Implications of Neurological Diseases to the Oral Health Care Provider
Presentation Overview1
This presentation addresses the clinical implications and management strategies for patients presenting with neurological diseases within a dental and oral health care setting.
Lecture Focus
This lecture focuses on the definitions, clinical manifestations, and specific dental management protocols for the four major neurological conditions listed below.
Presenter Information
- Specialist: Dr. Guru O
- Department: Oral Medicine
Topics to Cover2
The following neurological conditions and their implications for oral health care providers will be addressed:
- Epilepsy
- Multiple sclerosis
- Parkinson’s disease
- Stroke / cerebrovascular accident
Epilepsy3
Epilepsy is a chronic neurological disorder characterized by recurrent, unprovoked seizures.
Definitions and Epidemiology
Core Definitions4
- Seizure: A paroxysmal alteration of neurologic function caused by the excessive, hypersynchronous discharge of neurons in the brain.
- Epilepsy: The condition of recurrent, unprovoked seizures.
- Epilepsy Syndrome: A group of clinical characteristics that consistently occur together.
Causes of Seizures
- Epileptic seizures: Resulting from abnormal neuronal firing.
- Non-epileptic seizures: Resulting from reversible or secondary causes, such as psychogenic seizures, hypoglycemia, or fever.
Statistical Overview5
- Gender: Slight male predilection.
- Age: 75% of cases begin in childhood.
- Incidence: 61.4 new cases per 100,000 persons per year.
- Prevalence:
- 1% of the general population.
- 0.33% suffer from refractory epilepsy (epilepsy not controlled by more than two anti-epileptic drugs [AEDs]).
Diagnosis and Classification
ILAE Categories of Seizures6
According to the International League Against Epilepsy (ILAE), seizures are categorized based on their origin:
- Generalised: Originate from bilateral distributed neuronal networks.
- Focal (formerly Partial): Originate from neuronal networks limited to part of one cerebral hemisphere.
- Spasms.
Key Characteristics
- Seizures can begin focally and later generalize.
- Seizures can originate in the cerebral cortex or subcortical structures.
Detailed Seizure Classification7
- Generalised Seizures
- Absence (petit mal): Characterized by unresponsiveness to external verbal stimuli, sometimes accompanied by eye blinking or head nodding.
- Generalised tonic-clonic (GTC) (grand mal): Bilateral symmetric convulsive movements of all limbs with impairment of consciousness.
- Myoclonic: Sudden, brief (lightning-fast) movements not associated with obvious disturbance of consciousness; can be general or focal.
- Atonic: Involves the loss of body tone, often resulting in a head drop or fall.
- Focal Seizures
- Clinical manifestations depend on the specific area of the cortex involved.
- Occipital lobe involvement may cause visual phenomena
- Post-central gyrus involvement may cause paresthesia
- Epileptic Spasms
- Sudden extension or flexion of extremities, held for several seconds, typically occurring in clusters.
