Medication-Related Osteonecrosis of the Jaws and Osteoradionecrosis
Clinical Overview1
This presentation covers the critical aspects of Medication-Related Osteonecrosis of the Jaws (MRONJ) and Osteoradionecrosis (ORN), presented by David Power, OMS 2 Registrar.
The lecture begins with a clinical overview grounded in real-world emergency scenarios encountered during oral and maxillofacial surgery on-call duties. These cases highlight the complexity of facial trauma and infection, setting the stage for discussing bone pathology.
Introduction23
 |  |
 |
Presentation Outline4
-
Medication-Related Osteonecrosis of the Jaws (MRONJ)
- Primary causes and pharmacological triggers
- Underlying pathophysiology
- Identification of patient risk factors
- Established treatment goals and clinical options
-
Osteoradionecrosis (ORN)
- Prevention strategies for patients undergoing radiation therapy
- Current treatment modalities
American Association of Oral and Maxillofacial Surgeons’ Position Paper on Medication-Related Osteonecrosis of the Jaws—2022 Update
The content is based primarily on position papers from surgical and research societies, such as the American Association of Oral and Maxillofacial Surgeons (AAOMS). These papers provide high-level evidence and recommendations for assessment, treatment, and risk classification, which are crucial for clinical practice and examinations.
Salvatore L. Ruggiero, DMD, MD; Thomas B. Dodson, DMD, MPH; Tara Aghaloo, DDS, MD, PhD; Eric R. Carlson, DMD, MD, EdM; Brent B. Ward, DDS, MD; and Deepak Kademani, DMD, MD
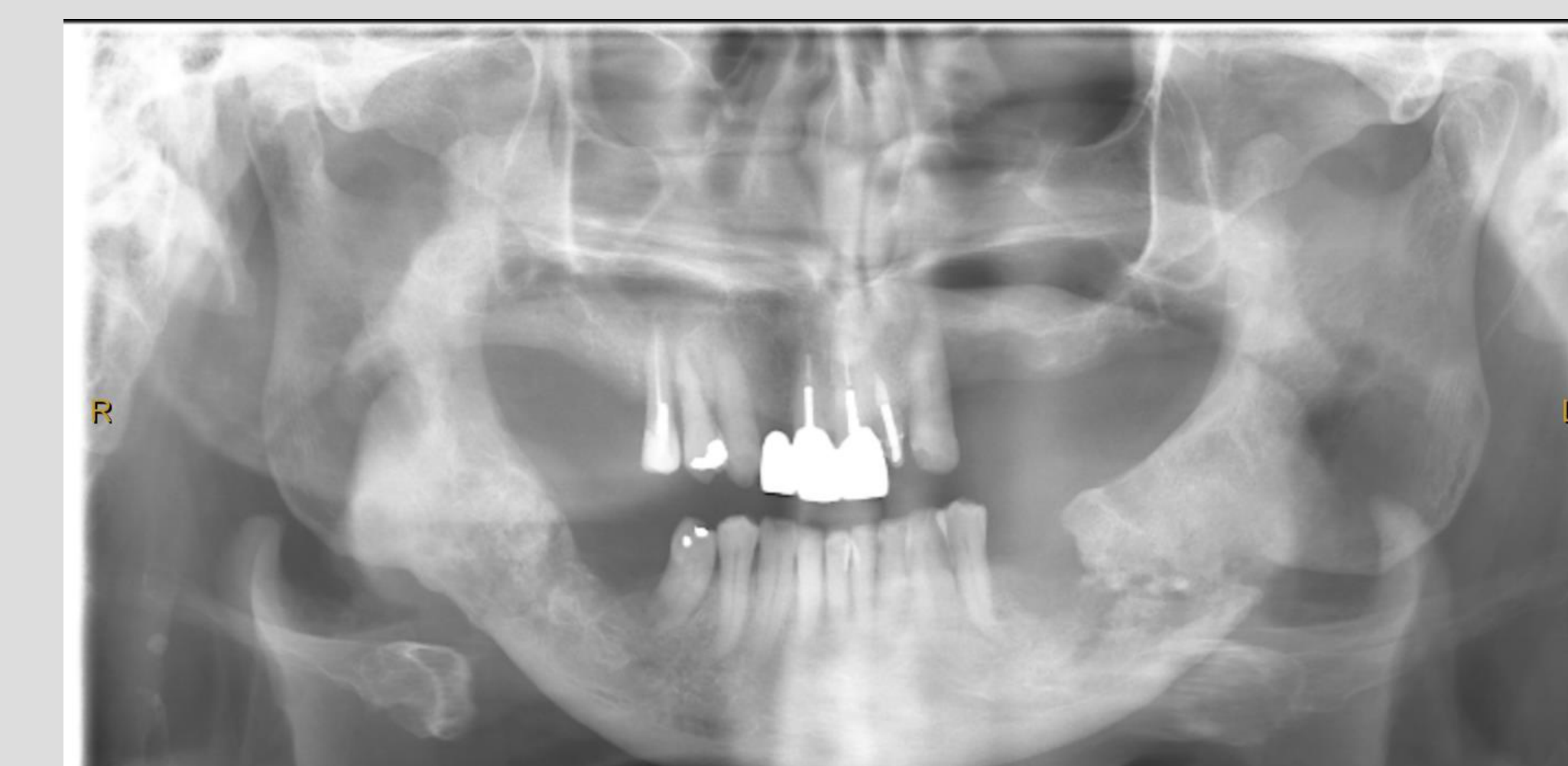
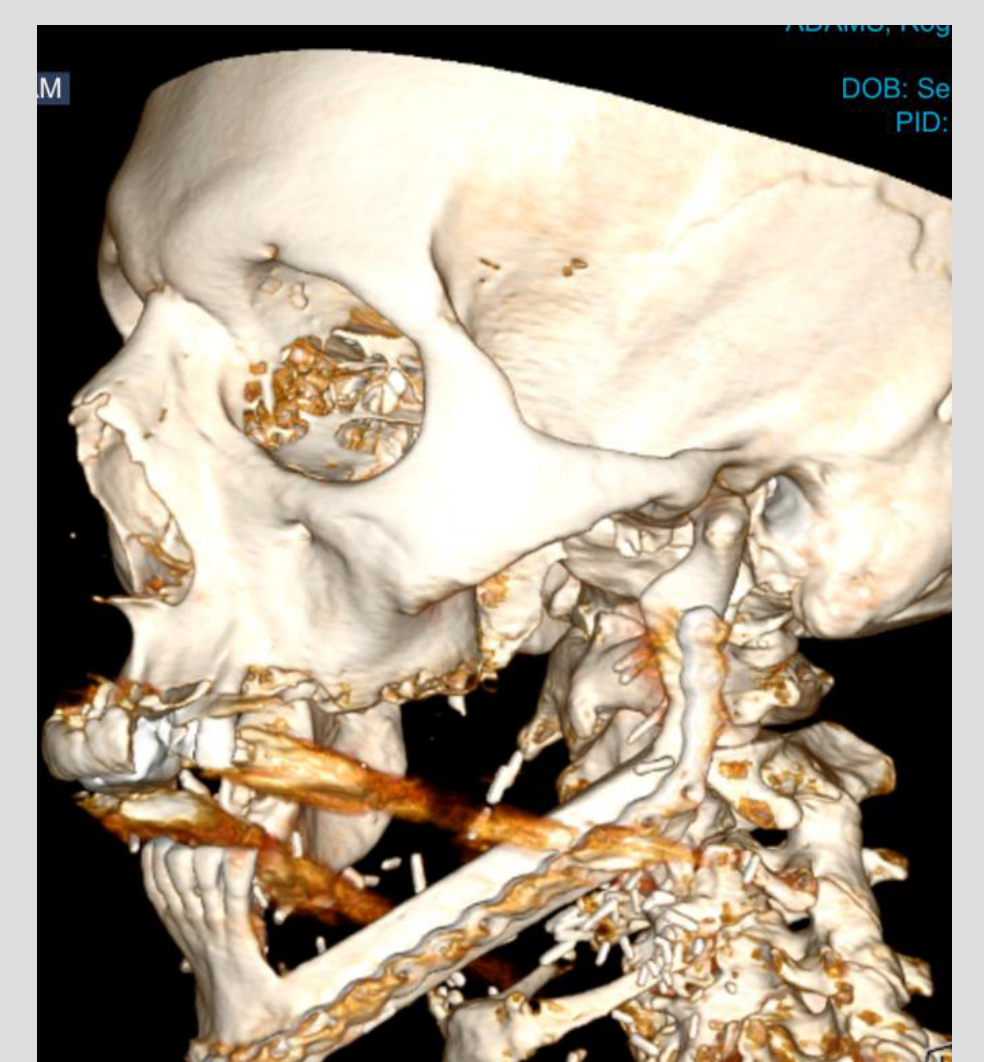
Case Study: Trauma and Infection Scenarios
- Chainsaw Injury: Patient from Karatha with facial ricochet injury, proptosis, optic nerve constriction, globe rupture, and nasal bone into frontal sinus.
