Intracapsular Disorders Of The Temporomandibular Joint
Pathophysiology, Diagnosis & Management1
Presented by Dr. Supeetha Suntharamoorthy, Oral Medicine Specialist.
Reference:
- Devaraj SD, Pradeep D. 2014. Internal Derangement of Temporomandibular Joint - A Review. IOSR Journal of Dental and Medical Sciences, 13, 66-73.
 |  |
Learning Objectives
Core Competencies
- Understand intracapsular TMJ disorders
- Understand the different types of conditions occurring within the temporomandibular joint (TMJ).
- Recognise clinical features
- Recognize clinical features of intracapsular disorders.
- Apply diagnostic frameworks
- Follow the diagnostic framework to determine appropriate management strategies.
- Develop management plans
Recommended Reading Resources
- Farah CS, Balasubramaniam R, McCullough MJ. 2019. Contemporary Oral Medicine. Springer Nature Switzerland.
- Okeson J. 2020. Management of Temporomandibular Disorders and Occlusion. 8th ed. Elsevier: Missouri.
- Schiffman et al. 2014. The Diagnostic Criteria for Temporomandibular Disorders (DC/TMD). J Oral & Facial Pain & Headache.
Key Temporomandibular Joint Anatomy
Anatomical Components2
- Mandibular condyle
- Mandibular/Glenoid fossa of the temporal bone
- Articular/TMJ disc
- Bilaminar zone
- Superior retrodiscal lamina
- Inferior retrodiscal lamina
- Retrodiscal tissue
- Capsular ligaments
- Synovial membrane and joint fluid
- The TMJ apparatus also includes the two bellies of the lateral pterygoid muscle.
- Dysfunction in these structures manifests as clicking, crepitus, limited opening, or jaw deviation.
 |  |
Condyle And Mandibular Fossa
Condyle Characteristics
- The articular surface on the posterior aspect of the condyle is greater than on the anterior aspect.
- During mouth opening, the condyle slides forward (translates) along the mandibular fossa toward the articular eminence.
Bony Structures of the Fossa
- Articular eminence (AE)
- Mandibular fossa (MF)
- Squamotympanic fissure (STF)
Anatomical Context
The glenoid fossa (mandibular fossa) is part of the squamous portion of the temporal bone.
Articular Disc And Retrodiscal Tissues
Articular Disc Properties3
- Biconcave structure
- Dense fibrous connective tissue
- Avascular and aneural
- Flexible and adaptive
- Morphology is affected by destructive forces
 |  |
 |
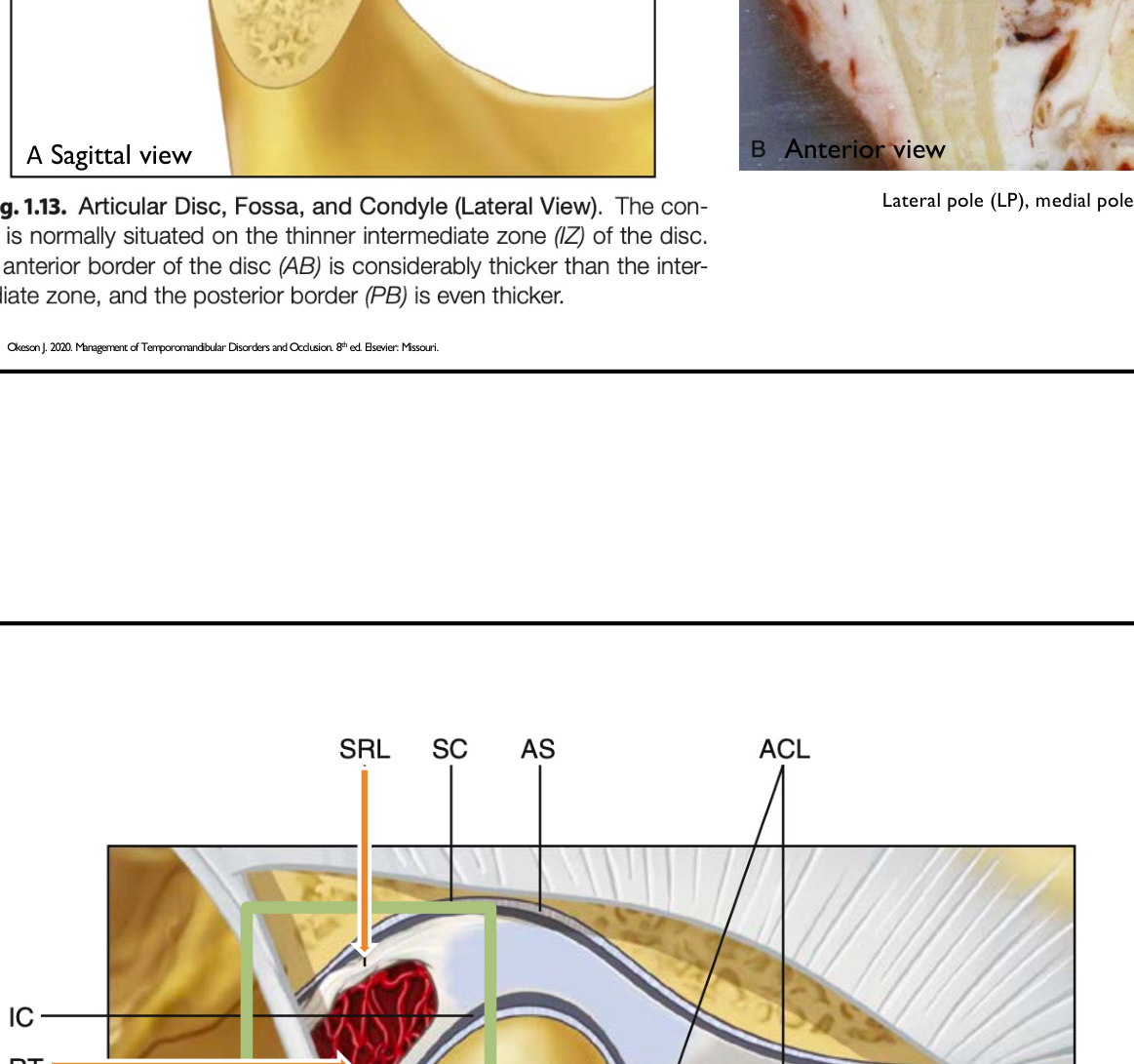
Disc Zones
- Anterior (AB)
- Intermediate (IB)
- Posterior (PB)
- Intermediate Zone: The thinnest part of the disc where the condyle articulates.
- Anterior Border: Thicker than the intermediate zone.
- Posterior Border: The thickest part of the disc in a normal joint.
