Occlusal Splint Therapy
The University of Western Australia
Affiliated Organizations1
- Perth Oral Medicine & Dental Sleep Centre
- Perth Childrens Hospital
- Perigold
- Oral Medicine Australia
- Dental Sleep Society Western Australia
- Australian Dental Association
- Australasian Dental Sleep Association
Transclude of image_url |
|
|
|
|
|
|
Presenter Information2
Ramesh Balasubramaniam OAM
Associate Professor, Oral Medicine
UWA Dental School
The University of Western Australia
Conflict of Interest Disclosure
Neither I nor my immediate family have any financial interests that would create a conflict of interest or restrict my independent judgment with regard to the content of this presentation.
Disclosure
The presenter has no financial interests to declare.
Presentation Agenda3
- Occlusal Splints Revisited
- Occlusal Splints Design Secrets
- Mechanisms of Action
- Scientific Evidence for Occlusal Splints
- Take Home Message
- Theory behind occlusal splints for Temporomandibular Disorders (TMD) and bruxism.
- Historical context and early concepts.
- Design variations and materials.
- Mechanisms of action (Facts vs. Fiction).
- Scientific evidence and clinical efficacy.
Occlusal Splints Revisited4
 |  |
Historical Context and Early Concepts
Pioneering Contributions of Dr. Norman William Kingsley5
Dr. Norman William Kingsley (1829 – 1913) of New York, USA, was a foundational figure in the development of dental appliances:
-
Kingsley was an apprentice who originally worked as a barber doubling as a dentist.
-
1866: First to utilize the “occipital appliance.”
-
1877: First to publish research regarding intraoral appliances for the Temporomandibular Joint (TMJ) in Dental Cosmos.
Source: The Glossary of Prosthodontic Terms: Ninth Edition. J Prosthet Dent. 2017 May;117(5S):e1-e105.
 |  |
Treatment Goals and Clinical Indications
Applications for TMD and Bruxism6
Occlusal splints are utilized to address temporomandibular disorders and bruxism, specifically targeting:
-
Splints are also used for managing sleep bruxism and headaches.
-
Related occlusal disharmonies
-
Related skeletal discrepancies
Primary Treatment Objectives
- Occlusal disengagement: Preventing adverse tooth contact.
- Restoring vertical dimension: Establishing proper interarch distance.
- TMJ repositioning: Aligning the joint structures.
- TMJ unloading: Reducing pressure and stress on the joint components.
Modern Objectives for Stabilization Splints
- Stabilizing the joint.
- Protecting teeth from sleep bruxism.
- Redistributing occlusal forces.
- Relaxing jaw muscles (short-term effect).
Source: Klasser GD, Greene CS. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009 Feb;107(2):212-23.
Occlusal Splints Design Secrets
Agenda7
- Occlusal Splints Revisited
- Occlusal Splints Design Secrets
- Mechanisms of Action
- Scientific Evidence for Occlusal Splints
- Take Home Message
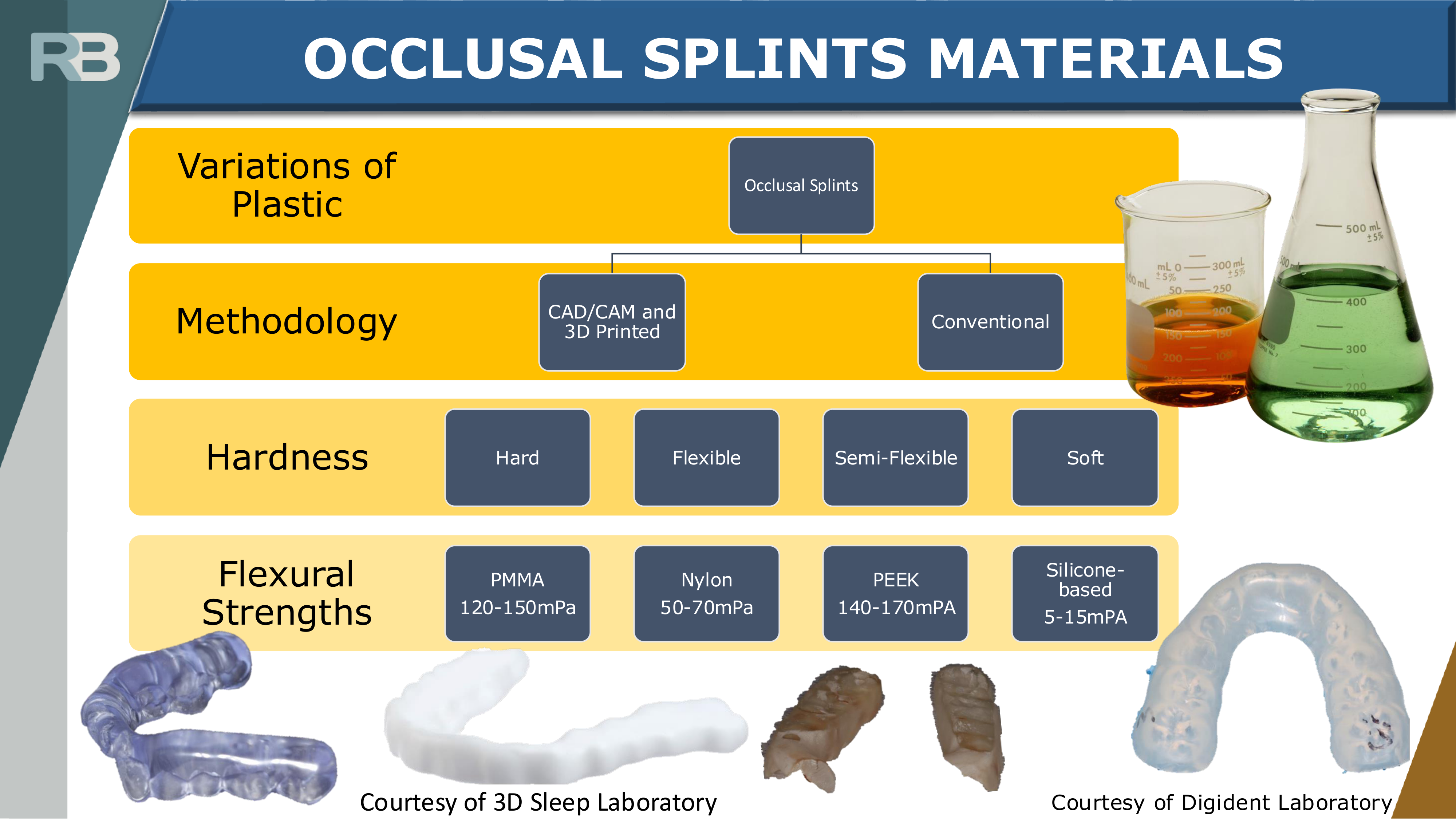
Materials and Manufacturing Methods
Material Classification and Properties8
Occlusal splints are categorized by manufacturing method (Conventional vs. CAD/CAM and 3D Printed) and material hardness.
- Hard (PMMA)
- Flexural Strength: 120-150 mPa
- Semi-Flexible (PEEK)
- Flexural Strength: 140-170 mPa
- Flexible (Nylon)
- Flexural Strength: 50-70 mPa
- Soft (Silicone-based)
- Flexural Strength: 5-15 mPa
Flat Plane Stabilisation Splints
Design and Clinical Application9
- Arch Placement: Maxillary or mandibular arch; designed to uniformly occlude with opposing dentition.
- Guidance: Research indicates no difference in TMD symptom reduction between designs with canine guidance versus those without canine guidance.
- Commonly known as the "Michigan splint" (maxillary) or "Tanner appliance" (mandibular).
- Canine guidance is often emphasized by prosthodontists to decrease loading, but there is no scientific evidence it protects teeth better than other designs.
 |  |
Clinical Purpose
- Joint stabilisation
- Protection of teeth
- Redistribution of occlusal forces
- Relaxation of elevator muscles
- Decrease in bruxism
Hard Versus Soft Splint Comparison
Clinical Efficacy10
- Soft Splints:
- No significant difference in TMD symptom reduction compared to hard splints.
- Considered a cheaper, short-term alternative.
- Associated with increased EMG activity and a short-term increase in sleep bruxism.
- This increase in EMG activity is known as the "chewing gum effect," which can have a counter-effect on muscle relaxation.
- Hard Splints:
- Supported by most studies.
- Stronger and easier to adjust clinically.

Anterior Bite Plane Appliances
Design Characteristics11
- Variations include orthodontic appliances such as Hawley, Sved, and Shore designs.
- Features a horseshoe-shaped palatal coverage with an occlusal platform covering 6-8 maxillary anterior teeth.
 |  |
Clinical Perspectives
- Advocates: Suggests the design prevents teeth clenching.
- Critics: Note the lack of posterior support, which may lead to overeruption of posterior teeth and overloading of the TMJs.
