Renal Disease and Nutritional Deficiencies1
Bobby Joseph Associate Professor 2026
Learning Objectives2
Upon completion of this section, students should be able to:
- Demonstrate familiarity with the oral manifestations of chronic renal failure.
- Understand the dental management protocols for renal patients undergoing dialysis.
- Identify the oral complications associated with renal transplants.
- Recognize the significance of nutrition in maintaining oral health and the integrity of the oral mucous membrane.
- Understand how nutritional deficiencies relate to dysplastic lesions within the oral cavity.
Renal Anatomy and Physiology
Anatomical Structures of the Renal System3
- Left Kidney (in cross-section)
- Right Kidney
- Adrenal Gland
- Diaphragm
- Pelvis of Kidney
- **Renal Arteries (red) & Veins (blue)
- Renal Artery: Controls blood flow into the kidney (approx. 1.2 liters per minute)
- Renal Vein: Carries filtered blood out of the kidney back to the heart**
- Inferior Vena Cava
- Descending Aorta
- Ureters
- **Bladder
- Location: Kidneys are located below the ribcage, behind the belly, on either side of the spine
- Size: Approximately 4 to 5 inches long (roughly the size of a fist)
- Capsule: Three layers of connective tissue/fat that protect the kidney and connect it to surrounding tissues
- Renal Cortex: The outer layer where blood filtering begins; it secretes the hormone erythropoietin
- Renal Papillae: Pyramid-shaped structures that transfer urine to the ureters. These are susceptible to damage from dehydration and misuse of NSAIDs
- Renal Pelvis: A funnel-shaped structure that collects urine **

Functions of the Kidney4
- Elimination of waste products, particularly urea
- Excretion of metabolites and drugs
- Crucial for dental prescribing
- Regulation of blood volume and electrolyte concentration
- Regulation of acid-base (pH) balance
- Regulation of RBC production in the bone marrow by secreting erythropoietin
- Participation in calcium homeostasis and synthesize vitamin D, renin and prostaglandins
- Glucose Synthesis: Can produce sugar if blood levels are low
- Adrenal Glands: Located on top of the kidneys; produce cortisol to manage stress
Chronic Renal Failure
Significance in Dental Practice5
- Renal disease is of great significance in general dental practice.
- Dental management needs to be modified to prevent complications.
- Oral changes occur due to:
- Chronic renal failure
- Results of medical management
Clinical Overview6
