Bruxism: Evolution, Epidemiology, and Management
Learning Outcomes1
Upon completion of this module, you should be able to describe the following aspects of bruxism:
- Evolution
- Epidemiology
- Risk factors
- Aetiology and pathophysiology
- Clinical features
- Diagnosis
- Management
Presenter Information
Dr Amanda Phoon Nguyen
BDSc (UniMelb), MRACDS (GDP), DClinDent (Oral Med) (UWA), MRACDS (OralMed), Cert ADL, FOMAA, FPFA, FICD, FADI, MAICD, GCHL, MICDA, FDSM
Oral Medicine Specialist
Clinical Case Presentations
Patient Profile2
- Age/Sex: 60-year-old male
- The patient is a dentist.
- Clinical Findings: Dentist noted excessive tooth wear and tongue scalloping
- Symptoms: No pain

Case Study: Excessive Tooth Wear and Tongue Scalloping
Case Study: Snoring and Sleep Disordered Breathing3
 |  |
 |
Patient Profile4
- Age/Sex: 26-year-old male
- Primary Complaint: Snoring and sleep disordered breathing

OSA Assessment5
- ESS: 7/24
- Stop-Bang: 4/8
 |  |  |
 |  |
Anthropometrics and Blood Pressure
- Height: 177.0 cm
- Weight: 70.0 kg
- BMI: 22.3 kg/m²
- Neck Circumference: 37 cm
- Waist/Hip Ratio: 0.87
- Night BP: 120/55 mmHg
- Morning BP: 113/53 mmHg
Sleep Data
- Time in Bed: 427.7 min (7.13 hrs)
- Sleep Time: 283.9 min (4.73 hrs)
- Sleep Efficiency: 66.4%
- Sleep Latency: 22.8 min
- REM Latency: 220.0 min
- WASO: 121.0 min
- Sleep Architecture:
- REM: 25.2% (71.5 min)
- Stage N1: 4.1% (11.5 min)
- Stage N2: 57.9% (164.4 min)
- Stage N3: 12.9% (36.5 min)
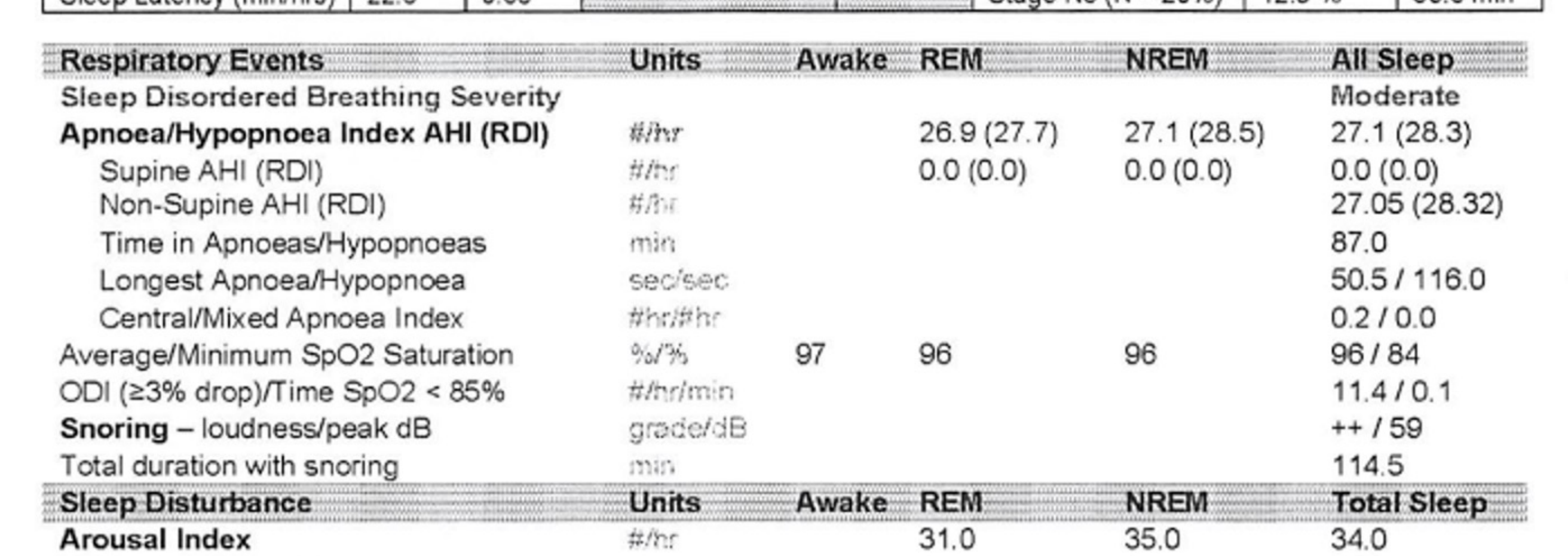
Respiratory Events
- Severity: Moderate Sleep Disordered Breathing
- AHI (RDI): 27.1 (28.3)
- Non-Supine AHI (RDI): 27.05 (28.32)
- Time in Apnoeas/Hypopnoeas: 87.0 min
- Longest Event: 50.5 sec (Apnoea) / 116.0 sec (Hypopnoea)
- Central/Mixed Apnoeas: 0.2 / 0.0 per hour
- SpO2 Saturation: 96% average / 84% minimum
- ODI (≥3%): 11.4 per hour
- Snoring: Grade ++; 59 dB peak; 114.5 min total duration
Sleep Disturbance
- Arousal Index: 34.0 per hour (Total: 161)
- Respiratory Arousal Index: 24.9 per hour
- Leg Arousal Index: 1.3 per hour
- Arousals with Bruxism: 0
Diagnostic Considerations for Bruxism in Sleep Studies
Sleep studies often use sensors on the chin or masseter to detect activity, but this is not always accurate as movement or stretching can register as bruxism. The most accurate method is video monitoring to observe lead movement and confirm grinding.
- Awakenings: 17 total (13 Respiratory-related)
Limb Movements
- Limb Movement Index: 1.9 per hour
- PLM Index: 0.9 per hour
- Total Movements: 13
Additional Factors
- Night Sedation: Nil
- Alcohol: Nil
Case Study: Masseter and Temporalis Hypertrophy
- ==Patient Profile: 30-something-year-old female==
Clinical Findings6
- Dental: No tooth wear
- Respiratory: No sleep disordered breathing, snoring, or OSA
- Muscular: Masseter and temporalis hypertrophy; occasional tenderness to palpation of muscles of mastication
- TMJ: No jaw clicking, deviation, locking, or pain
- Systemic: Some daytime tiredness
Case Study: Toothache and Tonsillar Hypertrophy
Clinical Presentation7
- Patient presents with a toothache.
- Tonsillar hypertrophy noted on clinical examination.

Case Summary8
- 60-year-old male
- Dentist noted excessive tooth wear and tongue scalloping
- No pain
Clinical Considerations
- Is management required?
- Are there any other possible diagnoses?
Case Summary9
- 26-year-old male
- Snoring and sleep disordered breathing
 |  |
 |
Clinical Considerations
- Does bruxism affect our management or treatment plan?
- Patient presenting for orthodontic consultation.
- Clinical observation: Generalized splint wear and flattened mandibular molars suggesting occlusal history.
Management Considerations10
-
Is a splint always the right or best management?
-
No tooth wear
-
No sleep disordered breathing, snoring, or OSA
-
Some daytime tiredness
-
Masseter and temporalis hypertrophy
-
No jaw clicking or deviation, locking, or pain
-
Occasional tenderness to palpation of muscles of mastication
 |  |
 |
Clinical Presentation and Follow-up11
- Patient presents with a toothache.
- Tonsillar hypertrophy noted on clinical examination.
Diagnostic Considerations
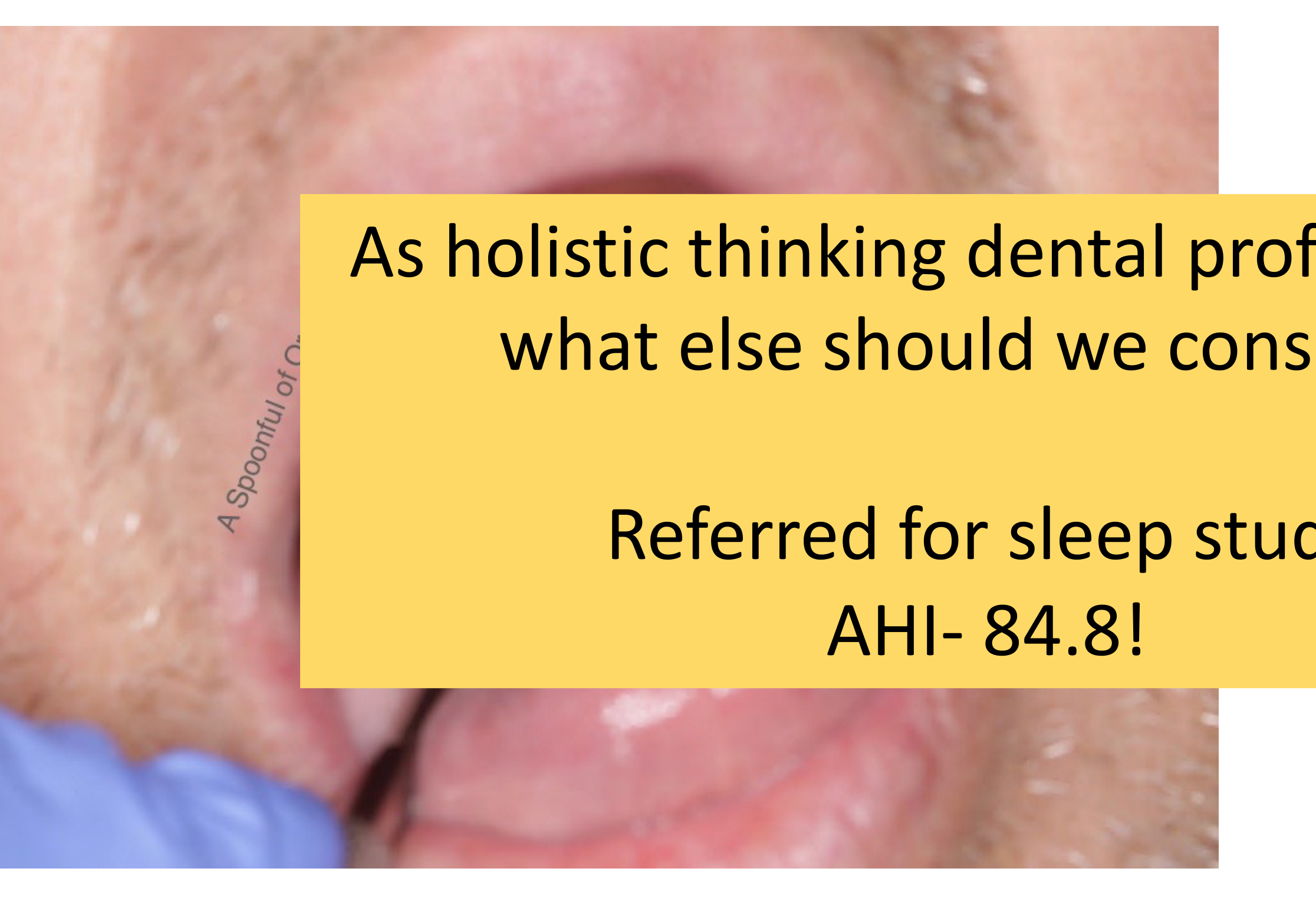
- As holistic thinking dental professionals, what else should we consider?
- Referred for sleep study.
- Result: AHI- 84.8!
Definitions and Diagnostic Criteria
Sleep Bruxism12
Sleep bruxism is a masticatory muscle activity during sleep that is characterised as rhythmic (phasic) or non-rhythmic (tonic) and is not a movement disorder or a sleep disorder in otherwise healthy individuals.
2018 Global Consensus
In 2018, a global consensus of experts redefined bruxism to clarify that it is not always a disease or disorder and does not always require treatment.
Sleep Versus Awake Bruxism
Awake Bruxism
Awake bruxism is a masticatory muscle activity during wakefulness that is characterised by repetitive or sustained tooth contact and/or by bracing or thrusting of the mandible and is not
Association with Bruxism
- The relationship between OSA and bruxism is not strong; only a minority of sleep bruxism cases have OSA.
- In some cases, bruxism may actually be a protective behavior to keep the airway patent. a movement disorder in otherwise healthy individuals.
