Prevention and Management of Osteoradionecrosis in Patients With Head and Neck Cancer Treated With Radiation Therapy: ISOO-MASCC-ASCO Guideline
Osteoradionecrosis (ORN) is characterized by the following clinical and radiographic criteria:
Definition of Osteoradionecrosis1
- Radiographic evidence of a lytic or mixed sclerotic lesion of the bone.
- Visibly exposed bone or bone that can be probed through a periodontal probe or fistula.
- The condition must occur at an anatomical site previously exposed to radiotherapy (RTx).
Clinical Context
While most common in the head and neck, ORN is also observed in the thorax and long bones. When radiation history is present, clinicians must investigate the specific cancer treated, the radiation dose administered, and the exact radiation fields.
Guideline Authors2
-
Douglas E. Peterson, DMD, PhD, FDS RCSEd, FASCO (University of Connecticut Health)
-
Shlomo A. Koyfman, MD (Cleveland Clinic)
-
Noam Yarom, DMD, MPH (Tel-Aviv University; Sheba Medical Center)
-
Charlotte Duch Lynggaard, MD, PhD (Rigshospitalet, Copenhagen University Hospital)
-
Nofisat Ismaıla, MD, MSc (American Society of Clinical Oncology)
-
Lone E. Forner, DDS, PhD (Rigshospitalet, Copenhagen University Hospital)
-
Clifton David Fuller, MD, PhD (The University of Texas MD Anderson Cancer Center)
-
Yvonne M. Mowery, MD, PhD (Duke University Medical Center; Durham VA Health Care System)
-
Barbara A. Murphy, MD (Vanderbilt University Medical Center)
-
Erin Watson, DMD, MHSc (Princess Margaret Cancer Centre)
-
David H. Yang, DDS, FRCD(C) (BC Cancer)
-
Ivan Alajbeg, DMD, MSc, PhD (University of Zagreb)
-
Paolo Bossi, MD (University of Brescia; ASST Spedali Civili di Brescia)
-
Michael Fritz, MD (Cleveland Clinic)
-
Neal D. Futran, MD, DMD (University of Washington)
-
Daphna Y. Gelblum, MD (Memorial Sloan Kettering Cancer Center)
-
Edward King, JD (Patient Representative)
-
Salvatore Ruggiero, DMD, MD, FACS (New York Center for Orthognathic and Maxillofacial Surgery)
-
Derek K. Smith, DDS, PhD, MPH (Vanderbilt University Medical Center)
-
Alessandro Villa, DDS, MPH, PhD (University of California San Francisco)
-
Jonn S. Wu, BMSc, MD, FRCPC (BC Cancer)
-
Deborah Saunders, DMD (Health Sciences North
-
Guidelines published around 2022
-
Collaboration between ASCO, ISOO, and MASCC
-
Derived from systematic reviews and higher-level evidence papers)
DOI: https://doi.org/10.1200/JCO.23.02750
Literature Search and Study Characteristics
Methodology
The guideline development process involved a comprehensive review of existing literature to establish evidence-based protocols.
