Endocrine and Metabolic Disorders
Learning Outcomes1
- Understanding of the oral manifestations of systemic disease and care of the medically compromised patient
- Disorders affecting the:
- Pancreas – Diabetes Mellitus
- Adrenal Glands – Cushing’s syndrome, Addison’s disease
- Thyroid glands – Grave’s disease, Hashimoto’s thyroiditis
- Pituitary glands – Gigantism, Acromegaly
- Parathyroid glands – Hyperparathyroidism, Hypoparathyroidism
- Pregnancy
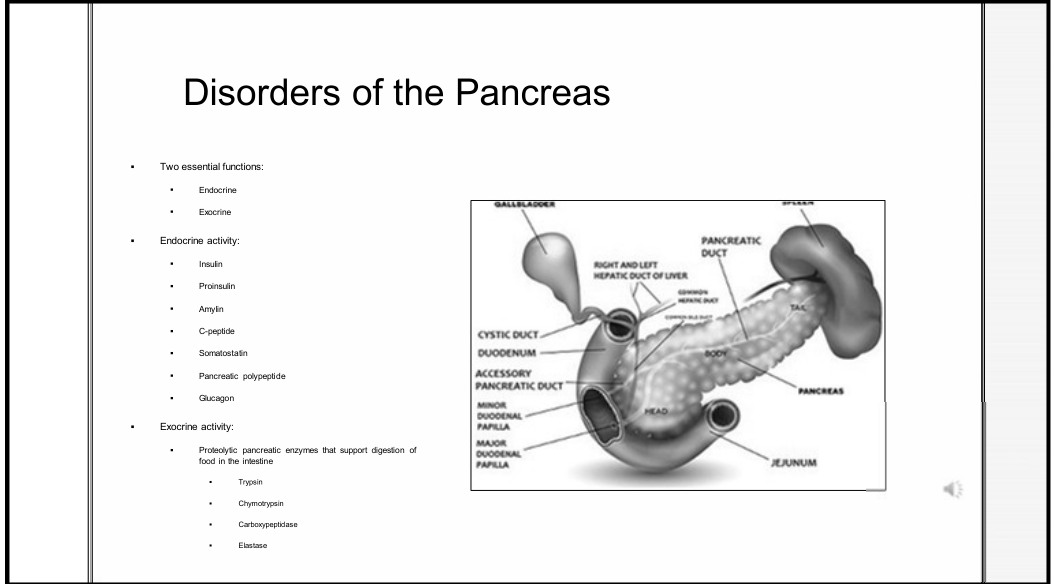
Disorders of the Pancreas
The pancreas performs two essential functions: endocrine and exocrine activity.
Endocrine Activity
The endocrine system involves the secretion of:
- The endocrine function is performed specifically by the Islets of Langerhans
- Insulin acts to lower blood sugar, while glucagon acts to raise blood sugar levels
- Insulin
- Proinsulin
- Amylin
- C-peptide
- Somatostatin
- Pancreatic polypeptide
- Glucagon
Exocrine Activity
The exocrine system involves proteolytic pancreatic enzymes that support the digestion of food in the intestine:
Exocrine Secretions
The exocrine system produces isoosmotic alkaline juices containing these proteolytic enzymes to facilitate digestion.
- Trypsin
- Chymotrypsin
- Carboxypeptidase
- Elastase
Disorders Affecting Pancreatic Functions
Inflammatory Diseases2
- Chronic and acute pancreatitis
- Chronic pancreatitis is the most common cause of exocrine pancreatic insufficiency in adults.
- Exocrine pancreatic insufficiency
- Pathophysiology: Enzymes produced by the pancreas start working before they reach the small intestine
- Inflammation in the gland disrupts insulin production
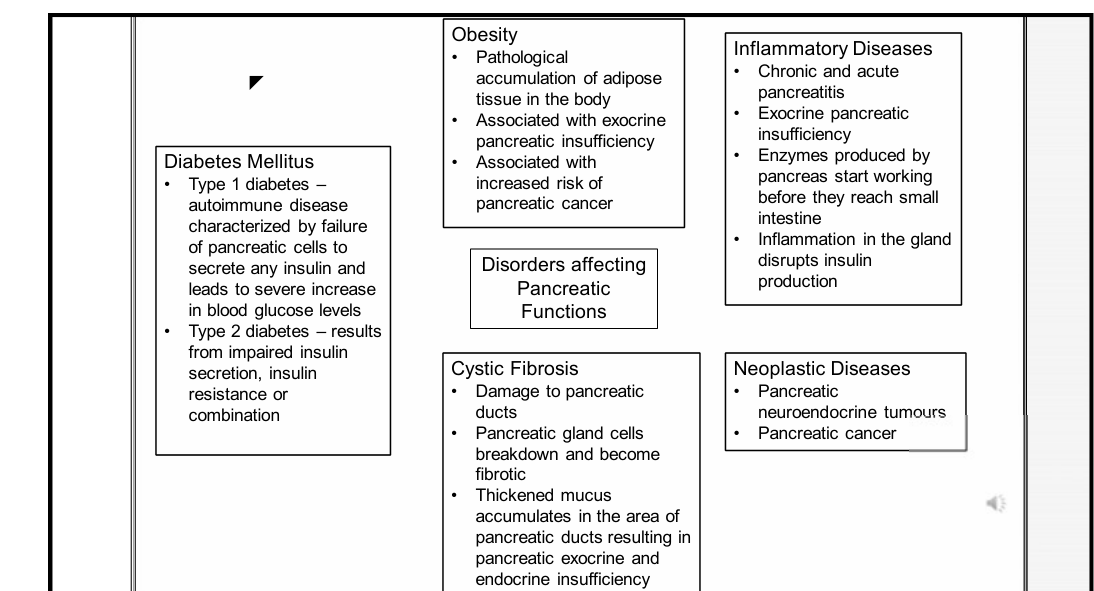 |  |
Neoplastic Diseases
- Pancreatic neuroendocrine tumours
- Pancreatic cancer
- Pancreatic cancer is often resistant to chemotherapy and radiation; early surgical intervention is rare due to late-stage diagnosis.
Cystic Fibrosis
- Damage to pancreatic ducts
- Pancreatic gland cells breakdown and become fibrotic
- Thickened mucus accumulates in the area of pancreatic ducts resulting in pancreatic exocrine and endocrine insufficiency
Obesity
- Pathological accumulation of adipose tissue in the body
- Associated with exocrine pancreatic insufficiency and increased risk of pancreatic cancer
- Obesity before age 50 is strongly correlated with an increased risk of death from pancreatic cancer.
Pancreatic Pathologies and Inflammation
Diabetes Mellitus Overview
- Metabolic disease characterized by an elevation of blood glucose levels.
- Mechanism: Pancreatic beta cells produce insulin which facilitates absorption of glucose into cells. DM occurs due to lack of insulin production or insulin sensitivity.
- Type 1 DM: Failure in insulin production resulting from destruction of pancreatic beta cells by T-cell mediated autoimmunity.
- Type 2 DM: Characterized by insulin resistance and reduction of insulin production.
- Long-term complications include neuropathy, retinopathy, and cardiovascular disease.
- Clinical Importance: Early diagnosis and management are essential to prevent or slow down potential complications.
Prevalence of Oral Manifestations
More than 90% of diabetic patients suffer from oral complications. Mechanisms include impaired neutrophil function, increased collagenase activity, reduction in collagen synthesis, microangiopathy, and neuropathy.
| Oral Manifestation | Prevalence in Controlled Type 2 Diabetes (%) | Prevalence in Uncontrolled Type 2 Diabetes (%) |
|---|---|---|
| Hyposalivation | 68 | 84 |
| Halitosis | 52 | 76 |
| Periodontitis | 32 | 48 |
| Burning mouth sensation | 32 | 24 |
| Candidiasis | 28 | 36 |
| Taste alteration | 28 | 44 |
Oral Manifestations of Diabetes Mellitus
Salivary Gland Hypofunction and Xerostomia3
- Prevalence: 52-76% (Xerostomia observed in up to 80% of cases).
- Highest level of hypofunction is observed in diabetics with poor glycaemic control.
- Reduced salivary flow results from polyuria and dehydration.
- Salivary Composition: Urea and glucose levels in saliva are significantly higher in DM patients.
- Impact: Salivary glucose promotes bacterial colonization and candida development; results in dysgeusia, dental caries, oral pain, dysphagia, and lower quality of life.
 |  |
 |
Dental Caries and Pulpal Pathology
- Increased incidence of new and recurrent dental caries due to reduced cleansing/buffering capacity of saliva and increased carbohydrate/yeast levels (Streptococci mutans and lactobacilli).
