History and Examination Including DC/TMD1
Ramesh Balasubramaniam OAM
DENT5310
Orofacial Pain and Dental Sleep Medicine Module
16th April 2026
Disclosures
Presenter Information2
Ramesh Balasubramaniam OAM Associate Professor Discipline Lead in Oral Medicine UWA Dental School The University of Western Australia
Additional Contributors
The lecture includes contributions from colleagues Dr. Sabina (internal arrangements), Dr. Lasan, and Dr. Sapita.
Conflict of Interest Statement
Neither I nor my immediate family have any financial interests that would create a conflict of interest or restrict my independent judgment with regard to the content of this presentation.
Introduction to Temporomandibular Disorders3
“Temporomandibular Disorders (TMD) is a collective term for a group of musculoskeletal and neuromuscular conditions which includes several clinical signs and symptoms involving the muscles of mastication, the temporomandibular joint and associated structures” – DC/TMD
Joint Stability
The lecturer describes the TMJ as inherently unstable, comparing its shape to "knocking a ball on a hill." There is "nothing stable" about the TMJ.
Temporomandibular Joint Anatomy
Anatomical Overview4
- Two incongruent parts: Mandibular condyle and Glenoid fossa
- Articular disc positioned between the condyle and fossa
- Disc divides the joint cavity into upper and lower compartments
- Central part of the disc: Avascular, not innervated
- Retrodiscal tissue: Highly innervated and vascularised
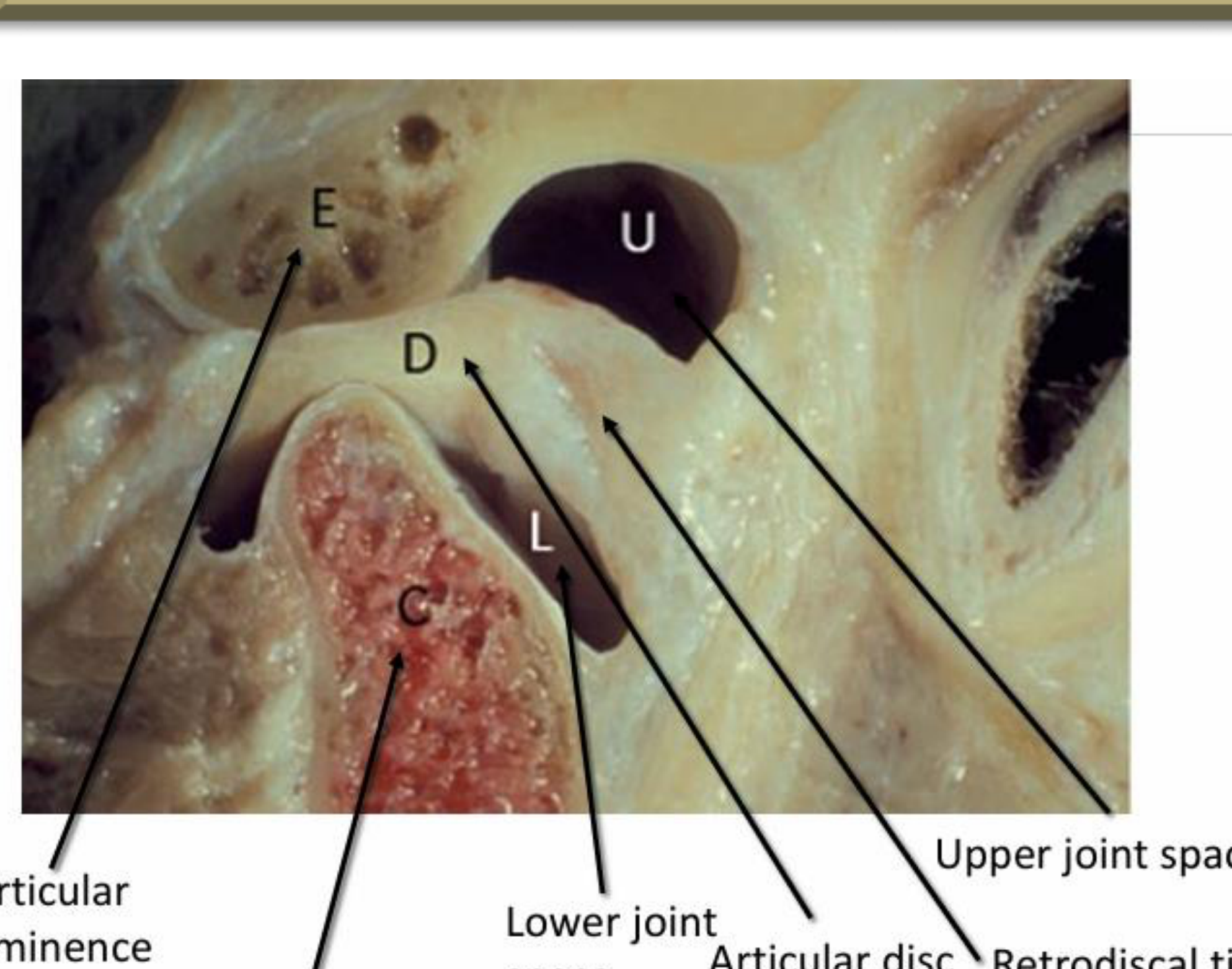
Anatomical Label Guide
- (E) Articular eminence
- (C) Condyle
- (L) Lower joint space
- (D) Articular disc
- (U) Upper joint space
- (B) Retrodiscal tissue
Joint Structure and Components
Fibrous Capsule and Attachments5
 |  |
Characteristics of the Joint Capsule6
- Joint is encapsulated by a fibrous capsule
- Attached to temporal bone along fossa and condyle
- Loose arrangement of connective tissue
Aetiology and Risk Factors of TMD
Historical Perspectives on Occlusion7
Historically, it was thought that TMD was caused by occlusal factors. This perspective resulted in therapies involving changing the patient’s occlusion.
- There is no strong association or correlation between malocclusions and TMD, including edentulous patients, overbites, balancing/non-balancing contacts, canine guidance, or vertical dimension issues.
- The concept of "centric relation" is challenged as a non-reproducible position that changes based on head tilt or posture (sitting up vs. lying down).
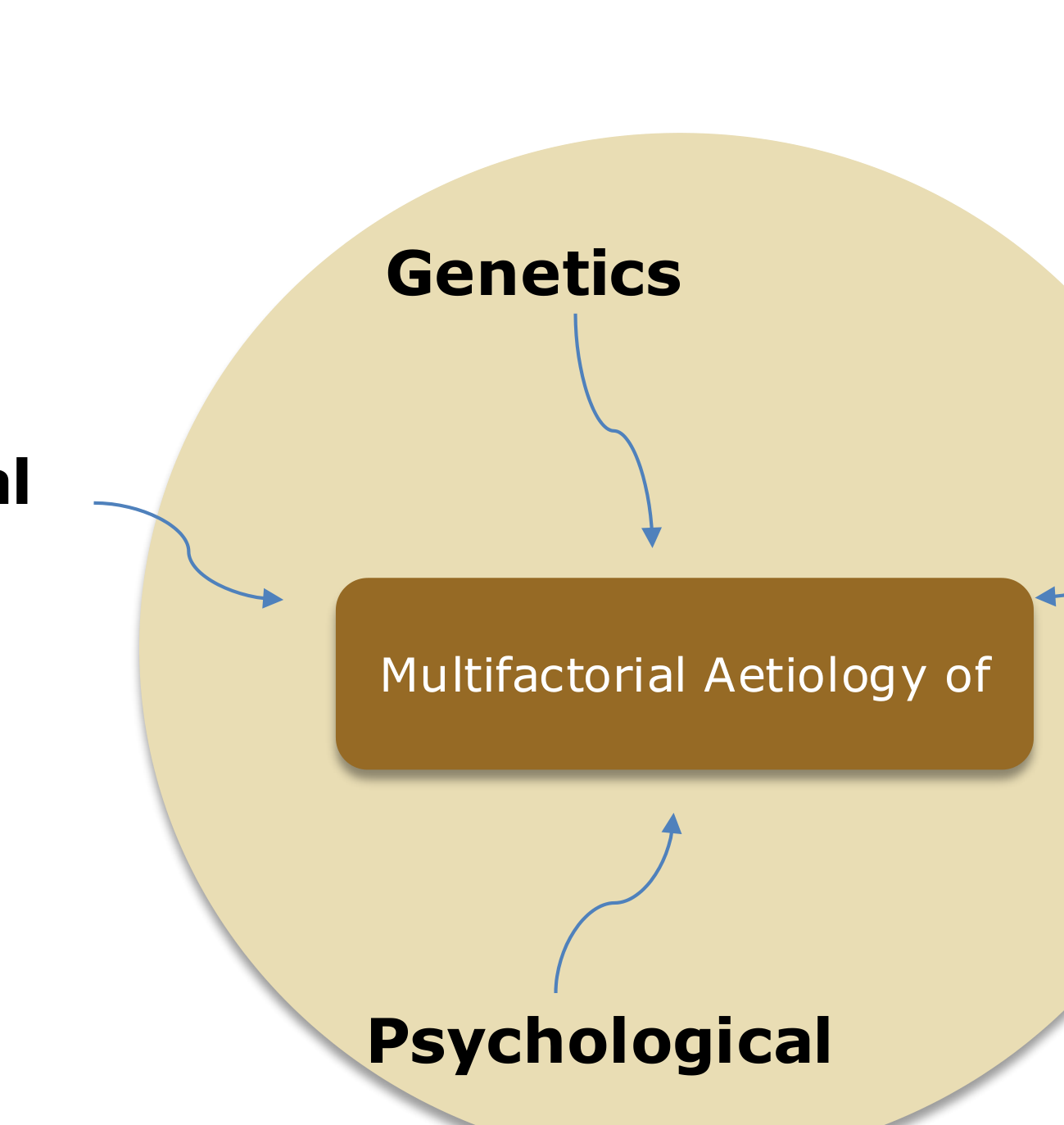
Contemporary Biopsychosocial Model
Risk Factors and Phenotypes8
- Occlusion is not considered a contributor to TMD.
- TMD is a complex interaction of genetics, environment, and psychology rather than a simple cause-and-effect relationship.
- Two principal intermediate phenotypes contribute to onset and persistence (constellation of risk factors).
- Genetic regulation and environmental contributions interact with intermediate phenotypes to contribute to onset and persistence.
- Time is a critical factor.
Environmental Contributions
- Physical: Trauma, abuse, infection, smoking
- Specific physical triggers include trauma from motor vehicle accidents, excessive gum chewing habits, or clinical procedures requiring the mouth to be open for extended periods.
- Psychological: Life stressors
- Culture: Health beliefs
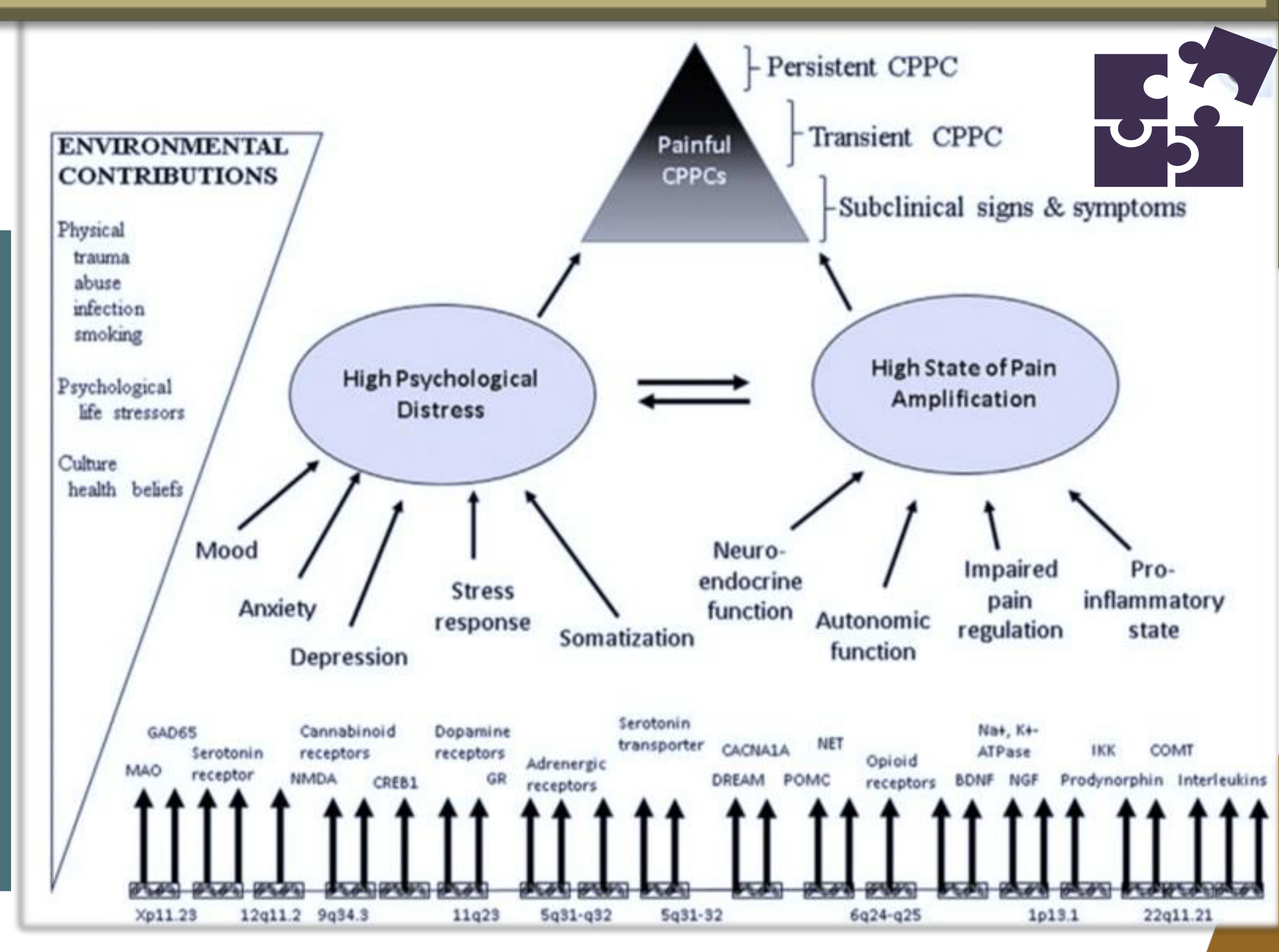
Psychological Distress and Pain Amplification
High Psychological Distress correlates with a High State of Pain Amplification:
- Psychological Factors: Increased mood disturbances, anxiety, depression, stress response, and somatization.
- Physiological Factors: Increased neuroendocrine function, autonomic function, impaired pain regulation, and pro-inflammatory state.
Clinical Presentations
- Painful Chronic Overlapping Pain Conditions (COPCs)
- Persistent CPPC
- Transient CPPC
- Subclinical signs and symptoms
Genetic Markers
Various genetic markers and receptors are associated with these conditions, including:
- GAD65, MAO, Serotonin receptors/transporters, Cannabinoid receptors, NMDA, Dopamine receptors, CREB1, Adrenergic receptors, GR, CACNA1A, DREAM, NET, POMC, Opioid receptors, Na+, K+ ATPase, BDNF, NGF, IKK, Prodynorphin, COMT, and Interleukins.
Genetic and Psychological Contributions
Behavioral and Psychological Factors9
Factors associated with the risk of TMD onset and chronicity include:
- Depression
- Anxiety
- Somatization
- Catastrophising
- PTSD
- Affective distress
 |  |  |
 |  |
Genetic and Biological Factors
- 5 main gene polymorphisms
- Nociceptive pathways
- Inflammation
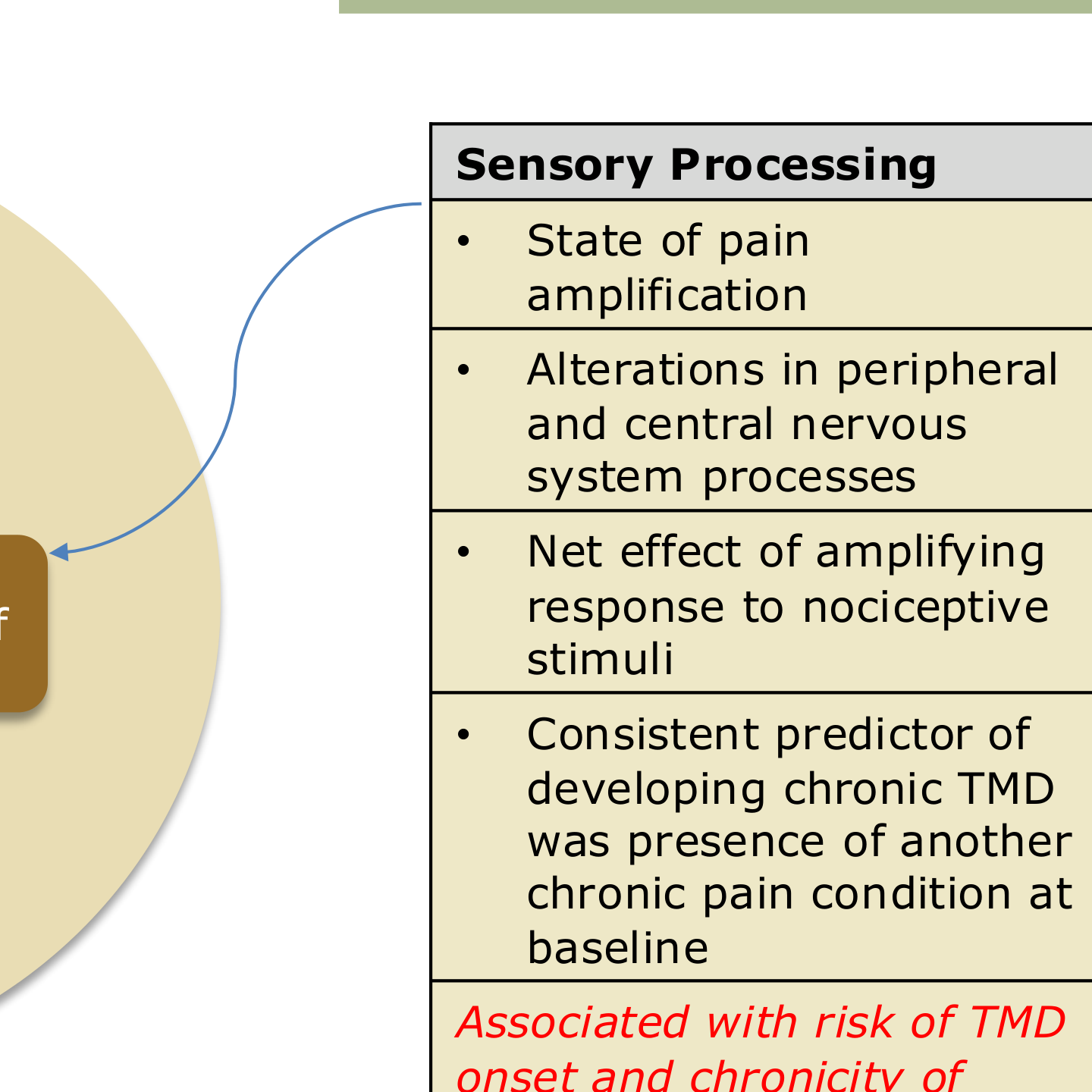
Sensory Processing
- State of pain amplification
- Alterations in peripheral and central nervous system processes
- Net effect of amplifying response to nociceptive stimuli
- A consistent predictor of developing chronic TMD was the presence of another chronic pain condition at baseline.
