Allergies and Immune Mediated Disease II
Course Presentation Overview1
This session continues the examination of immunological conditions, specifically focusing on allergies and immune-mediated diseases as presented by Dr. Agnieszka Frydrych at The University of Western Australia.
Scope Clarification
The lecture specifically continues the discussion on inflammatory diseases affecting the oral mucosa.
Introduction
Why is this important?2
- Common Conditions: Crucial to recognize them correctly for appropriate management
- Life-Threatening Conditions: Vital to recognize because they can be life-threatening if left untreated
Transient Lingual Papillitis
The cause of this condition is currently unknown, though several potential factors have been suggested:
Aetiology and Pathogenesis3
- Local irritation
- Stress
- Gastrointestinal (GI) disease
- Hormonal factors
- Infection
- Hypersensitivity
Clinical Features4
-
Hyperkeratosis or ulceration
-
Small vascular channels in the underlying lamina propria
-
Inflammatory cell infiltrate
-
Enlarged filiform papillae
-
Papillae may appear red or covered by yellow ulcerated cap
-
Patients may experience mild to moderate pain
-
Systemic symptoms may include fever and cervical lymphadenopathy

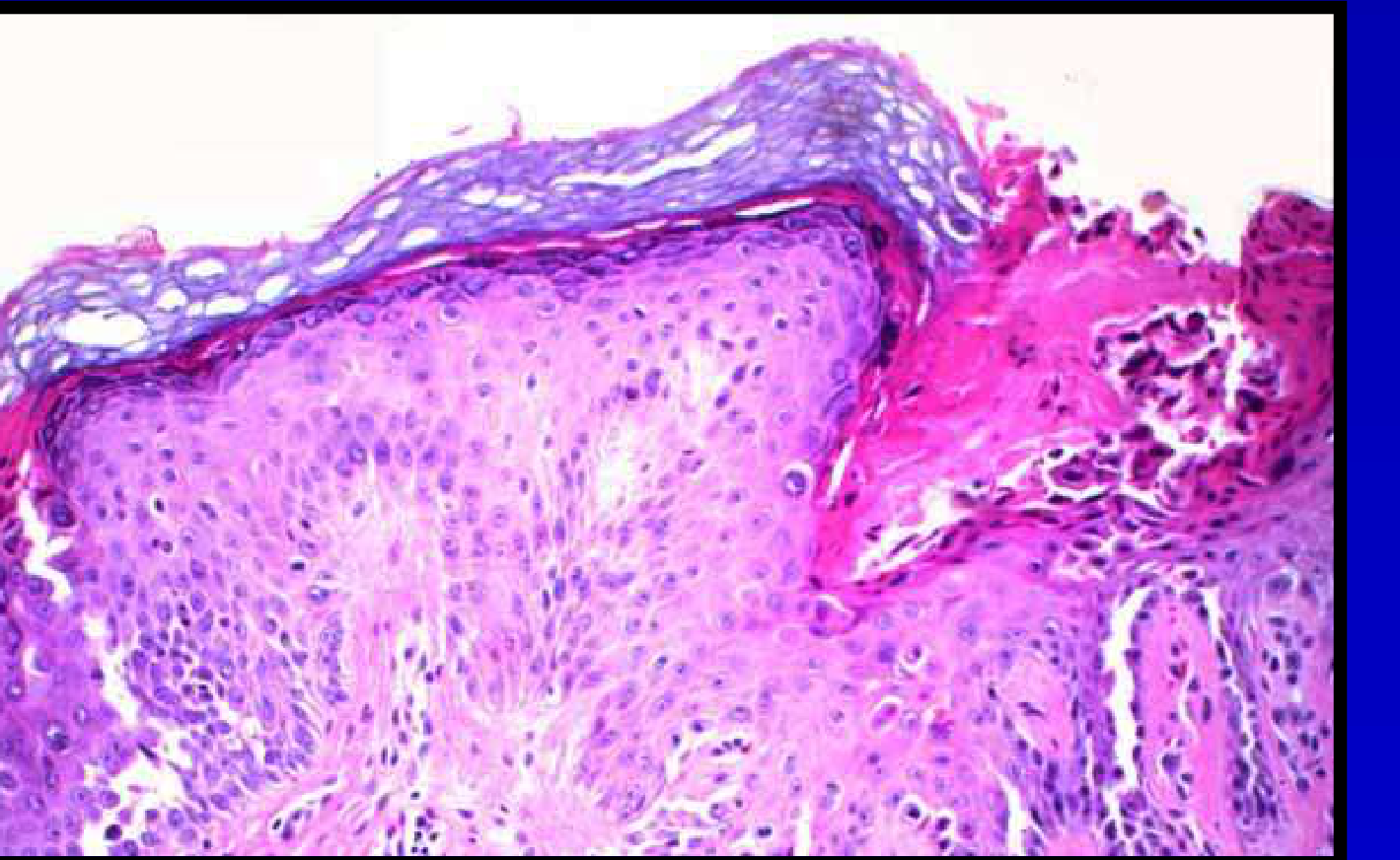
Histopathology5
-
The condition typically resolves without therapy.
-
Surface epithelium: Exhibits hyperkeratosis or ulceration
-
Underlying connective tissue: Small vascular channels evident, Mixed inflammatory cell infiltrate present
Treatment6
- Condition tends to resolve without any therapy
- To reduce pain or discomfort: Topical corticosteroids, Anti-inflammatory agents, Anesthetics

Recurrent Aphthous Stomatitis
-
Idiopathic
-
Local cell-mediated immune response involving:
- CD8+ T-cells
- NK cells
- Macrophages
- Mast cells
-
Genetic predisposition
-
Family History: 40% of affected individuals have a first-degree relative. 90% risk if both parents suffer.
Aetiology and Pathogenesis7
The condition presents in three clinical forms:

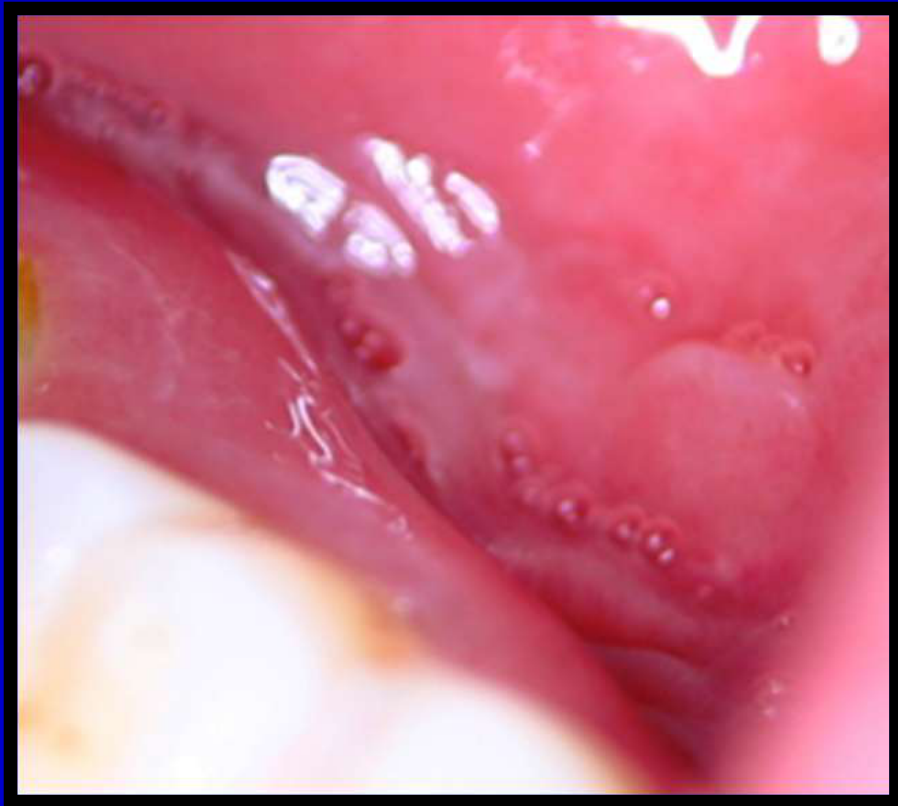
Clinical Features8
- Minor
- Major
- Herpetiform
(Visual evidence of inflammation under the epithelium provided in source)
Clinical Criteria
- Minor: 1 to 6 ulcers, 2-5mm, heal in 2 weeks, non-keratinized.
- Major: 1 to 6 ulcers, >5mm, heal in 1 month, both mucosa types.
- Herpetiform: Multiple ulcers, heal in 2 weeks, both mucosa types.
 |  |  |
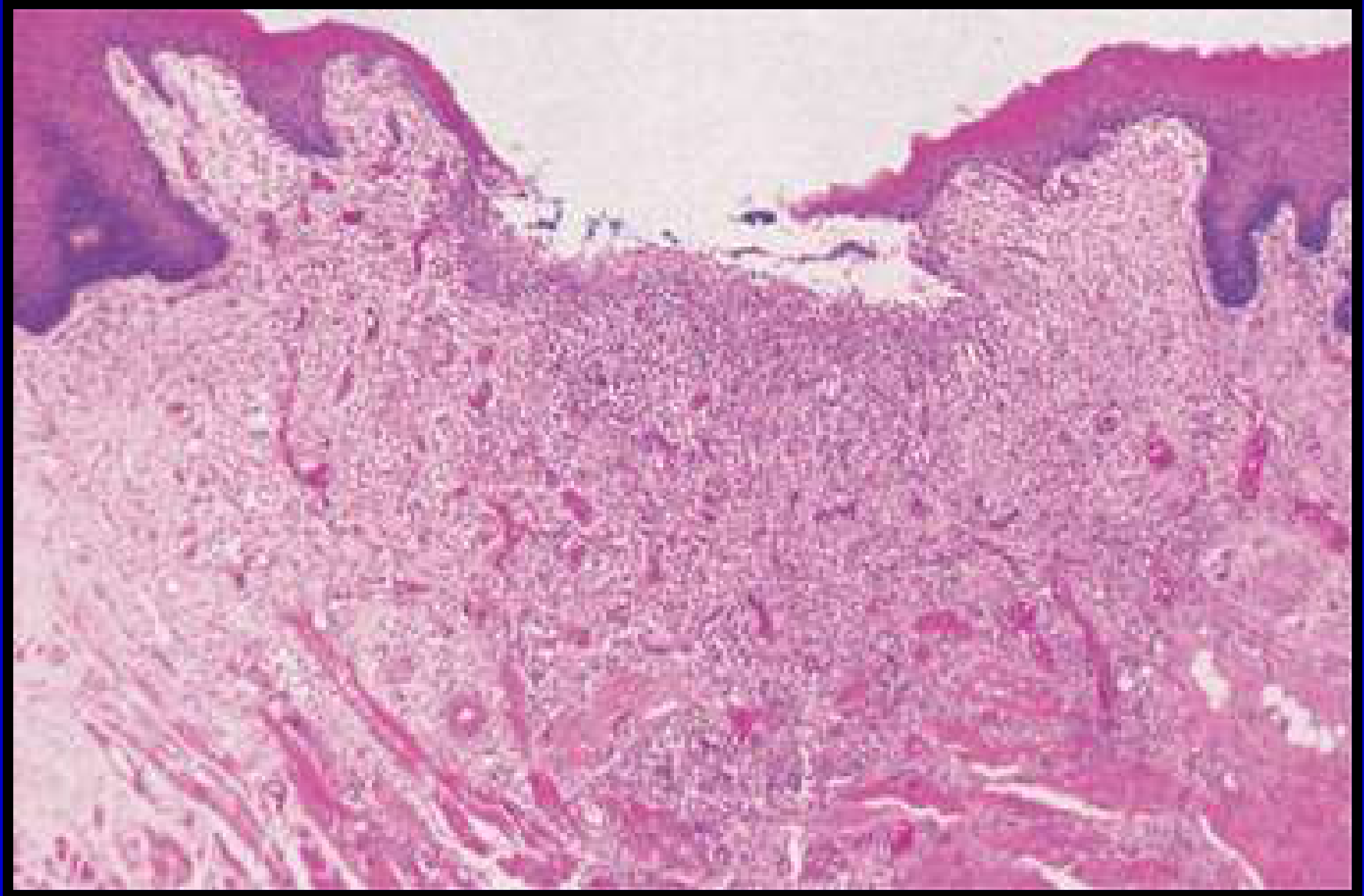
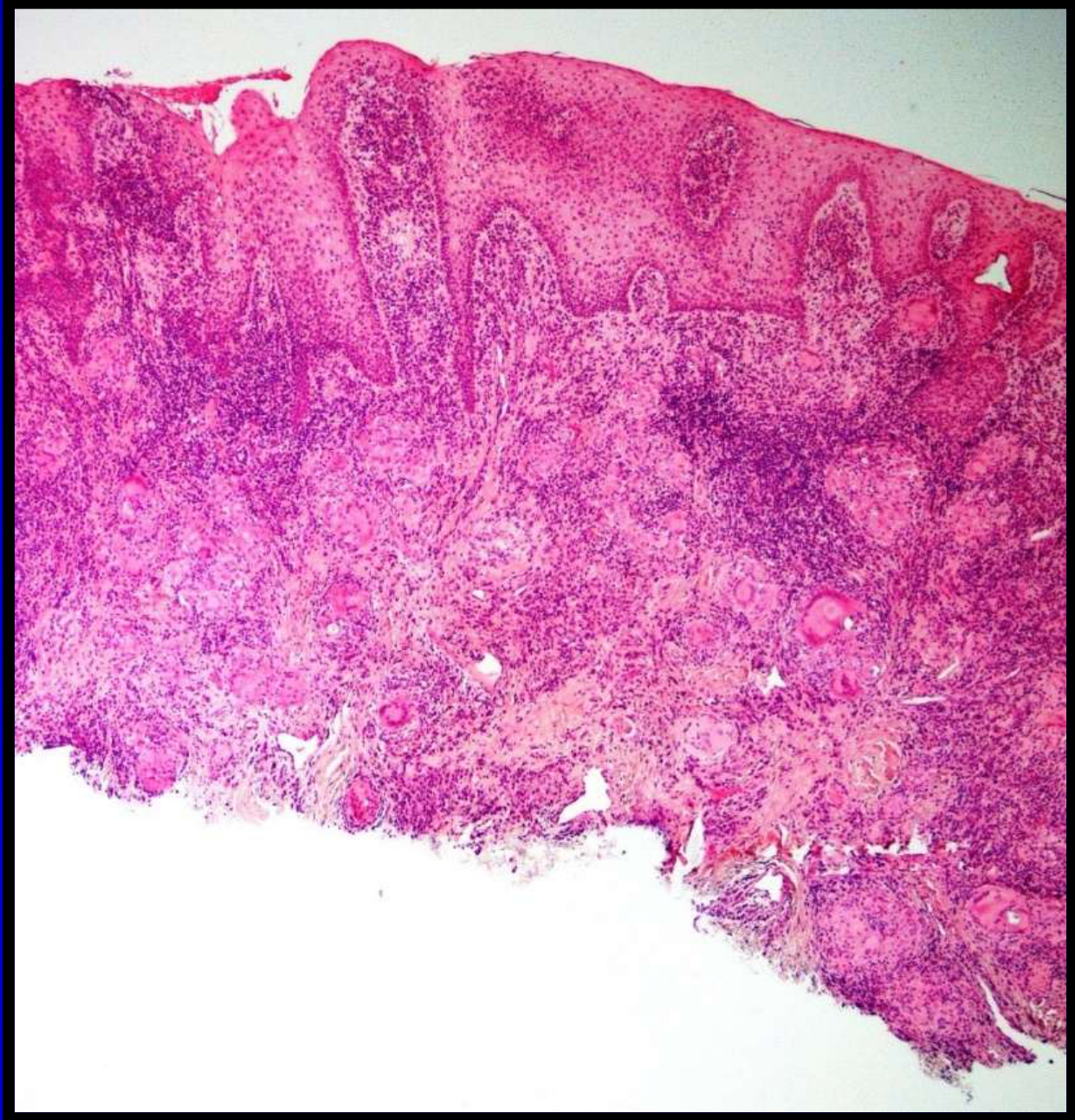
Histopathology9
Histopathology Findings
- Ulceration: Loss of epithelium.
- Inflammatory Infiltrate: Lymphocytes, histiocytes, and polymorphs.
[!info] Differential Diagnosis Specifics
- Nutritional deficiencies: Vitamin B12, folate, and iron.
- Immunodeficiencies: IgA deficiency, HIV.
Differential Diagnosis10
Behcet’s syndrome
- Celiac disease
- Cyclic neutropenia
- Nutritional deficiencies
- Immunodeficiency
- Inflammatory bowel disease
- Other related systemic conditions

Treatment11
- Remove predisposing factors
- Maintain good oral hygiene (OH)
- Medication:
- Corticosteroids
- Tetracycline
- Systemic immuno-modulators - Severe cases: Azathioprine, Dapsone, Colchicine.
Orofacial Granulomatosis
-
Unknown
-
Considered a delayed type of hypersensitivity reaction
-
The inflammatory response is associated with non-caseating granulomas in the connective tissue.
-
Granulomas appear to cause lymphatic obstruction and lymphoedema, explaining the significant soft tissue swelling.
Aetiology and Pathogenesis12
Clinical Features1314
- Swollen erythematous gingiva.
- Erythematous, slightly swollen buccal mucosa with a cobblestone appearance.
- Linear ulcers affecting mucosa (e.g., mandibular buccal sulcus).
- Classic non-tender swelling affecting one or both lips.
- Episodes may be associated with:
- Fever
- Cervical node enlargements
- Defects of cranial nerves (e.g., facial palsy)
Case Study: Young Lady with Orofacial Granulomatosis
- Presentation: Swollen erythematous gingiva and erythematous, slightly swollen buccal mucosa exhibiting a cobblestone appearance.
- Ulceration: Linear ulcers were observed affecting the mucosa of the left mandibular buccal sulcus.
- Swelling: Classic non-tender swelling was noted affecting the lips.

 |  |  |
 |  |
Histopathology15
- Oedema in the superficial connective tissue with dilatation of lymphatic vessels.
- Presence of epithelioid histiocytes, lymphocytes, and multinucleated giant cells.
 |  |
Differential Diagnosis16
- Idiopathic OFG
- Crohn’s Disease
- Sarcoidosis
- Infections
- Food or Contact Allergies
- Other granulomatous diseases
Treatment17
-
Address underlying cause
-
Corticosteroids
-
Other therapies as indicated
-
Note: All patients presenting with orofacial granulomatosis need to undergo an extensive workup to ensure the final diagnosis is correct.
-
Centered around addressing the cause if identified.
-
Corticosteroids: Often used as topical treatment, systemic treatment, or intralesional injections (particularly for swollen lips).
-
Severe cases: Immunomodulating agents may be required.