- Patients with kidney disorders are seen in dental practice due to improvements in medical care leading to prolonged life expectancy.
- It is essential to have a working knowledge of renal disorders to provide appropriate and safe dental care.
- Oral changes occur as a result of chronic renal failure.
- Dental management must be modified to prevent complications.
Key Areas of Dental Concern7
- Renal function assessment
- Chronic renal failure: oral manifestations
- Dental management of renal patients undergoing dialysis
- Oral complications in renal transplant patients
Relevant Medical History for Renal Patients8
- History of diabetes mellitus
- Chronic renal failure (CRF)
- Related bony disorders
- Anaemia
- Dialysis details:
- Type of dialysis
- Frequency
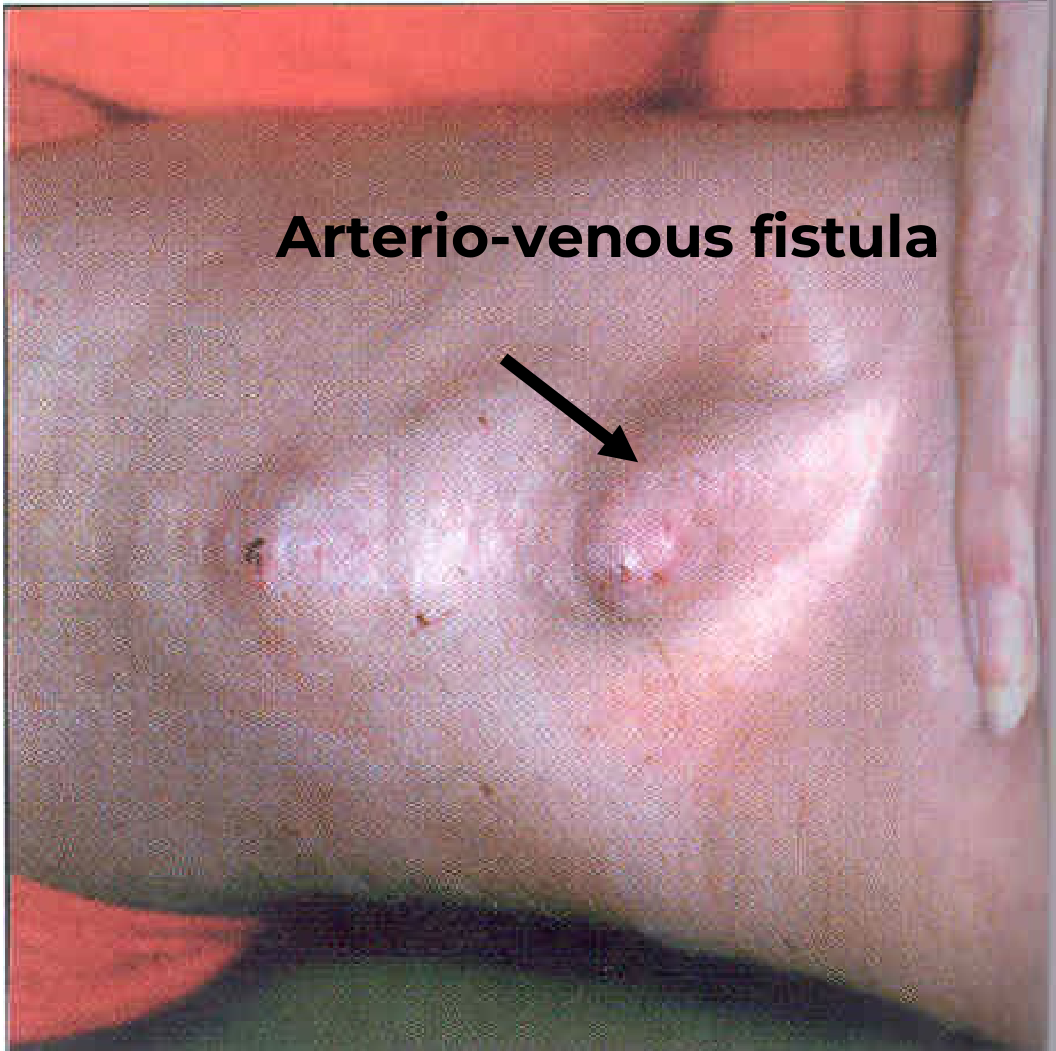
- Presence of A-V fistula
- Transplant history:
- Date of transplant
- Associated medication (including steroids)
- Cyclosporine (often used in transplant patients)
- Bleeding tendencies associated with renal failure
- Susceptibility to infections or recent history of repeated infections (dental or generalised)
Clinical Presentation and Systemic Features
Progression of Chronic Renal Failure (CRF)9
- CRF involves progressive kidney damage.
- Early symptoms include nocturia (frequent urination at night).
- Patients may notice an uncharacteristically poor appetite.
- Adult CRF leads to hypertension and uraemia.
- The condition can affect diverse body systems.
Diagnostic Indicators10
- Irreversible deterioration in renal function.
- Plasma creatinine persistently exceeds 300µmol/l (normal range: 80-120µmol/l).
- Low glomerular filtration rate (GFR) persisting over 3 months (normal: 120ml/min).
Systemic Clinical Features11
Cardiovascular
- Hypertension
- Congestive cardiac failure
- Atheroma
Gastrointestinal
- Anorexia, nausea, vomiting
- Peptic ulcer
Neurological
- Lassitude
- Headaches
- Tremor
- Sensory disturbances
Additional Systemic Features12
Dermatological
- Itching
- Hyperpigmentation
Haematological/Immunological
- Bleeding tendency
- Anaemia
- Susceptibility to infection
Metabolic “Uraemia”
- Thirst
- Nocturia/polyuria
- Electrolyte disturbances
- Secondary hyperparathyroidism
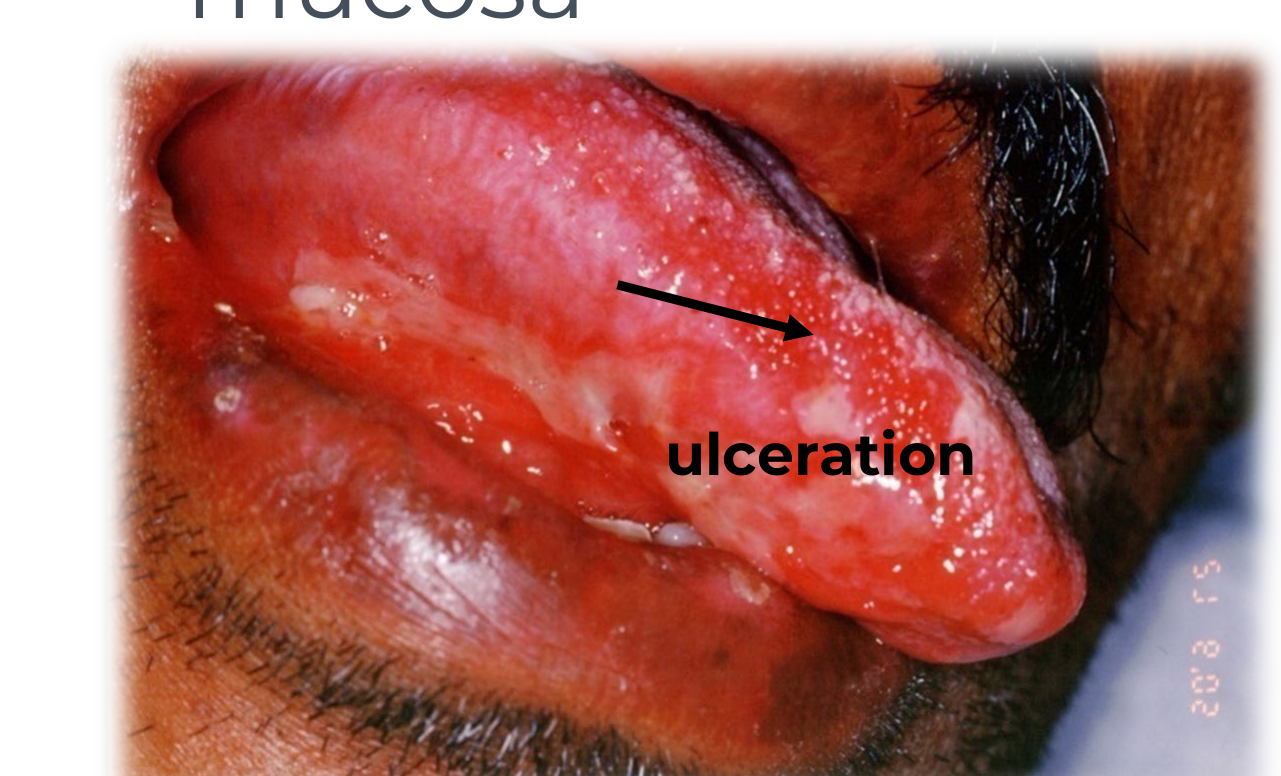
Oral Manifestations of Chronic Renal Failure13
- Dry mouth
- Mucosal ulceration
- Bacterial & fungal plaques
- Pallor of the mucosa
- Mucosal pallor is specifically due to underlying anemia
- Oral purpura
- Giant cell lesions (osteolytic lesions in jaws)
- White plaques (uraemic stomatitis)
 |  |
