Botulinum Toxin for Orofacial Pain1
Dr Lasanthini Weerakkody
Oral Medicine Specialist
Table of Contents2
- Overview
- Mechanism of action
- BoNT Preparations
- Indications
- Practical applications & protocols
- Adverse effects
- Complications
- Contraindications
Overview of Botulinum Toxin
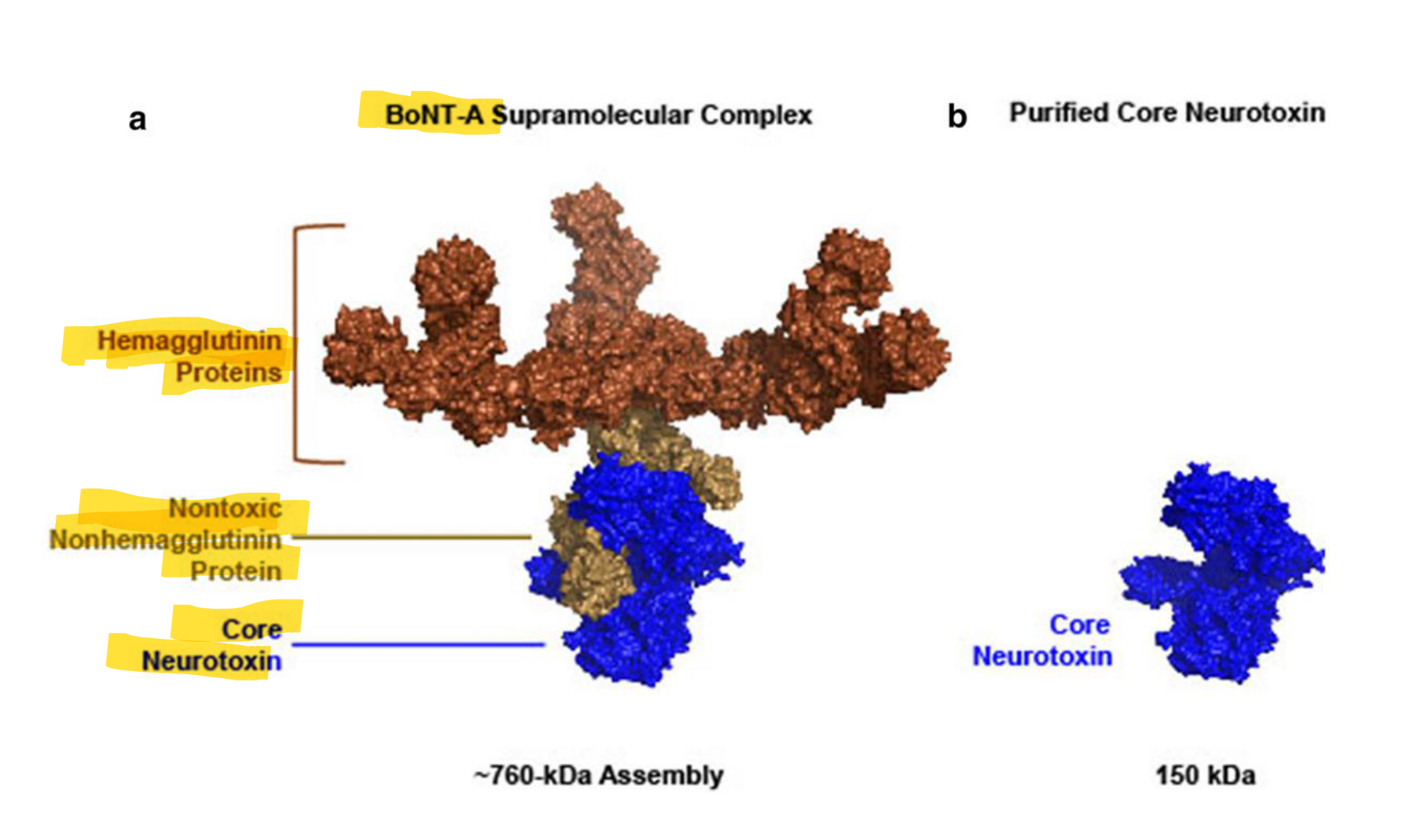
Structural Composition of Botulinum Toxin (BoNT)3
BoNT-A Supramolecular Complex (~760-kDa Assembly)
- Core Neurotoxin (150 kDa): The active component
- The core neurotoxin consists of two polypeptide chains: a heavy chain and a light chain.
- The protein is stable in acid but decomposes to yield the 150 kDa neurotoxin in a physiological state.
