Oral Surgery Instruments — Reference Guide
This document summarizes common oral surgery instruments, their variants, indications, handling techniques, and important cautions. Instruments are grouped by function (cutting, elevation, retraction, extraction, suturing, suction, bone work). Where applicable, holding technique and typical motions are described.
1. Cutting Instruments
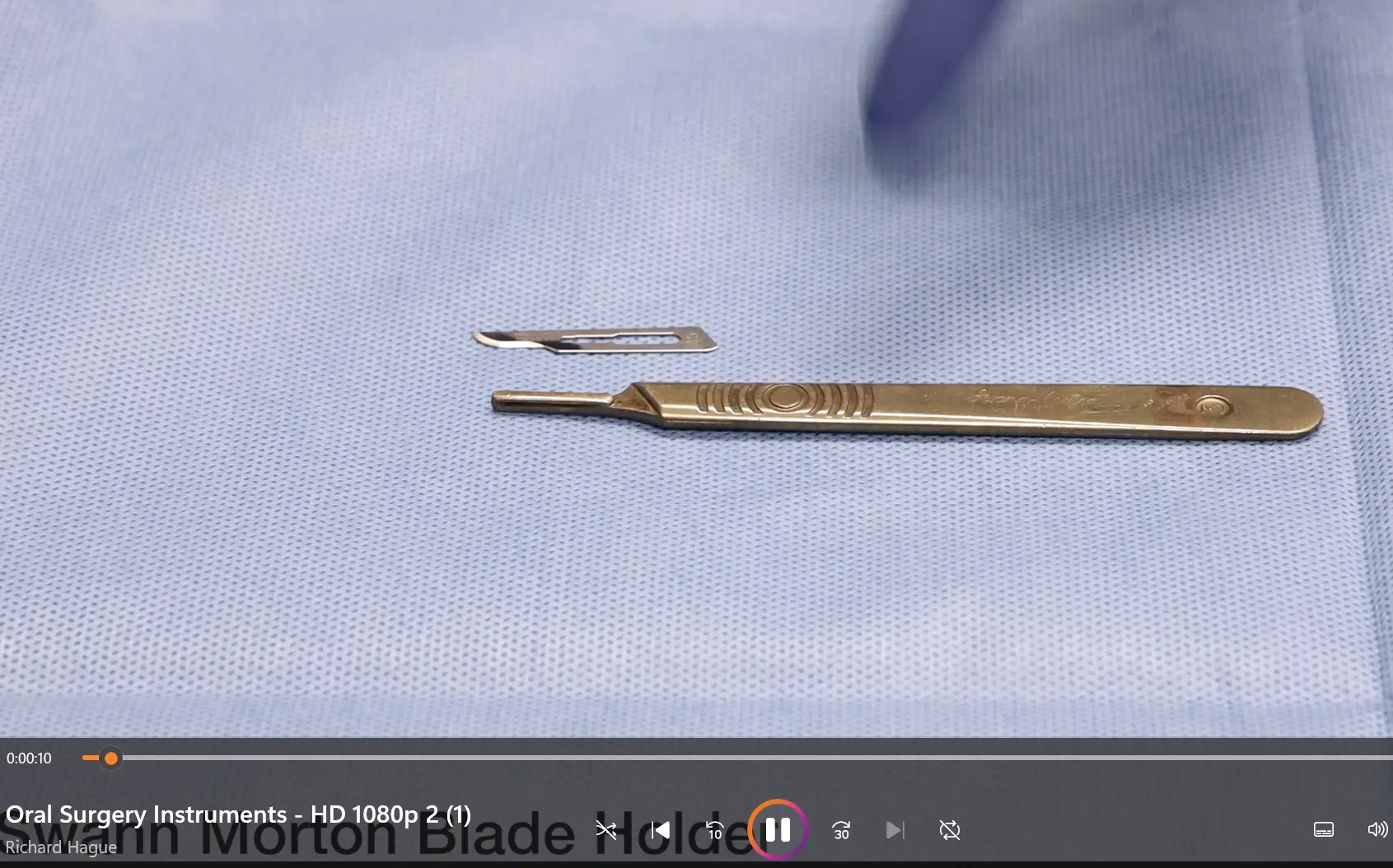
Blade Holder and Surgical Blades
- Blade holder: accepts detachable scalpel blades for soft-tissue incisions.
- Common blades used in alveolar/dental surgery:
- No. 15 (most common)
- No. 12
- No. 15C
- Loading and disposal:
- Use needle holders to load and remove blades safely.
- Hold the blade holder with a pencil grip.
- Apply the blade perpendicular to the bone and perform a single cutting motion for incisions.
- Remove and dispose blades using the needle holders; ensure the blade is not in the way of others when discarding.

