Lichen Planus
Course Presentation Overview1
This session focuses on allergies and immune-mediated diseases, specifically addressing Oral Lichen Planus (OLP).
Presenter Information
- Lecturer: Dr Agnieszka Frydrych
- Institution: The University of Western Australia
Introduction2345
Lichen planus is a chronic, systemic disease characterized by an established immune-mediated pathogenesis.
- It is among the most common oral mucosal diseases not caused by infection
- It is an inflammatory condition, not a communicable disease
- The term "lichen" translates to "flat tree moss", often causing patient anxiety regarding infection
- Clinicians must clarify that it is non-infectious
- Visual examination alone provides limited information and can lead to misdiagnosis



Clinical Patterns678
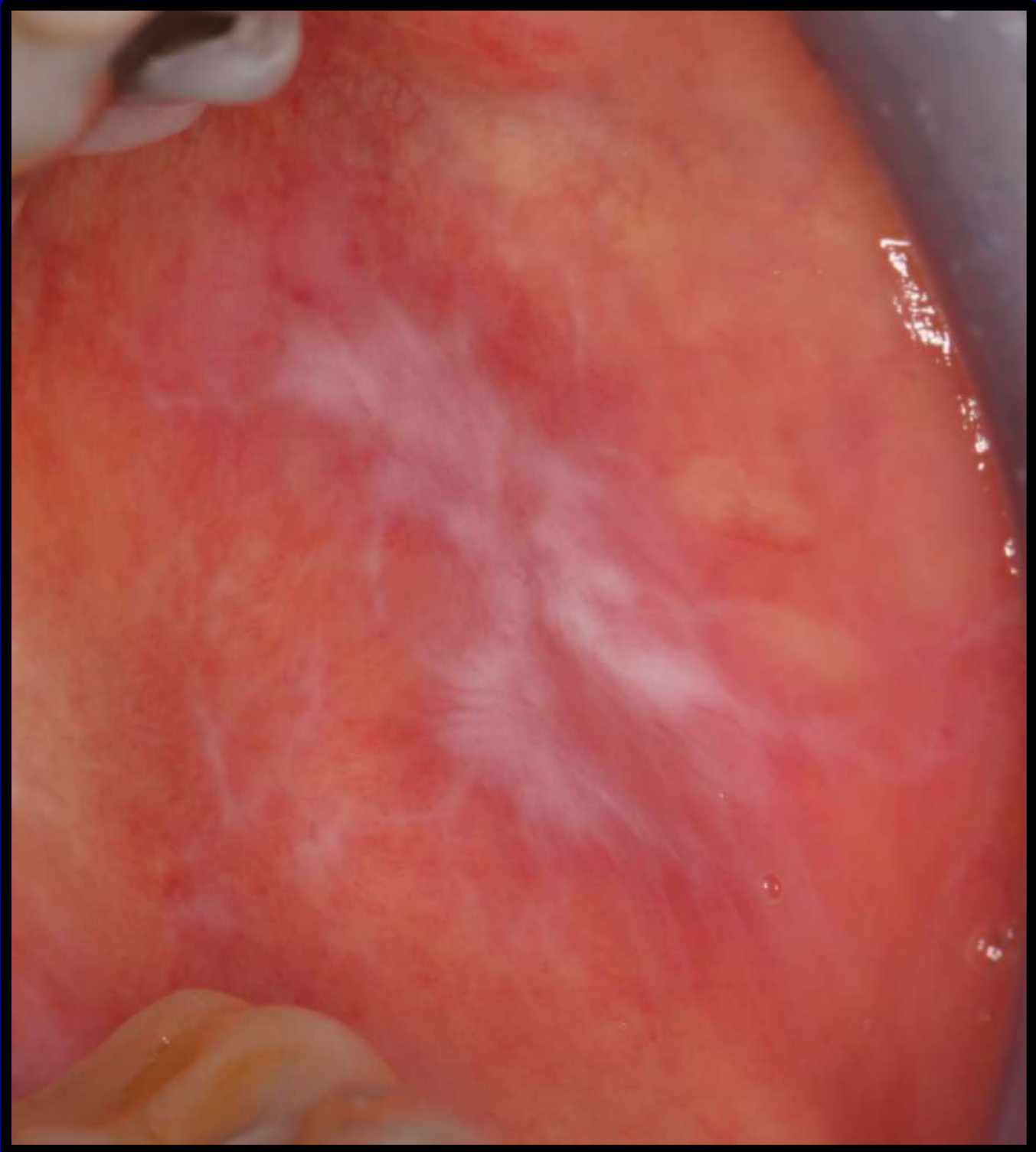
The clinical presentation of Lichen Planus manifests in several distinct patterns:
-