- Chronic hyperglycaemia may cause irreversible pulpitis.
- Higher prevalence of periapical lesions in poorly controlled diabetes with lower success rates for endodontic treatment.
Periodontal Disease
- Most common oral manifestation.
- Prevalence: Severe periodontitis in diabetic vs. non-diabetic patients is 59.6% vs. 39%.
- Mechanisms:
- Alterations in host defence (neutrophil dysfunction)
- Changes in subgingival microflora
- Altered collagen structure and metabolism
- Vascularity changes and gingival crevicular fluid alterations
- Two-way relationship: Elimination of pathogens reduces inflammation, which reduces insulin resistance and glucose levels.
Two-Way Relationship
Active periodontal infection worsens glycemic control by increasing insulin resistance, creating a cyclical effect with diabetes.
Oral Infections4
- Fungal and bacterial infections are common due to decreased salivary flow, impaired defense mechanisms, and poor metabolic control.
- Candida colonization: Higher in T1DM (84%) than T2DM (68%); non-diabetics at 27%.
- Common lesions: Denture stomatitis, angular cheilitis, and median rhomboid glossitis.
- Risk factors: Smoking, denture use, poor glycaemic control, steroids, and broad-spectrum antibiotics.
 |  |
Sensory and Mucosal Alterations
- Burning Mouth: Attributed to poor glycaemic control, metabolic alterations in mucosa, angiopathy, candida infection, and neuropathy.
- Taste Dysfunction: Sweet or salty taste disorders seen in poorly controlled diabetes; exacerbated by salivary dysfunction.
- Mucosal Changes: Coated or fissured tongue, recurrent aphthous stomatitis, and oral lichen planus/lichenoid reactions (though controversial
- Higher incidence of geographic tongue and Oral Lichen Planus is specifically noted in Type 1 diabetics.).
Wound Healing
- Delayed vascularization, diminished blood flow, and hypoxia.
- Reduction in innate immunity and growth factor production.
- Psychological stress also contributes to poor healing outcomes during oral surgeries.
Clinical Management of Diabetic Patients
Professional Responsibilities5
- Dentists must be familiar with diagnosis and prevention techniques for DM-related oral manifestations.
- Management requires cooperation between the patient, physician, and dentist.
- Regular check-ups facilitate anticipation of patient needs and inter-professional interaction.
- Clinical focus: Examination of mucosa, periodontal inflammation, bleeding, and general tooth state.
- Dentists should screen for diabetes in patients presenting with unexplained xerostomia or rapid periodontal destruction.
 |  |
Adrenal Gland Disorders
Pathophysiology and Prevalence6
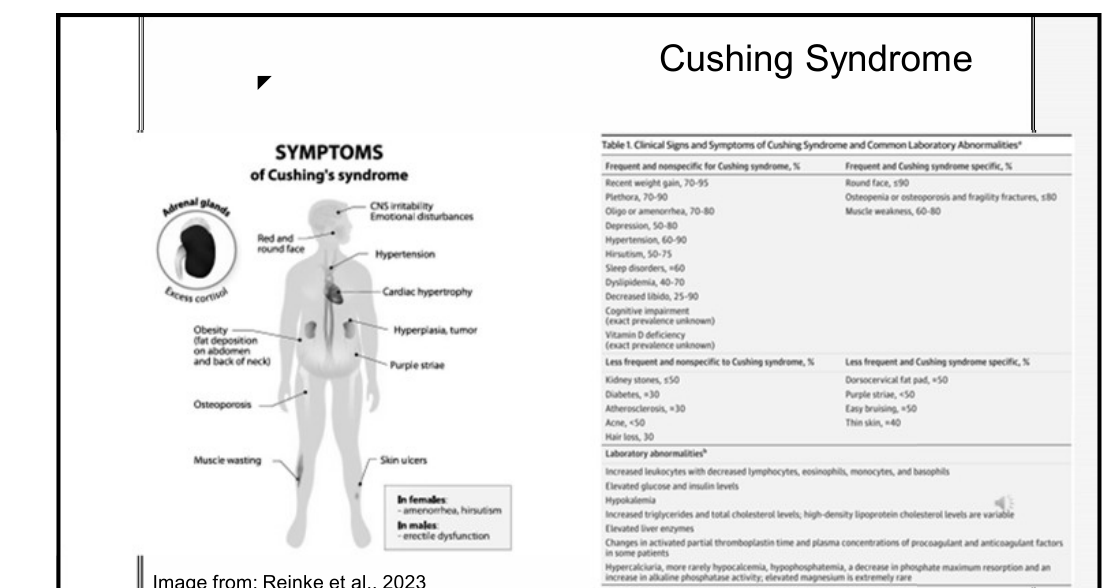
- Characterized by prolonged elevation in plasma cortisol.
- Exogenous cause: Glucocorticoid use.
- Endogenous causes: Benign pituitary adenoma, or adrenal tumours (benign/malignant).
- Clinical Features: "Moon face," buffalo hump, purple striae, hypertension, and osteoporosis.
- Estimated prevalence: 2-8 per million persons annually.
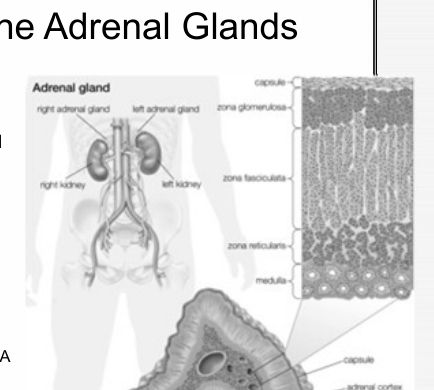
Adrenal Gland Anatomy
The adrenal glands consist of the Medulla (chromaffin cells) and the Cortex. The cortex has three zones:
- ==Zona Glomerulosa: Produces aldosterone (blood pressure/sodium regulation).==
- ==Zona Fasciculata: Produces cortisol (metabolism/immune response).==
- ==Zona Reticularis: Produces androgens.==
 |  |
 |
Oral Manifestations
- Increased risk of periodontal disease.
- Inhibition of new bone formation leading to osteoporosis of the jaw bone.
- Delayed wound healing.
- Higher risk of oral candidiasis and recurrent aphthous ulcers.
- Cortisol inhibits WBC migration, which contributes to the increased risk of periodontal disease.
Cushing Syndrome
Dental Management Considerations
- Obtain comprehensive medical records, including dosage and frequency of glucocorticoids.
- Consult with physicians; avoid abrupt discontinuation of corticosteroids.
- Monitor vital signs (baseline and during procedures) to avoid hypertensive episodes.
- Limit epinephrine use to avoid hypertensive episodes.
- Abrupt cessation of steroids can trigger a crisis (hypotension, vomiting).
- Exercise caution with drug interactions.
- Evaluate pain management carefully; aspirin and NSAIDs pose a risk for peptic ulcers in these patients.
- Be aware of drug interactions with fluconazole or clarithromycin.
