Gastrointestinal Diseases
Course Information1
- Institution: The University of Western Australia | Oral Health Centre of Western Australia
- Presenter: Bobby Joseph, Associate Professor
Lecture Focus
This lecture focuses on the intersection of gastroenterology and dentistry, specifically how systemic GI conditions manifest in the oral cavity.
- Year: 2026
Learning Objectives
Clinical Competencies and Knowledge2
- Develop a sound knowledge of the oral manifestations of gastrointestinal (GI) diseases.
- Understand the necessary modifications required in the treatment plan for patients presenting with these conditions.
- Gain comprehensive knowledge of the investigations and common laboratory tests available to assess the status of gastrointestinal diseases.
- Gain familiarity with investigations and lab tests used to assess disease status
- Understand the oral features associated with common GI diseases
Oral Manifestations of Gastrointestinal Tract Diseases
General Characteristics3
-
Oral lesions may occur in several gastrointestinal tract (GIT) diseases.
-
Primary oral lesions: In a few cases, these resemble the lesions found in the lower gut.
-
Secondary lesions: In almost all cases, these may be due to malabsorption and surgical resection of the gut
- Secondary lesions are often caused by deficiencies in iron, B12, or folic acid resulting from gut issues.
-
Fatty meals are also a significant predisposing factor for reflux.
Gastro-Oesophageal Reflux Disorder
Pathophysiology and Predisposing Factors
Gastro-oesophageal Reflux in Healthy Individuals4
- This term describes the backflow of acid from the stomach into the oesophagus.
Gastro-oesophageal Reflux Disorder (GORD)5
- Characterized by increased frequency and duration of reflux.
- Damage is caused to the oesophageal mucosa by the regurgitation of gastric contents.
Predisposing Factors6
Gastrointestinal Disorders
- High acidity of gastric contents
- Impaired gastro-oesophageal motility
Extra-Gastrointestinal Conditions
- Obesity
- Large meals
- Smoking
- Excessive alcohol consumption
Clinical Features and Complications
Clinical Symptoms7
- Heartburn
- Uncomfortable burning sensation behind the sternum after a meal
- Acid taste
- Epigastric pain
- Dysphagia
- Chronic cough
 |  |
 |
Complications
- Stricture
- Ulceration
- Iron deficiency anaemia
- Reflux oesophagitis
- Epithelial metaplasia (Barrett’s oesophagus)
Dental Aspects and Erosion
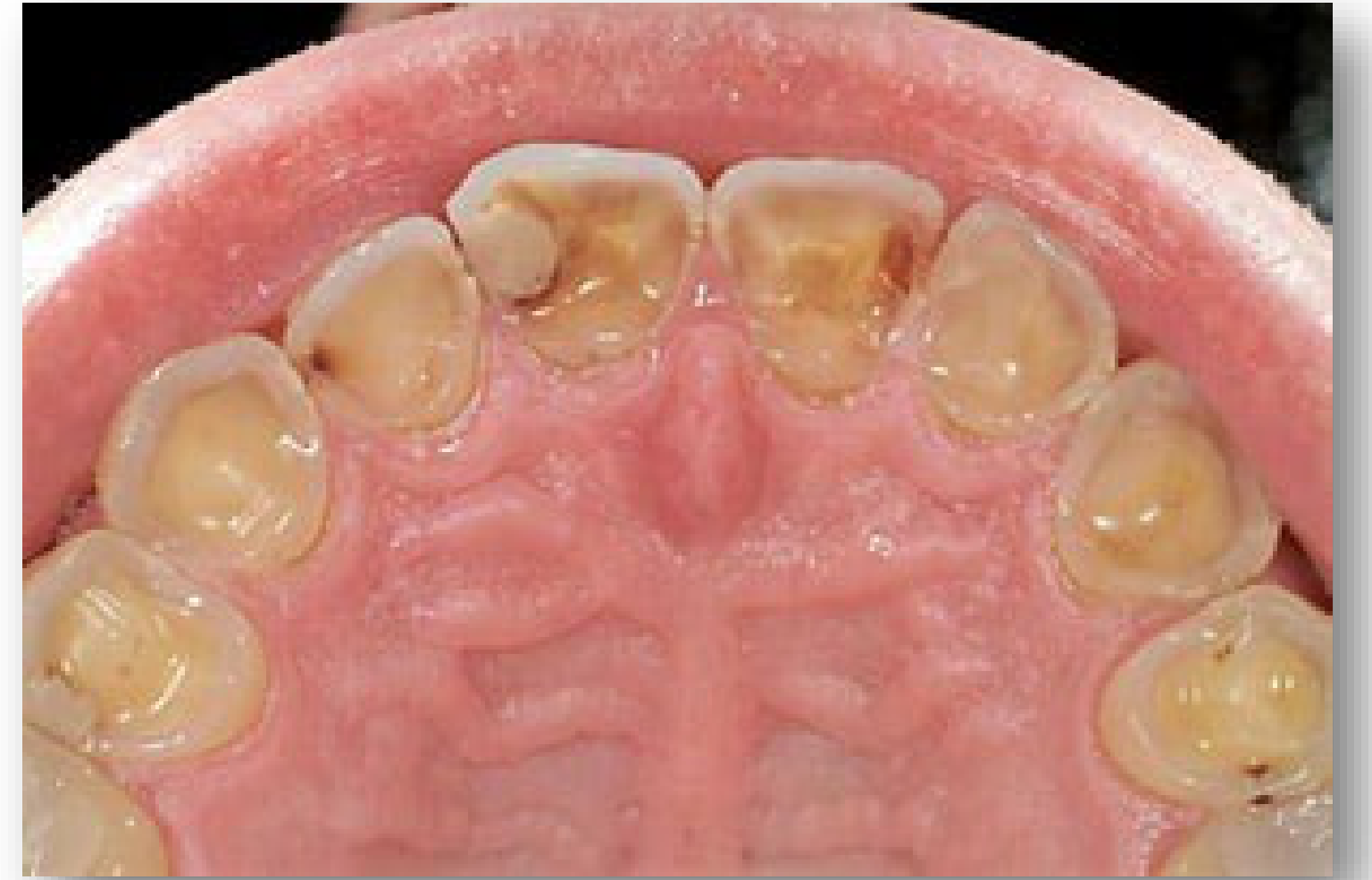
Dental Erosion and GORD8
- Gastric contents with a pH as low as 1 cause dental erosion.
- Erosion is typically seen on the palatal aspects of upper anterior teeth and premolars.
- The gastric acid is strong enough to erode enamel, which is the hardest substance in the human body.
- The condition is exacerbated if salivation is impaired.
 |  |
Clinical Assessment9
- Patients presenting with palatal dental erosion should be assessed for GORD.
- Dentists may be the first to identify GORD based on clinical signs like thin enamel and exposed dentin.
- Affected teeth are often highly sensitive to temperature and touch.
Management and Drug Therapy
Diagnosis and Lifestyle Management10
- Diagnosis: Confirmed by oesophageal pH monitoring.
- Symptom Relief:
- Losing weight
- Raising the head of the bed at night
- Frequent small meals with antacids
- Regular exercise is also recommended as part of lifestyle management.
Pharmacological Therapy
- H₂ blockers:
- Cimetidine
- Ranitidine
- Proton-pump inhibitors:
- Omeprazole
- Lansoprazole
H2 Blockers (Histamine H2 Receptor Antagonists)11
- Histamine stimulates parietal cells to release acid.
- H2 blockers stop parietal cells from responding to histamine, thereby reducing acid production.
- Examples: Cimetidine, ranitidine.
Proton Pump Inhibitors
- Reduce the amount of acid made by the stomach.
- Block a chemical system known as hydrogen-potassium adenosine triphosphatase.