Wegener’s Granulomatosis
Aetiology and Pathogenesis18
- Unknown
- Abnormal immune reaction
==* Characterized by non-caseating granulomas and vasculitis.==
==* Uncommon but important to recognize as it can be fatal if left untreated.==
==* Believed to reflect an abnormal immune reaction secondary to: non-specific infection and/or aberrant hypersensitive response to an inhaled antigen.==
==* Can present at any age with equal predisposition between males and females.==
==* Can involve almost every organ.==
Clinical Features19
Head and Neck Region: * Nasal discharge, chronic sinus pain, nasal ulceration. * Destruction of the nasal septum can lead to the “saddle nose” deformity. * Congestion, fever, epistaxis, and sore throat.
- Intraoral Lesions:
- Not particularly common.
- Classic presentation: “Strawberry gingivitis”.
- May be associated with destructive bone loss.
 |  |
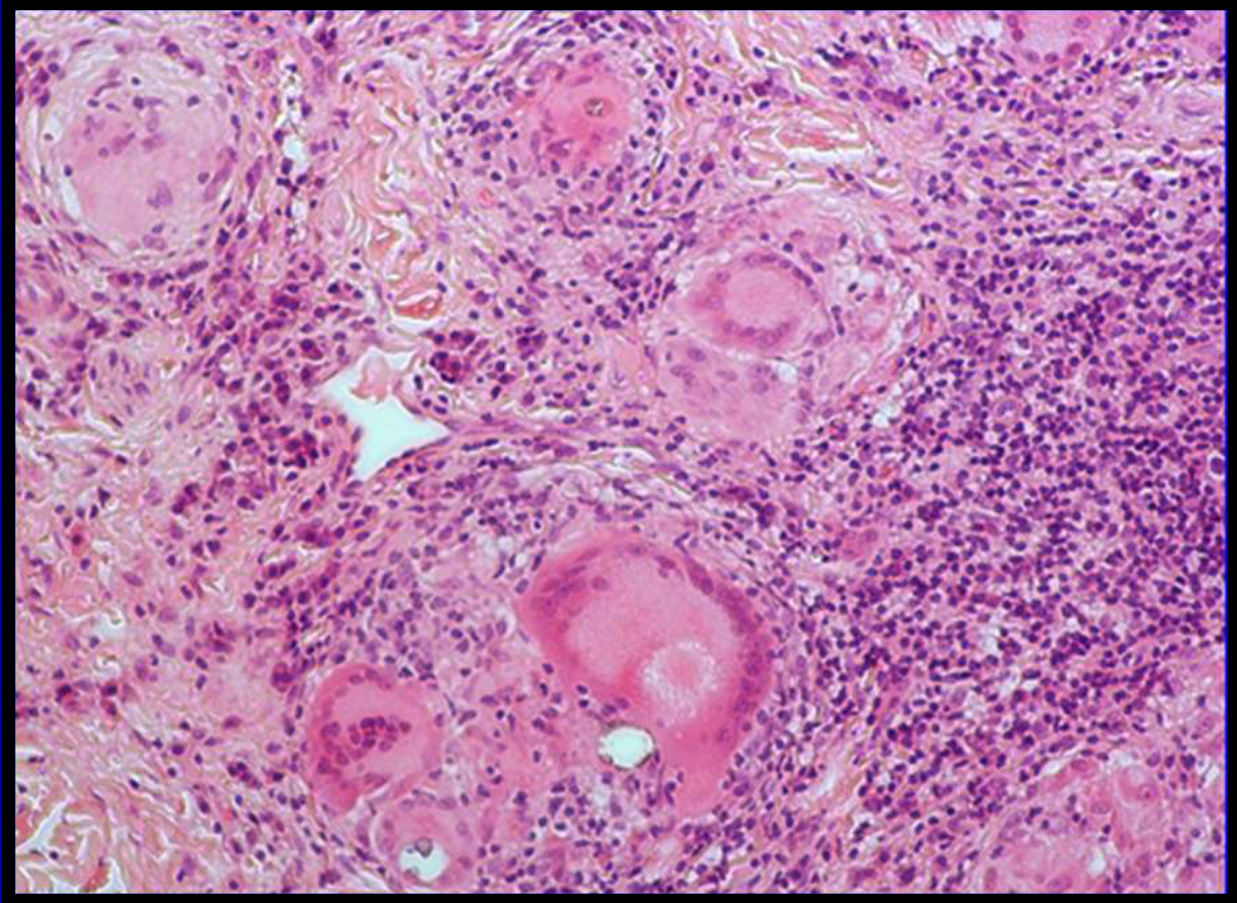
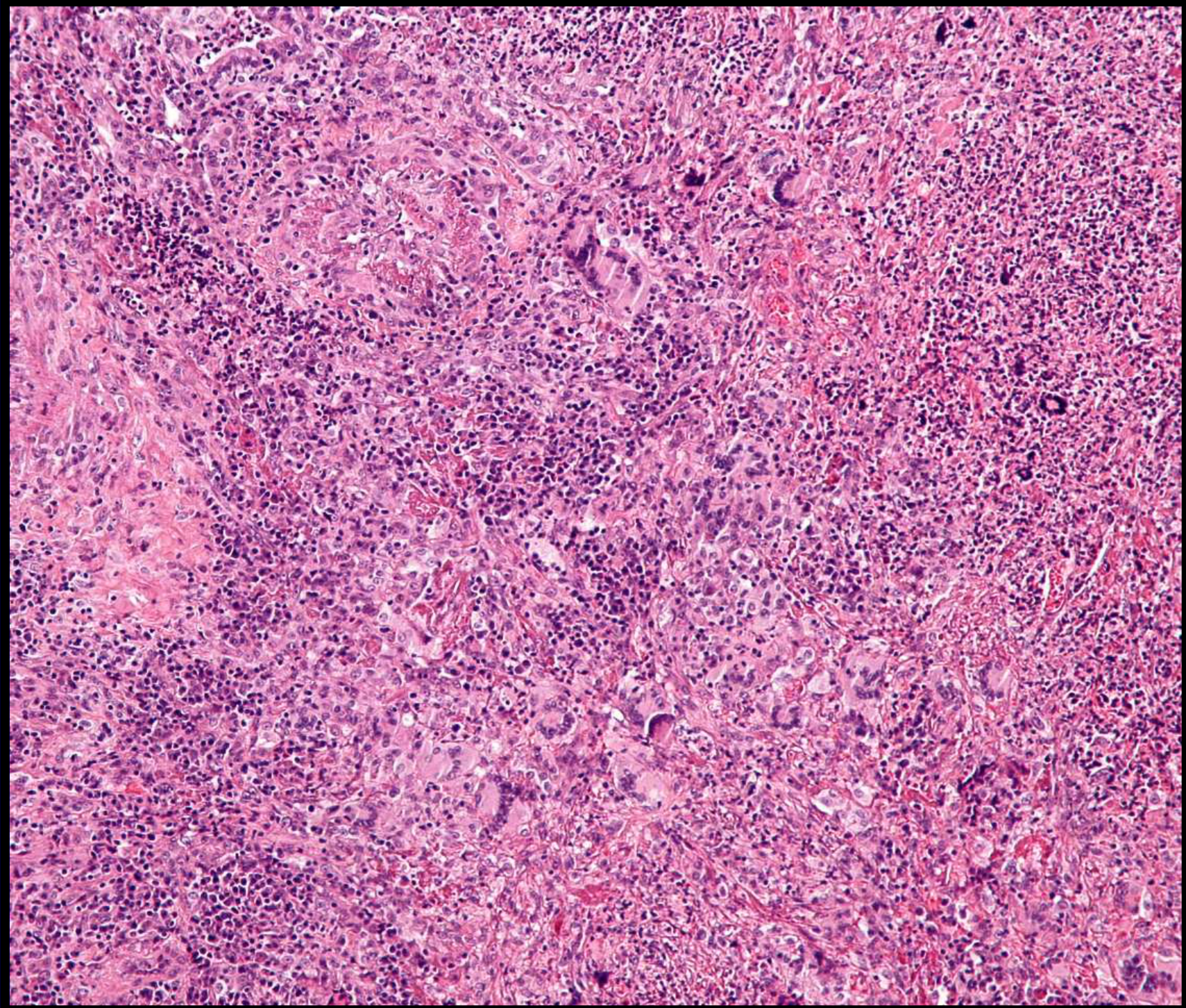
Histopathology20
- Histopathology
- ANCA (anti-neutrophil cytoplasm antibodies)
==* Mixed inflammation centered around blood vessels.==
==* Transmural inflammation of vessels, often with heavy neutrophilic inflammation.==
==* Necrosis in connective tissue adjacent to the vessel.==
==* Infiltrate may include histiocytes, lymphocytes, eosinophils, and multinucleated giant cells.==
Diagnosis21
- Oral prednisolone
- Cyclophosphamide
==* Based on clinical presentation + microscopic findings of necrotizing and granulomatous vasculitis.==
==* Serum ANCA supports the diagnosis.==
Treatment22
==* First line: Oral prednisolone and cyclophosphamide.==
Perioral Dermatitis
- Idiosyncratic response to a variety of exogenous substances:
- Tartar control toothpaste
- Bubble gum
- Cosmetic products
- These may produce irritant/allergic contact dermatitis or induce proliferation of skin flora.
Aetiology and Pathogenesis23
(Clinical features section placeholder)
Clinical Features24
-
Presents with dermatitis around the oral region (examples shown in lecture slides).
-
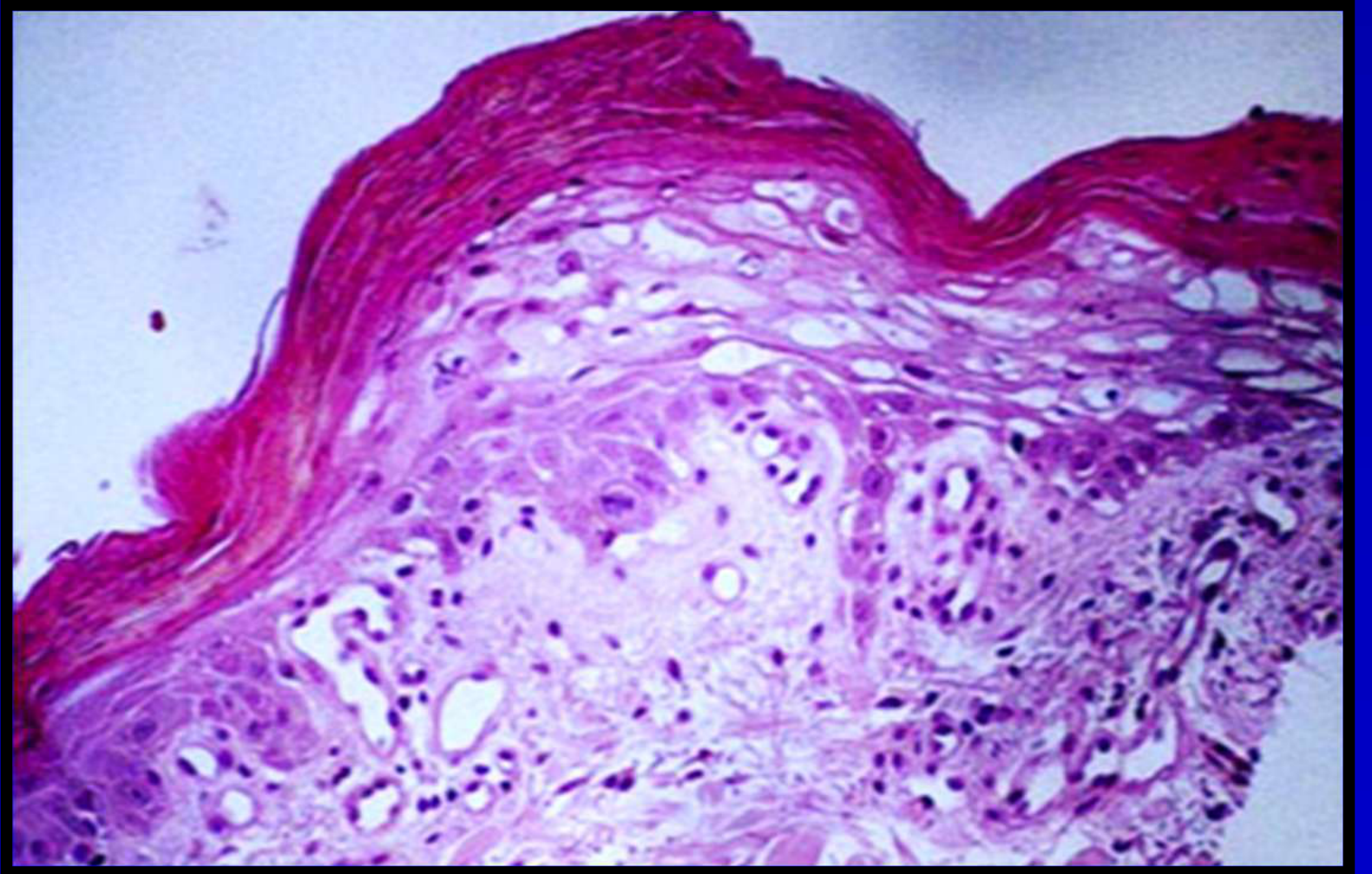
Chronic lymphohistiocytic dermatitis
-
Peri-follicular granulomatous inflammation
 |  |
Histopathology25
- Oral tetracycline or erythromycin
- Topical metronidazole or erythromycin
Treatment26
Allergic Contact Stomatitis
- Hypersensitivity to allergens is commonly observed in the oral cavity.
- Numerous substances may be involved.
- Specific substances include foods, dental materials, and medications
- Reaction types range from localized to anaphylactic reactions
Aetiology and Pathogenesis27
- Erythema
- Oedema
Clinical Features28
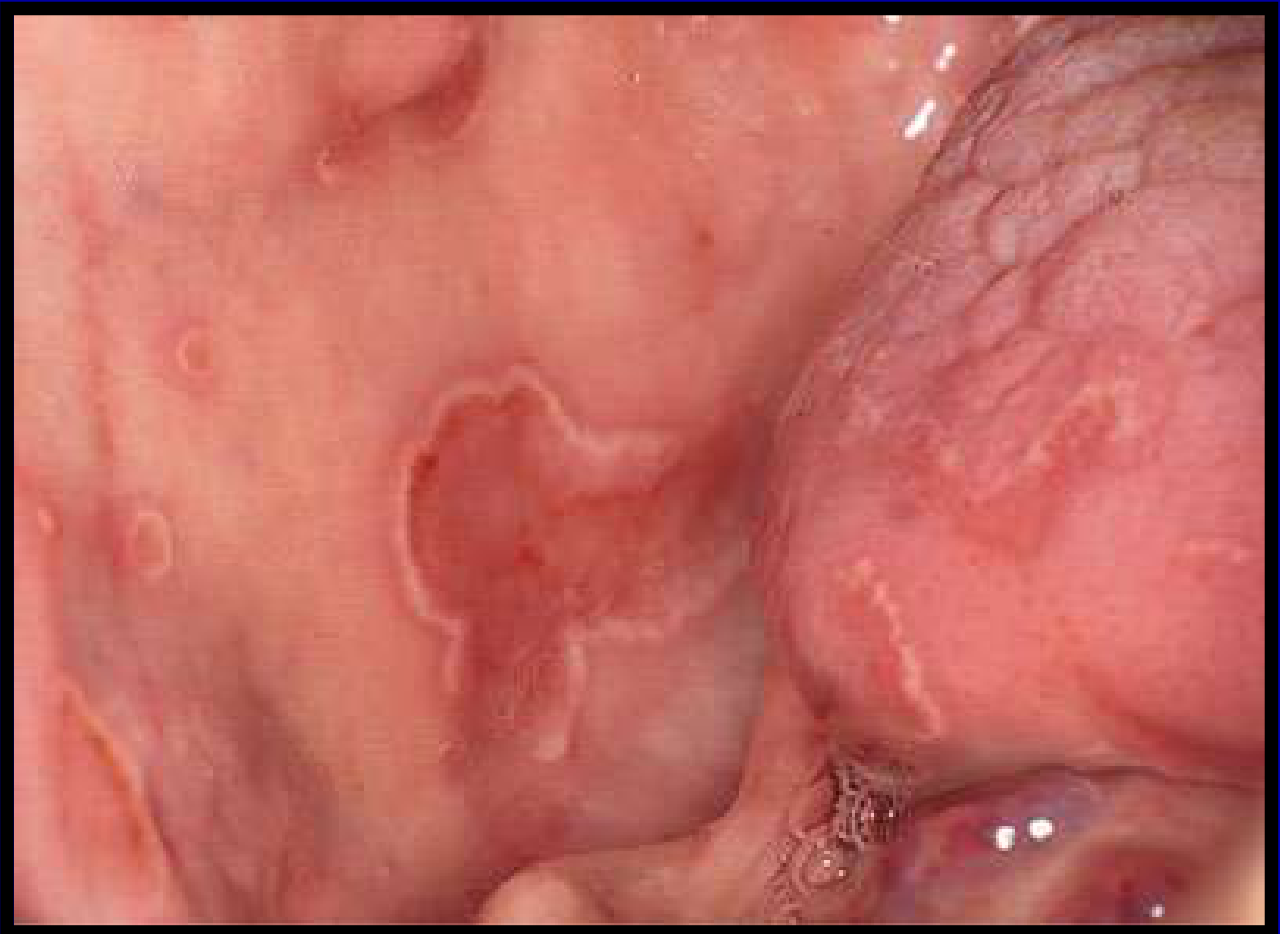
Findings often seen in cases such as contact stomatitis from cinnamon:
- Redness and swelling of the oral mucosa
- Examples include reactions associated with toothpaste and denture material
Case Example: Toothpaste and Denture Material Sensitivity
- Scenario 1: Allergic contact stomatitis associated with toothpaste components
- Scenario 2: Allergic contact stomatitis associated with denture material
- Presentation: Both presented with redness and swelling of the oral mucosa
 |  |
Histopathology29
-
Spongiosis
-
Engorged and dilated blood vessels
-
Lymphocytes
-
Plasma cells
-
Spongiosis: Presence of intra- and intercellular oedema
-
Infiltrate: Inflammatory infiltrate containing lymphocytes and plasma cells
-
Eliminate allergen
-
Antihistamine
-
Topical corticosteroid
Treatment30
- Elimination of the allergen: Allergy tests may need to be undertaken to identify the allergen
Angioedema
- Allergic
- Drug-induced (non-allergic)
- Hereditary (C1 esterase inhibitor deficiency)
Aetiology and Pathogenesis31
- A potentially lethal condition characterized by rapidly developing swelling.
- Affects lips, tongue, and oral facial tissues.
- Swelling is usually transient.
- Three Types:
- Allergic: Associated with Type I hypersensitivity reaction.
- Drug-induced (Non-allergic): Associated with ACE inhibitors and NSAIDs.
- Hereditary: Due to deficiency of C1 esterase inhibitor.
(Clinical features section placeholder)
Clinical Features32
-
History
-
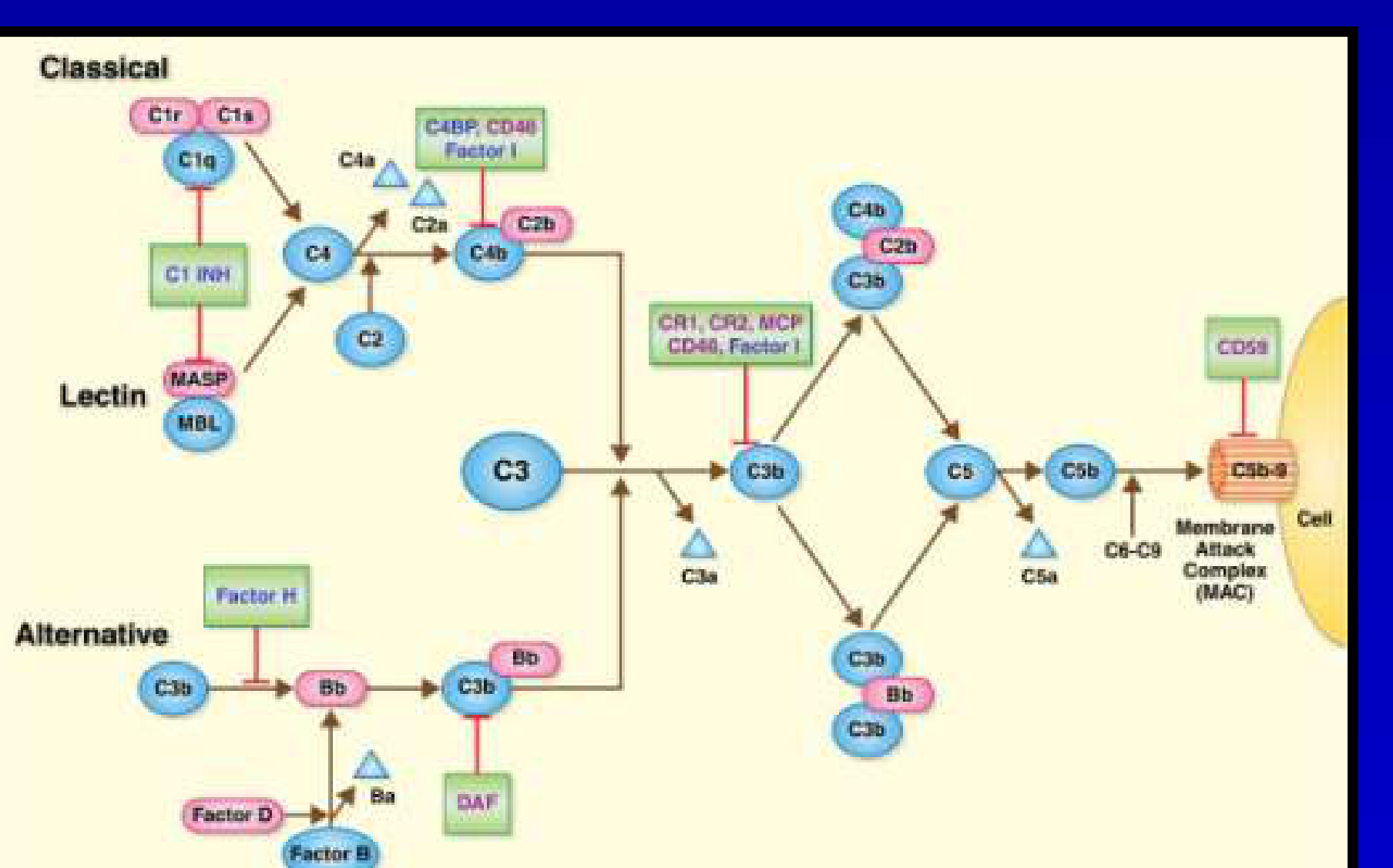
Serum C3, C4 levels and C1 esterase inhibitor activity
-
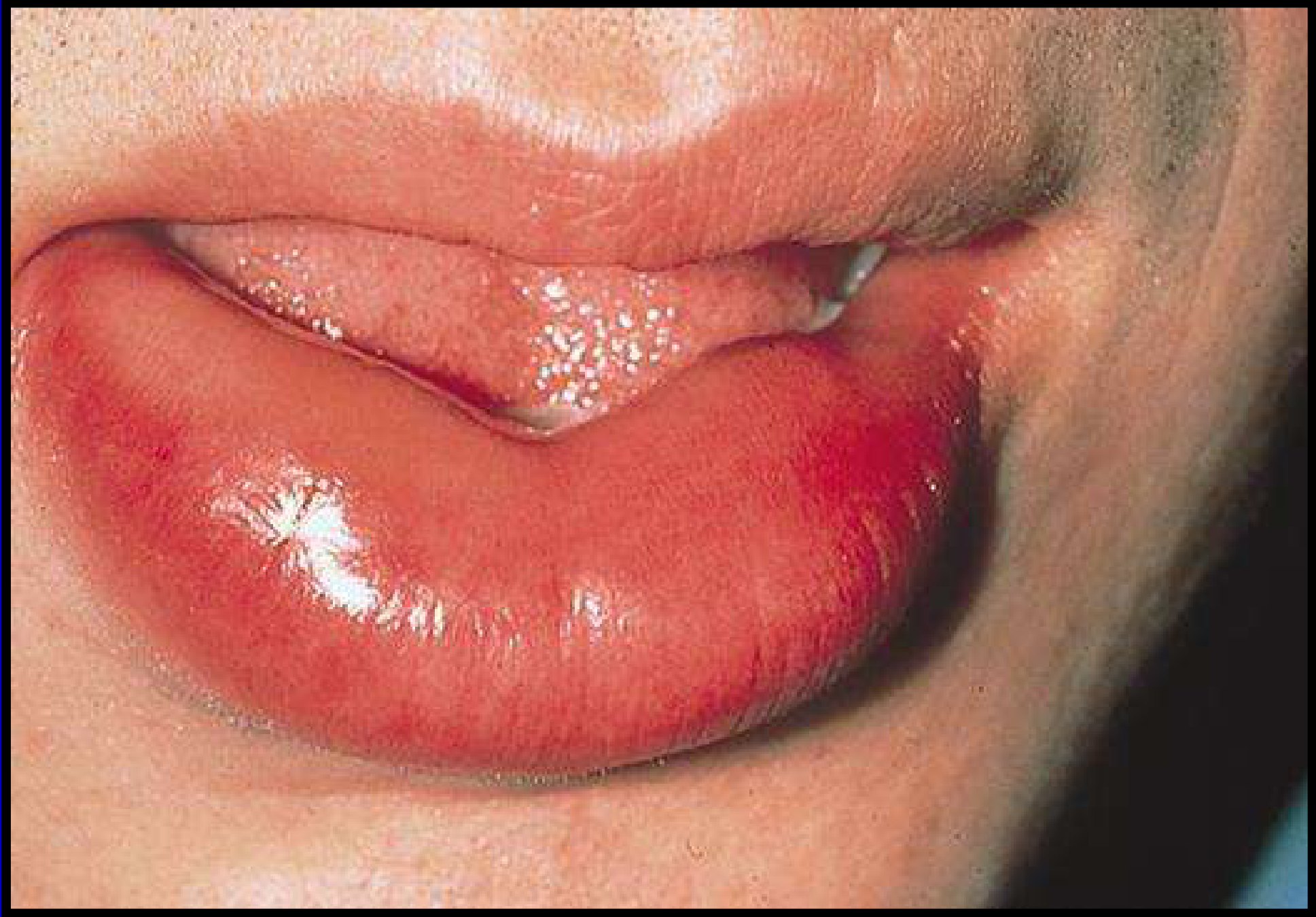
Swelling can affect the lower lip (cosmetic problem) or the tongue (potential airway obstruction).
-
Hereditary Angioedema Blood Tests:
- Normal level of C3 complement factor.
- Low level of C4.
- Decreased C1 esterase inhibitor activity.
Case Example: Lower Lip Angioedema
- Presentation: Swelling affecting the lower lip.
- Significance: When just the lip is involved, it is primarily a cosmetic problem.
Diagnosis33
Treatment34
-
Prevention: Avoid the allergen which triggers the reaction.
-
Hereditary Angioedema: Requires C1 esterase inhibitor replacement.
-
Severe cases: medical emergency – adrenaline
-
Corticosteroids
-
Antihistamines
-
Prevention is important
Erythema Migrans35
Also referred to as geographic tongue and benign migratory glossitis.
 |  |  |
Aetiology and Pathogenesis36
- Common genetic condition of unknown cause
- May be associated with other conditions
- May be associated with other conditions such as psoriasis.
Clinical Features37
- Common (2% of US population)
- Females > Males
- More common in young, non-smokers, and atopic individuals
- Usually affects the dorsal surface of the tongue
- Usually asymptomatic
- May be associated with fissured tongue
- Location: Can affect other areas (floor of the mouth, buccal mucosa).
- Symptoms: Can be associated with:
- Oral burning sensation.
- Sensitivity to toothpaste, spicy, or acidic foods.
Histopathology38
- White lesion margins: Correspond to hyperkeratosis and acanthosis.
- Red areas: Loss of keratin and intraepithelial infiltrates with neutrophils and lymphocytes.
- Underlying connective tissue: Inflammatory infiltrate composed of polymorphs, lymphocytes, and plasma cells.
 |  |
Differential Diagnosis39
- Candidiosis
- Leukoplakia
- Oral lichen planus
- Lupus erythematosus