Addison Disease
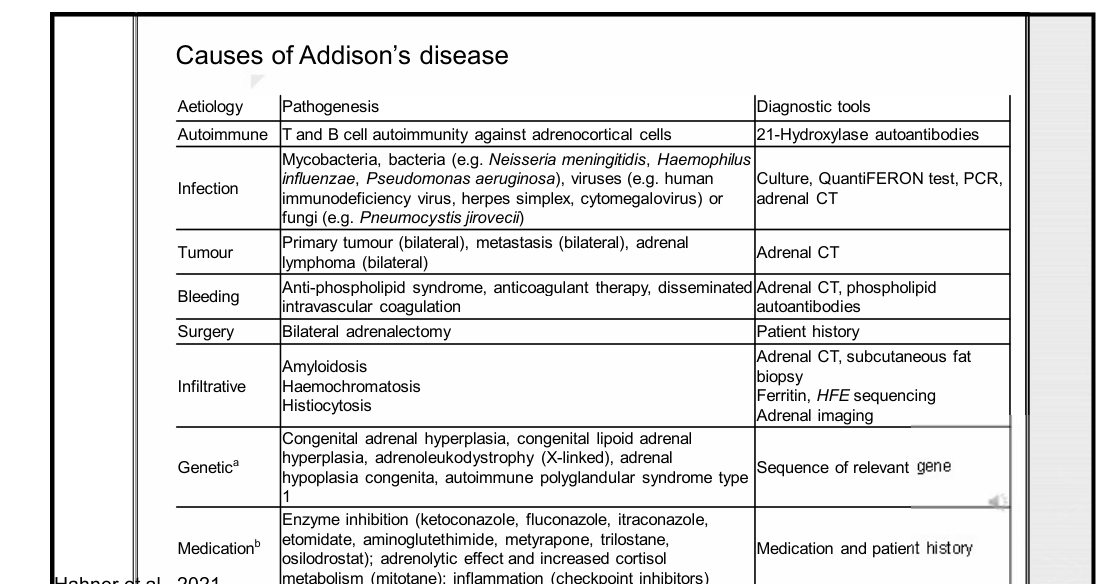
Classification and Etiology7
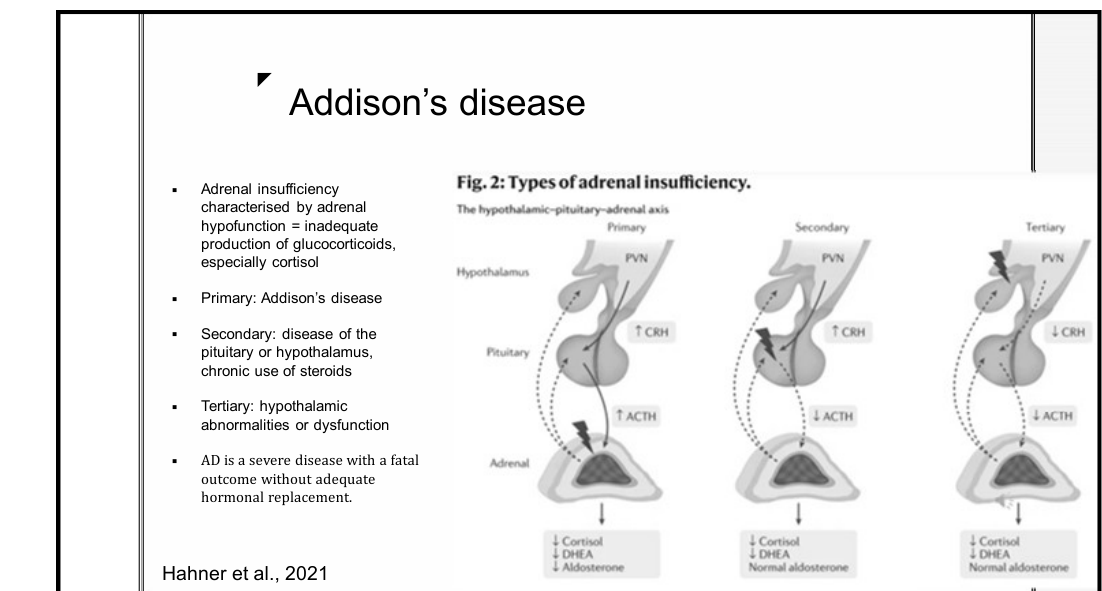
Adrenal insufficiency characterized by inadequate production of glucocorticoids (especially cortisol). Without replacement, the disease can be fatal.
- Primary (Addison’s Disease): Autoimmune (21-Hydroxylase autoantibodies), infection (TB, HIV, fungi), tumours, or genetic factors.
- Autoimmune adrenalitis is the most common cause in developed countries; TB/HIV are more common in others.
- Secondary: Pituitary or hypothalamic disease, or chronic steroid use.
- Tertiary: Hypothalamic dysfunction.
- Secondary/Tertiary insufficiency is often due to long-term exogenous steroid suppression.
| Aetiology | Pathogenesis | Diagnostic Tools |
|---|---|---|
| Autoimmune | T and B cell autoimmunity | 21-Hydroxylase autoantibodies |
| Infection | Bacterial, viral, or fungal pathogens | Culture, PCR, Adrenal CT |
| Tumour | Primary or metastatic | Adrenal CT |
| Bleeding | Anti-phospholipid syndrome, anticoagulants | Adrenal CT, antibodies |
| Infiltrative | Amyloidosis, Haemochromatosis | Biopsy, Adrenal imaging |
| Genetic | Congenital adrenal hyperplasia, etc. | Gene sequencing |
| Medication | Enzyme inhibition (e.g., ketoconazole) | History |
 |  |
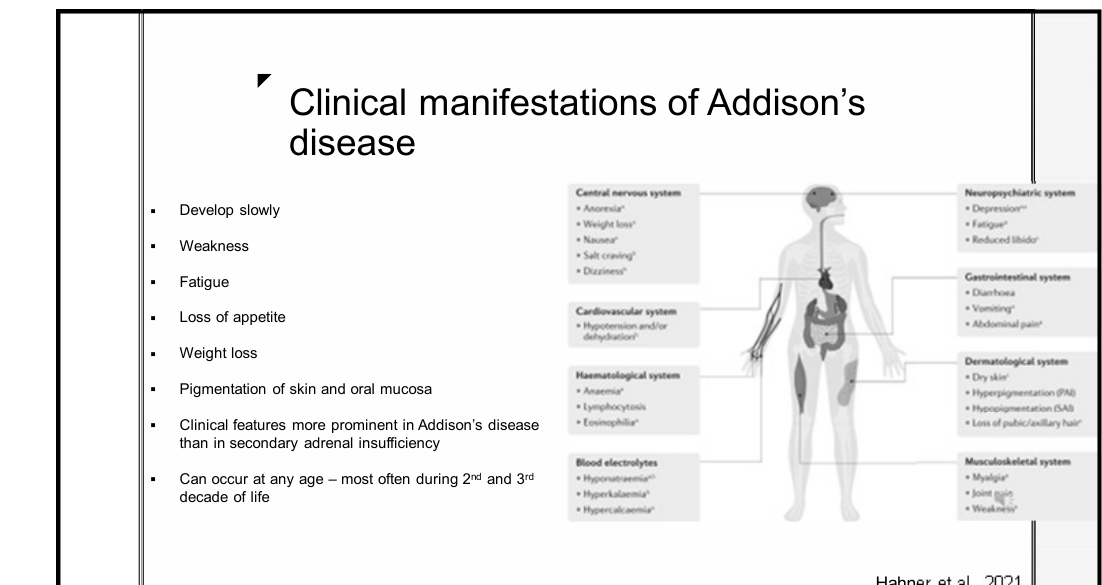 |
Clinical Manifestations
Symptoms develop slowly and are more prominent in primary disease:
- Fatigue, weakness, and loss of appetite/weight.
- Skin "bronzing" or generalized hyperpigmentation.
- Pigmentation of skin and oral mucosa.
- Gastrointestinal issues: Diarrhoea, vomiting, abdominal pain.
- Musculoskeletal: Muscle/joint pain.
- Electrolyte imbalance: Hyponatremia, hyperkalemia.
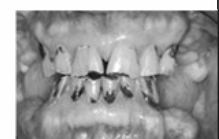
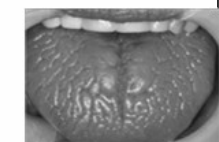
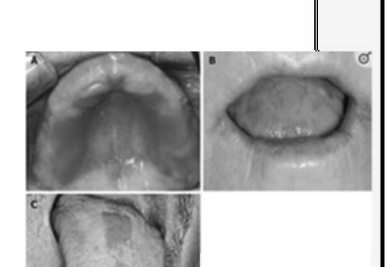
Oral Pigmentation8
- Locations: Gingiva, vermillion border of lip, buccal mucosa, palate, and tongue.
- Appearance: Patchy, macular-like or nodular-like; dark brown to black.
- Pigmentation may also present with blue tints.
- Clinical Significance: Usually occurs before extra-oral manifestations; asymptomatic.
- Differential Diagnosis: Peutz-Jeghers syndrome, McCune-Albright syndrome.

Management and Adrenal Crisis
- Adrenal crisis is a life-threatening emergency requiring intensive fluid resuscitation (IV saline, dextrose) and hormone replacement (Hydrocortisone).
- Dental Risks: Crisis can be precipitated by stress, pain, infection, or invasive procedures.
- Supplementation: For minor to moderate oral surgery in at-risk patients, supplementation of 25-75 mg hydrocortisone equivalent may be required.
- Dentists must recognize unrecognized adrenal insufficiency or poor health stability before treatment.
