Implications of Liver Disease to the Oral Health Care Provider
Clinical Presentation and Professional Overview1
Dr. Guru O., an Oral Medicine Specialist, provides an overview of the clinical implications of liver disease within the context of oral health care. This presentation focuses on the systemic considerations and management strategies necessary for dental professionals treating patients with hepatic impairment.
Pathophysiology of Liver Disease
Liver disease must be viewed through a broad lens, specifically distinguishing between the pre-cirrhotic stage and cirrhosis. The liver responds to various inflammatory insults by fibrosing; when this fibrosis becomes severe, the liver is deemed cirrhotic. This condition significantly impairs function and increases the risk of hepatocellular carcinoma.
Physiology and Functions of the Liver
Homeostasis
The liver maintains homeostasis through a multitude of complex roles. When diseased, a shift in homeostasis occurs, which can manifest as systemic disease or contribute to the progression of existing oral conditions.
Storage Functions2
- Vitamins: Primarily Vitamin A, D, and B12. Lesser amounts of Vitamin K and B9 (folate) are also stored.
- Minerals: Iron (stored in the form of ferritin and hemosiderin) and copper.
- Glycogen: Storage of glucose for energy regulation.
Synthetic Functions
- Circulating Proteins: Synthesis of most plasma proteins, with the exception of gamma globulins.
- Albumin: Essential for the transport of substances like unconjugated bilirubin in the blood.
- Coagulation Factors: Production of essential clotting factors, excluding a portion of factor VIII.
- In patients with severe liver disease, bleeding risks are a primary concern for dental procedures.
- Complement System: Synthesis of components required for the innate immune response.
- Bile Formation: Production of bile necessary for digestion and absorption of fats.
- Bilirubin Processing: The liver converts heme-derived toxins into excretable bile.
Detoxification and Metabolism
- Nitrogenous Waste: Conversion of toxic ammonia into urea for excretion.
- Hormone and Drug Metabolism: Processing and inactivation of various hormones and pharmacological agents.
- The liver is the primary site for drug biotransformation. In cirrhotic patients, the "hepatic reserve" is limited, making them highly susceptible to drug-induced injury.
- Red Blood Cell (RBC) Processing: Breakdown and recycling of aged or damaged red blood cells.
- Macronutrient Metabolism: Regulation and processing of glucose, proteins, and lipids.
Surveillance and Immunity
- Reticuloendothelial System: Active participation in immune surveillance and the removal of pathogens or debris from the bloodstream.
- In advanced disease (cirrhosis with ascites), patients lose certain immune protections and become highly susceptible to conditions like bacterial peritonitis.
Pathophysiology and Classification of Liver Disease
Progression of Chronic Liver Disease
Stages of Liver Disease Progression3
-
Precirrhotic Disease: Typically spans a duration of 10–35 years
-
Hepatitis: Acute or chronic inflammation.
-
Fibrosis: The liver's scarring response to inflammation.
-
Cirrhosis: Severe fibrosis leading to impaired function.
- Compensated Cirrhosis: The liver is scarred but can still perform most functions.
- Decompensated Cirrhosis: The liver can no longer compensate, leading to instability and symptoms. .
-
Compensated Cirrhosis: Typically lasts 10–15 years.
-
Decompensated Cirrhosis: Typically lasts 3–5 years, leading eventually to liver transplantation or death.
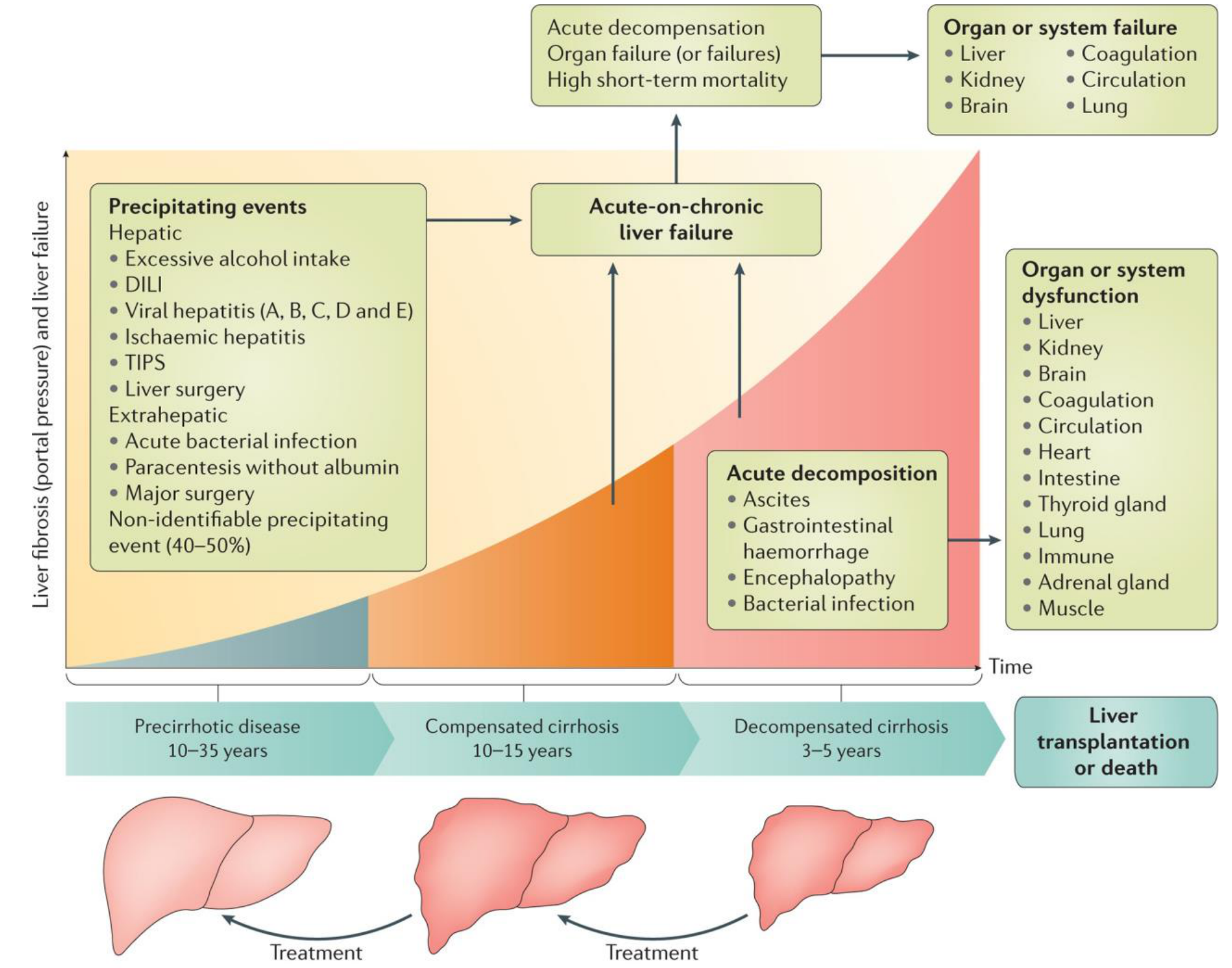
Acute Decompensation and Failure
Acute decompensation (ADC) and Acute-on-chronic liver failure (ACLF) represent severe clinical shifts characterized by:
Clinical Concern
Any further insult to the hepatocytes in a cirrhotic patient can trigger acute decompensation or systemic failure.
- Acute Decompensation (ADC): Manifests as ascites, gastrointestinal haemorrhage, encephalopathy, and bacterial infection. This leads to multi-system dysfunction affecting the liver, kidneys, brain, heart, thyroid, and immune system.
- Acute-on-chronic Liver Failure (ACLF): Characterized by organ failure (liver, coagulation, kidney, circulation, brain, or lung) and high short-term mortality
- Acute Decompensation: Organ dysfunction with a significant mortality rate.
- Acute-on-Chronic Liver Failure: Systemic failure with an even higher mortality rate.
Precipitating Events
Events that can trigger rapid decline include:
- Hepatic Factors: Excessive alcohol intake, Drug-Induced Liver Injury (DILI), viral hepatitis (A, B, C, D, and E), ischaemic hepatitis, Transjugular Intrahepatic Portosystemic Shunt (TIPS), or liver surgery.
- Extrahepatic Factors: Acute bacterial infection, major surgery, or paracentesis performed without albumin.
- Non-identifiable Events: In 40–50% of cases, the specific precipitating event remains unknown.
Etiology of Chronic Hepatitis
Chronic hepatitis is defined as any inflammatory condition of the liver lasting for six months or longer. It is classified according to its underlying aetiology.
Primary Etiological Categories4
- Metabolic: Non-alcoholic fatty liver disease (NAFLD).
- Alcohol-Induced: Liver damage resulting from chronic alcohol consumption.
- Viral Infections:
- Hepatitis B (with or without Hepatitis D co-infection).
- Hepatitis C.
- Hepatitis E (primarily observed in immunosuppressed patients).
- Drug-Induced: Chronic inflammation caused by medications such as Ketoconazole, Isoniazid, and Nitrofurantoin.
- Autoimmune: Liver disease resulting from autoimmune disorders.
- Hereditary Conditions: Wilson’s Disease and Haemochromatosis.
Unusual and Infiltrative Causes
- Infections: Syphilis, tuberculosis, and various tropical infections.
- Infiltrative Diseases: Amyloidosis and lymphoma.
- Toxins: Ingestion of environmental or chemical toxins.
Alcoholic Liver Disease
Classification of Liver Diseases5
- Alcoholic liver disease
- Nonalcoholic fatty liver disease (NAFLD)
- Viral Hepatitis
- Autoimmune hepatitis
- Drug induced hepatitis / Drug induced liver injury (DILI)
Info
Alcoholic liver disease (ALD) results from hepatocellular injury caused by alcohol consumption exceeding the liver's tolerance.
