Non-Odontogenic Toothache1
Ramesh Balasubramaniam OAM
DENT5310 Orofacial Pain and Dental Sleep Medicine Module 24th April 2026
Introduction and Disclosures2
Academic and Professional Affiliations3
- Ramesh Balasubramaniam OAM
- Associate Professor
- Discipline Lead in Oral Medicine
- UWA Dental School
- The University of Western Australia
Conflict of Interest Statement
Neither I nor my immediate family have any financial interests that would create a conflict of interest or restrict my independent judgment with regard to the content of this presentation.
Presentation Topics4
- Odontogenic Pains
- Site vs Source of Orofacial Pain
- Non-Odontogenic Pains
- Take Home Message
Odontogenic Pains5
Odontogenic pain originates from the teeth, dental pulp, periodontal ligaments, or surrounding structures like the alveolar bone. This type of pain presents with multiple clinical “faces” depending on the nature of the insult.
Clinical Context
Odontogenic pain is the most common orofacial pain, affecting approximately one in three people. These toothaches are highly painful, often keeping patients awake at night, which is a distinguishing feature from most other orofacial pains. They are generally predictable to diagnose as clinical findings usually correlate with microscopic observations.
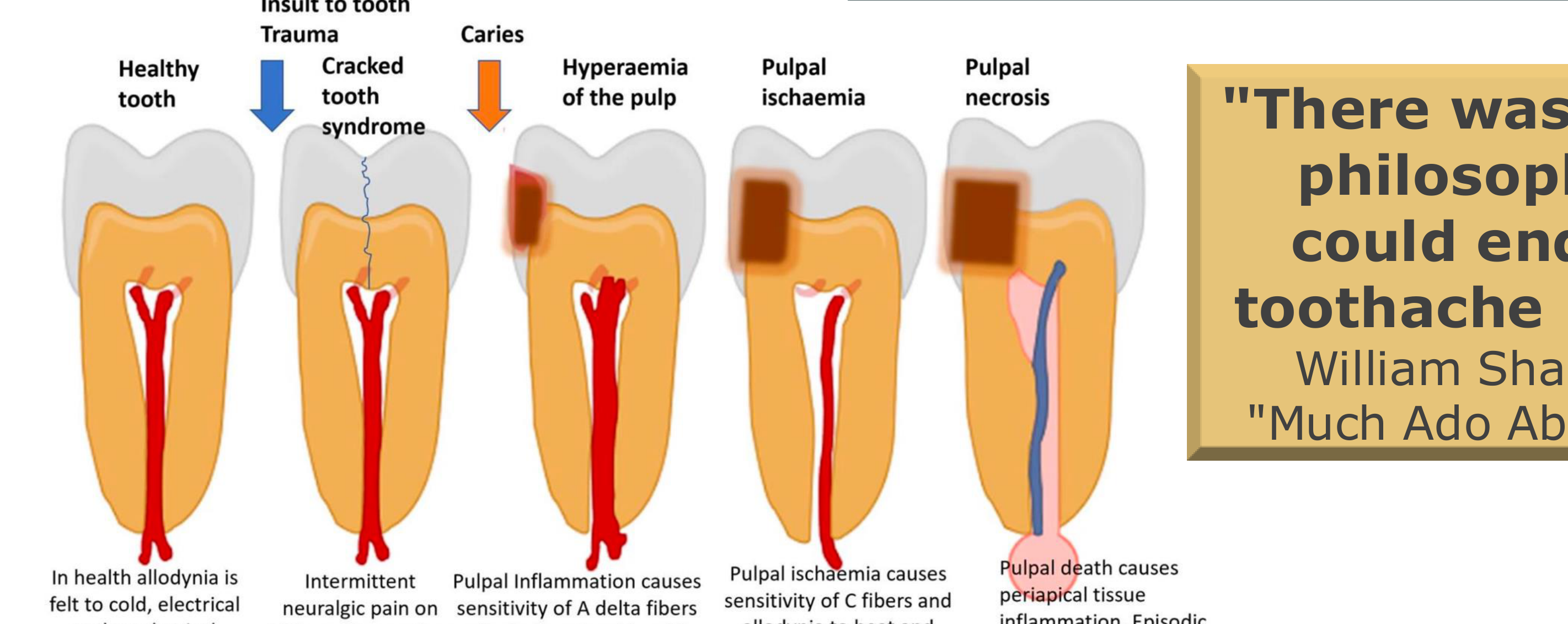
Clinical Progression of Odontogenic Pain6
-
Healthy Tooth
- In health, allodynia is felt to cold, electrical, and mechanical stimuli.
-
Cracked Tooth Syndrome (Trauma)
- Characterized by intermittent neuralgic pain on biting with no other symptoms.
-
Hyperaemia of the Pulp (Caries)
- Pulpal inflammation causes sensitivity of A-delta fibers.
- Results in allodynic pain triggered by cold and sugary stimuli.
-
Pulpal Ischaemia
- Causes sensitivity of C-fibers.
- Results in allodynia to heat and spontaneous episodic throbbing pain.
-
Pulpal Necrosis
- Pulpal death causes periapical tissue inflammation.
- Results in episodic spontaneous throbbing pain and allodynia on biting.
-
Dental pain can refer to other structures; for example, pain in a maxillary molar (26) might be felt in a mandibular molar (36), or it can radiate down the mandible or up the face.
No unique content provided for Page 6.
Presentation Outline7
- ODONTOGENIC PAINS
- SITE VS SOURCE OF OROFACIAL PAIN
- NON-ODONTOGENIC PAINS
- TAKE HOME MESSAGE
Site Versus Source of Orofacial Pain89
Definitions10
-
Site of Pain
- The location where the patient feels the pain.
-
Source of Pain
- The specific tissue from which the pain actually originates.
Classification of Pain Location11
-
Primary Pain
- The Site (where it hurts) is equal to the Source (where it originates).
- Example: Pulpitis in tooth 36 where the patient feels pain exactly where the inflammation is located.
- The Site (where it hurts) is equal to the Source (where it originates).
-
Heterotopic Pain
- The Site is not equal to the Source.
- Includes Projected Pain or Referred Pain.
- This can be projected down a nerve or referred from one nerve to another.
Clinical Application
Treatment success is achieved by treating the Source of Pain, NOT the Site of Pain
Clinical Importance
Treating the site (e.g., extracting a tooth when the pain is actually referred from a muscle) will not resolve the pain. No unique content provided for Page 10.
Outline12
- ODONTOGENIC PAINS
- SITE VS SOURCE OF OROFACIAL PAIN
- NON-ODONTOGENIC PAINS
- TAKE HOME MESSAGE
Non-Odontogenic Pains of Myofascial Origin1314
Non-odontogenic pains can be classified by their systems of origin:
Clinical Significance
Approximately 7% of patients with myofascial pain receive unnecessary endodontic treatment because the pain refers to the teeth.
