Case 1:
- Patient is healthy
- Had root canal filling done 1 month ago and radiolucent area hasn’t resolved
Treatment Plan
- Is it going to be a re-endodontic treatment?
Quality of endo?
- Will the radiolucency resolve with re-treatment
- Probably not it might be an incisive canal cyst
- The lesion is too big it probably won’t resolve
Next steps
- Cone beam CT to properly diagnose the type of cyst
- Cyst is probably benign because its well corticated
Case 2 OPG 
Case 2 OPG
- Patient is fit and well
OPG analysis
- Periapical radiolucency spanning from 11 - 15
Next Steps
- More imaging :
- CBCT or CT
- probably ameloblastoma
Case 3 OPG
#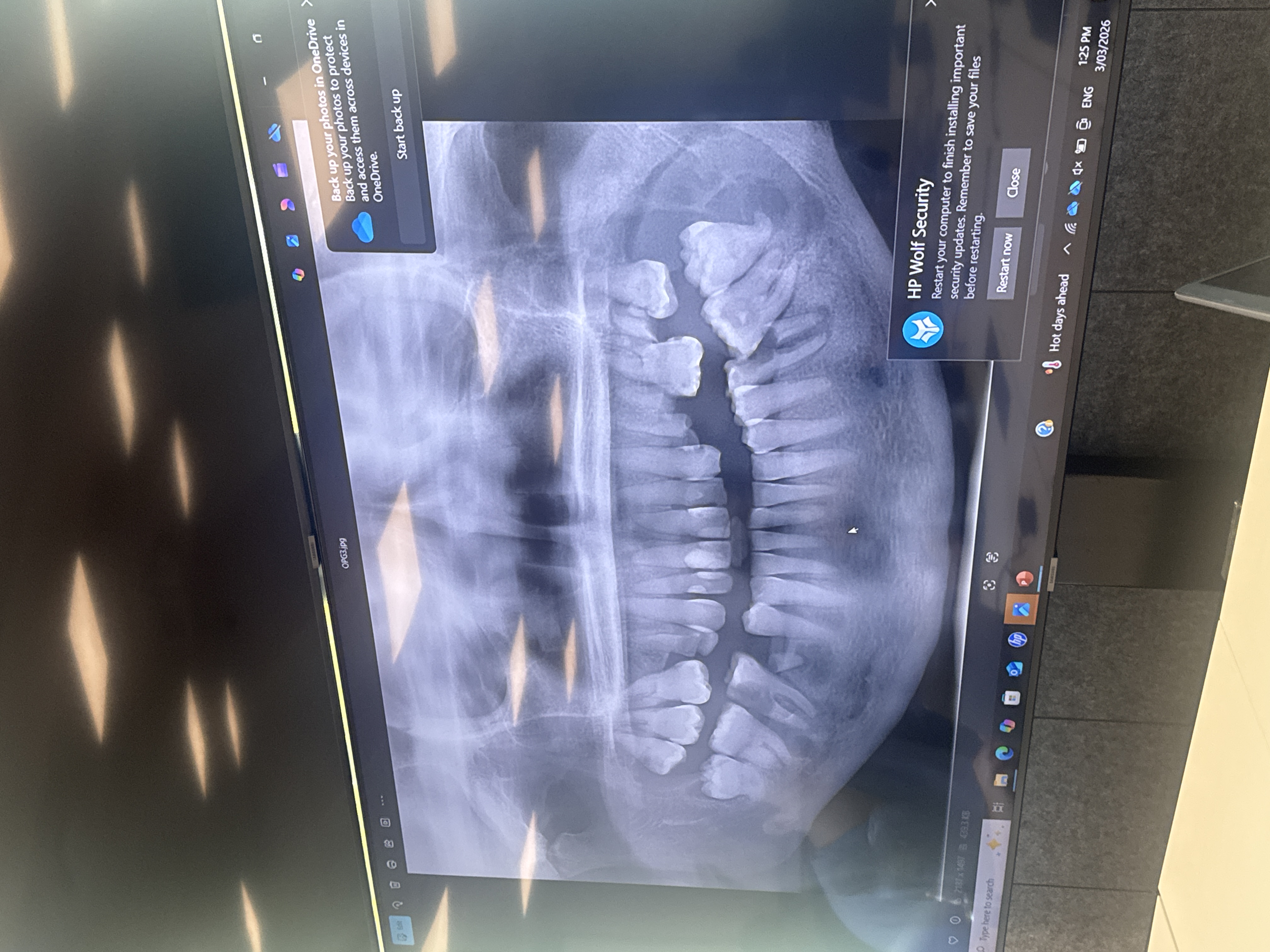
- Lesions on 46, 47, 37, 36
Patient consideration
- Patient has kidney disease
- Kidneys secrete hormones that allow you to absorb calcium
- this patient is low in calcium!