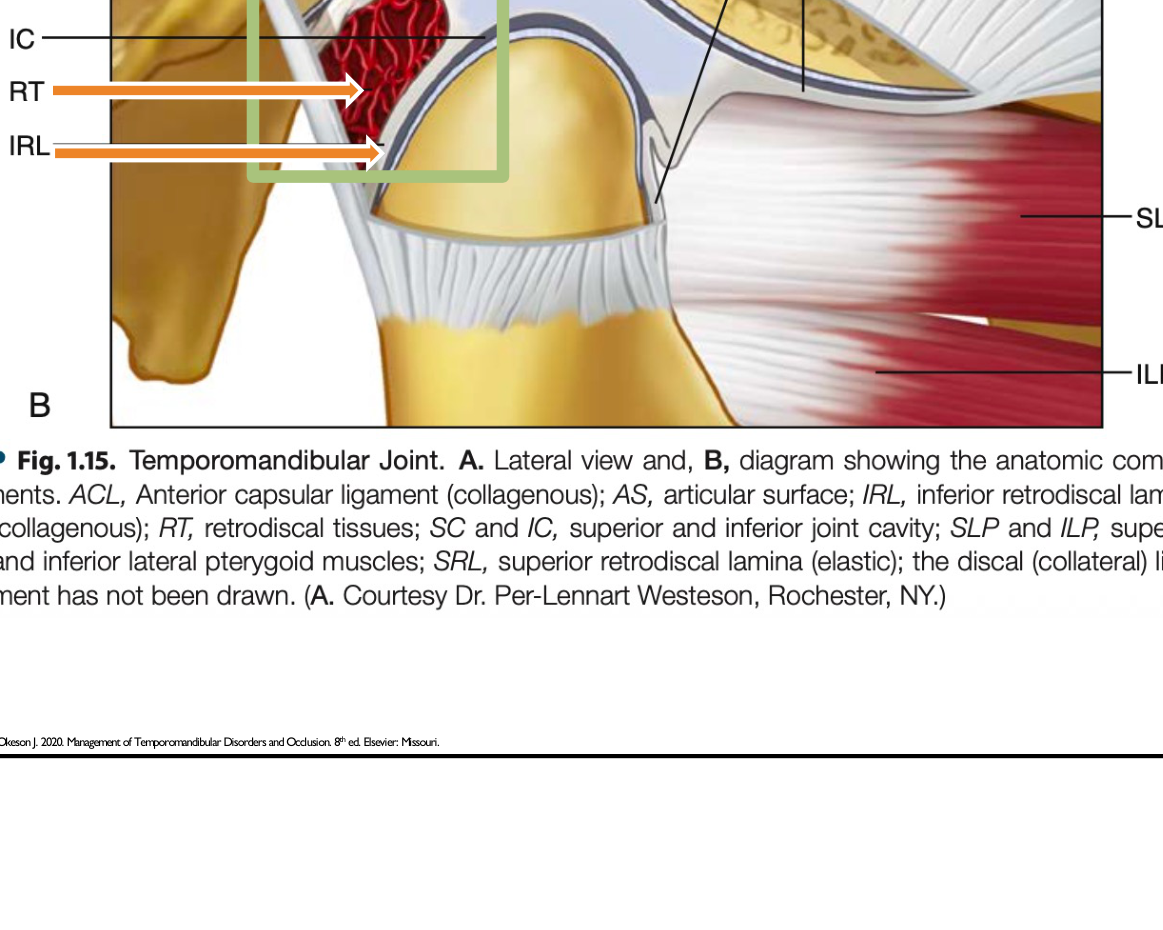
Retrodiscal Tissues
- Includes the bilaminar zone consisting of superior and inferior laminae.
- This area is highly innervated and vascularized; pain in the joint often arises from this region.
- Superior Lamina: Composed of elastic tissue that stretches during opening.
- Inferior Lamina: Non-elastic connective tissue that does not stretch.
Capsular Ligaments And Compartments
Ligamentous Structures4
- Capsular Ligament: Extends anteriorly to include the articular eminence and encompasses the entire articular surface of the joint
- Attaches superiorly to the temporal bone and inferiorly to the coronoid process.
- Temporomandibular Ligament: Consists of two distinct parts:
- Outer oblique portion (OOP): Limits normal rotational opening movement.
- Inner horizontal portion (IHP): Limits posterior movement of the condyle and disc.
- Accessory Ligaments:
- Stylomandibular ligament
- Sphenomandibular ligament
- Accessory ligaments provide stability rather than assisting in movement.
- If these ligaments elongate due to destructive forces, they do not return to their original length, leading to dysfunction.
- Discal Ligaments:
- Lateral discal ligament (LDL)
- Medial discal ligament (MDL)
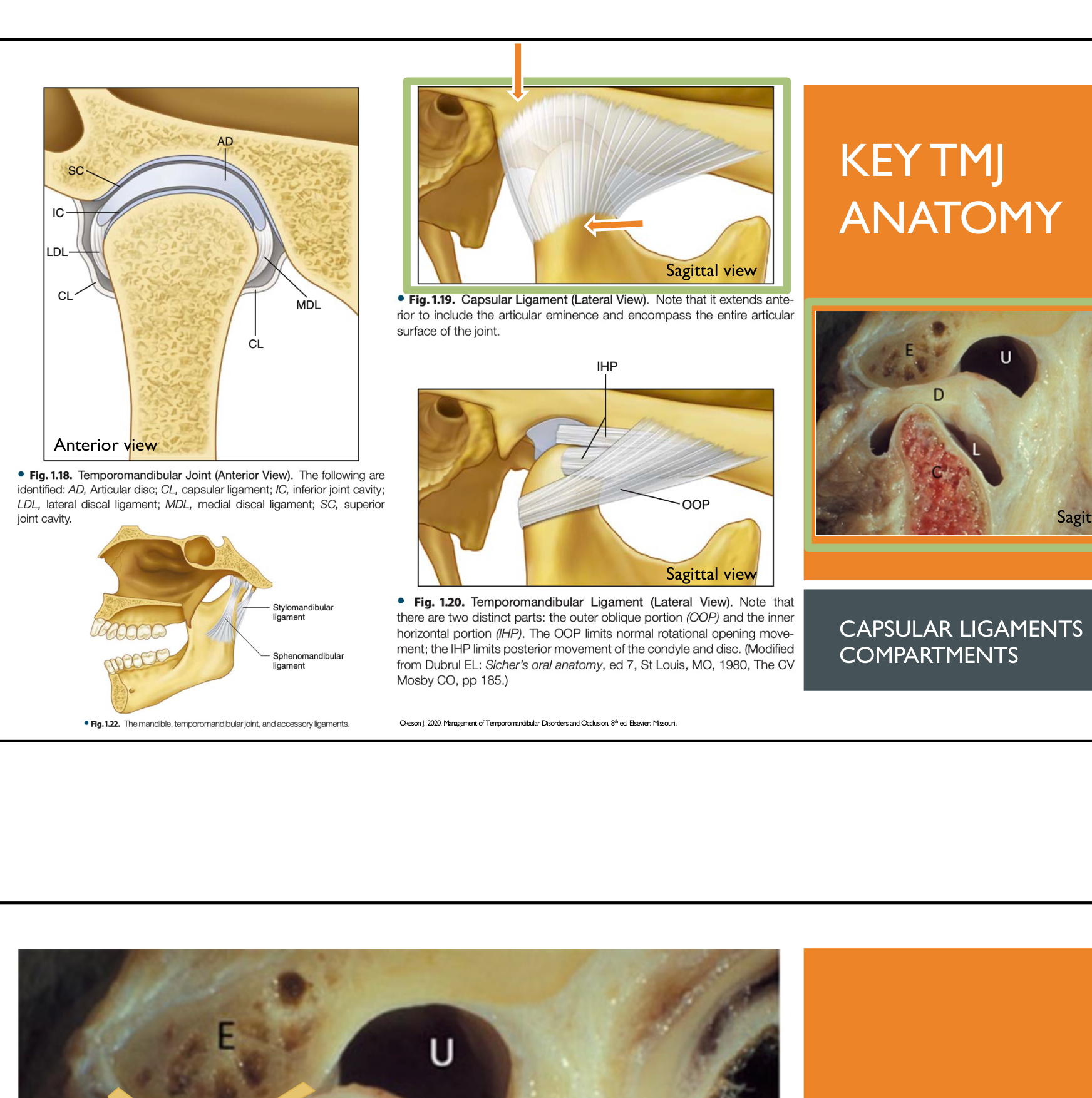 |  |
Joint Compartments
- Superior joint cavity (SC): Upper compartment between the disc and the eminence.
- Inferior joint cavity (IC): Lower compartment between the disc and the condyle.
Synovial Membrane
- Lines the joint cavities and produces synovial fluid for lubrication and nutrient transport.
- Lined by endothelial cells, the membrane secretes synovial fluid which provides metabolic activity to the articulating surfaces.
Temporomandibular Joint Biomechanics5
 |  |
Normal Joint Movement6
- Rotation: Occurs during early opening (20-35 mm
- Occurs in the lower compartment during the first 20–35 mm of opening.).
- Translation: Occurs during late opening
- Occurs in the upper compartment as the condyle moves down the articular eminence.