- Submandibular Abscess: Lady with good hygiene, lingual breach of tooth 37, periapical radiolucency tracked lingually (path of least resistance) instead of buccally.
- Maxillary Fracture: Elderly lady, mechanical fall, incomplete fracture (no pterygoid plates), edentulous so no malocclusion risk, managed with denture adjustment.
Definition of Medication-Related Osteonecrosis of the Jaws
Clinical Criteria for Diagnosis5
Medication-Related Osteonecrosis of the Jaws (MRONJ) is defined by the following three criteria:
- A breach in oral mucosa leading to exposed bone (or bone that can be probed through an intraoral or extraoral fistula) that fails to heal within 8 weeks.
- A history of receiving antiresorptive therapy.
- No history of previous head and neck radiation.
- Medication history includes both antiresorptive and antiangiogenic agents.
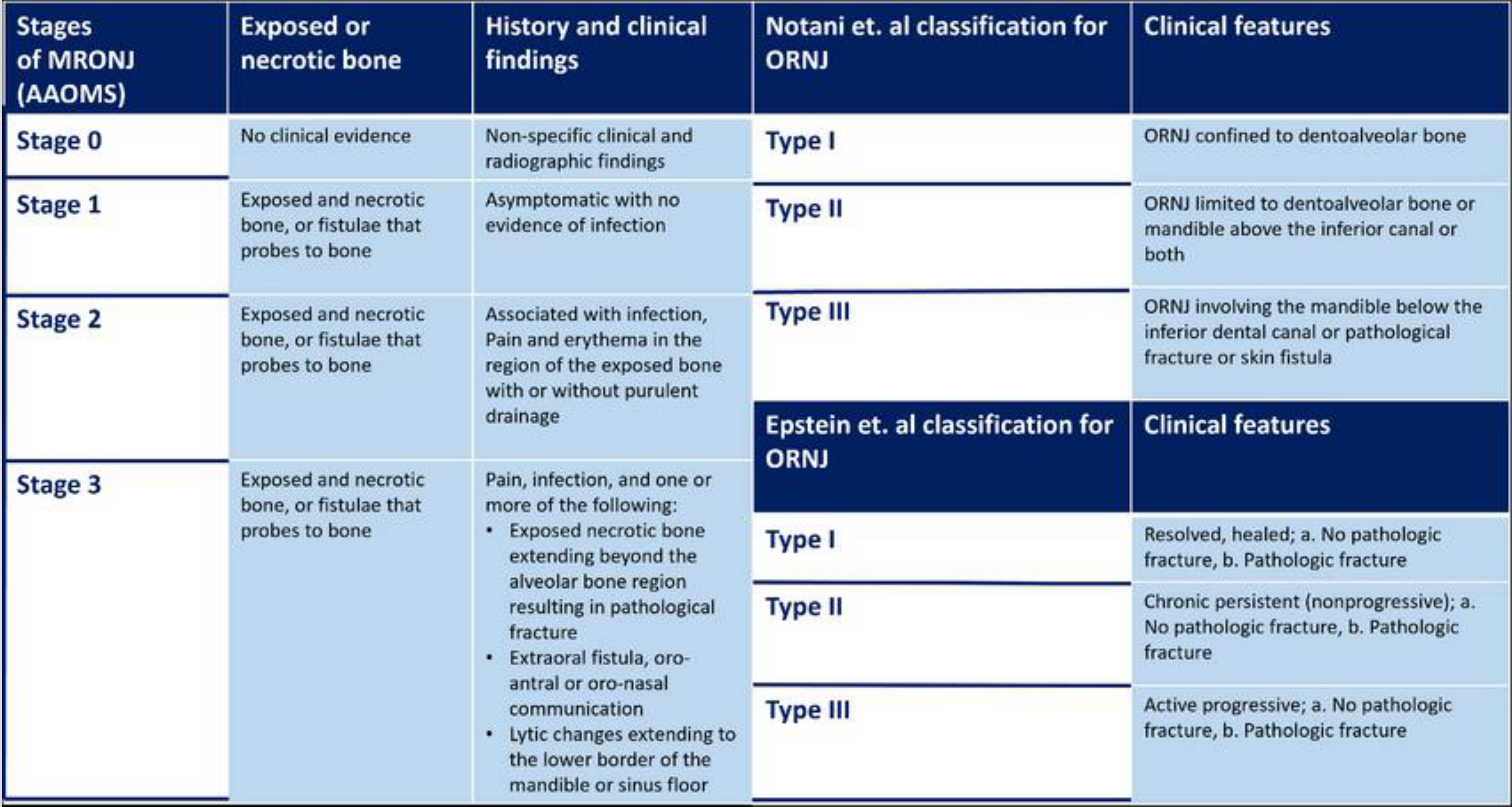
AAOMS Staging of MRONJ6
- Stage 0
- Exposed or necrotic bone: No clinical evidence.
- Clinical findings: Non-specific clinical and radiographic findings.