- These factors are associated with the risk of TMD onset and chronicity.
Classification and Diagnostic Criteria
Selection of Diagnostic Framework10
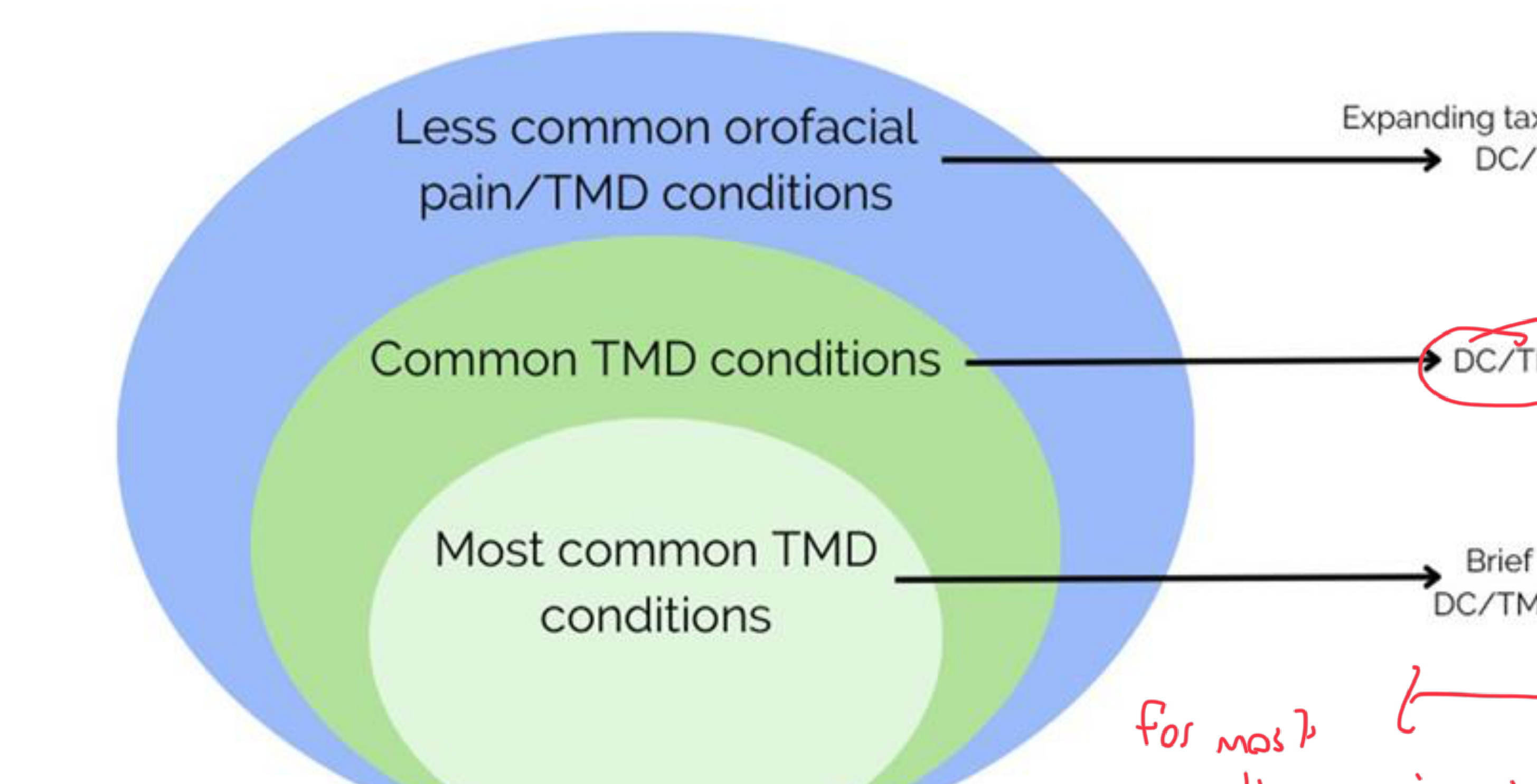
The choice of diagnostic criteria depends on the prevalence and complexity of the condition:
- Brief DC/TMD: Utilized for the most common TMD conditions.
- ==Brief DC/TMD (bDC/TMD): A newer, non-validated version recommended for general dental practice to save time (takes less than 10 minutes).==
- DC/TMD: Utilized for common TMD conditions. (Note: For most practitioners, this framework is adequate).
- Expanding Taxonomy of the DC/TMD: Utilized for less common orofacial pain and TMD conditions.
- Used primarily in specialist-level practice for detailed or serious conditions (e.g., tumors, ankylosis, fibromyalgia).
Overview of DC/TMD Framework
Dual Axis Diagnostic Criteria11
The Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) provides a standardized, reliable protocol (achieving 80%–90% sensitivity) for clinical and research applications.
- Axis I: Physical Diagnoses
- Covers the most common pain and non-pain related TMDs.
- Note: Relies on clinical examination; has low specificity for disc displacements compared to CT/MRI.
- Axis II: Biobehavioral Assessments
- Evaluates psychosocial assessment and status.
- Evaluates the patient’s pain disorder.
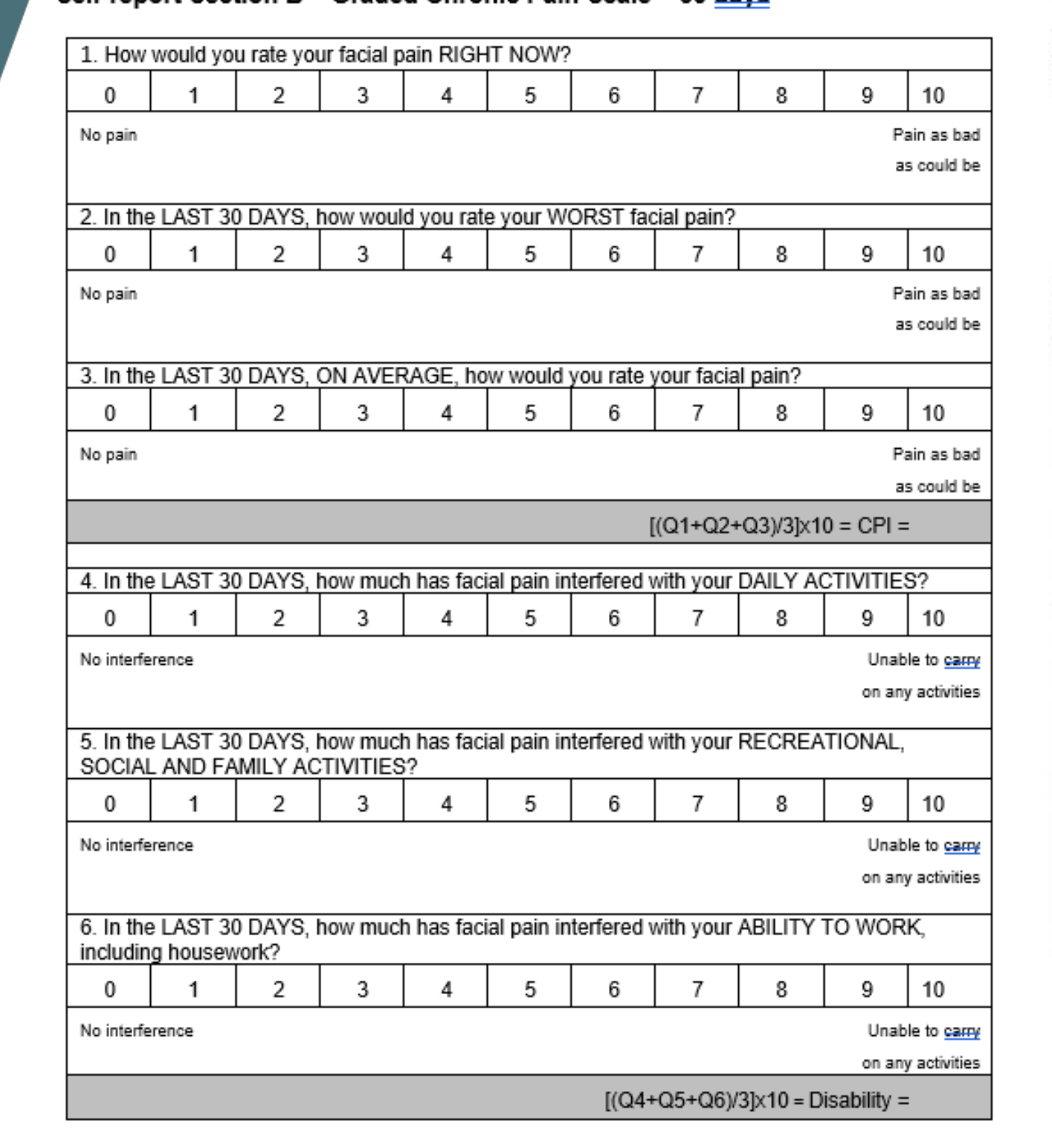
- Includes the Graded Chronic Pain Scale to measure pain intensity and disability.
Implementation Notes
- Expanded Taxonomy: Serves as a preliminary diagnosis for less common disorders.
- Resources: Documentation is available for download at the International RDC/TMD Consortium Network website.
Diagnostic Criteria for Pain Disorders
Myalgia (ICD-9 729.1)12
- History Criteria: Pain in a masticatory structure (SQ3) modified by jaw movement, function, or parafunction (SQ4).
- Examination Criteria: Confirmation of pain in masticatory muscle(s) (E1a) and familiar pain in the temporalis or masseter with palpation or maximum opening (E4b, E4c, E9, or E10).
- Statistics: Sensitivity 0.90; Specificity 0.95.
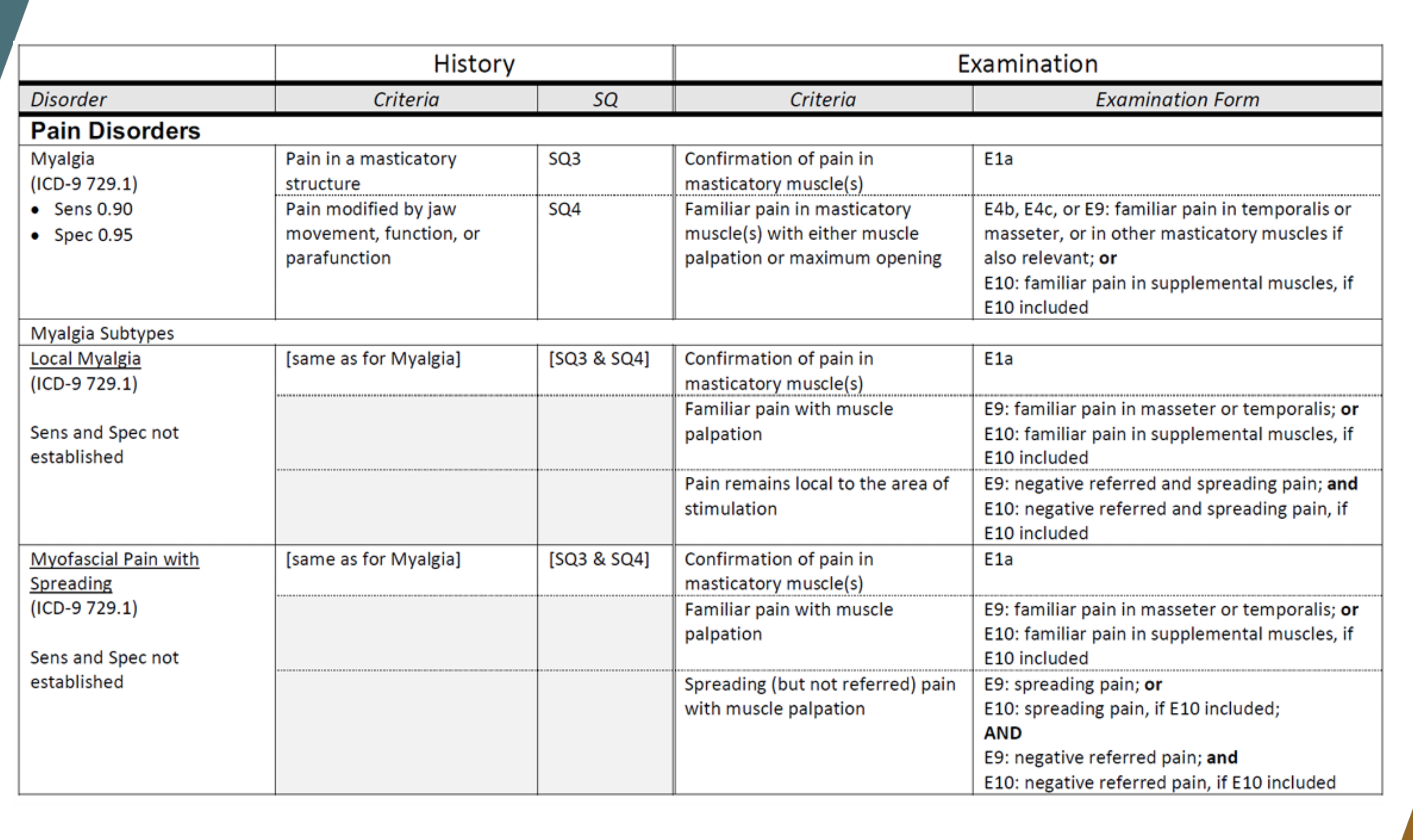
Myalgia Subtypes
Local Myalgia
- History: Same as Myalgia (SQ3 & SQ4).
- Examination: Familiar pain with muscle palpation (E9 or E10) that remains local to the area of stimulation (negative referred and spreading pain).
Myofascial Pain with Spreading
- History: Same as Myalgia (SQ3 & SQ4).
- Examination: Familiar pain with muscle palpation (E9 or E10) and spreading pain (but not referred pain) with muscle palpation.
Myofascial Pain with Referral (ICD-9 729.1)13
- History: Same as Myalgia (SQ3 & SQ4).
- Examination: Confirmation of pain in masticatory muscle(s) (E1a) and familiar pain with muscle palpation (E9 or E10) resulting in positive referred pain. - Example: Pressing the masseter refers a headache.
- Statistics: Sensitivity 0.86; Specificity 0.98.
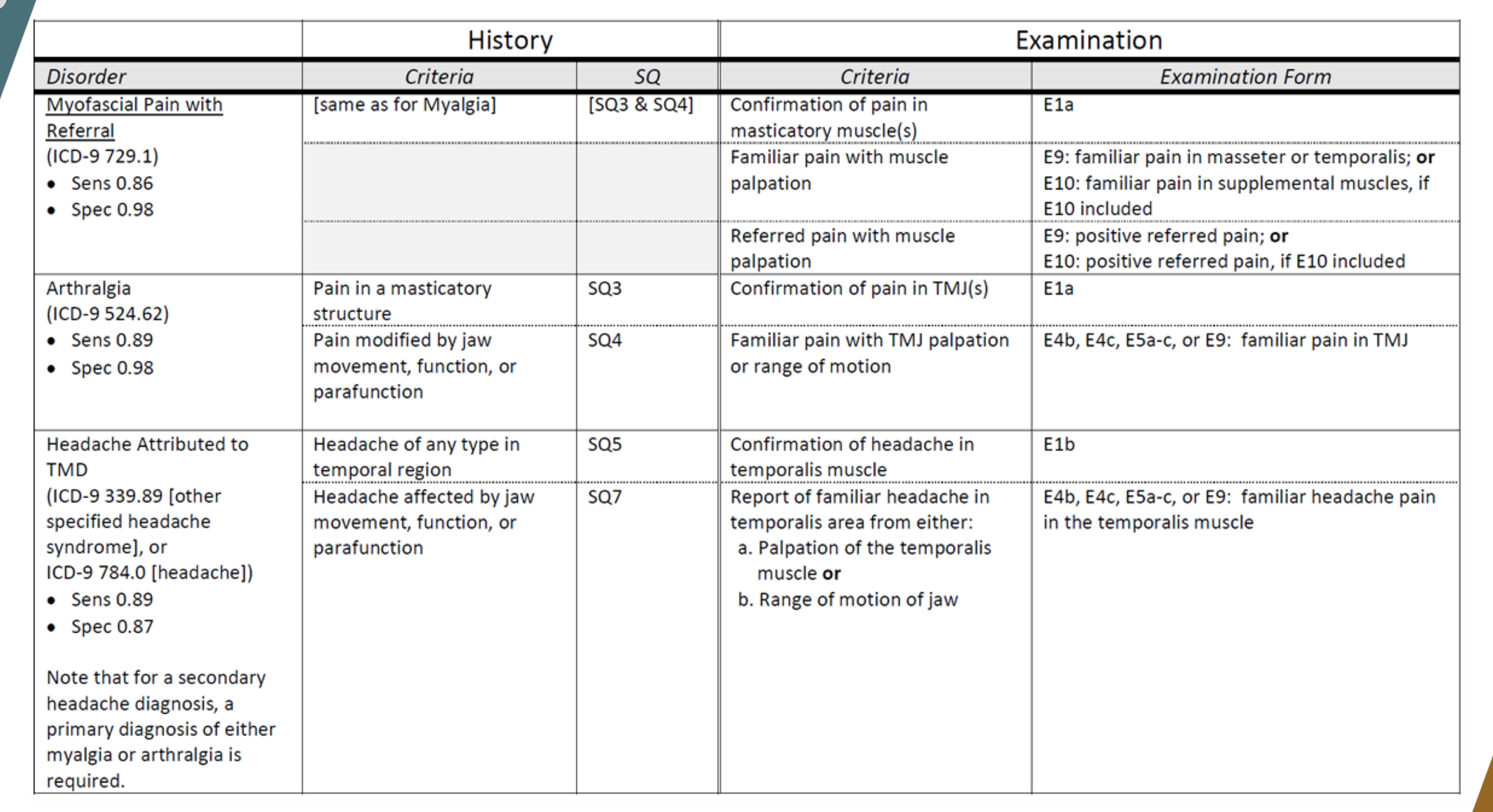
Arthralgia (ICD-9 524.62)
- History: Pain in a masticatory structure (SQ3) modified by jaw movement, function, or parafunction (SQ4).