2. Periosteal Elevators and Flap Retractors
Periosteal Elevators
- Molt (Molt) periosteal elevator
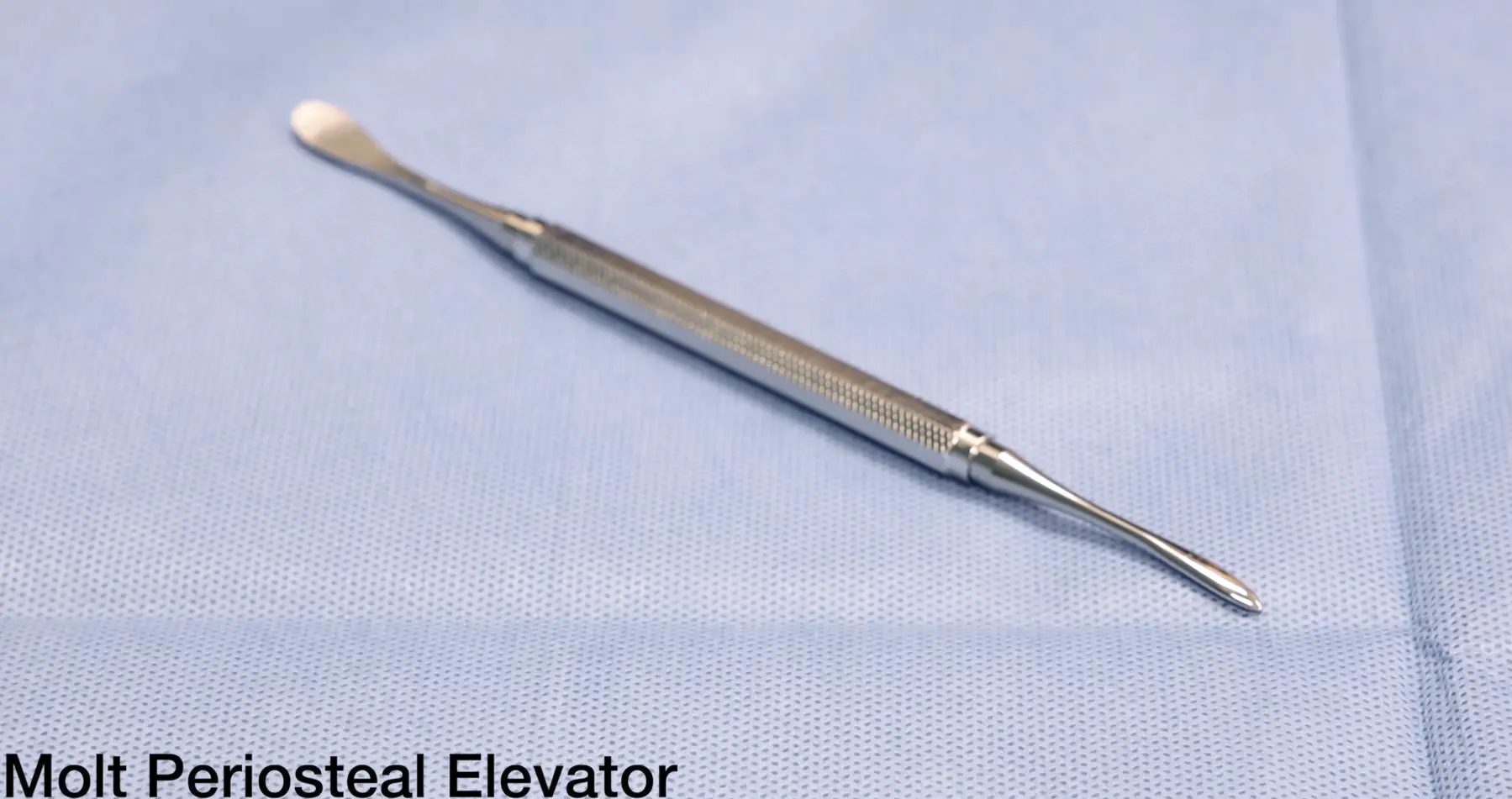
- Ends: a sharper (narrow) end and a wider, blunter end.
- Use: sharp end to lift papillae; wider/blunt end to reflect and retract mucoperiosteal flaps.
- Haworth’s (Howarth’s/Haworth’s) periosteal elevator

- Blade shapes: wider spoon-shaped end and flatter blade end.
- Use: similar to Molt elevator for flap reflection and retraction.