Reticular
-
Plaque-like
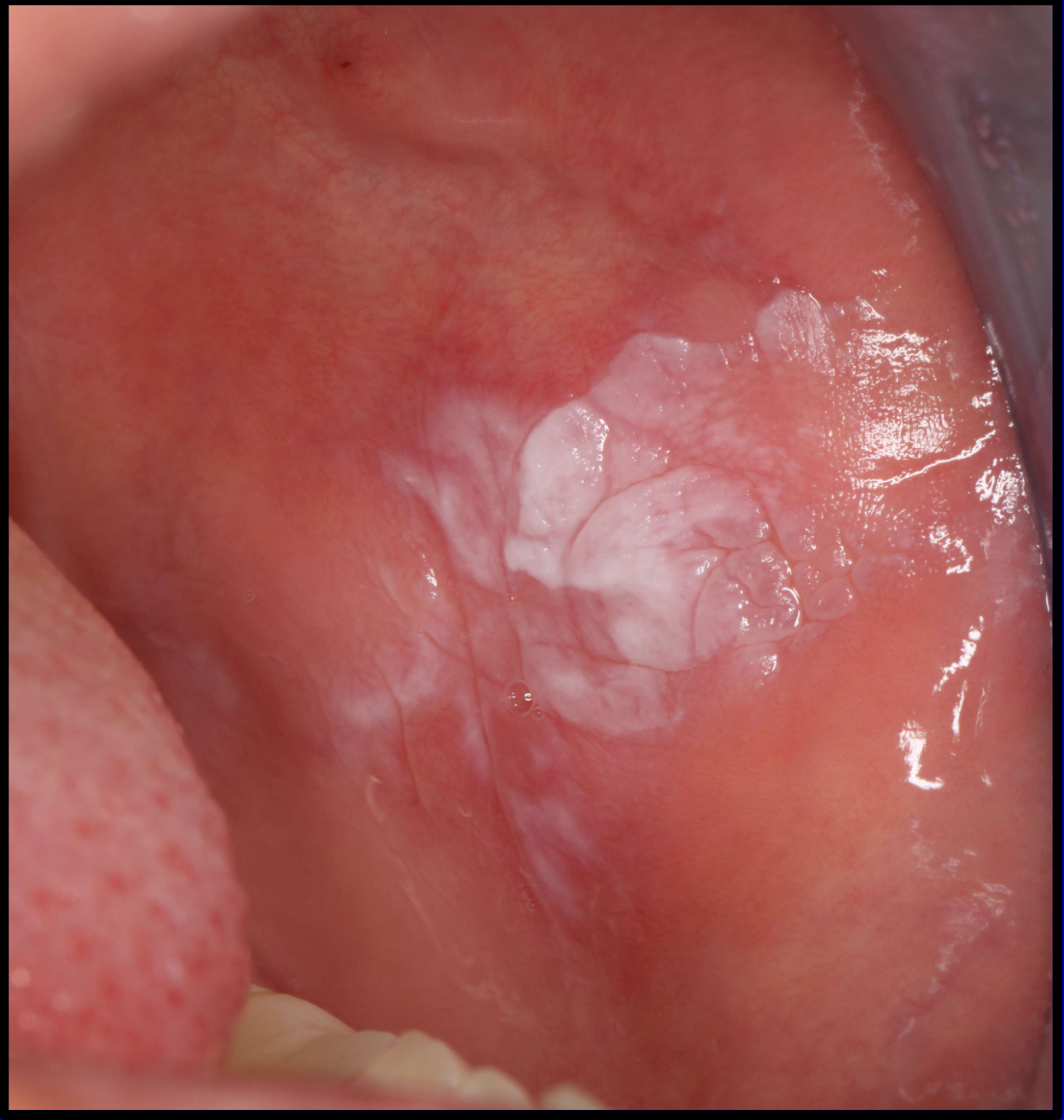
- Note that plaque-like lichen planus can actually be easily confused with thinks like leukoplakia
-
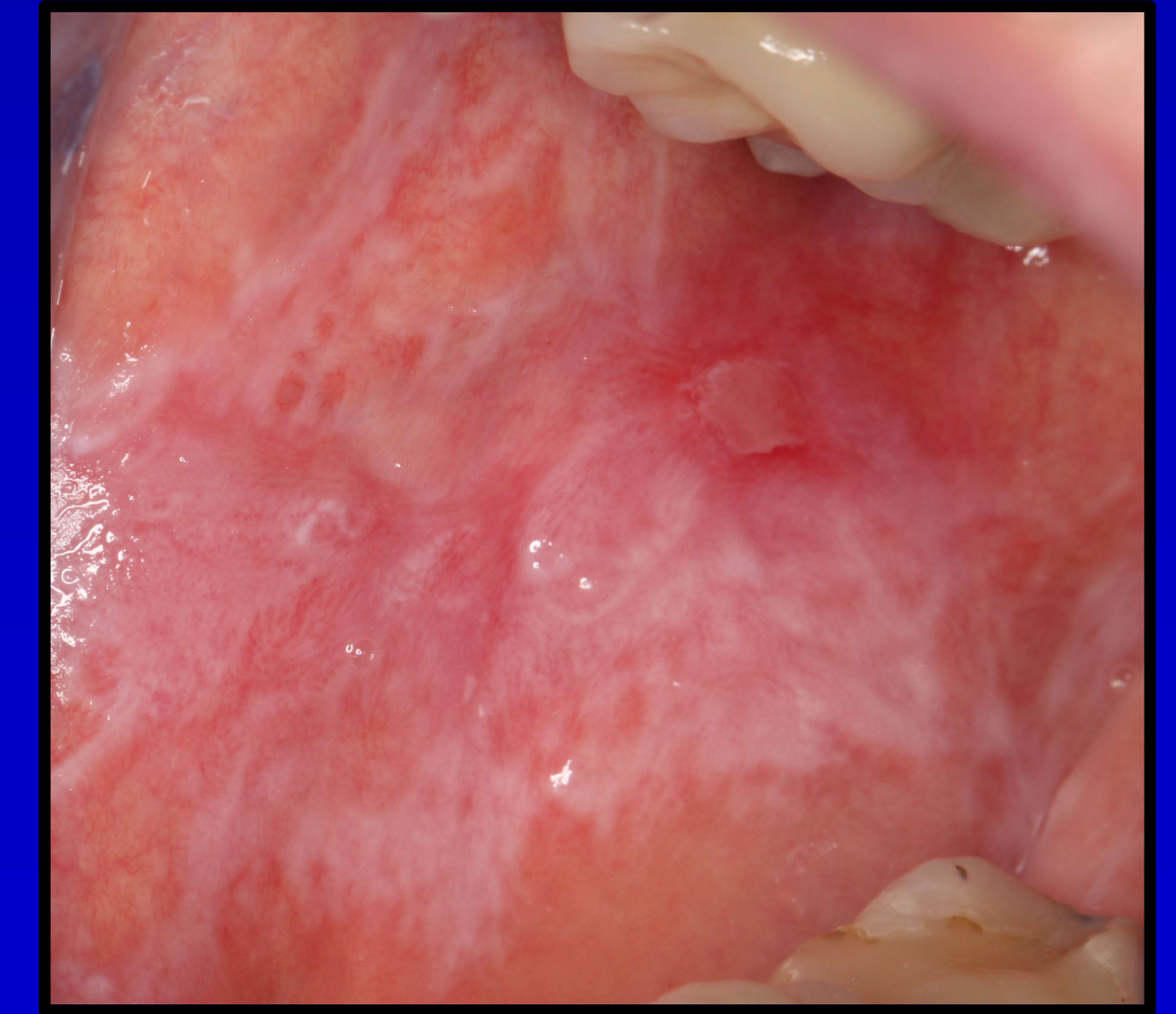
Erythematous
-
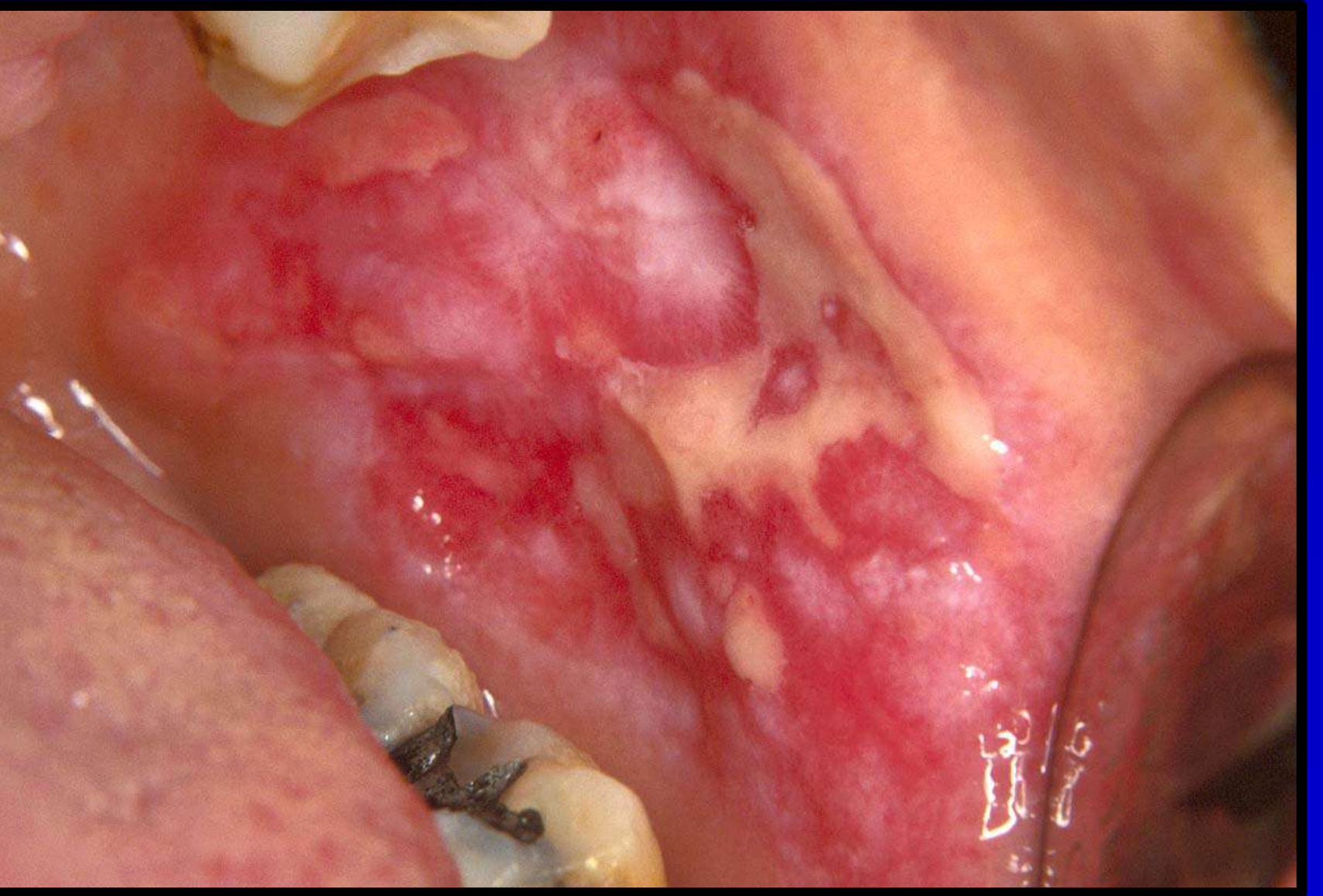
Erosive / ulcerative
-
Papular
-
Bullous
-
Recognition of these patterns is essential
-
Some patterns can be mistaken for other oral pathoses
-
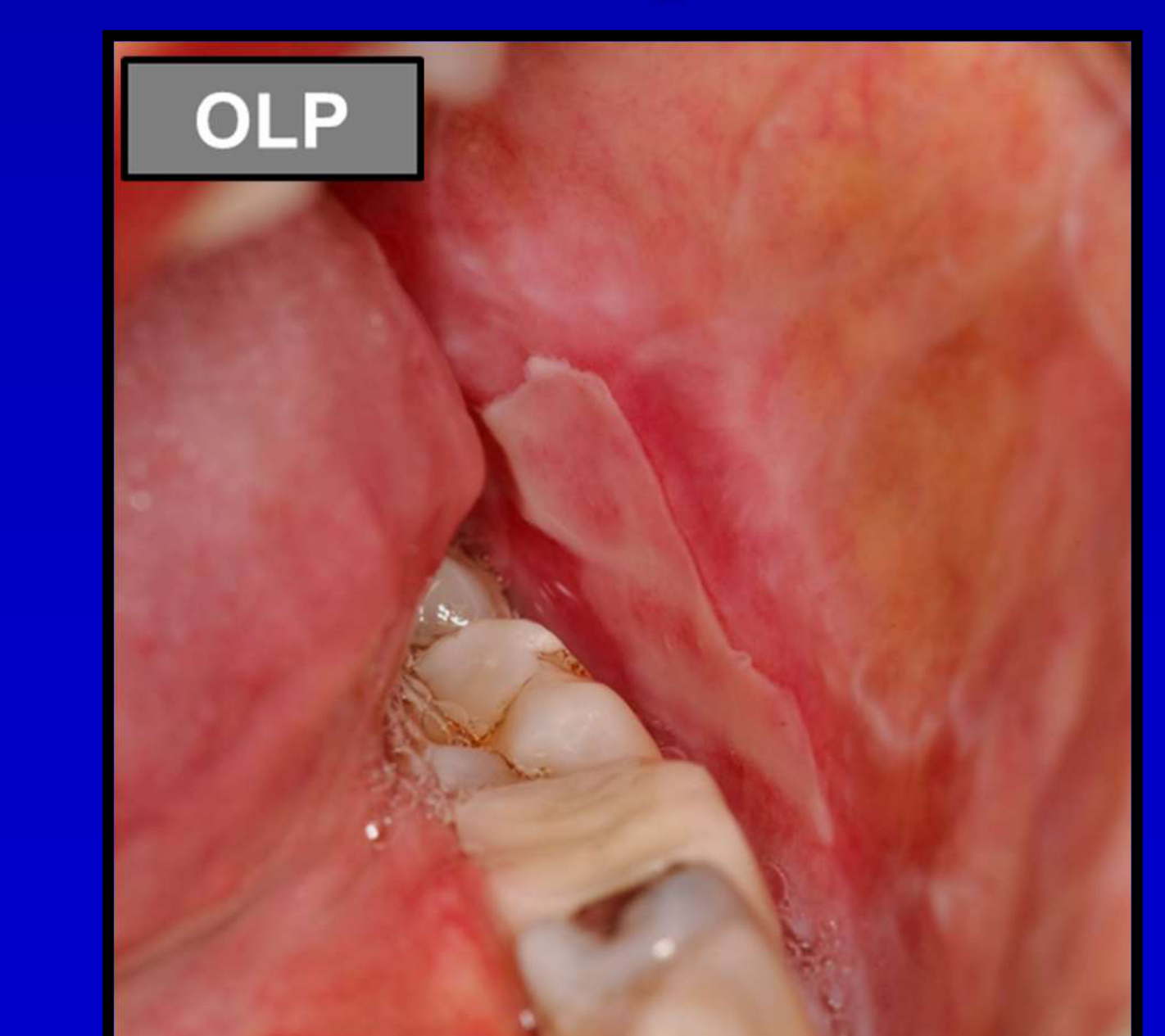
Reticular: Characterized by white, lacy streaks (Wickham's striae), most easy to recognize
-
Plaque-like: Appears as white patches, can be mistaken for oral leukoplakia
-
Erythematous: Red, inflamed mucosal areas, carcinoma in situ can mimic this
-
Erosive/Ulcerative: Involves ulceration, often symptomatic and requires management
-
Papular: Characterized by small, raised papules
-
Bullous: Involves blister formation, rare, do not miss Mucous Membrane Pemphigoid