Clinical Signs of Bruxism in Adults13
Clinical Identification14
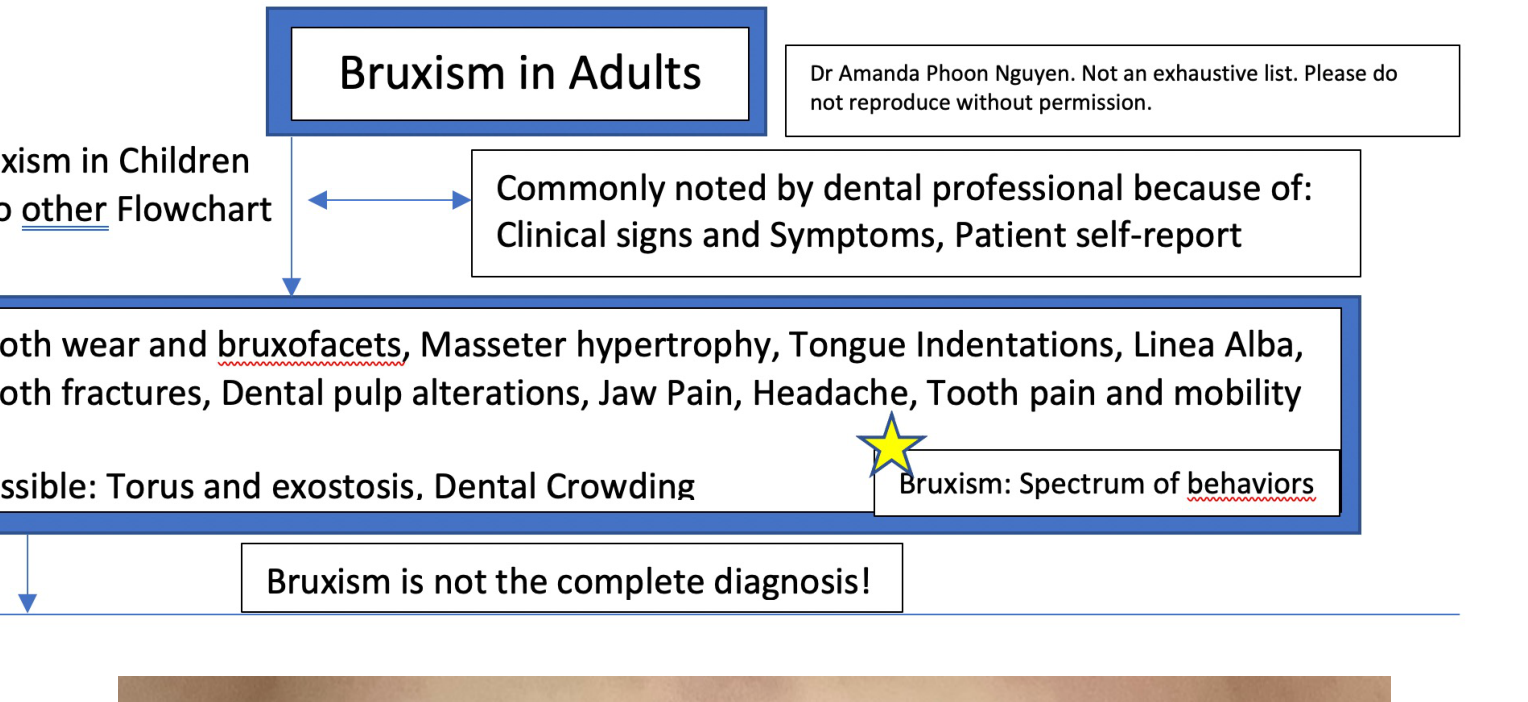
Bruxism is commonly noted by dental professionals through clinical signs, symptoms, and patient self-reports. It is important to note that bruxism represents a spectrum of behaviors and is not the complete diagnosis.
- Patients may not realize they "brux" because they associate the term only with grinding; it also includes clenching, bracing, or thrusting.
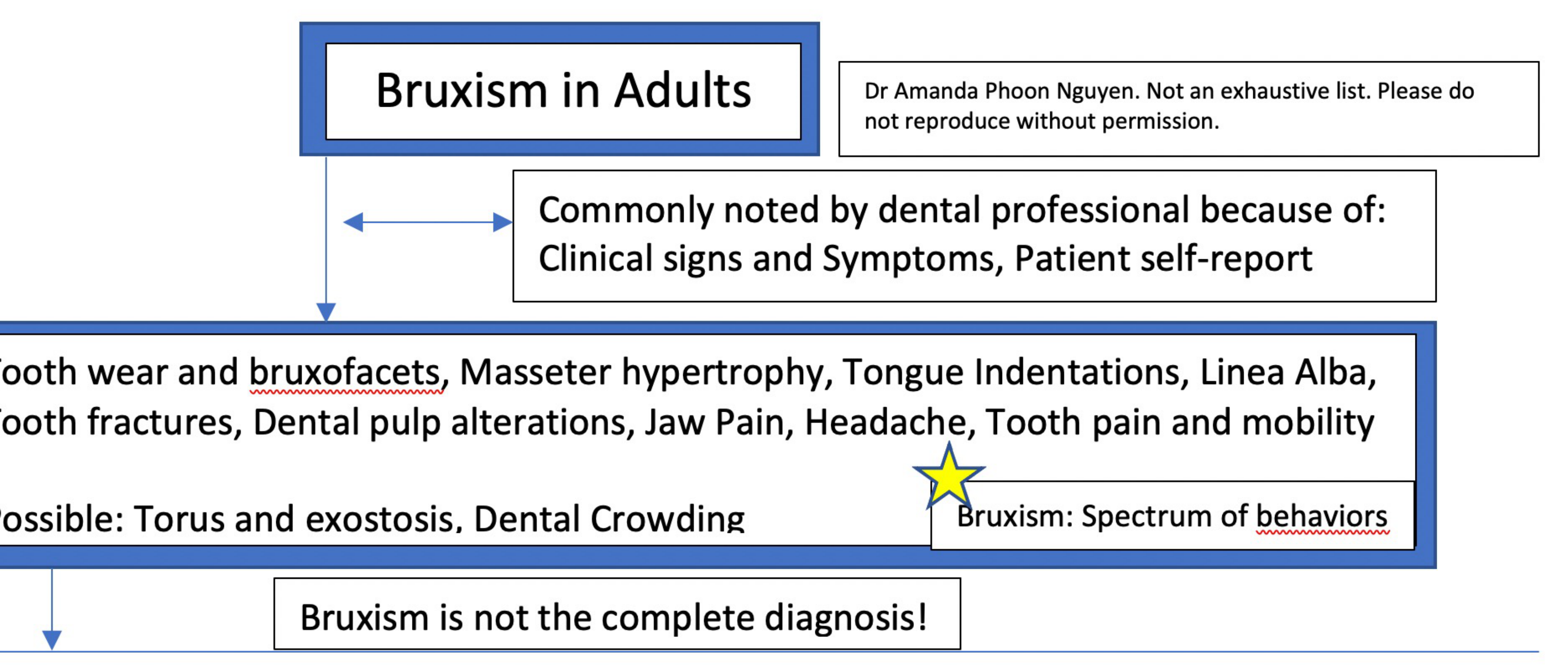
Common Signs and Symptoms
- Tooth wear and bruxofacets
- Masseter hypertrophy
- Tongue indentations
- Linea alba
- Tooth fractures
- Dental pulp alterations
- Jaw pain
- Headache
- Tooth pain and mobility
Possible Associated Findings
- Torus and exostosis
- Dental crowding
Toothwear and Bruxofacets15
- Not caused exclusively by bruxism.
- Erosion is usually the main cause.
- Not reliable as a single diagnostic indicator.
- Consideration of the spectrum of bruxism and its formal definition is required.
- Abrasion is often a main cause of tooth wear.
- In children, reflux is a common cause of wear facets.
 | 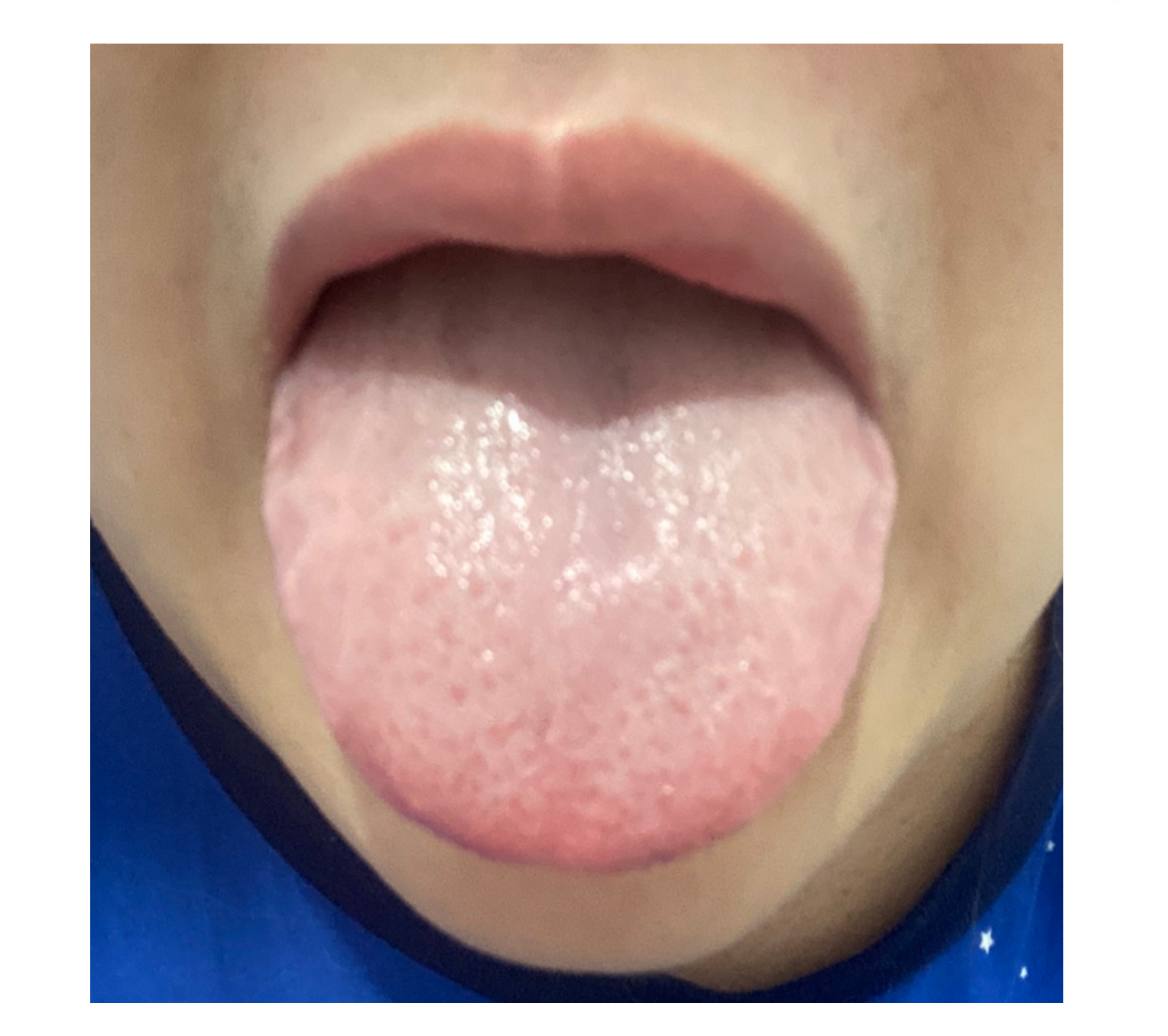 |
Tongue Scalloping
- Associated with causes of macroglossia.
- More common in the general population than the percentage of bruxers would suggest.
- Not reliable as a single diagnostic indicator.
Masseter Hypertrophy16
- Usually asymptomatic.
- May be unilateral or bilateral.
- Masticatory muscle hyperactivity cannot be verified in all instances of masseter hypertrophy.
Linea Alba
- Thought to be associated most with clenching.
- A common clinical finding, though its specificity is not known.
- It is more common in the general population than in those with bruxism.
Tooth Fractures
- A common finding.
- Nocturnal bite force may exceed the maximum amplitude recorded during daytime hours.
- Multiple tooth fractures or restorative fractures are significant indicators for treatment.
Diagnostic Flowchart and Classification
Diagnostic Steps17
-
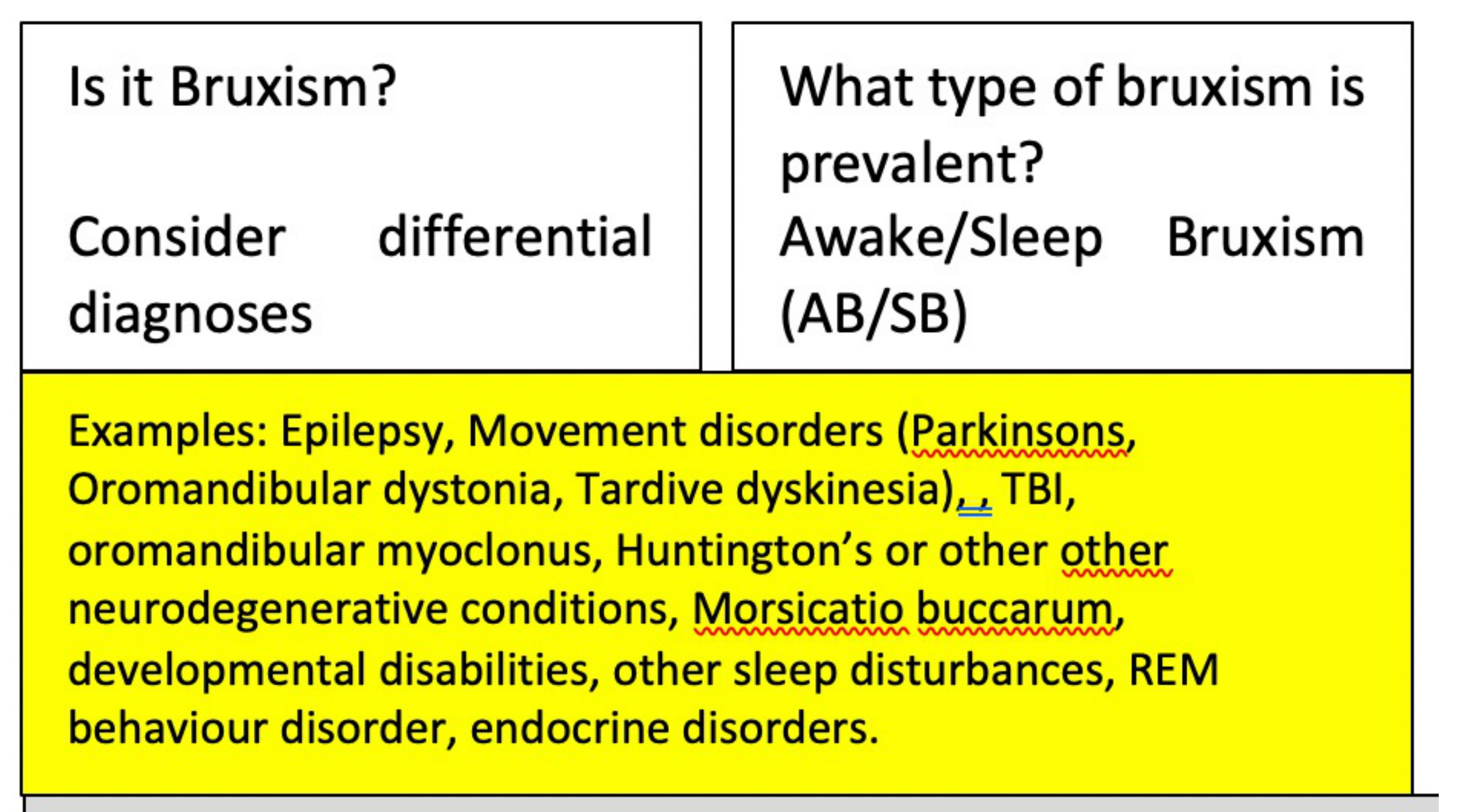
Is it Bruxism?