Histological Stages of Alcoholic Liver Disease
Pathological Progression6
- Alcoholic fatty liver (Steatosis)
- Characterized by fat accumulation in the liver parenchyma.
- Often asymptomatic.
- If inflammation or necrosis is present, it is termed steatohepatitis.
- Steatohepatitis
- Fat accumulation accompanied by inflammation and necrosis; also often asymptomatic.
- Alcoholic hepatitis
- Characterized by active inflammation of the liver cells.
- Symptomatic inflammation (jaundice, nausea, abdominal pain).
- Alcoholic cirrhosis
- Involves irreversible liver damage and leads to severe clinical complications.
Consumption Guidelines and Standard Drinks
NHMRC Consumption Guidelines7
One standard drink is defined as 10g of ethanol.
- General Health: No more than 10 standard drinks per week and no more than 4 standard drinks per sitting.
- Under 18s: Should not consume alcohol.
- Pregnancy/Breastfeeding: Should not consume alcohol.
Risk Thresholds for Liver Damage8
One standard drink = 10g of ethanol.
- Alcoholic Liver Disease: Can be caused by daily consumption of 30–50 grams over 5 years.
- Steatosis: 90% probability if consumption exceeds 60 grams per day.
- Cirrhosis: 30% probability if consumption exceeds 40 grams per day.
Clinical Manifestations and Physical Examination
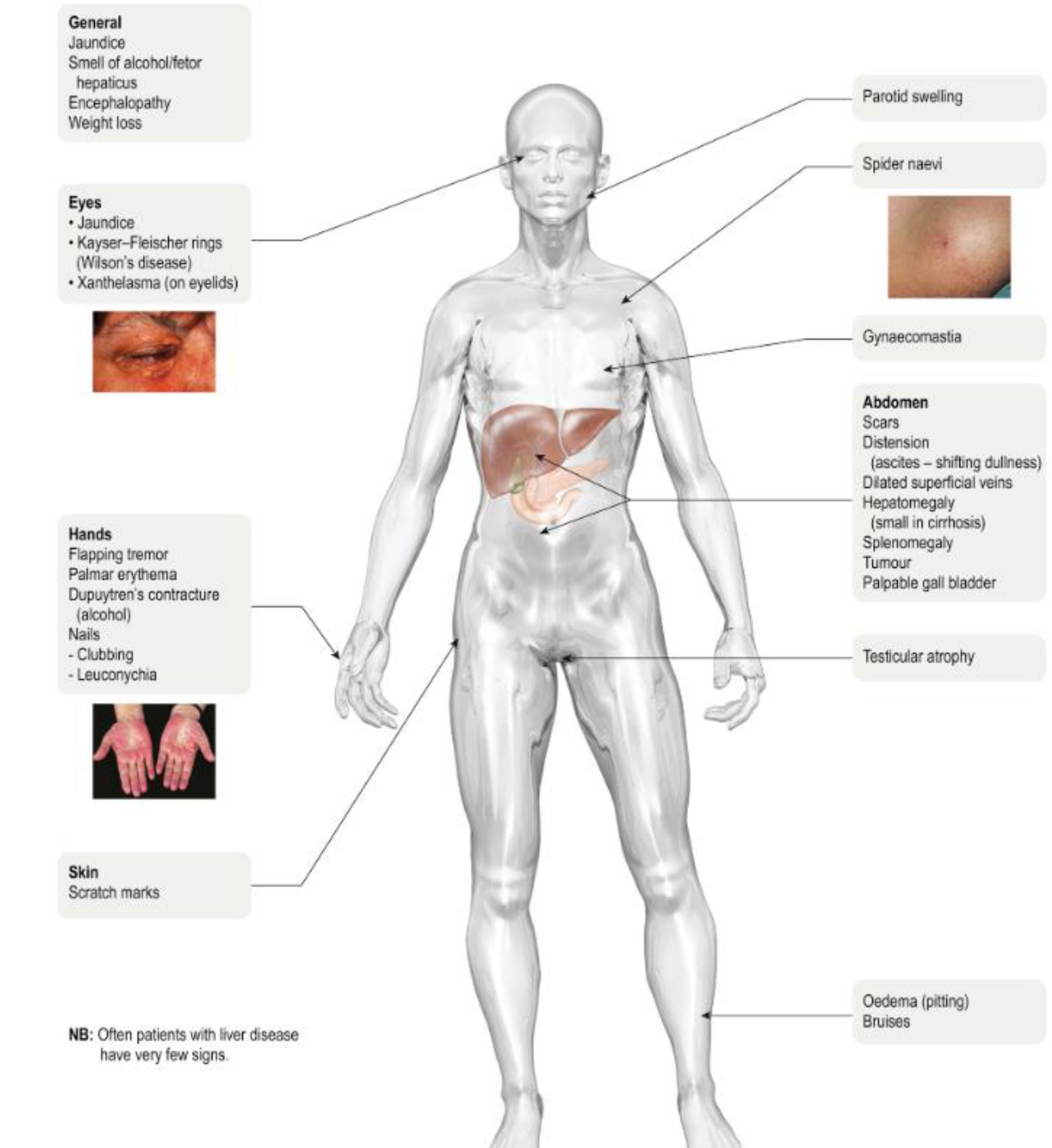
Physical Examination Findings9
Note: Patients with liver disease often present with very few clinical signs.
- General Appearance
- Jaundice
- Smell of alcohol / fetor hepaticus
- Encephalopathy
- Weight loss
- Many patients are asymptomatic; it is often a "silent disease."
- Eyes
- Jaundice
- Kayser-Fleischer rings (indicative of Wilson’s disease)
- Xanthelasma (on eyelids)
- Hands
- Flapping tremor
- Palmar erythema
- Dupuytren’s contracture
- Nails: Clubbing or Leuconychia
- Skin and Body
- Scratch marks
- Parotid swelling
- Spider naevi
- Bilateral parotid swelling is a classic sign.
- Spider naevi (spider angiomas), particularly on the bridge of the nose, face, hands, and legs.
- Bilateral parotid swelling is a classic sign.
- Gynaecomastia
- Testicular atrophy
- Pitting oedema
- Bruises
- Abdomen
- Scars
- Distension (ascites – shifting dullness)
- Dilated superficial veins
- Hepatomegaly (liver may be small in cirrhosis)
- Splenomegaly
- Tumours
- Palpable gall bladder
 |  |
 |  |
Practice Implications for Alcohol Use Disorder
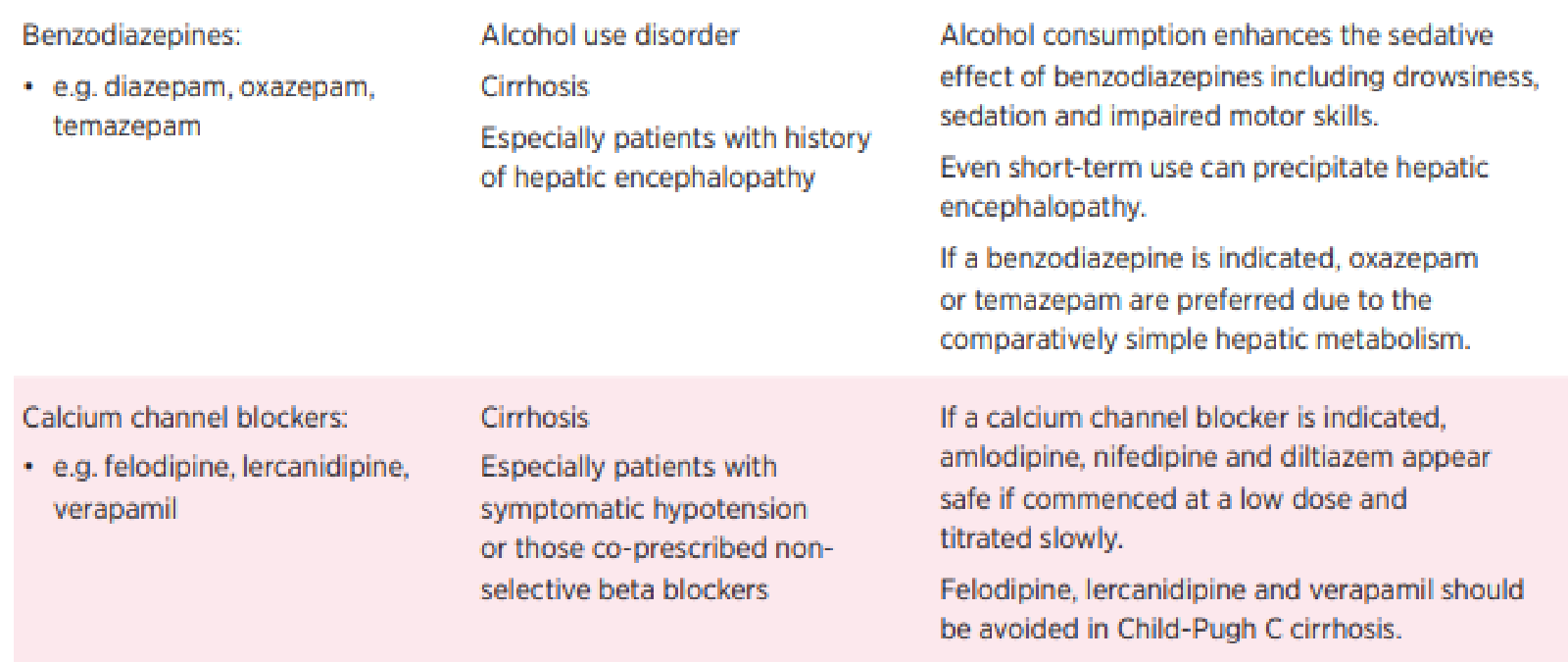
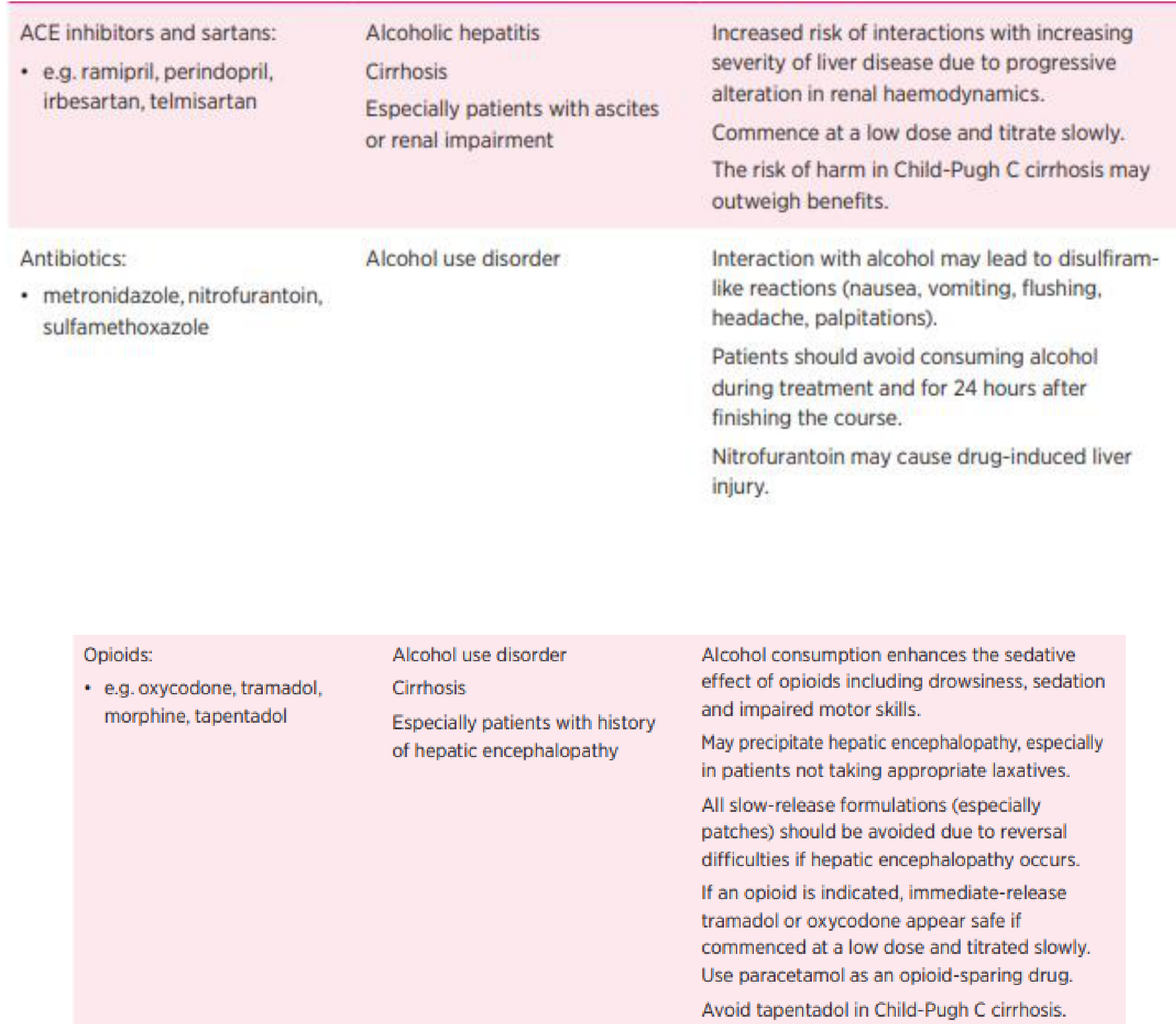
Medication Management and Interactions10
| Drug Class | Condition / Risk Group | Clinical Implications and Recommendations |
|---|---|---|
| ACE Inhibitors and Sartans (e.g., ramipril, irbesartan) | Alcoholic hepatitis, Cirrhosis, Ascites, Renal impairment | Increased interaction risk due to altered renal haemodynamics. Start at low dose and titrate slowly. Risk may outweigh benefits in Child-Pugh C cirrhosis. |
| Antibiotics (e.g., metronidazole, nitrofurantoin) | Alcohol use disorder | Risk of disulfiram-like reactions (nausea, vomiting, palpitations). Avoid alcohol during and 24 hours after treatment. Nitrofurantoin may cause drug-induced liver injury. |