Epidemiology9
Oral Lichen Planus (OLP) is a global condition with specific demographic trends:
- Global Prevalence: OLP affects people of all ethnic groups with a worldwide prevalence of approximately 2.2%.
- Gender Distribution: The condition is more frequently observed in women than in men.
- Age of Onset: The typical age of presentation for patients is between 30 and 60 years of age.
Pediatric Prevalence10
While primarily an adult condition, Oral Lichen Planus can occur in children, though it is significantly less common, with an estimated prevalence of 0.03%.
Pediatric Presentation Case Study
- Patient: A seven-year-old boy
- Presentation: Presented with oral lichen planus
- Significance: Demonstrates that while the typical age range is 30-60, the condition affects children as well

Sites and Extraoral Manifestations1112
Lichen planus commonly involves the oral mucosa, but the condition can also manifest across various other anatomical sites, including:
-
Dermatological and Appendageal Sites
- Skin
- Scalp
- Nails
-
Mucosal Sites
- Genital mucosa
- Anal mucosa
- Oesophageal mucosa
- Pharyngeal mucosa
- Gastric mucosa
- Conjunctiva
-
Lichen planus is a systemic disease
-
Skin presents as a pruritic (itchy) rash
-
Scalp involvement can lead to permanent hair loss
-
Undiagnosed esophageal lichen planus can cause scarring, strictures, and malignant transformation
-
Patients with dysphagia or odynophagia should be referred to a gastroenterologist






==
Aetiology and Pathogenesis
While the exact aetiology of Oral Lichen Planus (OLP) remains unknown, several factors are considered potential triggers or contributors to the condition:
Potential Etiological Factors13
- Inducers of Hypersensitivity: Local or systemic inducers of cell-mediated hypersensitivity may play a role.
- Psychological Factors: Stress is frequently cited as a possible contributing factor.
- Autoimmune Response: The condition may involve an autoimmune response directed against epithelial antigens.
- Microbial Influence: The role of various microorganisms is under consideration.
- Curative Treatment: Due to the unknown etiology, there is no curative treatment available at this time.
Immunopathogenesis
- The disease is characterized by a dominant Type 1 (Th1) cell-mediated immune response.
- This response leads to the damage of the oral mucosal epithelium.
- Treatment focuses on suppressing this immune response to manage the condition.
There are many diseases which can mimick OLP and infact each one of htese diseases is managed differently
Lupus Erythematosus Details
- Pathology: Systemic autoimmune disease.
- Diagnosis: Routine histopathology, Direct Immunofluorescence, and patient history.
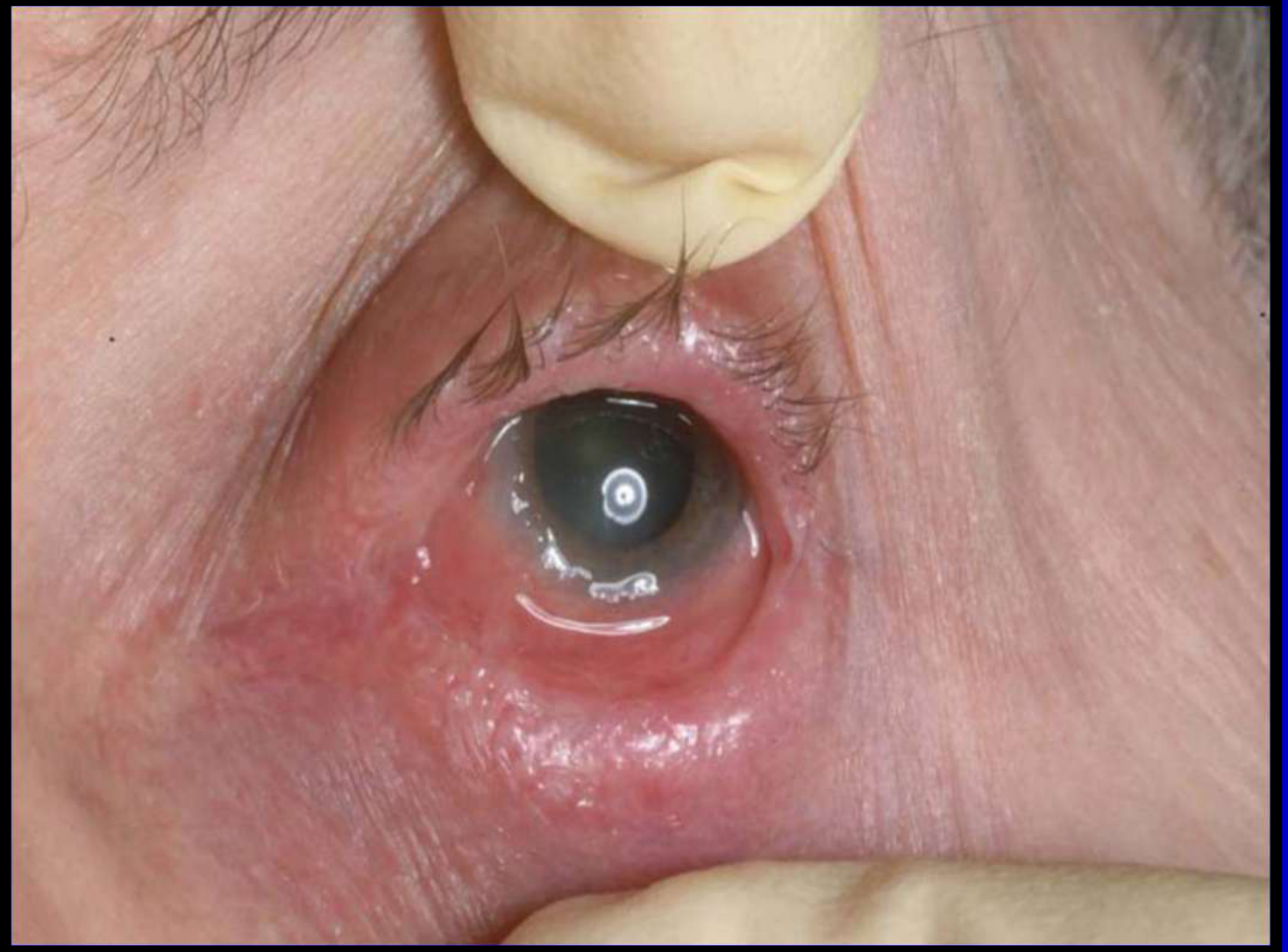
Critical Risk
- Pathology: Autoimmune disease where antibodies are produced against components of the basement membrane zone.
- Ocular Risk: 25% of patients have ocular involvement which can lead to blindness if untreated.
- Referral: Patients should be referred to an ophthalmologist for examination.
Diagnostic Challenge
Mucosal lesions can be clinically and histologically identical to OLP. Asymmetric lesion distribution may provide clues, along with history of lesion development after starting a particular medication. Withdrawal of the offending drug (if possible) leads to resolution.
Diagnostic Challenge
Diagnosis is not obvious due to numerous conditions that mimic OLP. Many conditions require different management strategies.
Differential Diagnosis141516
This section covers the differential diagnosis for Oral Lichen Planus (OLP).
The differential diagnosis for Oral Lichen Planus (OLP) includes the following conditions:
- Lichenoid drug reactions
- Contact lichenoid reactions
- Chronic ulcerative stomatitis
- Linear IgA disease
- Mucous membrane pemphigoid
- Pemphigus vulgaris
- Lupus erythematosus
- Graft versus host disease
- Other related conditions






