Physical & Chemical Injuries
Presentation Overview1
This session covers the various manifestations and management of physical and chemical injuries within the oral cavity, presented by Dr. Lalima Tiwari, Oral Medicine Specialist and Clinical Senior Lecturer.
Learning Objectives2
Upon completion of this module, students should be able to:
- Describe the repertoire of physical and chemical injuries that can affect the oral hard and soft tissues.
- Describe the repertoire of responses of oral soft tissues to trauma.
- Discuss the aetiology, pathogenesis, clinical and histopathologic features, diagnosis, and treatment of:
- Frictional keratosis
- Linea alba
- Morsicatio buccarum
- Traumatic ulceration
- Burns
- Discuss exfoliative cheilitis.
- Including etiology, pathogenesis, clinical and histopathologic features, diagnosis, and treatment
- Discuss the aetiology, pathogenesis, clinical and histopathologic features, diagnosis, and treatment of:
- Amalgam tattoos and other localized exogenous pigmentations
- Smoker’s melanosis
- Drug-related discoloration of oral mucosa
- Explain oral complications of radiation therapy.
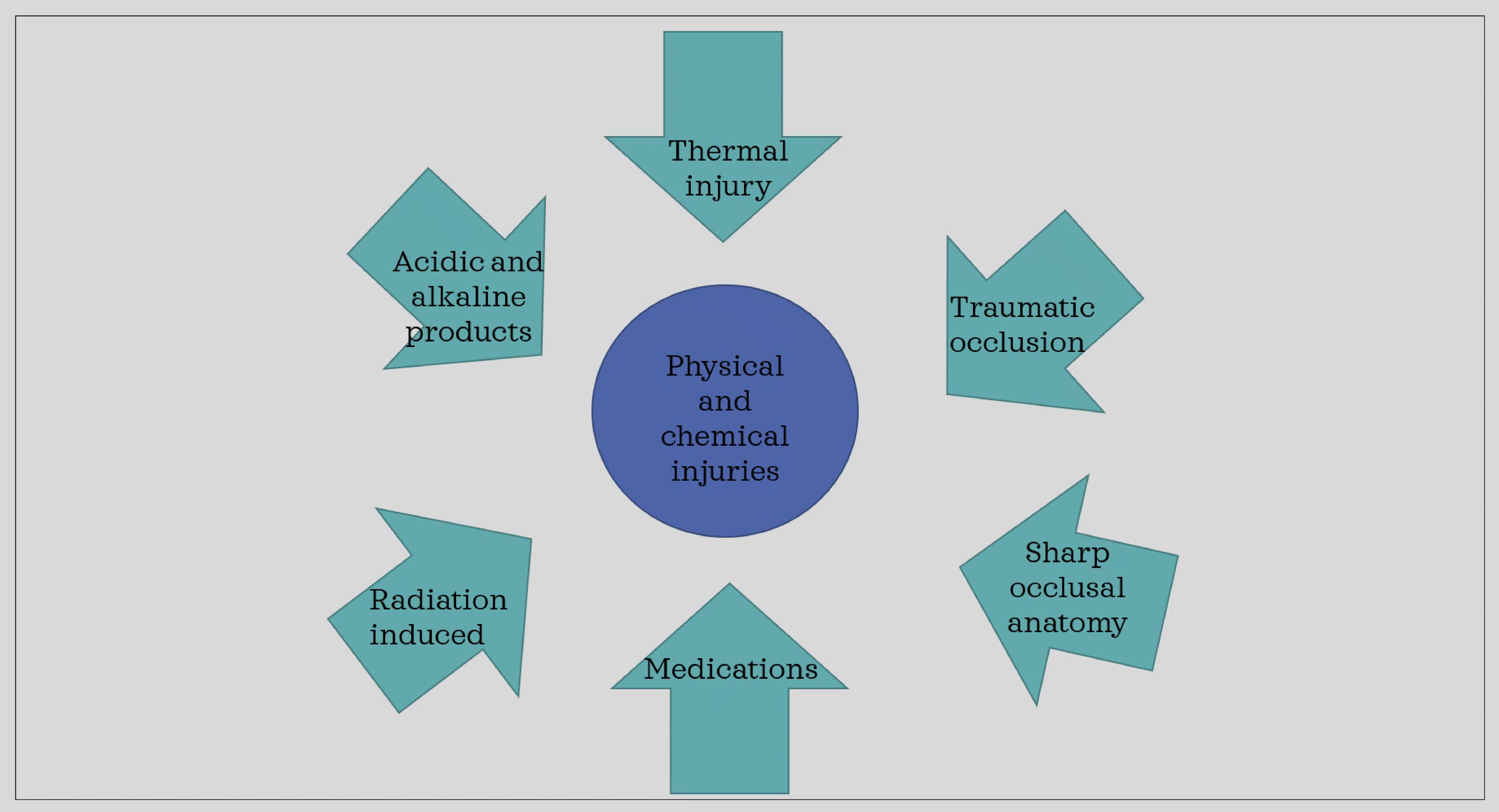
Aetiological Factors3
The following factors contribute to physical and chemical injuries in the oral cavity:
- Thermal injury
- Traumatic occlusion
- Sharp occlusal anatomy
- Medications
- Radiation induced injury
- Acidic and alkaline products
- Accidental Trauma: Falls in young children traumatizing lips
- Iatrogenic Injury: Dentists causing lesions during fillings or procedures
Frictional Keratosis45
- Represents increased keratin production in response to chronic mechanical irritation.
- Can be from:
- Fractured teeth
- Rough Restorations
- Dental prosthesis
- Abrasive foods
- Vigorous tooth brushing
- playing wind instruments
- Can be from:
The oral mucosa responds with keratin deposition and benign epithelial hyperplasia, manifesting clinically as thicker, white mucosa.


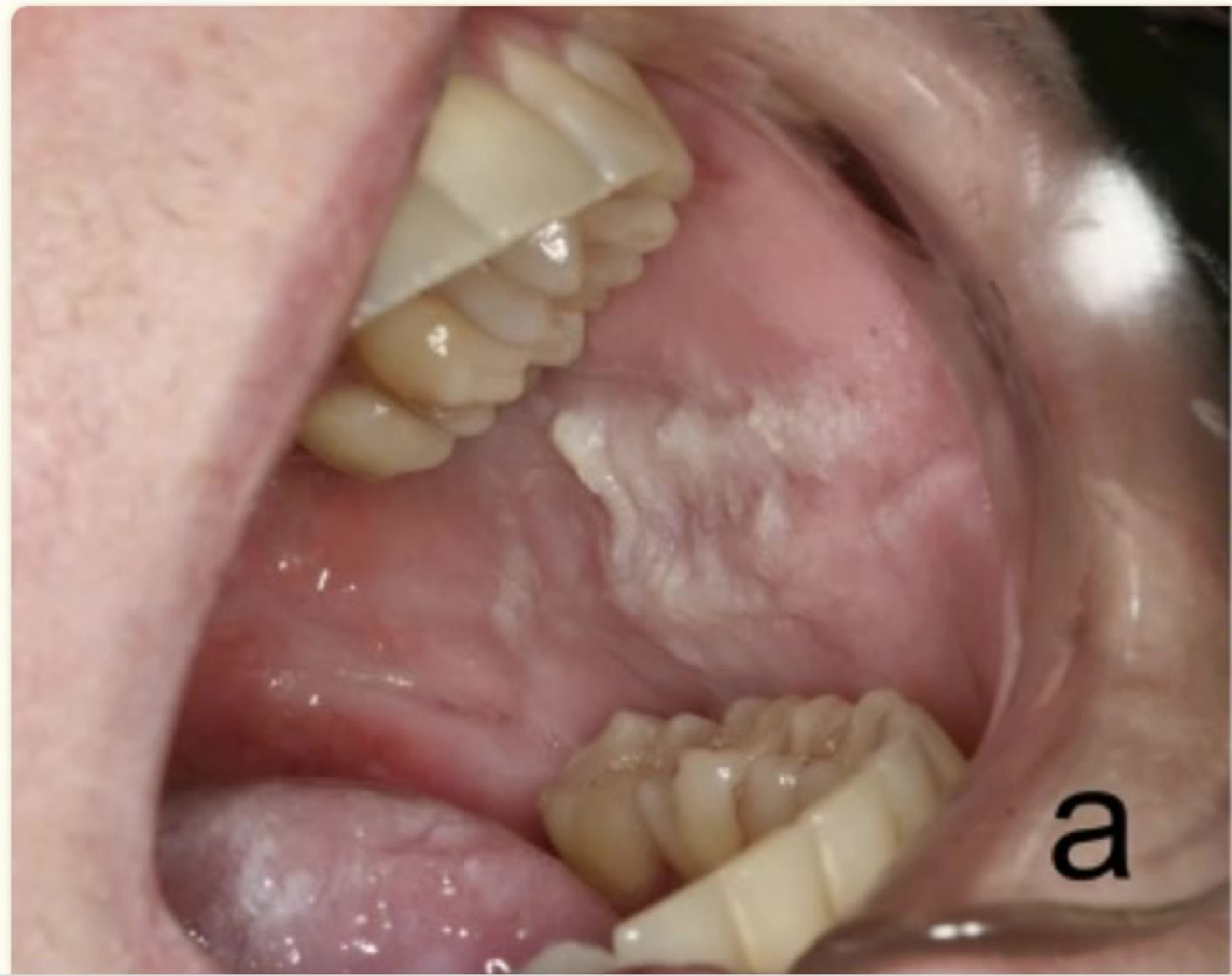
Clinical Features
- Benign alveolar ridge keratosis on retromolar pad, present bilaterally.
- Benign alveolar ridge keratosis of previously extracted teeth.
- Appearance: Ill-defined area of gray or white papules and plaques
- Texture: May be rough and diffuse
- Margins: Usually blend with the adjacent mucosa
- Complications: Associated erosions and ulcers may occur if trauma is extensive
(Content consists of clinical imagery documentation)

Clinical Variations6
- Frictional keratosis on left lateral tongue.
- Non-homogenous leukoplakia on left lateral tongue.
Case Study: Frictional Keratosis vs. Leukoplakia
Scenario 1 (Gingiva): Frictional keratosis presents as a roughish white lesion along the marginal attached gingiva. In contrast, Verrucous Leukoplakia extends the entire length of the attached gingiva. Scenario 2 (Lateral Tongue): Frictional keratosis on the left lateral tongue presents as a diffuse roughish white lesion. This can resemble Non-Homogeneous Leukoplakia. Diagnostic Approach: Identify potential trauma. If trauma is identified, manage it. If the lesion persists after trauma management, a biopsy is indicated.
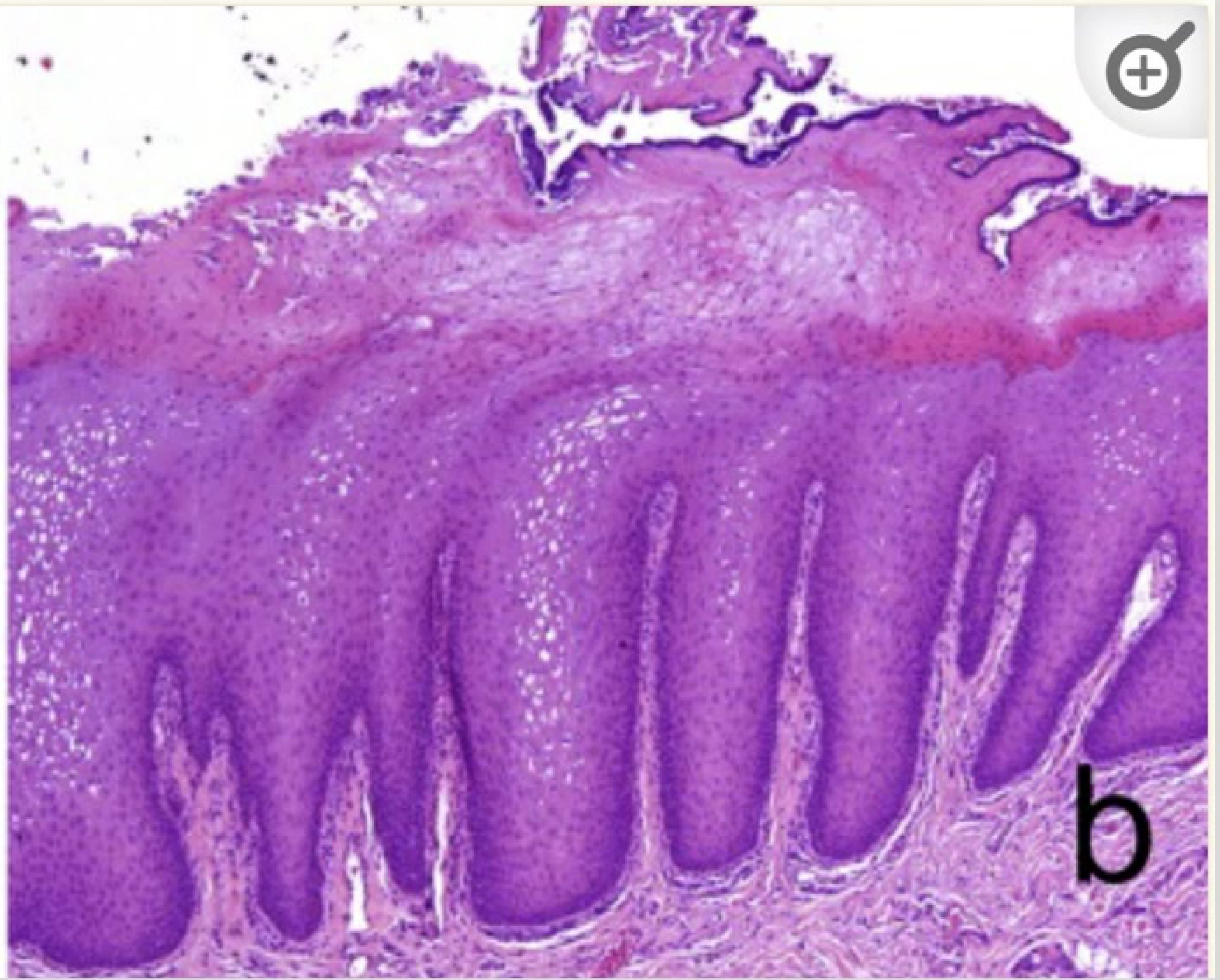
Histopathology7
-
Orthokeratosis or hyperparakeratosis
-
Shaggy keratin surface
-
Prominent granular cell layer
-
Intracellular oedema – ballooned cells in spinous layer
-
Acanthosis
-
Lack of inflammation in superficial connective tissue
-
Features of dysplasia absent
-
Acanthosis refers to epithelial hyperplasia
-
Connective tissue is usually uninflamed with thick epithelium
Diagnosis
Differential Diagnosis and Assessment8
-
Distinguish from other oral potentially malignant disorders.