- Examination: Confirmation of pain in TMJ(s) (E1a) and familiar pain with TMJ palpation or range of motion (E4b, E4c, E5a-c, or E9).
- Statistics: Sensitivity 0.89; Specificity 0.98.
Headache Attributed to TMD (ICD-9 339.89 or 784.0)
- History: Headache of any type in the temporal region (SQ5) affected by jaw movement, function, or parafunction (SQ7).
- Examination: Confirmation of headache in the temporalis muscle (E1b) and report of familiar headache in the temporalis area from palpation or range of motion (E4b, E4c, E5a-c, or E9).
- Statistics: Sensitivity 0.89; Specificity 0.87.
- Note: A secondary headache diagnosis requires a primary diagnosis of either myalgia or arthralgia.
Diagnostic Criteria for Joint Disorders
Disc Displacement with Reduction (ICD-9 524.63)14
- History: Current TMJ noises (SQ8) or patient reports noise during examination.
- Examination: Click(s) with opening and closing (E6), or click with opening/closing AND click with lateral/protrusive movements (E7).
- Statistics: Sensitivity 0.34; Specificity 0.92.
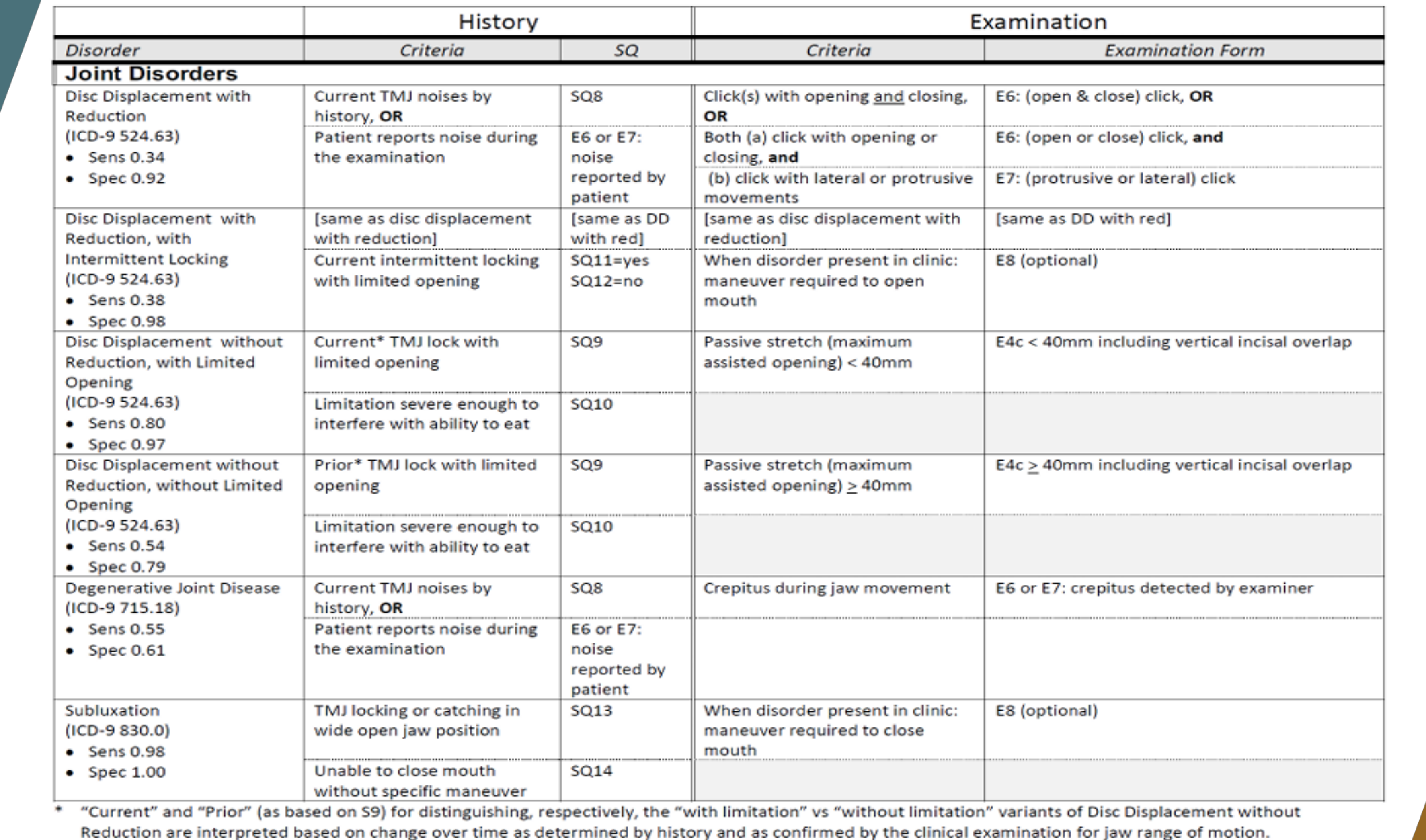
Disc Displacement with Reduction, with Intermittent Locking (ICD-9 524.63)
- History: Same as DD with reduction, plus current intermittent locking with limited opening (SQ11=yes, SQ12=no).
- Examination: Maneuver required to open mouth when disorder is present in clinic (E8).
- Statistics: Sensitivity 0.38; Specificity 0.98.
Disc Displacement without Reduction, with Limited Opening (ICD-9 524.63)
- History: Current TMJ lock with limited opening (SQ9) severe enough to interfere with eating (SQ10).
- Examination: Passive stretch (maximum assisted opening) < 40mm (E4c).
- Statistics: Sensitivity 0.80; Specificity 0.97.
Disc Displacement without Reduction, without Limited Opening (ICD-9 524.63)
- History: Prior TMJ lock with limited opening (SQ9) severe enough to interfere with eating (SQ10).
- Clinical Note: The joint is considered "completely locked" in this state.
- Examination: Passive stretch (maximum assisted opening) ≥ 40mm (E4c).
- Statistics: Sensitivity 0.54; Specificity 0.79.
Degenerative Joint Disease (ICD-9 715.18)
- History: Current TMJ noises (SQ8) or patient reports noise during examination.
- Examination: Crepitus detected by examiner during jaw movement (E6 or E7).
- Represents arthritic changes in the joint.
- Statistics: Sensitivity 0.55; Specificity 0.61.
Subluxation (ICD-9 830.0)
- History: TMJ locking or catching in wide open jaw position (SQ13) and unable to close mouth without specific maneuver (SQ14).
- Examination: Maneuver required to close mouth when disorder is present in clinic (E8).
- The joint catches or feels "catchy" when opening wide.
- ==Luxation: The joint completely comes out of the socket.==
- Statistics: Sensitivity 0.98; Specificity 1.00.
Expanded Taxonomy for TMD
I. Temporomandibular Joint Disorders15
- Joint Pain
- A. Arthralgia
- B. Arthritis
- Joint Disorders
- A. Disc disorders
- Disc displacement with reduction
- Disc displacement with reduction with intermittent locking
- Disc displacement without reduction with limited opening
- Disc displacement without reduction without limited opening
- B. Hypomobility disorders other than disc disorders
- Adhesions/Adherence
- Ankylosis (Fibrous or Osseous)
- C. Hypermobility disorders
- Dislocations (Subluxation or Luxation)
- A. Disc disorders
- Joint Diseases
- A. Degenerative joint disease (Osteoarthrosis or Osteoarthritis)
- B. Systemic arthritides
- C. Condylitis/Idiopathic condylar resorption
- D. Osteochondritis dissecans
- E. Osteonecrosis
- F. Neoplasm
- G. Synovial Chondromatosis
- Fractures
- Congenital/Developmental Disorders
- A. Aplasia
- B. Hypoplasia
- C. Hyperplasia
II. Masticatory Muscle Disorders16
- Muscle Pain
- A. Myalgia (Local myalgia, Myofascial pain, Myofascial pain with referral)
- B. Tendonitis
- C. Myositis
- D. Spasm (extremely rare)
- Contracture
- Hypertrophy
- Neoplasm
- Movement Disorders
- A. Orofacial dyskinesia
- B. Oromandibular dystonia
- Masticatory muscle pain attributed to systemic/central pain disorders
- A. Fibromyalgia/widespread pain
III. Headache
- Headache attributed to TMD
IV. Associated Structures
- Coronoid hyperplasia
History Taking Protocol17
“Nothing is more critical to success than beginning with all the necessary data”

Chief Complaint and Pain Location
Patient Interview18
- What brings you in today?
- Can you describe in your own words what you’re experiencing?
- Determine if the reported site of pain is the actual source.
Pain Characteristics
- Pain location
- Pain onset
- Was there a trigger associated? - Identify the onset (e.g., two weeks ago) and triggers (e.g., trauma).
Pain Quality and Intensity
Pain Quality19
- Bright or dull
- Pricking
- Itching
- Stinging
- Burning
- Aching
- Pulsating
- Throbbing
Pain Quality Associations
- Dull/aching pain is often musculoskeletal.
- Burning/stinging pain is typically neuropathic.
- Pulsating/throbbing pain can be migraine-like.
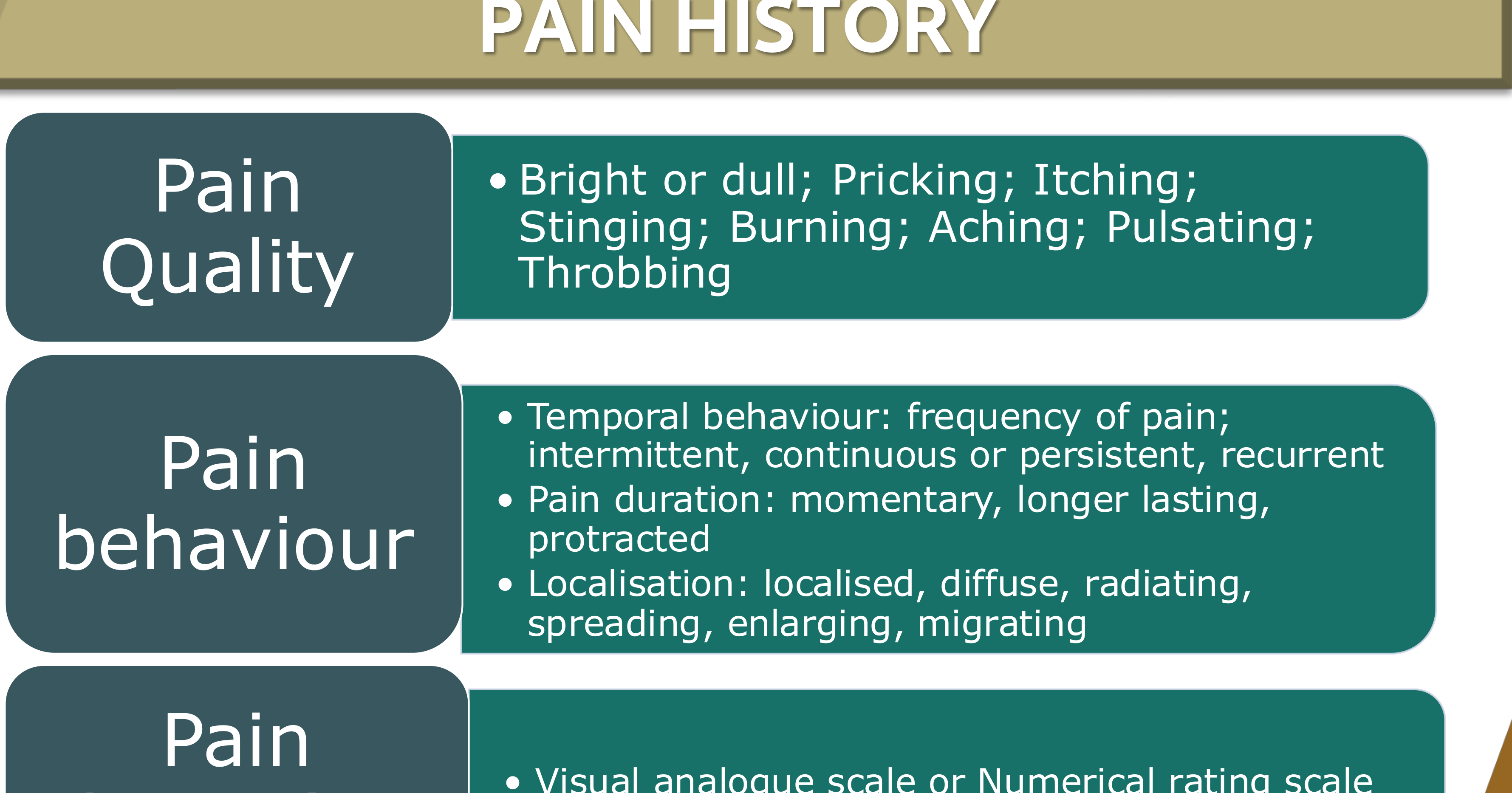
Pain Behavior
- Temporal behavior: frequency of pain; intermittent, continuous or persistent, recurrent - Check if the pain is constant or occurs only in the morning.
- Pain duration: momentary, longer lasting, protracted
- Localization: localized, diffuse, radiating, spreading, enlarging, migrating
Pain Intensity
- Visual analogue scale or Numerical rating scale
- No pain ------- X ------- Most severe pain
- Intensity can also be measured using Wong-Baker smiley faces.
Concomitant Symptoms20
- Sensory: hyperaesthesia, hypoaesthesia, anaesthesia, dysaesthesia, paraesthesia
- Motor: muscular weakness, muscular contractions, spasms
- Autonomic: lacrimation, pupillary changes, oedema of the lids, nasal secretions - Check for tearing, runny nose, or swelling.
Flow of Pain
- Steady
- Paroxysmal
Functional and Parafunctional Activities
Effects of Functional Activities21
- Pain when eating
- Restriction in opening
- Pain when yawning
- Pain when laughing
- Jaw joint noises: Have you had any jaw joint noises when you moved or used your jaw - Identify noises like clicking or "grating" (crepitation).?
- Closed locking of the jaw: Have you ever had your jaw lock or catch, even for a moment, so that it would not open all the way? Was it severe enough to limit your ability to eat?
- Open locking of the jaw: When you opened your mouth, did your jaw catch, even for a moment so that you could not close it from this wide position? Did you have to do something to get it to close?
- Headaches?
Effects of Parafunctional Activities22
- Awareness of day-time clenching
- Bracing
- Grinding or clenching while asleep
- Bruxism
- Chin resting
- Biting nails
- Sleeping on stomach
- Biting on back of pens/pencils
- Chewing lips, cheeks, tongue
Note: In clinical practice, prioritize the DC/TMD protocol over older indices.
History Protocol in DC/TMD23
Screening Questions and Symptom Questionnaire
3Q/TMD Screening Questions24
- Do you have pain in your temple, face, jaw or jaw joint once a week or more?
- Do you have pain once a week or more when you open your mouth or chew?
- Does your jaw lock or become stuck once a week or more?
Note: “Yes” responses to any of these indicate a high probability of TMD.
DC/TMD Symptom Questionnaire: Pain25
-
Have you ever had pain in your jaw, temple, in the ear, or in front of the ear on either side?
- No / Yes (If NO, skip to Question 5)
-
How many years or months ago did your pain in the jaw, temple, in the ear, or in front of the ear first begin?
- ____ years | ____ months
-
In the last 30 days, which of the following best describes any pain in your jaw, temple, in the ear, or in front of the ear on either side?
- No pain (If NO, skip to Question 5)
- Pain comes and goes
- Pain is always present
-
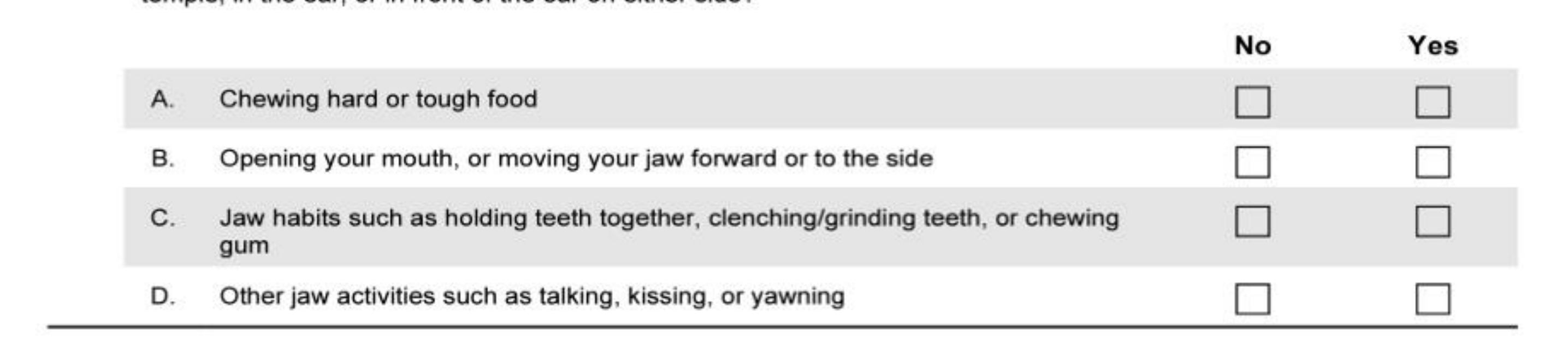
In the last 30 days, did the following activities change any pain (make it better or worse) in your jaw, temple, in the ear, or in front of the ear on either side?
- A. Chewing hard or tough food (No/Yes)
- B. Opening your mouth, or moving your jaw forward or to the side (No/Yes)
- C. Jaw habits such as holding teeth together, clenching/grinding teeth, or chewing gum (No/Yes)
- D. Other jaw activities such as talking, kissing, or yawning (No/Yes)
DC/TMD Symptom Questionnaire: Headache26
-
In the last 30 days, have you had any headaches that included the temple areas of your head?
- No / Yes (If NO, skip to Question 8)
-
How many years or months ago did your temple headache first begin?
- ____ years | ____ months
-
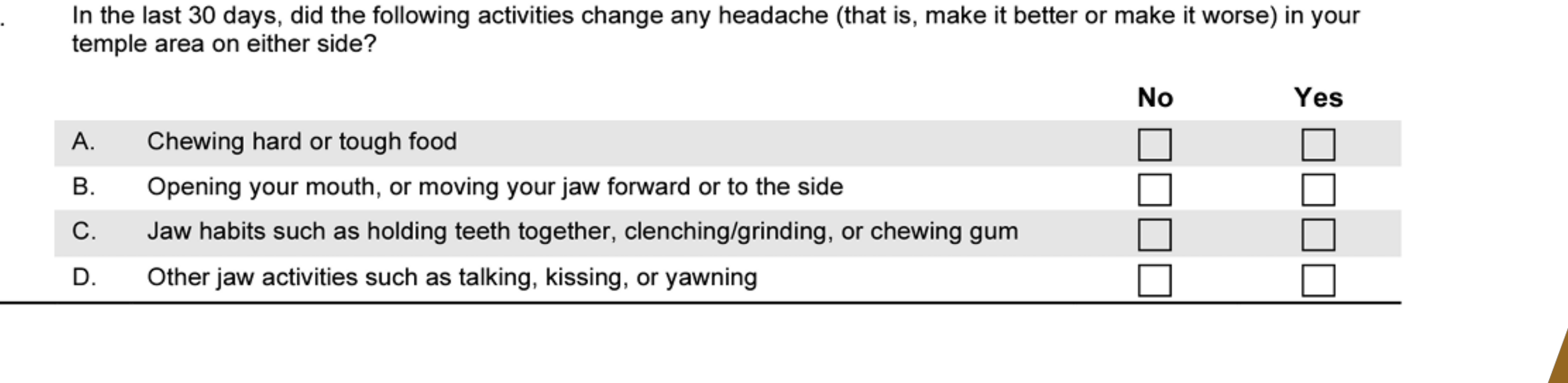
In the last 30 days, did the following activities change any headache (make it better or worse) in your temple area on either side?