Lichenoid Drug Reactions1718

Medications Associated with Lichenoid Drug Reactions
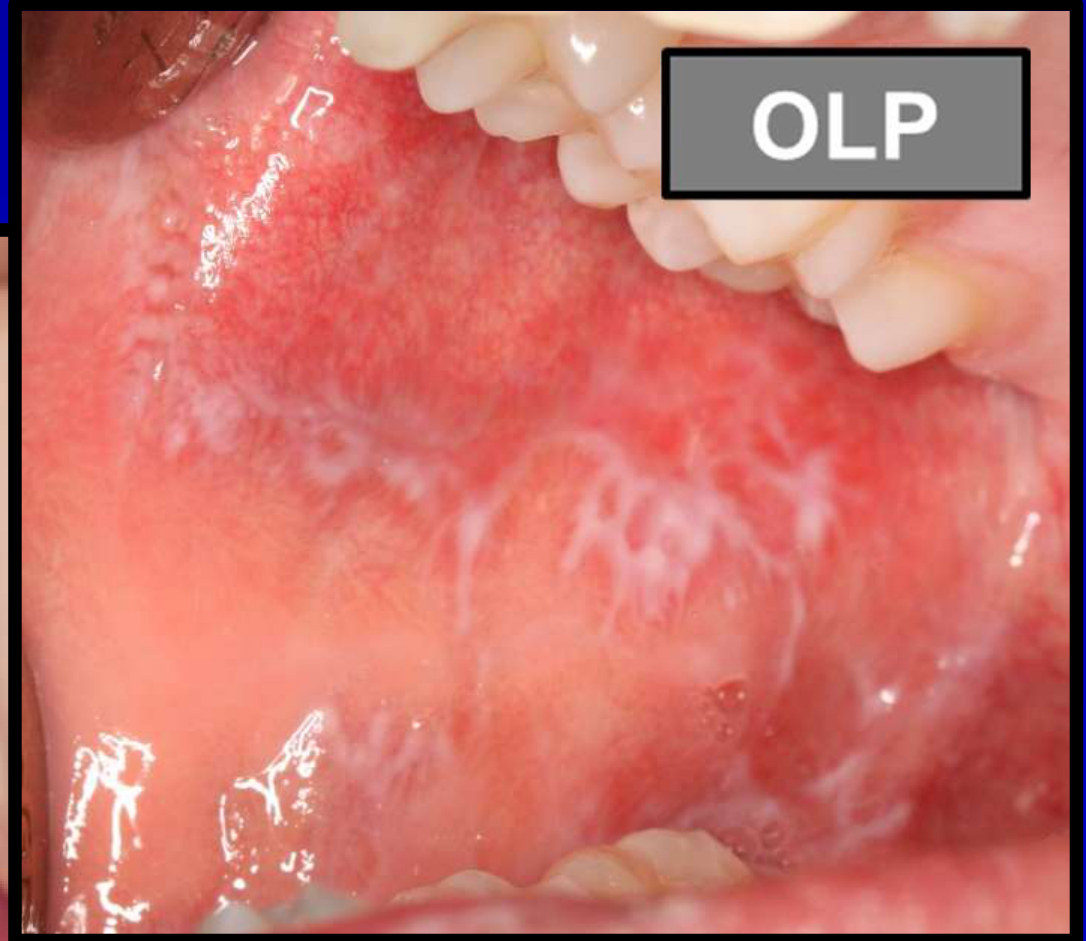
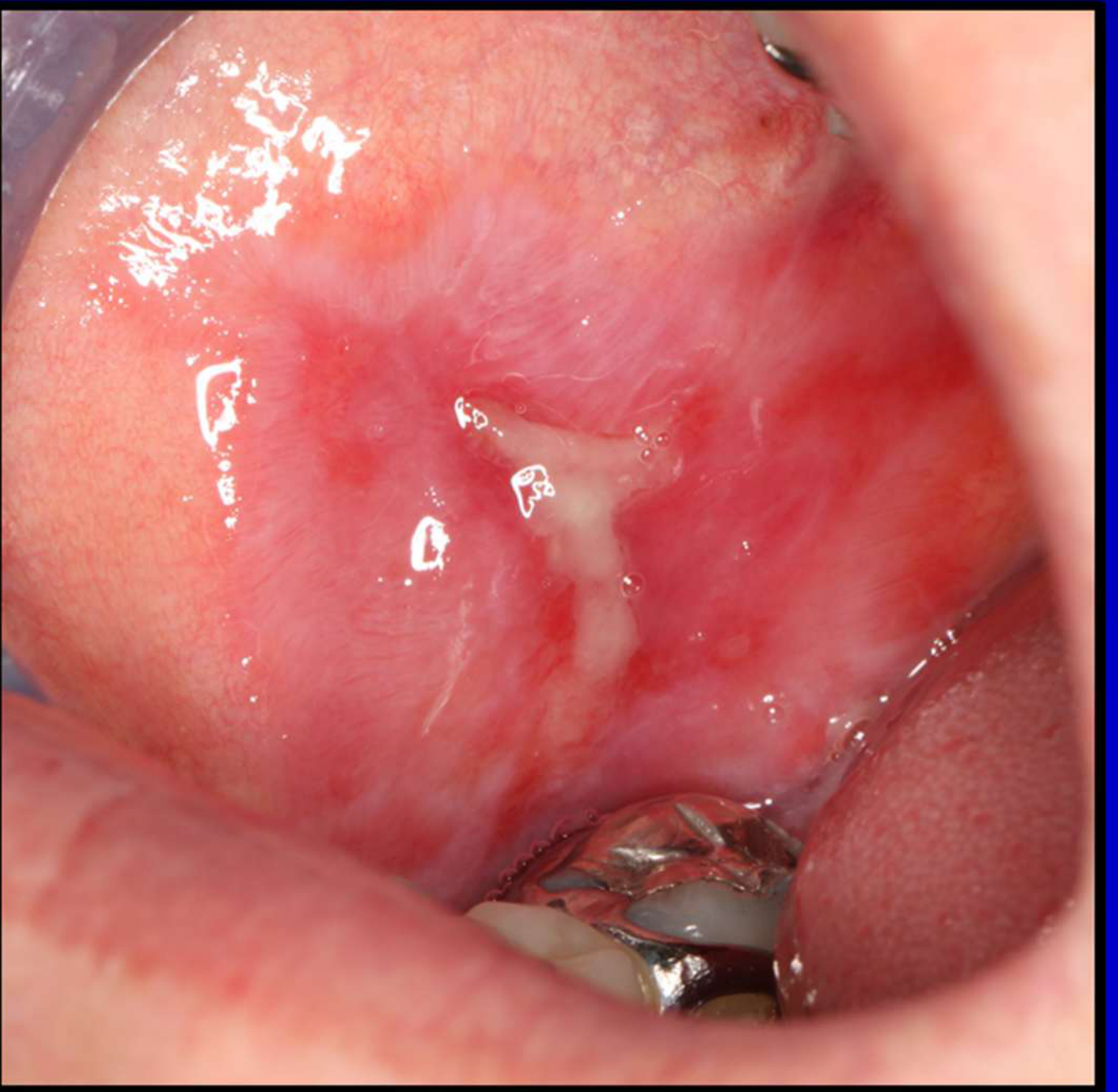
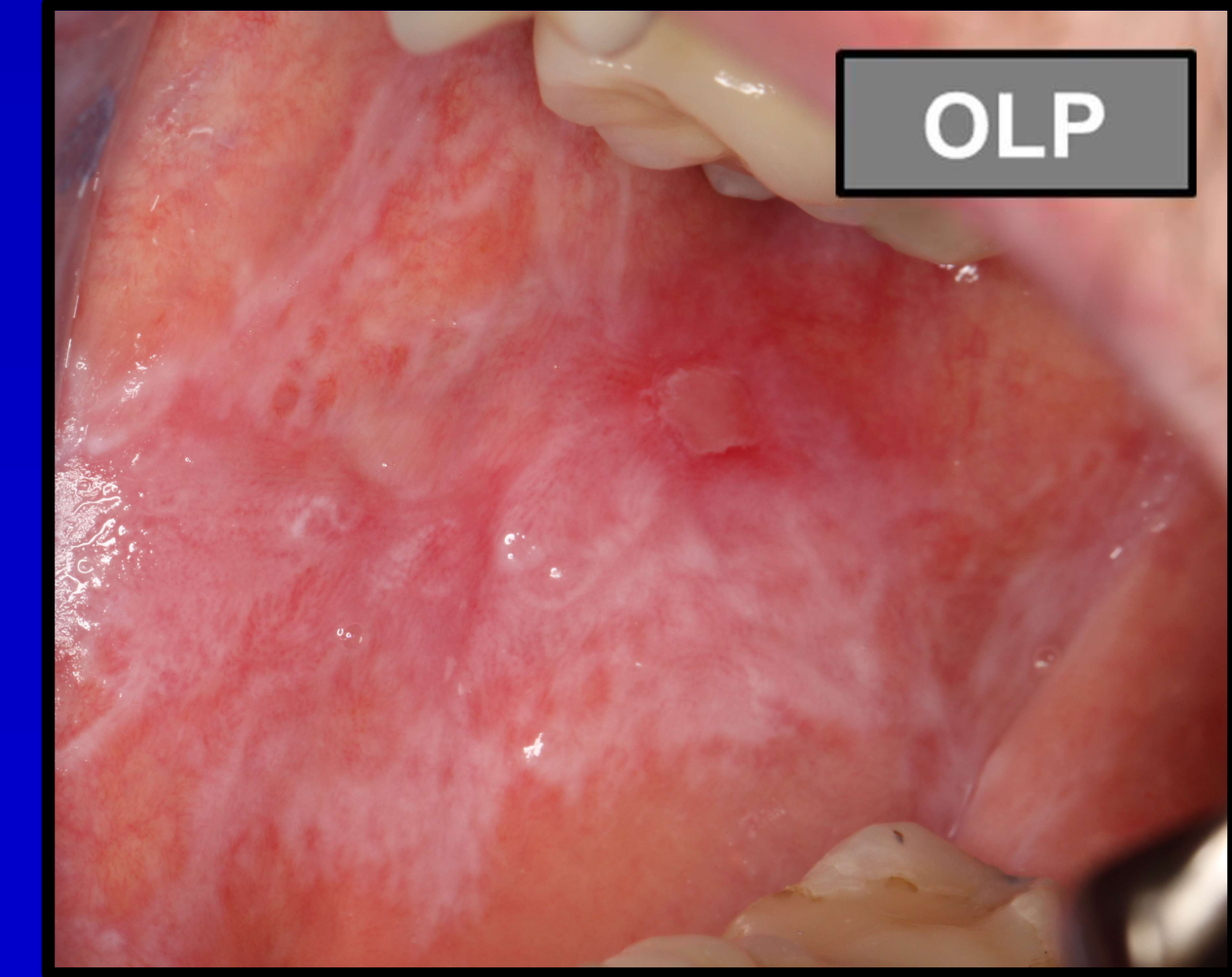
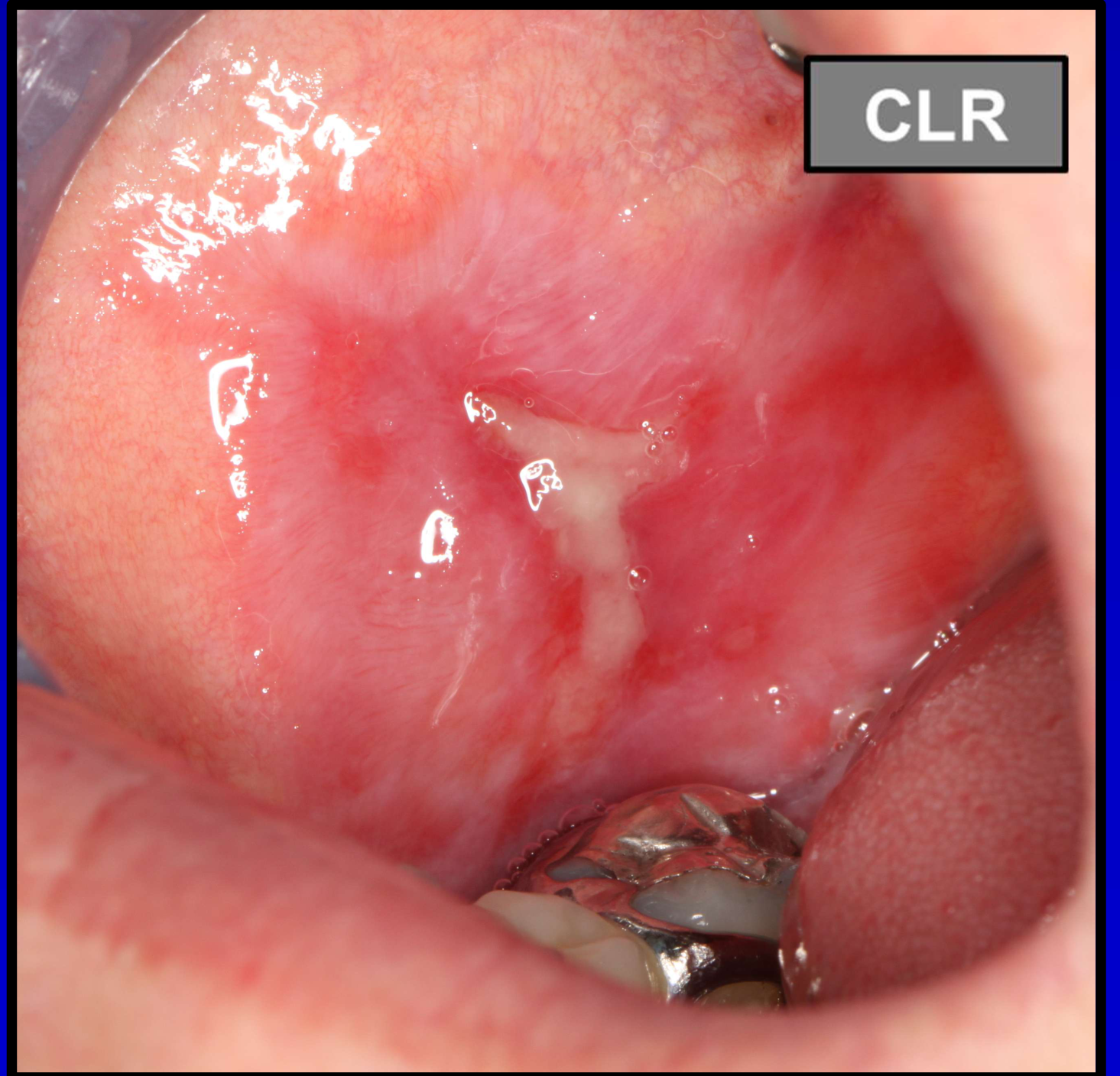
Contact Lichenoid Reactions19
Focus on contact lichenoid reactions specifically related to mercury exposure.
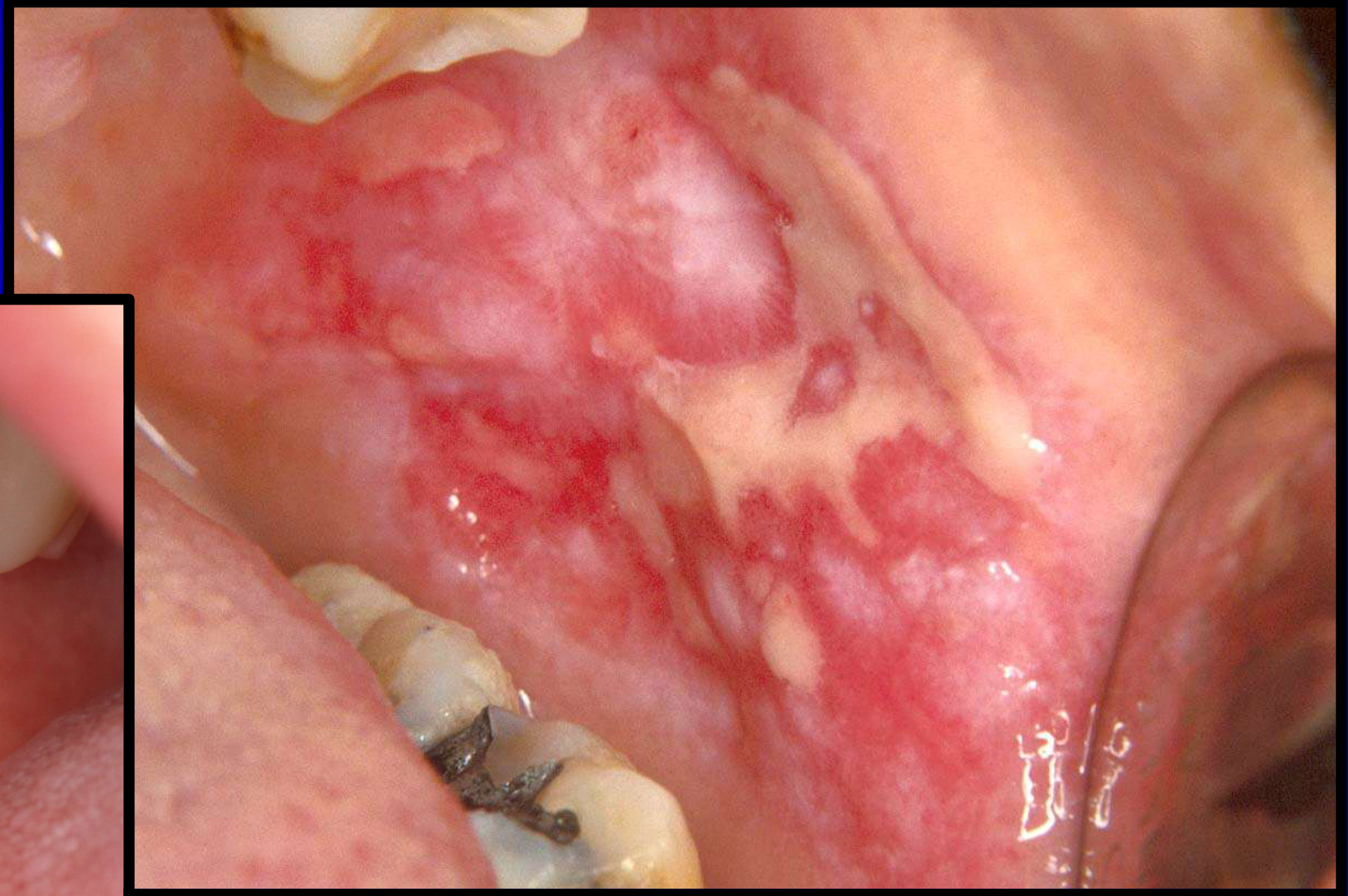
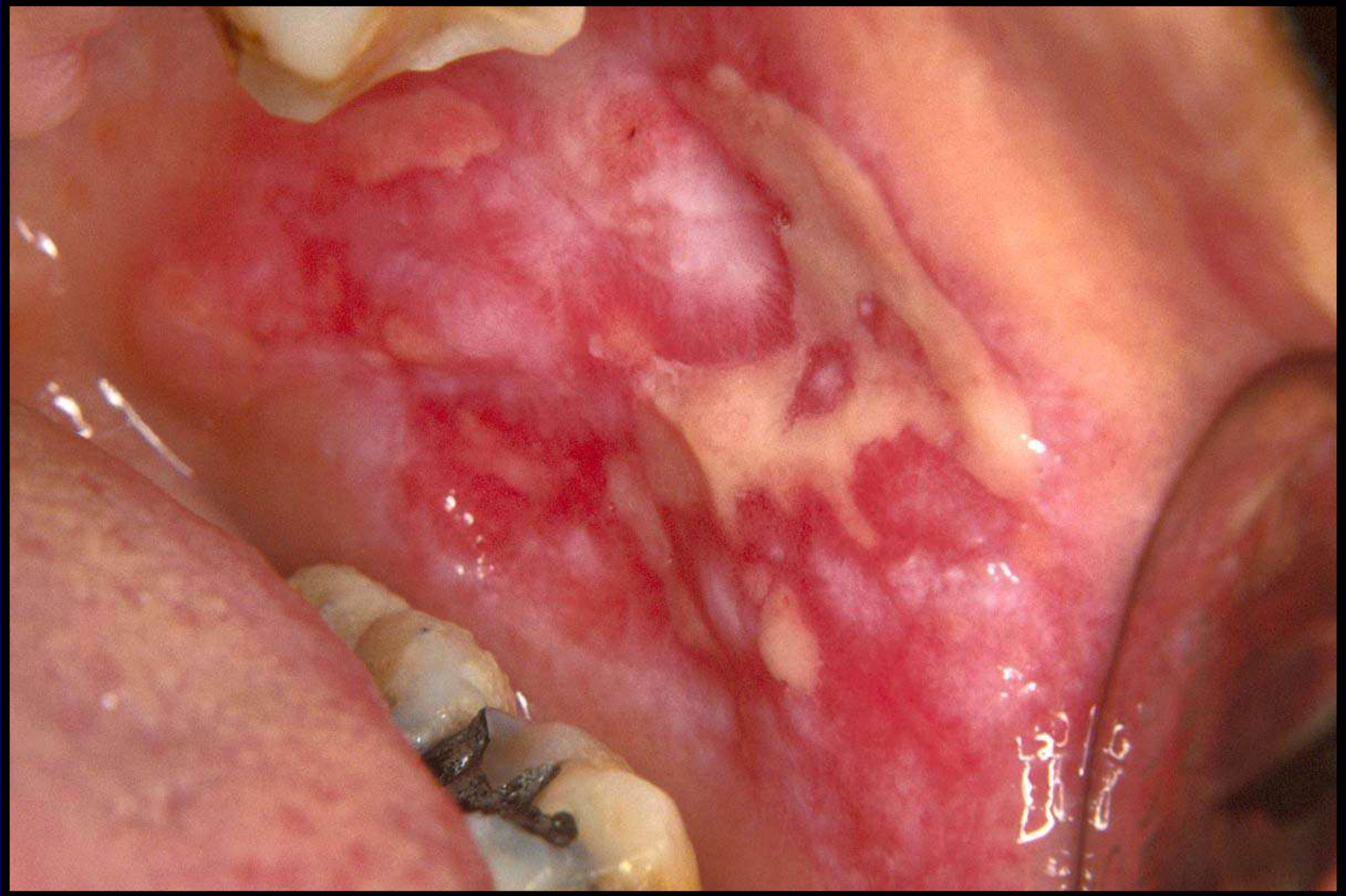
Presentation Clues
Lesions mimic OLP clinically and histologically. Lesions tend to occur in close proximity and opposition to a particular dental material. Mercury is by far the most common culprit reported in the literature.
Dental Materials Implicated in Contact lichenoid reactions
Diagnostic Considerations20
- Skin patch testing is a useful diagnostic tool for contact lichenoid reactions, though results are not absolute.
Chronic Ulcerative Stomatitis21
Clinical presentation of Chronic Ulcerative Stomatitis.
Chronic Ulcerative Stomatitis Details
- Pathology: A true autoimmune disease where antibodies are produced against nuclear proteins responsible for cell growth and differentiation.
- Diagnosis: Requires Direct Immunofluorescence (DIF).
- Treatment: Lesions do not necessarily respond to topical corticosteroids. Plaquenil is the drug of choice.