- Stage 1
- Exposed or necrotic bone: Exposed and necrotic bone, or fistulae that probes to bone.
- Clinical findings: Asymptomatic with no evidence of infection.
- Stage 2
- Exposed or necrotic bone: Exposed and necrotic bone, or fistulae that probes to bone.
- Clinical findings: Associated with infection, pain, and erythema in the region of the exposed bone with or without purulent drainage.
- Stage 3
- Exposed or necrotic bone: Exposed and necrotic bone, or fistulae that probes to bone.
- Clinical findings: Pain, infection, and one or more of the following:
- Exposed necrotic bone extending beyond the alveolar bone region resulting in pathological fracture.
- Extraoral fistula, oro-antral or oro-nasal communication.
- Lytic changes extending to the lower border of the mandible or sinus floor.
Case Study: MRONJ Progression
- Stage 1 Example: Patient had teeth 4 and 5 removed, breach in mucosa, no signs of infection or pain.
- Stage 3 Example: Patient presented with a fistula, infected, painful, involves significant bony sequestra.
Comparative Classifications for Osteoradionecrosis (ORNJ)
Notani et al. Classification:
- Type I: ORNJ confined to dentoalveolar bone.
- Type II: ORNJ limited to dentoalveolar bone or mandible above the inferior canal or both.
- Type III: ORNJ involving the mandible below the inferior dental canal or pathological fracture or skin fistula.
Epstein et al. Classification:
- Type I: Resolved, healed (a. No pathologic fracture; b. Pathologic fracture).
- Type II: Chronic persistent (nonprogressive) (a. No pathologic fracture; b. Pathologic fracture).
- Type III: Active progressive (a. No pathologic fracture; b. Pathologic fracture).
Case Study: Osteoradionecrosis and Reconstruction
- Patient Profile: 75-year-old gentleman, tongue squamous cell carcinoma resected followed by radiotherapy.
- Condition: Developed ORN on left and right side, tooth extraction aggravated situation.
- Reconstruction: Fibula bone from lower leg harvested to replace necrotic mandibular bone.
Causality and Pathophysiology

Multifactorial Nature of MRONJ7
- MRONJ is rare and multifactorial; patients may present with the same clinical symptoms without exposure to antiresorptive medication.
- Potential links include infections, trauma, smoking, steroids, autoimmune disease, diabetes, and chemotherapy.
- Many patients receiving antiresorptives have other comorbidities that likely act as exacerbating or contributing factors.
- Proving definitive causality remains difficult due to numerous confounding variables, making incidence and prevalence estimates challenging.
Clinical Scenario: Cumulative Risk Factors
A patient on antiresorptives for osteoporosis who also smokes, has a large dental abscess, and takes steroids for rheumatoid arthritis is at a much higher risk than a patient on medication alone. The combination significantly elevates risk.
Medications and Mechanisms
Bisphosphonates
Characteristics and Indications8
Bisphosphonates are pyrophosphate analogues used for:
- Prevention and treatment of postmenopausal and steroid-induced osteoporosis.
- Paget’s disease of bone.
- Hypercalcaemia of malignancy and multiple myeloma.
- Bony metastases (e.g., breast, prostate, lung).
- Improving quality of life (QOL), though their effect on cancer-specific survival remains controversial.
- High prevalence in aging populations (e.g., post-menopausal women)
- 20% mortality indirectly or directly after hip fracture in those over 70
Mechanism of Action
Bisphosphonates bind to hydroxyapatite binding sites on the bone surface. Subsequent uptake by osteoclasts impairs bone resorption.
- Non-nitrogen-containing bisphosphonates (e.g., Etidronate, tiludronate):
- Metabolized intracellularly to inhibit ATP-dependent enzymes, resulting in osteoclast apoptosis.
- Nitrogen-containing bisphosphonates (e.g., Alendronate, risedronate, pamidronate, ibandronate, zoledronic acid):
- More potent; they bind and block the enzyme farnesyl pyrophosphate synthase.
- This prevents the attachment of osteoclasts to the bone surface, causing them to detach and impairing resorption.
Half-Life Characteristics
They have an extremely long half-life in bone (e.g., Alendronate approx. 10 years) They remain in the system for years
Adverse Effects
- General Effects:
- Hypocalcaemia and hypophosphatemia (usually transient and mild).
- Osteonecrosis of the Jaw (ONJ).
- Atypical fractures (particularly of the femur).
- Musculoskeletal (MSK) pain.
- Atrial Fibrillation (AF).
- Renal impairment.
- Ocular inflammation and visual disturbances.
- Route-Specific Effects:
- Oral bisphosphonates: Oesophageal inflammation (patients should swallow with water and remain upright for 30 minutes).
- IV bisphosphonates: Acute-phase reaction with flu-like symptoms 24-72 hours post-administration.
- Risk of MRONJ is rare in osteoporosis patients but higher in oncology patients
- Medication remains in the bone long after cessation due to long half-life
Denosumab
Mechanism of Action
Denosumab is a monoclonal antibody and RANK ligand (RANKL) inhibitor:
- It targets RANKL (receptor activator of nuclear factor kappa B ligand) by mimicking osteoprotegerin.
- It reversibly inhibits bone resorption by reducing osteoclast formation and differentiation and increasing apoptosis.
- Unlike bisphosphonates, RANKL inhibitors do not bind to bone; effects on bone remodeling typically diminish within 6 months of cessation.
- It has a much shorter half-life (approximately 30 days)
Indications
- Significant reduction in fracture risk (vertebral, nonvertebral, hip) in osteoporotic patients when administered subcutaneously every 6 months.
- Reduction of skeletal-related events in metastatic bone disease from solid tumors when administered monthly.
- Proven efficacy in treating giant cell tumors and fibrous dysplasia.
Clinical Management
Timing of extractions relative to the injection cycle is critical for risk management Drug is largely gone after 4-5 months due to faster washout
Bone Cell Biology
Osteoblasts
- Origin: Derived from mesenchymal osteoprogenitor (stem) cells located under the periosteum and in medullary spaces.
- Function: Secrete osteoid to form the organic matrix for hydroxyapatite deposition and regulate mineralization.
- Transition: Some osteoblasts become enclosed in lacunae as osteocytes upon completion of bone formation.
- RANKL Expression:
- Expressed on osteoblasts and marrow stromal cells.
- Binds to RANK receptors on macrophages (osteoclast precursors) to activate NF-kB, essential for osteoclast differentiation and survival.
- Osteoprotegerin (OPG):
- Secreted by osteoblasts as a high-affinity decoy ligand for RANKL, restricting osteoclast differentiation.
- Osteoblasts regulate resorption via PTH-activated expression of RANKL and downregulation of OPG.
Osteocytes
Characteristics and Functions9
- Major cell type of mature bone, distributed throughout the matrix and interconnected by dendritic processes.
- Derived from osteoblasts enclosed within the rigid matrix.
- Mechanotransduction: Detect mechanical forces and translate them into biologic activity.
- Regulation: Help control calcium and phosphate levels.