- Myofascial Origin
- Neurovascular Origin
- Cardiac Origin
- Neuropathic Origin
- Sinus Origin
- Psychogenic Origin
 |  |  |
 |  |  |
Trigger Point Characteristics151617
Non-odontogenic pain of myofascial origin refers to pain originating from muscles and fascia that presents as tooth pain.
Active Trigger Points18
- Definition: A localized hyperexcitable nodule representing neuromuscular dysfunction at the motor endplate.
- Physical Characteristics: Located within a taut band of skeletal muscle.
- Clinical Presentation: A firm nodule that is tender to palpation; it will refer pain to a distant site 80% of the time.

Mechanism of Referred Pain
- Convergence Theory: Pain referral is mediated through the trigeminal sensory complex
- Second-order neurons transmit pain signals to a different site via antidromic sensation..
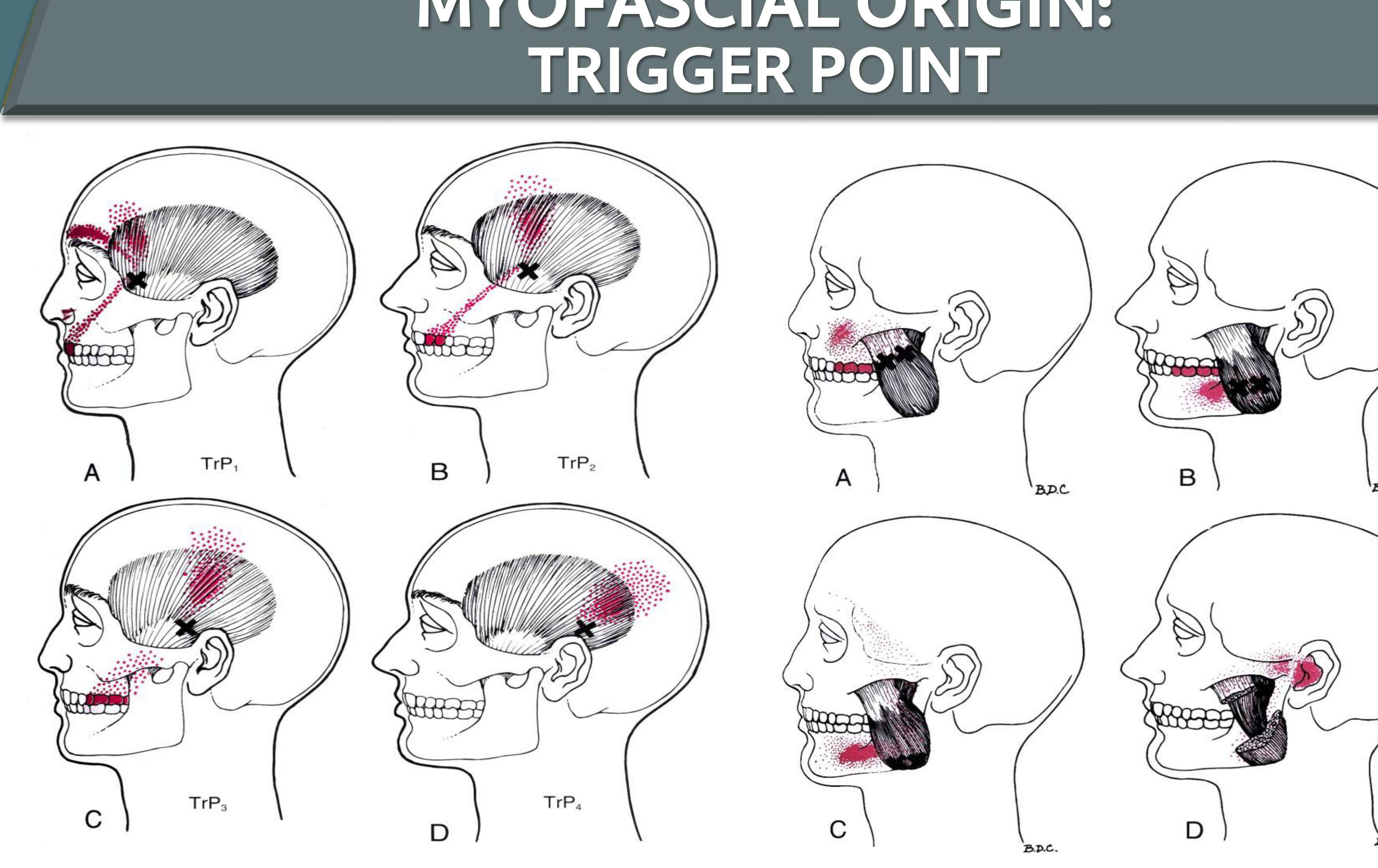
Trigger Point Mapping19
Trigger point locations and their associated referral patterns (B.D.C.):
-
Anterior Temporalis: Can refer pain to the anterior teeth and up the head
-
Middle/Posterior Temporalis: Refers to premolars and molars
-
Masseter: Refers to the mandible and posterior teeth
-
Sternocleidomastoid: Can refer to the back of the head or across the frontalis muscle
-
TrP1: Associated with referral pattern A
-
TrP2: Associated with referral pattern B
-
TrP3: Associated with referral pattern C
-
TrP4: Associated with referral pattern D
Management of Myofascial Pain20
Conservative and Behavioral Interventions21
- Education & Reassurance
- Inform the patient that the pain is self-limiting and identify the source
- Identify if psychosocial distress is driving muscle tension for potential psychotherapy referral
- Pain-Free Jaw Function
- Habit Awareness & Reversal
- Cautioning against habits like clenching or nail-biting
- Spray & Stretch
- Uses ethyl chloride technique
- Jaw Strengthening & Stretching Exercises
- Physical Therapy
 |  |  |
 |  |  |
 |  |  |
 |  |
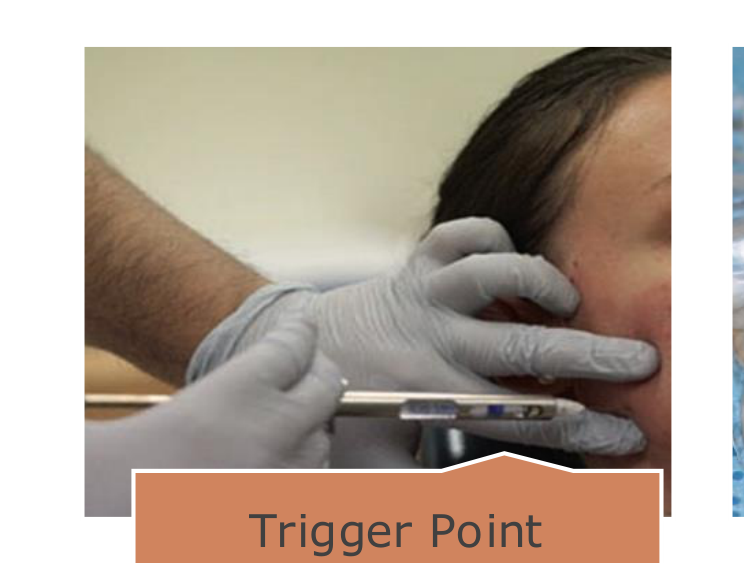
Clinical and Therapeutic Interventions
- Trigger Point Injections
- Injecting the source (e.g., masseter or temporalis) with local anesthetic
- Use anesthetic without adrenaline to avoid necrosis to block referred tooth pain
- Oral Appliance Therapy
- Occlusal splints are used if bruxism is a contributing factor
- Pharmacotherapy
- Botulinum Toxin Injections
- Psychological Therapy
Non-Odontogenic Pains of Neurovascular Origin22
Info
These are essentially "headaches of the face."