Linear IgA Disease22
Clinical documentation regarding the presentation of Linear IgA disease in the context of OLP differential diagnosis.
Linear IgA Disease Details
- Pathology: Characterized by the linear deposition of IgA antibodies at the basement membrane zone.
- Diagnosis: Relies on routine histopathology and Direct Immunofluorescence.
- Treatment: Lesions may not respond well to topical corticosteroids. Dapsone is the medication of choice.

Mucous Membrane Pemphigoid2324





- we rely on histopathology and Direct immunofluorescence to differentitat beetwen mmp and OLP
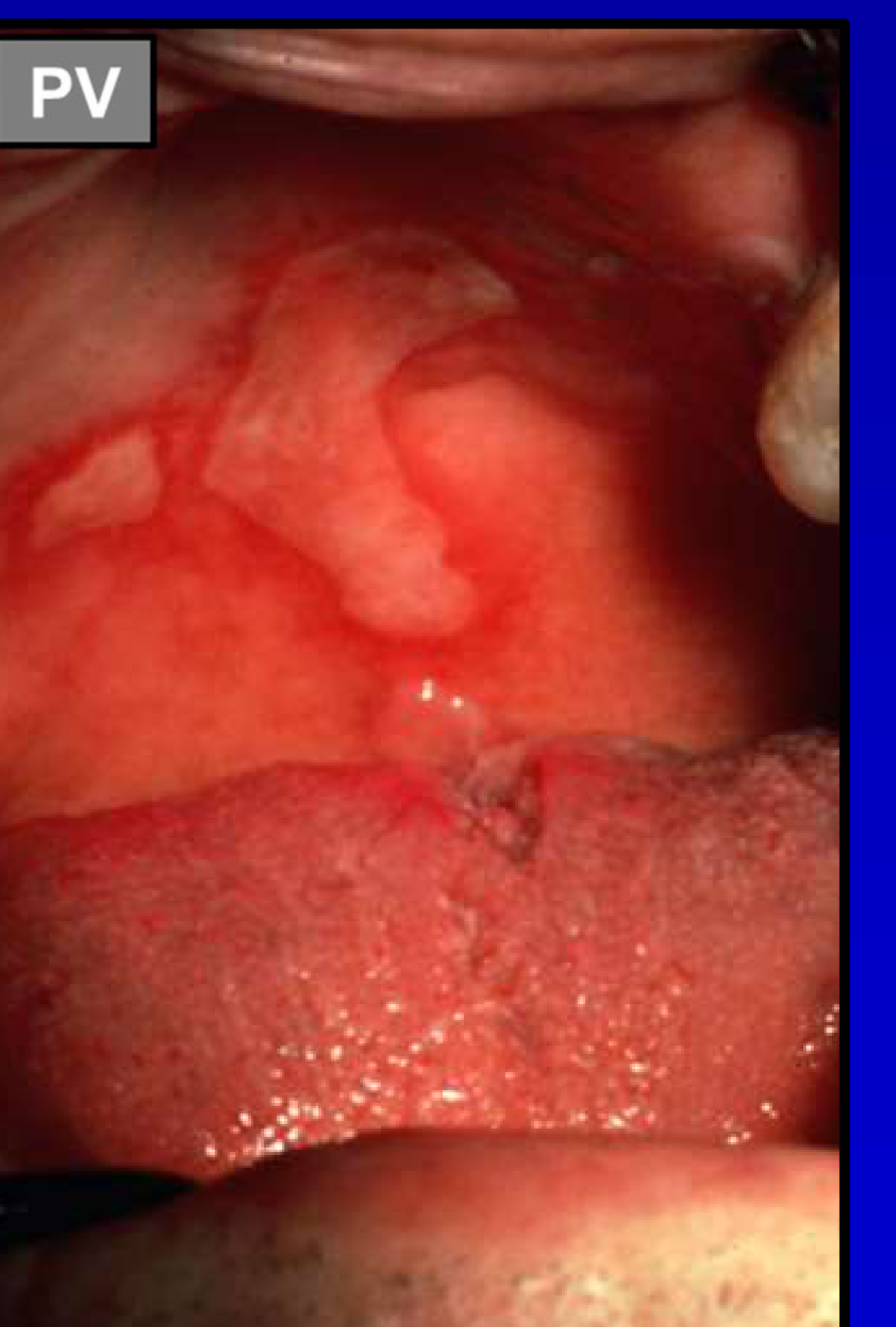
Pemphigus Vulgaris2526
Introduction to Pemphigus Vulgaris as a differential diagnosis.
Pemphigus Vulgaris Details
- Pathology: Autoimmune disease characterized by autoantibodies against components of the desmosomes.
- Significance: Oral lesions often precede skin involvement, which can be life-threatening.
- Treatment: Prudent to initiate treatment with systemic immunosuppressants early in the course of the disease.
Lupus Erythematosus