- Signaling:
- Secretes RANKL to activate osteoclasts.
- Produces Sclerostin, which inhibits osteoblasts.
- New medications like romosozumab are sclerostin inhibitors, effectively inhibiting the inhibitor to densify bone.
Osteoclasts
Characteristics and Functions10
- Large, specialized multinucleated macrophages located on the bone surface.
- Bone Resorption: Responsible for decalcifying and removing bone during growth and remodeling.
- Differentiation: Develop from myeloid stem cells via macrophage-colony-forming units, regulated by M-CSF and RANKL (secreted/expressed by osteoblasts).
- Mechanism: Dissolve bone minerals by secreting acid and neutral proteases (predominantly matrix metalloproteases).
- Regulation: Stimulated by signals from osteoblasts, macrophages, lymphocytes, PTH, and calcitriol. Calcitonin reduces osteoclast activity.
RANKL and OPG Pathway
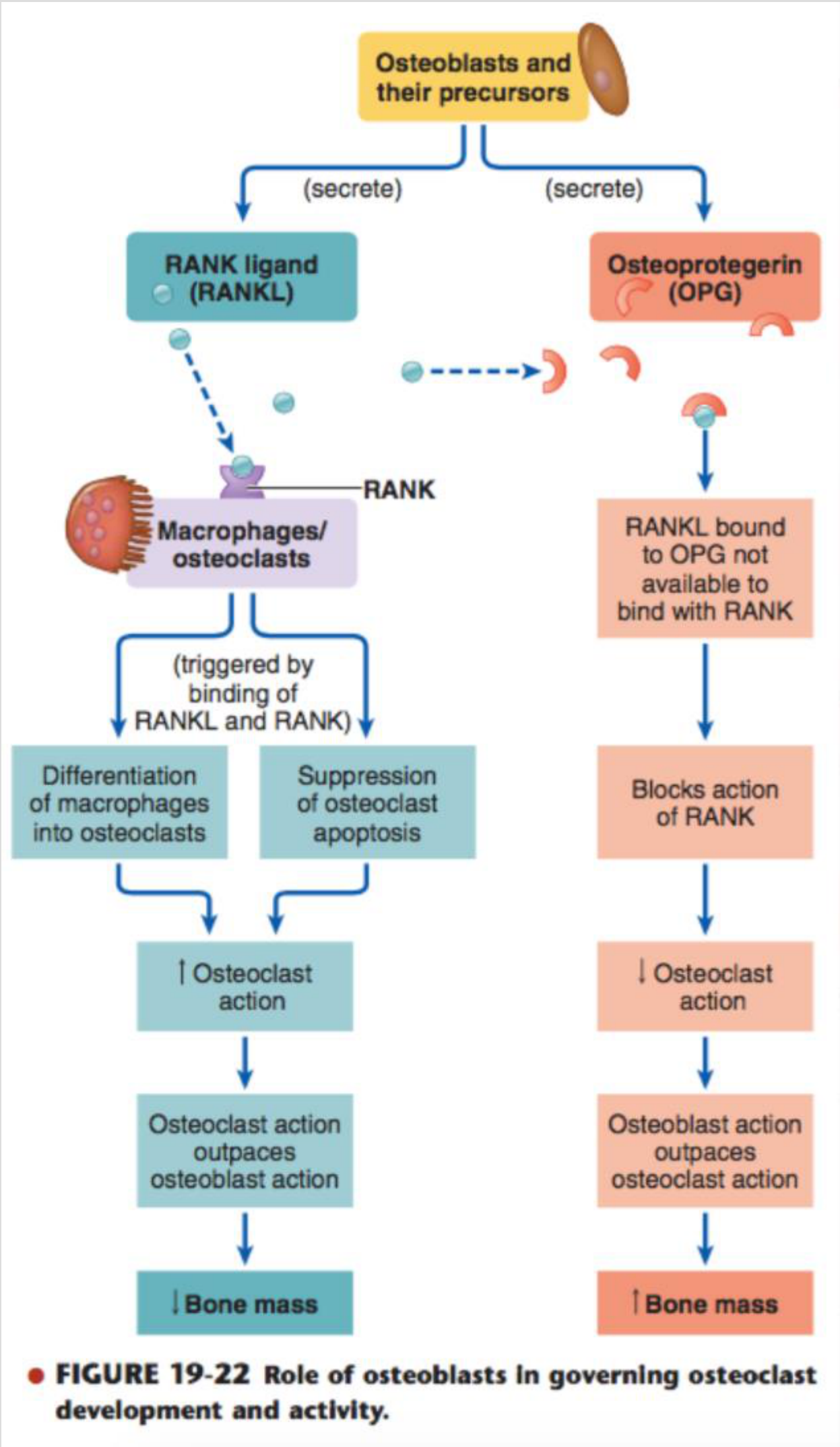
Role of Osteoblasts in Governing Osteoclast Activity11
- RANKL Pathway: Osteoblasts and their precursors secrete RANK ligand (RANKL), which binds to RANK on macrophages/osteoclasts. This triggers differentiation and suppresses apoptosis, leading to increased osteoclast action and decreased bone mass.
- OPG Pathway: Osteoblasts also secrete Osteoprotegerin (OPG), which acts as a decoy. RANKL bound to OPG is unavailable to bind with RANK. This blocks RANK action, allowing osteoblast activity to outpace osteoclast activity, leading to increased bone mass.
Summary of Denosumab Characteristics12
- Mechanism: Reversibly inhibits bone resorption by targeting RANKL; effects diminish within 6 months of cessation as it does not bind to bone.
- Indications:
- Osteoporosis (6-monthly SC).
- Metastatic bone disease (monthly).
- Giant cell tumors and fibrous dysplasia.
Pathophysiology Hypotheses13
MRONJ is a multifactorial process likely explained by several overlapping mechanisms:
Hypothesis Ordering
There are five main hypotheses regarding why MRONJ occurs, listed generally in order of likelihood based on current literature.
- Bone Remodelling Inhibition
- Inflammation or Infection
- Angiogenesis Inhibition
- Innate or Acquired Immune Dysfunction
- Genetic Factors
Bone Remodeling Inhibition
Impact of Antiresorptives14
- This is the leading hypothesis for MRONJ pathophysiology.
- While this strengthens bone against fractures, it prevents the normal micro-repair of the jawbone, making it susceptible to necrosis when challenged (e.g., by extraction).
- Antiresorptive medications directly affect osteoclast formation, differentiation, and function.
- Evidence:
- Animal models show absent osteoclasts in alveolar bone following treatment.
- Human specimens show non-functional osteoclasts surrounding necrotic bone in bisphosphonate (BP) treated patients.
- Drug Withdrawal Studies:
- Established ONJ in rodents did not resolve upon withdrawal of antiresorptives.
- However, discontinuing Denosumab (but not BPs) prior to extraction successfully prevented MRONJ development in rats.
Inflammation or Infection
Role of Dental Disease and Biofilm15
- Tooth extraction is the major inciting event, but most cases involve pre-existing periodontal or periapical disease.