| Opioids (e.g., oxycodone, tramadol, morphine) | Alcohol use disorder, Cirrhosis, Hepatic encephalopathy | Alcohol enhances sedation. May precipitate hepatic encephalopathy. Avoid slow-release formulations/patches. Immediate-release tramadol or oxycodone at low doses are preferred. Use paracetamol as opioid-sparing. Avoid tapentadol in Child-Pugh C. |
| Benzodiazepines (e.g., diazepam, oxazepam) | Alcohol use disorder, Cirrhosis, Hepatic encephalopathy | Alcohol enhances sedation and motor impairment. Even short-term use can precipitate encephalopathy. Oxazepam or temazepam are preferred due to simpler metabolism. |
| Calcium Channel Blockers (e.g., felodipine, verapamil) | Cirrhosis, Symptomatic hypotension | Amlodipine, nifedipine, and diltiazem appear safe at low doses. Avoid felodipine, lercanidipine, and verapamil in Child-Pugh C cirrhosis. |
| NSAIDs (e.g., ibuprofen, diclofenac, celecoxib) | Alcohol use disorder, Alcoholic hepatitis, Cirrhosis | Increased risk of peptic ulcers, GI bleeding, and renal impairment/hepatorenal syndrome. All NSAIDs should be avoided. Paracetamol is a safe alternative (max 2–3g daily in cirrhosis/malnutrition). |
 |  |
Nonalcoholic Fatty Liver Disease
Common Types of Liver Disease11
Pathogenesis and Spectrum of Disease
Prevalence and Clinical Overview12
Nonalcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease in many developed countries.
Disease Progression and Spectrum
NAFLD represents a spectrum of liver conditions with varying risks of progression:
- Nonalcoholic Steatosis (Fatty Liver)
- Characterized by simple fatty change.
- Generally carries no risk of progression.
- Nonalcoholic Steatohepatitis (NASH)
- Characterized by fat and inflammation.
- May lead to fibrosis and cirrhosis.
- Approximately 10–30% of cases may develop cirrhosis or hepatocellular carcinoma (HCC).
Etiology and Pathogenesis
- Metabolic Syndrome: NAFLD is considered the hepatic component of metabolic syndrome, associated with obesity, hypertension (HTN), hyperlipidemia (HLD), and Type 2 Diabetes Mellitus (T2DM).
- Oxidative Stress: Pathogenesis involves oxidative stress injury and other factors leading to lipid peroxidation in the presence of fatty infiltration and inflammation.
Management and Surgical Interventions
Clinical Management Strategies13
-
Lifestyle Interventions:
- Weight loss.
- Increased physical activity.
- Attention to cardiovascular risk factors.
-
Medical Management:
- Orlistat: An enteric lipase inhibitor that causes malabsorption of dietary fat.
- Pioglitazone: An antidiabetic medication used for biopsy-proven NASH when lifestyle interventions have failed.
- Vitamin E: Utilized in specific treatment protocols.
Surgical and Long-term Care
-
Surgical Interventions:
- Bariatric surgery.
- Liver transplantation for cases of NASH-related cirrhosis.
-
Monitoring and Surveillance:
- Regular monitoring for Hepatocellular Carcinoma (HCC), which has a 2.6% cumulative incidence in patients with NASH.
Implications for Oral Health Care Providers
Providers should consider the possibility of NAFLD in patients presenting with metabolic syndrome.