- Function relies on disc-condyle coordination and effective load distribution.
 |  |
Role of Disc Morphology
- Disc morphology is critical for maintaining correct positioning during joint function.
- Normal shape combined with intra-articular pressure enables self-positioning of the disc, ensuring smooth and stable movement.
- In a normal state, the biconcave shape ensures even pressure distribution.
- The ligaments play a passive, supportive role in positioning the disc while muscles drive movement.
- Ligamentous attachments have minimal functional impact when disc morphology is intact.
Pathophysiological Changes
- Significant alteration of disc morphology compromises the system.
- Ligaments do not stretch but become elongated with excessive force.
- Articular surfaces are no longer maintained in constant contact.
- Disruption leads to the development of TMJ dysfunction signs and symptoms.
Causes of Disruption
- Microtrauma: Repetitive low-grade loading (e.g., bruxism, clenching, bracing).
- Macrotrauma: Sudden falls or hits to the jaw.
- Ligament Laxity: Often seen in hypermobility disorders.
- Systemic Factors: Emotional stress, poor sleep, and altered pain processing (e.g., fibromyalgia).
Clinical Features And Classification
Common Clinical Signs7
- Joint pain (preauricular)
- Clicking, popping, or crepitus
- Restricted or deviated mouth opening
- Deviation (moves to one side and corrects) vs. deflection (moves to one side and stays there)
- Locking (intermittent or persistent)
- Pain on function (chewing, yawning)
- Parafunction features (e.g., occlusal wear)
- Intraoral signs: Linea alba (thickened buccal mucosa) and tongue scalloping
 |  |
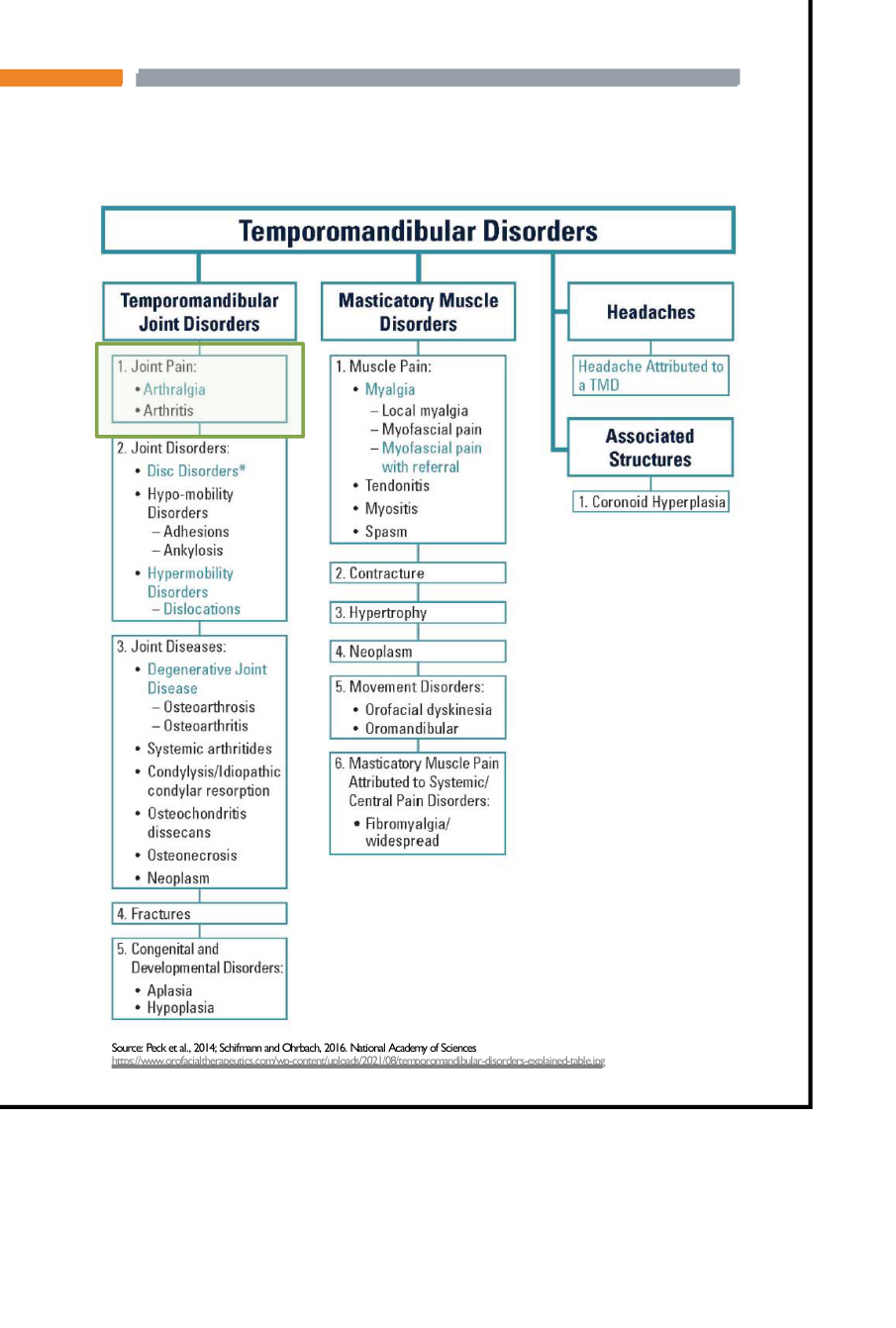
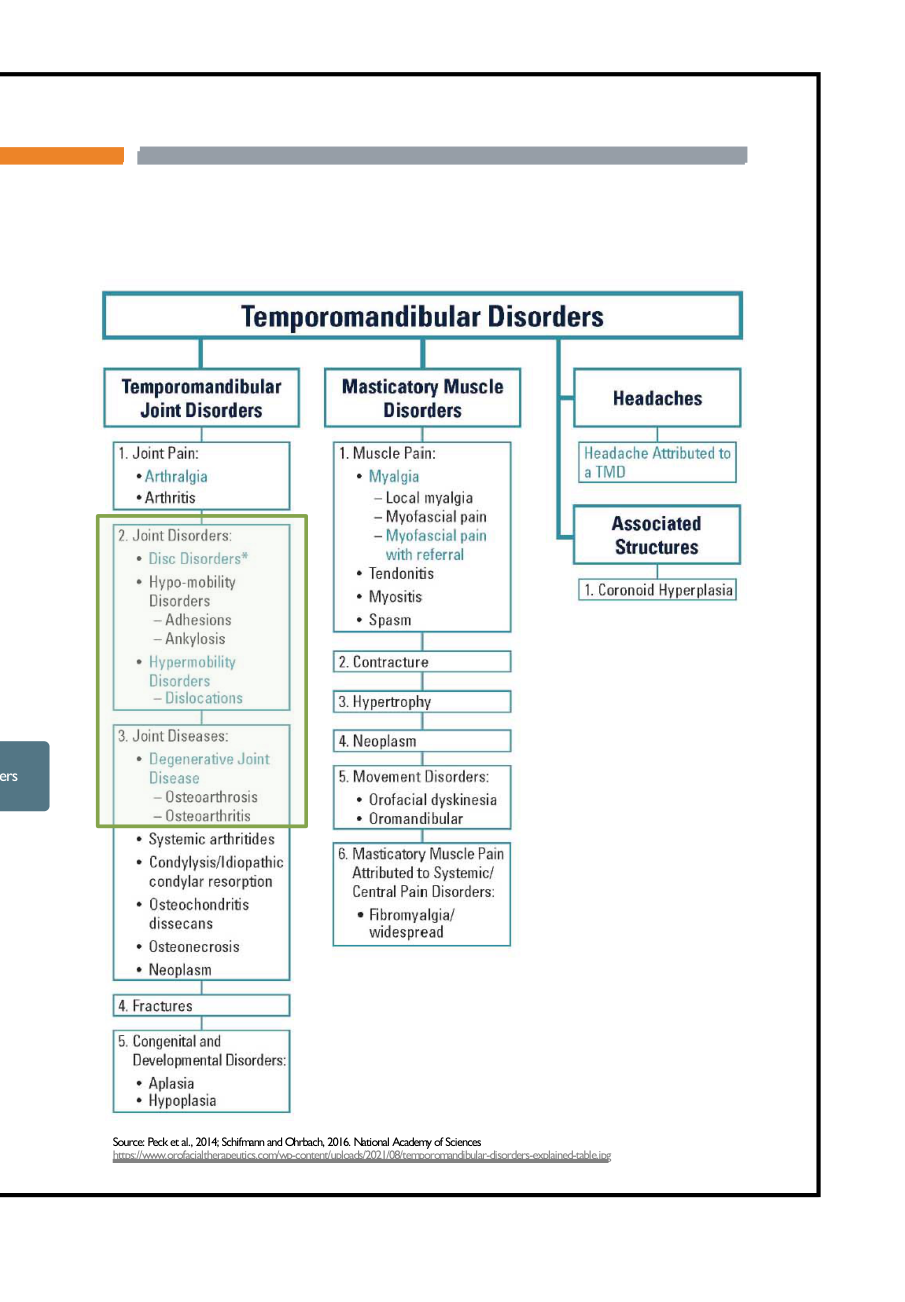
Diagnostic Criteria For Intracapsular Disorders
DC-TMD Classification
- Disc displacement with reduction
- Disc displacement with reduction with intermittent locking
- Disc displacement without reduction with limited opening
- Disc displacement without reduction without limited opening
Broad Categorization
Conditions are broadly categorized by location:
- Condyle-Disc Derangement: Disturbance in the relationship between the condyle and disc.
