DISCUSSION CASE
Case description: 51-year-old Male presenting with asymptomatic lesions shown. His medical history is non-contributory. He is a non-smoker and consumes minimal alcohol.
Activity:
- Identify the pathosis and describe the clinical features
- What is the differential diagnosis?
- What are the relevant clinical investigations?
- What is the diagnosis?
- How would you manage this patient?
1. Identify the pathosis and describe clinical features
- The primary pathosis involves white plaques that are soft upon palpation.
- A key diagnostic feature is that the lesions wipe off, leaving an underlying surface, which is characteristic of pseudomembranous candidiasis.
- Patients often present with pain, an inability to eat, or difficulty brushing their teeth.
Case Study: 51-Year-Old Male
- Profile: Fit and healthy, non-smoker, no significant medical history.
- Symptoms: Presents with acute oral candidosis.
- Key Observation: No history of antibiotic use or steroid inhalers. This suggests an underlying systemic issue, as "Candidosis is a disease of the diseased."
2. What is the differential diagnosis?
- ==Candidiasis (Candidosis): Specifically the acute pseudomembranous type==
- ==Leukoplakia: Standard differential for white patches, though these typically do not wipe off==
- ==Lichen Planus: Can present with white striations or plaques==
3. What are the relevant clinical investigations?
- Remember patients presenting with candidosis and ulcerations ==hematinics
- the standard protocol
- FBC
- Iron studies
- B12
- Folate
- Fasting Glucose
- the standard protocol
Hematinic tests
Clinical Rationale