- Examples: Omeprazole, lansoprazole.
Barrett Oesophagus
Characteristics of Barrett Oesophagus12
- A premalignant condition where normal squamous epithelium is replaced by metaplastic columnar epithelium.
- Occurs as a consequence of chronic gastro-oesophageal reflux.
- It is a common but often under-diagnosed entity, frequently found incidentally during endoscopy.

Pseudomembranous Colitis
Etiology and Clostridium Difficile
Pseudomembranous Colitis (Antibiotic Associated Colitis)13
- Inflammation of the colon associated with the overgrowth of Clostridium difficile.
- Overgrowth is related to recent antibiotic use.
- Pathogenesis involves the production of enzymes and toxins A and B.
- Toxins A and B specifically damage the gut lining.
Clostridium Difficile Profile14
- Gram-positive, spore-forming anaerobic rod found in soil, sand, and faeces.
- Spores are implicated in the spread of infection.
- Colonizes 2-3% of asymptomatic adults and up to 50% of the elderly.
Clinical Presentation and Risk Factors
Clinical Presentation15
- Symptoms usually begin after a few days of antibiotic therapy or up to several weeks after finishing the course.
- Abdominal cramps, pain, or tenderness.
- Presence of pus or mucus in the stool.
- Watery diarrhea (5 to 10 times per day) or bloody stools.
Risk Factors for Pseudomembranous Colitis16
- Frail elderly patients.
- Patients staying in hospitals or nursing homes.
- Patients on tube feeding.
- HIV patients.
- Increased inhalation of spores (e.g., in farm environments).
- Rarely affects infants or children.
Diagnosis and Complications
Diagnostic Procedures17
- Stool cytotoxin test (high sensitivity).
- Immunoassay for C. difficile toxin in the stool.
- Colonoscopy.
- Plain X-rays and CT scanning may be helpful.
Complications of Colitis18
- Low levels of potassium
- Dehydration
- Metabolic acidosis
- Hypotension
- Peritonitis
- Toxic megacolon: Swelling of the colon where it is incapable of expelling gas and stool, potentially causing the colon to rupture.
Management and Dental Considerations
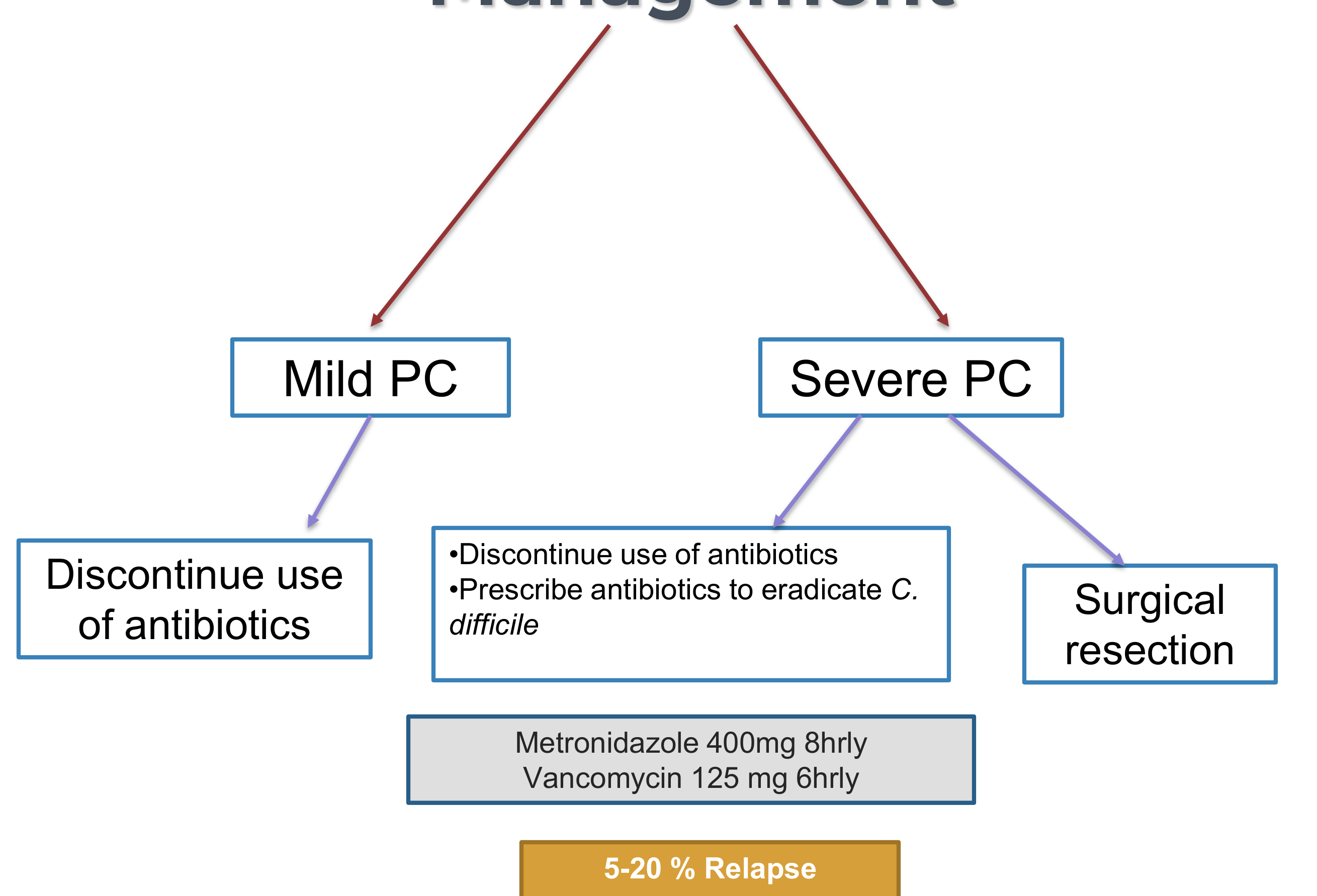
Management Protocols19
Mild Pseudomembranous Colitis
- Discontinue use of the causative antibiotics.
Severe Pseudomembranous Colitis
- Discontinue use of the causative antibiotics.
- Prescribe antibiotics to eradicate C. difficile:
- Metronidazole 400mg every 8 hours.
- Vancomycin 125mg every 6 hours.
Metronidazole Considerations
Metronidazole can cause a metallic taste and is strictly contraindicated with alcohol consumption or in patients with liver damage.
- Surgical resection may be required in extreme cases.
- Relapse occurs in 5-20% of cases.
Dental Considerations20
- Maintain knowledge of antibiotics that predispose elderly, debilitated, or previously affected patients to PC.
- PC following short-term use of Clindamycin has not been reported when used for AHA prophylactic regimens.
- No elective treatment should be performed until the resolution of PC.
- Monitor for oral candidiasis following PC therapy.
Coeliac Disease
Overview of Coeliac Disease21
- Also known as gluten-sensitive enteropathy.
- ==Also known as Gluten-Induced Enteropathy==
- ==A permanent intolerance to gliadin (found in wheat, rye, and barley)==
- Not uncommon; frequently associated with the Celtic ethnic group.
- May not be recognized if symptoms are not severe.
- A genetically determined hypersensitivity to gluten that affects the jejunum.
Clinical Features and Oral Manifestations
Clinical Features22
- Patients may appear healthy despite the disease.
- Manifestations of malabsorption are common.
- Diarrhoea, weight loss, and weakness.