- Nontoxic Proteins (Complexing Proteins):
- Hemagglutinin (HA) Proteins
- Nonhemagglutinin (NHA) Protein
Bacterial Origin
==Botulinum toxin is a neurotoxin produced by the anaerobic rod-shaped bacterium Clostridium botulinum.==
 | 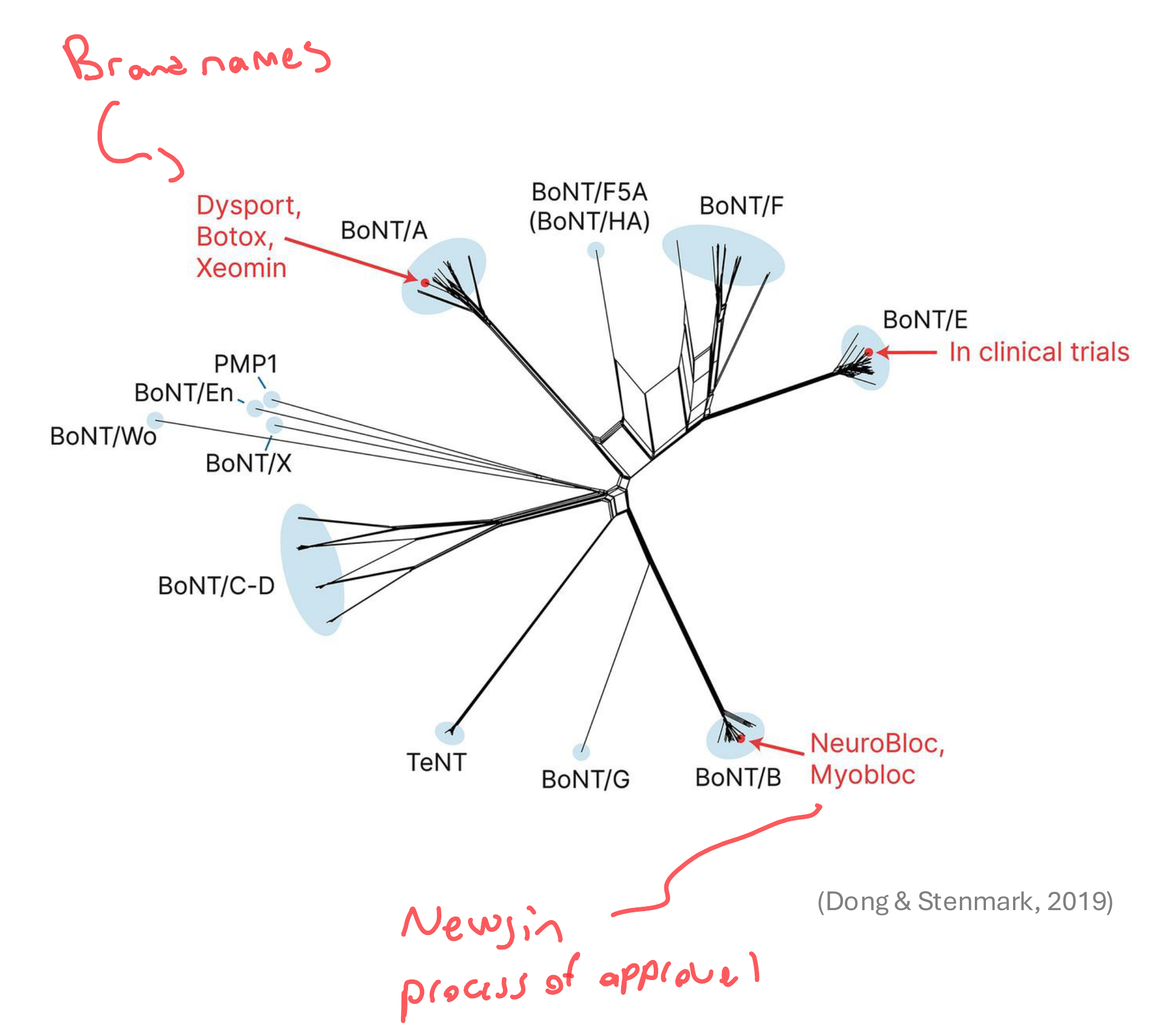 |
Classification and Commercial Brands
- BoNT/A: Botox, Dysport, Xeomin
- BoNT/B: NeuroBloc, Myobloc
Regulatory Approval
These agents are approved by the FDA and TGA for various medical and cosmetic uses.
- BoNT/E: Currently under clinical trials.
- Other Serotypes (Clinical Trials/Research): BoNT/F, BoNT/E, BoNT/F5A, BoNT/HA, PMP1, BoNT/En, BoNT/Wo, BoNT/X, BoNT/C-D, TeNT, BoNT/G, Newjin
Mechanism of Action4
 |  |
 |
Physiological Pathway5
- Normal Motor Neuron Function: Acetylcholine (ACh) release leads to muscle contraction.
- By preventing acetylcholine release, the toxin limits the firing of the postsynaptic nerve, thereby reducing muscle contraction and glandular secretion.
- Pain Transmission: ACh and other neurotransmitters (Substance P, CGRP, Glutamate) contribute to pain signaling and central/peripheral sensitization.
 | 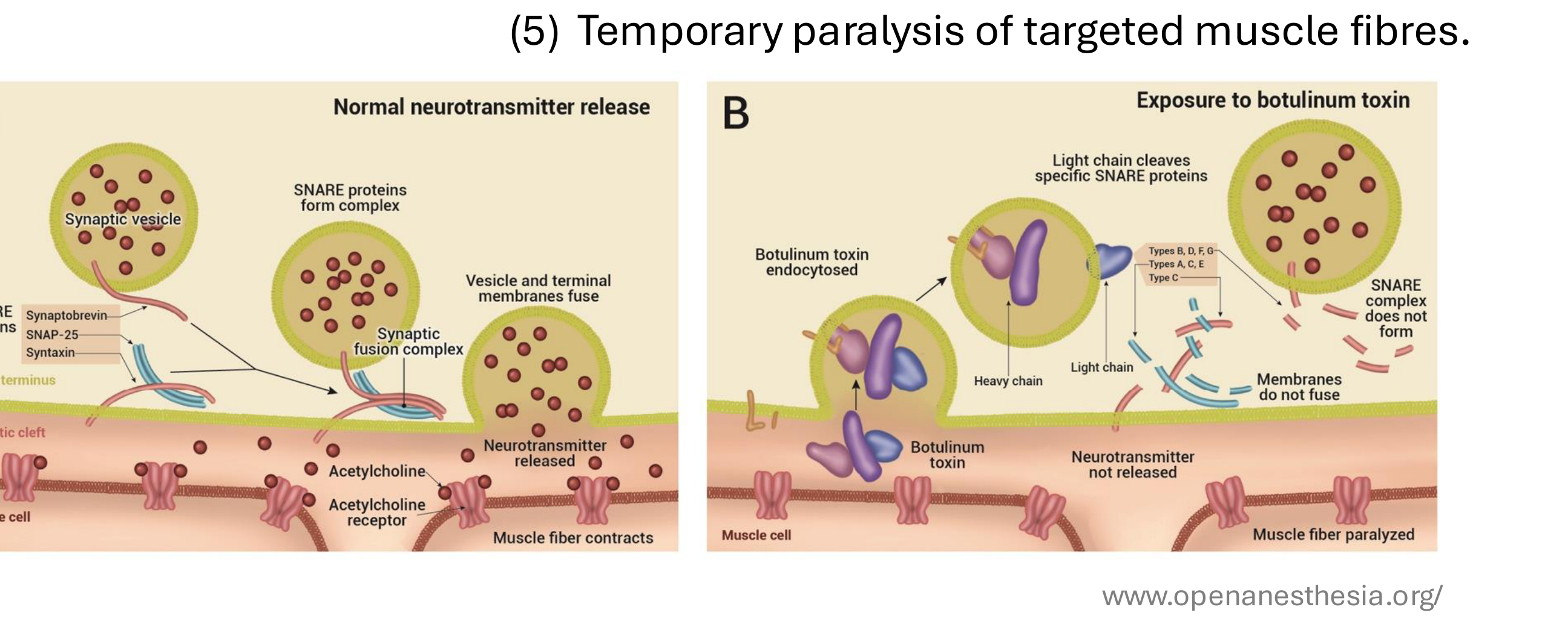 |
Cellular Mechanism of Action
- Binding: The toxin binds to specific receptors on the presynaptic surface of cholinergic neurons.