- Infection drives the inflammatory process that leads to bone exposure.
- Inflammatory cytokines at MRONJ sites support the role of inflammation.
- Systemic Factors: Mice with induced Rheumatoid Arthritis (RA) showed more severe MRONJ features (increased bone resorption and necrosis).
- Bacterial Contribution:
- Bacteria on exposed necrotic bone contribute to disease severity.
- Poor oral hygiene and biofilm presence are associated with MRONJ development.
- Dental prophylaxis before initiating therapy can decrease prevalence. Clinical protocols focusing on biofilm reduction are important alternatives to surgical debridement.
Angiogenesis Inhibition
Vascular Impact16
- Bisphosphonates (e.g., zoledronic acid) inhibit angiogenesis in vitro and in vivo.
- Reduced vascularity leads to less oxygen and nutrition for the bone tissue, contributing to necrosis.
- Animal models show decreased vascularity and microvessel numbers at MRONJ sites and during socket healing.
- Both BPs and Denosumab decrease arterial and venous area in periodontal tissues.
- Antiangiogenic Medications: VEGF inhibitors, tyrosine kinase inhibitors, and immunomodulatory drugs are associated with MRONJ (though at a lower incidence than antiresorptives).
- Combination Therapy: Multiple Myeloma (MM) patients on both antiresorptive and antiangiogenic medications show a higher MRONJ prevalence.
Innate or Acquired Immune Dysfunction
Comorbidities and Therapeutic Interests17
- Patients with diabetes, RA, or immunocompromised states are at significantly higher risk for MRONJ.
- Patients who develop MRONJ are often older and have significant comorbidities. These systemic conditions impair healing and immune response, increasing risk.
- Mesenchymal Stem Cells (MSCs): There is therapeutic interest in using MSCs to overcome immune dysfunction. Preclinical studies show healing or prevention of MRONJ lesions after systemic infusion of adipose or bone marrow-derived MSCs.
Genetic Factors
Single-Nucleotide Polymorphisms (SNPs)18
- Evidence suggests a role for SNPs in genes associated with bone turnover, collagen formation, or metabolic bone diseases.
- Other implicated genes involve angiogenesis and immune response (e.g., PPAR gamma, CYP2C8).
- Current Consensus: Most studies document a weak or no association between measured genetic factors and MRONJ risk.
- Genetic predisposition is an area of research interest (e.g., SNPs), though currently, it represents a lower level of evidence compared to the other hypotheses.
Risk Factors for Medication-Related Osteonecrosis of the Jaws
 |  |
Overview of Risk Categories19
- Medication-related factors: (Cancer, Osteoporosis, and Non-malignant bone disease patients)
- Local factors
- Demographic and systemic factors
Medication-Related Factors
Risk in Oncology Patients20
- General Risk: MRONJ risk is higher in the malignancy group (<5%) compared to the osteoporosis group (<0.05%).
- Patients receiving IV bisphosphonates or Denosumab for multiple myeloma or bone metastases are at the highest risk.
- Zoledronate: Risk clusters <5% (range 0-18%), which is 2-10 times higher than placebo.
- Denosumab: Risk ranges from 0-6.9% (most studies <5%), comparable to zoledronate.
- Other Medications: Level 5 evidence (case reports) implicates other drugs, though a single etiologic agent is unlikely:
- Tyrosine Kinase Inhibitors (sunitinib)
- Monoclonal antibodies (bevacizumab)
- Fusion proteins (aflibercept)
- mTOR inhibitors (everolimus)
- Selective oestrogen receptor modulators (raloxifene)
- Immunosuppressants (methotrexate and corticosteroids)
Osteoporosis Patients
Risk Estimates
- Bisphosphonates:
- Clinical trials: 0.02-0.05% (Placebo: 0-0.2%).
- Studies show incidence rates ranging from 1 in 10,000 to 5 in 10,000, compared to placebo rates of 0 to 2 in 1,500; risk is not zero.
- IV Zoledronate: <0.02% (approx. 2 per 10,000).
- Oral Bisphosphonates: <0.05%.
- RANK-L Inhibitors:
- Denosumab: Reported at 0.3% (range 0.04-0.3) after 10 years of follow-up, which is significantly higher than BPs.
- Romosuzumab: 0.03-0.05%, comparable to alendronate.
Non-Malignant Bone Disease
Giant Cell Tumors and Pediatric Data
- Giant Cell Tumors: Denosumab treatment carries a risk of 0.7-5%, comparable to malignancy risks.
- Patients treated for conditions like Paget's disease also carry risk.
- Pediatric Population: Very limited data regarding osteogenesis imperfecta. One systematic review of 486 subjects found no cases of MRONJ, though sample sizes were small.
Duration of Therapy
Cumulative Exposure Risk
- Zoledronate (Cancer patients): Risk is 1.6-4% after 2 years, increasing to 3.8-18% after more than 2 years.
- Denosumab: Risk is 1.9% at <2 years, increasing to 6.9% after more than 2 years of exposure.
Summary of Risk Factors21
- Medication-related: Cancer, osteoporosis, and non-malignant bone disease.
- Local factors: Dento-alveolar operations, anatomic factors, and concomitant oral disease.
- Demographic and systemic factors.
Local Factors
Dento-alveolar Operations
- Tooth Extraction: The most common predisposing factor, cited in 62-82% of MRONJ cases.
- Risk Post-Extraction:
- Osteoporotic patients: BPs (0-0.15%), Denosumab (1%).
- Cancer patients: BPs (1.6-14.8%), similar to ORN risk in irradiated patients.
- Implants and Other Procedures:
- Risk for implants, endodontic, or periodontal procedures is unknown.
- AAOMS recommends caution in cancer patients and informing osteoporosis patients of low risks for MRONJ and implant failure.
- Implant Failure Types:
- Early: Triggered by surgery.
- Late: Triggered by the presence of the implant; often presents as “en bloc” failure where the implant is maintained within a sequestrum.
Anatomic Factors
Site and Appliance Factors
- Location: More common in the mandible (75%) than the maxilla (25%); both sites are involved in 4.5% of cases.
- The mandible is more commonly affected due to denser bone and poorer blood supply.
- Denture Use: Associated with increased MRONJ risk among cancer patients exposed to zoledronate.
Concomitant Oral Disease
Pre-existing Conditions
- Inflammatory dental diseases (periodontal or periapical pathology) are significant risk factors.
- Ill-fitting dentures cause ulceration penetrating to the periosteum, compromising blood supply; poor oral hygiene and plaque accumulation also drive risk.
- Among cancer patients with MRONJ, pre-existing dental disease was present in 50% of cases.
- Pre-existing disease may confound the relationship between extraction and MRONJ (i.e., whether the extraction caused the condition or simply exposed a pre-existing necrotic site).
Demographic and Systemic Factors
Systemic Influences22
- Sex: Higher prevalence in females, likely reflecting the demographics of osteoporosis and breast cancer.
- Age: Patients <24 years old treated for benign bone disease have not demonstrated MRONJ risk even after extended therapy.