Treatment40
- Usually none required
- Topical corticosteroids for symptomatic cases
- For discomfort:
- Topical preparations: Benzydamine hydrochloride mouthwash or Difflam mouthwash.

Pemphigus
- Group of chronic autoimmune diseases characterised by epithelial blistering affecting mucocutaneous surfaces
- Autoantibodies directed against desmosomes
- Desmosomes are epithelial adhesion proteins; damage causes cells to detach
- Pemphigus Vulgaris is the most common and severe form
 |  |
Aetiology and Pathogenesis41
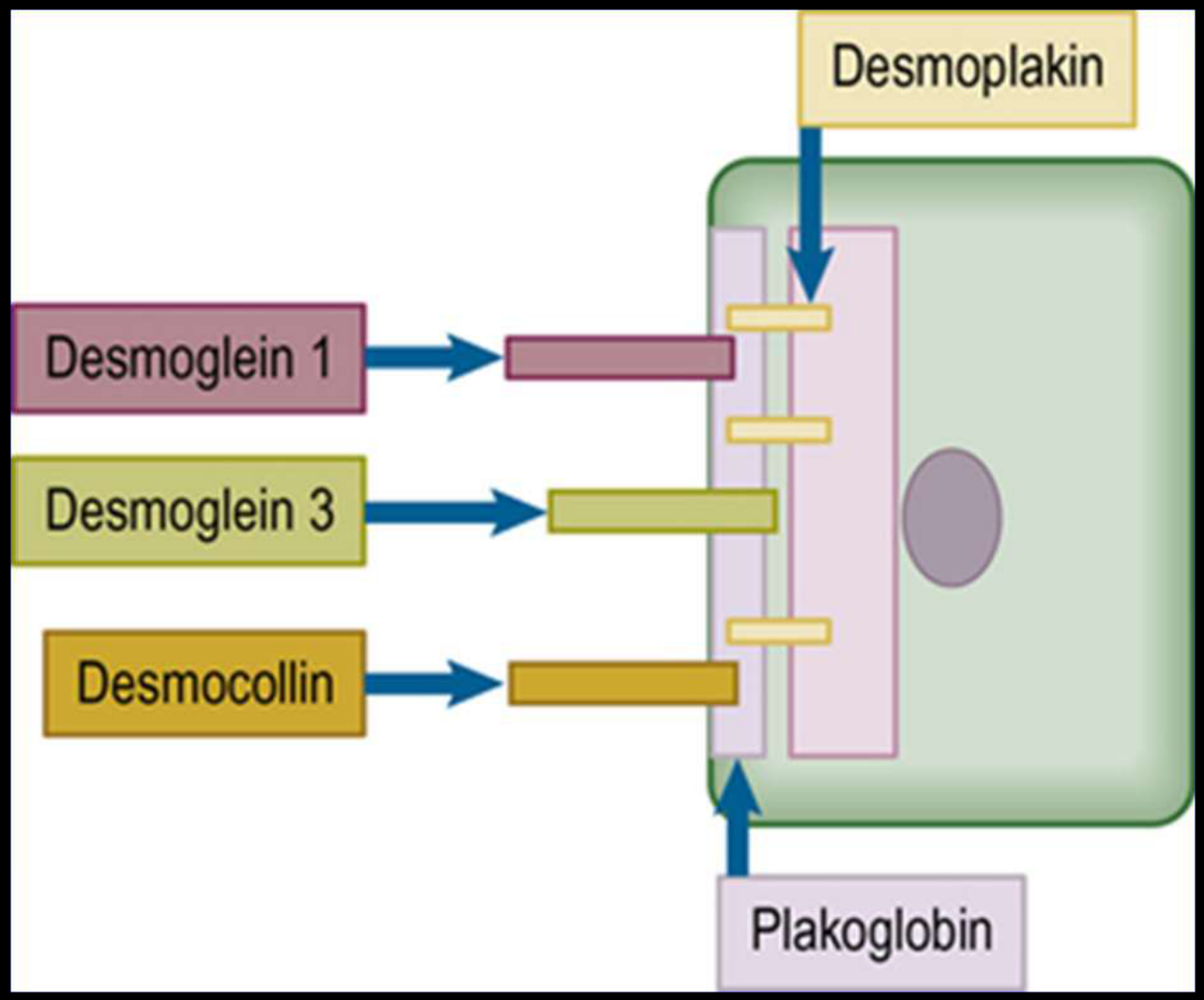
Desmosomal Components and Autoantibodies42
- Desmoglein 1
- Desmoglein 3
- Desmocollin
- Desmoplakin
- Plakoglobin
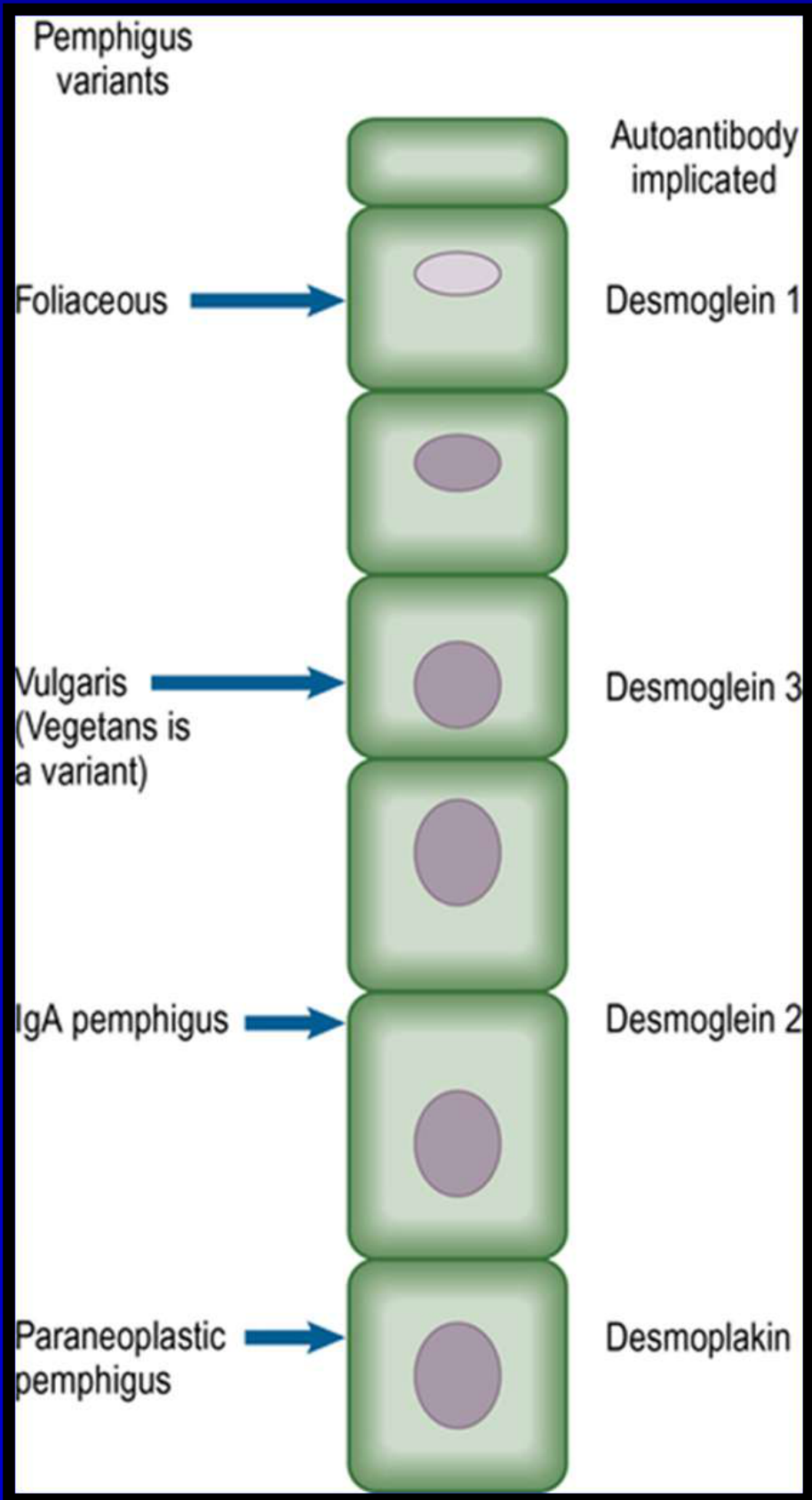
Pemphigus Variants and Implicated Autoantibodies43
- Foliaceous: Desmoglein 1
- Vulgaris (Vegetans is a variant): Desmoglein 3
- IgA pemphigus: Desmoglein 2
- Paraneoplastic pemphigus: Desmoplakin
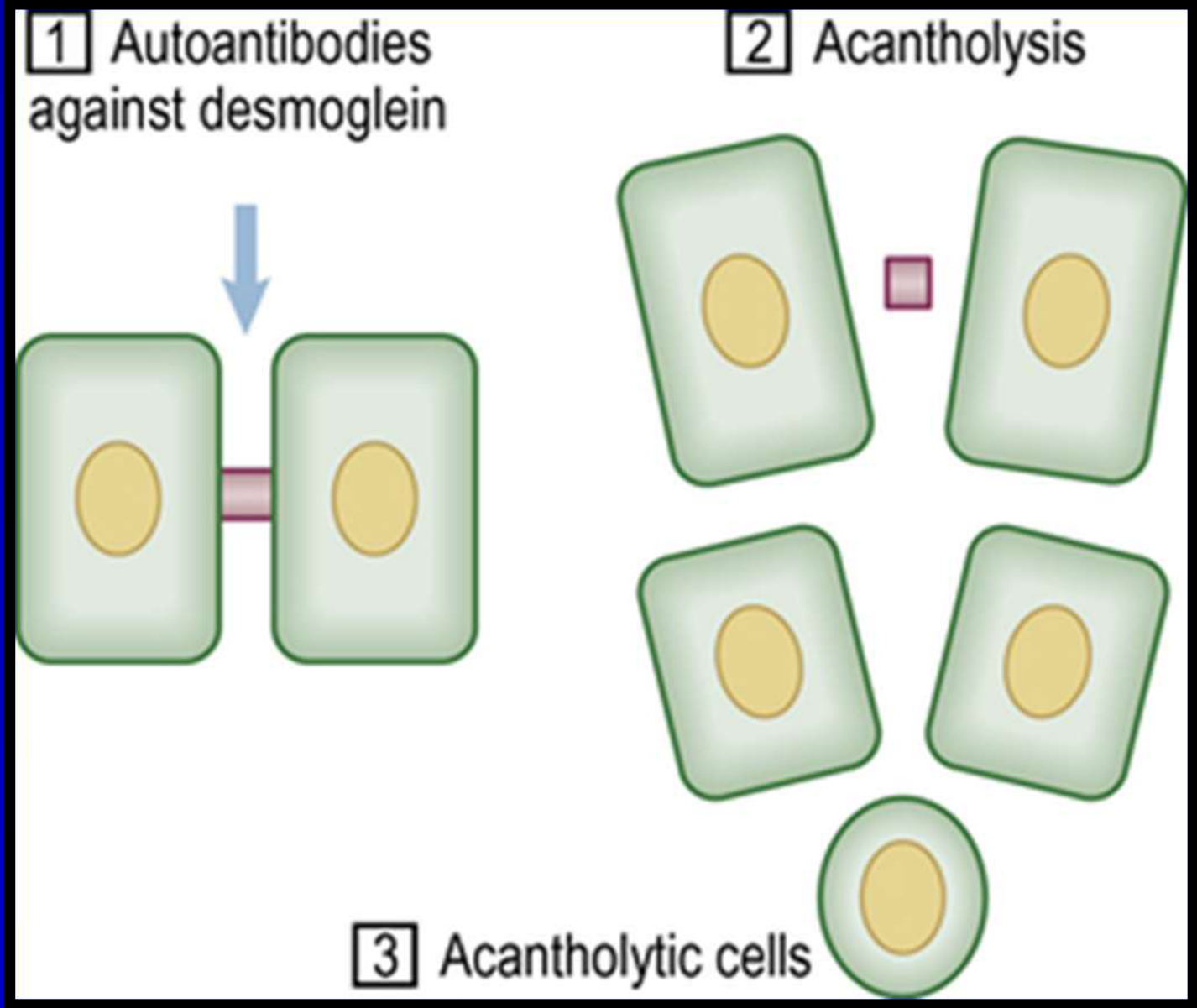
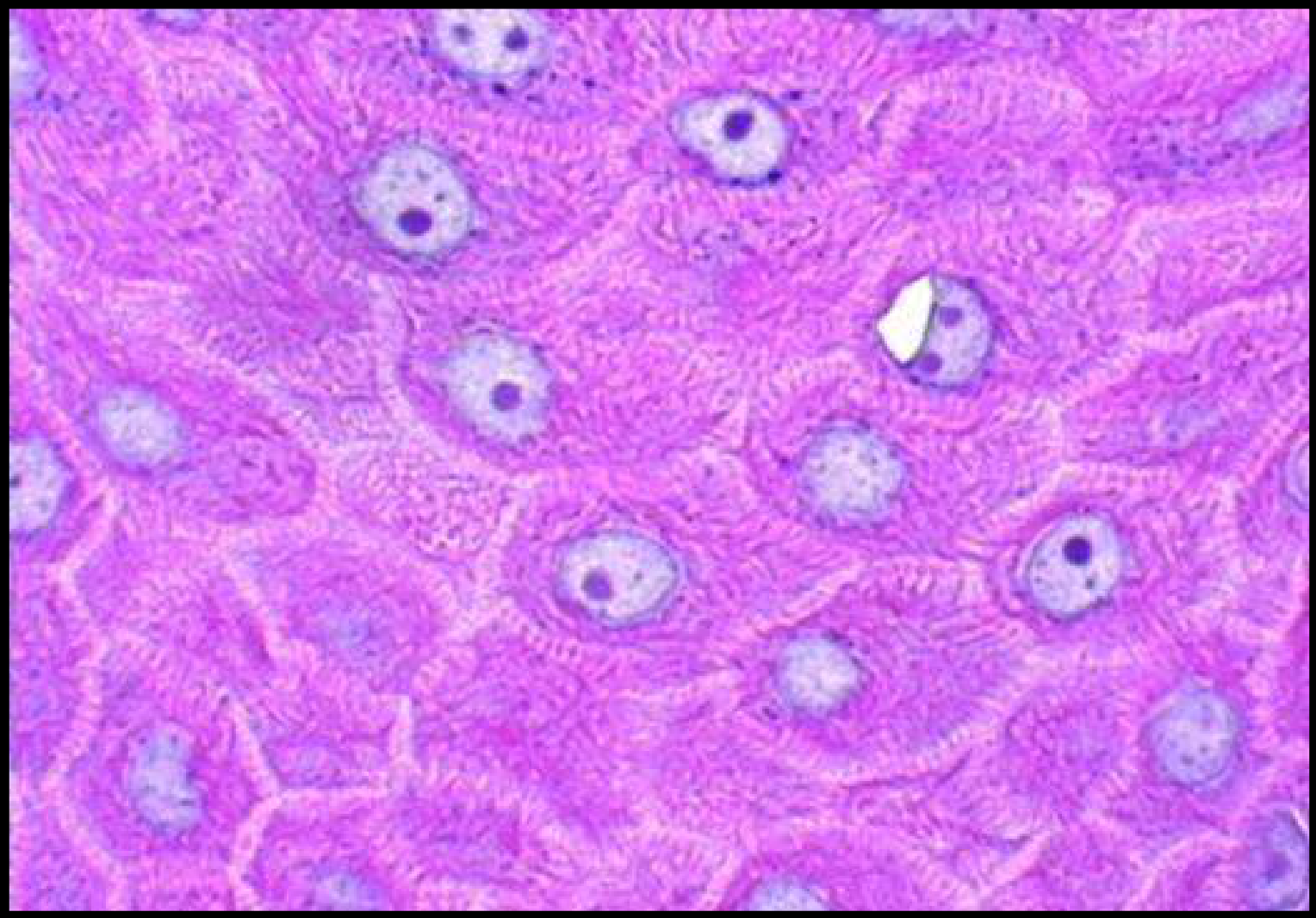
Pathological Process
- Autoantibodies against desmoglein
- Acantholysis
- Acantholytic cells
- Results in intraepithelial clefting and blistering
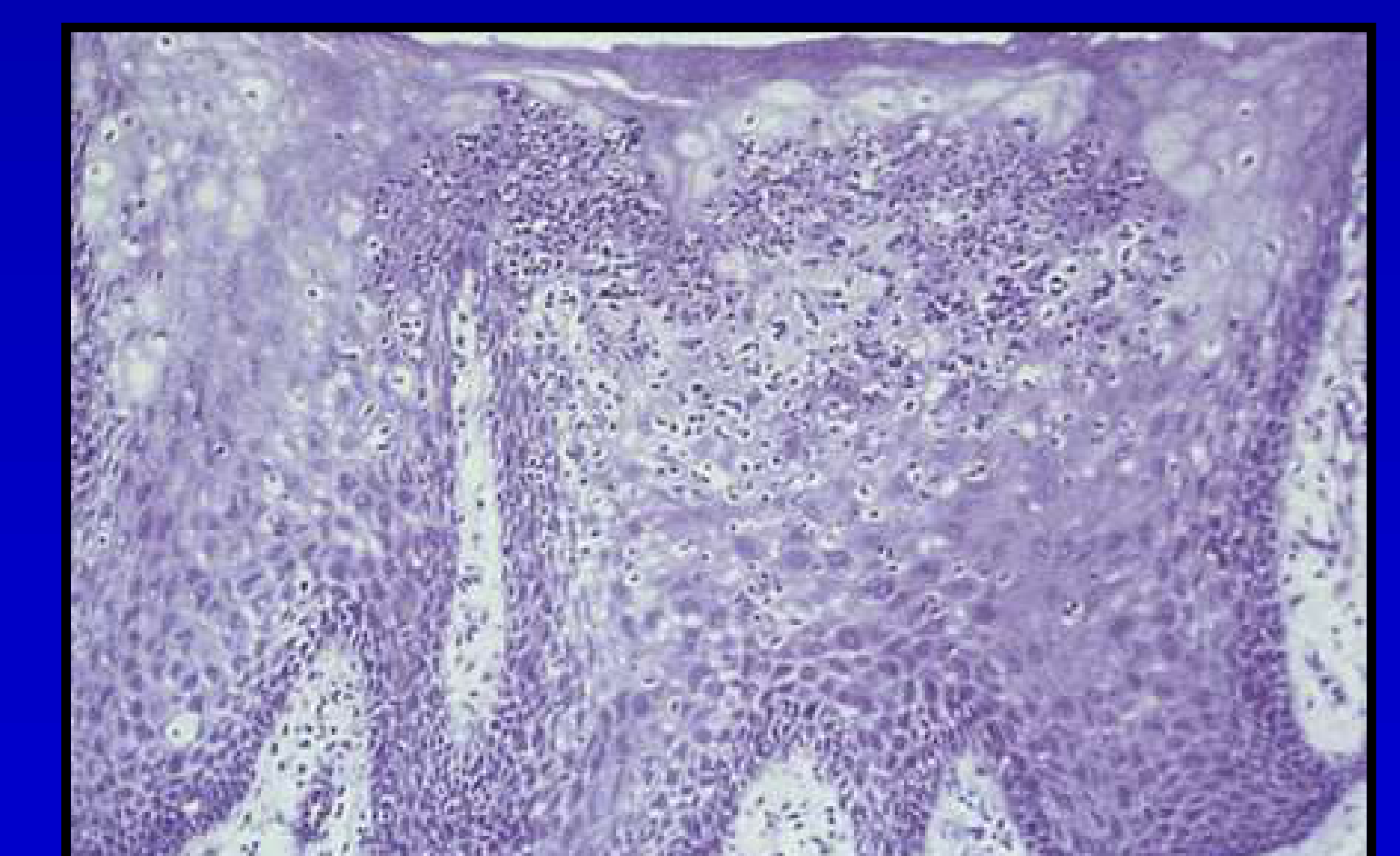
Histopathology
(Micrograph shows intercellular space enlargement/acantholysis)
 |  |
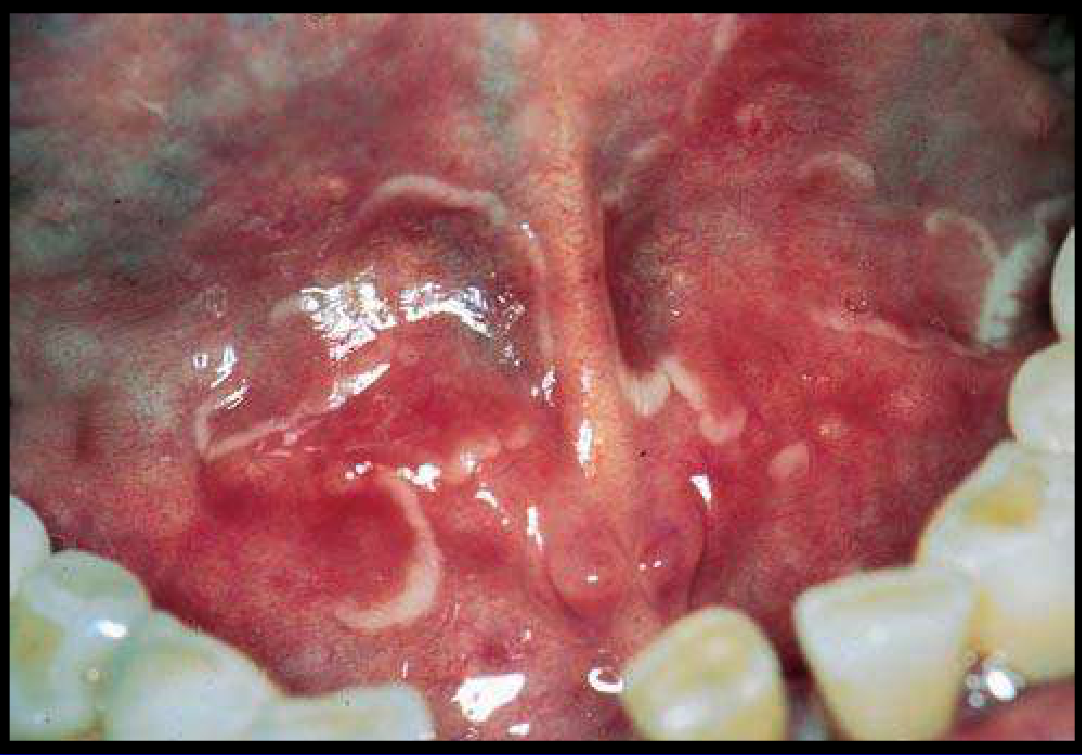
Pemphigus Vulgaris44
 |  |
Clinical Features4546
- Most severe form
- Middle-aged and older individuals
- Females > Males
- Individuals of Ashkenazi, Asian, or Mediterranean descent
- Genetic and other predisposing factors
- Oral and skin lesions
==* Involvement: Skin and mucosal sites (oral, pharyngeal, laryngeal, oesophageal, nasal, conjunctiva, anogenital).==
==* Drug reaction: Can occur as a drug reaction (e.g., ACE inhibitors).==
==* Severity: Severe cutaneous involvement can be life-threatening; early recognition is vital.==
 |  |
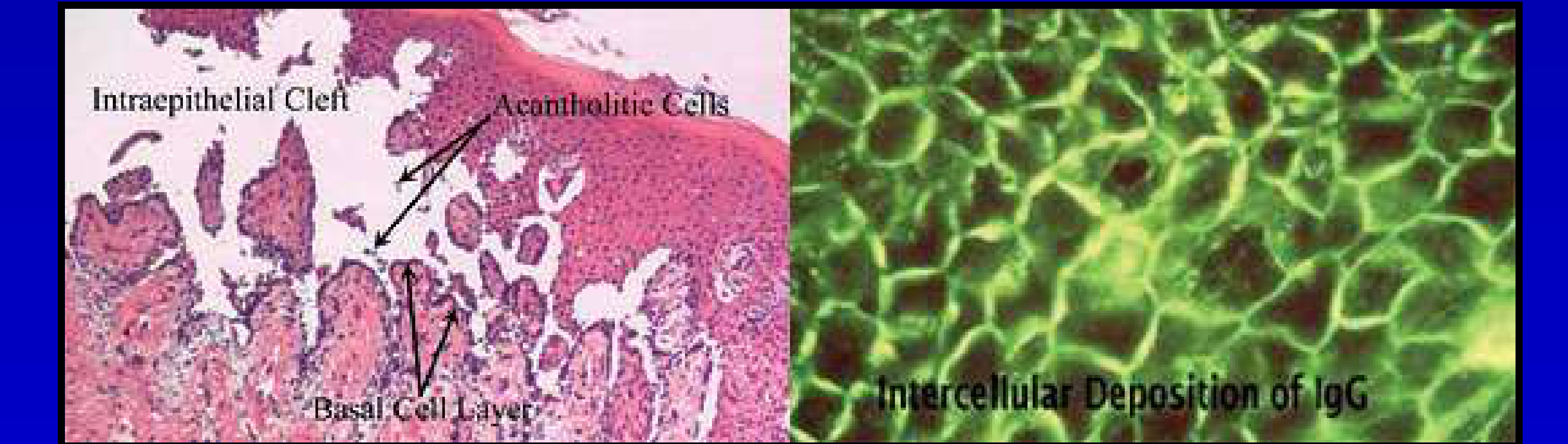
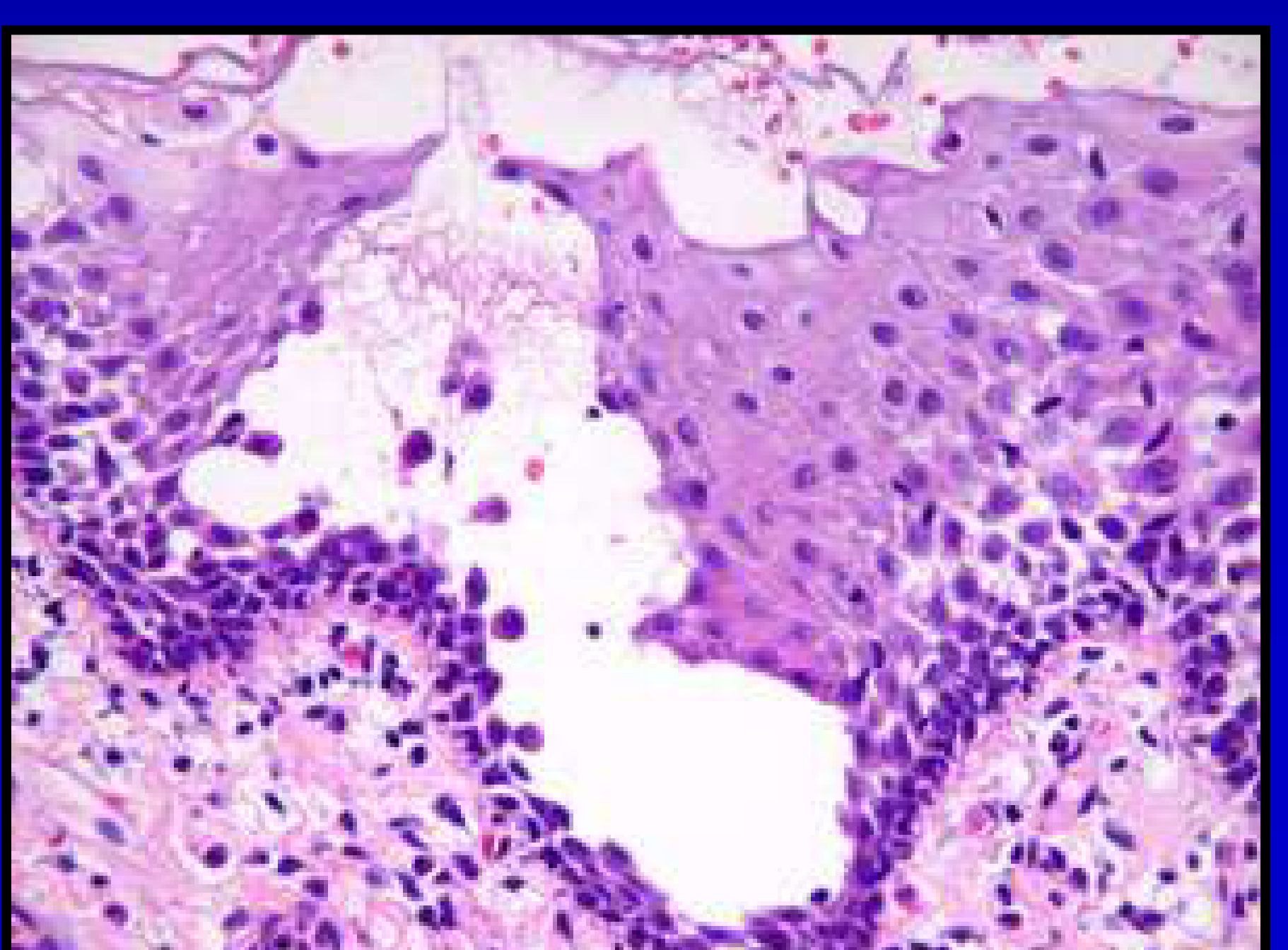
Histopathology4748
- Intraepithelial Cleft
- Acantholytic Cells
- Basal Cell Layer involvement
- Intercellular Deposition of IgG in a “chicken-wire” pattern (Direct Immunofluorescence)
 |  |
Differential Diagnosis49
- Paraneoplastic pemphigus
- Mucous membrane pemphigoid
- Erythema multiforme