- Increased risk of osteoporosis, infertility, and malignancy
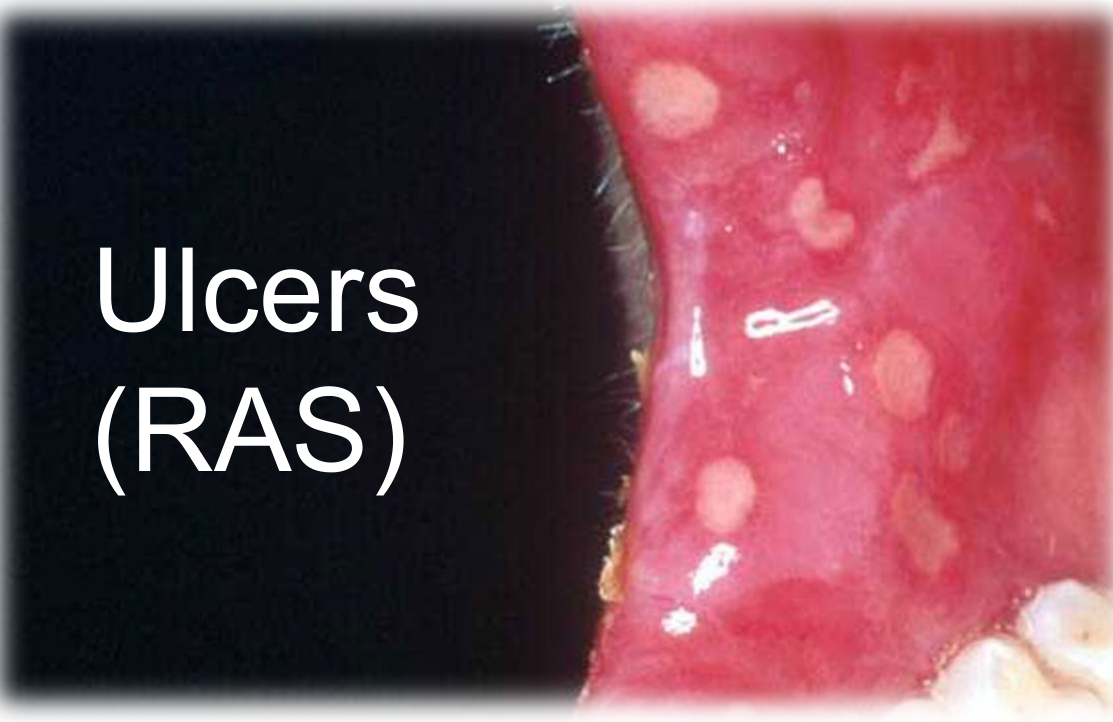
- Approximately 3% of patients with aphthae (mouth ulcers) have underlying coeliac disease.
- Ulcers are typically well-circumscribed and painful
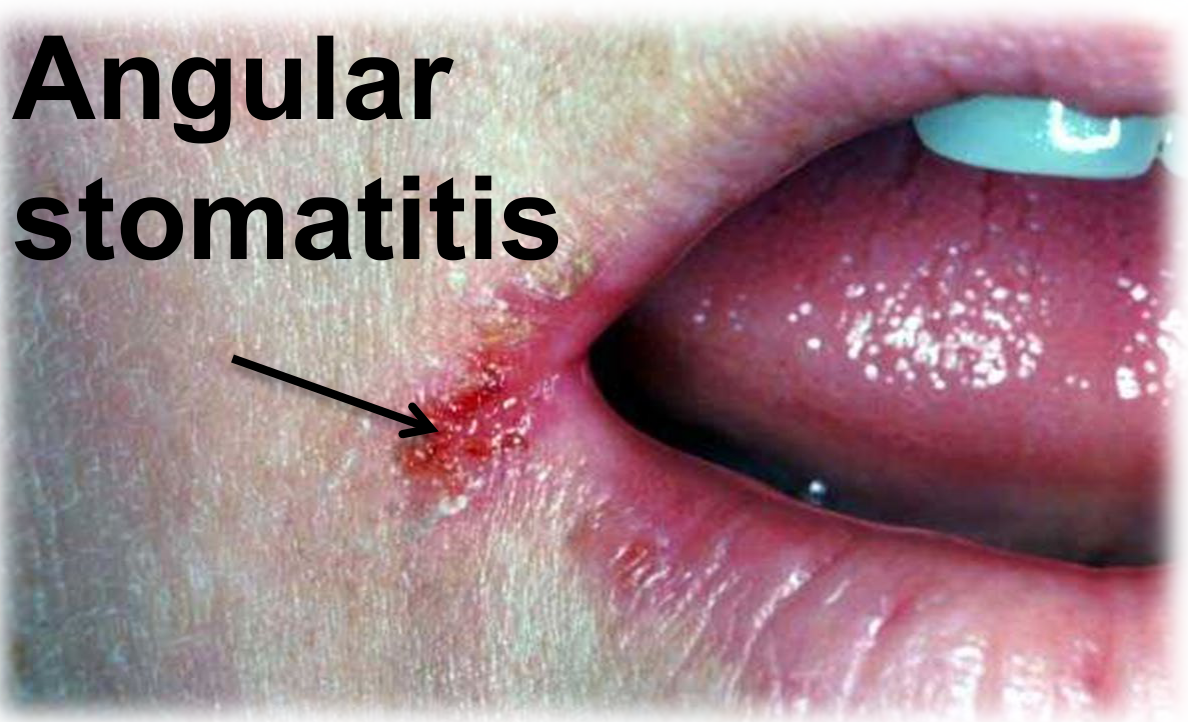
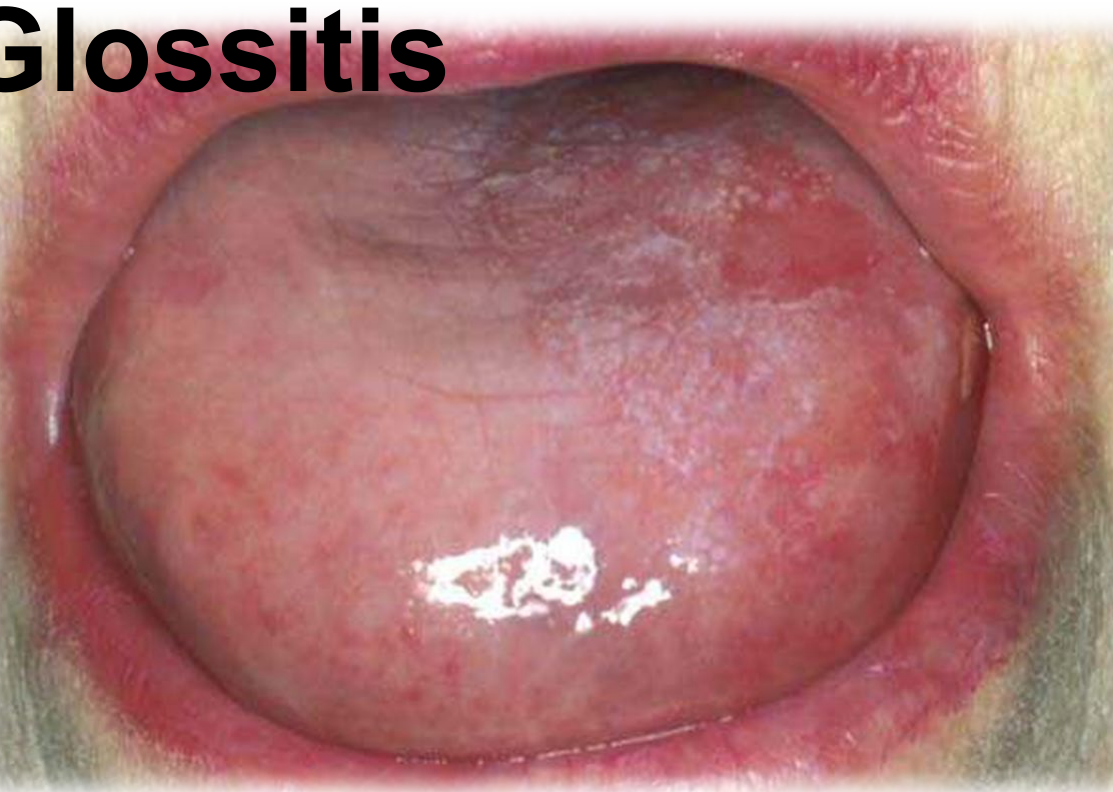
Oral Manifestations23
- Recurrent Aphthous Stomatitis (RAS) / Ulcers
- Angular stomatitis
- Glossitis
- Presents as a "bald" tongue due to atrophy of papillae from hematinic deficiencies
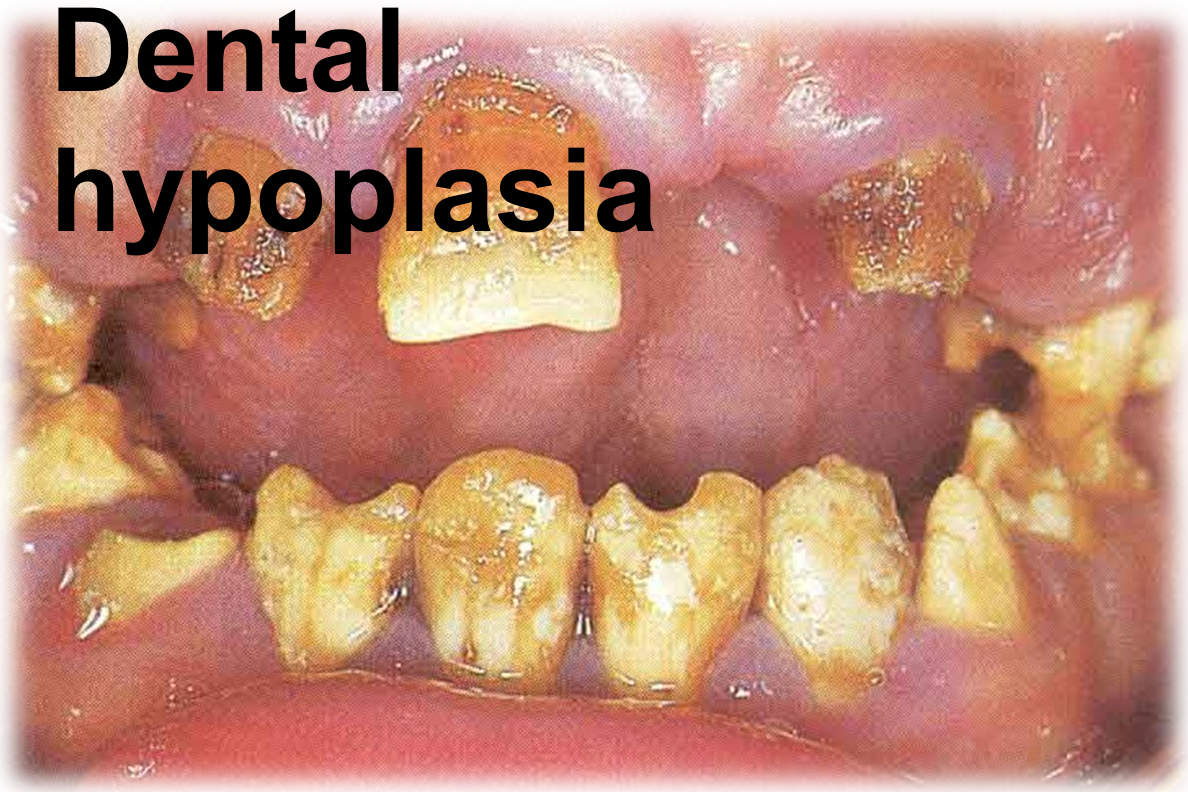
- Dental hypoplasia
- Includes enamel defects and pitting
 |  |
 |  |
Diagnosis and Management
- Specialist referral is necessary for definitive diagnosis.
- Haematological and gastrointestinal investigations are indicated.
