**Clinical Case Discussion:
Asymptomatic Oral Lesion**
Case presentation
Patient presentation1
- Patient: 78-year-old male
- Chief issue: Asymptomatic oral lesion
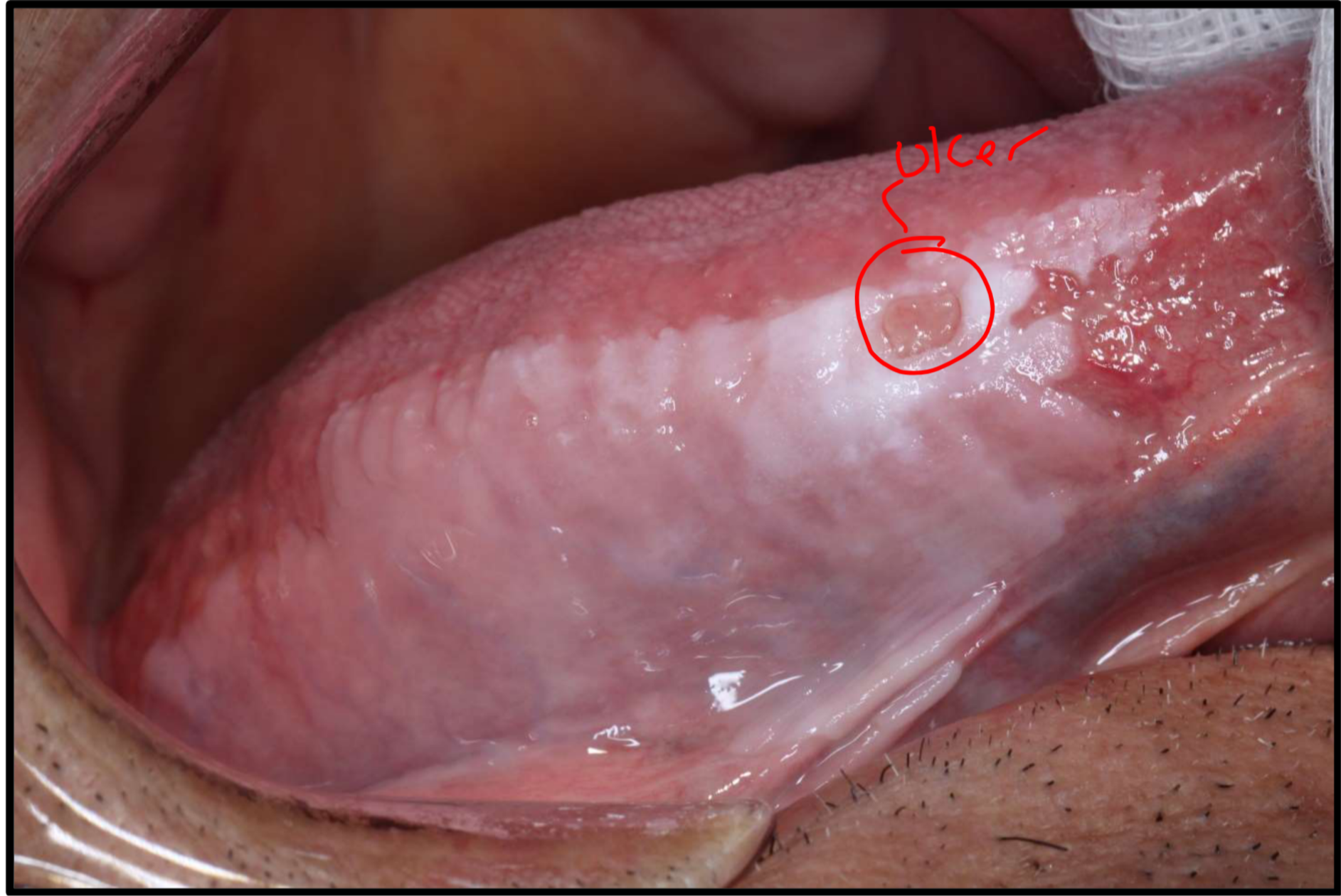
- Site: Right lateral surface of the tongue
- Duration: ~2 years
- Clinical description: Large, white, mostly homogeneous patch; some areas are thicker and “more white” (heterogeneous in parts). A critical feature is an ulceration within the lesion.
Medical and social history
- Medical history: Hypertension, hypercholesterolaemia, ischaemic heart disease. The patient is elderly with a complex medical history.
- Social history: Past smoker; currently consumes six alcoholic drinks per day, described as a heavy alcohol consumer who “drinks like a fish”.
Clinical assessment
Identify the pathosis and describe the clinical features.