- Corticosteroids: Associated with increased risk, especially when used with antiresorptives.
- Comorbidities: Conditions such as anaemia, diabetes, and specific cancer types are inconsistently reported as risk factors.
- Tobacco: Variably reported as a risk factor.
Clinical History Verification
Many patients are unaware they are on bone-affecting medications; dentists must actively query medical history. If history is unclear or risk is high, delay treatment and obtain a medical summary.
Risk Factor Summary
Key Risk Findings23
- The risk of MRONJ is significantly greater in cancer patients compared to osteoporosis patients.
- In osteoporosis patients, the risk remains very low regardless of drug type (BPs, Denosumab, romosozumab) or dosing schedule.
Assessment and Referral
Risk Evaluation24
Assessment should be based on:
- Reason for medication use.
- Dose and duration of therapy.
- Concomitant drug use.
- Surgical insult (e.g., number of teeth, periodontal status, location in maxilla/mandible).
Referral Strategy
For complex surgeries in high-risk patients, specialist referral reduces morbidity compared to general practice. Dentists should operate within their comfort level and contact oncologists for collaboration.
Management

Management Components25
- Treatment goals
- Prevention
- Treatment strategies (Non-operative and Operative)
Treatment Goals
Primary Objectives26
- Prevention of MRONJ.
- Prioritization of continued oncologic treatment and bone health (prevention of fragility fractures).
- Specific focus on not stopping medications that prevent hip fractures or manage cancer pain unnecessarily.
- Preservation of quality of life through:
- Patient education and reassurance.
- Pain control.
- Control of secondary infection.
- Prevention of lesion extension and new areas of necrosis.
Prevention
Pre-treatment Management27
- Multidisciplinary Approach: Coordinated dental care is essential before starting antiresorptive therapy.
- Oral Health Optimization: Early screening and treatment of acute or potential infection sites.
- Patients educated to report sore spots (e.g., from dentures) early to prevent ulceration and periosteal disruption.
- Assessment Factors: Evaluate patient motivation, fluoride needs, tooth mobility, periodontal status, root fragments, caries, and denture stability (especially the posterior lingual flange).
- Timing: If systemic conditions allow, delay antiresorptive therapy until dental health is optimized and surgical sites have mucosalized or achieved adequate osseous healing.
Drug Holidays and Biomarkers28
- Drug Holidays: The practice of suspending medication to mitigate risk is recommended by some societies, but evidence remains inconclusive.
- Risks include loss of antiresorptive efficacy and fragility fractures.
- RANKL Inhibitor Caution: Cessation in osteoporosis patients can cause a rebound increase in bone resorption and multilevel vertebral fractures.
- Timing: Planned surgery may be performed 3-4 months after the last dose (when inhibition wanes) and reinstituted 6-8 weeks post-surgery.
- Bone Turnover Markers: No biomarkers are currently validated for clinical decision-making.
- The CTX test (C-terminal telopeptide) measures bone turnover and is used in some regions (e.g., South Australia) to assess risk, though its value is debated elsewhere.
Treatment Strategies

Clinical Considerations29
- Decisions must be patient-specific, weighing the risk-benefit ratio and quality of life.
- Treatment aggressiveness depends on overall prognosis (e.g., palliative comfort for Stage 4 cancer vs. aggressive treatment for healthy 60-year-old).
- Factors include the ability to perform wound care, surgical morbidity, and post-resection oral function.
- Imaging: 3D imaging is critical for identifying sequestra and planning less invasive surgery.
Case Context30
- Example: 72-year-old male, 6 months of Denosumab for osteoporosis
Case Study: Management of Stage 1 MRONJ
- Patient: 72-year-old gentleman on 6-monthly Denosumab for osteoporosis.
- Presentation: Tooth 3.5 extracted 3.5 months prior with slow healing socket and mucosal defect.
- Symptoms: No pain, discharge, pus, or sequestra.
- Management: Non-operative approach (monitoring, chlorhexidine rinses, regular dental review).
- Lesson: Not all exposed bone requires surgery. .
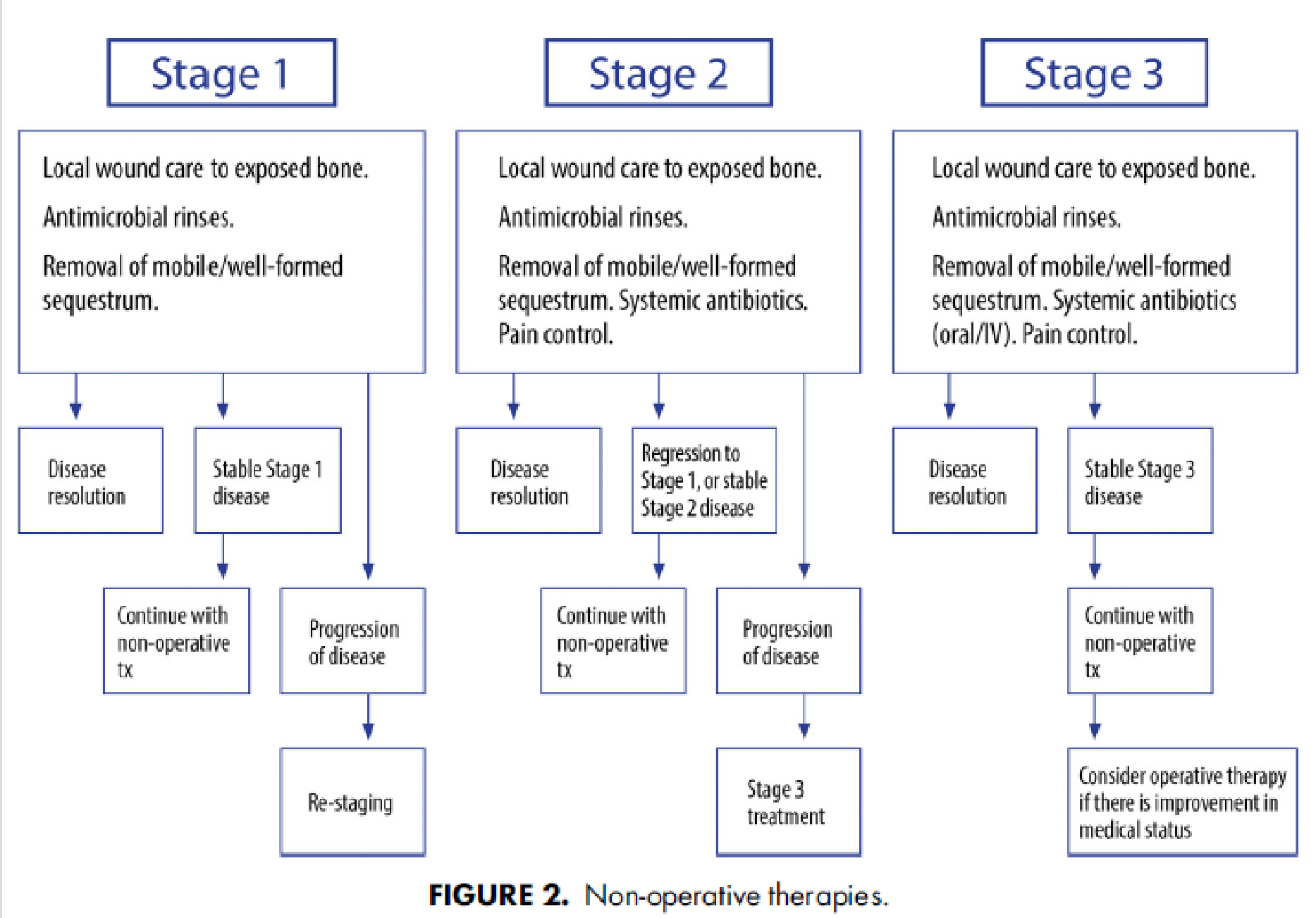
Non-Operative Therapy
Protocol by Stage
- Stage 1: Local wound care, antimicrobial rinses, and removal of mobile/well-formed sequestrum. If resolved or stable, continue non-operative care.