- A. Chewing hard or tough food (No/Yes)
- B. Opening your mouth, or moving your jaw forward or to the side (No/Yes)
- C. Jaw habits such as holding teeth together, clenching/grinding, or chewing gum (No/Yes)
- D. Other jaw activities such as talking, kissing, or yawning (No/Yes)
DC/TMD Symptom Questionnaire: Jaw Joint Noises27
- In the last 30 days, have you had any jaw joint noise(s) when you moved or used your jaw?
- No / Yes (Specify: Right, Left, or Don’t Know)
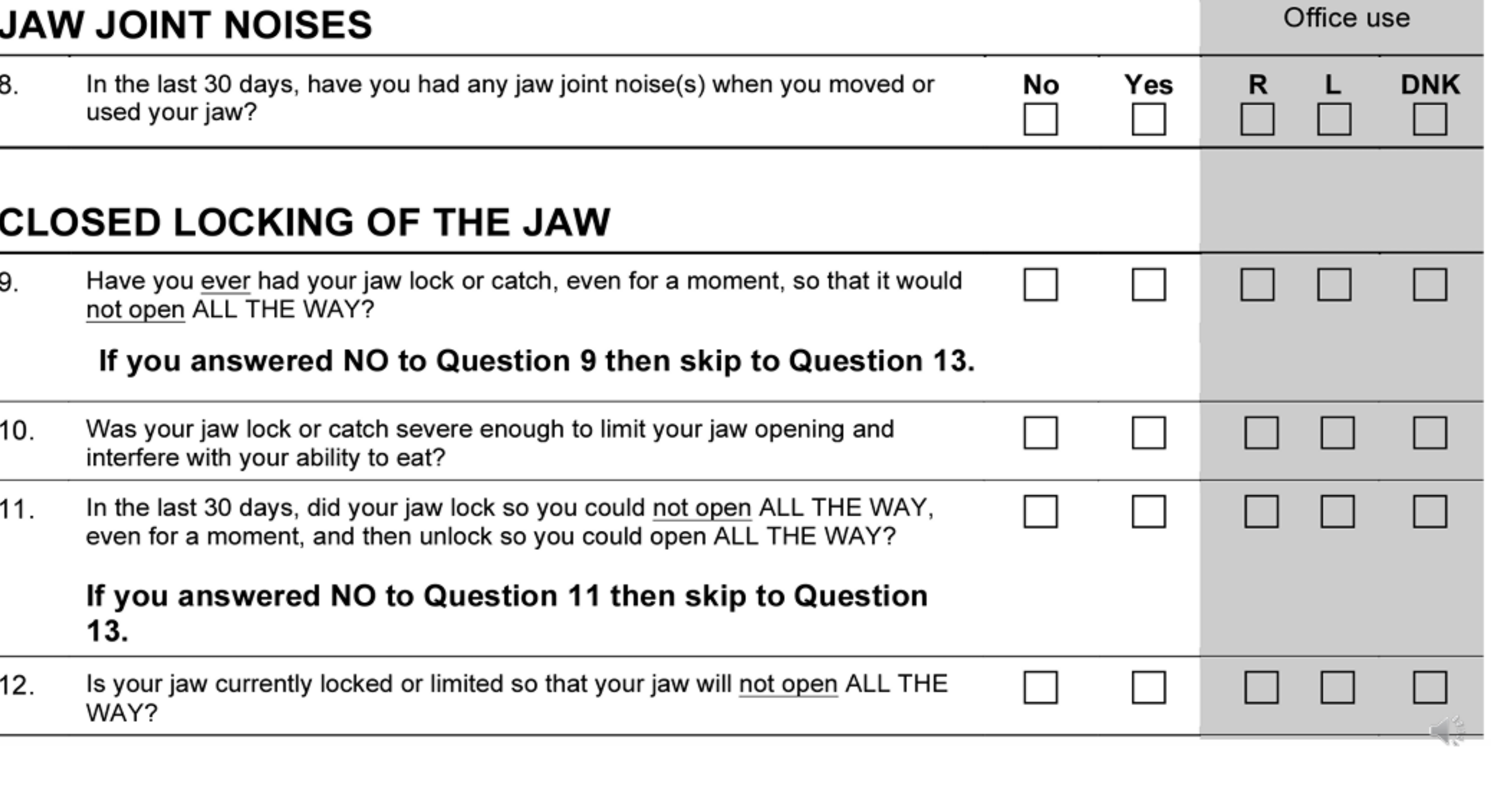
DC/TMD Symptom Questionnaire: Closed Locking
-
Have you ever had your jaw lock or catch, even for a moment, so that it would not open ALL THE WAY?
- No / Yes (If NO, skip to Question 13)
-
Was your jaw lock or catch severe enough to limit your jaw opening and interfere with your ability to eat?
- No / Yes
-
In the last 30 days, did your jaw lock so you could not open ALL THE WAY, even for a moment, and then unlock so you could open ALL THE WAY?
- No / Yes (If NO, skip to Question 13)
-
Is your jaw currently locked or limited so that your jaw will not open ALL THE WAY?
- No / Yes
DC/TMD Symptom Questionnaire: Open Locking28
-
In the last 30 days, when you opened your mouth wide, did your jaw lock or catch even for a moment such that you could not close it from this wide open position?
- No / Yes (If NO, questionnaire is finished)
-
In the last 30 days, when your jaw locked or caught wide open, did you have to do something to get it to close including resting, moving, pushing, or maneuvering it?
- No / Yes
Medical and Psychosocial History
Clinical Assessment Components29
- Past Medical History
- Review of Systems
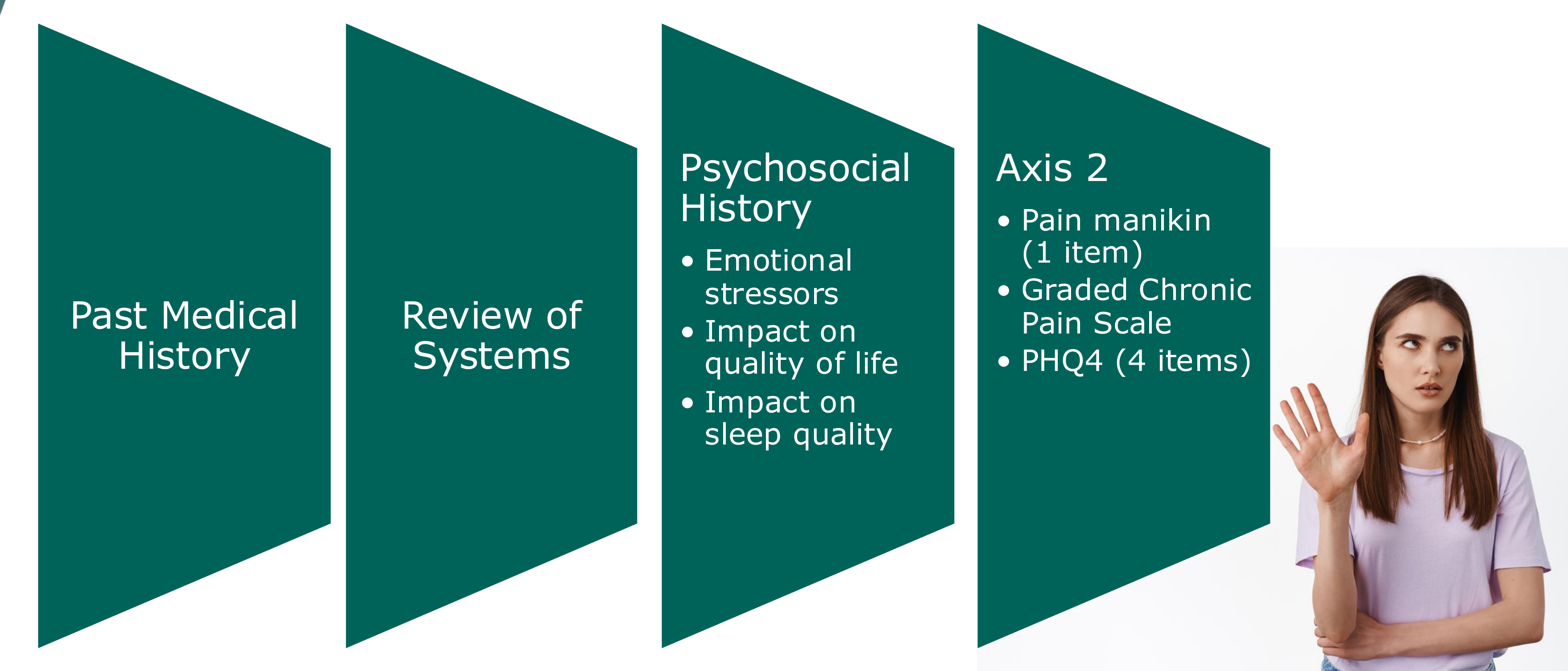
Psychosocial History
- Emotional stressors
- Identify stressors such as marital issues, financial ruin, or high-stress jobs.
- Impact on quality of life
- Impact on sleep quality
- Inquire about sleep latency, waking up during the night, and total hours.
Axis 2 Assessment
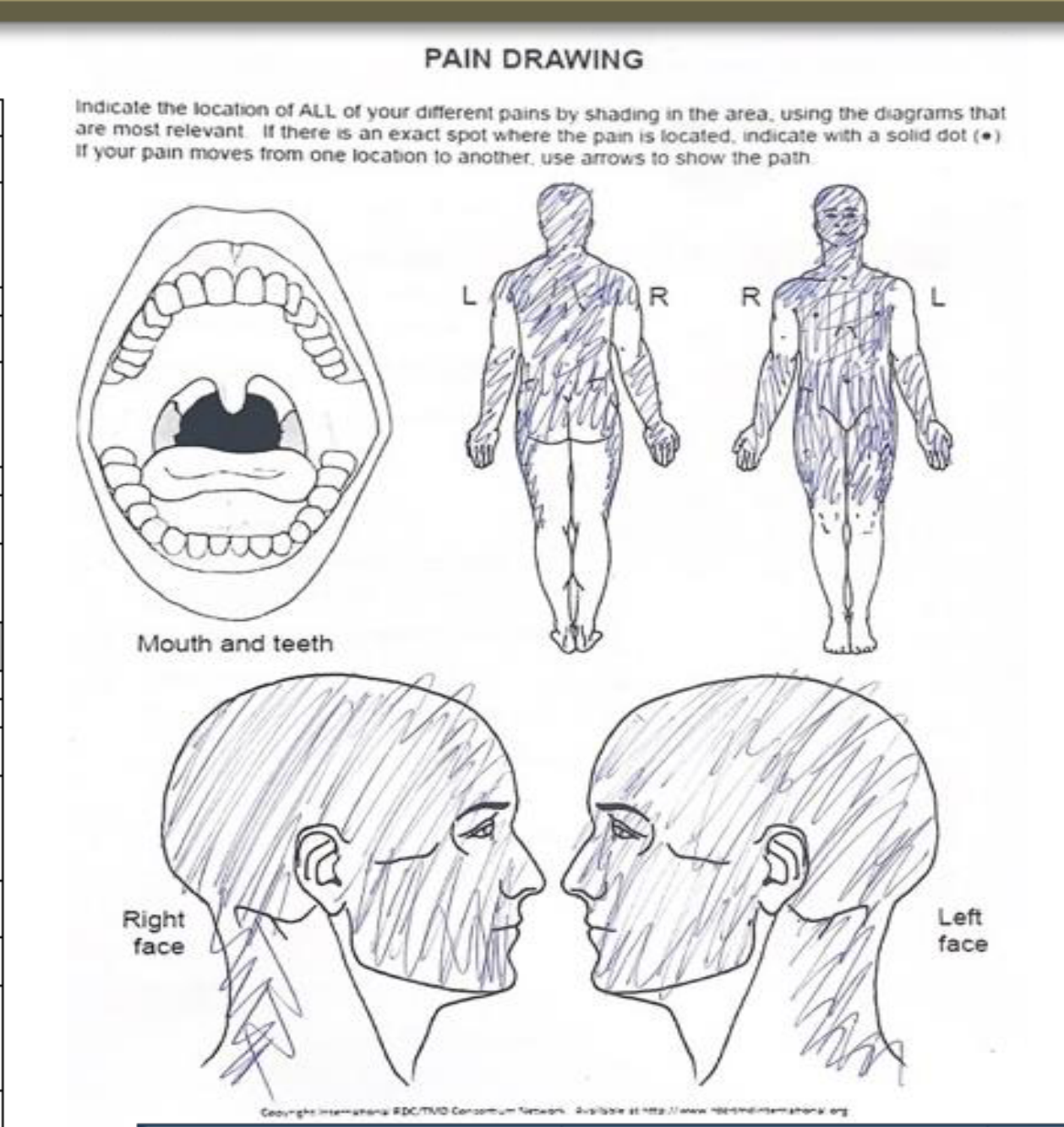
- Pain manikin (1 item)
- Graded Chronic Pain Scale
- PHQ4 (4 items)
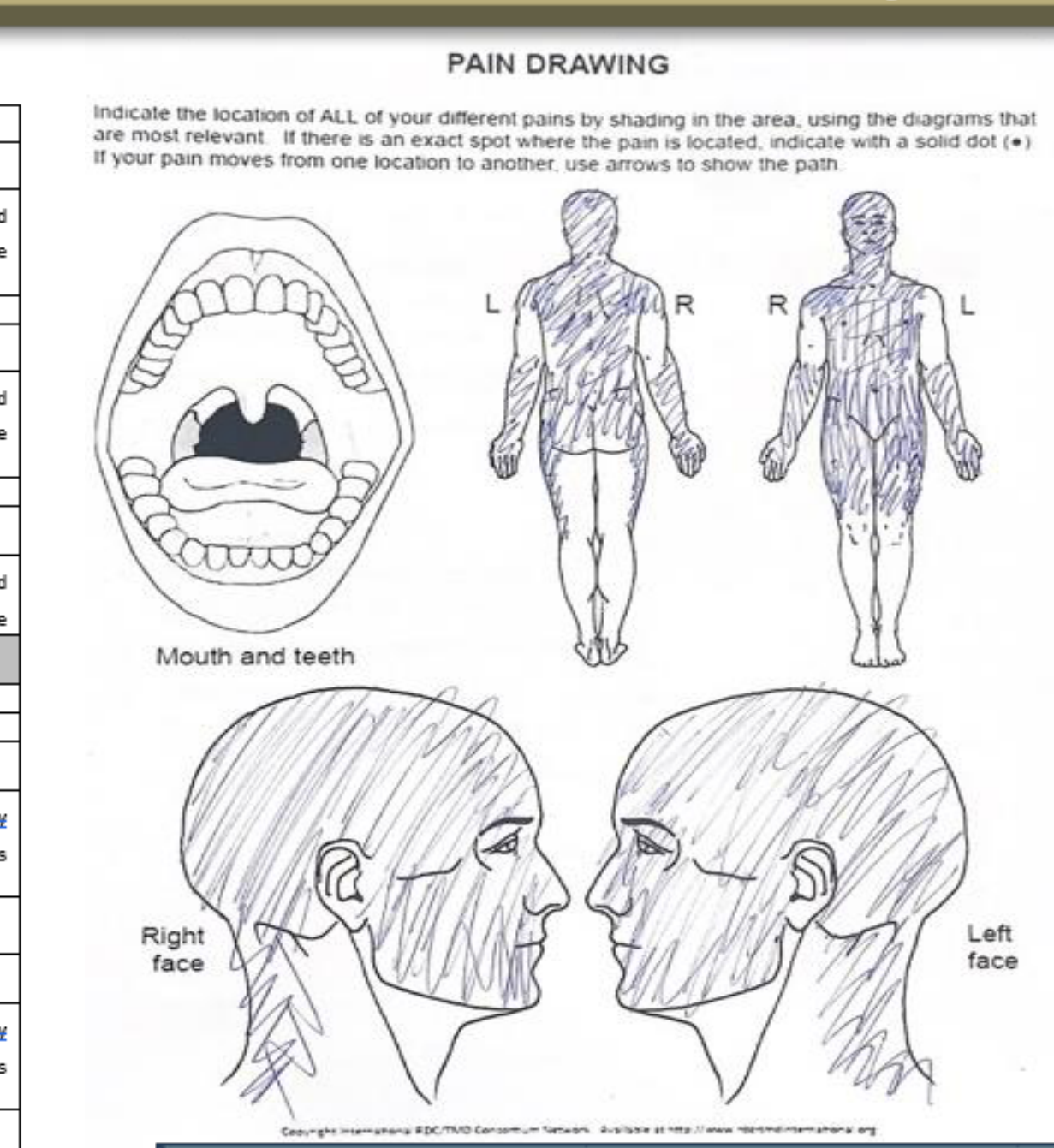
- Pain Mapping: Patients who draw many arrows or boxes on a pain diagram often have a poorer prognosis.