- Testing for antibodies to gluten, reticulin, endomysin, and transglutaminase.
- Small bowel biopsy is required for confirmation.
- Management includes a strict gluten-free diet.
- Diet is curative for most, though some may still require topical corticosteroids or chlorhexidine mouthwash for persistent ulcers
- Deficiencies in Iron (Fe), folate, and Vitamin B₁₂ should be rectified.
Orofacial Granulomatosis and Crohn Disease
Orofacial Granulomatosis Syndrome
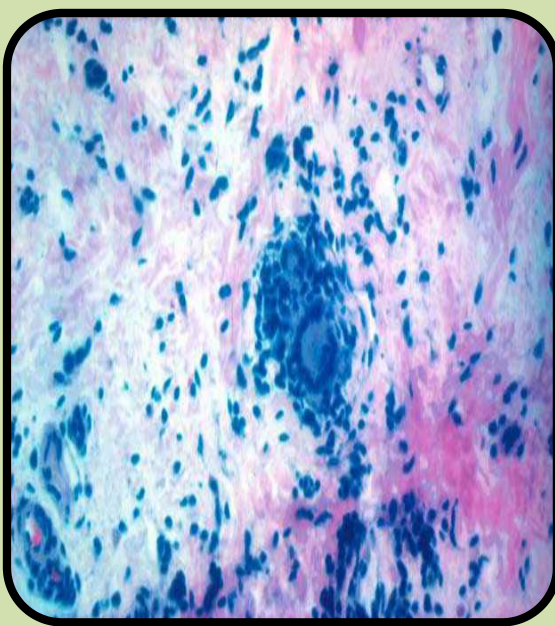
Definition and Characteristics24
- Describes a clinical syndrome presenting with swelling of the face, lips, and oral tissues.
- Histological evidence shows non-caseating granulomatous inflammation.
- Note: Caseating granulomas are characteristic of tuberculosis.