- Consider differential diagnoses.
- Rule out: Epilepsy, movement disorders (Parkinson’s, Oromandibular dystonia, Tardive dyskinesia), TBI, oromandibular myoclonus, Huntington’s or other neurodegenerative conditions, Morsicatio buccarum, developmental disabilities, sleep disturbances, REM behaviour disorder, and endocrine disorders.
-
What type of bruxism is prevalent?
- Determine if it is Awake Bruxism (AB) or Sleep Bruxism (SB).
-
Classification of Behavior
- Harmless behavior: Not a risk or protective behavior.
- Risk factor: Associated with one or more negative health outcomes.
- Protective factor: Associated with one or more positive health outcomes.
-
Primary or Secondary?
- Determine if the AB or SB is primary or secondary to other conditions.
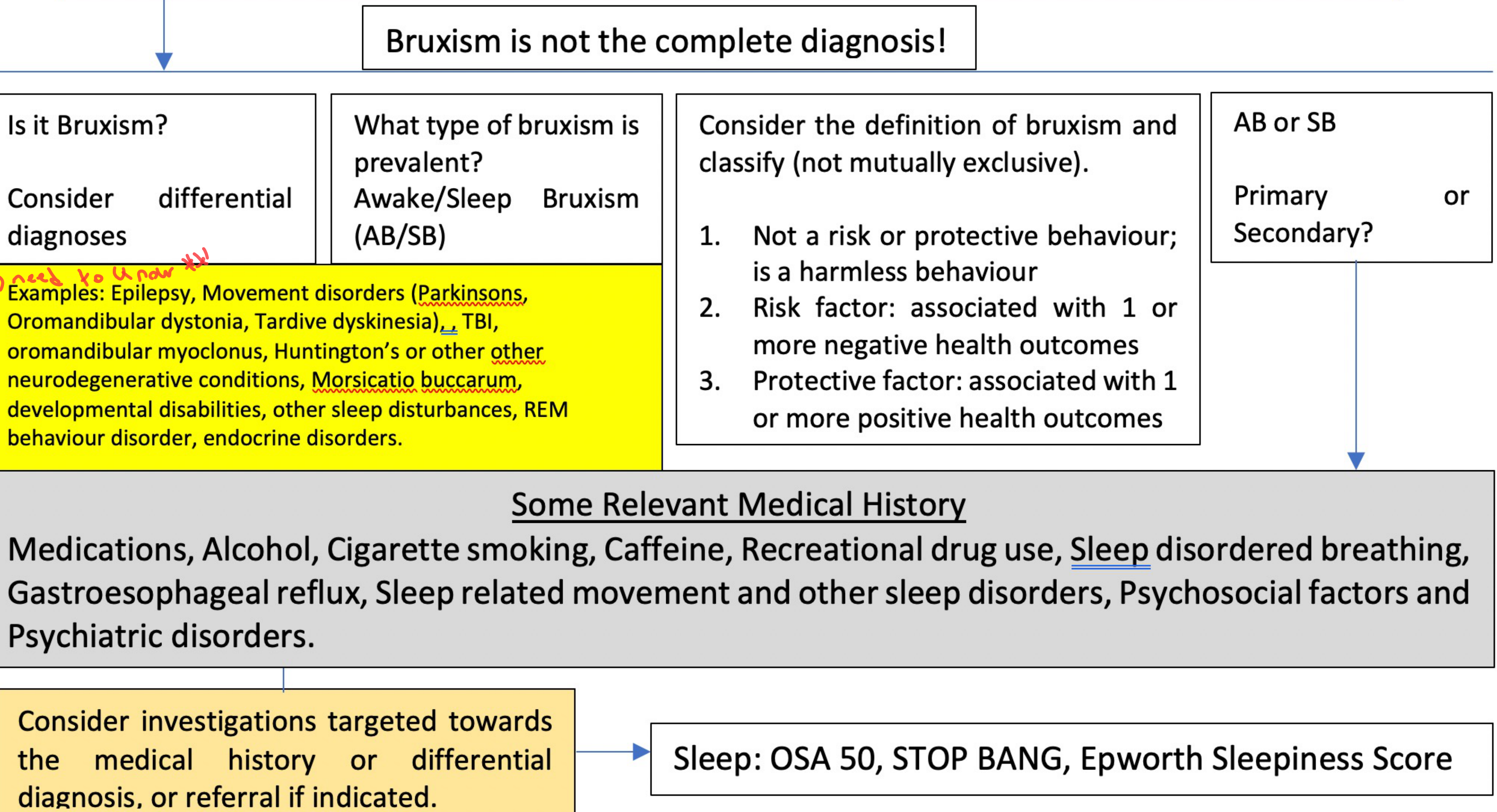
Medical History and Risk Factors
- Medications and recreational drug use
- Alcohol, cigarette smoking, and caffeine
- Sleep-disordered breathing (e.g., Gastroesophageal reflux, OSA)
- Psychosocial factors and psychiatric disorders
Investigations and Referrals
- Targeted investigations based on medical history.
- Sleep assessments: OSA 50, STOP BANG, Epworth Sleepiness Score.
- Referral if indicated.
Differential Diagnosis Screening18
Is it Bruxism? Consider differential diagnoses including:
- Epilepsy
- Movement disorders (e.g., Tardive dyskinesia)
- Traumatic Brain Injury (TBI)
- Oromandibular myoclonus
- Huntington’s or other neurodegenerative conditions
- Morsicatio buccarum
- Developmental disabilities
- Sleep disturbances (e.g., REM behaviour disorder)
- Endocrine disorders
Prevalence Type
- Awake Bruxism (AB)
- Sleep Bruxism (SB)
Differential Diagnosis and Movement Disorders
Patient Profile19
- Age/Gender: 55-year-old female
- Referral: Referred from General Practitioner (GP) on 07/10/16
Case Study: Dementia and Chronic Bruxism
Clinical Presentation
- Diagnosis: Fronto-temporal dementia.
- Functional Status: Patient can walk but cannot speak or follow instructions; unable to cooperate with dental procedures or treatment.
- Primary Concern: Chronic bruxism requiring a dental examination and splint therapy.
Medical History20
- Endocrine/Metabolic:
- Total thyroidectomy (performed in India for benign causes)
- Vitamin D deficiency (2016)
- Hematologic: B12 deficiency anaemia (2007)
- Neurological/Psychiatric:
- Fronto-temporal dementia (2014)
- Type 2 Diabetes Mellitus (T2DM) (2013)
- Allergies: Penicillin
Current Medications and Supplements
- Prescriptions:
- Aspirin 100mg
- Thyroxine 100mcg
- Supplements: Fish oil, magnesium, melatonin, Vitamin D, lecithin
- Previous Medications:
- Escitalopram 20mcg
- Risperidone 1mg (½ a night)
Treatment Timeline21
- Dental Management
- Initial management for bruxism.
- An occlusal splint was fabricated but could not be worn as the patient was unable to tolerate it.
Case Study Update: Dementia and Chronic Bruxism
- Video analysis revealed the movement was not bruxism; the patient was sticking her tongue out at regular intervals and moving her jaw.
- Final Diagnosis: Tardive dyskinesia (a movement disorder) rather than chronic bruxism.
Oromandibular Dystonia
Epidemiology and Characteristics22
- Prevalence: Approximately 3 to 30 per 100,000 individuals.
- Demographics: Possible female predilection (F>M); mean age of symptom onset is between 31 and 58 years.
- Clinical Presentation: Oromandibular dystonias (ODs) are intermittent, presenting as short, sustained muscle contractions that result in abnormal movements and posturing.
Etiology
- Primary: Idiopathic focal dystonias.
- Secondary: Resulting from underlying central nervous system pathology, such as tumors or infarctions.
Clinical Classifications23
Oromandibular dystonia may present as:
- Jaw-opening dystonia
- Jaw-closing dystonia
- Jaw-deflecting dystonia
- Jaw-retruding dystonia
- A combination of the above
Movement Patterns
Involuntary or uncontrolled mandibular movements can be characterized as either repetitive or sustained.
- Clinical Observation: A patient with dementia exhibited repetitive toe-curling motions (observed via open-toed shoes), leading to a neurology referral for a movement disorder rather than a bruxism diagnosis.
Statistical Etiology
Most cases of OD are idiopathic, accounting for 63% of reported cases.
Drug-Induced Extrapyramidal Syndrome Reactions2425
 |  |
 |
Extrapyramidal Syndrome Reactions26
| Reaction Type | Clinical Manifestation |
|---|---|
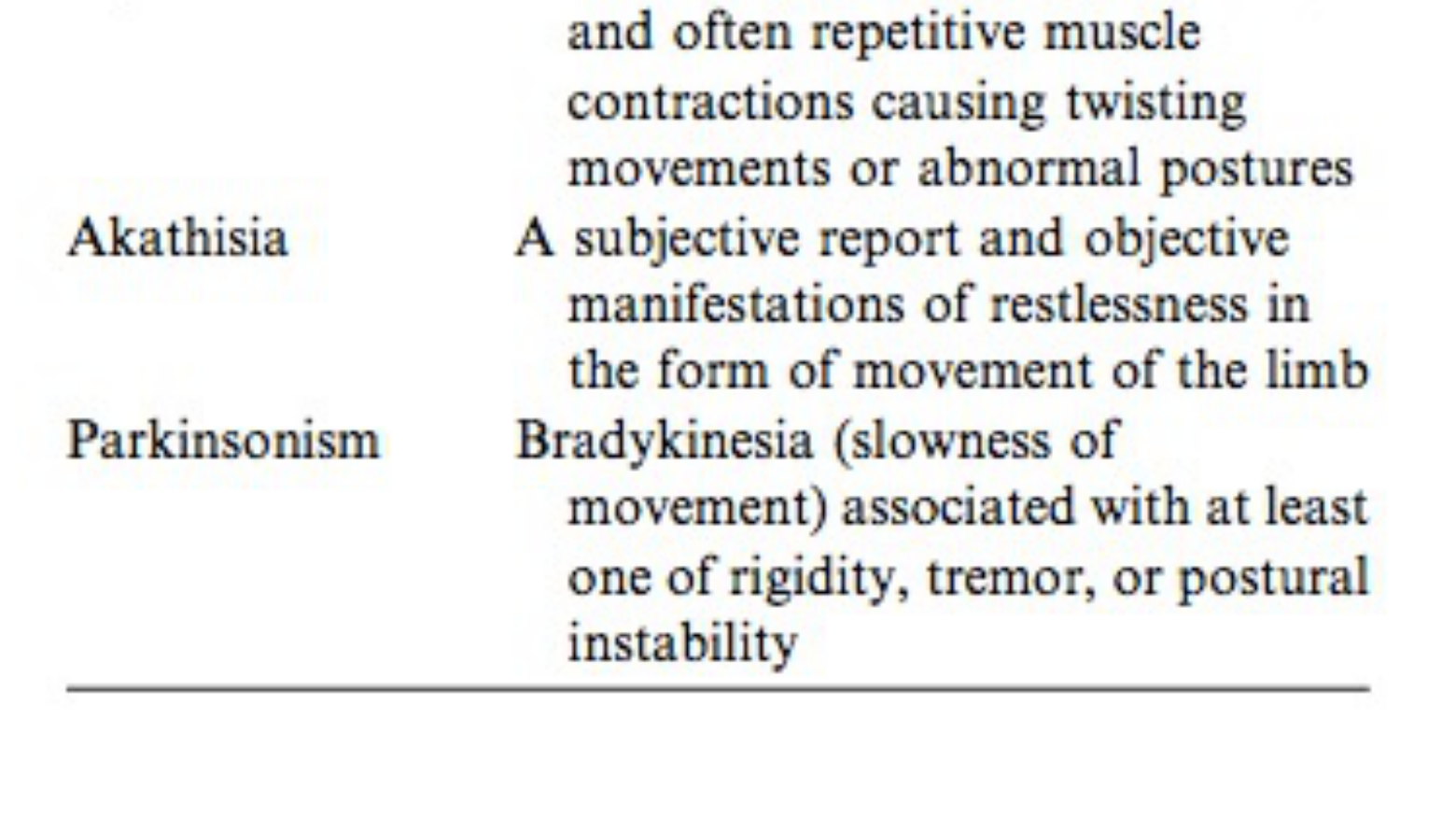
| Dystonia | Involuntary, sustained, patterned, and often repetitive muscle contractions causing twisting movements or abnormal postures. |
| Akathisia | Subjective reports and objective manifestations of restlessness, typically involving limb movement. |
| Parkinsonism | Bradykinesia (slowness of movement) associated with at least one of: rigidity, tremor, or postural instability. |
 | 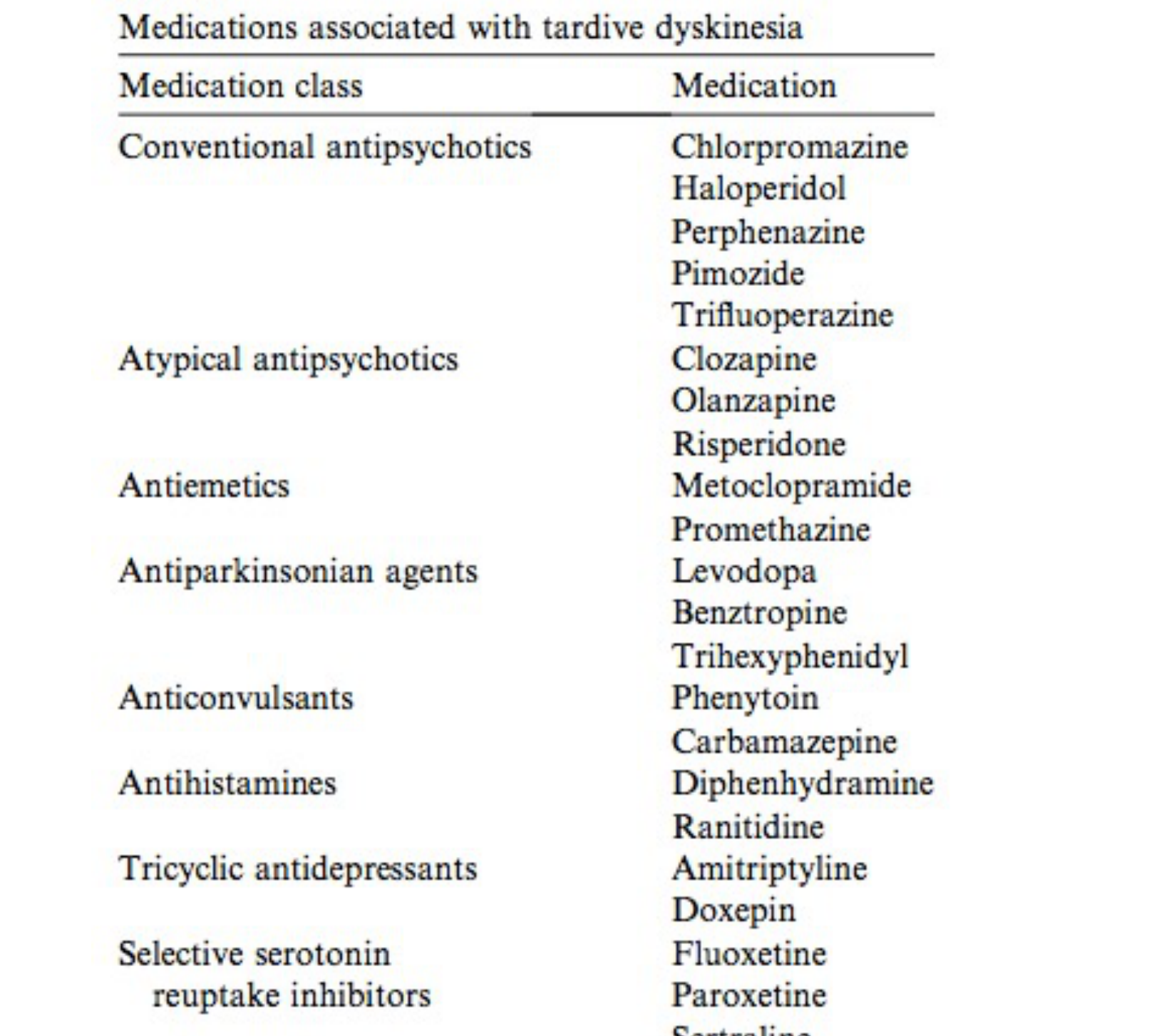 |
Medications Associated with Tardive Dyskinesia
-
Conventional Antipsychotics: Chlorpromazine, Haloperidol, Perphenazine, Pimozide, Trifluoperazine
-
Atypical Antipsychotics: Clozapine, Olanzapine, Risperidone
-
Antiemetics: Metoclopramide, Promethazine
-
Antiparkinsonian Agents: Levodopa, Benztropine, Trihexyphenidyl
-
Anticonvulsants: Phenytoin, Carbamazepine
-
Antihistamines: Diphenhydramine
-
Tricyclic Antidepressants: Amitriptyline, Doxepin
-
SSRIs: Fluoxetine, Paroxetine, Sertraline
-
Other: Ranitidine
-
Clinical photograph showing maxillo-mandibular fixation with elastics.