- Oral lichen planus
- C
Treatment50
orticosteroids
- Steroid-sparing immuno-suppressants:
- Azathioprine
- Dapsone
- Mycophenolate
- Cyclophosphamide
- Rituximab
Pemphigoid51
Aetiology and Pathogenesis52
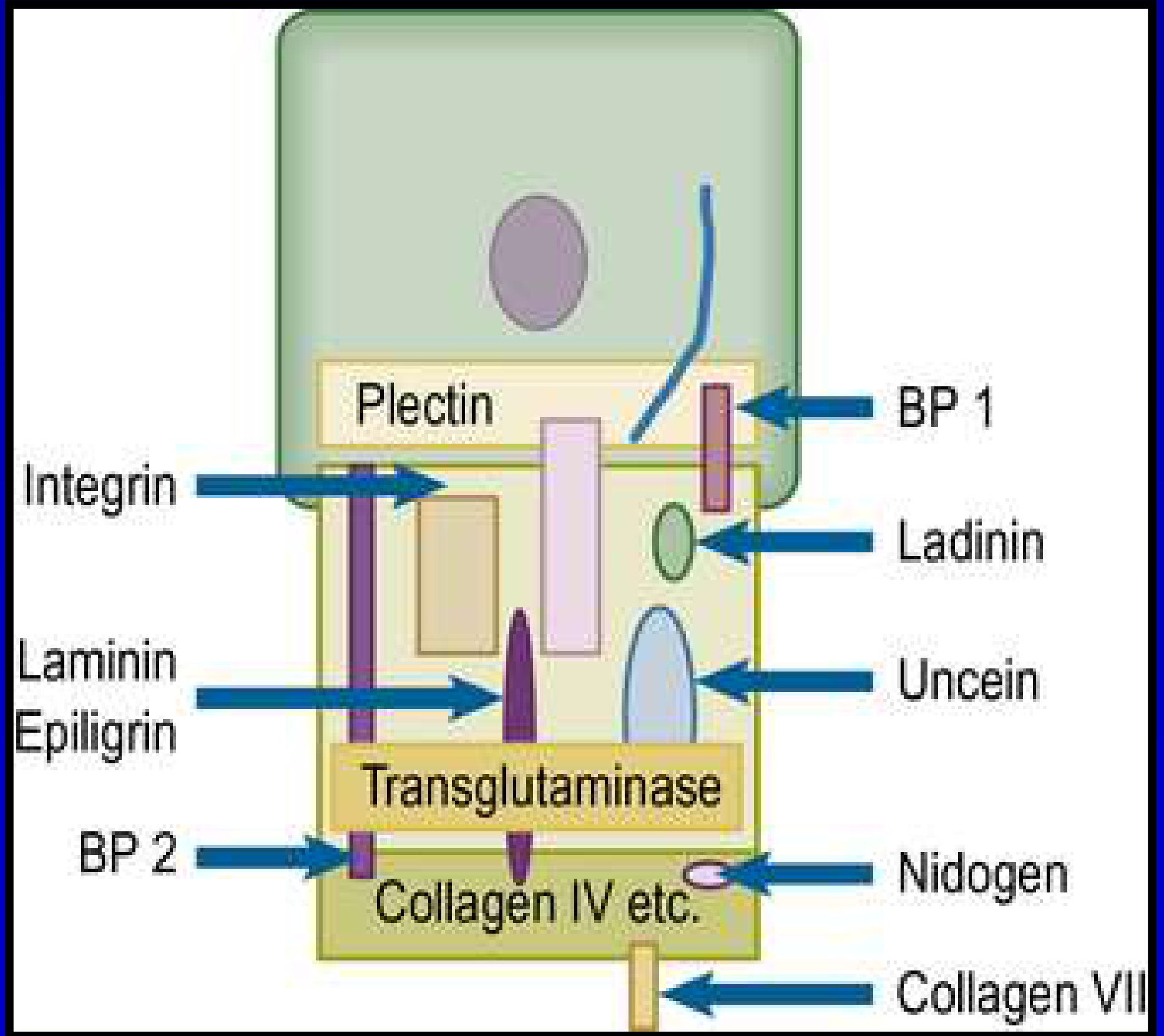
- Group of sub-epithelial immunologically mediated vesiculobullous disorders
- Affects stratified squamous epithelium
- Characterised by damage to protein constituents of the Basement Membrane Zone (BMZ) anchoring filament components
- Specific targets include integrin, laminin, and BP antigen
Mucous Membrane Pemphigoid
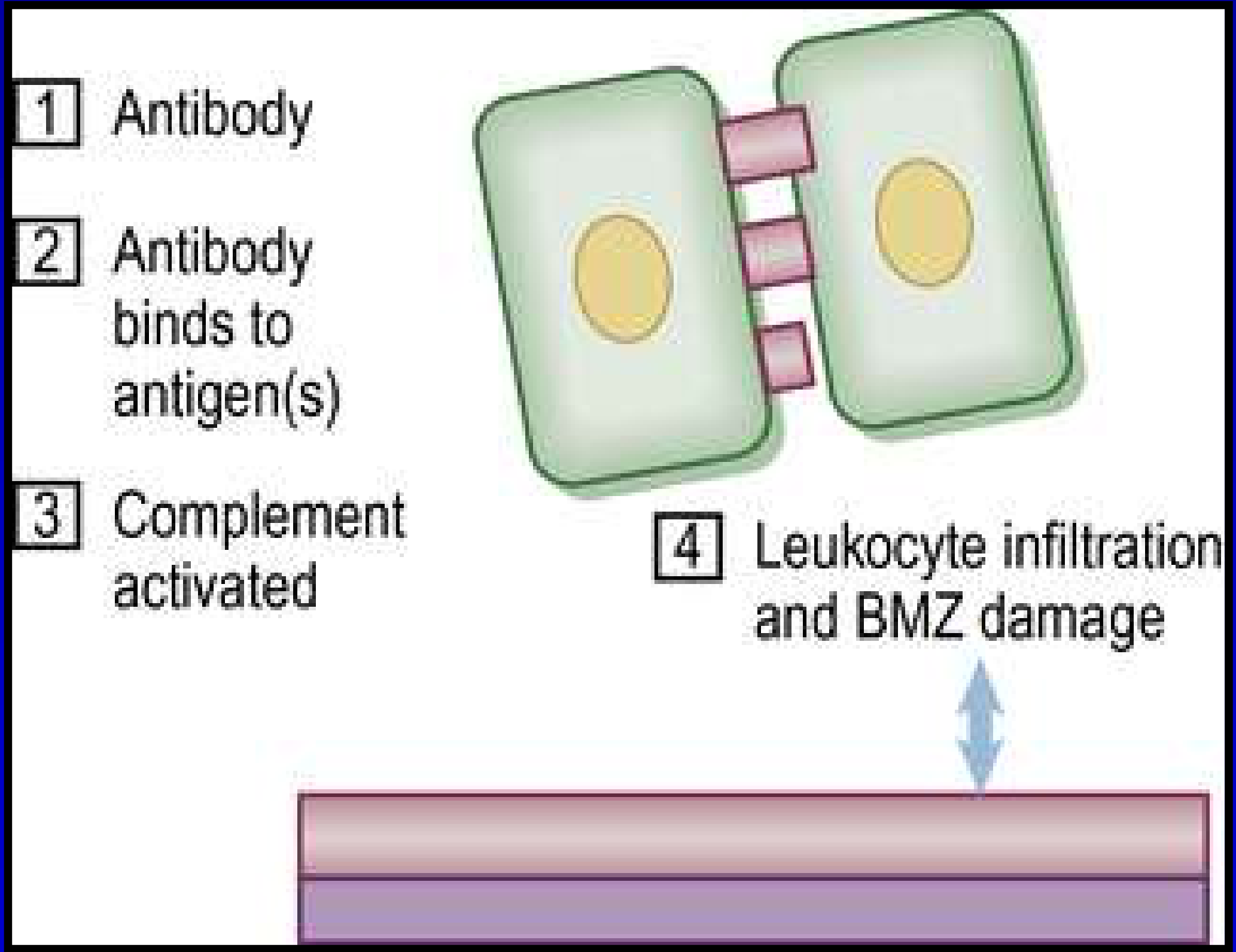
Pathogenesis Sequence53
- Antibody production
- Antibody binds to antigen(s)
- Complement activated
- Leukocyte infiltration and BMZ damage
Clinical Features5455
- Females > Males
- 5th–6th decade
- No known geographic incidence
- Genetic predisposition
- May be drug-induced
- Extra-oral involvement: ocular, laryngeal, nasal, genital, skin
- Associated medications include furosemide and NSAIDs
- Presentation often involves ulcers and erosions rather than blisters
 |  |  |
 |  |
Extra and intraoral Manifestations56
- Ocular involvement (conjunctival inflammation/lesions)
- Skin erosions and ulcerations
- Approximately 20% of patients develop ocular manifestations
- Untreated ocular involvement can lead to blindness
- Ophthalmological consultation required for all diagnosed patients
Case Examples
- Oral: Mucous membrane pemphigoid affecting oral mucosa (blisters, ulcers, erosions)
- Ocular: Photographs demonstrated ocular involvement (risk of blindness)
- Skin: Photographs demonstrated skin involvement
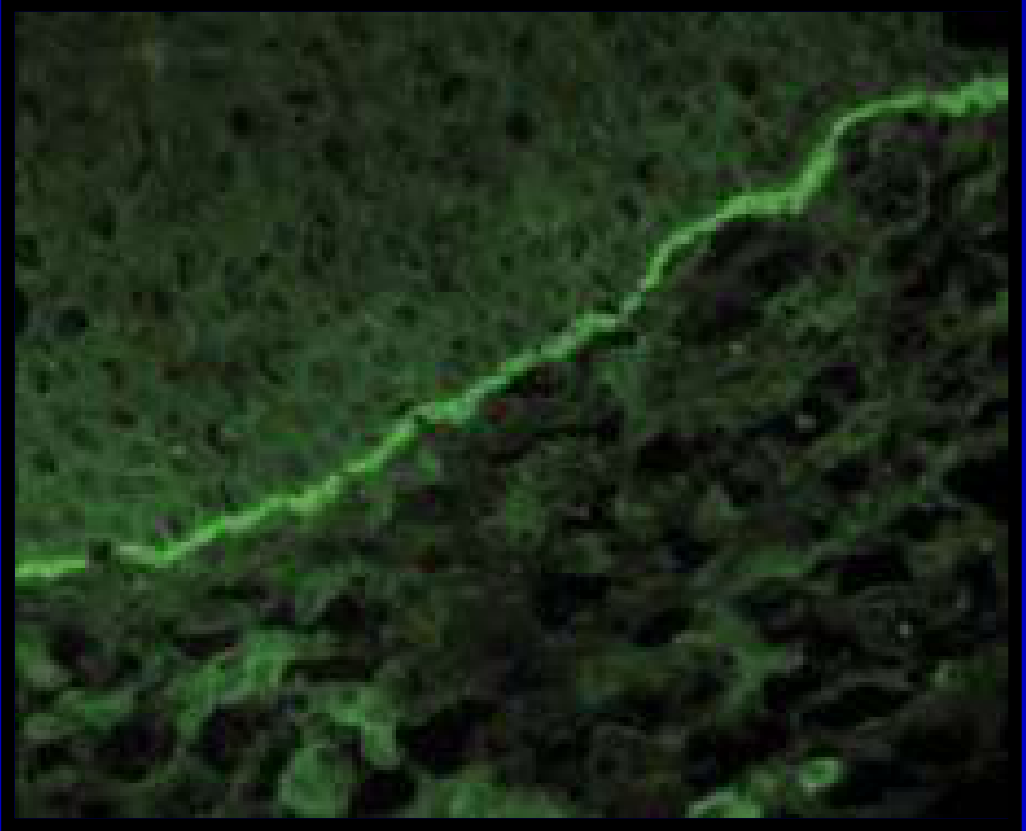
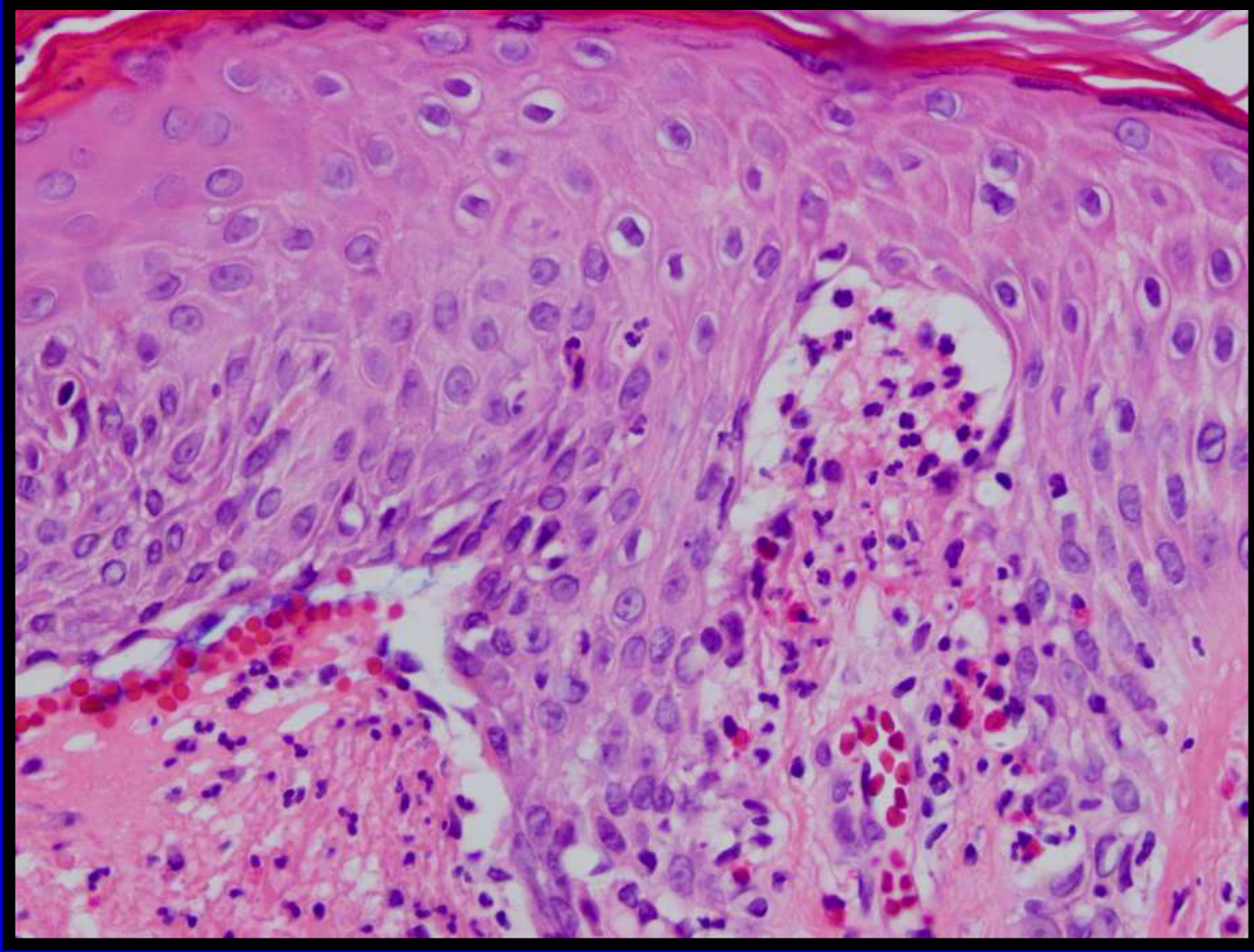
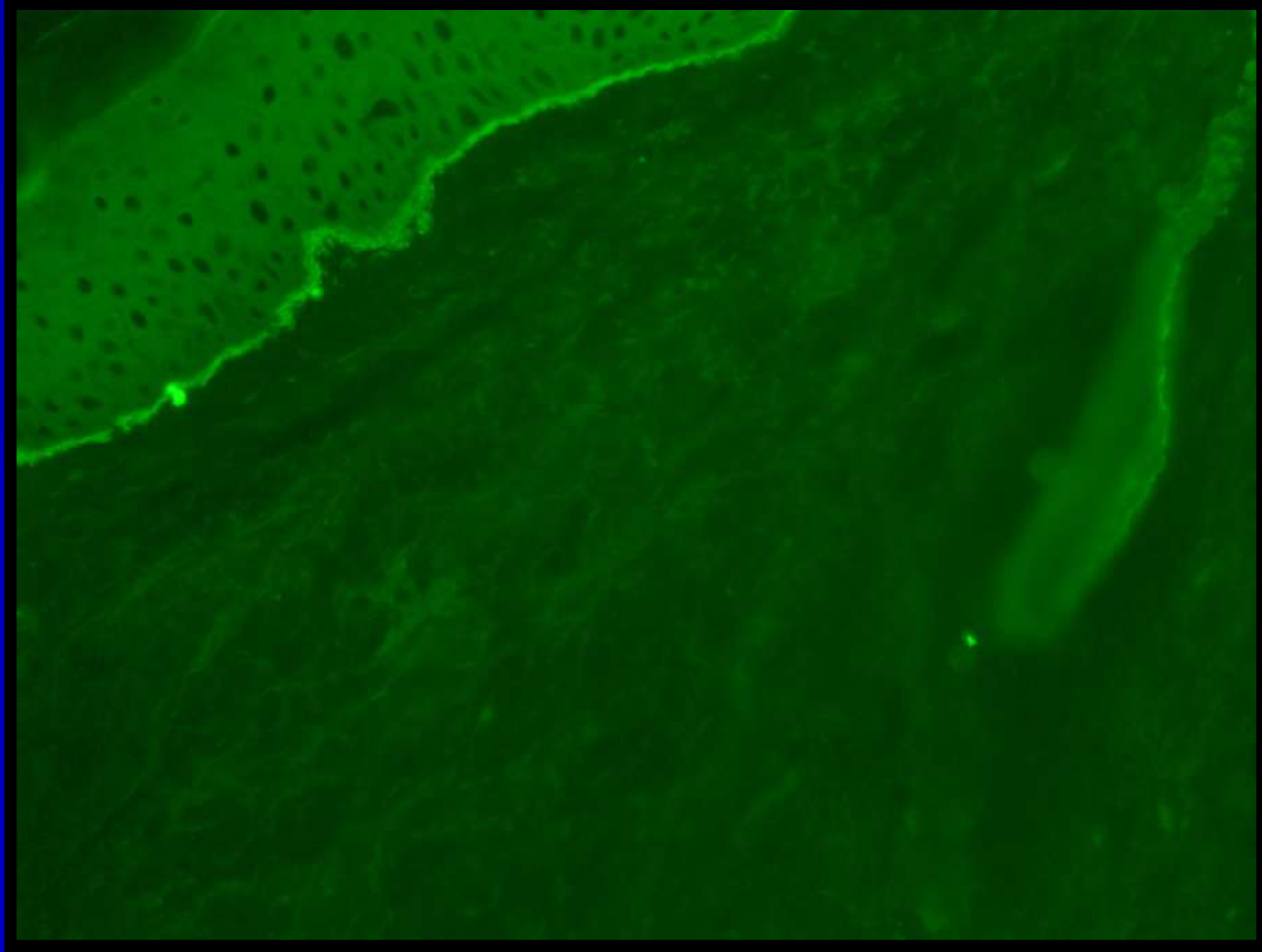
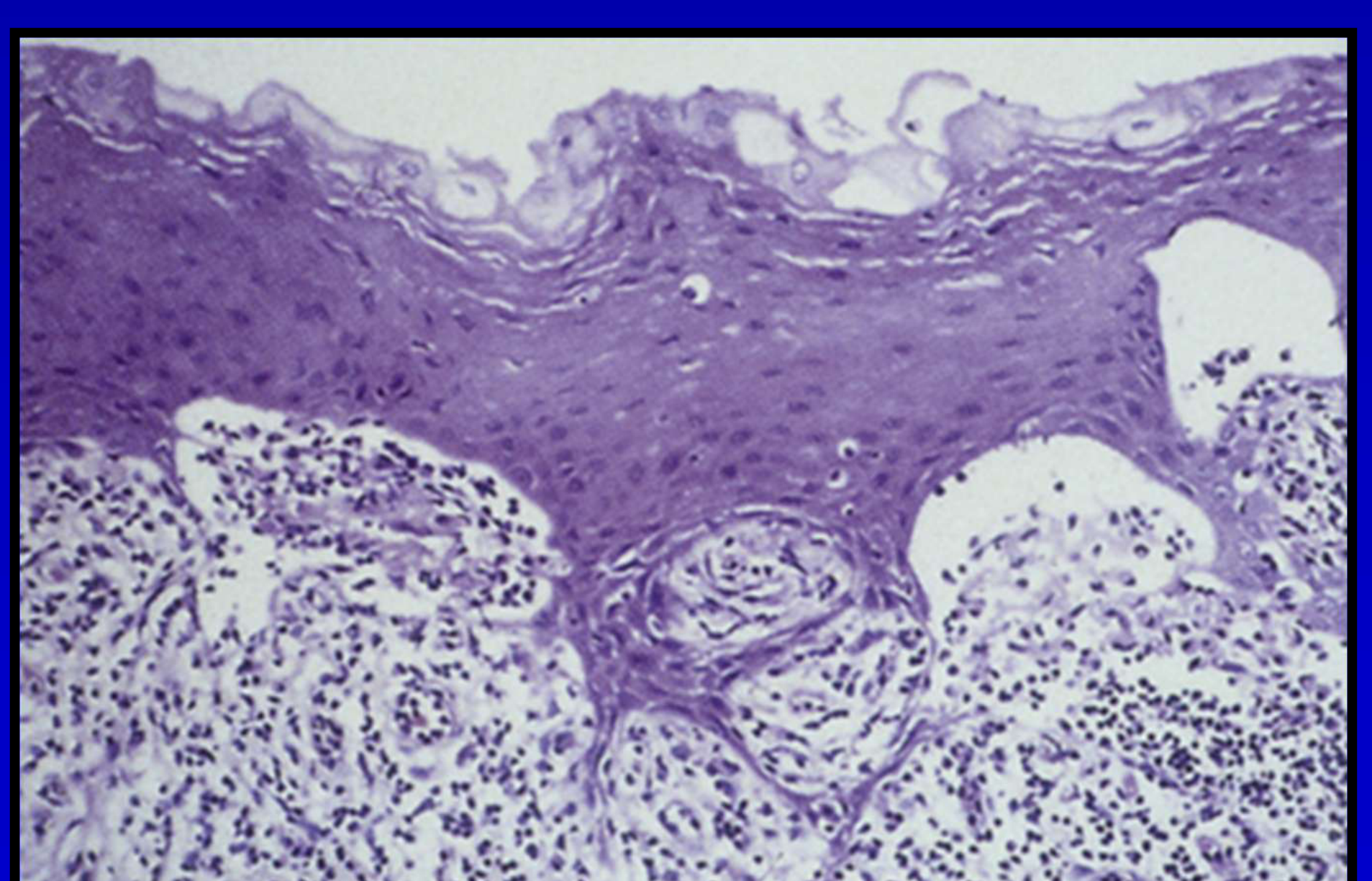
Histopathology57
H&E: Epithelial tissue separation from the underlying connective tissue with inflammatory infiltrate
- Direct Immunofluorescence: Linear pattern of immune deposits along the basement membrane zone
- Direct immunofluorescence shows linear deposition of IgG and C3
 |  |
Differential Diagnosis58
- Oral lichen planus
- Pemphigus
- Angina bullosa haemorrhagica
- Dermatitis herpetiformis
- Linear IgA disease
- Erythema multiforme