 |  |
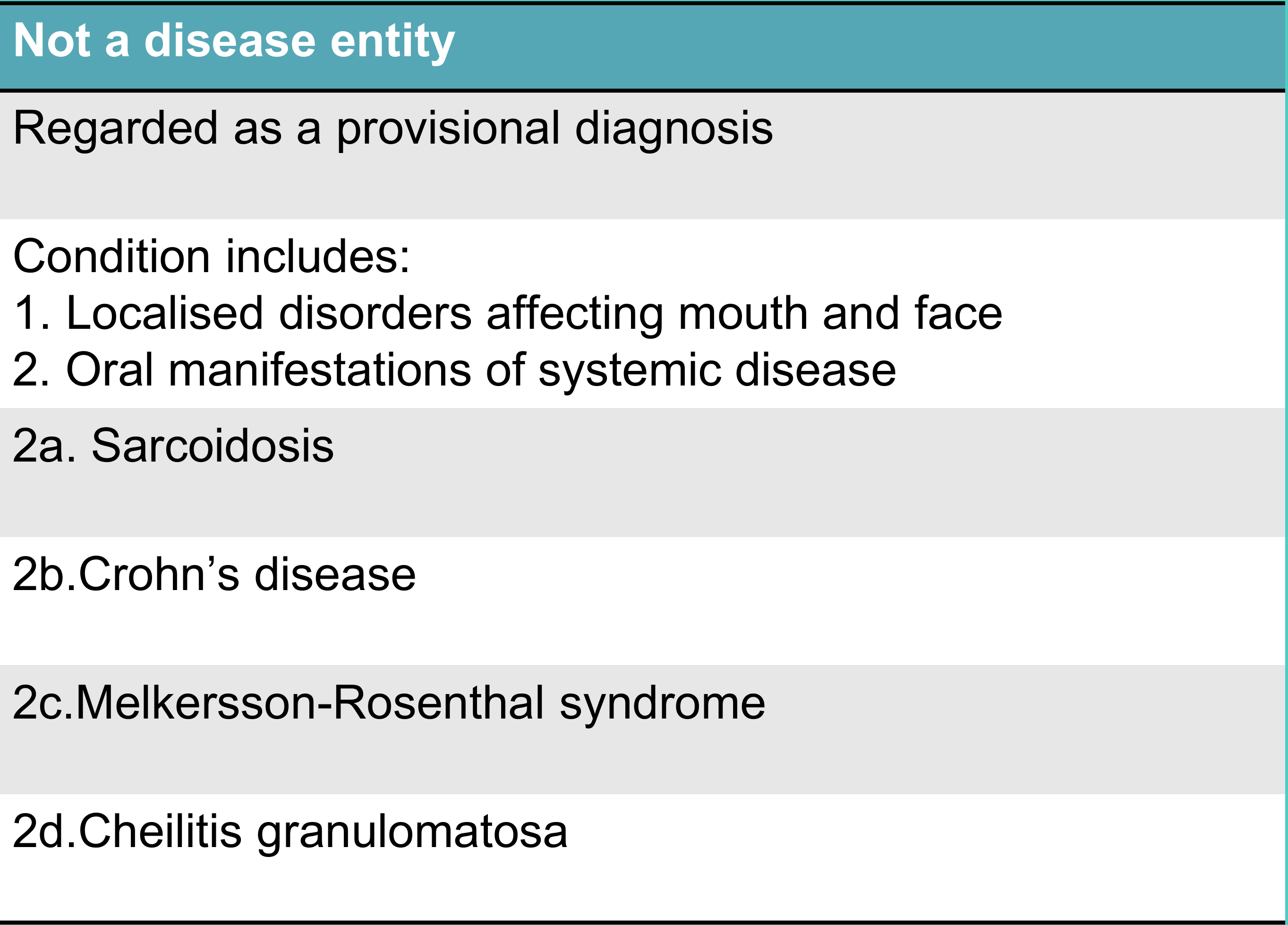
Diagnostic Classification25
- OFG is regarded as a provisional diagnosis rather than a final disease entity.
- The condition includes:
- Localised disorders affecting the mouth and face.
- Oral manifestations of systemic diseases:
- Sarcoidosis
- Crohn’s disease
- Melkersson-Rosenthal syndrome
- Cheilitis granulomatosa
Aetiology and Associations26
- The cause remains unclear; suggested causes include allergy, infection, and heredity.
- Intolerance to certain foods, flavourings, or toothpaste constituents.
- Dietary preservatives: cinnamaldehyde, cocoa, benzoates.
- Occasionally associated with dental materials.
Crohn Disease Clinical Features
Crohn Disease Overview27
- A chronic inflammatory idiopathic granulomatous disorder.
- Affects mainly the small intestine (ileum), but can affect any part of the GIT, including the mouth.
- 10% of patients with Crohn’s disease of the bowel have oral lesions.
- Oral lesions can occur in the absence of GIT involvement, presenting similarly to OFG.
Systemic Clinical Features28
- Mucosal inflammation with ulceration and fistulae formation.
- Lymph node hyperplasia leading to obstructive oedema.
- Abdominal pain and diarrhoea, often with the passage of blood and mucus.
- Extra-GI involvement: Can affect the skin, joints, liver, and bone marrow.
- Anaemia and weight loss.
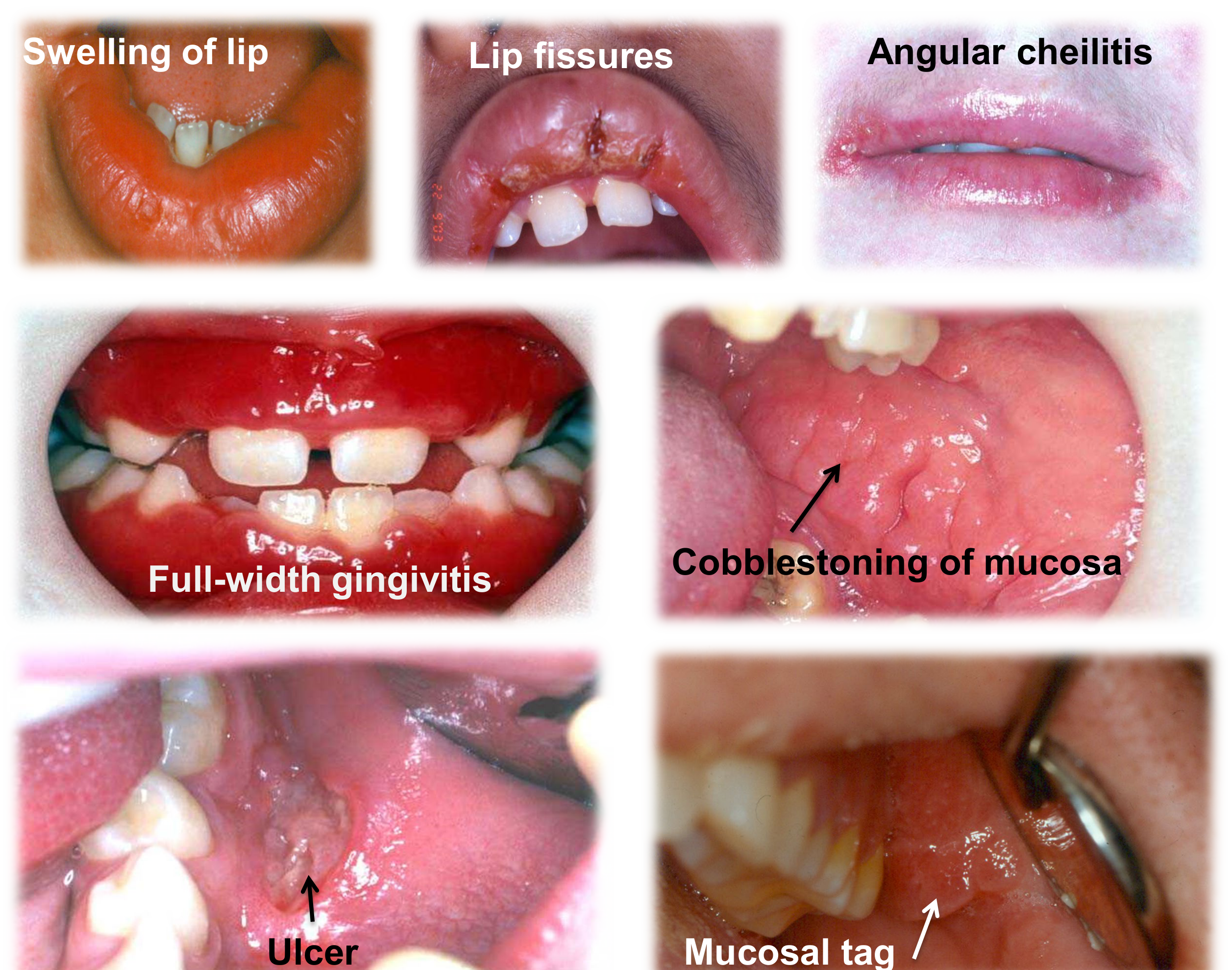
Shared Orofacial Features
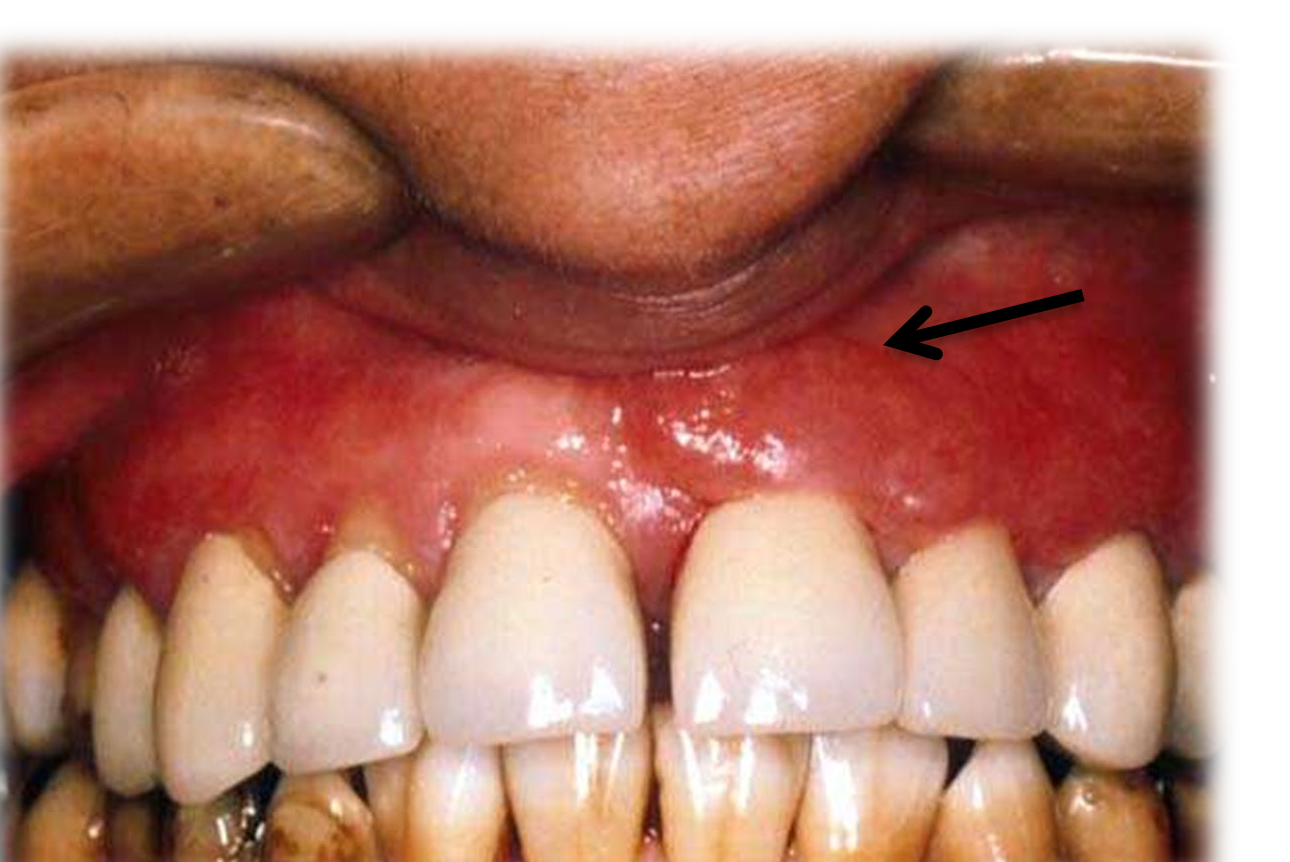
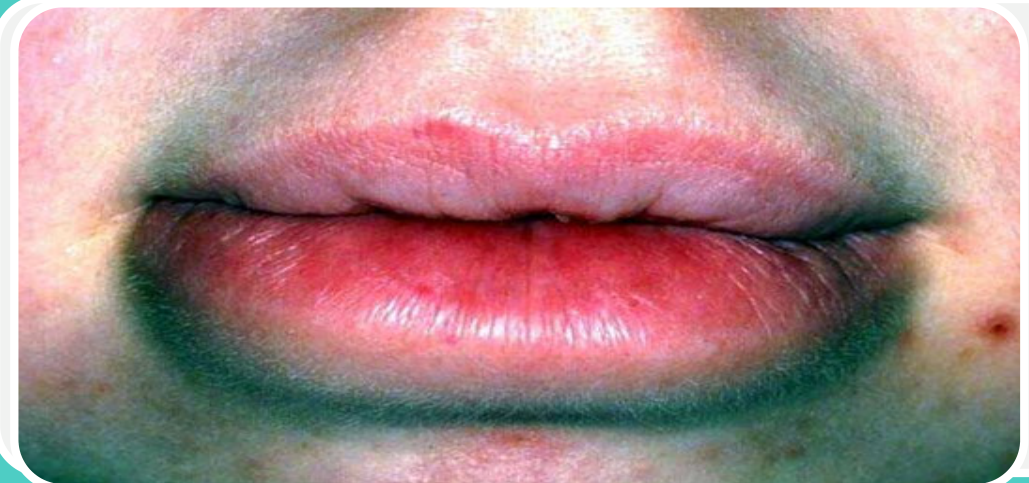