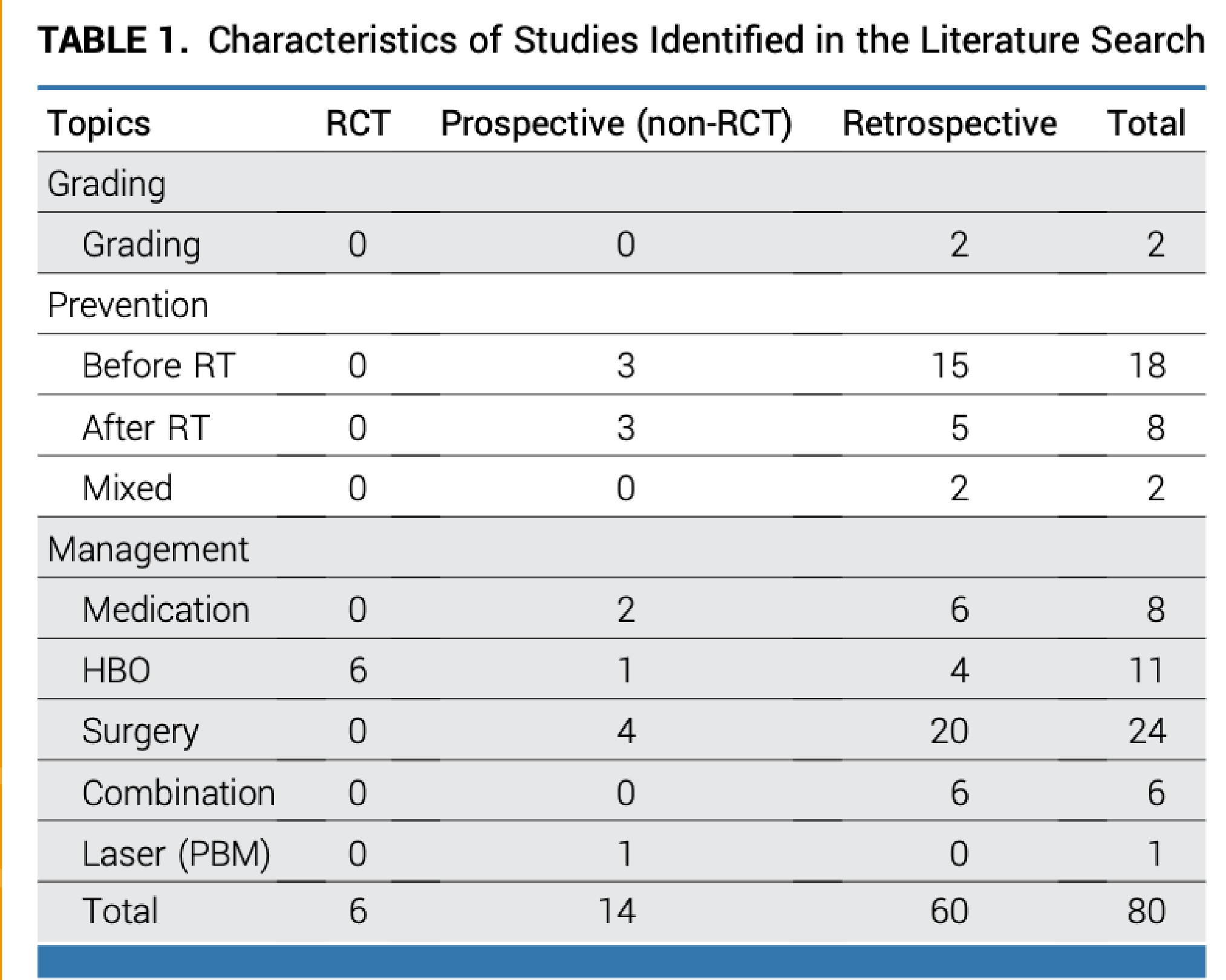
Literature Search Summary3
| Topics | RCT | Prospective (non-RCT) | Retrospective | Total |
|---|---|---|---|---|
| Grading | 0 | 0 | 2 | 2 |
| Prevention | ||||
| Before RT | 0 | 3 | 15 | 18 |
| After RT | 0 | 3 | 5 | 8 |
| Mixed | 0 | 0 | 2 | 2 |
| Management | ||||
| Medication | 0 | 2 | 6 | 8 |
| HBO | 6 | 1 | 4 | 11 |
| Surgery | 0 | 4 | 20 | 24 |
| Combination | 0 | 0 | 6 | 6 |
| Laser (PBM) | 0 | 1 | 0 | 1 |
| Total | 6 | 14 | 60 | 80 |
Abbreviations: RCT, randomized controlled trial; RT, radiation therapy; HBO, hyperbaric Oxygen; PBM, photobiomodulation.
- Methodology: The authors conducted a series of systematic reviews and analyzed higher-level evidence papers.
- Scope of Review: The studies included focused on characterization of ORN, prevention strategies (pre- and post-radiotherapy), and treatment modalities (both surgical and non-surgical) for established ORN.
Key Study Questions4
- How should ORN be characterized, graded, and reported?
- The primary objectives of the guideline and associated literature review were to address how we characterize osteoradionecrosis.
- What are the recommended best practices for the prevention of ORN of the head and neck prior to radiation therapy?
- What are the recommended best practices for the prevention of ORN after radiation therapy?
- The review focused on how we prevent osteoradionecrosis and how we treat patients once they have developed the condition.
- How should ORN be managed nonsurgically?
- How should ORN be managed surgically?