Mini Anterior Appliances and Adverse Effects
Device Variations
Mini-anterior appliances typically engage 2-4 incisors. Common variations include: - NTI-tss (Nociceptive Trigeminal Inhibitory Tension Suppressor System)
- NTI-tss
- Best Bite
- AMPS
- Lucia Jig
Clinical Indications
- Function: Disengages posterior teeth.
- Applications: Utilized for TMDs, sleep bruxism, and headaches.
- Systematic Review Findings: NTI-tss may be useful for bruxism and TMD by reducing jaw-closing muscle activity, particularly in cases of acute pain and limited opening.
Potential Adverse Effects
- Occlusal Changes: Posterior teeth overeruption and development of an anterior open bite.
- Dental Displacement: Mandibular anterior teeth mobility and maxillary anterior teeth displacement.
- Safety Risks: Risk of swallowing or aspiration of the small appliance.
Scientific Evidence for Anterior Appliances
Comparative Research Findings
- NTI-tss vs. Stabilisation Splints:
- No difference found in TMD symptoms or headaches in some studies.
- Other research suggests NTI-tss is less effective than flat plane stabilisation appliances for TMD.
- AMPS vs. Stabilisation Splints: No differences found for myogenous pain.
- Muscle Effects: Thickness and elasticity of the masseter muscle significantly decreased after NTI-tss use among bruxers.
- Headache Treatment: One study suggested NTI-tss was more effective than full coverage appliances, though the study was noted to have flaws regarding controls and statistics.
Anterior Repositioning Splints
Mechanism and Goals12
- Function: Positions the mandible anteriorly using an anterior guiding ramp.
- Advocates’ View:
- Intended to “recapture” the disc in cases of clicking, catching, or locking.
- Positions the disc temporarily by reducing pressure.
- Often intended as a precursor to comprehensive dental or surgical procedures.
Clinical Perspective on Repositioning
The presenter argues that comprehensive dental work or surgery to "re-establish" the bite after repositioning therapy is often unnecessary.

Indications for Internal Derangement13
- Acute TMJ pain.
- Sleep bruxers who awaken with TMJ pain.
- Nocturnal TMJ locking.
 |  |
Clinical Concerns14
- Critics: Highlight the risk of permanent occlusal and skeletal changes associated with long-term use.
 |  |
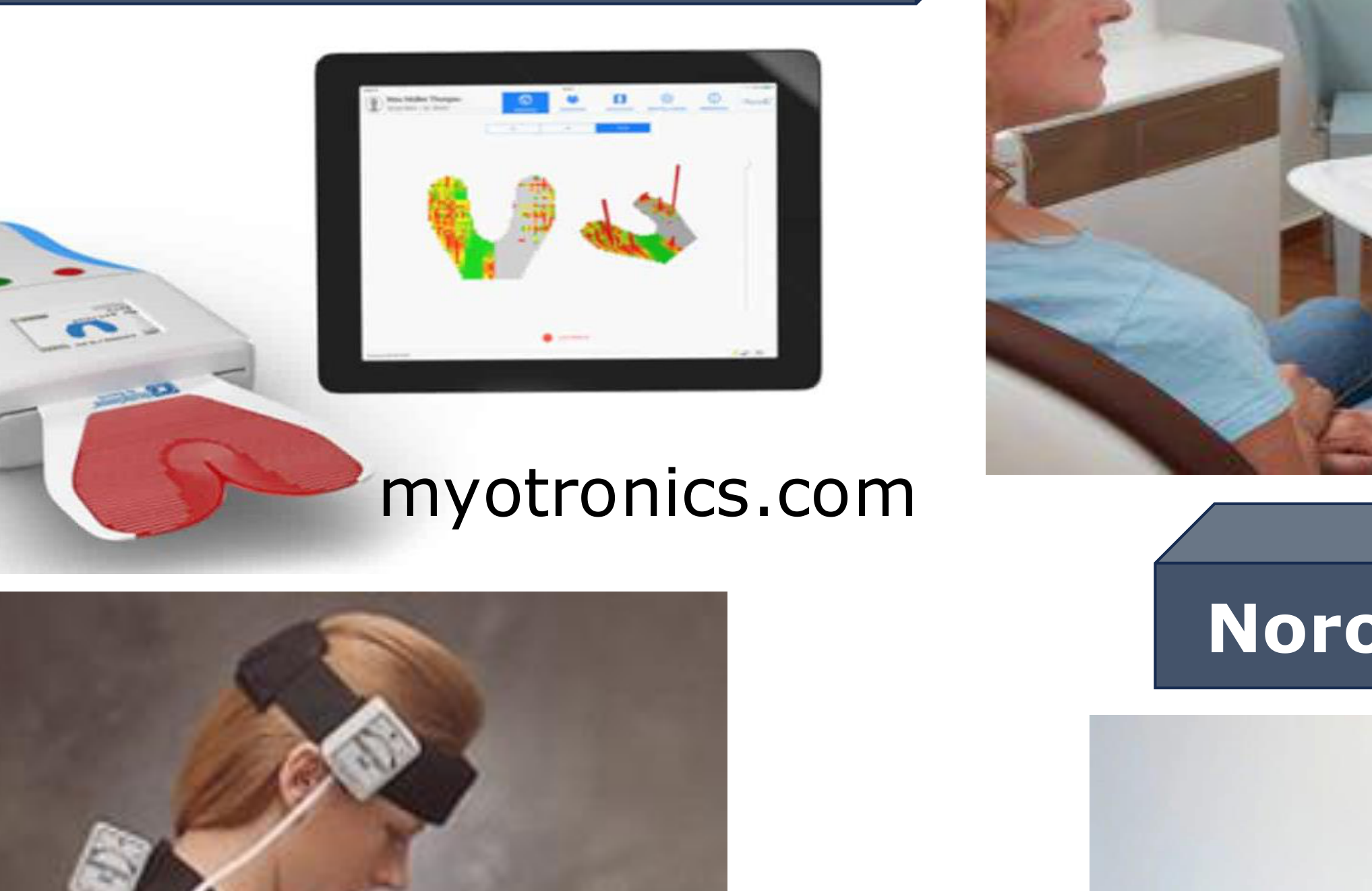
Neuromuscular Splints and Myocentric Position151617

Myocentric Position and Technology18
- Methodology: Uses jaw muscle stimulators, surface EMG, and jaw-tracking machines (such as the K7x Evaluation System) to determine the ideal “myocentric” vertical and horizontal position of the mandible.
- Clinical Application: Dental reconstruction is performed at this new jaw position.
- Athletic Performance: Research indicates neuromuscular mouthguards do not enhance the performance of competitive athletes.
- Claims regarding enhanced athletic ability are noted as "made up."
 |  |
 |
Diagnostic and Analysis Systems19
- OccluSense by Bausch: A system utilizing a device and tablet for digital occlusal analysis.
- Noromed MES 9000: A diagnostic facility including a console, scanner, and related attachments for neuromuscular evaluation.
RB
myotronics.com
REALITY !!!
Myotronic.com
Transclude of png;base64,DO_NOT_LOAD_OR_DISPLAY_THERE_IS_NO_RESTRICTED_VISUAL_DATA |
|  |
 |  |  |
Scientific Evidence for Neuromuscular Therapy
Research Summary
- Digital Limitations: Digital devices cannot accurately recreate the complex variations in jaw motion and muscle contractions.
- Athletic Impact: Neuromuscular mouthguards show no evidence of enhancing performance in competitive athletes.
- Philosophical Basis: Scientific evidence supporting the “Neuromuscular Dentistry” philosophy is currently lacking.
Critique of Neuromuscular Technology
There is no normative data for these measurements; they are confounded by jaw size, condyle shape, and individual function. Digital devices cannot accurately recreate complex jaw movements.
Posterior Bite Plane Splints
Design Variations20
- Common Names: MORA (Mandibular Orthopaedic Repositioning Appliance), Modified MORA, Posterior Plane Splint.
- Construction: Acrylic resin platforms placed over posterior mandibular teeth, often connected by a lingual wire.
- Mechanism: Causes disocclusion of anterior teeth and alters the vertical and horizontal maxillomandibular relationship.

Claims Regarding Physical Strength21
- Seated Press: Studies show no difference in power during a seated press when using a MORA versus a placebo splint.
- Muscular Strength: Research indicates the MORA has no significant effect on muscular strength compared to no splint or a placebo splint.
- Studies including those on American football players show no difference in muscular strength or power when wearing a MORA.
 |  |
Adverse Effects22
- Occlusal Risk: Potential development of a posterior open bite.

Pivot Splints and Fulcrum Designs
Design and Indications23
- Variations: Fulcrum-type splint.
- Construction: Hard acrylic with a single posterior contact point in each quadrant.
- Advocates’ View: The mandible is intended to fulcrum around the pivot, thereby unloading the articular surface.
- Clinical Use: Proposed as a treatment for osteoarthritis and internal derangements.
 |  |
 |
Research and Adverse Effects24
- Condylar Movement: Studies postulate that clenching on a pivot results in anterior downward condylar movement, while the pivot prevents protrusion (upward movement of ~0.3mm).