Common Orofacial Presentations of Chron’s disease and OFG29
- Swelling of the lip
- Lip fissures
- Deep cuts specifically in the midline of the lip.
- Angular cheilitis
- Cobblestoning of the mucosa
- Edematous, hyperplastic thickening of the buccal or labial mucosa.
- Full-width gingivitis
- Persistent redness and swelling of the attached gingiva.
- Ulcers
- Mucosal tags
- Polypoid-like lesions or deep folds that can mimic denture-induced irritation.
Diagnosis and Management of Crohn Disease
Diagnostic Investigations30
- Thorough investigation including screening for underlying systemic conditions.
- Oral biopsy.
- Haematological, GIT, and biochemical investigations (specifically to rule out sarcoidosis).
- Patch testing.
- Consultation with a gastroenterologist.
Biopsy Technique
A deep biopsy is required because granulomas are often located deep within the muscle; superficial biopsies may result in a false negative.
Management Strategies31
- Oral Ulcers: Treated with topical or intralesional corticosteroids, and antiseptic or analgesic mouthwashes.
- Systemic Treatment: Short courses of systemic steroids (e.g., budesonide, which has fewer side effects).
- Medication: Mesasalazine (aminosalicylates
- Biologicals and Immunosuppressants: Use of anti-TNF alpha antibodies such as Infliximab and Adalimumab.).
- Referral: Mandatory referral to a gastroenterologist.
Sarcoidosis
Systemic and Orofacial Features
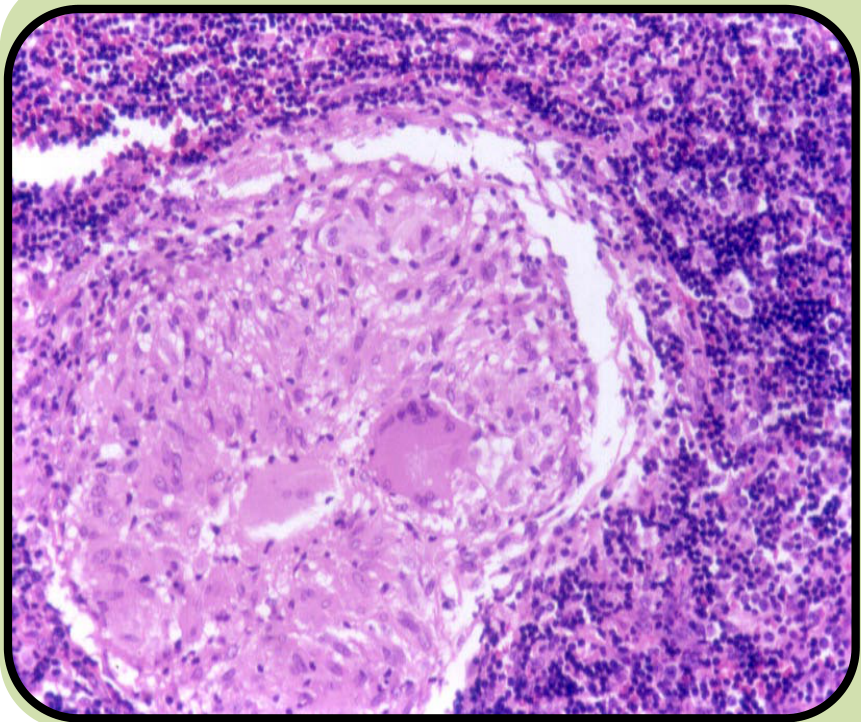
Sarcoidosis Overview32
- A multi-system granulomatous disorder of unclear aetiology.