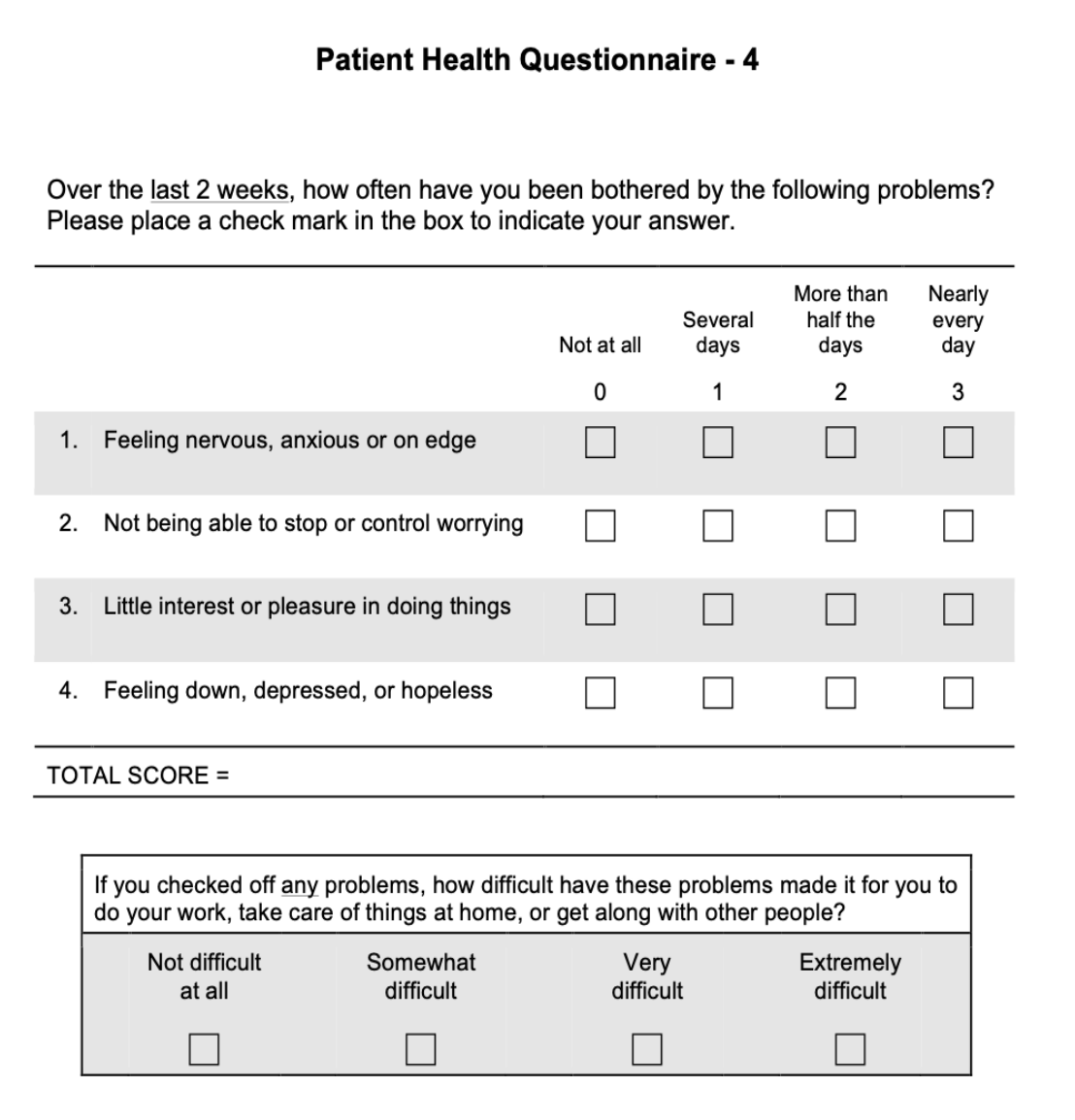
Patient Health Questionnaire - 4 (PHQ-4)30
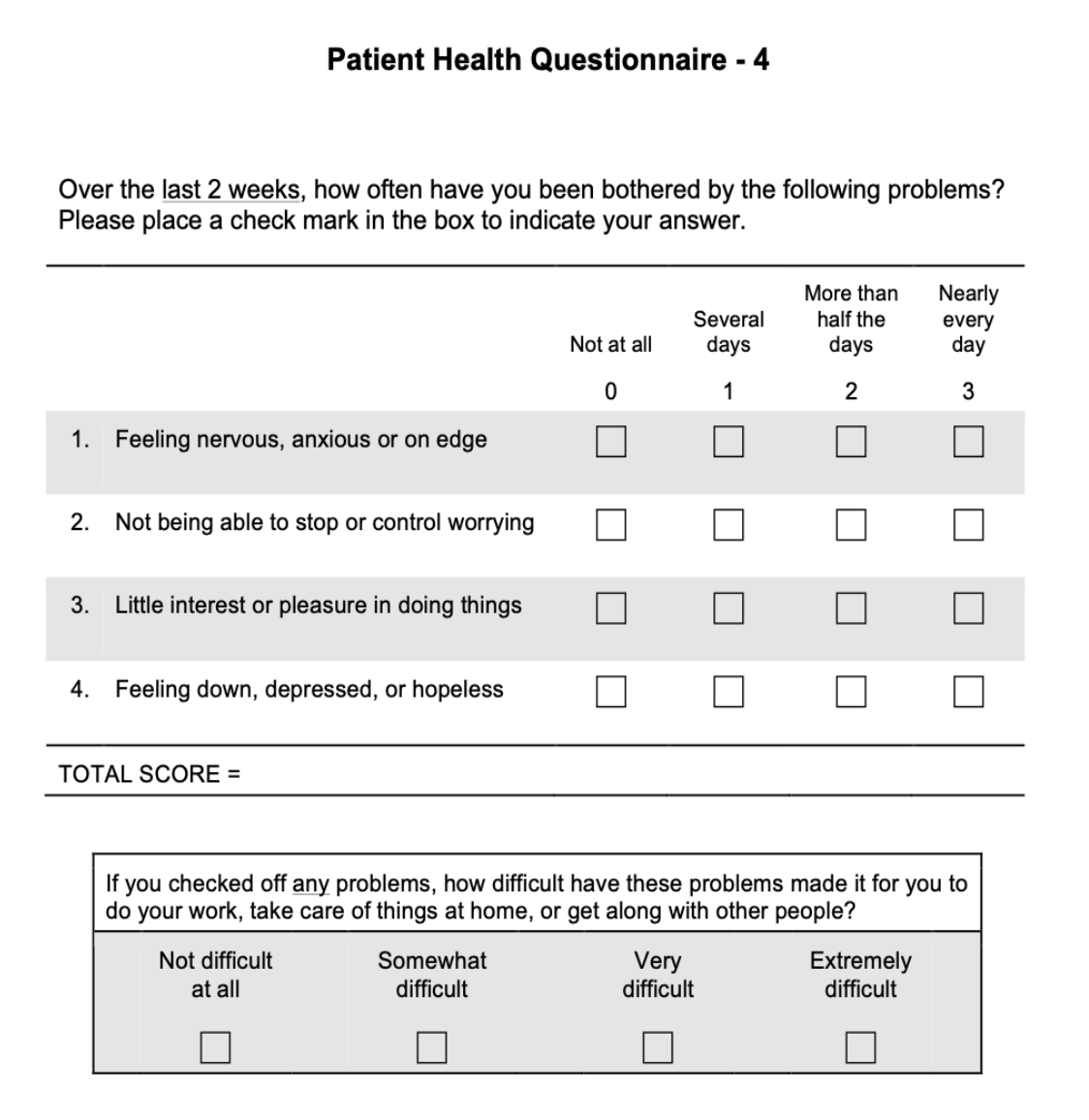
Over the last 2 weeks, how often have you been bothered by the following problems? (Scoring: 0 = Not at all; 1 = Several days; 2 = More than half the days; 3 = Nearly every day)
- Feeling nervous, anxious or on edge
- Not being able to stop or control worrying
- Little interest or pleasure in doing things
- Feeling down, depressed, or hopeless
PHQ-4 Interpretation
High scores on this four-question tool indicate significant distress and are used to screen for anxiety and depression.
TOTAL SCORE = ________
 |  |
 |  |
Functional Impact
If you checked off any problems, how difficult have these problems made it for you to do your work, take care of things at home, or get along with other people?
- Not difficult at all
- Somewhat difficult
- Very difficult
- Extremely difficult
Examination Protocol31
General Assessment Guidelines32
- The default time frame for assessing pain in the expanded taxonomy is in “the last 30 days”; the examiner must identify with the patient all anatomical locations that they have experienced pain in the last 30 days. However, the examiner may choose a different time frame as dictated by clinical circumstances.
- For a given diagnosis, the location of pain induced by the specified provocation test(s) must be in an anatomical structure consistent with that diagnosis.
- “Familiar pain” or “familiar headache” is based on patient report that the pain induced by the specified provocation test(s) has replicated the patient’s pain, as identified by respective location and within the specified time frame.
- The phrase “pain modified” is used in the diagnostic criteria for arthralgia and myofascial pain to emphasize that the pain may be made better or worse by jaw function, movement or parafunction, by history. The phrase is more inclusive than either phrase “pain made worse” or “pain made better” and is used to differentiate a musculoskeletal pain from other pain conditions of the trigeminal system.
- Whilst jaw muscle pain is diagnosed based on examination of the masseter and temporalis muscles, other masticatory muscles may be examined as required.
- Diagnostic imaging should only be considered after a history and physical examination indicates that information from imaging will influence patient care.
- Magnetic resonance imaging (MRI) and computerized tomography (CT) are often the preferred imaging modalities. CT includes either conventional CT or cone beam computerized tomography (CBCT).
- Where intramuscular electromyography monitoring is indicated, this would be performed with fine wire or needle electrodes.
- Palpation Force: Use 0.5 kg for the lateral pole of the TMJ and 1.0 kg for the muscle and surrounding joint areas
- 1.0 kg is roughly the force required to make a fingernail blanch
- For all pain-related diagnoses, the pain/headache is not better accounted for by another pain/headache diagnosis.
Standard of Care
The Helkimo Index is considered "archaic" and is no longer the standard of care; DC/TMD is the modern standard.
Clinical Examination Form and Pain Mapping33
 |  |
Pain Location and Incisal Relationships34
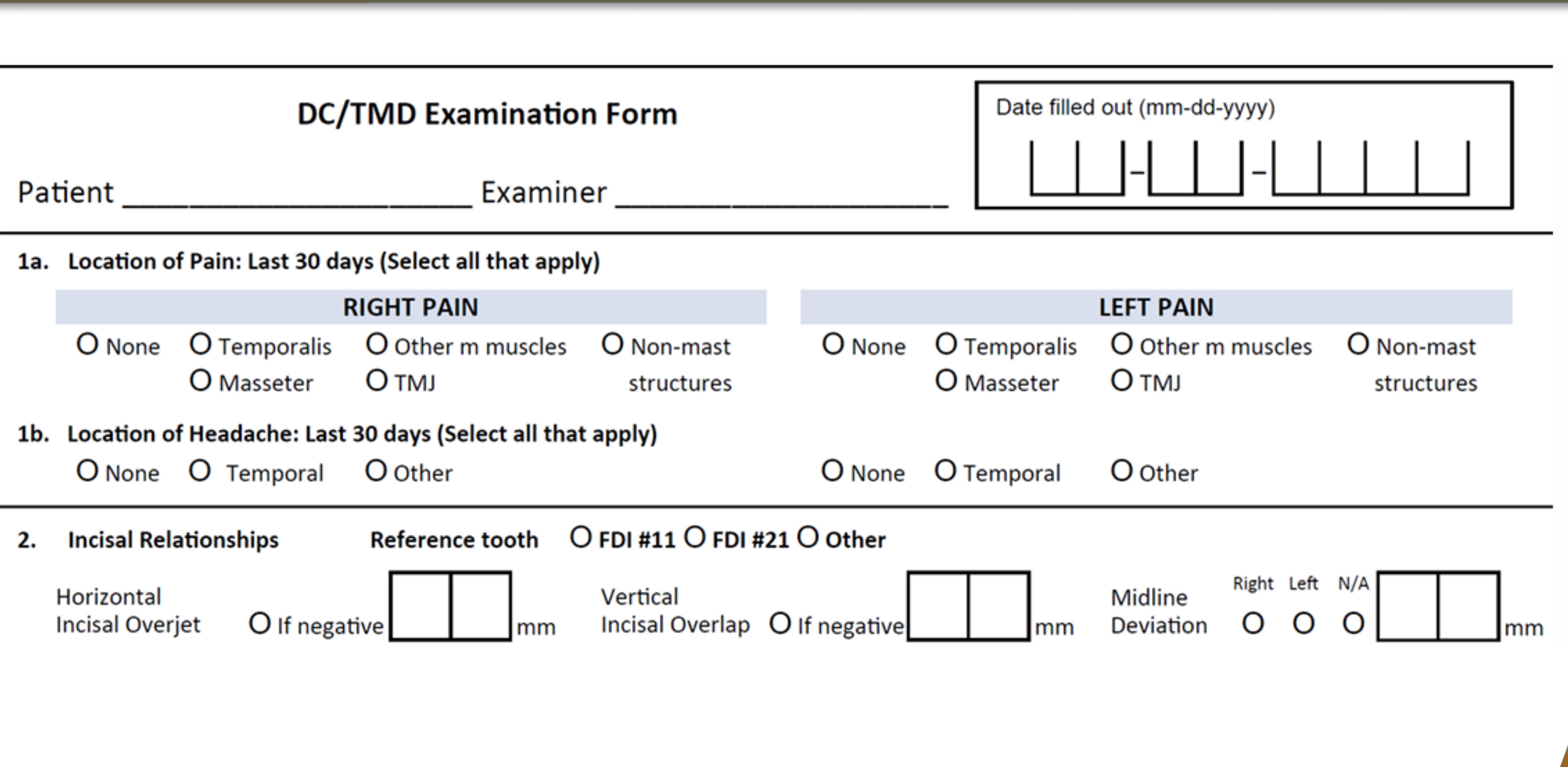
1a. Location of Pain: Last 30 days (Select all that apply)
- Right Pain: None, Temporalis, Masseter, TMJ, Other masticatory muscles, Non-masticatory structures
- Left Pain: None, Temporalis, Masseter, TMJ, Other masticatory muscles, Non-masticatory structures
1b. Location of Headache: Last 30 days (Select all that apply)
- Left: None, Temporal, Other
2. Incisal Relationships
- Reference tooth: FDI #11, FDI #21, Other
- Horizontal Incisal Overjet: [ ] mm (Note if negative)
- Vertical Incisal Overlap: [ ] mm (Note if negative)
- Midline Deviation: [ ] mm (Direction: Right, Left, or N/A)
Mandibular Opening Patterns and Movements3536
Opening Pattern (Supplemental)37
- Corrected Deviation: Mandible returns to center position on opening (Abbreviation: DD w/R)
- Uncorrected Deviation (Deflection): Continuous displacement of mandibular midline (Abbreviation: DD w/o R)
- Straight: No deviation or deflection noted.