- The study specifically evaluated the efficacy and protocols for surgical versus non-surgical interventions.
- When, how, and by whom should patients diagnosed with ORN be assessed for adverse events associated with and/or caused by ORN?
Characterization and Grading of Osteoradionecrosis
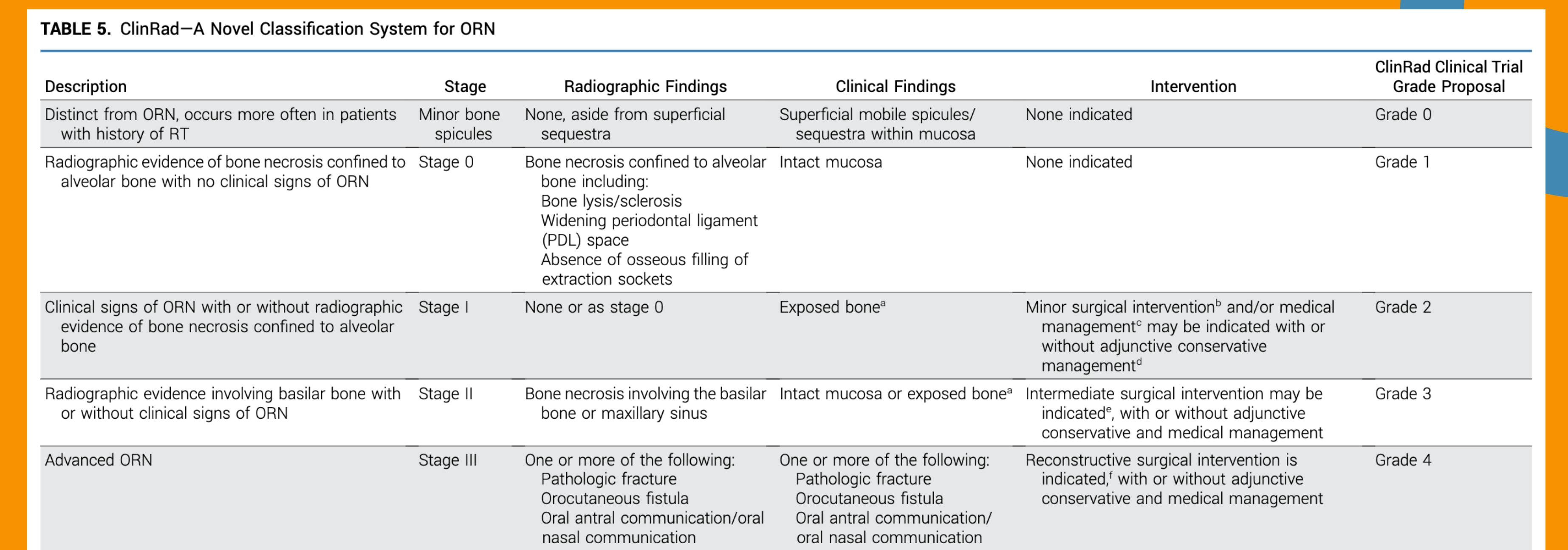
Overview of the ClinRad Model5
The ClinRad system was developed to provide a standardized, risk-based model for the classification of osteoradionecrosis (ORN) in head and neck cancer patients.
Historical Context: Notani Classification
Historically, the Notani system was used for its simplicity, categorizing ORN into three stages: Stage 1 (alveolar bone), Stage 2 (beyond alveolar bone), and Stage 3 (fracture or fistula). The ClinRad system is now preferred as it integrates imaging data with clinical findings to better guide specific interventions.
ClinRad Classification System
| Description | Stage | Radiographic Findings | Clinical Findings | Intervention | ClinRad Grade |
|---|---|---|---|---|---|
| Distinct from ORN; occurs more often in patients with history of RT | Minor bone spicules | None, aside from superficial sequestra | Superficial mobile spicules/sequestra within mucosa | None indicated | Grade 0 |
| Radiographic evidence of bone necrosis confined to alveolar bone; no clinical signs | Stage 0 | Bone necrosis (lysis/sclerosis, widened PDL space, lack of socket filling) | Intact mucosa | None indicated | Grade 1 |
| Clinical signs of ORN with or without alveolar bone necrosis | Stage I | None or as stage 0 | Exposed bone* | Minor surgical intervention** and/or medical management*** | Grade 2 |
| Radiographic evidence involving basilar bone or without clinical signs | Stage II | Bone necrosis involving the basilar bone or maxillary sinus | Intact mucosa or exposed bone* | Intermediate surgical intervention**** | Grade 3 |
| Advanced ORN | Stage III | Pathologic fracture, orocutaneous fistula, or oral antral/nasal communication | Pathologic fracture, orocutaneous fistula, or oral antral/nasal communication | Reconstructive surgical intervention***** | Grade 4 |
Notes on Findings and Interventions:
- *Includes pinpoint mucosal breach (intraoral fistula) probing to bone or probing along periodontal tissues.