Viral Hepatitis14
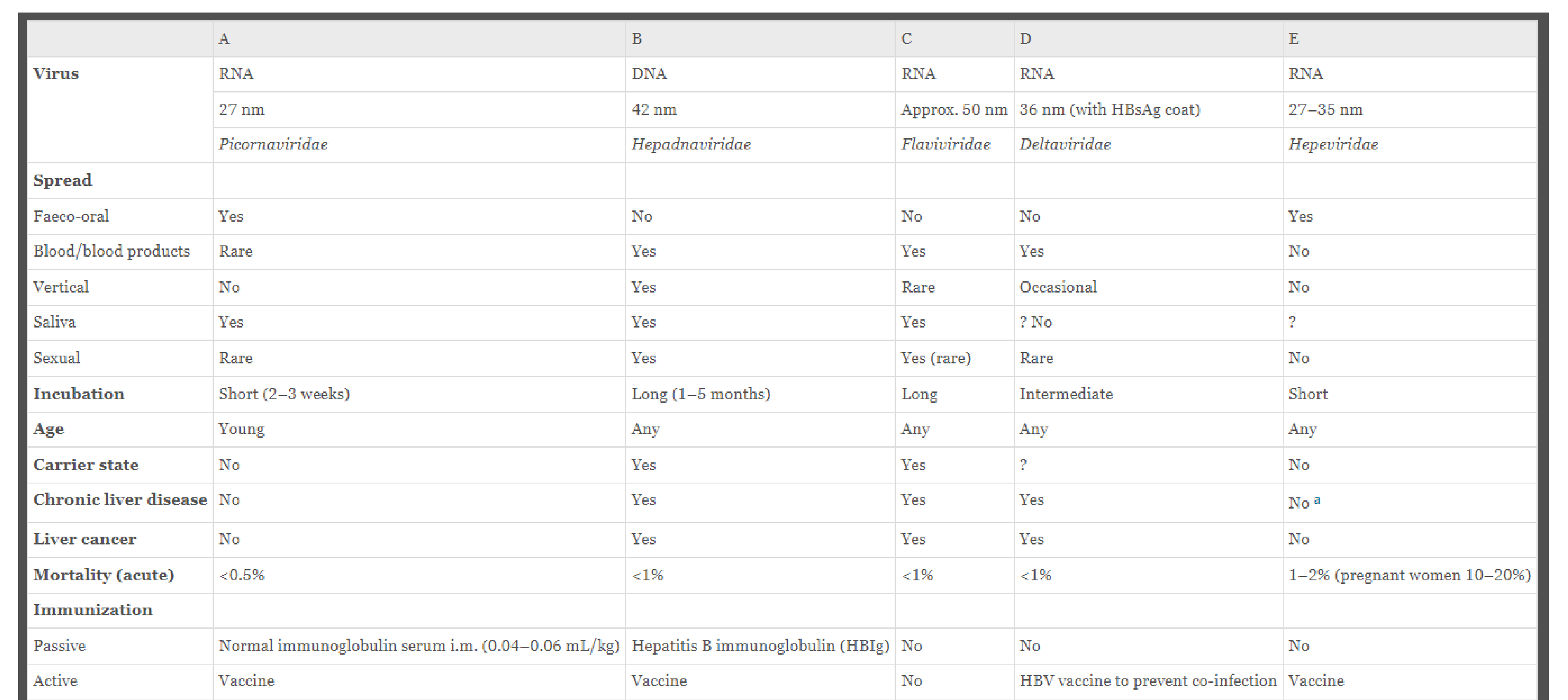
Comparison of Hepatitis Viruses A through E15
| Feature | Hepatitis A | Hepatitis B | Hepatitis C | Hepatitis D | Hepatitis E |
|---|---|---|---|---|---|
| Virus Type | RNA (27 nm) Picornaviridae | DNA (42 nm) Hepadnaviridae | RNA (~50 nm) Flaviviridae | RNA (36 nm with HBsAg coat) Deltaviridae | RNA (27–35 nm) Hepeviridae |
| Transmission | |||||
| Faeco-oral | Yes | No | No | No | Yes |
| Blood/products | Rare | Yes | Yes | Yes | No |
| Vertical | No | Yes | Rare | Occasional | No |
| Saliva | Yes | Yes | Yes | ? No | ? |
| Sexual | Rare | Yes | Yes (rare) | Rare | No |
| Incubation | Short (2–3 weeks) | Long (1–5 months) | Long | Intermediate | Short |
| Age Group | Young | Any | Any | Any | Any |
| Carrier State | No | Yes | Yes | ? | No |
| Chronic Disease | No | Yes | Yes | Yes | No |
| Liver Cancer | No | Yes | Yes | Yes | No |
| Acute Mortality | <0.5% | <1% | <1% | <1% | 1–2% (Pregnant: 10–20%) |
| Immunization | |||||
| Passive | Normal immunoglobulin serum i.m. | Hepatitis B immunoglobulin (HBIG) | No | No | No |
| Active | Vaccine | Vaccine | No | HBV vaccine (prevents co-infection) | Vaccine |
Clinical Implications for Dental Practitioners
Occupational Transmission Risks16
The risk of transmission following a needlestick injury varies by virus:
- Hepatitis B: 6–30%
- Hepatitis C: 1–3%
Prognosis and Resolution Rates
- Hepatitis B: There is an 80% chance of resolution of acute hepatitis, with less than 20% progressing to a chronic state
- It cannot be "cured" due to its episomal DNA structure in the host nucleus, but it can be prevented via vaccine.
- Hepatitis C: There is a 20% chance of resolution of acute hepatitis, with an 80% chance of progressing to a chronic state
- Hepatitis C can now be cured with direct-acting antivirals.
- Even if cured, the risk of liver cancer remains, requiring lifelong monitoring.
Hepatitis C Diagnostic Testing
Diagnostic Methodology17
- Hepatitis C (HCV) is an RNA virus.
- PCR for RNA is the only method available to distinguish between a chronic infection and a cleared infection.
- Any patient testing positive for HCV RNA should receive treatment.
Hepatitis B Structure and Serologic Markers
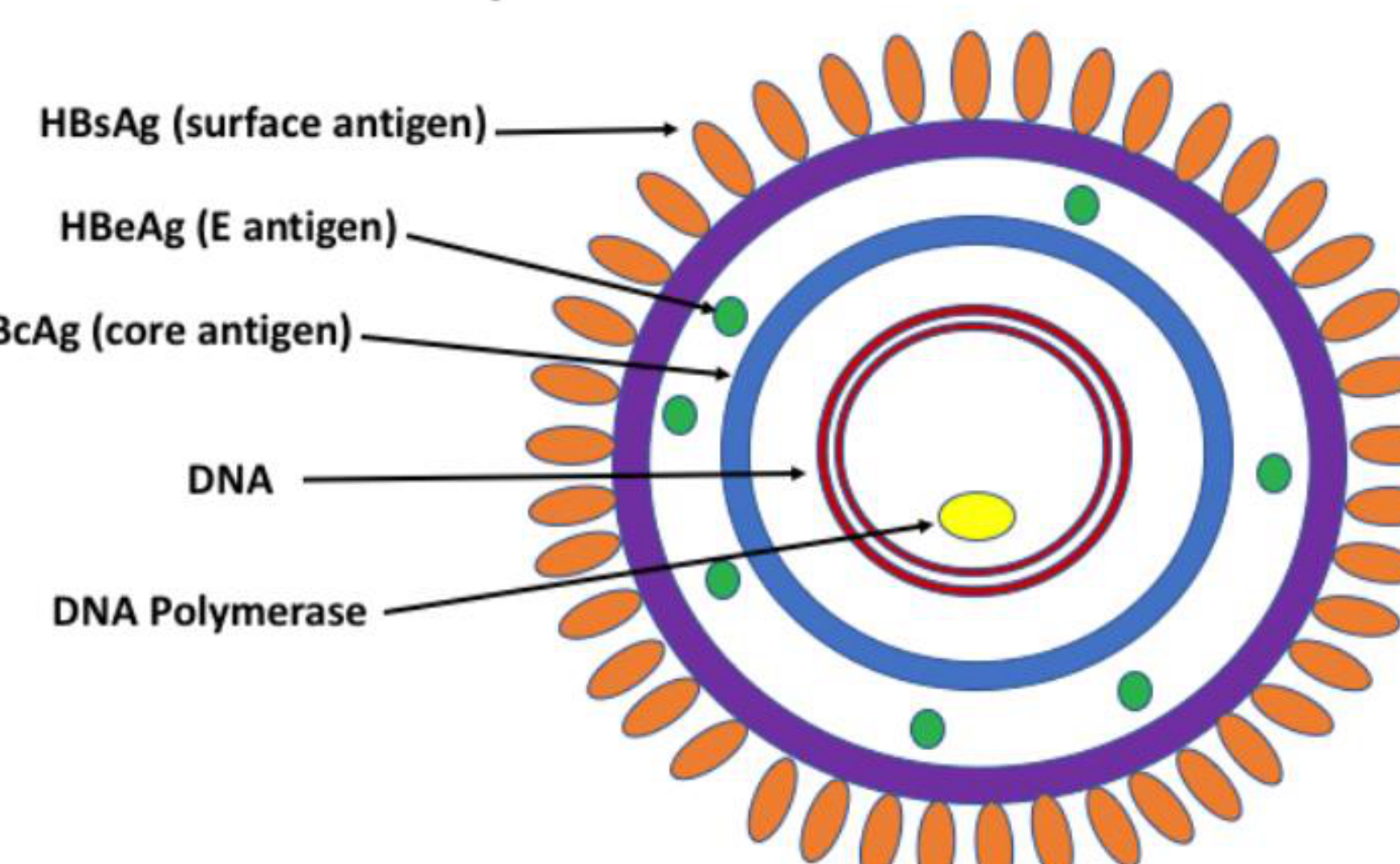
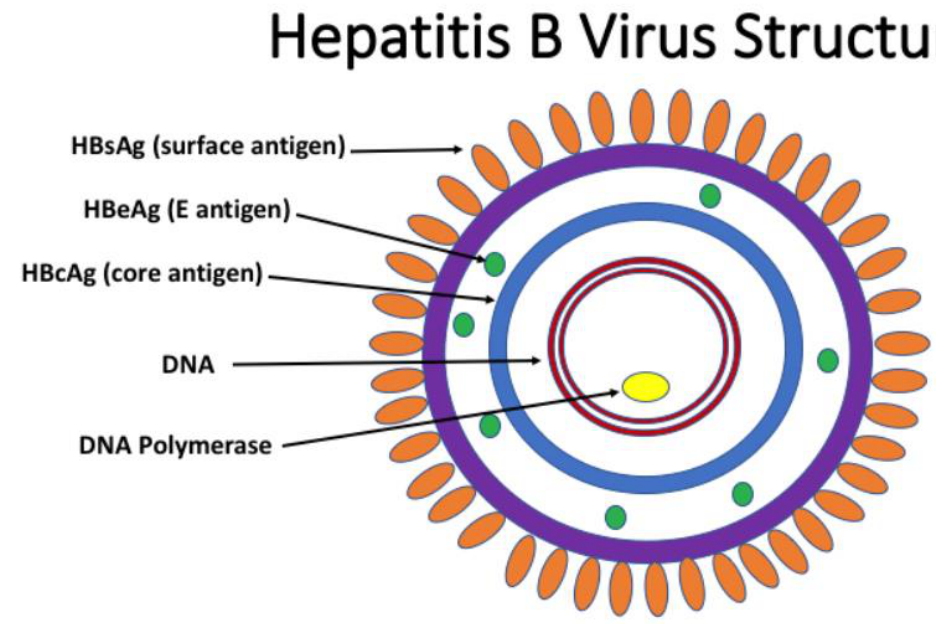
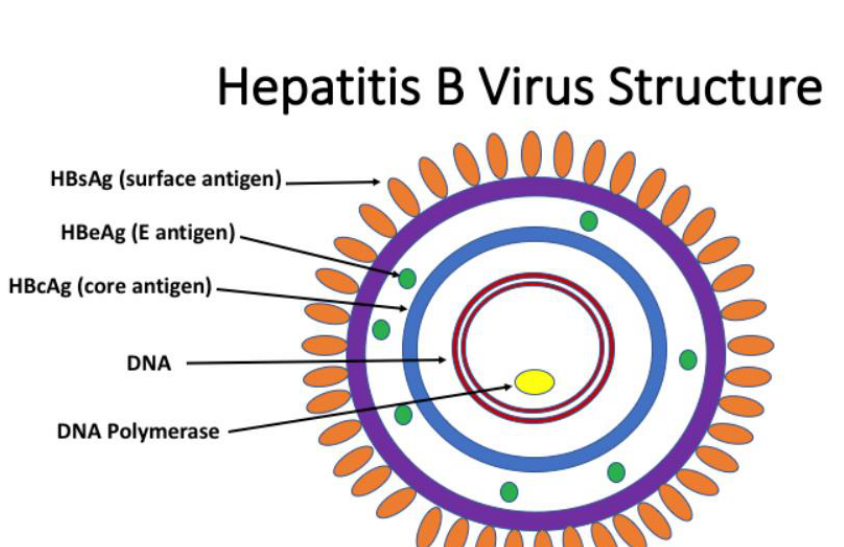
Hepatitis B Virus Structure18
The Hepatitis B virus structure is characterized by specific serologic targets used for diagnostic testing and monitoring.