- TMJ Impact: Evidence suggests the design causes TMJ compression rather than distraction.
- Studies show that clenching on a pivot actually causes upward condylar movement and compression rather than distraction/unloading.
- Adverse Effect: Risk of developing a posterior open bite.
 |  |
Hydrostatic Splints
Design and Theory25
- Construction: A maxillary appliance featuring bilateral water-filled plastic chambers (intended for short-term use).
- Advocates’ View: Suggests the mandible will automatically find an ideal position because it is not mechanically directed by the appliance
- Example: The "Aqualizer" system.
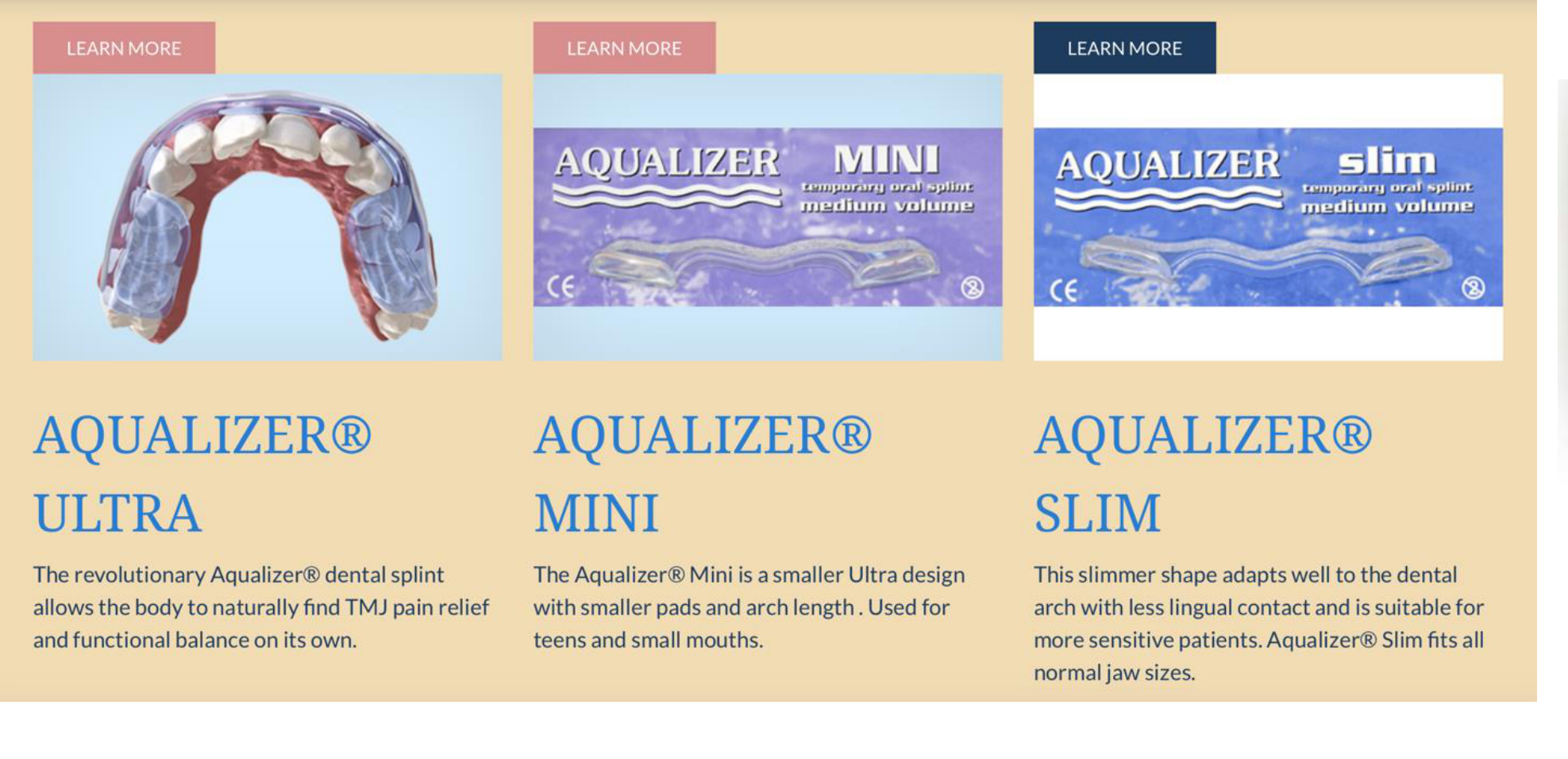 |  |
Scientific Evidence26
- Effectiveness: Research indicates the Aqualizer system is no better than chin point guidance in establishing the maxillomandibular relationship.
 |  |
 |  |
Biofeedback and Experimental Splints
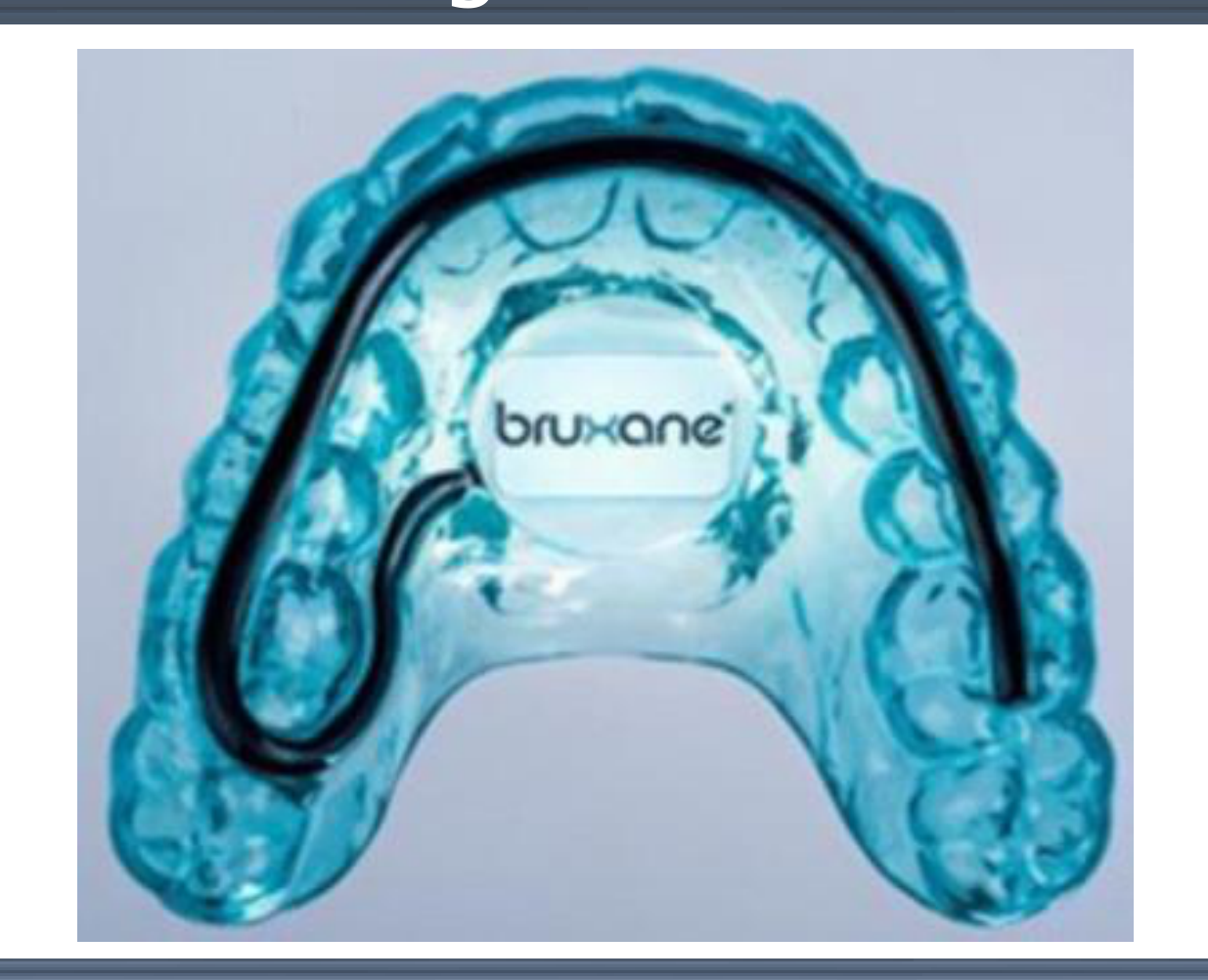
Design and Function27
- Mechanism: Incorporates a pressure sensor and microcontroller that provides an intrabuccal vibratory stimulus when triggered (typically at 10-20kg of pressure).
- Study Findings: Biofeedback splints (BFS) significantly reduce the frequency and duration of clenching bursts, thereby reducing pathological load on the masticatory system.