Treatment59
- Corticosteroids
- Steroid-sparing immuno-suppressants
- Rituximab
Linear IgA Disease
- Chronic autoimmune disease of the skin that commonly affects the mucous membranes, including the gingiva
- Autoantibodies to BP180 (collagen XVII)
Aetiology and Pathogenesis60
==* Characterized by the production of antibodies against Collagen 17.==
Clinical Features61
- Skin lesions: May be urticarial, annular, targetoid, or bullous
- Oral lesions: Ulcerative (preceded by bullae) or erosive
 |  |
Histopathology62
==* Separation: At the basement membrane zone.==
==* Clefts: Contain eosinophils and polymorphs.==
==* Direct immunofluorescence: Linear deposition of IgA at the epithelium–connective tissue interface.==
 |  |
Differential Diagnosis63
- Oral lichen planus
- Mucous membrane pemphigoid
- Pemphigus vulgaris
- Chronic ulcerative stomatitis
Treatment64
- Topical / systemic corticosteroids
- Other immunosuppressive agents may be used in more severe or refractory cases ==* Other agents (severe/refractory): Dapsone, cyclosporine, or other immunosuppressive agents.==
Erythema Multiforme65
- Acute, often recurrent, non-immediate allergic hypersensitivity reaction affecting mucocutaneous tissues
- Characterised by:
- Serosanguinous exudates on the lips
- Mucosal ulceration
- Target-like lesions on the skin
 |  |  |
Aetiology and Pathogenesis66
Note: Stevens-Johnson syndrome / toxic epidermal necrolysis are related conditions.
==* Extent: In most cases, affects oral mucosa only; severe acute reactions can be potentially life-threatening.==