Uraemia Overview14
- Defined as the presence of excessive amounts of urea and nitrogenous waste compounds in the blood.
- Results from kidney failure.
- Clinical symptoms include nausea, vomiting, lethargy, and drowsiness.
- Treatment may require haemodialysis.
Uraemic Stomatitis15
- Caused by markedly elevated levels of urea and other nitrogenous wastes in the bloodstream.
- Clinical Presentation:
- White plaques on the buccal mucosa, floor of the mouth, and tongue.
- Pain, unpleasant taste, and burning sensation.
- Odour of ammonia or urine on the breath.
- Differential Diagnosis: Clinical appearance can mimic oral hairy leukoplakia.
Classification of Uraemic Stomatitis
- Ulcerative
- Haemorrhagic
- Non-ulcerative, pseudomembranous
- Hyperkeratotic (White lesions)
Clinical Subtypes
- Ulcerative: Characterized by painful superficial ulcers covered by a pseudomembrane.
- Non-ulcerative: Characterized by painful diffuse oedematous erythema and a thick greyish pseudomembrane.
Osseous Lesions and Renal Osteodystrophy16
- Loss of lamina dura
- Osteoporosis
- Osteolytic areas (renal osteodystrophy)
- Secondary hyperparathyroidism
General Signs of CRF
Common physical signs include muscle cramps, swollen ankles, and puffy eyes.
- ==Disturbances in calcium and Vitamin D metabolism==
- Abnormal bone repair after extractions
- Note: Renal disease patients should be screened for bone disease before dental implant placement.
Effects on Tooth and Periodontium
- Delayed eruption
- Enamel hypoplasia
- Loss of lamina dura
- Widening of the periodontal ligament
- Severe periodontal destruction
- Tooth mobility
- Drifting
- Pulp calcifications
- Pulp narrowing
 |  |
Medical Management of Renal Disease
Dialysis Considerations
Dialysis Mechanism17
- Removes metabolites by exposing the patient’s blood across a semi-permeable membrane to a hypotonic solution.
- Essential if renal function worsens to end-stage renal disease (ESRD).
Types of Dialysis18
- Haemodialysis: Requires an arteriovenous (A-V) shunt.
- Continuous Ambulatory Peritoneal Dialysis (CAPD): No hospitalization required.
- Continuous Cyclic Peritoneal Dialysis (CCPD): A machine performs exchanges at night.
Dental Management of Haemodialysed Patients19
- Impaired excretion of drugs by the kidney.
- Bleeding tendency.
- Heparinization prior to dialysis.
- A-V shunts are susceptible to infection.
- ==Never use the fistula arm for blood pressure readings or injections.==
- Anaemia.
- Increased carriage of Hepatitis B & C.
- Hypertension.