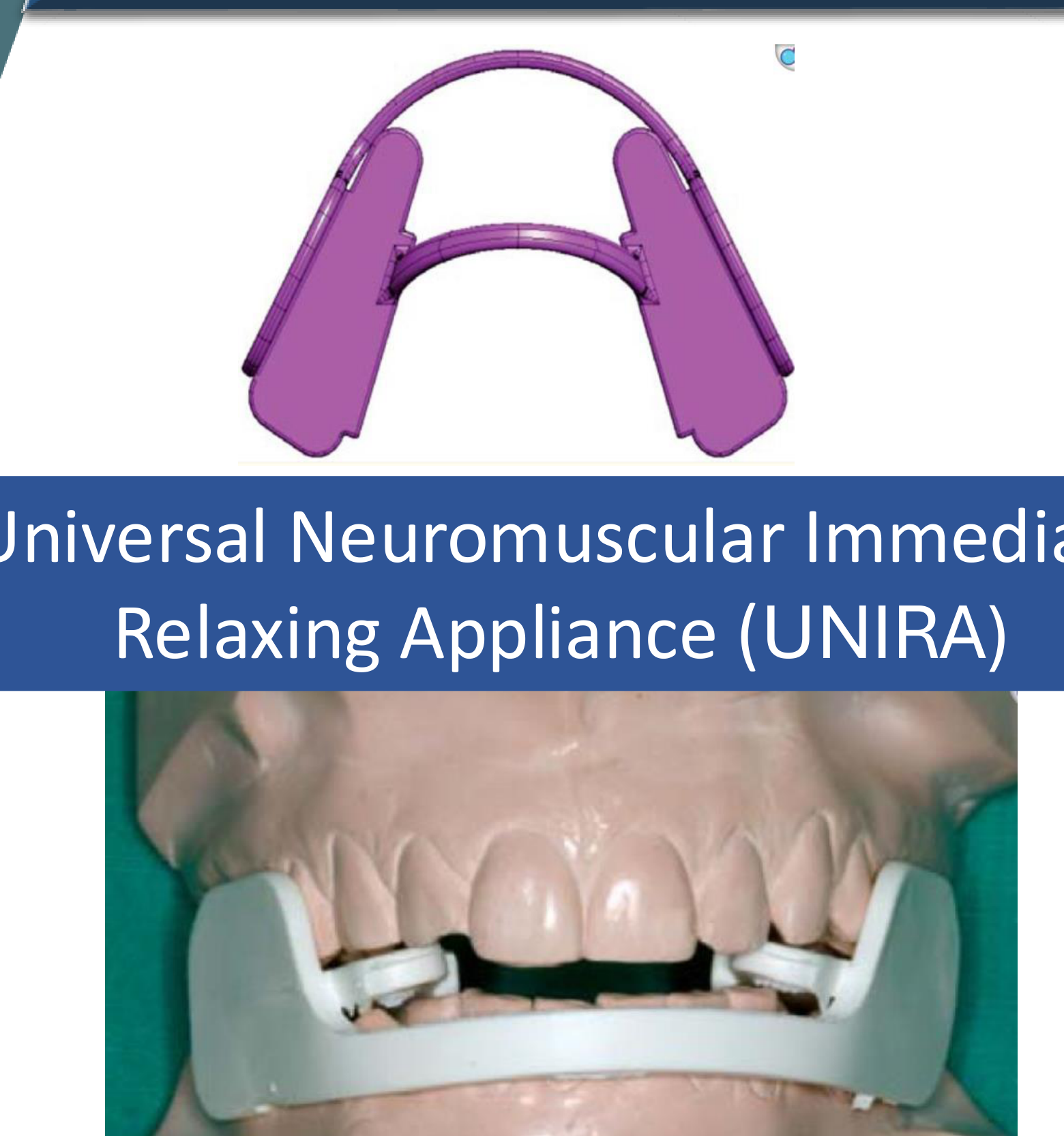
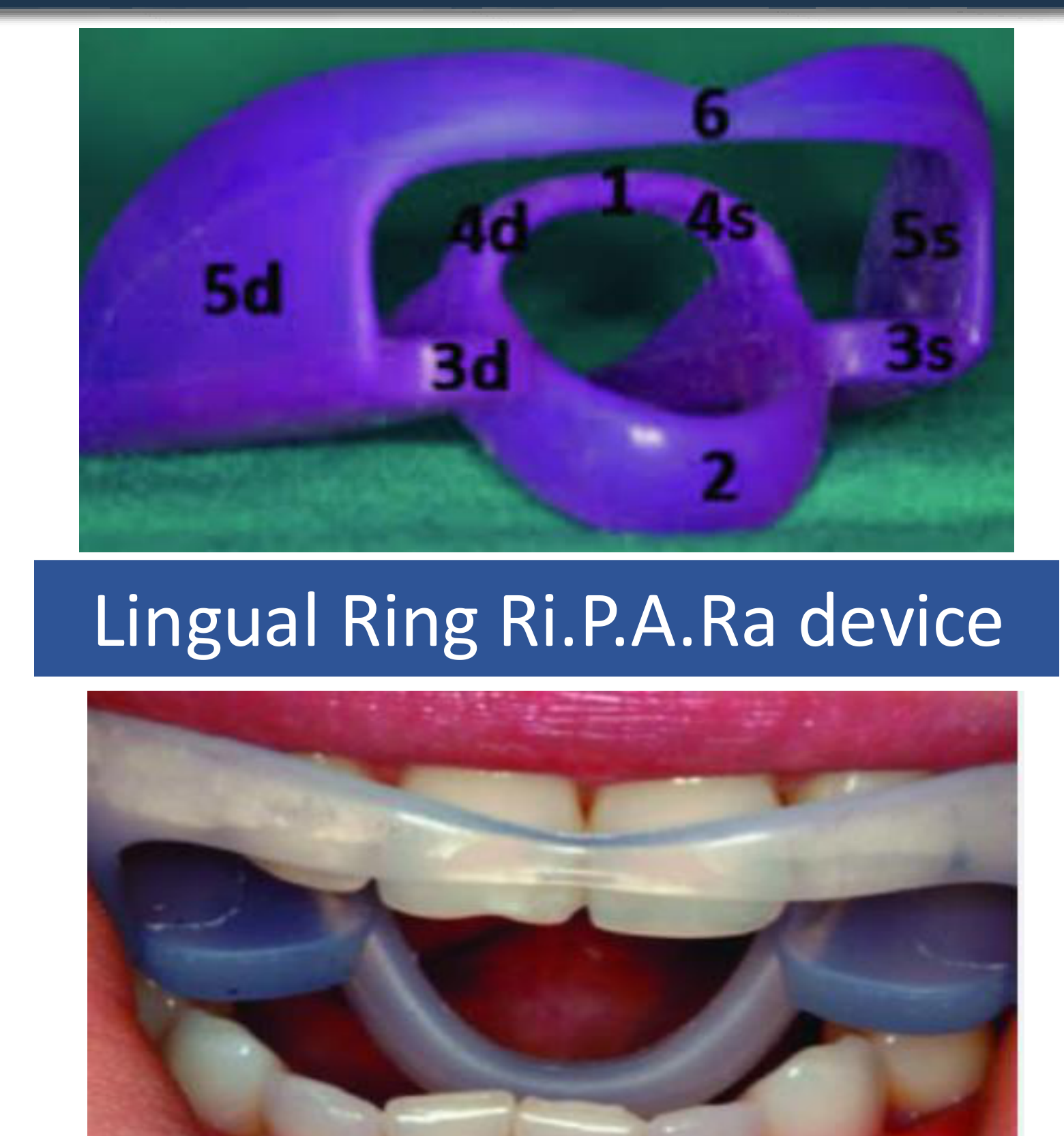
Alternative Device Designs28
- Universal Neuromuscular Immediate Relaxing Appliance (UNIRA)
- Lingual Ring Ri.P.A.Ra device
- Reference markings: 5d, 4d, 3d, 5s, 4s, 3s, 2.
 |  |
Mechanisms of Action
Agenda29
- Occlusal Splints Revisited
- Occlusal Splints Design Secrets
- Mechanisms of Action
- Scientific Evidence for Occlusal Splints
- Take Home Message
Theories of Treatment Success
8 Explanations For Treatment Success30
- Alteration of the occlusal condition
- Alteration of the condylar position
- Increase in the vertical dimension of occlusion
- Cognitive awareness
- Increase peripheral input to CNS hence decreasing motor activity
- Muscle relaxation/decreased motor activity
- Regression to the mean i.e. the natural fluctuation of symptoms
- Placebo effect
Note: These are only theories; nothing is confirmed.
