Defining Orofacial Pain
Ramesh Balasubramaniam OAM
DENT5310
Orofacial Pain and Dental Sleep Medicine Module
16th April 2026
Affiliations and Organizations1
- The University of Western Australia
- Perth Oral Medicine & Dental Sleep Centre
- Perth Children’s Hospital
- Periogold®
- Oral Medicine Academy of Australasia
- DSSWA
- Australian Dental Association
- Australasian Sleep Association
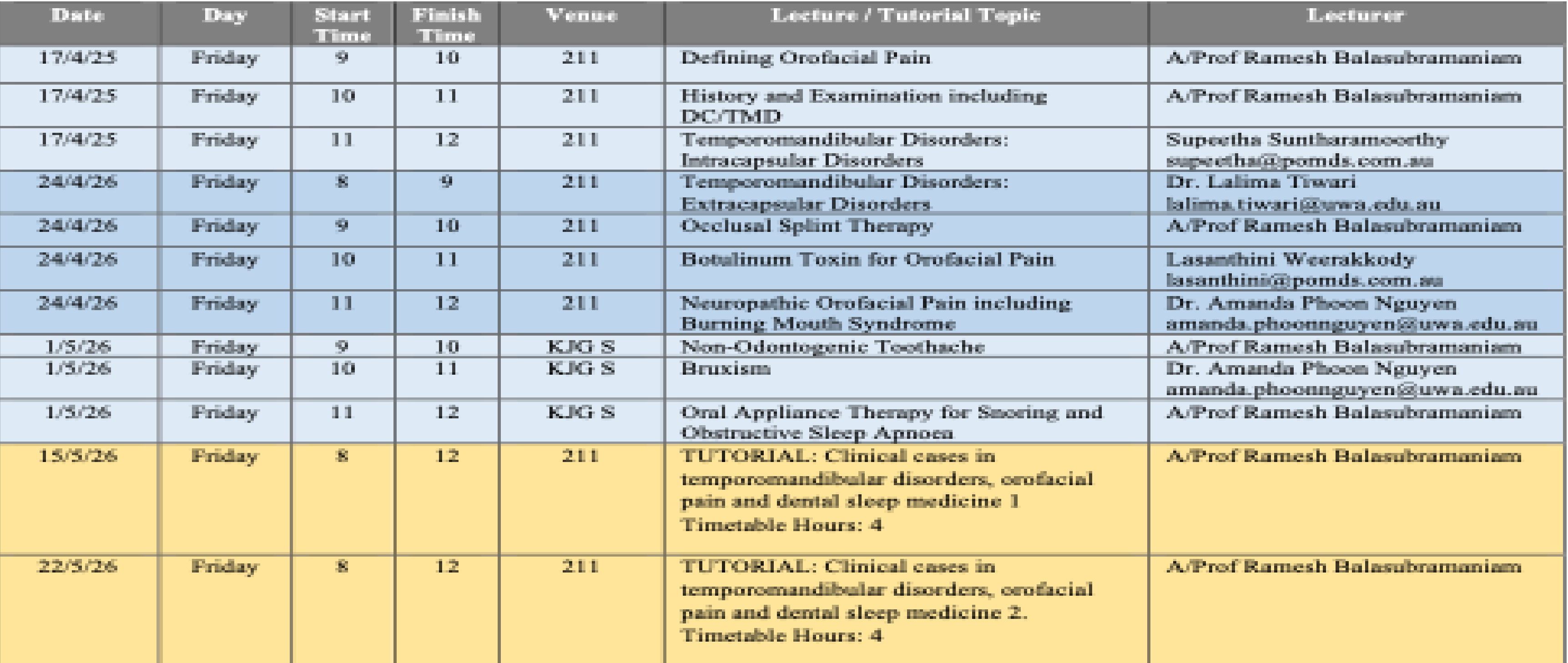
Course Overview and Learning Outcomes
Presenter Information2
Ramesh Balasubramaniam OAM
Associate Professor, Oral Medicine
UWA Dental School
The University of Western Australia
Conflict of Interest Disclosure
Neither I nor my immediate family have any financial interests that would create a conflict of interest or restrict my independent judgment with regard to the content of this presentation.
Specific Learning Outcomes
Unit Learning Outcome 263
Explain the common causes and mechanisms of orofacial pain.
Scope of Learning
The learning outcomes are visible across the entire unit. The series of lectures over the next four weeks will focus on outcomes relevant to facial pain and TMD.
- Pain Mechanisms: Ability to define, classify, and differentiate between various mechanisms of pain including orofacial pain.
- Pain Presentations: Distinguish various pain presentations including acute vs chronic pain; physiological vs pathophysiological pain and understand how the biopsychosocial model contributes to the experience and perception of orofacial pain.
- Temporomandibular Disorders (TMD): Define, classify and discuss the aetiological factors of TMD and understand the anatomy and function of the temporomandibular joint (TMJ) and masticatory muscles.
- Clinical Assessment: Learn to perform a comprehensive history for orofacial pain patients including the effective use of examination tools for TMD assessment and apply diagnostic criteria for TMD.
Clinical Conditions and Management4
- Intracapsular Disorders: Understand common intracapsular disorders with regards to aetiology, pathophysiology, diagnosis, clinical features and management including subluxation and luxation of the TMJs.
- Extracapsular Disorders: Understand common extracapsular disorders with regards to aetiology, pathophysiology, diagnosis, clinical features and management.
- Splint Therapy: Outline the rationale for splint therapy including mechanisms of action, various types of splint designs, indications, and the evidence supporting their use in managing temporomandibular disorders and bruxism.
- Neuromodulators: Discuss the indications, mechanism of action, contraindications, side effects, and complications of neuromodulators.
- Neuropathic Pain: Outline the aetiology, pathogenesis, clinical features, diagnosis and management of neuropathic orofacial pain conditions.
Specialized Topics5
- Non-Odontogenic Toothache: Describe prevalence, aetiology, pathophysiology, clinical features, diagnosis and management of various conditions that may present as non-odontogenic toothache.
- Bruxism: Describe evolution, epidemiology, risk factors, aetiology and pathophysiology, clinical features, diagnosis and management of bruxism.
- Sleep Medicine: Understand the relationship between sleep and overall health, identify risk factors for sleep-disordered breathing, recognise tools for evaluating sleep disorders, and understand available treatment options, including effective management with oral appliance therapy.
The Definition of Pain6
Presentation Agenda7
-
Pain Definition
-
Is Pain Good or Bad?
-
3 Pains
-
Biopsychosocial Model for Pain
-
Definition & Classification of Orofacial Pain
-
Take Home Message
-
Pain Definition
-
Is Pain Good or Bad?
-
3 Pains
-
Biopsychosocial Model for Pain
-
Definition & Classification of Orofacial Pain
-
Take Home Message
Evolution of the IASP Definition8
NEW DEFINITION OF PAIN

Historical Context and Revision9
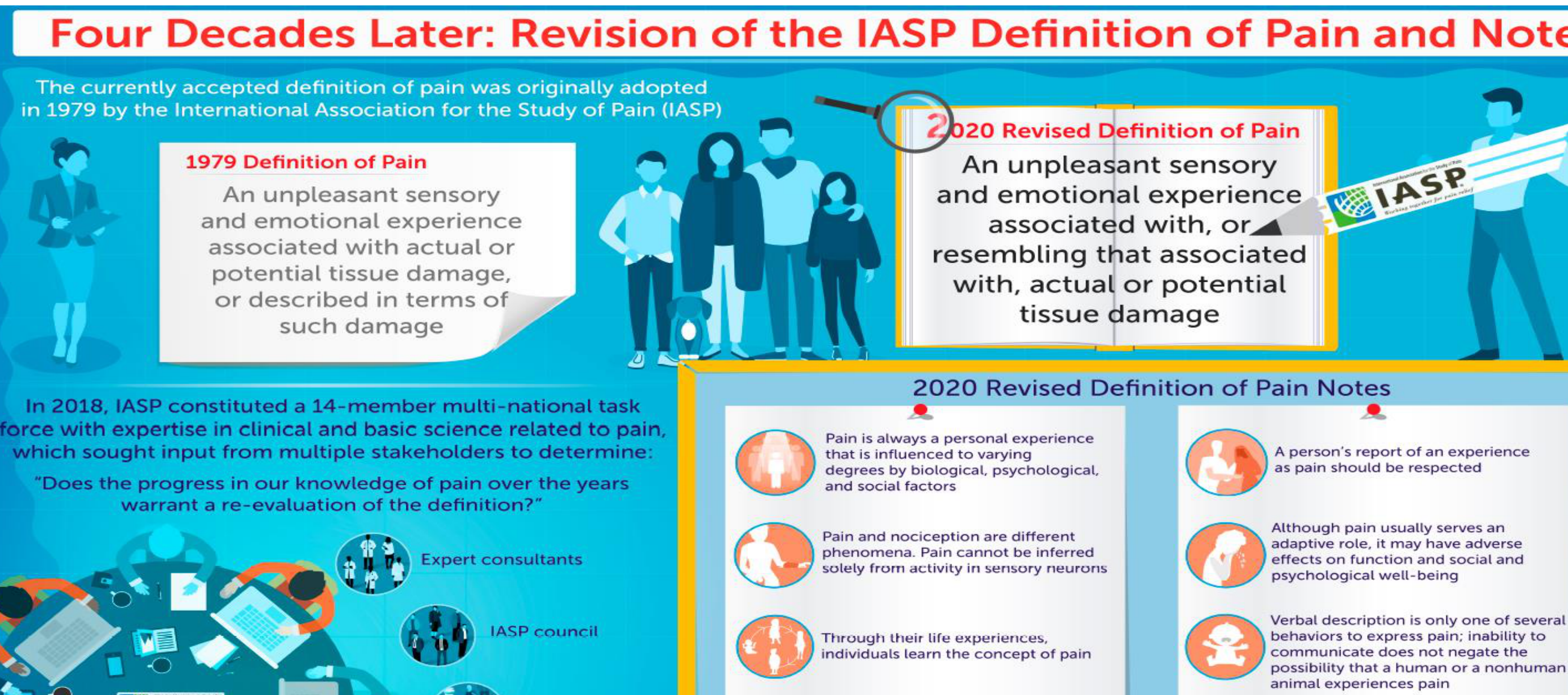
The currently accepted definition of pain was originally adopted in 1979 by the International Association for the Study of Pain (IASP). In 2018, IASP constituted a 14-member multi-national task force with expertise in clinical and basic science related to pain, which sought input from multiple stakeholders to determine if progress in the knowledge of pain warranted a re-evaluation.