Viral Antigens
The virus contains Surface antigens (HBsAg), E antigens (HBeAg), and Core antigens (HBcAg).
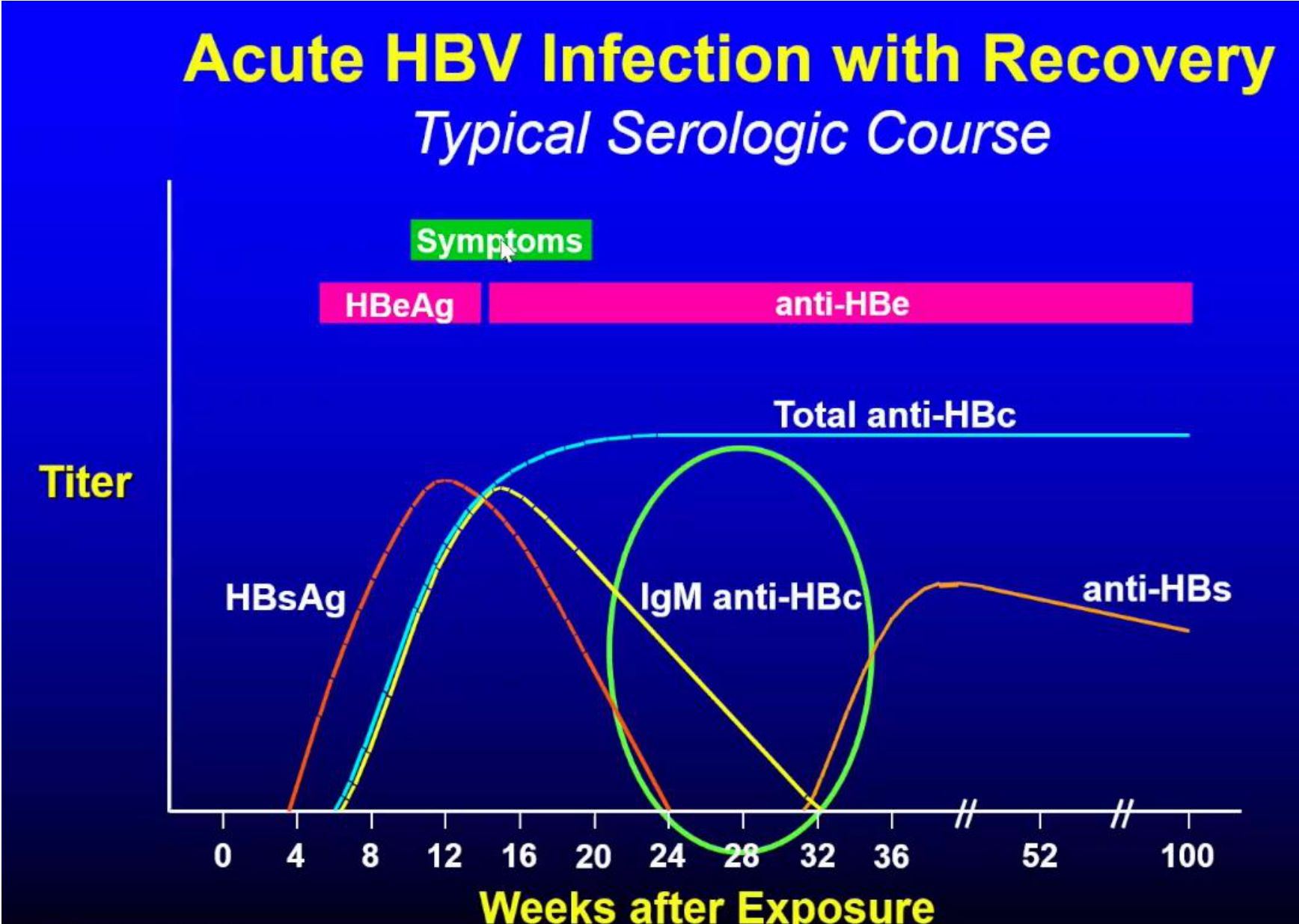
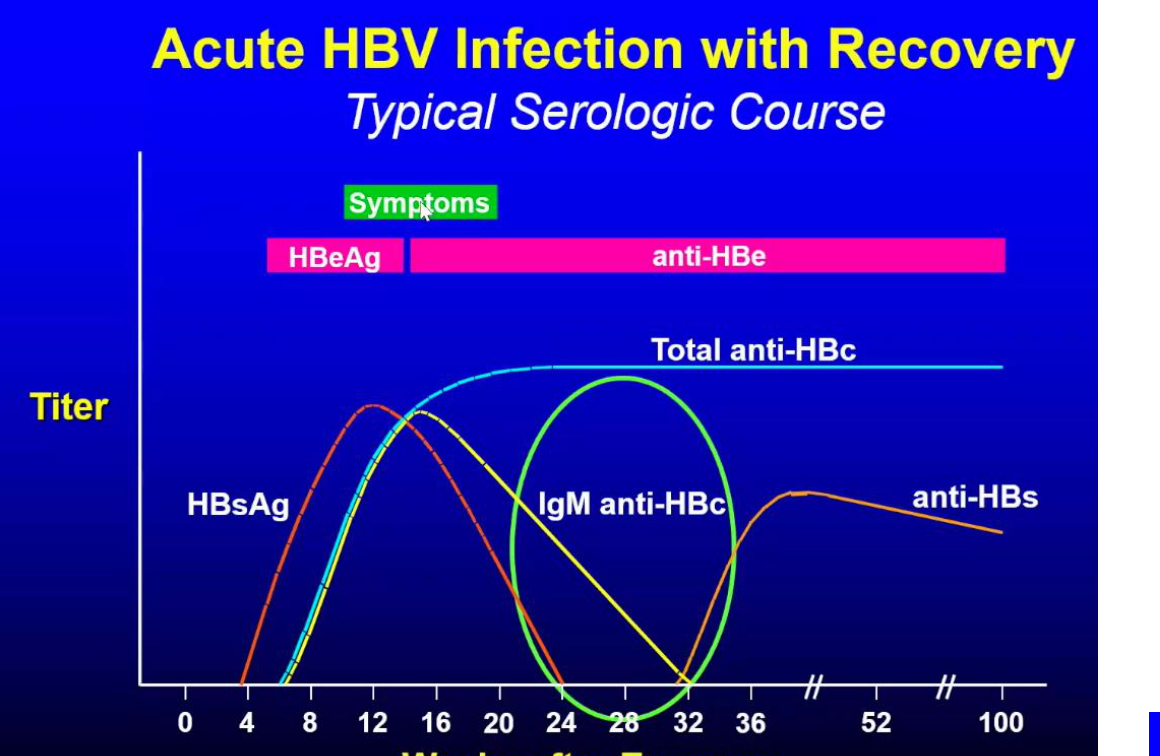
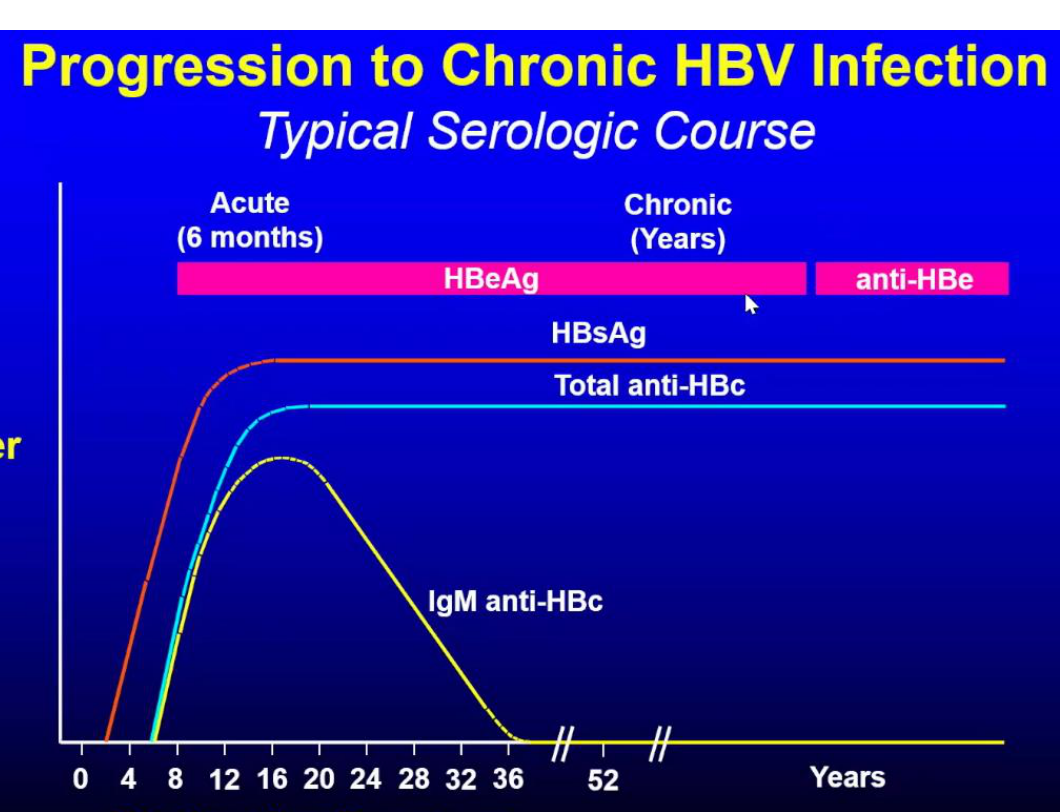
Clinical Course and Serology19
- Acute HBV Infection with Recovery (Typical Serologic Course)
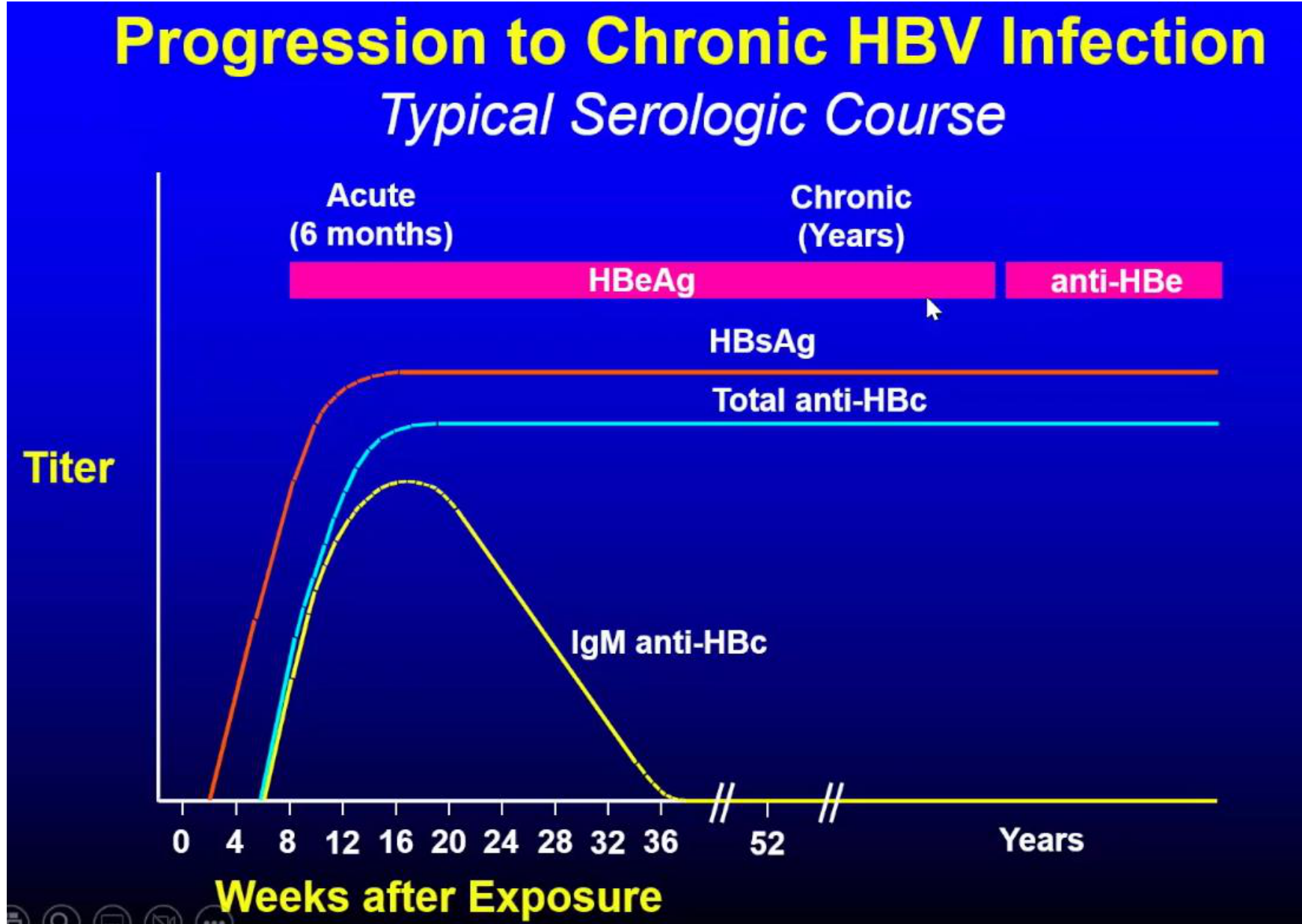
- Progression to Chronic HBV Infection (Typical Serologic Course)
 |  |
 |
Initial Screening and Testing
The following markers are used for the initial screen of Hepatitis B:
-
HBsAg: Indicates any active infection or carrier state (which has the potential to be re-activated).
-
Anti-HBs: Indicates immunity
-
Immunity can be from either recovery or vaccination.
-
Anti-HBc: Indicates any history of infection.
-
IgM Anti-HBc: Indicates recency of infection; also used for detection during the surface antigen seronegative window.
-
Acute HBV Infection with Recovery (Typical Serologic Course)
-
Progression to Chronic HBV Infection (Typical Serologic Course)
-
HBsAg: Any active infection or carrier state (can be re-activated).
-
Anti-HBs: Immunity.
-
Anti-HBc: Any history of infection.
-
IgM Anti-HBc: Recency of infection and/or detection in surface antigen seronegative window.
Supplemental Testing for HBsAg Positive Patients20
If a patient is HBsAg positive, further tests are required:
- HBV DNA (PCR)
- HBeAg
- Anti-Hbe
 |  |
 |
Replicative State Identification
HBV DNA is the single test capable of distinguishing an active replicative state; however, it is very expensive.
Autoimmune Hepatitis21
Epidemiology and Etiology of Autoimmune Hepatitis
Disease Description and Pathogenesis22
Autoimmune hepatitis is an immune-mediated inflammatory disease of the liver. It is characterized by circulating antibodies (Abs), increased concentrations of IgG, and distinctive histological features. The pathogenesis involves antibodies directed against proteins expressed in liver cells.
Epidemiology
- Gender: Significant female predominance (4:1 ratio)