How Do Splints Work?31
Mechanisms are often influenced by:
- Ideology (Downward Pressure)
- Confirmational Bias (Upward Pressure)
Occlusal Splints: Facts vs Fiction
Clinical Facts and Common Fictions
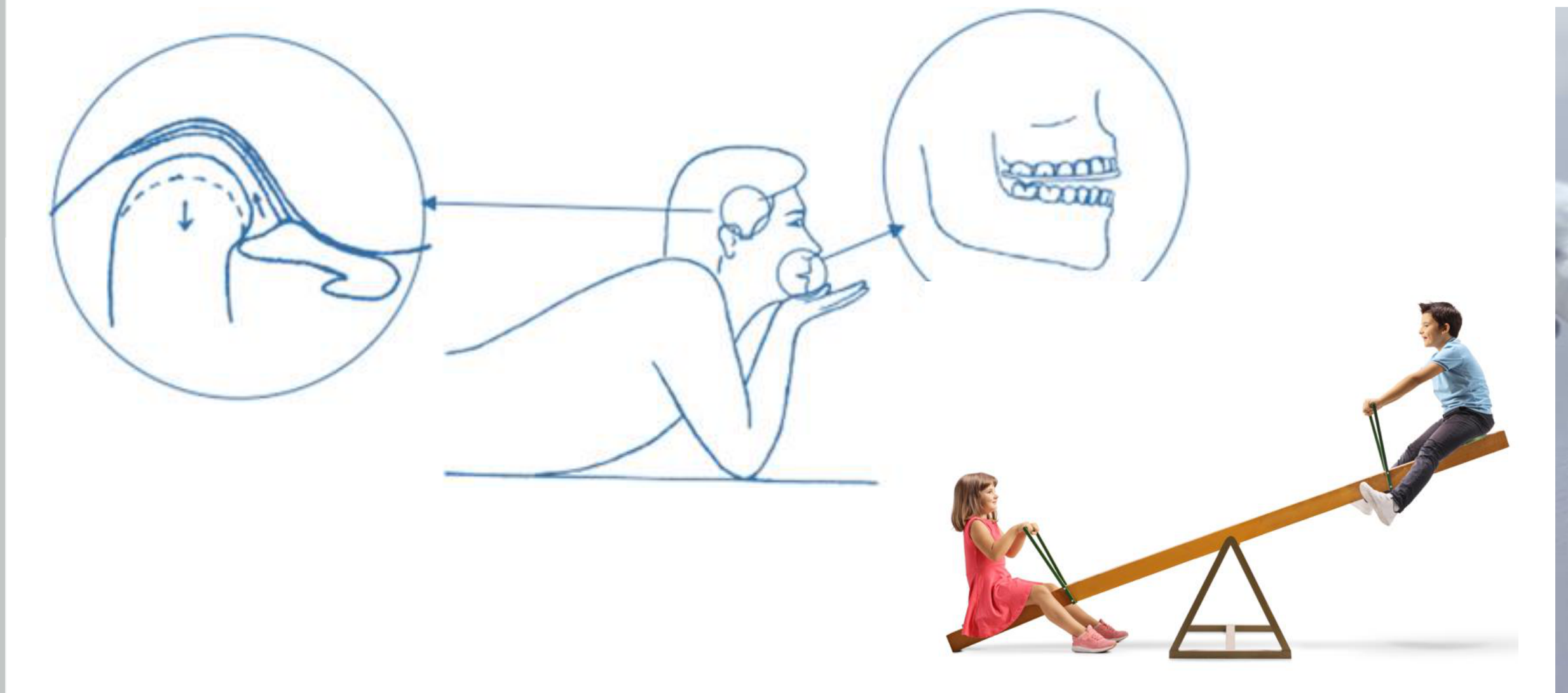
Fiction: TMJ Unloading32
Occlusal splints cannot “unload the TMJ”!
- The mandible is a class III lever: it cannot fulcrum at any point anterior to the masticatory muscles.
- Fact: Splints can reduce or redirect the condylar loading.
- Effort = Muscle

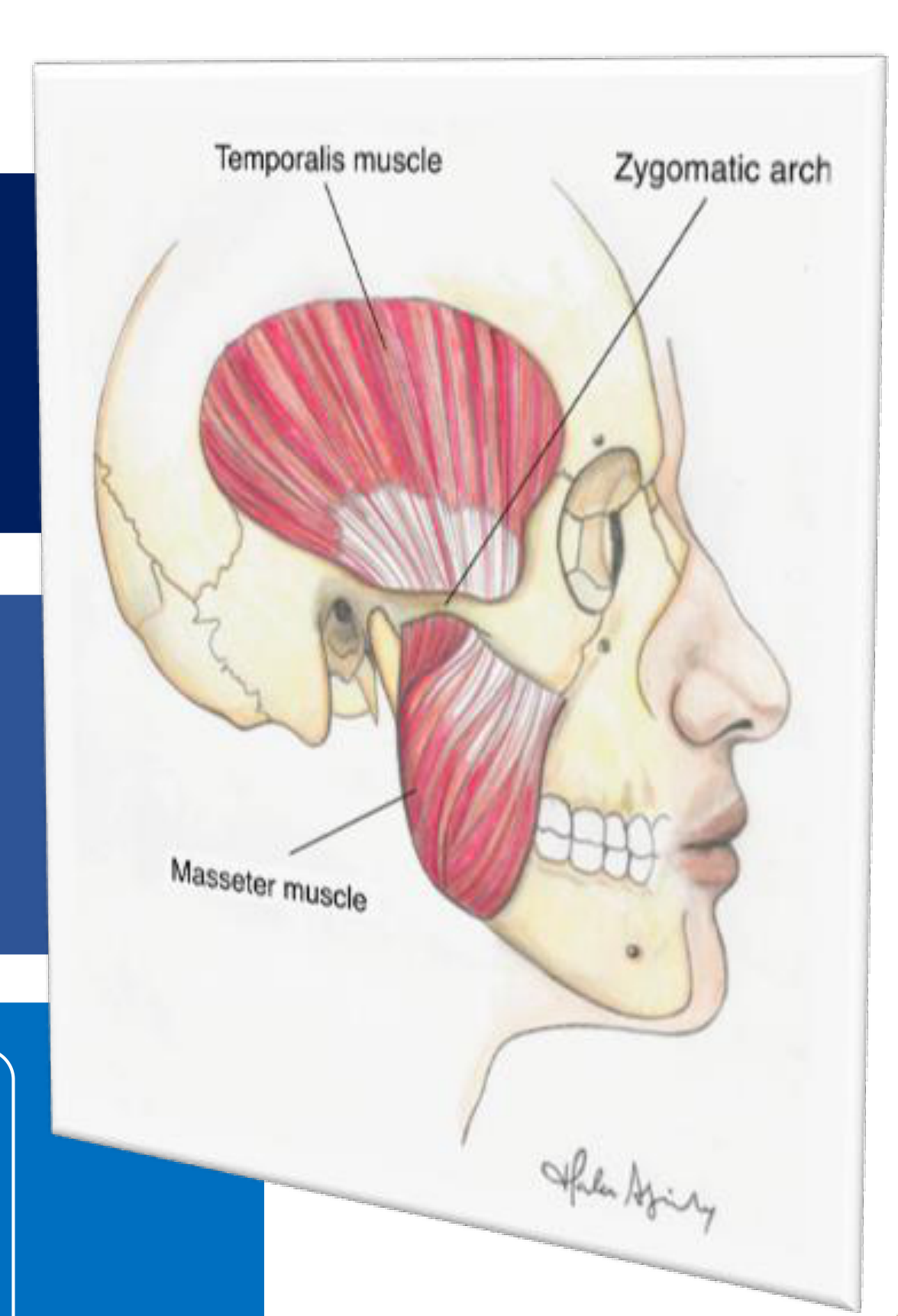
Muscle Activity and Headache Management
Fact: Decreases Muscle Activity
Occlusal splints can decrease nocturnal muscle activity.
- Reflective response to “foreign objects” between teeth.
- Nocturnal muscle activity returns to baseline after discontinuing splint use.
- Activity may return to baseline even while using the splint.
- Muscle activity can increase in asymptomatic bruxers.
Treatment for Headache
- Headache attributed to temporomandibular disorders:
- Over 70% of TMD patients report headache.
- Sleep bruxism generated myalgia may trigger tension-type headache and migraine.
Clinical Evidence for Headache Management
Randomised controlled trial (60 patients):
- Subjects with TMJ arthralgia and tension-type headache.
- Stabilisation splint was effective in headache improvement at 6 and 12 months compared to controls.
Prospective controlled study (60 patients):
- Subjects with myogenous TMD and tension-type headache.
- Stabilisation splint was effective in headache improvement compared to control appliance at 10 weeks, 6, and 12 months.
Comorbid Migraine and TMD Treatment
Double-blind, randomized, placebo-controlled study:
- Assessed separate or joint effects of treatment for comorbid migraine and TMD.
- 4 treatment groups:
- Propranolol & stabilisation splint
- Placebo pill & stabilisation splint
- Propranolol & non-occluding splint
- Placebo pill & non-occluding splint
- Finding: Migraine in women with TMD and migraine only improved when both conditions were treated.