Comparison of Definitions
- 1979 Definition of Pain: An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
- 2020 Revised Definition of Pain: An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.
2020 Revised Definition Notes
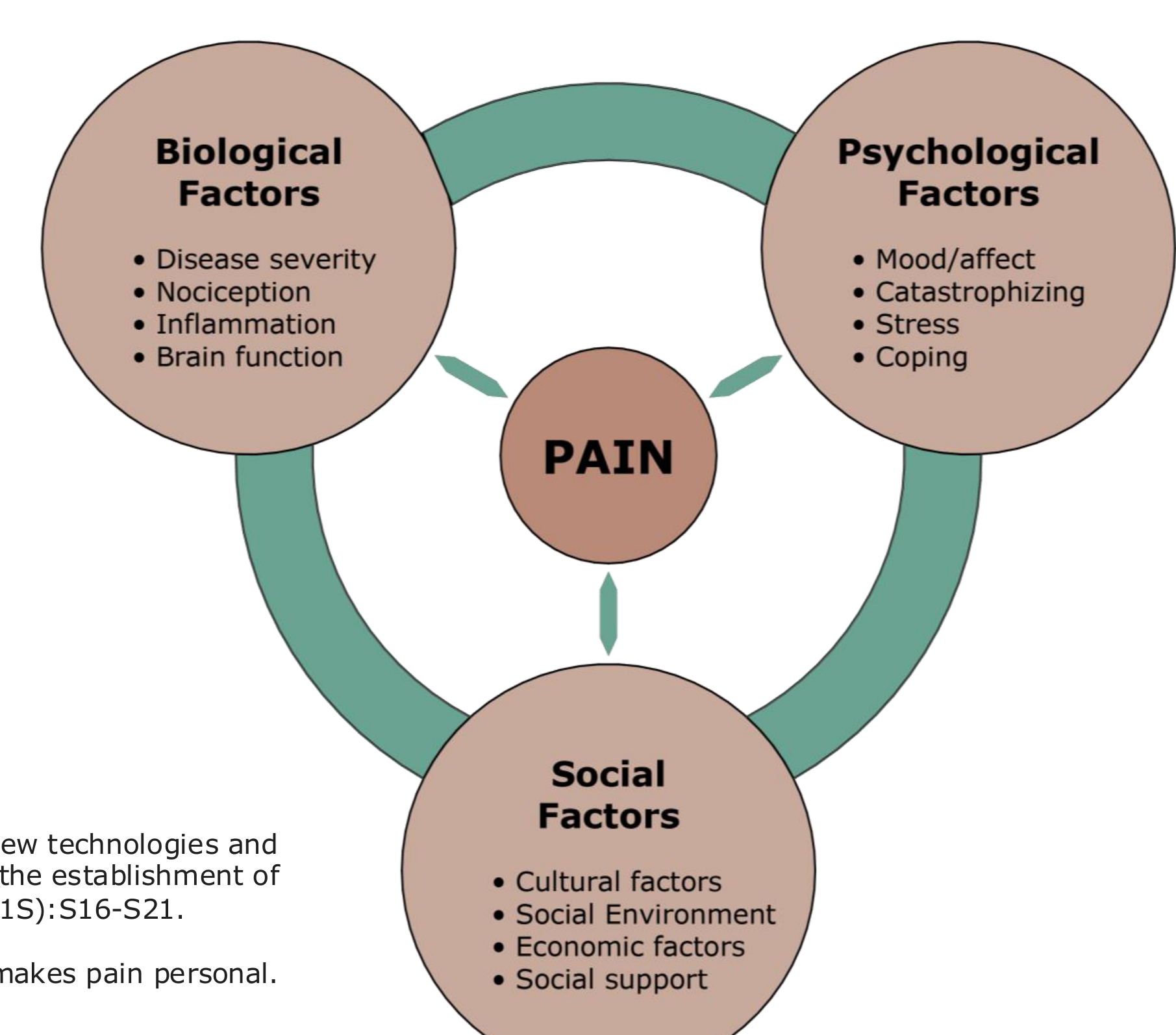
- Pain is always a personal experience that is influenced to varying degrees by biological, psychological, and social factors.
The Mind-Body Connection
Pain is a marriage between the physical body and the mind. Psychological inputs, context, emotion, and expectations significantly influence the pain experience.
- Pain and nociception are different phenomena. Pain cannot be inferred solely from activity in sensory neurons.
- Nociception is the sensory input, while pain is the emotional response and experience.
- Through their life experiences, individuals learn the concept of pain.
- A person’s report of an experience as pain should be respected.
- Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
- Verbal description is only one of several behaviors to express pain; inability to communicate does not negate the possibility that a human or a nonhuman animal experiences pain.
The 2020 IASP Definition10
“An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.”
Source: Raja SN et al. The revised International Association for the Study of Pain definition of pain: concepts, challenges, and compromises. Pain. 2020.
Key Concepts and Clinical Notes
Biological and Psychological Factors11
- Pain is always a personal experience that is influenced to varying degrees by biological, psychological, and social factors.
- Pain and nociception are different phenomena. Pain cannot be inferred solely from activity in sensory neurons.
Source: Raja SN et al. (2020).

Learning and Respecting the Pain Experience12
- Through their life experiences, individuals learn the concept of pain.
- A person’s report of an experience as pain should be respected.
- Because pain is a personal reality, clinicians should focus on the individual rather than just the number on a pain scale. A patient's "10 out of 10" is their reality regardless of the physical stimulus.
Source: Raja SN et al. (2020).

Adaptation and Communication13
- Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
- Verbal description is only one of several behaviours to express pain; inability to communicate does not negate the possibility that a human or a non-human animal experiences pain.
Source: Raja SN et al. (2020).
Pain Characteristics and Mechanisms
Presentation Overview14
- Pain Definition
- Is Pain Good or Bad?
- 3 Pains
- Biopsychosocial Model for Pain
- Definition & Classification of Orofacial Pain
- Take Home Message
The Dual Nature of Pain15
- No one wants to be in pain
- Important for health & survival

Physiological vs Pathophysiological Pain
Physiological Pain Characteristics16
- Consequence of tissue injury or noxious stimuli
- Site of injury = source of pain
- “Normal Pain” / protective
- When noxious stimuli is removed, inflammation resolves and pain ceases
- Helps the body heal by encouraging protection of the area.

Pathophysiological Pain Characteristics17
- Pain persists after noxious stimuli has ceased and tissue healed
- Lesion / dysfunction of the PNS or CNS
- Chronic pain
- Serves no protective or reparative role.
Biomedical vs Biopsychosocial Perspectives
Comparative Perspectives18
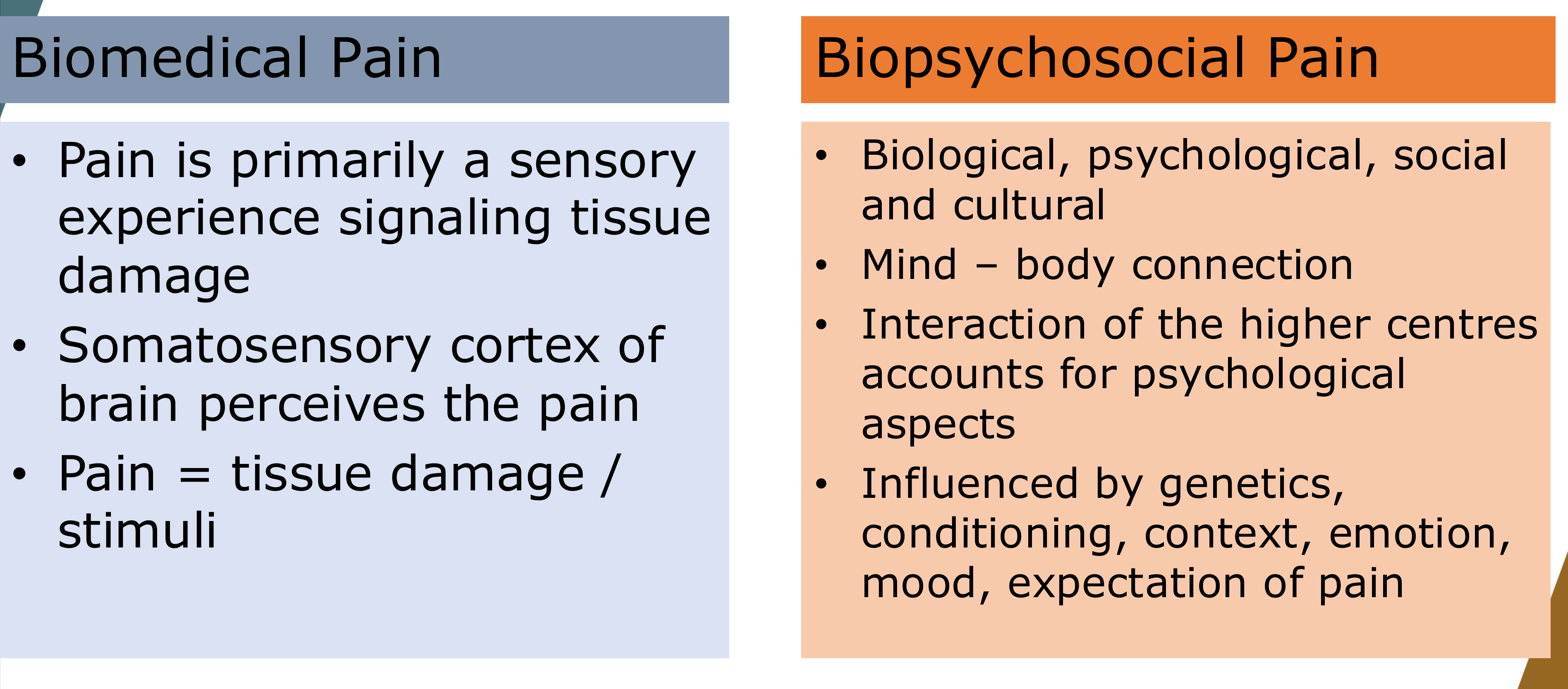
Biomedical Pain
- Pain is primarily a sensory experience signaling tissue damage.