- Age: Typically affects individuals over 18 years of age
- Race: Higher prevalence in Europeans and individuals in the US of Caucasian background, though it can affect any population
- Incidence: 1 per 100,000
- Prevalence: 22.8 per 100,000
Etiology and Risk Factors
The etiology is multifactorial, involving:
- Genetic factors
- Altered immune tolerance
- Environmental triggers (e.g., smoking, toxins)
- Individual risk factors
- Viral infections
- Drug-induced liver injury (DILI)
Diagnosis
Diagnosis is achieved through a combination of:
- Blood tests (to exclude other forms of hepatitis)
- Ultrasound imaging
- Liver biopsy
Clinical Management
- Prednisolone: Used as bridging therapy; dosage is typically 0.5 mg/kg, increasing up to 1.0 mg/kg for acute cases.
- Azathioprine: Utilized as the first-line treatment.
- Mycophenolate mofetil: Utilized as a second-line treatment option
Prognosis
Untreated cases of autoimmune hepatitis can lead to death within five years.
Drug Induced Liver Injury23
Considerations for Cirrhotic Patients24
Drug Induced Liver Injury (DILI) must be considered in the cirrhotic patient, as hepatic reserve is limited.
Prescribing any drugs with potential hepatotoxicity should be done with caution. Any drug-related hepatic injury may precipitate decompensation in these patients.
Pathogenesis and Classification of Hepatotoxicity
Definition and Categorization25
Drug Induced Liver Injury (DILI) is defined as an acute or chronic liver response to a natural or manufactured compound (Francis 2022). It can be categorized by:
- Liver Function Tests (LFTs)
- Histology
- Acute vs. chronic presentation
Pathogenesis Mechanisms
- Direct/Intrinsic: Predictable and dose-dependent.
- Indirect/Idiosyncratic: Unpredictable and non-dose dependent.
Clinical Management of Drug Induced Liver Injury26
Clinical Presentation27
Common signs and symptoms of DILI include:
- Jaundice
- Weakness
- Abdominal pain
- Dark stools or urine
- Nausea
- Pruritis
Treatment Protocols
- Withdrawal of the offending agent.