-
History: Determine if the patient is aware of trauma or mechanical irritation. Assess if the source of trauma can be addressed.
-
Clinical: Observe appearance. Eliminate the source of irritation to see if the lesion resolves.
-
Investigations: Biopsy persistent or suspicious lesions, or when clinical information is limited.
-
Response: Elimination of trauma should result in improvement or elimination of the lesion (reactive lesion)
Treatment Protocols
-
Address and eliminate the source of trauma.
-
Review the patient in 2 weeks; the lesion should be eliminated if the cause is removed.
-
Chronic irritation may require habit awareness techniques.
-
These lesions do not undergo malignant transformation.
- Condition waxes and wanes depending on the parafunctional habit
- Biopsy rarely needed unless suspicion of oral potentially malignant disorder exists
Linea Alba

Characteristics and Etiology9
- Known as the “white line.”
- Common alteration of the buccal mucosa associated with pressure, irritation, or sucking trauma from teeth.
- Linked to parafunctional habits: cheek biting, clenching, and teeth grinding.
- Nature is asymptomatic and benign
Clinical Presentation
- Asymptomatic, horizontal, linear white keratotic line/ridge on the buccal mucosa approximating the occlusal plane (often bilateral).
- Can be associated with scalloping of the lateral border of the tongue (often linked to bruxism).
- Frequently mistaken for leukoplakia.
Pathology and Management
- Histopathology: Hyperkeratosis overlying normal oral mucosa; occasional intracellular oedema.
- Similar to frictional keratosis
- Diagnosis: Usually a clinical diagnosis.
- Treatment: No treatment required; no documented complications. Spontaneous regression may occur.
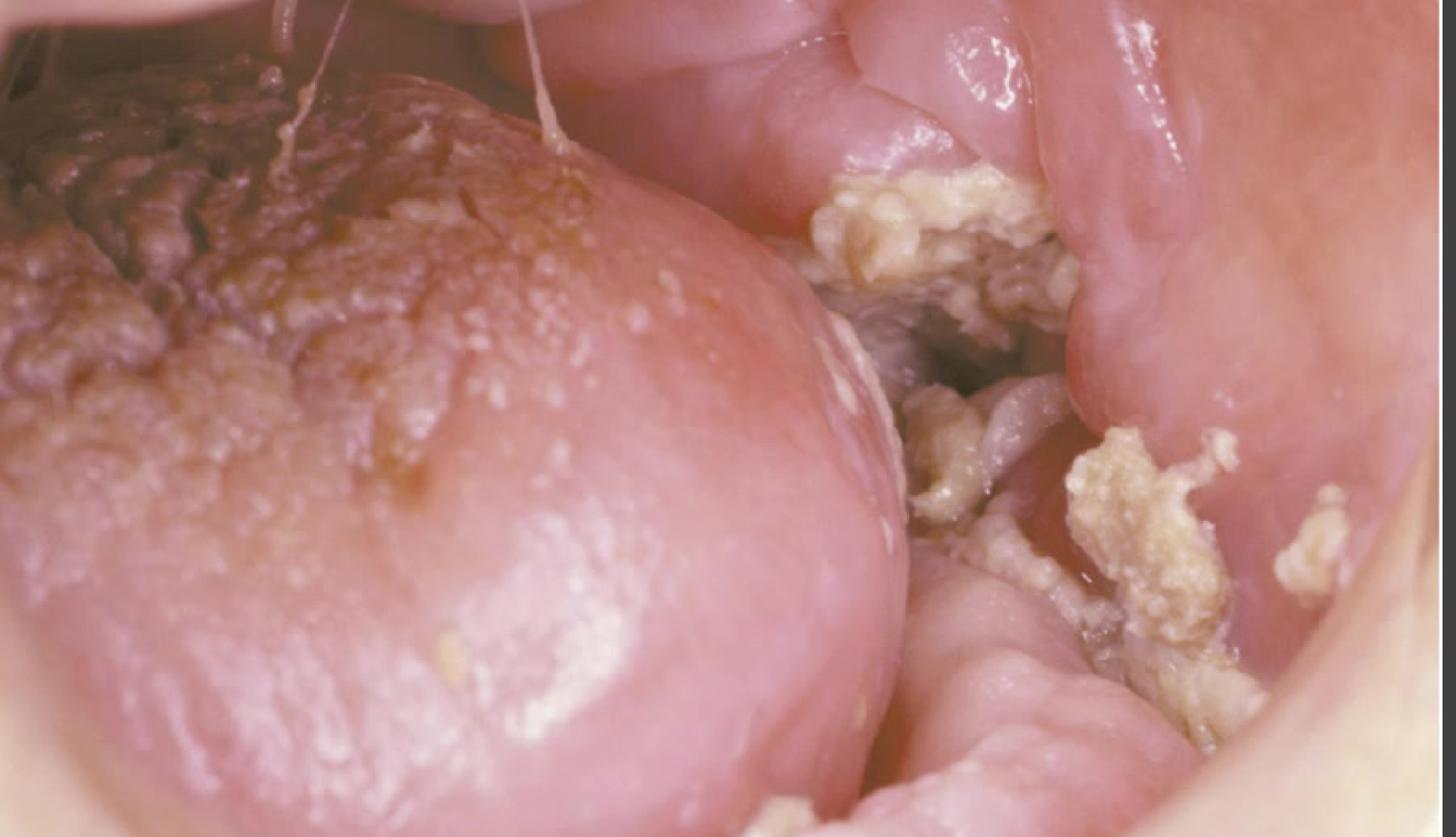
Morsicatio Buccarum
Overview10
- Chronic bite keratosis.
- Benign, trauma-induced lesion of the oral mucosa.
Etiology and Pathogenesis
-
Aetiology: Chronic trauma to non-keratinized mucosa caused by parafunctional habits (nibbling, sucking on mucosa, rubbing against dentures or orthodontic appliances).
-
Pathogenesis: Parakeratosis and benign epithelial hyperplasia.
-
==Patient Profile: Often seen in anxious or worried patients.==
-
==Location: Localized to non-keratinized mucosa (buccal, lower labial, ventral tongue); unlikely on gingiva. Primarily presents bilaterally.==
Clinical Features
-
Irregular, shaggy, macerated appearance of the buccal mucosa (morsicatio mucosae).
-
==Symptoms: Usually asymptomatic; patients are often unaware of the habit.==
-
==Surface: Top layer of white plaques can sometimes be rubbed off with gauze.==
-
==Severity: Can be associated with erythema and ulceration depending on trauma significance.==
Case Study: Clinical Appearance
Presentation: Classic presentation on the buccal mucosa. Features: Irregular, shaggy, macerated appearance indicating chewing on oral mucosa. Histopathology Correlation: Demonstrates hyperparakeratosis with shaggy epithelial surface. Epithelium is hyperplastic/acanthotic with balloon cells. Bacterial colonies may be present without inflammatory response.
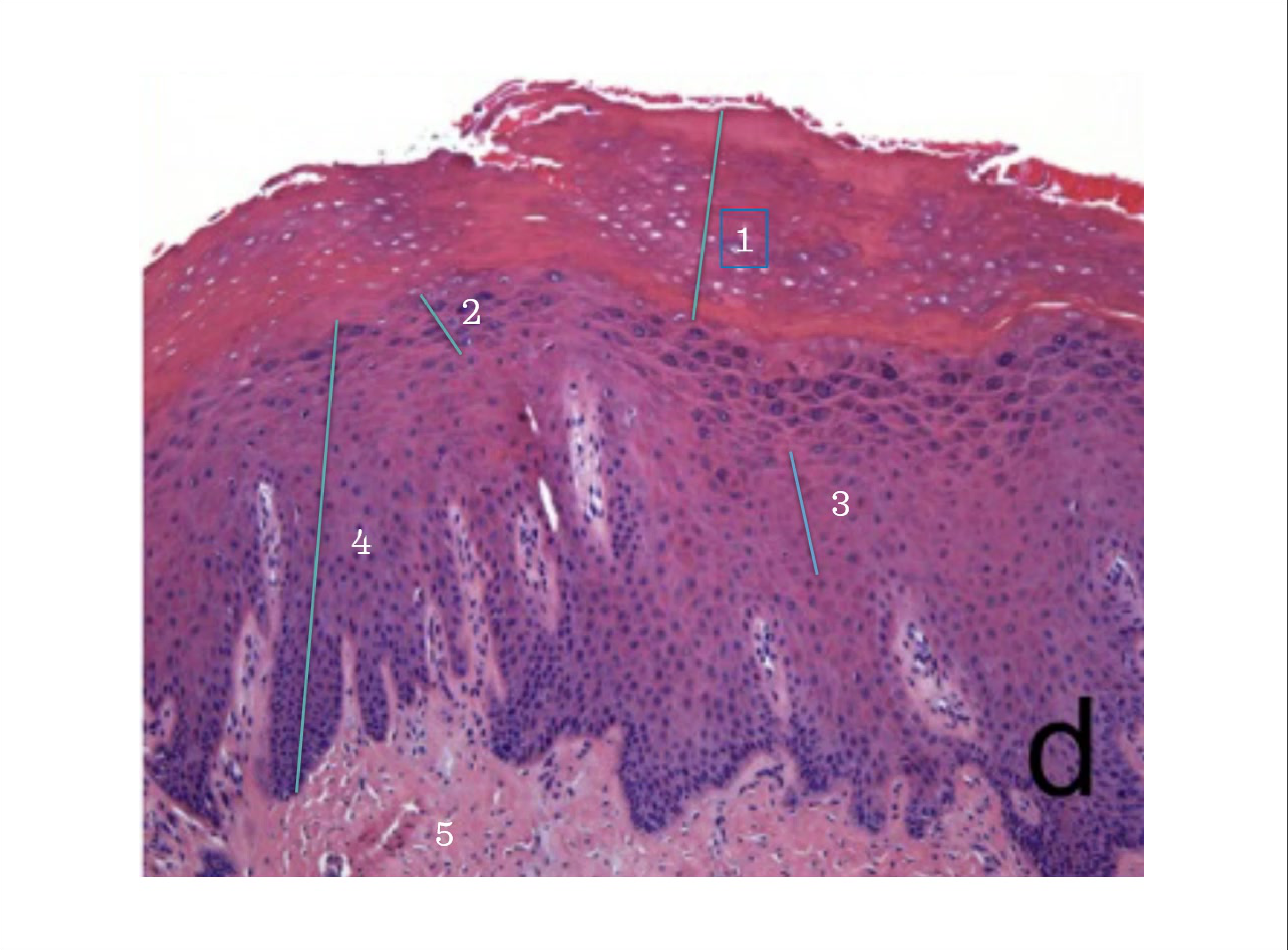
Histopathology11
-
Marked hyperparakeratosis with a shaggy appearance featuring surface fissures and clefts.
-
Acanthotic epithelium with ballooned cells.
-
Presence of bacterial colonies on the keratin surface without an inflammatory response.
-
==Comparison: Same as benign alveolar ridge keratosis.==
-
==Diagnosis: Primarily clinical. Biopsy considered to exclude underlying dysplasia if patient has risk factors (smoking, high alcohol history).==
-
==Management: Reassurance and education. Habit awareness is key, though difficult if patients are unaware of the habit.==
 |  |
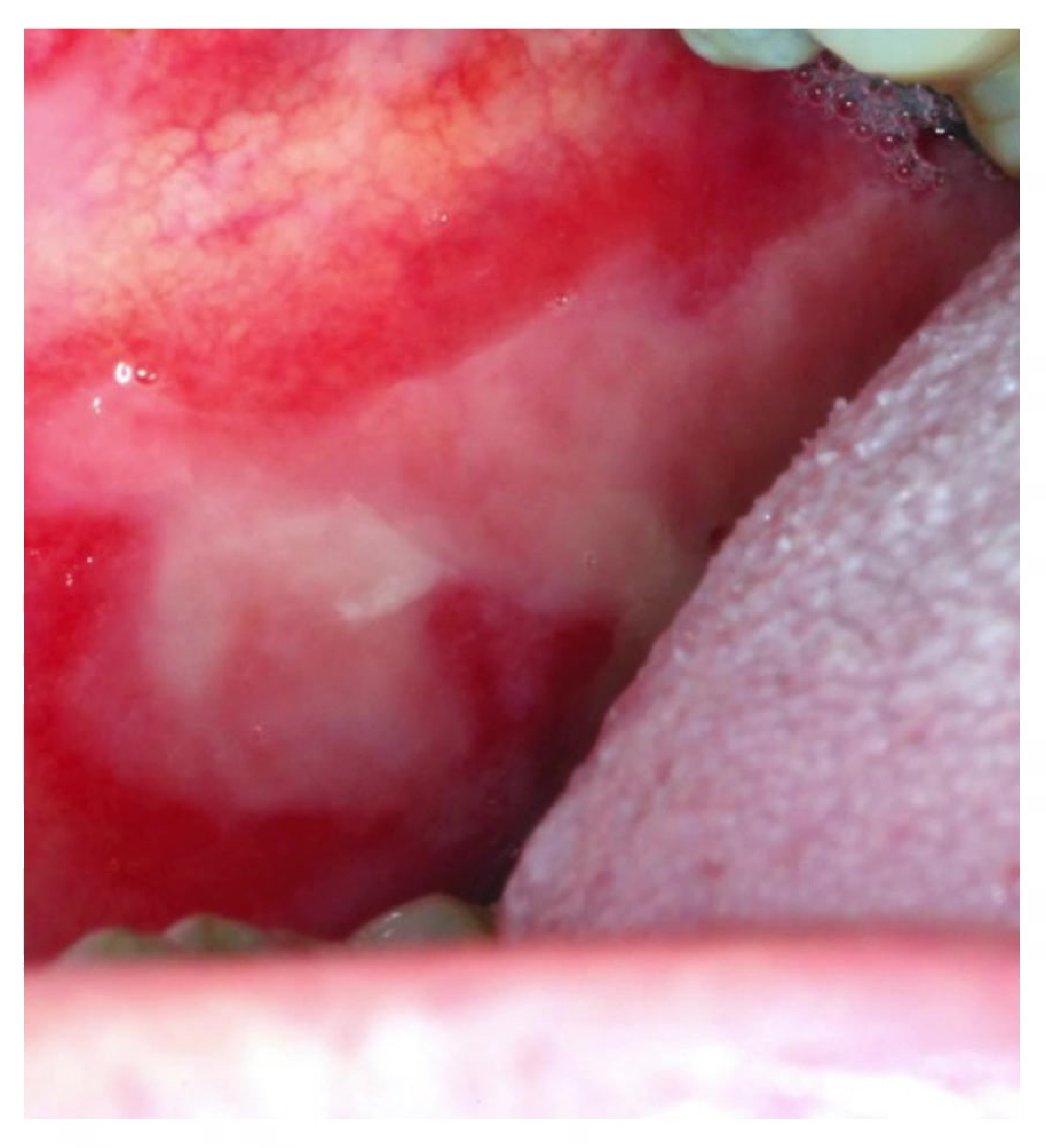
Traumatic Ulceration1213


Reactive Oral Ulcers14
- Trauma affecting the mucosal lining of the mouth.