- Endocytosis: Botulinum toxin is taken up by the nerve terminus
- Separation: It separates into its heavy and light polypeptide chains.
- Cleavage: The light chain of the toxin is released and cleaves specific SNARE proteins.
- Types A, C, E: Cleave SNAP-25.
- Types B, D, F, G: Cleave Synaptobrevin.
- Type C: Cleaves Syntaxin.
- Inhibition: The SNARE complex fails to form, preventing the fusion of synaptic vesicles with the terminal membrane.
- Inhibition: The SNARE complex fails to form, preventing the fusion of synaptic vesicles with the terminal membrane
- Effect: Exocytosis of ACh into the synaptic cleft is blocked, resulting in temporary localized muscle relaxation (typically lasting ~3 months)..
- Effect: Exocytosis of ACh into the synaptic cleft is blocked, resulting in temporary paralysis of targeted muscle fibers (typically lasting
Analgesic Mechanism
Beyond motor neurons, BoNT may act on sensory nerves and nociceptors. It is suggested to inhibit the release of pain-mediating neurotransmitters such as Substance P, glutamate, and CGRP. ~3
Info
Over time, the nerve terminal regenerates SNARE proteins and forms new synaptic contacts, restoring muscle function. months).
Botulinum Toxin Preparations and Excipients
Composition of BoNT Preparations6
- Neurotoxin Core: Consists of a Light Chain and a Heavy Chain.
- Complexing Proteins (NAPs): Includes Hemagglutinin (HA) and Non-Hemagglutinin (NHA) proteins.
- Excipients: Added substances for stability and formulation.
- Human serum albumin, sodium chloride, lactose, or sucrose are added to prevent product inactivation during storage.

Therapeutic Formulations and Brands
Classification of Therapeutic Preparations7
- BoNT/A + NAPs (Neurotoxin Associated Proteins):
- Botox®
- Dysport®
- Isolated BoNT/A (Pure Neurotoxin):
- Xeomin® - Xeomin is derived from the same strain as Botox but undergoes further purification to remove NAPs.
- BoNT/B + NAPs:
- Myobloc®
 |  |
TGA Registered Agents in Australia8
There are currently three botulinum toxin agents with TGA registration. They are not bioequivalent or dose equivalent.
-
BOTOX® (Onabotulinumtoxin A)
- Manufacturer: Allergan, Irvine, CA, USA
- Formulation: Powder for injection
-
DYSPORT® (Abobotulinumtoxin A)
- Manufacturer: Ipsen-Pharma, Berkshire, UK
- Formulation: Clostridium botulinum type A toxin - haemagglutinin complex; powder for injection vial
-
XEOMIN® (Incobotulinumtoxin A)
- Manufacturer: Merz Pharma, Frankfurt am Main, Germany
- Formulation: Powder for solution for injection
Potency and Conversion Factors
Potency Measurement9
- Biologic activity is measured in Mouse Units (MU).
Mouse Units (MU)
One unit is defined as the amount of toxin required to cause death in 50% of a group of mice. Because manufacturers use different testing methods, units are not directly interchangeable between brands.
- Units are proprietary to each brand.
Clinical Conversion Ratios
Based on movement disorder studies, the following ratios are often utilized in clinical practice:
- OnabotulinumtoxinA : IncobotulinumtoxinA = 1:1
- OnabotulinumtoxinA : AbobotulinumtoxinA = 1:2.5
- OnabotulinumtoxinA : RimabotulinumtoxinB = 1:50
Note: While the 1:1 ratio for ONA and INCO is widely accepted, conversion factors for other preparations remain controversial.
Clinical Administration and Protocols
Preparation and Dilution10
- Vials are typically diluted with 0.5–5 mL of saline prior to injection.
- Most BoNT-A preparations are freeze-dried or vacuum-dried powders requiring reconstitution with sterile saline, whereas Myobloc (Type B) is available as a ready-to-use solution.
- Higher dilution increases the spread of the toxin.
- Most require specific temperature regimens, though Xeomin can be stored at room temperature.

Factors Influencing Administration
- Condition being treated
- Size of the target muscle
- Risk of toxin spread beyond the target muscle
- Response to previous injection courses
Localization Techniques
Methods used to determine and confirm the injection site include:
- Palpation and anatomical landmarks
- Electrical stimulation
- Electromyography (EMG)
- Ultrasound
- Combination of the above methods
- A 30-gauge needle is typically used for injection.
First-Line Therapy
BoNT is considered first-line therapy for head and neck movement disorders.
Clinical Indications for Orofacial Pain11

Applications in Orofacial Pain and Dysfunction12
- Head and Neck Movement Disorders
- Temporomandibular Disorders (TMD)
- Neuropathic Orofacial Pain (OFP)
- Headache Disorders
- Other Conditions:
- Facial paralysis
- Sialorrhea
- Head and neck cancer complications

Oromandibular Dystonia
Injection Sites and Approaches13
- Masseter and Temporalis Muscles: Standard injection sites for dystonia management.