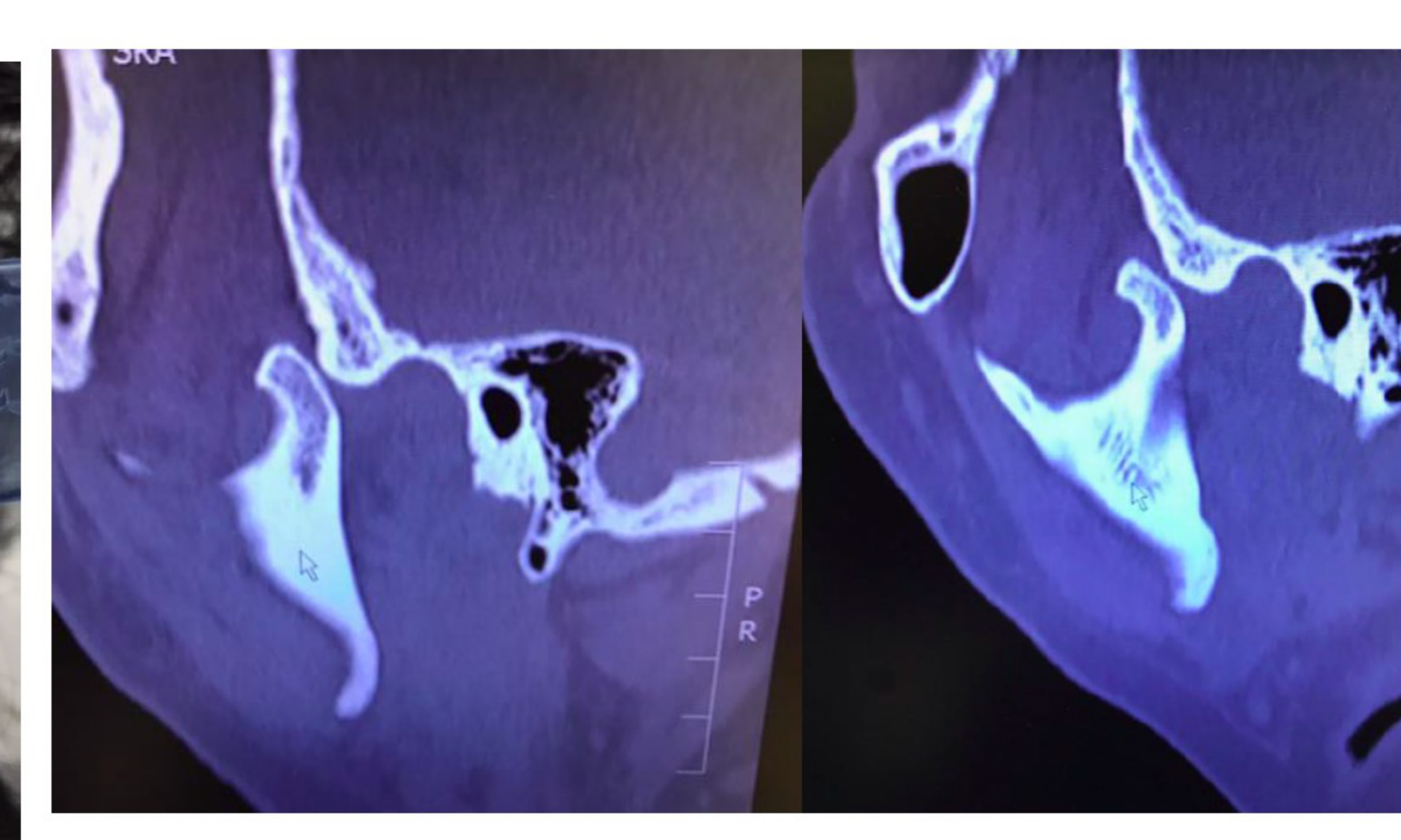
-
Computed tomography images showing dislocation of the left and right TM joints.
Lateral view of a male patient’s head showing loose skin on the scalp.
Diagnostic Considerations27
Bruxism is often not the complete diagnosis. Clinicians should evaluate the following:
- Classification: Determine if it is Awake Bruxism (AB) or Sleep Bruxism (SB), and whether it is Primary or Secondary.
- Behavioral Impact:
- Harmless behavior (not a risk or protective factor).
- Risk factor (associated with negative health outcomes).
- Protective factor (associated with positive health outcomes).
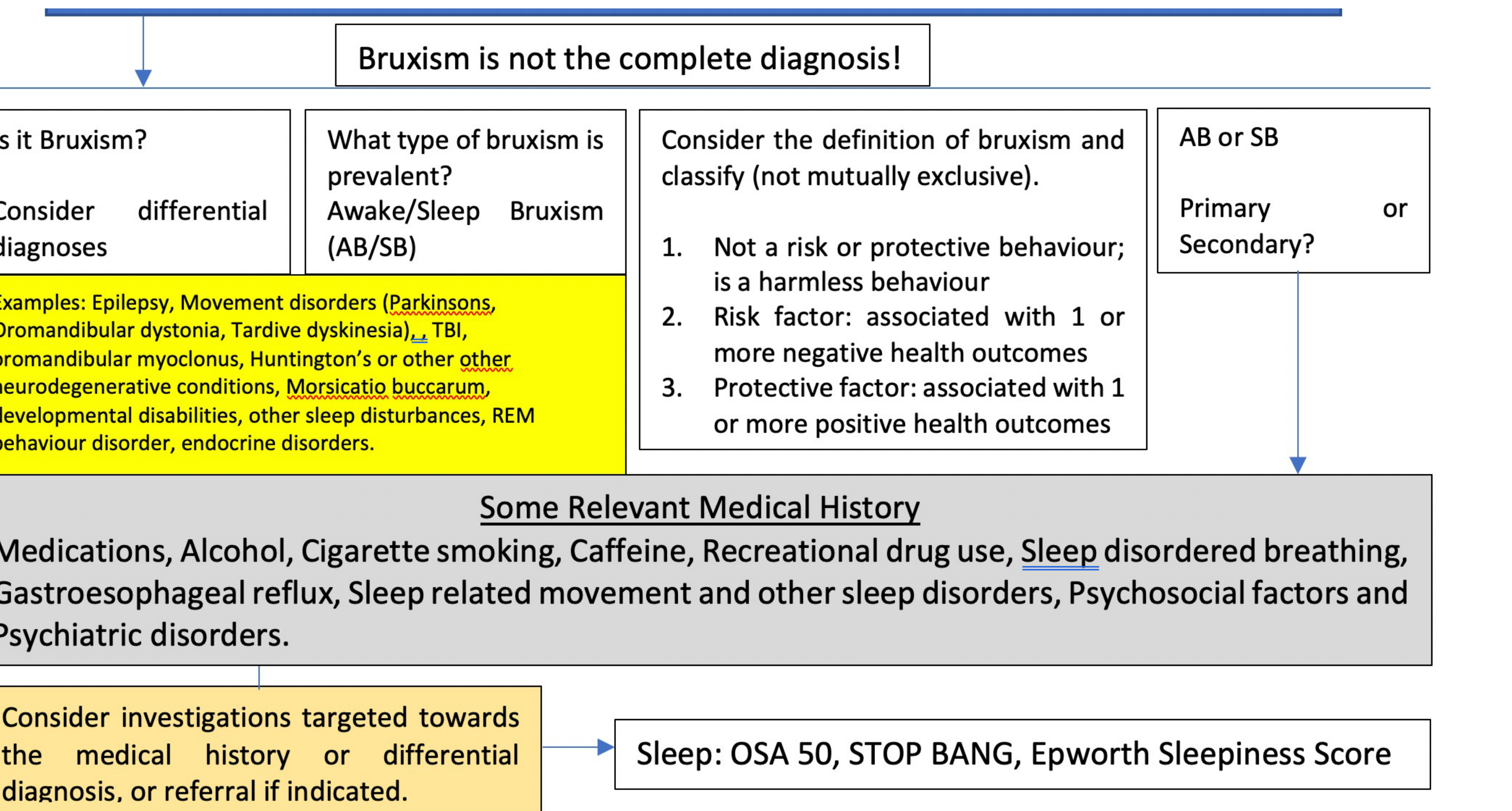
Differential Diagnoses
Consider the following conditions that may mimic or coexist with bruxism:
- Movement Disorders: Parkinson’s disease, Oromandibular dystonia, Tardive dyskinesia, Oromandibular myoclonus.
- Neurological/Neurodegenerative: Epilepsy, Traumatic Brain Injury (TBI), Huntington’s disease.
- Other: Morsicatio buccarum, developmental disabilities, REM behavior disorder, endocrine disorders, and various sleep disturbances.
Medical History and Risk Factors
Evaluate the influence of:
- Substances: Alcohol, Cigarette smoking, Caffeine, Recreational drug use.
- Systemic Health: Gastrooesophageal reflux, Sleep-disordered breathing (e.g., OSA), endocrine disorders.
- Psychosocial: Psychiatric disorders and psychosocial factors.
Investigations and Referrals
Targeted investigations or referrals should be considered based on medical history:
- Sleep Assessment Tools: OSA 50, STOP-BANG, Epworth Sleepiness Score.
