Dent 5301: Oral Medicine I1
Diagnostic Investigations in Oral Medicine
This course covers the essential diagnostic tools and procedures used in clinical practice to identify and manage oral diseases. The primary areas of focus include:
- Blood testing: Analysis of systemic markers to identify underlying conditions affecting oral health.
- Histopathology: Microscopic examination of tissue samples to diagnose lesions and malignancies.
- Microbiological investigations: Identification of bacterial, viral, and fungal pathogens.
- Skin testing: Diagnostic procedures, such as patch testing, used to identify hypersensitivities and allergic reactions.
Presented by Dr Agnieszka Frydrych at The University of Western Australia.
Introduction2
Rationale for Investigations
In some instances, investigations may be required to help:
- Make or confirm the diagnosis
- Establish prognosis
- Exclude some diagnosis
Investigations are a critical extension of history-taking and clinical examination in oral medicine practice. They serve three primary functions:
- ==Diagnosis and Confirmation: Essential for establishing definitive diagnoses, particularly for cancers and potentially malignant disorders (PMDs) where histopathological confirmation is mandatory.==
- ==Prognosis: Critical in determining outcomes, especially in oral cancer patients.==
- ==Exclusion: Necessary to rule out specific pathologies (e.g., performing a biopsy on a non-healing ulcer to exclude neoplasia).==
Appropriateness of Testing
However, investigations must be appropriate and justified. Inappropriate testing can create unnecessary patient anxiety, consume significant time (e.g., a glucose tolerance test requires two hours), incur substantial costs (not all tests are fully covered by Medicare), and potentially cause adverse effects (particularly with invasive procedures like biopsy).
The main investigations utilized in oral medicine include:
- Blood tests
- Skin tests (patch testing)
- Biopsy
- Microbiological investigations
- Imaging (covered in a separate dedicated lecture)
Critical Importance
If a histopathology report is inconsistent with clinical impression (e.g., a benign report when malignancy is suspected), the pathologist must be contacted immediately. Accepting a benign conclusion for a clinically malignant lesion has serious consequences.
Case Study: Discrepant Histopathology Report
A patient with suspected oral lichen planus underwent biopsy of the left lateral tongue. The report conclusion stated “oral lichen planus”; however, the microscopic description did not describe lichen planus features. Knowledge of lichen planus histopathology allowed recognition of this discrepancy. Upon contacting the pathologist, the case was reviewed, confirming oral lichen planus, and an amended report was issued.
The clinician is ultimately responsible for reading, interpreting, and conveying histopathology results to patients. This requires thorough understanding of oral mucosal disease histopathology.
Investigations
Common Diagnostic Tests
Blood Testing34567
- FBC / FBP (Full Blood Count / Full Blood Picture)
- CRP (C-Reactive Protein)
- Coagulation screen
- Iron studies
- B12
- Folate
- Blood glucose
- GTT (Glucose Tolerance Test)
- Glycated haemoglobin
- U & E (Urea and Electrolytes)
- LFT (Liver Function Test)
- Ca (Calcium)
- Phosphate
- Alkaline phosphatase
- Serology
C Reactive Protein (CRP)
CRP is produced by the liver and functions in opsonization and complement activation. It is a valuable marker for assessing acute phase reactions in inflammation, infection, and neoplastic disorders.
Full Blood Count And Red Cell Indices89
Routine Haematology Results
| Parameter | Result | Reference Range | Units |
|---|---|---|---|
| HAEMOGLOBIN | 124 | (115 - 155) | g/L |
| MCV | 92 | (82 - 98) | fL |
| RDW | 13 | (< 16) | % |
| MCHC | 343 | (320 - 360) | g/L |
| PLATELETS | 219 | (150 - 400) | 9/L |
| WHITE CELLS | 7.9 | (4.0 - 11.0) | 9/L |
| Neutrophils (75%) | 5.9 | (1.8 - 7.5) | 9/L |
| Lymphocytes (18%) | 1.4 | (1.2 - 4.0) | 9/L |
| Monocytes (7%) | 0.6 | (0.1 - 1.2) | 9/L |
| Eosinophils (0%) | 0.0 | (< 0.7) | 9/L |
Indices:
- RCC: 3.90
- PCV: 0.360
Comment: Red cells, white cells and platelets within normal limits.