- Structural Incompatibility: Breakdown of bony surfaces or ligaments.
- Inflammatory Disorders: Pain driven by inflammation.
Pathophysiology Of Joint Pain
Pain Classifications8
- Arthralgia: Pain in TMJ structures arising from nociceptors in soft tissues (ligaments, retrodiscal tissues, synovial lining). It is non-inflammatory and provoked by movement or palpation.
- Arthritis: Inflammation in TMJ structures characterized by pain, swelling, warmth, and erythema. Often associated with systemic disease; pain may occur at rest
- Retrodiscitis: Pain arising from the retrodiscal tissues.
- Synovitis: Inflammation of the synovial lining.
 |  |
 |
Clinical Effects of Pain
- Limited mandibular movement
- Protective co-contraction
- Soft end feel: Suggests muscle issues (can be stretched further).
- Hard end feel: Suggests an intracapsular condition (mechanical stop).
Joint Disorders and Degenerative Disease
- Joint Disorders: Conditions affecting the articular disc, bony surfaces, and supporting ligaments (e.g., displacements, hypermobility).
- Joint Diseases: Degenerative Joint Disease (DJD) including Osteoarthrosis (non-inflammatory) and Osteoarthritis (inflammatory).
Disc Displacement Disorders
Disc Displacement With Reduction
Diagnostic Criteria Summary9
- History: Clicking or popping during opening and/or closing.
- The disc is displaced in a closed position but returns to its proper position upon opening.
- Clinical Examination:
- Reproducible click on opening and/or closing (at least 1 of 3 cycles).
- Normal range of mouth opening.
- Ipsilateral jaw deviation on opening with correction.
- Possible TMJ pain on movement, function, or palpation.
 | 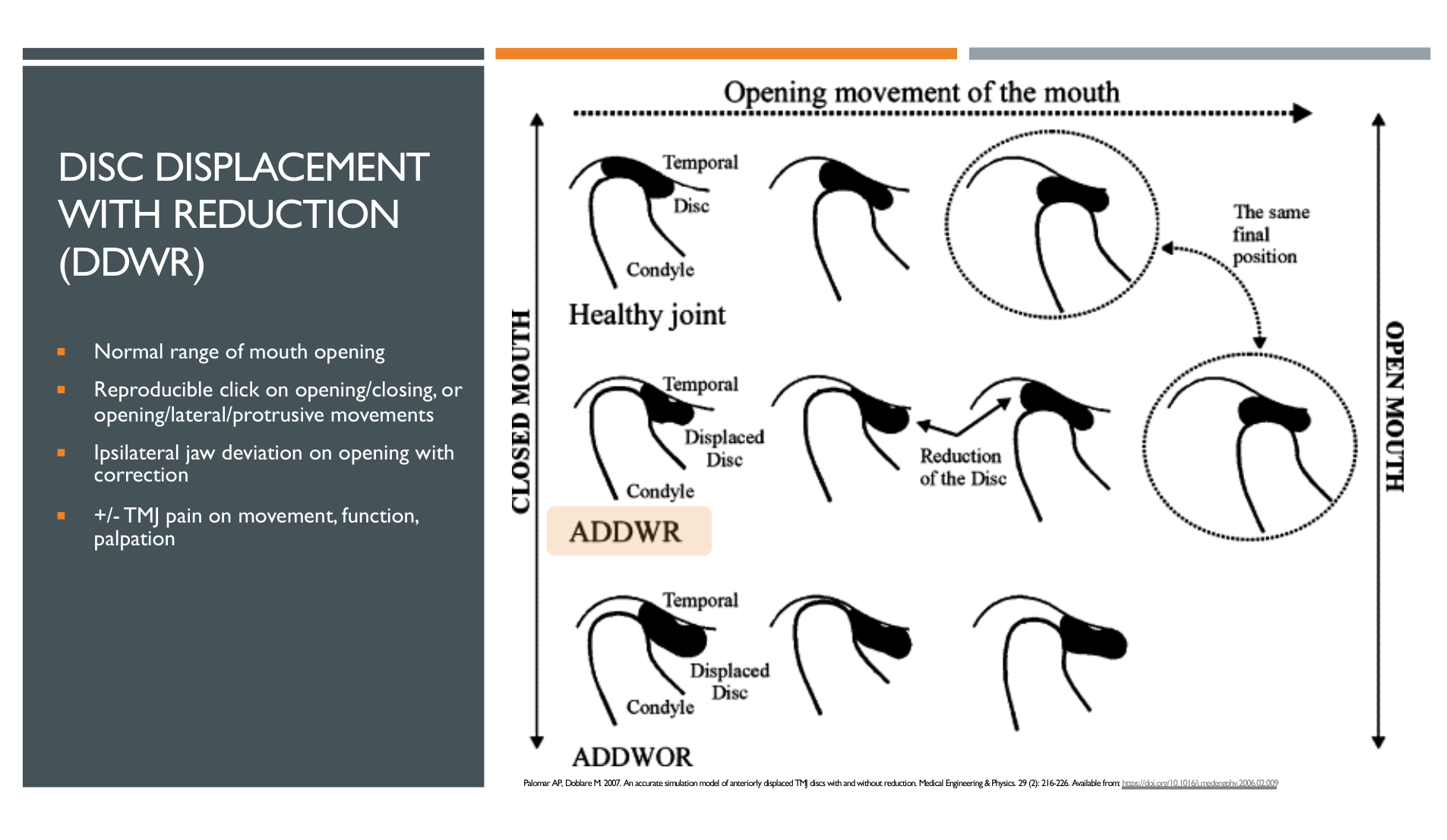 |
Pathophysiology Progression10
- Evaluation involves assessing anatomical variations via MRI or X-ray.