For classic presentations of candidiasis, a swab or smear may not be necessary as they incur costs for the patient. However, if the patient is otherwise healthy and presenting with a fungal infection, systemic investigations are mandatory to rule out nutritional deficiencies that predispose the patient to infection.
FBC
FBC Interpretation
- ==High Neutrophil Count: Suggests a bacterial infection==
- ==High Lymphocyte Count: Suggests a viral infection==
- ==White Cell Count: Used to identify infection types==
- ==Platelet Count: General health indicator==
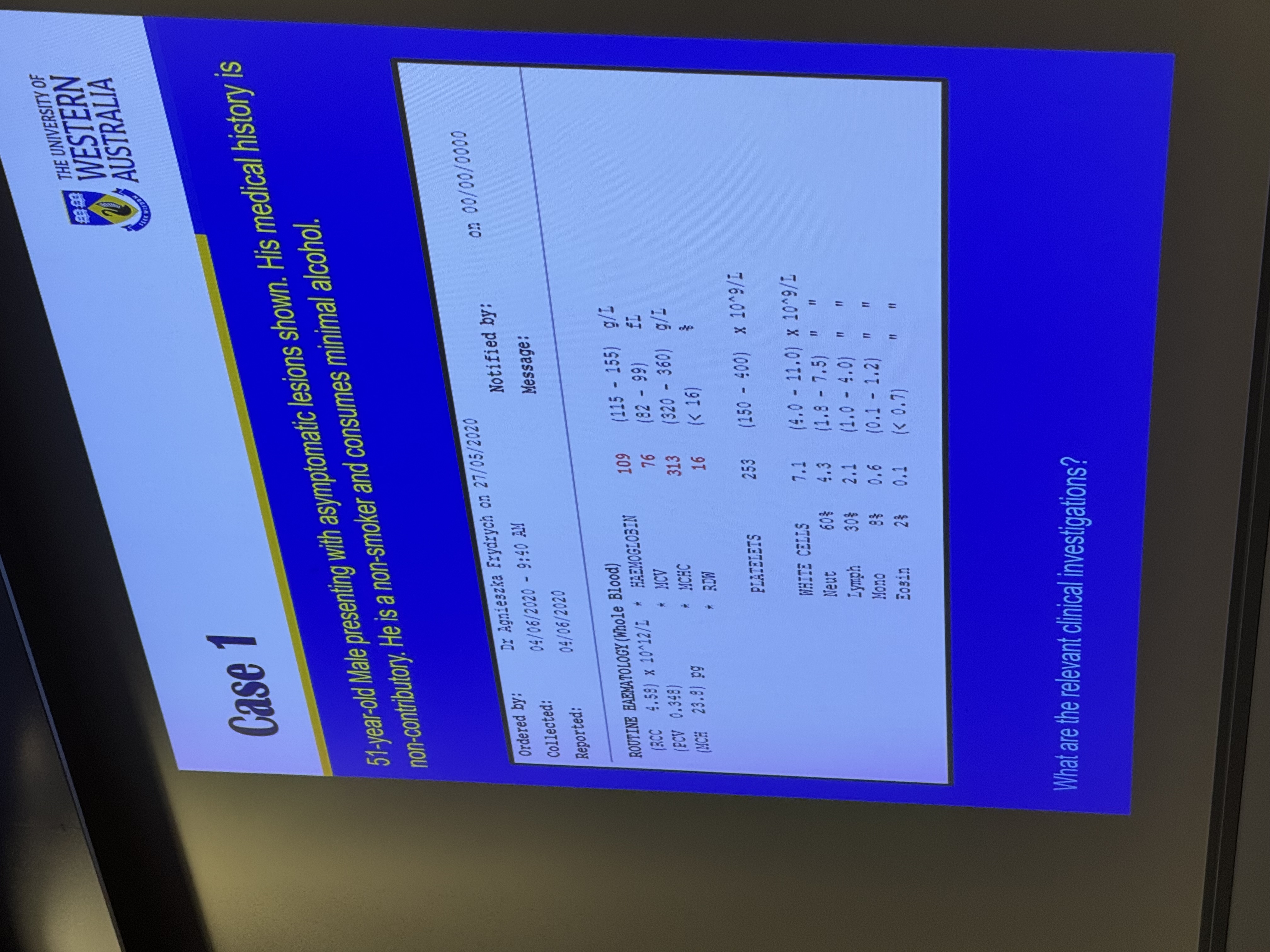 The patient has an FBC that shows the following:
The patient has an FBC that shows the following:
- they have low haemoglobin which shows they have anemai
- they have a low MCV : indicates microcytic anemia
Causes of anemia :
- microcytic: iron deficiency
- macrocytic: b12 or folate
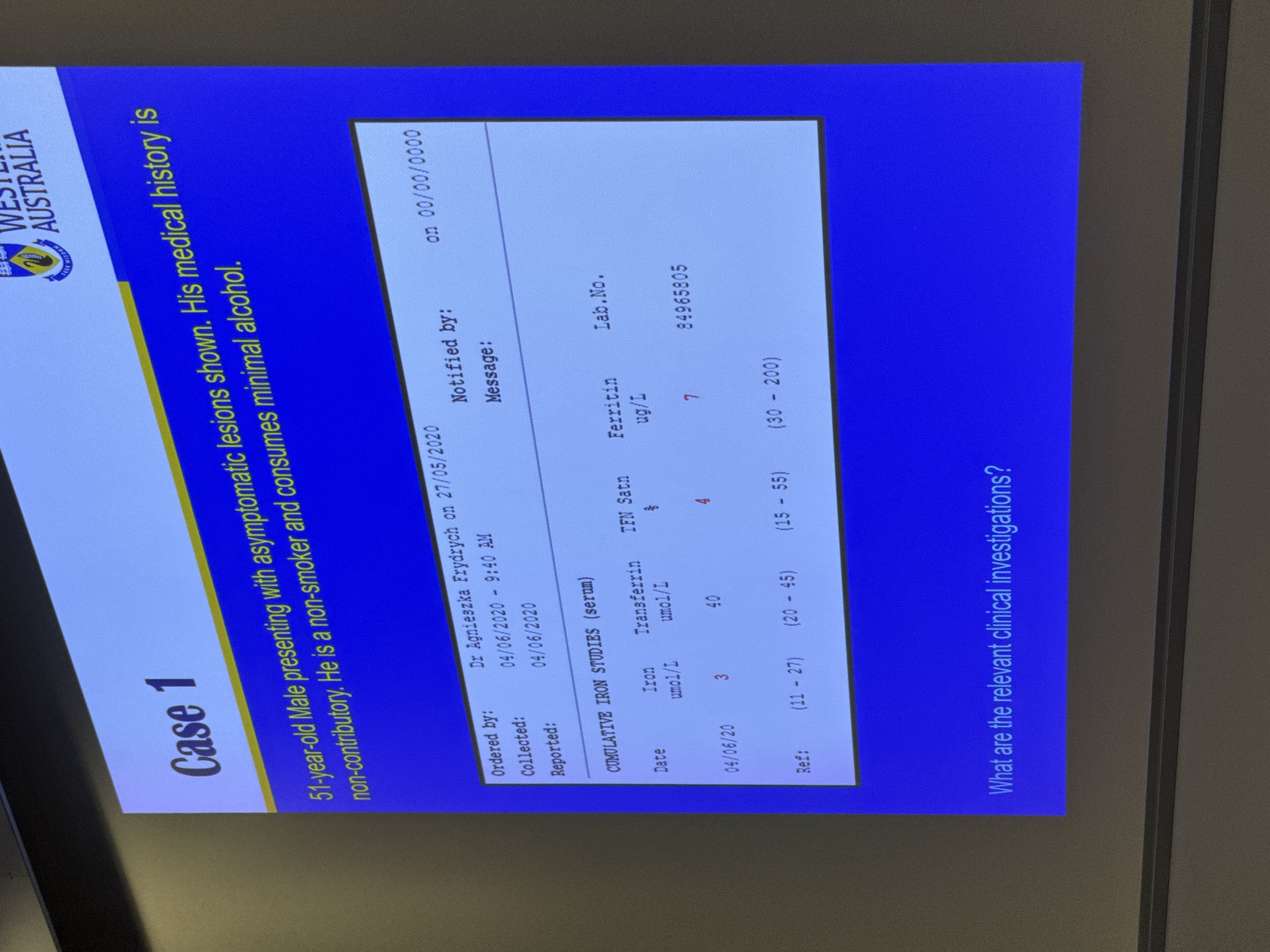
Iron studies
- ==Ferritin: This is the primary marker checked within iron studies to confirm deficiency==
B12
- Deficiency can lead to macrocytic anemia and oral mucosal changes
Folate
- Deficiency is a known risk factor for oral ulceration and candidiasis
Fasting glucose
- this is at the very least but you can diagnose diabetes from the HbA1c
What ifs?
What if patient is on a corticosteroid inhaler
-
If an inhaler explains the infection, an HIV test might be less urgent, but hematinics are still recommended because a patient can have multiple problems simultaneously.
-
You would still give them the tests you can have multiple things going on
What if patient has microcytic anemia
-
what would we expect to see in the full iron studies?
- low hemoglobin
-
Why would he have low iron? 3. ==Urgent Referral: In a “fit and healthy” male, iron deficiency anemia is a major red flag for internal bleeding; the patient must be referred for a colonoscopy and endoscopy to rule out gastrointestinal malignancy.==
