Oral Appliance Therapy for Snoring and Obstructive Sleep Apnoea1
Ramesh Balasubramaniam OAM
DENT5310
Orofacial Pain and Dental Sleep Medicine Module 1st May 2026
Professional Affiliations2
- Ramesh Balasubramaniam OAM
- Associate Professor
- Discipline Lead in Oral Medicine
- UWA Dental School
- The University of Western Australia
Conflict of Interest Statement
Neither I nor my immediate family have any financial interests that would create a conflict of interest or restrict my independent judgment with regard to the content of this presentation.
Presentation Agenda3
- Role of Dentistry in Sleep Medicine
- Screening for Sleep Disordered Breathing
- Oral Appliance Therapy for Sleep Disordered Breathing
- Take Home Message
- Clinical practice and implementation
- Oral appliance therapy (OAT)
Presentation Flow4
- Role of Dentistry in Sleep Medicine
- Screening for Sleep Disordered Breathing
- Oral Appliance Therapy for Sleep Disordered Breathing
- Take Home Message

Role of Dentistry in Sleep Medicine
Core Clinical Areas5
Dental sleep medicine encompasses the management and study of several conditions that intersect dental practice and sleep health:
-
Primary focus includes snoring, sleep apnoea, and sleep bruxism.
-
Associated areas involve pain management, dry mouth (xerostomia) resulting from mouth breathing, and GERD's effects on oral health.
-
Snoring and Obstructive Sleep Apnoea
-
Sleep Bruxism
-
Orofacial Pain and Sleep
-
Xerostomia
-
Gastro-oesophageal reflux disease
Scope of Practice and Discipline Overview
Discipline Definition
The discipline was formally described by Lavigne et al. (1999) in the publication “Sleep disorders and the dental patient: an overview.”
- The term "Dental Sleep Medicine" was specifically coined by Gilles Lavigne in 1999 to describe this role.
International Classification of Sleep Disorders (3rd Ed)6
The American Academy of Sleep Medicine identifies 60 diagnoses across 7 major categories:
- Sleep-related breathing disorders
- Sleep-related movement disorders
- Central disorders of hypersomnia
- Insomnia
- Parasomnias
- Circadian rhythm sleep-wake disorders
- Other sleep disorders
Clinical Focus
Sleep medicine is a complex medical specialty primarily managed by respiratory physicians. Dentists typically focus on a small subset: Obstructive Sleep Apnoea (OSA), sleep-disordered breathing, and sleep bruxism.

Professional Responsibilities and Scope
Dental practitioners operating within this field must adhere to the following professional standards:
- Stay within the defined scope of practice for dental practitioners.
- Engage in ongoing education and training specifically in Dental Sleep Medicine.
- Communicate and collaborate effectively with medical practitioners.
- Advanced training is available, such as fellowships through the Australasian Sleep Association.
- Scope of practice is determined by individual training and competence; dentists should refer to specialists when a case exceeds their comfort level (e.g., orthognathic surgery or prescribing specific medical weight-loss drugs).
Presentation Agenda7
-
Role of Dentistry in Sleep Medicine
-
Screening for Sleep Disordered Breathing
-
Oral Appliance Therapy for Sleep Disordered Breathing
-
Take Home Message
- Mid-face deficiency

Screening for Sleep Disordered Breathing8
THE DENTAL PERSPECTIVE!!!

Clinical Screening and Medical History
Medical History9
- Snoring
- Witnessed Apnoea
- Tiredness
- Comorbidities
- Hypertension
- Diabetes
- Depression
- Obesi - Cardiovascular disease - History of strokety
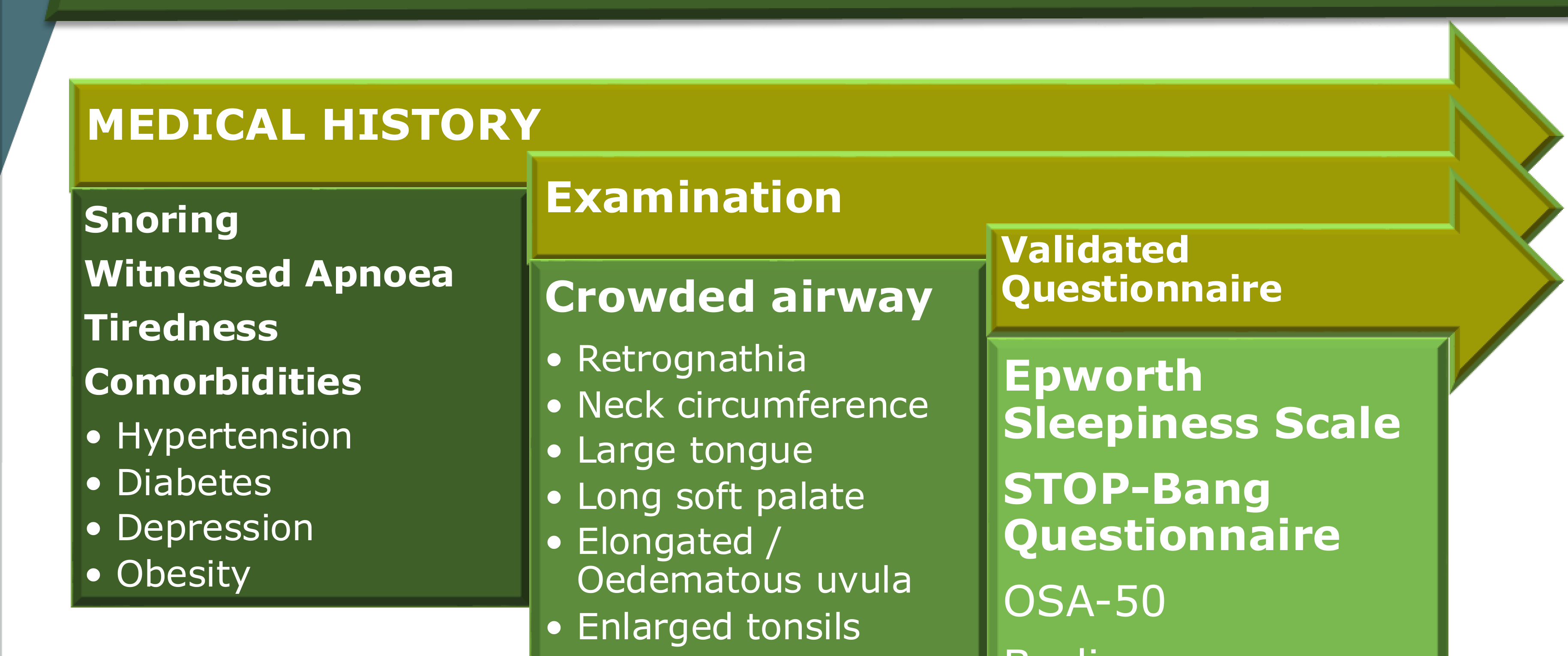
Clinical Examination
- Crowded airway
- Retrognathia
- Neck circumference
- Large tongue
- Long soft palate
- Elongated / Oedematous uvula
- Enlarged tonsils
- Enlarged "kissing" tonsils
- Dangling uvula
Validated Questionnaires
- Epworth Sleepiness Scale
- STOP-Bang Questionnaire
- OSA-50
- Berlin Questionnaire
Validated Questionnaires
Epworth Sleepiness Scale (ESS)10
Origin
The Epworth Sleepiness Scale was developed in Australia.
How likely are you to nod off or fall asleep in the following situations, in contrast to feeling just tired? This refers to your usual way of life in recent time.
Even if you haven’t done some of these things recently, try to work out how they would have affected you. It is important that you answer each question as best you can.
Scoring Scale:
- 0 = Would never nod off
- 1 = Slight chance of nodding off
- 2 = Moderate chance of nodding off
- 3 = High chance of nodding off
Situations:
- Sitting and reading
- Watching TV
- Sitting, inactive, in a public place (e.g., in a meeting, theater, or dinner event)
- As a passenger in a car for an hour or more without stopping for a break
- Lying down to rest when circumstances permit
- Sitting and talking to someone
- Sitting quietly after a meal without alcohol
- In a car, while stopped for a few minutes in traffic or at a light
Results Interpretation: Add up your points to get your total score.
A score of 10 or greater raises concern: you may need to get more sleep, improve your sleep practices, or seek medical attention to determine why you are sleepy.