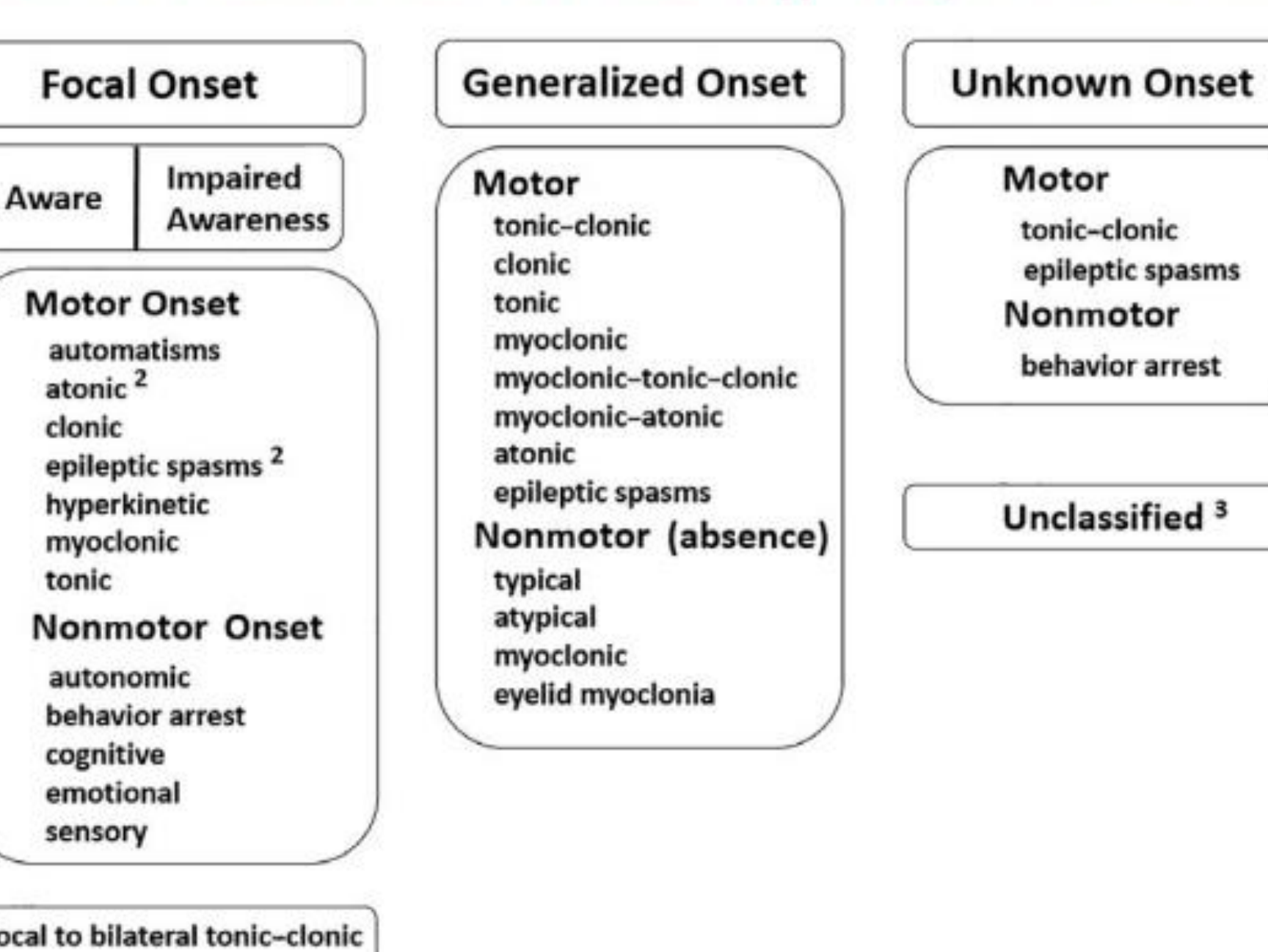
ILAE 2017 Classification of Seizure Types (Expanded)8
| Focal Onset | Generalized Onset | Unknown Onset |
|---|---|---|
| Aware / Impaired Awareness | ||
| Motor Onset | Motor | Motor |
| - Automatisms | - Tonic-clonic | - Tonic-clonic |
| - Atonic | - Clonic | - Epileptic spasms |
| - Clonic | - Tonic | |
| - Epileptic spasms | - Myoclonic | |
| - Hyperkinetic | - Myoclonic-tonic-clonic | |
| - Myoclonic | - Myoclonic-atonic | |
| - Tonic | - Atonic | |
| Nonmotor Onset | Nonmotor (absence) | Nonmotor |
| - Autonomic | - Typical | - Behavior arrest |
| - Behavior arrest | - Atypical | |
| - Cognitive | - Myoclonic | |
| - Emotional | - Eyelid myoclonia | |
| - Sensory |
Diagnostic Protocols9
- Clinical Assessment: Comprehensive history and physical examination.
- Electroencephalogram (EEG): Preferably capturing wakefulness, drowsiness, and sleep.
- Neuroimaging:
- MRI: Standard imaging modality.