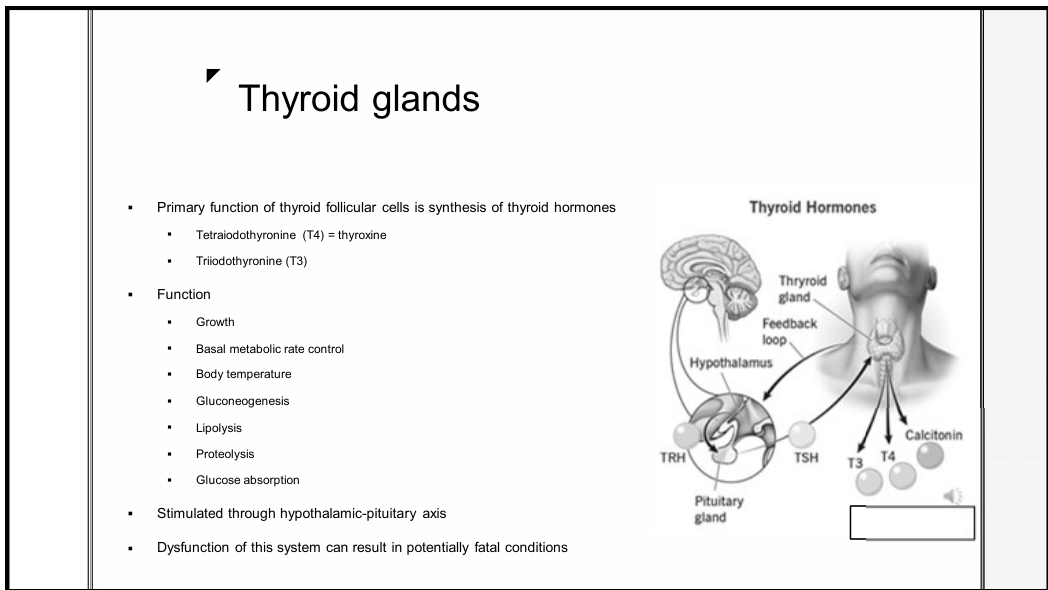
Thyroid Gland Disorders
Thyroid Function Overview9
- Follicular cells synthesize T4 (thyroxine) and T3 (triiodothyronine).
- Controls basal metabolic rate, growth, body temperature, and various metabolic processes (gluconeogenesis, lipolysis).
 |  |
 |
Grave’s Disease Pathophysiology
- Autoimmune hyperthyroidism where autoantibodies stimulate TSH receptors.
- Results in low TSH levels due to negative feedback.
- Most common in women aged 20–40.
Grave Disease and Hyperthyroidism
Clinical Presentation
- Enlarged, overactive thyroid (goitre).
- Ocular abnormalities and localized dermopathy.
- Systemic symptoms: Anxiety, weight loss, palpitations, insomnia, tachycardia, and atrial fibrillation.
- Tremors and exophthalmos (bulging eyes).
- Characterized by a sudden onset of symptoms.
Oral Manifestations10
- Increased susceptibility to caries and periodontal disease.
- Maxillary or mandibular osteoporosis.
- Accelerated dental eruption and early primary tooth exfoliation.
- Loss of taste and oral burning.
- Enlargement of extra-glandular thyroid tissue.
- Association with Sjogren’s syndrome or Systemic Lupus Erythematosus.
 |  |
 |
Dental Management
- Haemostasis: Elevated BP/heart rate and anti-thyroid drugs (causing hypoprothrombineamia) can prolong bleeding.
- Infection Risk: Inadequate wound healing.
- Drug Precautions: Epinephrine is contraindicated as stress/surgery can trigger a thyrotoxic crisis; use NSAIDs with caution.
Thyrotoxic Crisis
Stress or surgery can trigger a fatal "thyroid storm" in uncontrolled patients. Avoid Aspirin (ASA) as it increases free T4/T3 levels.
Hashimoto Thyroiditis and Hypothyroidism
Clinical Features11
- Characterized by decreased thyroid hormone and slower metabolic rate.
- Symptoms: Weight gain, lethargy, cold intolerance, dry/cool skin, facial puffiness, and bradycardia.
 |  |
Oral Manifestations
- Cretinism (Childhood Hypothyroidism): Thick lips and protruding tongue (macroglossia
- Macroglossia (enlarged tongue) is a very common finding in adult hypothyroidism.).
- General Findings:
- Delayed eruption of teeth and impacted mandibular second molars.
- Dysgeusia.
- Poor periodontal health and altered tooth morphology.
- Delayed wound healing.
Dental Considerations
- Haemostasis: Longer time required to achieve.
- Infection: Increased susceptibility due to delayed healing.
- Drug Interactions: L-thyroxine increases the metabolism of phenytoin and carbamazepine and enhances the effects of warfarin.
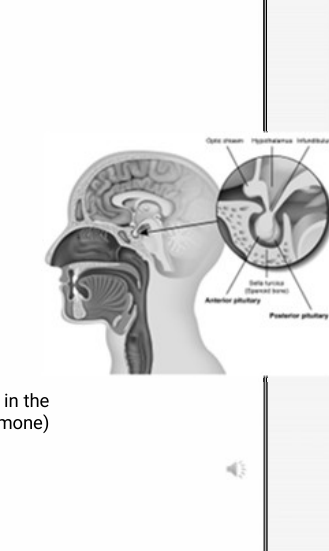
Pituitary Gland Disorders
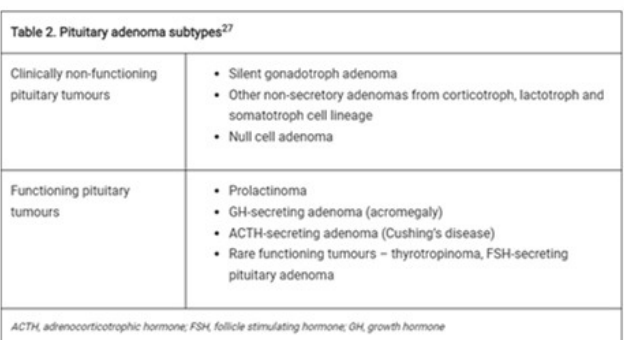
Pituitary Adenoma Subtypes12
- Non-functioning: Silent gonadotroph, null cell, or other non-secretory adenomas
Pathogenesis
Most pituitary disorders arise from benign adenomas. Hypersecretion of Growth Hormone (GH) leads to Gigantism or Acromegaly. .
- Functioning: Prolactinoma, GH-secreting (Acromegaly), ACTH-secreting (Cushing’s), and rare TSH/FSH-secreting tumours.
 |  |
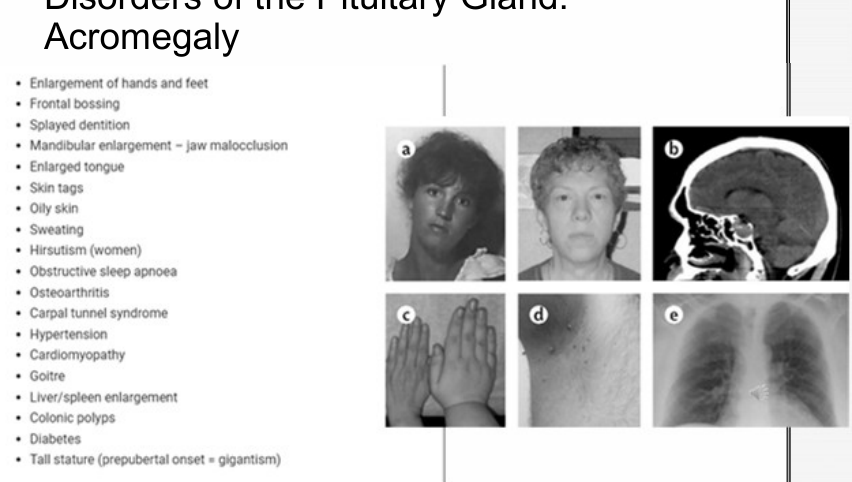 |
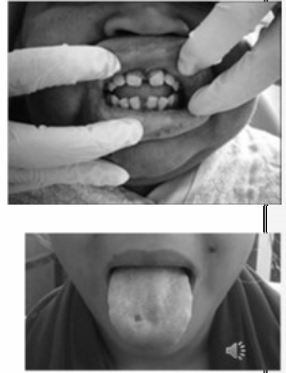
Clinical Features of Acromegaly
- Enlargement of hands, feet, and mandible (jaw malocclusion).
- Frontal bossing and splayed dentition (diastema).
- Macroglossia (enlarged tongue).
- Systemic: Sleep apnoea, hypertension, cardiomyopathy, diabetes, and osteoarthritis.