Mean Cell Volume (MCV) Assessment
| Parameter | Result | Reference Range | Units |
|---|---|---|---|
| HAEMOGLOBIN | 124 | (115 - 155) | g/L |
| MCV | 92 | (82 - 98) | fL |
| RDW | 13 | (< 16) | % |
| MCHC | 343 | (320 - 360) | g/L |
| PLATELETS | 219 | (150 - 400) | 9/L |
| WHITE CELLS | 7.9 | (4.0 - 11.0) | 9/L |
| Neutrophils (75%) | 5.9 | (1.8 - 7.5) | 9/L |
| Lymphocytes (18%) | 1.4 | (1.2 - 4.0) | 9/L |
| Monocytes (7%) | 0.6 | (0.1 - 1.2) | 9/L |
| Eosinophils (0%) | 0.0 | (< 0.7) | 9/L |
Comment: Red cells, white cells and platelets within normal limits. - Decreased total white cell count: Indicates bone marrow failure or suppression (e.g., medication-induced).
- ==Basophils↑==: Ulcerative colitis, certain malignancies
- ==Eosinophils↑==: Allergies, parasitic infections
- ==Monocytes↑==: Infection, leukemia, lymphoma
- ==Lymphocytes↑==: Viral infections
- ==Neutrophils↑==: Bacterial infections
- ==Differential Count==:
-
White Cell Count (Total): Elevated in infection, inflammation, and occasionally neoplastic processes.
-
Platelet Count: Increased in malignancy; decreased in sequestration. Essential to check prior to surgical procedures or when patients present with prolonged bleeding history.
-
Packed Cell Volume (Hematocrit): Percentage of total blood volume occupied by RBCs.
-
Red Cell Count: Decreased in hemorrhage, hemolysis, or decreased production. Increased physiologically (high altitude) or pathologically (malignancy).
-
Mean Cell Hemoglobin Concentration (MCHC): Average hemoglobin amount per RBC; used in anemia classification.
-
Red Cell Distribution Width (RDW): Indicates variation in RBC size (anisocytosis). Increased in iron and vitamin B deficiencies.
- Normocytic: Normal size
- Macrocytic: e.g., Vitamin B12 or folate deficiency
- Microcytic: e.g., Iron deficiency anemia
-
MCV (Mean Cell Volume): The average volume/size of red blood cells (RBCs). Critical for classifying anemias. (Normocytic, macrocytic or microcytic)
-
Hemoglobin: Reduced levels indicate anemia, which is associated with intraoral manifestations including oral burning sensation, increased risk of oral candidosis, ulceration, and glossitis.
Coagulation Screen10
Components of a Coagulation Screen
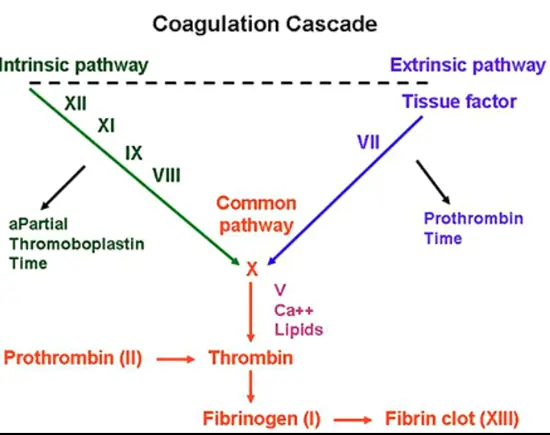
- APTT (Activated Partial Thromboplastin Time)
- PT (Prothrombin Time)
- Fibrinogen
- Thrombin time
- FBC (Full Blood Count)
- Platelet count
- Platelet function
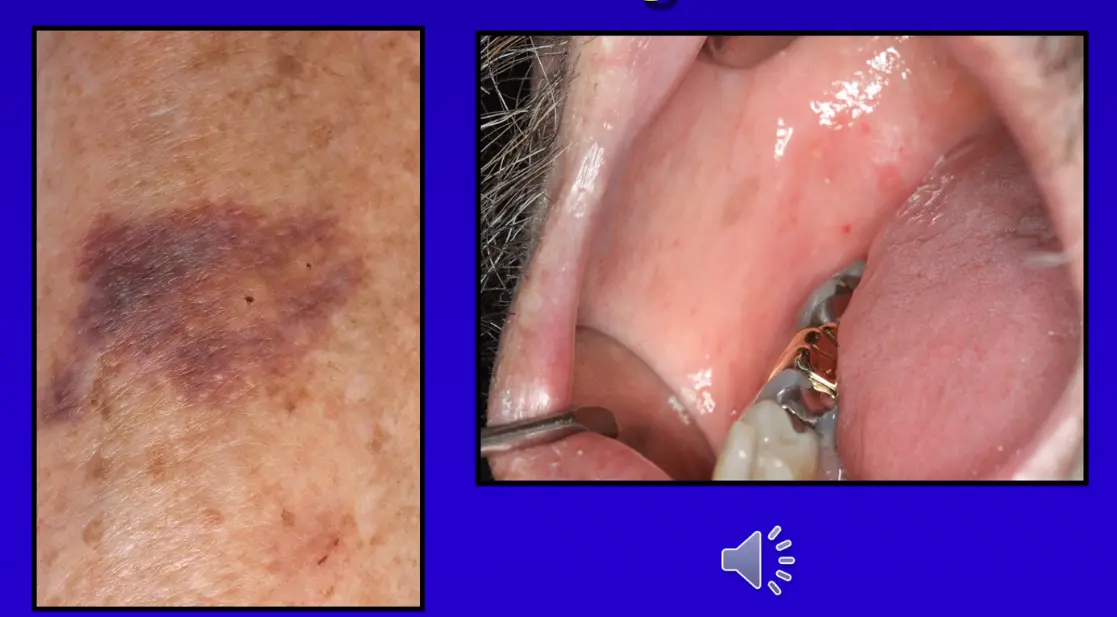
Case Study: Idiopathic Thrombocytopenic Purpura (ITP)
A middle-aged gentleman, previously treated successfully for oral cancer and undergoing routine mucosal surveillance, presented with extensive skin bruising and numerous oral petechiae. The patient was unaware of the bruising until examination. Laboratory investigations included a coagulation screen, full blood examination, platelet function test, and liver function test. Results revealed idiopathic thrombocytopenic purpura (ITP), a rare autoimmune disorder causing platelet destruction. The platelet count was critically low, requiring immediate emergency department admission.