- Somatosensory cortex of brain perceives the pain.
- Pain = tissue damage / stimuli
- The traditional model suggests a direct correlation between the size of the injury and the amount of pain. If no tissue damage is visible, the pain is often dismissed.
Biopsychosocial Pain
- Biological, psychological, social and cultural.
- Mind – body connection.
- Interaction of the higher centres accounts for psychological aspects.
- Influenced by genetics, conditioning, context, emotion, mood, expectation of pain.
Individual Experience of Pain19
Pain is an individual experience shaped by several factors:
- In spite of same noxious stimuli, the experience varies.
- Subjective intensity: “My 10 is not the same as your 10.”
- Particularly influenced by childhood experiences.
 |  |  |
 |  |  |
Clinical Insight
Sir William Osler: “It is more important to know what type of individual has the pain rather the type of pain the patient has.”
Sensory and Affective Components of Suffering
Components of the Pain Experience20
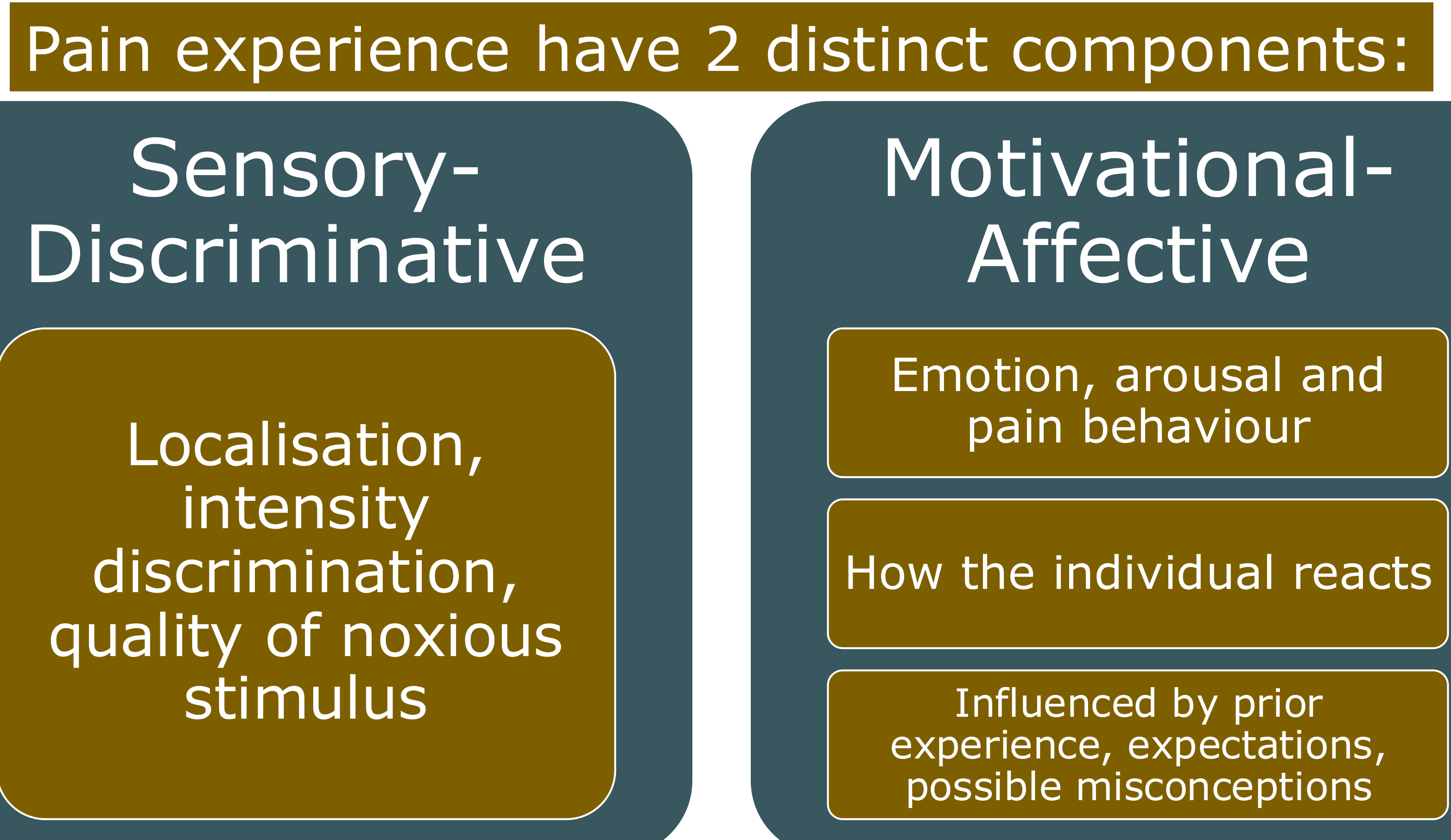
Sensory-Discriminative
- Localization, intensity discrimination, and quality of noxious stimulus.
- Deals with the location, intensity (e.g., 8/10), quality (e.g., aching), and duration of the pain.
Motivational-Affective
- Emotion, arousal, and pain behavior.
- How the individual reacts.
- Influenced by prior experience, expectations, and possible misconceptions.
- Deals with the emotional response, including anxiety, depression, guilt, and catastrophizing.
The Three Types of Pain
Presentation Agenda21
- Pain Definition
- Is Pain Good or Bad?
- 3 Pains
- Biopsychosocial Model for Pain
- Definition & Classification of Orofacial Pain
- Take Home Message
Nociceptive Pain
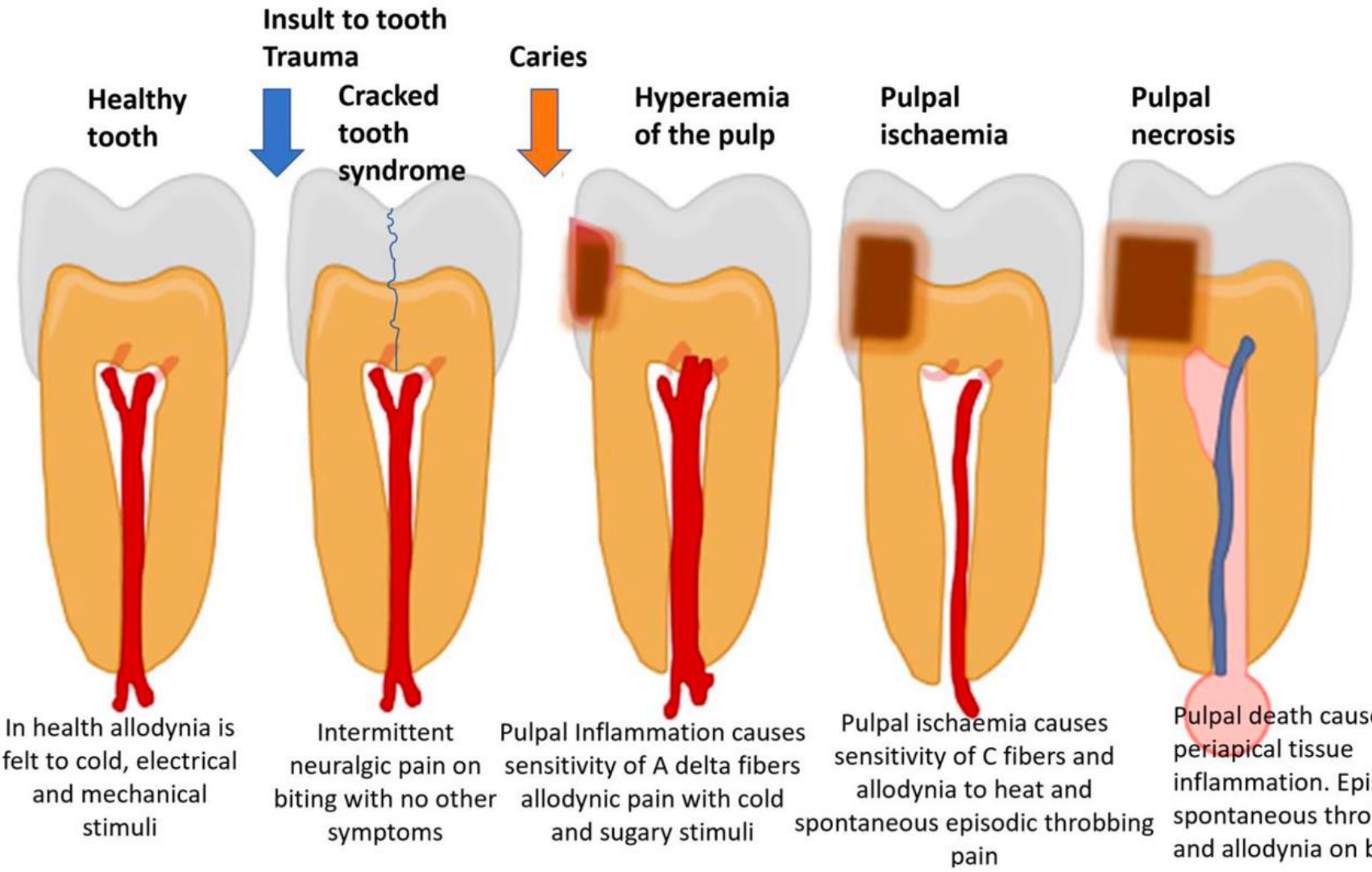
Clinical Manifestations in Dentistry22
Nociceptive pain in the context of toothache presents through various stages of health and disease:
-
Pulpitis is classified as a form of visceral pain.