- Causes include self-inflicted injury and mechanical trauma (sharp tooth margins, prostheses, denture flanges, self-biting, or factitious injuries).
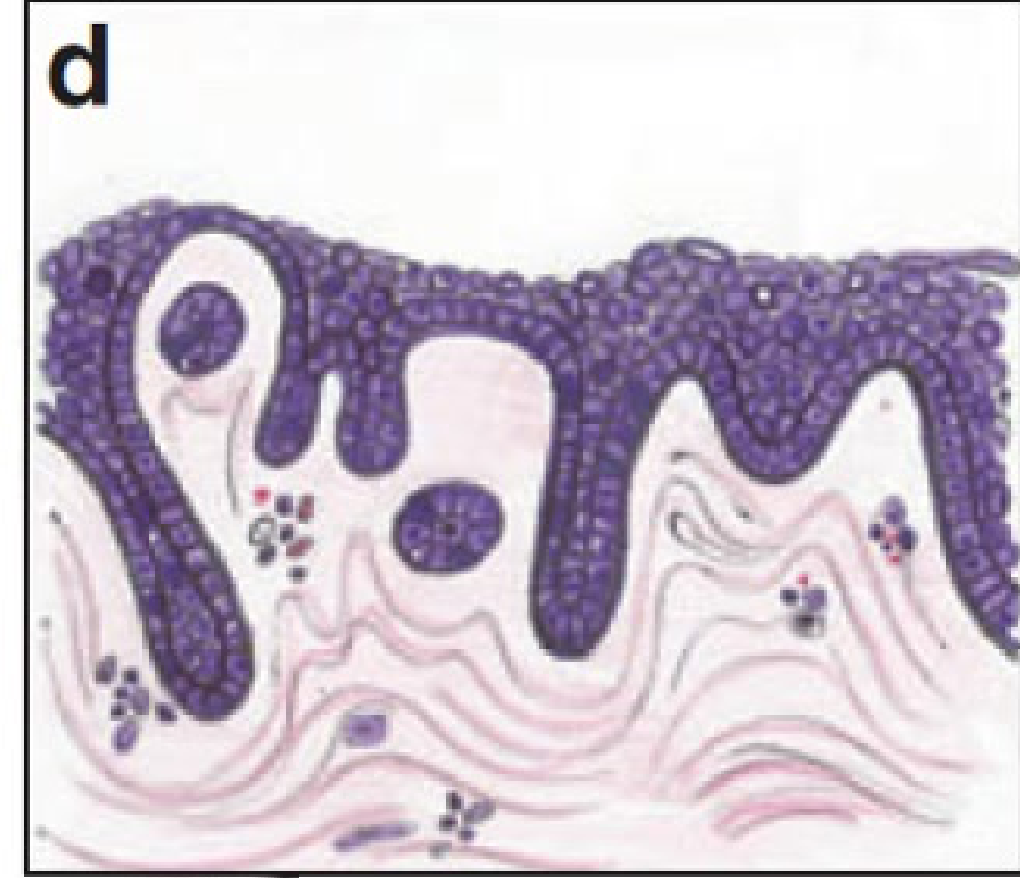
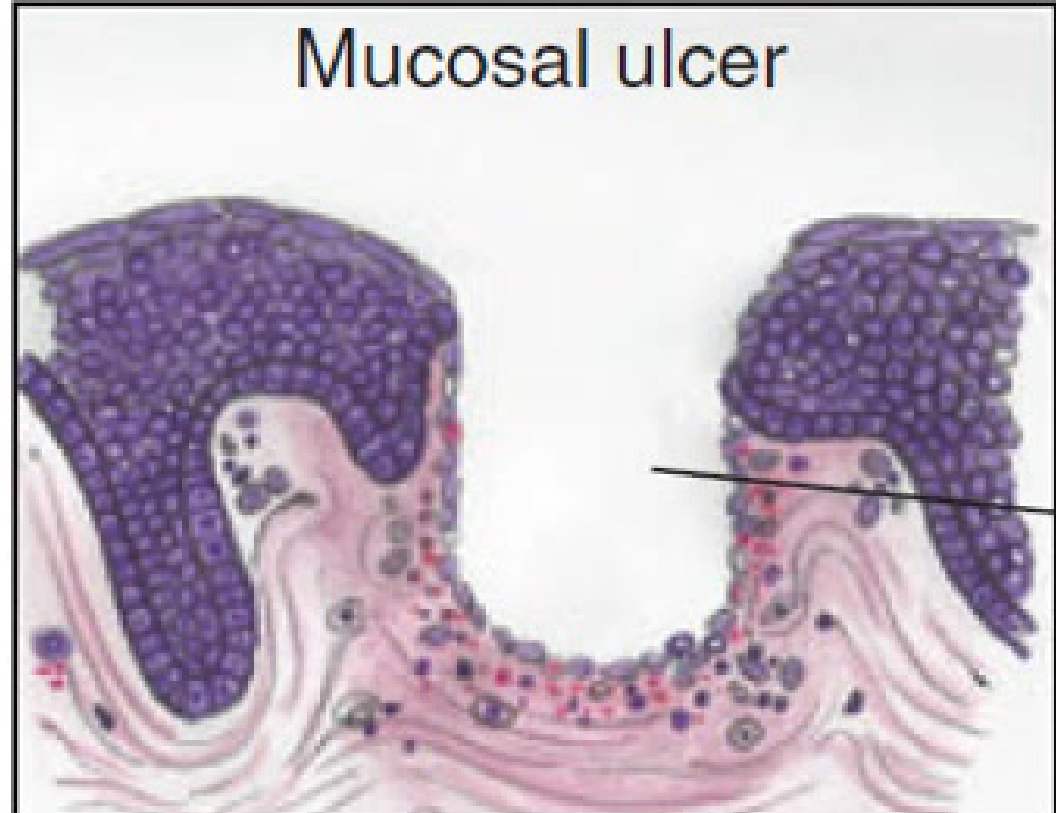
- Yellow appearance due to exposed connective tissue (epithelium/pink part is gone).
- Definition: Complete loss of epithelium exposing underlying connective tissues.
Clinical Presentation
- Mechanical appearance: Areas of erythema surrounding a central removable, yellow fibrinopurulent membrane.
- May develop a rolled white border of hyperkeratosis adjacent to the ulcer.
- Can affect any mucosal surface (tongue, lips, buccal mucosa).
Specific Conditions
- Riga-Fede disease:
- Affects children aged 1 week to 12 months.
- Associated with natal teeth.
- Most common site: anterior ventral surface of the tongue.
- Associated with neurologic conditions such as cerebral palsy and Tourette syndrome.
Diagnosis
- Based on history and clinical presentation.
- Identify the source of trauma.
- Lesions typically resolve spontaneously within 10–14 days once the causative factor is removed.
(Content consists of clinical imagery documentation)
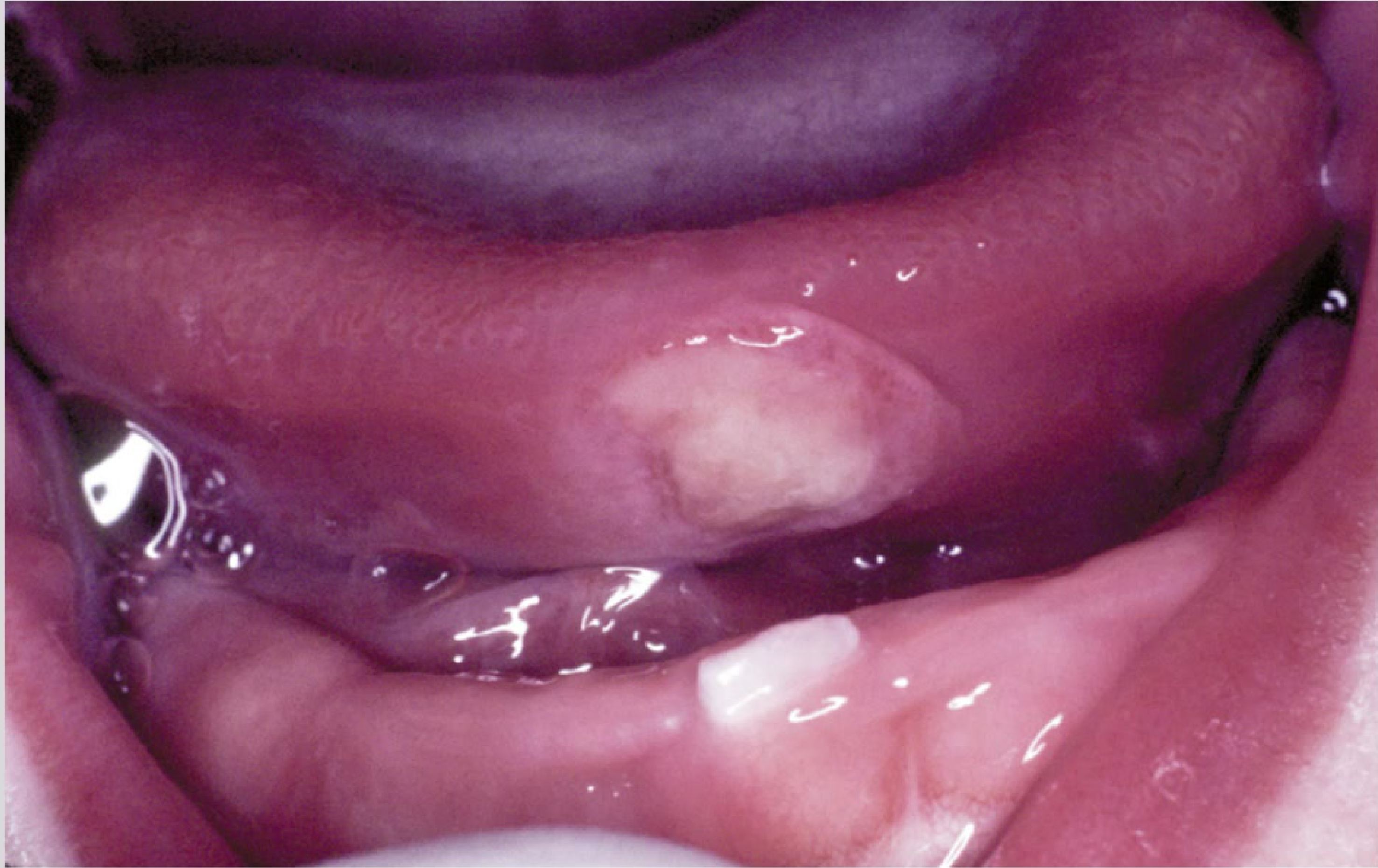
Riga-Fede Disease Case Study15
- Newborn presenting with traumatic ulceration of the anterior ventral surface of the tongue.
- Mucosal damage resulted from contact with an adjacent tooth during breastfeeding.
Traumatic Ulcer vs Squamous Cell Carcinoma
- Scenario: A classic traumatic ulcer secondary to a sharp tooth is compared with an image of squamous cell carcinoma.
- Differentiation: Suspected traumatic ulcers require identification and management of the causative trauma (e.g., adjustment of sharp tooth).
- Outcome: Review patient in two weeks. If the lesion heals, it was reactive. If it remains persistent, it is suspicious for malignancy (SCC) and requires biopsy.