- Deviation suggests reduction
- Deflection suggests no reduction
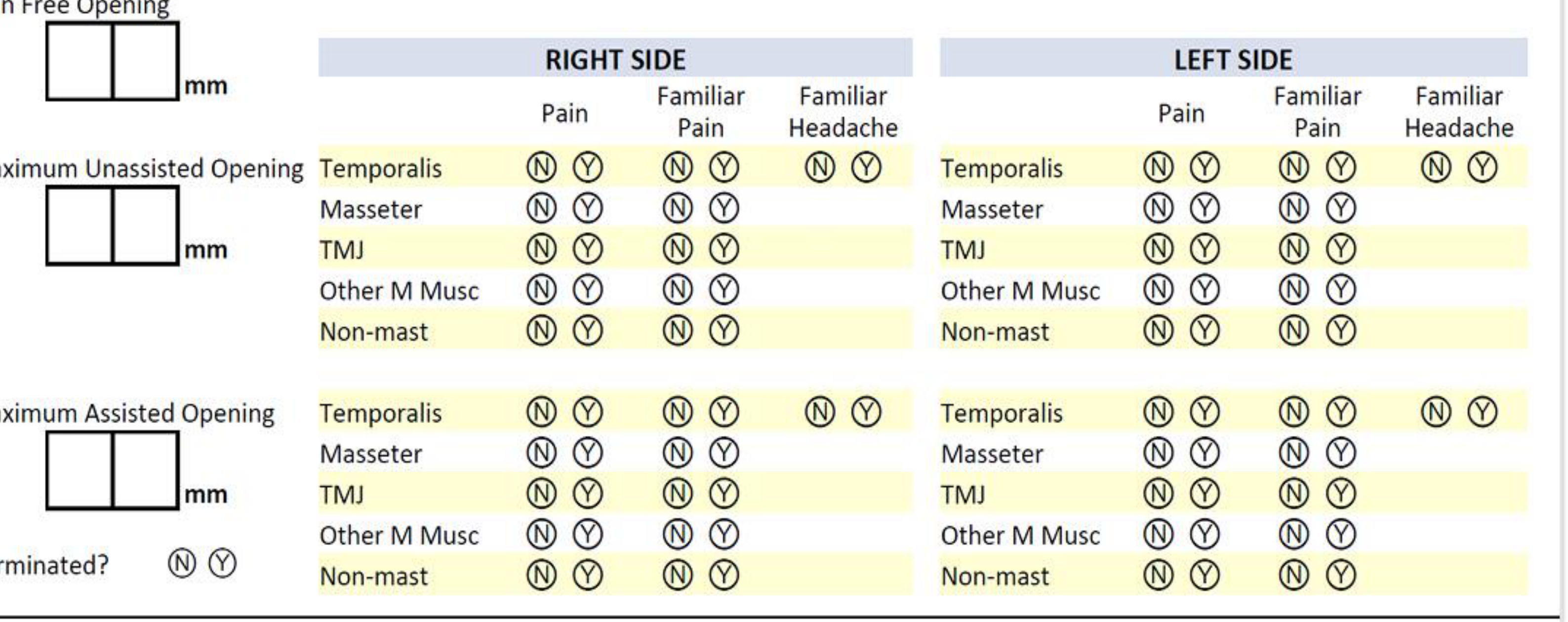
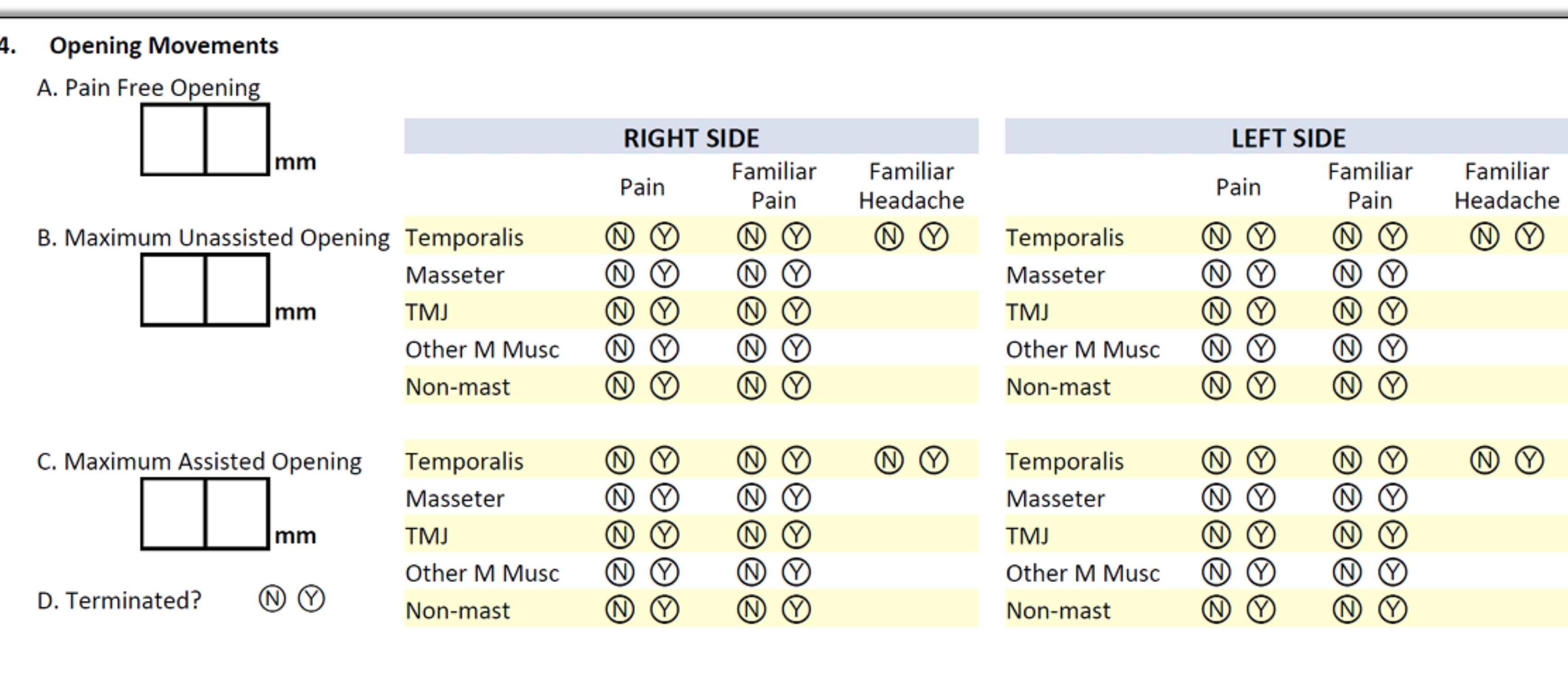
Opening Movements Assessment38
- A. Pain Free Opening: [ ] mm
- B. Maximum Unassisted Opening: [ ] mm
- C. Maximum Assisted Opening: [ ] mm
- D. Terminated? No / Yes
| Structure | Right Pain | Right Familiar Pain | Right Familiar Headache | Left Pain | Left Familiar Pain | Left Familiar Headache |
|---|---|---|---|---|---|---|
| Temporalis | N / Y | N / Y | N / Y | N / Y | N / Y | N / Y |
| Masseter | N / Y | N / Y | - | N / Y | N / Y | - |
| TMJ | N / Y | N / Y | - | N / Y | N / Y | - |
| Other M Musc | N / Y | N / Y | - | N / Y | N / Y | - |
| Non-mast | N / Y | N / Y | - | N / Y | N / Y | - |
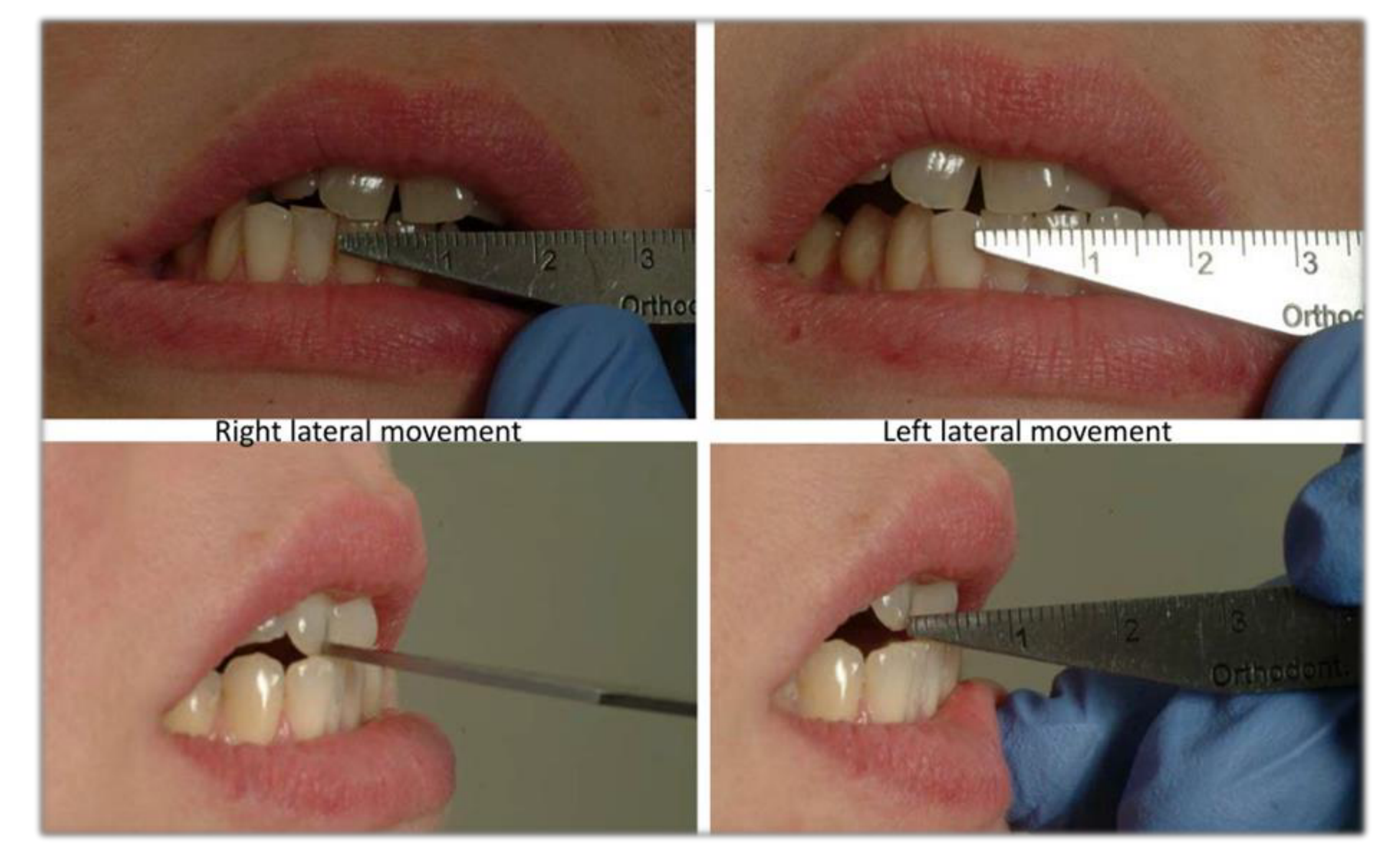
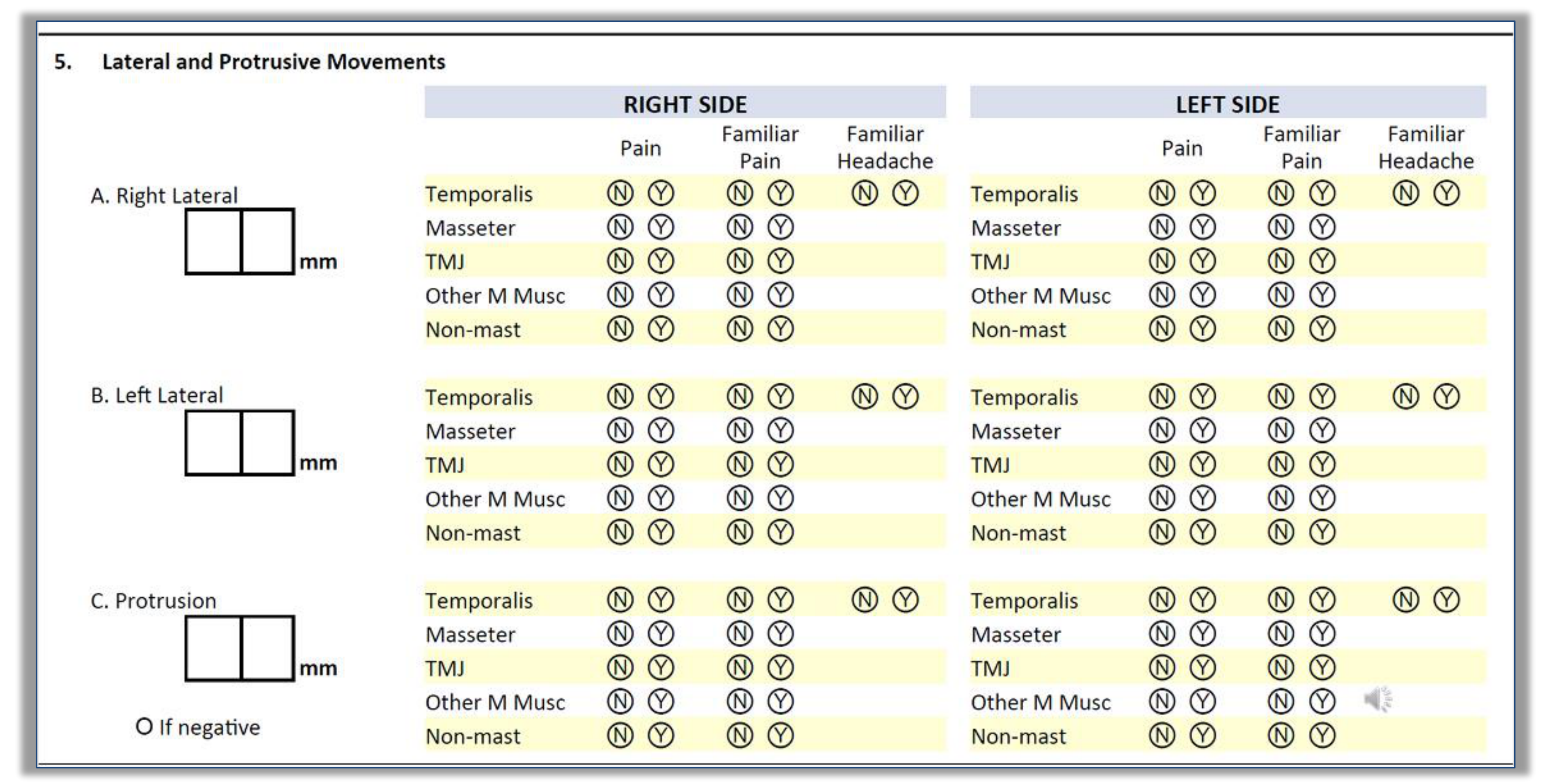
Lateral and Protrusive Movements39
- A. Right Lateral: [ ] mm
- B. Left Lateral: [ ] mm
- C. Protrusion: [ ] mm
Pain Provocation Scale
- None
- Mild
- Moderate / Modest
- Severe / Strong
- Very Severe / Completely Cannot Stand
Temporomandibular Joint Noises and Locking
TMJ Noises During Movements40
Open & Close Movements
- Right TMJ: Click (Open/Close), Crepitus (Open/Close). Note if patient reports pain with click or if pain is familiar.
- Left TMJ: Click (Open/Close), Crepitus (Open/Close). Note if patient reports pain with click or if pain is familiar.
- Clicking is a discrete sound during movement
- Crepitation is a grating sound like "walking in gravel or snow," suggestive of degenerative changes
Lateral & Protrusive Movements
- Right TMJ: Click (Yes/No), Crepitus (Yes/No). Note if pain with click is familiar.
- Left TMJ: Click (Yes/No), Crepitus (Yes/No). Note if pain with click is familiar.
 |  |
 |
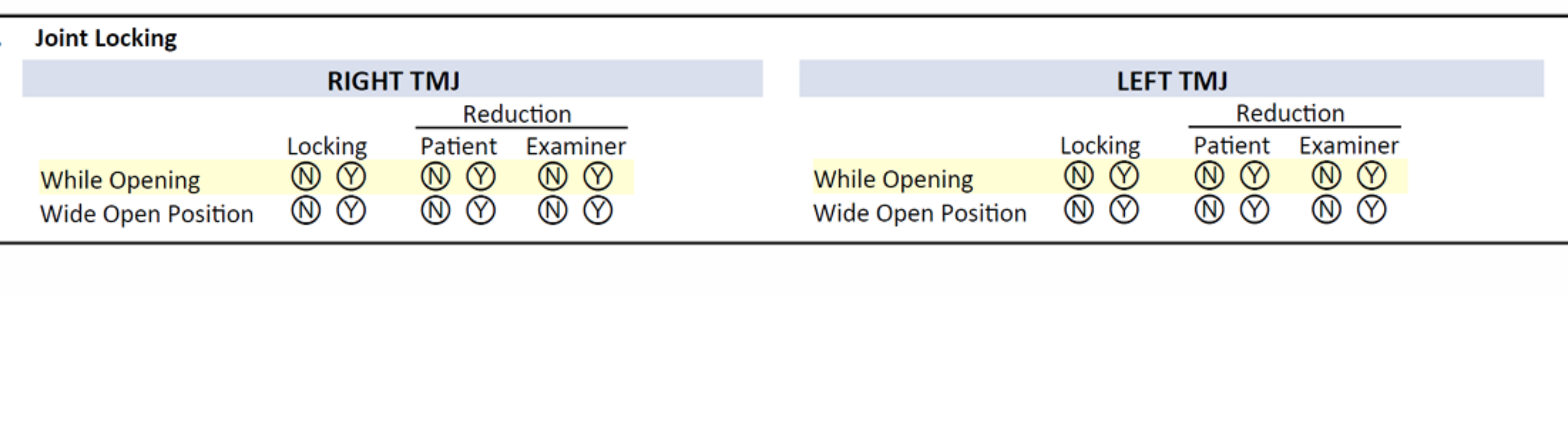
Joint Locking Assessment41
- Right TMJ Locking:
- While Opening: Yes/No
- Wide Open Position: Yes/No
- Reduction: Patient (Yes/No), Examiner (Yes/No)
- Left TMJ Locking:
- While Opening: Yes/No
- Wide Open Position: Yes/No
- Reduction: Patient (Yes/No), Examiner (Yes/No)
Muscle and Joint Palpation
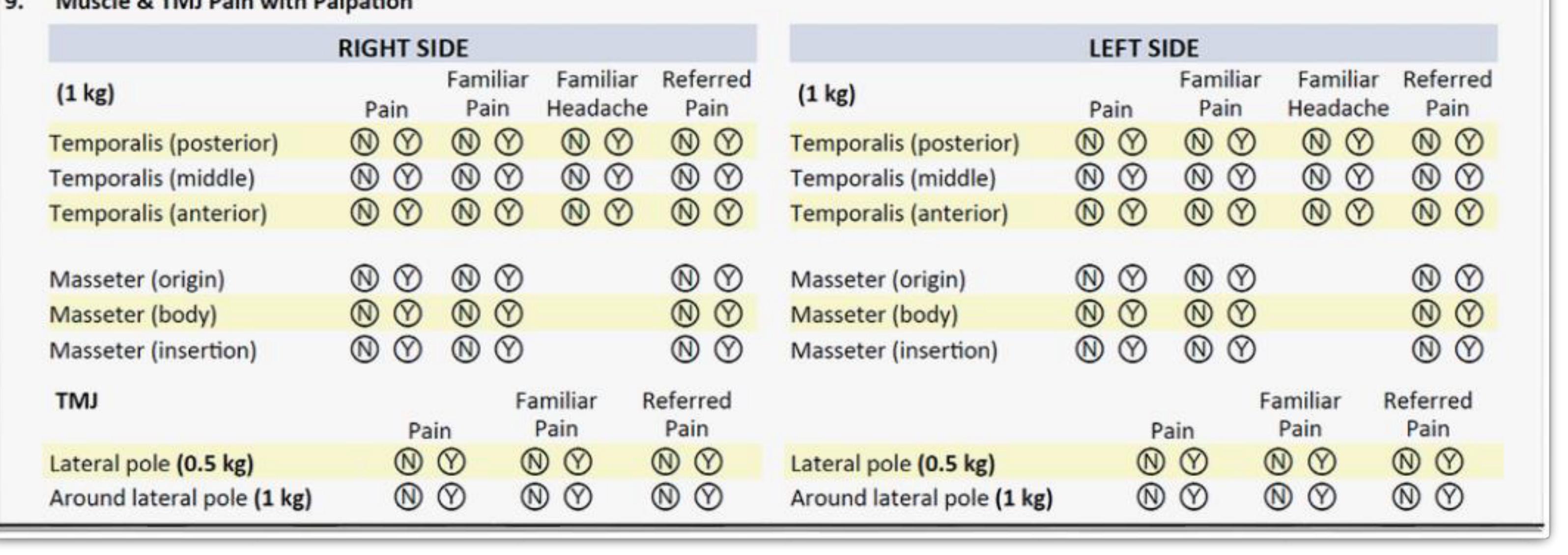
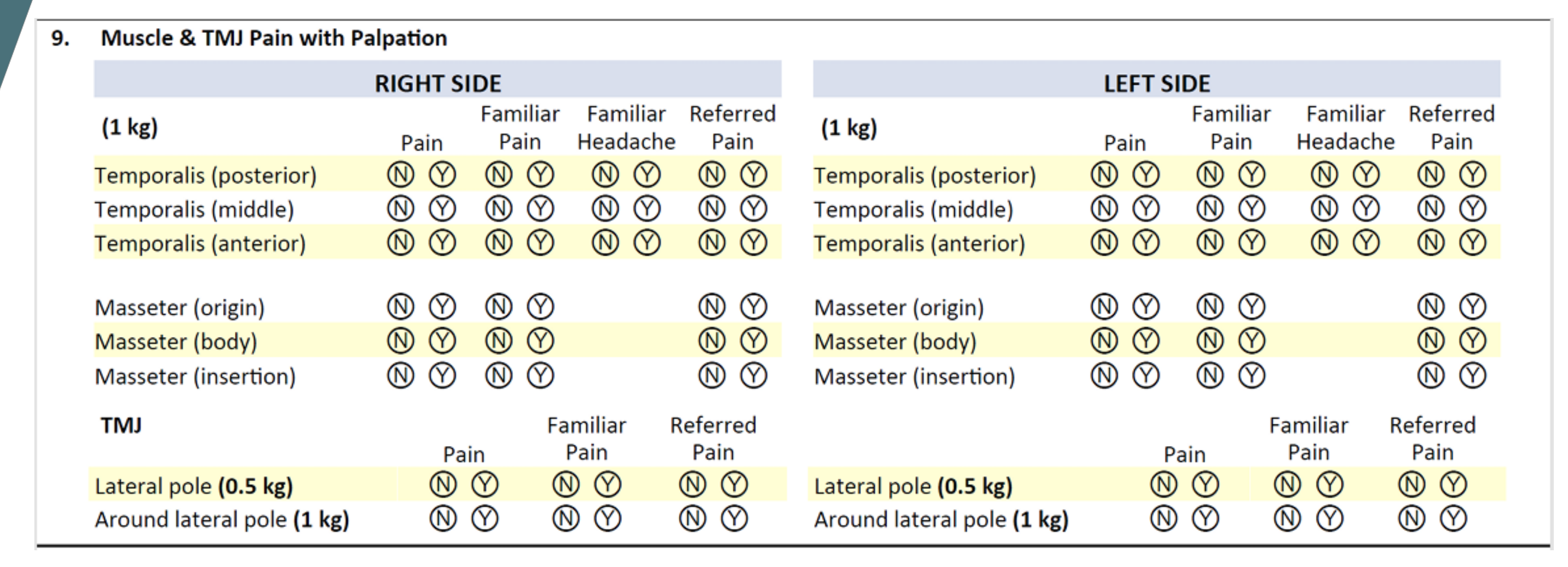
Muscle & TMJ Pain with Palpation42
| Structure | Right Pain | Right Familiar Pain | Right Familiar Headache | Right Referred Pain | Left Pain | Left Familiar Pain | Left Familiar Headache | Left Referred Pain |
|---|---|---|---|---|---|---|---|---|
| Temporalis (post) | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y |
| Temporalis (mid) | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y |
| Temporalis (ant) | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y | N/Y |
| Masseter (origin) | N/Y | N/Y | - | N/Y | N/Y | N/Y | - | N/Y |
| Masseter (body) | N/Y | N/Y | - | N/Y | N/Y | N/Y | - | N/Y |
| Masseter (ins) | N/Y | N/Y | - | N/Y | N/Y | N/Y | - | N/Y |
| TMJ Lat. Pole (0.5kg) | N/Y | N/Y | - | N/Y | N/Y | N/Y | - | N/Y |
| TMJ Around Pole (1kg) | N/Y | N/Y | - | N/Y | N/Y | N/Y | - | N/Y |
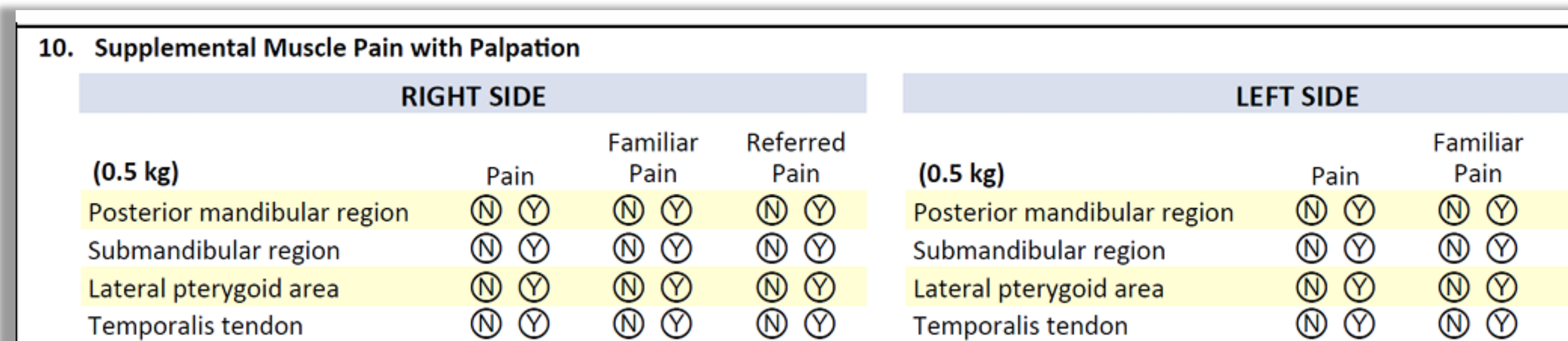
Supplemental Muscle Palpation Areas43
- Lateral Pterygoid Area (x-area): Specific anatomical region for supplemental examination.