Important
This should not be the only test ordered; a Full Blood Count (for platelet count) and platelet function tests must also be considered, as bleeding disorders may have multiple etiologies.
Iron Studies11
Cumulative Iron Studies
-
Ferritin: Intracellular storage protein; the most reliable measure of iron deficiency (low in deficiency).
-
Transferrin Saturation: Total iron binding capacity; decreased in deficiency.
-
Transferrin: Protein that binds and transports iron; elevated when iron demand increases (deficiency states).
-
Serum Iron: Decreased in deficiency; increased in overload states (hemosiderosis, hemochromatosis).
-
B12 deficiency can cause lesions, as can folate
Clinical Presentation
Intraoral examination reveals an erythematous, slightly raised lesion on the buccal mucosa adjacent to teeth with dental restorations.
Case Study: Vitamin B12 Deficiency Mimicking Oral Lichen Planus
A patient presented with oral mucosal lesions clinically identical to oral lichen planus. Laboratory investigation revealed vitamin B12 deficiency as the underlying cause. Notably, folate deficiency can produce similar clinical presentations.
Vitamin B12 and Folate
Deficiencies in these vitamins are associated with oral burning sensations, candidosis, and mucosal ulceration.
Glucose Tolerance Test12
Case Study: Recurrent Oral Candidosis and Poor Glycemic Control
A patient presented with recurrent oral candidosis (white mucosal lesions). Although claiming to be a well-controlled non-diabetic (actually diabetic), HbA1c testing revealed very poor glycemic control. Following improvement in diabetes management, the oral candidosis resolved.
Glycated Hemoglobin (HbA1c)
Indicates glycemic control over the preceding three months. Based on the principle of non-enzymatic glycosylation (glucose chemically attaching to proteins), the degree of glycosylation is directly proportional to blood glucose levels
- Ordered when impaired glucose tolerance or diabetes is suspected. This test requires significant patient commitment:
- Duration: 2 hours
- Procedure: Patient presents fasted; fasting blood glucose measured; sugary drink administered; blood drawn at 1-hour and 2-hour intervals.
- Patient Education: Essential to explain the time requirement so patients can plan accordingly.
Electrolytes And Renal Function13
Cumulative Electrolytes (Serum) are important:
- include:
- Sodium
- Potassium
- Chloride
- HCO3
Renal Function:
- eGFR: > 90 mL/min/1.73m²
- Calculation method: CKD-EPI (as per Med J Aust 2012 guidelines).