- Stage 2: Local wound care, antimicrobial rinses, removal of mobile sequestrum, systemic antibiotics, and pain control. If disease progresses, restage for Stage 3 treatment.
- Stage 3: Local wound care, antimicrobial rinses, removal of mobile sequestrum, systemic antibiotics (oral/IV), and pain control. Consider operative therapy if medical status allows.
Efficacy and Surveillance
- Non-operative therapy is useful for all stages, particularly when comorbidities preclude surgery.
- Many patients can remain stable without progression if hygiene is maintained.
- Stage 1 Focus: Chlorhexidine rinses and biofilm removal; surgery is often not indicated if asymptomatic.
- Stage 2 Focus: Symptom control via antibiotics. Adjunctive therapies (HBO, ozone, Vitamin E, pentoxifylline) lack strong evidence; trials are ongoing.
- Surveillance: Active clinical and radiographic monitoring is essential to detect progression early.
Operative Therapy
Indications and Techniques
- Operative therapy is a viable option with high success rates across all stages, improving quality of life and allowing resumption of medication.
- Medication cessation is often decided by the prescribing specialist (oncologist/endocrinologist), not the dentist alone.
- Surgical Timing: For progressive or advanced disease, resection should be performed without prolonged non-operative delays.
- Resection Margins: Segmental or marginal resections require margins extending to vital, bleeding bone.
- Comorbidities: Physiologically compromised patients (e.g., those with distant metastases) may have a higher risk of refractory disease.
- Drug Holiday: The benefit of a pre-operative drug holiday has not been substantiated.
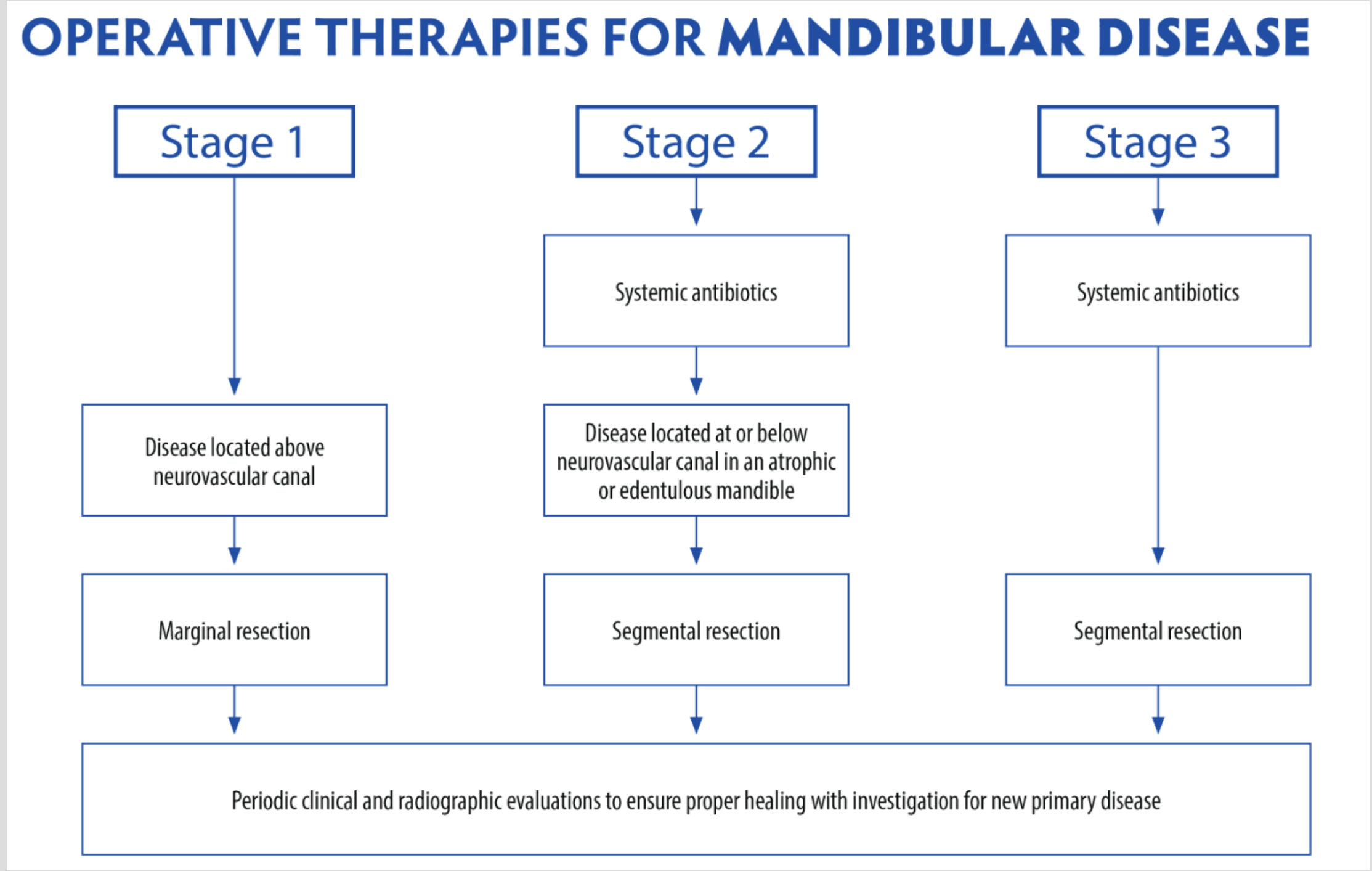
Operative Therapies for Mandibular Disease
Mandibular Surgical Management
- Stage 1: Marginal resection (if disease is located above the neurovascular canal).
- Stage 2:
- Systemic antibiotics.
- Segmental resection (if disease is at or below the neurovascular canal in an atrophic/edentulous mandible).
- Stage 3:
- Systemic antibiotics.
- Segmental resection.
Note: All stages require periodic clinical and radiographic evaluation to ensure healing and monitor for new disease.