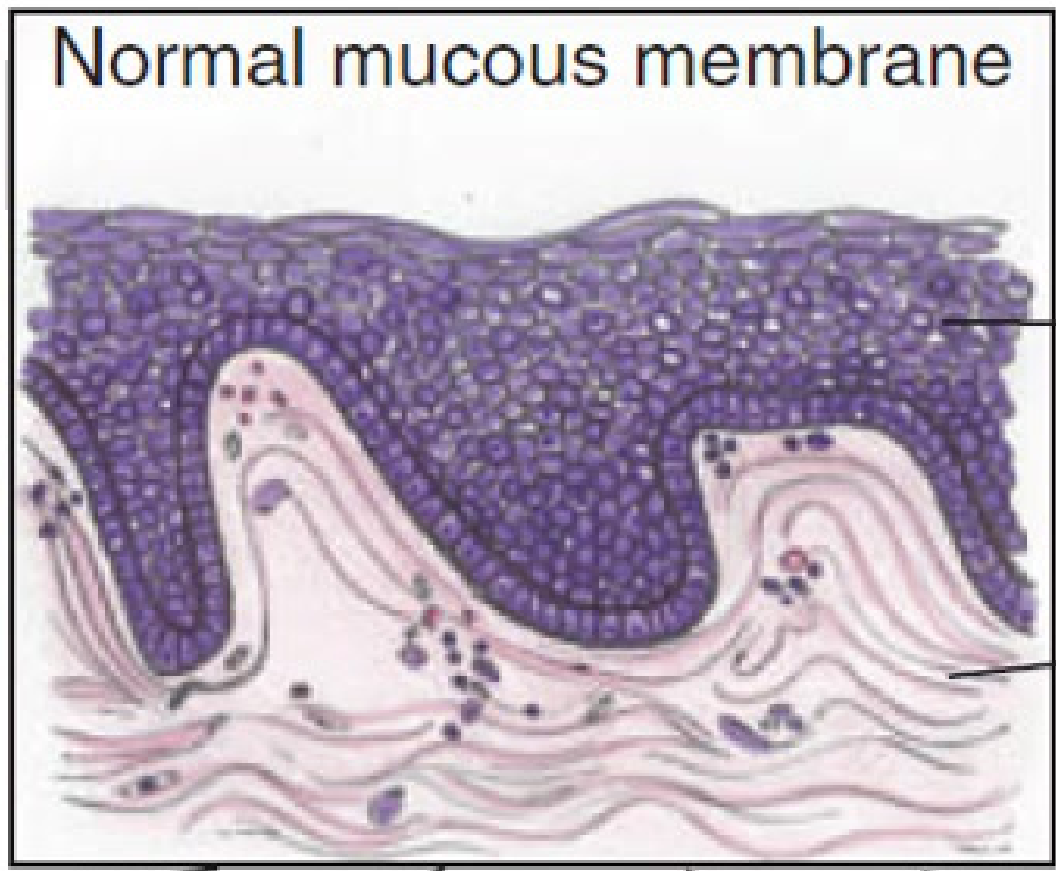
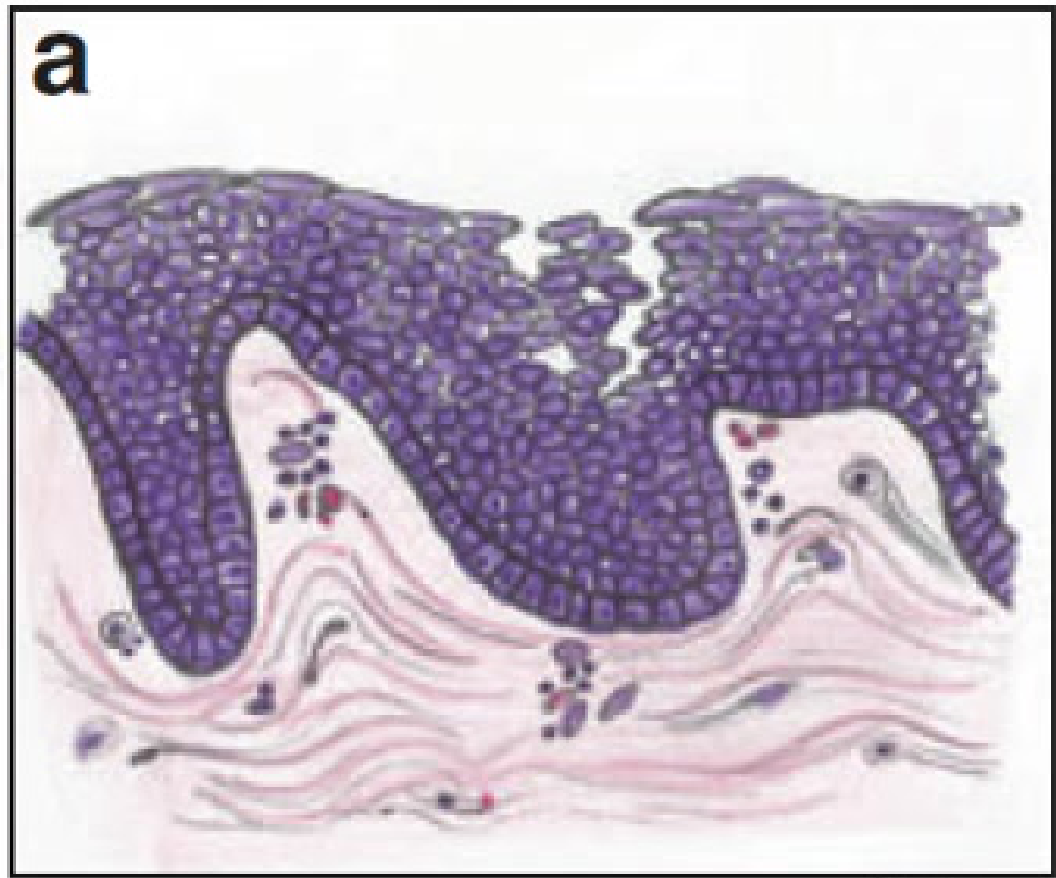
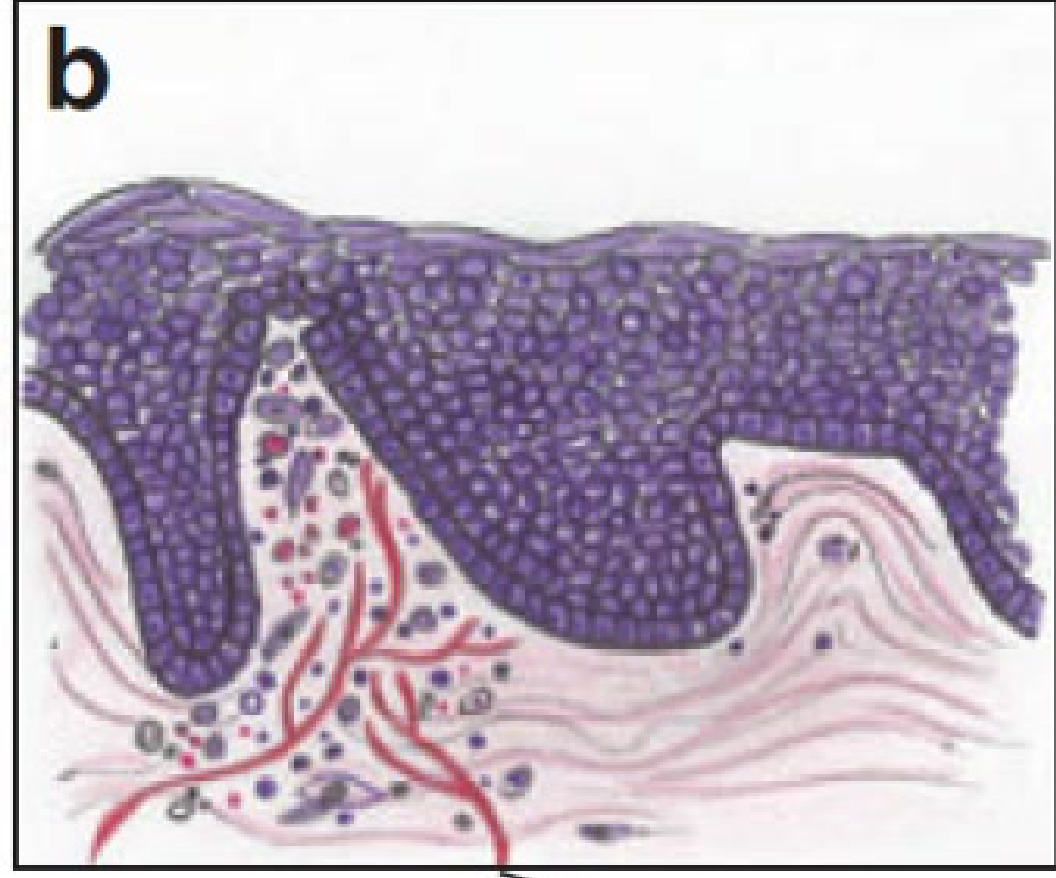
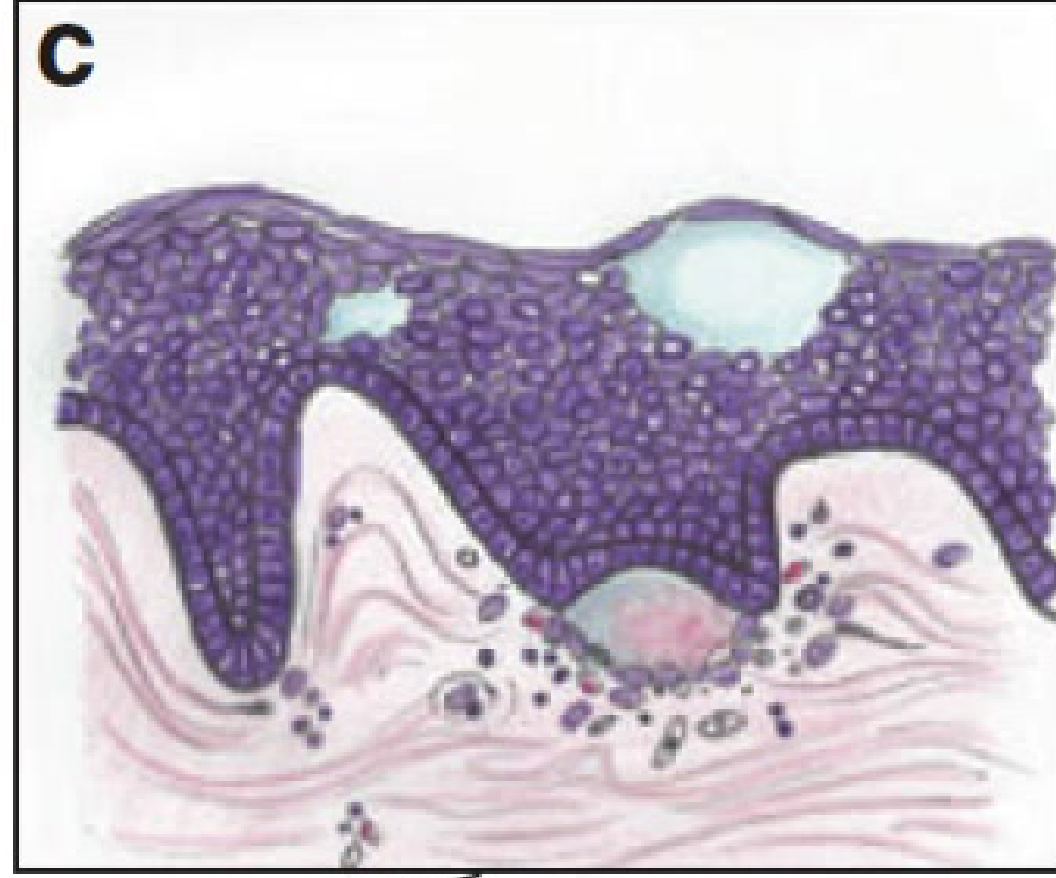
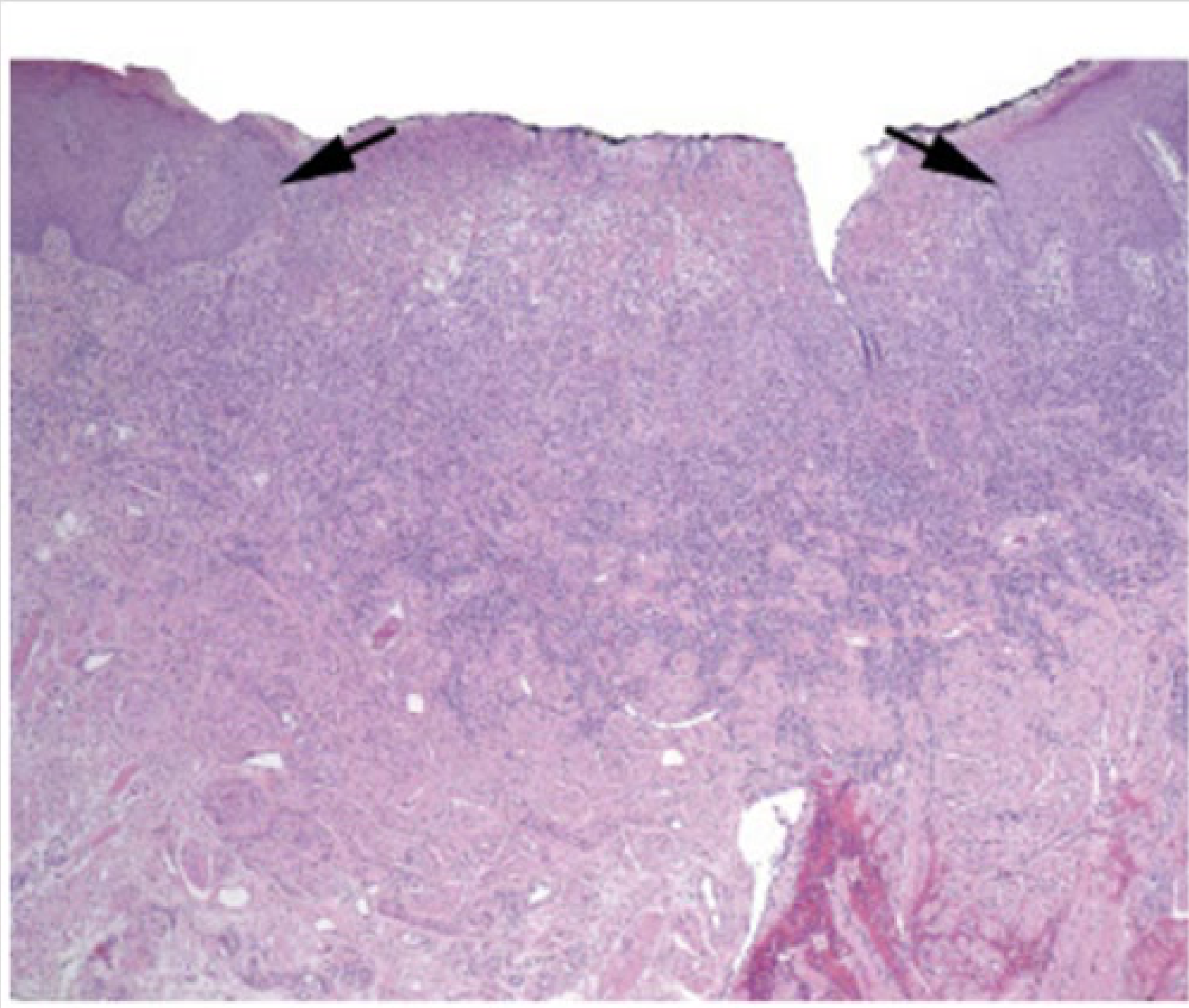
Histopathology16
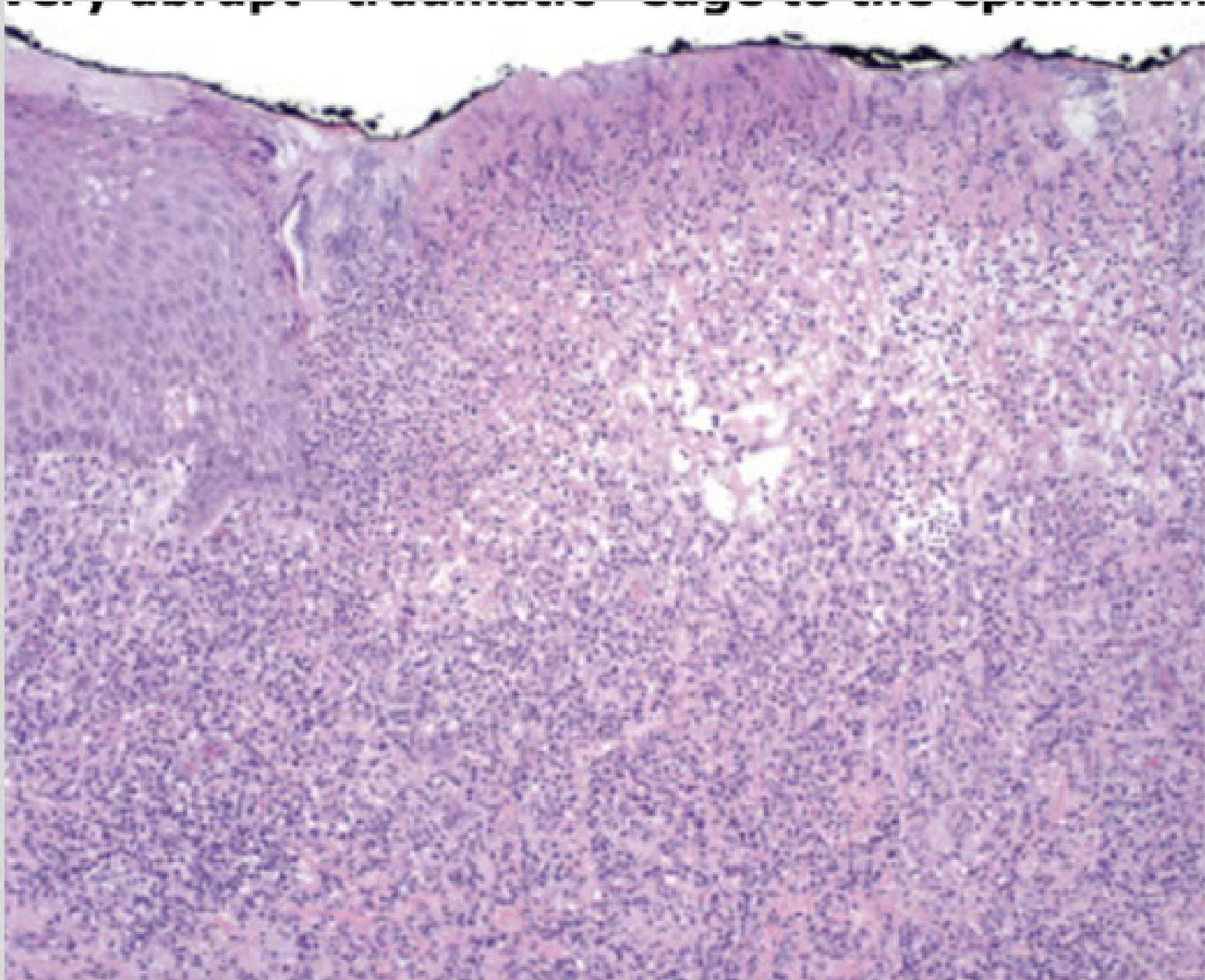
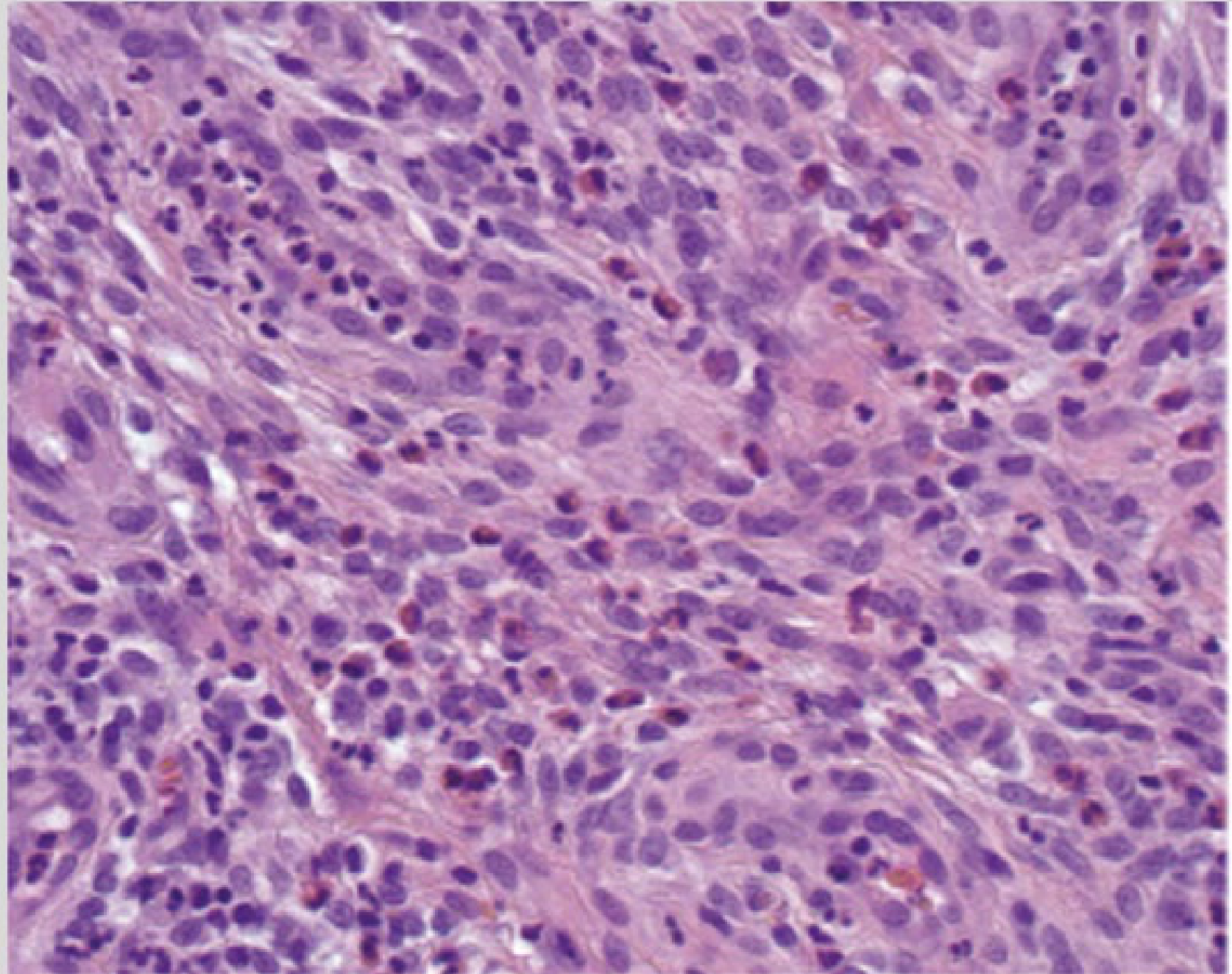
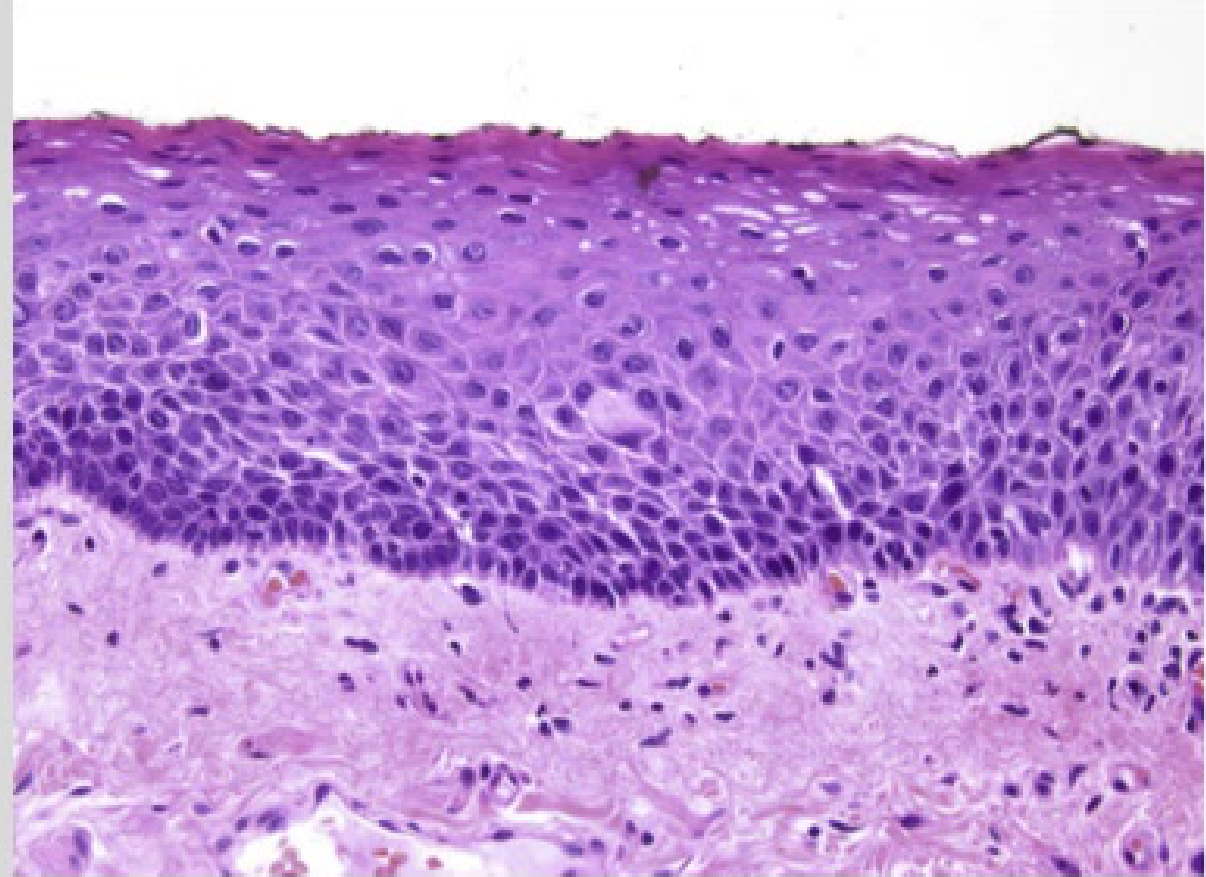
- Low-power view: Hypertrophic squamous epithelium immediately adjacent to the ulcer with an abrupt transition. Inflammatory infiltrate may extend into underlying muscle.
- Intermediate-power view: Fibrinopurulent exudate and an abrupt “traumatic” epithelial edge. Inflammation fills the stroma.
- High-power view: Granulation tissue with a mixed inflammatory infiltrate, including eosinophils and associated vessels.
Management
General Protocols17
- Identify and remove the source of trauma.
- Expect spontaneous resolution within 10–14 days post-removal.
- Supportive care:
- Chlorhexidine gel or mouthrinse.
- Lignocaine gel.
- Anti-inflammatory mouthrinse (e.g., Difflam).
- Chlorhexidine acts as an antiseptic while Lignocaine provides pain relief.
- Critical Note: Review after treatment. If the lesion persists, further investigations (including biopsy) are required to rule out malignancy.
Chronic Variants
- Traumatic Ulcerative Granuloma with Stromal Eosinophilia (TUGSE): A deep pseudoinvasive inflammatory reaction that is slow to resolve
- Unique chronic traumatic ulcers that mimic malignancy.
- Do not resolve even after addressing trauma.
- Confirmed on biopsy..
Burns

Thermal Burns
-
Caused by extreme temperatures.
-
Sources: Hot foods/drinks, microwavable items, cryogenic burns from very cold foods, and e-cigarette explosions.
-
Pathology: Tissue injury resulting in epithelial sloughing and exposure of vascularized connective tissue, leading to an erythematous appearance.
-
Presentation: Oval or circular pattern of erosion with erythematous borders and surrounding keratosis.
-
Sites: Primarily anterior hard palate or anterior dorsal tongue.
-
Severity: Cryogenic burns cause necrosis and higher risk of secondary infection.
-
Treatment: If upper airway involved with breathing difficulties, antibiotics or corticosteroids may be required.
Chemical Burns
Mechanism of Injury18
-
Acids: Bind to epithelium and denature proteins (coagulative necrosis). The resulting coagulum typically limits deeper acid penetration.
-