“Headache” may present as a variant in the orofacial region, frequently mimicking toothache.
Primary Classifications of Neurovascular Orofacial Pain23
- Migraine
- Trigeminal Autonomic Cephalalgias
- Includes cluster headaches, paroxysmal hemicrania, and SUNCT.
Pain of neurovascular origin.
 |  |
 |
Clinical Presentation of Neurovascular Pain
Demographics and Onset24252627282930
- Gender Ratio (F:M): 3.2:1
- Average Age of Onset: 40 years
 | 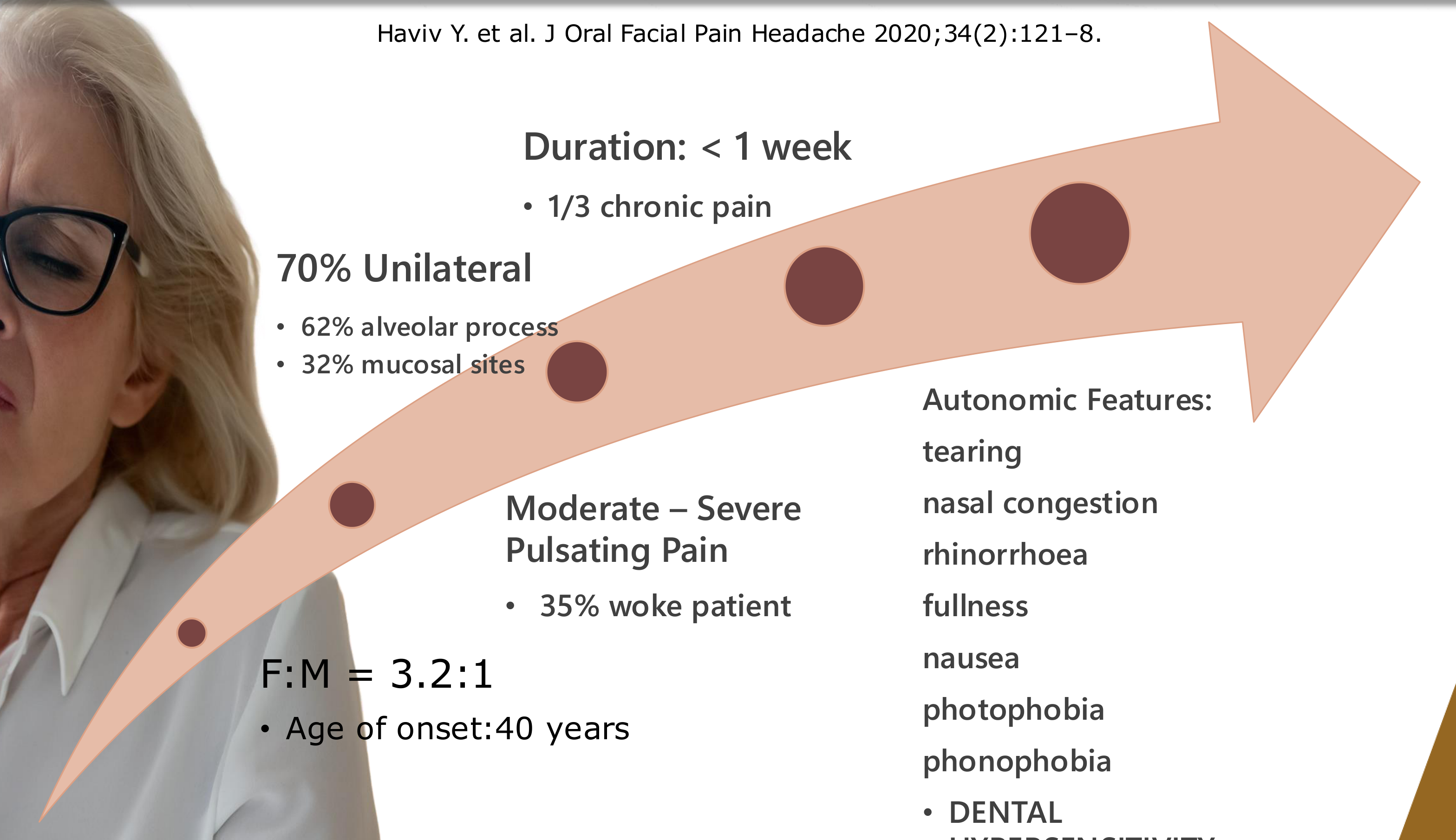 |
Pain Characteristics and Location
- Laterality: 70% Unilateral
- Distribution:
- 62% Alveolar process
- 32% Mucosal sites
- Intensity and Quality:
- Moderate to Severe
- Pulsating pain
- 35% of cases woke the patient from sleep
- Duration:
- Typically < 1 week
- 1/3 of cases involve chronic pain
Associated Symptoms and Autonomic Features
- Tearing
- Nasal congestion
- Rhinorrhoea
- Fullness
- Nausea
- Photophobia
- Phonophobia
- Allodynia: Teeth may feel hypersensitive to light touch.
- Dental hypersensitivity
Non-Odontogenic Pains of Sinus Origin
Abstract
Pain referred from the sinus mucosa, transmitted via the maxillary branch of the trigeminal nerve.
- Clinical Presentation: Constant, dull, aching pain in the maxillary posterior teeth.
- Teeth may be sensitive to percussion and temperature (hyperalgesia).
- Diagnostic Indicators: Pain often increases when the patient bends over due to fluid shifts.
- If a "virgin" tooth (no decay or fractures) is painful, sinusitis should be ruled out.