- Administration of N-acetyl cysteine (NAC) for paracetamol toxicity to facilitate regeneration of glutathione.
- Steroid therapy for DILI cases resembling Autoimmune Hepatitis (AIH).
- Inpatient assessment if Acute Liver Failure (ALF) is suspected.
Identification of specific hepatotoxic drugs is essential for clinical management.
Hepatotoxic Drug Categories and Likelihood
LiverTox Resource and Likelihood Categories28
LiverTox serves as an online resource for information on Drug-Induced Liver Injury (Research Update April 1, 2022). Drugs are classified into five categories based on the likelihood of causing liver injury (Bjornsson 2016):
- Category A: > 50 published reports
- Category B: > 12 but < 50 published reports
- Category C: > 4 but < 12 published reports
- Category D: 1–3 case reports
- Category E: No implication
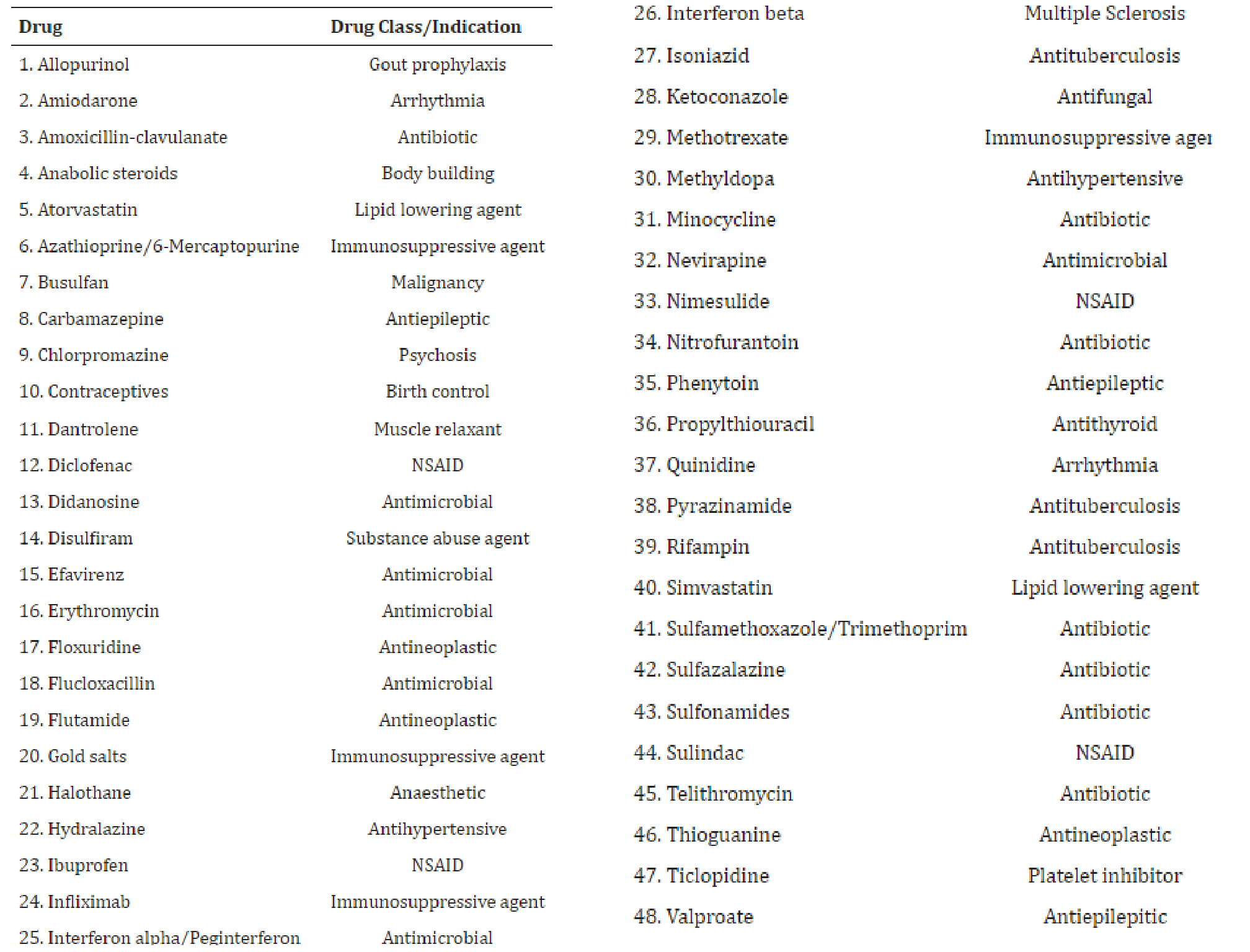
Category A Drugs (> 50 Published Reports)29
| Drug | Drug Class/Indication |
|---|---|
| 1. Allopurinol | Gout prophylaxis |
| 2. Amiodarone | Arrhythmia |
| 3. Amoxicillin-clavulanate | Antibiotic |
| 4. Anabolic steroids | Body building |
| 5. Atorvastatin | Lipid lowering agent |
| 6. Azathioprine/6-Mercaptopurine | Immunosuppressive agent |
| 7. Busulfan | Malignancy |
| 8. Carbamazepine | Antiepileptic |
| 9. Chlorpromazine | Psychosis |
| 10. Contraceptives | Birth control |
| 11. Dantrolene | Muscle relaxant |
| 12. Diclofenac | NSAID |
| 13. Didanosine | Antimicrobial |
| 14. Disulfiram | Substance abuse agent |
| 15. Efavirenz | Antimicrobial |
| 16. Erythromycin | Antimicrobial |
| 17. Floxuridine | Antineoplastic |
| 18. Flucloxacillin | Antimicrobial |
| 19. Flutamide | Antineoplastic |
| 20. Gold salts | Immunosuppressive agent |
| 21. Halothane | Anaesthetic |
| 22. Hydralazine | Antihypertensive |
| 23. Ibuprofen | NSAID |
| 24. Infliximab | Immunosuppressive agent |
| 25. Interferon alpha/Peginterferon | Antimicrobial |
| 26. Interferon beta | Multiple Sclerosis |
| 27. Isoniazid | Antituberculosis |
| 28. Ketoconazole | Antifungal |
| 29. Methotrexate | Immunosuppressive agent |
| 30. Methylpoda | Antihypertensive |
| 31. Minocycline | Antibiotic |
| 32. Nevirapine | Antimicrobial |
| 33. Nimesulide | NSAID |
| 34. Nitrofurantoin | Antibiotic |
| 35. Phenytoin | Antiepileptic |
| 36. Propylthiouracil | Antithyroid |
| 37. Quinidine | Arrhythmia |
| 38. Pyrazinamide | Antituberculosis |
| 39. Rifampin | Antituberculosis |
| 40. Simvastatin | Lipid lowering agent |
| 41. Sulfamethoxazole/Trimethoprim | Antibiotic |
| 42. Sulfazalazine | Antibiotic |
| 43. Sulfonamides | Antibiotic |
| 44. Sulindac | NSAID |
| 45. Telithromycin | Antibiotic |
| 46. Thioguanine | Antineoplastic |
| 47. Ticlopidine | Platelet inhibitor |
| 48. Valproate | Antiepileptic |
 |  |
Notable Hepatotoxic Agents
Of particular note in clinical practice (Bjornsson 2016, Chalasani et al 2015):
- Amoxicillin-clavulanate
- Azathioprine
- Carbamazepine
- Diclofenac
- Erythromycin
- Ibuprofen
- Methotrexate
- Minocycline
- Sulfamethoxazole/Trimethoprim
Jaundice and Bilirubin Metabolism30
Jaundice is a clinical manifestation of elevated bilirubin levels in the blood, resulting in the yellowing of the skin and mucous membranes.
Physiology of Bilirubin Production and Excretion
Bilirubin Production and Initial Processing31
The conversion of heme to bilirubin is a two-step process:
- Heme to Biliverdin: Heme (derived from erythrocytes) is converted to biliverdin, occurring mainly in the spleen.
- Biliverdin to Unconjugated Bilirubin (UCB): Biliverdin is converted to unconjugated bilirubin, also primarily in the spleen.
Transport and Hepatic Processing
- Transport: UCB is transported through the bloodstream bound to albumin.
- Hepatocyte Entry: UCB enters the hepatocytes.
- Conjugation: Inside the hepatocytes, unconjugated bilirubin is conjugated with glucuronic acid.
- Secretion: Conjugated bilirubin is then secreted into the bile.
Excretion and Metabolism of Conjugated Bilirubin32
- Duodenal Secretion: Conjugated bilirubin is water-soluble and is excreted via the bile duct into the middle duodenum.
- Breakdown by Gut Flora: In the intestines, conjugated bilirubin is broken down by gut flora into urobilinogen.
Pathways of Urobilinogen
Urobilinogen follows one of two primary pathways:
- Stool Excretion: It is excreted in the stool as stercobilinogen.
- Enterohepatic Circulation: It is reabsorbed via the portal vein, after which:
- The liver excretes it back into the bile duct along with bile salts, OR
- It enters the systemic circulation and is excreted through the kidneys.
Summary of Hepatic Transformation33
- UNCONJUGATED BILIRUBIN → LIVER → CONJUGATED BILIRUBIN

Causes of Unconjugated Hyperbilirubinemia
Increased Bilirubin Production34
This occurs due to the increased breakdown of heme, which can be caused by:
- Accelerated or prolonged hemolysis.
- Large hematomas.
Impaired Bilirubin Uptake
- Reduced Hepatic Flow: Decreased delivery of bilirubin to the liver (e.g., congestive heart failure or portosystemic shunts).