Graft Versus Host Disease2728
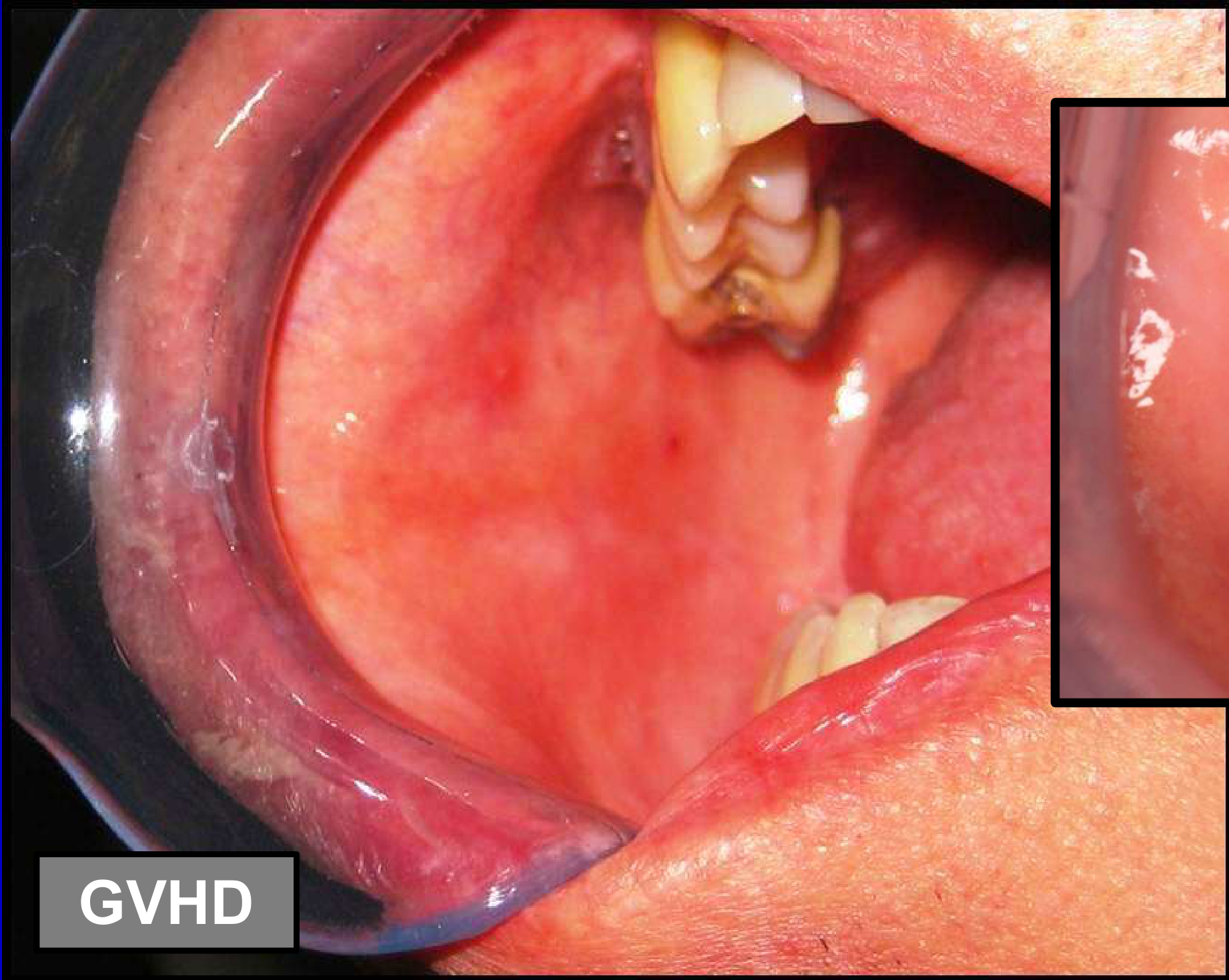
Examination of Graft Versus Host Disease (GVHD) as a lichenoid-presenting condition.
GVHD Presentation
Classic lesions of chronic graft versus host disease can be indistinguishable clinically from OLP. Diagnosis relies on patient history (transplant status) and histopathology.
Clinical characteristics of Graft Versus Host Disease (GVHD).


Diagnosis29
Clinical Criteria
Clinical Diagnostic Requirements30
- Presence of bilateral, more or less symmetric lesions.
- Presence of a lacelike network of slightly raised grey-white lines (reticular pattern).
- Erosive, atrophic, bullous, and plaque-type lesions are only accepted as a subtype in the presence of reticular lesions elsewhere in the oral mucosa.
In all other lesions that resemble Oral Lichen Planus (OLP) but do not complete the aforementioned criteria, the term “clinically compatible with” should be used. Cheng et al., 2016, p. 332
Histopathologic Diagnostic Requirements
- Presence of a well-defined, band-like zone of cellular infiltration that is confined to the superficial part of the connective tissue, consisting mainly of lymphocytes.
- Signs of liquefaction degeneration in the basal cell layer.
- Absence of epithelial dysplasia.
When the histopathologic features are less obvious, the term “histopathologically compatible with” should be used.
Final Diagnosis and Oral Lichenoid Lesions (OLL)
To achieve a final diagnosis, clinical as well as histopathologic criteria should be included. A diagnosis of OLP requires fulfilment of both clinical and histopathologic criteria.
The term OLL will be used in the following conditions:
- Clinically typical of OLP but histopathologically only compatible with OLP.
- Histopathologically typical of OLP but clinically only compatible with OLP.
- Clinically compatible with OLP and histopathologically compatible with OLP.
This distinction prompts consideration of the differential diagnoses listed above.
Histopathological Evaluation
Biopsy Indications313233
Clinical Consideration34
- Should every case of OLP be biopsied?
- Answer: Yes. Visual examination alone gives limited information. Biopsy increases the chances of an accurate diagnosis.
Differential Diagnosis Comparison35
- Verrucous carcinoma
- Oral Lichen Planus (OLP)
Case Study: Early Verrucous Carcinoma Mimicking OLP
Patient: 53-year-old non-smoking female. Presentation: Suspected OLP. Plaque-like lesion associated with the canine. Biopsy Findings: Generalized lesions: Oral Lichen Planus. Plaque-like lesion: Very early verrucous carcinoma. Outcome: Five years post-treatment, patient has an intact maxilla with no recurrence. Lesson: Relying on clinical presentation alone could have attributed the carcinoma to OLP.


Case Study: Solitary Unilateral Lesion
Patient: Referred with suspected OLP. Suspicious Feature: Lesion was solitary and unilateral, which does not fit OLP criteria. Histopathology: Revealed verrucous carcinoma. Lesson: Unilateral solitary lesions should raise immediate suspicion for pathology other than OLP.



Routine Investigations36
Laboratory Screening37
- Full Blood Count (FBC)
- Vitamin B12
- Folate
- Iron studies
- Other relevant investigations
- Deficiencies can be associated with oral mucosal atrophy, ulceration, burning sensation, and increased risk of oral candidosis.
- Autoimmune Screening: ANA (if suspecting Lupus), Anti-skin antibodies (if suspecting Pemphigus).
- Systemic Disease Screening: Test for diseases associated with OLP, such as Diabetes, Thyroid disease, and Hepatitis C infection.
Comparative Clinical Presentation38
-
Folate deficiency: Presentation of reticular white lesions on the palate.
-
Oral Lichen Planus (OLP): Presentation of white lacy patterns (Wickham’s striae) on the hard palate.
-
Full Blood Count (FBC)
-
Vitamin B12
-
Folate
-
Iron studies
-
Other relevant investigations
Management39
- No cure available.
- Treatment is supportive and palliative only.
- Patients must understand OLP is chronic and may last a lifetime
- Condition can be associated with reduced Quality of Life (QOL).
Malignant Transformation Risk
OLP is classified as an oral potentially malignant disorder. The risk of malignant transformation is reported to be about 1%.
Oral Hygiene and Trauma Prevention
Physical Irritants and Oral Care40
- Smooth sharp cusps.
- Eliminate ill-fitting dental prosthesis.
- Maintain meticulous oral hygiene.
Koebner Phenomenon
The Koebner phenomenon (isomorphic response) is a relevant consideration in management where trauma can trigger new lesions.. This phenomenon demonstrated the importance of oral care in patients with these lesions
Alcohol and Lifestyle Considerations

Alcohol and Cancer Risk41
Drinking as little as one standard drink a day increases your risk of mouth cancer.
- Patients should be counseled to quit smoking due to the increased risk of oral squamous cell carcinoma
Australian Alchol Guidelines (NHMRC)
Periodontal Disease and Implants
Periodontal Associations42
Are there associations with periodontal disease?
- Literature is limited, conflicting, and often methodologically flawed. There is no convincing evidence of a definite association
- It is unknown if microorganisms trigger or sustain OLP, or if OLP compromises hygiene leading to periodontal disease
Plaque Control43
Plaque control is important in the management of Oral Lichen Planus (OLP).
Dental Implants44
Implant loss does not appear to be directly related to OLP.
- Studies suggest implant success in OLP patients does not differ from the general population, provided OLP is well controlled
- Implants do not appear to adversely impact the clinical course of OLP
Medication45
Pharmacological management is a primary component of OLP treatment.
- Treat patients who are symptomatic (sensitivity/pain) or present with oral mucosal ulceration (whether symptomatic or asymptomatic)
- First Line: Topical Corticosteroids
- Second Line: Systemic corticosteroids (reserved for severe cases)