Pathosis
A large white patch on the lateral tongue.
Clinical features
- Homogeneity: Mostly homogeneous, but with some thicker, whiter areas indicating heterogeneity in parts.
- Ulceration: A non-healing ulcer is present, which represents a worrying clinical sign.
- Texture/stretch test: Does not disappear when stretched (helps differentiate from leukoedema).
- Vascularity/erythema: Some red areas are visible, though these may be superficial vessels rather than active pathology.
Red flag feature
Non-healing ulceration within a white lesion is worrying, especially with risk factors (e.g., alcohol use/past smoking).
Differential diagnosis
What is the differential diagnosis?
- Leukoplakia: Primary clinical suspicion. White patch that cannot be scraped off and is not attributable to any other specific condition.
- Lichen planus: Considered within the differential, particularly plaque-form lichen planus which can mimic leukoplakia.
- Frictional keratosis: Possible—check for sharp teeth/restorations. Reactive lesion from chronic mechanical irritation.
- Leukoedema: Ruled out because the lesion is not uniform and does not disappear upon stretching.
- Squamous cell carcinoma (SCC): Must be considered due to the presence of a non-healing ulcer (red flag), particularly given the patient’s risk factors.
Investigations
What are the relevant clinical investigations?
Blood tests
Exam note
Simply writing “blood test” is insufficient for exams; specific tests must be named.
- Fasting glucose: To check for underlying conditions like diabetes, especially with non-healing ulcers.
Hematinics
- Focus on ulcer (relevant for investigating the cause of oral ulcerations).
Full blood count (FBC)
- Performed as a routine screening measure.
Liver function tests (LFTs)
- Rationale: Necessary because the patient is a heavy consumer of alcohol.
Coagulation profile
- Rationale: Essential screening before performing a biopsy to prevent surgical bleeding complications in a patient with high alcohol intake.
Biopsy
Technique and site selection
Biopsy approach
- Take the worst-looking area: thickest and heterogeneous (mix of red/white).
- Because the lesion is large, multiple samples may be required to “map” the area and ensure representativeness.
- ==Do not biopsy only the center of an ulcer (necrotic tissue); biopsy the margin.==
- Incisional biopsy is preferred over punch biopsy for this case.
Transport/processing
Specimen handling
==Routine (H&E): formalin pot; no cooling required.
Direct immunofluorescence (DIF): fresh tissue in special medium (e.g., Michel’s solution) or saline.==
Histopathology findings
- Lab report shows atypia confined to the lower third (basal third) → mild epithelial dysplasia.
- Therefore need to rule out lichen planus because there is dysplasia.
Diagnosis
What is the diagnosis?
- ==Mild epithelial dysplasia consistent with leukoplakia==
- ==Atypia confined to the basal third (lower third) of the epithelium==
- Note: Lichen planus is excluded if dysplasia is the primary feature
Management plan
How would you manage this patient?
If leukoplakia there are only 2 options:
- ==Observation / surveillance==
- ==Surgical excision==
Decision for this patient: due to the lesion’s large size and the “mild” grade of dysplasia, observation is often preferred over extensive surgery.
Excision considerations (downsides)
- Large lesion → excessive surgery
- Doesn’t guarantee no recurrence
- Excision does not guarantee SCC won’t develop later, but it may decrease the risk of progression
Aim: get the ulcer to heal / risk reduction
- Risk reduction strategies:
- Smoking cessation and reducing alcohol intake
- Eliminate trauma: smooth sharp teeth or fractured restorations
- Chlorhexidine to try and heal it and see if the ulcer resolves
Recall intervals
- Initial phase (after ulcer healing / first couple visits):
- ==Every 3 months to establish behaviour==
- Stable phase (no change):
- 6-monthly intervals
- Long-term:
- Recalls remain forever (indefinitely) as risk is for life
- ==Highest risk of malignant transformation is within first 5 years==
- After 5 years of stability, interval may be increased to once a year
Risk determination (leukoplakia)
Risk determination of leukoplakia
Factors that increase the risk of malignant transformation:
- readings
- premalignant conditions of the oral cavity
- Gender: females are at higher risk
- Habits: non-smokers with leukoplakia have higher statistically relative risk of transformation; alcohol use is a significant factor
- Duration: lesions present for less than 5 years are higher risk (if they haven’t transformed after 5 years, risk drops)
- Location (high-risk areas): lateral border of the tongue, floor of mouth, retromolar area, soft palate
- Clinical appearance: large lesions, multifocal lesions, or non-homogeneous (erythroleukoplakia) appearance
- Pathology: presence of any grade of dysplasia
Footnotes
-
Original PDF page 1: OPMD Case 1, p.1 ↩