Risk Factors for Sleep Bruxism28
 |  |
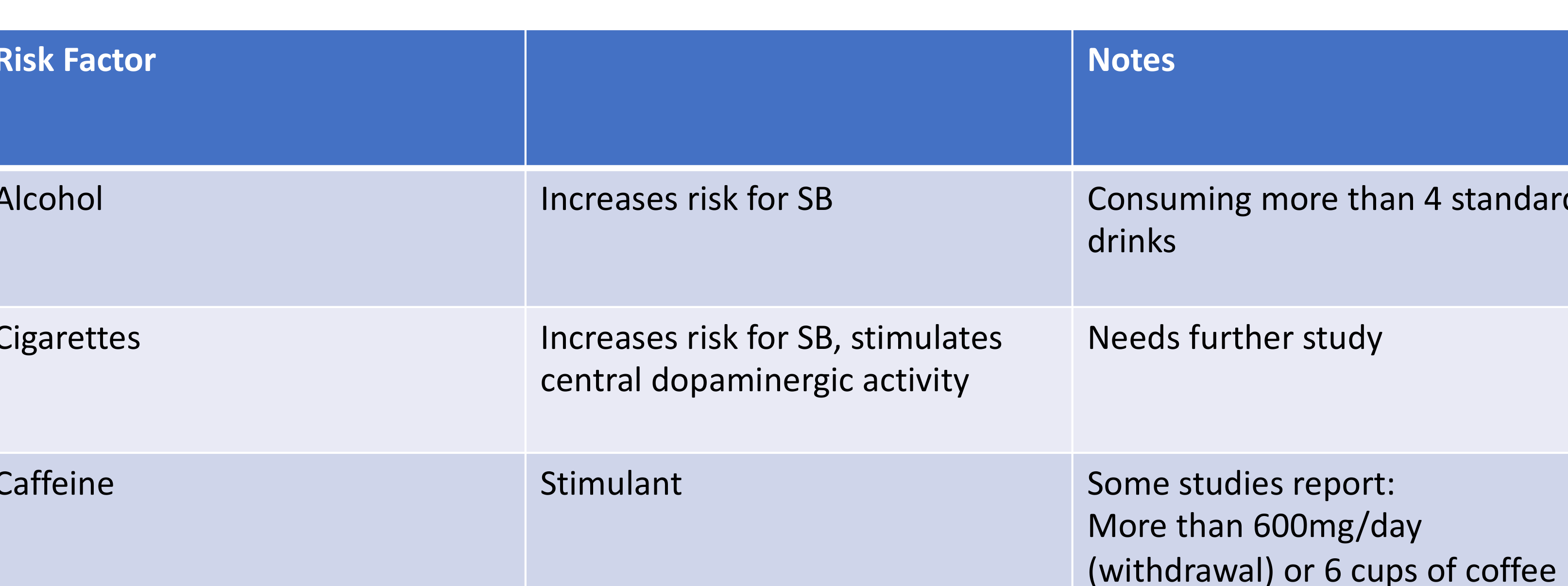
Lifestyle and Substance-Related Risk Factors29
- Alcohol
- Consuming more than 4 standard drinks increases the risk for Sleep Bruxism (SB).
- Cigarettes
- Smoking increases the risk for SB and stimulates central dopaminergic activity. Further study is required to fully understand this relationship.
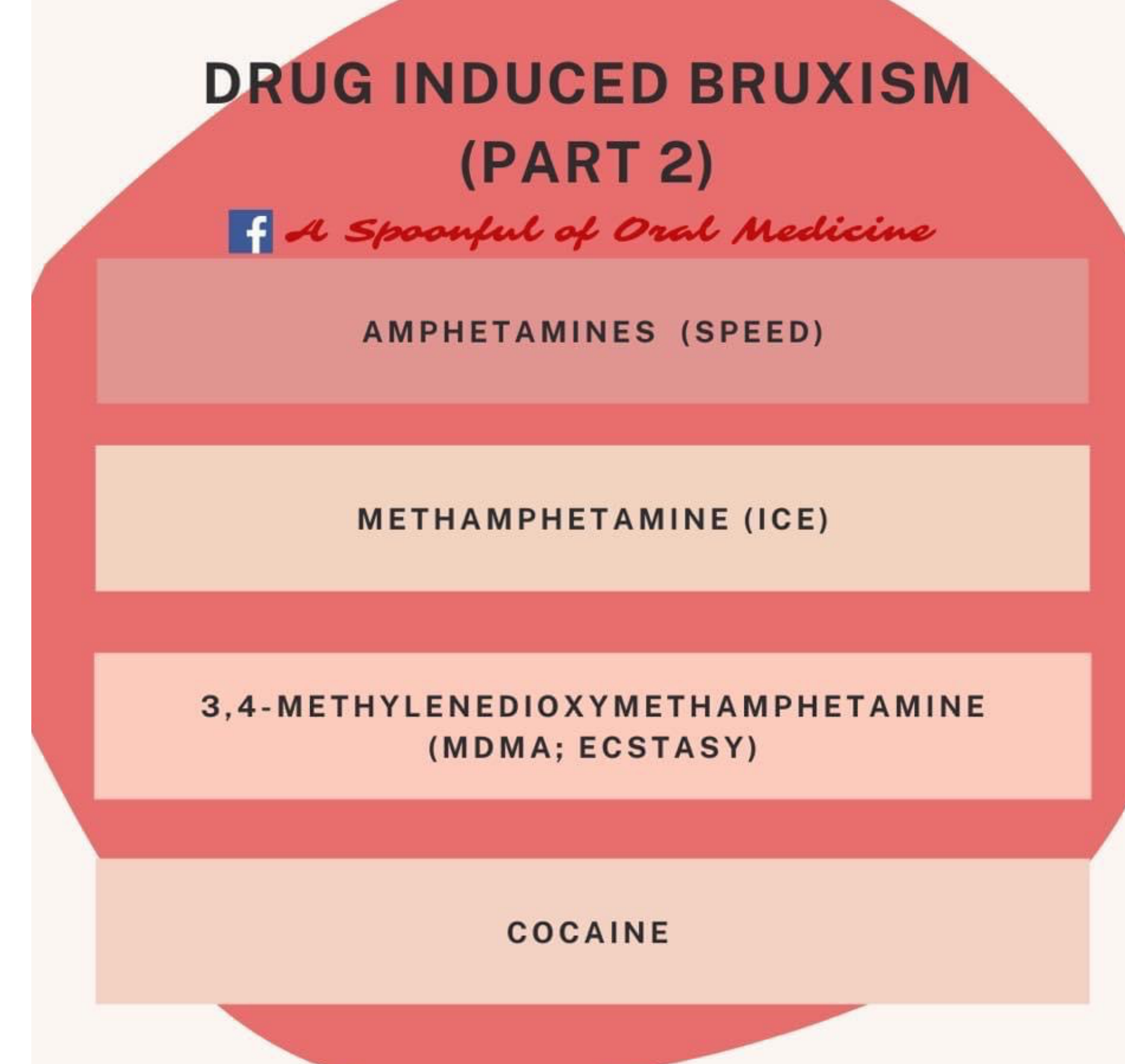
- Recreational drugs such as speed, ice, ecstasy, and cocaine may also induce bruxism.
- Caffeine
- Acts as a stimulant. Some studies report increased risk with consumption exceeding 600mg per day (or 6 cups of coffee) or during withdrawal.
 |  |
Clinical Assessment and Diagnostic Pathways
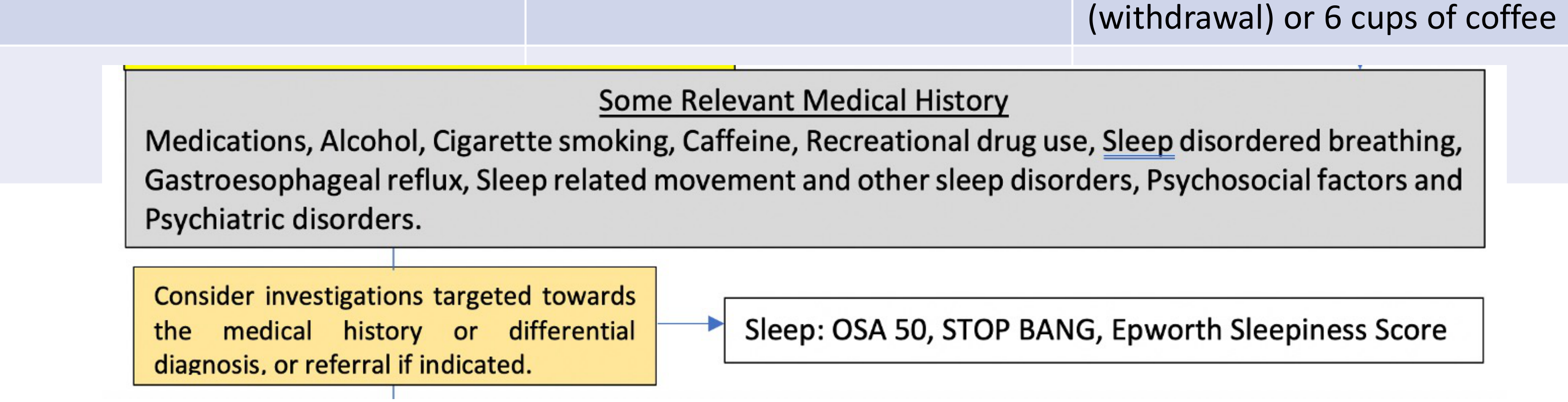
When evaluating a patient’s medical history, consider the following factors that may influence or coexist with Sleep Bruxism:
-
Medical and Lifestyle History
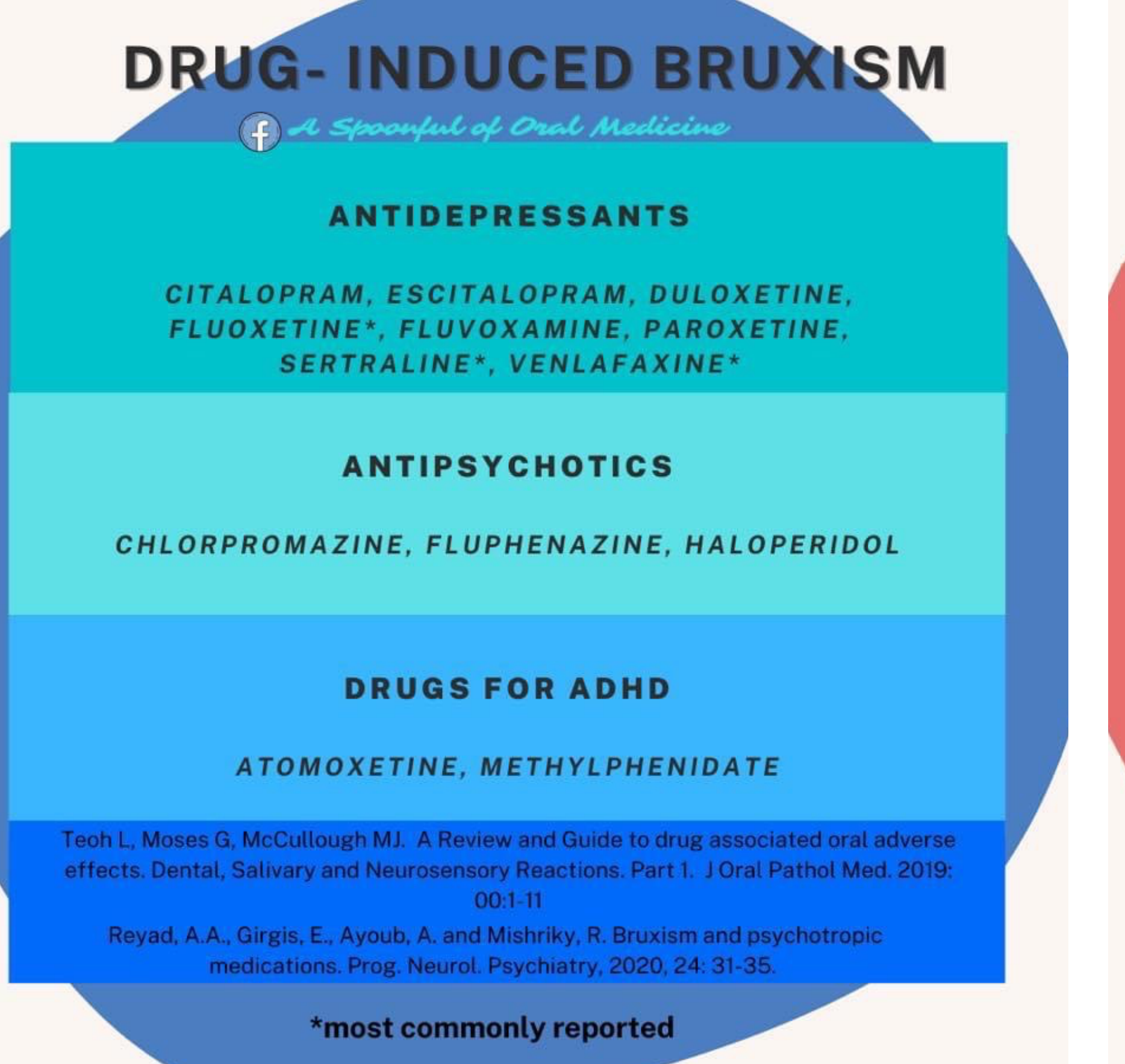
- Medications and recreational drug use
- Common triggers for medication-induced bruxism include antidepressants, antipsychotics, and ADHD drugs.
- If bruxism is significant, dentists should not stop these medications but should write to the psychiatrist to discuss alternatives.
- Alcohol, cigarette, and caffeine consumption
- Sleep-disordered breathing and other sleep-related movement disorders
- Gastroesophageal reflux
- Psychosocial factors and psychiatric disorders
- Medications and recreational drug use
-
Diagnostic Investigations
- Targeted investigations should be directed toward the medical history or differential diagnosis.
- Referrals should be made if clinically indicated.