- Temporalis Tendon (y-area): Specific anatomical region for supplemental examination.
- Mandibular Region (z-area): Specific anatomical region for supplemental examination.
- Submandibular Region (w-area): Specific anatomical region for supplemental examination.
 |  |
 |
Diagnostic Decision Trees
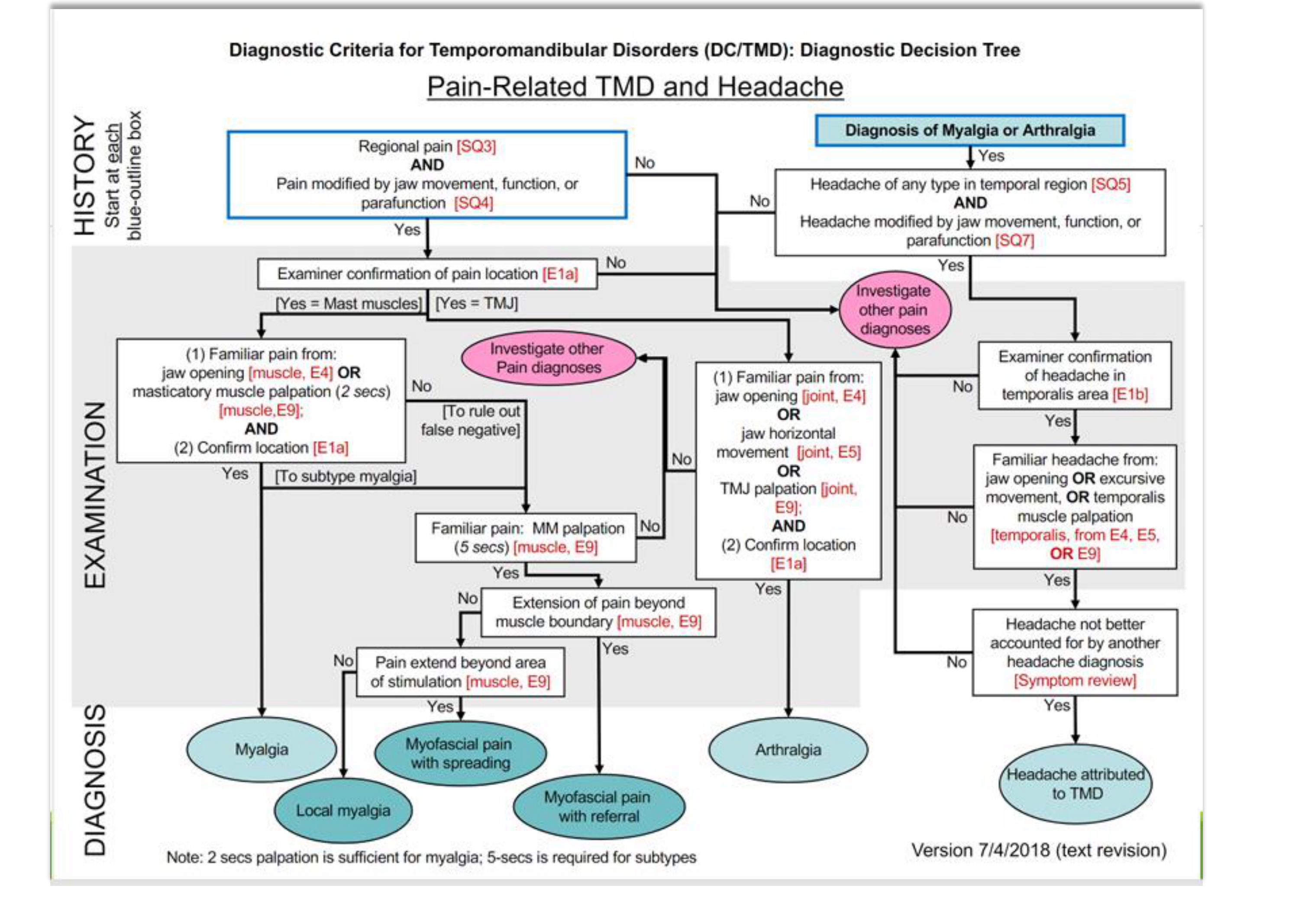
Pain-Related TMD and Headache Decision Tree44
History Requirements:
- Regional pain [SQ3] AND pain modified by jaw function [SQ4].
- Headache in temporal region [SQ5] AND headache modified by jaw function [SQ7].
Examination Confirmation:
- Myalgia: Familiar pain from jaw opening [E4] OR masticatory muscle palpation (2 seconds) [E9].
- Arthralgia: Familiar pain from jaw opening [E4], horizontal movement [E5], OR TMJ palpation [E9].
- Headache Attributed to TMD: Familiar headache from jaw opening, excursive movement, or temporalis palpation [E4, E5, E9].
Myalgia Subtyping (5-second palpation):
- Local Myalgia: Pain localized to site of palpation.
- Myofascial Pain with Spreading: Pain extends beyond the area of stimulation but remains within the muscle boundary.
- Myofascial Pain with Referral: Pain extends beyond the boundary of the muscle.
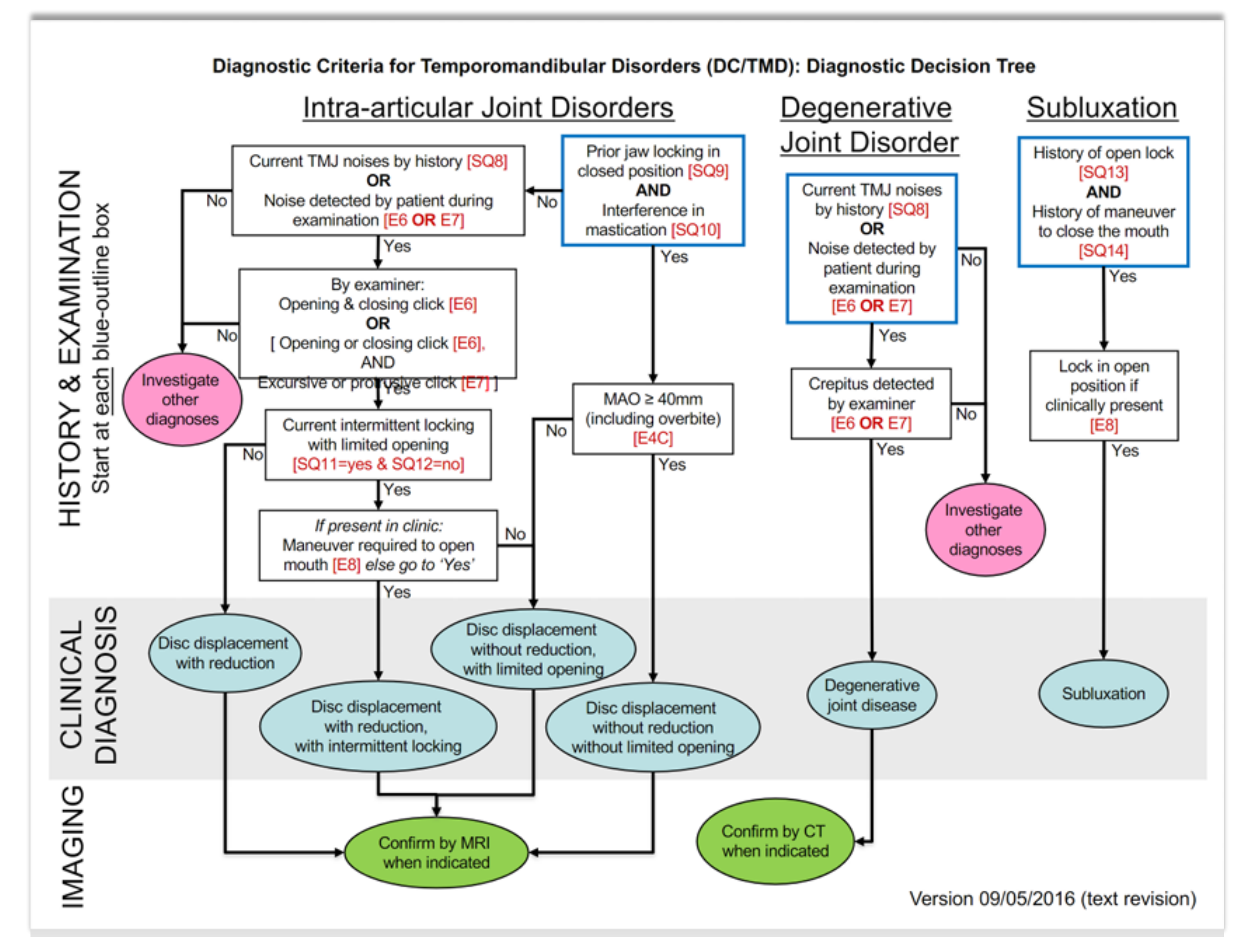
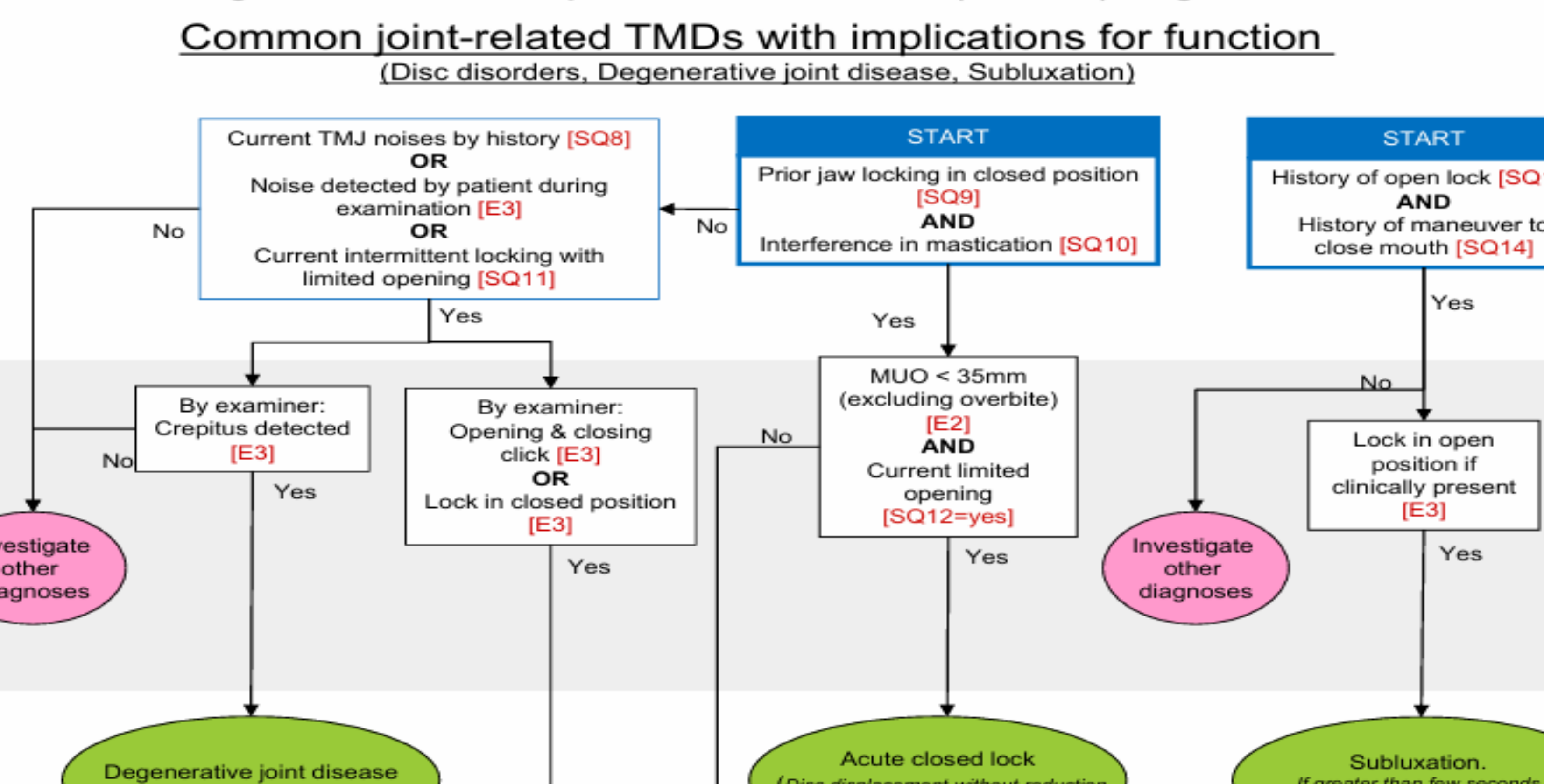
Intra-articular and Degenerative Disorders Decision Tree45
Disc Displacement with Reduction (DDwR):
- History of TMJ noises [SQ8] OR noise detected during exam [E6, E7].
- Examiner detects opening/closing click.
Disc Displacement without Reduction (DDwoR):
- With Limited Opening: History of locking [SQ11], MAO < 40mm [E4C].
- Without Limited Opening: History of prior locking [SQ9], interference in mastication [SQ10], MAO ≥ 40mm.
Degenerative Joint Disease (DJD):
- History of TMJ noises [SQ8] OR noise detected during exam [E6, E7].
- Crepitus detected by examiner [E6, E7].
Subluxation:
- History of open lock [SQ13] AND history of maneuver to close mouth [SQ14].
- Lock in open position clinically present [E8].
DC/TMD Examination Protocol Contributors46
- Yoly Gonzalez, DDS, MS, MPH
- Jason Chwirut, MS
- Thomas List, DDS, PhD
- Richard Orhbach, DDS, PhD
- University at Buffalo School of Dental Medicine
Brief DC/TMD Protocol47
Durham J, Ohrbach R, Baad-Hansen L, et al. Constructing the brief diagnostic criteria for temporomandibular disorders (bDC/TMD) for field testing. J Oral Rehabil. 2023; 00: 1-10.
bDC/TMD Objectives and Structure48
- Efficiency: Axis I and Axis II should take no more than 10 minutes of provider time, maximizing patient self-report instrumentation
- Designed for general practice to be completed in under 10 minutes.
- Diagnostic Groupings: Focuses on broad clinical utility groupings
- Focuses on core categories (Muscle Pain, Joint Pain) rather than detailed sub-classifications.:
- Painful TMDs: Myalgia, arthralgia, and headache attributed to TMD.
- Joint-related TMDs: Degenerative joint disease, subluxation, acute closed lock, and disc-based TMDs.
- Axis II: Ultra-brief screen for psychosocial yellow or red flags.
- Training: Provided via distance learning and video materials.
Brief Examination Items49

Summary of Brief Examination Items50
- E1a (Pain Identification): Retained and revised. Focuses on Temporalis, Masseter, and TMJ. Removed “other masticatory muscles” and “non-masticatory structures.”
- E1b (Headache Area) & E2 (Incisal Relationship): Removed as unnecessary for broad grouping diagnoses.
- E3 (Opening Pattern): Removed due to poor reliability.
- E4 (Opening Movements): Retained and revised. Simplified to pain-free and maximum unassisted opening. Combined with E6 and E8.
- E5 (Lateral Movements) & E7 (Excursive Noises): Removed due to low reliability and low diagnostic yield.
- E6 (Joint Noises) & E8 (Joint Locking): Retained and revised. Integrated into a simplified 3-step movement examination.
- E9 (Palpation): Retained and revised. Reporting simplified to muscle level (Temporalis/Masseter) rather than sub-sections (origin/body/insertion). Focuses on anterior temporalis and masseter body.