- CT: Useful in acute settings to detect hemorrhage, calcification, or tumors.
- Laboratory Testing: Metabolic evaluation and genetic testing.
Comorbidities
Psychiatric and Developmental Comorbidities10
- Common comorbidities include depression, anxiety, learning disabilities, ADHD, intellectual disability, and autism.
- These conditions are now recognized as integral parts of the seizure disorder rather than merely secondary effects of medication or uncontrolled seizures; they may even precede the onset of seizures.
Dental Chairside Management
Pre-operative and Procedural Precautions11
- Obtain a thorough medical history, specifically the level of seizure control.
- Determine the patient’s "normal" seizure pattern and parameters to better recognize deviations
- Place a ligated mouth prop at the beginning of the procedure.
- Utilize the supine position.
Management of Intra-operative Seizures
- Clear the immediate area of hazards.
- Turn the patient to their side to prevent aspiration.
- Provide passive restraint (do not use force).
Post-seizure Protocol
- Examine the patient for traumatic injuries.
- Discontinue dental treatment and arrange for safe transport.
- If it is the patient’s first seizure, they must be evaluated in an emergency room.
Seizure Duration and Status Epilepticus12
Most tonic-clonic seizures resolve within 1–2 minutes, followed by a post-ictal phase.
Status Epilepticus is defined as an emergency occurring when:
- The active part of a tonic-clonic seizure lasts 5 minutes or longer.
- A person experiences a second seizure without recovering consciousness from the first.
- Repeated seizures occur for 30 minutes or longer.
Risks of Status Epilepticus
Status epilepticus carries significant risks including cardiac damage, arrhythmia, respiratory failure, hypoxia, and aspiration pneumonia.
Non-convulsive Status Epilepticus13
- Characterized by prolonged or repeated absence or complex partial seizures.
- The patient may appear confused or lack full awareness but is not “unconscious” in the traditional tonic-clonic sense.
- Recognition is difficult as symptoms are subtle and may mimic the recovery period.
- Emergency designation depends on the individual’s typical seizure patterns and frequency.
Multiple Sclerosis14
Multiple Sclerosis (MS) is a chronic, inflammatory, demyelinating disease of the central nervous system.
Definition and Epidemiology
Definition15
MS is an autoimmune disease of the Central Nervous System (CNS) characterized by inflammation, axonal injury, demyelination, gliosis, and neuronal loss.
Epidemiology
- Gender: 3:1 female-to-male ratio.
- Age: Onset typically occurs between 20–40 years; however, 10% of cases present before age 18.
- Race and Geography:
- Higher prevalence in European populations compared to East Asian or African descent.
- Latitude-based prevalence: Higher incidence in northern latitudes of Europe and the United States.
Etiology and Pathogenesis
Risk Factors and Etiology16
- Genetic Susceptibility: Associated with HLA-DRB1*15.
- Epstein-Barr Virus (EBV): Symptomatic infection increases MS risk, likely through molecular mimicry.
- Environmental Factors:
- Vitamin D deficiency (related to UVB exposure).
- Historical latitude trends (though these are currently decreasing).
- Gender Trends: The increasing female-to-male ratio since the early 1900s has been partially attributed to smoking habits.
Pathological Hallmarks17
- Demyelinating Plaques: Perivenular inflammatory lesions found commonly in the periventricular area, pons, and spinal cord.
- Inflammatory Infiltrates: Predominantly composed of CD8+ T lymphocytes, with smaller numbers of B cells and plasma cells.
- Neurodegeneration: Microscopic damage to axons, neurons, and synapses throughout the CNS.
Clinical Features and Classification
Clinical Features Prevalence18
| Feature | Percentage |
|---|---|
| Numbness / Tingling | 63.5% |
| Walking difficulty | 48.9% |
| Vision problems | 40.2% |
| Fatigue | 40.1% |
| Weakness | 25.3% |
| Dizziness | 23.2% |
| Pain | 19.3% |
| Muscle Spasms | 17.2% |
| Depression | 14.7% |
| Cognitive dysfunction | 13.4% |
| Bladder dysfunction | 11.1% |
| Bowel dysfunction | 5.7% |
- Dysesthesia
- Anxiety
- Dysphagia

Disease Classifications19
- Relapsing-remitting (RR): (70-80% of cases) New or recurrent neurological symptoms lasting 24–48 hours, developing over days to weeks.
