Clinical Case Discussion: Asymptomatic Oral Lesion
Patient Presentation1
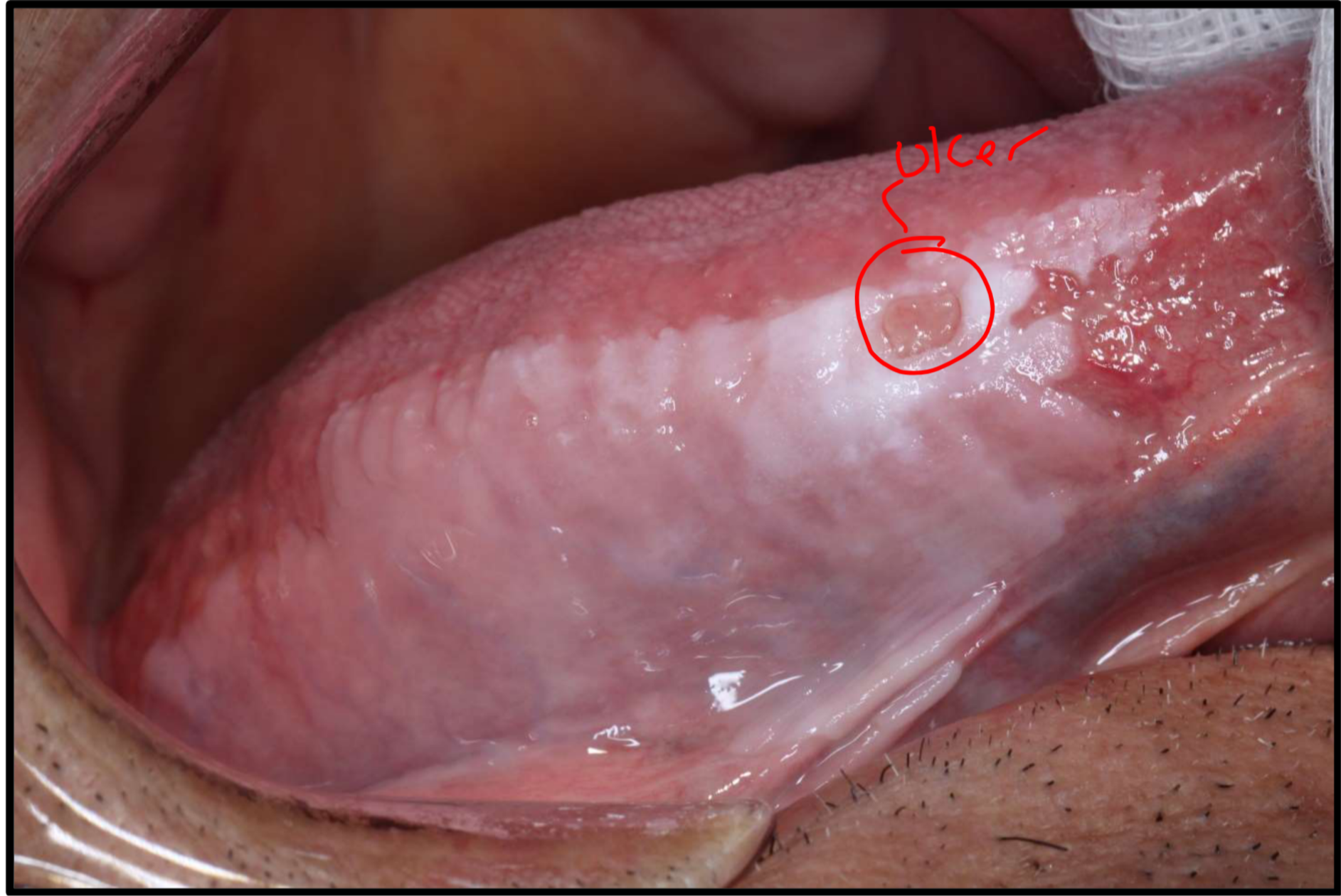
A 78-year-old male presents with an asymptomatic oral lesion. The patient has been aware of the lesion’s presence for approximately two years.
- Duration (patient-reported): approximately two years
- Duration (clarified from case details): approximately three years
- Location: right lateral surface of the tongue
- Appearance: large, non-homogeneous white lesion with varying thickness and a non-healing ulcer
Medical and Social History
- Medical History: Significant for hypertension, hypercholesterolaemia, and ischaemic heart disease.
- Social History: Past smoker; currently consumes six alcoholic drinks per day.
- High alcohol consumption (described as “drinks like a fish”) and smoking are major risk factors for oral malignancy and necessitate specific medical investigations like liver function and coagulation tests.
Identify the pathosis and describe the clinical features.
What is the differential diagnosis?
- lichen planus
- leukoplakia
- Frictional keratosis
Investigations
Blood Tests
- Full Blood Count (FBC): Routine baseline.
- Fasting Glucose (HbA1c): To check for diabetes given the non-healing ulcer.
- Liver Function Tests (LFTs) and Coagulation Screening: Critical due to high alcohol intake to ensure hemostasis before biopsy.
What are the relevant clinical investigations?
Blood test
Hematinics
- cus of ulcer
Full blood count
Liver Function
Coagulation
Biopsy
- take the worst looking area
- take a sample from further back
Biopsy Protocol
- Type: An incisional biopsy is preferred over a punch biopsy for large lesions.
- Site Selection: Sample the most heterogeneous/thickest area near the ulcer margin; avoid the necrotic center of the ulcer.
- Mapping: Multiple samples may be needed to map large lesions.
- Transport Media: Formalin for routine H&E; Michel’s Medium if Direct Immunofluorescence (DIF) is required.
Pathology and Diagnosis
-
Findings: Pathology report indicates Epithelial Dysplasia.
-
Grading: Diagnosed as Mild Epithelial Dysplasia because atypia is confined to the basal third of the epithelium.
-
Final Diagnosis: Leukoplakia.
-
after lab report we get atypia , in the lowe rthrid
- thus mild epithelial dysplasia
- so we have to rule out lichen planus because theres dysplasia
What is the diagnosis?
- After lab report we can tell its leukoplakia
Management and Surveillance
Treatment and Actions
- Options: Surgical excision (reduces risk but doesn’t guarantee non-recurrence) or Surveillance (monitoring if the ulcer heals).
- Clinical Actions: Address local trauma (sharp teeth), use Chlorhexidine mouthwash, and advise smoking/alcohol cessation.
How would you manage this patient?
If leukoplakia there are only 2 options:
- observe
- excise
- downsides:
- large lesion so its excessive
- doesn’t guarantee that the lesion won’t recur
- downsides:
We also want to try and get the ulcer to heal:
- so chlorhexidine to try and heal it
Follow-up and Risk Factors
- Schedule: Every 3 months initially, then 6 months if stable, continuing indefinitely (for life).
- High-Risk Factors: Females, non-smokers (paradoxically), non-homogeneous appearance, and high-risk locations like the floor of mouth or lateral tongue.
- Leukoedema: Differentiated because it does not disappear when stretched and is typically uniform, unlike this heterogeneous lesion.
Recall intervals
- first couple visits after ulcer healing
- 3 months
- Then if the lesion is doing nothing (not changing)
- keep patient on 6 monthly review
- Recalls remain forever as their risk is for life
- the highest risk is within 5 years, if the lesion has been there for longer than five years then you’ll see them once a year
Risk determination of leukoplakia
- readings
- premalignant conditions of the oral cavity
Footnotes
-
Original PDF page 1: OPMD Case 1, p.1 ↩