-
Sleep Quality Screening Tools
- OSA 50
- STOP-BANG
- Epworth Sleepiness Score
Obstructive Sleep Apnea Screening and Assessment
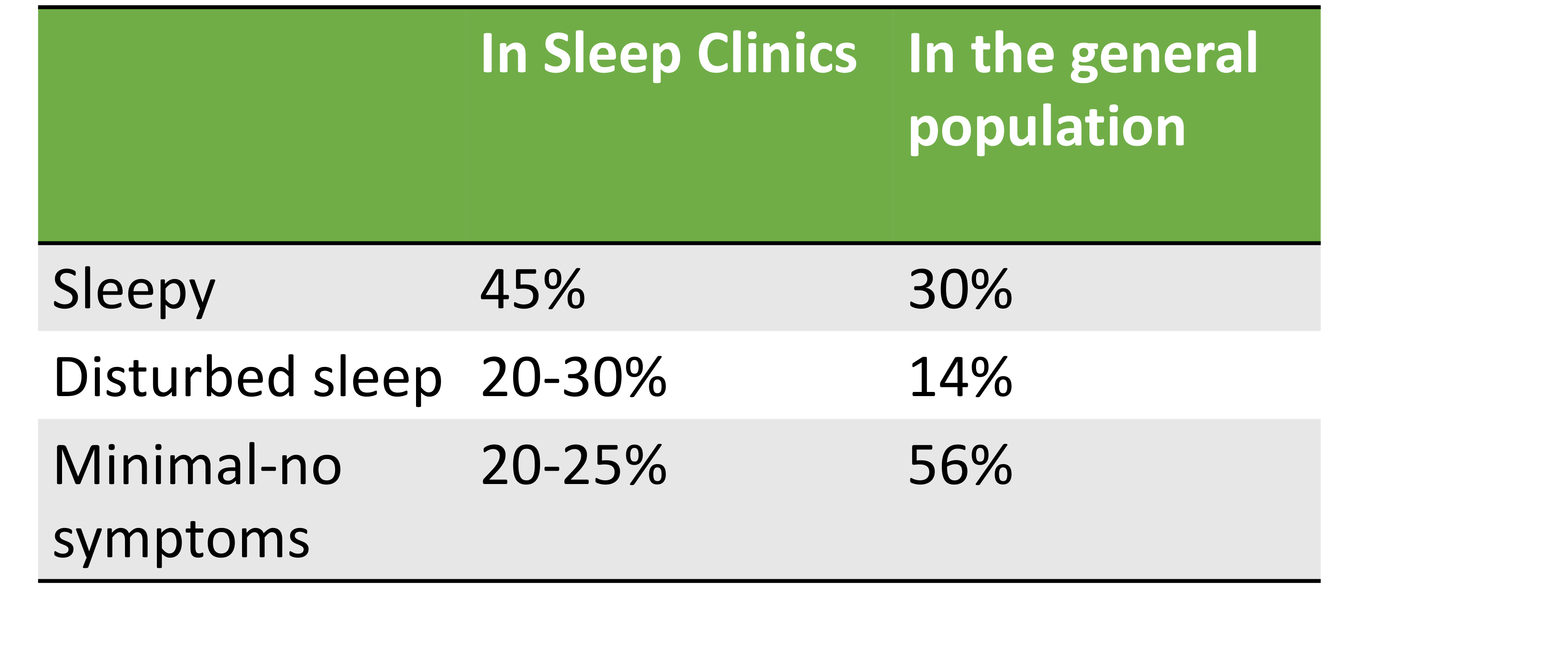
Prevalence of Sleepiness in OSA Patients30
| Symptom Category | In Sleep Clinics | In the General Population |
|---|---|---|
| Sleepy | 45% | 30% |
| Disturbed sleep | 20-30% | 14% |
| Minimal-no symptoms | 20-25% | 56% |
Clinical Significance of Obstructive Sleep Apnea
Comorbidities and Risks Associated with OSA31
- Accidents
- Depression
- Hypertension
- Diabetes
- Cardiovascular disease
Warning Signs of Microsleep32
- Head nodding: Indicates microsleep.
- Earlier warning signs: Difficulty keeping eyes open or blurred vision.
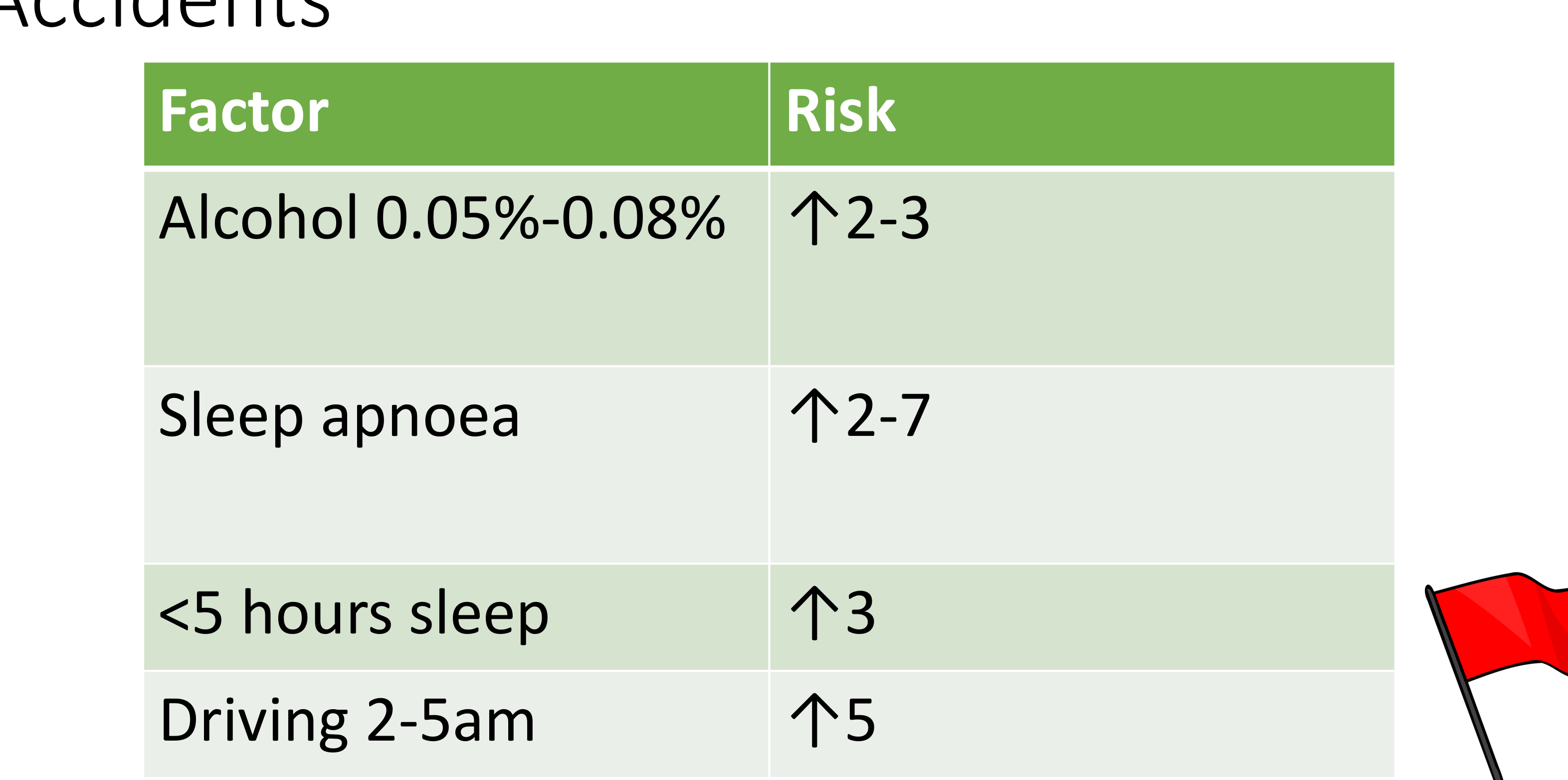
Comparative Risk Factors for Accidents33
| Factor | Risk Increase |
|---|---|
| Alcohol (0.05%-0.08%) | ↑ 2-3 |
| Sleep apnoea | ↑ 2-7 |
| < 5 hours sleep | ↑ 3 |
| Driving 2-5am | ↑ 5 |
 |  |
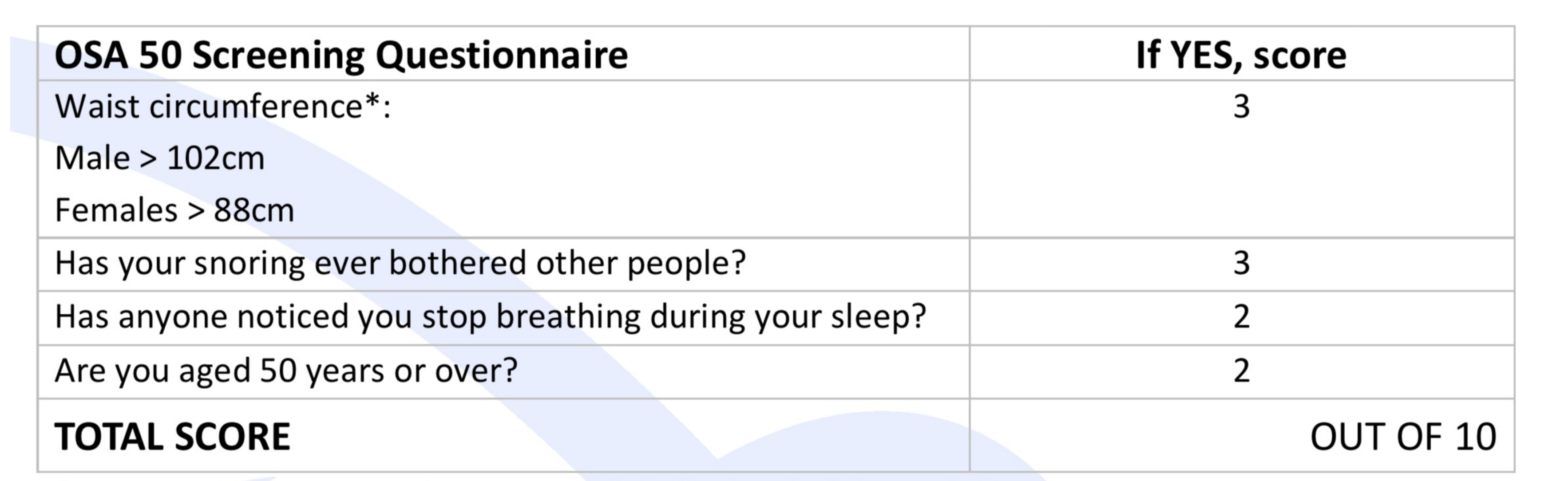
OSA 50 Screening Questionnaire
Scoring Criteria34
| Question | If YES, score |
|---|---|
| Waist circumference (measured at umbilicus): Male > 102cm; Female > 88cm | 3 |
| Has your snoring ever bothered other people? | 3 |
| Has anyone noticed you stop breathing during your sleep? | 2 |
| Are you aged 50 years or over? | 2 |
| TOTAL SCORE | OUT OF 10 |
Threshold: 5/10
STOP-BANG Assessment Tool
Screening Criteria35
- Snoring: Do you Snore Loudly (loud enough to be heard through closed doors or your bed-partner elbows you for snoring at night)?
- Tired: Do you often feel Tired, Fatigued, or Sleepy during the daytime (such as falling asleep during driving or talking to someone)?
- Observed: Has anyone Observed you Stop Breathing or Choking/Gasping during your sleep?
- Pressure: Do you have or are being treated for High Blood Pressure?
- Body Mass Index: More than 35 kg/m²?
- Age: Older than 50?
- Neck size large: (Measured around Adam’s apple)
- Male: Shirt collar 17 inches / 43cm or larger?
- Female: Shirt collar 16 inches / 41cm or larger?
- Gender: Male?
Risk Stratification36
- OSA - Low Risk: Yes to 0 - 2 questions
- OSA - Intermediate Risk: Yes to 3 - 4 questions
- OSA - High Risk: Yes to 5 - 8 questions
Alternative High Risk Criteria:
- Yes to 2 or more of 4 STOP questions + male gender
- Yes to 2 or more of 4 STOP questions + BMI > 35kg/m²
- Yes to 2 or more of 4 STOP questions + neck circumference (17 inches / 43cm in male or 16 inches / 41cm in female)
Note: Different cut-off scores can be used to trade off sensitivity and specificity.
Berlin Questionnaire
Patient Information37
Height (m) _____ Weight (kg) _____ Age _____ Male / Female
Category 1: Snoring
- Do you snore?
- a. Yes
- b. No
- c. Don’t know
If you answered ‘yes’: 2. Your snoring is:
- a. Slightly louder than breathing
- b. As loud as talking
- c. Louder than talking
Category 2: Daytime Sleepiness
-
How often do you feel tired or fatigued after your sleep?
- a. Almost every day
- b. 3-4 times per week
- c. 1-2 times per week
- d. 1-2 times per month
- e. Rarely or never
-
During your waking time, do you feel tired, fatigued or not up to par?
- a. Almost every day
- b. 3-4 times per week
- c. 1-2 times per week
- d. 1-2 times per month
- e. Rarely or never
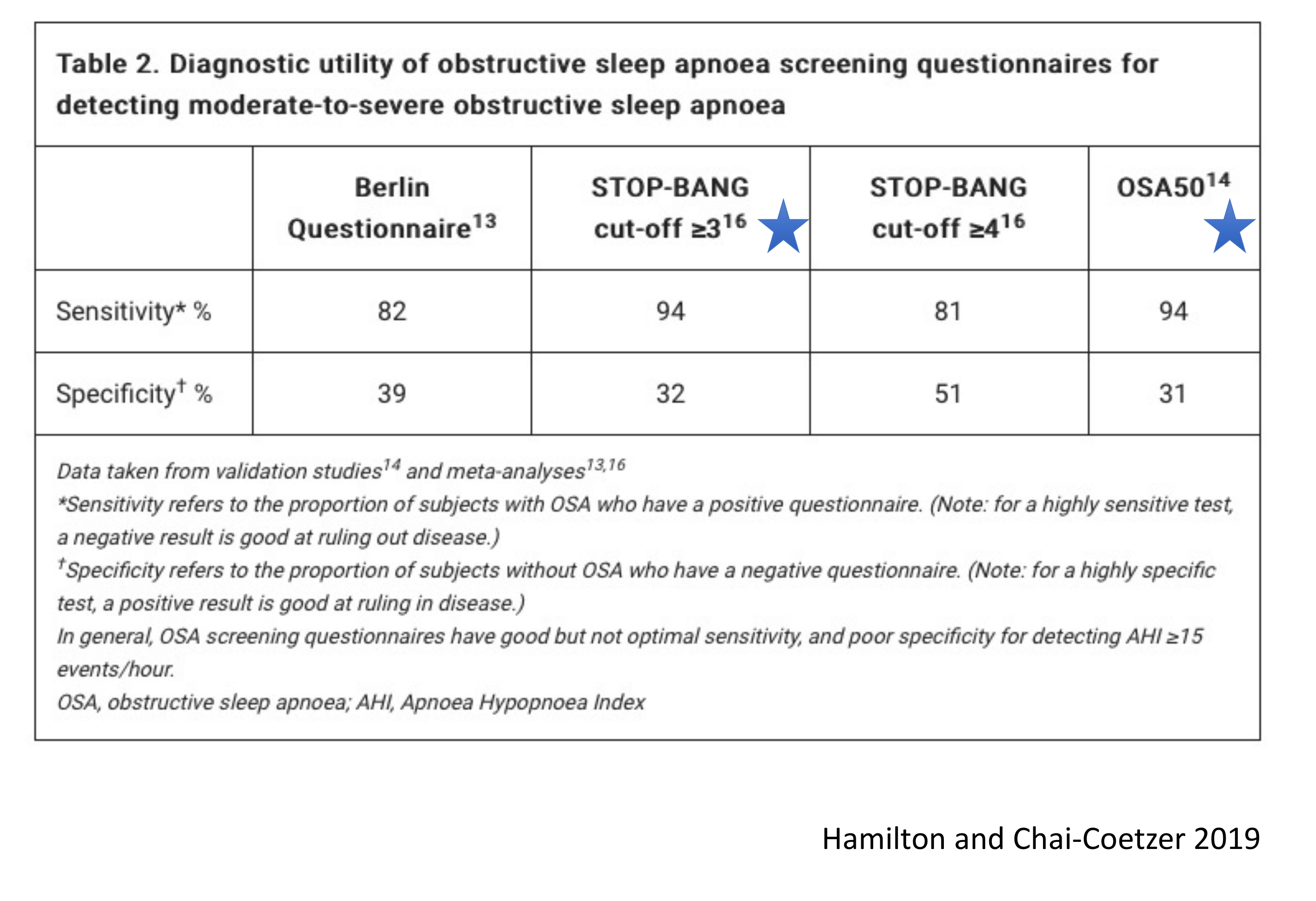
Diagnostic Utility for Moderate-to-Severe OSA38
| Metric | Berlin Questionnaire | STOP-BANG (≥3) | STOP-BANG (≥4) | OSA50 |
|---|---|---|---|---|
| Sensitivity % | 82 | 94 | 81 | 94 |
| Specificity % | 39 | 32 | 51 | 31 |
Definitions and Notes:
- Sensitivity: Proportion of subjects with OSA who have a positive questionnaire. (A highly sensitive test is good at ruling out disease with a negative result).