-
Ligament-related pains are also common clinical manifestations.
-
Healthy tooth: In health, allodynia is felt to cold, electrical, and mechanical stimuli.
-
Insult to tooth/Trauma:
- Cracked tooth syndrome: Intermittent neuralgic pain on biting with no other symptoms.
-
Caries:
- Pulpal Inflammation: Causes sensitivity of A delta fibers; allodynic pain with cold and sugary stimuli.
- Hyperaemia of the pulp.
-
Pulpal ischaemia: Causes sensitivity of C fibers and allodynia to heat; spontaneous episodic throbbing pain.
-
Pulpal necrosis: Pulpal death causes periapical tissue inflammation. Results in episodic spontaneous throbbing pain and allodynia on biting.
Definition
Nociceptive Pain is pain that arises from actual or threatened damage to non-neural tissue and is due to the activation of nociceptors. It involves a normally functioning somatosensory nervous system.
Mechanism and Function23
- Stimuli: Noxious stimuli may be mechanical, thermal, or chemical, resulting in damage or potential damage.
- Processing: Nociception is modified on the way to the CNS; it can be amplified, reduced, or inhibited.
- Perception: It is only classified as pain when it reaches the Central Nervous System (CNS).
- Purpose: The primary function is to prevent further injury.
 |  |
Neuropathic Pain
Definition24
Neuropathic Pain is pain caused by a lesion or disease of the somatosensory nervous system.
 |  |
Characteristics of Neuropathic Pain25
- Systemic Origin: Arises from an abnormality of the nervous system.
- Stimulus Independence: There is no need for noxious stimuli.
- Presentation: Pain may be spontaneous.
- Function: It serves no protective role.
- Classification: Can be categorized as Episodic vs. Continuous Neuropathic Pain.
- Pain is often described as electric shock-like in nature.
- Specific examples include post-traumatic trigeminal neuropathic pain.
 |  |
 |
Nociplastic Pain
Definition26
Nociplastic Pain is pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain.
 | 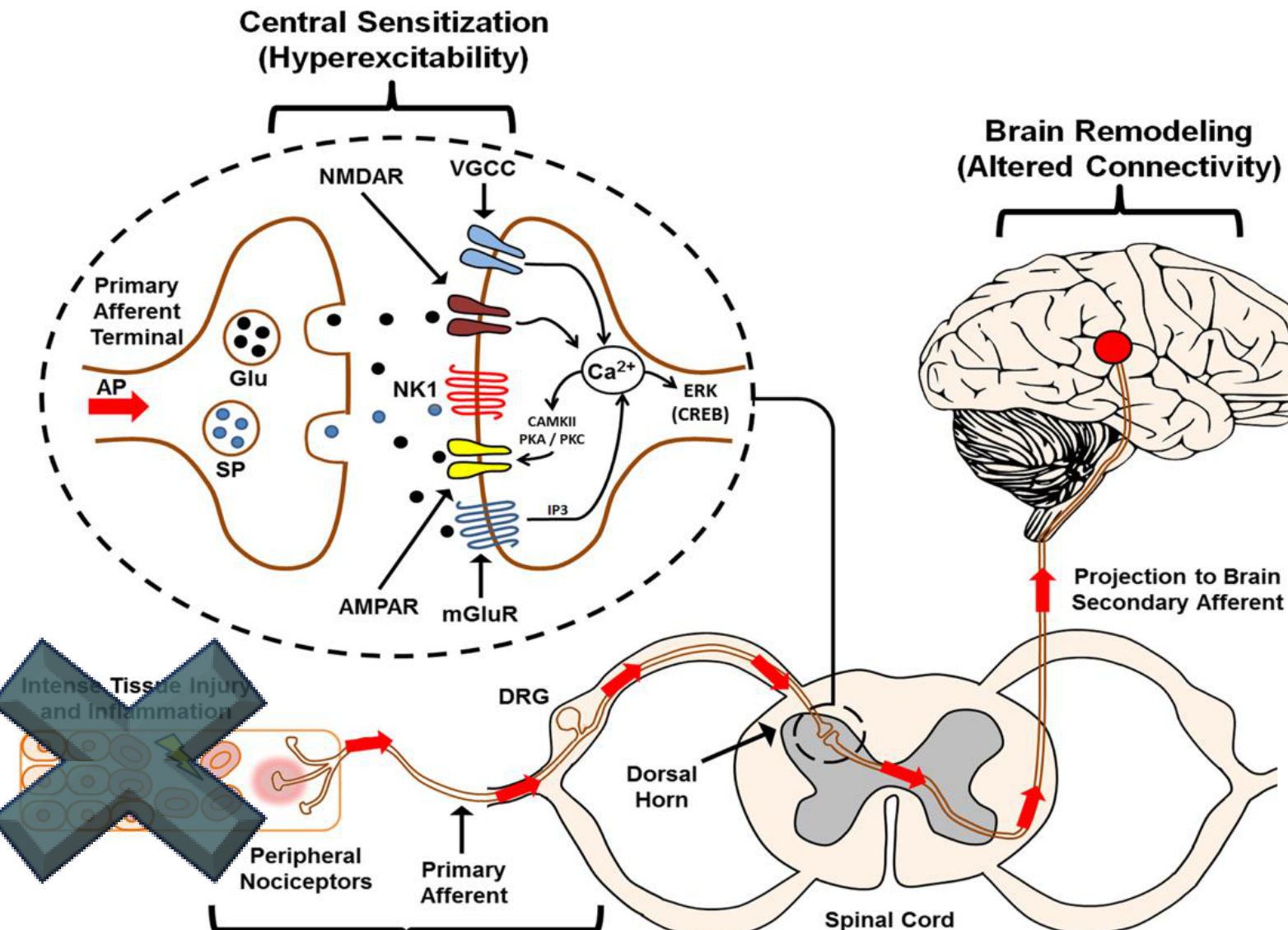 |
Pathophysiology
- Characterized by maladaptive plasticity.
- Involves altered connectivity within the central nervous system.
Clinical Nature of Nociplastic Pain27
- Evidence: Pain occurs without evidence of tissue damage or a clear physiological cause.
- Validity: The pain is “real” and has a neurophysiological basis.
- Contributing Factors: May be influenced by psychological stress.
- The pain is often triggered or maintained by emotional distress rather than physical injury.
 |  |
Comparative Analysis of Pain Types
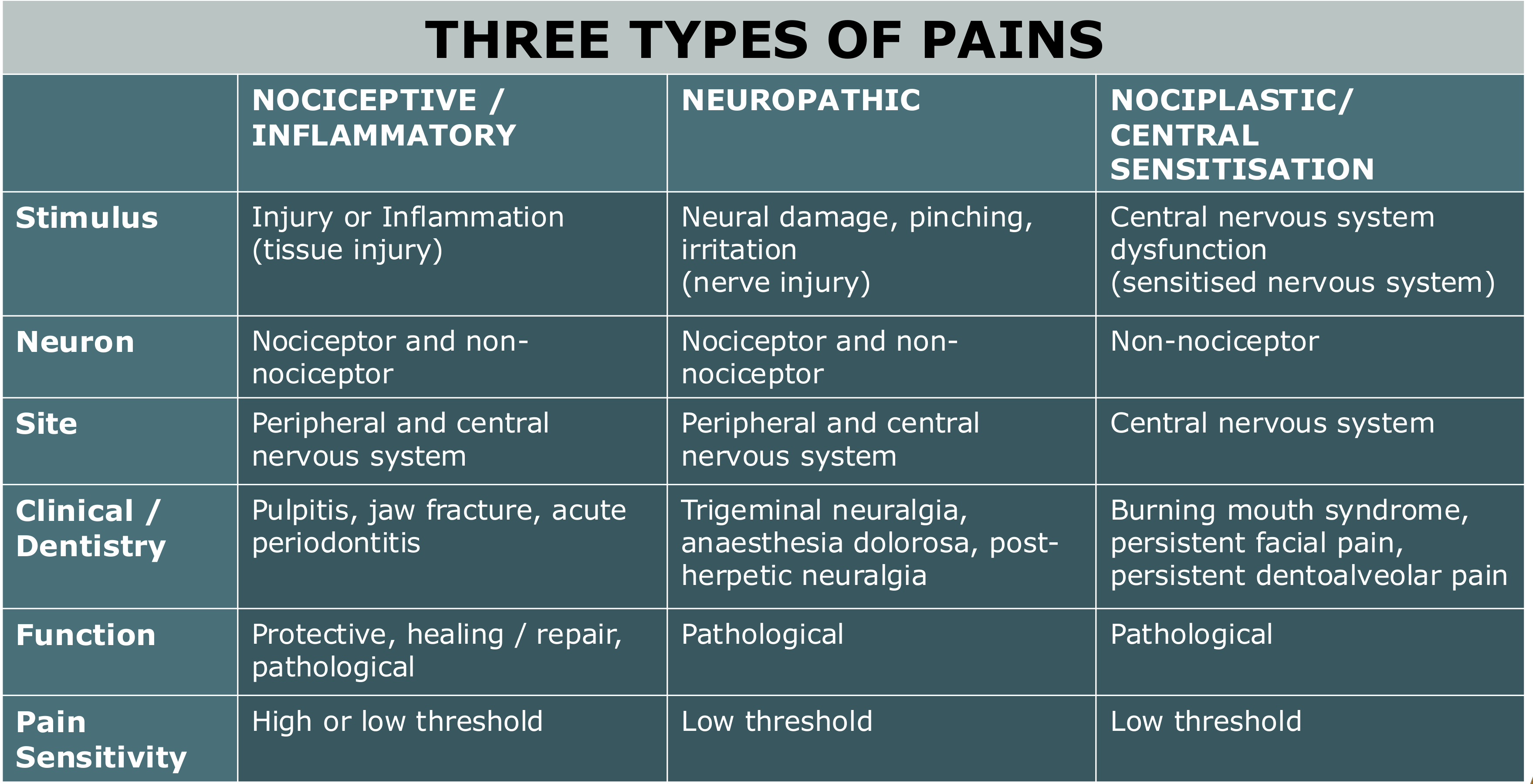
Comparison Table of Pain Types28
| Feature | Nociceptive / Inflammatory | Neuropathic | Nociplastic / Central Sensitisation |
|---|---|---|---|
| Stimulus | Injury or Inflammation (tissue injury) | Neural damage, pinching, irritation (nerve injury) | Central nervous system dysfunction (sensitised nervous system) |
| Neuron | Nociceptor and non-nociceptor | Nociceptor and non-nociceptor | Non-nociceptor |
| Site | Peripheral and central nervous system | Peripheral and central nervous system | Central nervous system |
| Clinical / Dentistry | Pulpitis, jaw fracture, acute periodontitis | Trigeminal neuralgia, anaesthesia dolorosa, post-herpetic neuralgia | Burning mouth syndrome, persistent facial pain, persistent dentoalveolar pain |
| Function | Protective, healing / repair, pathological | Pathological | Pathological |
| Pain Sensitivity | High or low threshold | Low threshold | Low threshold |
The Biopsychosocial Model of Pain
Presentation Overview29
- Pain Definition
- Is Pain Good or Bad?