Acromegaly and Pituitary Adenomas
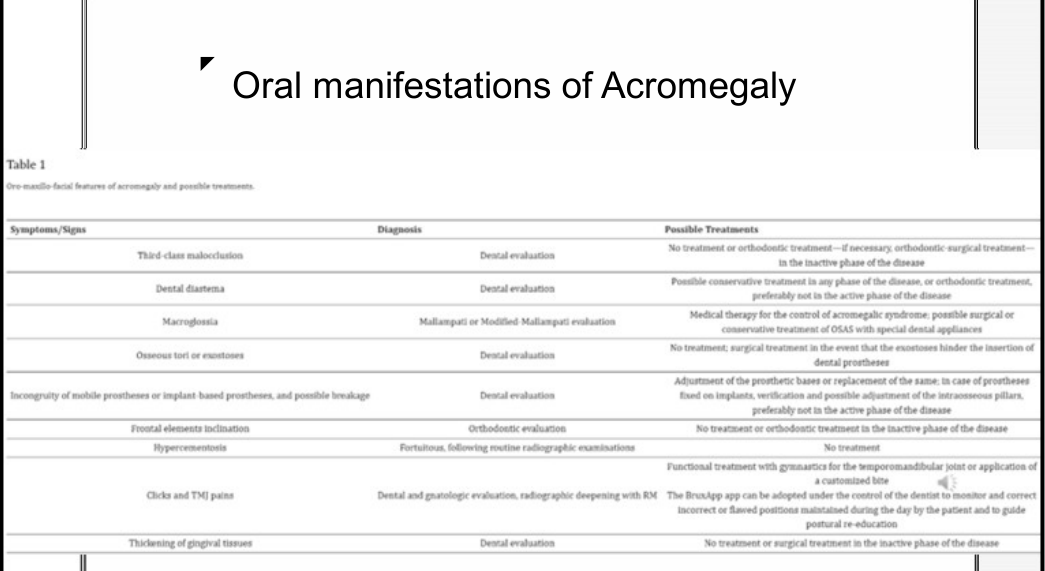
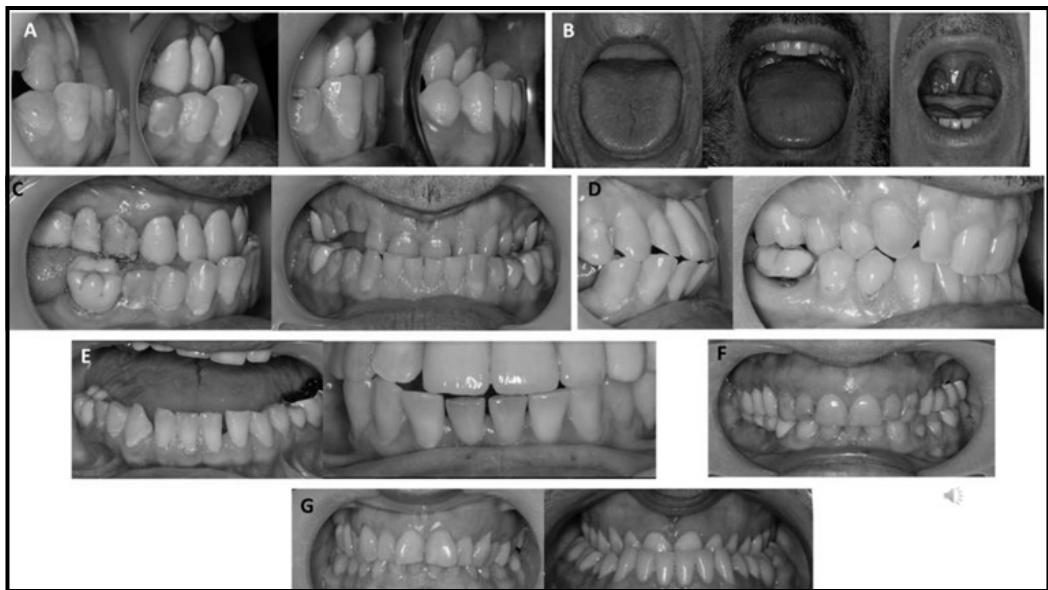
Oral Signs and Treatment Approaches
| Symptoms/Signs | Diagnosis | Possible Treatments |
|---|---|---|
| Class III Malocclusion | Dental eval | Orthodontic/Surgical (in inactive phase) |
| Dental Diastema | Dental eval | Conservative or Orthodontic |
| Macroglossia | Mallampati eval | Medical control of GH; OSA appliances |
| Osseous exostoses | Dental eval | Surgical only if hindering prostheses |
| Gingival Thickening | Dental eval | No treatment or surgery (inactive phase) |
| TMJ Pain | Dental/Radiographic | Functional treatment or customized bite |
- Mandibular Prognathism: Class III malocclusion due to reactivation of condylar growth.
- Diastemas: Splayed teeth (seen in 40-43% of patients).
- Macroglossia: Seen in over 50% of cases; contributes to sleep apnea.
- Hypercementosis: Thickening of the roots.
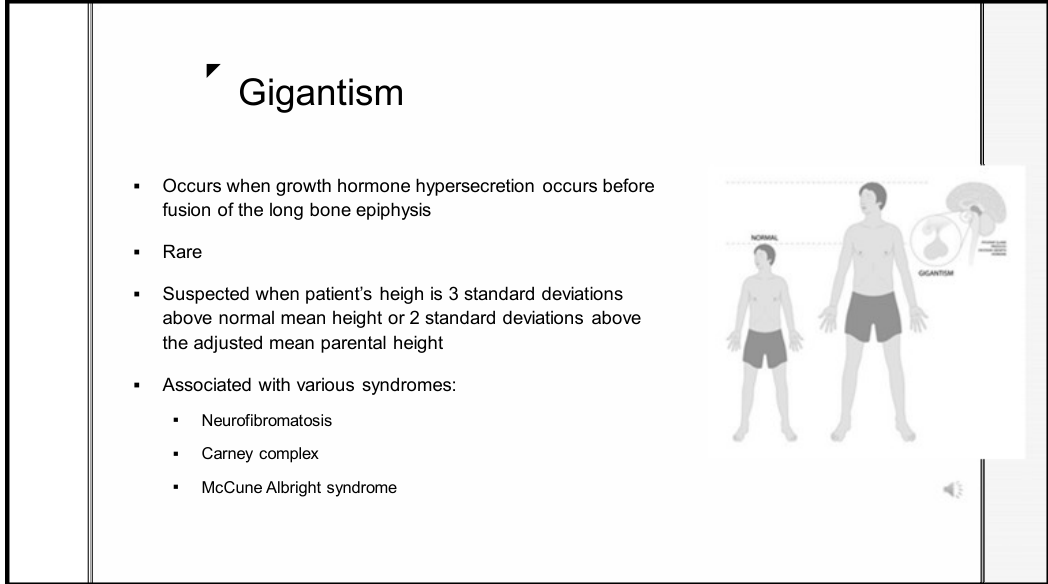
Gigantism
Overview13
- Occurs when GH hypersecretion happens before the fusion of long bone epiphyses.
- This condition specifically affects children.
- Rare condition; suspected when height is >3 standard deviations above the mean.
- Associated syndromes: Neurofibromatosis, Carney complex, and McCune Albright syndrome.
 |  |
 |
Oral Manifestations
- Teeth size proportional to generalized enlarged body size.
- Interdental spacing and dental malocclusion.
- Hypercementosis of roots.
- Prognathic mandible and frontal bossing.
- General symmetrical overgrowth of the oral structures.
Parathyroid Gland Disorders
Physiology of Parathyroid Hormone (PTH)14
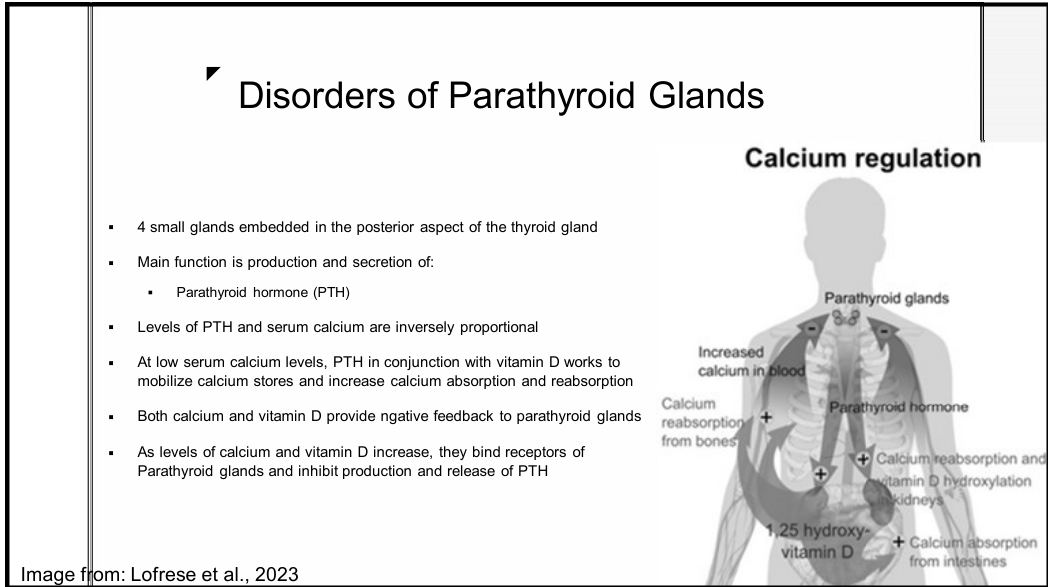
- Four small glands that produce PTH to regulate calcium homeostasis.