Alkaline substances: Dissolve protein and collagen, leading to saponification of fatty tissue and liquefactive necrosis. These do not limit tissue penetration and can cause more extensive, deeper damage than acids.
-
Prolonged contact may lead to systemic effects due to absorption.
-
Clinical Response: Immediate erythema and edema with white slough pseudomembrane covering underlying ulceration. Ulcers bleed easily and are irregular.
-
Complications: Can involve ductal openings of major salivary glands causing transient obstructive sialadenitis.
Toxic Agents19
Reported Toxic Agents Linked to Chemical Oral Burns
| Chemical Toxic Substances | Utilisation / Comment |
|---|---|
| Dental Materials | |
| Cavity varnish | Restorative liquid/gel |
| Dentine bonding agent | Restorative liquid |
| Phosphoric acid etching solutions | Restorative gel/liquid |
| Iodine / Phenol (carbolic acid) | Antiseptic liquids |
| Trichloroacetic acid / Ferric sulphate | Astringents for gingival retraction |
| Chromic acid | Therapeutic antiseptic |
| Hydrofluoric acid | Porcelain and metal etching |
| Sodium hypochlorite | Root canal irrigant |
| Calcium hydroxide | Restorative cement |
| Formocresol | Endodontic pulp medicament |
| Paraformaldehyde / Arsenic | Devitalising agents |
| Medications | |
| Chlorpromazine / Promazine | Antipsychotic drugs |
| Aspirin | Non-opioid analgesic |
| Alendronate | Bisphosphonate |
| Non-Pharmaceutical Substances | |
| Mouthwashes / Hydrogen peroxide | Oral antiseptics |
| Gasoline / Rubbing alcohol | Fuel / High-volume alcohol |
| Battery acid | Sulphuric acid |
| Minard’s liniment / Arrack | Pain relief / Distilled spirit |
| Silver nitrate | Chemical cauterisation |
| Denture cleansers | Cleaning tablets |
| Fresh fruit and fruit juices | Acidic liquids |
| Garlic | Culinary/medicinal vegetable |
| Drugs | |
| Cocaine / MDMA / Amphetamine | Recreational drugs |
(Page intentionally blank or contains no unique text content)
- Note: Use of rubber dam is critical when using dental materials.
- Medications: Aspirin burns often occur when patients place tablet in buccal mucosa.
Case Study: Aspirin Induced Chemical Burn
- Presentation: Patient placed aspirin tablet in the buccal sulcus.
- Features: Local burn in the area. Residual aspirin visible on the premolar tooth.
Case Study: Sulfuric Acid Burn
- Presentation: Extensive ulceration of the palate and lateral aspects of the tongue.
- Cause: Secondary to the application of sulfuric acid.