- 3 Pains
- Biopsychosocial Model for Pain
- Definition & Classification of Orofacial Pain
- Take Home Message
Acute vs Chronic Pain Paradigms
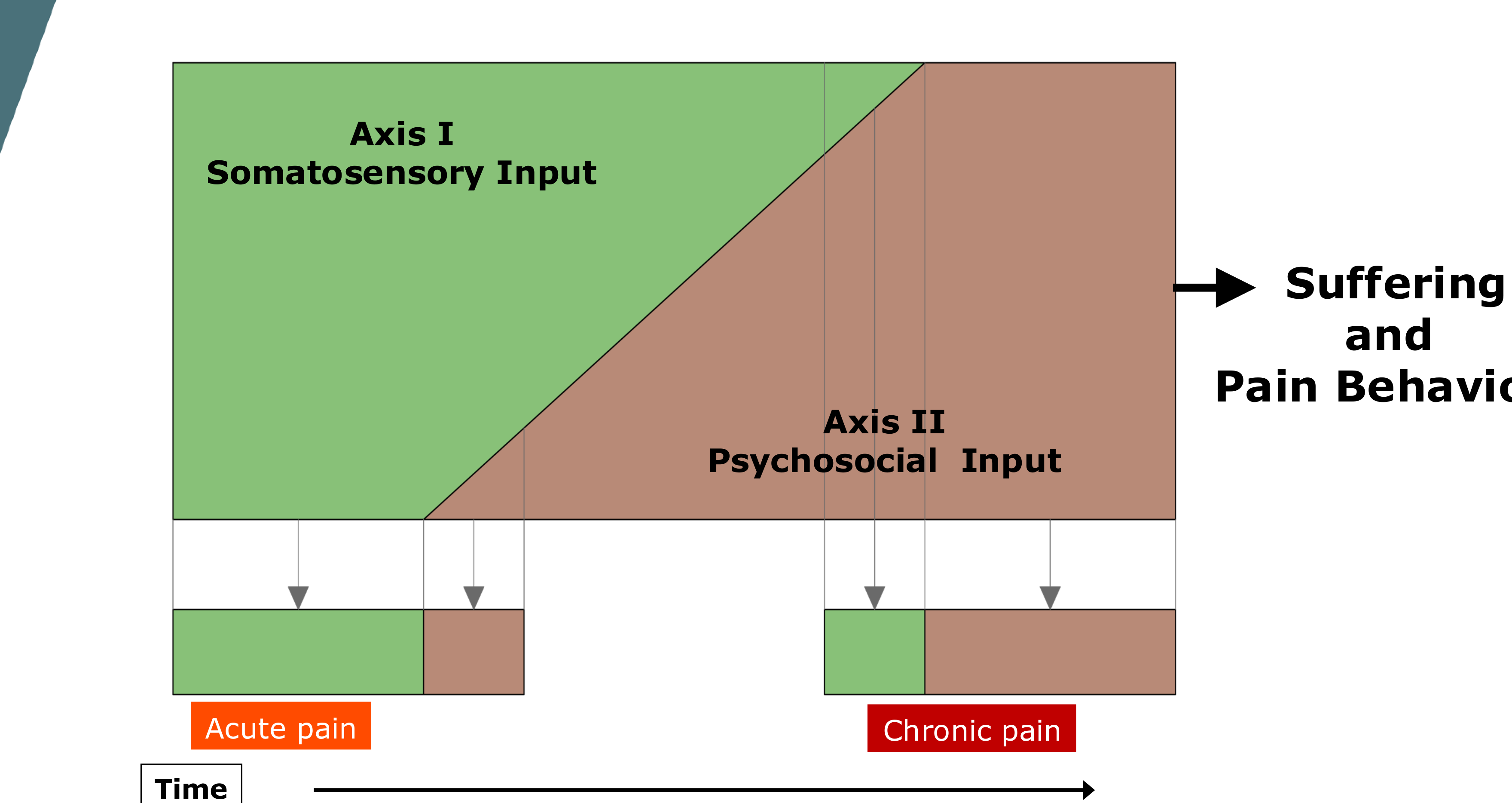
Characteristics of Chronic Pain30
- Chronic pain is defined as pain persisting beyond normal healing time.
- In chronic pain, the physical input is often small, while the psychosocial input is massive.
- Neuroplasticity may prolong and maintain the pain state.
 |  |
Chronic vs. Recurrent Pain Disorders
- Behavioral and psychological changes begin to manifest in chronic and recurrent states.
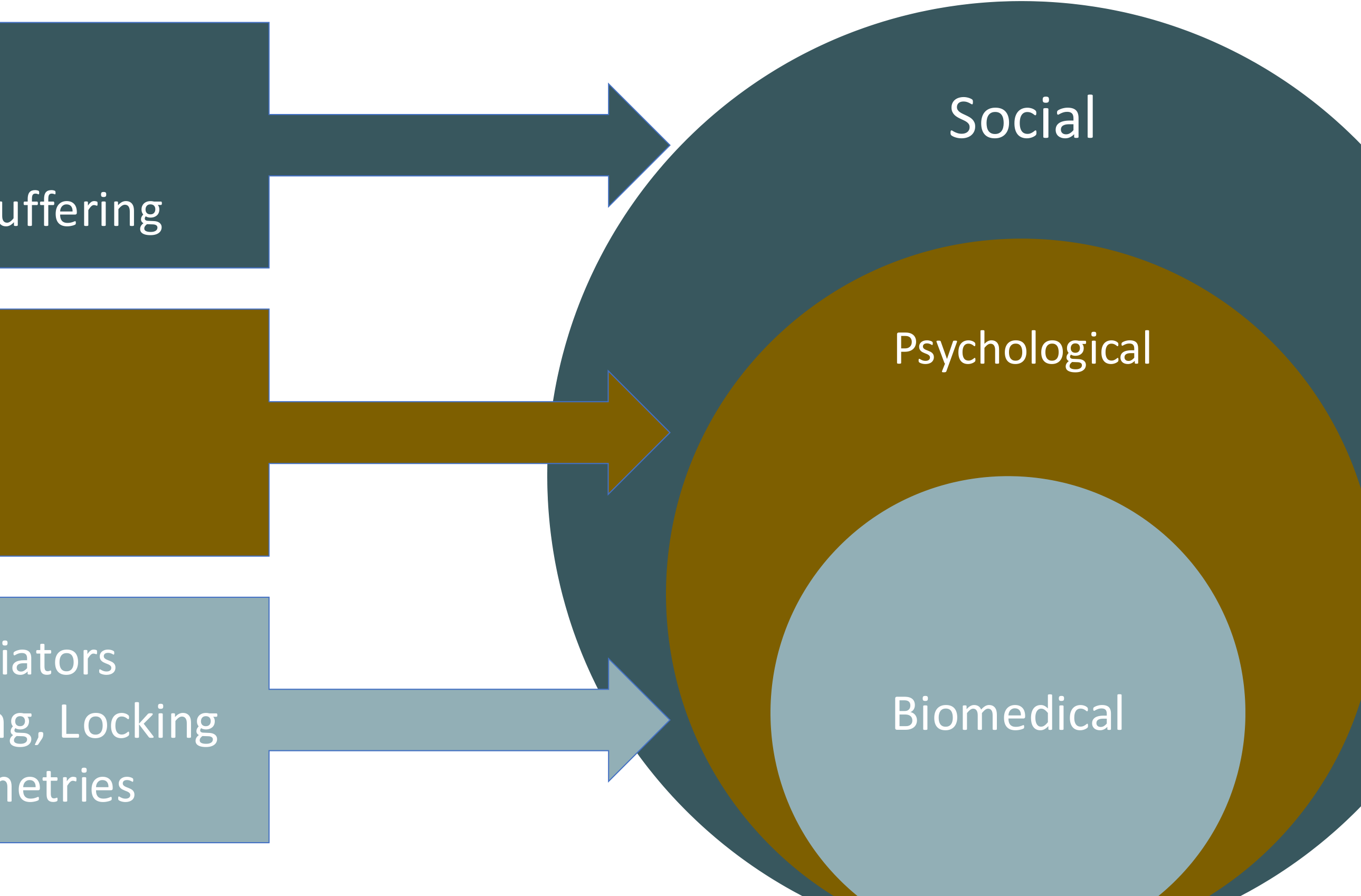
Axis I and Axis II Inputs31
 |  |
 |
Model Components32
- Axis I: Somatosensory Input (Green)
- Axis II: Psychosocial Input (Brown)
 |  |
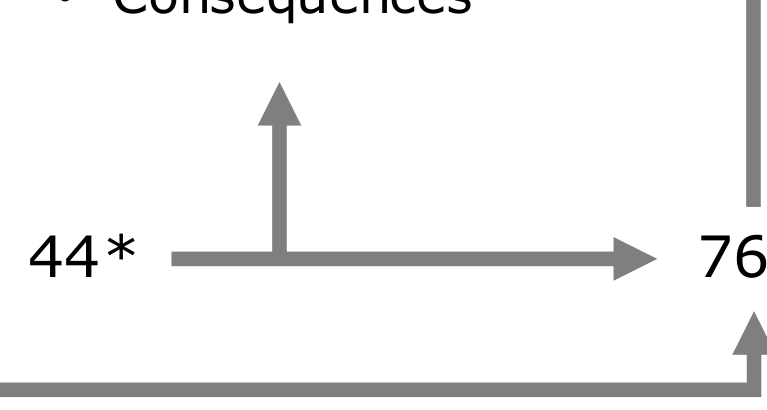
Outcomes of Combined Influences
- Combined inputs lead to Suffering and Pain Behavior.