- Primary progressive (PP): (15-20% of cases) Gradual deterioration from onset without distinct relapses.
- Secondary progressive (SP): Gradual neurological decline following an initial relapsing course.
- Progressive relapsing (PR): (5% of cases) Gradual deterioration with superimposed relapses.
- Fulminant: Severe course with multiple relapses and rapid progression.
- Benign: Mild disability with rare relapses.
Diagnosis
Diagnosis is based on clinical history, physical examination, and MRI findings.
Management and Prognosis
Acute and Long-term Management20
- Short-term Goals: Decrease MRI lesion activity and address triggers (infection/metabolic issues).
- Acute Flare Management:
- IV Methylprednisolone: 500–1000mg daily for 3–7 days.
- Oral Prednisone: 1250mg/day.
- Plasmapheresis (PLEX): 3–7 treatments every other day.
- Long-term Goals: Prevent progression using Disease-Modifying Therapies (DMTs) such as Glatiramer acetate, interferon beta, natalizumab, mitoxantrone, and fingolimod.
- Symptomatic management and prevention of progression to secondary MS
- Challenges: Patient compliance and monitoring for drug toxicity.
Prognosis and Complications21
While MS causes significant functional deterioration, mortality is usually due to secondary complications rather than the disease itself:
- Infections (Respiratory and Urinary Tract).
- Aspiration pneumonia (due to dysphagia).
- Chronic respiratory disease.
- Sepsis.
- Skin disease.
Dental Management and Oral Manifestations
Oral Manifestations (2-3% of patients)22
- Facial Pain:
- Trigeminal Neuralgia (TN): Occurs in 5% of MS patients; may lack trigger zones and present as continuous lower-intensity pain.
- Trigeminal Neuropathies: Burning, tingling, or reduced sensation in V2 and V3 distributions.
- Motor and Sensory Disturbances:
- Dysarthria: “Scanning speech” (slow, irregular speech with separated syllables).
- Facial Myokymia: Wave-like muscle undulations (“bag of worms” sensation) during attacks.
- Facial paresthesia and muscle weakness.
- **Visual disturbances
- Reduced facial sensation
- Vertigo**.
Dental Treatment Considerations23
- Scheduling: Perform elective care during periods of remission. Morning appointments are preferred due to afternoon fatigue.
- Clinical Management:
- Monitor for opportunistic infections (e.g., Candidosis) following high-dose corticosteroid use.
- Manage xerostomia and medication-induced hyposalivation.
- Keep appointments short; advanced stages may require General Anesthesia (GA).
Parkinsons Disease24
Parkinson’s Disease (PD) is a progressive neurodegenerative movement disorder.
Description and Epidemiology
Epidemiology25
- Gender: More common in males.
- Age: Incidence increases with age, though 25% of patients are under 65 (Young Onset).
- Prevalence:
- 150,000 patients in Australia.
- Second most common neurological disease after dementia.
- Global burden has doubled in the last 20 years.
Etiology and Pathogenesis
Etiological Factors26
- Genetic Factors: Mutations in SNCA, LRRK2, PRKN, PINK1, and GBA.
- Environmental Risks: Pesticide exposure, head injuries, and Traumatic Brain Injury (TBI). Possible links to COVID-19 are being explored.
- Negative Associations (Protective Factors):
- Smoking (linked to high dopamine levels).
- Coffee consumption.
- Use of anti-inflammatory drugs.
- High plasma urate levels.
- Physical activity.
Pathogenesis27
The disease involves a complex interaction resulting in the accelerated death of dopaminergic neurons and disruption of motor/non-motor circuits, driven by:
- Alpha-synuclein aggregation.
- Mitochondrial and lysosomal dysfunction.