- Specificity: Proportion of subjects without OSA who have a negative questionnaire. (A highly specific test is good at ruling in disease with a positive result).
- General Finding: Screening questionnaires have good but not optimal sensitivity, and poor specificity for detecting AHI ≥15 events/hour.
Abbreviations: OSA, obstructive sleep apnoea; AHI, Apnoea Hypopnoea Index.
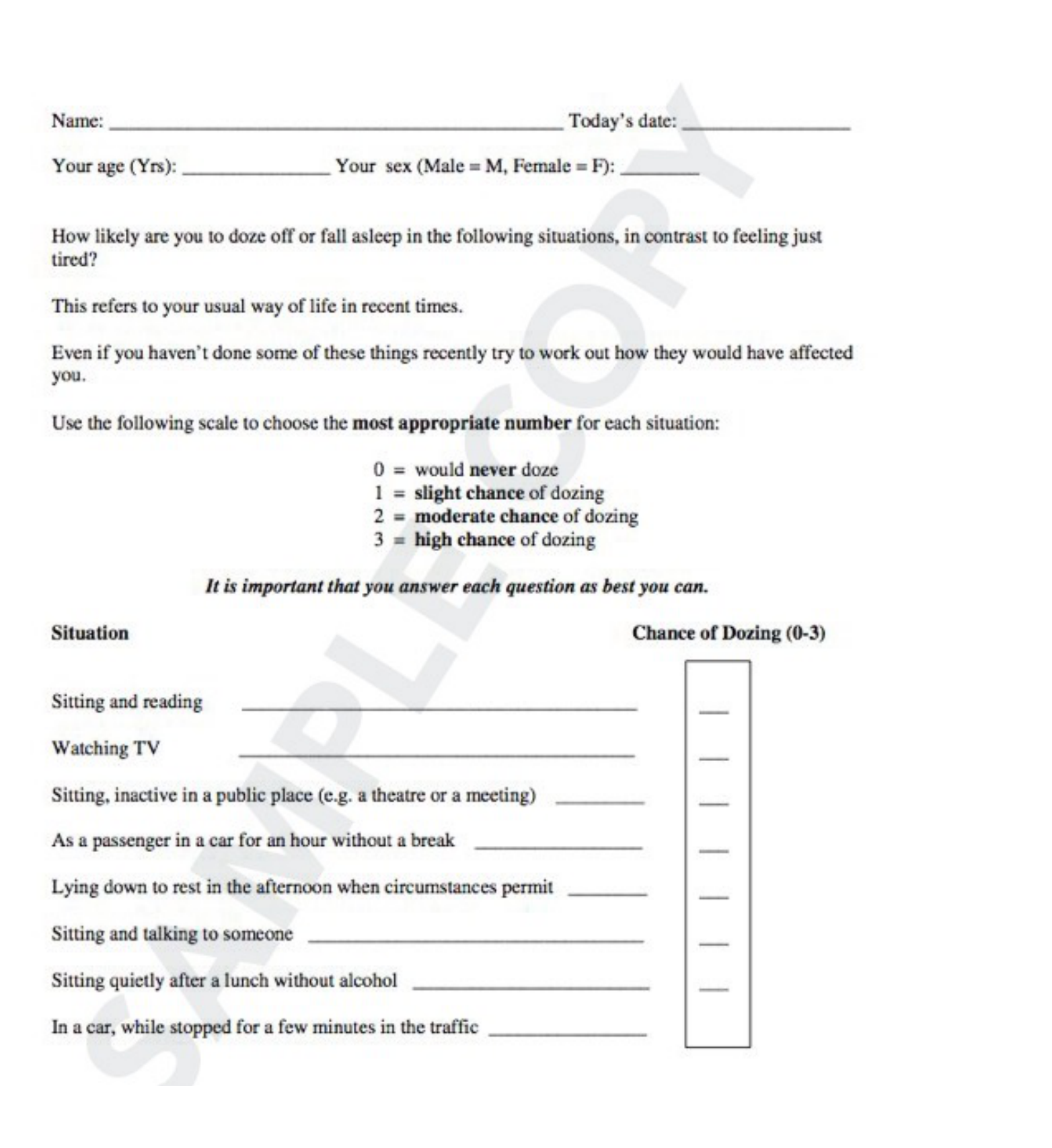
Epworth Sleepiness Scale
Assessment of Dozing Probability39
How likely are you to doze off or fall asleep in the following situations, in contrast to feeling just tired?
- While sitting and reading (not too challenging): Doze off
- As a passenger in a motor vehicle when not feeling tired: Fall asleep
- Later in the afternoon when not active (e.g., lecture, watching TV, movie, lunch with friends): Fall asleep
- When sitting and talking to another person (business meetings, etc.): Doze off
- When lying down to rest/snooze while awake but eyes closed: Fall asleep
- Just before lunchtime or immediately after: Doze off
- While sitting and inactively watching TV: Fall asleep
- While sitting in a public place reading: Fall asleep
Scoring Scale40
- 0: Would NEVER doze
- 1: Slight chance of dozing
- 2: Moderate chance of dozing
- 3: High chance of dozing
Situations for Assessment41
- Sitting and reading
- Watching TV
- Sitting, inactive in a public place (e.g. a theatre or a meeting)
- As a passenger in a car for an hour without a break
- Lying down to rest in the afternoon when circumstances permit
- Sitting and talking to someone
- Sitting quietly after a lunch without alcohol
- In a car, while stopped for a few minutes in the traffic
Score Interpretation42
- 0–5: Lower Normal Daytime Sleepiness
- 6–10: Higher Normal Daytime Sleepiness
- 11–12: Mild Excessive Daytime Sleepiness
- 13–15: Moderate Excessive Daytime Sleepiness
- 16–24: Severe Excessive Daytime Sleepiness
Note: A score of 8 or more may indicate a need for Medicare.
Clinical Considerations43
- ESS is not correlated with Sleep Disordered Breathing (SDB) at mild to moderate levels in women and has a smaller association than in men with severe SDB.
- It is a poor marker of OSA but does predict response to treatment when elevated.
(Lipford et al. 2019)
Management Principles and Interventions
Clinical Diagnostic Framework44
When evaluating the facets of bruxism, clinicians should address the following diagnostic questions:
Clinical Categorization of Behavior
- Harmless Behavior: No pain or dental damage; treatment is not required.
- Risk Behavior: Causes pain or structural damage; intervention is needed.
- Protective Behavior: Such as maintaining an airway in OSA; the underlying condition should be managed instead.
- Is it Bruxism?
- Is it Awake or Sleep Bruxism?
- Is it harmless, a risk, or a protective behavior?
- Is it primary or secondary?
- How bad is it?
- Are there modifiable factors (e.g., stress)?
- Am I going to manage this?
- How?
Research Case Study: Awake Bruxism in College Preparatory Students
Study Overview
-
Objective: To assess the frequency of reported masticatory muscle activity during wakefulness (awake bruxism [AB]), levels of anxiety, depression, stress, and oral health–related quality of life (OHRQoL) in college preparatory students.
-
Methods: Sixty-nine students participated. AB was evaluated via the Oral Behavioural Checklist (OBC) and smartphone-based ecological momentary assessment (EMA). Psychosocial factors were measured using the Hospital Anxiety and Depression Scale, the Perceived Stress Scale, and the Oral Health Impact Profile 14.
-
Results: The average EMA-reported frequency of AB behaviors was 38.4%. Significant correlations were found between AB and the OBC, anxiety, depression, stress, and OHRQoL.
-
Conclusion: College preparatory students demonstrated a moderate frequency of AB, which was significantly correlated with psychosocial factors.
-
Awake bruxism is more strongly associated with stress than sleep bruxism.
Introduction to Awake Bruxism (AB) Bruxism is a behavior characterized by clenching and/or grinding of teeth, and/or by bracing or thrusting of the jaw muscles. It has two circadian manifestations: sleep and awake bruxism. AB has a multifaceted etiology involving biological and psychosocial factors. Genetics, environment, and lifestyle factors contribute to susceptibility across different age groups. Literature suggests a prevalence of approximately 22-30% in the population, with higher rates in younger individuals, often associated with increased pain and reduced quality of life.
Psychosocial Impact on Students High prevalence of Temporomandibular Disorder (TMD) signs and symptoms has been observed in college preparatory students, linked to emotional tension and anxiety. The competitive nature of college entrance exams, accompanied by social and family pressure, creates an extremely stressful environment. Frequent AB in this group may lead to orofacial pain, which can cyclically worsen psychological symptoms.
Assessment Methodology Smartphone-based ecological momentary assessment (EMA) has been introduced to quantify AB frequency. This method provides real-time data collection within an individual’s natural environment. While previous studies associated oral parafunctions with academic stages, this research specifically highlights the correlation between AB frequency and psychological factors in the college preparatory demographic.
Assessment of Severity
Instrumental and Non-Instrumental Approaches45
If management is required, the severity of bruxism should be assessed using the following methods:
- Non-Instrumental:
- Self-report: evaluating time frame and presence
- Bed partner report
- Smartphone applications
- Instrumental:
- Electromyographic recordings
- Ecological Momentary Assessment (EMA)
- Polysomnography
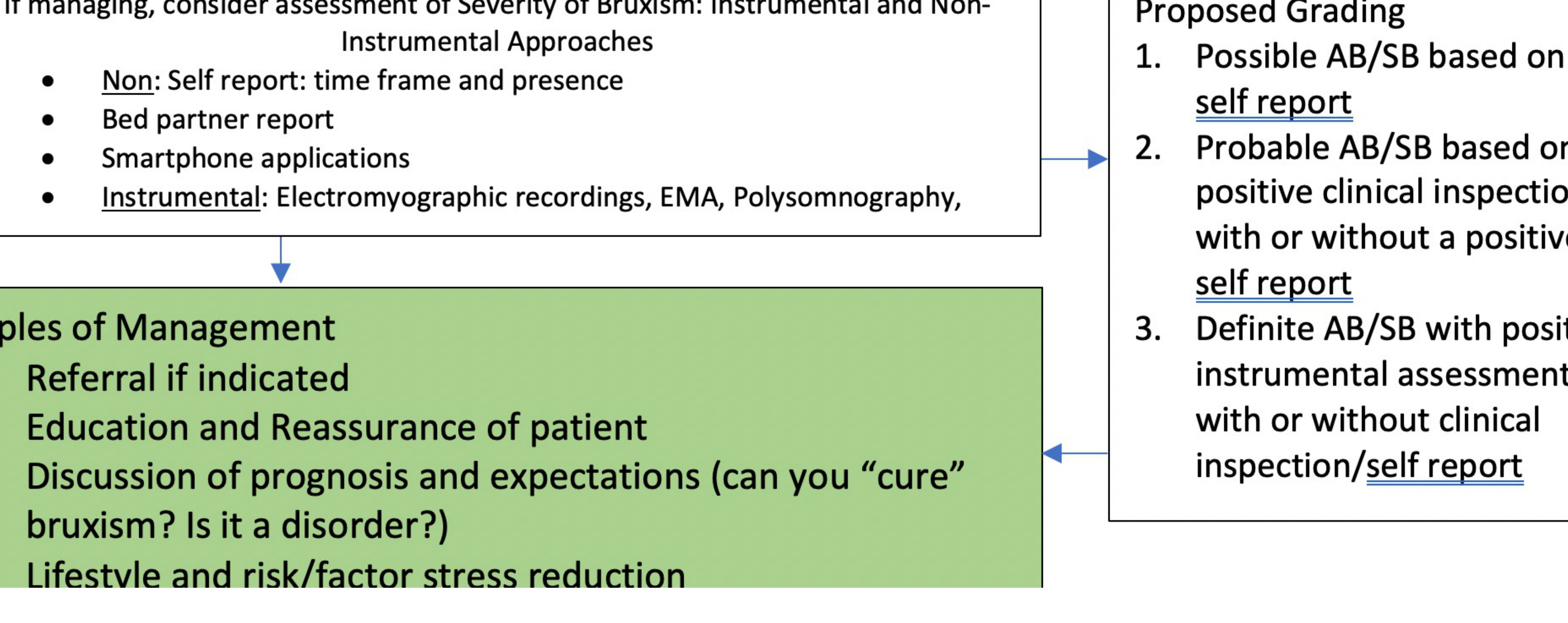
Principles of Management
- Referral if indicated
- Education and reassurance of the patient
- Discussion of prognosis and expectations (e.g., addressing whether bruxism can be “cured” or if it is classified as a disorder)
- Lifestyle modifications and reduction of risk factors/stress
Proposed Diagnostic Grading
- Possible AB/SB: Based on self-report alone.