- Clinical symptoms follow a progression flowchart from initial displacement to potential functional impairment.
 |  |
 |
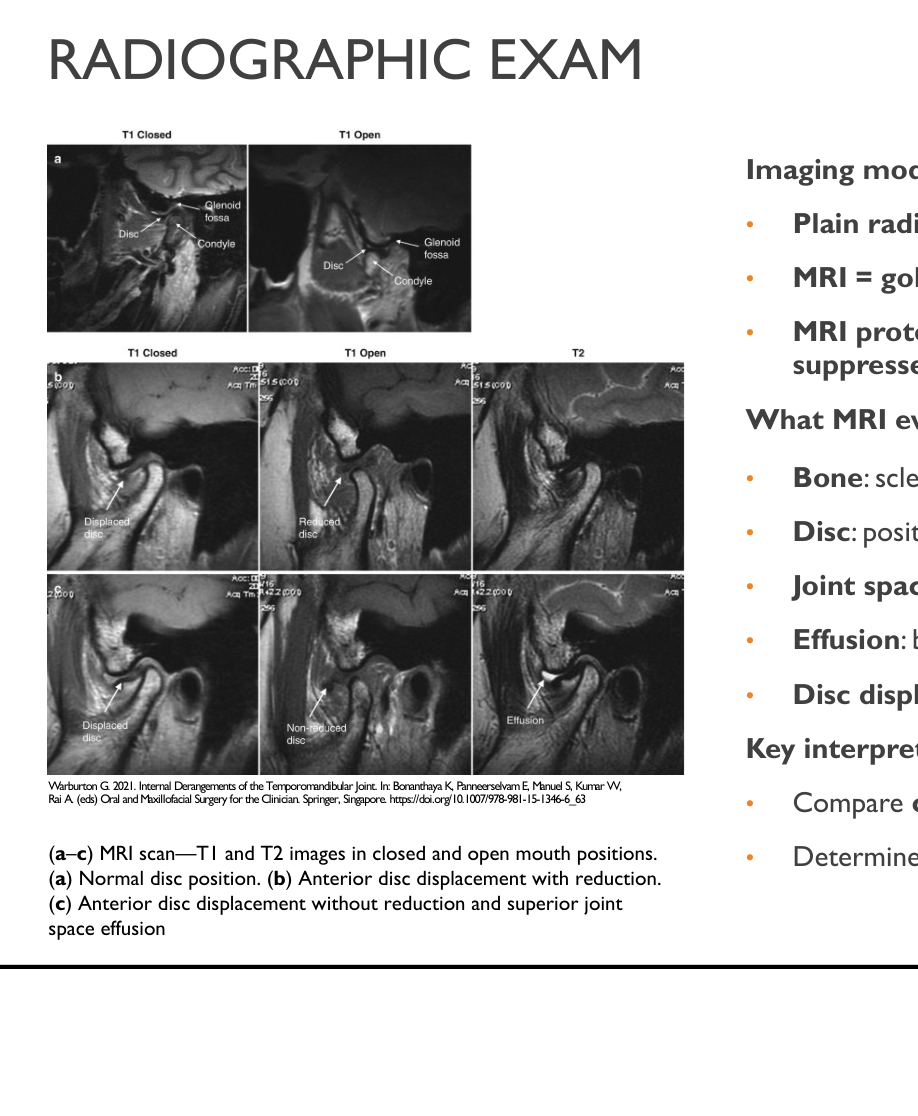
Imaging Observations11
- MRI (fat-saturation T2 sagittal) may show anterior disc displacement of a crumpled disc in the closed-mouth position.
- Reduction of the disc occurs in the open-mouth position.
- Associated findings may include effusion and changes in the bilaminar zone.
 |  |
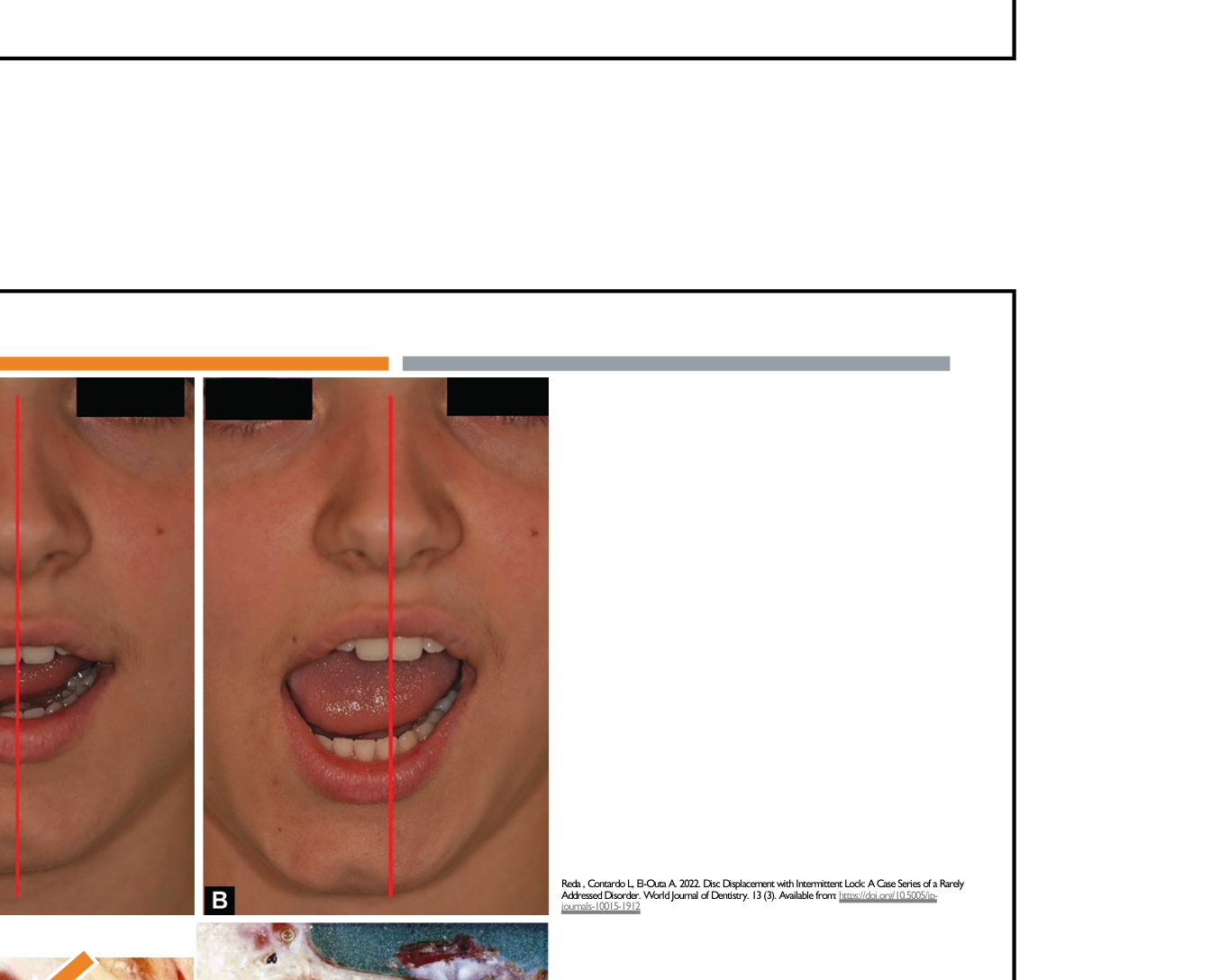
Disc Displacement With Intermittent Locking
Clinical Presentation
- Episodes of “catching” or intermittent locking.
- Normal mouth opening, though intermittently limited during locking episodes.
- Clicking on opening and closing (may become inconsistent).
- Ipsilateral jaw deviation on opening with correction when reduction occurs.
- Increased joint instability and risk of progression to persistent mechanical restriction.
Clinical Note
The patient often experiences periodic episodes where the jaw "catches" or gets stuck, requiring manual adjustment to open.