- Masseter: Injected at three points. Care must be taken to avoid the parotid gland.
- Temporalis: Usually injected at three sites simultaneously with the masseter.
- Medial Pterygoid Muscle: Can be accessed via intraoral or extraoral approaches. - Intraoral: Palpated in relation to the occlusal plane (EMG recommended). - Extraoral: Needle inserted 10mm anterior to the mandibular angle.
- Lateral Pterygoid Muscle: Can be accessed via intraoral or extraoral approaches. - Intraoral: Entry at the mucobuccal fold near the upper second molar. - Extraoral: Needle inserted through the mandibular notch below the zygomatic arch.

Temporomandibular Disorders14
Muscular Temporomandibular Disorders
Efficacy in Muscular TMD
Recent systematic reviews (Li et al., 2024) indicate that BTX-A:
- Reduces pain intensity.
- Improves range of movement.
- Decreases masseter muscle intensity (μV) and occlusal force (kg).
- Optimal Dosage: A bilateral dose of 60–100 U is suggested, though no universal consensus exists.
Clinical Considerations and Limitations
- Conservative Management: Evidence suggests BTX can improve outcomes in patients who have failed at least three months of appropriate conservative management.
- Evidence Quality: Some reviews (Thambar et al., 2020) note moderate to high bias in existing studies, leading to a lack of clear consensus on therapeutic benefits.
- Mechanism: Provides both muscle relaxation and analgesic effects.
Articular Temporomandibular Disorders
Refractory TMD and Disk Dislocation
- IncobotulinumtoxinA Treatment:
- Protocol: 20 U into each masseter and 20 U into each lateral pterygoid muscle.
- Guidance: EMG or ultrasound-guided.
- Outcomes: Reduction in pain and maximum unassisted mouth opening.
Habitual TMJ Dislocation
- BTX-A Treatment:
- Protocol: 20–25 U injected into the lateral pterygoid muscle following manual reduction.
- Outcomes: Studies have shown no recurrences in treated patients. - Follow-up: Studies reporting no recurrence for up to two years.
Ultrasound-Guided Injection Technique
- Target: Lateral Pterygoid muscle.
- Anatomical Landmarks: Parotid gland, Condyle process, Coronoid process.
- Vascular Considerations: Color Doppler imaging is used to identify the maxillary artery to ensure safe needle trajectory and positioning.
Bruxism and Clenching
Clinical Outcomes in Bruxism15
Research into BTX for bruxism has yielded controversial results across various RCTs and systematic reviews.
Reported Positive Effects:
- Reduction in bruxism events and clenching force.
- Decreased intensity of muscle contractions.
- Reduction in pain severity.
- Increase in maximum mouth opening (MMO).
Limitations and Mixed Findings:
- Effects are transient, typically lasting 3–4 months, requiring ongoing management.
- Some studies show no significant improvement in range of motion or occlusal force compared to placebo.
- Long-term cost-benefit ratio remains a concern.
Evidence Summary for TMD and Bruxism16
A review of 24 RCTs (Delcanho et al., 2022) highlighted the following:
- Masseter Hypertrophy: Sufficient evidence for use.
- Masticatory Myofascial Pain: Equivocal evidence; not necessarily superior to less invasive, less expensive conservative treatments.
- Bruxism: Inconclusive research; insufficient evidence to support routine use.
- TMJ Articular Disorders: Insufficient evidence for effectiveness.
Administration Variability
- Target Muscles: Most commonly masseter and temporalis together; occasionally masseter or lateral pterygoid alone.
- Guidance: Palpation is most common, followed by EMG and Ultrasound.
- Dosing: Significant variability exists in the units injected per muscle.
Neuropathic Orofacial Pain17
Neuropathic OFP
Trigeminal Neuralgia
Efficacy in Classical Trigeminal Neuralgia (TN)
- Third-Division TN: Injected submucosally or subcutaneously into trigger zones.
- Second-Division TN: Injected into the sphenopalatine ganglion.
- V2 Injections: Sometimes made into the sphenopalatine ganglion using CAD-CAM needle guides.
- Dosing and Outcomes:
- Average dose: 43 U.
- Mean pain improvement reported between 83% and 91%.
- Conclusion: BTX-A is considered a highly effective and safe treatment for TN, myofascial TMD, and Oromandibular Dystonia (OMD).
Systematic Review Findings
A review of 6 RCTs covering TN and post-herpetic neuralgia found:
- Site Selection: Based on subjective pain perception and tactile allodynia.
- Dosing Variability: 25 U to 140 U across 8 to 25 injection sites.
- Clinical Benefits:
- Significant reduction in pain intensity compared to placebo and lidocaine.
- Improvement in Quality of Life (QoL).
- Adjunct Therapy: Weak evidence suggests further pain reduction when used alongside anti-epileptic drugs.
- Protocol: No common or recommended protocol has been identified yet.
Persistent Idiopathic Dentoalveolar Pain
Persistent Idiopathic Dentoalveolar Pain (PIDAP)
- Evidence Level: Currently insufficient to fully evaluate pain-relieving effects, though it appears to be a safe management option.
- Reported Outcomes: Pain reduction of 50–72% in some cases.
- Dosing: 10–30 U across 3–12 sites over 1–10 sessions.
Post-Traumatic Trigeminal Neuropathic Pain (PTTNP)
- Administration: 3–35 units injected subcutaneously or submucosally into affected regions (e.g., buccal vestibule, gingiva, hard palate).
- Status: Potential treatment modality for refractory cases; large-scale RCTs are required.
Burning Mouth Syndrome
Clinical Data for Burning Mouth Syndrome18
- Evidence: Scarce; only one placebo-controlled trial exists.
- Dosing: Ranges from 50 U to 100 U.