Timing of Treatment20
The optimum time for renal patients to undergo dental procedures is 12-24 hours post-haemodialysis.
- This timing is ideal because heparin has worn off and the patient is physiologically most stable.
Renal Transplantation21
- Patients face side-effects from immunosuppressive regimes.
- Presents several dental and management challenges.
- Cyclosporin: A nephrotoxic drug.
- Nifedipine: Used for hypertension in renal patients.
Oral Complications of Transplantation22
- Drug-induced gingival overgrowth
- Bacterial & fungal plaques
- Increased incidence of oral malignancy (reported with cyclosporin)
- Oral candidosis
- Secondary herpes simplex infections
Clinical Presentations
- Gingival overgrowth
- Carcinoma of the gingiva
- Herpes simplex
- Oral candidosis
Immunosuppressive Therapy and Related Disorders
Common Immunosuppressive Agents
- Cyclosporin
- Combined cyclosporin and nifedipine
- Tacrolimus (may result in less gingival enlargement)
- Corticosteroids
Steroid Cover
Corticosteroids are used to prevent organ rejection; clinicians must consider the need for "steroid cover" during stressful dental procedures.
Associated Pathologies
-
Lymphoma
-
Skin cancers
-
Hairy leukoplakia
-
Leukoplakia
-
Kaposi’s sarcoma
-
General Rule: Reduce the dose or increase the interval for drugs excreted by the kidney to avoid toxicity.
-
Always consult the patient's nephrologist before prescribing.
Dental Management and Pharmacology
Prescribing for Renal Patients23
- Many drugs prescribed by dentists are excreted by the kidneys.
- Failure to excrete drugs or metabolites leads to toxicity.
- Nephrotoxic drugs (e.g., gentamicin) should be avoided.
- Drugs may require dose reduction.
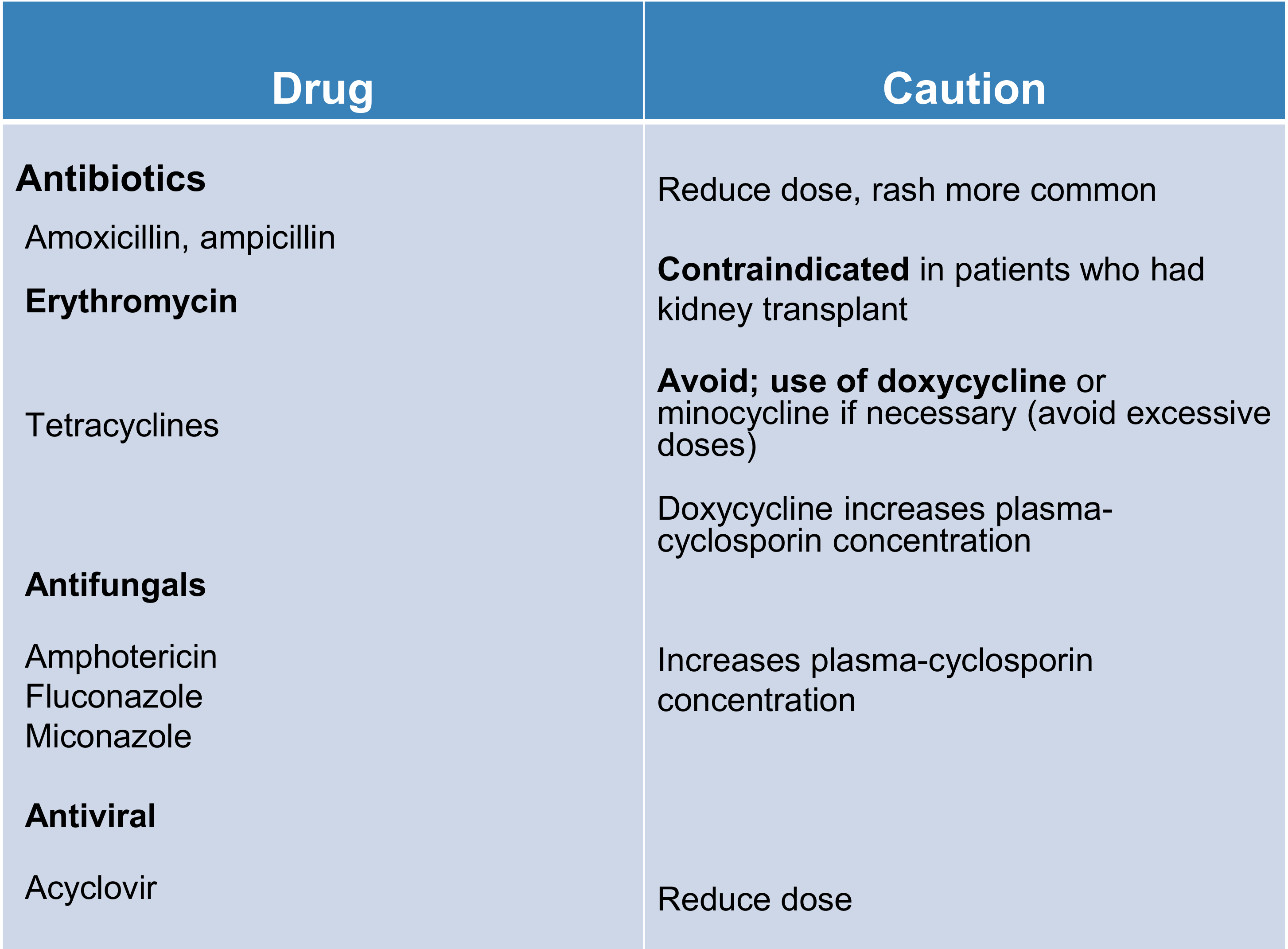
Antibiotic and Antifungal Considerations24
- Amoxicillin, ampicillin: Reduce dose; rash is more common.