Potential Triggers67
==* Infections: e.g., Herpes Simplex Virus (HSV).==
==* Medications: e.g., NSAIDs, anticonvulsants.==
==* Vaccines: e.g., Hepatitis B vaccine.==
==* Others: Food additives, chemicals (e.g., benzoates), radiation therapy.==
Immunological Mechanism68
-
Presentation of antigens to T lymphocytes initiates the immune reaction
-
Effector cells: CD8+ T-cells, Macrophages, and PMNL
-
Peak incidence: 20–40 years
-
Males > Females
-
Worldwide occurrence
-
Genetic predisposition
Clinical Features69
==* Presentation: Intraoral, lip, and skin involvement.==
Histopathology70
==* Epithelium: Hyperplasia and spongiosis.==
==* Vesicles: At the epithelium–connective tissue interface.==
==* Necrosis: Epithelial necrosis present.==
==* Connective tissue: Inflammatory infiltrate containing lymphocytes and macrophages.==
Differential Diagnosis71
- Herpes Simplex Virus (HSV)
- Aphthous ulcers
- Pemphigus vulgaris
- Mucous membrane pemphigoid
- Oral lichen planus
Treatment72
- Corticosteroids
- May require hospitalization
- Avoid triggers

Chronic Ulcerative Stomatitis
Aetiology and Pathogenesis73
- Rare immune-mediated mucocutaneous disorder that produces desquamation and ulceration of oral mucosa
Clinical Features7475
-
Resembles other mucocutaneous conditions
-
Very similar in presentation to oral lichen planus.
-
Usually affects older white women
-
Tongue, buccal mucosa, and gingiva are usually affected
Case Examples: Clinical Photographs
- Presentation: Lesions resembling oral lichen planus.
- Observation: Visual resemblance makes clinical differentiation difficult without immunofluorescence.


Histopathology76
- H&E: Resembles Oral Lichen Planus (OLP)
- Direct Immunofluorescence (DI): Perinuclear deposits of IgG in the basal layer and lower 1/3 of epithelial layers
Differential Diagnosis77
- Oral lichen planus
- Mucous membrane pemphigoid
- Linear IgA disease
- Pemphigus vulgaris

Treatment78
- Hydroxychloroquine
- Does not tend to respond well to corticosteroids (in contrast to other immune-mediated mucocutaneous disorders).
- Treatment of Choice: Hydroxychloroquine.