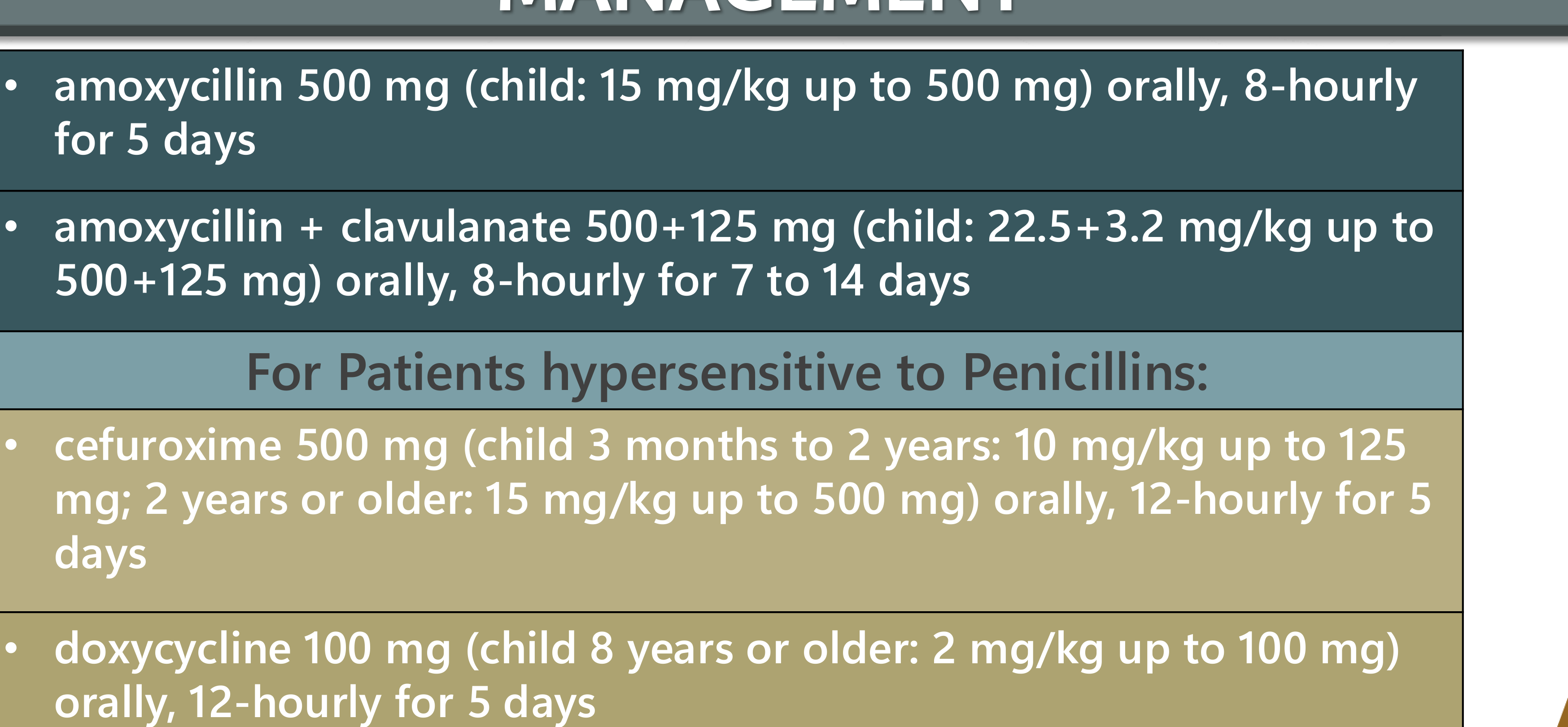
Management of Sinus Origin Pain
- Viral vs. Bacterial: Most cases are viral and do not require antibiotics.
- Treatments: Decongestants, analgesics, nasal sprays/washes, or nasal steroids.
- Antibiotics: Reserved for bacterial etiology (e.g., symptoms lasting >7 days, high fever, or worsening after initial improvement).
Non-Odontogenic Pains of Cardiac Origin
Warning
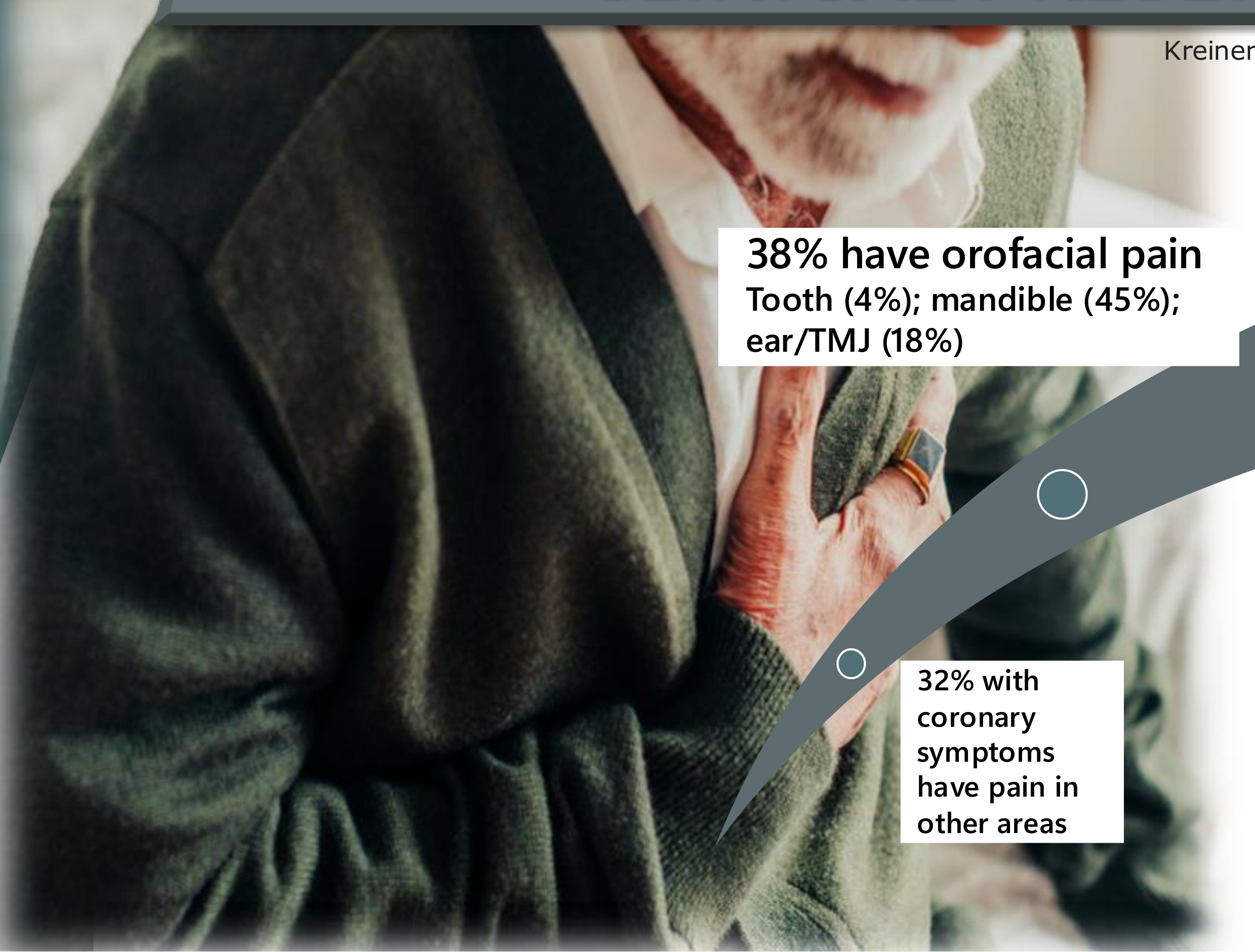
Myocardial ischemia (insufficient oxygen to the heart) can cause referred facial and dental pain.
