Case Discussion Of Oral Mucosal Discomfort
Patient Profile and Chief Complaint1
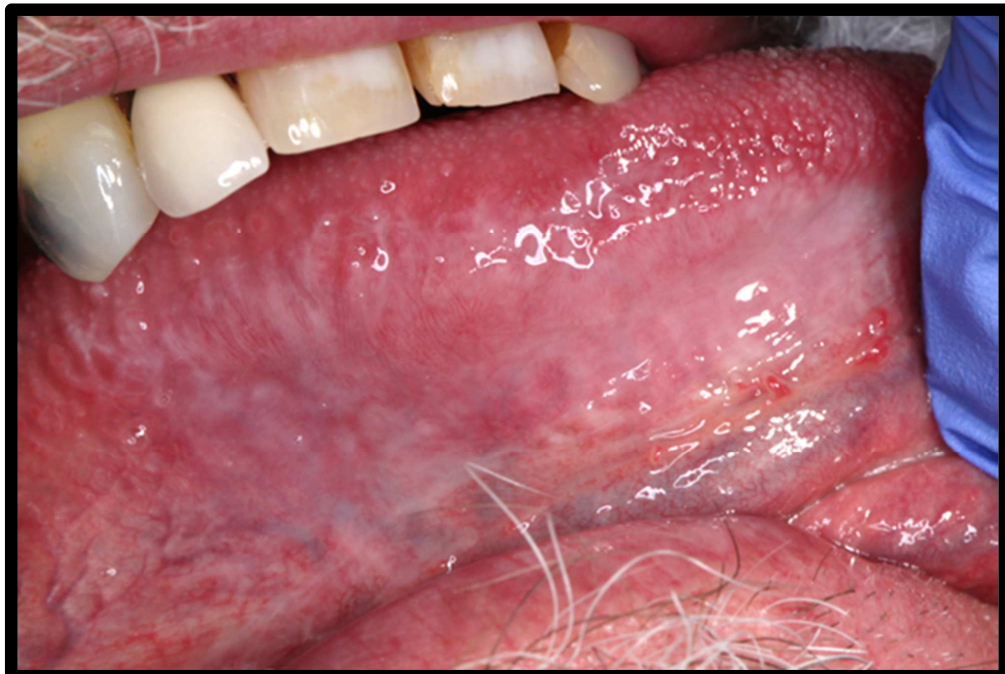
A 63-year-old male presents with a 12-month history of oral mucosal discomfort and irritation. The symptoms are specifically associated with:
- Consumption of food
- Use of toothpaste
 |  |
 |  |
Medical and Social History
- Medical History: Hypertension, currently managed with ramipril.
- Smoking History: Past smoker; quit 8 years ago. Previously smoked 20 cigarettes per day for 35 years.
- Alcohol Consumption: Reports an average of 2-4 alcoholic drinks per week.

Clinical Case Description
Dental History
- Heavily restored dentition.
- Last dental visit was 2 years ago.
Clinical Assessment Activity
Clinical Evaluation Tasks212
- Identify the pathosis and describe the clinical features.
- What is the differential diagnosis?
- What are the relevant clinical investigations?
- What is the diagnosis?
- How would you manage this patient?
1. Identify the pathosis and describe the clinical features
- ==Clinical Presentation: The patient presents with oral ulceration and inflammation in the background.==
- ==Key Features:==
- Lesions are typically bilateral and symmetric.
- The lesions should feel "nice and soft" upon palpation; any thickness or asymmetry is a red flag.