- Frequently affects young adult females, particularly those of Afro-Caribbean descent.
- Granulomas form in the lungs, lymph nodes, salivary glands, and mouth.
- Characterized by non-caseating granulomas in the lungs and lymph nodes.
- Key features include bilateral hilar lymphadenopathy and erythema nodosum.
Orofacial Features of Sarcoidosis33
- Heerfordt’s Syndrome: Characterized by salivary and lacrimal gland swelling, facial palsy, and uveitis.
- Xerostomia (dry mouth).
- Mucosal nodules.
- Commonly found on the palate.
- Gingival swelling.
- Labial swelling.
 |  |
Management and Referral Criteria
Diagnostic Management34
- Biopsy of labial salivary glands.
- Serum angiotensin-converting enzyme (SACE) levels are typically raised.
- Positive gallium scan of lacrimal and salivary glands.
- Chest radiography to check for enlarged hilar lymph nodes.
Referral Criteria
- Suspected malignancy in the neck, including lymphoma.
- Suspected metastatic disease in the neck.
- Unexplained lymphadenopathy.
Melkersson-Rosenthal Syndrome
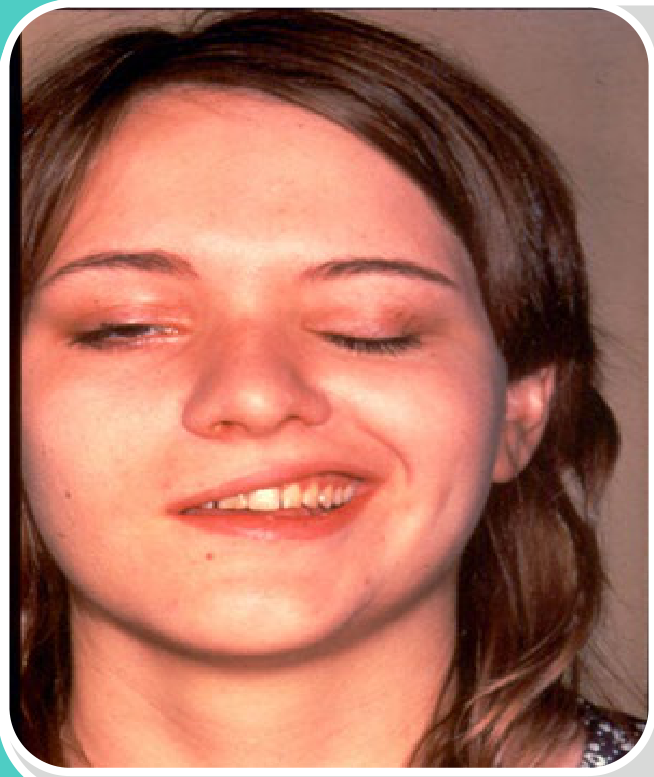
Clinical Triad35
- Lip or facial swelling
- Often presents as recurrent swelling (Orofacial Granulomatosis).
- Fissured tongue
- Lower motor neurone facial palsy
 |  |
 |
Ulcerative Colitis
Clinical Features and Complications
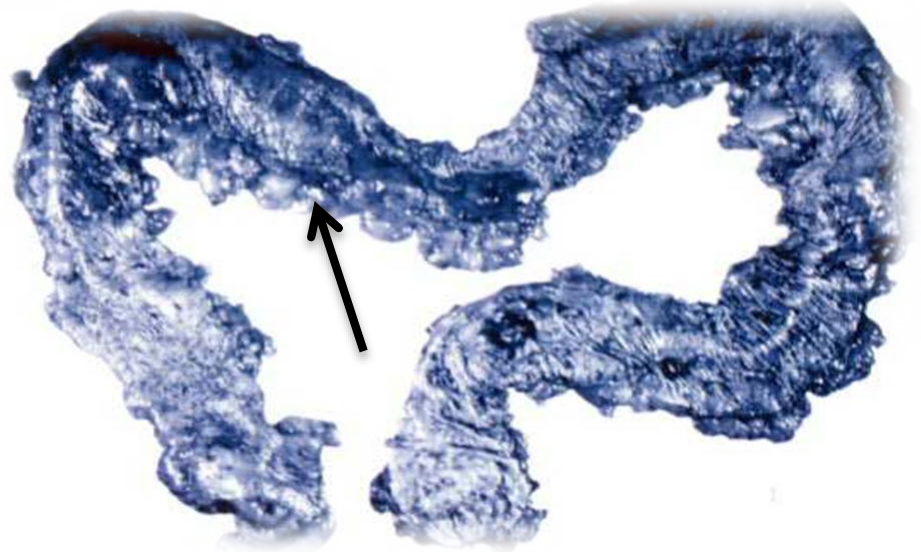
Ulcerative Colitis Overview36
- An uncommon inflammatory disease mainly affecting adults.
- Non-infectious inflammation limited to the colorectal mucosa, extending proximally from the anal margin.
- Characterized by ulcers and polyps in the colon.
- Associated with a risk of malignant change.
- Symptoms include persistent diarrhoea, passage of blood and mucus, iron deficiency anaemia, and weight loss.
Complications and Oral Manifestations37
- Systemic Complications: Widespread ulceration of the colon, haemorrhage, perforation, and malignancy.
- Oral Manifestations: Severe aphthae and candida infections
- Oral features are less common than in Crohn's disease.
- Secondary Effects: Oral lesions may be secondary to nutritional deficiencies resulting from malabsorption.

Management of Ulcerative Colitis
- Specialist referral is necessary.
- Diagnostic tests: Biopsy, Full Blood Count (FBC), and sigmoidoscopy.
- Treatment of secondary deficiencies using haematinics.
- Pharmacological treatment: Topical steroids (pessaries or enemas) and systemic sulfasalazine.
- Additional pharmacological management includes aminosalicylates and immunosuppressants.