- Inefficient Hepatocyte Uptake: Interference with the uptake process, often due to drugs or the administration of contrast agents.
Impaired Bilirubin Conjugation
This involves defects within the hepatocytes, often resulting from hereditary conditions such as:
- Gilbert syndrome.
- Gilbert Syndrome: A common, benign hereditary defect in conjugation that causes low-level jaundice.
- Crigler-Najjar syndrome.
Causes of Conjugated Hyperbilirubinemia
Extrahepatic Cholestasis35
- Biliary Obstruction: Caused by conditions such as primary sclerosing cholangitis or AIDS cholangiopathy.
- Gallstones or duct obstruction.
- Mechanism: Pressure from the obstructed bile duct allows conjugated bilirubin to overcome the resistance of hepatocyte tight junctions, resulting in reflux into the plasma.
Intrahepatic Cholestasis
- Transport and Structural Defects: Involves aberrations in conjugated bilirubin transport, bile canalicular membrane fluidity, and hepatocyte cytoskeletal function.
- Hereditary Factors: These deviations are often caused by hereditary processes, such as:
- Dubin-Johnson syndrome: A specific defect in the MRP2 protein.
Hepatocellular Injury
Injury to the liver cells leads to the release of intracellular proteins into the plasma. Common causes include:
- Acute hepatitis.
- Chronic hepatitis (cirrhotic stage).
Summary of Clinical Key Points
Medication and Drug Considerations36
- Be mindful of Drug-Induced Liver Injury (DILI) in patients with cirrhosis, particularly regarding the use of antibiotics, NSAIDs, and paracetamol dosages, as these patients have limited hepatic reserve.
- Consult the LiverTox database for Category A drugs to assess potential hepatotoxicity.
- Apply special drug considerations for patients with alcohol use disorder.
Bleeding Risks and Complications
- Query bleeding risks in cirrhotic patients, specifically assessing clotting ability and the risk of variceal bleeding.
- The liver produces clotting factors; expect prolonged bleeding in advanced disease and consult with the patient's GP or specialist.
Infection Control and Prophylaxis
- Antibiotic prophylaxis may be considered for patients with ascites to prevent spontaneous bacterial peritonitis; this should be discussed with the patient’s medical GP.
Gilbert Syndrome
Gilbert Syndrome is a common, hereditary defect in the conjugation of bilirubin. Patients are generally healthy but may present with mild, intermittent jaundice because they cannot process bilirubin efficiently when the system is stressed. It is considered an "inert" or benign condition.
- Unstable or decompensated patients (e.g., those with ascites) should be treated in a hospital dental setting.
References37
-
Alcohol (2020) NHMRC. Available at: https://www.nhmrc.gov.au/health-advice/alcohol (Accessed: 23 January 2025).
-
Arroyo, V., Moreau, R., Kamath, P. et al. Acute-on-chronic liver failure in cirrhosis. Nat Rev Dis Primers 2, 16041 (2016). https://doi.org/10.1038/nrdp.2016.41
-
Björnsson ES. Hepatotoxicity by Drugs: The Most Common Implicated Agents. Int J Mol Sci. 2016 Feb 6;17(2):224. doi: 10.3390/ijms17020224. PMID: 26861310; PMCID: PMC4783956.
-
Chalasani N, Bonkovsky HL, Fontana R, Lee W, Stolz A, Talwalkar J, Reddy KR, Watkins PB, Navarro V, Barnhart H, Gu J, Serrano J; United States Drug Induced Liver Injury Network. Features and Outcomes of 899 Patients With Drug-Induced Liver Injury: The DILIN Prospective Study. Gastroenterology. 2015 Jun;148(7):1340-52.e7. doi: 10.1053/j.gastro.2015.03.006. Epub 2015 Mar 6. PMID: 25754159; PMCID: PMC4446235.
-
Francis P, Navarro VJ. Drug-Induced Hepatotoxicity. [Updated 2022 Nov 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK557535/
-
Muratori L, Lohse AW, Lenzi M. Diagnosis and management of autoimmune hepatitis. BMJ. 2023;380:e070201. doi: 10.1136/bmj-2022-070201.
-
Patel R, Mueller M. Alcoholic Liver Disease. [Updated 2023 Jul 13]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK546632/
-
Singh A, Koritala T, Jialal I. Unconjugated Hyperbilirubinemia. [Updated 2023 Feb 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK549796/
-
Tripathi N, Jialal I. Conjugated Hyperbilirubinemia. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK562172/
-
LiverTox Database (National Institute of Diabetes and Digestive and Kidney Diseases).
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Nonalcoholic Fatty Liver Disease (NAFLD)
Common Types of Liver Disease
NAFLD is the most common cause of chronic liver disease in developed countries.
Pathogenesis and Spectrum of Disease
Prevalence and Clinical Overview
NAFLD is considered the “liver component” of Metabolic Syndrome.
Disease Progression and Spectrum
The spectrum mirrors ALD: Steatosis Steatohepatitis Fibrosis Cirrhosis Hepatocellular Carcinoma.
Etiology and Pathogenesis
Associated with obesity, hypertension, hyperlipidemia, and Type 2 diabetes. Oxidative stress leads to fatty infiltration and inflammation.
Management and Surgical Interventions
Clinical Management Strategies
Focuses on lifestyle modification: weight loss, physical activity, and managing cardiovascular risk factors.
Surgical and Long-term Care
NAFLD is monitored similarly to a pre-malignant lesion due to a 2.6% incidence of transformation to carcinoma.
Implications for Oral Health Care Providers
Dentists should screen for liver status in any patient presenting with signs of metabolic syndrome.
Drug Induced Liver Injury (DILI)
Considerations for Cirrhotic Patients
DILI is perhaps the most critical topic for dentists. Patients with cirrhosis have limited hepatic reserve; a drug-induced insult can trigger fatal decompensation.
Pathogenesis and Classification of Hepatotoxicity
Definition and Categorization
- Direct (Dose-Dependent): Predictable; higher doses cause more damage (e.g., Paracetamol).
- Idiosyncratic (Indirect): Unpredictable and non-dose dependent. Occurs at normal doses due to host/environmental factors.
Clinical Management of Drug Induced Liver Injury
Clinical Presentation
Jaundice, dark urine, itchiness, and abdominal pain.
Treatment Protocols
- Withdraw the offending agent.
- Paracetamol overdose: Administer N-acetyl cysteine to regenerate glutathione.
Hepatotoxic Drug Categories and Likelihood
LiverTox Resource and Likelihood Categories
The LiverTox database (NIH) categorizes drugs by their documented potential for injury.
Category A Drugs (> 50 Published Reports)
These are “real potential hepatotoxins.” Dentists must be extremely cautious with these in cirrhotic patients.
Notable Hepatotoxic Agents
- Many Antibiotics and NSAIDs fall into Category A.
- Clinical Tip: Always check LiverTox before prescribing to a patient with poor hepatic function.
Footnotes
-
Original PDF page 1: L23 Liver Diseases, p.1 ↩
-
Original PDF page 2: L23 Liver Diseases, p.2 ↩
-
Original PDF page 3: L23 Liver Diseases, p.3 ↩
-
Original PDF page 4: L23 Liver Diseases, p.4 ↩
-
Original PDF page 5: L23 Liver Diseases, p.5 ↩
-
Original PDF page 6: L23 Liver Diseases, p.6 ↩
-
Original PDF page 7: L23 Liver Diseases, p.7 ↩
-
Original PDF page 8: L23 Liver Diseases, p.8 ↩
-
Original PDF page 9: L23 Liver Diseases, p.9 ↩
-
Original PDF page 10: L23 Liver Diseases, p.10 ↩
-
Original PDF page 11: L23 Liver Diseases, p.11 ↩
-
Original PDF page 12: L23 Liver Diseases, p.12 ↩
-
Original PDF page 13: L23 Liver Diseases, p.13 ↩
-
Original PDF page 14: L23 Liver Diseases, p.14 ↩
-
Original PDF page 15: L23 Liver Diseases, p.15 ↩
-
Original PDF page 16: L23 Liver Diseases, p.16 ↩
-
Original PDF page 17: L23 Liver Diseases, p.17 ↩
-
Original PDF page 18: L23 Liver Diseases, p.18 ↩
-
Original PDF page 19: L23 Liver Diseases, p.19 ↩
-
Original PDF page 20: L23 Liver Diseases, p.20 ↩
-
Original PDF page 21: L23 Liver Diseases, p.21 ↩
-
Original PDF page 22: L23 Liver Diseases, p.22 ↩
-
Original PDF page 23: L23 Liver Diseases, p.23 ↩
-
Original PDF page 24: L23 Liver Diseases, p.24 ↩
-
Original PDF page 25: L23 Liver Diseases, p.25 ↩
-
Original PDF page 27: L23 Liver Diseases, p.27 ↩
-
Original PDF page 26: L23 Liver Diseases, p.26 ↩
-
Original PDF page 28: L23 Liver Diseases, p.28 ↩
-
Original PDF page 29: L23 Liver Diseases, p.29 ↩
-
Original PDF page 30: L23 Liver Diseases, p.30 ↩
-
Original PDF page 31: L23 Liver Diseases, p.31 ↩
-
Original PDF page 32: L23 Liver Diseases, p.32 ↩
-
Original PDF page 33: L23 Liver Diseases, p.33 ↩
-
Original PDF page 34: L23 Liver Diseases, p.34 ↩
-
Original PDF page 35: L23 Liver Diseases, p.35 ↩
-
Original PDF page 36: L23 Liver Diseases, p.36 ↩
-
Original PDF page 37: L23 Liver Diseases, p.37 ↩