Systematic Review and Meta-analysis:
- Stabilisation splints decrease both headache frequency and intensity in TMD patients.
Internal Derangements and Deprogramming Myths33
Fiction: Treatment of TMJ Internal Derangements
Misconceptions about treating TMJ disc displacements:
- Treatment of disc displacement with catching and locking is recommended.
- Advocates suggest: Avoid progression from TMJ clicking to locking
Asymptomatic Clicking
Asymptomatic clicking does not require treatment. Splints do not stop the progression of clicking to locking, nor do they permanently "recapture" a disc. .
Patient Adaptation and Pain Management
- Treatment versus no treatment did not change the outcome of patient adaptation.
- Fact: Splints provide symptomatic relief.
When To Treat TMD?
- Assessment via Pain VAS (Visual Analogue Scale) monitored over a 17-week period.
Fiction: Deprogram the Muscles
- Advocates: Claim splints deprogram TMJ musculature and produce “ideal” jaw relationships.
- Flawed Study Claims: Deprogramming splints and occlusal equilibration alleviated TMD and caused “minor changes in condylar position.”
Facts:
- Muscle engram is a learned pattern determined by the morphology of moving structures.
- Changing the occlusal scheme (morphology) can change the engram, but this does not necessarily establish “the” centric relation.
No evidence that ideal occlusal and skeletal treatment positions for dental patients based on “deprogramming” should be adapted for TMD patients.

Vertical Dimension of Occlusion Myths
Fiction: Ideal Vertical Dimension
- Advocates: Claim occlusal splints reduce abnormal muscle activity and pain by restoring VDO “lost” to tooth wear and lost posterior support. Success is attributed to increased VDO.
Facts:
- VDO is highly variable.
- Most individuals with decreased VDO do not have TMD.
Scoping Review: Concept of Vertical Dimension of Occlusion
- No evidence for a trial phase of new VDO to assess patient adaptation.
- Stability of VDO changes does not cause or cure TMD.
- Increasing VDO is done to create space for dental restorations, not to "cure" TMD.
Almost everything we were taught about VDO is a myth!
Summary of Facts Versus Fiction
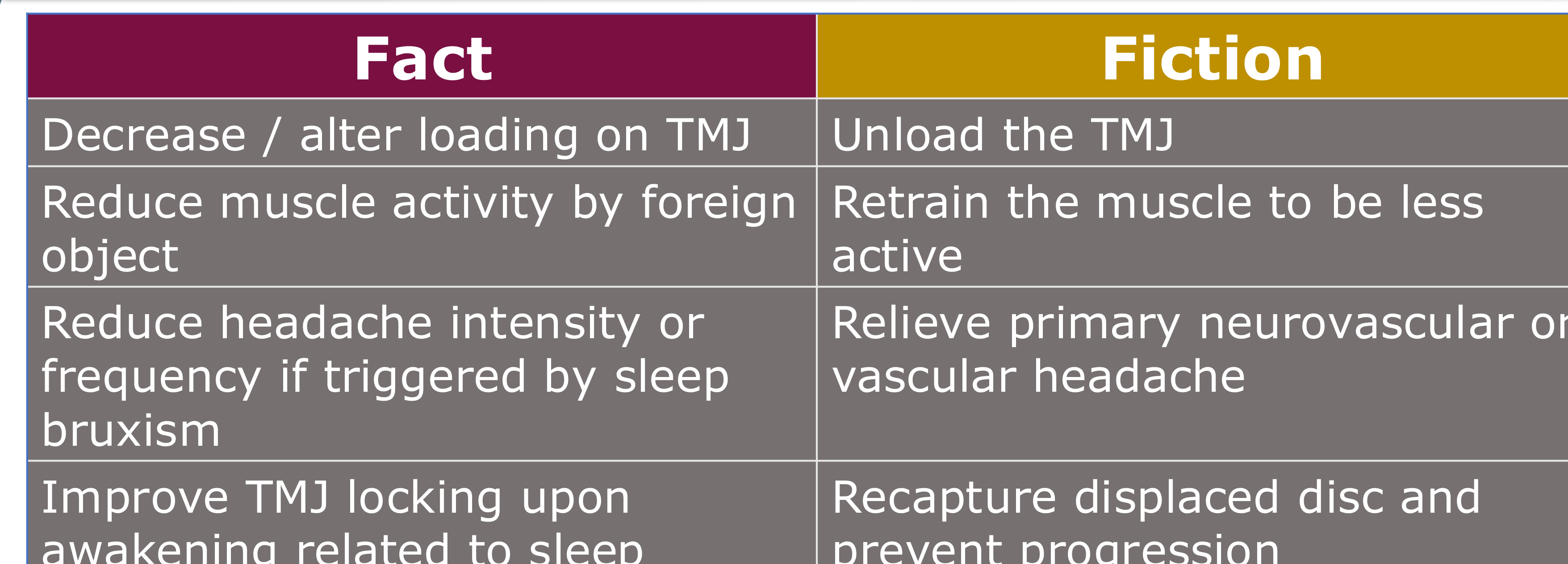
The Simple Facts of Occlusal Splints34
| Fact | Fiction |
|---|---|
| Decrease / alter loading on TMJ | Unload the TMJ |
| Reduce muscle activity by foreign object | Retrain the muscle to be less active |
| Reduce headache intensity or frequency if triggered by sleep bruxism | Relieve primary neurovascular or vascular headache |
| Improve TMJ locking upon awakening related to sleep bruxism | Recapture displaced disc and prevent progression |
 |  |
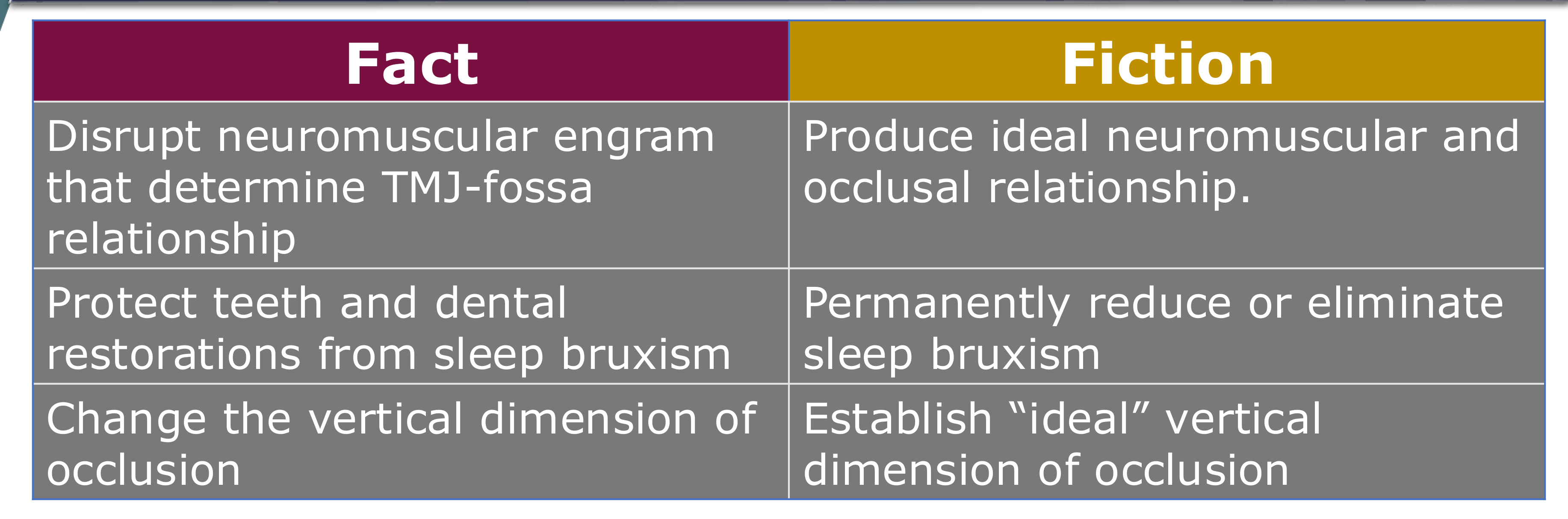
The Simple Facts of Occlusal Splints (Continued)35
| Fact | Fiction |
|---|---|
| Disrupt neuromuscular engram that determine TMJ-fossa relationship | Produce ideal neuromuscular and occlusal relationship |
| Protect teeth and dental restorations from sleep bruxism | Permanently reduce or eliminate sleep bruxism |
| Change the vertical dimension of occlusion | Establish “ideal” vertical dimension of occlusion |
 |  |
Scientific Evidence for Occlusal Splints36
 |  |
Efficacy in Temporomandibular Disorders
Meta-analysis of RCTs (2025)37
An analysis of 18 articles compared the efficacy of occlusal splints to other conservative treatments for Temporomandibular Disorders (TMDs).
Comparative Efficacy:
- Not superior in pain management when compared to other conservative treatments.
- Not superior in improving mouth opening when compared to other conservative treatments.