- Urea
- Creatinine
- HCO3
Liver Function Tests
Commonly ordered for suspected liver impairment (history of hepatitis, alcohol abuse) or before prescribing hepatotoxic medications.
Parameters:
- Bilirubin: Hemoglobin breakdown product; increased in liver disease.
- Alkaline Phosphatase (ALP): Enzyme from liver, biliary tract, and bone; elevated in liver disease.
- Gamma-Glutamyltransferase (GGT): Enzyme involved in amino acid/peptide transfer; elevated in liver disease.
- Alanine Aminotransferase (ALT): Enzyme in amino acid metabolism; elevated in liver disease.
- Albumin: Protein maintaining plasma colloid osmotic pressure; decreased in liver disease, malnutrition, overhydration, and protein-losing disorders (e.g., kidney disease).
Calcium, Phosphate, And Alkaline Phosphatase
Bone Markers
-
Ca (Calcium)
-
Phosphate
-
Alkaline phosphatase
-
Collectively useful for diagnosing metabolic bone disorders such as Paget's disease.
Serology14
Viral and Immune Status
- Serology
Biopsy15161718
Clinical Indications for Biopsy
Clinical Indications19
- Lesions that have neoplastic or pre-malignant features
- Lesions that are enlarging
- Confirmation of Clinical Diagnosis==: Even when clinical diagnosis seems certain, histopathological confirmation is required for serious conditions.
- Persistent Lesions Not Responding to Treatment: For example, in biopsy-proven oral lichen planus where all lesions resolve with corticosteroids except one persistent ulcer; biopsy required to exclude early SCC developing at that site.
- Persistent Lesions of Uncertain Etiology: Any lesion persisting for weeks/months without clear cause requires biopsy to ascertain precise nature.
- Neoplastic and Potentially Malignant Disorders: Diagnosis of oral squamous cell carcinoma (SCC) or oral potentially malignant disorders must be based on histopathology, not clinical impression alone.
Skin Testing (Patch Testing)
Used to detect delayed hypersensitivity (Type IV) contact allergies. Particularly valuable for diagnosing or excluding contact lichenoid lesions. This topic will be covered in detail when discussing Oral Lichen Planus; it is mentioned here for completeness.
Serology
Refers to the diagnostic identification of antibodies in serum. Used extensively in diagnosing autoimmune diseases (detailed coverage in later lectures on autoimmune oral conditions).
Critical Principle
Whenever lesions are excised for functional or cosmetic reasons, regardless of clinical confidence, tissue must always be submitted for histopathological examination.
Case Study: Nerve Sheath Myxoma
A lady presented with a small tongue swelling clinically resembling a fibroepithelial polyp (a common benign lesion). Despite the benign clinical appearance, excised tissue was submitted for histopathology as per standard protocol. The lesion was diagnosed as a nerve sheath myxoma, a rare benign peripheral nerve sheath tumor. This case was subsequently published due to its rarity (fewer than a handful described in the oral cavity).

Case Study: Pigmented Lesion (Melanotic Macule)
A young lady presented with a recent-onset pigmented lesion on the left maxillary labial gingiva. While clinically appearing as a melanotic macule, biopsy was undertaken to confirm the diagnosis and exclude melanoma.

Case Study: Persistent Non-Healing Ulcer (Squamous Cell Carcinoma)
A patient presented with an 8-week history of a chronic non-healing ulcer affecting the right buccal mucosa, previously managed conservatively by the patient and dentist. Although clinically appearing as a chronic traumatic ulcer, biopsy was performed to exclude other pathologies. Histopathology revealed squamous cell carcinoma.

Clinical Presentation
Close-up examination of the tongue showing a small white bump on the dorsal surface.