- Injection Sites: Masticatory muscles, tongue, and lips.
- Onset and Duration: Effects start between 48 hours and 3 weeks, lasting up to 20 weeks.
- Conclusion: Efficacy cannot be definitively drawn due to limited data.
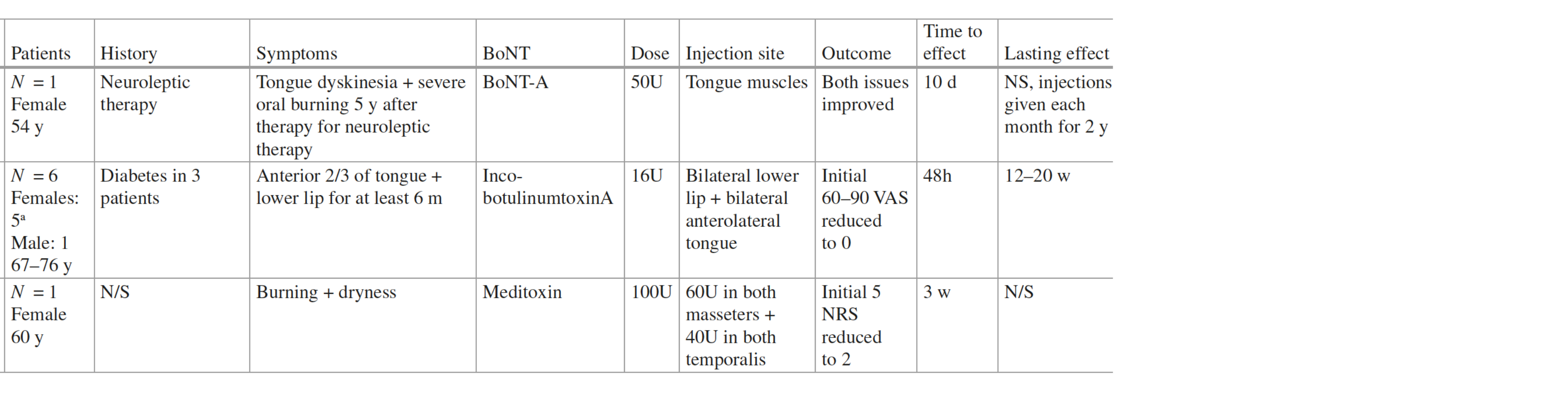
Case Study Summaries19
- Tongue Dyskinesia/Burning: 50 U BoNT-A injected into tongue muscles; improved both issues (Seo et al. 2009).
- Anterior Tongue/Lower Lip Burning: 16 U IncobotulinumtoxinA injected into bilateral lower lip and anterolateral tongue; VAS reduced from 60–90 to 0 (Restivo et al. 2017).
- Burning and Dryness: 100 U (60 U masseters, 40 U temporalis); NRS reduced from 5 to 2 (Kwon and Park 2020).
Chronic Migraine Prophylaxis
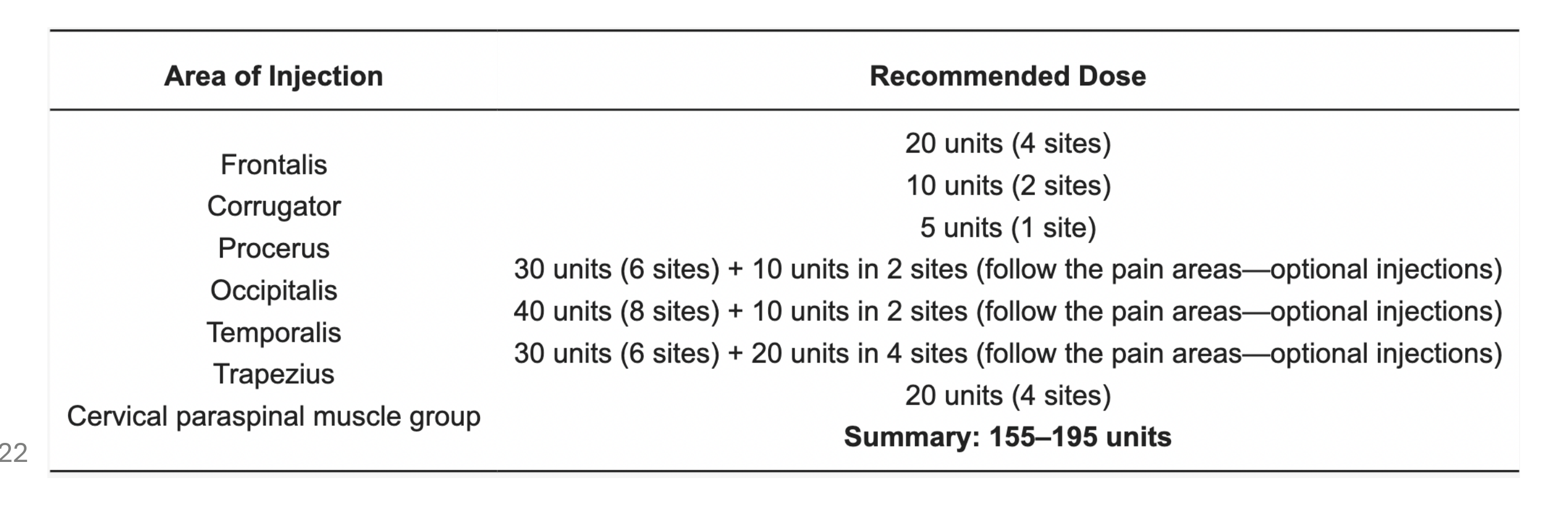
PREEMPT Protocol for Chronic Migraine20
Phase III studies established that OnabotulinumtoxinA (ONA-BoNTA) is safe and effective for prophylactic treatment.
Dosing Summary: 155–195 units across 31 injection sites.