 3.webp]]
3.webp]]


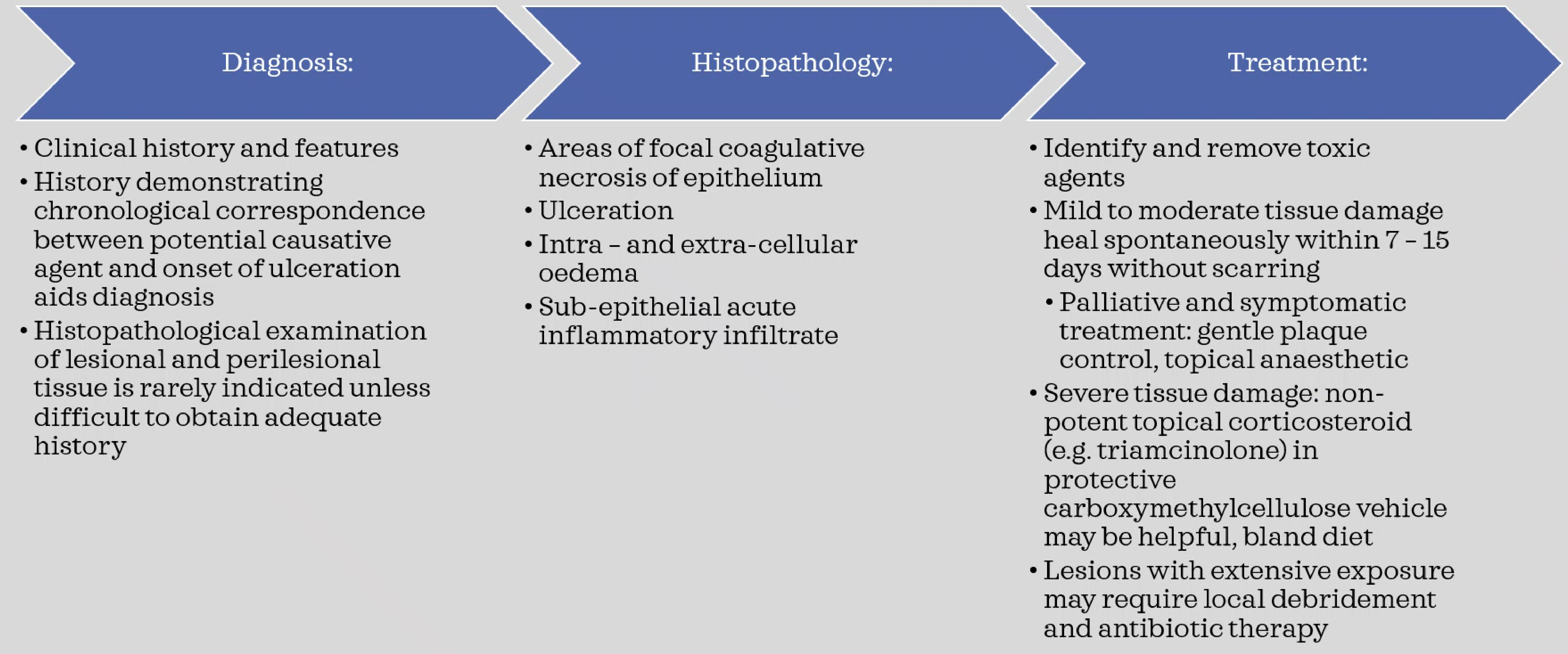
Diagnosis20
- Based on clinical history and features.
- Chronological correspondence between agent exposure and ulcer onset is key.
- Histopathology (showing focal coagulative necrosis, ulceration, and oedema) is rarely indicated unless history is unobtainable.
- Histopathology Details: Shows intra and extracellular edema, and subepithelial acute inflammatory infiltrate in addition to necrosis.
Treatment21
- Identify and remove toxic agents.
- Mild to moderate damage typically heals in 7–15 days without scarring.
- Palliative care: Gentle plaque control and topical anaesthetics.
- Severe cases: Non-potent topical corticosteroids (e.g., triamcinolone) in a protective vehicle; bland diet.
- May require stronger agents beyond non-potent corticosteroids for severe cases.
- Extensive lesions may require local debridement and antibiotic therapy.
Exfoliative Cheilitis




Overview22
- Rare inflammatory dermatologic condition of unknown etiology.
- Often associated with stress, anxiety, or parafunctional habits (lip licking/chewing).
- Characterized by chronic excessive keratin production and desquamation.
Clinical Features
- Symptoms: Sensitivity and burning of the lips.
- Demographics: More common in females.
- Presentation: Scaling, peeling, erythema, crusting, and bleeding involving both upper and lower lip vermillion.
- Differential Diagnosis: Must be distinguished from allergic contact cheilitis and atopic cheilitis via history or patch testing.
Treatment Observations23
- Cases show partial response to pimecrolimus ointment after one month of treatment in elderly patients.
Case Study: 79-Year-Old Female Patient
- ==Presentation: Exfoliative cheilitis affecting both lips.==
- ==Treatment Response:==
- ==Patient 1: Showed partial response after one month of pimecrolimus ointment.==
- ==Patient 2: Had decent response to pimecrolimus ointment but some remaining scale.==
- ==Features: Classic thick scale present, which is recurring.==
Histopathology
- Parakeratosis or hyperkeratosis.
- Benign epithelial hyperplasia.
- Acute or chronic inflammation and fibrosis.
- Presence of superficial fungal or bacterial microorganisms.
- Overall histopathology is primarily bland tissue.
Management24
Management is often difficult and includes:
- Topical Treatments: Corticosteroids, antibacterial/antifungal ointments, sunscreen, petroleum jelly, 2-3% salicylic acid, 0.1% tacrolimus, or cryotherapy.
- Systemic Treatments: Antidepressants, antifungal agents, or corticosteroids.
- Rarely used; antidepressants indicated specifically if patient is visibly anxious.
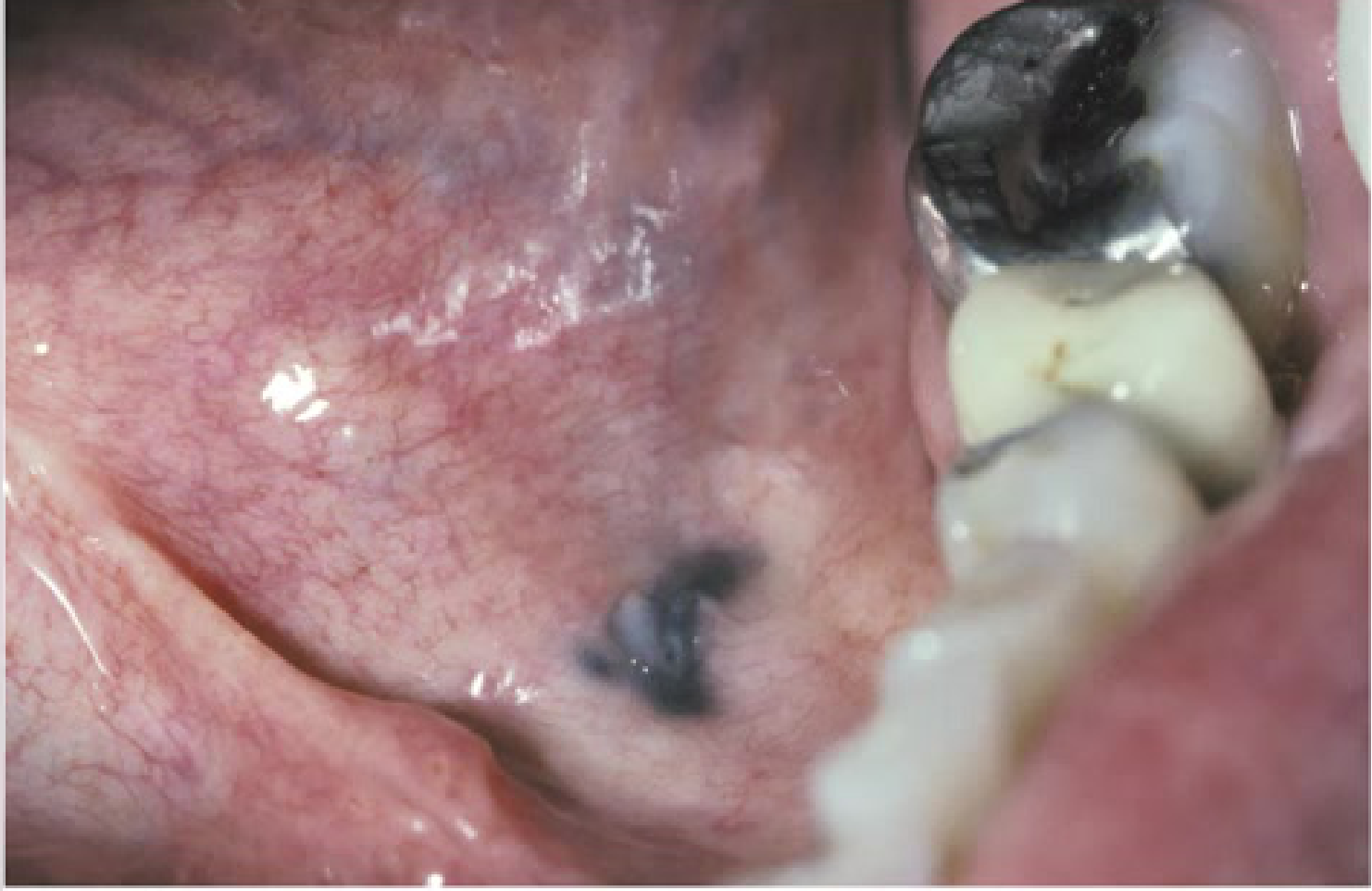
Amalgam Tattoo And Other Exogenous Pigmentation
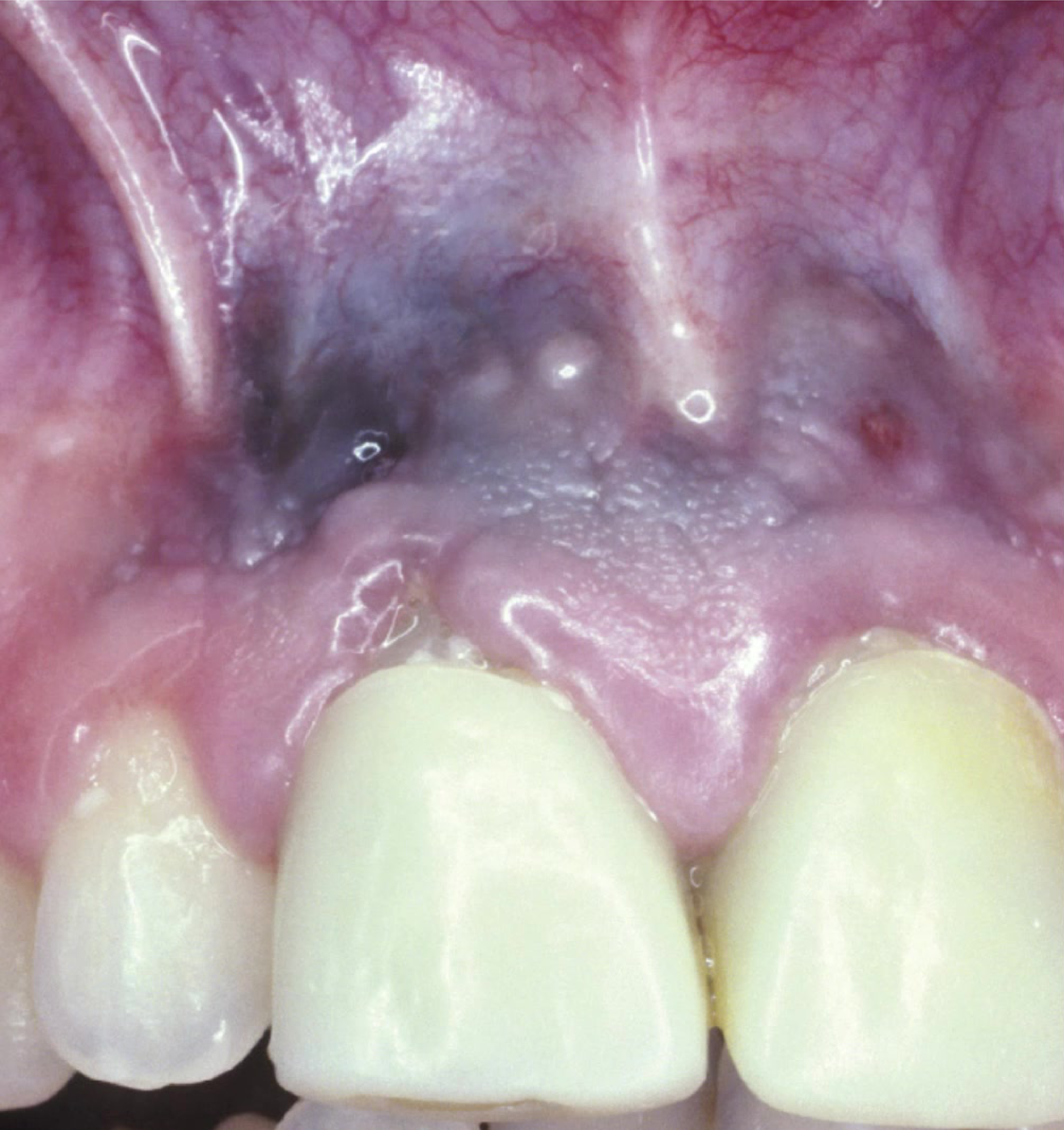
Amalgam Tattoo Etiology25
- Implantation of dental amalgam into the oral mucosa.
- Contamination of mucosal abrasions by amalgam dust during procedures.
- Broken amalgam pieces falling into extraction sites.
- Residual material from endodontic root fills.
- Metallic particles driven into tissue by high-speed air turbines.
Clinical Features
- Presents as macules or slightly raised lesions.
- Colors: Black, blue, or grey.
- Borders: Well-defined, irregular, or diffuse.
- Location: Any mucosal surface (gingiva, alveolar mucosa, buccal mucosa).
- Lateral spread may occur for several months following initial pigmentation.