Clinical Presentation of Cardiac Pain
- Symptoms: Substernal pressure, crushing sensation, radiating to the left neck, shoulder, or arm.
- Associated signs: Dyspnea (shortness of breath), nausea, fatigue, or a sense of "impending doom."
- Triggers: Physical exercise (walking upstairs) or heavy meals.
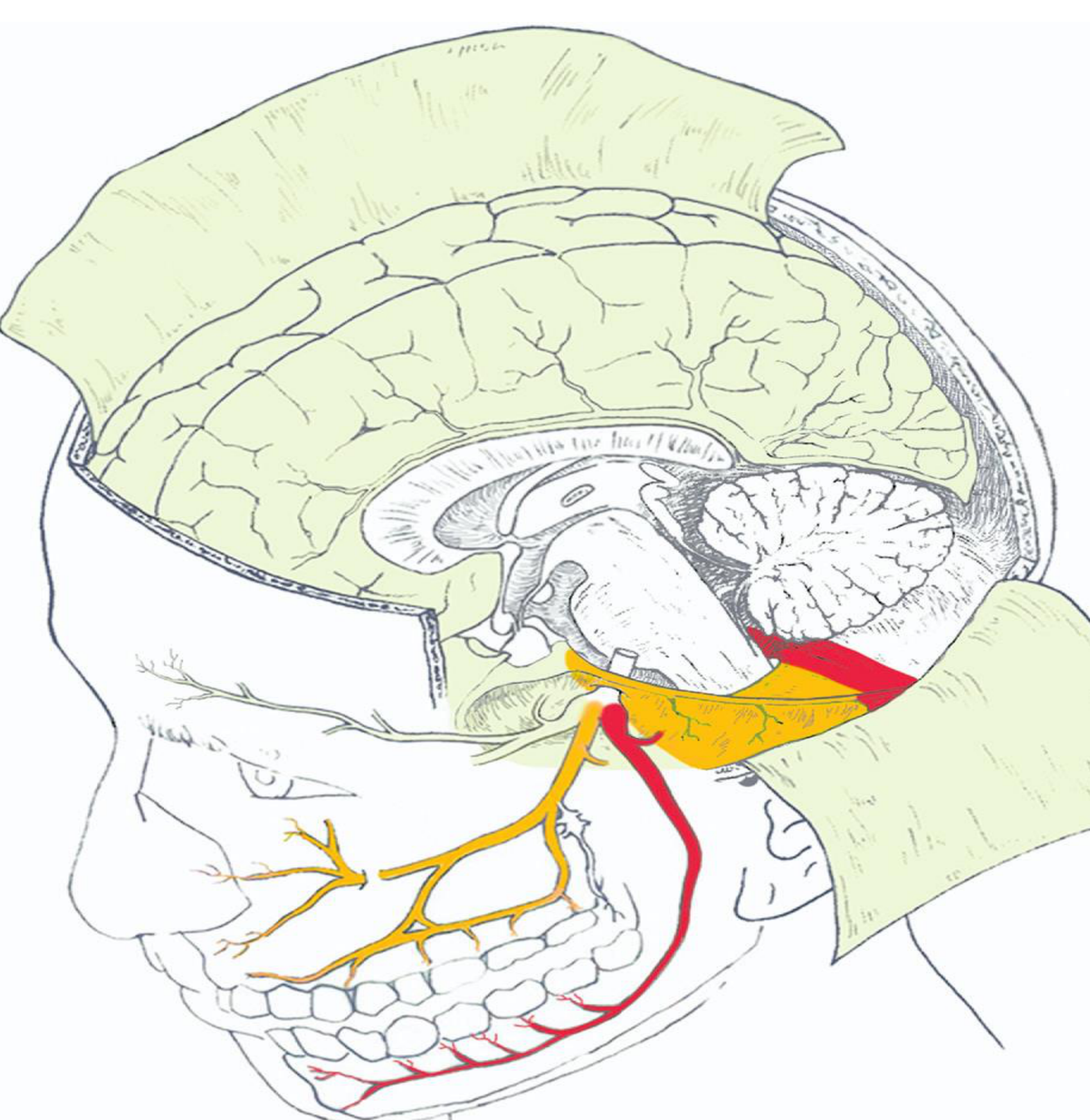
- Mechanism: Convergence of the vagus nerve and trigeminal nerve at the medulla/C1-C3 levels.
- Statistics: 6% of cardiac patients may have solely orofacial symptoms.
 |  |  |
 |  |
Management of Cardiac Pain
- Emergency services should be called immediately.
- Aspirin may be beneficial.
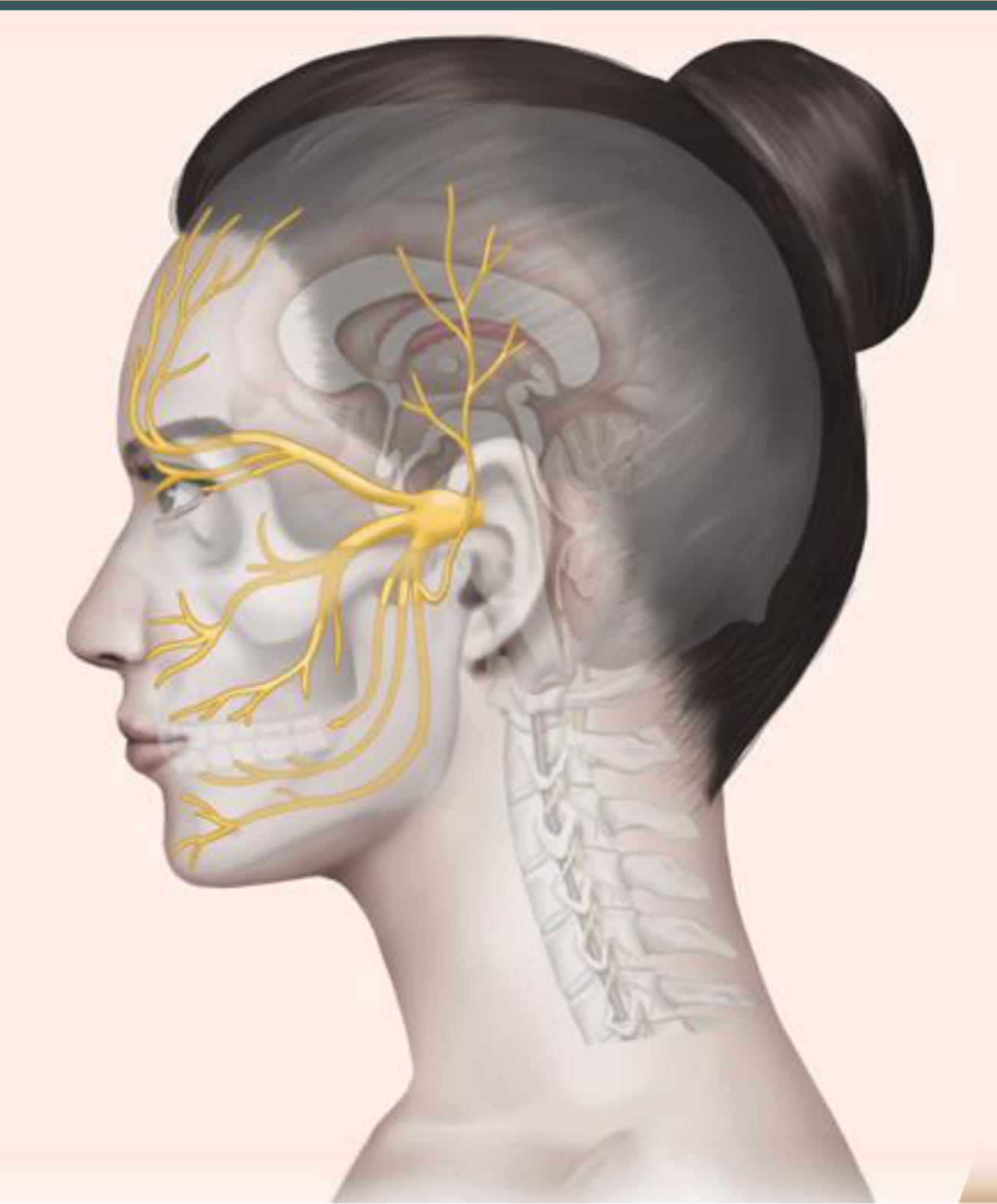
Non-Odontogenic Pains of Neuropathic Origin
Info
Pain arising from a lesion or disease of the somatosensory system.