- That is the the cause of the lesion between the 46 and 47
Case 4 OPG
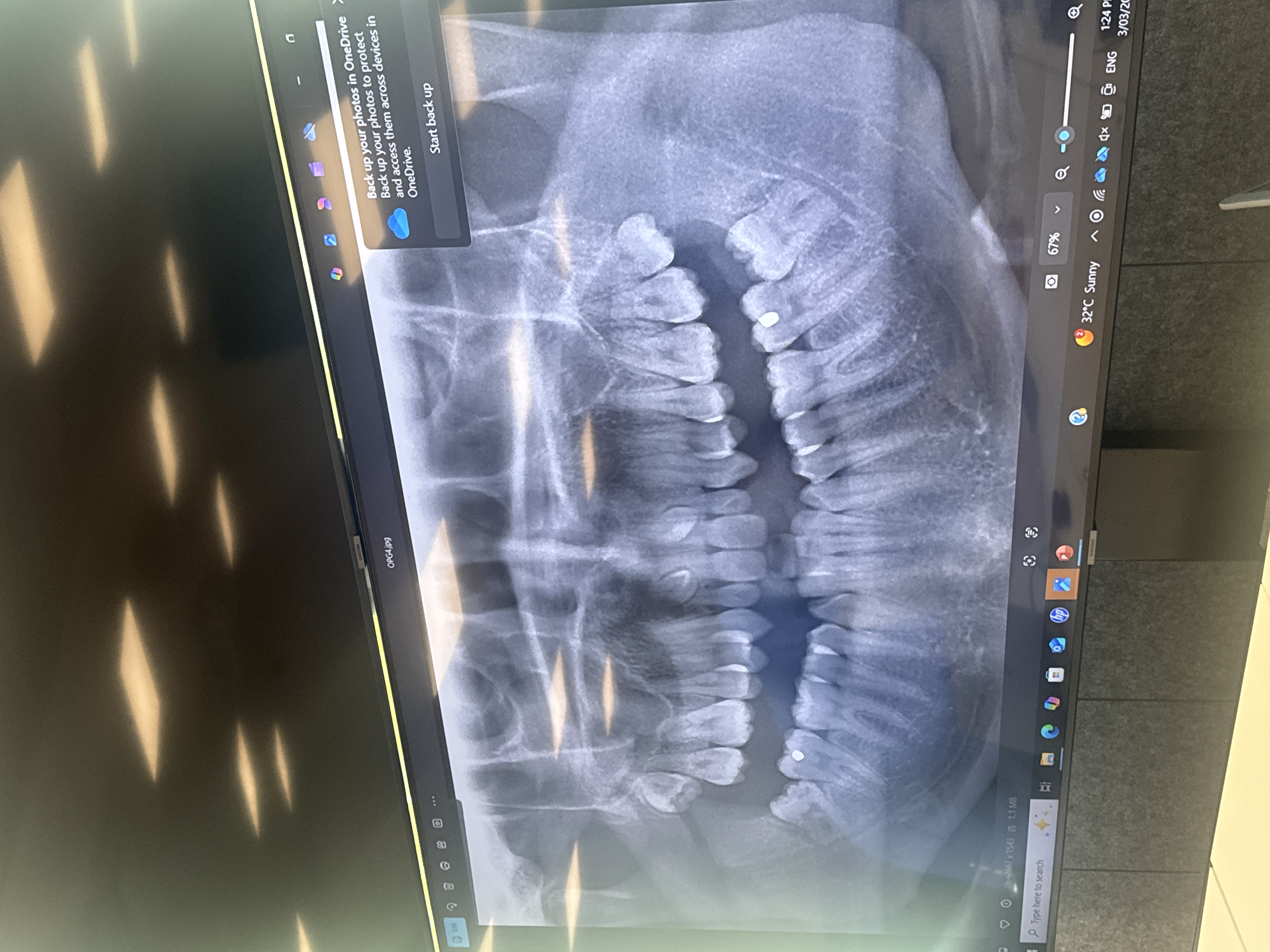
Diagnosis
- supernumerary teeth
Management
- you ned to know if they are buccal or palatal
- to do this you can use the parallel technique (SLOB) or take a cone beam CT
- You also want to use the ct to see if its causing resorption on the 1 or 2
- Patient asks what happens if we live them?