Temporal Progression
- The model tracks the transition over time from Acute pain to **Chronic pain
- In acute pain, the somatosensory input is high. As pain becomes chronic, the psychosocial factors become the dominant drivers of suffering and behavior.**.
Economic Impact33
- 1 in 15 Australians live with chronic pain.
- Estimated cost: 44,979 per year.
Acute Pain Characteristics
- An unpleasant, dynamic psychophysiological process.
- Occurs in response to tissue trauma and related inflammatory processes.
- Provides survival value and plays a role in healing.
Chronic Pain Characteristics
- Maladaptive with little evolutionary benefit.
- Requires a shift in mindset from eradicating the problem to management.
- Focuses on functional and emotional resilience.
Longitudinal vs. Cross-Sectional Perspectives34
Pain assessment involves viewing the condition as a “motion picture” (longitudinal) rather than just a “snapshot” (cross-sectional), considering socioeconomic and healthcare contexts.
- A longitudinal view reveals that factors like generational trauma, childhood experiences, and lifestyle influence the pain experience long before the patient seeks treatment.
 |  |
 |
Influencing Factors Across the Lifespan
- Premorbid Characteristics and Demographics:
- Genes
- Lifestyle
- Learning history
- Culture
- Clinical Factors:
- Age at symptom onset and consult age
- Pathology and changes in pathology
- Treatments
- Psychological and Behavioral Factors:
- Beliefs and expectancies
- Behavior and consequences
- Resources:
- Interpersonal support
- Economic resources
Neurobiological Basis for Facial Pain
Amygdala Activation35
fMRI studies show higher amygdala activation for facial pain compared to hand pain, even when the pain intensity is rated the same.
 |  |
Neural Circuitry
- The Lateral parabrachial nucleus (PBL) is activated more strongly by noxious facial stimulation.
- A specific craniofacial monosynaptic connection exists between cranial sensory neurons and PBL-nociceptive neurons, enabling heightened affective pain.
- Unlike other body parts, the face does not habituate well to repeated painful stimuli (e.g., repeated slaps feel equally intense).
Clinical Case Application
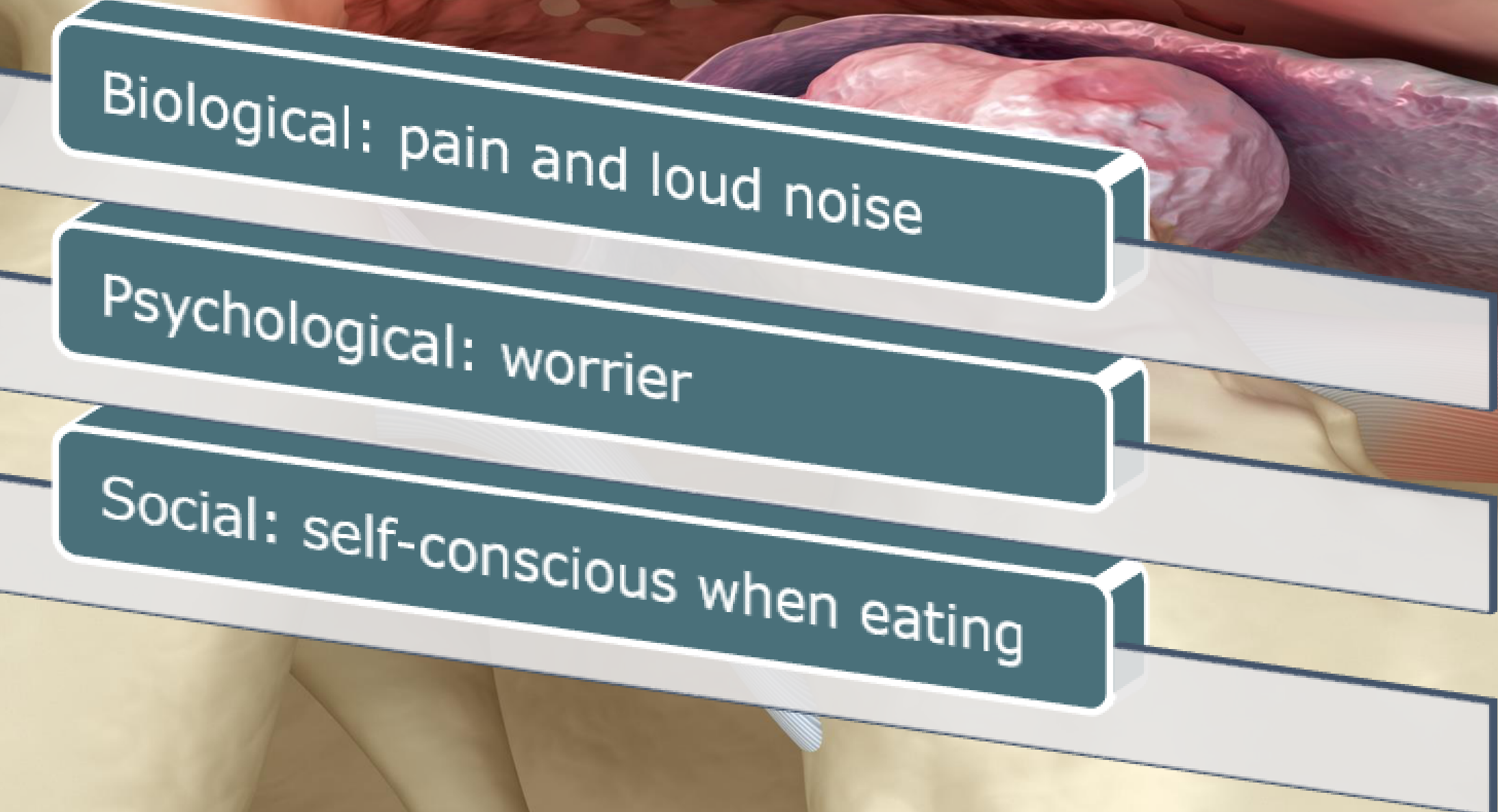
Case Presentation36
- Patient: 33-year-old female.
- Chief Complaint: Temporomandibular joint (TMJ) clicking and pain.
Psychological and Social Factors37
- Empathy and Social Bonding
- Isolation Induced Suffering
- Depression and Anxiety
- Somatisation
Clinical and Physical Factors
- Mechanisms and Mediators
- Clinical Pain, Clicking, and Locking
- Occlusion and Asymmetries
Case Study: 33-year-old Female
- Physical Symptoms: TMD clicking and pain diagnosed as disk displacement with reduction.
- Psychosocial Context: The patient is extremely embarrassed by the clicking. She recently broke up with a partner and believes a second date failed because of her "clicky jaw" during dinner.
- Clinical Insight: The primary issue is her anxiety and catastrophizing regarding her social life and relationships rather than the physical displacement.
Classification of Orofacial Pain
Presentation Agenda38
- Pain Definition
- Is Pain Good or Bad?