- ==Lichenoid Reactions: Can be caused by amalgam restorations or medications (specifically blood pressure medication).==
- ==Differentiation from Leukoedema: Unlike leukoedema, these lesions do not disappear when stretched and exhibit inflammation and ulceration, which are not present in leukoedema.==
2. What is the differential diagnosis
- Oral lichenoid lesions
- could be the amalgam or medications
- check for this iwth patch testing first (i.e. suspect amalgam first )
- ==Oral Lichen Planus (OLP): The primary consideration, but must satisfy both clinical and histopathological criteria.==
- ==Lichenoid Lesions:==
- ==Contact Allergy: Specifically to amalgam restorations.==
- ==Drug-Induced: Reactions to systemic medications like blood pressure drugs (e.g., the patient’s ramipril).==
- ==Lupus Erythematosus: Can present with similar mucosal lesions; requires investigation if skin lesions or medical history suggest autoimmune disease.==
- ==Pemphigus/Pemphigoid: Considered if the patient is not responding to standard treatment.==
- ==Erythema Multiforme (EM): Some mucosal lesions can resemble EM.==
- ==Dysplasia/Squamous Cell Carcinoma: An ulcer can mimic early mouth cancer; dysplasia can exist even in lesions that look like “textbook” lichen planus.==
3. Clinical investigations
- Biopsy
- needed to satisfy histopathological criteria
- ==Rationale: Necessary to confirm diagnosis and rule out dysplasia. You cannot have a diagnosis of OLP if dysplasia is present.==
- need at least tow for the H&E and one for DIF
- ==Site Selection: If lesions look identical, one side may suffice. If there is asymmetry or a “thick” feeling upon palpation, multiple sites should be biopsied.==
- ==Histopathological Features of OLP: Keratinized structure, band-like lymphocytic infiltrate (predominantly mature lymphocytes), and degeneration of the basal epithelial cells.==
- Patch testing for diffrential
- could send to a dermatologist, some immunologists do it too
- “Please do patch testing to the Dental Series”
- ==Indication: Used when lesions do not respond to treatment and a contact allergy (e.g., to amalgam) is suspected.==
- ==Process: Referral to a dermatologist for a “Dental Series” patch test on the back.==
- ==Interpretation: A negative result does not 100% rule out allergy due to potential delayed reactions (past 5 days) or local irritant reactions.==
- ==Blood Tests==
- ==Full Blood Exam (FBE): Routine examination.==
- ==Nutritional Deficiencies: Iron, B12, and folate studies, as deficiencies increase the risk of oral ulceration and candidosis.==
- ==Autoimmune Markers: Anti-double stranded DNA and anti-skin antibodies if lupus or pemphigoid is suspected.==
- ==Systemic Associations:==
- ==Diabetes: Should be checked as it is a common association.==
- ==Thyroid Disease: Increased risk/association, though not routinely tested unless indicated by history.==
- ==Hepatitis: Possible association, but only tested if history suggests it.==
4. What is the diagnosis
- ==The diagnosis is confirmed as Oral Lichen Planus (satisfying clinical and histological criteria) or Lichenoid Reaction (if linked to a specific trigger like amalgam or medication).==
5. How would you manage this patient
- ==Observation vs. Medication==
- ==Observation: Appropriate for widespread, asymptomatic lesions.==
- ==Active Treatment: Required if the patient is symptomatic (burning/discomfort) or if there is ulceration (due to the risk of dysplasia/cancer).==
- Corticosteroids
- be careful as thee can speed up dysplasia in dysplastic sessation
- Kenalog is the only oral preparation in australia but its mild and hard to use
- Triamcinolone acetonide (Kenalog in Orabase) is a skin preparation used off-label; difficult to apply to wet mucosa.
- Therapeutic guidelines recommeneds beclamethasone ointment
- ointments are hard to apply to wet oral mucosa
- need to tell patient to dry the area
- can use corticosteroid mouthwash/mouthspray but its expensive and costs $80 a bottle
- Dexamethasone mouthwash: Effective but expensive.
- beclamethasone mouthspray dosage
- 2 sprays 3 times a day
- use everyday until discomfort goes away , then add 3 extra days
- Protocol: Use daily until symptoms resolve, then continue for 2–3 extra days to prevent immediate flare-ups.
- Clue for failure of symptom management - super imposed candida
- “the topical steroids were working then all of a sudden it started to get worse ”
- Steroid use increases the risk of fungal infection.
- In this case, give amphoteracin B for the fungal infect
- ==Management: Combine steroids with an antifungal (e.g., Fungilin/Amphotericin B lozenges).==
- Mildly symptomatic:
- can use Difflam
- Difflam (benzydamine) for mild symptoms to avoid steroid side effects.
- ==Refractory Cases: If no response after one month:==
- Check compliance.
- Rule out fungal infection.
- Consider systemic steroids for severe ulceration.
- Investigate lichenoid triggers (replace amalgam restorations one at a time).
- ==Follow-up and Review==
- ==Initial Review: Within one month of starting medication.==
- ==Long-term: Lichen planus requires lifelong observation. Frequency ranges from every 3 months to once a year depending on disease activity and symptom control.==
: Original PDF page 1: 15. Allergies and Immune mediated disease case 1, p.1 : Original PDF page 2: 15. Allergies and Immune mediated disease case 1, p.2