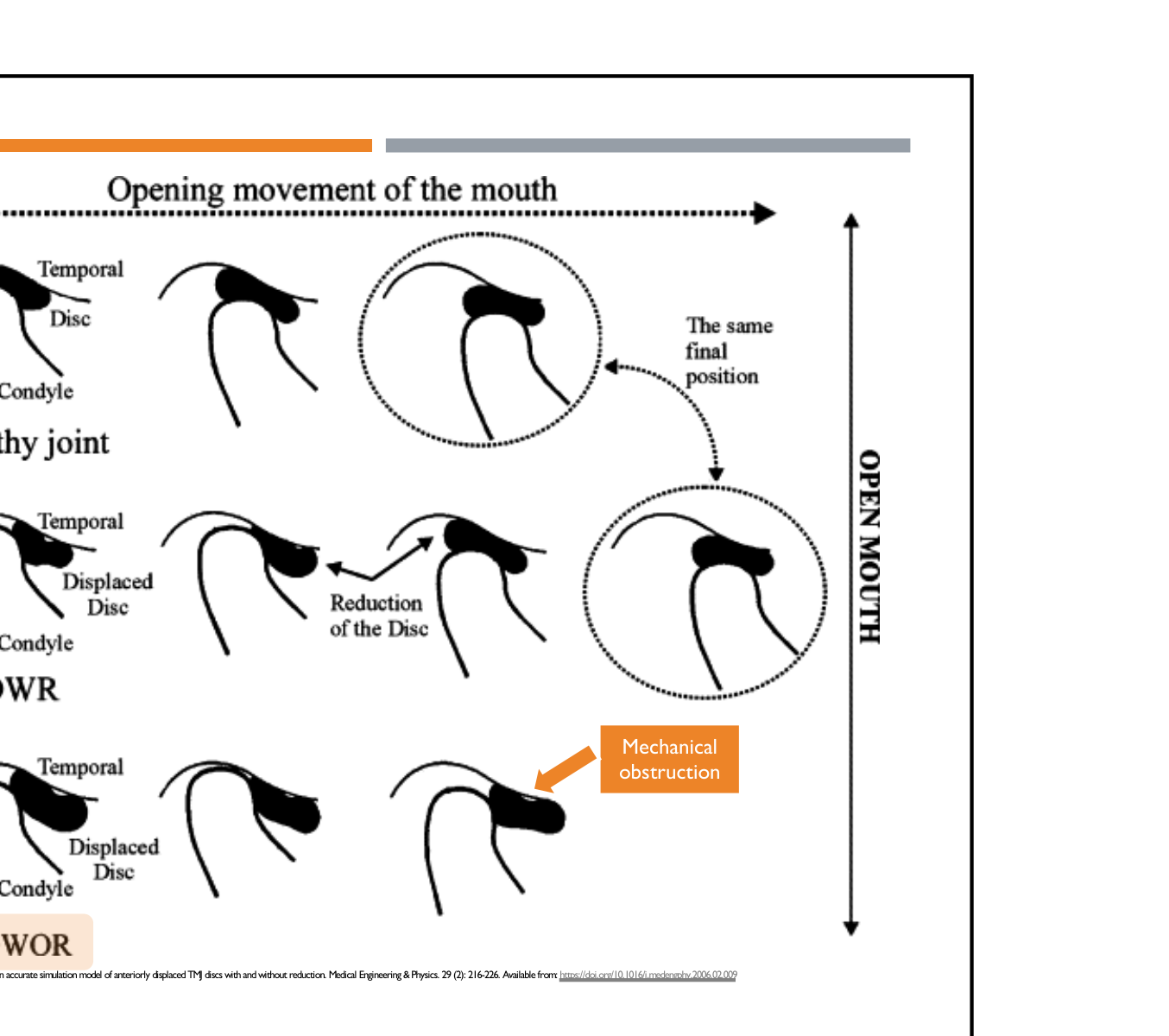
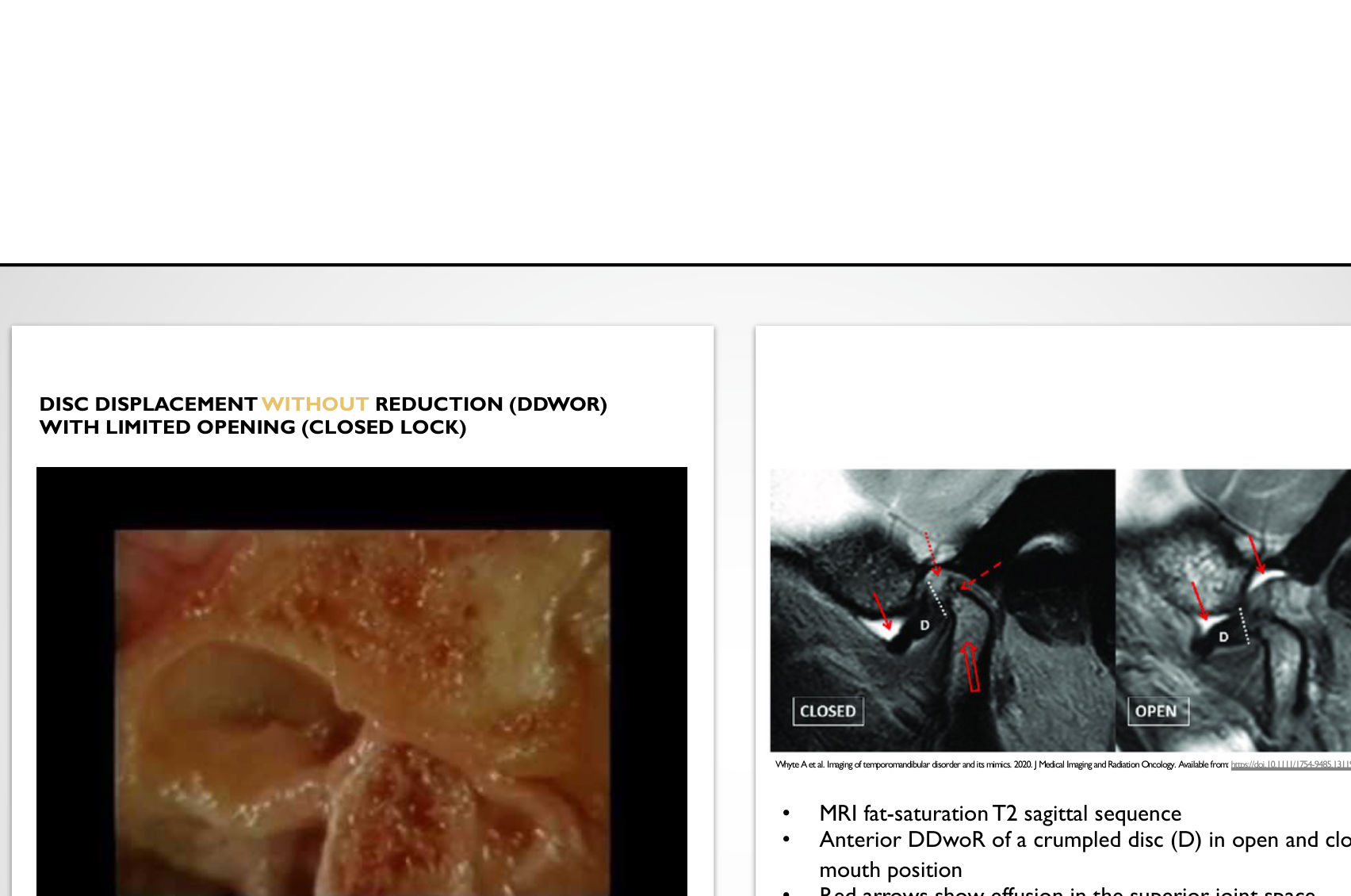
Disc Displacement Without Reduction With Limited Opening
Clinical Features (Closed Lock)12
-
Limited range of mouth opening (typically <35-40 mm; often 25-30 mm initially).
-
No clicking on opening and closing (loss of prior joint sounds).
-
Ipsilateral jaw deflection on opening (no correction).
-
Restricted contralateral excursion.
-
Possible TMJ pain on movement, function, or palpation.
-
This represents a mechanical problem where the disc fails to reduce.
-
The disc is permanently displaced and acts as a mechanical obstruction.
 |  |
Disc Displacement Without Reduction Without Limited Opening
Clinical Features13
- History of prior limited opening (“closed lock”).
- Normal or near-normal range of mouth opening (≥ 40 mm) as opening is no longer limited.
- No clicking on opening and closing.
- Ipsilateral jaw deflection may reduce or become minimal.
- Possible TMJ pain on movement, function, or palpation.