- Vesicle and synaptic transport issues.
- Neuroinflammation.
Management and Prognosis
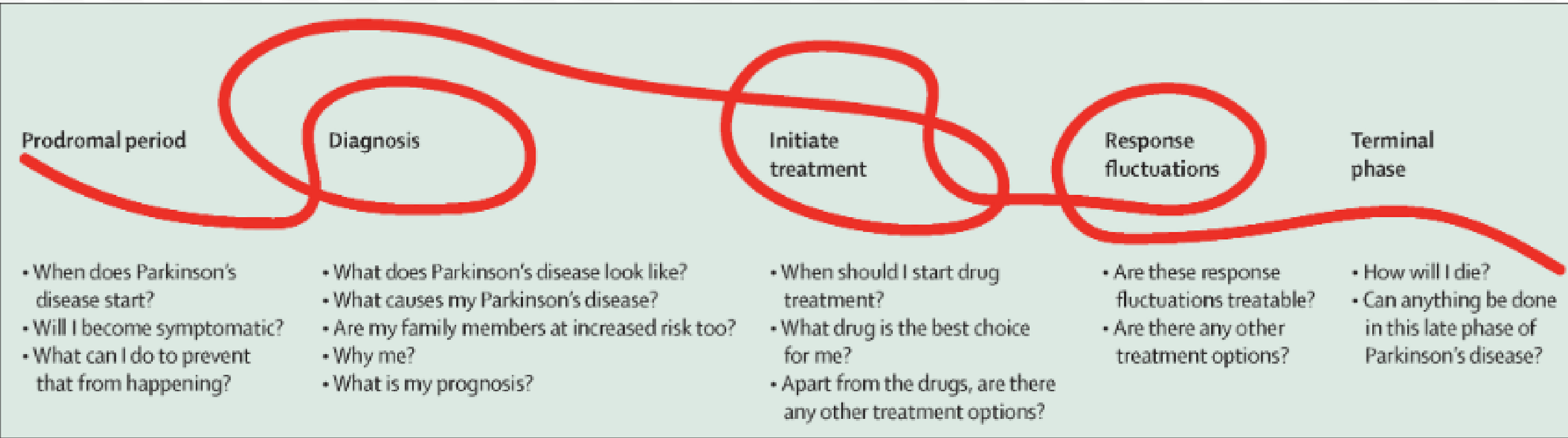
Clinical Phases and Patient Concerns28
- Prodromal Period: Focus on prevention and symptom onset.
- Diagnosis: Focus on cause, prognosis, and familial risk.
- Initiate Treatment: Selection of drug therapies and non-pharmacological options.
- Response Fluctuations: Management of treatment-related motor fluctuations.
- Terminal Phase: End-of-life care and late-stage management.
Oral Manifestations
Hard Tissue and Muscular Issues29
- Caries and Periodontal Disease: Increased risk due to motor impairment, apathy, depression, and dementia affecting oral hygiene.
- Mastication Disorders: Impaired chewing and facial movements in moderate-to-advanced stages.
- Bruxism: Higher prevalence of rhythmic masticatory muscle activity during both REM and nREM sleep.
Salivary Issues30
- Sialorrhea and Drooling: Primarily caused by decreased clearance of saliva (dysphagia) rather than overproduction.
- Angular Cheilitis: Often secondary to chronic drooling.
Sensory and Secretory Disturbances31
- Xerostomia: Primarily drug-induced (TCAs, antipsychotics, anticholinergics, beta-blockers).
- Taste Disturbances: Frequency increases with disease progression. Potential causes include CNS degeneration, poor oral hygiene, zinc deficiency, and medications.
Burning Mouth Syndrome (BMS)32
- Reported prevalence varies significantly (1.9% to 24%).
- Clinical studies suggest the prevalence is actually low (1%–5.4%), similar to the general population.
- Many cases may be misdiagnosed xerostomia or ill-fitting dentures.
- There is a possible link between BMS symptoms and high-dose Levodopa therapy.
Dental Management
Clinical Management33
- Hygiene: Rigorous plans involving caregivers; tailored recall intervals.