Injection Areas and Recommended Doses:
- Frontalis: 20 units (4 sites)
- Corrugator: 10 units (2 sites)
- Procerus: 5 units (1 site)
- Occipitalis: 30–40 units (6–8 sites)
- Temporalis: 40–50 units (8–10 sites)
- Trapezius: 30–50 units (6–10 sites)
- Cervical Paraspinal Group: 20 units (4 sites)
FDA Approval and Frequency
Approved by the FDA in 2010 based on the PREEMPT 1 and 2 trials. The protocol is recommended at least three times over 12 months.
Summary of Efficacy and Injection Sites
Efficacy and Injection Site Matrix21
| Orofacial Pain Type | Efficacy Summary | Clinical Notes | Injection Sites |
|---|---|---|---|
| Trigeminal Neuralgia | Viable addition to treatment options. | Used when standard meds fail; one-time injection advantage. | Trigger areas (gums), intradermal/submucosal. |
| Post-Traumatic Neuropathy | Limited evidence; small trials/case reports. | Some benefit in peripheral neuropathic pain. | Near affected peripheral nerve (e.g., mental foramen). |
| Myofascial Pain (TMD) | Conflicting data; moderate to low certainty. | Benefit in refractory cases; similar to anesthetics. | Masseter, temporalis, medial pterygoid. |
| Facial Migraine | Key prophylactic therapy for chronic migraine. | Supported by trigeminovascular mechanisms. | Forehead, scalp, or subdermal facial areas. |
Evidence Levels and Protocols
- Trigeminal Neuralgia/Neuropathic Pain: Limited but showing efficacy in studies.
- TMD: Limited; effective for muscular/myofascial subtypes but not necessarily superior to conservative treatment.
- Migraine: Established safety and efficacy via PREEMPT protocol.

Safety and Contraindications
Adverse Effects
Common Side Effects22
Adverse effects are usually mild, transient, and occur 1–2 weeks post-injection.
- Localized pain, tenderness, or bruising.
- Hemorrhage at the injection site.
- Hyperesthesia.
- Localized muscle weakness, transient facial weakness, or asymmetry.
- Headache and flu-like symptoms.
Immune Response
Flu-like symptoms following injection are typically an immune response to the toxin.
Complications and Long Term Risks
Functional and Systemic Complications23
- Transient Impairments: Dysphagia, nasal speech, painful chewing, nasal regurgitation, and dysarthria (typically subside within 2–4 weeks).
- Rare Reactions: Skin rash, pruritus, and allergic reactions.
- Overdose (Botulism symptoms): Ptosis, diplopia, respiratory failure, and generalized weakness.
- Inadvertent spread of the toxin can be the underlying cause of functional complications like dysphagia or nasal speech.
Long-Term Risks
- Mandibular Bone Loss: Preclinical studies show persistent bone loss at the TMJ and mandible due to muscle underloading; correlation with human dosage is still being studied.
- Human studies, in addition to animal studies, suggest potential mandibular or TMJ bone loss due to muscle paralysis.
- Immunogenicity: Development of neutralizing antibodies can lead to loss of treatment effect.
- Risk Factors: Higher doses, short intervals (< 3 months), and long-term use (> 10 years).
Contraindications and Drug Interactions24
Absolute and Relative Contraindications25
- Hypersensitivity to the active substance or any ingredients (e.g., albumin).
- Infection or inflammation at the proposed injection site.
- Generalized disorders of muscle activity (e.g., Myasthenia Gravis, Lambert-Eaton Syndrome).
- Pregnancy and breastfeeding.
Drug Interactions and Safety Notes
-
Neuromuscular Transmission: Potential interactions with aminoglycosides or curare-like compounds.
-
Biological Risk: Toxin preparations contain albumin, carrying a theoretical risk for transmission of viral or prion diseases.
-
Treatment Failure: May be due to preparation errors, poor muscle selection, or insufficient dosage, in addition to antibody formation.
Thank You
References26272829
-
Sim WS. Application of botulinum toxin in pain management. The Korean journal of pain. 2011 Mar 31;24(1):1-6.
-
Carr WW, Jain N, Sublett JW. Immunogenicity of botulinum toxin formulations: potential therapeutic implications. Advances in therapy. 2021 Oct;38(10):5046-64.
-
Dong, M., Stenmark, P. (2019). The Structure and Classification of Botulinum Toxins. In: Whitcup, S.M., Hallett, M. (eds) Botulinum Toxin Therapy. Handbook of Experimental Pharmacology, vol 263. Springer, Cham. https://doi.org/10.1007/164_2019_342.
-
Kukreja R, Singh BR. The botulinum toxin as a therapeutic agent: molecular and pharmacological insights. Research and Reports in Biochemistry. 2015 Dec 8:173-83.
-
Therapeutic Goods Administration. Australian Public Assessment Report (AusPAR) for Xeomin [Internet]. Canberra: TGA; 2024. Available from: https://www.tga.gov.au
-
Therapeutic Goods Administration. Product Information: BOTOX® [Internet]. Canberra: TGA; 2024. Available from: https://www.tga.gov.au
-
Therapeutic Goods Administration. Product Information: DYSPORT [Internet]. Canberra: TGA; 2024. Available from: https://www.tga.gov.au
-
Yoshida K. Botulinum toxin therapy for oromandibular dystonia and other movement disorders in the stomatognathic system. Toxins. 2022 Apr 14;14(4):282.
-
Anandan C, Jankovic J. Botulinum toxin in movement disorders: an update. Toxins. 2021 Jan 8;13(1):42.
-
Jankovic J. Botulinum toxin: State of the art. Movement Disorders. 2017 Aug;32(8):1131-8.
-
Dressler D, Altavista MC, Altenmueller E, Bhidayasiri R, Bohlega S, Chana P, Chung TM, Colosimo C, Fheodoroff K, Garcia-Ruiz PJ, Jeon B. Consensus guidelines for botulinum toxin therapy: general algorithms and dosing tables for dystonia and spasticity. Journal of Neural Transmission. 2021 Mar;128:321-35.