- **Examples: sequestrectomy.
- ***Examples: pentoxifylline-tocopherol, hyperbaric oxygen, chlorhexidine rinses, and antibiotics.
- ****Examples: transoral surgical intervention, debridement, alveolectomy, and soft tissue closure.
- *****Examples: segmental maxillectomy/mandibulectomy with vascularized free tissue reconstruction.
Clinical Recommendations for Grading and Workup
Characterization and Risk Assessment6
-
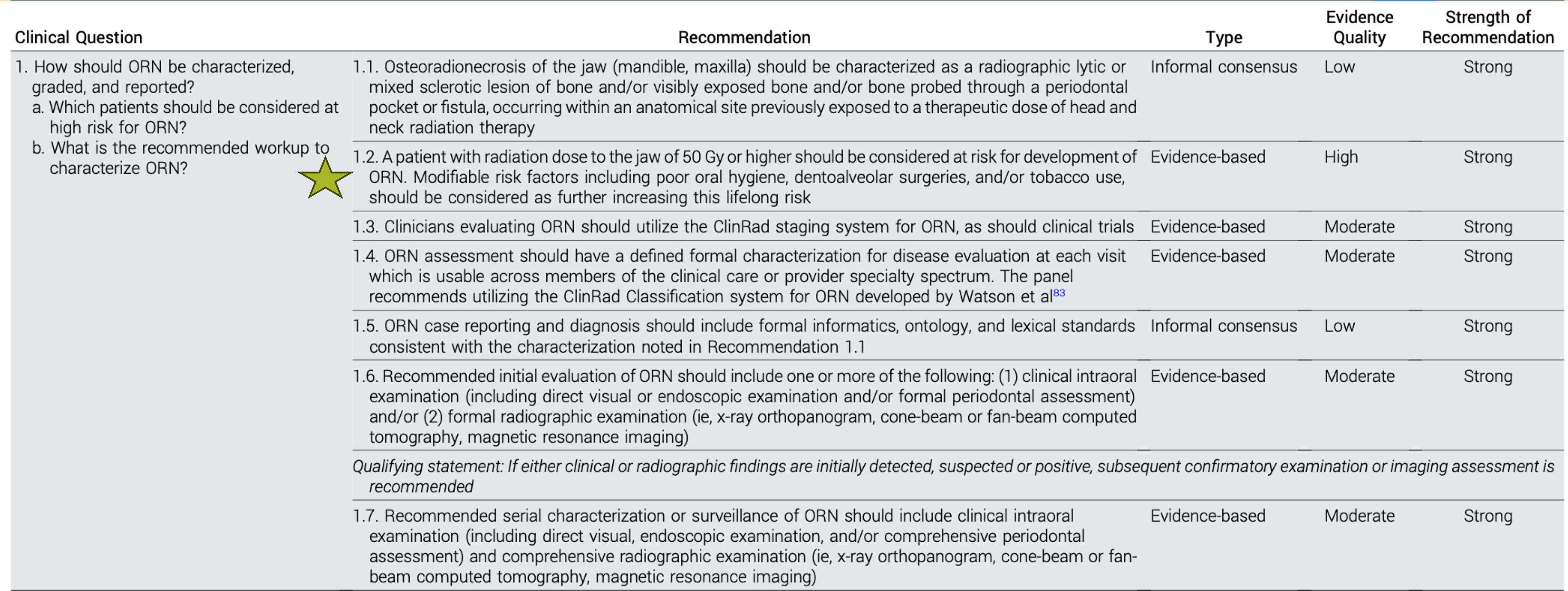
1.1. Definition: Osteoradionecrosis (ORN) of the jaw should be characterized as a radiographic lytic or mixed sclerotic lesion of bone and/or visibly exposed bone and/or bone probed through a periodontal pocket or fistula, occurring within an anatomical site previously exposed to therapeutic head and neck radiation. (Type: Informal consensus; Quality: Low; Strength: Strong)
-
1.2. Risk Factors: Patients receiving a radiation dose to the jaw of 50 Gy or higher are at risk. Modifiable factors such as poor oral hygiene, dentoalveolar surgeries, and tobacco use further increase this lifelong risk. (Type: Evidence-based; Quality: High; Strength: Strong)
-
Pathophysiology (The 3 Hs): Radiation damage is characterized by hypoangiogenesis, hypocellularity, and hypoxia.