STOP-BANG Questionnaire11
- Snoring? Do you Snore Loudly (loud enough to be heard through closed doors or your bed-partner elbows you for snoring at night)?
- Tired? Do you often feel Tired, Fatigues, or Sleepy during the daytime (such as falling asleep during driving)?
- Observed? Has anyone Observed you Stop Breathing or Choking/Gasping during your sleep?
- Key Questions: Does the patient snore? Has anyone observed them gasping or snorting for breath? Do they wake up tired or fall asleep during sedentary activities?
- Pressure? Do you have or are being treated for High Blood Pressure?
- Body Mass Index more than 35kg/m2?
- Age older than 50 years old?
- Neck size large? (Measured around Adams apple) For male, is your shirt collar 17 inches/43 cm or larger?
- Gender = Male?
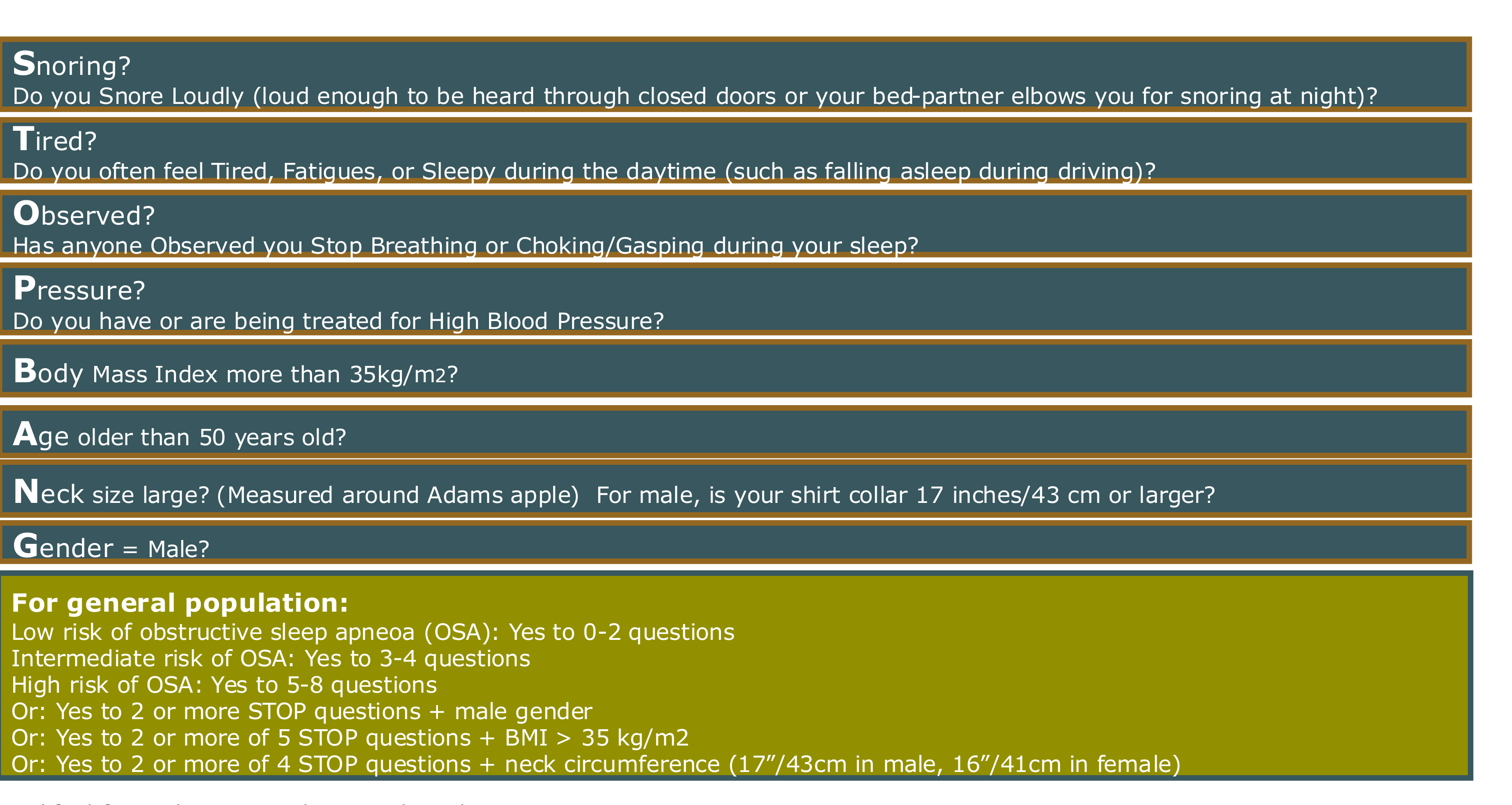
Risk Assessment Scoring
For general population:
- Low risk of obstructive sleep apneoa (OSA): Yes to 0-2 questions
- Intermediate risk of OSA: Yes to 3-4 questions
- High risk of OSA: Yes to 5-8 questions
High Risk Criteria Alternatives:
- Yes to 2 or more STOP questions + male gender
- Yes to 2 or more of 5 STOP questions + BMI > 35 kg/m2
- Yes to 2 or more of 4 STOP questions + neck circumference (17″/43cm in male, 16″/41cm in female)
Wearable Device Performance Comparison12
| Device | Sleep vs Wake Sensitivity | Stage Classification Sensitivity* | Precision / Bias Notes | Comments & Limitations |
|---|---|---|---|---|
| Oura Ring Gen 3 | ≥95% for sleep detection | 76.0-79.5% sensitivity across stages (light/deep/REM) | Very close to PSG estimates — no significant overestimation / underestimation of wake, light, deep, or REM | Best performers in head-to-head comparisons. But tested in healthy adults, single night. |
| Fitbit Sense 2 | ≥95% for sleep detection | 61.7-78% sensitivity across stages | Overestimate light sleep by ≈18mins. Underestimate deep sleep by ≈15 mins. | Good for overall sleep vs wake. Stage estimates show systematic bias. |
| Apple Watch Series 8 | ≥95% for sleep detection | 50.5-86.1% sensitivity (wider spread) | Underestimate wake by ~7mins. Underestimate deep sleep by ~43mins. Overestimate light sleep by ~45mins. | More variability and bias in stage estimates. Reasonably good at distinguishing sleep vs wake. |
Clinical Utility of Wearables
Consumer devices like the Oura ring and Apple Watch are becoming increasingly useful for screening, though they are not yet replacements for clinical diagnostics.

Clinical Workflow and Objectives13
- Role of Dentistry in Sleep Medicine
- Screening for Sleep Disordered Breathing
- Oral Appliance Therapy for Sleep Disordered Breathing
- Take Home Message

Definitions and Diagnostics
Clinical Definitions14
Key Definitions in Sleep Medicine
- Snoring: Sound generated by vibration of the oropharyngeal tissues during sleep that typically occurs with inspiration.
- Hypopnoea: Reduction of airflow (30-50%) and/or effort with associated reduction in SaO₂ (3-4%) and/or arousal from sleep.
- Apnoea: Cessation of airflow for ≥10 seconds.
- Obstructive Sleep Apnoea: Repetitive episodes of complete or partial airway obstruction during sleep resulting in the cessation of airflow despite continuing respiratory efforts.
Imagine a baby sleeping peacefully, dreaming of the future. The voice of a sleeping child is like a lullaby, soft and gentle.
Comparative Sound Levels (Decibels)15
- Painful Acoustic Trauma (140 dB): Shotgun blast
- Extremely Loud:
- 130 dB: Jet engine 100 feet away
- 120 dB: Rock concert
- 110 dB: Car horn, snowblower
- 100 dB: Blow dryer, subway, helicopter, chainsaw
- Very Loud:
- 90 dB: Motorcycle, lawn mower, convertible ride on highway
- Loud:
- 80 dB: Factory, noisy restaurant, vacuum, screaming child
- 70 dB: Car, alarm clock, city traffic
- Moderate:
- 60 dB: Conversation, dishwasher
- Faint:
- 50 dB: Moderate rainfall
- 40 dB: Refrigerator
- 30 dB: Whisper, library
- 20 dB: Watch ticking
Snoring Intensity
The highest recorded snoring level is 87.5 decibels, which is comparable to the noise levels of a factory, noisy restaurant, or lawnmower.
 |  |
 |
Signs and Symptoms of Obstructive Sleep Apnoea
Common Clinical Presentations16
- Snoring
- Daytime sleepiness
- Gasping / choking sensation
- Non-restorative sleep
- Poor memory
- Decrease concentration
- Dry mouth
- Morning headaches
- Morning headaches are typically hypoxia-related.
- Restless sleep

Comorbidities and Associated Conditions17
- Reflux
- Low mood & depression
- Insomnia
- Libido & erectile dysfunction
- Nocturia
- Bed-wetting (nocturnal enuresis).
- Personality changes
- Relationship and work problems
- Nocturnal angina or palpitations
- Vivid dreams

Health Risks and Odds Ratios18
| Effect | Magnitude Odds ratio (95% CI) | Study |
|---|---|---|
| Cardiovascular | ||
| Incident hypertension | 2.89 (1.46-5.64) | Peppard et al. (2000) |
| Prevalent coronary artery disease | 1.27 (0.99-1.62) | Shahar et al. (2001) |
| Incident stroke | 3.08 (0.74-12.81) | Arzt et al (2005) |
| Prevalent congestive heart disease | 2.38 (1.22-4.62) | Shahar et al. (2001) |
| Metabolic | ||
| Prevalent impaired fasting glucose | 1.35 (1.04-1.76) | Stamatakis et al. (2008) |
| Prevalent diabetes | 2.3 (1.28-4.11) | Reichmuth et al. (2005) |
| Neurocognitive | ||
| Motor vehicle accidents | 7.2 (2.4-21.8) | Teran-Santos et al. (1999) |
| Occupational accidents | 2.2 (1.3-3.8) | Lindberg et al. (2001) |
| Incident depression | 2.6 (1.7-3.9) | Peppard et al. (2006) |
| Mortality | ||
| All cases (Hazard ratio) | 3.0 to 4.4 | Marshall et al. (2008); Young et al (2008) |
| Cardiovascular | 2.87 (1.17-7.51) | Marin et al. (2005) |
- Untreated sleep apnoea is associated with a 52% increase in cardiovascular mortality.