- PTH and serum calcium are inversely proportional: low calcium triggers PTH and Vitamin D to mobilize calcium stores and increase absorption.
- PTH also plays a critical role in regulating phosphate levels alongside calcium.
- Negative feedback: High calcium and Vitamin D inhibit PTH release.
Classification of Disorders
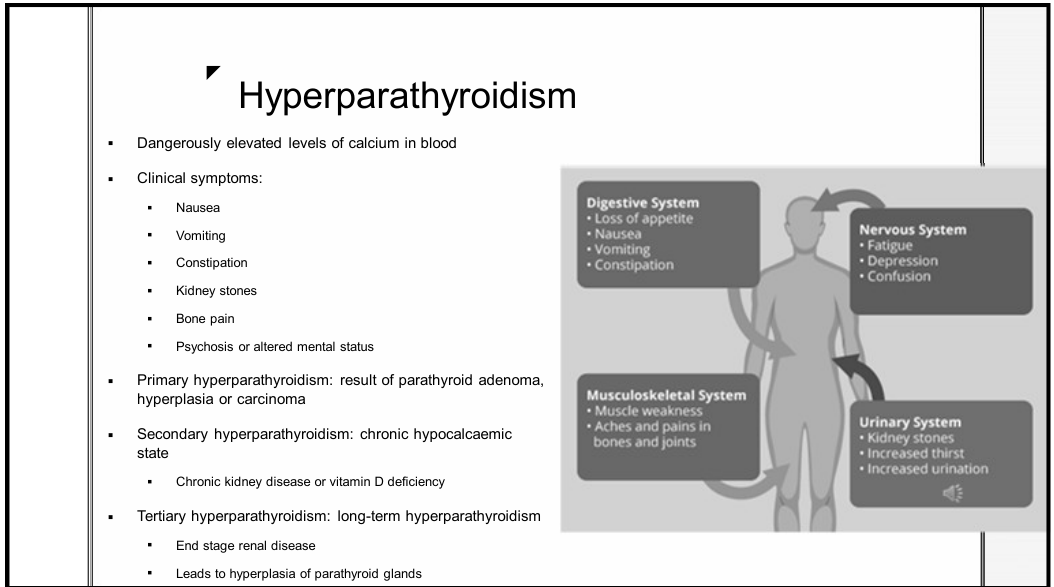
- Primary Hyperparathyroidism: Most common; hypercalcaemia with increased PTH.
- Hypoparathyroidism: Less common; low serum calcium due to inadequately low PTH.
Role of the Dentist
- Early diagnosis of Acromegaly/Gigantism through assessment of macroglossia, diastemas, and prognathism.
- Identification of co-morbidities like obstructive sleep apnoea.
Hyperparathyroidism
Clinical Types15
- Primary: Result of parathyroid adenoma, hyperplasia, or carcinoma
Clinical Mnemonic
"Moans, stones, bones, and psychic overtones" summarizes the classic presentation: Nausea (moans), kidney stones, bone pain, and psychosis (psychic overtones). .
- Secondary: Chronic hypocalcaemic state (e.g., chronic kidney disease, Vitamin D deficiency).
- Tertiary: Long-term hyperparathyroidism leading to autonomous hyperplasia (e.g., end-stage renal disease).
 |  |
 |
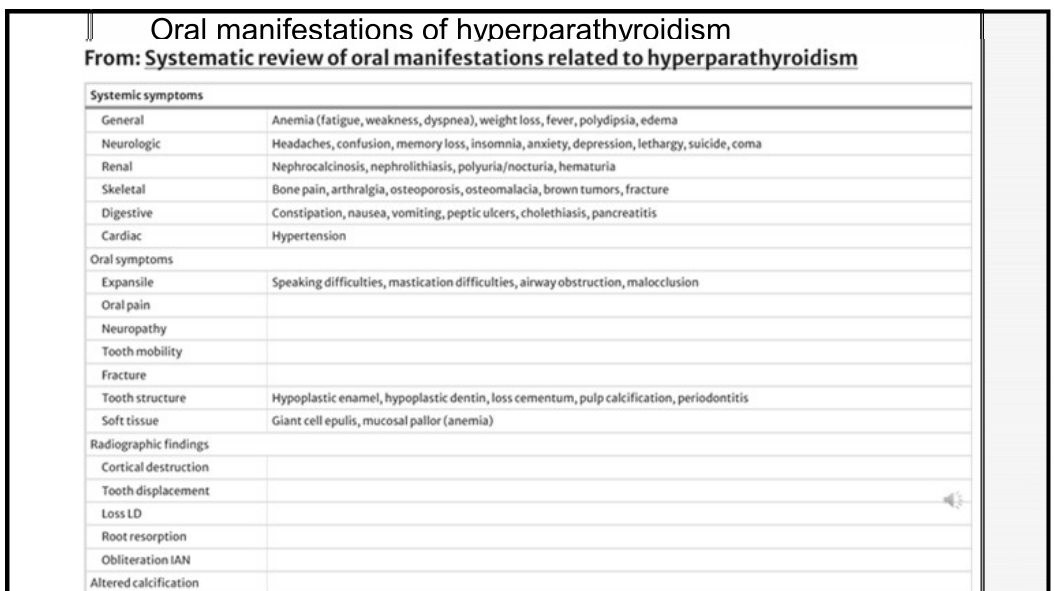
Systemic and Oral Symptoms
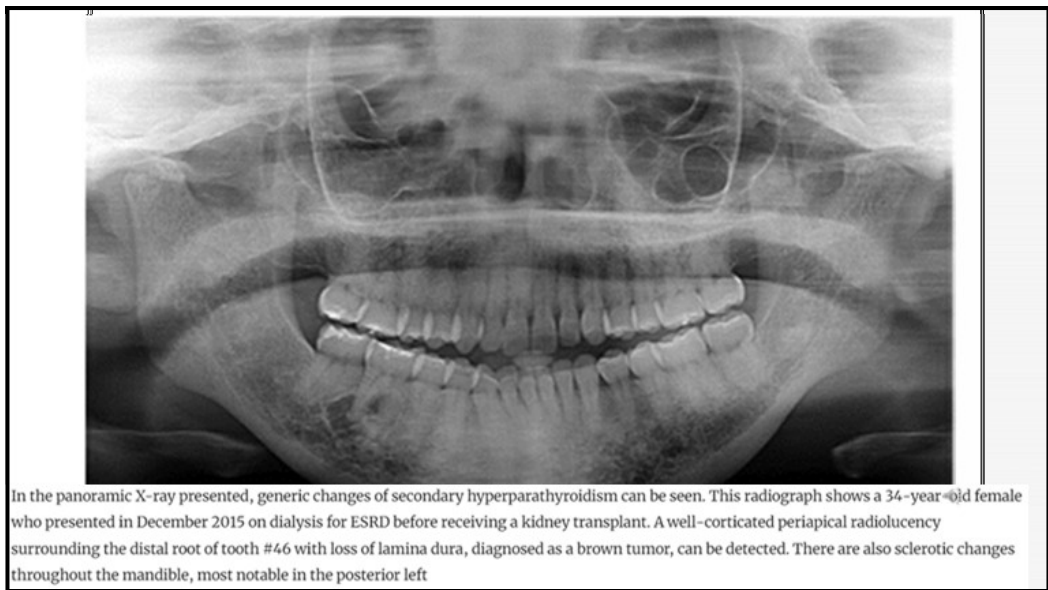
- Systemic: Nausea, kidney stones, bone pain (“brown tumors”), and altered mental status.