- Defects larger than 2.5 cm often require a free flap (e.g., fibula free flap) involving microsurgical connection to facial vessels.
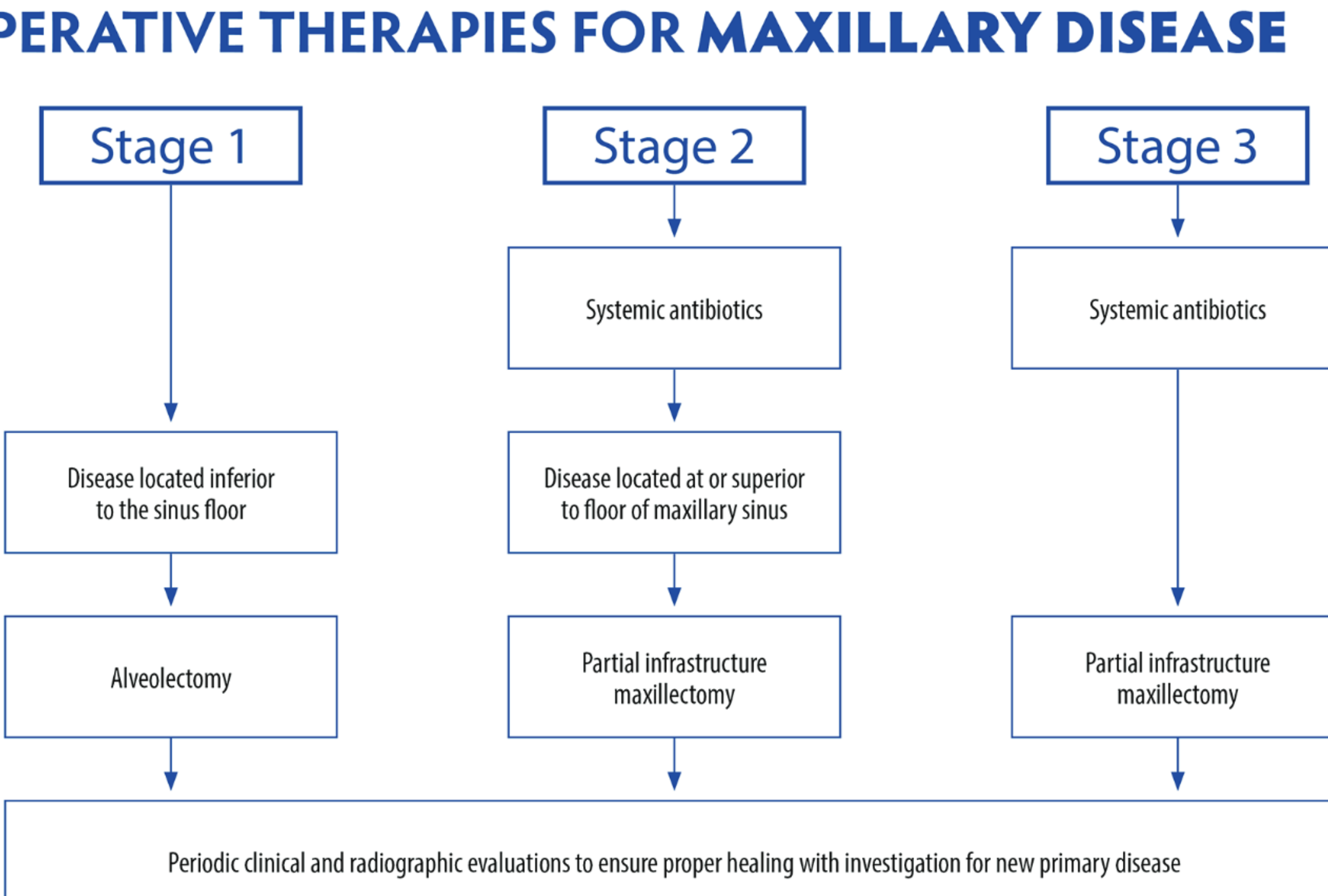
Operative Therapies for Maxillary Disease
Maxillary Surgical Management
- Stage 1: Alveolectomy (if disease is located inferior to the sinus floor).
- Stage 2:
- Systemic antibiotics.
- Partial infrastructure maxillectomy (if disease is at or superior to the floor of the maxillary sinus).
- Stage 3:
- Systemic antibiotics.
- Partial infrastructure maxillectomy.
Note: Periodic clinical and radiographic evaluations are required to ensure proper healing and investigate for new primary disease.
- Surgery is more conservative in the maxilla to preserve critical structures like the orbital floor.
Scheduled Break31
- Duration: 15 minutes
Audio Appendix
Additional Audio Content
The following sections from the lecture audio did not correspond to any heading in the main document.
Clinical Overview
Footnotes
-
Original PDF page 1: W2.1 MRONJ, p.1 ↩
-
Original PDF page 3: W2.1 MRONJ, p.3 ↩
-
Original PDF page 4: W2.1 MRONJ, p.4 ↩
-
Original PDF page 2: W2.1 MRONJ, p.2 ↩
-
Original PDF page 5: W2.1 MRONJ, p.5 ↩
-
Original PDF page 6: W2.1 MRONJ, p.6 ↩
-
Original PDF page 7: W2.1 MRONJ, p.7 ↩
-
Original PDF page 8: W2.1 MRONJ, p.8 ↩
-
Original PDF page 13: W2.1 MRONJ, p.13 ↩
-
Original PDF page 14: W2.1 MRONJ, p.14 ↩
-
Original PDF page 15: W2.1 MRONJ, p.15 ↩
-
Original PDF page 16: W2.1 MRONJ, p.16 ↩
-
Original PDF page 17: W2.1 MRONJ, p.17 ↩
-
Original PDF page 18: W2.1 MRONJ, p.18 ↩
-
Original PDF page 19: W2.1 MRONJ, p.19 ↩
-
Original PDF page 20: W2.1 MRONJ, p.20 ↩
-
Original PDF page 21: W2.1 MRONJ, p.21 ↩
-
Original PDF page 22: W2.1 MRONJ, p.22 ↩
-
Original PDF page 23: W2.1 MRONJ, p.23 ↩
-
Original PDF page 24: W2.1 MRONJ, p.24 ↩
-
Original PDF page 28: W2.1 MRONJ, p.28 ↩
-
Original PDF page 32: W2.1 MRONJ, p.32 ↩
-
Original PDF page 33: W2.1 MRONJ, p.33 ↩
-
Original PDF page 34: W2.1 MRONJ, p.34 ↩
-
Original PDF page 35: W2.1 MRONJ, p.35 ↩
-
Original PDF page 36: W2.1 MRONJ, p.36 ↩
-
Original PDF page 37: W2.1 MRONJ, p.37 ↩
-
Original PDF page 38: W2.1 MRONJ, p.38 ↩
-
Original PDF page 39: W2.1 MRONJ, p.39 ↩
-
Original PDF page 40: W2.1 MRONJ, p.40 ↩
-
Original PDF page 46: W2.1 MRONJ, p.46 ↩