- Probable AB/SB: Based on positive clinical inspection, with or without a positive self-report.
- Definite AB/SB: Confirmed with positive instrumental assessment, with or without clinical inspection or self-report.
The assessment of bruxism severity is a critical step in determining the necessity and type of clinical intervention. Because bruxism is often considered a behavior rather than a disorder in otherwise healthy individuals, severity is judged based on the presence and extent of clinical consequences.
Clinical Indicators of Severity46
- Dental Damage: Evaluation of tooth wear (attrition), fractured restorations, or cracked teeth that exceed what is expected for the patient’s age.
- Musculoskeletal Symptoms: Presence of morning jaw muscle stiffness, fatigue, or pain in the masticatory muscles.
- Temporomandibular Joint (TMJ) Status: Assessment of joint sounds, locking, or pain associated with jaw movement.
- Hypertrophy: Noticeable enlargement of the masseter or temporal muscles resulting from chronic overactivity.
Diagnostic Grading System
To standardize the assessment, a grading system is utilized to categorize the certainty of the bruxism diagnosis:
- Possible Bruxism: Based solely on self-report via questionnaires or clinical history.
- Probable Bruxism: Based on self-report plus a clinical examination confirming signs such as masseter hypertrophy or specific patterns of tooth wear.
- Definite Bruxism: Based on self-report, clinical examination, and confirmed by instrumental assessment, such as polysomnography (for sleep bruxism) or electromyography (for awake bruxism).
Impact on Management
Severity assessment dictates the transition from observation to active management. While mild, non-symptomatic bruxism may only require monitoring, severe cases involving significant pain or rapid dental destruction necessitate immediate multi-modal intervention strategies.
Psychosocial and Physical Therapies
Management Strategies47
- Education and reassurance
- Psychosocial management
- Habit reversal
- Ecological momentary assessment
- Physiotherapy
- Occlusal splinting
- Biofeedback and Physiotherapy can be helpful management strategies.

Bruxism Splint Specifications
- Flat plane design
- Hard material
- Light, even contacts
- Note: Do not use in conjunction with retainers
- Purpose: To protect the dentition, not necessarily to stop the muscle activity.
- Contraindications: Soft splints or "soft retainers" may increase masticatory muscle activity.
- Risks: All splints, including flat-plane ones, can cause tooth movement; this must be included in informed consent.
- Maintenance: Splints must be checked regularly for evenness and kept in a case to avoid damage (e.g., by pets).
Occlusal Splint Therapy484950
Don’t just “Splint and Split”!
Your Splint’s Worst Enemy!
BruxApp
 |  |
Pharmacotherapy and Botulinum Toxin
- BruxApp acts as a reminder system for patients to check their jaw position and keep teeth apart.
Additional Considerations51
- Botulinum toxin (Botox) injections
- Pharmacotherapy

Clinical Study Overview52
This double-blinded, randomised, placebo-controlled, cross-over study (N=35) reviewed the Bruxism Index (average bruxism events per hour of sleep using surface EMG) across three groups injected with BTX-A compared to a placebo group:
- Bilateral masseter muscles (60U)
- Bilateral masseter and temporalis muscles (90U)
- Bilateral masseter, temporalis, and medial pterygoid muscles (120U)
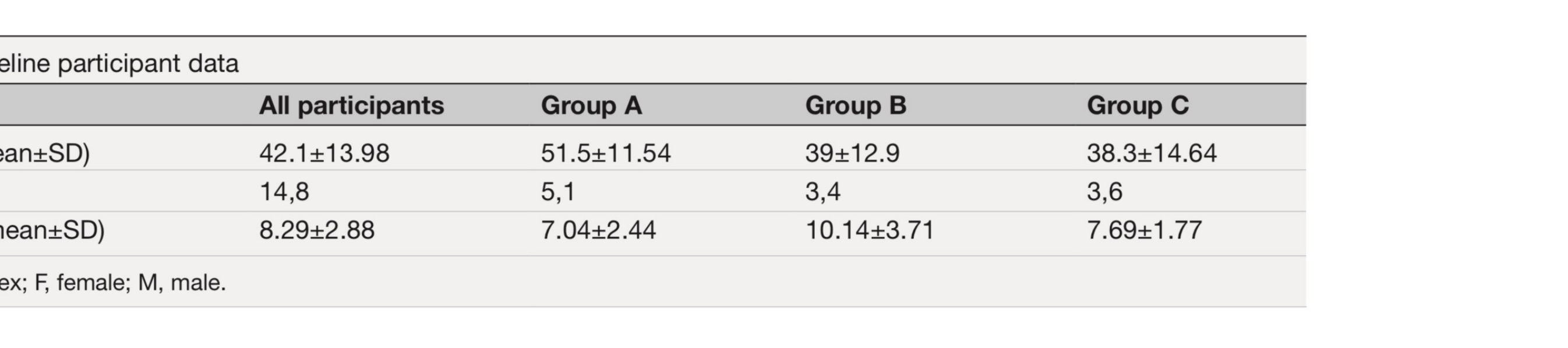
Baseline Participant Data
| Variables | All participants | Group A | Group B | Group C |
|---|---|---|---|---|
| Age years (mean±SD) | 42.1±13.98 | 51.5±11.54 | 39±12.9 | 38.3±14.64 |
| Sex (F, M) | 14, 8 | 5, 1 | 3, 4 | 3, 6 |
| Baseline BI (mean±SD) | 8.29±2.88 | 7.04±2.44 | 10.14±3.71 | 7.69±1.77 |
BI: Bruxism Index; F: female; M: male.
Study Results and Summary53
- The Bruxism Index was significantly lower at 4 weeks after active treatment compared with placebo in all groups, but this improvement was not sustained at 12 weeks.
- Improvement was greater with higher doses of BTX-A injected.
- Greatest benefit was observed when BTX-A was administered into more muscles (masseter, temporalis, and medial pterygoid) and at a higher dose in subjects with a higher baseline Bruxism Index.
- Question for consideration: What happens at 3 months?
Clinical Considerations for Botox
- Cost: High cost (approx. $1,000 per treatment) makes it unsustainable for most.
- Indications: May be used for acute flare-ups or in specific movement disorders like Parkinson’s, but not generally indicated for simple bruxism.
Research Publication Details
Title: Efficacy of botulinum toxin type a in the targeted treatment of sleep bruxism: a double-blind, randomised, placebo-controlled, cross-over study.
Authors: Belinda Cruse, Thanuja Dharmadasa, Elise White, Callum Hollis, Andrew Evans, Sifat Sharmin, Tomas Kalinicik, Lynnette Kiers.
Journal: BMJ Neurology Open
Abstract Highlights
- Background: Intramuscular injections of botulinum toxin A (BTX-A) have been used for sleep bruxism (SB), but controlled trials are limited, and optimal injection strategies/doses are unknown.
- Methods: This double-blind, randomised, placebo-controlled, cross-over study evaluated efficacy.
Current Knowledge
- Botulinum-toxin A (BTX-A) is used in the treatment of sleep bruxism (SB), with varying doses and muscles targeted.
- Controlled studies and objective evidence of efficacy are currently limited.
References and Supplementary Material54
 |  |
Recommended Literature55
- Lobbezoo, F., Ahlberg, J., Raphael, K., Wetselaar, P., Glaros, A., Kato, T., Santiago, V., Winocur, E., De Laat, A., De Leeuw, R., Koyano, K., Lavigne, G., Svensson, P. and Manfredini, D., 2018. International consensus on the assessment of bruxism: Report of a work in progress. Journal of Oral Rehabilitation, 45(11), pp.837-844.
- Manfredini, D., Ahlberg, J., Aarab, G., Bracchi, A., Durham, J., Ettlin, D., Gallo, L., Koutris, M., Wetselaar, P., Svensson, P. and Lobbezoo, F., 2020. Towards a Standardized Tool for the Assessment of Bruxism (STAB)—Overview and general remarks of a multidimensional bruxism evaluation system. Journal of Oral Rehabilitation, 47(5), pp.549-556
- Works by Manfredini (world leader in bruxism and TMJ) and Bracci (creator of the BruxApp).
Answering Commonly Asked Questions about Bruxism with Professor Daniele Manfredini.
Topics include:
- Teeth grinding
- Bruxism
- A Spoonful of Medicine

Genetic Factors and Inheritance
Hereditary Patterns and Research56
- Evidence suggests a genetic component to bruxism.
- While not yet extensively studied, there appears to be a significant association with parental grinding.
- The condition is currently postulated to follow an autosomal dominant inheritance pattern.
 |  |
Summary and Key Takeaways
Clinical Considerations and Definitions57
- Tooth wear and other single clinical indicators are not pathognomonic for bruxism.
- Bruxism is a common condition that requires looking at the bigger clinical picture.
- Bruxism should not be viewed as a single entity.
- In otherwise healthy individuals, bruxism is not classified as a movement disorder or a sleep disorder.
 |  |  |
 |  |  |
Future Research Needs
- Current knowledge is incomplete; divergences in data collection and methodologies underscore the critical need for further research.
Footnotes
-
Original PDF page 1: L36 bruxism dmd 2026, p.1 ↩
-
Original PDF page 2: L36 bruxism dmd 2026, p.2 ↩
-
Original PDF page 9: L36 bruxism dmd 2026, p.9 ↩
-
Original PDF page 3: L36 bruxism dmd 2026, p.3 ↩
-
Original PDF page 4: L36 bruxism dmd 2026, p.4 ↩
-
Original PDF page 5: L36 bruxism dmd 2026, p.5 ↩
-
Original PDF page 6: L36 bruxism dmd 2026, p.6 ↩
-
Original PDF page 7: L36 bruxism dmd 2026, p.7 ↩
-
Original PDF page 8: L36 bruxism dmd 2026, p.8 ↩
-
Original PDF page 10: L36 bruxism dmd 2026, p.10 ↩
-
Original PDF page 11: L36 bruxism dmd 2026, p.11 ↩
-
Original PDF page 12: L36 bruxism dmd 2026, p.12 ↩
-
Original PDF page 15: L36 bruxism dmd 2026, p.15 ↩
-
Original PDF page 13: L36 bruxism dmd 2026, p.13 ↩
-
Original PDF page 14: L36 bruxism dmd 2026, p.14 ↩
-
Original PDF page 16: L36 bruxism dmd 2026, p.16 ↩
-
Original PDF page 17: L36 bruxism dmd 2026, p.17 ↩
-
Original PDF page 18: L36 bruxism dmd 2026, p.18 ↩
-
Original PDF page 19: L36 bruxism dmd 2026, p.19 ↩
-
Original PDF page 20: L36 bruxism dmd 2026, p.20 ↩
-
Original PDF page 21: L36 bruxism dmd 2026, p.21 ↩
-
Original PDF page 22: L36 bruxism dmd 2026, p.22 ↩
-
Original PDF page 23: L36 bruxism dmd 2026, p.23 ↩
-
Original PDF page 25: L36 bruxism dmd 2026, p.25 ↩
-
Original PDF page 26: L36 bruxism dmd 2026, p.26 ↩
-
Original PDF page 24: L36 bruxism dmd 2026, p.24 ↩
-
Original PDF page 27: L36 bruxism dmd 2026, p.27 ↩
-
Original PDF page 29: L36 bruxism dmd 2026, p.29 ↩
-
Original PDF page 28: L36 bruxism dmd 2026, p.28 ↩
-
Original PDF page 30: L36 bruxism dmd 2026, p.30 ↩
-
Original PDF page 31: L36 bruxism dmd 2026, p.31 ↩
-
Original PDF page 32: L36 bruxism dmd 2026, p.32 ↩
-
Original PDF page 33: L36 bruxism dmd 2026, p.33 ↩
-
Original PDF page 34: L36 bruxism dmd 2026, p.34 ↩
-
Original PDF page 35: L36 bruxism dmd 2026, p.35 ↩
-
Original PDF page 36: L36 bruxism dmd 2026, p.36 ↩
-
Original PDF page 37: L36 bruxism dmd 2026, p.37 ↩
-
Original PDF page 38: L36 bruxism dmd 2026, p.38 ↩
-
Original PDF page 39: L36 bruxism dmd 2026, p.39 ↩
-
Original PDF page 40: L36 bruxism dmd 2026, p.40 ↩
-
Original PDF page 41: L36 bruxism dmd 2026, p.41 ↩
-
Original PDF page 42: L36 bruxism dmd 2026, p.42 ↩
-
Original PDF page 43: L36 bruxism dmd 2026, p.43 ↩
-
Original PDF page 44: L36 bruxism dmd 2026, p.44 ↩
-
Original PDF page 45: L36 bruxism dmd 2026, p.45 ↩
-
Original PDF page 46: L36 bruxism dmd 2026, p.46 ↩
-
Original PDF page 47: L36 bruxism dmd 2026, p.47 ↩
-
Original PDF page 48: L36 bruxism dmd 2026, p.48 ↩
-
Original PDF page 49: L36 bruxism dmd 2026, p.49 ↩
-
Original PDF page 50: L36 bruxism dmd 2026, p.50 ↩
-
Original PDF page 51: L36 bruxism dmd 2026, p.51 ↩
-
Original PDF page 52: L36 bruxism dmd 2026, p.52 ↩
-
Original PDF page 53: L36 bruxism dmd 2026, p.53 ↩
-
Original PDF page 55: L36 bruxism dmd 2026, p.55 ↩
-
Original PDF page 54: L36 bruxism dmd 2026, p.54 ↩
-
Original PDF page 56: L36 bruxism dmd 2026, p.56 ↩
-
Original PDF page 57: L36 bruxism dmd 2026, p.57 ↩