Diagnostic Testing and Polysomnography
Physical Measurements in Polysomnography19
- Brain waves: EEG
- Eye movements: EOG
- Leg and jaw movements: EMG
- Heart rate and rhythm: ECG
- Air movement through nose/mouth: Thermistor, CO2
- Chest/abdomen movement: Strain gauges
- Blood SaO2: Pulse oximeter
 |  |
Ambulatory Monitoring Classifications20
| Type | Number of Channels |
|---|---|
| II | Similar to Type I but no video recording |
| III | 2 - 4 Channels |
| IV | 1 Channel |

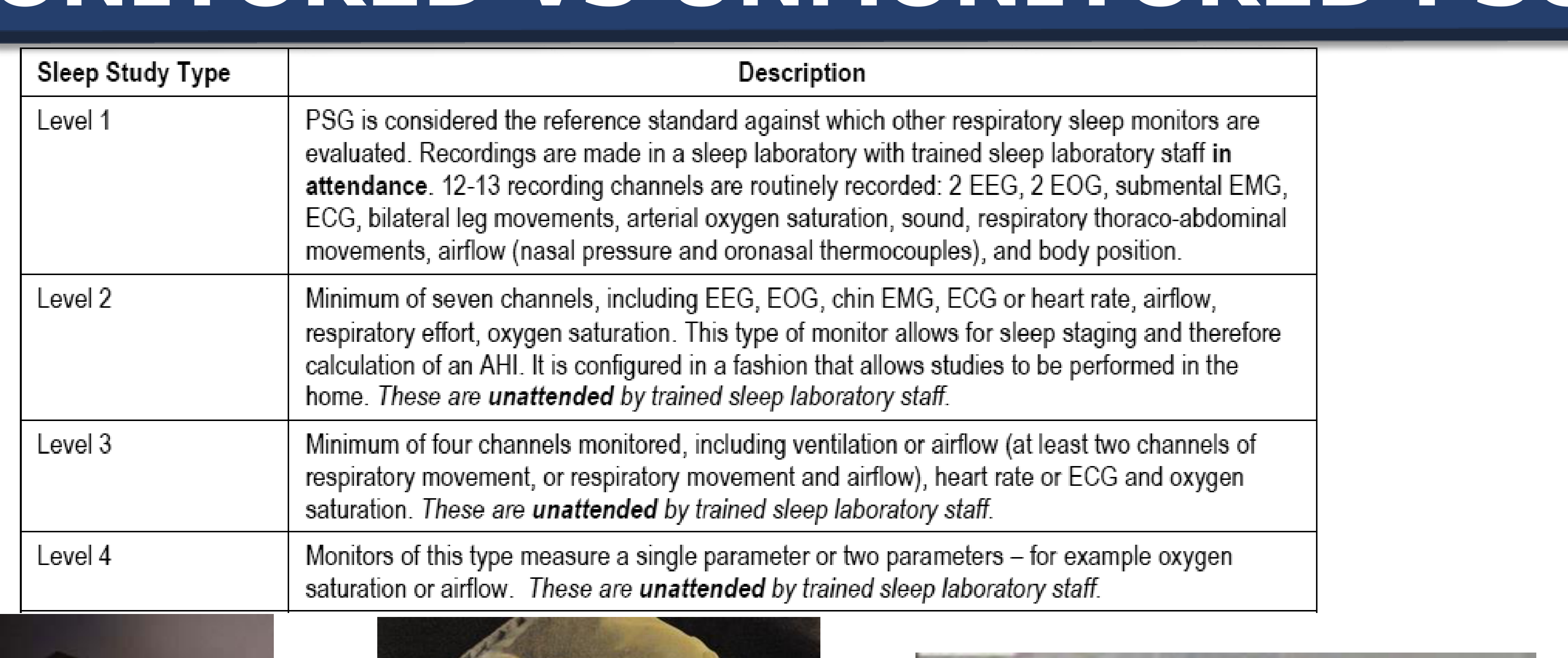
Comparison of Sleep Study Levels21
- Level 1: PSG reference standard. Recorded in a sleep laboratory with trained staff in attendance. Includes 12-13 channels: 2 EEG, 2 EOG, submental EMG, ECG, bilateral leg movements, arterial oxygen saturation, sound, respiratory thoraco-abdominal movements, airflow (nasal pressure and oronasal thermocouples), and body position.
- Level 2: Minimum of seven channels (EEG, EOG, chin EMG, ECG/heart rate, airflow, respiratory effort, oxygen saturation). Allows for sleep staging and AHI calculation. Performed unattended in the home.
- Level 3: Minimum of four channels (ventilation/airflow, heart rate/ECG, and oxygen saturation). Performed unattended in the home.
- These devices are often found in pharmacies and measure fewer channels than Level 2 studies.
- Level 4: Measures a single parameter or two parameters (e.g., oxygen saturation or airflow). Performed unattended in the home.
- Basic screening that sometimes utilizes just a wrist-worn device.
 |  |
 |  |
Apnoea-Hypopnoea Index (AHI) Calculation22
Formula: AHI = (Number of Apnoeas + Number of Hypopnoeas) / Number Hours of Sleep
Example:
- 25 Apnoeas + 25 Hypopnoeas / 5 Hours Sleep
- AHI: 50 / 5 = 10
Diagnostic Severity Criteria
- Mild: 5-15
- Moderate: 15-30
- Severe: >30
Respiratory Disturbance Index (RDI): The number of apnoeas, hypopnoeas & RERAs per hour.
Polysomnogram Channel Identifiers2324
- C3A2 / A1A2 (EEG)
- EOG
- EMG
- SpO2
- PFlow
- Therm
- Thor
- Abd
- Leg(R) / Leg(L)
- Snore
- Body
- Slumber Sound
POLYSOMNOGRAM
 |  |
 |
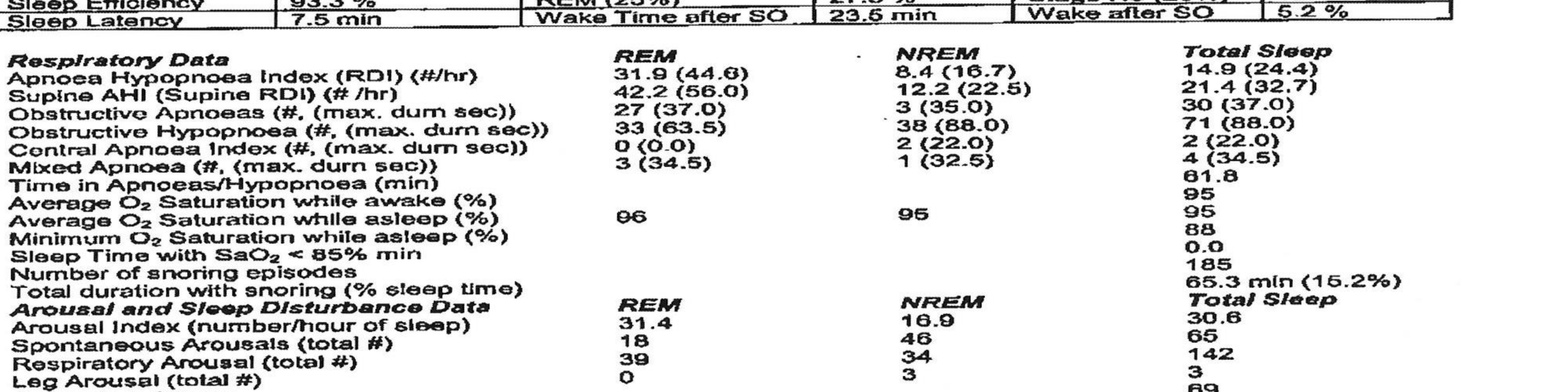
Diagnostic Polysomnography Report25
Patient Metrics:
- Height: 182.5 cm | Weight: 80.5 kg | BMI: 24.17
- Night B.P.: 122/74 | Morn B.P.: 117/84
- Indications: Observed apnoeas, nocturnal epilepsy, palpitations, reflux
Sleep Architecture:
- Sleep Efficiency: 89.3%
- Sleep Latency: 7.5 min
- REM Latency: 77.5 min
- Stages: N1 (1.7%), N2 (58.7%), N3 (12.1%), REM (27.5%)
Respiratory Data:
- Total AHI (RDI): 14.9 (24.4)
- REM AHI (RDI): 31.9 (44.6)
- Supine AHI (RDI): 21.4 (32.7)
- Oxygen Saturation: Average 95%, Minimum 88%