Etiological Assessment And Monitoring20
Management Flowchart for Non-Pigmented Mucosal Lesions
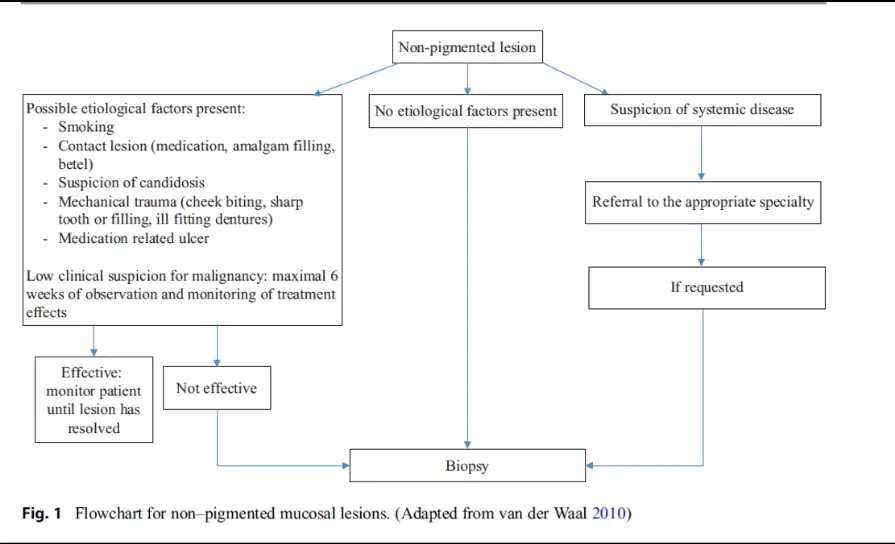
-
Identify Possible Etiological Factors:
- Smoking
- Contact lesions (medication, amalgam, betel)
- Suspicion of candidosis
- Mechanical trauma (cheek biting, sharp teeth/fillings, ill-fitting dentures)
- Medication-related ulcers
-
Low Clinical Suspicion for Malignancy:
- Observe and monitor treatment effects for a maximum of 6 weeks.
- If effective: Monitor until resolved.
- If not effective: Proceed to biopsy.
-
No Etiological Factors or Suspicion of Systemic Disease:
- Referral to appropriate specialty.
- Biopsy if requested.
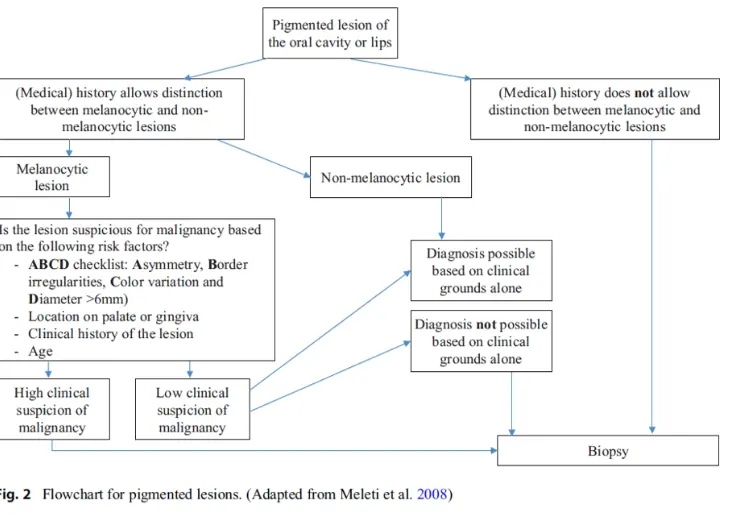 Pigmented Lesions:
Pigmented Lesions:
- Divide into melanocytic vs. non-melanocytic.
- If uncertain of nature: Always biopsy.
- Non-melanocytic: If clinically diagnosable (e.g., amalgam tattoo), biopsy may be avoided.
- Melanocytic: If low suspicion of malignancy and certain of clinical diagnosis, may monitor. If reasonable suspicion of malignancy or unusual presentation: Always biopsy.
Non-Pigmented Lesions:
- If etiological factors are identifiable and clinical suspicion for sinister pathology is low: Monitor short-term.
- If lesion resolves after cause elimination: No biopsy required.
- If lesion persists or has unknown cause, or represents suspected systemic manifestation: Biopsy indicated.
Pathology Request Form Requirements
Standard pathology request forms require the following data points:
- Patient Information: Name, DOB, Sex, Address, Medicare/DVA details.
- Clinical Notes: Relevant history, fasting status, pregnancy, or diabetic status.
- Tests Requested: Specific investigations (e.g., Histopathology, SST, EDTA, Swabs).
- Hospital Status: Private vs. public patient status.
- Transfusion History: Pregnancy or transfusion in the last 3 months.
- Collection Certification: Signature of collector and time/date of draw.
Specimen Requirements21
-
Laboratory Selection: Know your preferred pathology laboratory and pathologist. Ensure appropriate referral pads are available.
-
Transport Medium:
- Routine histopathology: Formalin pots.