- Erythromycin: Contraindicated in patients who have had a kidney transplant.
- Tetracyclines: Avoid; use doxycycline or minocycline if necessary (avoid excessive doses). Doxycycline increases plasma-cyclosporin concentration.
- Antifungals (Amphotericin, Fluconazole, Miconazole): Increases plasma-cyclosporin concentration.
- Acyclovir: Reduce dose.
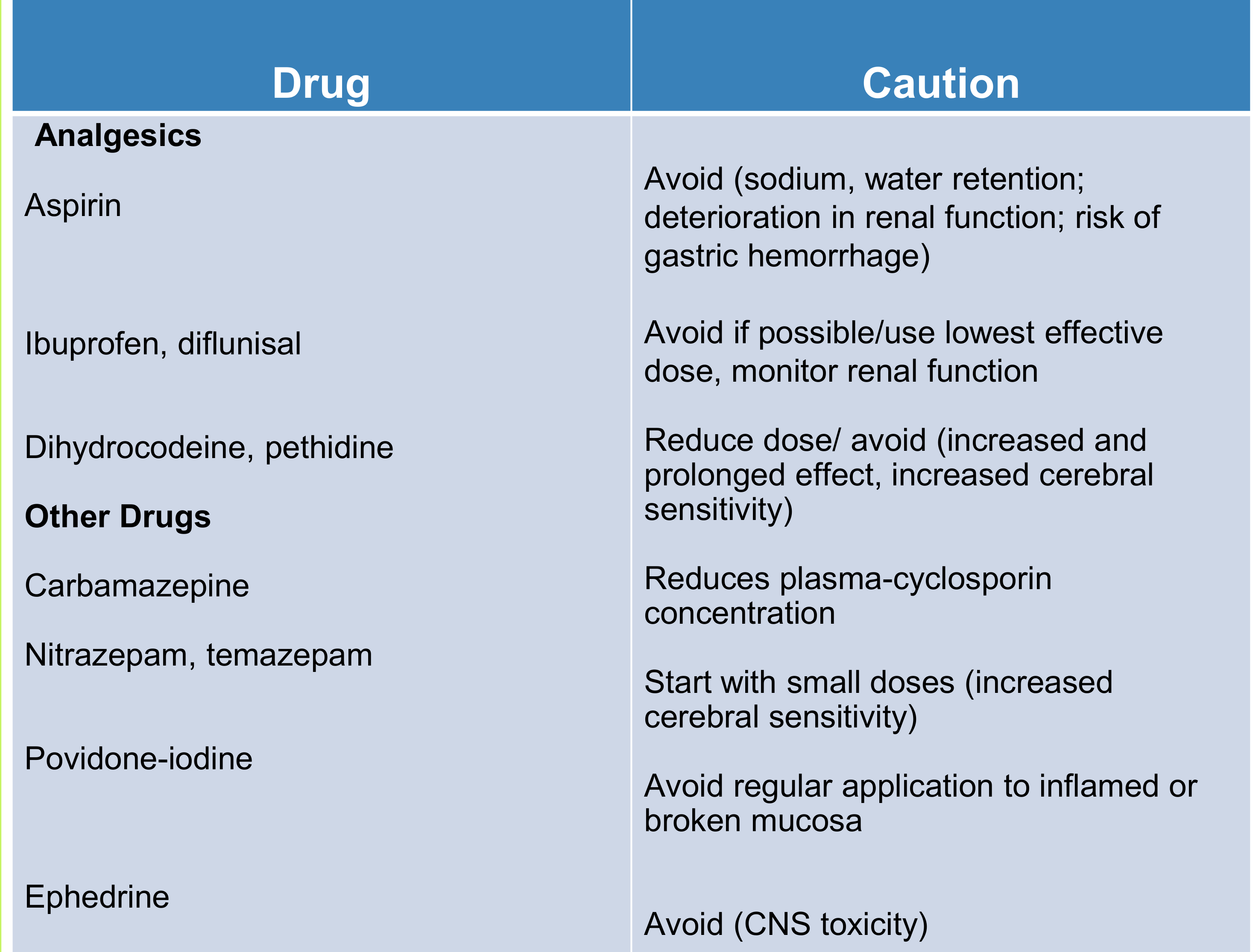
Analgesic and Other Drug Considerations25
- Aspirin: Avoid (causes sodium/water retention, deterioration in renal function, and risk of gastric hemorrhage
- Aspirin also carries a risk of interference with platelets in renal patients.).