 |  |  |
 |  |  |
 |
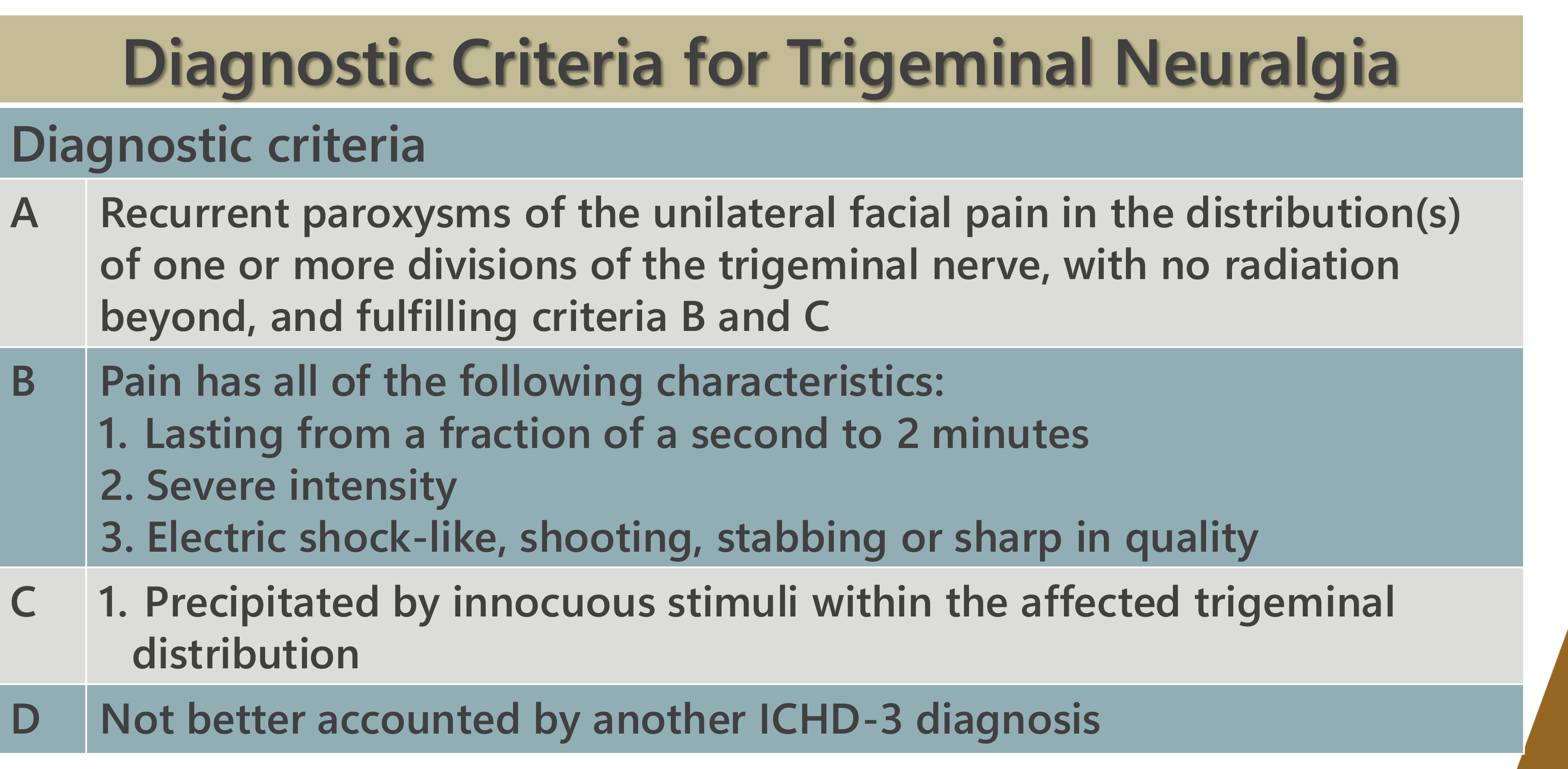
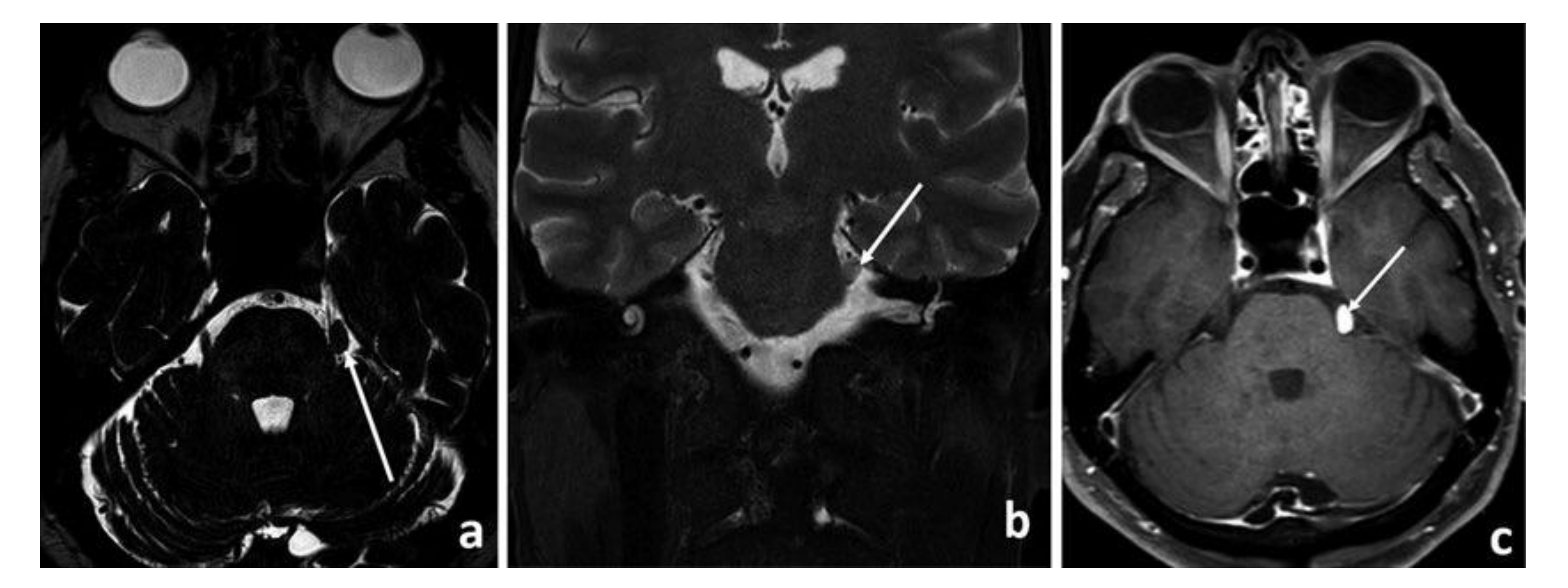
Trigeminal Neuralgia Presentation
- Characteristics: Brief, electric shock-like, stabbing, or shooting pain.