- Characterized as an adapted, non-reducing disc.
 |  |
Hypermobility And Luxation
Subluxation Characteristics
Clinical Presentation14
- Excessive anterior translation of the condyle beyond the articular eminence.
- Mouth opening > 40 mm.
- The patient can "wiggle" the jaw back into place.
- Sudden “jump” or “thud” at maximal opening.
- No clicking (not a disc displacement).
- Often visible preauricular depression at full opening.
- Usually painless and non-pathological; may be associated with ligamentous laxity.
- Repetitive episodes may predispose to joint instability.
 |  |
 |
Luxation And Emergency Management
Clinical Presentation15
- Condyle displaced anterior to the articular eminence.
- Inability to close the mouth.
- Typically occurs after wide opening (yawning, dental procedures).
- Often referred to as an "open lock" where the condyle is trapped in front of the articular eminence.
- Often preceded by hypermobility or subluxation tendency.
- Patient may appear anxious and unable to self-reduce.
- This is a clinical emergency and not a disc disorder.
 | |
 |
Emergency Management
- Syringe Method (First-line): Place 5-10 mL syringe between posterior molars; patient gently bites and rolls to allow self-reduction
- The syringe acts as a rotating fulcrum to reseat the condyle.
- Manual Reduction: Thumbs on lower molars, apply downward then posterior force to disengage the condyle and guide it back into the fossa
- Apply firm pressure while lifting the chin and use gauze to protect fingers during manual reduction.
- Adjuncts: Local anesthetic or auriculotemporal nerve block to reduce pain and muscle spasm.
- Post-reduction Care: Avoid wide opening, soft diet, NSAIDs, and specialist follow-up.
Inflammatory And Degenerative Disorders
Synovitis And Capsulitis
Inflammatory Conditions16
- Synovitis: Inflammation of the synovial lining; constant deep pain that increases with movement.
- Often causes localized pain and potentially joint effusion (fluid buildup).
- Capsulitis: Inflammation of the capsular ligament; localized tenderness at the lateral pole, pain at rest and during function.
- Retrodiscitis: Inflammation of retrodiscal tissues; constant dull aching pain worsened by clenching; may cause acute malocclusion.

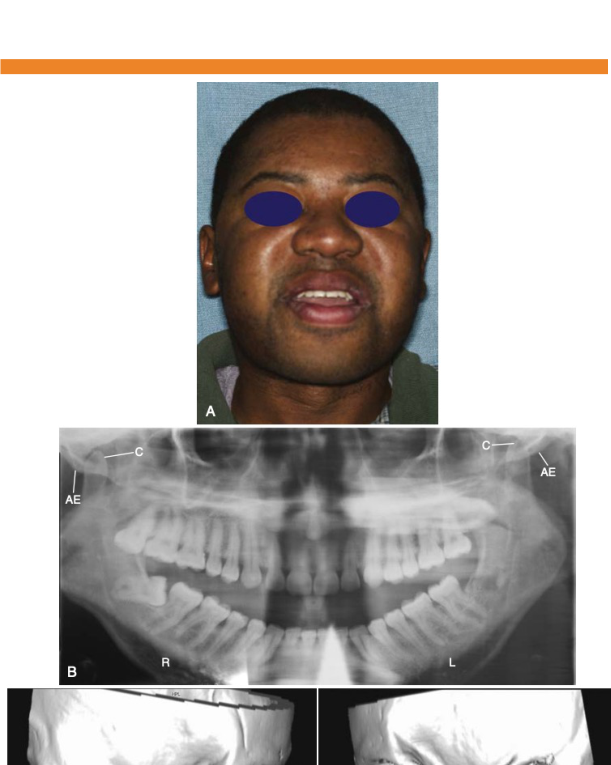
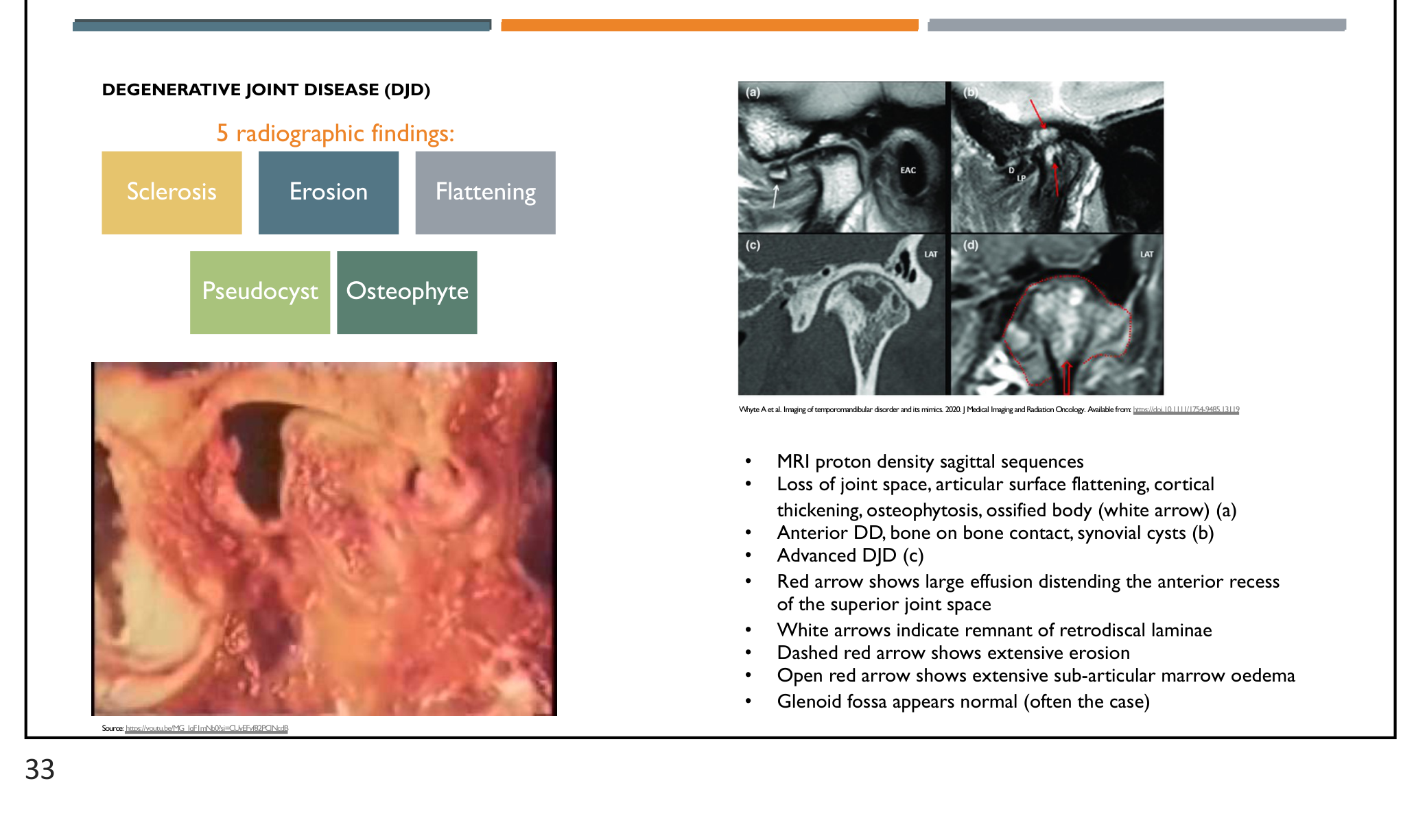
Degenerative Joint Disease
Clinical and Radiographic Features17
- Crepitus: Coarse, grating, or grinding joint noise.
- Described as a grating sound like "rubble".
- Limited Opening: Typically <35 mm.
- Osteoarthrosis: Non-inflammatory structural change (wear-and-repair imbalance).
- Osteoarthritis: Inflammatory DJD with pain.
- Radiographic Findings: Sclerosis, erosion, flattening, pseudocysts, and osteophytes.
- Commonly visualized via CT or OPG.