- Pharmacological Interactions:
- COMT Inhibitors (e.g., Entacapone): Limit epinephrine in local anesthesia to two cartridges (36 micrograms).
- Dopamine Agonists (e.g., Pramipexole): Interacts with erythromycin.
- Safety: Monitor for orthostatic hypotension; incline the dental chair slowly.
- Scheduling: Time appointments 1–3 hours after medication intake for maximum effect.
Stroke and Cerebrovascular Accident34
Stroke, or Cerebrovascular Accident (CVA), is a critical condition resulting from disrupted blood flow to the brain.
Definition and Risk Factors
Definition35
A sudden interruption of oxygenated blood to the brain, leading to ischemic injury and focal necrosis.
- Causes: Thrombosis, emboli, or hemorrhage.
Risk Factors
- Hypertension and Congestive Heart Failure.
- Diabetes Mellitus.
- Previous CVA or Transient Ischemic Attacks (TIAs).
- Age > 75 years.
- Hypercholesterolemia and Coronary Atherosclerosis.
- Smoking.
Complications and Oral Manifestations
Mortality and Disability Outcomes36
- Mortality Rates:
- Ischemic stroke: 8%
- Hemorrhagic stroke: 38–47%
- Overall: 23% die within the first year.
- Recovery Statistics:
- 10% full recovery.
- 50% mild residual disability.
- 15–30% severe disability.
- 10–20% require institutional care.
Oral and Neurological Manifestations37
- Slurred speech and difficulty swallowing.
- Unilateral facial paralysis and loss of sensation.
- Weakened musculature.
- Impaired ability to maintain oral hygiene due to motor deficits.
Dental Implications and Communication
Dental Treatment Modifications38
- Stability: Defer elective treatment until the patient is medically stable.
- Appointment Management: Short, stress-free appointments with good anxiety control.
- Anxiety control is particularly important to manage hypertension in these patients.
- Physical Assistance: Help with maneuvering in the chair and modified oral hygiene instructions.
- Pharmacology: Be aware of antiplatelet or anticoagulant therapy (e.g., Warfarin) and potential drug interactions.
Communication Strategies39
- Face the patient directly and do not wear a mask while speaking.
- Removing the mask allows the patient to utilize lip-reading to aid comprehension.
- Use slow, deliberate speech and drawings for explanations.
- Seek immediate feedback to ensure understanding.
- Communicate with personal caregivers.
- Avoid underestimating or overestimating the patient’s cognitive or physical abilities.
References4041
-
Abe S., Gagnon J.-F., Montplaisir J. Y., Postuma R. B., Rompré P. H., Huynh N. T., Kato T., Kawano F., and Lavigne G. J., Sleep bruxism and oromandibular myoclonus in rapid eye movement sleep behavior disorder: a preliminary report, Sleep Medicine. (2013) 14, no. 10, 1024–1030, 2-s2.0-84883826735.
-
Armstrong MJ, Okun MS. Diagnosis and Treatment of Parkinson Disease: A Review. JAMA. 2020 Feb 11;323(6):548-560. doi: 10.1001/jama.2019.22360. PMID: 32044947.
-
Beghi E. The Epidemiology of Epilepsy. Neuroepidemiology. 2020;54(2):185-191. doi: 10.1159/000503831. Epub 2019 Dec 18. PMID: 31852003.
-
Bloem BR, Okun MS, Klein C. Parkinson’s disease. Lancet. 2021 Jun 12;397(10291):2284-2303. doi: 10.1016/S0140-6736(21)00218-X. Epub 2021 Apr 10. PMID: 33848468.
-
Dobson R, Giovannoni G. Multiple sclerosis - a review. Eur J Neurol. 2019 Jan;26(1):27-40. doi: 10.1111/ene.13819. Epub 2018 Nov 18. PMID: 30300457.