Other Topical and Systemic Agents
Therapeutic Categories
- Corticosteroids
- Topical
- Systemic
- Intralesional
- Calcineurin inhibitors (limited evidence)
- Cyclosporine
- Tacrolimus
- Other agents

Topical Corticosteroids
Corticosteroid Options organized by potency
- Clobetasol propionate
- Fluocinonide
- Betamethasone dipropionate
- Beclomethasone dipropionate
- Fluocinonide acetonide
- Betamethasone valerate
- Triamcinolone acetonide
- Hydrocortisone
Specific Topical Formulations46 TGA
Betamethasone Dipropionate
For biopsy-proven symptomatic OLP:
- Australian Therapeutic Guidelines recommend use only in patients with a biopsy-proven diagnosis
- Agent: Betamethasone dipropionate 0.05% ointment (Diprosone)
- Frequency: 2 times per day
Beclomethasone Dipropionate
- Formulation: Inhaler
- Dosage: 50-100mcg/dose
- Frequency: Up to 2 sprays, 4 times per day
Dexamethasone Mouthwash
- Dosage: 0.5-1mg/5ml
- Frequency: Up to 4 times per day
Clinical application of topical formulations often involves dental models or trays to increase contact with inflamed gingival tissues.
- Potency: Clobetasol is the most potent; Hydrocortisone is the least potent
- General preference is to pick the least potent topical corticosteroid that is effective
- Alternatives:
- Ointments: Can be difficult to apply to wet mucosa; dosage control is poor
- Inhaler Spray (Beclomethasone): Metered dose (greater control); Requires coordination/dexterity
- Mouthwash (Dexamethasone): Easy to use for widespread lesions; High cost
- Medication Stent: For gingival lesions; Apply ointment to stent and wear for 5-10 minutes twice daily
Factors Influencing Treatment Effectiveness47
The effectiveness of topical corticosteroids (TC) is influenced by: - Contact Time: Patients should not eat or drink for 30 minutes following application
- Drug potency
- Contact time
- Vehicle / formulation
Causes of Treatment Failure48
Common reasons for treatment failure include:
- Incorrect diagnosis
- Superimposed candidal infection
- Topical corticosteroid (TC) of inadequate potency
- Poor patient compliance
Local Complications
Oral Candidiasis
-
Development of oral candidiasis is a known local complication of topical steroid use.
-
Acute: Easy to diagnose (white plaques removable)
-
Chronic: Difficult to diagnose (lesions look like OLP)
-
Clue: Patient history where medication worked initially but now symptoms worsen
-
Management: Stop topical steroid for 2 weeks, initiate topical antifungal. Restart steroid after 2 weeks while continuing antifungal
-
Antifungal Agents:
- Miconazole oral gel: Works well (watch for drug interactions)
- Amphotericin lozenges: Work well (difficult to dissolve in dry mouth)
- Nystatin oral drops: Not generally recommended due to high sugar content (caries risk) and lower efficacy
Other local complication of topical corticosteroids
- Oral candidosis
- Stomatopyrosis (burning mouth)
- Hypogeusia (reduced taste)
- Oral hairy leukoplakia



Systemic Adverse Effects49
Systemic adverse effects may include: - Adrenal Suppression: Potential risk with high potency/long-term use - Monitoring: Patients need close monitoring for mood changes, sleep patterns, weight changes, etc.
- Changes in:
- Mood
- Weight
- Blood pressure
- Blood glucose
- Plasma cortisol
- Other effects:
- Insomnia
- Moon face
- Hirsutism
Systemic Prednisolone
- ==Considered for severe/non-responders (high doses, e.g., 40mg/day). Systemic side effects are more problematic==
- Dosage: 0.5-1.0 mg/kg/day
Follow-Up and Monitoring50
Cancer Surveillance51
- Regular follow-up is required, at least annually.
- Frequency depends on disease activity
- Persistently ulcerated lesions that do not respond to treatment, or indurated lesions, should be re-biopsied to rule out malignant transformation
- Monitoring is essential due to the risk of Squamous Cell Carcinoma (SCC) developing in OLP.
Ongoing clinical review is necessary for the long-term management of OLP patients.
Case Study: Malignant Transformation Detected During Surveillance
Patient: Lady with biopsy-proven OLP, generally asymptomatic. Event: During a routine review, a small indurated lesion was noted (completely asymptomatic; patient unaware). Outcome: Five years later, the patient remains disease-free. Because the squamous cell carcinoma was picked up very early due to regular follow-up, she only required a small operation. Significance: Quality of life was not significantly compromised due to early detection.



Summary52
Oral Lichen Planus (OLP) is characterized by the following key features:
- Nature of the Disease: It is a common, chronic, systemic, and immunologically mediated condition.
- Aetiology: The exact cause remains unknown.
- Diagnosis: Identification is based on the fulfillment of both clinical and histopathological criteria.
- Biopsy is critical.
- Management: Topical corticosteroids serve as the first line of treatment.
- Monitoring: Regular clinical follow-up is recommended for all patients.
- Requires regular lifelong follow-up due to the risk of malignant transformation.
Footnotes
-
Original PDF page 1: L7 Allergies and immune disease I, p.1 ↩
-
Original PDF page 2: L7 Allergies and immune disease I, p.2 ↩
-
Original PDF page 3: L7 Allergies and immune disease I, p.3 ↩
-
Original PDF page 4: L7 Allergies and immune disease I, p.4 ↩
-
Original PDF page 5: L7 Allergies and immune disease I, p.5 ↩
-
Original PDF page 6: L7 Allergies and immune disease I, p.6 ↩
-
Original PDF page 9: L7 Allergies and immune disease I, p.9 ↩
-
Original PDF page 11: L7 Allergies and immune disease I, p.11 ↩
-
Original PDF page 15: L7 Allergies and immune disease I, p.15 ↩
-
Original PDF page 16: L7 Allergies and immune disease I, p.16 ↩
-
Original PDF page 17: L7 Allergies and immune disease I, p.17 ↩
-
Original PDF page 21: L7 Allergies and immune disease I, p.21 ↩
-
Original PDF page 22: L7 Allergies and immune disease I, p.22 ↩
-
Original PDF page 23: L7 Allergies and immune disease I, p.23 ↩
-
Original PDF page 24: L7 Allergies and immune disease I, p.24 ↩
-
Original PDF page 36: L7 Allergies and immune disease I, p.36 ↩
-
Original PDF page 25: L7 Allergies and immune disease I, p.25 ↩
-
Original PDF page 26: L7 Allergies and immune disease I, p.26 ↩
-
Original PDF page 28: L7 Allergies and immune disease I, p.28 ↩
-
Original PDF page 32: L7 Allergies and immune disease I, p.32 ↩
-
Original PDF page 33: L7 Allergies and immune disease I, p.33 ↩
-
Original PDF page 35: L7 Allergies and immune disease I, p.35 ↩
-
Original PDF page 38: L7 Allergies and immune disease I, p.38 ↩
-
Original PDF page 40: L7 Allergies and immune disease I, p.40 ↩
-
Original PDF page 42: L7 Allergies and immune disease I, p.42 ↩
-
Original PDF page 43: L7 Allergies and immune disease I, p.43 ↩
-
Original PDF page 45: L7 Allergies and immune disease I, p.45 ↩
-
Original PDF page 46: L7 Allergies and immune disease I, p.46 ↩
-
Original PDF page 47: L7 Allergies and immune disease I, p.47 ↩
-
Original PDF page 48: L7 Allergies and immune disease I, p.48 ↩
-
Original PDF page 51: L7 Allergies and immune disease I, p.51 ↩
-
Original PDF page 53: L7 Allergies and immune disease I, p.53 ↩
-
Original PDF page 54: L7 Allergies and immune disease I, p.54 ↩
-
Original PDF page 50: L7 Allergies and immune disease I, p.50 ↩
-
Original PDF page 55: L7 Allergies and immune disease I, p.55 ↩
-
Original PDF page 58: L7 Allergies and immune disease I, p.58 ↩
-
Original PDF page 56: L7 Allergies and immune disease I, p.56 ↩
-
Original PDF page 57: L7 Allergies and immune disease I, p.57 ↩
-
Original PDF page 59: L7 Allergies and immune disease I, p.59 ↩
-
Original PDF page 60: L7 Allergies and immune disease I, p.60 ↩
-
Original PDF page 61: L7 Allergies and immune disease I, p.61 ↩
-
Original PDF page 65: L7 Allergies and immune disease I, p.65 ↩
-
Original PDF page 66: L7 Allergies and immune disease I, p.66 ↩
-
Original PDF page 67: L7 Allergies and immune disease I, p.67 ↩
-
Original PDF page 68: L7 Allergies and immune disease I, p.68 ↩
-
Original PDF page 75: L7 Allergies and immune disease I, p.75 ↩
-
Original PDF page 76: L7 Allergies and immune disease I, p.76 ↩
-
Original PDF page 77: L7 Allergies and immune disease I, p.77 ↩
-
Original PDF page 84: L7 Allergies and immune disease I, p.84 ↩
-
Original PDF page 87: L7 Allergies and immune disease I, p.87 ↩
-
Original PDF page 86: L7 Allergies and immune disease I, p.86 ↩
-
Original PDF page 88: L7 Allergies and immune disease I, p.88 ↩