- Osteophytes may present with a "bird’s beak" appearance.
- Pathophysiology: Response to chronic mechanical overload leading to cartilage softening (chondromalacia) and progressive bone remodeling.
 |  |
Radiographic Examination And Imaging
Imaging Modalities18
- Plain Radiographs / CT: Used to assess bony changes.
- ==CT: Best for assessing bony changes and degeneration.==
- MRI: Gold standard for disc position and soft tissues (~90% accuracy).
- T1 and T2 sequences evaluate bone, disc position/shape, joint space, and effusion.
- Comparison of closed vs. open mouth views determines reducibility.
- ==OPG: Limited use; can show gross condylar morphology but not disc position.==
 | 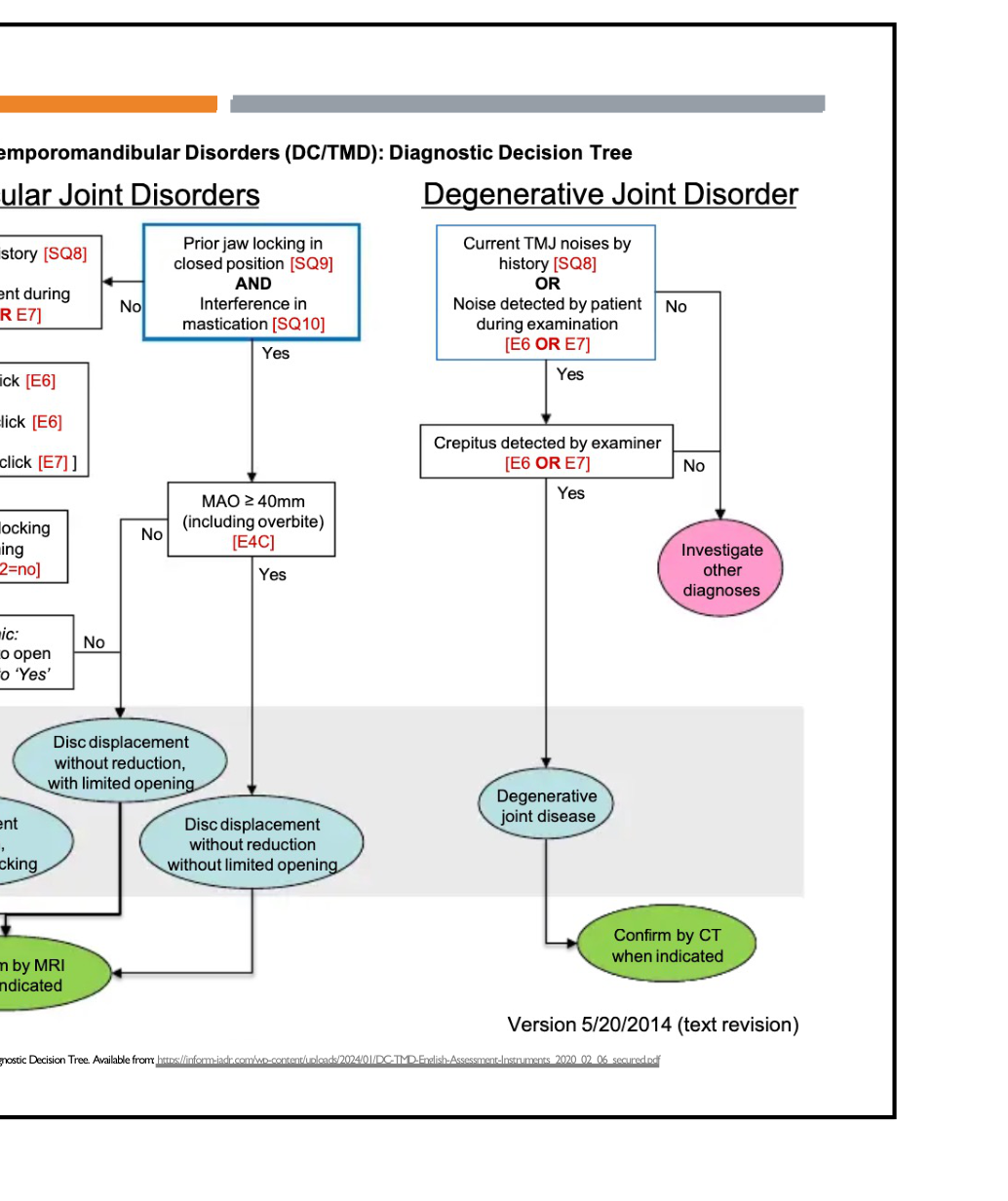 |
Diagnostic Decision Tree
- Evaluation starts with history of joint noises and locking.
- Clinical examination confirms presence of clicks or crepitus.
- Imaging (MRI or CT) is used to confirm clinical diagnoses of disc displacements or degenerative disorders.
Management Strategies
Conservative And Specialist Management
Conservative Measures19
- Education and reassurance.
- Explain the condition to reduce anxiety.
- Nutrient-dense soft diet and habit control.
- Soft foods to avoid loading the joint.
- Cues to relax shoulders and jaw; avoid gum or wind instruments.
- Thermotherapy and physical therapy (jaw exercises, massage).
- Heat packs (10–15 mins) or ice.
- "Tongue-to-roof" controlled opening to correct deviation.
- Stress management and oral appliances.
- Used to offload the joint and protect teeth from bruxism.
- Pharmacotherapy: NSAIDs, muscle relaxants, TCAs, SSRIs, or Botox.
Specialist Referral and Procedures
- Indications: Persistent symptoms, recurrent locking, diagnostic uncertainty, or significant functional limitation.
- Specialist Options:
- Custom stabilization splints.
- Intra-articular injections (e.g., corticosteroids).
- Arthrocentesis (joint lavage).
- Flushing the joint to remove inflammatory markers.
- Arthroscopy (adhesiolysis, synovial assessment).
- Open joint surgery (rare) for disc repositioning or repair.
Prognostic Factors
Factors Influencing Outcome20
- Compliance
- Severity of the disorder
- Chronicity
- Psychosocial factors
- Genetic predisposition.
- Presence of chronic pain elsewhere.

Footnotes
-
Original PDF page 1: L29 TMJ Intracapsular Disorders, p.1 ↩
-
Original PDF page 2: L29 TMJ Intracapsular Disorders, p.2 ↩
-
Original PDF page 3: L29 TMJ Intracapsular Disorders, p.3 ↩
-
Original PDF page 4: L29 TMJ Intracapsular Disorders, p.4 ↩
-
Original PDF page 6: L29 TMJ Intracapsular Disorders, p.6 ↩
-
Original PDF page 5: L29 TMJ Intracapsular Disorders, p.5 ↩
-
Original PDF page 7: L29 TMJ Intracapsular Disorders, p.7 ↩
-
Original PDF page 8: L29 TMJ Intracapsular Disorders, p.8 ↩
-
Original PDF page 9: L29 TMJ Intracapsular Disorders, p.9 ↩
-
Original PDF page 10: L29 TMJ Intracapsular Disorders, p.10 ↩
-
Original PDF page 11: L29 TMJ Intracapsular Disorders, p.11 ↩
-
Original PDF page 12: L29 TMJ Intracapsular Disorders, p.12 ↩
-
Original PDF page 13: L29 TMJ Intracapsular Disorders, p.13 ↩
-
Original PDF page 14: L29 TMJ Intracapsular Disorders, p.14 ↩
-
Original PDF page 15: L29 TMJ Intracapsular Disorders, p.15 ↩
-
Original PDF page 16: L29 TMJ Intracapsular Disorders, p.16 ↩
-
Original PDF page 17: L29 TMJ Intracapsular Disorders, p.17 ↩
-
Original PDF page 18: L29 TMJ Intracapsular Disorders, p.18 ↩
-
Original PDF page 19: L29 TMJ Intracapsular Disorders, p.19 ↩
-
Original PDF page 20: L29 TMJ Intracapsular Disorders, p.20 ↩