-
Fisher RS, Cross JH, French JA, Higurashi N, Hirsch E, Jansen FE, Lagae L, Moshé SL, Peltola J, Roulet Perez E, Scheffer IE, Zuberi SM. Operational classification of seizure types by the International League Against Epilepsy: Position Paper of the ILAE Commission for Classification and Terminology. Epilepsia. 2017 Apr;58(4):522-530. doi: 10.1111/epi.13670. Epub 2017 Mar 8. PMID: 28276060.
-
Harding K, Zhu F, Alotaibi M, Duggan T, Tremlett H, Kingwell E. Multiple cause of death analysis in multiple sclerosis: A population-based study. Neurology. 2020 Feb 25;94(8):e820-e829. doi: 10.1212/WNL.0000000000008907. Epub 2020 Jan 13. PMID: 31932517; PMCID: PMC7136054.
-
Kalf JG, Bloem BR, Munneke M. Diurnal and nocturnal drooling in Parkinson’s disease. J Neurol. 2012 Jan;259(1):119-23. doi: 10.1007/s00415-011-6138-2. Epub 2011 Jun 23. PMID: 21698387; PMCID: PMC3251785.
-
Little J, Miller C, Rhodus N. Little and Falace’s Dental Management of the Medically Compromised Patient. 9 ed: Elsevier Health Sciences; 2018.
-
O G, Balasubramaniam R, Klasser GD. Burning mouth disorder and Parkinson’s disease: A scoping review of the literature. J Oral Rehabil. 2023 Jun;50(6):488-500. doi: 10.1111/joor.13443. Epub 2023 Mar 22. PMID: 36855821.
-
Parkinsons UK, 2024, ‘Mouth and dental issues’, accessed 19.09.2024, URL: https://www.parkinsons.org.uk/information-and-support/mouth-and-dental-issues
-
Rana AQ, Yousuf MS, Awan N, Fattah A. Impact of progression of Parkinson’s disease on drooling in various ethnic groups. Eur Neurol. 2012;67(5):312-4. doi: 10.1159/000336054. Epub 2012 Apr 20. PMID: 22517489.
-
Stafstrom CE, Carmant L. Seizures and epilepsy: an overview for neuroscientists. Cold Spring Harb Perspect Med. 2015 Jun 1;5(6):a022426. doi: 10.1101/cshperspect.a022426. PMID: 26033084; PMCID: PMC4448698.
-
Tafti D, Ehsan M, Xixis KL. Multiple Sclerosis. [Updated 2024 Mar 20]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK499849/
-
USF Health (2024), ‘Symptoms of MS’, accessed 19.09.2024, URL: https://health.usf.edu/medicine/neurology/multiple-sclerosis/symptoms-ms
-
Wylie T, Sandhu DS, Murr NI. Status Epilepticus. [Updated 2023 May 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430686/
-
Zlotnik Y, Balash Y, Korczyn AD, Giladi N, Gurevich T. Disorders of the oral cavity in Parkinson’s disease and parkinsonian syndromes. Parkinsons Dis. 2015;2015:379482. doi: 10.1155/2015/379482. Epub 2015 Jan 15. PMID: 25685594; PMCID: PMC4312641.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Parkinson’s Disease
Description and Epidemiology
Epidemiology
- Progressive movement disorder; second most common neurological disease after dementia.
- More prevalent in males; incidence increases with age.
Etiology and Pathogenesis
Etiological Factors
- Risk Factors: Genetics, pesticides, head/traumatic brain injury.
- Protective Factors: Smoking, coffee, anti-inflammatory drugs, and physical activity (linked to higher dopamine levels).
Pathogenesis
- Death of dopaminergic neurons, which are critical for motor control.
Management and Prognosis
Clinical Phases and Patient Concerns
- Treatment ranges from pharmacotherapy (Levodopa) to neurosurgery.
- Treatment is highly heterogeneous and tailored to individual needs.
Oral Manifestations
Hard Tissue and Muscular Issues
- Increased risk of caries and periodontal disease (due to motor impairment and reliance on caregivers).
- Bruxism: High prevalence of rhythmic masticatory muscle activity.
Salivary Issues
- Sialorrhea (Drooling): Usually due to decreased clearance (dysphagia) rather than overproduction.