-
Scheinberg A. Clinical use of botulinum toxin. Aust Prescr 2009;32:39-42
-
Yoshida K, Kaji R. Treatment with OnabotulinumtoxinA for Oromandibular Dystonia: A Systematic Review and Meta-Analysis. Toxins. 2024 Dec 16;16(12):546.
-
Okeson JP. Management of temporomandibular disorders and occlusion. 8th ed. St. Louis: Elsevier; 2019.
-
Tambasco N, Filidei M, Nigro P, Parnetti L, Simoni S. Botulinum toxin for the treatment of hemifacial spasm: an update on clinical studies. Toxins. 2021 Dec 9;13(12):881.
-
Wang B, Wei X, Qi H, Bao X, Hu M, Ma J. Efficacy and safety of botulinum neurotoxin in the treatment of hemifacial spasms: a systematic review and meta-analysis. BMC neurology. 2024 Oct 29;24(1):420.
-
Li K, Tan K, Yacovelli A, Bi WG. Effect of botulinum toxin type A on muscular temporomandibular disorder: A systematic review and meta‐analysis of randomized controlled trials. Journal of Oral Rehabilitation. 2024 May;51(5):886-97.
-
Thambar S, Kulkarni S, Armstrong S, Nikolarakos D. Botulinum toxin in the management of temporomandibular disorders: a systematic review. British Journal of Oral and Maxillofacial Surgery. 2020 Jun 1;58(5):508-19.
-
Ferreira EF, Camões-Barbosa A. IncobotulinumtoxinA in refractory temporomandibular disorder due to disk dislocation: a prospective study. Journal of Stomatology, Oral and Maxillofacial Surgery. 2024 Sep 1;125(5):101804.
-
Fu KY, Chen HM, Sun ZP, Zhang ZK, Ma XC. Long-term efficacy of botulinum toxin type A for the treatment of habitual dislocation of the temporomandibular joint. British Journal of Oral and Maxillofacial Surgery. 2010 Jun 1;48(4):281-4.
-
De la Torre Canales G, Câmara-Souza MB, Do Amaral CF, Garcia RC, Manfredini D. Is there enough evidence to use botulinum toxin injections for bruxism management? A systematic literature review. Clinical oral investigations. 2017 Apr;21:727-34.
-
Saini RS, Ali Abdullah Almoyad M, Binduhayyim RI, Quadri SA, Gurumurthy V, Bavabeedu SS, Kuruniyan MS, Naseef PP, Mosaddad SA, Heboyan A. The effectiveness of botulinum toxin for temporomandibular disorders: A systematic review and meta-analysis. PLoS One. 2024 Mar 14;19(3):e0300157.
-
Hosgor H, Altindis S. Efficacy of botulinum toxin in the management of temporomandibular myofascial pain and sleep bruxism. Journal of the Korean Association of Oral and Maxillofacial Surgeons. 2020 Oct 31;46(5):335-40.
-
Ågren M, Sahin C, Pettersson M. The effect of botulinum toxin injections on bruxism: A systematic review. Journal of oral rehabilitation. 2020 Mar;47(3):395-402.
-
Chen Y, Tsai CH, Bae TH, Huang CY, Chen C, Kang YN, Chiu WK. Effectiveness of botulinum toxin injection on bruxism: a systematic review and meta-analysis of randomized controlled trials. Aesthetic plastic surgery. 2023 Apr;47(2):775-90.
-
Patel J, Cardoso JA, Mehta S. A systematic review of botulinum toxin in the management of patients with temporomandibular disorders and bruxism. British dental journal. 2019 May;226(9):667-72.
-
Buzatu R, Luca MM, Castiglione L, Sinescu C. Efficacy and safety of botulinum toxin in the management of temporomandibular symptoms associated with sleep bruxism: a systematic review. Dentistry Journal. 2024 May 23;12(6):156.
-
Serrera-Figallo MA, Ruiz-de-Leon-Hernandez G, Torres-Lagares D, Castro-Araya A, Torres-Ferrerosa O, Hernandez-Pacheco E, Gutierrez-Perez JL. Use of botulinum toxin in orofacial clinical practice. Toxins. 2020 Feb 11;12(2):112.
-
Delcanho R, Val M, Nardini LG, Manfredini D. Botulinum toxin for treating temporomandibular disorders: what is the evidence?. Journal of oral & facial pain and headache. 2022 Jun 2;36(1):3023.
-
Yoshida K. Effects of botulinum toxin type A on pain among trigeminal neuralgia, myofascial temporomandibular disorders, and oromandibular dystonia. Toxins. 2021 Aug 29;13(9):605.
-
Jabbari B. Botulinum Toxin Treatment of Chronic Facial Pain: Trigeminal Neuralgia and Temporo-Mandibular Disorders. In Botulinum Toxin Treatment of Pain Disorders 2022 Jun 3 (pp. 191-213). Cham: Springer International Publishing.
-
Val M, Delcanho R, Ferrari M, Guarda Nardini L, Manfredini D. Is Botulinum Toxin Effective in Treating Orofacial Neuropathic Pain Disorders? A Systematic Review. Toxins. 2023 Sep 1;15(9):541.
-
Dawson A, Dawson J, Ernberg M. The effect of botulinum toxin A on patients with persistent idiopathic dentoalveolar pain—A systematic review. Journal of Oral Rehabilitation. 2020 Sep;47(9):1184-91.
-
Tan HL, Yakkaphan P, Beke A, Renton T. Onabotulinum toxin a treatment for posttraumatic trigeminal neuropathic pain: case series and literature review. Journal of Oral & Facial Pain and Headache. 2024 Mar 12;38(1):93.
-
Etemad-Moghadam S, Alaeddini M, Jabbari B. Botulinum Toxin in Dentistry and Treatment of Chronic Orofacial Pain. In Botulinum Toxin Treatment of Pain Disorders 2022 Jun 3 (pp. 311-357). Cham: Springer International Publishing.