- Snoring: 185 episodes (15.2% of sleep time)
Arousal Data:
- Arousal Index: 20.6 /hr
- Respiratory Arousals: 142
- Respiratory Awakenings: 17
Clinical Conclusion: Moderate obstructive sleep apnoea/hypopnoea, severe in REM sleep. Recommend MAS therapy or as an alternative nasal CPAP therapy.
 |  |  |
 |  |
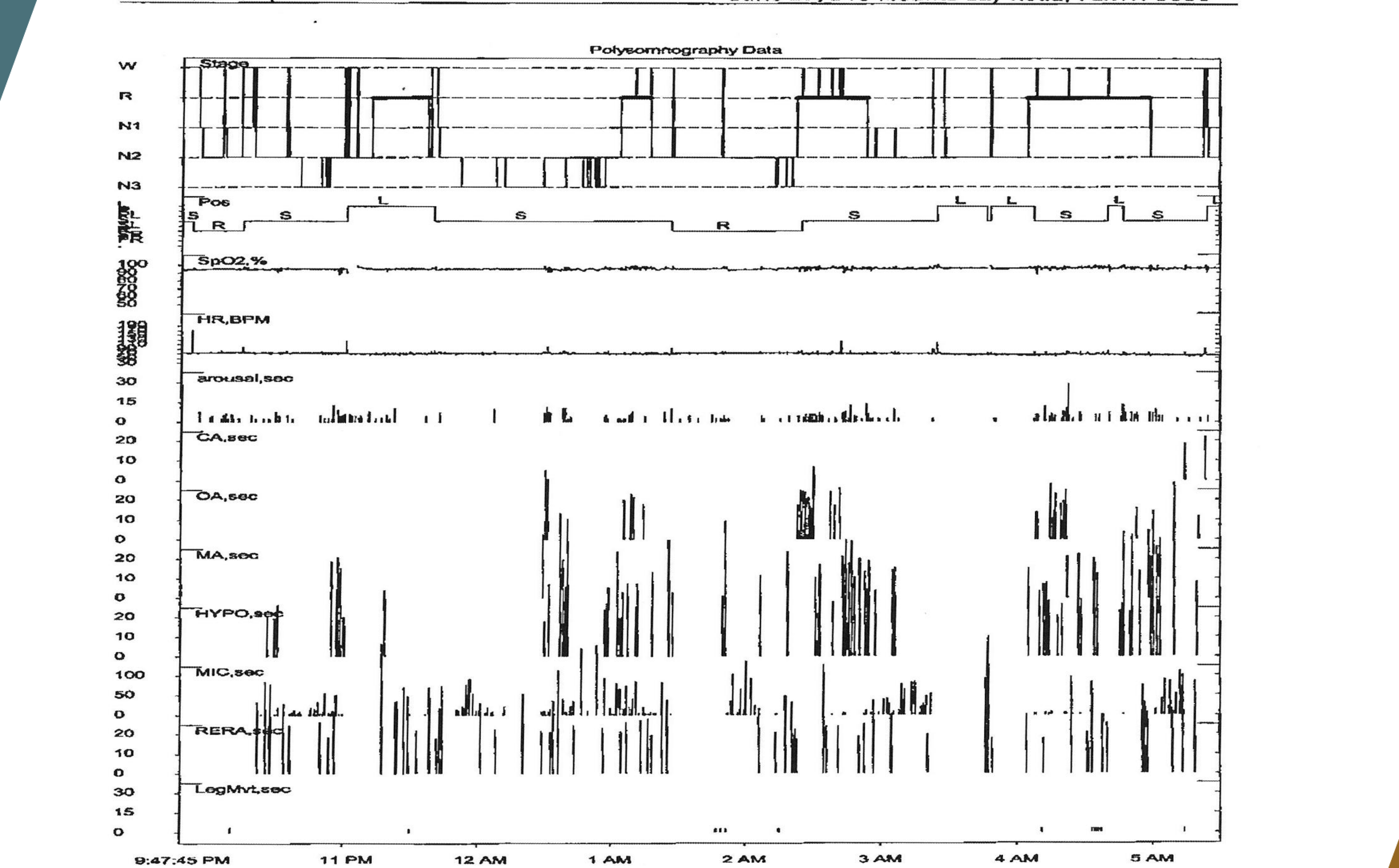
Polysomnography Data Tracing Labels26
- W: Wake
- R: REM
- N1, N2, N3: Sleep Stages
- Pos: Position
- SpO2%: Oxygen Saturation
- HR, BPM: Heart Rate
- arousal, sec: Arousal duration
- OA, sec: Obstructive Apnoea
- MA, sec: Mixed Apnoea
- HYPO, sec: Hypopnoea
- MIC, sec: Microarousal
- RERA, sec: Respiratory Effort Related Arousal
- LogMvt, sec: Leg Movement
Timeframe: 9:47:45 PM to 5:00:00 AM
Oral Appliance Therapy
Categories of Oral Appliances27
 |  |
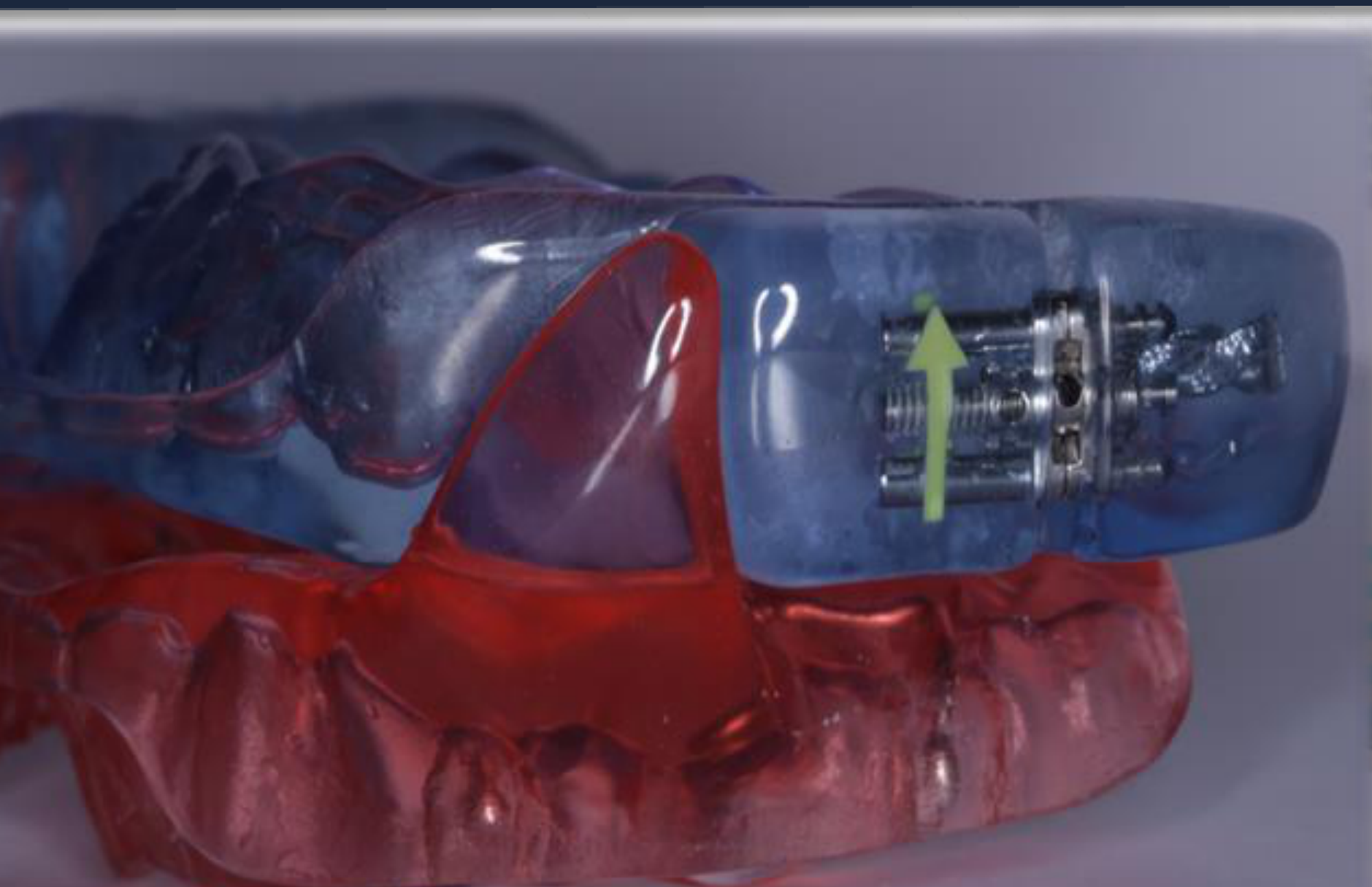
Mechanism of Action and Indications28
- Mandibular advancement appliance
- Tongue retaining device: Designed to engage and hold the tongue in a forward position without affecting the mandible or teeth.
- A silicone bulb that holds the tongue forward using suction; useful for edentulous patients but often uncomfortable.
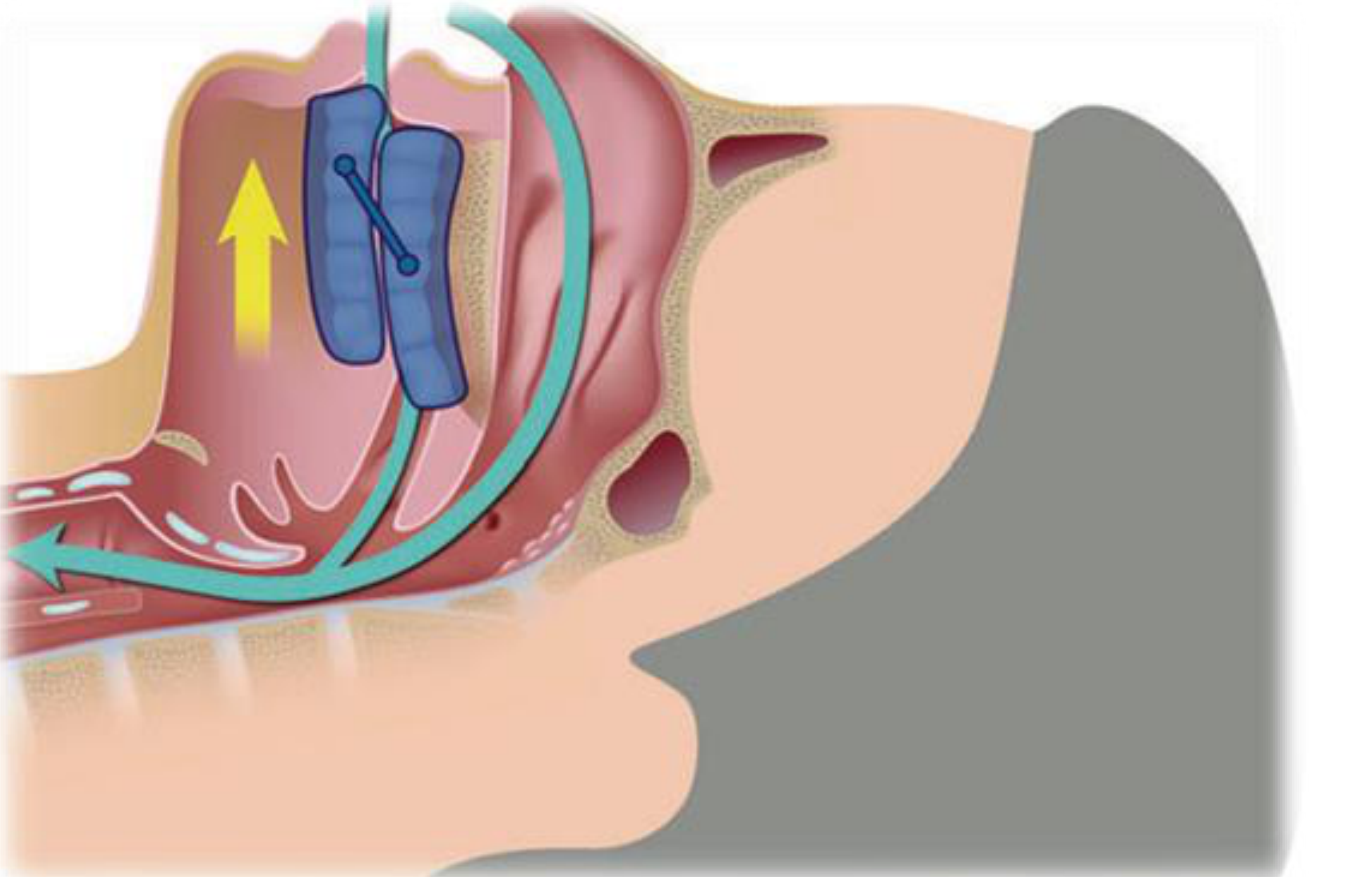
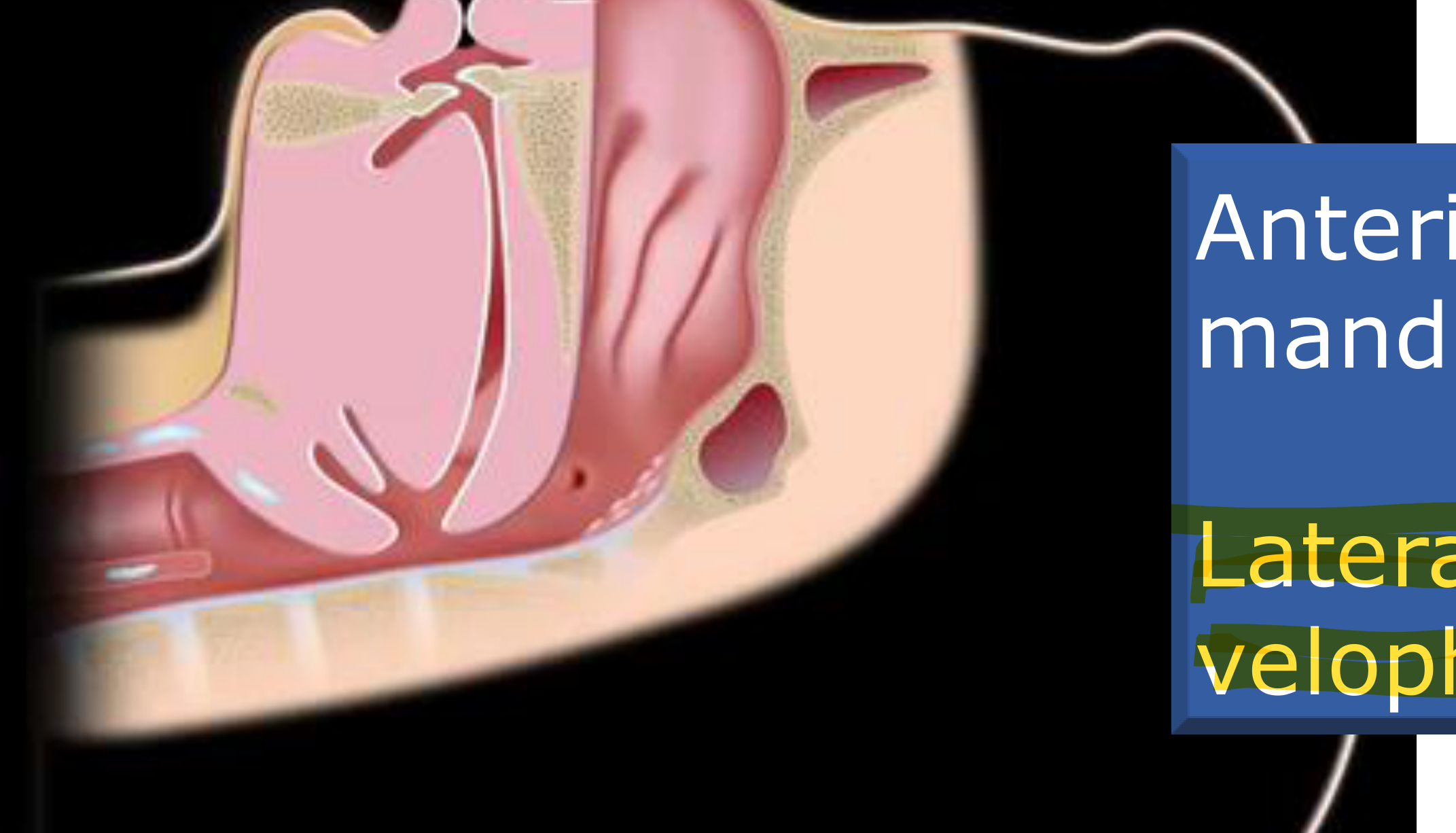
Physiological Effects29
Mandibular advancement appliances increase pharyngeal space and reduce collapsibility, thereby improving pharyngeal airflow through:
- Anterior movement of the mandible and tongue
- Lateral increase in velopharyngeal airway space
- The greatest effect is seen in the velopharyngeal airspace.
Clinical Indications30
- Primary snoring
- Mild to Moderate Obstructive Sleep Apnoea (OSA)
- Severe OSA in patients who have failed a CPAP trial
 |  |
Clinical Efficacy and Health Outcomes
Introduction to Oral Appliance Therapy31
Oral appliance (OA) therapy involves a removable appliance worn over the maxillary and mandibular teeth to advance the mandible during sleep. This treatment is used for snoring and obstructive sleep apnoea (OSA). While various terms exist (mandibular advancement device/splint), OA is the generally accepted generic term in dental sleep medicine.
Prevalence of OSA in Australia
- Primary Snoring: Estimated at 2%.
- Moderate to Severe OSA (AHI ≥15):
- Men (30–49 years): 10%
- Men (50–70 years): 17%
- Women (30–49 years): 3%
- Women (50–70 years): 9%
Untreated OSA is linked to cardiovascular, metabolic, and neurocognitive comorbidities, increasing mortality risk.
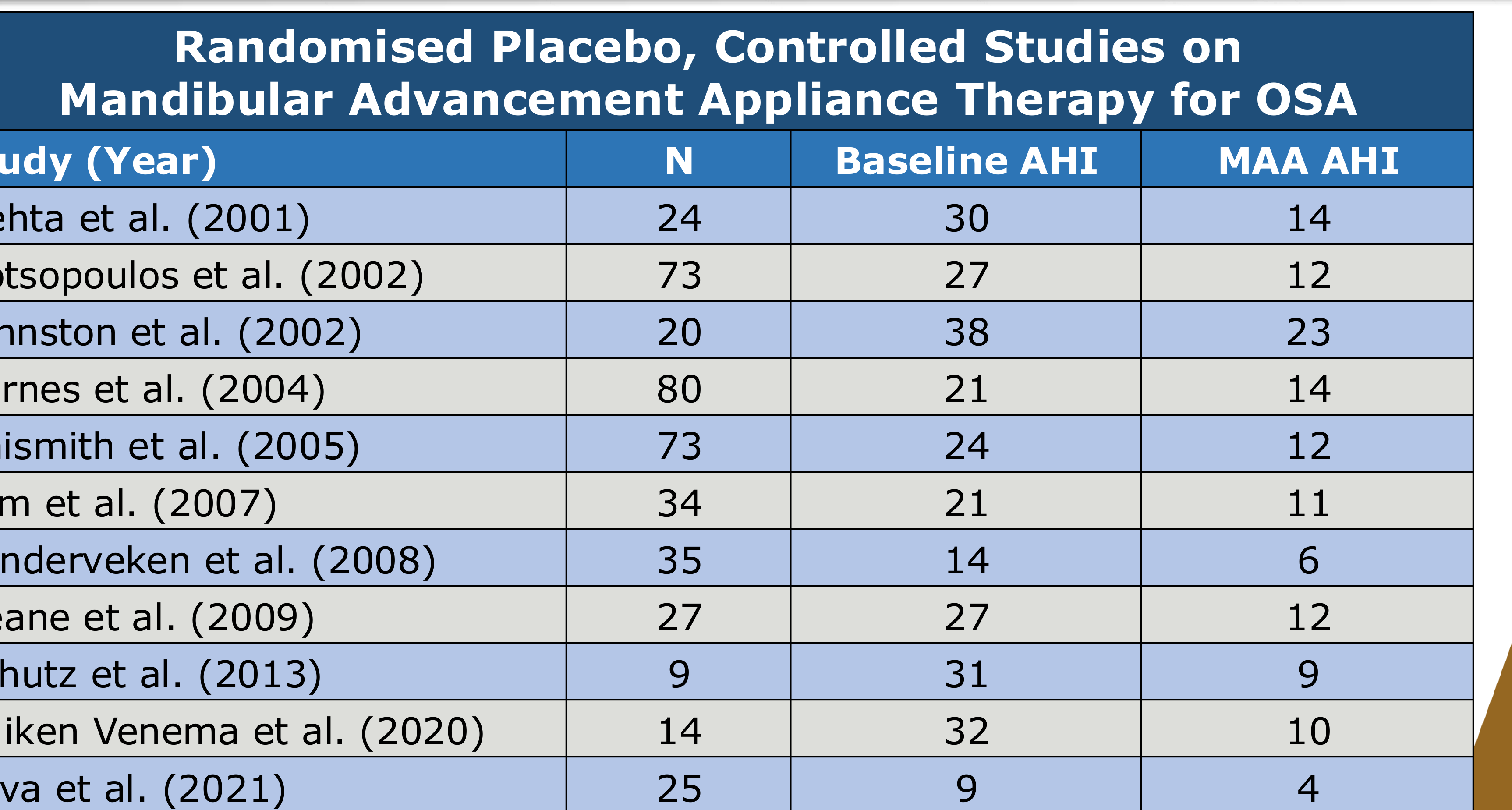
Impact of Mandibular Advancement Appliances (MAA) on AHI32
| Study (Year) | N | Baseline AHI | MAA AHI |
|---|---|---|---|
| Mehta et al. (2001) | 24 | 30 | 14 |