- Angular Cheilitis: High incidence due to constant moisture from drooling.
- Xerostomia: Often a side effect of medications.
Sensory and Secretory Disturbances
- Taste Disturbances: Higher frequency due to CNS degeneration, poor hygiene, or medications.
Burning Mouth Syndrome (BMS)
- Recent epidemiological data suggests the association between BMS and Parkinson’s is weak; there is no significant difference in prevalence compared to the general population.
Dental Management
Clinical Management
- Medication Interactions:
- COMT Inhibitors: Theoretically interact with Epinephrine in LA (though no reports exist; use caution).
- Dopamine Agonists (e.g., Pramipexole): Interact with Erythromycin.
- Orthostatic Hypotension: Incline the chair slowly, especially for patients on COMT inhibitors.
- Appointment Timing: Schedule 1–3 hours after medication intake (peak effect).
Footnotes
-
Original PDF page 1: L25 Neurological diseases, p.1 ↩
-
Original PDF page 2: L25 Neurological diseases, p.2 ↩
-
Original PDF page 3: L25 Neurological diseases, p.3 ↩
-
Original PDF page 4: L25 Neurological diseases, p.4 ↩
-
Original PDF page 5: L25 Neurological diseases, p.5 ↩
-
Original PDF page 6: L25 Neurological diseases, p.6 ↩
-
Original PDF page 7: L25 Neurological diseases, p.7 ↩
-
Original PDF page 8: L25 Neurological diseases, p.8 ↩
-
Original PDF page 9: L25 Neurological diseases, p.9 ↩
-
Original PDF page 10: L25 Neurological diseases, p.10 ↩
-
Original PDF page 11: L25 Neurological diseases, p.11 ↩
-
Original PDF page 12: L25 Neurological diseases, p.12 ↩
-
Original PDF page 13: L25 Neurological diseases, p.13 ↩
-
Original PDF page 14: L25 Neurological diseases, p.14 ↩
-
Original PDF page 15: L25 Neurological diseases, p.15 ↩
-
Original PDF page 16: L25 Neurological diseases, p.16 ↩
-
Original PDF page 17: L25 Neurological diseases, p.17 ↩
-
Original PDF page 18: L25 Neurological diseases, p.18 ↩
-
Original PDF page 19: L25 Neurological diseases, p.19 ↩
-
Original PDF page 20: L25 Neurological diseases, p.20 ↩
-
Original PDF page 21: L25 Neurological diseases, p.21 ↩
-
Original PDF page 22: L25 Neurological diseases, p.22 ↩
-
Original PDF page 23: L25 Neurological diseases, p.23 ↩
-
Original PDF page 24: L25 Neurological diseases, p.24 ↩
-
Original PDF page 25: L25 Neurological diseases, p.25 ↩
-
Original PDF page 26: L25 Neurological diseases, p.26 ↩
-
Original PDF page 27: L25 Neurological diseases, p.27 ↩
-
Original PDF page 28: L25 Neurological diseases, p.28 ↩
-
Original PDF page 29: L25 Neurological diseases, p.29 ↩
-
Original PDF page 30: L25 Neurological diseases, p.30 ↩
-
Original PDF page 31: L25 Neurological diseases, p.31 ↩
-
Original PDF page 32: L25 Neurological diseases, p.32 ↩
-
Original PDF page 33: L25 Neurological diseases, p.33 ↩
-
Original PDF page 34: L25 Neurological diseases, p.34 ↩
-
Original PDF page 35: L25 Neurological diseases, p.35 ↩
-
Original PDF page 36: L25 Neurological diseases, p.36 ↩
-
Original PDF page 37: L25 Neurological diseases, p.37 ↩
-
Original PDF page 38: L25 Neurological diseases, p.38 ↩
-
Original PDF page 39: L25 Neurological diseases, p.39 ↩
-
Original PDF page 40: L25 Neurological diseases, p.40 ↩
-
Original PDF page 41: L25 Neurological diseases, p.41 ↩