- Ibuprofen, diflunisal: Avoid if possible; use lowest effective dose and monitor renal function
Nephrotoxicity
NSAIDs like Ibuprofen are inherently nephrotoxic and can significantly worsen existing renal function. .
- Dihydrocodeine, pethidine: Reduce dose or avoid (increased/prolonged effect and cerebral sensitivity).
- Carbamazepine: Reduces plasma-cyclosporin concentration.
- Nitrazepam, temazepam: Start with small doses due to increased cerebral sensitivity.
- Povidone-iodine: Avoid regular application to inflamed or broken mucosa.
- Ephedrine: Avoid due to CNS toxicity.
Other Renal Pathologies
Polycystic Kidney Disease26
- Common genetic disease (1 in 800 people).
- Mostly affects teenagers and young adults.
- Clinical Features:
- Kidneys enlarge and fill the abdomen.
- Lumbar pain, haematuria, and hypertension.
- High levels of circulating ammonia.
- Breath smells of urine.
- Treatment: Dialysis or renal transplantation.

Kidney Tumours
Wilms’ Tumour27
- Common in children (ages 1-4 years).
- Accounts for 6-7% of all childhood cancers.
- Associated with mutation of the WT 1 gene.
Renal Cell Carcinoma
- Accounts for 85% of all renal malignancies.
- Often presents as an incidental mass.
- Symptoms: Haematuria, abdominal pain, or no symptoms.
- Smokers have an increased risk.
Dental Considerations
Rare cases of metastasis to the dental pulp have been reported in patients with Renal Cell Carcinoma.
Clinical Case Study and Summary
Clinical Scenario28
A 45-year-old male with chronic renal failure on regular haemodialysis presents with severe toothache. He appears tired post-dialysis. Examination reveals a grossly carious maxillary first molar requiring extraction. No soft tissue swelling is present, but non-wipeable white plaques are noted on the tongue and buccal mucosa, which the patient says “come and go.”
Discussion Questions:
- How would you manage the dental extraction of this patient?
- What is the most likely diagnosis of the white plaques on the patient’s oral mucosa?
Case Study Answers29
Management of Extraction (Q1):
- Perform extraction at least 12 hours post-haemodialysis.
- Obtain a recent Full Blood Count (FBC) to exclude thrombocytopaenia.
- Consult the renal unit regarding preoperative antibiotic prophylaxis protocols.
- Use routine local anaesthesia (LA).
- Suture the wound, insert haemostatic gauze, and monitor for postoperative bleeding due to potential bleeding tendencies.
- Use specific haemostatic gauze such as Surgicel to prevent post-operative bleeding.
Diagnosis of White Plaques (Q2):
- Likely diagnosis: Uraemic stomatitis.
- No treatment is required for these plaques.
- Differential: If plaques rub off, consider Candida. Treatment: Antifungal agent (e.g., fluconazole). Culture and sensitivity should guide therapy
- Miconazole may also be used for Candida, but ensure careful monitoring of drug interactions.
Summary of Dental Considerations for Renal Patients30
-
Renal patients may have impaired drug excretion. Drugs for sedation and GA should be used with caution in consultation with a physician.
-
Renal disease influences the use of NSAIDs and certain antimicrobials.
-
Platelet dysfunction may cause a bleeding tendency.
-
Dental treatment should ideally be carried out the day after dialysis.
-
Surgically created arterio-venous fistulas should not be used for venepuncture by the dentist.
-
Kidney transplant patients may require corticosteroid cover.
-
Anticoagulation therapy may increase bleeding risk.
-
Cyclosporin use may lead to gingival hyperplasia.
-
Immunosuppression makes patients prone to infection.
-
Maintain meticulous oral hygiene to prevent infections in immunosuppressed patients.
-
Always consult the patient's physician before prescribing any new medications.
Nutritional Deficiencies and Oral Health
Nutrition is defined by the W.H.O as the “intake of food considered in relation to the body’s dietary needs.”
Impact of Nutrition on Oral Health31
- Malnutrition can significantly affect oral health.
- Poor oral health in turn can result in malnutrition.
- Dietary recommendations for intake of both macro and micronutrients differ for various population sub-types.