Lupus Erythematosus7980
- Autoimmune disease involving both humoral and cell-mediated arms of the immune system
- Antibodies directed against various cellular antigens in the nucleus and the cytoplasm
 |  |  |
 |  |
Aetiology and Pathogenesis81
Occurs in three forms:
- Systemic (Acute): Impacts many organ systems
- Discoid (Chronic): Less aggressive, predominantly affects skin
- Subacute (Intermediate)
Clinical Features82
 |  |
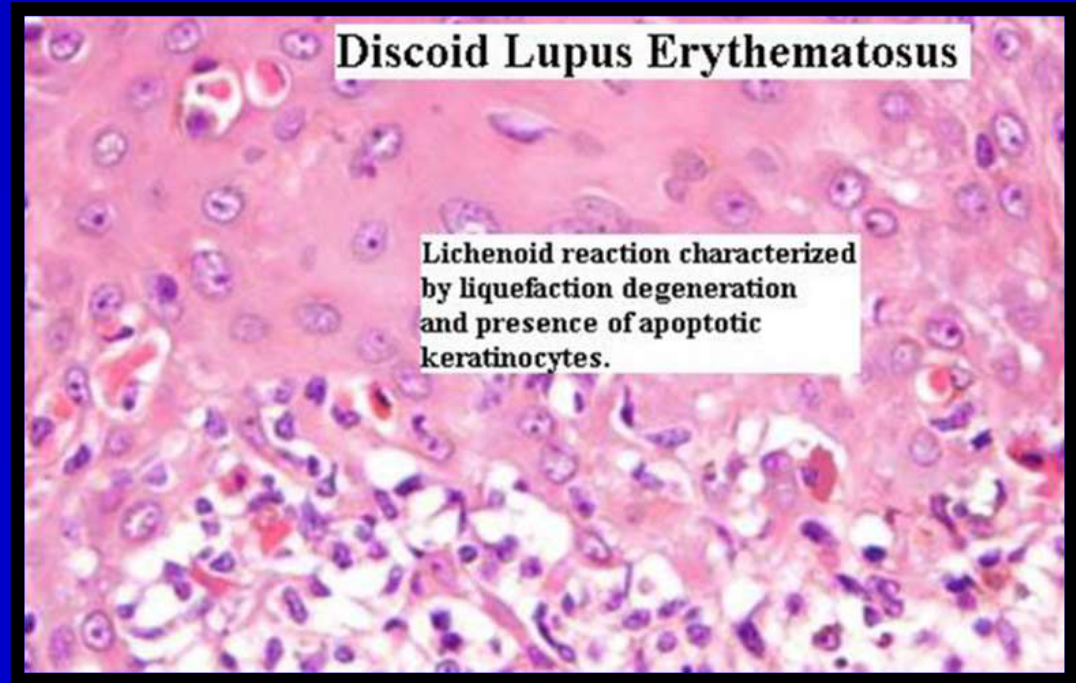
Discoid Lupus Erythematosus (DLE)83
- Females > Males
- Skin lesions are disk-shaped erythematous plaques with hyper-pigmented margins
- Similar appearance to OLP
(Page contains title only)
Systemic Lupus Erythematosus (SLE)84
-
Skin and mucosal lesions are mild
-
Multiple organ involvement
-
Serologic tests positive for autoantibodies:
- ANA (Antinuclear Antibody)
- Other specific markers
-
Skin: May result in the classic "butterfly rash"
-
Systemic Symptoms: Fever, weight loss, malaise
-
Organ Involvement: Joints, kidney, heart, lungs
- Kidney: Most important involvement; responsible for significant morbidity and mortality
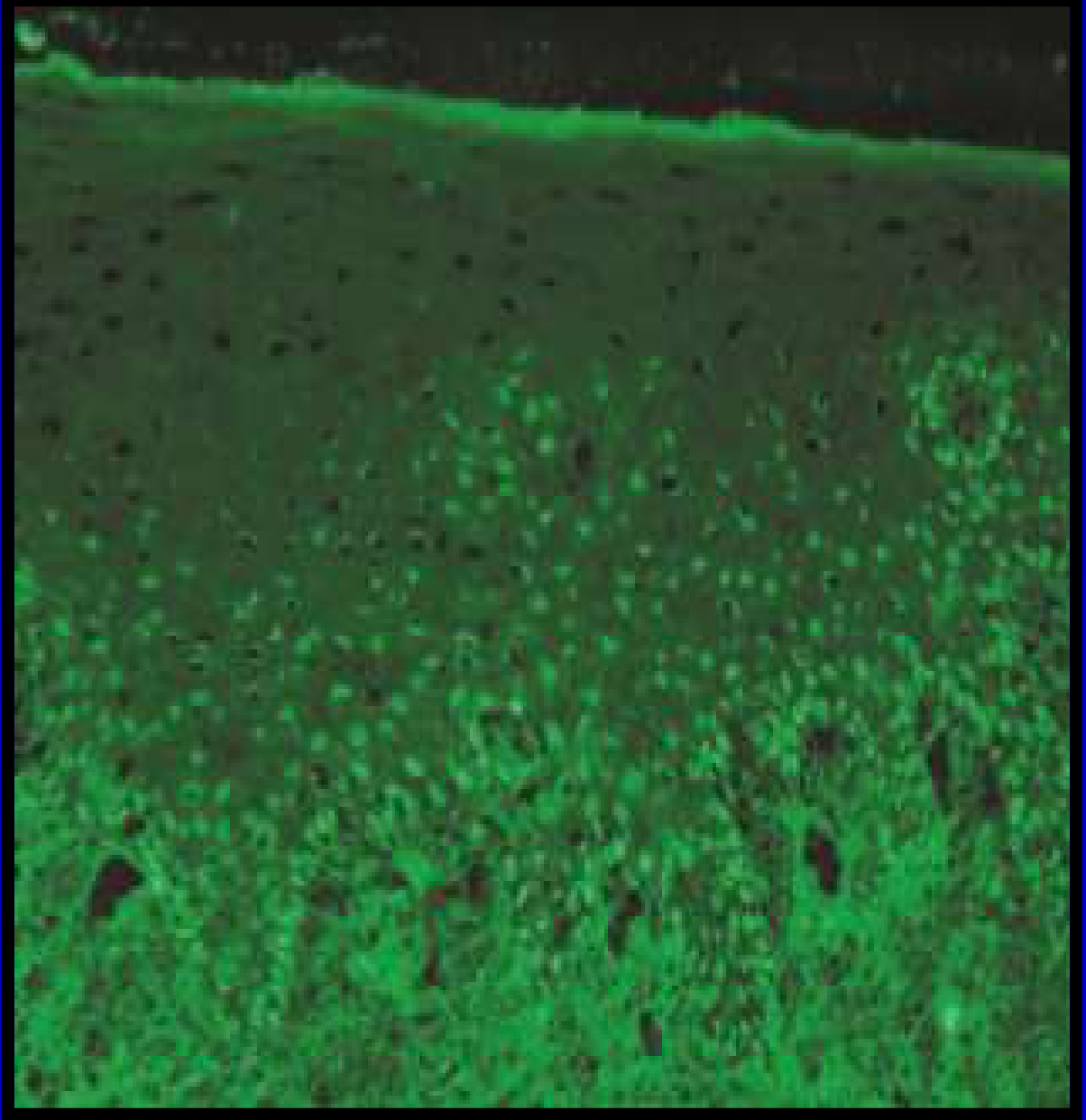
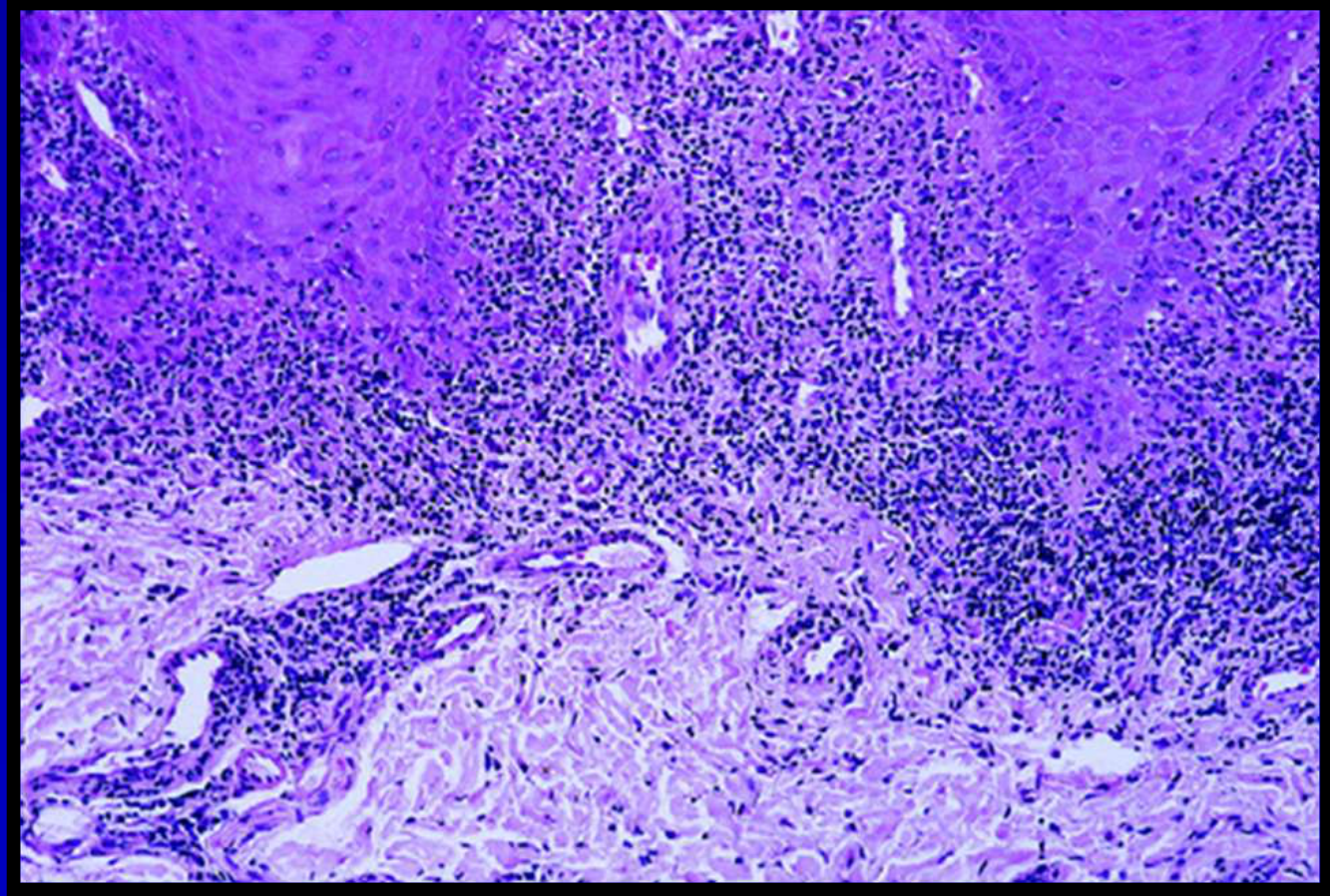
Histopathology85
- Basal cell destruction
- Hyperkeratosis
- Epithelial atrophy
- Lymphocytic infiltration
- Vascular dilation and oedema
Direct Immunofluorescence
Shows granular linear deposits of immunoglobulins and complement C3
 |  |
Differential Diagnosis86
- Oral lichen planus
- Mucous membrane pemphigoid
- Pemphigus vulgaris
- Erythematous candidiasis
- Contact hypersensitivity

Treatment87
-
Topical and systemic corticosteroids
-
Other immunosuppressive agents
-
Skin: Taut, smooth appearance.
-
Organ fibrosis (lungs, heart, kidney, GI tract) leads to organ failure and death