- 3 Pains
- Biopsychosocial Model for Pain
- Definition & Classification of Orofacial Pain
- Take Home Message
Definitions and Prevalence
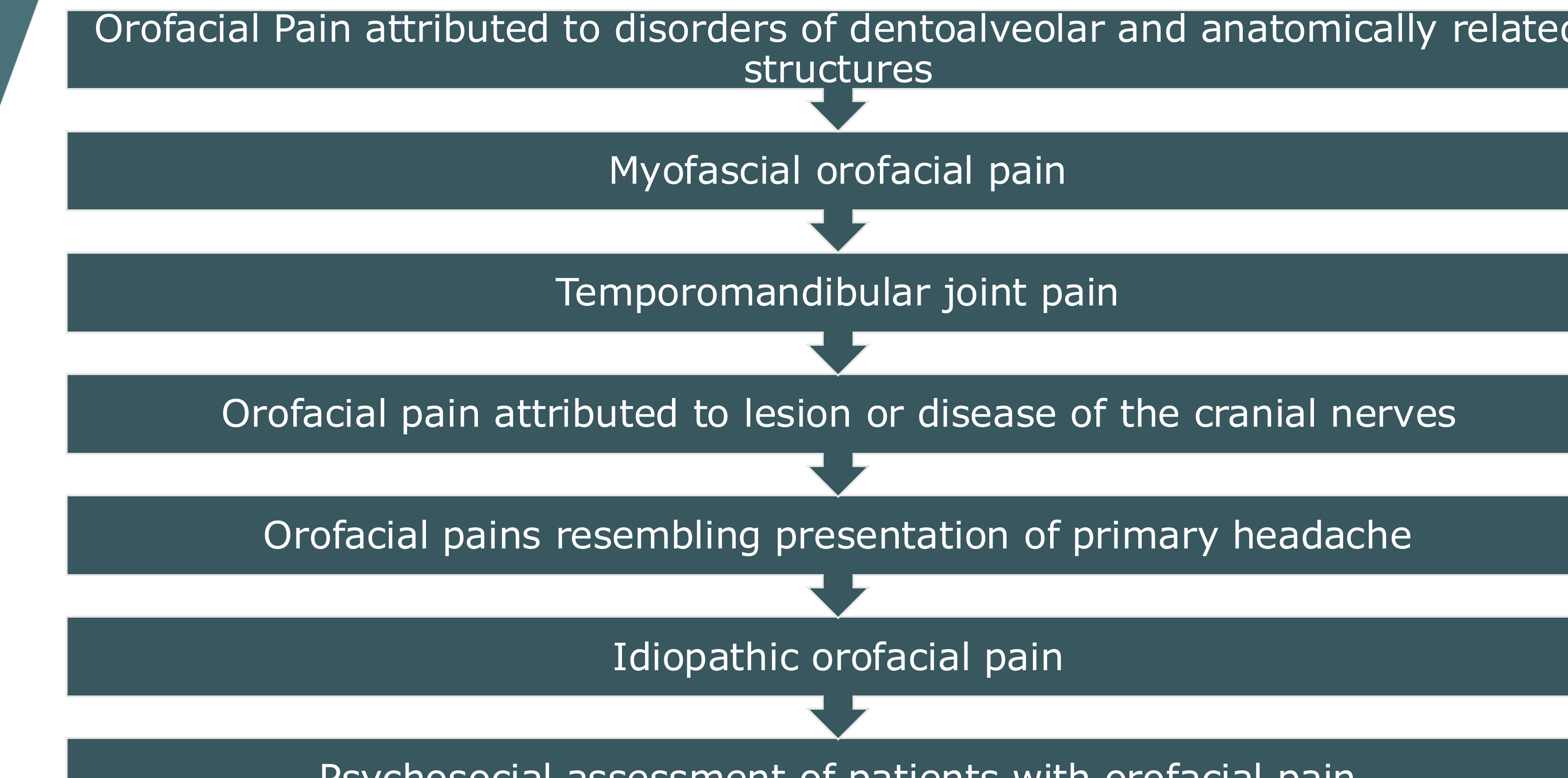
Orofacial Pain39
- Definition: Orofacial pain is pain perceived in the face and/or oral cavity.
- Prevalence: 17-26%
- Source: Porporatti AL et al. J Oral Facial Pain Headache. 2024 Sep;38(3):1-14.
Temporomandibular Disorders (TMD)
- Definition: A diverse group of musculoskeletal and neuromuscular conditions involving the TMJs, masticatory muscles, and associated structures.
- Prevalence: 4.6% (Isong et al. 2008)
- Source: Klasser & Romero Reyes (2023) Orofacial Pain: Guidelines for Assessment, Diagnosis, and Management 6th Ed. Quintessence Publishing
Diagnostic Framework and TMD Criteria40
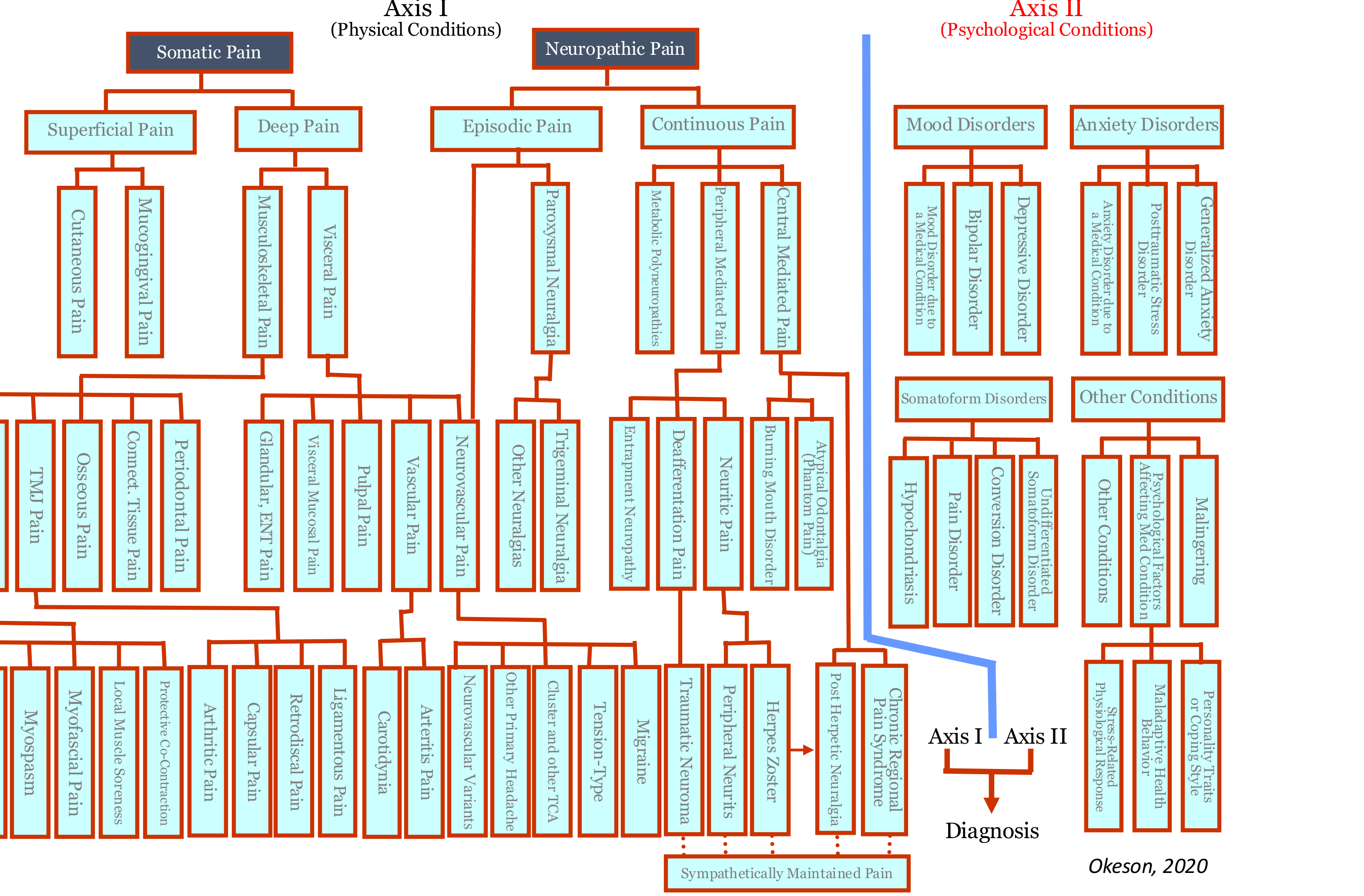
Diagnostic Axis Framework41
Axis I (Physical Conditions) + Axis II (Psychological Conditions) → Diagnosis
 |  |
 |
Axis I: Physical Conditions
- Somatic Pain
- Superficial Pain
- Cutaneous Pain
- Mucogingival Pain
- Deep Pain
- Musculoskeletal Pain
- Muscle Pain (Myospasm, Myofascial Pain, Central Mediated Myalgia, Myofascial Pain Syndrome)
- Musculoskeletal Pain
- Superficial Pain
- Neuropathic Pain
- Peripheral Mediated Pain
- Metabolic Polyneuropathies
- Entrapment Neuropathy
- Deafferentation Pain
- Neuritic Pain (e.g., Burning Mouth Disorder, Atypical Odontalgia)
- Trigeminal Neuralgia
- Other Primary Headache
- Cluster and other Trigeminal Autonomic Cephalalgias (TCA)
- Peripheral Mediated Pain
- Visceral Pain
- Musculoskeletal Pain
- Visceral Mucosal Pain
- Glandular, ENT Pain
- Pulpal Pain
- Vascular Pain
- Neurovascular Pain
- Capsular Pain
- Arthritic Pain
- Retrodiscal Pain
- Ligamentous Pain
- Central Mediated Pain
- Peripheral Neuritis
- Herpes Zoster
- Post Herpetic Neuralgia
- Complex Regional Pain Syndrome
- Sympathetically Maintained Pain
Axis II: Psychological Conditions
- Mood Disorders
- Mood Disorder due to a Medical Condition
- Bipolar Disorder
- Depressive Disorder
- Anxiety Disorders
- Anxiety Disorder due to a Medical Condition
- Posttraumatic Stress Disorder
- Generalized Anxiety Disorder
- Somatoform Disorders
- Conversion Disorder
- Pain Disorder, Undifferentiated
- Stress-Related Physiological Response
- Personality Traits or Coping Style
- Other Conditions
- Psychological Factors Affecting Medical Condition
- Malingering
- Hypochondriasis
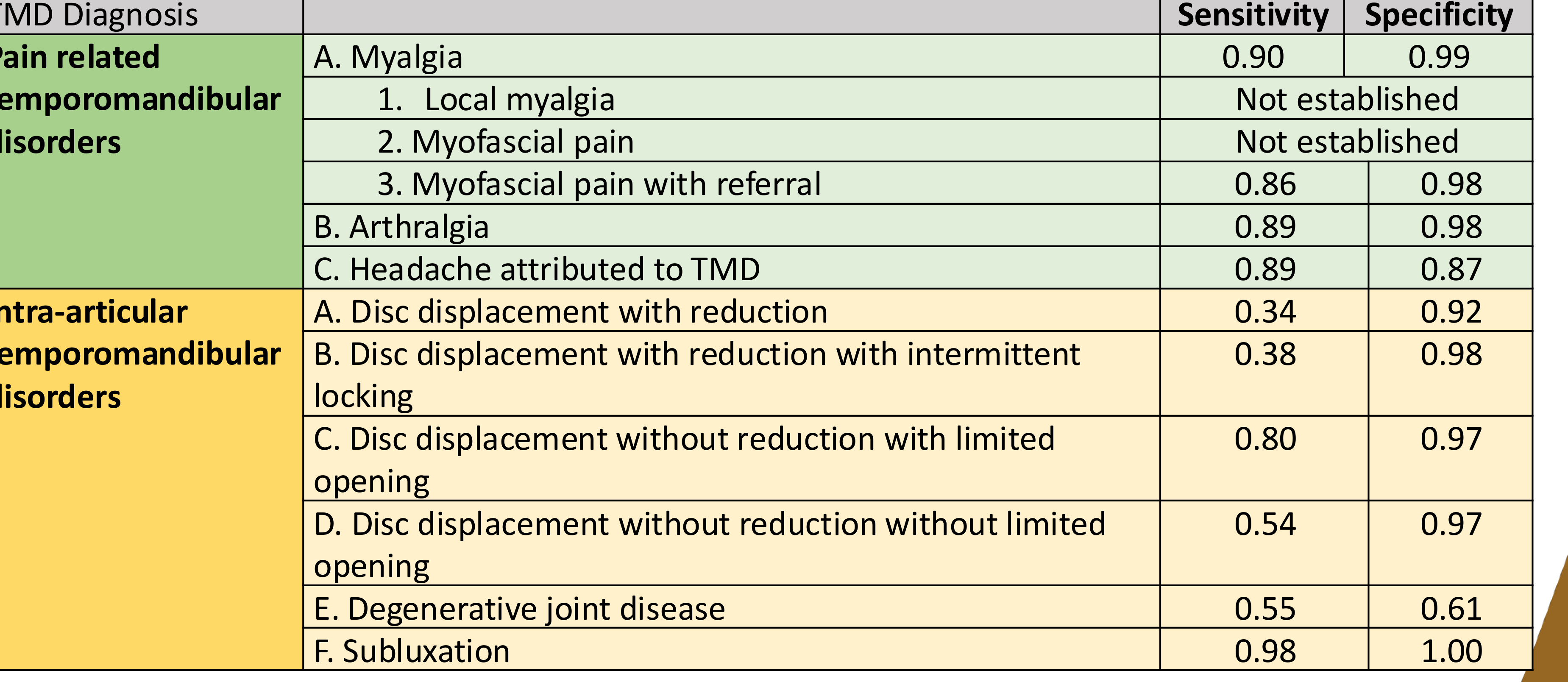
Diagnostic Criteria for TMD (DC/TMD)42
| TMD Diagnosis | Sensitivity | Specificity |
|---|---|---|
| Pain-Related TMD | ||
| A. Myalgia | 0.90 | 0.99 |
| 1. Local myalgia | Not established | Not established |
| 2. Myofascial pain | Not established | Not established |
| 3. Myofascial pain with referral | 0.86 | 0.98 |
| B. Arthralgia | 0.89 | 0.98 |
| C. Headache attributed to TMD | 0.89 | 0.87 |
| Intra-articular TMD | ||
| A. Disc displacement with reduction | 0.34 | 0.92 |
| B. Disc displacement with reduction with intermittent locking | 0.38 | 0.98 |
| C. Disc displacement without reduction with limited opening | 0.80 | 0.97 |
| D. Disc displacement without reduction without limited opening | 0.54 | 0.97 |
| E. Degenerative joint disease | 0.55 | 0.61 |
| F. Subluxation | 0.98 | 1.00 |
*Source: Schiffman et al. J Oral Facial Pain Headache 2014;28:6–27.
International Classification Standards
- The International Classification of Orofacial Pain (ICOP) serves as the primary international classification system for these conditions.
- There is no established relationship between occlusion (the bite) and orofacial pain.*
Conclusion and Summary4344

Presentation Overview45
- Pain Definition
- Is Pain Good or Bad?
- 3 Pains
- Biopsychosocial Model for Pain