-
Risk Progression: Unlike other bone pathologies, radiation damage does not improve; the risk of ORN increases over time (e.g., risk at 10 years is higher than at 1 year).
Staging and Reporting Standards
- 1.3. Staging System: Clinicians and clinical trials should utilize the ClinRad staging system for ORN. (Type: Evidence-based; Quality: Moderate; Strength: Strong)
- 1.4. Formal Characterization: ORN assessment must have a defined formal characterization usable across all clinical specialties. The panel recommends the ClinRad Classification system. (Type: Evidence-based; Quality: Moderate; Strength: Strong)
- 1.5. Informatics Standards: Case reporting and diagnosis should include formal informatics, ontology, and lexical standards consistent with Recommendation 1.1. (Type: Informal consensus; Quality: Low; Strength: Strong)
Evaluation and Surveillance
- 1.6. Initial Evaluation: Should include clinical intraoral examination (visual, endoscopic, or periodontal assessment) and/or formal radiographic examination (orthopanogram, CT, or MRI). (Type: Evidence-based; Quality: Moderate; Strength: Strong)
- Qualifying statement: If findings are suspected or positive, subsequent confirmatory examination or imaging is recommended.
Case Study: Risk Assessment and Referral Efficiency
Scenario: A patient with a history of Tonsil SCC requires an extraction. A new graduate might refer immediately due to liability concerns. Assessment: Upon requesting radiation maps, it is found the radiation targeted the oropharynx with no jaw involvement. Outcome: The general dentist performs the extraction safely, saving the patient significant costs and avoiding specialist burden.
> [!tip] Verifying Radiation Fields
> Clinicians should ==request radiation field maps== from oncology departments (via hospital switchboards or private rooms). If the radiation was localized (e.g., top of skull) with ==no involvement of the jaws==, the risk for ORN during dental extractions is significantly lower, potentially avoiding unnecessary specialist referrals.
- 1.7. Serial Surveillance: Recommended monitoring includes clinical intraoral examination and comprehensive radiographic examination (orthopanogram, CT, or MRI). (Type: Evidence-based; Quality: Moderate; Strength: Strong)
Case Study: Spontaneous ORN in Reconstructed Mandible
Scenario: A patient received a fibula free flap reconstruction followed by radiation therapy. Complication: The patient developed spontaneous ORN within the fibula graft despite compliance. Consequences: This is a disastrous complication often requiring the removal of the necrotic graft and harvesting a second fibula for reconstruction.
Pre-Radiotherapy Prevention Strategies
Clinical Protocols Before Radiation Therapy7
- Use IMRT to reduce the radiation dose to the bone to less than 50 Gy.
- Conduct a comprehensive dental or hospital dentist review prior to radiotherapy.
- Extract teeth with poor prognosis or moderate-to-severe periodontal disease within the radiation field.
- Consider extraction of teeth with periapical disease, caries, and partially erupted third molars, depending on individual patient factors and time available for healing.
- Ideally, allow at least 2 weeks of healing prior to radiotherapy, provided it does not delay the start of cancer treatment.
- Root Canal Viability: Endodontic treatment is permissible pre-radiation if the tooth has a good long-term prognosis; however, retreatment cases or those with significant bone loss should be extracted.
- Optimal Healing Window: While 2 weeks is the minimum for mucosal closure, 4 to 6 weeks is preferred to allow for bone healing if cancer treatment timelines permit.
- Aim to complete extractions prior to mask fabrication if the procedure will alter the vertical dimension (VD).
- Prescribe high-fluoride toothpaste.
