Clinical Discussion Case
Patient Profile and History1
- Patient: 58-year-old female
- Medical History: Hypertension
- Social History: Non-smoker; social alcohol consumption
- Dental History: Wears a removable partial denture
- Chief Complaint: Troublesome gingival lesion in the 21 region
- Previous Diagnosis: 2-year history of oral lichen planus


Identify the pathosis and describe the clinical features.
- Red and white patches on gingiva
- Transcript notes: Red and white lesions, including a white patch with a "sakila white" appearance.
- Areas are described as red and pink compared to the surrounding tissue.
- ulcer
- The ulcerated area is located on the gingiva (predominantly maxillary).
- Swelling within the lesions (Note: Lichen planus is typically flat, so swelling is a significant clinical finding).
- ==Clinical History Details:==
- The patient has a two-year history of biopsy-proven lichen planus.
- She experiences periodic soreness that usually settles within a few days with corticosteroids.
- The current area has been sore for six weeks and is not responding to topical steroid ointment (betamethasone).
- The soreness is interfering with the patient's ability to wear her denture.
What is the differential diagnosis?
- SCC
- A primary concern due to the non-healing nature of the ulcer and the known (small) risk of malignancy associated with lichen planus.
- Lichenoid drug reaction
- due to medications for hypertension
- The patient takes antihypertensive medication, which can be associated with these reactions.
- Lichen Planus
- The patient has a known history; however, the lack of response to steroids in this specific area is a concern.
- Traumatic ulcer
- Denture Trauma: Irritation from an ill-fitting denture causing gingival swelling and ulceration.
- ==Erythroleukoplakia: Considered if the lesion is isolated and inflammatory causes are ruled out.==
- ==Desquamative Gingivitis: Discussed as a descriptive clinical term rather than a final diagnosis; it encompasses conditions like Lichen planus, Linear IgA disease, or other autoimmune/inflammatory diseases.==
- ==Pyogenic Granuloma: Mentioned as a possibility for the clinical appearance.==
- ==Secondary Infection: Specifically candidal infection (secondary to steroid use or denture wear).==
What are the relevant clinical investigations?
Make sure to look at the denture
that its seating well and not irritating the gingiva
- Ask the paitent how she manages the lichen planus:
- she uses topical corticosteroids and bethamethasone ointment to settle flare ups
- her flareups settle within a few days and she stops the ointment, but this area she has been treating it daily for 6 weeks
- she uses topical corticosteroids and bethamethasone ointment to settle flare ups
Treatment of Traumatic vs Inflammatory Ulcers