- Duration: Fraction of a second to two minutes.
- Triggers: Precipitated by innocuous stimuli (light touch).
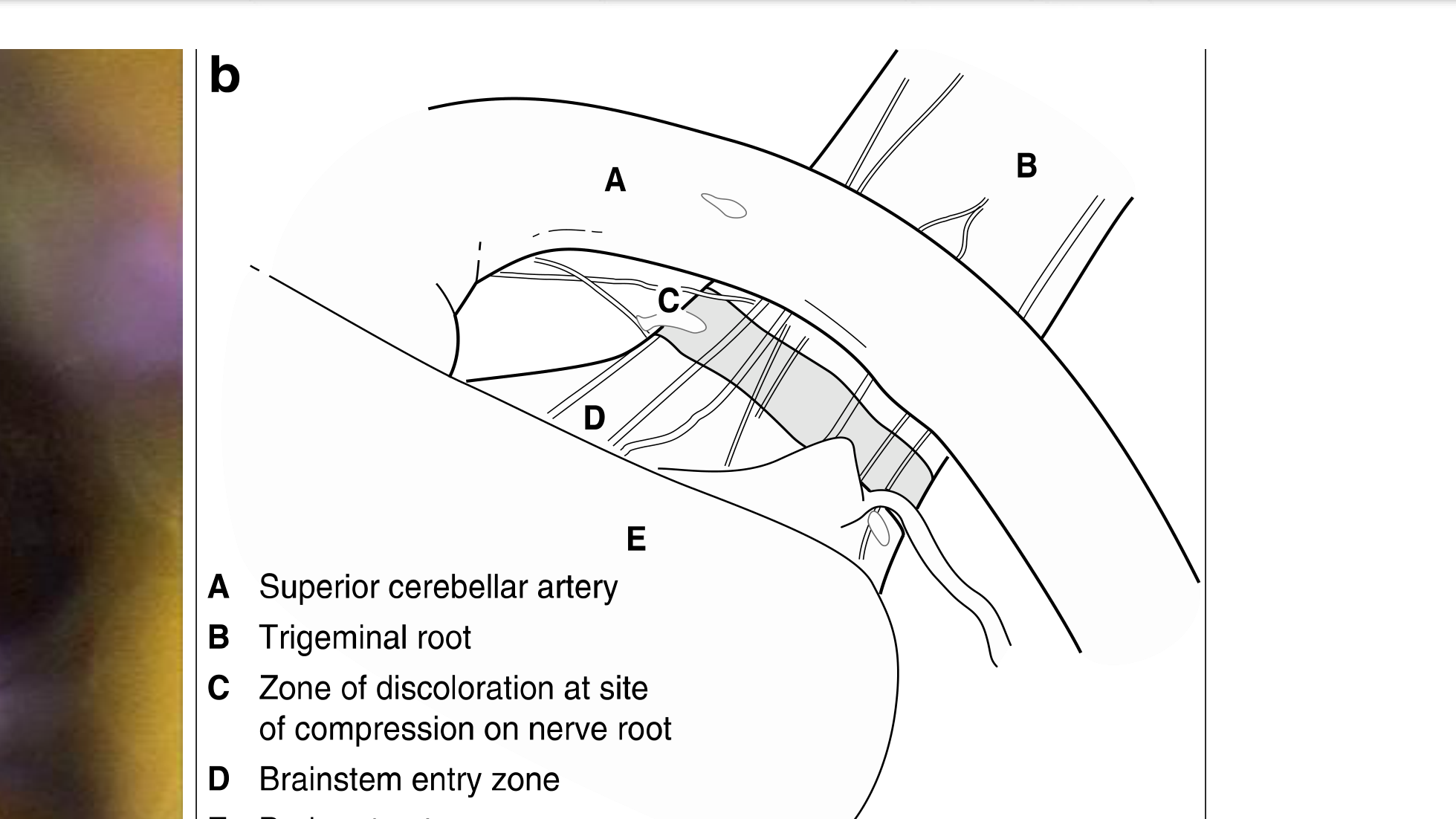
- Etiology: Often caused by neurovascular compression (e.g., superior cerebellar artery impinging on the nerve) or secondary causes like tumors (schwannomas) or Multiple Sclerosis (especially if bilateral).
Management of Trigeminal Neuralgia
- First-line: Carbamazepine (requires blood/liver monitoring).
- Second-line: Gabapentin, Pregabalin, or Baclofen.
- Surgical: Microvascular decompression (using a Teflon wedge), Gamma Knife radiation, or percutaneous procedures.
 |  |
 |
Non-Odontogenic Pains of Psychogenic Origin
Somatic Symptom Disorder Presentation
- Definition: One or more somatic symptoms causing significant distress, with excessive/disproportionate thoughts and anxiety regarding the health concern.
- Clinical Signs: Diffuse, vague pain that frequently changes location (e.g., moves from left to right side). It is inconsistent with physiology and lacks identifiable pathology.
- Risk Factors: History of psychological or childhood trauma, or co-existing conditions like OCD or Bipolar disorder.