Retractors for Soft Tissue Control
- Lax tongue depressor
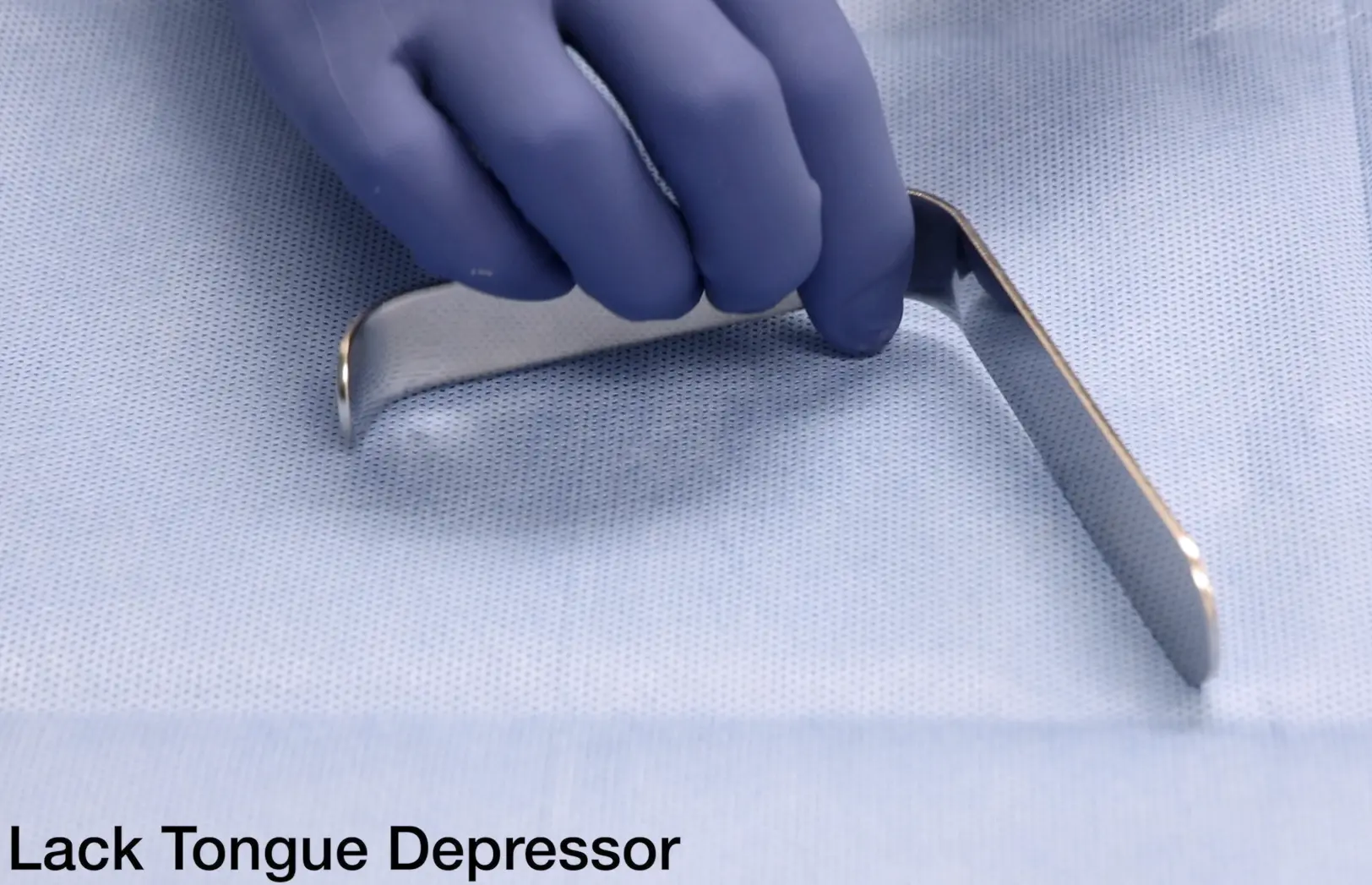
- Use: control and retract the tongue to clear the operating field and reduce trauma.
- Minnesota retractor

- Use: cheek/tongue retraction and clearing the field; can function similarly to a rake retractor.
- Also useful as an adjunct when using the surgical handpiece.
- Rake retractor
- Use: hold back mucoperiosteal flaps, protect soft tissues, and provide direct access to bone.