Consequences of Nutritional Deficiencies
Nutritional deficiencies can lead to:
- Disease progression through altered tissue homeostasis.
- Reduced resistance to microbial biofilm.
- Decrease in tissue healing.
- General symptoms include glossitis (sore, red tongue), angular stomatitis, and recurrent aphthous ulcers.
Vitamin Deficiencies32
| Vitamin Deficiencies | Systemic Effects | Oral Effects |
|---|---|---|
| Vitamin A | Night blindness, Xerophthalmia | Decreases epithelial tissue development; may contribute to leukoplakia/cancer |
| Vitamin B1 (Thiamine) | Neuritis, cardiac failure | Cracked lips? |
| Vitamin B2 (Riboflavin) | Dermatitis | Angular stomatitis, glossitis |
| Vitamin B3 (Niacin) | Dermatitis, CNS disease | Glossitis, stomatitis and gingivitis |
| Vitamin B12 | Pernicious anaemia | Glossitis, aphthae |
| Folic acid | Macrocytic anaemia | Glossitis, aphthae |
| Vitamin C | Scurvy (purpura, delayed wound healing, bone lesions in children) | Gingival swelling and bleeding |
| Vitamin D | Rickets | Hypocalcification of teeth |

Vitamin A
Vitamin A is a nutrient important for vision, growth, cell division, reproduction, and immunity. It possesses antioxidant properties.
Dietary Sources
- Found in many foods such as spinach, dairy products, and liver.
- Other sources rich in beta-carotene include green leafy vegetables and carrots.
Research Findings
- Acne: Large doses have shown no effect.
- Macular degeneration: May reduce risk by 25%.
- Cancer: Effects on lung and prostate cancer remain unclear.
- Measles: Shown to reduce death rates.
Effects of Deficiency
- Severe effects on secretory epithelium (observed in rats).
- Columnar cells become squamous and keratinised.
- Dental development is severely affected.
- Note: There is no evidence in humans for these specific cellular changes.
Clinical Applications and Studies
- Treatment of keratotic plaques (leukoplakia) with retinoids (Vitamin A derivatives).
- Retinoid drugs have toxic side effects.
- Epidemiological studies suggest low Vitamin A intake is associated with oral and other cancers.
Vitamin B Complex
Riboflavin (B2) Deficiency
- Often results from malabsorption syndrome.
- Severe cases: Angular stomatitis, characterized by painful red fissures at the angles of the mouth.
- The tongue may appear "magenta" (purplish-red) in color.
- Glossitis: The tongue becomes magenta in color and granular.
- Treatment: Resolution follows after administering riboflavin (5 mg 1 tds).
Nicotinamide (B3) Deficiency (Pellagra)
- Affects the skin, GI tract, and nervous system.
- General symptoms include weakness, loss of appetite, and changes in mood.
Oral Manifestations of Pellagra
- Glossitis: The tip and lateral margins of the tongue appear red and swollen.
- Tongue Appearance: The dorsum of the tongue is coated with thick, greyish fur.
- Gingiva: Gingival margins are red, swollen, and ulcerated.
Aetiology of Vitamin B12 Deficiency
- Autoimmune: Pernicious anemia is an autoimmune condition in which antibodies to intrinsic factor are produced.
- Malabsorption: Parietal cells in the stomach produce intrinsic factor; therefore, any patient with a history of gastric bypass surgery may be at risk for developing a B12 deficiency.
- Dietary Insufficiency: Observed in vegans.
Folic acid deficiency
- Can result from malnutrition, anticonvulsant therapy, pregnancy, and alcoholism.
- Women are advised to take folic acid supplements to reduce the risk of neural tube defects.
- Supplementation may also reduce the risk of orofacial clefts.
Combined B12 and Folic Acid Deficiency
Oral manifestations include:
- Glossitis
- Raw beefy tongue
- Recurrent aphthous ulcers.
- The tongue often appears smooth and shiny.
Vitamin D
Vitamin D is obtained mainly from exposure to sunlight and diet. A rich source of Vitamin D is fish liver oils.
Clinical Implications of Deficiency
- Causes rickets during skeletal development.
- In severe cases, induces defective tooth mineralization.
- Associated with a higher prevalence of periodontitis and gingival inflammation.
- May be linked to osteonecrosis of the jaws.
- Potentially linked to oral cancer development.
Vitamin C
Vitamin C deficiency leads to Scurvy, which was once common among crews of sailing ships.
Prevalence and Risk Groups
- Rarely seen today.
- Cases still occur in elderly, neglected, and younger patients with markedly restricted diets.
Manifestations
- Skin: Capillary fragility and spontaneous bruising.
- Oral:
- Friable, swollen, bleeding gingiva.
- Marked false pocketing.
- Mobility of teeth.
Mineral Deficiencies
Iron Deficiency
Systemic Symptoms
- Fatigued, listless, and weak.
