caused by Mycobacterium tuberculosis.
Disease Progression and Classification
- Latent TB: Asymptomatic, non-infectious, bacteria dormant in calcified nodules.
- Active/Secondary TB: Symptomatic and infectious; common in immunocompromised (HIV) patients.
Diagnosis of Tuberculosis
- Mantoux (PPD) Skin Test: Measured after 72 hours (>15mm is positive).
- IGRA Blood Test: Fast results but cannot distinguish latent from active TB.
Dental Management of Tuberculosis
- Protocols: Consult a physician. Active TB requires treatment in a hospital setting with isolation and high-filtration masks.
- Aerosol Control: Use rubber dams and high-speed suction.
Pharmacological Side Effects
- Isoniazid/Rifampicin: Hepatotoxicity; avoid Acetaminophen.
- Streptomycin: Ototoxicity (ear damage); avoid Aspirin.
Oral Findings in Tuberculosis
- Tuberculous Ulcer: Most common on the dorsum of the tongue; undermined, painless, mimics squamous cell carcinoma.
- Cervical Lymphadenitis: “Collar stud” abscess.
- Histology: Caseating epithelioid granulomas with Langhans giant cells.
Chronic Obstructive Pulmonary Disease (COPD)
Irreversible, progressive airflow limitation, primarily caused by smoking.
Primary Disease Classifications
- Chronic Bronchitis: Inflammation and excessive mucus.
- Emphysema: Destruction of alveolar walls and airspace enlargement.
Aetiology and Pathogenesis of COPD
- Smoking: The primary cause (1 in 5 smokers develop COPD).
- Genetics: Alpha-1 antitrypsin deficiency.
Clinical Presentation of COPD
Clinical Phenotypes
- “Blue Bloaters” (Chronic Bronchitis): Obese, cyanotic, edematous, productive cough.
- “Pink Puffers” (Emphysema): Barrel-chested, weight loss, severe dyspnea.
Oral Manifestations of COPD
Smoking-Related Manifestations
- Halitosis, tooth staining, Nicotine Stomatitis (white palate), and increased risk of periodontal disease and oral cancer (e.g., speckled leukoplakia).
Drug-Related Manifestations
- Dry mouth and oral candidiasis from inhalers.
Dental Management of COPD Patients
Patient Assessment and History
- Assess stability: Oxygen saturation < 91% is unstable; > 95% is stable.
Clinical Precautions and Contraindications
- Positioning: Upright or semi-supine.
- Avoid: Rubber dams (in severe cases), bilateral mandibular blocks, narcotics, and barbiturates.
- Anesthesia: Outpatient general anesthesia is contraindicated.
Footnotes
-
Original PDF page 1: L20 cardiovascular and respiratory disease, p.1 ↩
-
Original PDF page 2: L20 cardiovascular and respiratory disease, p.2 ↩
-
Original PDF page 3: L20 cardiovascular and respiratory disease, p.3 ↩
-
Original PDF page 4: L20 cardiovascular and respiratory disease, p.4 ↩
-
Original PDF page 5: L20 cardiovascular and respiratory disease, p.5 ↩
-
Original PDF page 6: L20 cardiovascular and respiratory disease, p.6 ↩
-
Original PDF page 7: L20 cardiovascular and respiratory disease, p.7 ↩
-
Original PDF page 9: L20 cardiovascular and respiratory disease, p.9 ↩
-
Original PDF page 8: L20 cardiovascular and respiratory disease, p.8 ↩
-
Original PDF page 10: L20 cardiovascular and respiratory disease, p.10 ↩
-
Original PDF page 11: L20 cardiovascular and respiratory disease, p.11 ↩
-
Original PDF page 12: L20 cardiovascular and respiratory disease, p.12 ↩
-
Original PDF page 13: L20 cardiovascular and respiratory disease, p.13 ↩
-
Original PDF page 14: L20 cardiovascular and respiratory disease, p.14 ↩
-
Original PDF page 15: L20 cardiovascular and respiratory disease, p.15 ↩
-
Original PDF page 16: L20 cardiovascular and respiratory disease, p.16 ↩
-
Original PDF page 17: L20 cardiovascular and respiratory disease, p.17 ↩
-
Original PDF page 18: L20 cardiovascular and respiratory disease, p.18 ↩
-
Original PDF page 19: L20 cardiovascular and respiratory disease, p.19 ↩
-
Original PDF page 20: L20 cardiovascular and respiratory disease, p.20 ↩
-
Original PDF page 21: L20 cardiovascular and respiratory disease, p.21 ↩
-
Original PDF page 22: L20 cardiovascular and respiratory disease, p.22 ↩
-
Original PDF page 23: L20 cardiovascular and respiratory disease, p.23 ↩
-
Original PDF page 24: L20 cardiovascular and respiratory disease, p.24 ↩
-
Original PDF page 25: L20 cardiovascular and respiratory disease, p.25 ↩
-
Original PDF page 26: L20 cardiovascular and respiratory disease, p.26 ↩
-
Original PDF page 27: L20 cardiovascular and respiratory disease, p.27 ↩
-
Original PDF page 28: L20 cardiovascular and respiratory disease, p.28 ↩
-
Original PDF page 29: L20 cardiovascular and respiratory disease, p.29 ↩
-
Original PDF page 33: L20 cardiovascular and respiratory disease, p.33 ↩
-
Original PDF page 34: L20 cardiovascular and respiratory disease, p.34 ↩
-
Original PDF page 35: L20 cardiovascular and respiratory disease, p.35 ↩
-
Original PDF page 36: L20 cardiovascular and respiratory disease, p.36 ↩
-
Original PDF page 37: L20 cardiovascular and respiratory disease, p.37 ↩
-
Original PDF page 38: L20 cardiovascular and respiratory disease, p.38 ↩
-
Original PDF page 39: L20 cardiovascular and respiratory disease, p.39 ↩
-
Original PDF page 40: L20 cardiovascular and respiratory disease, p.40 ↩
-
Original PDF page 42: L20 cardiovascular and respiratory disease, p.42 ↩
-
Original PDF page 41: L20 cardiovascular and respiratory disease, p.41 ↩
-
Original PDF page 43: L20 cardiovascular and respiratory disease, p.43 ↩
-
Original PDF page 44: L20 cardiovascular and respiratory disease, p.44 ↩
-
Original PDF page 45: L20 cardiovascular and respiratory disease, p.45 ↩
-
Original PDF page 46: L20 cardiovascular and respiratory disease, p.46 ↩
-
Original PDF page 47: L20 cardiovascular and respiratory disease, p.47 ↩