- Direct immunofluorescence (for chronic mucosal inflammatory disease): Requires specific transport medium and refrigeration of tissue.
-
Equipment: Ensure appropriate equipment not only for the procedure itself but also for managing potential complications (e.g., hemorrhage control).
Tissue Selection Criteria
An appropriate biopsy must contain tissue that is:
- Representative of the most severe and significant change in the lesion.
- Suitable for pathologic assessment.
- Request Forms: Provide detailed clinical impression to assist the pathologist in reaching appropriate conclusions.
Procedure22
Surgical Considerations
- Site selection
- Local Anaesthesia (LA)
- Size of specimen
- Haemostasis
Additional Procedural Considerations:
- Anesthesia: Selection of local anesthetic, patient cooperation, and accessibility of the lesion.
- Tissue Size: Must be adequate; samples containing only epithelium without connective tissue yield nonspecific results.
- Hemostasis: Advance planning for bleeding control, including suturing requirements.
Site Selection (Critical)
A proper biopsy must contain tissue representative of the most severe and significant change in the lesion and be suitable for pathological assessment. Inappropriate sampling risks false-negative results or wrong diagnoses.
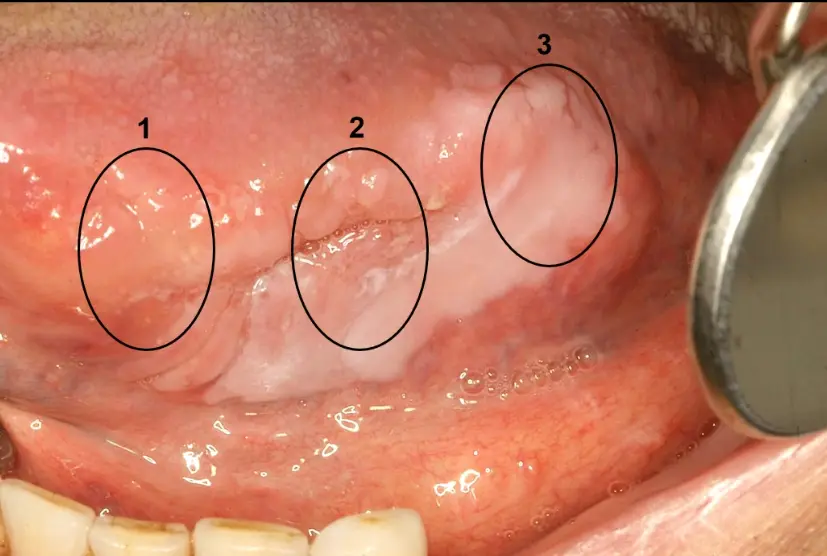
Case Study: Site Selection in Tongue Lesion (Squamous Cell Carcinoma)
A patient presented with a painful, 2-month duration lesion on the left lateral tongue. Three sites were evaluated:
- Site 1: Soft on palpation, minimal mucosal change (would yield benign results).
- Site 2: Correct site—indurated, ulcerated, included the white lesion (yielded diagnosis of oral squamous cell carcinoma).
- Site 3: Soft on palpation (would yield benign results).
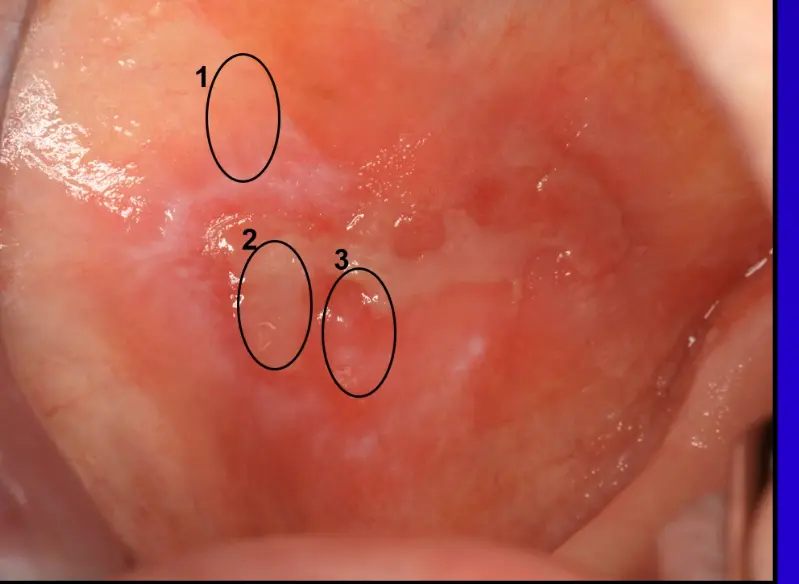
Case Study: Site Selection in Reticular Erythematous Lesion (Oral Lichen Planus)
A patient presented with a reticular erythematous, ulcerated lesion on the right buccal mucosa. Three potential biopsy sites were considered:
- Site 1: Predominantly normal tissue (would yield normal mucosa or mild nonspecific changes).