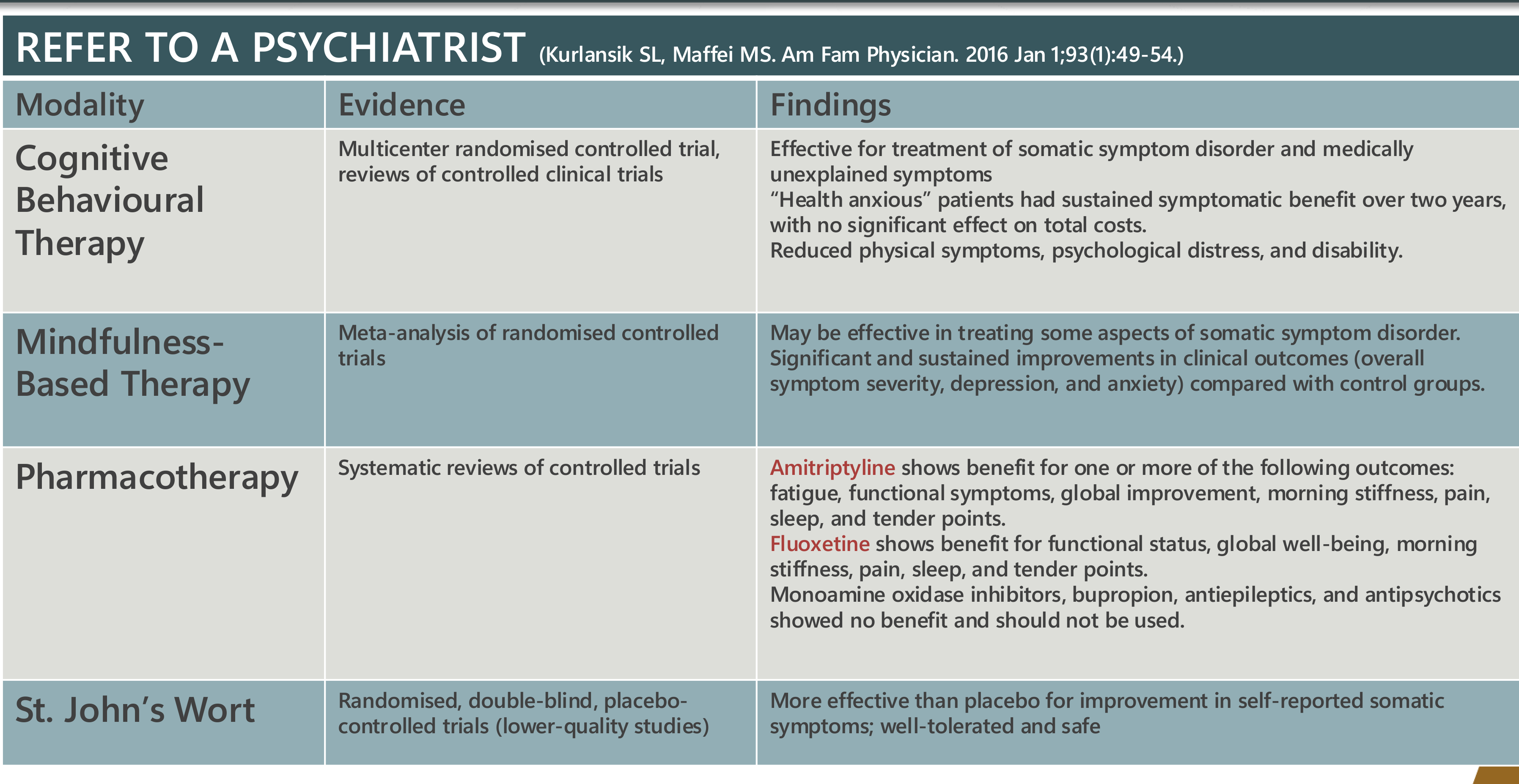
Somatic Symptom Disorder Management
- Approach: Short, regular consultations to prevent "doctor shopping."
- Communication: Believe the patient and show empathy; the pain is real to them even if not odontogenic.
- Referral: Coordination between Oral Medicine and Psychiatry for long-term support (CBT, mindfulness).
Conclusion and Take Home Message
- Toothache does not always mean the source is the tooth.
- The site of pain is not necessarily the source of pain.
- Early diagnosis of non-odontogenic pain prevents unnecessary and expensive dental treatments (like extractions or root canals).
- Other miscellaneous causes include sickle cell disease, giant cell arteritis, and barodontalgia (diving-related pain).
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Post-Traumatic Trigeminal Neuropathic Pain
- Origin: Follows macro-trauma, third molar extractions, root canals (described as a form of “amputation”), or local anesthetic injections.
- Symptoms: Can be “positive” (hyperalgesia/allodynia) or “negative” (anesthesia/numbness).
- Management: Topical neurosensory stents (compounded with amitriptyline, ketamine, etc.), systemic medications (SNRIs, TCAs), or Botox. Surgery usually makes this worse.
Footnotes
-
Original PDF page 1: L32 Non-Odontogenic Toothache, p.1 ↩
-
Original PDF page 4: L32 Non-Odontogenic Toothache, p.4 ↩
-
Original PDF page 2: L32 Non-Odontogenic Toothache, p.2 ↩
-
Original PDF page 3: L32 Non-Odontogenic Toothache, p.3 ↩
-
Original PDF page 6: L32 Non-Odontogenic Toothache, p.6 ↩
-
Original PDF page 5: L32 Non-Odontogenic Toothache, p.5 ↩
-
Original PDF page 7: L32 Non-Odontogenic Toothache, p.7 ↩
-
Original PDF page 10: L32 Non-Odontogenic Toothache, p.10 ↩
-
Original PDF page 12: L32 Non-Odontogenic Toothache, p.12 ↩
-
Original PDF page 8: L32 Non-Odontogenic Toothache, p.8 ↩
-
Original PDF page 9: L32 Non-Odontogenic Toothache, p.9 ↩
-
Original PDF page 11: L32 Non-Odontogenic Toothache, p.11 ↩
-
Original PDF page 13: L32 Non-Odontogenic Toothache, p.13 ↩
-
Original PDF page 14: L32 Non-Odontogenic Toothache, p.14 ↩
-
Original PDF page 16: L32 Non-Odontogenic Toothache, p.16 ↩
-
Original PDF page 17: L32 Non-Odontogenic Toothache, p.17 ↩
-
Original PDF page 19: L32 Non-Odontogenic Toothache, p.19 ↩
-
Original PDF page 15: L32 Non-Odontogenic Toothache, p.15 ↩
-
Original PDF page 18: L32 Non-Odontogenic Toothache, p.18 ↩
-
Original PDF page 21: L32 Non-Odontogenic Toothache, p.21 ↩
-
Original PDF page 20: L32 Non-Odontogenic Toothache, p.20 ↩
-
Original PDF page 23: L32 Non-Odontogenic Toothache, p.23 ↩
-
Original PDF page 22: L32 Non-Odontogenic Toothache, p.22 ↩
-
Original PDF page 24: L32 Non-Odontogenic Toothache, p.24 ↩
-
Original PDF page 25: L32 Non-Odontogenic Toothache, p.25 ↩
-
Original PDF page 26: L32 Non-Odontogenic Toothache, p.26 ↩
-
Original PDF page 27: L32 Non-Odontogenic Toothache, p.27 ↩
-
Original PDF page 28: L32 Non-Odontogenic Toothache, p.28 ↩
-
Original PDF page 29: L32 Non-Odontogenic Toothache, p.29 ↩
-
Original PDF page 30: L32 Non-Odontogenic Toothache, p.30 ↩