| Gotsopoulos et al. (2002) | 73 | 27 | 12 |
| Johnston et al. (2002) | 20 | 38 | 23 |
| Barnes et al. (2004) | 80 | 21 | 14 |
| Naismith et al. (2005) | 73 | 24 | 12 |
| Lam et al. (2007) | 34 | 21 | 11 |
| Vanderveken et al. (2008) | 35 | 14 | 6 |
| Deane et al. (2009) | 27 | 27 | 12 |
| Schutz et al. (2013) | 9 | 31 | 9 |
| Uniken Venema et al. (2020) | 14 | 32 | 10 |
| Silva et al. (2021) | 25 | 9 | 4 |
Clinical Observation
MAAs rarely "normalize" AHI (below 5) in moderate-to-severe cases, unlike CPAP.
Comparison: Mandibular Advancement Appliance vs. CPAP33
| Reference | N | AHI Base | AHI Appl | AHI CPAP | Comments |
|---|---|---|---|---|---|
| Ferguson et al. (1996) | 19 | 20 | 10 | 10 | 68% satisfied with OAm |
| Clark et al. (1996) | 21 | 34 | 20 | 11 | OAm preferred |
| Ferguson et al. (1997) | 20 | 25 | 14 | 4 | 65% preferred OAm |
| Randerath et al. (2002) | 20 | 18 | 14 | 4 | OAm easier to use |
| Engleman et al. (2002) | 48 | 31 | 15 | 8 | Neither preferred |
| Tan et al. (2002) | 24 | 22 | 8 | 3 | OAm preferred |
| Barnes et al. (2004) | 80 | 21 | 14 | 5 | CPAP more effective but difficult |
| Gagnadoux et al. (2009) | 59 | 34 | 6 | 2 | OAm preferred |
| Phillips et al. (2013) | 132 | 26 | 11 | 5 | OAm preferred |
 |  |
 |
Clinical Effectiveness
- CPAP shows better improvement in AHI compared to Mandibular Advancement Appliances.
- Mandibular Advancement Appliances are generally preferred by patients over CPAP.
- Mean Disease Alleviation (Effectiveness) = Efficacy + Compliance.
Subjective Health Outcomes34
Evidence levels for Mandibular Advancement Appliances:
- Snoring: Excellent (⭐⭐⭐)
- Quality of Life: Excellent (⭐⭐⭐)
- Sleepiness: Good (⭐⭐)
- Mood: Weak (⭐)
- Neurocognitive Function: Weak (⭐)
 |  |  |
 |  |  |
 |
Objective Health Outcomes35
| Health Outcome | Evidence Level |
|---|---|
| Driving Simulator Performance | Good (★★) |
| Sleepiness | Weak (★) |
| Psychomotor Speed | Weak (★) |
| Cardiovascular Outcomes | Weak (★) |
| Mortality | Weak (★) |
 |  |  |
 |  |  |
Treatment Responders vs. Non-Responders36
Clinical Characteristics
- Responders: Younger individuals, lower BMI, female gender, lower prevalence of cardiovascular disease.
- Non-Responders: Older individuals, higher BMI, larger neck circumference, male gender, increased cardiovascular burden.
Anatomical Characteristics
- Responders: Retracted maxilla or mandible, lower facial height, shorter airway length, forward tongue movement.
- Non-Responders: Nasal abnormalities, minimal tongue movement.
Polysomnographic Parameters
- Responders: Low loop gain, low AHI, higher arousal threshold.
- Non-Responders: Lower oxygen desaturations.