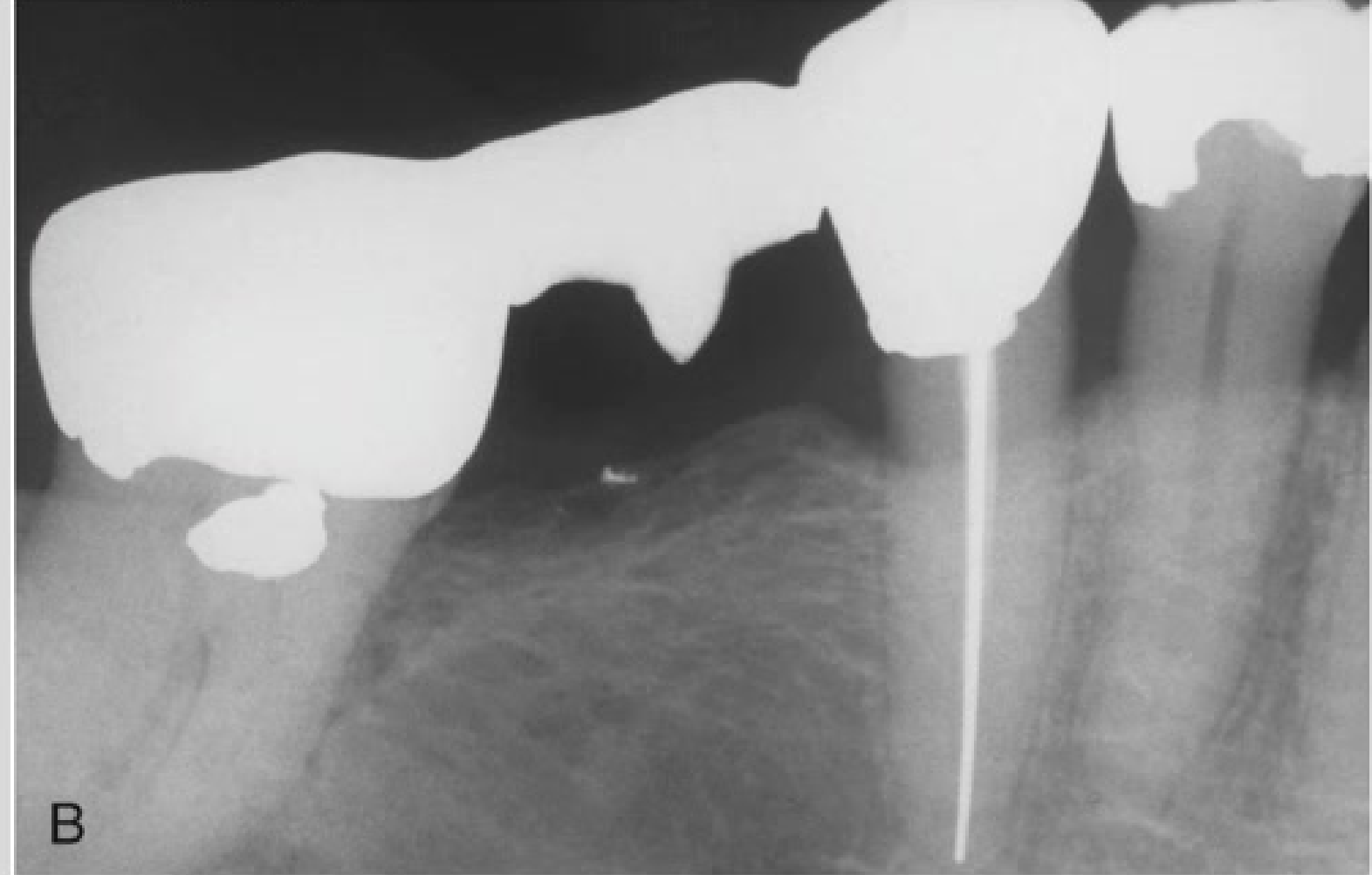
Radiographic Features26
- Metallic fragments may be visible as densely radiopaque spots.
- Metallic fragments can often be picked up on radiographs, aiding diagnosis without biopsy.

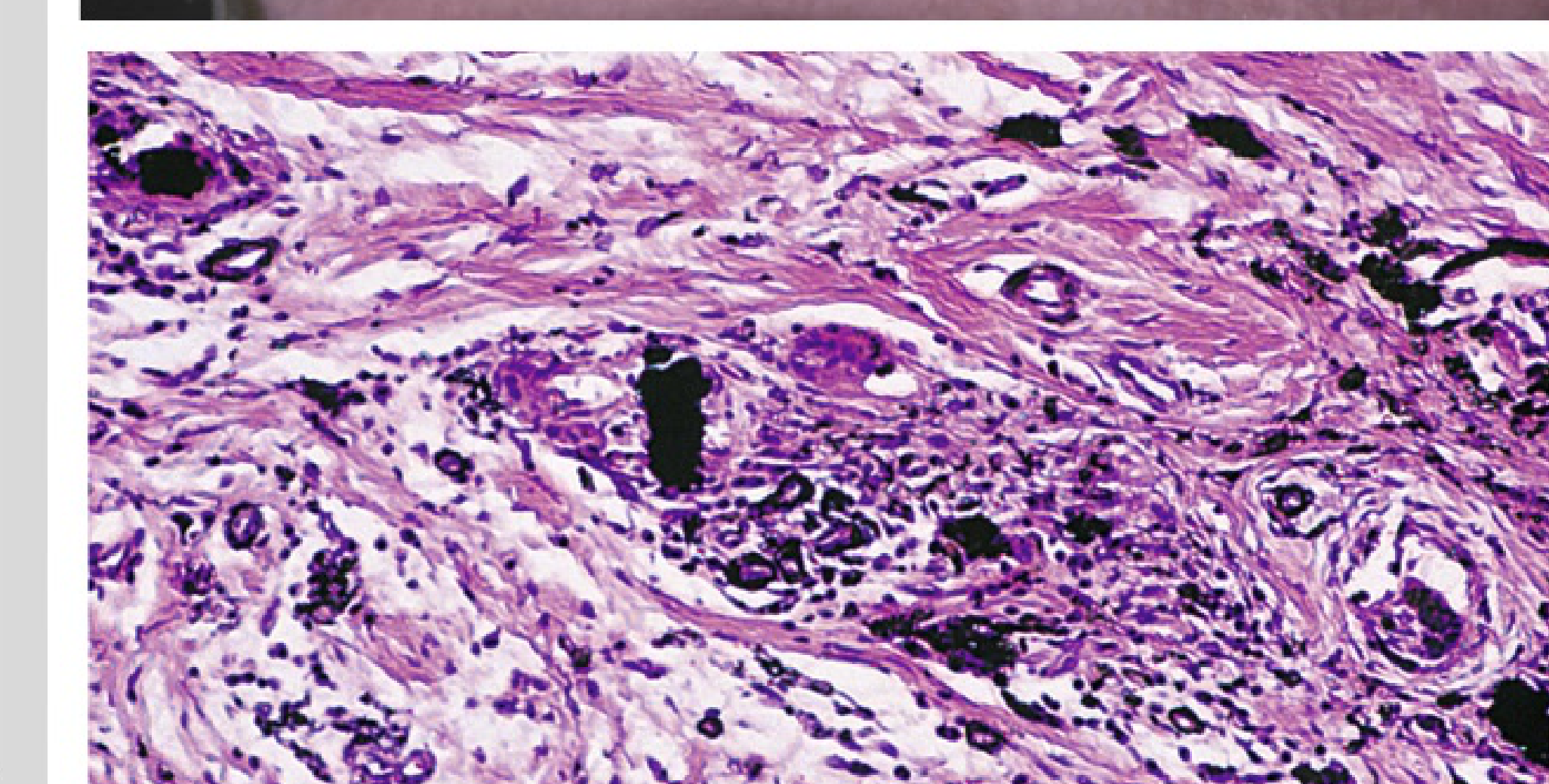
Histopathology

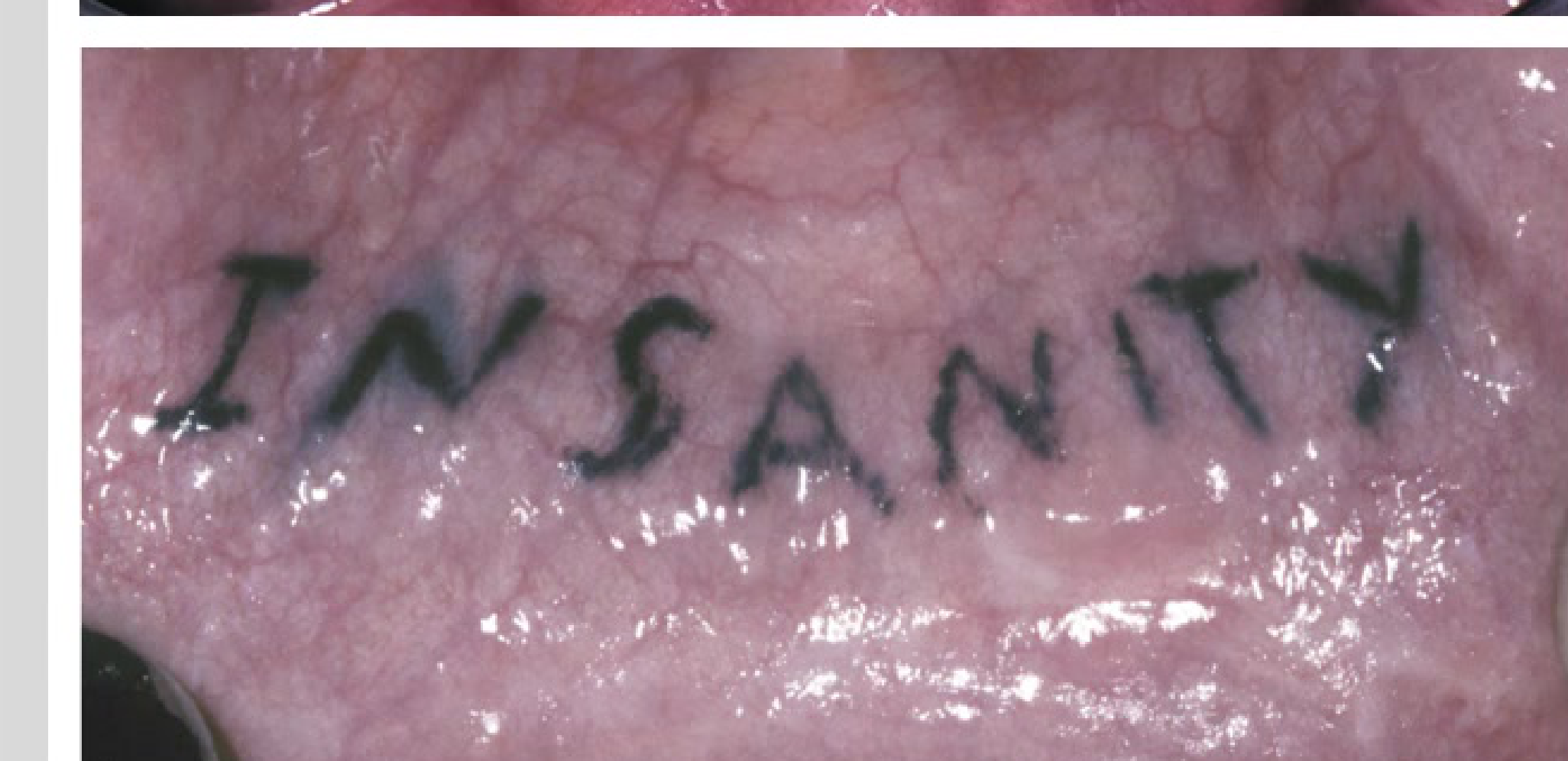
Other Exogenous Pigmentation27
- Cosmetic tattooing: Vermilion border of the lips.
- Intentional tattooing: Maxillary labial gingiva (observed in some African countries).
- Silver solder on orthodontic brackets can leach into adjacent gingival crevices.
- Submucosal implantation of pencils or dental burs may also cause pigmentation.
Histopathology
- Pigmented metal fragments within connective tissue.
- Dark solid fragments or fine black/brown granules.
- Silver salts stain reticulin fibers, particularly around nerves and vessels.
- Histopathology is similar to amalgam tattoo depending on the exogenous material implanted.
Diagnosis and Treatment
- Diagnosis: Radiographs to confirm metallic fragments; biopsy required if melanoma is suspected.
- If fragments are too small for radiograph, biopsy is needed to rule out other reasons for pigmentation.
- Treatment: None required, though surgical removal is an option for cosmetic concerns.
Smoker’s Melanosis
Etiology and Pathogenesis28
- Oral pigmentation increases significantly in heavy smokers.
- Exposure to polycyclic amines (nicotine, benzpyrene) stimulates melanin production.
- Melanin serves as a protective response against harmful tobacco substances.
- Demographics: More common in females; pigmentation increases during first years of smoking
- Clinical Sites (Cigarette Users): Anterior labial gingiva (lower), diffused brown pigmentation
- Clinical Sites (Pipe Smokers): Buccal mucosa
- Clinical Sites (Reverse Smokers): Hard palate (lit end in mouth) - High Risk of oral cancer
Histopathology
- Increased melanin in the basal cell layer.
- Incontinent melanin pigmentation in superficial connective tissue.
- Presence of scattered melanophages.
Diagnosis29
- Assessment: Based on smoking history and clinical presentation.
- Differential Diagnosis: Rule out Peutz-Jeghers syndrome, drug-related pigmentation, and endocrine disturbances
- ==Confirmation: Biopsy==.
- Management: Smoking cessation leads to gradual disappearance of the lesion over approximately 3 years.