-
Kecpczinska K, Domitrz I. Botulinum toxin—a current place in the treatment of chronic migraine and other primary headaches. Toxins. 2022 Sep 5;14(9):619.
-
Aurora SK, Dodick DW, Turkel CC, DeGryse RE, Silberstein SD, Lipton RB, Diener HC, Brin MF. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 1 trial. Cephalalgia. 2010 Jul;30(7):793-803.
-
Diener HC, Dodick DW, Aurora SK, Turkel CC, DeGryse RE, Lipton RB, Silberstein SD, Brin MF. OnabotulinumtoxinA for treatment of chronic migraine: results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia. 2010 Jul;30(7):804-14.
-
Farham F, Onan D, Martelletti P. Non-Migraine Head Pain and Botulinum Toxin. Toxins. 2024 Oct 9;16(10):431.
-
Dhanasekara CS, Payberah D, Chyu JY, Shen CL, Kahathuduwa CN. The effectiveness of botulinum toxin for chronic tension-type headache prophylaxis: A systematic review and meta-analysis. Cephalalgia. 2023 Mar;43(3):03331024221150231
-
Roland SB, Pripp AH, Msomphora MR, Kvarstein G. The efficacy of botulinum toxin A treatment for tension-type or cervicogenic headache: a systematic review and meta-analysis of randomized, placebo-controlled trials. Scandinavian journal of pain. 2021 Oct 1;21(4):635-52.
-
Jahromi AH, Konofaos P. Contralateral facial botulinum toxin injection in cases with acute facial paralysis may improve the functional recovery: where we stand and the future direction. World journal of plastic surgery. 2021 May;10(2):89.
-
de Jongh FW, Schaeffers AW, Kooreman ZE, Ingels KJ, van Heerbeek N, Beurskens C, Monstrey SJ, Pouwels S. Botulinum toxin A treatment in facial palsy synkinesis: a systematic review and meta-analysis. European archives of oto-rhino-laryngology. 2023 Apr;280(4):1581-92.
-
Weikamp JG, Schinagl DA, Verstappen CC, Schelhaas HJ, De Swart BJ, Kalf JG. Botulinum toxin‐A injections vs radiotherapy for drooling in ALS. Acta Neurologica Scandinavica. 2016 Sep;134(3):224-31.
-
Gonzalez-L MD, Martinez C, y Fortuny IB, Suso-Vergara S. Factors in the efficacy, safety, and impact on quality of life for treatment of drooling with botulinum toxin type A in patients with cerebral palsy. American Journal of Physical Medicine & Rehabilitation. 2017 Feb 1;96(2):68-76.
-
Narayanaswami P, Geisbush T, Tarulli A, Raynor E, Gautam S, Tarsy D, Gronseth G. Drooling in Parkinson’s disease: A randomized controlled trial of incobotulinum toxin A and meta-analysis of Botulinum toxins. Parkinsonism & related disorders. 2016 Sep 1;30:73-7.
-
Ruiz-Roca JA, Pons-Fuster E, Lopez-Jornet P. Effectiveness of the botulinum toxin for treating sialorrhea in patients with Parkinson’s disease: a systematic review. Journal of Clinical Medicine. 2019 Mar 6;8(3):317.
Footnotes
-
Original PDF page 1: L30 Botulinum toxin for orofacial pain, p.1 ↩
-
Original PDF page 2: L30 Botulinum toxin for orofacial pain, p.2 ↩
-
Original PDF page 3: L30 Botulinum toxin for orofacial pain, p.3 ↩
-
Original PDF page 5: L30 Botulinum toxin for orofacial pain, p.5 ↩
-
Original PDF page 4: L30 Botulinum toxin for orofacial pain, p.4 ↩
-
Original PDF page 6: L30 Botulinum toxin for orofacial pain, p.6 ↩
-
Original PDF page 7: L30 Botulinum toxin for orofacial pain, p.7 ↩
-
Original PDF page 8: L30 Botulinum toxin for orofacial pain, p.8 ↩
-
Original PDF page 9: L30 Botulinum toxin for orofacial pain, p.9 ↩
-
Original PDF page 10: L30 Botulinum toxin for orofacial pain, p.10 ↩
-
Original PDF page 12: L30 Botulinum toxin for orofacial pain, p.12 ↩
-
Original PDF page 11: L30 Botulinum toxin for orofacial pain, p.11 ↩
-
Original PDF page 13: L30 Botulinum toxin for orofacial pain, p.13 ↩
-
Original PDF page 14: L30 Botulinum toxin for orofacial pain, p.14 ↩
-
Original PDF page 18: L30 Botulinum toxin for orofacial pain, p.18 ↩
-
Original PDF page 19: L30 Botulinum toxin for orofacial pain, p.19 ↩
-
Original PDF page 20: L30 Botulinum toxin for orofacial pain, p.20 ↩
-
Original PDF page 24: L30 Botulinum toxin for orofacial pain, p.24 ↩
-
Original PDF page 25: L30 Botulinum toxin for orofacial pain, p.25 ↩
-
Original PDF page 26: L30 Botulinum toxin for orofacial pain, p.26 ↩
-
Original PDF page 27: L30 Botulinum toxin for orofacial pain, p.27 ↩
-
Original PDF page 28: L30 Botulinum toxin for orofacial pain, p.28 ↩
-
Original PDF page 29: L30 Botulinum toxin for orofacial pain, p.29 ↩
-
Original PDF page 31: L30 Botulinum toxin for orofacial pain, p.31 ↩
-
Original PDF page 30: L30 Botulinum toxin for orofacial pain, p.30 ↩
-
Original PDF page 32: L30 Botulinum toxin for orofacial pain, p.32 ↩
-
Original PDF page 33: L30 Botulinum toxin for orofacial pain, p.33 ↩
-
Original PDF page 34: L30 Botulinum toxin for orofacial pain, p.34 ↩
-
Original PDF page 35: L30 Botulinum toxin for orofacial pain, p.35 ↩