Adherence and Compliance37
 |  |
Adherence Patterns38
- Self-reported adherence (7.2h) aligns closely with objective findings (7.1h).
- Usage during the first 20 days is a strong predictor of usage at 60 days.
- Compliance can be measured objectively using embedded microchips that activate via body temperature.
- Early follow-up is critical to ensure long-term adherence.
- Adherence is influenced by patient characteristics, appliance type, psychosocial factors, and side effects.
Effectiveness Formula: Effectiveness (Mean Disease Alleviation) = Efficacy + Compliance
Mandatory disclaimer: The Medical Disclaimer on this website is important for understanding this site. Please read before you start.
 |  |
Side Effects and Complications
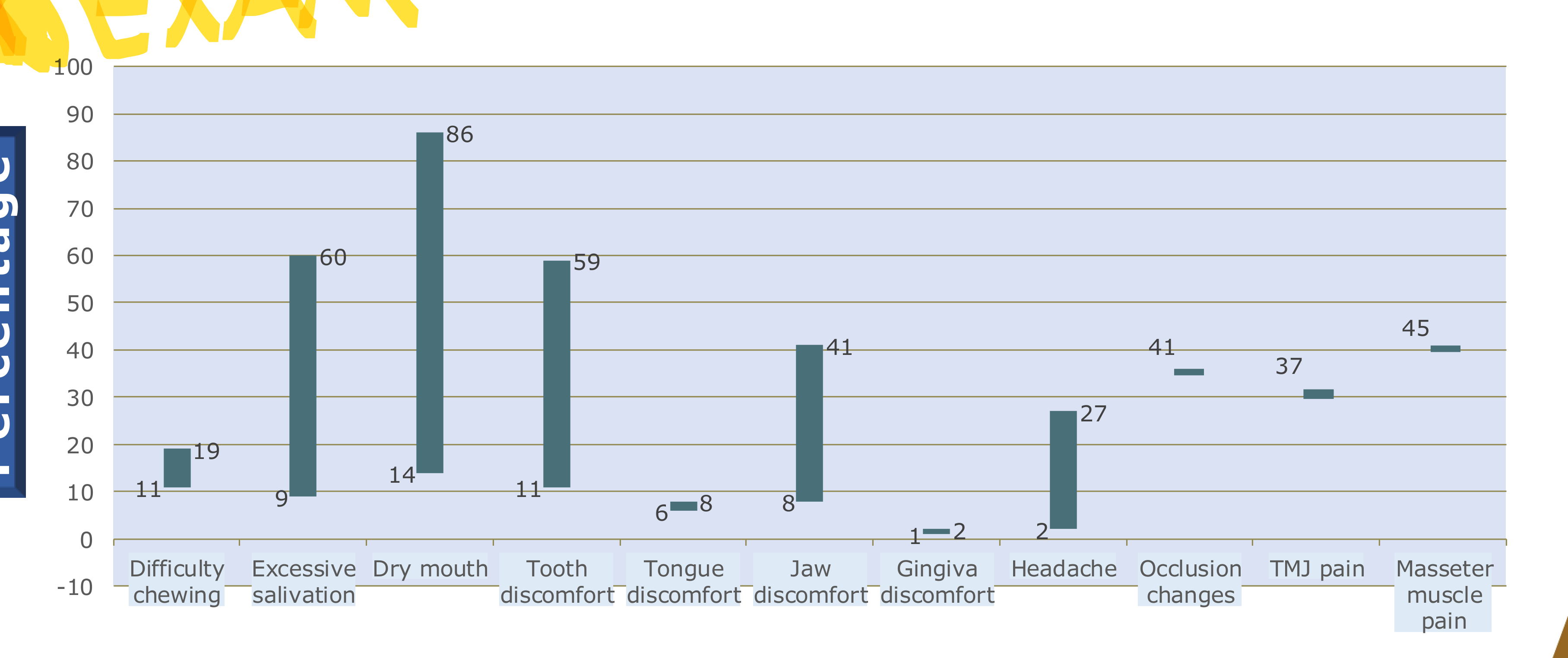
Prevalence of Side Effects39
| Side Effect | Percentage |
|---|---|
| Dry mouth | 86 |
| Excessive salivation | 60 |
| Tooth discomfort | 59 |
| Masseter muscle pain | 45 |
| Jaw discomfort | 41 |
| Occlusion changes | 41 |
| TMJ pain | 37 |
| Headache | 27 |
| Difficulty chewing | 19 |
| Tongue discomfort | 8 |
| Gingiva discomfort | 2 |
Tolerance
Approximately 2% of patients cannot tolerate the appliance due to persistent jaw pain.
Duration of Side Effects40
Short-term
- Dental and craniofacial changes
- Oral, gingiva, or teeth discomfort
- Jaw tenderness / TMD
- Salivation changes (excessive or dry)
Long-term
- Craniofacial Changes: Mandible rotates backwards and anterior facial height increases.
- Dental Changes:
- Decreased overjet, overbite, and mandibular teeth crowding.
- Development of posterior open bite.
Temporomandibular Joint Considerations
TMJ Morphological Observations
In a study of patients treated with Klearway MAA:
- AHI reduction (12.21 to 5.64) was related to the degree of mandibular protrusion.
- Condylar translation with MAA was typically less than or equal to the maximal open position.
- No significant TMJ morphological alterations were observed during a 1-year study period.
Systematic Review Findings
- Mandibular advancement appliances are not an absolute risk for TMD.
- TMD symptoms may occur initially but are typically transient.
- Clinical Management:
- If TMD is present, treat it before starting MAA.
- Chronic TMD is not a contraindication for therapy.
- New onset TMD should be diagnosed and treated promptly.
TMD Symptom Progression
Based on a systematic review of 13 studies:
- Many patients experience a significant reduction in the severity and frequency of TMD symptoms.
- Some patients show no significant changes from baseline.
- Temporary increases in TMJ-related pain may occur in the early follow-up period but usually subside.
Occlusal and Craniofacial Changes
Common Occlusal Changes
- Posterior Open Bite: Altered occlusal contacts.
- Incisor Changes: Decrease in overjet and overbite.
- Positional Changes: Altered position of mandibular canines and molars.
- Interproximal Gaps: Development of spaces between teeth
- Interproximal gaps often act as food traps.
Research Tiers on Overjet and Overbite Changes
Various studies have documented dental changes across different appliance types (Monoblock, TAP, Herbst, Somnomed, Silencor):
- Bondemark (1999)
- Doff et al. (2013)
- Fransson et al. (2004)
- Marklund (2006)
- Wang et al. (2015)
Long-term Case Observation (3 Years)
Comparison of dental alignment from baseline to after 3 years of Mandibular Advancement Appliance therapy.
Short-term Case Observation (3 Months)
Comparison of dental alignment from baseline to after 3 months of Mandibular Advancement Appliance therapy.
Extended Case Observation (5 Years)
Comparison of dental alignment from baseline to after 5 years of Mandibular Advancement Appliance therapy.
Clinical Perspective on Dental Changes
- Therapeutic efficacy for a life-threatening disorder like OSA should supersede the maintenance of baseline craniofacial morphology.
- Discontinuation of therapy due to dental side effects should only be considered if the patient can tolerate another effective treatment modality.
Multidisciplinary Care and Emerging Therapies41
 |  |
Multi-Disciplinary Treatment Protocol42
- Initial Presentation: Patient presents with snoring, apnoeas, or sleepiness.
- Medical Referral: Referred to a sleep physician or GP for PSG or home sleep testing.
- Diagnosis-Based Pathways:
- Snorer (No OSA): Behavioral treatment (weight loss, position) and OAm.
- Mild to Moderate OSA: Choice of OAm or CPAP.
- Severe OSA: CPAP treatment; behavioral treatment.
- Dental Implementation: Clinical assessment, insertion, and titration of OAm.
- Follow-up: Annual review by a dental practitioner
Provider Roles
The sleep physician is the primary provider in the multidisciplinary protocol. .
 |  |
Combination Therapy Study (Aishah A et al. 2023)43
Proof-of-concept study for severe OSA (Baseline AHI: 41.9) using stepwise add-on therapy:
- Step 1: MAA + EPAP + Supine Avoidance (10/20 participants successfully treated).
- Step 2: Add Oxygen (5/20 participants).
- Step 3: Add Medications (Atomoxetine-Oxybutynin) (1/20 participants).
- Step 4: Combination of all above (1/20 participants).
Results: 19/20 participants were successfully treated; 17/20 were treated without requiring CPAP.
 |  |  |
 |  |  |
 |
GIP/GLP-1 Receptor Agonists and OA Therapy44
Obesity-Related OSA Management:
- Sustained weight loss (18-20%) reduces fat deposition around the airway.
- Reduces AHI by an average of 14.45.
- Improves metabolic profiles and reduces systemic inflammation.
Combination Therapy Trends:
- Incretins (weight loss meds) combined with Oral Appliance Therapy are emerging as an alternative for those ceasing CPAP.
- Drugs like Mounjaro (Tirzepatide) and Ozempic are highly effective for weight loss and can significantly reduce OSA severity, sometimes allowing patients to discontinue appliance therapy.
Artificial Intelligence in Dental Sleep Medicine45
AI applications include:
- Diagnosis: Automated sleep studies and risk stratification.
- Personalised Therapy: Predicting responders and optimising appliance design/titration.
- Monitoring: Patient engagement support and big data research.
- Market Impact: Projected AUD >2 billion market in Australia by 2030 with significant time savings for clinicians.
 |  |
Clinical Practice and Implementation
Clinical Workflow46
- History and Clinical Examination (including Imaging).
- Discussion with Patient regarding options.
- Appliance Selection, Side Effects discussion, and Informed Consent.
- Scans and Bite Registration.
- Delivery, Titration, and Follow-up.
Examination and Treatment Planning
Patient History Requirements47
- Chief Complaints: Snoring, tiredness, headache, fatigue, lethargy, drowsiness.
- Screening: Epworth Sleepiness Scale.
- History: Comprehensive medical and dental history, including past treatments
- Document lethargy, past failed treatments such as CPAP or surgery, and medical comorbidities.