- could potentially turn cystic
- could cause resorption
- Management depends on p/t considerations:
- you won’t really do anything if its an 80 year old, but would consider it in someone younger
case 5

Diagnosis
- Severe bone loss which is not in conjunction with the rest of the mouth (in Q4)
- with the amount of bone loss you would be worried about some sort of resorption
- This turned out to be an ==intra-alveolar cancer
case 6
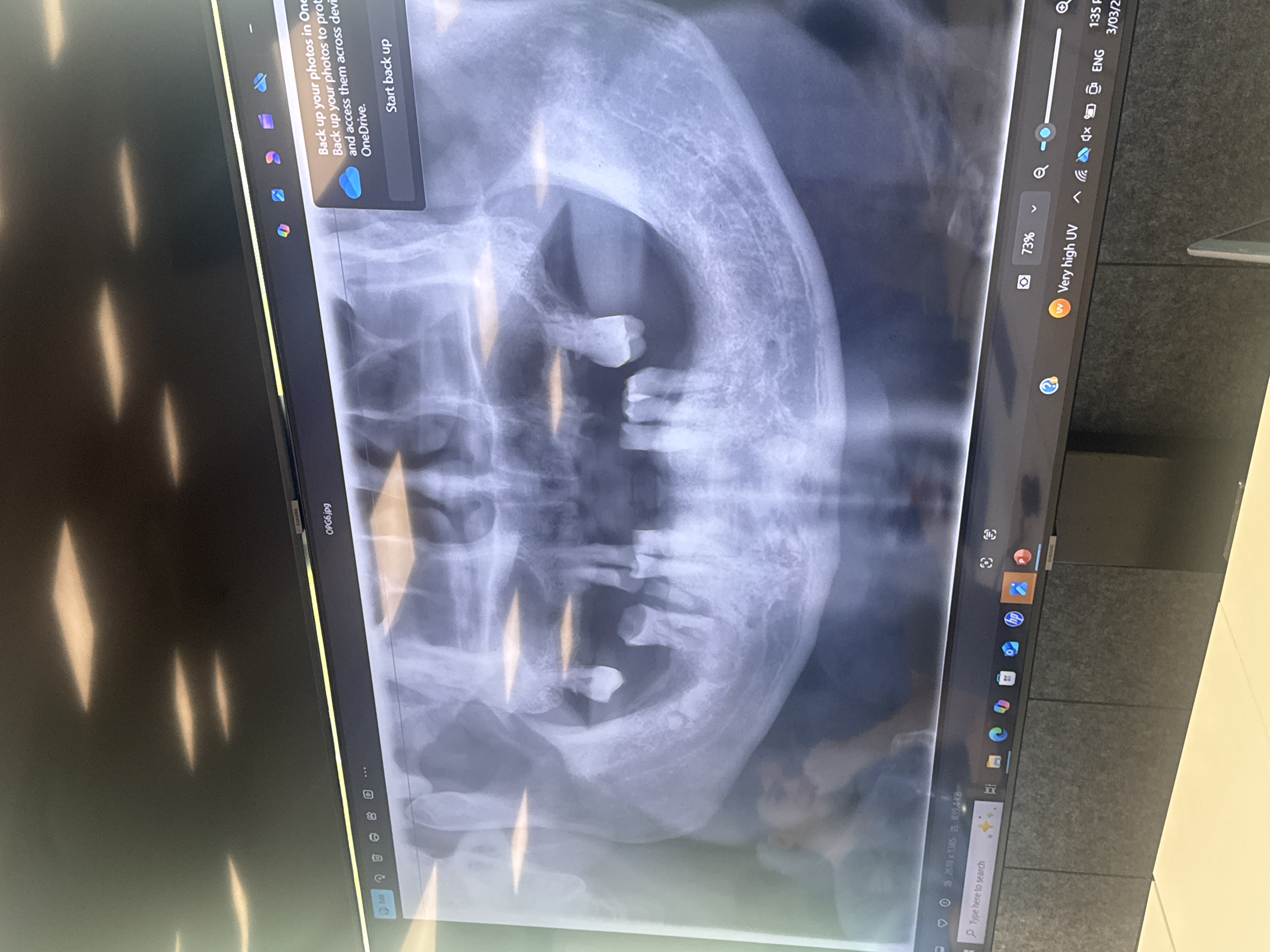
Patient Factors
- Teeth are all vital except for 45
Radiographic analysis
- Opacities in the mandible
Diagnosis
Obtaining diagnosis
- is it serious enough to refer?
- what is the best for the patient ?
- Patient will also ask what happens at / after the referral
- Florid Cemento dysplasia
Case 7

Radiographic analysis
- Radiolucency between 34, 41 periapically
Management
- Vitality testing
- all the teeth turn out to be vital, thus it isnn’t endodontic in origin
- Further imaging
- cone beam ct
- want to know if its perforated the buccal or lingual cortex
- cone beam ct
- Refer the lesion for biopsy
Diagnosis
- Haemorraghic/ traumatic bone cyst
Do you need to do anything for a haemorraghic bone cyst?
NO you don’t need to do anything about it