- Short of breath, dizzy, and light-headed.
- Struggling to concentrate.
- Increased susceptibility to infections.
- Decreased libido.
Oral Findings
- Depapillated atrophic tongue.
- Glossodynia (burning sensation).
- Candidiasis / angular cheilitis.
- Aphthous-like ulcers.
Tongue Manifestations
- Glossitis
- Smooth, depapillated tongu
- Increased susceptibility to Oral Candida infections.e
Eating Disorders
Anorexia Nervosa33
- Characteristics: Food avoidance, being underweight, distorted body image, and fear of obesity.
- Associated Medical Conditions: Renal failure, liver dysfunction, dehydration, and depression.
Oral and Clinical Findings
- Patients often present to the clinic due to general nutritional deficiencies (e.g., stomatitis).
- Parotid gland swelling.
- Acid erosion of dental hard tissues.
- Xerostomia (dry mouth).
Bulimia34
- Affects roughly 2% of young adult women.
- Characterized by binge eating alternating with self-induced vomiting or purging.
- Associated with psychiatric or psychological problems.
- Patients typically maintain a normal body weight.
Medical and Dental Complications
- Frequent vomiting and misuse of laxatives cause potassium depletion.
- Hypokalaemia: Predisposes the patient to myocardial instability.
- Erosion: Oesophageal and dental hard tissue erosions are common.
- Severe acid erosion of dental hard tissues is specifically known as perimylolysis.
- Soft tissue irritation in the oral cavity.
Dentist's Role
Dentists play a crucial role in identifying eating disorders early and should liaise with the patient's GP for comprehensive care.
Footnotes
-
Original PDF page 1: L24 Renal disease and nutritional deficiencies, p.1 ↩
-
Original PDF page 2: L24 Renal disease and nutritional deficiencies, p.2 ↩
-
Original PDF page 3: L24 Renal disease and nutritional deficiencies, p.3 ↩
-
Original PDF page 4: L24 Renal disease and nutritional deficiencies, p.4 ↩
-
Original PDF page 5: L24 Renal disease and nutritional deficiencies, p.5 ↩
-
Original PDF page 6: L24 Renal disease and nutritional deficiencies, p.6 ↩
-
Original PDF page 7: L24 Renal disease and nutritional deficiencies, p.7 ↩
-
Original PDF page 8: L24 Renal disease and nutritional deficiencies, p.8 ↩
-
Original PDF page 9: L24 Renal disease and nutritional deficiencies, p.9 ↩
-
Original PDF page 10: L24 Renal disease and nutritional deficiencies, p.10 ↩
-
Original PDF page 11: L24 Renal disease and nutritional deficiencies, p.11 ↩
-
Original PDF page 12: L24 Renal disease and nutritional deficiencies, p.12 ↩
-
Original PDF page 13: L24 Renal disease and nutritional deficiencies, p.13 ↩
-
Original PDF page 14: L24 Renal disease and nutritional deficiencies, p.14 ↩
-
Original PDF page 15: L24 Renal disease and nutritional deficiencies, p.15 ↩
-
Original PDF page 18: L24 Renal disease and nutritional deficiencies, p.18 ↩
-
Original PDF page 20: L24 Renal disease and nutritional deficiencies, p.20 ↩
-
Original PDF page 21: L24 Renal disease and nutritional deficiencies, p.21 ↩
-
Original PDF page 22: L24 Renal disease and nutritional deficiencies, p.22 ↩
-
Original PDF page 23: L24 Renal disease and nutritional deficiencies, p.23 ↩
-
Original PDF page 24: L24 Renal disease and nutritional deficiencies, p.24 ↩
-
Original PDF page 25: L24 Renal disease and nutritional deficiencies, p.25 ↩
-
Original PDF page 29: L24 Renal disease and nutritional deficiencies, p.29 ↩
-
Original PDF page 30: L24 Renal disease and nutritional deficiencies, p.30 ↩
-
Original PDF page 31: L24 Renal disease and nutritional deficiencies, p.31 ↩
-
Original PDF page 32: L24 Renal disease and nutritional deficiencies, p.32 ↩
-
Original PDF page 33: L24 Renal disease and nutritional deficiencies, p.33 ↩
-
Original PDF page 34: L24 Renal disease and nutritional deficiencies, p.34 ↩
-
Original PDF page 35: L24 Renal disease and nutritional deficiencies, p.35 ↩
-
Original PDF page 36: L24 Renal disease and nutritional deficiencies, p.36 ↩
-
Original PDF page 37: L24 Renal disease and nutritional deficiencies, p.37 ↩
-
Original PDF page 38: L24 Renal disease and nutritional deficiencies, p.38 ↩
-
Original PDF page 50: L24 Renal disease and nutritional deficiencies, p.50 ↩
-
Original PDF page 51: L24 Renal disease and nutritional deficiencies, p.51 ↩