Post-Radiotherapy Surgical Prevention
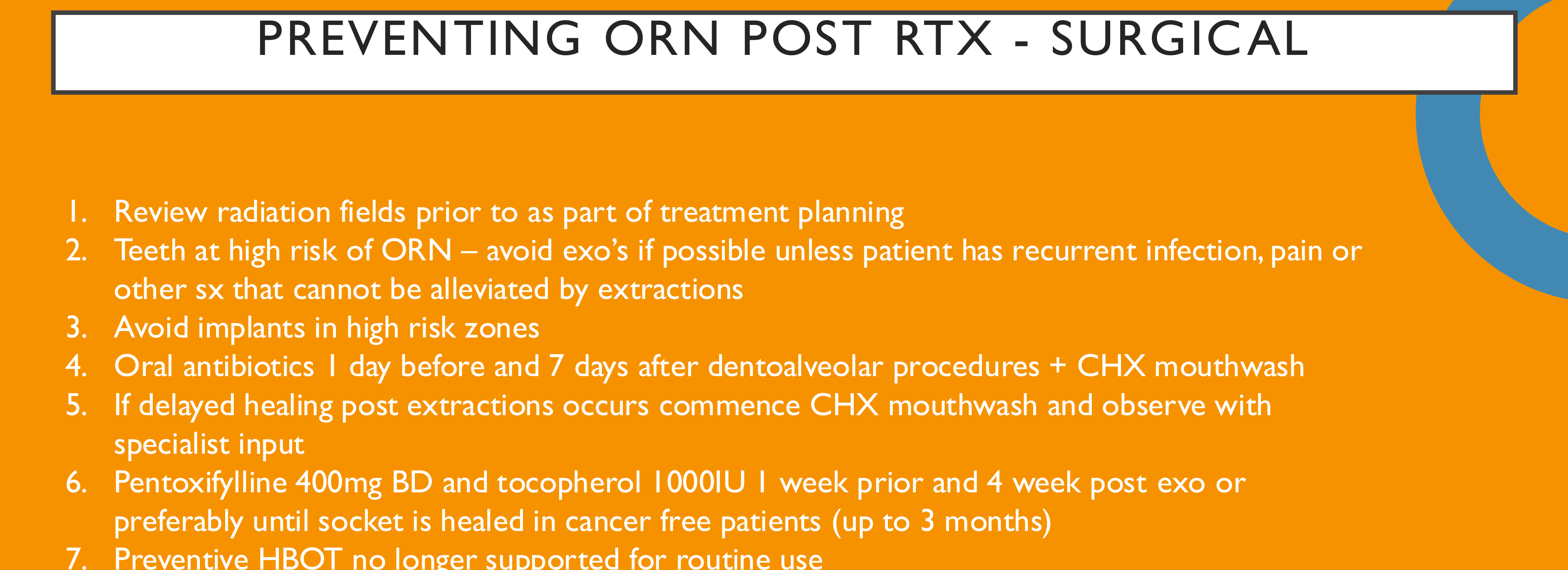
Surgical Protocols After Radiation Therapy8
-
Review radiation fields as part of treatment planning prior to any surgical procedure.
-
For teeth at high risk of ORN, avoid extractions if possible unless the patient has recurrent infection, pain, or other symptoms that cannot be otherwise alleviated.
-
Avoid dental implants in high-risk radiation zones.
-
Root Burying (Decoronation): For compromised teeth where extraction is high-risk, consider decoronation and root canal treatment of the roots to bury them under the mucosa, avoiding irradiated bone trauma.
-
Administer oral antibiotics 1 day before and 7 days after dentoalveolar procedures, supplemented with chlorhexidine (CHX) mouthwash.
-
If delayed healing occurs post-extraction, commence CHX mouthwash and observe with specialist input.
-
Administer Pentoxifylline (400mg BD) and Tocopherol (1000IU) starting 1 week prior and continuing 4 weeks post-extraction, or preferably until the socket is healed in cancer-free patients (up to 3 months).
- PENTOCLO Protocol: This combination is increasingly used both for prevention and treatment of established ORN to improve vascular supply.
- Preventive hyperbaric oxygen therapy (HBOT) is no longer supported for routine use.
Non-Surgical Treatment Modalities
Pharmacological Management9
- Pentoxifylline: May be used in cancer-free patients. It is potentially beneficial when combined with tocopherol, antibiotics, and prednisolone.