- We need to figure out hte cause, it could be colorectal cancer!
4. what is the diagnosis?
- acute candidosis
- ==Primary Diagnosis: Acute Pseudomembranous Candidiasis==
- ==Underlying Diagnosis: Potential Iron Deficiency Anemia or Diabetes Mellitus==
5. How would you manage this patient?
How to treat acute candidiasis
Would you do topical or systemic?:
- systemic has more significant side effects ex. fluconazole
Topical Options
- Nystatin droplets
- Has a very high sugar content can cause caries
- the nystatin drops tend to be swallowed quickly so it doesn’t stay around the mouth
- Amphotericin tablets
- very pasty sugar free tablets, it is annoying for patients to take
- If someone presents with a dry mouth they may not tolerate it
- ==Advantage: doesn’t have any drug interactions
- Stimulates saliva flow
- Stays in the mouth longer than drops
- Miconazole (Gel formulation)
- Causes drug interactions specifically with warfrin
- can get patients INRs going up to 9
- Avoid in patients with liver disease
- Sugar-free and comfortable gel formulation
- Causes drug interactions specifically with warfrin
what is the dosing options?
- this is a debate but
- 4x a day for a month
- 7-14 days is not enough to control the candidiasis
- Treatment should last at least three weeks to prevent recurrence
- 4x a day for a month
- there are no australian guidelines for treating f
Management Strategy
Management involves treating the local infection while simultaneously investigating and addressing the underlying systemic cause. ungal infections > - in different parts of the world there are different preparations