- You shouldn’t treat traumatic ulcers with topical corticosteroids, but you can treat inflammtory ones with them
Blood Tests
- ==Hematomics: Full blood count.==
Glucose tolerance
- we don’t know if the patient is diabetic
- Fasting Glucose: To check for underlying systemic issues like diabetes.
Dentures
- adjustment or asking patient to stop earing them
- ==Clinical Examination: Check if the denture is well-fitting.==
- ==Adjustment: Adjust the denture to see if the lesion resolves once the source of irritation is removed.==
Biopsy
- she is at 1% risk of malignancy due to having OLP
- We are worried about swelling because lichen planus is flat so there shouldn’t be any swelling
- ==Timing: Can be performed on the first visit if there is high clinical suspicion of malignancy, or after a two-week trial of conservative management (denture adjustment/antiseptics).==
- ==Procedure: Multiple biopsies can be performed if other areas are also not responding to treatment, though the primary focus is the non-healing ulcerated area.==
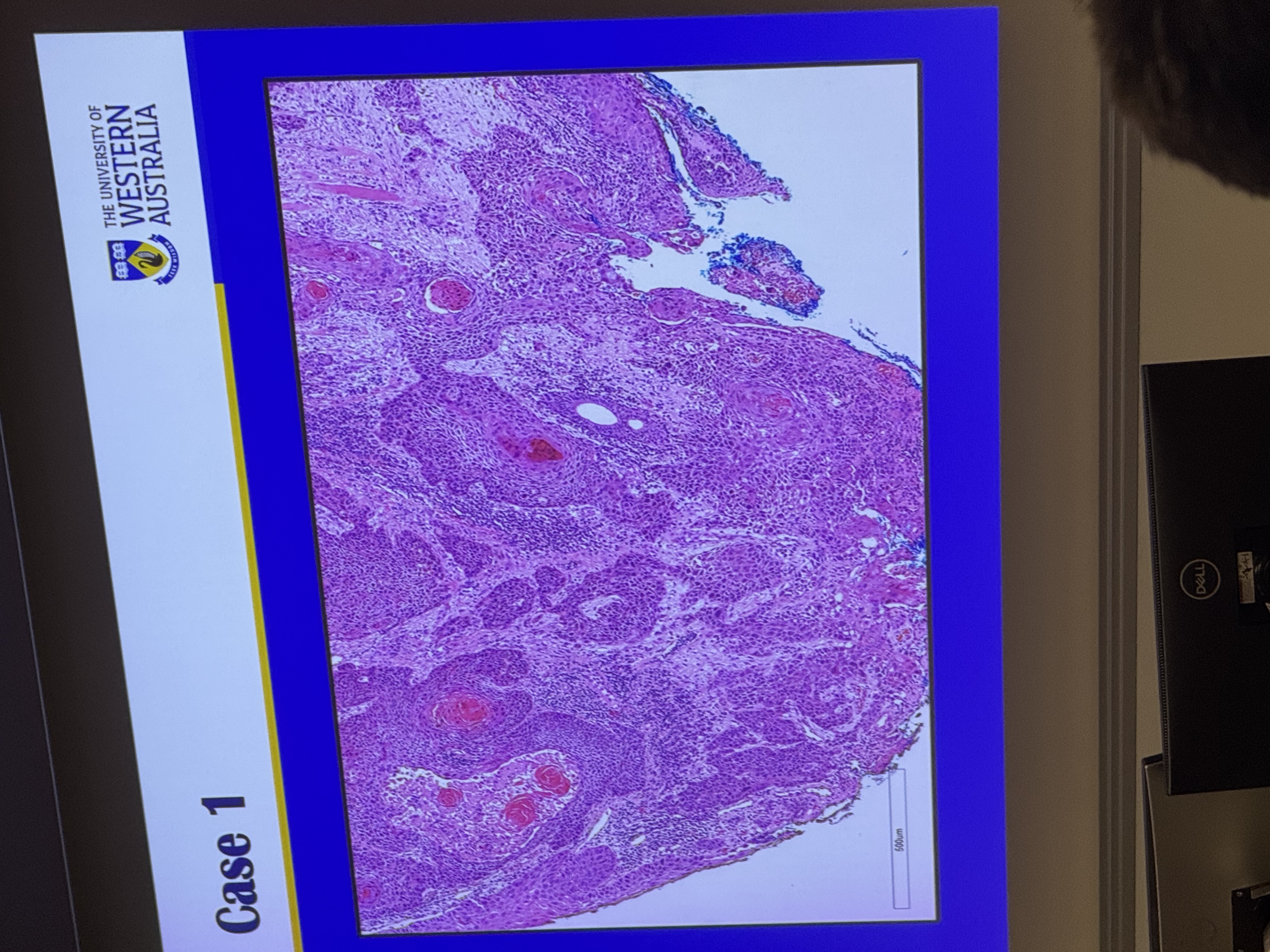
Histology
- Nuclear pleomorphism
- Variation in the shape and size of epithelial cells and nuclei.
- Lymphocytic infiltrate
- Hyperchromatism: Dark-staining lymphocytic infiltrate (seen as small blue dots).
- Mitotic figures
- Presence of abnormal mitotic figures (nuclear material arranged in lines).
- The histology is classic for a sqaumous cell carcinoma
- ==Invasion: Epithelial cells invading the underlying connective tissue; small islands of keratin-producing cells seen within the tissue.==
- ==Differentiation: Presence of “keratin pearls” or well-formed keratin indicates a well-differentiated malignancy.==
What is the diagnosis?
- Early Squamous cell carcinoma that has developed
- Developed within a pre-existing area of lichen planus.
How would you manage this patient?
- should still make the patient wait 2 weeks without hte dneture, as those two weeks wont make a difference , but two months will
- ==Conservative Trial (Initial Phase):==
- Adjust the denture and instruct the patient to leave the denture out.
- Prescribe antiseptic mouthwash (e.g., Chlorhexidine) instead of steroids if trauma is suspected.
- ==Review in two weeks: This is the critical window; if the lesion does not improve, a biopsy is mandatory.==
- ==Communication:==
- Be honest but careful. Inform the patient that while the denture might be the cause, lichen planus carries a small risk of mouth cancer, and a biopsy is necessary if it doesn't heal.
- ==Referral:==
- Once a biopsy confirms SCC, refer the patient to a specialist head and neck surgeon.
- The patient will then be managed through a multidisciplinary team (MDT) process.
Footnotes
-
Original PDF page 1: 9. epithelial Pathosis II, p.1 ↩