Brief Opening Movements Assessment51
- A. Pain Free Opening: [ ] mm
- B. Maximum Unassisted Opening: [ ] mm
- C. Maximum Assisted Opening: [ ] mm
- D. Terminated? No / Yes
Provocation Findings:
- Temporalis: Pain, Familiar Pain, Familiar Headache (Right/Left)
- Masseter: Pain, Familiar Pain (Right/Left)
- TMJ: Pain, Familiar Pain (Right/Left)
Brief TMJ Noises and Locking52
TMJ Noises (Open/Close)
- Examiner detects Click or Crepitus.
- Patient reports noise.
- Note if pain with click is familiar.
Joint Locking
- Reduction: Note if achieved by patient or examiner.
- Locking types: While opening or in wide open position.
Simplified Protocol: Combined examination of E4, E6, and E8 using 3 steps; if any one movement is positive, no further movement is required.
Brief Muscle & TMJ Palpation53
- Palpation Sites: Temporalis (anterior, middle, posterior) and Masseter (origin, body, insertion).
- TMJ Sites: Lateral pole (0.5 kg) and around lateral pole (1 kg).
- Data Points: Pain, Familiar Pain, Familiar Headache, and Referred Pain.
Protocol Note: For the bDC/TMD, reporting is simplified to the muscle level. Examiners focus on the anterior temporalis and masseter body. Supplemental muscles are removed from this brief protocol.
Brief Diagnostic Decision Tree54
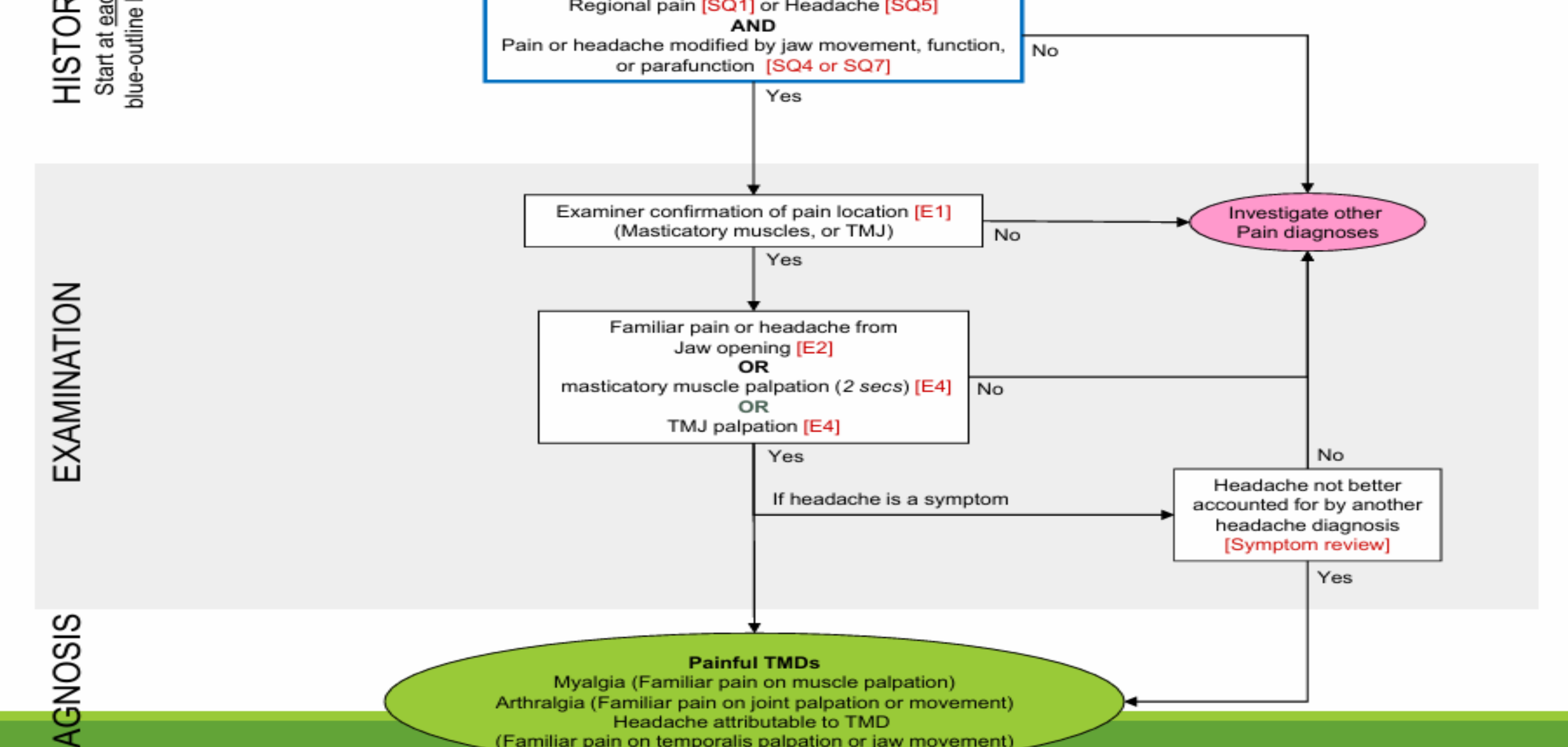
Painful TMDs Decision Tree55
- History: Regional pain [SQ1] or Headache [SQ5] AND modification by jaw function [SQ4/SQ7].
- Examination:
- Confirm pain location [E1] in masticatory muscles or TMJ.
- Identify familiar pain/headache from jaw opening [E2], muscle palpation [E4], or TMJ palpation [E4].
- Diagnosis:
- Myalgia: Familiar pain on muscle palpation.
- Arthralgia: Familiar pain on joint palpation or movement.
- Headache attributable to TMD: Familiar pain on temporalis palpation or jaw movement (if not better accounted for by another diagnosis).
Imaging is not considered at this stage of evaluation, diagnosis, and initial treatment.
Axis II Assessment Tools56
REMEMBER YOUR AXIS-II
Axis II Screening Tools57
- Pain Drawing: Identification of pain location.
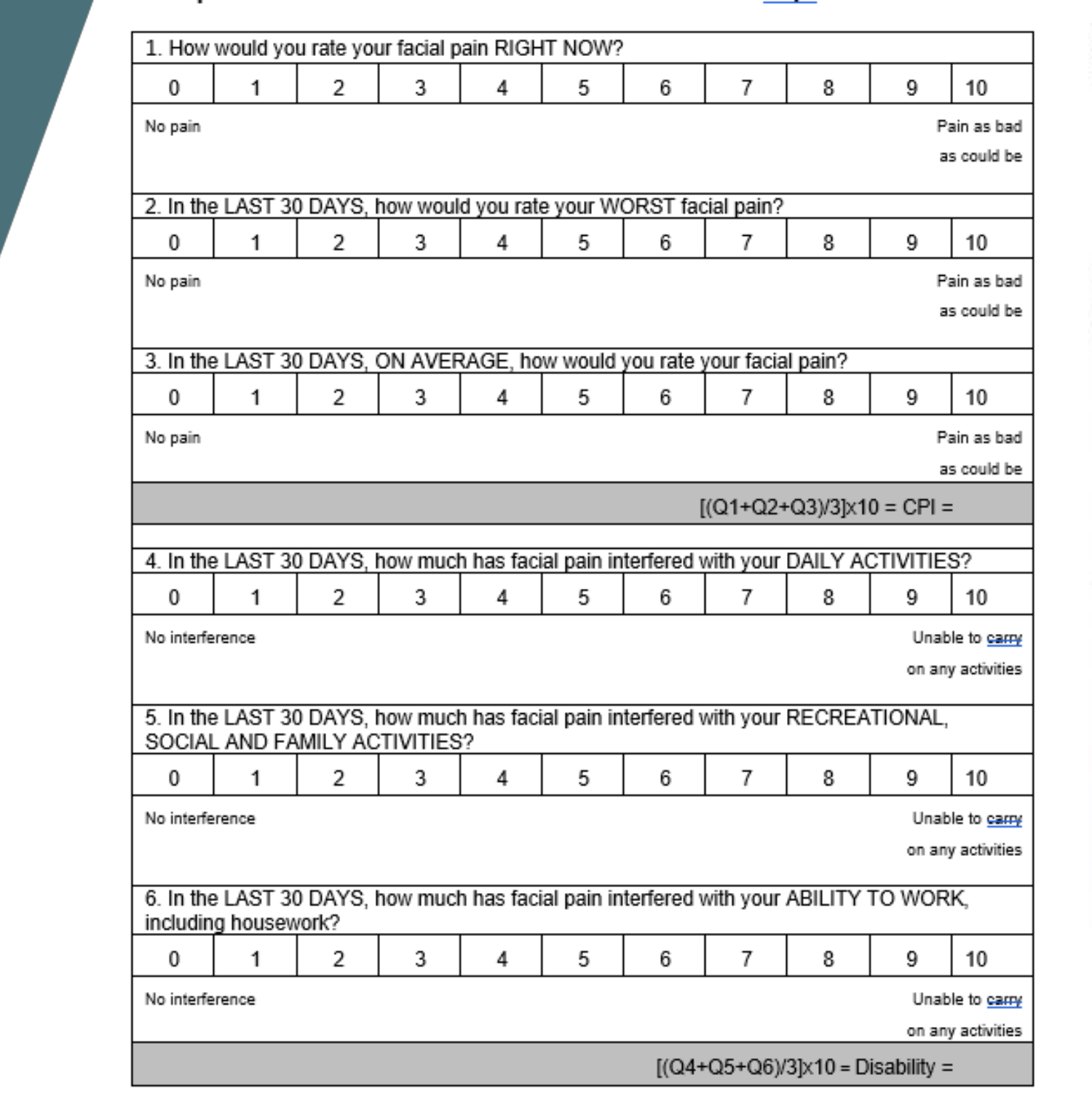
- Graded Chronic Pain Scale (GCPS): Assessment of pain intensity and disability over the last 30 days.
- PHQ-4: Screening for psychological distress (anxiety and depression).
 |  |
 |  |
Graded Chronic Pain Scale (30 Days)
- Pain Intensity (CPI): Average of “Right Now,” “Worst,” and “Average” pain ratings (0-10 scale).
- Disability Score: Average of interference with “Daily Activities,” “Recreational/Social Activities,” and “Ability to Work” (0-10 scale).
Patient Health Questionnaire - 4 (PHQ-4)
- Anxiety: Feeling nervous/anxious; unable to control worrying.
- Depression: Little interest/pleasure; feeling down/depressed.
- Scoring: 0 (Not at all) to 3 (Nearly every day). Total score indicates level of distress.
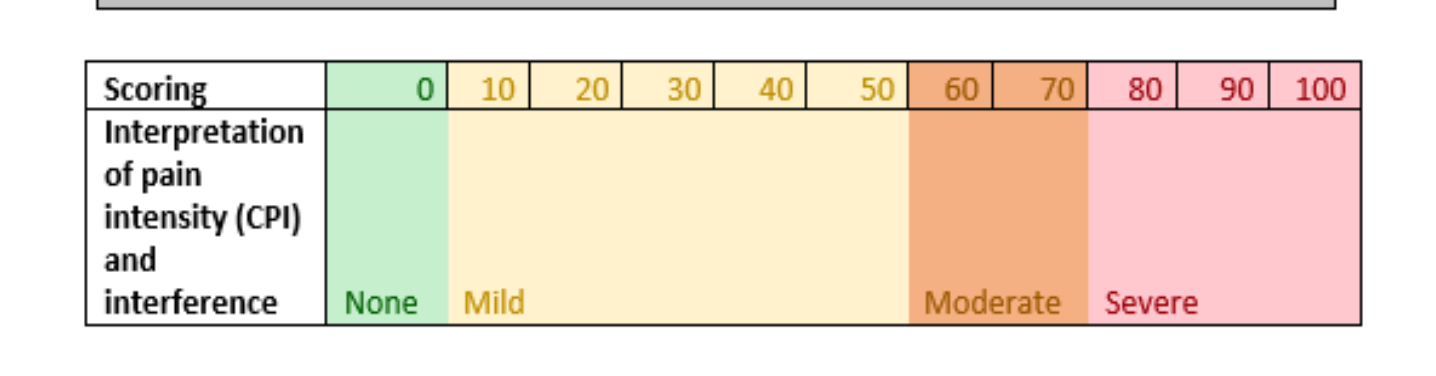
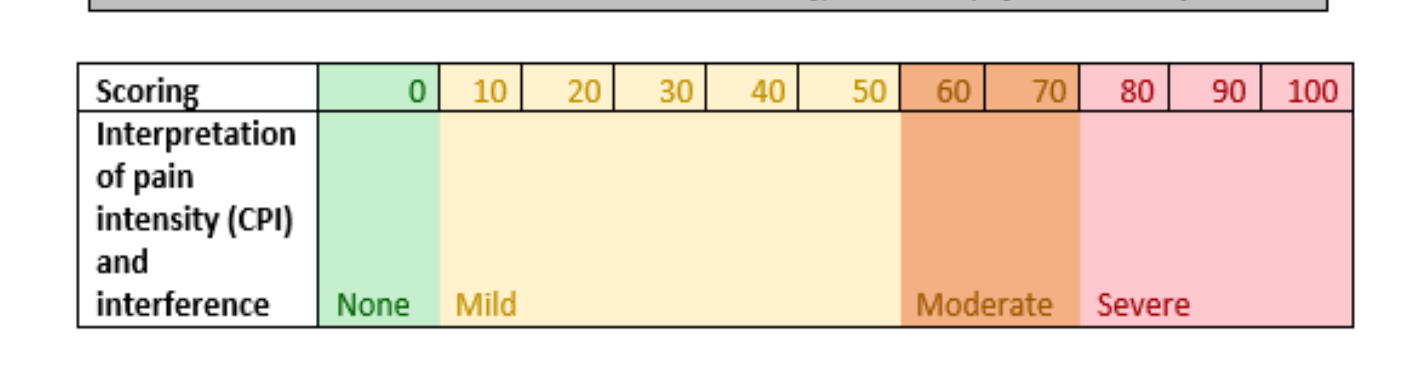
Scoring Interpretation
- 0-10: None
- 10-40: Mild
- 40-70: Moderate
- 70-100: Severe
Summary and Take Home Messages
Key Concepts of Temporomandibular Disorders58
- Temporomandibular Disorders (TMD) is a collective term.
- TMD is caused by the combination of genetics, sensory processing, psychological, and behavioural factors.
Occlusion and TMD
Malocclusion does not cause TMD, but TMD can cause acute changes in occlusion, such as an inflammatory "sliding bite" or an anterior open bite resulting from joint breakdown.
Diagnostic Protocols and Clinical Practice
- History of the pain patient develops 80% of the diagnosis.
- The history is the most critical component of diagnosis, even more so than the physical examination.
- DC/TMD is a reliable and standardized protocol for diagnosing TMD in specialist settings.
- Brief DC/TMD has been developed to increase utility and expedite diagnosis in TMDs in non-specialist general dental practice.
- Refer to a specialist when the diagnosis remains unclear or if the condition does not respond to simple management strategies like a soft diet and jaw stretches.
Conclusion and Acknowledgments
Footnotes
-
Original PDF page 1: L28 TMD, p.1 ↩
-
Original PDF page 2: L28 TMD, p.2 ↩
-
Original PDF page 3: L28 TMD, p.3 ↩
-
Original PDF page 4: L28 TMD, p.4 ↩
-
Original PDF page 6: L28 TMD, p.6 ↩
-
Original PDF page 5: L28 TMD, p.5 ↩
-
Original PDF page 7: L28 TMD, p.7 ↩
-
Original PDF page 8: L28 TMD, p.8 ↩
-
Original PDF page 9: L28 TMD, p.9 ↩
-
Original PDF page 10: L28 TMD, p.10 ↩
-
Original PDF page 11: L28 TMD, p.11 ↩
-
Original PDF page 12: L28 TMD, p.12 ↩
-
Original PDF page 13: L28 TMD, p.13 ↩
-
Original PDF page 14: L28 TMD, p.14 ↩
-
Original PDF page 15: L28 TMD, p.15 ↩
-
Original PDF page 16: L28 TMD, p.16 ↩
-
Original PDF page 17: L28 TMD, p.17 ↩
-
Original PDF page 18: L28 TMD, p.18 ↩
-
Original PDF page 19: L28 TMD, p.19 ↩
-
Original PDF page 20: L28 TMD, p.20 ↩
-
Original PDF page 21: L28 TMD, p.21 ↩
-
Original PDF page 22: L28 TMD, p.22 ↩
-
Original PDF page 23: L28 TMD, p.23 ↩
-
Original PDF page 24: L28 TMD, p.24 ↩
-
Original PDF page 25: L28 TMD, p.25 ↩
-
Original PDF page 26: L28 TMD, p.26 ↩
-
Original PDF page 27: L28 TMD, p.27 ↩
-
Original PDF page 28: L28 TMD, p.28 ↩
-
Original PDF page 29: L28 TMD, p.29 ↩
-
Original PDF page 30: L28 TMD, p.30 ↩
-
Original PDF page 31: L28 TMD, p.31 ↩
-
Original PDF page 32: L28 TMD, p.32 ↩
-
Original PDF page 34: L28 TMD, p.34 ↩
-
Original PDF page 33: L28 TMD, p.33 ↩
-
Original PDF page 37: L28 TMD, p.37 ↩
-
Original PDF page 39: L28 TMD, p.39 ↩
-
Original PDF page 35: L28 TMD, p.35 ↩
-
Original PDF page 36: L28 TMD, p.36 ↩
-
Original PDF page 38: L28 TMD, p.38 ↩
-
Original PDF page 40: L28 TMD, p.40 ↩
-
Original PDF page 41: L28 TMD, p.41 ↩
-
Original PDF page 42: L28 TMD, p.42 ↩
-
Original PDF page 43: L28 TMD, p.43 ↩
-
Original PDF page 44: L28 TMD, p.44 ↩
-
Original PDF page 45: L28 TMD, p.45 ↩
-
Original PDF page 46: L28 TMD, p.46 ↩
-
Original PDF page 47: L28 TMD, p.47 ↩
-
Original PDF page 48: L28 TMD, p.48 ↩
-
Original PDF page 50: L28 TMD, p.50 ↩
-
Original PDF page 49: L28 TMD, p.49 ↩
-
Original PDF page 51: L28 TMD, p.51 ↩
-
Original PDF page 52: L28 TMD, p.52 ↩
-
Original PDF page 53: L28 TMD, p.53 ↩
-
Original PDF page 55: L28 TMD, p.55 ↩
-
Original PDF page 54: L28 TMD, p.54 ↩
-
Original PDF page 56: L28 TMD, p.56 ↩
-
Original PDF page 57: L28 TMD, p.57 ↩
-
Original PDF page 58: L28 TMD, p.58 ↩