- Definition & Classification of Orofacial Pain
- Take Home Message
Key Takeaways46
- There is a new definition of pain.
- Understand the 2020 IASP definition of pain.
- Three types of pain are enveloped around the biopsychosocial model.
- Recognize the three types of pain: Nociceptive, Neuropathic, and Nociplastic.
- Always conduct a psychosocial history with empathy.
- If you don’t believe the pain, believe the suffering.
- If you cannot find a physical cause for the pain, believe the patient's suffering.
- Orofacial pain… never a boring day.
THANK YOU!!!
Ramesh Balasubramaniam OAM
DENT5310 Orofacial Pain and Dental Sleep Medicine Module 16th April 2026

Footnotes
-
Original PDF page 1: L27 Defining Orofacial Pain-Final, p.1 ↩
-
Original PDF page 2: L27 Defining Orofacial Pain-Final, p.2 ↩
-
Original PDF page 3: L27 Defining Orofacial Pain-Final, p.3 ↩
-
Original PDF page 4: L27 Defining Orofacial Pain-Final, p.4 ↩
-
Original PDF page 5: L27 Defining Orofacial Pain-Final, p.5 ↩
-
Original PDF page 8: L27 Defining Orofacial Pain-Final, p.8 ↩
-
Original PDF page 7: L27 Defining Orofacial Pain-Final, p.7 ↩
-
Original PDF page 9: L27 Defining Orofacial Pain-Final, p.9 ↩
-
Original PDF page 10: L27 Defining Orofacial Pain-Final, p.10 ↩
-
Original PDF page 11: L27 Defining Orofacial Pain-Final, p.11 ↩
-
Original PDF page 12: L27 Defining Orofacial Pain-Final, p.12 ↩
-
Original PDF page 13: L27 Defining Orofacial Pain-Final, p.13 ↩
-
Original PDF page 14: L27 Defining Orofacial Pain-Final, p.14 ↩
-
Original PDF page 15: L27 Defining Orofacial Pain-Final, p.15 ↩
-
Original PDF page 16: L27 Defining Orofacial Pain-Final, p.16 ↩
-
Original PDF page 17: L27 Defining Orofacial Pain-Final, p.17 ↩
-
Original PDF page 18: L27 Defining Orofacial Pain-Final, p.18 ↩
-
Original PDF page 19: L27 Defining Orofacial Pain-Final, p.19 ↩
-
Original PDF page 20: L27 Defining Orofacial Pain-Final, p.20 ↩
-
Original PDF page 21: L27 Defining Orofacial Pain-Final, p.21 ↩
-
Original PDF page 22: L27 Defining Orofacial Pain-Final, p.22 ↩
-
Original PDF page 23: L27 Defining Orofacial Pain-Final, p.23 ↩
-
Original PDF page 24: L27 Defining Orofacial Pain-Final, p.24 ↩
-
Original PDF page 25: L27 Defining Orofacial Pain-Final, p.25 ↩
-
Original PDF page 26: L27 Defining Orofacial Pain-Final, p.26 ↩
-
Original PDF page 27: L27 Defining Orofacial Pain-Final, p.27 ↩
-
Original PDF page 28: L27 Defining Orofacial Pain-Final, p.28 ↩
-
Original PDF page 29: L27 Defining Orofacial Pain-Final, p.29 ↩
-
Original PDF page 30: L27 Defining Orofacial Pain-Final, p.30 ↩
-
Original PDF page 31: L27 Defining Orofacial Pain-Final, p.31 ↩
-
Original PDF page 35: L27 Defining Orofacial Pain-Final, p.35 ↩
-
Original PDF page 32: L27 Defining Orofacial Pain-Final, p.32 ↩
-
Original PDF page 33: L27 Defining Orofacial Pain-Final, p.33 ↩
-
Original PDF page 34: L27 Defining Orofacial Pain-Final, p.34 ↩
-
Original PDF page 36: L27 Defining Orofacial Pain-Final, p.36 ↩
-
Original PDF page 37: L27 Defining Orofacial Pain-Final, p.37 ↩
-
Original PDF page 38: L27 Defining Orofacial Pain-Final, p.38 ↩
-
Original PDF page 39: L27 Defining Orofacial Pain-Final, p.39 ↩
-
Original PDF page 40: L27 Defining Orofacial Pain-Final, p.40 ↩
-
Original PDF page 43: L27 Defining Orofacial Pain-Final, p.43 ↩
-
Original PDF page 41: L27 Defining Orofacial Pain-Final, p.41 ↩
-
Original PDF page 42: L27 Defining Orofacial Pain-Final, p.42 ↩
-
Original PDF page 45: L27 Defining Orofacial Pain-Final, p.45 ↩
-
Original PDF page 47: L27 Defining Orofacial Pain-Final, p.47 ↩
-
Original PDF page 44: L27 Defining Orofacial Pain-Final, p.44 ↩
-
Original PDF page 46: L27 Defining Orofacial Pain-Final, p.46 ↩