Clinical Examination Components48
- Mandibular Function: Mouth opening, lateral movement, and protrusion.
- TMJs & Muscles: Pain, clicking, catching, or locking.
- Occlusion: Classification, midlines, and occlusal contacts.
- Dentition: Missing teeth, crown height, caries, and periodontal health
- Crown heights are specifically evaluated as they are needed for appliance retention.
- Soft Tissue: Tongue, palate, uvula, and tonsils
Contraindications
Contraindications for treatment include severe periodontal disease, mobile teeth, or an extreme gag reflex. .
 |  |
 |  |
Treatment Planning Discussion49
- Determine if the patient is a suitable candidate and discuss other options.
- Explain how MAA works, different designs, and expected effectiveness.
- Review potential side effects and obtain informed consent.
Appliance Selection and Impression Techniques
Appliance Selection50
Determining the most appropriate device for the individual patient. - While no single design is proven superior, most modern appliances are now 3D-printed nylon.
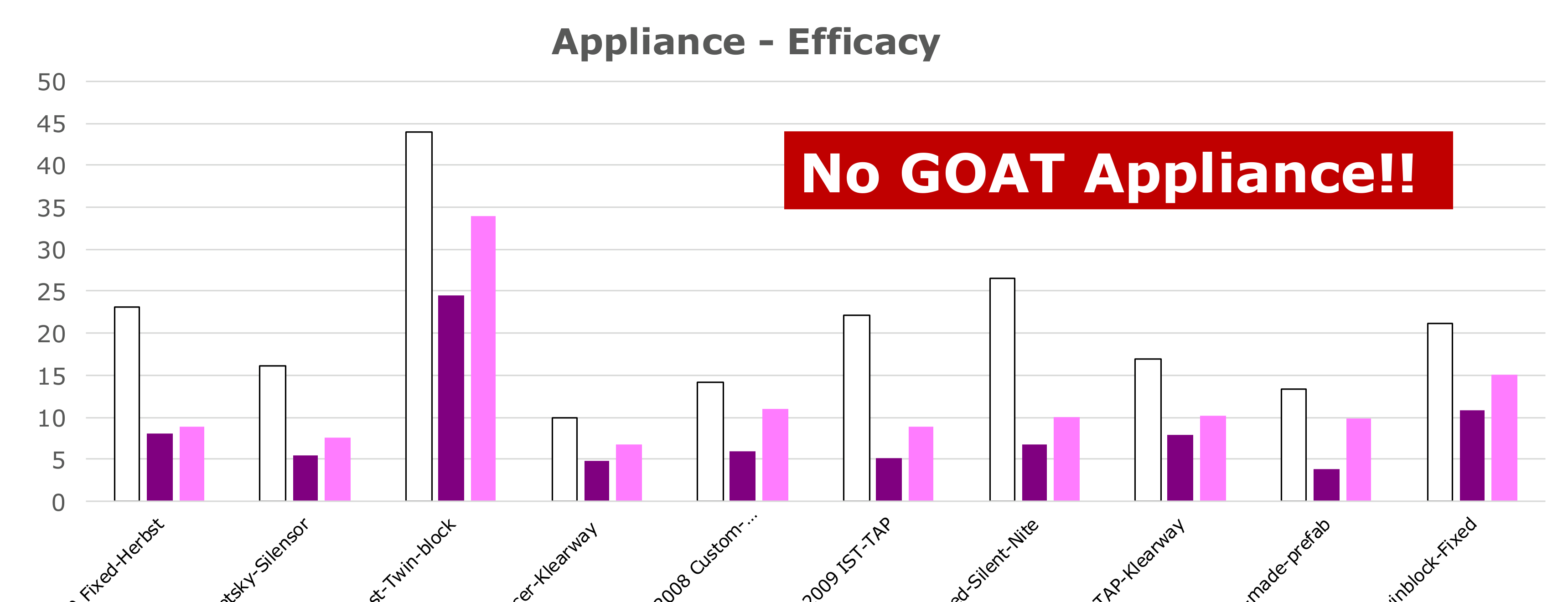
Comparative Efficacy of Appliances51
There is no single “best” appliance; multiple designs show significant AHI reduction:
- Herbst Designs: Reduced AHI from ~23 to ~8 (Bloch 2000).
- TAP Designs: Reduced AHI from ~22 to ~5 (Ghazal 2009).
- Silensor/Klearway: Consistent reductions across various studies.
- Custom vs. Prefab: Custom-made appliances generally show superior AHI reduction (Johal 2017).
Documentation52
- Extraoral and intraoral photography.
- Digital or physical records for appliance fabrication.