Systemic Sclerosis88
 |  |  |
Aetiology and Pathogenesis89
- Rare immunologically mediated disease
- Dense collagen is deposited in the tissues of the body
Clinical Features90
- Most patients are adults
- Females > Males
- Raynaud’s phenomenon
- Diffuse, hard skin texture
- Multi-organ involvement
 |  |
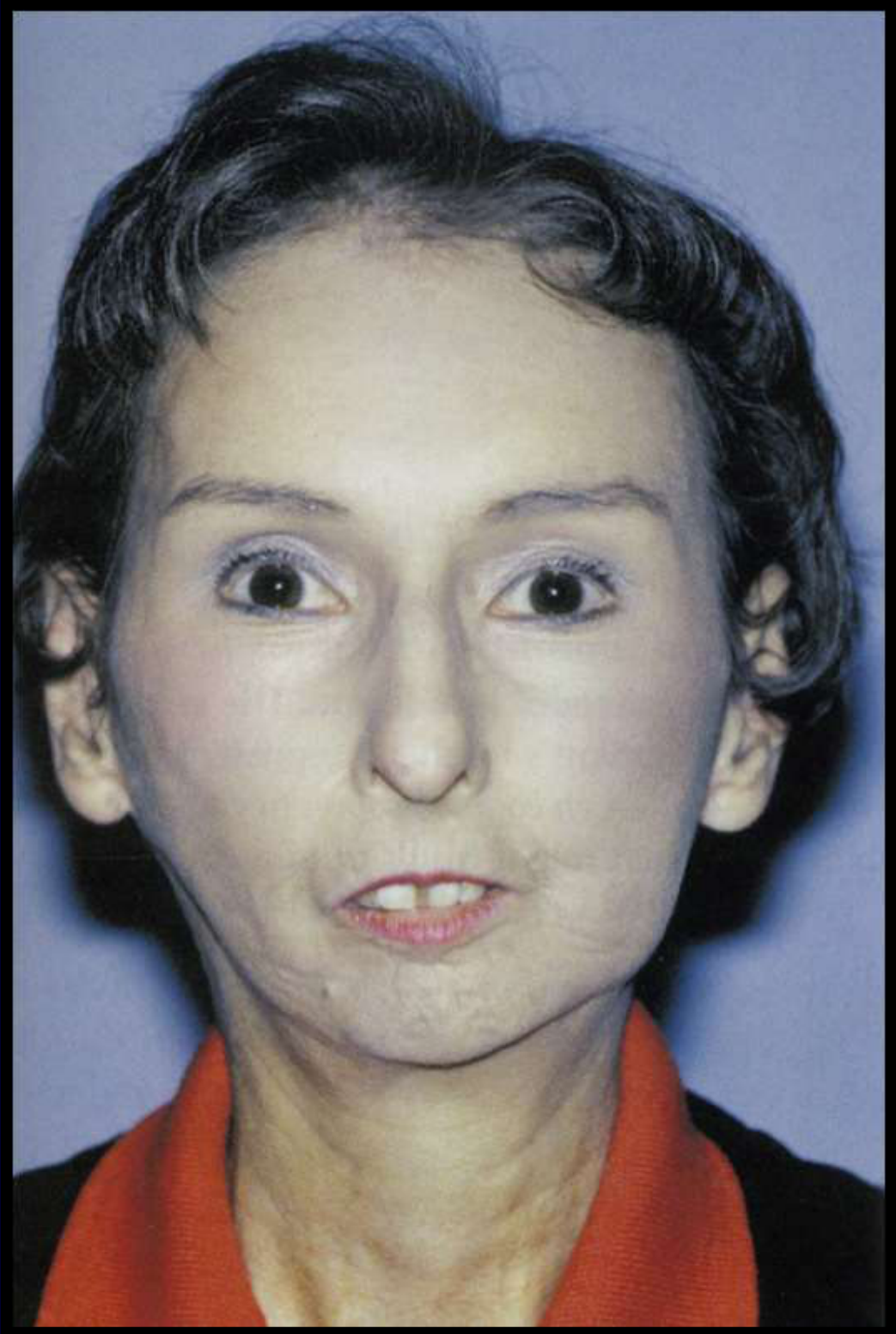
Oral Manifestations91
- Microstomia
- Dysphagia
- Xerostomia
- Widening of the PDL space
Case Examples
- Skin: Photographs showed smooth and taut skin.
- Oral: Photograph demonstrated microstomia. Oral hygiene difficult; complicates dental treatment.
- Radiographic: OPG showed widening of PDL spaces.
Histopathology92
- Diffuse deposition of collagen within and around normal structures
- Abnormal collagen replaces and destroys normal tissue, leading to loss of normal function
Treatment93
- No effective treatment.
- Corticosteroids also have limited success.
- Various systemic agents have been trialed with limited success
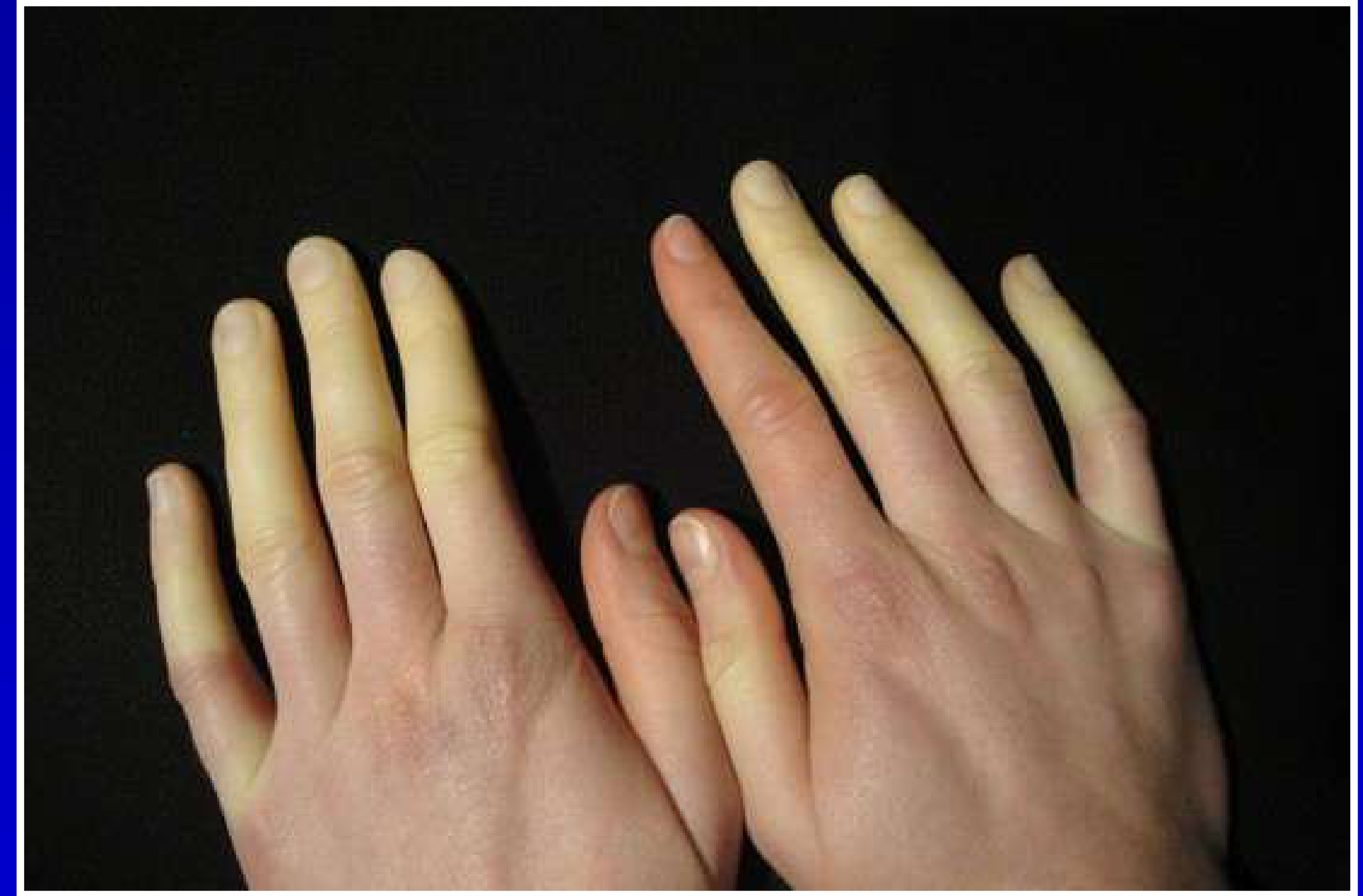
CREST Syndrome949596
Uncommon condition that is a mild variant of systemic sclerosis, defined by the acronym:
- ==Demographics: Tends to affect women, predominantly older women==.
 |  |  |
 |  |  |
Aetiology and Pathogenesis97
- C: Calcinosis cutis
- R: Raynaud’s phenomenon
- E: Esophageal dysfunction
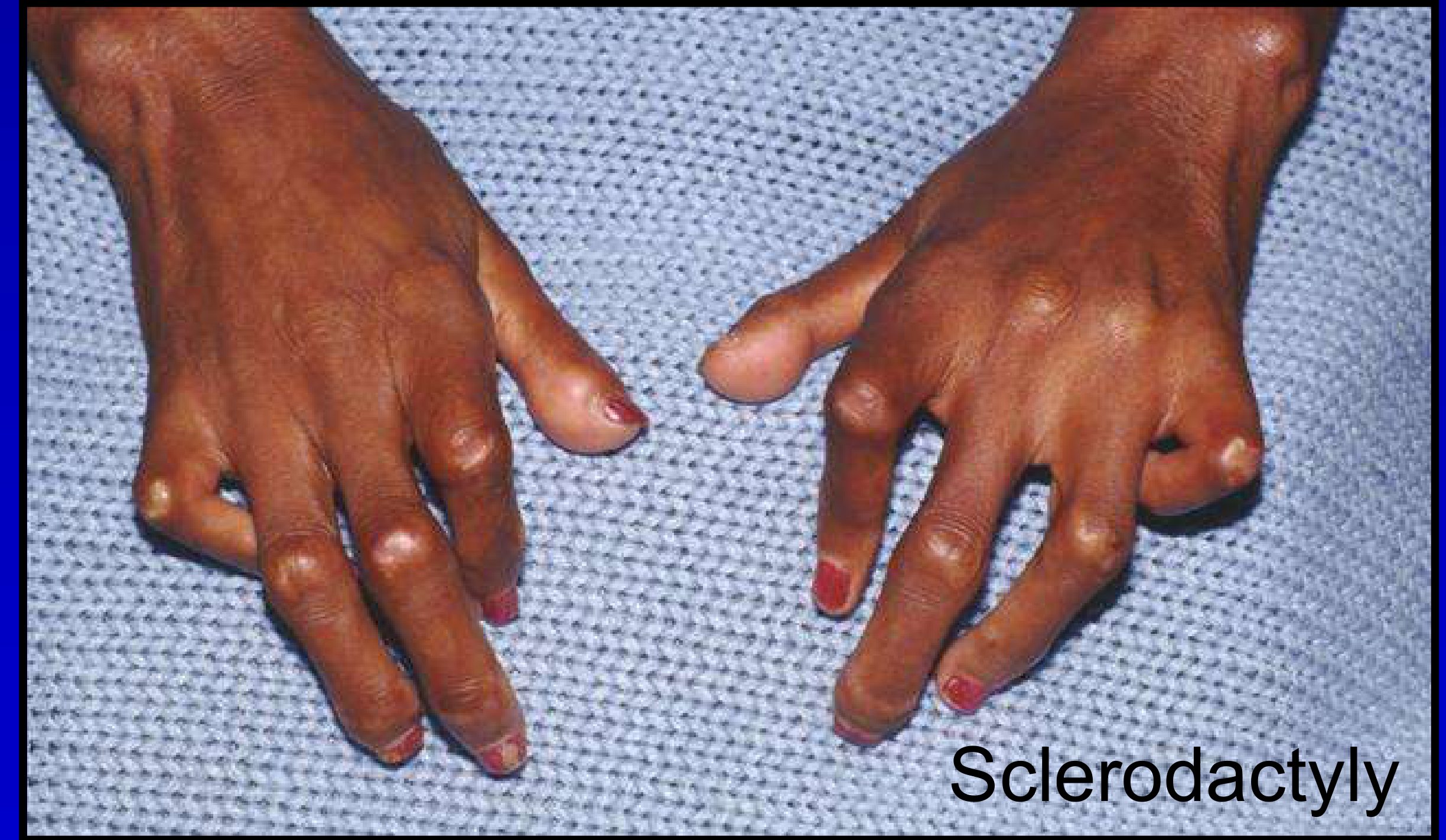
- S: Sclerodactyly
- T: Telangiectasia
Sclerodactyly98
-
Fingers become stiff with a smooth, shiny appearance.
-
May undergo permanent flexion resulting in claw-like deformity.
-
Similar to systemic sclerosis
-
Presence of telangiectatic vessels
Histopathology99
- Hereditary haemorrhagic telangiectasia
- Diagnosis supported by anti-centromere antibodies
- Histopathology is basically very similar to systemic sclerosis.
Differential Diagnosis100
- ==Hereditary Haemorrhagic Telangiectasia is a key differential diagnosis==.
Treatment101
- Treatment protocols are the same as for systemic sclerosis
- Treatment options are very limited.
- ==Prognosis: Much better than for systemic sclerosis==.
Manifestations of CREST Syndrome
- ==Calcinosis Cutis: Images showed dystrophic calcification==.
- ==Raynaud’s Phenomenon: Vasoconstrictive event triggered by stress or cold==.
- ==Sclerodactyly: Stiff fingers with smooth, shiny skin==.
- ==Telangiectasia: Superficial dilated capillaries; facial skin and lips commonly affected==.
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Pemphigus Vulgaris
Clinical Features
- Most severe form of pemphigus.
- Involvement: Skin and mucosal sites (oral, pharyngeal, laryngeal, oesophageal, nasal, conjunctiva, anogenital).
- Demographics: Tends to affect middle-aged and older individuals.
- Predisposition: Female and genetic predisposition.
- Drug Reaction: Can occur as a drug reaction (e.g., ACE inhibitors).
- Severity: Severe cutaneous involvement can be life-threatening; early recognition is vital.
Case Example: Patient with Cutaneous and Oral Involvement
- Presentation: Patient presented with both cutaneous and oral involvement.
- Significance: Highlights the mucocutaneous nature of the disease and the potential severity when skin involvement is present.
Histopathology
- Intraepithelial clefting: Separation of epithelial cells within the epithelium.
- Basal Layer: Remains attached to the basement membrane (“Tombstoning” appearance).
- Direct Immunofluorescence (DIF): Shows intercellular deposition of IgG and C3.
- Microscopy: Separation of epithelial cells and free-floating cells within intraepithelial clefts.
Differential Diagnosis
- Paraneoplastic pemphigus (occurs in context of lymphoproliferative disorders such as lymphoma).
- Mucous membrane pemphigoid.
- Erythema multiforme.
- Oral lichen planus.
Treatment
- Corticosteroids.
- Steroid-sparing immunosuppressants.
- Rituximab.
Linear IgA Disease
Aetiology and Pathogenesis
- An autoimmune skin disease.
- Characterized by the production of antibodies against Collagen 17.
Clinical Features
- Skin Lesions: Tend to be urticarial, annular, targetoid, or bullous.
- Oral Lesions: Tend to be erosive, ulcerative, and preceded by blistering.
Case Example: Skin Presentation
- Presentation: Photograph showed skin presentation characterized by urticarial or bullous lesions.
- Contrast: Oral lesions typically present as erosions or ulcers rather than intact bullae.
Histopathology
- Separation: At the basement membrane zone.
- Clefts: Contain eosinophils and polymorphs.
- Direct Immunofluorescence: Linear deposition of IgA at the epithelium-connective tissue interface.
Differential Diagnosis
- Oral lichen planus.
- Mucous membrane pemphigoid.
- Pemphigus vulgaris.
- Chronic ulcerative stomatitis.
Treatment
- Topical and systemic corticosteroids (condition does not always respond).
- Other agents: Dapsone, cyclosporine, or other immunosuppressive agents.
Erythema Multiforme
Aetiology and Pathogenesis
- An acute, often recurrent, non-immediate allergic hypersensitivity reaction affecting mucocutaneous tissues.
- Characterized by serosanguineous exudate on the lips, mucosal ulceration, or target-like lesions on the skin.
- Extent: In most cases, affects oral mucosa only. However, severe acute reactions can occur and are potentially life-threatening.
Potential Triggers
- Infections: e.g., Herpes Simplex Virus (HSV).
- Medications: e.g., NSAIDs, anticonvulsants.
- Vaccines: e.g., Hepatitis B vaccine.
- Others: Food additives, chemicals (e.g., benzoates), radiation therapy.
Immunological Mechanism
- Presentation of antigens to T lymphocytes initiates the immune reaction.
- Effector cells (CD8+ T cells, macrophages, and polymorphs) drive epithelial injury.
Clinical Features
- Demographics: Predominantly seen in young adults.
- Gender: Males tend to be more commonly affected than females.
- Presentation: Intraoral, lip, and skin involvement.
Case Examples: Intraoral, Lip, and Skin Involvement
- Presentation: Slides demonstrated examples of intraoral ulceration, lip crusting (serosanguineous exudate), and skin target lesions.
- Severity: Highlighted the range from oral-only involvement to severe mucocutaneous reactions.
Histopathology
- Epithelium: Hyperplasia and spongiosis.
- Vesicles: Occur at the epithelium-connective tissue interface.
- Necrosis: Epithelial necrosis is present.
- Connective Tissue: Inflammatory infiltrate containing lymphocytes and macrophages.
Differential Diagnosis
- Herpes simplex virus infection.
- Aphthous ulceration.
- Pemphigus vulgaris.
- Mucous membrane pemphigoid.
- Oral lichen planus.
Treatment
- Corticosteroids.
- Severe cases: May require hospitalization.
- Prevention: Very important to avoid triggers where known.
Wegener’s Granulomatosis
Aetiology and Pathogenesis
- Characterized by non-caseating granulomas and vasculitis.
- Uncommon but important to recognize as it can be fatal if left untreated.
- Etiology not entirely understood but believed to be the result of an abnormal immune reaction secondary to:
- Non-specific infection
- Aberrant hypersensitive response to an inhaled antigen
- Hereditary predisposition has been suggested in some cases.
- Can present at any age with equal predisposition between males and females.
- Can involve almost every organ.
Clinical Features
Histopathology
- Mixed inflammation centered around blood vessels.
- Involved vessels demonstrate transmural inflammation, often with areas of heavy neutrophilic inflammation.
- Necrosis in the connective tissue adjacent to the vessel.
- Inflammatory cell infiltrate contains a mixture of histiocytes, lymphocytes, eosinophils, and multinucleated giant cells.
Diagnosis
- Based on clinical presentation and microscopic findings of necrotizing and granulomatous vasculitis.
- Serum detection: Antibodies directed against cytoplasmic components of neutrophils (ANCA) supports the diagnosis.
Treatment
- First line: Oral prednisolone and cyclophosphamide.
Footnotes
-
Original PDF page 1: L8 Allergies and immune disease II, p.1 ↩
-
Original PDF page 2: L8 Allergies and immune disease II, p.2 ↩
-
Original PDF page 3: L8 Allergies and immune disease II, p.3 ↩
-
Original PDF page 4: L8 Allergies and immune disease II, p.4 ↩
-
Original PDF page 5: L8 Allergies and immune disease II, p.5 ↩
-
Original PDF page 6: L8 Allergies and immune disease II, p.6 ↩
-
Original PDF page 7: L8 Allergies and immune disease II, p.7 ↩
-
Original PDF page 8: L8 Allergies and immune disease II, p.8 ↩
-
Original PDF page 9: L8 Allergies and immune disease II, p.9 ↩
-
Original PDF page 10: L8 Allergies and immune disease II, p.10 ↩
-
Original PDF page 11: L8 Allergies and immune disease II, p.11 ↩
-
Original PDF page 12: L8 Allergies and immune disease II, p.12 ↩
-
Original PDF page 13: L8 Allergies and immune disease II, p.13 ↩
-
Original PDF page 14: L8 Allergies and immune disease II, p.14 ↩
-
Original PDF page 15: L8 Allergies and immune disease II, p.15 ↩
-
Original PDF page 16: L8 Allergies and immune disease II, p.16 ↩
-
Original PDF page 17: L8 Allergies and immune disease II, p.17 ↩
-
Original PDF page 18: L8 Allergies and immune disease II, p.18 ↩
-
Original PDF page 19: L8 Allergies and immune disease II, p.19 ↩
-
Original PDF page 20: L8 Allergies and immune disease II, p.20 ↩
-
Original PDF page 21: L8 Allergies and immune disease II, p.21 ↩
-
Original PDF page 22: L8 Allergies and immune disease II, p.22 ↩
-
Original PDF page 23: L8 Allergies and immune disease II, p.23 ↩
-
Original PDF page 24: L8 Allergies and immune disease II, p.24 ↩
-
Original PDF page 25: L8 Allergies and immune disease II, p.25 ↩
-
Original PDF page 26: L8 Allergies and immune disease II, p.26 ↩
-
Original PDF page 27: L8 Allergies and immune disease II, p.27 ↩
-
Original PDF page 28: L8 Allergies and immune disease II, p.28 ↩
-
Original PDF page 29: L8 Allergies and immune disease II, p.29 ↩
-
Original PDF page 30: L8 Allergies and immune disease II, p.30 ↩
-
Original PDF page 31: L8 Allergies and immune disease II, p.31 ↩
-
Original PDF page 32: L8 Allergies and immune disease II, p.32 ↩
-
Original PDF page 33: L8 Allergies and immune disease II, p.33 ↩
-
Original PDF page 34: L8 Allergies and immune disease II, p.34 ↩
-
Original PDF page 37: L8 Allergies and immune disease II, p.37 ↩
-
Original PDF page 35: L8 Allergies and immune disease II, p.35 ↩
-
Original PDF page 36: L8 Allergies and immune disease II, p.36 ↩
-
Original PDF page 38: L8 Allergies and immune disease II, p.38 ↩
-
Original PDF page 39: L8 Allergies and immune disease II, p.39 ↩
-
Original PDF page 40: L8 Allergies and immune disease II, p.40 ↩
-
Original PDF page 41: L8 Allergies and immune disease II, p.41 ↩
-
Original PDF page 42: L8 Allergies and immune disease II, p.42 ↩
-
Original PDF page 43: L8 Allergies and immune disease II, p.43 ↩
-
Original PDF page 46: L8 Allergies and immune disease II, p.46 ↩
-
Original PDF page 44: L8 Allergies and immune disease II, p.44 ↩
-
Original PDF page 45: L8 Allergies and immune disease II, p.45 ↩
-
Original PDF page 47: L8 Allergies and immune disease II, p.47 ↩
-
Original PDF page 48: L8 Allergies and immune disease II, p.48 ↩
-
Original PDF page 49: L8 Allergies and immune disease II, p.49 ↩
-
Original PDF page 50: L8 Allergies and immune disease II, p.50 ↩
-
Original PDF page 52: L8 Allergies and immune disease II, p.52 ↩
-
Original PDF page 51: L8 Allergies and immune disease II, p.51 ↩
-
Original PDF page 53: L8 Allergies and immune disease II, p.53 ↩
-
Original PDF page 54: L8 Allergies and immune disease II, p.54 ↩
-
Original PDF page 55: L8 Allergies and immune disease II, p.55 ↩
-
Original PDF page 56: L8 Allergies and immune disease II, p.56 ↩
-
Original PDF page 57: L8 Allergies and immune disease II, p.57 ↩
-
Original PDF page 58: L8 Allergies and immune disease II, p.58 ↩
-
Original PDF page 59: L8 Allergies and immune disease II, p.59 ↩
-
Original PDF page 60: L8 Allergies and immune disease II, p.60 ↩
-
Original PDF page 61: L8 Allergies and immune disease II, p.61 ↩
-
Original PDF page 62: L8 Allergies and immune disease II, p.62 ↩
-
Original PDF page 63: L8 Allergies and immune disease II, p.63 ↩
-
Original PDF page 64: L8 Allergies and immune disease II, p.64 ↩
-
Original PDF page 69: L8 Allergies and immune disease II, p.69 ↩
-
Original PDF page 65: L8 Allergies and immune disease II, p.65 ↩
-
Original PDF page 66: L8 Allergies and immune disease II, p.66 ↩
-
Original PDF page 67: L8 Allergies and immune disease II, p.67 ↩
-
Original PDF page 68: L8 Allergies and immune disease II, p.68 ↩
-
Original PDF page 70: L8 Allergies and immune disease II, p.70 ↩
-
Original PDF page 71: L8 Allergies and immune disease II, p.71 ↩
-
Original PDF page 72: L8 Allergies and immune disease II, p.72 ↩
-
Original PDF page 73: L8 Allergies and immune disease II, p.73 ↩
-
Original PDF page 74: L8 Allergies and immune disease II, p.74 ↩
-
Original PDF page 75: L8 Allergies and immune disease II, p.75 ↩
-
Original PDF page 76: L8 Allergies and immune disease II, p.76 ↩
-
Original PDF page 77: L8 Allergies and immune disease II, p.77 ↩
-
Original PDF page 78: L8 Allergies and immune disease II, p.78 ↩
-
Original PDF page 82: L8 Allergies and immune disease II, p.82 ↩
-
Original PDF page 84: L8 Allergies and immune disease II, p.84 ↩
-
Original PDF page 79: L8 Allergies and immune disease II, p.79 ↩
-
Original PDF page 80: L8 Allergies and immune disease II, p.80 ↩
-
Original PDF page 81: L8 Allergies and immune disease II, p.81 ↩
-
Original PDF page 83: L8 Allergies and immune disease II, p.83 ↩
-
Original PDF page 85: L8 Allergies and immune disease II, p.85 ↩
-
Original PDF page 86: L8 Allergies and immune disease II, p.86 ↩
-
Original PDF page 87: L8 Allergies and immune disease II, p.87 ↩
-
Original PDF page 91: L8 Allergies and immune disease II, p.91 ↩
-
Original PDF page 88: L8 Allergies and immune disease II, p.88 ↩
-
Original PDF page 89: L8 Allergies and immune disease II, p.89 ↩
-
Original PDF page 90: L8 Allergies and immune disease II, p.90 ↩
-
Original PDF page 92: L8 Allergies and immune disease II, p.92 ↩
-
Original PDF page 93: L8 Allergies and immune disease II, p.93 ↩
-
Original PDF page 95: L8 Allergies and immune disease II, p.95 ↩
-
Original PDF page 96: L8 Allergies and immune disease II, p.96 ↩
-
Original PDF page 98: L8 Allergies and immune disease II, p.98 ↩
-
Original PDF page 94: L8 Allergies and immune disease II, p.94 ↩
-
Original PDF page 97: L8 Allergies and immune disease II, p.97 ↩
-
Original PDF page 99: L8 Allergies and immune disease II, p.99 ↩
-
Original PDF page 100: L8 Allergies and immune disease II, p.100 ↩
-
Original PDF page 101: L8 Allergies and immune disease II, p.101 ↩