- Mechanism: Promotes vasodilation, improves RBC deformation, and acts as an antifibrotic by inhibiting TNF-alpha.
- Dosage: 400mg BD from 3 months pre-extraction until healed.
- Tocopherol (Vitamin E): Used to scavenge free radicals.
Adjunctive Therapy
- Hyperbaric Oxygen Therapy (HBOT): May be used in conjunction with surgical management in cancer-free patients. It shows the most potential benefit in mild cases.
Surgical Treatment Modalities
 |  |
 |  |
Surgical Intervention Strategies10
- Early Stage (ClinRad Stage 1 or 2): Initiate treatment with transoral minor interventions, including debridement, sequestrectomy, alveolectomy, and soft tissue flap closure.
- Advanced Stage (ClinRad Stage 2, 3, or 4): Segmental resection and free flap reconstruction are recommended, especially if the lesion is greater than 2.5 cm in length.
- Sequestra Management: Removal of superficial bony sequestra should be performed if assessed as low risk by the clinic. Reducing the disease burden and biofilm environment can act synergistically with ongoing systemic therapy.
MDT Considerations
Surgical decision-making involves a Multidisciplinary Team (MDT). Key factors for radical surgery include the patient’s living situation, caregiver support, and ability to withstand a 10-hour operation.
Conservative Surgical Interventions11
Conservative surgical approaches are typically employed for early-stage osteoradionecrosis (ORN) or as a preliminary measure to control infection and stabilize the affected area. These interventions include:
- Sequestrectomy and Debridement: Removal of necrotic bone fragments (sequestra) and infected soft tissue to promote healing of the surrounding healthy structures.
- Clinical Outcomes: While conservative surgery may provide symptomatic relief, the success rates vary depending on the extent of the disease and the vascularity of the remaining tissue.
Radical Surgical Resection and Reconstruction
For advanced or refractory ORN (Stages II and III), more extensive surgical procedures are often required to restore function and aesthetics.
- Segmental Mandiburectomy: Complete removal of the involved segment of the mandible when the bone is fractured or extensively necrotic.
- Microvascular Free Tissue Transfer: This is considered the gold standard for reconstructing large defects. Common donor sites include:
- Fibula free flap (preferred for long bony defects).
- Radial forearm osteocutaneous flap.
- Scapular flap.
- Benefits of Vascularized Bone Grafts: Unlike non-vascularized grafts, free flaps bring a new blood supply to the irradiated field, which is critical for successful healing and integration in a hypoxic environment.
Surgical Adjuncts and Considerations
- Antibiotic Prophylaxis: Perioperative antibiotics are standard practice to manage secondary infections, although they do not treat the underlying radiation-induced bone damage.
- Pathologic Fractures: The presence of an orocutaneous fistula or a pathologic fracture generally necessitates radical resection rather than conservative management.
- Timing of Intervention: Early identification and surgical referral are crucial for patients who do not respond to conservative medical management to prevent further bone loss and soft tissue complications.
Advice for New Graduates
For acute issues like a buccal abscess in a rural setting, call a specialist registrar for immediate management advice (e.g., incision and drainage) rather than just referring. Build extraction skills on healthy patients before managing high-risk head and neck cancer cases.
Case Study: Management of Oroantral Communication (OAC) Risk
Scenario: Extraction of an upper molar with roots near the sinus. Technique: If the tooth is immobile, section the tooth to allow for quicker removal with less force, reducing the risk of a large OAC. Inform the patient that small holes often heal with sinus precautions in healthy patients.
Footnotes
-
Original PDF page 1: W2.2 ORN, p.1 ↩
-
Original PDF page 2: W2.2 ORN, p.2 ↩
-
Original PDF page 3: W2.2 ORN, p.3 ↩
-
Original PDF page 4: W2.2 ORN, p.4 ↩
-
Original PDF page 5: W2.2 ORN, p.5 ↩
-
Original PDF page 6: W2.2 ORN, p.6 ↩
-
Original PDF page 7: W2.2 ORN, p.7 ↩
-
Original PDF page 8: W2.2 ORN, p.8 ↩
-
Original PDF page 9: W2.2 ORN, p.9 ↩
-
Original PDF page 10: W2.2 ORN, p.10 ↩
-
Original PDF page 11: W2.2 ORN, p.11 ↩