Key Findings and Conclusions:
- More effective than counseling alone in pain management.
- Reduced the incidence of TMJ clicking.
- More effective than placebo splints for both pain reduction and mouth opening.
Source: Zhang et al. Oral Surg Oral Med Oral Pathol Oral Radiol. 2025 May;139(5):509-520.
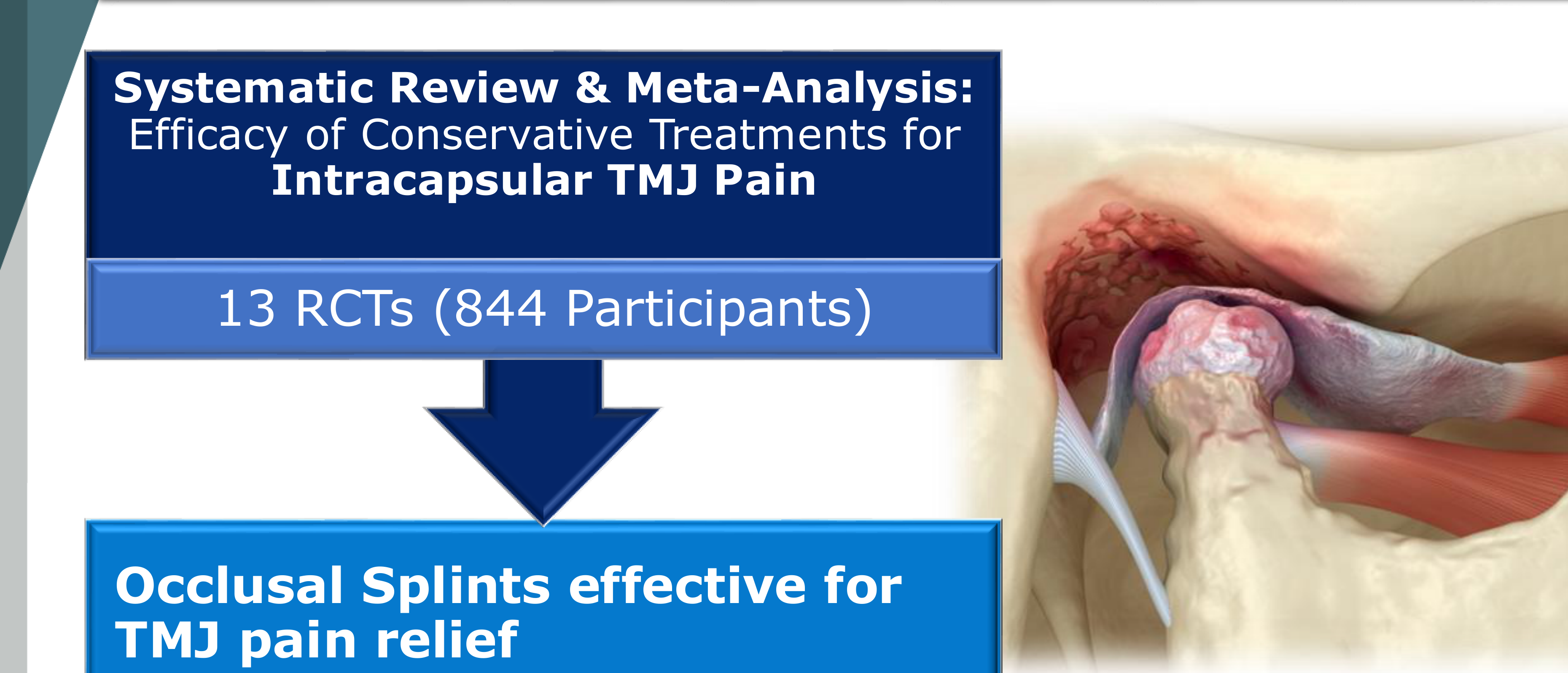
Systematic Review & Meta-Analysis: Intracapsular TMJ Pain38
A review of 13 Randomized Controlled Trials (RCTs) involving 844 participants examined the efficacy of conservative treatments for intracapsular TMJ pain.
Key Finding:
- Occlusal splints are effective for TMJ pain relief.
- Occlusal splints are specifically effective for treating arthralgia.
Source: Ferrillo et al. Cranio. 2025 Mar;43(2):258-274.
Efficacy in Masticatory Muscle Pain
Systematic Review (2024): Stabilisation Splints39
A systematic review of 10 articles evaluated the use of stabilisation splints for masticatory muscle pain.
Clinical Parameters Evaluated:
- Pressure pain threshold
- Pain during chewing
- Mouth opening
- Spontaneous pain
- Palpation pain
Results:
- Stabilisation splints (n=160) were found to be as effective as other treatments (n=209).
- Stabilization splints are as effective as physiotherapy or anti-inflammatories for muscle pain.
Source: Honnef et al. Cranio. 2024 Nov;42(6):718-729.
Appliance Selection Based on Diagnosis
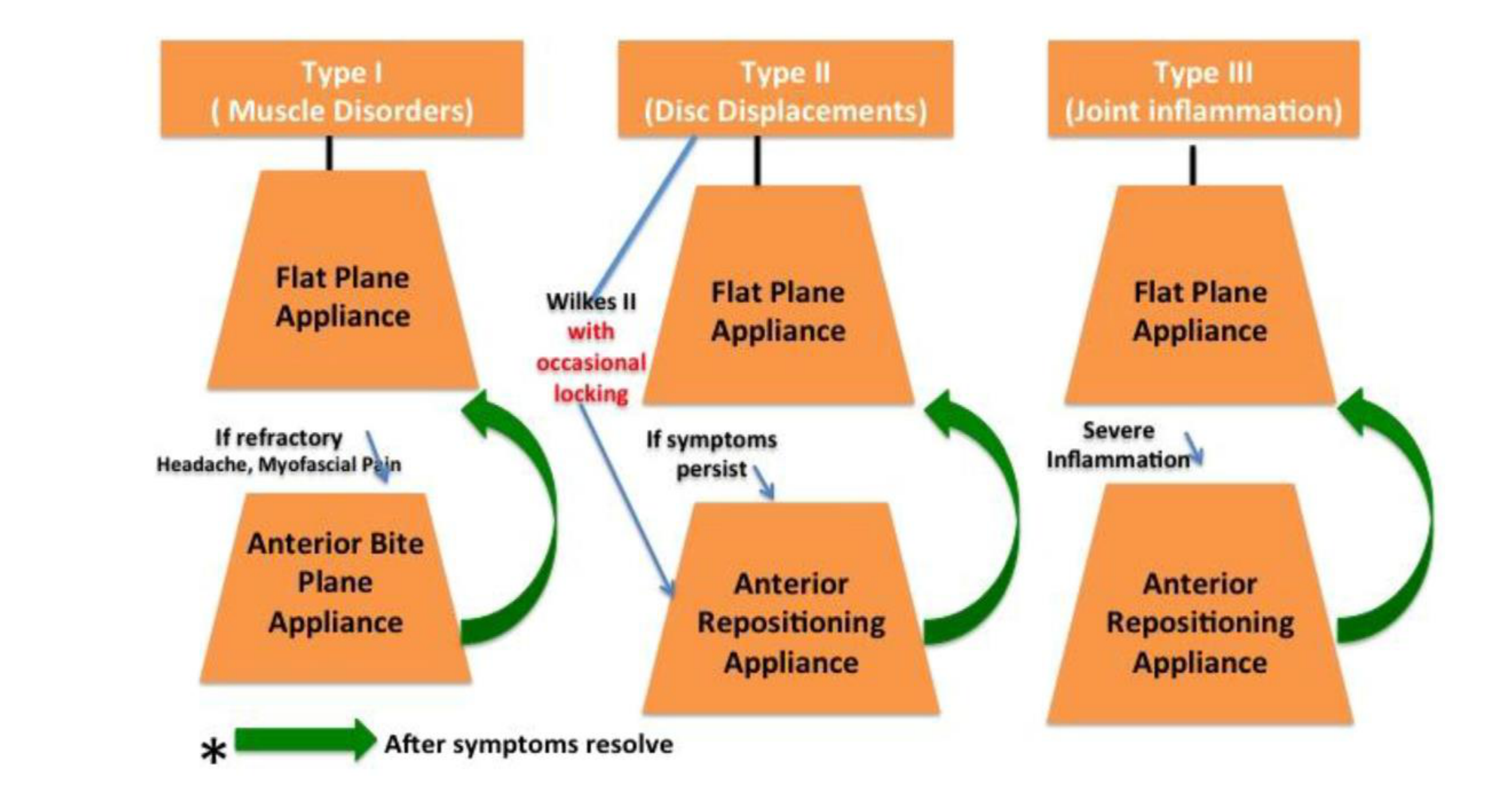
Diagnostic-Based Appliance Selection40
-
Type I: Muscle Disorders
- Initial Selection: Flat Plane Appliance
- Common examples include the Michigan or Tanner splints.