- Lester’s (Lastres in original transcript) retractor
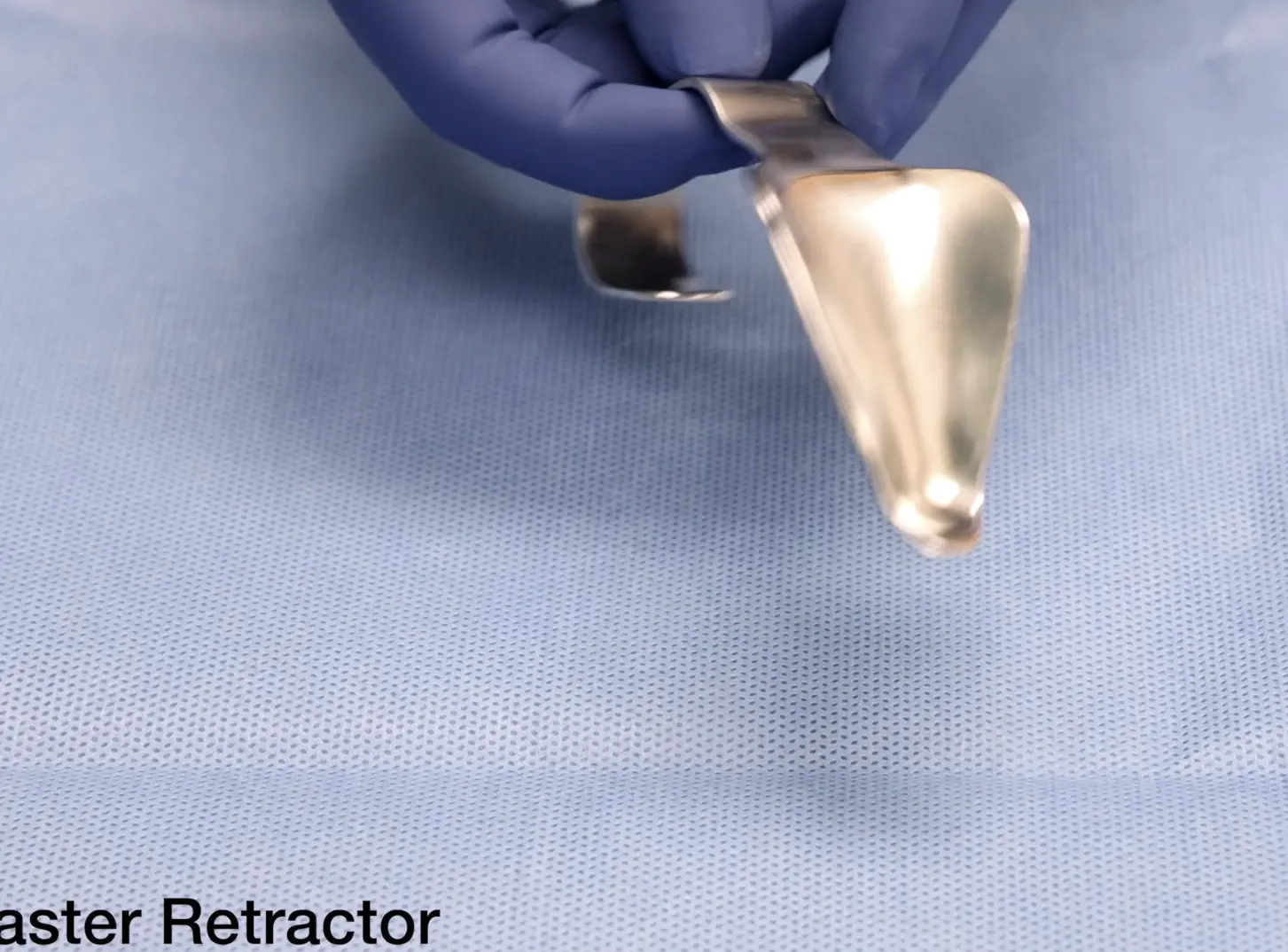
- Use: commonly placed behind the maxillary tuberosity to retract the cheek and gain access/vision of maxillary third molars.
- Shape enhances posterior cheek retraction and focuses light on the posterior maxilla for better illumination.
- Kilner (kilna in transcript) retractor
- Use: cheek retraction during suturing; features a wider and a narrower end.

3. Mouth Props
- McKesson (McKeeson) mouth props
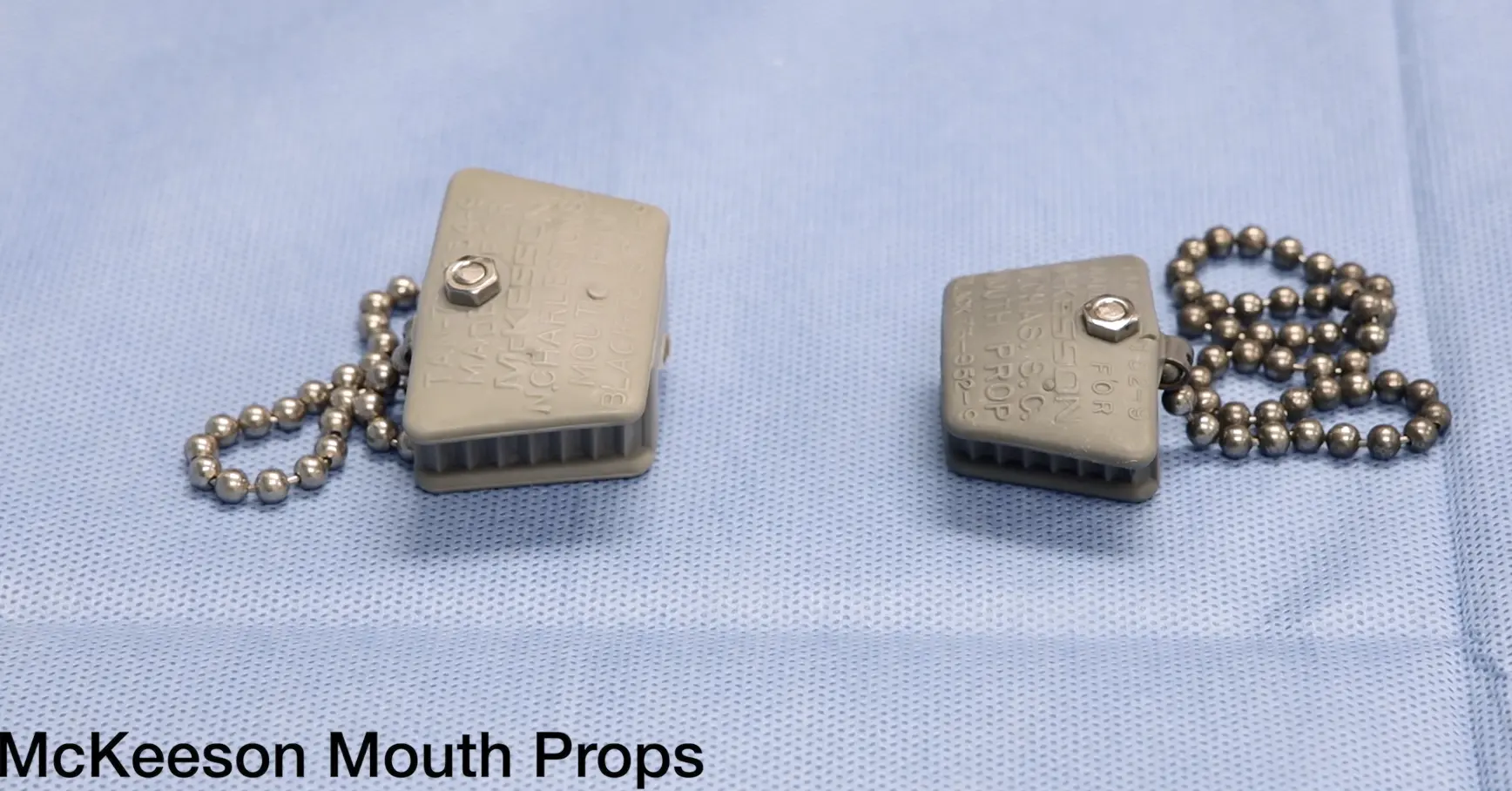