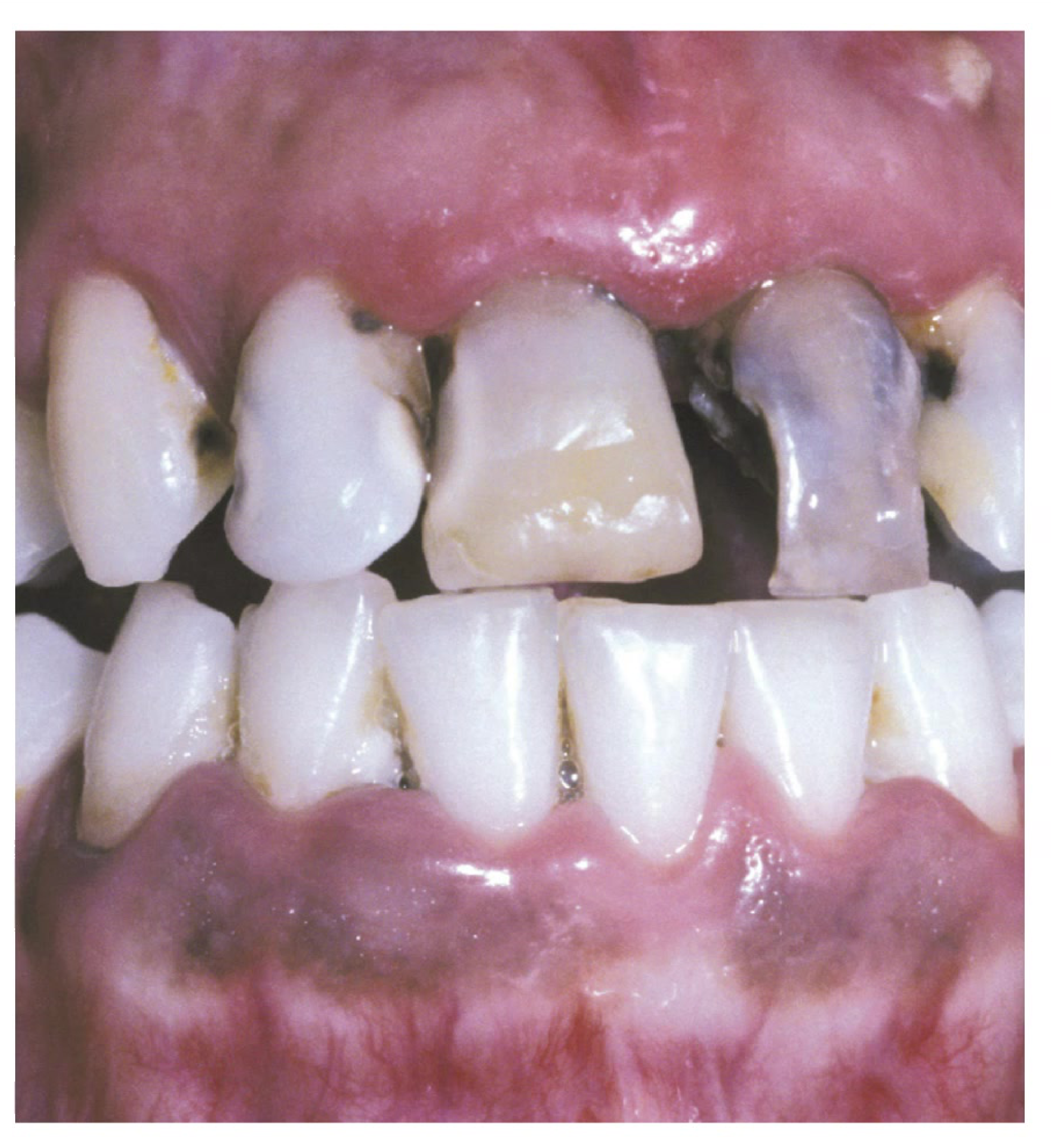
Drug Related Discolouration Of The Oral Mucosa


Mechanisms30
- Medications may stimulate melanin production or result in the deposition of drug metabolites.
- Timing: Pigmentation may occur immediately, after several days, or take years (can be hard to diagnose).
- Appearance: Multiple and diffuse. Colors vary (blue, brown, gray, black, yellow).
- Sites: Most often dorsal tongue, followed by buccal mucosa, gingiva, hard palate, and lips.
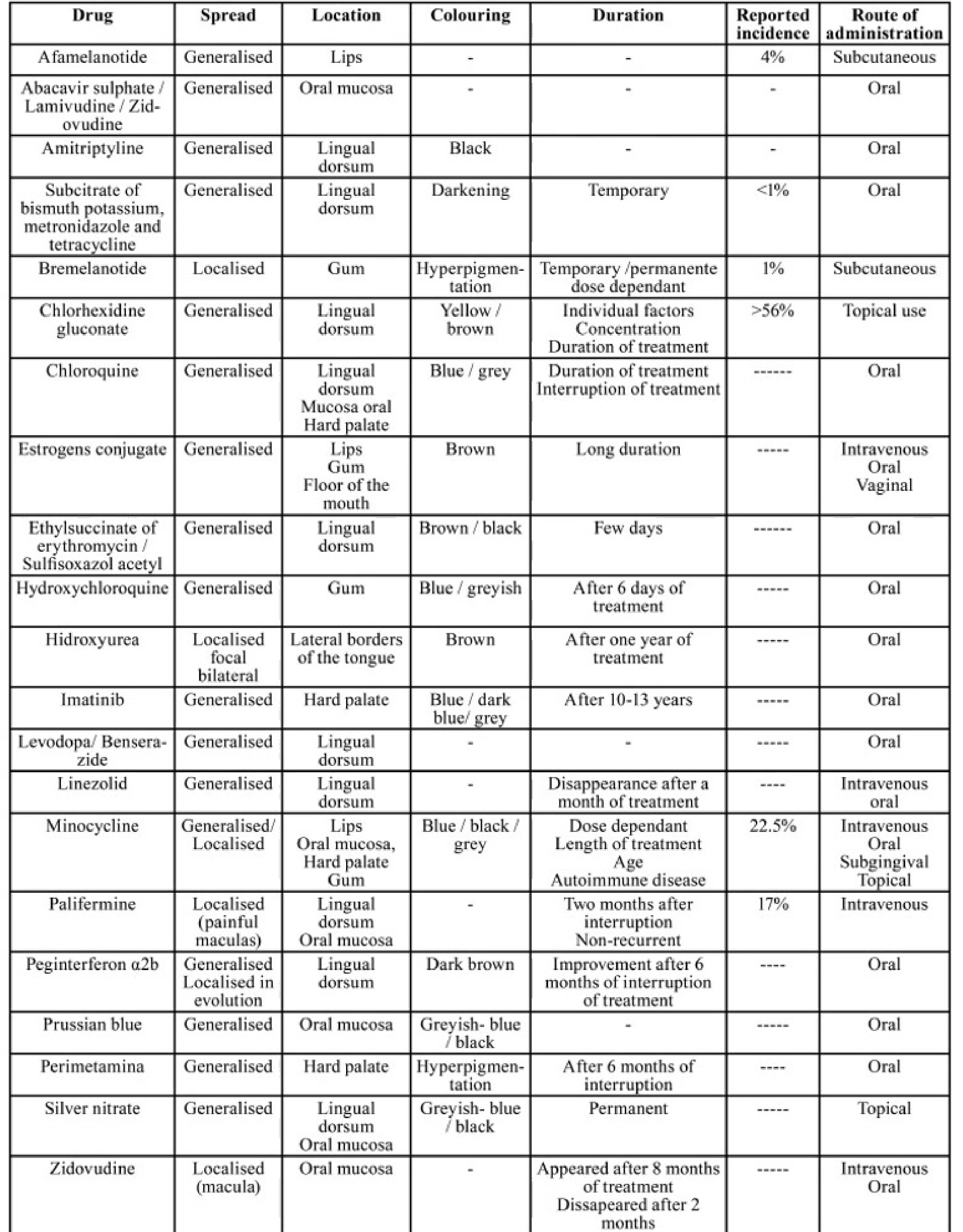
Common Drug-Induced Discolourations
| Drug | Location | Colouring | Duration/Incidence |
|---|---|---|---|
| Amitriptyline | Lingual dorsum | Black | - |
| Chlorhexidine | Lingual dorsum | Yellow/brown | >56% incidence |
| Chloroquine | Palate/Mucosa | Blue/grey | During treatment |
| Imatinib | Hard palate | Blue/grey | After 10-13 years |
| Minocycline | Lips/Gingiva/Palate | Blue/black/grey | 22.5% incidence |
| Silver nitrate | Mucosa | Grey-blue/black | Permanent |
Minocycline-related Discolouration31
- Specific instance of drug-induced pigmentation affecting oral tissues, often presenting with a blue-grey hue in the bone or mucosa.
Histopathology
- Dark brown granulated pigments in the lamina propria.
- Infiltration of fibroblasts and macrophages in subepithelial and perivascular areas.
Diagnosis
- Diagnosis: Based on medical/clinical history and examination; biopsy may be used for confirmation.
- Management: No long-term health problems; hyperpigmentation typically fades gradually upon discontinuing the medication.
- Prognosis: Occasionally fades once medication is discontinued (not in all cases).
Oral Complication Of Radiotherapy32
- Cancer patients undergoing head and neck radiation therapy experience both acute and chronic soft tissue changes.
- Acute Effects: Mucositis, thickening of secretions, mucosal infections, pain, sensory disruptions.
- Chronic Effects: Tissue fibrosis, salivary gland dysfunction, increased susceptibility to dental caries and periodontal disease, osteoradionecrosis.
Mucositis33
- An acute response to treatment.
- Affects approximately 80% of head and neck radiation patients.
- Typically begins within the first 2-3 weeks of treatment, peaking near the end and persisting for 2-4 weeks post-radiation.
- Progression: Progresses to ulcerations and pseudomembranes as radiation dose increases; associated with pain.
- Sites: Non-keratinized oral mucosa is more susceptible than keratinized.
- Severity: Worse with concurrent chemotherapy; affects oral function significantly (nutrition impacted; severe cases may require gastric tube).
- Management: Milder cases use compounded Diflam mouth rinses, lignocaine gels, low-level laser therapy; severe cases may require opioids.
Candidiasis
- Associated with mucosal pain, taste changes, and dysphagia.
- Includes pseudomembranous and erythematous forms, as well as angular cheilitis.
- Cause: Opportunistic infection associated with salivary gland dysfunction.
- Symptoms: Includes burning in mouth alongside mucosal pain and taste changes.
Neurosensory Disorders34
- Symptoms: Mucosal pain and taste dysfunction (dysgeusia).
- Causes: Inflammation, ulceration, atrophy, or neuroepithelial damage.
- Management: Analgesics (topical, NSAIDs, mild opioids), centrally acting medications, and Low-Level Laser Therapy (LLLT).
- Recovery: Taste usually improves 3-6 months post-RT, though sensitivity may persist.
- Duration: Mucosal sensitivity persists even after clinical mucositis resolves due to neuroepithelial damage; worsened by dry mouth.
Xerostomia And Salivary Gland Dysfunction
- Salivary glands are highly radiation-sensitive.
- Flow decreases dramatically within the first 6 weeks.
- Management: Symptomatic relief using salivary replacements.
- Timing: Changes start within one week; dramatic decrease around six-week mark.
- Caries Prevention: Strong protocol required due to high risk of Radiation Caries.
- Recommendations: NutraFlow 5000 toothpaste twice daily.
- Recall: Dentist visits at least 3 to 6 monthly.
- Hygiene/Diet: Good oral hygiene, very low sugar diet.
Caries
- Often cervical in location, secondary to salivary dysfunction.
- Requires rigorous caries prevention protocols.

Post-radiation Fibrosis35
- Can lead to trismus (mouth opening < 35 mm) due to masticatory muscle fibrosis.
- Managed with jaw rehabilitation systems or LLLT.
- Definition: Fibrosis of the mastication muscles.
- Management: Jaw muscle stretching exercises during treatment, Therabite jaw motion rehabilitation system, Low-level laser therapy (some evidence).
Osteoradionecrosis36
- Defined as nonvital irradiated bone that persists for longer than 3 months in the absence of local neoplastic disease.
- Risk Factors: Radiation dose greater than 50 Grays (very high risk), risk is lifelong, Mandible more susceptible than maxilla.
- Cause: Usually occurs secondary to trauma (tooth extractions, denture trauma), sometimes spontaneous.
- Clinical/Radiographic: Ill-defined area of radiolucency, pain, cortical perforations, fistula, pathological fractures.
- Prevention: Pre-radiation Dental Screening imperative; remove at-risk teeth before radiation starts (allow at least three weeks healing); extractions can occur about four months post-radiation.

Contact Information37
Thank you for your attention. For further inquiries or information regarding this presentation on physical and chemical injuries, please contact:
- Lalima Tiwari
- Email: Lalima.Tiwari@uwa.edu.au
Footnotes
-
Original PDF page 1: L6 Physical and chemical injuries slides, p.1 ↩
-
Original PDF page 2: L6 Physical and chemical injuries slides, p.2 ↩
-
Original PDF page 3: L6 Physical and chemical injuries slides, p.3 ↩
-
Original PDF page 4: L6 Physical and chemical injuries slides, p.4 ↩
-
Original PDF page 6: L6 Physical and chemical injuries slides, p.6 ↩
-
Original PDF page 7: L6 Physical and chemical injuries slides, p.7 ↩
-
Original PDF page 8: L6 Physical and chemical injuries slides, p.8 ↩
-
Original PDF page 9: L6 Physical and chemical injuries slides, p.9 ↩
-
Original PDF page 10: L6 Physical and chemical injuries slides, p.10 ↩
-
Original PDF page 11: L6 Physical and chemical injuries slides, p.11 ↩
-
Original PDF page 12: L6 Physical and chemical injuries slides, p.12 ↩
-
Original PDF page 14: L6 Physical and chemical injuries slides, p.14 ↩
-
Original PDF page 15: L6 Physical and chemical injuries slides, p.15 ↩
-
Original PDF page 13: L6 Physical and chemical injuries slides, p.13 ↩
-
Original PDF page 16: L6 Physical and chemical injuries slides, p.16 ↩
-
Original PDF page 17: L6 Physical and chemical injuries slides, p.17 ↩
-
Original PDF page 18: L6 Physical and chemical injuries slides, p.18 ↩
-
Original PDF page 20: L6 Physical and chemical injuries slides, p.20 ↩
-
Original PDF page 22: L6 Physical and chemical injuries slides, p.22 ↩
-
Original PDF page 31: L6 Physical and chemical injuries slides, p.31 ↩
-
Original PDF page 23: L6 Physical and chemical injuries slides, p.23 ↩
-
Original PDF page 24: L6 Physical and chemical injuries slides, p.24 ↩
-
Original PDF page 25: L6 Physical and chemical injuries slides, p.25 ↩
-
Original PDF page 26: L6 Physical and chemical injuries slides, p.26 ↩
-
Original PDF page 27: L6 Physical and chemical injuries slides, p.27 ↩
-
Original PDF page 28: L6 Physical and chemical injuries slides, p.28 ↩
-
Original PDF page 29: L6 Physical and chemical injuries slides, p.29 ↩
-
Original PDF page 30: L6 Physical and chemical injuries slides, p.30 ↩
-
Original PDF page 34: L6 Physical and chemical injuries slides, p.34 ↩
-
Original PDF page 32: L6 Physical and chemical injuries slides, p.32 ↩
-
Original PDF page 33: L6 Physical and chemical injuries slides, p.33 ↩
-
Original PDF page 35: L6 Physical and chemical injuries slides, p.35 ↩
-
Original PDF page 36: L6 Physical and chemical injuries slides, p.36 ↩
-
Original PDF page 37: L6 Physical and chemical injuries slides, p.37 ↩
-
Original PDF page 38: L6 Physical and chemical injuries slides, p.38 ↩
-
Original PDF page 39: L6 Physical and chemical injuries slides, p.39 ↩
-
Original PDF page 40: L6 Physical and chemical injuries slides, p.40 ↩