- Oral Symptoms:
- Mastication and speaking difficulties, malocclusion.
- Tooth mobility and neuropathy.
- Structural changes: Hypoplastic enamel/dentin, pulp calcification, and periodontitis.
- Soft tissue: Giant cell epulis, mucosal pallor.
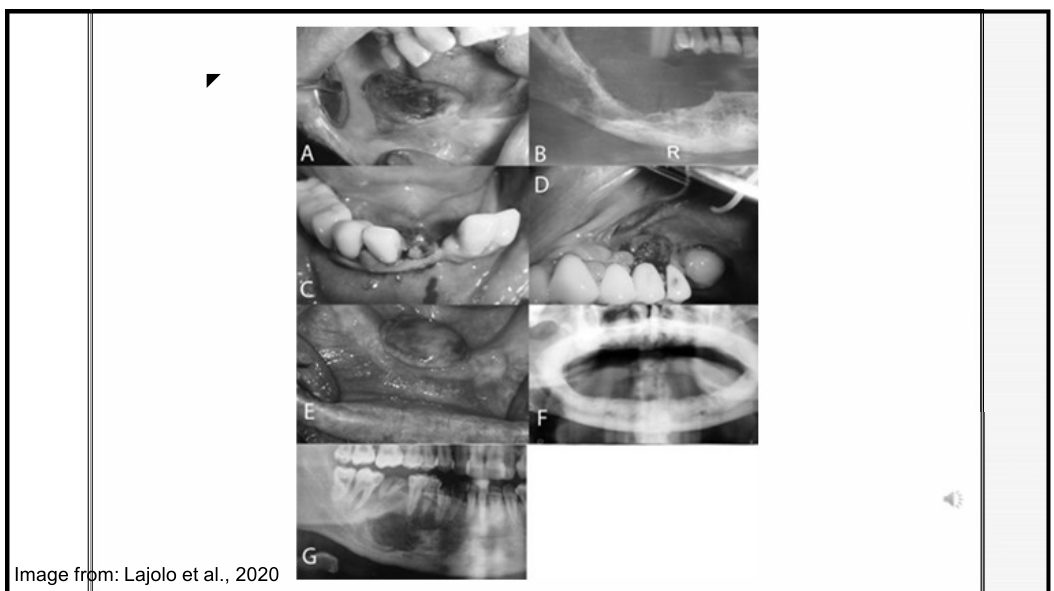
- Brown Tumors: Radiolucent giant cell lesions that are most commonly found in the mandible.
- Bony Expansion: Can lead to visible facial asymmetry and significant malocclusion.
- Radiographic Findings: Cortical destruction, loss of lamina dura (LD), root resorption, and altered calcification
- Loss of Lamina Dura is considered an early radiographic sign indicating increased bone turnover.
Management and Diagnosis16
- Diagnostic requirements: Serum PTH, 24-h urinary calcium, and 25-hydroxy vitamin D.
- Primary treatment: Parathyroidectomy.
- Dental Role: Recognition of jaw growths or radiographic changes can lead to early diagnosis of secondary hyperparathyroidism.
Hypoparathyroidism Overview
- Rare disease resulting in hypocalcaemia.
- Causes: Most commonly injury to or removal of glands during neck surgery.
- Symptoms: Paresthesias, muscle cramps, seizures, and laryngospasms.
- Associated features: Basal ganglia calcification, cataracts, and neuropsychiatric symptoms.
- Treatment: Oral calcium and active Vitamin D to maintain calcium at the low end of the normal range.
Hypocalcemia and Hypoparathyroidism
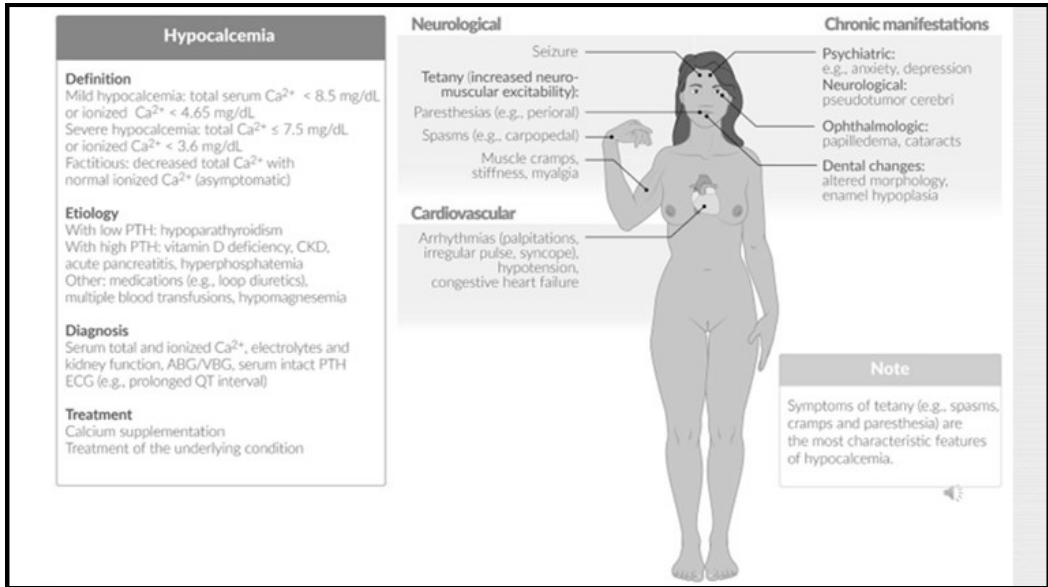
Hypocalcemia Definitions and Etiology17
- Mild: Total serum Ca²⁺ < 8.5 mg/dl.
- Severe: Total Ca²⁺ < 7.5 mg/dl.
- Etiology: Hypoparathyroidism (low PTH); Vitamin D deficiency, CKD, or acute pancreatitis (high PTH).
 |  |
 |
Clinical Manifestations of Hypoparathyroidism
- Neuromuscular: Tetany (characteristic feature), seizures, perioral paresthesia, and muscle cramps.
- Chronic: Anxiety, depression, cataracts, and dental changes.
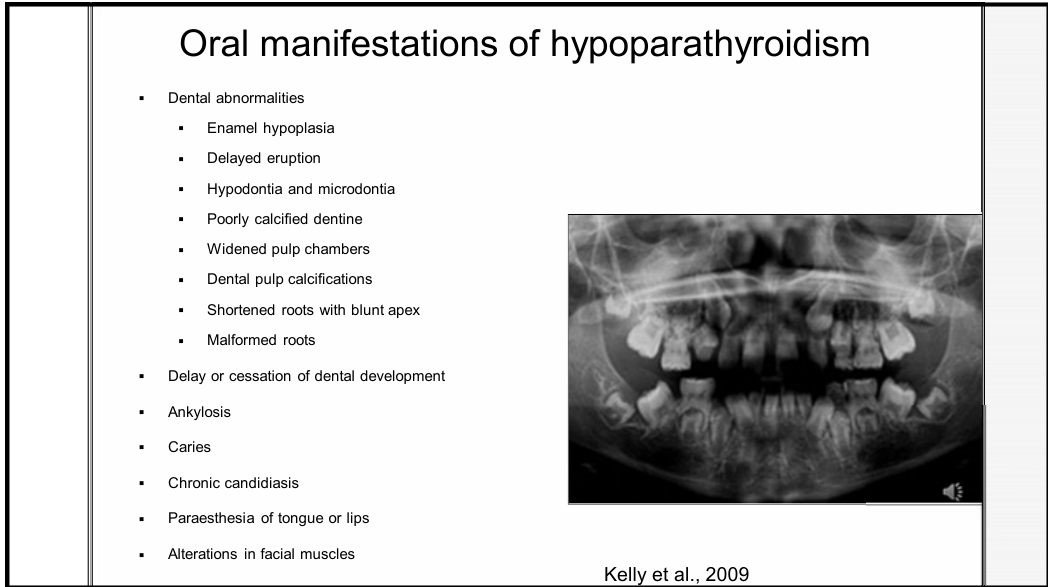
- Oral/Dental Abnormalities:
- Enamel hypoplasia, hypodontia, and microdontia.
- Delayed eruption and malformed/shortened roots with blunt apices.
- Widened pulp chambers and pulp calcifications.
- Radiographic findings may also include a thickened lamina dura.
- Enamel hypoplasia often presents specifically as pitting of the enamel surface.
- Chronic candidiasis and paresthesia of the tongue or lips.
Dental Management
- Focus on caries prevention (diet, hygiene, check-ups).