Impression Techniques53
Maxillary and Mandibular records can be obtained via:
- Polyvinyl siloxane (PVS) impressions.
- Intraoral digital scans.
 |  |
Bite Registration54
- Protrusive bite registration is typically performed using a George Gauge.
- The George Gauge is used to capture the mandible at 60–70% of its maximum protrusion.

Delivery and Titration Protocols
Fitting and Patient Education55
- Fit Appointment: Ensure the appliance is comfortable and the patient can insert/remove it easily.
- Adjustment Period: Use the first week to habituate before beginning titration.
- Maintenance: Instructions on care (e.g., keeping away from pets).
- Review: Reiterate potential side effects.
Titration Protocol56
Systematic advancement of the appliance to achieve optimal clinical results. - Start titration at 60–70% protrusion. - Gradually advance in 0.5mm increments over 8–12 weeks based on symptom improvement.
Defining Treatment Success57
Subjective Success
- Cessation of snoring.
- Awakening more refreshed.
- Decreased lethargy.
- Meeting patient goals (e.g., lifestyle improvements, partner satisfaction).
Objective Success
- Polysomnography results after the appliance has been optimally titrated.
- The follow-up sleep study should be conducted with the appliance in situ.
 |  |
 |  |
Clinical Workflow Agenda58
- Role of Dentistry in Sleep Medicine
- Screening for Sleep Disordered Breathing
- Oral Appliance Therapy for Sleep Disordered Breathing
- Take Home Message
Conclusion and Take Home Messages59

Key Clinical Considerations60
- Educate and train in Dental Sleep Medicine
- Sleep Medicine is complex beyond snoring and OSA
- Work closely with medical physicians due to the complexity of sleep medicine.
- Dental practitioners may screen for sleep disordered breathing
- Role of dentistry in OSA crucial given the evidence for mandibular advancement appliance therapy
- Mean Disease Alleviation is emerging as the standard for assessing treatment effectiveness
- Overall treatment effectiveness is a product of both clinical efficacy and patient compliance.
- Side effects with mandibular advancement appliance therapy do occur, but manageable!
- Bite changes are often inevitable side effects but remain manageable.
QUESTIONS?
Footnotes
-
Original PDF page 1: L35 Oral Appliance Therapy for Snoring and OSA, p.1 ↩
-
Original PDF page 2: L35 Oral Appliance Therapy for Snoring and OSA, p.2 ↩
-
Original PDF page 3: L35 Oral Appliance Therapy for Snoring and OSA, p.3 ↩
-
Original PDF page 4: L35 Oral Appliance Therapy for Snoring and OSA, p.4 ↩
-
Original PDF page 5: L35 Oral Appliance Therapy for Snoring and OSA, p.5 ↩
-
Original PDF page 6: L35 Oral Appliance Therapy for Snoring and OSA, p.6 ↩
-
Original PDF page 7: L35 Oral Appliance Therapy for Snoring and OSA, p.7 ↩
-
Original PDF page 8: L35 Oral Appliance Therapy for Snoring and OSA, p.8 ↩
-
Original PDF page 9: L35 Oral Appliance Therapy for Snoring and OSA, p.9 ↩
-
Original PDF page 10: L35 Oral Appliance Therapy for Snoring and OSA, p.10 ↩
-
Original PDF page 11: L35 Oral Appliance Therapy for Snoring and OSA, p.11 ↩
-
Original PDF page 12: L35 Oral Appliance Therapy for Snoring and OSA, p.12 ↩
-
Original PDF page 13: L35 Oral Appliance Therapy for Snoring and OSA, p.13 ↩
-
Original PDF page 14: L35 Oral Appliance Therapy for Snoring and OSA, p.14 ↩
-
Original PDF page 15: L35 Oral Appliance Therapy for Snoring and OSA, p.15 ↩
-
Original PDF page 16: L35 Oral Appliance Therapy for Snoring and OSA, p.16 ↩
-
Original PDF page 17: L35 Oral Appliance Therapy for Snoring and OSA, p.17 ↩
-
Original PDF page 18: L35 Oral Appliance Therapy for Snoring and OSA, p.18 ↩
-
Original PDF page 19: L35 Oral Appliance Therapy for Snoring and OSA, p.19 ↩
-
Original PDF page 20: L35 Oral Appliance Therapy for Snoring and OSA, p.20 ↩
-
Original PDF page 21: L35 Oral Appliance Therapy for Snoring and OSA, p.21 ↩
-
Original PDF page 22: L35 Oral Appliance Therapy for Snoring and OSA, p.22 ↩
-
Original PDF page 23: L35 Oral Appliance Therapy for Snoring and OSA, p.23 ↩
-
Original PDF page 24: L35 Oral Appliance Therapy for Snoring and OSA, p.24 ↩
-
Original PDF page 25: L35 Oral Appliance Therapy for Snoring and OSA, p.25 ↩
-
Original PDF page 26: L35 Oral Appliance Therapy for Snoring and OSA, p.26 ↩
-
Original PDF page 27: L35 Oral Appliance Therapy for Snoring and OSA, p.27 ↩
-
Original PDF page 30: L35 Oral Appliance Therapy for Snoring and OSA, p.30 ↩
-
Original PDF page 28: L35 Oral Appliance Therapy for Snoring and OSA, p.28 ↩
-
Original PDF page 29: L35 Oral Appliance Therapy for Snoring and OSA, p.29 ↩
-
Original PDF page 31: L35 Oral Appliance Therapy for Snoring and OSA, p.31 ↩
-
Original PDF page 32: L35 Oral Appliance Therapy for Snoring and OSA, p.32 ↩
-
Original PDF page 33: L35 Oral Appliance Therapy for Snoring and OSA, p.33 ↩
-
Original PDF page 34: L35 Oral Appliance Therapy for Snoring and OSA, p.34 ↩
-
Original PDF page 35: L35 Oral Appliance Therapy for Snoring and OSA, p.35 ↩
-
Original PDF page 36: L35 Oral Appliance Therapy for Snoring and OSA, p.36 ↩
-
Original PDF page 38: L35 Oral Appliance Therapy for Snoring and OSA, p.38 ↩
-
Original PDF page 37: L35 Oral Appliance Therapy for Snoring and OSA, p.37 ↩
-
Original PDF page 39: L35 Oral Appliance Therapy for Snoring and OSA, p.39 ↩
-
Original PDF page 40: L35 Oral Appliance Therapy for Snoring and OSA, p.40 ↩
-
Original PDF page 52: L35 Oral Appliance Therapy for Snoring and OSA, p.52 ↩
-
Original PDF page 50: L35 Oral Appliance Therapy for Snoring and OSA, p.50 ↩
-
Original PDF page 51: L35 Oral Appliance Therapy for Snoring and OSA, p.51 ↩
-
Original PDF page 53: L35 Oral Appliance Therapy for Snoring and OSA, p.53 ↩
-
Original PDF page 54: L35 Oral Appliance Therapy for Snoring and OSA, p.54 ↩
-
Original PDF page 55: L35 Oral Appliance Therapy for Snoring and OSA, p.55 ↩
-
Original PDF page 56: L35 Oral Appliance Therapy for Snoring and OSA, p.56 ↩
-
Original PDF page 57: L35 Oral Appliance Therapy for Snoring and OSA, p.57 ↩
-
Original PDF page 58: L35 Oral Appliance Therapy for Snoring and OSA, p.58 ↩
-
Original PDF page 59: L35 Oral Appliance Therapy for Snoring and OSA, p.59 ↩
-
Original PDF page 60: L35 Oral Appliance Therapy for Snoring and OSA, p.60 ↩
-
Original PDF page 61: L35 Oral Appliance Therapy for Snoring and OSA, p.61 ↩
-
Original PDF page 62: L35 Oral Appliance Therapy for Snoring and OSA, p.62 ↩
-
Original PDF page 63: L35 Oral Appliance Therapy for Snoring and OSA, p.63 ↩
-
Original PDF page 64: L35 Oral Appliance Therapy for Snoring and OSA, p.64 ↩
-
Original PDF page 65: L35 Oral Appliance Therapy for Snoring and OSA, p.65 ↩
-
Original PDF page 66: L35 Oral Appliance Therapy for Snoring and OSA, p.66 ↩
-
Original PDF page 67: L35 Oral Appliance Therapy for Snoring and OSA, p.67 ↩
-
Original PDF page 69: L35 Oral Appliance Therapy for Snoring and OSA, p.69 ↩
-
Original PDF page 68: L35 Oral Appliance Therapy for Snoring and OSA, p.68 ↩