- Sizes: available in multiple sizes (example: small and large shown).
- Use: maintain mouth opening and patient comfort during surgery.
4. Elevators and Luxation Instruments
Coupland Elevators

- Set originally of 9–12; commonly a set of 1–3 (small, medium, large).
- Use: apply force perpendicular to tooth/bone interproximal area to elevate tooth; can split partially sectioned teeth.
- Technique: progress to larger sizes only after some movement has been achieved with a smaller instrument.

Luxators

- Common sizes: 3 mm and 5 mm (other sizes/shapes may be encountered).
- Use: separate the periodontal ligament to facilitate extraction when used with appropriate forceps.
- Technique:
- Hold with index finger for stability.
- Insert between tooth and bone parallel to long axis of tooth; advance apically with careful controlled movement.
- Caution: avoid luxating adjacent teeth — tactile feedback by stabilizing the mandible/maxilla with the non‑dominant hand is helpful.
Cryer (Cryer/Cryo in transcript) Elevators

- Left and right variants with a sharp tip.
- Use: engage and elevate roots of multi‑rooted teeth; remove buccally placed upper third molars.
- Technique: place in interproximal space perpendicular to bone and rotate.
- Caution: single-point contact concentrates force — take care to avoid trauma.
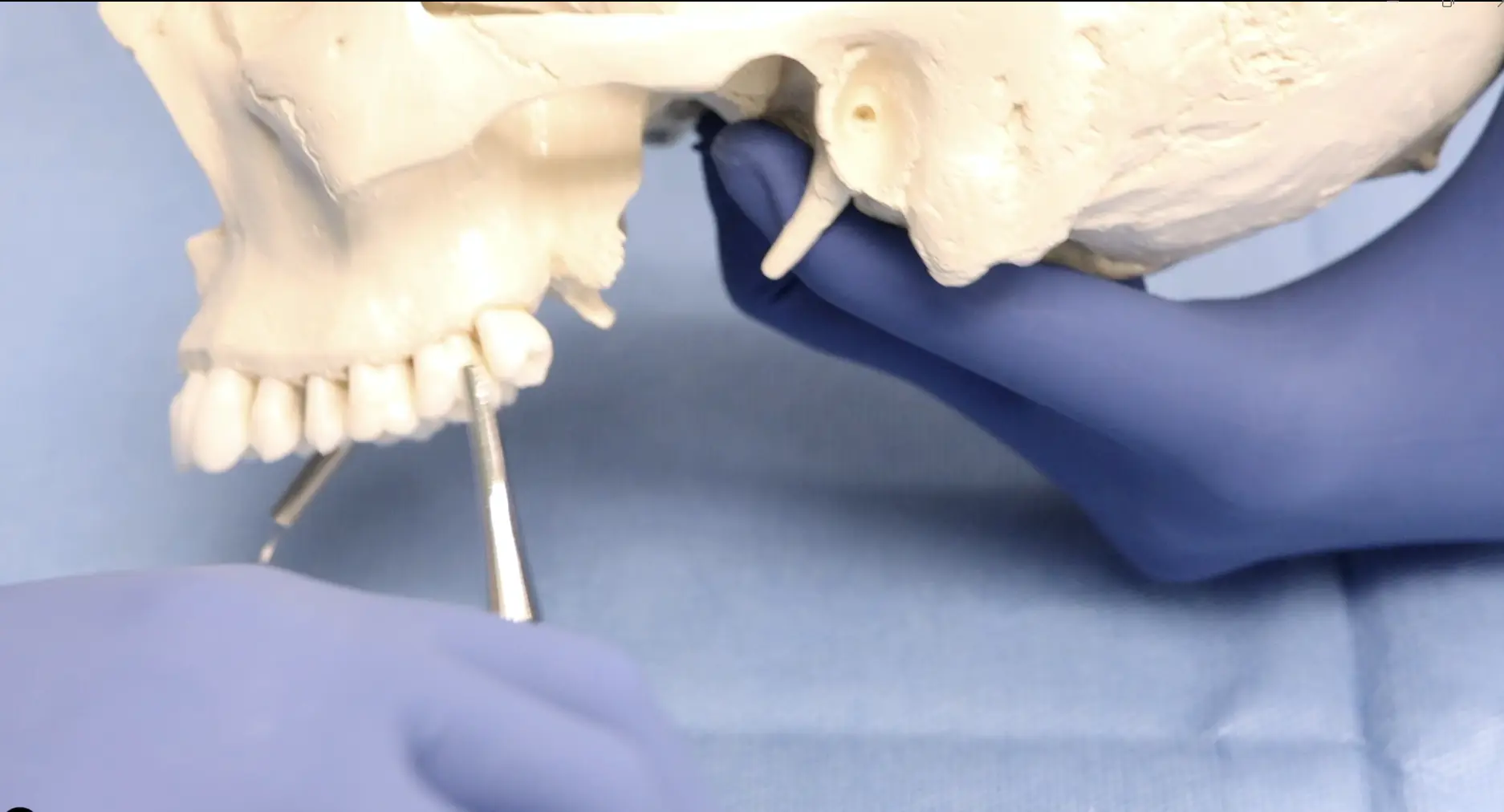
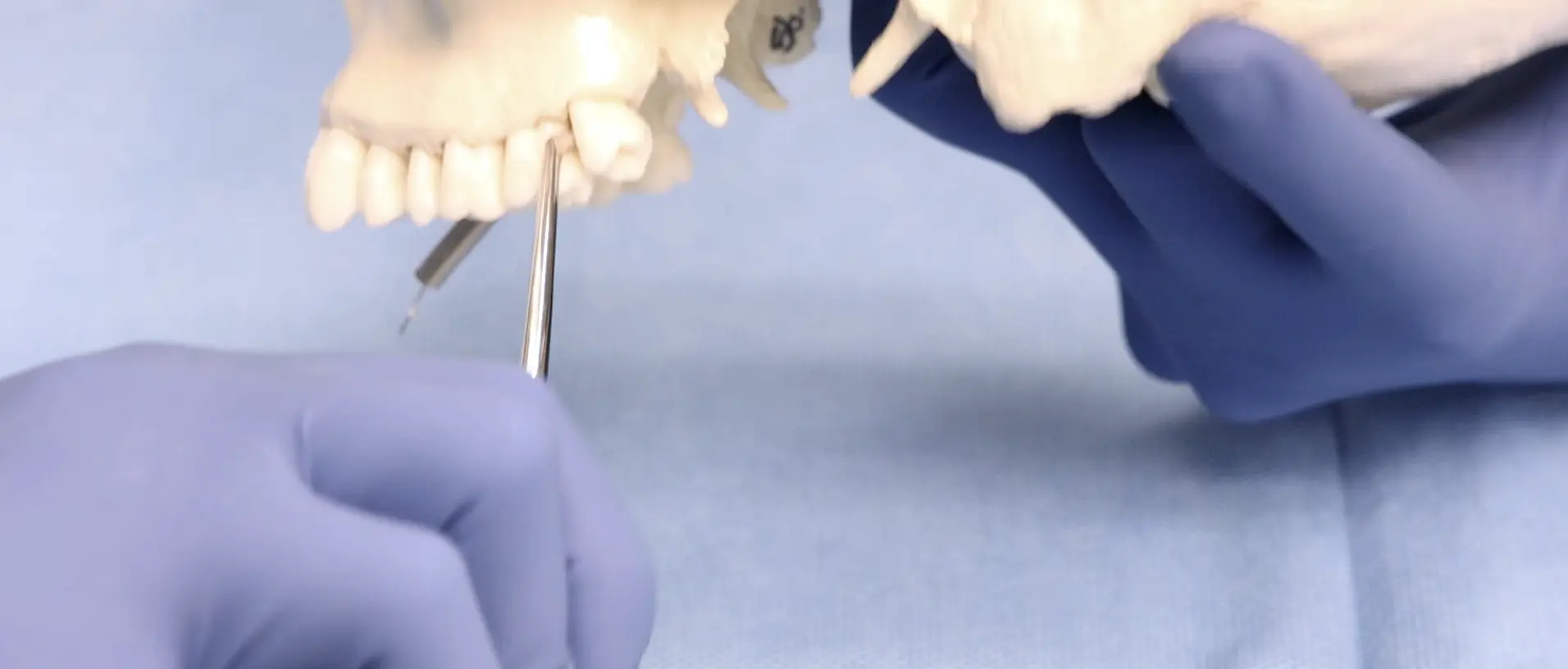
Warwick-James Elevators
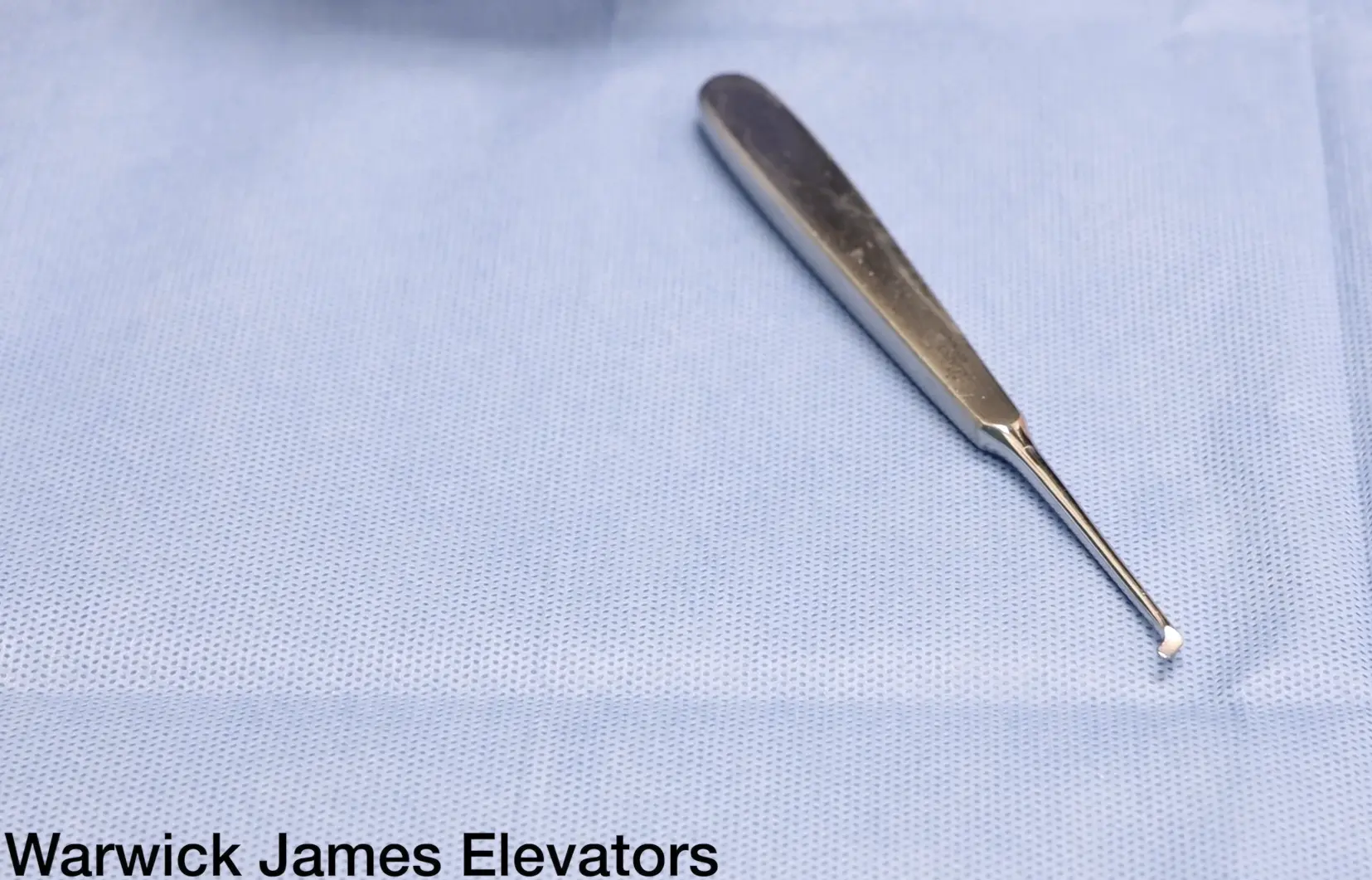
- Variants: left, straight, and right.
- Use: function as a lever placed perpendicular to tooth/bone and rotated; commonly remove retained roots and upper third molars.