- Safety Threshold: Serum calcium levels should be determined before treatment and should be > 8 mg/100 ml to prevent arrhythmias, seizures, and spasms.
Endocrine Changes in Pregnancy
Systemic and Oral Changes18
- Increased oestrogen and progesterone induce cardiovascular, haematologic, and endocrine changes.
- Estrogen levels increase 10x and Progesterone levels increase 30x during pregnancy.
- Oral Manifestations:
- Gingivitis and gingival hyperplasia.
- Pyogenic granuloma.
- Reduced stimulated salivary flow rate.
- Increased facial pigmentation.
- Exacerbation of pre-existing periodontal disease.
- Increased tooth mobility.
- Pyogenic granuloma is often referred to as a "pregnancy tumor".

Dental Treatment Guidelines
- Timing: Most treatment is safe; elective treatment is best performed in the second trimester.
- Sedation: Defer elective procedures requiring GA or IV sedation until after birth/breastfeeding.
- Radiographs: If necessary for infection or trauma, do not defer; use a leaded drape.
- Prescribing: Follow general principles for drug use during pregnancy/breastfeeding; defer decisions if pregnancy status is unknown
Medication Safety
Always carefully check specific pregnancy categories and safety classifications before prescribing any medications to pregnant patients.
References and Contact Information
Contact Information19
-
Speaker: Dr. Lalama Tiwari
-
Email: lalima.tiwari@uwa.edu.au
 |  |
 |
Literature References
- Mauri-Obradors E, Estrugo-Devesa A, Jané-Salas E, Viñas M, López-López J. Oral manifestations of Diabetes Mellitus. A systematic review. Med Oral Patol Oral Cir Bucal. 2017 Sep 1;22(5):e586-e594. doi: 10.4317/medoral.21655. PMID: 28809366; PMCID: PMC5694181.
- Rohani B. Oral manifestations in patients with diabetes mellitus. World J Diabetes. 2019 Sep 15;10(9):485-489. doi: 10.4239/wjd.v10.i9.485. PMID: 31558983; PMCID: PMC6748880.
- Maya S. Indurkar, Arati S. Maurya, Sanjiv Indurkar; Oral Manifestations of Diabetes. Clin Diabetes 1 January 2016; 34 (1): 54–57. https://doi.org/10.2337/diaclin.34.1.54
- Kumari M, Kumar T, Rai S, Rai A, Sultana R, Priya L. Evaluation of Dental Health in Terminally Ill Patients. J Med Life. 2020 Jul-Sep;13(3):321-328. doi: 10.25122/jml-2020-0023. PMID: 33072203; PMCID: PMC7550152.
- Reincke M, Fleseriu M. Cushing Syndrome: A Review. JAMA. 2023;330(2):170–181. doi:10.1001/jama.2023.11305
- Mirfarsi, Sahar, Dalia Seleem and Airani Sathananthan, “Dental Considerations and Precautions Associated with Oral Excisional Biopsy on a Patient with Cushing’s Syndrome (Hypercortisolism)” (2023) 67(4) The Dental clinics of North America 581
- Hahner, S., Ross, R.J., Arlt, W. et al. Adrenal insufficiency. Nat Rev Dis Primers 7, 19 (2021). https://doi.org/10.1038/s41572-021-00252-7
- Adel Bouguezzi, Hela Zouaghi. Oral Pigmentation as a Sign of Addison’s disease. On J Dent & Oral Health. 3(1): 2020. OJDOH. MS.ID.000551.
- Bugălă NM, Carsote M, Stoica LE, Albulescu DM, Ţuculină MJ, Preda SA, Boicea AR, Alexandru DO. New Approach to Addison Disease: Oral Manifestations Due to Endocrine Dysfunction and Comorbidity Burden. Diagnostics (Basel). 2022 Aug 28;12(9):2080. doi: 10.3390/diagnostics12092080. PMID: 36140482; PMCID: PMC9497746.
- Chandna S, Bathla M. Oral manifestations of thyroid disorders and its management. Indian J Endocrinol Metab. 2011 Jul;15(Suppl 2):S113-6. doi: 10.4103/2230-8210.83343. PMID: 21966646; PMCID: PMC3169868.
- Davies, T.F., Andersen, S., Latif, R. et al. Graves’ disease. Nat Rev Dis Primers 6, 52 (2020). https://doi.org/10.1038/s41572-020-0184-y
- Preo, G., De Stefani, A., Dassie, F. et al. The role of the dentist and orthodontist in recognizing oro-facial manifestations of acromegaly: a questionnaire-based study. Pituitary 25, 159–166 (2022). https://doi.org/10.1007/s11102-021-01183-y
- De Stefani A, Dassie F, Wennberg A, Preo G, Muneratto A, Fabris R, Maffei P, Gracco A, Bruno G. Oral Manifestations and Maxillo-Facial Features in the Acromegalic Patient: A Literature Review. Journal of Clinical Medicine. 2022; 11(4):1092. https://doi.org/10.3390/jcm11041092
- Lajolo, Carlo et al, “Brown Tumors of the Oral Cavity: Presentation of 4 New Cases and a Systematic Literature Review” (2020) 129(6) ORAL SURGERY ORAL MEDICINE ORAL PATHOLOGY ORAL RADIOLOGY 575
- Palla, B., Burian, E., Fliefel, R. et al. Systematic review of oral manifestations related to hyperparathyroidism. Clin Oral Invest 22, 1–27 (2018). https://doi.org/10.1007/s00784-017-2124-0
- Letícia Martins Guimarães, Alline Teixeira Valeriano, Hélder Antônio Rebelo Pontes, Ricardo Santiago Gomez, Carolina Cavalieri Gomes, Manifestations of hyperparathyroidism in the jaws: Concepts, mechanisms, and clinical aspects, Oral Surgery, Oral Medicine, Oral Pathology and Oral Radiology, Volume 133, Issue 5, 2022, Pages 547-555,
- Mittal, S., Gupta, D., Sekhri, S., & Goyal, S. (2014). Oral manifestations of parathyroid disorders and its dental management. J Dent Allied Sci, 3(1), 34-8.
- Alice Kelly, Luciana Pomarico, Ivete Pomarico Ribeiro de Souza, Cessation of dental development in a child with idiopathic hypoparathyroidism: a 5-year follow-up, Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, Volume 107, Issue 5, 2009, Pages 673-677,
- Therapeutic guidelines: Dental treatment during pregnancy and breastfeeding; 2022
- Vt H, T M, T S, Nisha V A, A A. Dental considerations in pregnancy-a critical review on the oral care. J Clin Diagn Res. 2013 May;7(5):948-53. doi: 10.7860/JCDR/2013/5405.2986. Epub 2013 Mar 21. PMID: 23814753; PMCID: PMC3681080.
Footnotes
-
Original PDF page 1: L26 Endocrine and Metabolic Disorders, p.1 ↩
-
Original PDF page 2: L26 Endocrine and Metabolic Disorders, p.2 ↩
-
Original PDF page 3: L26 Endocrine and Metabolic Disorders, p.3 ↩
-
Original PDF page 4: L26 Endocrine and Metabolic Disorders, p.4 ↩
-
Original PDF page 5: L26 Endocrine and Metabolic Disorders, p.5 ↩
-
Original PDF page 6: L26 Endocrine and Metabolic Disorders, p.6 ↩
-
Original PDF page 7: L26 Endocrine and Metabolic Disorders, p.7 ↩
-
Original PDF page 8: L26 Endocrine and Metabolic Disorders, p.8 ↩
-
Original PDF page 9: L26 Endocrine and Metabolic Disorders, p.9 ↩
-
Original PDF page 10: L26 Endocrine and Metabolic Disorders, p.10 ↩
-
Original PDF page 11: L26 Endocrine and Metabolic Disorders, p.11 ↩
-
Original PDF page 12: L26 Endocrine and Metabolic Disorders, p.12 ↩
-
Original PDF page 13: L26 Endocrine and Metabolic Disorders, p.13 ↩
-
Original PDF page 14: L26 Endocrine and Metabolic Disorders, p.14 ↩
-
Original PDF page 15: L26 Endocrine and Metabolic Disorders, p.15 ↩
-
Original PDF page 16: L26 Endocrine and Metabolic Disorders, p.16 ↩
-
Original PDF page 17: L26 Endocrine and Metabolic Disorders, p.17 ↩
-
Original PDF page 18: L26 Endocrine and Metabolic Disorders, p.18 ↩
-
Original PDF page 19: L26 Endocrine and Metabolic Disorders, p.19 ↩