- Site 2: Center of ulcer only (would yield nonspecific inflammatory results).
- Site 3: Correct site—included both the ulcer and the surrounding reticular erythematous lesion, providing diagnostic features of oral lichen planus.
Histopathology Report23
Microbiological Investigations
Swab Collection and Analysis
Swab Collection24
- Culture and sensitivity
- PCR (Polymerase Chain Reaction)
Imaging25
- Determine or confirm bacterial, fungal, or viral infections.
- Guide antibiotic selection.
Imaging Modalities
- Radiography
- Computed axial tomography (CT)
- Bone scans
- Positron emission tomography (PET)
- Magnetic resonance imaging (MRI)
- Ultrasound scanning
Communication26
Patient Education and Results
Effective communication involves discussing diagnostic findings with the patient, often utilizing visual aids such as digital scans to explain the condition and treatment plan.
Competence in Ordering Investigations
Clinicians must never order investigations they do not thoroughly understand. Competence must extend through the entire investigative process:
- ==Interpretation: Ability to read and understand laboratory and pathology reports.==
- ==Patient Discussion: Clearly conveying implications of results to patients.==
- ==Follow-up Management: Knowing how to arrange appropriate follow-up for abnormal findings (e.g., abnormal blood results, diagnosis of oral squamous cell carcinoma).==
- ==Crisis Management: Knowing how to manage patient care upon receiving serious diagnoses.==
Resources27
Pathology and Laboratory Manuals
- The Royal College of Pathologists of Australasia (RCPA)
The RCPA Manual provides comprehensive guidance on pathology tests and interpretations.
Access the manual here: https://www.rcpa.edu.au/Manuals/RCPA-Manual- A comprehensive resource providing detailed information on various pathology and blood tests, including interpretation guidelines and clinical applicability. This resource is invaluable for understanding specific investigations and their appropriate application in clinical practice.
Footnotes
-
Original PDF page 1: L3 Investigations slides, p.1 ↩
-
Original PDF page 2: L3 Investigations slides, p.2 ↩
-
Original PDF page 3: L3 Investigations slides, p.3 ↩
-
Original PDF page 5: L3 Investigations slides, p.5 ↩
-
Original PDF page 8: L3 Investigations slides, p.8 ↩
-
Original PDF page 10: L3 Investigations slides, p.10 ↩
-
Original PDF page 12: L3 Investigations slides, p.12 ↩
-
Original PDF page 4: L3 Investigations slides, p.4 ↩
-
Original PDF page 6: L3 Investigations slides, p.6 ↩
-
Original PDF page 7: L3 Investigations slides, p.7 ↩
-
Original PDF page 9: L3 Investigations slides, p.9 ↩
-
Original PDF page 11: L3 Investigations slides, p.11 ↩
-
Original PDF page 13: L3 Investigations slides, p.13 ↩
-
Original PDF page 14: L3 Investigations slides, p.14 ↩
-
Original PDF page 16: L3 Investigations slides, p.16 ↩
-
Original PDF page 18: L3 Investigations slides, p.18 ↩
-
Original PDF page 19: L3 Investigations slides, p.19 ↩
-
Original PDF page 21: L3 Investigations slides, p.21 ↩
-
Original PDF page 15: L3 Investigations slides, p.15 ↩
-
Original PDF page 17: L3 Investigations slides, p.17 ↩
-
Original PDF page 20: L3 Investigations slides, p.20 ↩
-
Original PDF page 22: L3 Investigations slides, p.22 ↩
-
Original PDF page 23: L3 Investigations slides, p.23 ↩
-
Original PDF page 24: L3 Investigations slides, p.24 ↩
-
Original PDF page 25: L3 Investigations slides, p.25 ↩
-
Original PDF page 26: L3 Investigations slides, p.26 ↩
-
Original PDF page 27: L3 Investigations slides, p.27 ↩