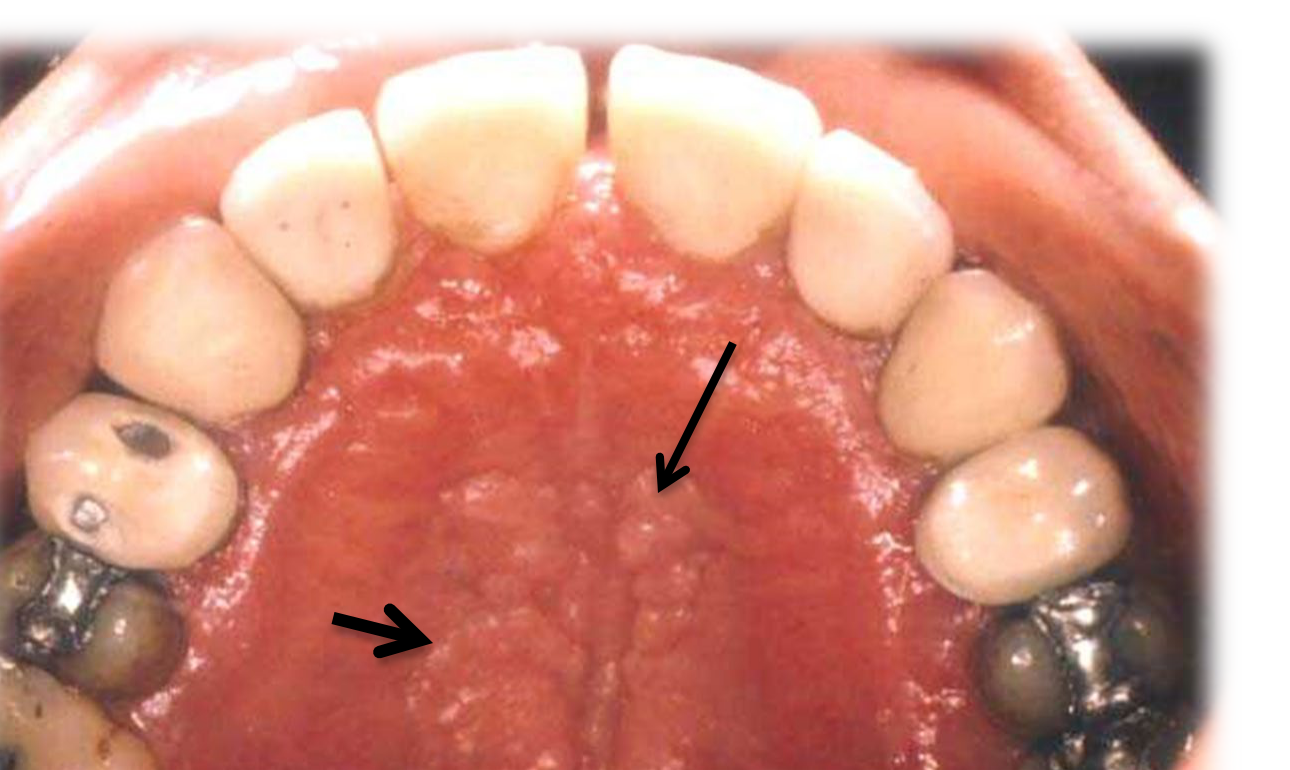
Pyostomatitis Vegetans
Clinical Presentation38
- A rare disorder where bowel symptoms typically precede oral involvement by months or years.
- Characterized by pustular lesions on the oral mucosa and gingiva.
- Vegetative outgrowths on inflamed, erythematous mucosa may also be present.
- Pustular lesions rupture to form erosions and “snail track” ulceration.

Management
- Topical steroids are often successful.
- Management of the associated Inflammatory Bowel Disease (IBD) typically leads to improvement of oral lesions.
- Systemic management of the underlying colitis is often the primary driver for resolving oral symptoms.
Diagnostic Significance39
- Pyostomatitis vegetans serves as an important oral marker for inflammatory bowel disease.
Clinical Action
Because this condition is a highly specific marker for IBD, its presence often necessitates an immediate referral for GI investigation.
 |  |
Gastrointestinal Polyposis Syndromes
Gardner Syndrome
Clinical Features of Gardner Syndrome40
- Multiple osteomas of the jaws.
- Visible on X-rays as radio-opacities
- Considered benign bone tumors
- Epidermal or sebaceous cysts of the skin.
- Multiple fibrous tumours.
- Polyposis coli: Characterized by a marked tendency to undergo malignant change.
 |  |
 |
Peutz-Jeghers Syndrome
Etiology and Systemic Features41
- An autosomal dominant inherited disorder.
- Caused by a germline mutation in the liver kinase B1 (LKB1) tumour suppressor gene.
- Associated with an increased cancer risk in adult life.
- Hamartomatous polyps develop early in life.
- Complications include abdominal pain, bleeding, anaemia, and acute intestinal obstruction.
Clinical Manifestations42
- Brown to blue-black macules (pigmentation) around the mouth, nose, and eyes.
- Pigmentation also commonly affects the oral mucosa
- Polyps primarily in the small intestine, though rare cases occur outside the GIT.
- Polyps may undergo intussusception or malignant changes.
 |  |
Footnotes
-
Original PDF page 1: L22 Gastrointestinal Diseases, p.1 ↩
-
Original PDF page 2: L22 Gastrointestinal Diseases, p.2 ↩
-
Original PDF page 3: L22 Gastrointestinal Diseases, p.3 ↩
-
Original PDF page 4: L22 Gastrointestinal Diseases, p.4 ↩
-
Original PDF page 5: L22 Gastrointestinal Diseases, p.5 ↩
-
Original PDF page 6: L22 Gastrointestinal Diseases, p.6 ↩
-
Original PDF page 7: L22 Gastrointestinal Diseases, p.7 ↩
-
Original PDF page 8: L22 Gastrointestinal Diseases, p.8 ↩
-
Original PDF page 9: L22 Gastrointestinal Diseases, p.9 ↩
-
Original PDF page 10: L22 Gastrointestinal Diseases, p.10 ↩
-
Original PDF page 11: L22 Gastrointestinal Diseases, p.11 ↩
-
Original PDF page 12: L22 Gastrointestinal Diseases, p.12 ↩
-
Original PDF page 13: L22 Gastrointestinal Diseases, p.13 ↩
-
Original PDF page 14: L22 Gastrointestinal Diseases, p.14 ↩
-
Original PDF page 15: L22 Gastrointestinal Diseases, p.15 ↩
-
Original PDF page 16: L22 Gastrointestinal Diseases, p.16 ↩
-
Original PDF page 17: L22 Gastrointestinal Diseases, p.17 ↩
-
Original PDF page 18: L22 Gastrointestinal Diseases, p.18 ↩
-
Original PDF page 19: L22 Gastrointestinal Diseases, p.19 ↩
-
Original PDF page 20: L22 Gastrointestinal Diseases, p.20 ↩
-
Original PDF page 21: L22 Gastrointestinal Diseases, p.21 ↩
-
Original PDF page 22: L22 Gastrointestinal Diseases, p.22 ↩
-
Original PDF page 23: L22 Gastrointestinal Diseases, p.23 ↩
-
Original PDF page 25: L22 Gastrointestinal Diseases, p.25 ↩
-
Original PDF page 26: L22 Gastrointestinal Diseases, p.26 ↩
-
Original PDF page 27: L22 Gastrointestinal Diseases, p.27 ↩
-
Original PDF page 28: L22 Gastrointestinal Diseases, p.28 ↩
-
Original PDF page 29: L22 Gastrointestinal Diseases, p.29 ↩
-
Original PDF page 30: L22 Gastrointestinal Diseases, p.30 ↩
-
Original PDF page 31: L22 Gastrointestinal Diseases, p.31 ↩
-
Original PDF page 32: L22 Gastrointestinal Diseases, p.32 ↩
-
Original PDF page 33: L22 Gastrointestinal Diseases, p.33 ↩
-
Original PDF page 34: L22 Gastrointestinal Diseases, p.34 ↩
-
Original PDF page 35: L22 Gastrointestinal Diseases, p.35 ↩
-
Original PDF page 36: L22 Gastrointestinal Diseases, p.36 ↩
-
Original PDF page 37: L22 Gastrointestinal Diseases, p.37 ↩
-
Original PDF page 38: L22 Gastrointestinal Diseases, p.38 ↩
-
Original PDF page 40: L22 Gastrointestinal Diseases, p.40 ↩
-
Original PDF page 41: L22 Gastrointestinal Diseases, p.41 ↩
-
Original PDF page 42: L22 Gastrointestinal Diseases, p.42 ↩
-
Original PDF page 43: L22 Gastrointestinal Diseases, p.43 ↩
-
Original PDF page 44: L22 Gastrointestinal Diseases, p.44 ↩