5. Extraction Forceps
A summary table of common forceps, numbers/variants, indications, and technique:
| Forceps | Number / Variant | Indication | Technique / Notes |
|---|---|---|---|
| Lower molar (lower hawk) | No. 73 | Lower molar teeth (commonly two roots) | Two beaks (buccal and lingual). Apply and use a figure-of-eight motion to extract. |
| Lower cow‑horn forceps |  | Severely broken-down or grossly carious mandibular molars | Two pointed beaks engage furcation; gentle handle pressure brings beaks together to lift tooth; fracture often occurs through furcation facilitating root separation. |
| Lower universal | No. 74; 74N (fine) | Lower incisors and lower premolars | Apply and use a rotating motion to remove tooth. |
| Maxillary molar | No. 95 (left); No. 94 (right) | Maxillary molars | Differ in shape from lower molar forceps due to tooth anatomy; apply with beak engaging buccal furcation — mnemonic: “beak to cheek.” |
| Maxillary premolar (upper universal) | No. 76; 76N (fine) | Maxillary premolars and roots | Apply and deliver bucco‑palatal force. |
| Upper anterior | No. 29 (straight) and No. 107 (shorter for canines) | Central/lateral incisors and canines | Apply as shown; often use rotation to extract. |
| Upper bayonet forceps | — | Aid extraction of upper third molars | Angled (bayonet‑like) shape helps positioning; apply and rotate to remove tooth. |
Notes:
- Select the forceps appropriate to the tooth anatomy and root configuration.
- Be prepared for potential tooth fracture (cow‑horn/cowhorn extractions) and manage accordingly.
6. Suturing and Tissue Handling Instruments
Needle Holders
- Use to hold needles when suturing and also to safely load and remove scalpel blades.
- Holding technique: thumb and ring finger in rings, index finger for stability; instruments often have a locking latch.
- Working surface: cross‑hatched for firm grip of needle.
Tissue Forceps
- Gillies tissue forceps
- Single‑toothed on one side to stabilize flaps when suturing.
- Caution: do not exert excessive pressure to avoid tissue trauma.
Scissors
- Surgical scissors vary by tip and purpose:
- Sharp‑tipped, blunt‑tipped, curved, straight.
- Metzenbaum scissors: commonly used in oral surgery for cutting sutures and for blunt dissection.
Curved Mosquito Forceps
- Small, curved blunt tips with internal serrations; used for fine haemostasis and soft‑tissue handling.
- Differ from needle holders by serration pattern and absence of cross‑hatched gripping surface.
7. Bone and Root Instruments
Mitchell’s Trimmer
- Two ends:
- Spoon‑shaped end: retraction of mucoperiosteal flaps.
- Sharp/pointed end: removal of soft bone.
Bone File
- Double‑ended; used to carve and smooth bone after extractions to promote healing.
- Caution: ensure adequate irrigation to remove bone chips generated by filing.
Root Pick (Root Elevator / Root Pick)
- Often double‑ended with opposing blade directions to aid elevation of small root fragments.
- Caution: instrument tips can be sharp and risk soft tissue injury.
Surgical Burs
- Common types used in clinics:
- Round surgical bur.
- Flat fissure surgical bur.
- Selection depends on surgeon preference and the specific procedure.
8. Suction Instruments
Jankauer (Janker in transcript)
- Large‑opening plastic suction with bulbous head designed for atraumatic suctioning; common in operating theatres.
Fraser Suction
- Features a 45° bend to aid access in difficult areas.
- Handle has a small hole that can be occluded to increase suction power.
- Narrow diameter can lead to blockages by debris; a stylet is typically supplied to clear obstructions by passing it through the tip to dislodge debris.
- Caution: avoid soft tissue trauma when increasing suction power or clearing blockages.
9. Curettes and Socket Debridement
- Curette
- Double‑ended, rounded mirror‑image blades.
- Use: scrape alveolar sockets post‑extraction to remove excess granulation tissue.
- Technique: scraping motion; ensure complete removal of necrotic or inflamed tissue to promote healing.
10. Key Handling Techniques and Safety Considerations
- Blade handling:
- Always load/unload blades with needle holders to minimise sharps risk.
- Use a single smooth cutting motion for incisions; avoid sawing motions.
- Elevator and forceps technique:
- Use appropriate instrument size and progress incrementally.
- Stabilize opposing jaw with the non‑dominant hand to reduce unintended force transmission to adjacent teeth.
- Apply forces in recommended directions (perpendicular, apical advancement, rotation, or figure‑of‑eight) depending on instrument and tooth.
- Soft tissue protection:
- Retractors and mouth props aid visibility and protect tissues; place carefully.
- Avoid excessive pressure with toothed forceps or tissue clamps.
- Bone work:
- Provide irrigation when filing bone to clear bone chips.
- Use appropriate burs and avoid unnecessary bone removal.
- Suction maintenance:
- Keep suction tips clear; use stylet if supplied.
- Modulate suction power to avoid soft tissue aspiration or trauma.
This reference condenses practical information on commonly used oral surgery instruments, their uses, handling techniques, and cautions. Use it as a quick guide during instrument selection and intraoperative decision‑making.