- Progression: If refractory (Headache, Myofascial Pain), transition to Anterior Bite Plane Appliance.
- Follow-up: Return to Flat Plane Appliance after symptoms resolve.
- Initial Selection: Flat Plane Appliance
-
Type II: Disc Displacements
- Initial Selection: Flat Plane Appliance
- Progression: For Wilkes II with occasional locking, transition to Anterior Repositioning Appliance if symptoms persist.
- Follow-up: Return to Flat Plane Appliance after symptoms resolve.
-
Type III: Joint Inflammation
- Initial Selection: Flat Plane Appliance
- Progression: For severe inflammation, transition to Anterior Repositioning Appliance.
- Follow-up: Return to Flat Plane Appliance after symptoms resolve.
Source: Greene CS, Menchel HF. Oral Maxillofac Surg Clin North Am. 2018;30(3):265-277.
Effects on Sleep Bruxism
Systematic Review & Meta-analysis of RCTs (2024)41
This review included 12 studies (3 RCTs) with a low to very low certainty of evidence, investigating whether occlusal splints influence masticatory muscle function in sleep bruxers.
Key Findings:
- Soft or hard splints did not affect muscle activity or bite force.
- Splints did not affect masticatory performance or muscle volume.
- Splints reduce tongue force.
Clinical Note on Bruxism
While splints protect teeth from wear, they do not stop the act of sleep bruxism itself.
Source: Ferreira et al. Eur J Oral Sci. 2024 Apr;132(2):e12979.
The Role of Occlusion in Treatment
Comparative Trial: Occlusal vs. Palatal Splints42
A randomised controlled trial of 80 TMD subjects compared treatment with an occlusal splint versus a palatal (non-occluding) splint.
Results at 6 and 12 Months (30% Pain Improvement):
- 50% of the occlusal splint group showed improvement.
- 42% of the palatal (non-occluding) splint group showed improvement.
Functional Outcome:
- Both groups demonstrated improvement in function.
- The fact that 42% of patients with non-occluding splints improved suggests that the "bite" itself is not the primary mechanism of healing.
Source: Nilsson H, Vallon D, Ekberg EC. J Oral Rehabil. 2011 Oct;38(10):713-21.
 |  |
Efficacy of Non-Occluding Splints43
There is weak evidence suggesting that non-occluding splints may be effective in treating TMDs.
Theories for Non-Occluding Splint Efficacy:
- Placebo effect
- Increased cognitive awareness
Clinical Recommendation: When selecting a splint for TMD, it is advised to “cover the occlusion,” as occluding splints are more effective for pain reduction.
Sources: Dao TTT. et al. 1994; Nilsson H. et al. 2011; Ekberg E. et al. 2003; Alkhutari AS. et al. 2012.
Take Home Message44

Presentation Overview45
- Occlusal Splints Revisited
- Occlusal Splints Design Secrets
- Mechanisms of Action
- Scientific Evidence for Occlusal Splints
- Take Home Message
Why does one patient need all of these splints?
Explanations for Treatment Success46
- Alteration of the occlusal condition
- Alteration of the condylar position
- Increase in the vertical dimension of occlusion
- Cognitive awareness
- Increase peripheral input to CNS hence decreasing motor activity
- Regression to the mean (the natural fluctuation of symptoms)
- Placebo effect
- Success is largely driven by Regression to the Mean (treating patients when their pain is at its natural peak) and the Placebo Effect.
- Placebo is enhanced by clinician reputation, environment (e.g., curved desks for approachability), and patient trust.
Clinical Considerations and Efficacy47
- Occlusal splints are “oromandibular crutches” no different to orthotics.
- Occlusal splints are "oromandibular crutches" or walking sticks for the jaw.
- Avoid full-time wear and designs that may lead to change in occlusion.
- Mechanism of action of occlusal splints remains unknown.
- Occlusal splints protect teeth from bruxism but do not stop bruxism.
- Bruxism is a sign, not a diagnosis; clinicians must look for secondary causes (medications like SSRIs, ADHD, sleep apnea, lifestyle factors).
- Botox reduces force but does not stop the activity of bruxism and is temporary/expensive.
- Occlusal splints may be effective for TMD and headache triggered by sleep bruxism.
 |  |  |
 |  |
Footnotes
-
Original PDF page 1: L31 OCCLUSAL SPLINT THERAPY, p.1 ↩
-
Original PDF page 2: L31 OCCLUSAL SPLINT THERAPY, p.2 ↩
-
Original PDF page 3: L31 OCCLUSAL SPLINT THERAPY, p.3 ↩
-
Original PDF page 4: L31 OCCLUSAL SPLINT THERAPY, p.4 ↩
-
Original PDF page 5: L31 OCCLUSAL SPLINT THERAPY, p.5 ↩
-
Original PDF page 6: L31 OCCLUSAL SPLINT THERAPY, p.6 ↩
-
Original PDF page 7: L31 OCCLUSAL SPLINT THERAPY, p.7 ↩
-
Original PDF page 8: L31 OCCLUSAL SPLINT THERAPY, p.8 ↩
-
Original PDF page 9: L31 OCCLUSAL SPLINT THERAPY, p.9 ↩
-
Original PDF page 10: L31 OCCLUSAL SPLINT THERAPY, p.10 ↩
-
Original PDF page 11: L31 OCCLUSAL SPLINT THERAPY, p.11 ↩
-
Original PDF page 15: L31 OCCLUSAL SPLINT THERAPY, p.15 ↩
-
Original PDF page 16: L31 OCCLUSAL SPLINT THERAPY, p.16 ↩
-
Original PDF page 17: L31 OCCLUSAL SPLINT THERAPY, p.17 ↩
-
Original PDF page 20: L31 OCCLUSAL SPLINT THERAPY, p.20 ↩
-
Original PDF page 21: L31 OCCLUSAL SPLINT THERAPY, p.21 ↩
-
Original PDF page 22: L31 OCCLUSAL SPLINT THERAPY, p.22 ↩
-
Original PDF page 18: L31 OCCLUSAL SPLINT THERAPY, p.18 ↩
-
Original PDF page 19: L31 OCCLUSAL SPLINT THERAPY, p.19 ↩
-
Original PDF page 24: L31 OCCLUSAL SPLINT THERAPY, p.24 ↩
-
Original PDF page 25: L31 OCCLUSAL SPLINT THERAPY, p.25 ↩
-
Original PDF page 26: L31 OCCLUSAL SPLINT THERAPY, p.26 ↩
-
Original PDF page 27: L31 OCCLUSAL SPLINT THERAPY, p.27 ↩
-
Original PDF page 28: L31 OCCLUSAL SPLINT THERAPY, p.28 ↩
-
Original PDF page 29: L31 OCCLUSAL SPLINT THERAPY, p.29 ↩
-
Original PDF page 30: L31 OCCLUSAL SPLINT THERAPY, p.30 ↩
-
Original PDF page 31: L31 OCCLUSAL SPLINT THERAPY, p.31 ↩
-
Original PDF page 32: L31 OCCLUSAL SPLINT THERAPY, p.32 ↩
-
Original PDF page 33: L31 OCCLUSAL SPLINT THERAPY, p.33 ↩
-
Original PDF page 34: L31 OCCLUSAL SPLINT THERAPY, p.34 ↩
-
Original PDF page 35: L31 OCCLUSAL SPLINT THERAPY, p.35 ↩
-
Original PDF page 36: L31 OCCLUSAL SPLINT THERAPY, p.36 ↩
-
Original PDF page 44: L31 OCCLUSAL SPLINT THERAPY, p.44 ↩
-
Original PDF page 47: L31 OCCLUSAL SPLINT THERAPY, p.47 ↩
-
Original PDF page 48: L31 OCCLUSAL SPLINT THERAPY, p.48 ↩
-
Original PDF page 49: L31 OCCLUSAL SPLINT THERAPY, p.49 ↩
-
Original PDF page 50: L31 OCCLUSAL SPLINT THERAPY, p.50 ↩
-
Original PDF page 51: L31 OCCLUSAL SPLINT THERAPY, p.51 ↩
-
Original PDF page 52: L31 OCCLUSAL SPLINT THERAPY, p.52 ↩
-
Original PDF page 53: L31 OCCLUSAL SPLINT THERAPY, p.53 ↩
-
Original PDF page 54: L31 OCCLUSAL SPLINT THERAPY, p.54 ↩
-
Original PDF page 55: L31 OCCLUSAL SPLINT THERAPY, p.55 ↩
-
Original PDF page 56: L31 OCCLUSAL SPLINT THERAPY, p.56 ↩
-
Original PDF page 58: L31 OCCLUSAL SPLINT THERAPY, p.58 ↩
-
Original PDF page 57: L31 OCCLUSAL SPLINT THERAPY, p.57 ↩
-
Original PDF page 59: L31 OCCLUSAL SPLINT THERAPY, p.59 ↩
-
Original PDF page 60: L31 OCCLUSAL SPLINT THERAPY, p.60 ↩